 Mamta Saxena
Mamta Saxena Dorothy J. Shedlock
Dorothy J. Shedlock- Department of Human Development, SUNY at Oswego, Oswego, NY, United States
Background: Family scientists strongly purport that structured family routines are associated with family stability and identity and may mediate the individuals' positive developmental outcomes. Family routines enhance the predictability of ambiguous situations, promote members' cohesion, and provide security and warmth. Investigating adverse changes in family routines during COVID-19 can inform on support required by families from other larger systemic institutions.
Theoretical background: Historically, family routines have universally been a gendered realm, and the contributions of females have been salient in maintaining them. Established and gendered contributions pre-COVID-19 predicted who does what and how much in the household. After the spread of COVID-19, the gendered practice continued and, in many households, strengthened. Therefore, exploration of proximal processes in the microsystem, such as family routines through the Bioecological perspectives, may offer insights into the historical rationale and repercussions of the gendered division of household labor on individual family members, especially women, and in times of crisis, such as a pandemic.
Purpose and method: The health implications of COVID-19 led to restrictive mandates, including remote employment and education directives resulting in additional stress and uncertainty in carrying out daily routines. Thus, there is a need to explore whether restrictive mandates during COVID-19 changed specific family routines and gender outcomes. In the current study, we surveyed (online) 378 adult participants about changes (disruptions) in their family routines, perceptions of disruptions in routines, and perceived stress levels. The research questions are:
(1) Does participants' gender continue to determine specific family routines?
(2) What are participants' perceptions of disruptions in family routines, and do those responses to family routines differ significantly by participants' gender?
(3) Are there significant gender differences in perceptions of stress among participants?
Findings and conclusions: Data analyses indicated that during COVID-19, both males and females were equally affected by changes in routines and had similar perceptions of disruptions and high-stress levels. However, item-level analyses indicate that females significantly spent more time on chores that would benefit others, whereas male participants spent more time on routines that would benefit them. Both males and females reported high-stress levels but differed in symptomatology. We provide a few selected narratives to supplement gender-based quantitative findings and establish descriptive evidence for differences in disruptions in routines and stress. In the end, implications for future practice and research are discussed.
Introduction
With 226,236,577 global confirmed cases and 4,654,548 deaths (WHO, 2021a), COVID-19 affected everyone regardless of race, gender, age, and nationality. In the US alone, there have been 41,229,421 confirmed cases of COVID-19, with 659,336 deaths (WHO, 2021b). Although WHO and national organizations reported the impact primarily on physical health and loss of lives, the adverse effects of mandates associated with COVID-19 spilled into every realm of family routines, including maintenance of physical and mental health, employment, schooling, travel, finances, and more.
In the current study, we adapted Fiese et al.'s (2002) and Spagnola and Fiese's (2007) concepts of family rituals and routines to define family routines. Family routines are defined as specific customary or non-customary tasks that family members must complete periodically and consistently to maintain family stability and identity and ensure positive developmental outcomes. Additionally, these tasks can be personal, i.e., for the benefit of self, such as activities of daily living, playing video games, or for the benefit of others, such as cooking family meals, supervising children's educational activities, or caregiving for the elderly.
The perceptions of stress are defined as “a negative affective state, ranging from unhappiness and discontent to an extreme feeling of sadness, pessimism, and despondency that interferes with daily life. Various physical, cognitive, and social changes also co-occur, including altered eating or sleeping habits, lack of energy or motivation, difficulty concentrating or making decisions, and withdrawal from social activities” (APA, 2022).
Gender differences in family routines and theoretical frameworks
Researchers (Masten and Motti-Stefanidi, 2020) called COVID-19 a multisystem disaster because of its widespread repercussions on every aspect of human life. To explore the role of gender in predicting specific family routines and associated stress, we will apply bioecological perspectives in the current article. The bioecological perspective sheds light on the impact of the multidimensional nature of COVID-19 mandates (macro) on transactional/proximal processes in families (micro) as determined by routines and stress. Therefore, rather than utilizing any single factor, such as the roles of hormones on mental health outcomes, reciprocal interactions between biological and sociocultural factors will lead to a more nuanced understanding of behavioral and mental health outcomes which may further escalate or moderate the gendered family routines and mental health outcomes.
Additionally, bioecological perspectives illuminate historical underpinnings and delineate the issue's complexity, contemporary family dynamics and processes, intergenerational transmission of beliefs and values, and intervention points.
Bioecological perspectives
According to the Bioecological framework (Bronfenbrenner and Morris, 2006), an individual's behaviors and development are influenced by reciprocal interactions between the person in the center of various systems: micro, meso, exo, macro, and chrono. Changes or conflicts in any one system ripple throughout other systems. Reciprocal interactions that occur within and between systems are called processes. Individuals are influenced indirectly by distal processes (events in the macrosystem/chronosytem) and directly by proximal processes within the elements of the microsystem, such as family.
The microsystem is the first layer closest to an individual and encompasses his/her relationships and interactions with immediate surroundings such as family, school, neighborhood, or childcare and may include gender roles within the family, expectations of being a breadwinner influencing academic performance, and more. The mesosystem (second layer) consists of connections between more than one element of the microsystem, for example, between school and family or family and neighborhood. The exosystem is the third layer comprises the more extensive social system, including places such as parents' work schedules, employment status, and health care. Exosystem relates explicitly to the intergenerational transmission of gender outcomes. For example, children who have never experienced employed mothers or grandmothers are more likely to attribute paid employment to their parent's gender. The fourth layer macrosystem consists of cultural values, customs, and laws at a national/state level. The absence of federally mandated paid maternity leave may discourage new mothers from working outside the home.
Finally, the chronosystem is the outermost layer and refers to social, historical, and age-specific changes over some time that can be considered milestones or turning points in history. For the current article, integrating sociological perspectives in the chronosystem rationalizes that traditionally females shared the bulk of households for three reasons. First, they have greater time availability as many females were part-time employed or unemployed. Second, females have lower relative resources because they either do not earn or earn less than their partners. Money offered special privileges to males; therefore, women had little say in delegating household tasks. Third, women have internalized the gender ideology (AKA internalized sexism). Therefore, it is no surprise that they enact traditional roles, prefer conforming to gender roles, and socialize their daughters to do the same even when men in the family may not impose or oppose them (Hiller, 1984).
To illustrate, part-time or unemployed females take on a more significant chunk of family responsibilities as they have more time to complete these tasks. In contrast, for similar reasons, individuals (generally males) with more resources such as money, power, and education could deflect household responsibilities and consider them demeaning. Gradually, traditional patterns were maintained and strengthened, promoting the internalization of gender ideology that further dictated societal norms of masculine and feminine activities at home (Hiller, 1984; Bearman and Amrhein, 2014).
