 Ivanka Pjesivac
Ivanka Pjesivac Leslie Klein
Leslie Klein Wenqing Zhao1
Wenqing Zhao1- 1University of Georgia, Athens, GA, United States
- 2University of Nebraska-Lincoln, Lincoln, NE, United States
- 3Oregon State University, Corvallis, OR, United States
This study examined the strength of different groups of individual-level variables in predicting conspiracy beliefs about Coronavirus disease (COVID-19) and related health behaviors by conducting a survey on a national online sample of U.S. adults. The results indicated that, among a wide range of individual-level variables, including psychopathological variables, cognitive variables, trust perceptions, trait emotions, health-related variables, and demographics, general belief in conspiracy theories (CTs) best predicted belief in specific COVID-19 CTs. In addition, our results showed that a stronger belief in COVID-19 CTs served as a significant predictor of engaging in less avoidance behavior. Furthermore, our results indicated that belief in general CTs does not directly lead to a change in avoidance behavior; the relationship is instead mediated by belief in COVID-19 CTs. Perceived severity of COVID-19 was the best predictor for proactive health behavior, whereas actual vaccination behavior was best predicted by confidence in COVID-19 vaccines. These results were interpreted using a framework that combines health communication theories with the concepts of path dependency and spillover effects in conspiratorial thinking.
Introduction
In recent years, the rapid spread of conspiracy theories (CTs) via digital media platforms has affected communication in many countries worldwide and captured both public and scholarly attention. Researchers, politicians, and journalists have warned that conspiratorial narratives, or beliefs that ultimate causes of events are secret plots by powerful people or organizations (e.g., Coady, 2006), have overtaken online (Wood and Douglas, 2015), popular (Brotherton and French, 2014), political (Oliver and Wood, 2014) and scientific and medical discourses (Goertzel, 2010). In the medical arena, the percentage of Americans accepting CTs has been alarmingly high. For example, Oliver and Wood (2014) published that 37% of Americans thought that the U.S. Food and Drug Administration (FDA) refused to release the cure for cancer, and that only 46% disagreed that fluoridation was a secret plot to poison people. In 2020, Pew Research Center found, through a nationally representative panel of randomly selected U.S. adults, that a quarter of the surveyed U.S. adults believed that there was at least some truth in CTs that powerful people intentionally planned the coronavirus outbreak (Schaeffer, 2020).
Researchers have warned that the spread of CTs could have potential detrimental effects (Hellinger, 2019; Oliver and Wood, 2014; Sunstein and Vermeule, 2009). Generally providing explanations for large-scale catastrophic events and containing generic content suggesting the suppression of information by governments, corporations, and scientists (Brotherton et al., 2013), conspiratorial narratives could play a major part in affecting individuals’ attitudes, intentions, and behaviors. They have been shown to delay preventative care, decrease the willingness to vaccinate against potentially deadly diseases (Cheruvu et al., 2017; Mills et al., 2005), decrease trust and health-seeking intentions (Natoli and Marques, 2021), and increase general feelings of powerlessness, disillusionment, and mistrust in authorities (Jolley and Douglas, 2014). Those who endorse medical CTs were also found to be more likely to report using alternative medicines and avoiding traditional medicines and less likely to have annual check-ups or get influenza vaccinations (Oliver and Wood, 2014). This shows that conspiratorial narratives can have significant consequences in shaping long-term health-related behaviors and risk-taking, especially because unverified narratives tend to linger in memory and are hard to correct (Pluviano et al., 2017; Pluviano et al., 2020).
Therefore, it is crucial to further explore the role of conspiratorial beliefs in health-related behaviors during a pandemic such as Coronavirus disease (COVID-19), focusing on their impact on decreased health-related behaviors and the mechanisms through which these beliefs originate. So far research has found that different types of variables can impact beliefs in misinformation: cognitive variables (e.g., Pennycook et al., 2020), including trust (e.g., van der Linden et al., 2021), psychopathological variables (e.g., de Zavala et al., 2020; Hughes and Machan, 2021), conspiratorial variables (e.g., Dyrendal et al., 2021), media-related variables (e.g., Lukito, 2020), health-related variables (e.g., Jolley and Douglas, 2014), emotional variables (e.g., Tomljenovic et al., 2020), and demographics (e.g., Vijaykumar et al., 2021). Despite these commendable efforts, less research has investigated how these factors function together in predicting beliefs in COVID-19 CTs, as well as their impact on health outcomes.
