 Qi Zhao1†
Qi Zhao1† YaoQian Bian2†XinJun Wei3†
YaoQian Bian2†XinJun Wei3† Shuzhen Xiao4Zizhen Xu4,5Hui Li4,5Qingtian Li4,5Beiwen Wei4,5Jiewen Huang4,5Zhen Song4,5*
Shuzhen Xiao4Zizhen Xu4,5Hui Li4,5Qingtian Li4,5Beiwen Wei4,5Jiewen Huang4,5Zhen Song4,5* Yanan Zhao4,5*
Yanan Zhao4,5*- 1Department of Laboratory MedIcine, The Affiliated Yantai Yuhuangding Hospital of Qingdao University, Yantai, China
- 2Department of Laboratory Medicine, Dachang Hospital of Baoshan District of Shanghai, Shanghai, China
- 3Department of Laboratory Medicine, The Eighth People’s Hospital of Qingdao, Qindao, China
- 4Department of Laboratory Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
- 5College of Health Science and Technology, Shanghai Jiao Tong University School of Medicine, Shanghai, China
Introduction: Clostridioides difficile Infection (CDI) is more prevalent in people with hematologic diseases. However, epidemiological characteristics are poorly understood.
Methods: From July 2016 to November 2021, we studied the epidemiology of CDI in patients with hematological diseases at a tertiary teaching hospital in Shanghai, China.
Results: In hematological patients, the prevalence of CDI was 21.6%, with 89.8% hospital-acquired infections. C. difficile ST81, which is a multidrug-resistant strain carrying only the toxin B, is the most common strain (38.1%), followed by ST3 (16.7%) and ST2 (9.5%). Clindamycin and moxifloxacin resistance rates of all C. difficile species were 64.3% and 31%, respectively, and no isolate was resistant to vancomycin, linezolid, metronidazole, teicoplanin, or daptomycin.
Discussion: This study provides a comprehensive characterization of CDI in hematological patients, highlighting the urgent need for enhanced surveillance and preventive strategies against this emerging nosocomial threat.
Introduction
Clostridioides difficile (C. difficile), a Gram-positive, obligate anaerobic bacterium, is recognized as the predominant causative agent of hospital-acquired diarrhea. Following colonization and invasion of the human gastrointestinal tract, this pathogen triggers a wide range of clinical manifestations (Aliramezani et al., 2019). C.difficile infection (CDI) is linked to an asymptomatic carrier state as well as severe illness, including watery diarrhea, abdominal pain and cramps, severe life-threatening fulminant colitis, and even death (Czepiel et al., 2019). Dramatically increased CDI has caused high mortality due to complications and growing economic pressures, which is posing a significant clinical challenge (Wiegand et al., 2012; Banaei et al., 2015; Lessa et al., 2015; Desai et al., 2016).
Furthermore, recurrence of infection, which occurring in up to 30% of patients after the initial episode (Gerding et al., 2015), has become a severe problem. The major virulence factors of C. difficile, toxin A (TcdA) and toxin B (TcdB), are encoded within a pathogenicity locus, which also includes both negative and positive regulators governing their expression (Kuehne et al., 2010). The third binary toxin (CDT) encoded by the cdtA and cdtB genes, on the other hand, is frequently found in C. difficile strains associated with increased CDI severity, such as ribotype (RT)027 and 078 C. difficile isolates (Clements et al., 2010; Persson et al., 2022). Antibiotic exposure, the elderly, weakened immune systems, and hospitalized patients have a higher risk of developing CDI, particularly in patients with inflammatory bowel disease(IBD), organ transplants, and hematological diseases (Riddle and Dubberke, 2008; Gweon et al., 2014; Zhang et al., 2016; Qin et al., 2017; Bushman et al., 2020).
Hematology patients are more easily to develop CDI due to damage of immune system, intensive chemotherapy, and extended exposure to broad-spectrum antibiotics (Gweon et al., 2014). Different research groups have reported higher incidence rates of CDI among hematological patients in comparison to other patient groups. However, previous studies mainly focusing on the risk factors that associated with the development of CDI in hematological patients and the results were often controversial (Gu et al., 2015; Dutta et al., 2021; Hung et al., 2021). In addition, C. difficile species differ in terms of genetic diversity, drug resistance and metabolic capacity. C. difficile RT027 and RT078 can use trehalose to increase infection. The most common IBD-associated lineage (Collins et al., 2018), C. difficile ST54, may use the host’s sorbitol and thus exacerbate clinical manifestations of IBD in vivo (Yang et al., 2023). However, there has been limited research on the genotyping of C.difficile in patients with hematologic diseases.
Therefore, we comprehensively described the epidemiology of CDI in patients with hematological diseases at a tertiary teaching hospital in Shanghai, China, from July 2016 to November 2021. The purpose of this study was to evaluate the characteristics and risk factors, molecular genotypes, antimicrobial resistance patterns to improve our comprehension of CDI in hematological patients.
Materials and methods
Study design and strains collection
The study was conducted in a 1, 400-bed general teaching hospital in Shanghai, China, from July 2016 to November 2021. Patients (≥18 years of age) with diagnosed acute myeloid leukaemia (AML), acute lymphoblastic leukaemia (ALL), chronic lymphocyte leukemia (CLL), chronic myeloid leukemia (CML), Hodgkin’s lymphoma (HL), and non-Hodgkin lymphoma (NHL), multiple myeloma (MM), myelodysplastic syndromes (MDS), hemophagocytic syndrome (HPS), poems syndrome, were included in the analysis. All hematological patients suspected with Clostridioides difficile infection (CDI) (passage of three or more unformed stools in 24 h or loose stools for more than 3 days) were tested for C. difficile. Glutamate dehydrogenase (GDH) assays and toxins A/B (TcdA/B) assays were performed on patient stool specimens using the C. DIFF QUIK CHEK COMPLETE immunochromatographic test kit (Alere, USA). Stools that tested positive for GDH were subsequently inoculated for 48 hours at 37 °C in an anaerobic environment with C. difficile CDIF selective medium (BioMerieux, France). MALDI-TOF MS was used to identify suspect isolates. Community-acquired Clostridioides difficile infection (CA-CDI) was defined as a CDI episode diagnosed within 72 hours of hospital admission in patients with no documented hospitalization in the preceding six months. Hospital-acquired Clostridioides difficile infection (HA-CDI) was defined as CDI diagnosed ≥4 days after hospital admission or CDI diagnosed within the first 72 hours of admission in patients with a documented hospitalization within the preceding six months. The collection of bacterial isolates from patient specimens and the use of related clinical information were reviewed and approved by ethics committee of Ruijin Hospital with the approval number: KY2023-083. No consent was needed for this study. Duplicate specimens from the same patients were excluded.