Bioecological perspectives and COVID-19
The government-mandated restrictions and safety measures during the spread of COVID-19 (distal processes in macrosytem) indirectly disrupted the normative proximal processes such as family routines (microsystem). These changed routines directly influenced individuals, challenging their ability to adapt and cope. For example, employed parents of young children had to identify how to care for their children (who were earlier in daycares and schools) while simultaneously completing their remote employment responsibilities (Cantillon et al., 2021). Similarly, individuals with elderly parents had to establish new routines for regular communication and celebration of special events such as birthdays and anniversaries, previously managed with face-to-face meetings and travel. Many families could not personally interact during sickness, childbirth, and death which led to enormous changes in family routines and renegotiation of proximal processes (family routines) (Usher et al., 2020; Tsibidaki, 2021). Additionally, distal processes (mandates) led to economic recession, loss of employment, travel and social distancing restrictions, remote work and education, and social isolation (Usher et al., 2020; Walsh, 2020). In sum, proximal and distal processes exacerbated stress and unpredictability in daily life, precluding the use of typical and established family routines that could help soothe the family and maintain family equilibrium.
Importance of family routines and their gendered nature
It seems well-established that family routines preserve family cohesion and connectedness, especially during uncertain times. Routines establish predictability, order, a sense of normality, and a positive emotional climate in the face of chaos. Thus, sustaining normality can be a powerful way to cope with and navigate adverse situations' challenges (Koome et al., 2012). Additionally, maintaining a sense of normality and structured routines is crucial because individuals feel a higher sense of personal agency and continuity when their environment is consistent and less chaotic. For example, firm and consistent routines in low-income families promoted positive behaviors (Lanza and Taylor, 2010) such as higher self-regulation, lower impulsivity (Brody and Flor, 1997), and higher academic performance because of consistent parent-child involvement and monitoring of academic activities (Budescu and Taylor, 2013).
Additionally, consistency in exercise, healthy food habits, and sleep moderated (lowered) the symptoms of chronic illnesses and physical health (Peterson-Sweeney, 2009; Anderson and Whitaker, 2010; Fritz, 2014). Furthermore, consistent routines may extend opportunities for developing family identity, a sense of belongingness, bonding among members, and a shared sense of responsibility (Koome et al., 2012). It is no surprise that during COVID-19, upholding daily routines from the past while maintaining family connections and work-life balance signaled warmth, security, and safety within relationships and helped to maintain positive family functioning (Killgore et al., 2020).
Despite their significant role in positive developmental outcomes, family routines implicate a gendered nature of family routines. During the pandemic, women bore the indirect effects of COVID-19 and its variants because of “structural dysfunction” historically affecting women (Connor et al., 2020; p. 1). Power (2020) clarified structural dysfunction, noting that women's burdens and participation in the care economy substantially rose during COVID-19, which bolstered traditionally sanctioned gender-regressive practices and gender-based inequalities at home. Employed mothers spent the same amount of time (not less) on childcare as unemployed fathers, and when unemployed, women spent twice the number of hours on childcare than their employed spouses/partners. Employed women also experienced frequent interruptions during the completion of employment responsibilities and inequitable household responsibilities, including caregiving (Andrew et al., 2020).
During COVID, working women participated more in unpaid and less attractive household obligations such as cooking, cleaning, caring for elders and children, schooling children, planning routines and schedules, and maintaining communication with family (Andrew et al., 2020; Power, 2020). Women completing household responsibilities after employment hours is not new and is popularly known as the second shift (Bianchi et al., 2000; Cohen, 2004). However, strengthening or reverting to traditional obligations can be considered unwelcome after longstanding efforts and emphasis on gender equality and women empowerment.
Gender differences and perceptions of stress
In large part, the female gender is associated with greater vulnerability to stress and depression worldwide, with females being twice more likely to report depression than males (Weissman and Klerman, 1977). Female vulnerability to depression exists even after accounting for diagnostic and reporting bias. Several propositions ranging from biological to environmental factors and their intersectionality have been offered to explain the predominance of depression and anxiety among females. Some factors that have been extensively explored include the roles of hormones, neurodevelopmental changes, gender inequality, violence, poverty, and other contextual variables (Salk et al., 2017).
Salk et al. (2017) conducted a meta-analysis of 158 articles and noted that gender differences in the etiology and symptomatology of stress and depressive symptoms peak around 16 years due to biological factors. However, gender differences begin to narrow after early adulthood if societies follow gender-equitable practices. Alternatively, higher rates of depression among females continue in adulthood, stemming from biological changes during childbearing years as well as contextual factors, including marital and employment status or intimate partner violence (Gutiérrez-Lobos et al., 2000; Chandan et al., 2020).
Higher stress and depression among female respondents remained worldwide during COVID-19. [For more details, see Xiong et al. (2020); who included several European and Asian countries and the US; Hou et al. (2020), Pappa et al. (2020) for the Chinese sample; Sønderskov et al. (2020) for the Danish sample and García-Fernández et al. (2021) for Spanish sample]. Various reasons for higher depression rates among females include higher unemployment or reduced employment hours (Pew Research Center, 2020), inequities with the division of chores at the home front (Heggeness, 2020), a surge in intimate partner violence (Usher et al., 2020) and susceptibility to social isolation (García-Fernández et al., 2021). Indeed, evidence suggests that during COVID-19, even though mortality was higher among males, emotional stress was higher among females because women were left to deal with the crises (Spagnolo et al., 2020).
Comparisons of long-term and short-term data indicated higher rates of stress among women initially. The significant gender gap in depression and anxiety narrowed after a few weeks into the spread of COVID-19, and women reported lower stress levels (Fenollar-Cortés et al., 2021). The authors argued that perhaps women adapted sooner and developed more emotion regulation strategies than men. Thus, faster recovery in females may be associated with their attitudes and behaviors. Worldwide, females were more disciplined than men in following government mandates and taking necessary precautions (Galasso et al., 2020; Barber and Kim, 2021). Fenollar-Cortés et al. speculated that women's behavior changes were more driven by higher functional fear that fostered compliance and quick adaptation to crises. Functional fear is adaptive in out-of-control situations as it lowers stress, offers protection, and prepares an individual for impending danger.
Correspondingly, we also know that gender intersects with other variables such as genetic predisposition, age, education level, employment, and race. For example, younger unemployed females with a predisposition to psychiatric illnesses were more likely to be depressed during COVID-19 (Xiong et al., 2020) and female healthcare providers reported more stress than male providers (Pappa et al., 2020).
