 Katelyn Murphy
Katelyn Murphy Devin Graham
Devin Graham- Texas A&M University AgriLife Extension Service, Family and Community Health, College Station, TX, United States
The COVID-19 pandemic and related rise of public distrust has called personal autonomy in health messaging into question, drawing attention to two competing forms of health messaging—communicating to persuade versus to inform. Communicating to persuade utilizes marketing techniques to promote behavior change whereas communicating to inform focuses on providing information to facilitate informed decision-making. Communicating to inform is supported by Self-Determination Theory (SDT), which posits that autonomy, coupled with competence and relatedness, is a basic psychological need, relevant to making health-decisions and maintaining behavior change. This study aims to assess the above mentioned dynamics of SDT in health messaging through the development of an autonomous scale and assessment criteria. The purpose of the scale is to guide the development of health messaging that aims to communicate to inform (autonomy-enhancing) rather than communicating to persuade or coerce the audience into adopting a specific health behavior (autonomy-diminishing). The results of the study suggest that individual perception of autonomy in health messaging is influenced by a variety of factors. As such, the criteria outlined in this scale can be used as a guide to develop health messaging that purposefully integrates and supports autonomy-enhancing principles.
1 Introduction
Health communication has been defined as, “the study and use of methods to inform and influence individual and community decisions that enhance health” (Nelson, 2002, pg. 6). The COVID-19 pandemic has called into question the efficacy of traditional health communication and messaging techniques to promote positive behavior change, without undermining personal autonomy. Further, the rise of public distrust in public health has created complexities for public health professionals delivering this messaging—now labeled an “infodemic” to describe the overload and perceived accuracy of information from different sources. Many of these conflicting messages are aimed at influencing health behaviors (e.g., vaccine uptake, masking, social distancing), and have drawn attention to two competing, and hard to differentiate, forms of health messaging: communicating to persuade versus communicating to inform.
Communicating to persuade utilizes marketing techniques to promote change in behavior, attitudes, or opinions related to a specific activity, most commonly seen in health messaging campaigns (Lum et al., 2002). McClaughlin et al. (2022) found that persuasion techniques, including moralizing messaging and fear appeals, triggered a range of highly negative emotional responses when testing COVID-19 messages. These negative emotions led to participant resistance and dismissal of the message, while others outright rejected the message. In the present study, a social media message from the Word Health Organization’s (WHO) COVID-19 immunization series attempted to persuade through the sensitive topic of pregnancy, and uses autonomy-diminishing language (should vs. could) to promote vaccination among pregnant individuals. The scoring of this image can be found in the Results and Analysis section (World Health Organization, 2022). While persuasive and coercive influences are not synonymous, priority audiences may perceive persuasive messages as such. Outlined above, the intent of persuasive communication is to change attitudes toward a particular health behavior, such as increasing fruit and vegetable uptake. These influences have been associated with internalization of behaviors, which is discussed below. Coercive influences may have a direct and more immediate impact on behavior change; however, they do not emphasize internalization. Because of this, coercive influences rely on an authoritative presence to reinforce behaviors and are not adhered to in the long term (Cassell et al., 1998).
Communicating to inform utilizes the extensive body of research on a particular health topic to supply the message with ample, research-and evidence-based information, so that the audience can make informed decisions regarding a health issue or uptake of a particular behavior (Arkin et al., 2002). Experiments conducted by Ryan and Deci (2006) found that conditions perceived as controlling (e.g., demanding language, minimization of choice) created individual loss in behavior change and well-being. Nyhan et al. (2014) found that solely providing information about disease risk did not improve attitudes or intention to engage in healthy behavior (e.g., vaccination). Thus, communicating to inform might be more effective if moved beyond only providing facts and information. Of interest here, engaging in autonomy-enhancing messages, which utilize non-persuasive, not controlling, nor coercive language and prioritize independence and choice, can help individuals internalize the behavior, meaning that the behavior is brought in-line with that individual’s personal values (internalization). This connection to one’s existing values can provide the rationale to motivate behavior change (Deci et al., 1994; Ryan et al., 2008; Legate and Weinstein, 2022). In the present study, the WHO posted a series of images utilizing autonomy-enhancing language (could vs. should) that described the ability for COVID-19 vaccination to save lives. The scoring of this image is later described in the Results and Analysis section (World Health Organization, 2021).