To address this gap, our study first examined the strength of different types of individual-level variables in predicting conspiracy beliefs about COVID-19 and related health behaviors. It also evaluated the role of beliefs in CTs about COVID-19 in mediating the relationship between its strongest individual-level predictor and COVID-19 health-related behaviors. Identifying the strongest predictors of COVID-19 conspiracy beliefs and related health behaviors allows us to distinguish among the potency of influence of cognitive, emotional, and psychopathological factors on the human propensity to explain the world using dogmatic epistemologies reflective of conspiratorial thinking. The present study helps integrate currently fragmented literature, examining different aspects of conspiratorial variables in different contexts by providing a comprehensive lens on individuals’ psychological and behavioral responses to pandemic information. Finally, understanding the role of CTs during pandemics will help public health organizations design more practical measures and policies to more effectively manage public health information communication that is increasingly impacted by users’ behaviors in online environments.
Medical conspiracy theories and COVID-19
Conspiracy theories (CTs) assume that “a powerful network of actors works in secret against the public good” (Natoli and Marques, 2021, p. 902). Research has shown that medical CTs have been widespread throughout human history. The rhetoric of conspiracy was already prominent in Ancient Greece and Rome (Roisman, 2006), as well as elsewhere in the world, even among ancient tribes (Chagnon, 1968; Evans-Pritchard, 1963; Von Rueden and Van Vugt, 2015), indicating their universal nature and deep psychological bases. In American public opinion, conspiracy themes have been persistent for more than a century (Uscinski and Parent, 2014). Although not always wrong (e.g., Watergate Affair, War in Iraq), CTs are worrisome when their underlying thought principle becomes the dominant, if not the sole, explanation for a variety of social, political, economic, and health outcomes.
In the medical arena, CTs about vaccines have been particularly prominent. The discovery of the smallpox vaccine triggered rumors that it would cause people to grow horns, while the DTP vaccine allegedly caused convulsions and cerebral damage (Dyer, 1988). In a study later refuted, Andrew Wakefield claimed in 1998 that the MMR vaccines were linked to autism, triggering a new wave of moral panic against vaccinations (Goldacre, 2008). In Pakistan, the belief that the polio vaccine was designed by the CIA to make Muslim men sterile is still prevalent, making this country one of the few where polio disease has not been eradicated (Andrade and Hussain, 2018). CTs about viruses such as AIDS and Ebola, both of which are often interpreted as inventions by the U.S. government to reduce populations, have also been widespread (Bogart and Bird, 2003; Knight, 2013). The U.S. government has also been blamed for the crack cocaine epidemic across the United States in the 1980s, with allegations that it specifically targeted African Americans to keep them addicted while profiting from the illegal trade to finance paramilitary groups in Nicaragua (Webb, 2019). Big pharmaceutical companies have often been targets of CTs, suggesting that they have been withholding cures for deadly diseases such as cancer to make a profit or control the population (Ernst, 2019). Another narrative suggested that ‘big pharma’ and medical doctors lie about the effectiveness of treatments for depression, suppress alternative natural cures, and overprescribe antidepressants for financial gain (Goertzel, 2010; Oliver and Wood, 2014). The fact that some companies have indeed engaged in concealing serious side effects of their products (e.g., Lipitor lawsuits against Pfizer; see Dye, 2014) and the fact that extraordinarily high prices of medication did indeed make some individuals rich (e.g., as the lifesaving EpiPen price rose by 400%, the salary of the CEO was increased to an astonishing $18 million; Popken, 2016) only put oil on the fire.
The COVID-19 pandemic proved to be a fertile ground for various CTs that spread through social media faster than the respiratory virus, affecting millions of people around the globe. CTs, including that the COVID-19 virus was created by the “deep state” in an effort to spread panic or by the Chinese government to harm the U.S. economy, ran rampant in the early days of the pandemic (Motta et al., 2020). In May of 2020, a 26-min video entitled “Plandemic” went viral and was viewed more than 8 million times across social media platforms (Frenkel et al., 2020). The video, which originally circulated on a QAnon Facebook group, claimed that the virus and a future potential vaccine were created by powerful people for profit and power (Frenkel et al., 2020). These conspiracies were adopted by a significant portion of the population. A survey of U.S. adult citizens conducted by the Pew Research Center found that while only 10% of Americans had watched “Plandemic,” 71% had heard of the CTs spread in the video, and 25% of respondents said they believed the theory (Mitchell et al., 2020).