Multi-locus sequence typing and toxin detection
MLST was performed according to previous publication (Griffiths et al., 2010). The genes Adk, atpA, dxr, glyA, recA, sodA and tpi were amplified by polymerase chain reaction (PCR) and sequenced. Results submitted to the MLST database (http://pubmlst.org/C.difficile) to obtain the allele profile and sequence type (ST). The evolutionary relatedness of different strains was analyzed through the online website PHYLOViZ (https://online.phyloviz.net/index) based on goeBURST algorithm and the VivaGraphJS library. After harvesting, genomic DNA was obtained and tcdA, tcdB, cdtA and cdtB were examined by a multiplex PCR, as previously described (Pituch et al., 2005).
Antimicrobial susceptibility of C. difficile isolates
The minimum inhibitory concentration (MIC) of nine antibiotic, including meropenem, vancomycin, linezolid, metronidazole, moxifloxacin, teicoplanin, rifaximin, daptomycin, clindamycin, was determined by the agar dilution method, according to Clinical and Laboratory Standards Institute (CLSI) guidelines [M11-A8]. ATCC 70057 was used as control. The breakpoints for meropenem, metronidazole, moxifloxacin, clindamycin were based on CLSI recommendations for anaerobes[M100-S35]. The vancomycin resistance breakpoint (MIC >2 mg/L) was defined according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST). The breakpoints for linezolid and rifaximin were based on published literature (Marin et al., 2015; Schwanbeck et al., 2025).
Whole-genome sequencing and analysis
The Gentra Purgene Yeast/Bact. Kit was used to harvest genomic DNA from C. difficile overnight cultures(Qiagen, Germany). The genome sequence of C. difficile was sequenced by Shanghai Majorbio Bio-Pharm Technology Co., Ltd. (Shanghai, China) according to Illumina instructions The SOAPdenove v2.04 tool (with GapCloser v1.12) was used to assemble the readings (http://soap.genomics.org.cn/). The ST81 cluster genomes were constructed and analyzed using CLC Genomics Workbench, with C. difficile M68 (FN668375.1) as a reference.
Statistical analysis
Statistical analyses were performed using software, SPSS Version 27.0 (SPSS, USA). Either the two-tailed unpaired Student’s t-test or the Mann–Whitney U-test was used for comparisons of continuous variables with or without a normal distribution. Chi-square were used to compare categorical variables if differences existed among groups. A P value of less than 0.05 was considered statistically significant.
Results
Prevalence and characteristics of CDI in hematological patients
Between July 2016 and November 2021, 227 diarrheal patients with hematological diseases were sampled in a teaching hospital. As shown in Table 1, the investigation included 53 (23.3%) patients with acute leukaemia, 93 (41.0%) patients with multiple myeloma (MM), 65 (28.6%) patients with non-lymphoma Hodgkin’s (NHL), and 16 (7.0%) patients with other hematological diseases. Among the participants, CDI was diagnosed in 49(21.6%) patients, with a mean age of 56.9 years and 53.1% (n=26) females. The prevalence for HA-CDI was 89.8% (44/49) and 10.2% (5/49) for CA-CDI (Not shown). Recurrence is a huge threat to CDI patients. The prevalence of recurrence was 8.1% (4/49) and ST81 was the causative strain in three of the four recurrence cases. CDI was more common in patients with acute leukemia, but the difference was not statistically significant (32.1% vs 16.1%, 20.0% and 25.0%, p = 0.152). Interestingly, 89.8% of CDI patients presented with at least one co-infectious disease. Furthermore, our analysis revealed that hematologic patients with a prior CDI within one year exhibited a significantly higher infection rate compared to those without prior infection (10.2% vs. 0%, p < 0.001). In addition, haemoglobin levels were lower in CDI patients than in the non-CDI group (74.8 ± 26.2 vs 84.0 ± 23.3, p = 0.020). There was no difference between the CDI+ and CDI- groups in other laboratory parameters such as white blood cell count, neutropenia, platelet count, albumin level, and serum creatinine level.
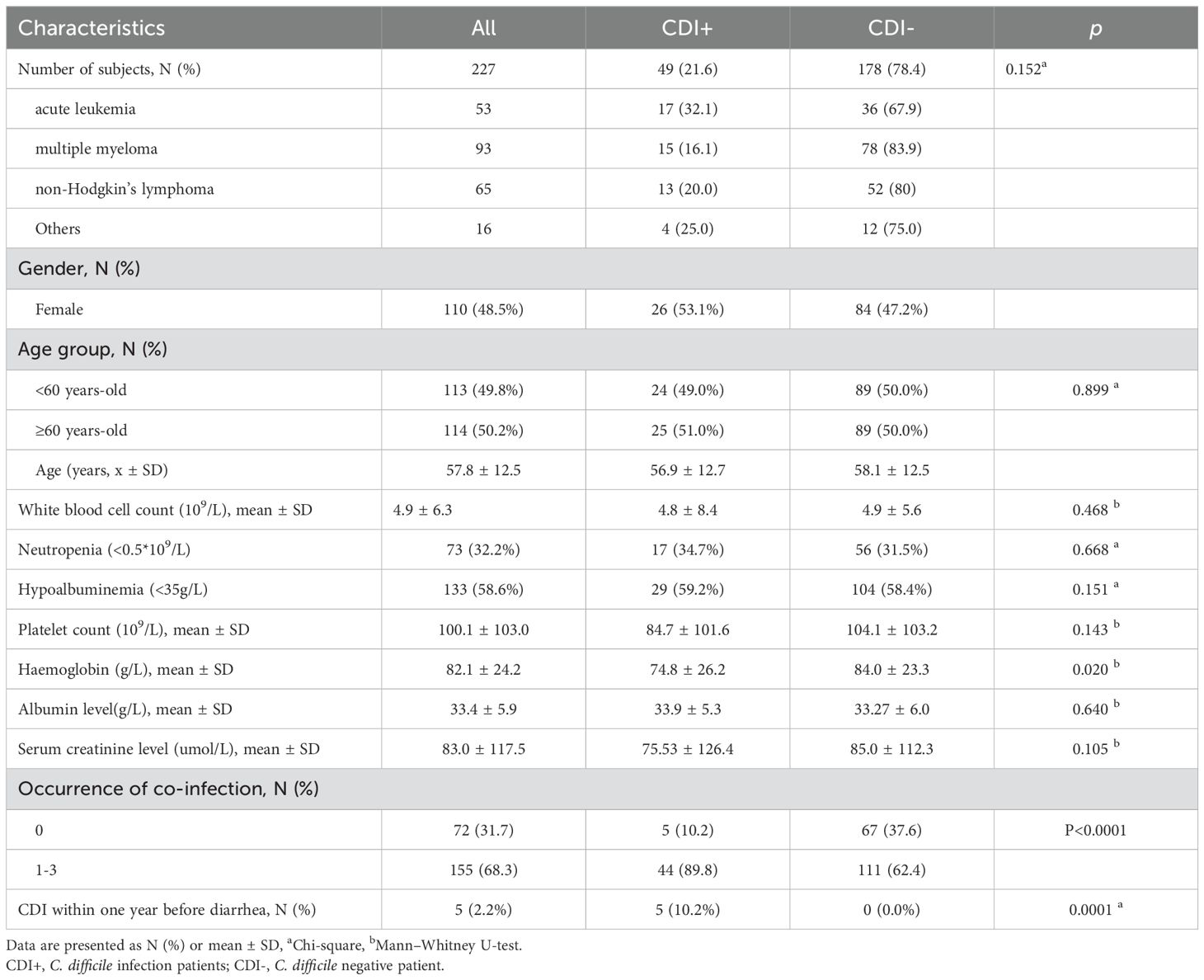
Table 1. Clinical characteristics of C.difficile infection in hematological patients.