These phenomena are supported by Self-Determination Theory (SDT), a theory of human motivation, which posits that autonomy, competence, and relatedness are essential to internalizing and subsequently sustaining behavior change. Autonomy—the capacity to make an informed, uncoerced decision—is an innate psychological need essential for human growth, engagement and wellness. Competence—experiencing confidence to change—is facilitated by autonomy. Once an individual is willing to change, they apply the tools and education provided by practitioners to act. Relatedness—the sense of connectedness and trust an individual experiences with their networks—further promotes adoption and maintenance of behaviors. Individuals are more likely to maintain these changes when those around them promote them. Support of these constructs allows for internalization of behaviors, in which an individual self-regulates and is likely to sustain the desired behavior change (Ryan et al., 2008).
SDT emphasizes that personal autonomy can be undermined by lack of choice, insufficient rationale, imposition of threats, deadlines, external rewards, or other forms of coercion strategies often included in health messaging (Moller et al., 2006). Utilization of tactics that support autonomy in turn support autonomous motivation and can lead to internalized motivation to change a specific behavior. Extensive research has shown that this type of motivation can lead to short and long-term behavior change (Legate and Weinstein, 2022). Through this theoretical lens, a public health practitioner or entity communicating to persuade could be viewed as inherently autonomy-diminishing, and communicating to inform is viewed as inherently autonomy-enhancing.
There are several justifications for a focus on autonomy support. There is currently a limited perspective of autonomy in health messaging development or effectiveness. A recent study by Parrish-Sprowl et al. (2023) established a framework, AIMS (Announce, Inquire, Mirror, Secure) for clinical healthcare professionals to structure conversations with patients and caregivers about vaccination and building trust. This framework focuses on interpersonal interaction between a patient and their provider. Yet, there is no known theory-based scale to assess whether a health message is perceived as autonomy-diminishing or-enhancing by both the public health practitioner and populations of focus. Such a scale could act as a fruitful guide in the development and evaluation of health education messaging aimed at communicating to inform (autonomy-enhancing), rather than communicating to persuade or coerce the audience into adopting a healthy behavior (autonomy-diminishing). Toward this end, the purpose of this pilot study was to develop and test the function of the Autonomy in Health Messaging Scale (AiHMS), focused specifically on public health messages consumed by broader populations.
2 Methods
2.1 Development and concept validity
To best inform the development of the AiHMS, an informal review of existing literature pertaining to SDT, autonomy, and motivation was conducted—particularly around health-related messaging and/or education. In summary, personal autonomy can be enhanced by providing freedom of choice, explanation/rationale, and acknowledging the feelings of the intended audience; and threatened or undermined by the imposition of control, tangible rewards, threats, deadlines, and/or imposed goals (Pittman et al., 1980; Deci et al., 1994; Reeve et al., 2002; Joussemet et al., 2004; Moller et al., 2006; Cook and Artino Jr, 2016). Based on this review, the following semantic differential criteria was created related to their autonomy-enhancing versus-diminishing qualities, respectively:
1. Message provides personal choice vs. controlled choice
2. Message contains concise language vs. extensive language
3. Message provides sufficient rationale vs. insufficient rationale
4. Message conveys respect to audience vs. no respect to audience
5. Message emphasizes internal vs. external motivation
6. Message is gain-framed vs. loss-framed
After comprehensive discussion regarding scale formatting for sensitivity and ease of use, the semantic differential scale format was maintained for rating on a 7-point scale—ranging from autonomy-diminishing (−3) to autonomy-enhancing (+3), with 0 being neutral/null (neither autonomy-diminishing nor-enhancing). See howdyhealth.tamu.edu/AiHMS for additional details and descriptions of each criterion.
2.2 Content and construct validity
To test the content validity of the scale, a panel of five individuals from various backgrounds (three public health professionals and two non-experts—members of the business and education professions, respectively) were asked to anonymously evaluate and score existing health messaging, and provide feedback. Twenty one samples were selected for review, and included language from vaccination campaigns, public health announcements, infographics, and other news media encouraging COVID-19 vaccine uptake. These examples were compiled from agencies, such as the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), academic institutions (e.g., Johns Hopkins Public Health), and state and local health departments. The images selected for review can be found at howdyhealth.tamu.edu/AiHMS. It is important to note that the timeframe of the assessment (April 2022) was 2 years into the COVID-19 pandemic, when COVID-19 was a contentious topic.