COVID-19 conspiracy theorists have also focused their attention on questioning the safety and efficacy of a vaccine, and they began spreading misinformation about it even before it was ready and available to the general public. One study found that 25% of respondents who answered their survey believed that the pandemic was being used as an excuse to “force a dangerous and unnecessary vaccine on Americans,” and 20% believed that it was an excuse for someone to install tracking devices into their bodies (Enders et al., 2020, p. 5). The study encompassed a nationwide online survey of U.S. adults, whose demographic data aligned with U.S. Census demographic data. A poll conducted by YouGov also found that 20% of Americans believed the government was using the COVID-19 vaccine to microchip the population, and 83% of respondents who reported that they would not take the vaccine also reported belief in the theory that the dangers of COVID-19 were exaggerated for political reasons (Frankovic, 2021). A survey of almost 5,000 U.K. residents found that a smaller number endorsed a similar theory; only 8% of respondents believed that Bill Gates wanted to vaccinate people in order to implant microchips in them (University of Bristol and King’s College London, 2021). However, the same survey also found that 14% of respondents believed a vaccine was only being developed to make money for pharmaceutical companies, while 13% did not know if that conspiracy was true or false (University of Bristol and King’s College London, 2021). Those who endorsed any conspiratorial belief about COVID-19 were also significantly less likely to say they would receive a vaccine if and when it became available (University of Bristol and King’s College London, 2021).
Other prominent COVID-19 CTs include the debunked claim that the Centers for Disease Control and Prevention (CDC) was exaggerating the death count from the virus (Rouan, 2021) and the false theory that 5G wireless networks accelerated the spread of the virus (Ahmed et al., 2020). In the early months of the pandemic, a video that circulated online featured a prominent doctor known for her extreme views and anti-vaccination beliefs who claimed that the CDC was encouraging medical examiners to report COVID-19 as the cause of death even when patients had underlying conditions (Dickson, 2020). Several months later, the CT was perpetuated in a report that has since been discredited, which alleged that comorbidity procedures had falsely inflated the number of COVID-19 deaths in the U.S. (Rouan, 2021). Misinformation about a link between 5G and COVID-19 quickly spread online on social media sites such as Twitter through the viral hashtag #5GCoronavirus and resulted in the destruction of 5G towers by conspiracy theorists (Ahmed et al., 2020). More than 2 years into the pandemic, new COVID-19 CTs continued to circulate, including a claim furthered by both a former NBA athlete and a U.S. senator for the state of Wisconsin that professional athletes were dying after being vaccinated (Cillizza, 2022).
Conspiracies: effects on health-related behaviors
Previous research has established that holding conspiratorial beliefs about the COVID-19 virus is inversely related to the likelihood that someone will take preventative measures or get vaccinated against the virus (Romer and Jamieson, 2020). Additionally, individuals who were exposed to anti-vaccination conspiratorial beliefs were initially more likely to believe vaccines were unsafe (Hornsey et al., 2020). Social media usage has also been identified as a factor that influences individuals’ conspiratorial thinking about COVID-19. Individuals who use social media as their primary source of information about COVID-19 are more likely to believe CTs about the virus and are less likely to take preventative measures (Allington et al., 2021). However, individuals who believe CTs about COVID-19 will engage in preventative measures if they are not government-driven (Marinthe et al., 2020). Some extreme preventative behaviors became CTs themselves during 2020. An online survey of over 500 U.S. adults conducted by the CDC found that approximately one-third of survey respondents had inhaled or ingested bleach or applied it to their food or skin in an effort to prevent COVID-19 (Gharpure et al., 2020). Research has also shown that individuals who believed hydroxychloroquine could cure or prevent COVID-19 were more likely to engage in conspiratorial ideation (Bertin et al., 2020).
Conspiratorial beliefs have been previously linked to vaccine hesitation beyond the context of the COVID-19 pandemic. Despite evidence to the contrary, for over two decades, there has been a persistent belief among the anti-vaccination community that vaccines, and specifically the measles, mumps, and rubella (MMR) vaccine, cause autism (Gross, 2009). Belief in this CT has resulted in lowered immunization rates and recurrent outbreaks of measles, which had previously been declared to have been eliminated thanks to high vaccination rates (Gross, 2009). Several studies have also linked conspiratorial beliefs with lower human papillomavirus (HPV) immunization rates. Exposure to conspiratorial messages about the HPV vaccine has been found to result in less favorable attitudes toward the vaccine and lower vaccination intentions (Chen et al., 2021), and previous research shows that parents with high levels of conspiratorial thinking are more likely to delay vaccination for their children (Callaghan et al., 2019). Finally, individuals who endorse general anti-vaccine CTs, such as “immunizations allow governments to track and control people” and “tiny devices are implanted in vaccines for use in mind control experiments,” have been found to have lower vaccine intentions for any virus than individuals who do not believe anti-vaccine CTs (Jolley and Douglas, 2014).