In summary, it is justifiable to state that the health complications of COVID-19 led to restrictive mandates, including remote employment and education mandates. In turn, that drove additional stress and uncertainty in carrying out daily routines for all individuals. Global evidence further suggested that traditional gender roles were reinforced during COVID-19 restrictions, and females were likelier to engage in family routines. Existing cross-sectional evidence suggests that females reported higher levels of depression and stress during COVID-19 than males. However, it remains unclear what specific family routines women engaged in and how they perceived disruptions. Similarly, the role of men in family routines deserves exploration because many experienced reduced hours or unemployment for an extended period. Therefore, did they experience different symptoms of stress than women can be examined? We did not find any study investigating men's role in maintaining family routines.
Therefore, the research questions of the study are:
(4) Does participants' gender continue to determine specific family routines?
(5) What are participants' perceptions of disruptions in family routines, and do those responses to family routines differ significantly by participants' gender?
(6) Are there significant gender differences in perceptions of stress among participants?
Method
Participants and recruitment
Following the Institutional Review Board approval, 378 participants were recruited across the United States. Eligible participants were adult and English-speaking US residents because surveys were unavailable in other languages. Undergraduate research methods students facilitated participant recruitment and data collection by sharing Qualtrics online survey links on their social media sites and emailing their contacts.
Qualtrics is an online survey tool with several enhanced features to maintain participant anonymity and confidentiality. No identifiers, including IP addresses, names, and addresses, were collected, and SPSS 27, a data analysis software, was used to analyze the data. Participants were not compensated for their time; on average, they completed the survey in 12–15 minutes.
Measures of the study
The original survey consisted of seven sections, but the current study involves only descriptive and inferential findings from four sections, i.e., demographics, changes in family routines, perceptions of disruptions in family routines, perceptions of stress, and two qualitative questions stated earlier. The quantitative sections and their details are as follows.
Section #1 Demographics consisted of six items to collect information about participants' age, gender, education level, income, marital status, and state of residence.
Section #2 Family Routines Scale*(CR) is a 5-point scale comprising 22 items (ranging from significantly lower than before to significantly higher than before). The measure ascertains how COVID-19 influenced time expenditures in family routines, such as cooking and traveling. Total scores on the scale could range from 22 to 110, with higher scores indicating more time spent by the family members on activities since COVID-19. The Cronbach's alpha for the sample was 0.70.
Some items from the scale are:
“With the spread of COVID-19, estimate the daily change in the average time you spend on cooking?”
“With the spread of COVID-19, estimate the daily change in the average time you spend playing video games?”
Section #3 Disruptions in the Family Routines Scale*(PCR) is a 5-point scale comprising 18 items (ranging from much worse to much better) to assess participants' perceptions of the disruptions in routine activities such as communication with family members or household chores. Total scores could range from 18 to 95, with lower scores indicating higher negative perceptions of the disruptions in routines. The Cronbach's alpha for the sample was 0.68.
Some items from the scale are:
“With the spread of COVID-19, what are your perceptions of the qualitative changes in the involvement of all family members in household chores?”
“With the spread of COVID-19, what are your perceptions of the qualitative changes in terms of fights among family members?”
“With the spread of COVID-19, what are your perceptions of the qualitative changes in terms of your family's participation in home improvement tasks such as painting, home décor, gardening, or more?”
Section #4 Perceptions of Stress (PSS) used a 5-point scale consisting of ten items (ranging from never to very often). The scale measured the degree to which life situations are appraised as stressful (Cohen et al., 1983). Total scores could range from 0 to 40 (very-low health concern, 0–7; low health concern, 8–11; average health concern, 12–15; high health concern, 16–20; very-high health concern, 21+). The scale has high reliability (Cronbach's Alpha = 0.84) and validity; it has been translated into several languages (Taylor, 2015). The Cronbach's alpha for the sample was 0.73.
Some items from the scale are given below.
“In the last month, how often have you been upset because something happened unexpectedly?”
“In the last month, how often have you felt confident about your ability to handle your problems?”
“In the last month, how often have you been able to control irritations in your life?”
Please note, in the absence of appropriate scales, Changes in Family Routines and Disruptions in the Family Routines were created explicitly for the current study, and some items in the scales are adapted from the Family Routines Inventory (Jensen et al., 1983). The scales Family Routines and Disruptions in the Family Routines were also used in data analysis of other published articles (see Saxena, 2021).
Findings and discussion
Little's MCAR test indicated that data were not missing at random, so three expectation-maximization imputations (EM) were conducted. After analyzing descriptives, gender differences in terms of time spent on specific family routines, perceptions of disruptions in family routines, and perceptions of stress were analyzed by conducting one-way ANOVAs with Bonferroni corrections. ANOVAs with Bonferroni correction for post hoc analyses are beneficial in group comparisons of categorical (IV) and continuous variables (DV) and avoid a type I error (Armstrong, 2014).
Overall, out of the 378 participants, most were younger (M = 32, SD = 13.6), their ages ranged between 18 and 84 years, and they resided across the US. Almost three-fourths of the participants were females; almost half were single, and their median education level was a Bachelor's degree. The mean score on Changes in Daily Routines was M = 70.85 (SD = 8.4), indicating that participants significantly spent more time on family routines after the spread of COVID-19. Likewise, the mean score on Perceptions of Stress was M = 31.5 (SD = 6.1), indicating very high health concerns among the participants.
RQ1 During COVID-19, did the participant's gender continue to determine specific family routines?
Data analyses indicated no significant gender differences in total scores of changes in daily routines: both men and women equally experienced changes in routine. One-way ANOVAs with Bonferroni corrections and analyses of individual items indicated that the gendered division of chores continued and strengthened during COVID-19 (see Table 1). Even though both men and women experienced changes, they spent their daily hours on different activities. For example, women engaged more in household chores (Mfvs.m= 2.56 vs. 2.48) and educational activities with children other than schoolwork (Mfvs.m = 2.18 vs. 1.99) than men. In comparison, men engaged in playing video games (Mfvs.m = 2.31 vs. 2.59) and pursuing hobbies or spending time alone (Mfvs.m = 2.14 vs. 2.42) (for others, see Table 1).