Panelists were given a draft of the scale and scoring criteria, and asked to independently complete the review and scoring of the 21 samples. The individual reviewer scores, mean scores, and variance (i.e., standard deviation, min, max) were analyzed for early stage construct validity. The panelists were then convened as a group to discuss the scale, subjective differences in scoring, and areas for scale improvement. Panelist ratings and feedback were analyzed for summary scale performance, and for key recommendations of revisions to guide future research.
Inter-rater reliability was measured using Fleiss’ kappa (k) statistic, an adaptation of Cohen’s kappa, used to measure agreement between 3 or more raters. Fliess’s kappa can range from-1 to +1, and interpreted as follows: values ≤0 indicate no observed agreement between raters, values 0.01–0.20 indicate none to slight agreement, 0.21–0.40 as fair, 0.41–0.60 as moderate level of agreement, 0.61–0.80 as substantial, and 0.81–1.00 as near perfect agreement (McHugh, 2012). Moreover, negative kappa values indicate that the agreement between raters was less than the agreement expected by chance, 0 indicates that agreement was no better than chance, and kappa values greater than 0 represent increasingly better than chance agreement between raters.
3 Results
3.1 Scale performance
Results of individuals review panel scores for each of the 21 health messaging images are shown in Table 1. As shown, the mean image scores varied from each other, however generally fell between −1 (somewhat autonomy-diminishing) to +1 (somewhat autonomy-enhancing). Image 3, a WHO graphic stating, “you should get vaccinated against COVID-19 if you are planning to get pregnant,” resulted in the lowest average score of −1.23 ± 0.76. Image 4, a WHO graphic, which displayed the text, “getting vaccinated against COVID-19 could save your life,” resulted in the highest average score of 1.31 ± 0.77.
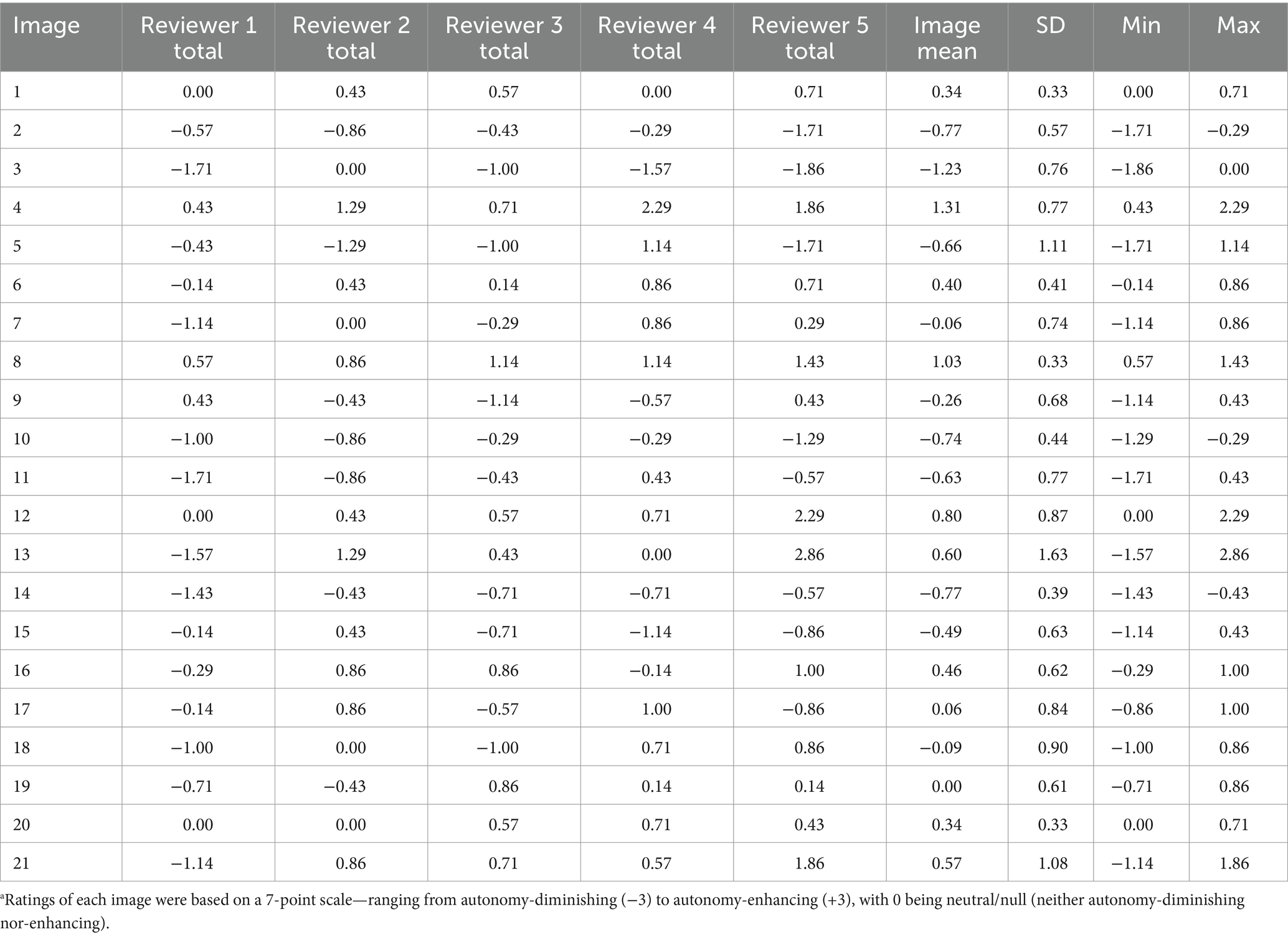
Table 1. Panelist review means scores and variance (standard deviation [SD], min, max) for panelists review of 21 health messaging imagesa.
Overall, there were large amounts of variance in rater scoring, with notable differences seen with images 5, 13, and 21 (SD = 1.11, 1.63, and 1.08, respectively). Fleiss’ kappa statistic, the relationship of agreement between raters, was found to be between no observed agreement and no more than chance (k = −0.022).
3.2 Scale revision