Microbiological characters of CDI patients
Of 49 toxin-positive CDI cases, 42 underwent microbial analysis, while seven culture-negative cases were excluded. Since toxin detection confirmed CDI diagnosis, culture failure in these seven cases may reflect prior antibiotic use or non-viable bacteria. As shown in Figure 1A, from 2018 to 2021, the detection rate of C. difficile increased year after year. All isolates were defined into 15 STs, with ST81 (38.1%, 16/42) being the most common clone identified, followed by ST3 (16.7%; 7/42), and ST2 (9.5%; 4/42) as illustrated in Table 2 and Figure 1B. The widely epidemic ST54, has a very low detection rate (n=2) as well as ST37(n=1), being considered as responsible for outbreak in China, Europe, and North America (Luo et al., 2018; Li et al., 2019). The phylogenetic relationships of the 42 isolates were analyzed using an online website based on the ST patterns, as shown in Figure 2. Three major clonal complexes (CCs) were identified, with clade 1 being the most common in this study. ST81, the most common clone, was classified as clade 4 (Table 2).
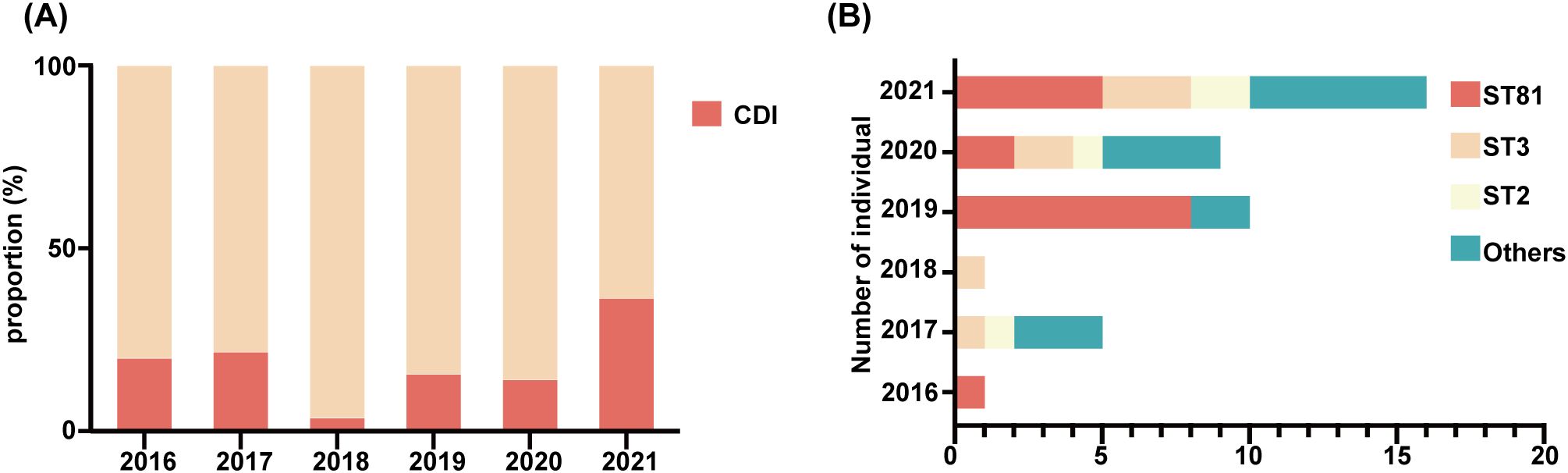
Figure 1. Detection and distribution of C. difficile subtypes from 2016 to 2021. (A) Dynamic changes in proportion of the CDI from 2016 to 2021. (B) Distribution of different genotypes per year, genotypes containing only one isolate were uniformly classified as “Others”.
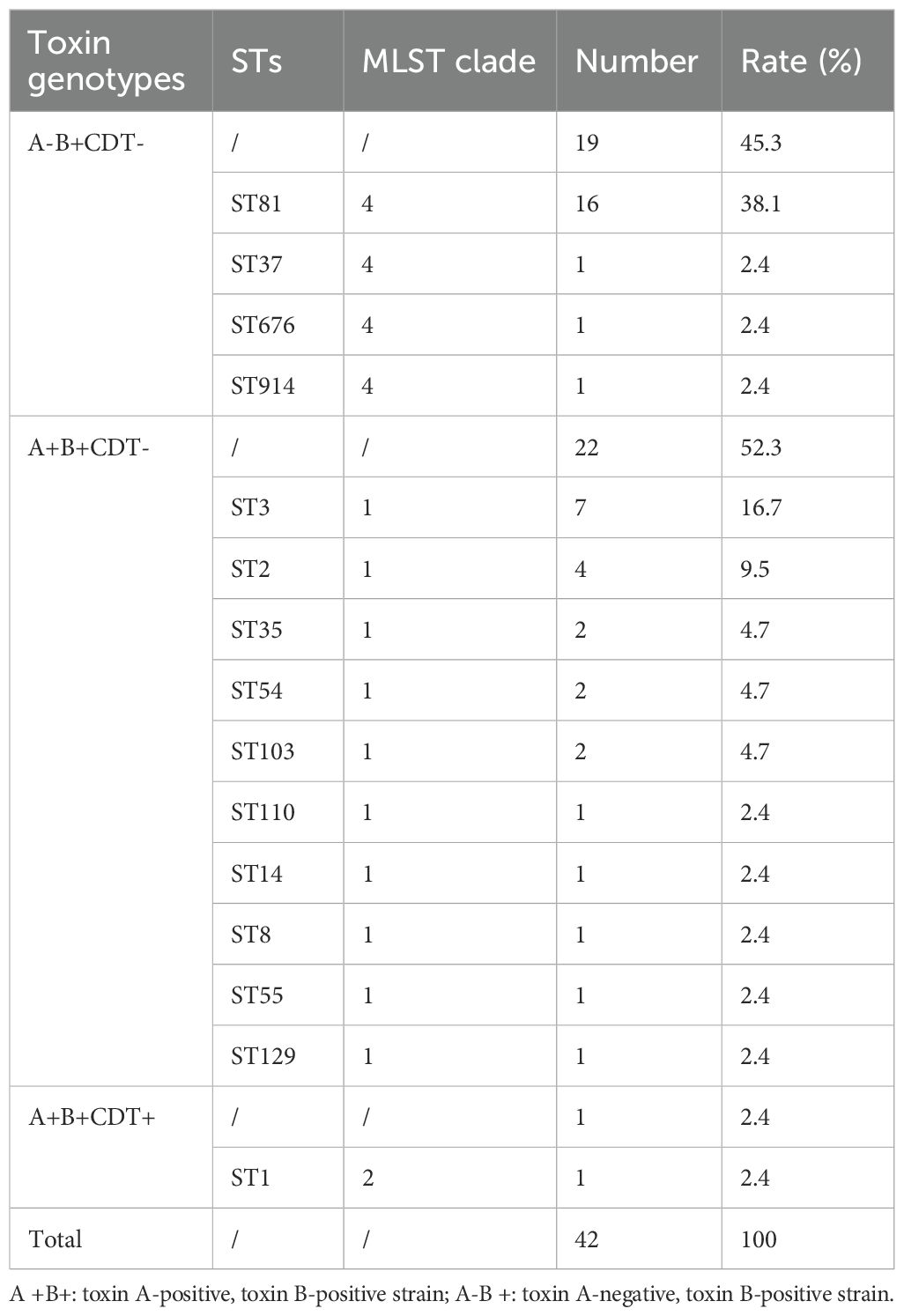
Table 2. Genotypes and toxin of C. difficile isolated from hematological patients.