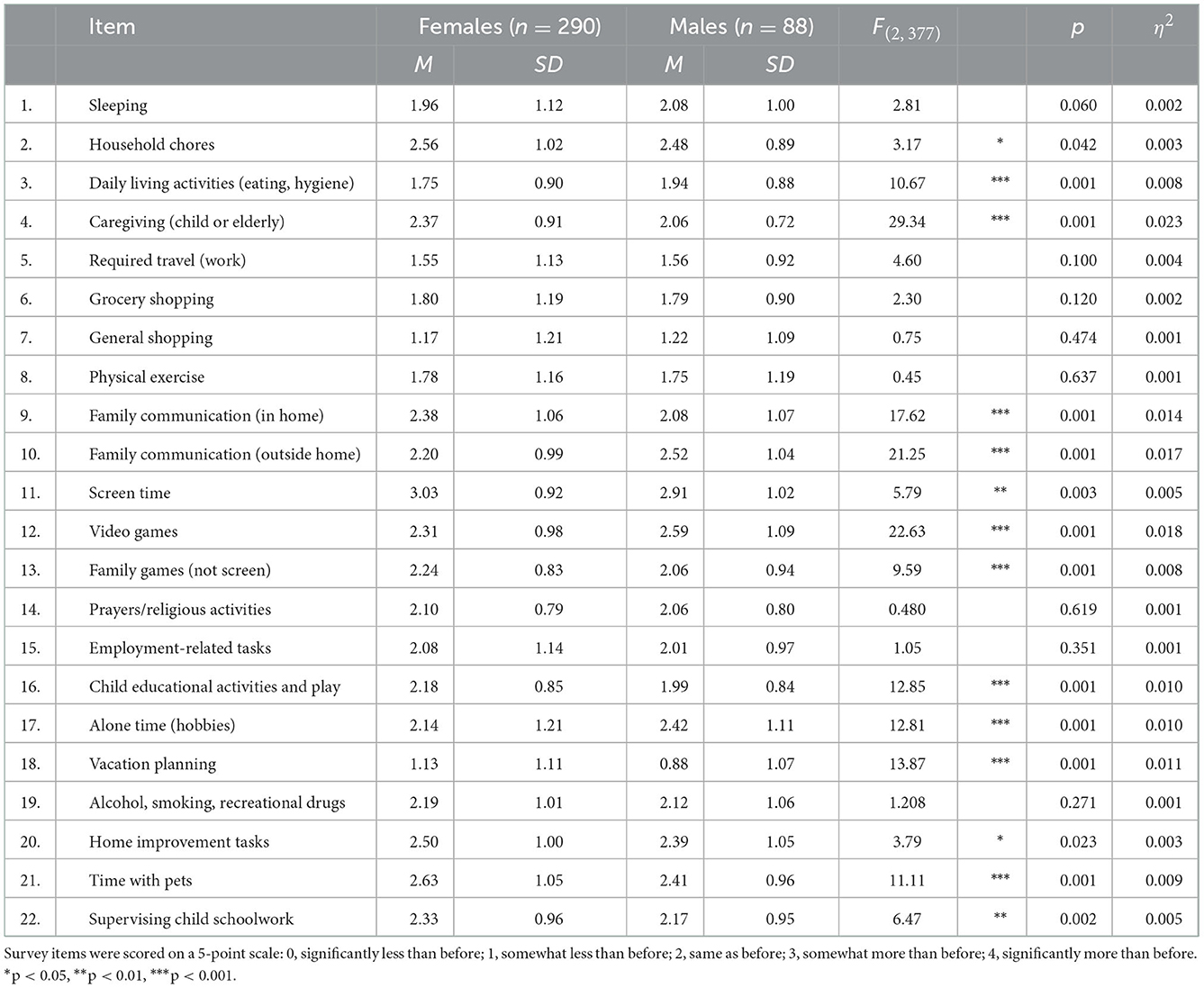
Table 1. Gender differences in daily time spent on family routines before and during COVID-19.
The above findings provide a nuanced understanding of family processes and who does what in a household. They concur with Andrew et al. (2020) that women spend more time in childcare, homework, and household chores in the UK. The authors further noted that even when males were more involved in childcare, they were more vested in passive activities, such as watching TV with children, than active activities, such as helping children with homework.
RQ2 Are there significant gender-based differences in perceptions of disruptions in specific family routines before and after the spread of COVID-19?
Similar to time spent on family routines, there were no significant gender differences in individuals' global reactions to perceptions of changes. However, since the findings of RQ1 suggested that during COVID-19, males and females spent significantly more time on different activities, we initiated analyses of gender differences in specific items of the scale (see Table 2).
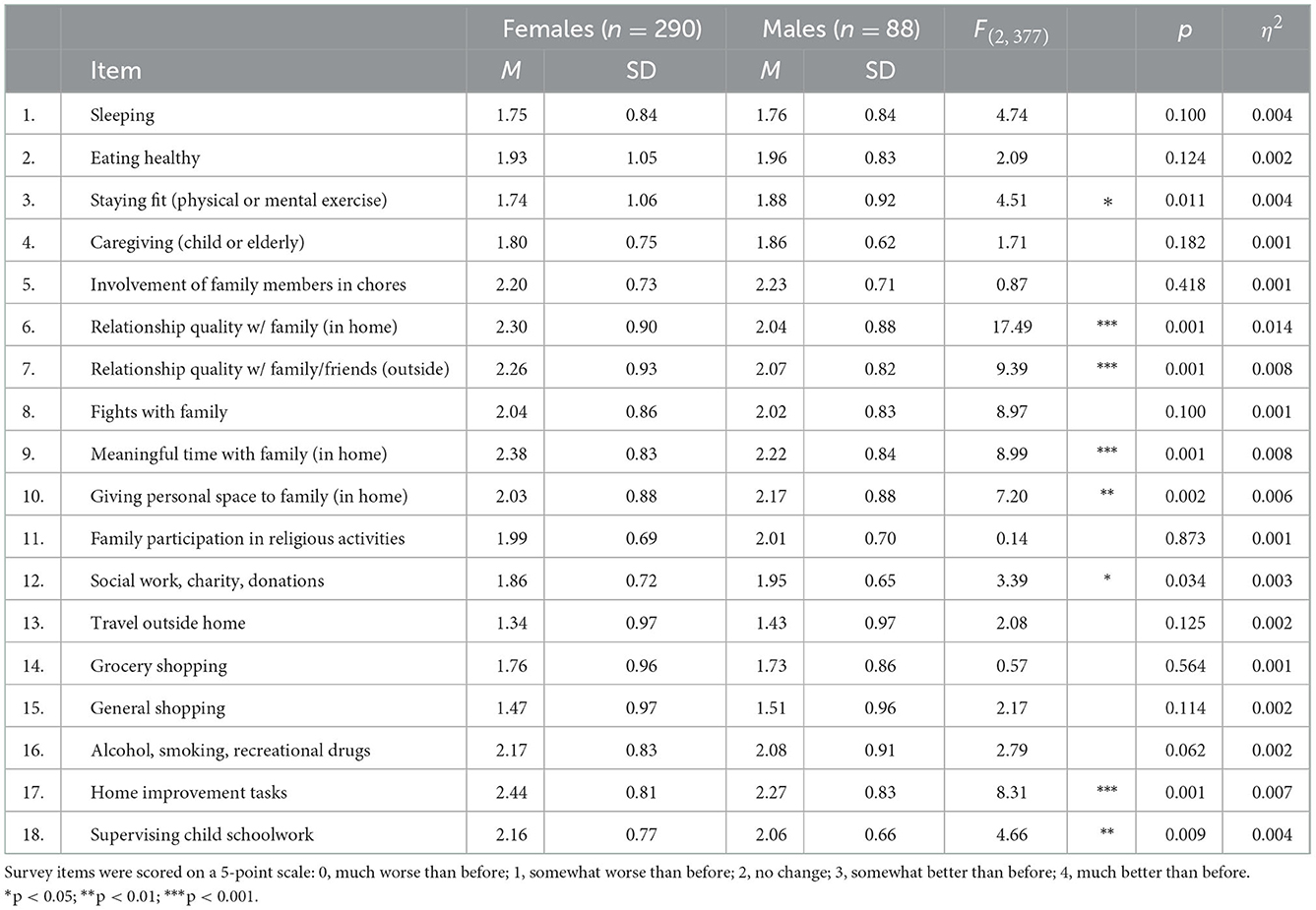
Table 2. Gender differences in perceived quality of family routines before and during COVID-19.