Belief in COVID-19 CTs has also been shown to reduce adherence to social distancing measures (Bierwiaczonek et al., 2020). It has been negatively associated with safeguarding behaviors that can reduce the spread of the virus, such as hand washing and mask wearing (van Mulukom et al., 2022). A failure to adhere to health professionals’ guidelines is consistent with the effects of belief in other health-related CTs. Research has shown that high levels of conspiracism correlate with avoidance of medical professionals, such as annual examinations by a physician or a dentist (Oliver and Wood, 2014). However, which CT individuals believe may impact their behavior and result in differing levels of health-related risk taking. For example, one study conducted in both the U.S. and the U.K. indicated that while individuals who believed that COVID-19 is a hoax were less likely to report engaging in proactive behaviors such as handwashing and social distancing, those who believed that it originated in a laboratory were more likely to rely on alternative remedies (Imhoff and Lamberty, 2020).
Factors impacting beliefs in conspiracy theories
In order to look for potential successful solutions, it is important to identify how belief in CTs may lead to decreased health-related behaviors and to investigate the sources of such beliefs. When it comes to individual characteristics of audience members susceptible to misinformation, existing literature has identified that different types of variables can impact beliefs in misinformation (general and COVID-19 specific), ranging from cognitive and psychopathological variables, media-related and health-related variables, emotion variables, to demographics, which might impact beliefs in CTs about COVID-19 and vaccines.
Regarding cognitive variables, by investigating the psychological profile of individuals who tend to fall prey to misinformation using online surveys, Pennycook et al. (2020) found that individuals’ cognitive “bullshit receptivity” (p. 189) is driven by their varied degree of reflexive open-mindedness, defined as “tendency to be overly accepting of weak claims” (p. 185). Such cognitive tendency can be manifested as (a) perceiving misinformation as accurate, (b) inability to discern the differences between real news and fake news, and (c) over-claiming one’s knowledge of the focal topic. Trust was found to be another cognitive predictor of conspiracy beliefs. As summarized by van der Linden et al. (2021), according to previous misinformation research findings, individuals tend to trust claims made by sources whose ideology are congruent with their own while discounting those from politically incongruent sources; as a result, the persuasiveness of misinformation might be boosted or retracted depending on whether individuals support the sources or not.
Researchers have also identified psychopathological variables, including Machiavellianism and collective narcissism, that lead to outgroup aggression (de Zavala et al., 2020; de Zavala et al., 2009), as well as individual susceptibility to conspiracy beliefs and intentional spread of CTs during the COVID-19 pandemic (Hughes and Machan, 2021). In their attempt to understand intergroup aggressiveness, de Zavala et al. (2009) posited the concept of collective narcissism as “an emotional investment in an unrealistic belief about the in-group’s greatness” (de Zavala et al., 2009, p. 1,074), later adding “resentment for insufficient external recognition of the in-group’s importance” (de Zavala et al., 2020, p. 741). According to de Zavala et al.’s (2020) studies, collective narcissism (a) predicts aggression against out-groups and (b) is related to “high private and low public collective self-esteem and low implicit group esteem” and “sensitivity to threats to the ingroup’s image and retaliatory aggression” (p. 1,074). Besides collective narcissism, Hughes and Machan (2021) further examined trait psychopathy. High Machiavellianism and primary psychopathy, manifested in “callousness and lack of emotion and secondary psychopathy” and characterized by “impulsivity and anti-social tendencies,” were found to predict more general and COVID-19-specific conspiracy beliefs (Hughes and Machan, 2021). Interestingly, in the same study, collective narcissism only predicted COVID-19-specific conspiracy beliefs but not general conspiracy beliefs (Hughes and Machan, 2021).
Media-related variables and health-related variables are found to predict misinformation beliefs, especially under the influence of disinformation campaigns (Lukito, 2020), including anti-vaccine CT spread (Jolley and Douglas, 2014). By analyzing activities of Russia’s Internet Research Agency (IRA) in U.S. social media (2015–2017), Lukito (2020) found IRA’s internally-coordinated multi-platform disinformation campaign activity on Reddit and Twitter, targeted at U.S. citizens, alerting the future of “increasingly complex disinformation campaigns, executed by countries who take advantage of the internet’s anonymity and viral possibilities to spread inciteful messages” (p. 250) and a more CT saturated disinformation landscape. Anti-vaccine-specific CTs, their spread on social media, and predictors of anti-vaccine conspiracy beliefs have been examined. For instance, Jolley and Douglas’s (2014) study with UK participants showed: (a) a significant negative relationship between anti-vaccine conspiracy beliefs and vaccination intentions; (b) this negative relationship was mediated by perceived dangers of vaccines, feelings of powerlessness and disillusionment, and mistrust in authorities. These health-related variables seem to indicate that vaccine perception, self-perceived power/powerlessness, and (mis)trust in public health authorities are important factors predicting conspiracy beliefs related to vaccine and anti-vaccine disinformation campaigns.