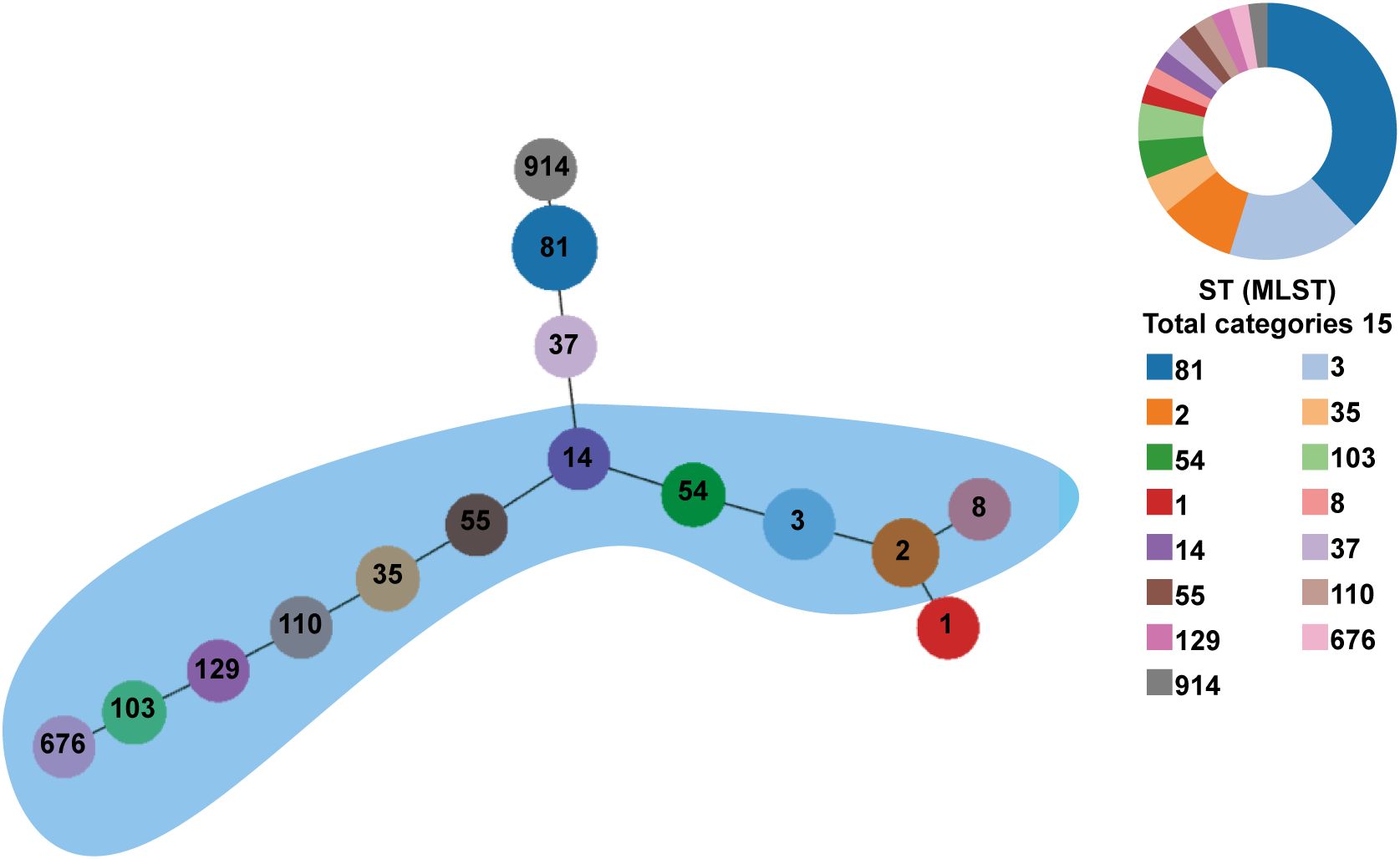
Figure 2. Phylogenetic tree of the C. difficile strains from Hematological Patients. PHYLOVIZ analysis showing the genetic relationship among 42 isolates collect from the hematological patients in this study. MLST was presented in different colors. The node size is proportional to the quantity of isolates. The links represent the relationship between the two STs. Clade 1 is clustered in a blue area.
Four toxin genes (tcdA, tcdB, cdtA, and cdtB) were analyzed in our study. The majority of isolates (52.3%, 22/42) were positive for both tcdA and tcdB genes, while 45.3% (19/42) were negative for tcdA but positive for and tcdB genes. All ST81, the most common strains, carried only the toxin B gene. A ST1 isolate carrying four toxin genes (tcdA, tcdB, cdtA, and cdtB) was identified, representing the only strain in our study capable of producing binary toxin.
Transmission of C.difficile ST81
Interestingly, combining Figures 1A, B, ST81 was revealed to be a contributor of the increase in CDI in 2019 (8/11 isolates), whereas 2021 isolates exhibited greater genetic diversity. Thus, we perform an epidemiological investigation to show spatial and temporal clustering of ST81 cases. Patient 2019-P1 (Bed 25) and 2019-P7 (Bed 03)was housed in two separate rooms from other cases. Furthermore, 2019-P5 and 2019-P8 (Beds 10 and 12, same ward) had a two-month interval between admissions (Figures 3A, B). In contrast, patients 2019-P2, 2019-P3, and 2019-P4 (Beds 17, 13, and 13, respectively) shared the same ward. Notably, 2019-P3 developed CDI following May 2019 hospitalization; one month later, 2019-P4 was admitted to the same bed (Bed 13) and contracted an ST81 strain. Phylogenomic analysis demonstrated that these isolates shared high genetic relatedness (Figure 3B), indicating that they were extremely similar, suggest probable transmission. Although 2019-P6 (Bed 19) was admitted >6 months later after 2019-P2 (Bed 17), since their proximity in adjacent rooms and phylogenetic clustering of the isolates suggest potential environmental persistence or undetected transmission. Collectively, those may indicate that ST81 was spreading in patients with hematologic disease.