Interestingly, males and females had more positive perceptions about the area they spent significantly more time in despite the disruptions imposed by COVID-19. For example, more males than females significantly reported positive perceptions about staying fit (Mmvs.f = 1.88 vs. 1.74) and allowing personal space to other family members (Mmvs.f = 2.17 vs. 2.03). In comparison, significantly more females than men reported improvements in the quality of relationships with immediate (Mfvs.m = 2.3 vs. 2.04) and children's educational activities (Mfvs.m = 2.16 vs. 2.06) (see Table 2 for more comparisons).
Although we did not find empirical research on perceptions of routine changes, both males and females adapted to the change and settled positively without complaints in traditional male and female-oriented tasks despite the availability of time (working from home) and fewer resources (reduced hours or unemployment). Given the evidence, we assume that women are uncomfortable with breaking gender roles and expectations and whether the concept of internalized sexism overrode the ideas of gender equality or whether women did not want to contribute to more chaos needs to be further investigated in later research.
RQ3 Are there significant gender differences in perceptions of stress among participants?
Once again, similar to RQ1 and RQ2, there were no significant gender differences in the total stress levels, and both males and females experienced very high-stress levels (see Table 3).
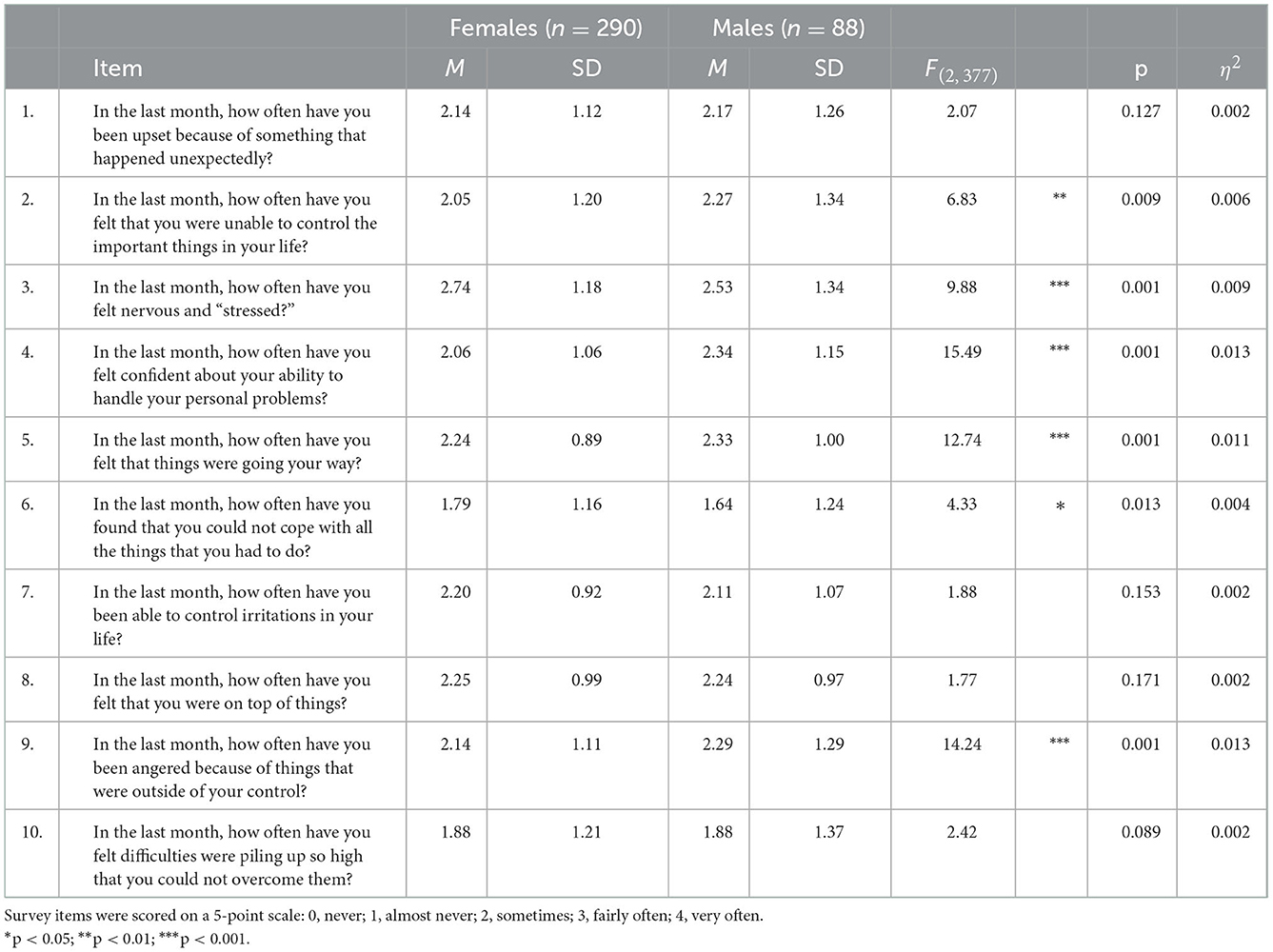
Table 3. Gender differences in perceived stress in the last month during COVID-19.