After rater scoring and analysis, the draft scale was adjusted to reflect the recommendations of the panel for practical and theoretical coherence. Per their recommendations, criteria 4, respect conveyed to audience, was revised to relevance to audience, to accommodate for the scoring of messages where there was no perceived target audience. See Table 2 for details on this revision. No additional modifications were made due to positive feedback from the panel regarding the clarity, ease of use, and applicability of both the scale and the provided ranking guidelines. Despite this feedback, the inconsistency among raters suggests that future research should assess multiple panels and panels of different professional compositions (public health professionals vs. non-experts). Additionally, panels assessing two scale versions could explore if language modifications to the assessment guidelines lead to enhanced differentiation of the criteria. Additional detail and definitions for all scoring criteria can be found at howdyhealth.tamu.edu/AiHMS. The final scale criteria were compiled as follows:
1. Message provides personal choice vs. controlled choice
2. Message contains concise language vs. extensive language
3. Message provides sufficient rationale vs. insufficient rationale
4. Message conveys relevance to audience vs. no relevance to audience
5. Message emphasizes internal vs. external motivation
6. Message is gain-framed vs. loss-framed

Table 2. Scale criteria revisionsa.
4 Discussion
The purpose of this study was to develop and provide an initial, pilot test of a theory-based scale—the Autonomy in Health Messaging Scale (AiHMS)—which was created to assess whether a health message is perceived as autonomy-diminishing or-enhancing by both the practitioner and intended audience of the message. In a small sample of assessors from both health and non-health backgrounds, the AiHMS appears to be sensitive to differing views of the same image, creating variability in assessors’ ratings. The relationship of agreement between raters fell between no observed agreement and agreement no more than chance (k = −0.02), suggesting that the raters scoring was inconsistent. It should be noted, however, that this finding does not necessarily reflect scale reliability, but rather expresses the unique variance in ratings between raters on the same images. Such variance, which should be further analyzed in future assessments, emphasizes the influence of the audience’s perception of public health messaging. As such, several relevant components of health messaging and potential future scale applications should be considered (Table 3).