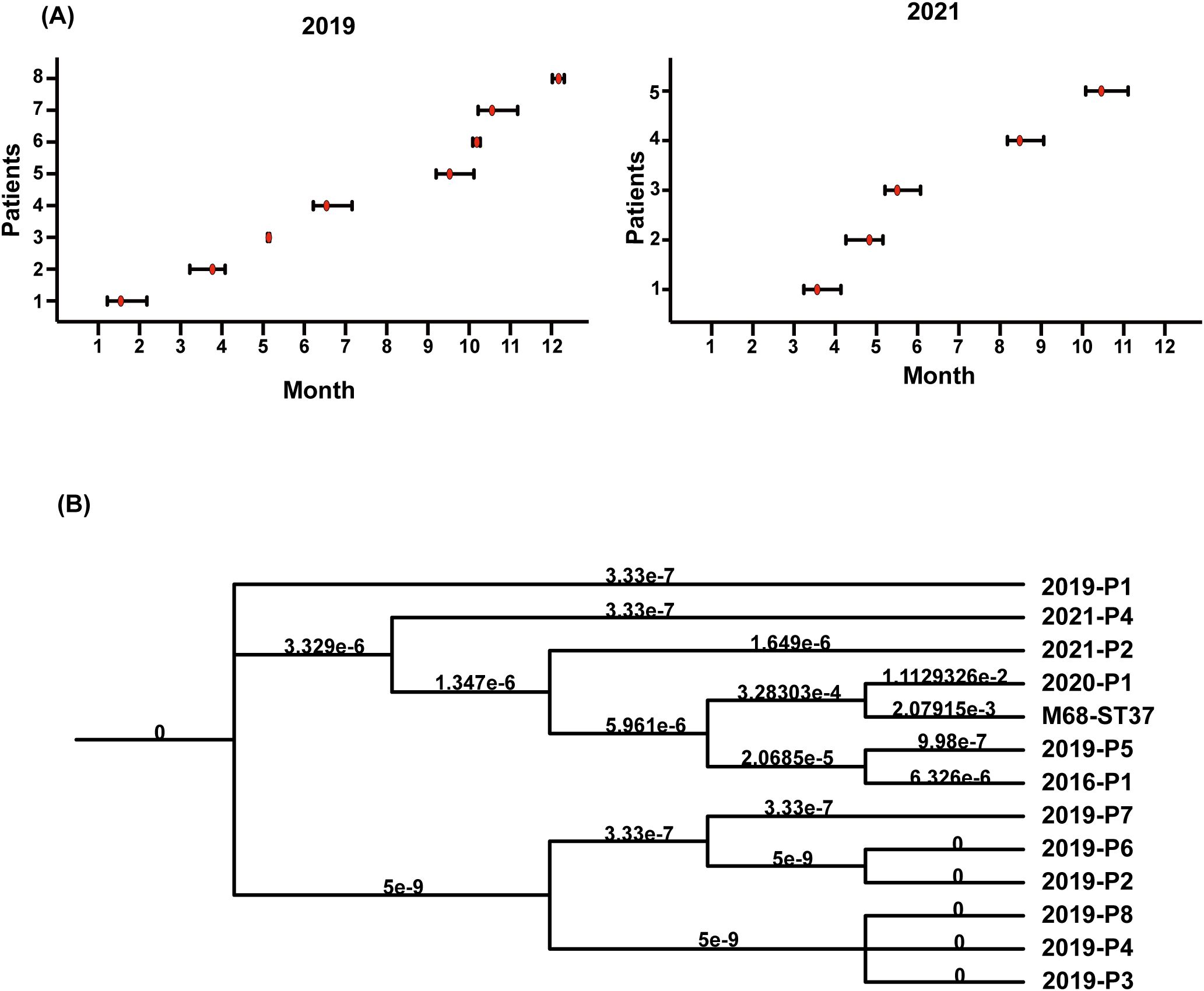
Figure 3. Temporal graph of 13 isolates of ST81 isolated in 2019 and 2021 and ST81 spread in Jan. and June 2019. (A) Temporal graph of 8 ST81 in 2019 and 5 ST81 in 2021. Line segments reflected the length of hospital stays and red dot represented detection time. (B) Analysis of phylogenetic tree within C. difficile genotype ST81. The reference genome was M68-ST37.
Antimicrobial resistance
All C.difficile isolates were evaluated for antimicrobial resistance to nine antibiotics (meropenem, vancomycin, linezolid, metronidazole, moxifloxacin, teicoplanin, rifaximin, daptomycin, and clindamycin). Table 3 shows the antibiotic resistance patterns of all C. difficile strains. 64.3% of the strains were resistant to clindamycin, and high degree of resistance persisted from 2016 to 2021 (MIC≥32 mg/L), with a MIC50 = 32 mg/L and a MIC90 = 128 mg/L (Figure 4A). Resistance to moxifloxacin was 31%, with a decreasing trend (Figure 4B). Meropenem and rifaximin had resistance rates of 9.5% and 7.1%, respectively. No isolate showed positive for resistance to vancomycin, linezolid, metronidazole, teicoplanin, or daptomycin. The dominant strains ST81 were more resistant than non-ST81 strains (p = 0.05). More than half of them had at least two drug resistances, with 31.3% having two and 18.8% having three. ST81 had a much higher rate of resistance to moxifloxacin than the other STs (50% VS 19.2% p = 0.036). No statistically significant differences in resistance rates were observed between ST81 and other STs for meropenem (6.3% VS 2.7%), rifaximin (12.5% vs 0), or clindamycin (75% VS 53.8%) (all p>0.05).