Focusing on anti-vaccine conspiracy beliefs, via an online survey among parents, Tomljenovic et al. (2020) further examined emotional variables in the context of comparing the impacts of analytically rational and experientially intuitive thinking styles, as well as the role of emotional functioning (i.e., optimism) and emotions toward vaccines, on participants’ child vaccine conspiracy beliefs. This study identified three factors associated with greater vaccine conspiracy beliefs: (a) stronger predisposition to react with negative emotions toward vaccination; (b) greater experientially intuitive thinking; (c) lower levels of education, highlighting the importance of emotions and different thinking styles, as well as the role of demographic factors, in understanding CT belief regarding vaccines, including COVID-19 vaccines.
Vijaykumar et al.’s (2021) study further echoed the importance of demographics in COVID-19 misinformation management, with age as the focal demographic factor that is associated with misinformation susceptibility and predicts COVID-19 misinformation beliefs. Based on online experiments conducted among adult WhatsApp users in the UK and Brazil, Vijaykumar et al. (2021) found that, in both countries, younger adults were more likely to (a) believe COVID-19 misinformation and (b) share such misinformation than older adults.
Despite the increasing knowledge on the effects of the factors contributing to health misinformation belief (general and COVID-19), how these factors might function together (with varied strengths among different factor groups) and which of these groups of variables might be most important in predicting beliefs in COVID-19 CTs, as well as their impacts on health behavioral outcomes, remain understudied. In order to fill this gap in the literature of health communication, we ask the following research questions:
RQ1: Which is the strongest individual-level predictor of the COVID-19 conspiratorial beliefs?
RQ2: Which is the strongest individual-level predictor of health-related behaviors (i.e., proactive behavior, avoidance behavior, and actual vaccination)?
Individual-level factors, including psychological factors and emotions, have been shown to impact vaccine acceptance directly and sometimes adversely. Some studies have found that the feelings of fear of dying, anguish, vulnerability, and insecurity could lead to higher levels of confidence and propensity to COVID-19 vaccination (Kang and Jung, 2020; Mannan and Farhana, 2020; Simione et al., 2021), while others have shown that anger and negative emotions could be related to lower levels of vaccine acceptance (Betsch and Böhm, 2016; Sun et al., 2021). In addition, previous literature points out that key factors in determining the influence of emotions and psychological factors on COVID-19 vaccine propensity could be conspiracy beliefs, mistrust, or skepticism (Chou and Budenz, 2020). Simione et al. (2021) further showed that death anxiety reduced the propensity to get vaccinated through a mediated path in believing in CTs; psychological distress reduced vaccination propensity by increasing both conspiracy beliefs and mistrust; whereas anxiety increased the propensity to get vaccinated through a decrease in both belief in CTs and mistrust in science. These results suggest that individual-level variables, including psychological and emotional dimensions, are differently related to beliefs in CTs and propensity to get vaccinated. Further investigation is needed to determine if and how the belief in COVID-19 CTs mediate the relationship between individual-level variables and health-related behaviors. Thus, we ask the following research question:
RQ3: How, if at all, does the belief in COVID-19 CTs mediate the relationship between its strongest individual-level predictor and health-related behaviors (i.e., proactive behavior, avoidance behavior, and actual vaccination)?
Method
Participants and recruitment
In October and November 2021, we conducted an online survey with a total of 1,024 U.S. adults recruited from a Qualtrics panel, using the proportional quota sampling method to match the age, gender, and race distributions of US population1 Since this study was designed to understand adult individuals’ COVID-19 and COVID-19 vaccine-related beliefs and behavioral intentions, screeners were placed. The first screened out the participants who did not want to indicate their vaccination status (4) (1: Have not been vaccinated against COVID-19; 2: Have received only the first dose of the COVID-19 vaccine (if your vaccine requires two doses); 3: Have received both doses of the COVID-19 vaccine; 4: Do not want to indicate any of the above). Then the following three screeners screened out all those who did not intend to vaccinate or fully vaccinate in the future regardless of their initial vaccination status indicated in the first screener. This was done to capture the adopters (i.e., who have already taken the vaccine) and hesitant adopters (i.e., who have not taken the vaccine, but intended to do it). We purposefully excluded definite vaccine rejectors as we estimated that they were likely to hold extreme and stable conspiracy beliefs as well as health-related behaviors.