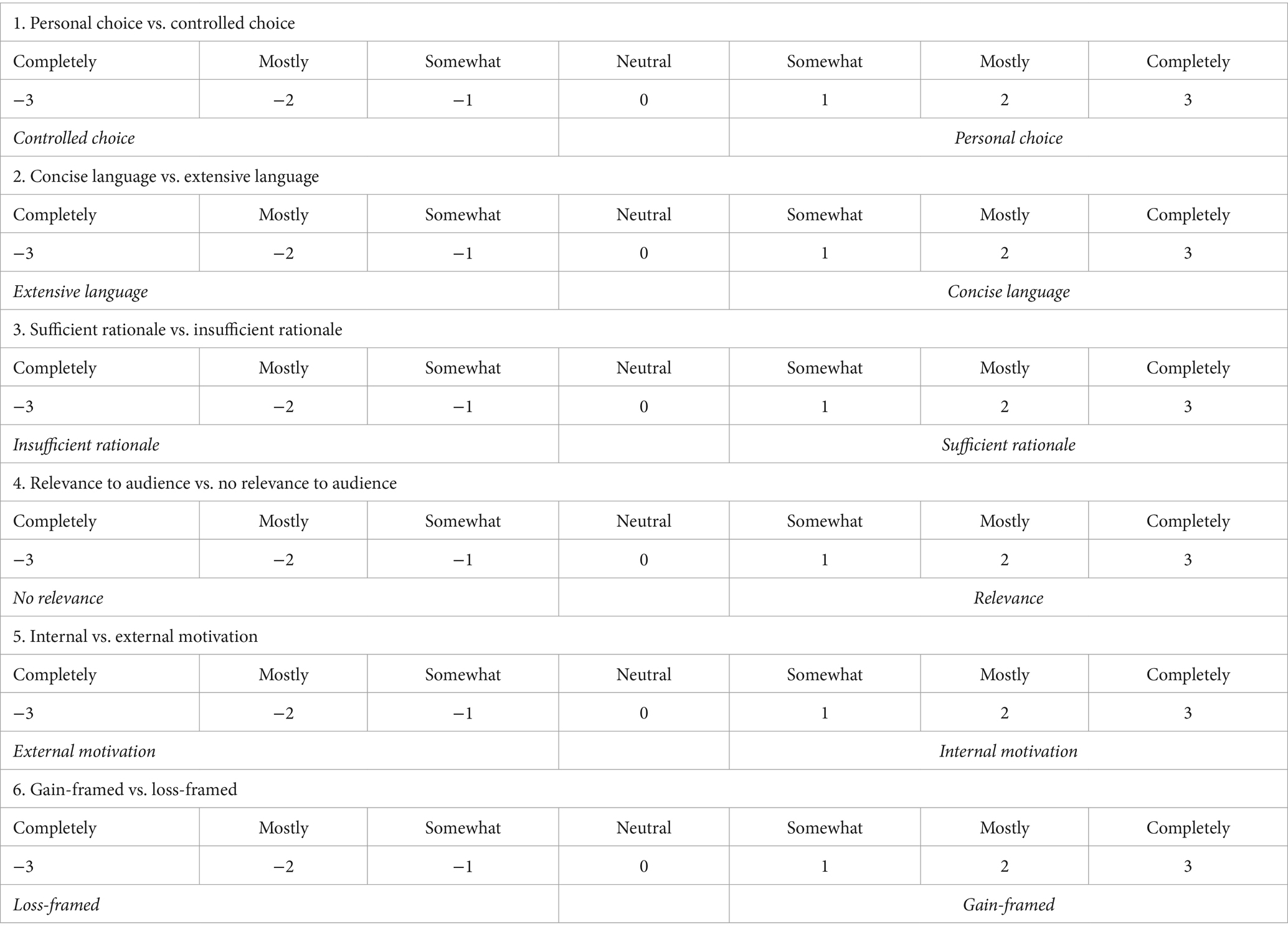
Table 3. Autonomy in public health messaging scale (AiHMS).