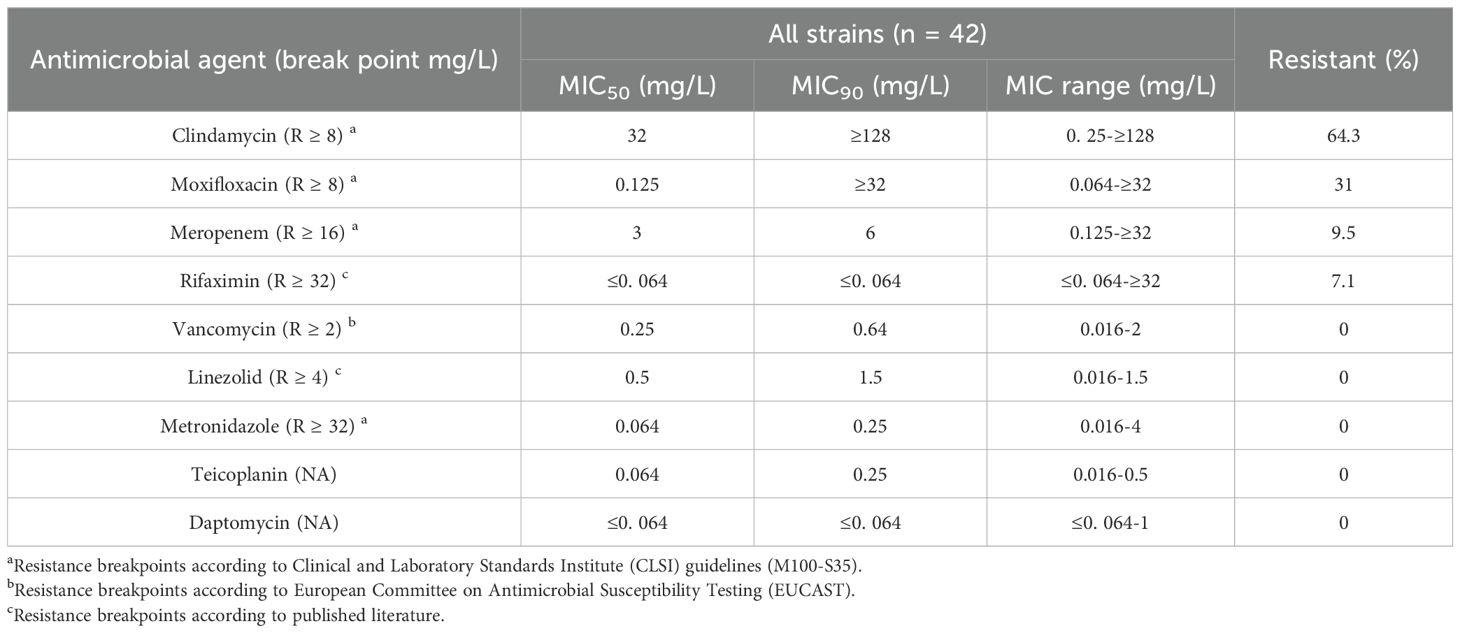
Table 3. Antimicrobial susceptibility profiles of C. difficile isolates (MIC50, MIC90, and MIC range).
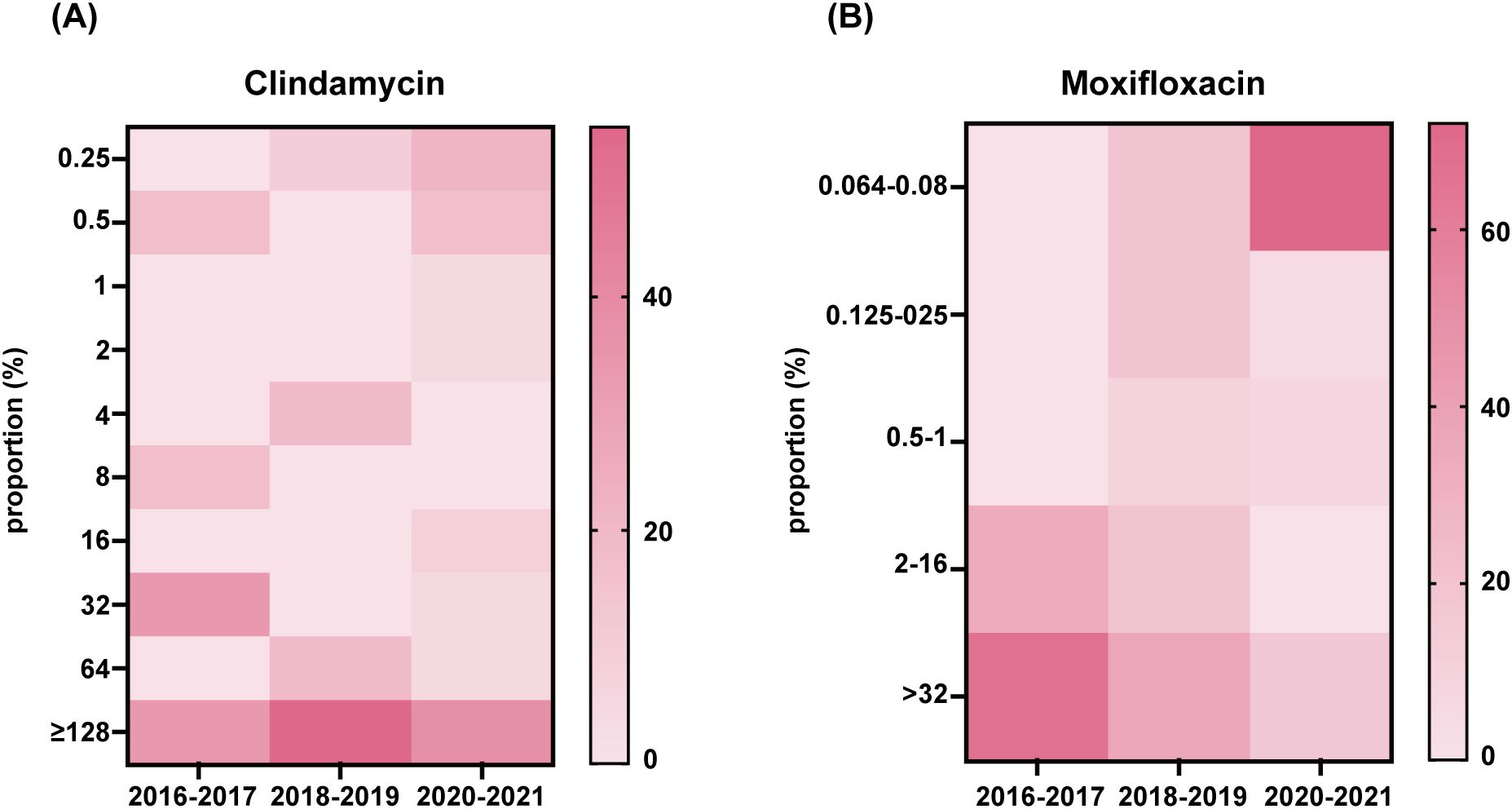
Figure 4. Clindamycin and moxifloxacin MIC distributions in 42 isolates. Distribution of the MIC to antibiotic clindamycin (A) and moxifloxacin (B) of all isolates was presented.
Discussion
Clostridioides difficile Infection (CDI) has been more common in recent years, and it is particularly prevalent in individuals with hematological illnesses, particularly those with hematological malignancies. A meta-analysis of 50 publications from 14 Chinese provinces found that the pooled prevalence of CDI in China was 11.4% (2696/26, 852) (Wen et al., 2023). In contrast, our 6-years study revealed a significantly higher CDI detection rate (21.6%) among patients with hematologic disorders, representing approximately twice the general population. These findings underscore the urgent need for targeted clinical strategies to address CDI management in this high-risk cohort.