Respondents had ages ranging from 18 to 81 (M = 49.91, SD = 16.87). The sample contained 566 (55.3%) females, 455 (44.4%) males, and 2 (0.2%) respondents identifying their gender as other. One respondent declined to report gender. The majority of the sample was White 691 (67.5%), whereas 120 participants (11.7%) were Black, 118 (11.5%) Hispanic, 62 (6.1%) Asian, 11 (1.1%) were American Indian or Alaska native, and 20 (2%) identified as some other race. Two respondents refused to answer. Three hundred seventy-three participants (36.4%) had a high school degree, 283 (27.6%) had a bachelor’s degree, 207 (20.2%) had an associate degree, 136 (13.3%) had a master’s degree, 19 (1.9%) had a doctoral degree, 3 (0.3%) had less than elementary school education, 1 (0.1%) respondent had an elementary school degree. Two respondents declined to report their education level. In terms of the average earning of household, 460 (44.9%) respondents reported household income less than $50,000, 192 (18.8%) reported $50,000 to $69,999, 171 (16.7%) reported $70,000 to $100,000, 182 (17.8) reported household earning more than $100,000, and 19 respondents declined to answer. For political party identification, 510 (49.8%) reported their identification with Democratic, 238 (23.2%) identified with Republican, 226 (22.1%) identified with Independent, 37 (3.6%) reported no party identification, 7 (0.7%) identified with some other party, and 6 (0.6%) refused to answer. Research has been approved by the University of Georgia Institutional Review Board.
Predictor variables
To assess analytical thinking, respondents were asked to answer seven problem-solving questions (e.g., “If you are running a race and you pass the person in second place, what place are you in?”). For each problem, participants got one point if they provided the correct answer. The scores were added up to obtain a final score for each participant, ranging between 0 and 7 (N = 1,023, M = 1.69, SD = 1.69).
Psychopathy was measured with a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7) with 26 items (N = 874, M = 2.82, SD = 1.00, α = 0.90). Example items include “Success is based on survival of the fittest; I am not concerned about the losers” and “For me, what’s right is whatever I can get away with” (Levenson et al., 1995).
Collective narcissism was measured using a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7) with nine items (N = 971, M = 3.63, SD = 1.34, α = 0.87). Respondents were asked to answer the question having in mind the national group with which they identify. Example items include “I wish other groups would more quickly recognize the authority of my group” and “My group deserves special treatment” (de Zavala et al., 2009).
Machiavellianism was measured using four sub-scales (i.e., amorality, desire for control, desire for status, distrust of others) with a total of 16 items. Respondents were asked to indicate their degree of agreement/disagreement on a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7) (N = 975, M = 3.00, SD = 1.25, α = 0.92). The items (e.g., “I like to give the orders in interpersonal situations”) were adopted from Dahling et al. (2009).
General belief in CTs was measured with 15 items taken from Brotherton et al. (2013). Participants were asked to rate statements on a seven-point Likert scale ranging from definitely not true (1) to definitely true (7) (N = 990, M = 3.38, SD = 1.57, α = 0.96). Example items included “The government is involved in the murder of innocent citizens and/or well-known public figures, and keeps this a secret.”
Trust in the government was measured on a scale from not at all (1) to complete trust (7) (N = 1,016, M = 4.10, SD = 1.64). Respondents were asked to indicate to what extent they think they can trust the government in Washington, D.C. to do what is right.
News media trust was measured with a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7) (N = 977, M = 4.96, SD = 1.25, α = 0.95). Respondents were asked to think about news media in the United States in general and their coverage of the COVID-19 pandemic to rate their level of agreement/disagreement with 16 items adapted from Kohring and Matthes (2007). Example statement included “the topic of COVID-19 receives necessary attention.”
Perceived severity of COVID-19 was measured with three items adapted from Zhao and Tsang (2022) on a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7). Items included “COVID-19 is serious,” “COVID-19 can cause death,” and “COVID-19 is more severe than most people realize” (N = 1,003, M = 6.35, SD = 1.09, α = 0.85).
Vaccine confidence in COVID-19 was measured with three items taken from Nowak et al. (2018). Respondents were asked to indicate their level of confidence about the COVID-19 vaccine on a scale from not confident at all (1) to completely confident (7). Items included “How confident are you in the safety of the COVID-19 vaccine or shot?” “How confident are you that you would benefit from receiving a COVID-19 vaccine or shot?” and “How confident are you in the effectiveness of the COVID-19 vaccine or shot?” (N = 1,016, M = 5.76, SD = 1.42, α = 0.95).
Sensation seeking was measured with eight items taken from Hoyle et al. (2002) on a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7). Example items included “I would like to explore strange places” and “I would like to take off on a trip with no pre-planned routes or timetables” (N = 1,012, M = 3.38, SD = 1.48, α = 0.88).
Anxiety trait was measured using five items taken from Zsido et al. (2020) on a seven-point Likert scale ranging from strongly disagree (1) to strongly agree (7). Example items included “I feel that difficulties are piling up so that I cannot overcome them” and “I worry too much over something that really does not matter” (N = 1,014, M = 3.52, SD = 1.67, α = 0.91).