First, regarding levels of health education and/or health literacy within the intended audience—the review panel was composed of a mix of public health professionals and laypersons, which might express the differing opinions and interpretations of vaccination, public health recommendations, and autonomy in the health messaging. Differences in interpretation of health messages between the practitioner and intended audience will likely be seen due to differing levels of health literacy, as up to one-half of American adults have reported difficulty in understanding health messaging communicated to them (Nielsen-Bohlman et al., 2004). Language used by practitioners might not be at appropriate literacy levels for the audience, further confirming that audience input is essential to health message success through autonomy enhancement.
Regarding distrust and/or polarization—COVID-19 vaccination and risk mitigation strategies have been a contentious topic throughout the pandemic, influenced by a variety of external factors including trust or distrust of healthcare, political ideologies, religious and spiritual beliefs, interpretation of scientific research, and other determinants that might impact individuals’ health decision-making (Peters, 2022). As such, reviewers might have existing biases that influence their perception and scoring of messages. The authors acknowledge that future testing of the AiHMS should be conducted utilizing health messaging examples from a less polarizing health topic to compare the relationship of agreement between raters.
For practice, use of the AiHMS by practitioners can serve as a guide during the initial phases of health communication campaigns, especially when autonomy-enhancing message development is at the forefront of focus. With help of the AiHMS, practitioners can prioritize pretesting health communication campaign materials with the intended audience and ensure that feedback is incorporated into final versions of the message before wider dissemination to key audiences (Nelson, 2002; Schiavo, 2014). This participatory, audience-centered approach to health communication can better position the intended audience for behavior change, including preparation for emerging health issues and/or emergencies, such as the COVID-19 pandemic (Schiavo, 2014).
As such, the AiMHS and its criteria can be viewed as a guide to craft more autonomous messaging, rather than exclusively as a tool to grade existing messaging, as well as message development with intention toward autonomy-enhancing communication to inform, while avoiding the autonomy-diminishing language that aims to persuade. Such recommendations are speculative at this time, as the present study was an initial step to warrant and encourage additional research to further confirm the reliability of this scale, to explore how health topics are perceived among different audiences, elucidate how variance might explain the differing impact that messages can have depending on the audience, and discover how different topics might influence perceived levels of autonomy in health decision-making.
4.1 Future considerations
Public health faces two primary challenges: (1) the desire to aid in the health of the population and (2) understand how diverse communities and individuals prefer and receive health information. To help, future health messaging, even if used for population-level dissemination, can be modified to consider and support personal autonomy of individuals in health messaging. This ‘bottom up’ approach minimizes the threat large-scale approaches to health messaging can have on established individual-level determinants of health, and is likely to enhance adherence to behavior change and improve health outcomes (Porat et al., 2020). More immediate testing could be done to compare individual and key audience perception of autonomy-enhancing and -diminishing messaging, utilizing the AiHMS components to build initial messages. After review and input from key audiences, these messages could then be dispersed into the wider community, also comparing perceptions between the two message types to better understand how autonomy-enhancing messages are received. A recent study, Ahmadi et al. (2023), provides a list of behaviors that practitioners could utilize during interventions to further support the constructs of SDT. These tactics could be of use and built upon in future studies.
Additionally, continued testing of AiHMS is warranted to further develop a more formal framework for creation of autonomous health messaging. Future research can consider exploring other health topics, including those less polarizing than COVID-19. Although previous research has shown that use of coercive methods can be effective in eliciting immediate behavior change, the efficacy of autonomy-promoting efforts is still largely unknown; in addition, this behavior change is not sustained over longer periods of time (Moller et al., 2006). Future research might also explore the balance between providing enough information (sufficient rationale) to audiences to make informed decisions about their health, while still promoting autonomy. For example, what kinds of messaging are effectively autonomy-promoting while still providing sufficient rationale, remaining concise and audience specific? What role does trust play, in both the recommendation and the messenger?
4.2 Limitations
There were several limitations throughout this study that should be noted. First, the AiMHS scale was tested only once, with a singular, small set of reviewers. Additional testing is warranted with a larger review panel to further assess scale and interrater reliability. Additionally, future panels might consider professional and educational backgrounds to evaluate how these putative moderating variables might affect an individual’s perception of autonomy in health messaging, and how health messaging might be tailored to different audiences.