According to molecular epidemiology studies C. difficile has distinct characteristics and genotypes in different areas or people. The ST1/RT027 lineage is widespread in Europe and North America, but the RT017 lineage, which includes ST37 and ST81, is abundant in Asia (Clements et al., 2010; Arvand and Bettge-Weller, 2016; Aptekorz et al., 2017; Imwattana et al., 2020). ST54 is more prevalent in people with inflammatory bowel disease (Yang et al., 2023). MLST analysis in our study identified 15 distinct sequence types (STs), with ST81 representing the predominant genotype (38.1%), followed by ST3 (16.7%) and ST2 (9.5%). The predominance of ST81 is consistent with recent epidemiological trends in China that ST81 has replacing the earlier dominance of ST54 and ST37 strains become the predominant circulating genotype (Cheng et al., 2020; Yang et al., 2020; Xia et al., 2024), suggesting that hematologic patients share similar genotype distributions with general populations. ST54, which is commonly epidemic, has an extremely low detection rate, as does ST37. One highly virulent C. difficile ST1/RT027 strain was found in our study. ST81 was not only the most common, but also the most resistant, with 75% demonstrating resistance to at least one antibiotic. Three of the four recurring cases was ST81. In 2019, whole-genome sequencing revealed that ST81 was transmitted in at least two wards. Multi-antibiotic resistance may make it simpler to be screened out and overgrow in the intestinal tract, developing CDI. Furthermore, it has been revealed that ST81 has a greater ability to form spores, which may contribute to its persistence in the external environment, transmission or recurrence among patients (Su et al., 2021). Therefore, ST81 should be of special concern in people suffering from hematological diseases. We strongly advocate for implementing molecular typing-based active surveillance of CDI, with particular emphasis on monitoring the hypervirulent ST81 clone, in hematology units. This approach should be prioritized as a critical strategy for future infection control.
This research has some limitations. For starters, the population is modest. Despite the fact that the trial ran from July 2016 to November 2021, just 227 patients were included. Second, bias is unavoidable in retrospective studies, and causality cannot be clearly deduced.
Data availability statement
The sequencing data reported in this study have been deposited in the NCBI Sequence Read Archive (SRA) under BioProject accession PRJNA1370298.
Ethics statement
The studies involving humans were approved by ethics committee of Ruijin Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
QZ: Conceptualization, Investigation, Writing – review & editing. YB: Writing – review & editing, Investigation. XW: Investigation, Writing – review & editing. SX: Data curation, Writing – review & editing. ZX: Writing – review & editing, Validation. HL: Writing – review & editing, Methodology. QL: Writing – review & editing. BW: Writing – review & editing. JH: Writing – review & editing. ZS: Writing – original draft, Resources, Methodology. YZ: Writing – original draft, Funding acquisition, Conceptualization, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the National Natural Science Foundation of China, grant number 82302538.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aliramezani, A., Talebi, M., Golbabaei, F., Baghani, A., Marjani, M., Afhami, S., et al. (2019). Characterization of Clostridioides difficile isolates recovered from hospitalized patients and the hospitals environment and air: A multicenter study. Anaerobe 59, 154–158. doi: 10.1016/j.anaerobe.2019.06.012
Aptekorz, M., Szczegielniak, A., Wiechuła, B., Harmanus, C., Kuijper, E., and Martirosian, G. (2017). Occurrence of Clostridium difficile ribotype 027 in hospitals of Silesia, Poland. Anaerobe 45, 106–113. doi: 10.1016/j.anaerobe.2017.02.002
Arvand, M. and Bettge-Weller, G. (2016). Clostridium difficile ribotype 027 is not evenly distributed in Hesse, Germany. Anaerobe 40, 1–4. doi: 10.1016/j.anaerobe.2016.04.006
Banaei, N., Anikst, V., and Schroeder, L. F. (2015). Burden of Clostridium difficile infection in the United States. N Engl. J. Med. 372, 2368–2369. doi: 10.1056/NEJMc1505190
Bushman, F. D., Conrad, M., Ren, Y., Zhao, C., Gu, C., Petucci, C., et al. (2020). Multi-omic analysis of the interaction between clostridioides difficile infection and pediatric inflammatory bowel disease. Cell Host Microbe 28, 422–433.e427. doi: 10.1016/j.chom.2020.07.020
Cheng, J. W., Liu, C., Kudinha, T., Xiao, M., Fan, X., Yang, C. X., et al. (2020). The tcdA-negative and tcdB-positive Clostridium difficile ST81 clone exhibits a high level of resistance to fluoroquinolones: a multi-centre study in Beijing, China. Int. J. Antimicrob. Agents 56, 105981. doi: 10.1016/j.ijantimicag.2020.105981
Clements, A. C., Magalhães, R. J., Tatem, A. J., Paterson, D. L., and Riley, T. V. (2010). Clostridium difficile PCR ribotype 027: assessing the risks of further worldwide spread. Lancet Infect. Dis. 10, 395–404. doi: 10.1016/s1473-3099(10)70080-3
Collins, J., Robinson, C., Danhof, H., Knetsch, C. W., van Leeuwen, H. C., Lawley, T. D., et al. (2018). Dietary trehalose enhances virulence of epidemic Clostridium difficile. Nature 553, 291–294. doi: 10.1038/nature25178
Czepiel, J., Drozdz, M., Pituch, H., Kuijper, E. J., Perucki, W., Mielimonka, A., et al. (2019). Clostridium difficile infection: review. Eur. J. Clin. Microbiol. Infect. Dis. 38, 1211–1221. doi: 10.1007/s10096-019-03539-6
Desai, K., Gupta, S. B., Dubberke, E. R., Prabhu, V. S., Browne, C., and Mast, T. C. (2016). Epidemiological and economic burden of Clostridium difficile in the United States: estimates from a modeling approach. BMC Infect. Dis. 16, 303. doi: 10.1186/s12879-016-1610-3
Dutta, D., Jafri, F., Stuhr, D., Knoll, B. M., and Lim, S. H. (2021). A contemporary review of Clostridioides difficile infections in patients with haematologic diseases. J. Intern. Med. 289, 293–308. doi: 10.1111/joim.13173
Gerding, D. N., Meyer, T., Lee, C., Cohen, S. H., Murthy, U. K., Poirier, A., et al. (2015). Administration of spores of nontoxigenic Clostridium difficile strain M3 for prevention of recurrent C. difficile infection: a randomized clinical trial. Jama 313, 1719–1727. doi: 10.1001/jama.2015.3725