The one-way ANOVAs with Bonferroni corrections suggested gender differences in perceptions of some stress scale items. The items on which more males than females reported significantly feeling stressed are losing control over their situation (Mmvs.f = 2.27 vs. 2.05) and being angry (Mmvs.f = 2.29 vs. 2.14). Interestingly, males felt significantly more confident handling the situation (Mmvs.f = 2.34 vs. 2.06) and were more optimistic about their current situation (Mmvs.f = 2.33 vs. 2.24) than females (see Table 3).
In terms of total stress levels, the current findings on perceived stress diverge somewhat from existing evidence that found significant differences between the stress levels of men and women (Hou et al., 2020; Pappa et al., 2020; Sønderskov et al., 2020; Xiong et al., 2020). The lack of gender difference in current findings may be because current data were collected in Oct- Nov 2020, i.e., almost 6 months into the spread of COVID-19. The concept of functional fear and related adaptation (Fenollar-Cortés et al., 2021) implies that females actively engaged in emotional regulation and successfully closed the gender gap in stress. Chronic functional fear can also set an individual on a negative mental health path (Harper et al., 2020). Thus, it is crucial to understand the gender differences in patterns and trajectories of stress symptoms and not just global stress levels. For example, we noted that females were not significantly higher on any of the positive items than men, which may indicate their underlying fears and hopelessness with the situation, despite the adaptation.
The current empirical evidence suggests that females spent more time cooking, caregiving, and other feminine activities and extended themselves to masculine tasks such as renovations and home improvements. In contrast, males spent more time pursuing personal hobbies and interests (see Tables 1, 2). Despite significant time spent on masculine and feminine family routines, female participants did not perceive the disruptions negatively and reported more positives than men.
Gender differences in perceptions of stress, as noted in Table 3, included that males reported significantly more anger, whereas females reported more nervousness and anxiety. Females reported feeling more disheartened by difficulties in maintaining relationships and reported more crying and feeling mournful because of the deaths of family and friends. Males had stronger reactions to financial struggles, challenged mandates and safety restrictions, and reported frequent frustrations and anger over the lack of support from the government.
Conclusions and implications
The current preliminary exploration of gender differences in changes in family routines, perceptions of changes, and stress indicate that COVID-19 equally impacted men and women. Although there are no significant gender-based disparities in total scores, findings indicate disparities in specific family routines, perceptions of disruptions, and their sources of stress. We found that family routines were divided mainly along traditional lines, and women focused on the responsibility to benefit others. Although remote employment offered opportunities for men to shoulder some of these responsibilities and ally with their partners, in the current sample, we did not find that men shouldered these responsibilities equally. Thus, the data suggest that the spread of COVID-19 magnified gender asymmetries in their homes and may place women at risk of adverse mental health outcomes.
The Bioecological perspectives lend a more profound and broader lens to the psychological and behavioral outcomes of males and females during the spread of COVID-19. The frameworks and findings allude to looking beyond the obvious and integrating contextual variables (that are multidimensional and multidisciplinary) in family interventions to promote healthy development. Additionally, and consonant with earlier work, current findings indirectly suggest that positive proximal processes (i.e., equity in household chores and caregiving) in the microsystem can lower socio-contextual risks in the face of adversity (Conger and Conger, 2002) and may cultivate resilience (Masten and Motti-Stefanidi, 2020; Saxena, 2022).
Applying theoretical frameworks to data analysis further underscores several potential messages.
First, males and females are equally vulnerable to stress and will benefit from inclusive and individualized counseling and other intervention programs to recover. Nevertheless, the intervention programs need to recognize the gender differences in stress behaviors and trajectory and develop programs that account for these differences. Significantly, more women than men reported overtasking themselves with activities for others, feeling less optimistic, and compensating for men in several areas of family routines without reporting negative reactions. We urge caution in concluding that women were content in their homes taking care of others because they successfully adapted and positively perceived changes in routines and mandates. Researchers have established that the cumulative effects of lack of self-care and high-stress levels resulting in compassion fatigue (Lynch et al., 2018) can be devastating for anyone and may influence women more because they are constantly involved in activities to benefit others. Without personal activities and time for respite, compensation in family routines may place them on the trajectory of chronic physical and mental health issues. Therefore, future studies should explore whether women's reported positive perceptions and practices of prioritizing others resulted in compassion fatigue or is sustainable in the long run. Without redistribution, this can foster more gender-regressive practices in our society. After all, gender equity in household chores (Power, 2020) and family routines has been consistently linked with positive outcomes.
Second, the current study findings indicate gender differences in negative emotional reactions, i.e., males are angrier than females, and females are more nervous than males. Despite the exploratory nature of the current study and modest sample size, our findings concur with several researchers on the issue. The gender differences in emotional responses are not surprising, and many public health officials, researchers, and social workers raised concerns regarding the upsurge in domestic violence during COVID-19 restrictions, especially for women and children (Knaul et al., 2020). The study suggests distal and proximal sources of anger, frustrations, and anxiety that can be part of intervention plans. In the future, it is also worth investigating if emotional responses pose a potential risk for domestic violence and abuse in families, for if they do, prevention programs and intervention programs are urgently needed.
Third, gender inequalities at home shape women's decisions about their careers, education, and progress in those specific realms. Many women enroll in degree programs that potentially lead to employment with flexible hours and successfully juggle between home and career. At the time of crisis on the home front, it appears that women either reduced their work hours or became full-time homemakers, not by consent but under the psychological pressure of gendered norms, thereby feeding into gender disparities at a societal level (Roig Berenguer et al., 2022).
Fourth, longitudinal research and lifespan perspectives are needed to understand the complex intersections of gender in family routines and mental health over time. We need to examine family and ecological factors and unravel their complex nature and consequences on mental health outcomes.
Finally, women's contributions are central to stable families, and women shoulder the bulk of the care economy worldwide is one of the established truisms. Therefore, recognizing, appreciating, and supporting women through community programs and interventions and fostering equal support and validation from men and women can go a long way to combat sexism. Programs can incorporate components such as progressive gender roles to reduce internalized sexism, stress, and conflict. Furthermore, interventions to encourage male family members to acknowledge their responsibilities and alliances in family routines may help all family members better address difficulties.
Limitations
The current study is exploratory and needs further confirmation from other similar research. It utilizes a cross-sectional design, so causality cannot be inferred. Additionally, the survey was available only in English and online; most respondents held Bachelor's degrees. Findings may have coverage bias and do not represent the US population. We also recognize that the sample size is moderate and may not represent accurate incidence rates. Nonetheless, our findings highlight some of the issues that families encountered and suggest new questions and a broader approach to the research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by SUNY OSWEGO IRB. The patients/participants provided their written informed consent to participate in this study.