Also of note, a limitation of this research is that the images evaluated were selected from the public domain. Therefore, many of the criteria we deemed important (autonomy-enhancing) during scale development were simply not present in the examples, leading to frequent scores of 0 (null). Future research might consider developing novel messaging containing the autonomy-enhancing criterion. Such could expand our understanding of how impactful various types or levels of autonomous messaging can be on intention and behavior, as well as understand how messaging interacts with individual biases, expertise, and personal opinions and preferences with them when interpreting these messages.
5 Conclusion
The COVID-19 pandemic and rise of disinformation has drawn attention to the need for more autonomous public health messaging. With concern of the coercive nature of public health messaging that undermines personal autonomy, the purpose of this study was to provide a pilot test of the AiHMS scale with real public health messaging utilized during the COVID-19 pandemic. The results provide preliminary support for the AiHMS scale to act as a guide in the development of health messaging, to craft better, more autonomous health messaging aimed at communicating to inform (autonomy-enhancing) rather than communicating to persuade or coerce (autonomy-diminishing).
However, the results also highlight individual differences in perception of messaging between health professionals and the general public, and present new opportunities for future research and practice for crafting optimal health messaging that positively influence, or at least not undermine, perceptions of autonomy, of which is theorized to have a greater impact on intention and subsequent behavior change.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Author contributions
KM: Writing – original draft, Writing – review & editing, Conceptualization, Investigation, Methodology, Resources, Supervision. DG: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Writing – original draft, Writing – review & editing. MF: Formal analysis, Funding acquisition, Project administration, Software, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Extension Foundation via CDC and USDA-NIFA under grant EXC1-2021-2063.
Acknowledgments
The authors would like to thank the Extension Foundation for their support and guidance during this grant project, as well as the rural communities that continue to participate in the EXCITE grant with our agency.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ahmadi, A., Noetel, M., Parker, P., Ryan, R. M., Ntoumanis, N., Reeve, J., et al. (2023). A classification system for teachers’ motivational behaviors recommended in self-deamination theory interventions. J. Educ. Psychol. 115, 1158–1176. doi: 10.1037/edu0000783
Arkin, E., Maibach, E., and Parvata, C. (2002). “General public: communicating to persuade” in Communicating public health information effectively: A guide for practitioners. eds. D. E. Nelson, R. C. Brownson, P. L. Remington, and C. Parvanta (Washington, DC: American Public Health Association), 60–71.
Cassell, M. M., Jackson, C., and Cheuvront, B. (1998). Health communication on the internet: an effective channel for health behavior change? J. Health Commun. 3, 71–79. doi: 10.1080/108107398127517
Cook, D. A., and Artino, A. R. Jr. (2016). Motivation to learn: an overview of contemporary theories. Med. Educ. 50, 997–1014. doi: 10.1111/medu.13074
Deci, E. L., Eghrari, H., Patrick, B. C., and Leone, D. R. (1994). Facilitating internalization: the self-determination theory perspective. J. Pers. 62, 119–142. doi: 10.1111/j.1467-6494.1994.tb00797.x
Joussemet, M., Koestner, R., Lekes, N., and Houlfort, N. (2004). Introducing uninteresting tasks to children: a comparison of the effects of rewards and autonomy support. J. Pers. 72, 139–166. doi: 10.1111/j.0022-3506.2004.00259.x
Legate, N., and Weinstein, N. (2022). Can we communicate autonomy support and a mandate? How motivating messages relate to motivation for staying at home across time during the COVID-19 pandemic. Health Commun. 37, 1842–1849. doi: 10.1080/10410236.2021.1921907
Lum, M., Parvanta, C., Maibach, E., Arkin, E., and Nelson, D. E. (2002). “General public: communicating to inform” in Communicating public health information effectively: A guide for practitioners. eds. D. E. Nelson, R. C. Brownson, P. L. Remington, and C. Parvanta (Washington, DC: American Public Health Association), 47–57.