Griffiths, D., Fawley, W., Kachrimanidou, M., Bowden, R., Crook, D. W., Fung, R., et al. (2010). Multilocus sequence typing of Clostridium difficile. J. Clin. Microbiol. 48, 770–778. doi: 10.1128/JCM.01796-09
Gu, S. L., Chen, Y. B., Lv, T., Zhang, X. W., Wei, Z. Q., Shen, P., et al. (2015). Risk factors, outcomes and epidemiology associated with Clostridium difficile infection in patients with haematological Malignancies in a tertiary care hospital in China. J. Med. Microbiol. 64, 209–216. doi: 10.1099/jmm.0.000028
Gweon, T. G., Choi, M. G., Baeg, M. K., Lim, C. H., Park, J. M., Lee, I. S., et al. (2014). Hematologic diseases: high risk of Clostridium difficile associated diarrhea. World J. Gastroenterol. 20, 6602–6607. doi: 10.3748/wjg.v20.i21.6602
Hung, Y. P., Tsai, C. S., Tsai, B. Y., Tsai, P. J., Lee, Y. T., Lee, J. C., et al. (2021). Clostridioides difficile infection in patients with hematological Malignancy: A multicenter study in Taiwan. J. Microbiol. Immunol. Infect. 54, 1101–1110. doi: 10.1016/j.jmii.2021.02.002
Imwattana, K., Knight, D. R., Kullin, B., Collins, D. A., Putsathit, P., Kiratisin, P., et al. (2020). Antimicrobial resistance in Clostridium difficile ribotype 017. Expert Rev. Anti Infect. Ther. 18, 17–25. doi: 10.1080/14787210.2020.1701436
Kuehne, S. A., Cartman, S. T., Heap, J. T., Kelly, M. L., Cockayne, A., and Minton, N. P. (2010). The role of toxin A and toxin B in Clostridium difficile infection. Nature 467, 711–713. doi: 10.1038/nature09397
Lessa, F. C., Mu, Y., Bamberg, W. M., Beldavs, Z. G., Dumyati, G. K., Dunn, J. R., et al. (2015). Burden of Clostridium difficile infection in the United States. N Engl. J. Med. 372, 825–834. doi: 10.1056/NEJMoa1408913
Li, H., Li, W. G., Zhang, W. Z., Yu, S. B., Liu, Z. J., Zhang, X., et al. (2019). Antibiotic resistance of clinical isolates of Clostridioides difficile in China and its association with geographical regions and patient age. Anaerobe 60, 102094. doi: 10.1016/j.anaerobe.2019.102094
Luo, Y., Zhang, W., Cheng, J. W., Xiao, M., Sun, G. R., Guo, C. J., et al. (2018). Molecular epidemiology of Clostridium difficile in two tertiary care hospitals in Shandong Province, China. Infect. Drug Resist. 11, 489–500. doi: 10.2147/idr.S152724
Marin, M., Martin, A., Alcala, L., Cercenado, E., Iglesias, C., Reigadas, E., et al. (2015). Clostridium difficile isolates with high linezolid MICs harbor the multiresistance gene cfr. Antimicrob. Agents Chemother. 59, 586–589. doi: 10.1128/AAC.04082-14
Persson, S., Nielsen, H. L., Coia, J. E., Engberg, J., Olesen, B. S., Engsbro, A. L., et al. (2022). Sentinel surveillance and epidemiology of Clostridioides difficile in Denmark 2016 to 2019. Euro Surveill 27, 2200244. doi: 10.2807/1560-7917.Es.2022.27.49.2200244
Pituch, H., Kreft, D., Obuch-Woszczatynski, P., Wultanska, D., Meisel-Mikolajczyk, F., Luczak, M., et al. (2005). Clonal spread of a Clostridium difficile strain with a complete set of toxin A, toxin B, and binary toxin genes among Polish patients with Clostridium difficile-associated diarrhea. J. Clin. Microbiol. 43, 472–475. doi: 10.1128/JCM.43.1.472-475.2005
Qin, J., Dai, Y., Ma, X., Wang, Y., Gao, Q., Lu, H., et al. (2017). Nosocomial transmission of Clostridium difficile Genotype ST81 in a General Teaching Hospital in China traced by whole genome sequencing. Sci. Rep. 7, 9627. doi: 10.1038/s41598-017-09878-8
Riddle, D. J. and Dubberke, E. R. (2008). Clostridium difficile infection in solid organ transplant recipients. Curr. Opin. Organ Transplant. 13, 592–600. doi: 10.1097/MOT.0b013e3283186b51
Schwanbeck, J., Laukien, F., Riedel, T., Bunk, B., Halama, P., Sproer, C., et al. (2025). Rifaximin resistance in Clostridioides difficile is associated with specific rpoB alleles and multilocus sequence typing (MLST) clades. BMC Microbiol. 25, 458. doi: 10.1186/s12866-025-04164-4
Su, T., Chen, W., Wang, D., Cui, Y., Ni, Q., Jiang, C., et al. (2021). Complete genome sequencing and comparative phenotypic analysis reveal the discrepancy between clostridioides difficile ST81 and ST37 isolates. Front. Microbiol. 12. doi: 10.3389/fmicb.2021.776892
Wen, B. J., Dong, N., Ouyang, Z. R., Qin, P., Yang, J., Wang, W. G., et al. (2023). Prevalence and molecular characterization of Clostridioides difficile infection in China over the past 5 years: a systematic review and meta-analysis. Int. J. Infect. Dis. 130, 86–93. doi: 10.1016/j.ijid.2023.03.009
Wiegand, P. N., Nathwani, D., Wilcox, M. H., Stephens, J., Shelbaya, A., and Haider, S. (2012). Clinical and economic burden of Clostridium difficile infection in Europe: a systematic review of healthcare-facility-acquired infection. J. Hosp Infect. 81, 1–14. doi: 10.1016/j.jhin.2012.02.004
Xia, X., Lv, T., Zheng, L., Zhao, Y., Shen, P., Zhu, D., et al. (2024). Genomic epidemiology of clostridioides difficile ST81 in multiple hospitals in China. Infect. Drug Resist. 17, 5535–5544. doi: 10.2147/IDR.S492668
Yang, Z., Huang, Q., Qin, J., Zhang, X., Jian, Y., Lv, H., et al. (2020). Molecular epidemiology and risk factors of clostridium difficile ST81 infection in a teaching hospital in eastern China. Front. Cell Infect. Microbiol. 10, 578098. doi: 10.3389/fcimb.2020.578098
Yang, Z., Qin, J., Zhao, L., Chen, T., Huang, Q., Jian, Y., et al. (2023). Host sorbitol and bacterial sorbitol utilization promote C. difficile infection in inflammatory bowel disease. Gastroenterology. 164, 1189–1201. doi: 10.1053/j.gastro.2023.02.046
Keywords: Clostridioides difficile, hematologic diseases, genotyping, epidemiology, drug resistance
Citation: Zhao Q, Bian Y, Wei X, Xiao S, Xu Z, Li H, Li Q, Wei B, Huang J, Song Z and Zhao Y (2025) Multi-drug resistant Clostridioides difficile isolate ST81 is prominent in hematological patients in a teaching hospital in China. Front. Cell. Infect. Microbiol. 15:1668584. doi: 10.3389/fcimb.2025.1668584
Received: 18 July 2025; Accepted: 17 November 2025; Revised: 24 October 2025;
Published: 08 December 2025.
Edited by:
Yuetian Yu, Shanghai Jiao Tong University, ChinaReviewed by:
Xiujuan Meng, Affiliated Hospital of Jining Medical University, ChinaLiliana Fernández Canigia, Hospital Alemán, Argentina
Copyright © 2025 Zhao, Bian, Wei, Xiao, Xu, Li, Li, Wei, Huang, Song and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yanan Zhao, eW56aGFvQHNoc211LmVkdS5jbg==; Zhen Song, c3o0MDU5N0ByamguY29tLmNu
†These authors have contributed equally to this work