Author contributions
MS led the following: conceptualization of the study, research design and survey development, data collection, interpretation of findings, as well as writing, revising, and editing the manuscript. DS assisted with the survey development and made revisions to the manuscript. ZG assisted with data analysis. All authors contributed to the article and approved the submitted version.
Acknowledgments
We would like to thank Dr. Randall Stetson, Visiting Assistant Professor in the Department of Human Development at SUNY Oswego. Dr. Stetson contributed extensively to the survey items for the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Anderson, S. E., and Whitaker, R. C. (2010). Household routines and obesity in US preschool-aged children. Pediatrics 125, 420–428. doi: 10.1542/peds.2009-0417
Andrew, A., Cattan, S., Costa Dias, M., Farquharson, C., Kraftman, L., Krutikova, S., et al. (2020). The Gendered Division of Paid and Domestic Work under Lockdown, IZA Discussion Papers, No. 13500. Bonn: Institute of Labor Economics (IZA).
APA (2022). APA Dictionary of Psychology. Retrieved from: https://dictionary.apa.org/stress (accessed November 14, 2022).
Armstrong, R. A. (2014). When to use the Bonferroni correction. Ophthal. Physiol. Opt. J. Br. Coll. Ophthal. Opticians (Optometrists) 34, 502–508. doi: 10.1111/opo.12131
Barber, S. J., and Kim, H. (2021). COVID-19 Worries and Behavior Changes in Older and Younger Men and Women. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 76, e17–e23. doi: 10.1093/geronb/gbaa068
Bearman, S., and Amrhein, M. (2014). “Girls, Women, and Internalized Sexism”. in Internalized Oppression: The Psychology of Marginalized Groups, ed. E. J. R. David (Berlin, Germany: Springer Publishing Company), 192.
Bianchi, S. M., Milkie, M. A., Sayer, L. C., and Robinson, J. P. (2000). Is anyone doing the housework? Trends in the gender division of household labor. Soc. Forces 79, 191–228. doi: 10.2307/2675569
Brody, G. H., and Flor, D. L. (1997). Maternal psychological functioning, family processes, and child adjustment in rural, single-parent, African American families. Dev. Psychol. 33, 1000–1011. doi: 10.1037/0012-1649.33.6.1000
Bronfenbrenner, U., and Morris, P. A. (2006). “The bioecological model of human development,” in Handbook of Child Psychology: Theoretical Models of Human Development, eds. W. Damon (Series Ed.) and R. M. Lerner (Vol. Ed.) (New York, NY: Wiley), 793–828.
Budescu Taylor, R. D. (2013). Order in the home: Family routines moderate the impact of financial hardship. J. Appl. Dev. Psychol. 34, 63–72. doi: 10.1016/j.appdev.2012.11.006
Cantillon, S., Moore, E., and Teasdale, N. (2021). COVID-19 and the pivotal role of grandparents: childcare and income support in the UK and South Africa. Fem. Econ. (2021) 27, 188–202. doi: 10.1080/13545701.2020.1860246
Chandan, J. S., Thomas, T., Bradbury-Jones, C., Russell, R., Bandyopadhyay, S., Nirantharakumar, K., et al. (2020). Female survivors of intimate partner violence and risk of depression, anxiety, and serious mental illness. Br. J. Psychiatry 217, 562–567. doi: 10.1192/bjp.2019.124
Cohen, P. N. (2004). The Gender Division of Labor: “Keeping House” and Occupational Segregation in the United States. Gender Soc. 18, 239–252. doi: 10.1177/0891243203262037
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 385–396. doi: 10.2307/2136404
Conger, R. D., and Conger, K. J. (2002). Resilience in Midwestern families: Selected findings from the first decade of a prospective, longitudinal study. J. Marr. Family 64, 361–373. doi: 10.1111/j.1741-3737.2002.00361.x
Connor, J., Madhavan, S., Mokashi, M., Amanuel, H., Johnson, N. R., Pace, L. E., et al. (2020). Health risks and outcomes that disproportionately affect women during the Covid-19 Pandemic: A review. Soc. Sci. Med. 266, 113364. doi: 10.1016/j.socscimed.2020.113364
Fenollar-Cortés, J., Jiménez, Ó., Ruiz-García, A., and Resurrección, D. M. (2021). Gender differences in psychological impact of the confinement during the COVID-19 outbreak in spain: a longitudinal study. Front. Psychol. 12, 682860. doi: 10.3389/fpsyg.2021.682860
Fiese, B. H., Tomcho, T., Douglas, M., Josephs, K., Poltrock, S., Baker, T., et al. (2002). Fifty years of research on naturally occurring rituals: Cause for celebration? J. Family Psychol. 16, 381–390. doi: 10.1037/0893-3200.16.4.381
Fritz, H. (2014). The influence of daily routines on engaging in diabetes self-management. Scandinavian J. Occup. Ther. 21, 232–240. doi: 10.3109/11038128.2013.868033
Galasso, V., Pons, V., Profeta, P., Becher, M., Brouard, S., Foucault, M., et al. (2020). Gender differences in COVID-19 attitudes and behavior: Panel evidence from eight countries. Proc. Natl. Acad. Sci. 117, 27285–27291. doi: 10.1073/pnas.2012520117
García-Fernández, L., Romero-Ferreiro, V., Padilla, S., David López-Roldán, P., Monzó-García, M., and Rodriguez-Jimenez, R. (2021). Gender differences in emotional response to the COVID-19 outbreak in Spain. Brain Behav. 11, e01934. doi: 10.1002/brb3.1934
Gutiérrez-Lobos, K., Wölfl, G., Scherer, M., Anderer, P., and Schmidl-Mohl, B. (2000). The gender gap in depression reconsidered: the influence of marital and employment status on the female/male ratio of treated incidence rates. Soc. Psychiatry Psychiatric Epidemiol. 35, 202–210. doi: 10.1007/s001270050229
Harper, C. A., Satchell, L. P., Fido, D., and Latzman, R. D. (2020). Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Mental Health Addict. 19, 1875–1888. doi: 10.31234/osf.io/jkfu3
Heggeness, M. L. (2020). Estimating the immediate impact of the COVID-19 shock on parental attachment to the labor market and the double bind of mothers. Rev. Econ. Household 18, 1053–1078. doi: 10.1007/s11150-020-09514-x
Hiller, D. V. (1984). Power Dependence and Division of Family Work. Sex Roles 10, 1003–1019. doi: 10.1007/BF00288521