The fear trait was measured with 22 items taken from Bernstein and Allen (1969). Respondents were asked to indicate how much fear each item causes them on a seven-point scale ranging from none (1) to terror (7). Example items included “death of a loved one” and “speaking before a group” (N = 984, M = 3.79, SD = 1.24, α = 0.94).
Outcome variables
COVID-19 conspiratorial belief was measured with seven items adapted from Brotherton et al. (2013). Participants were asked to rate the following statements about the COVID-19 pandemic on a seven-point Likert scale ranging from definitely not true (1) to definitely true (7). Example items included “I believe there are groups interested in spreading panic to achieve their own goals” and “I believe that the development of the pandemic may benefit certain groups of whose interests we have no idea” (N = 997, M = 3.79, SD = 1.74, α = 0.92).
Avoidance behavior was measured with six items taken from Zhao and Tsang (2022). Respondents were asked to indicate how often they have been engaging in the following preventive behaviors during the COVID-19 pandemic on a seven-point scale ranging from never (1) to all the time (7). Example items included “avoiding close contact with people who are sick” and “avoiding dining out” (N = 1,009, M = 5.55, SD = 1.31, α = 0.86).
Proactive behavior was measured with three items taken from Zhao and Tsang (2022). Participants were asked to indicate how often they have been engaging in the following preventive behaviors during the COVID-19 pandemic on a seven-point scale ranging from never (1) to all the time (7). Items included “washing your hands more often,” “washing your hands appropriately (about 20 s using soap),” and “covering coughs and sneezes” (N = 1,019, M = 6.20, SD = 1.04, α = 0.83).
Actual vaccination was measured with one question that asked participants about their COVID-19 vaccination status. The options included “have not been vaccinated against COVID-19” (coded as “1”), “have received only the first dose of the COVID-19 vaccine (if your vaccine requires two doses)” (coded as “2”), and “have received both doses of the COVID-19 vaccine” (coded as “3”; N = 1,024, M = 2.85, SD = 0.48).
Analysis
Hierarchical regression analyses were run to answer RQ1 and RQ2, controlling for age, gender, race, political ideology, level of education, income, personal religiosity, pregnancy status, and state of residency. RQ3 was answered using a simple mediation model [PROCESS macro model (4) with 5,000 bootstrap samples (Hayes, 2013)].
Results
RQ1 asked which individual-level variable best predicted the COVID-19 conspiratorial beliefs. The multicollinearity assumption was held as all variance inflation factor (VIF) values were lower than 4, and no tolerance value was below 0.2. The P–P plot of standardized residuals and the scatterplot of standardized residuals against standardized predicted values showed that the assumptions of residual normality and homoscedasticity were met. A multiple regression analysis with hierarchical entry was conducted to predict the COVID-19 conspiratorial beliefs using individual-level variables while controlling for demographic factors. The control variables (i.e., age, gender, race, political ideology, education, household income, personal religiosity, pregnancy status, state of residency) accounted for a significant amount of the variance in COVID-19 conspiratorial beliefs, R2 = 0.18, F(9,664) = 16.32, p < 0.001. After entering analytical thinking, psychopathy, collective narcissism, Machiavellianism, anxiety trait, fear trait, general belief in CTs, trust in the government, trust in news media, perceived severity of COVID-19, vaccine confidence in COVID-19, and sensation seeking, the model accounted for 73.1% of the variance in COVID-19 conspiratorial beliefs, F(21,652) = 84.39, p < 0.001. The second step, individual-level variables accounted for an additional 55% of the variance in COVID-19 conspiratorial beliefs, R2 change = 0.55, F change (12,652) = 111.09. In the complete model, general belief in CTs was the best individual predictor (β = 0.68, p < 0.001). Individuals’ collective narcissism (β = 0.06, p = 0.046) and Machiavellianism (β = 0.08, p = 0.043) were also positively associated with COVID-19 conspiratorial beliefs. Trust in the government (β = −0.09, p < 0.001) and news media (β = − 0.07, p = 0.018) were negatively associated with COVID-19 conspiratorial beliefs (see Table 1).