McClaughlin, E., Vilar-Lluch, S., Parnell, T., Knight, D., Nichele, E., Adolphs, S., et al. (2022). The reception of public health messages during the COVID-19 pandemic. Applied Corpus Linguistics 3, 100037–100020. doi: 10.1016/j.acorp.2022.100037
McHugh, M. L. (2012). Interrater reliability: the kappa statistic. Biochem. Med. 22, 276–282. doi: 10.11613/BM.2012.031
Moller, A., Ryan, R., and Deci, E. (2006). Self-determination theory and public policy: improving the quality of consumer decisions without using coercion. J. Public Policy Mark. 25, 104–116. doi: 10.1509/jppm.25.1.104
Nelson, D. E. (2002). “Current issues and challenges” in Communicating public health information effectively: A guide for practitioners. eds. D. E. Nelson, R. C. Brownson, P. L. Remington, and C. Parvanta (Washington, DC: American Public Health Association), 1–10.
Nielsen-Bohlman, L., Panzer, A. M., and Kindig, D. A. Institute of Medicine (US) Committee on Health Literacy (Eds.). (2004). Health literacy: a prescription to end confusion. National Academies Press (US).
Nyhan, B., Reifler, J., Richey, S., and Freed, G. L. (2014). Effective messages in vaccine promotion: a randomized trial. Pediatrics 133, e835–e842. doi: 10.1542/peds.2013-2365
Parrish-Sprowl, J., Thomas, A., Johnson, R. D., and Parrish-Sprowl, S. (2023). The AIMS approach: regulating receptivity in patient-provider vaccine conversations. Front. Public Health 11, 1–6. doi: 10.3389/fpubh.2023.1120326
Peters, M. J. D. (2022). Addressing vaccine hesitancy and resistance for COVID-19 vaccines. Int. J. Nurs. Stud. 131:104241. doi: 10.1016/j.ijnurstu.2022.104241
Pittman, T. S., Davey, M. E., Alafat, K. A., Wetherill, K. V., and Kramer, N. A. (1980). Informational versus controlling verbal rewards. Personal. Soc. Psychol. Bull. 6, 228–233. doi: 10.1177/014616728062007
Porat, T., Nyrup, R., Calvo, R. A., Paudyal, P., and Ford, E. (2020). Public health and risk communication during COVID-19- enhancing psychological needs to promote sustainable behavior change. Front. Public Health 8, 1–15. doi: 10.3389/fpubh.2020.573397
Reeve, J., Jang, H., Hardré, P., and Omura, M. (2002). Providing a rationale in an autonomy-supportive way as a strategy to motivate others during an uninteresting task. Motiv. Emot. 26, 183–207. doi: 10.1023/A:1021711629417
Ryan, R. M., and Deci, E. L. (2006). Self-regulation and the problem of human autonomy: does psychology need choice, self-determination, and will? J. Pers. 74, 1557–1586. doi: 10.1111/j.1467-6494.2006.00420.x
Ryan, R. M., Patrick, H., Deci, E. L., and Williams, G. C. (2008). Facilitating health behavior change and its maintenance: interventions based on self-determination theory. European Heal. Psychologist 10, 2–5.
Schiavo, R. (2014). Health communication: From theory to practice. 2nd Edn. San Francisco, CA: Jossey-Bass.
World Health Organization. (2021). DYK: unvaccinated people have at least 10 times higher risk of death from #COVID19 than someone who has been vaccinated. Vaccines work to save lives. Don’t delay. Instagram. Available at: https://www.instagram.com/p/CXimpLwD3r9/
World Health Organization. (2022). Q: can women who are trying to become pregnant receive #COVID19 vaccines? A: yes. Getting vaccinated beforehand is an important way for women to protect themselves and their future babies from COVID-19. There are no documented impacts of vaccination on fertility outcomes. Instagram. Available at: https://www.instagram.com/p/CaDjITajxvK/
Keywords: self-determination theory, health communication, autonomy, motivation, COVID
Citation: Murphy K, Graham D and Faries M (2024) Integrating autonomy in public health messaging. Front. Commun. 9:1346031. doi: 10.3389/fcomm.2024.1346031
Edited by:
Pier Luigi Sacco, University of Studies G. d’Annunzio Chieti and Pescara, ItalyReviewed by:
Henri Tilga, University of Tartu, EstoniaNatasha A. Rascon, Indiana State University, United States
Copyright © 2024 Murphy, Graham and Faries. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katelyn Murphy, a2F0ZS5tdXJwaHlAYWcudGFtdS5lZHU=