Hou, F., Bi, F., Jiao, R., Luo, D., and Song, K. (2020). Gender differences of depression and anxiety among social media users during the COVID-19 outbreak in China: a cross-sectional study. BMC Public Health 20, 1–11. doi: 10.1186/s12889-020-09738-7
Jensen, E. W., James, S. A., Boyce, W. T., and Hartnett, S. A. (1983). The family routines inventory: Development and validation. Soc. Sci. Med. 17, 201–211. doi: 10.1016/0277-9536(83)90117-X
Killgore, W. D. S., Taylor, E. C., Cloonan, S. A., and Dailey, N. S. (2020). Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 291, 113216. doi: 10.1016/j.psychres.2020.113216
Knaul, F. M., Bustreo, F., and Horton, R. (2020). Countering the Pandemic of gender-based violence and maltreatment of young people: The Lancet Commission. Lancet (London, England) 395, 98–99. doi: 10.1016/S0140-6736(19)33136-8
Koome, F., Hocking, C., and Sutton, D. (2012). Why Routines Matter: The Nature and Meaning of Family Routines in the Context of Adolescent Mental Illness. J. Occup. Sci. 19, 312–325. doi: 10.1080/14427591.2012.718245
Lanza, H. I., and Taylor, R. D. (2010). Parenting in moderation: Family routine moderates the relation between school disengagement and delinquent behaviors among African American adolescents. Cult. Div. Ethnic Minor. Psychol. 16, 540–547. doi: 10.1037/a0021369
Lynch, S. H., Shuster, G., and Lobo, M. L. (2018). The family caregiver experience examining the positive and negative aspects of compassion satisfaction and compassion fatigue as caregiving outcomes. Aging Mental Health 22, 1424–1431. doi: 10.1080/13607863.2017.1364344
Masten, A. S., and Motti-Stefanidi, F. (2020). Multisystem Resilience for Children and Youth in Disaster: Reflections in the Context of COVID-19. Adver. Resilience Sci. 1, 95–106. doi: 10.1007/s42844-020-00010-w
Pappa, S., Ntella, V., Giannakas, T., Giannakoulis, V. G., Papoutsi, E., Katsaounou, P., et al. (2020). Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 Pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 88, 901–907. doi: 10.1016/j.bbi.2020.05.026
Peterson-Sweeney, K. (2009). The relationship of household routines to morbidity outcomes in childhood asthma. J. Special. Pediatric Nurs. JSPN 14, 59–69. doi: 10.1111/j.1744-6155.2008.00175.x
Pew Research Center (2020). Unemployed Americans are feeling the emotional strain of job loss; most have considered changing occupations. Retrieved from: https://www.pewresearch.org/fact-tank/2021/02/10/unemployed-americans-are-feeling-the-emotional-strain-of-job-loss-most-have-considered-changing-occupations/ (accessed February 10, 2021).
Power, K. (2020). The COVID-19 Pandemic has increased the care burden of women and families. Sustain. Sci. Pract. Policy 16, 67–73. doi: 10.1080/15487733.2020.1776561
Roig Berenguer, R. M., Aybar, C., and Pavía, J. M. (2022). COVID-19, Gender Housework Division and Municipality Size in Spain. Soc. Sci. 11, 2022. doi: 10.3390/socsci11020037
Salk, R. H., Hyde, J. S., and Abramson, L. Y. (2017). Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychol. Bull. 143, 783–822. doi: 10.1037/bul0000102
Saxena, M. (2021). “This Too shall Pass”: Age-Based Perceptions of Changes in Routine, Coping, and Stress. J. Gerontol. Geriatric Med. 7, 2. doi: 10.24966/GGM-8662/100101
Saxena, M. (2022). “Navigating the pandemic: Protective proximal processes in the microsystem of families worldwide,” Family Focus, National Council of Family Relations Report. Retrieved from: https://www.ncfr.org/ncfr-report/spring-2022/navigating-pandemic-protective-proximal-processes-microsystem-families (accessed November 14, 2022).
Sønderskov, K. M., Dinesen, P. T., Santini, Z. I., and Østergaard, S. D. (2020). The depressive state of Denmark during the COVID-19 Pandemic. Acta neuropsychiatrica 32, 226–228. doi: 10.1017/neu.2020.15
Spagnola, M., and Fiese, B. H. (2007). Family routines and rituals: A context for development in the lives of young children. Infants Young Children 20, 284–299. doi: 10.1097/01.IYC.0000290352.32170.5a
Spagnolo, P. A., Manson, J. E., and Joffe, H. (2020). Sex and Gender Differences in Health: What the COVID-19 Pandemic Can Teach Us. Ann. Intern. Med. 173, 385–386. doi: 10.7326/M20-1941
Taylor, J. M. (2015). Psychometric analysis of the ten-item perceived stress scale. Psychol. Assess. 27, 90–101. doi: 10.1037/a0038100
Tsibidaki, A. (2021). Anxiety, meaning in life, self-efficacy, and resilience in families with one or more members with special educational needs and disability during COVID-19 pandemic in Greece. Res. Dev. Disabil. 109, 103830. doi: 10.1016/j.ridd.2020.103830
Usher, K., Bhullar, N., Durkin, J., Gyamfi, N., and Jackson, D. (2020). Family violence and COVID-19: Increased vulnerability and reduced options for support. Int. J. Mental Health Nurs. 29, 549–552. doi: 10.1111/inm.12735
Walsh, F. (2020). Loss and resilience in the time of COVID-19: Meaning-making, hope, and transcendence. Family Process 59, 898–911. doi: 10.1111/famp.12588
Weissman, M. M., and Klerman, G. L. (1977). Sex differences and the epidemiology of depression. Arch. Gener. Psychiatry 34, 98–111. doi: 10.1001/archpsyc.1977.01770130100011
WHO (2021a). WHO Coronavirus (COVID-19) Dashboard. Retrieved from https://covid19.who.int/table (accessed September 2021).
WHO (2021b). WHO Coronavirus. Retrieved from: https://covid19.who.int/region/amro/country/us (accessed September 2021).
Keywords: stress, COVID-19, family routines, gender, systemic dysfunction
Citation: Saxena M, Shedlock DJ and Gold ZS (2023) Gender and disruptions in family routines and stress amid COVID-19. Front. Commun. 7:820882. doi: 10.3389/fcomm.2022.820882
Received: 23 November 2021; Accepted: 28 December 2022;
Published: 12 January 2023.
Edited by:
Satarupa Dasgupta, Ramapo College, United StatesReviewed by:
Gigi Foster, University of New South Wales, AustraliaRuma Sen, Ramapo College, United States
Copyright © 2023 Saxena, Shedlock and Gold. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mamta Saxena,  bWFtdGEuc2F4ZW5hQG9zd2Vnby5lZHU=
bWFtdGEuc2F4ZW5hQG9zd2Vnby5lZHU=