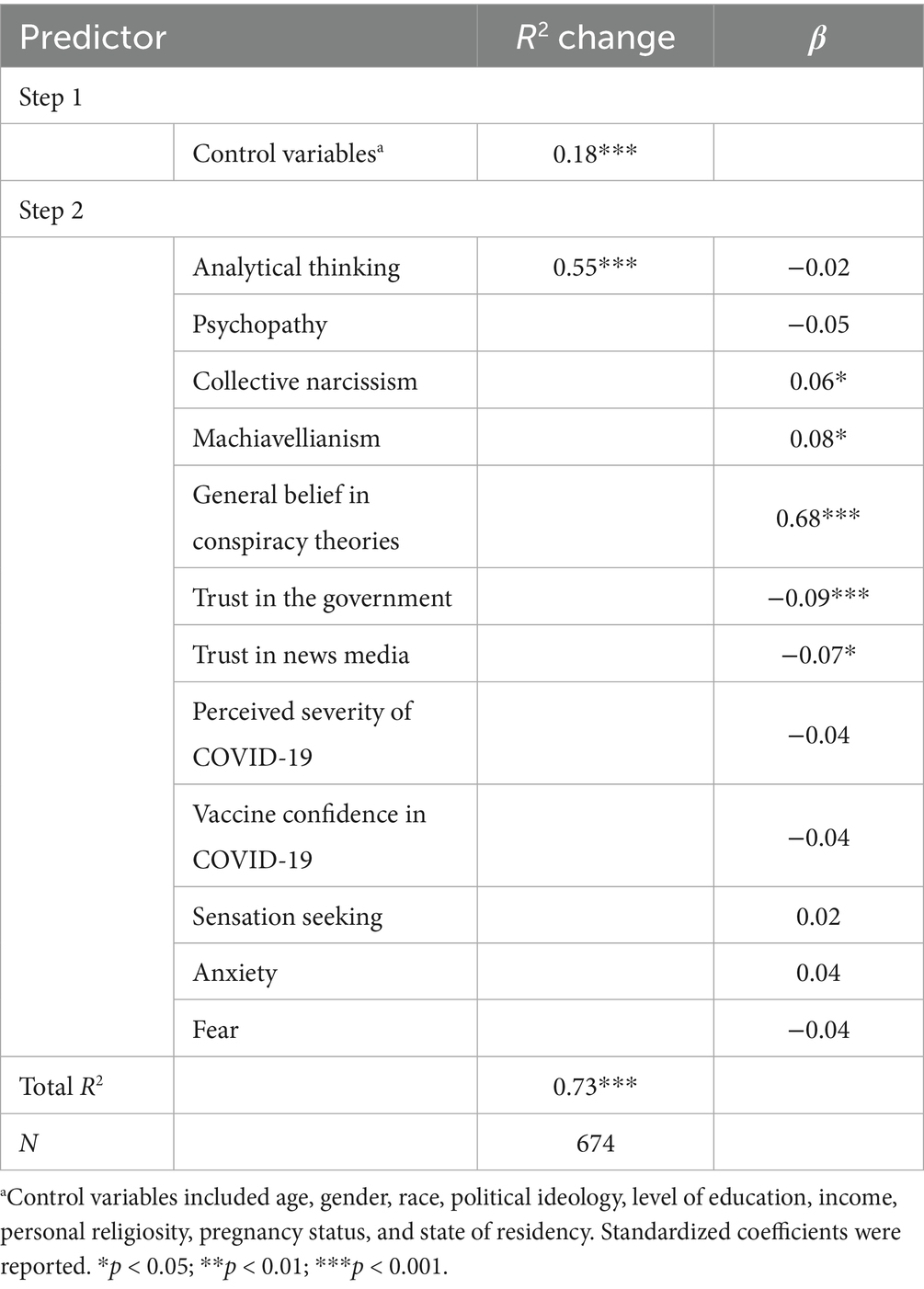
Table 1. Summary of hierarchical regression analysis predicting conspiracy beliefs in COVID-19.
RQ2 asked which one, among all individual-level variables, best predicted health-related behaviors. Three multiple hierarchical regression analyses were conducted to predict the proactive behavior, avoidance behavior, and actual vaccination, separately. Firstly, the results showed that the control variables (age, gender, race, political ideology, education, household income, personal religiosity, pregnancy status, state of residency) accounted for a significant amount of the proactive behavior variance, R2 = 0.07, F(9,666) = 5.25, p < 0.001. After entering analytical thinking, psychopathy, collective narcissism, Machiavellianism, general belief in CTs, trust in the government, trust in news media, perceived severity of COVID-19, vaccine confidence in COVID-19, sensation seeking, and anxiety trait, and fear trait, the model accounted for 23.5% of the variance in proactive behaviors F(21,654) = 9.58, p < 0.001. The second step, individual-level variables accounted for an additional 16.9% of variance in proactive behaviors, R2 change = 0.17, F change (12,654) = 12.04. Controlling for demographic factors, the perceived severity of COVID-19 was the best individual predictor (β = 0.27, p < 0.001). In addition, analytical thinking (β = −0.08, p = 0.03) and psychopathy (β = −0.25, p < 0.001) were negatively associated with proactive behaviors. Confidence in COVID-19 vaccines (β = 0.13, p = 0.004) and fear trait (β = 0.10, p = 0.015) were positive predictors of proactive behaviors (see Table 2).
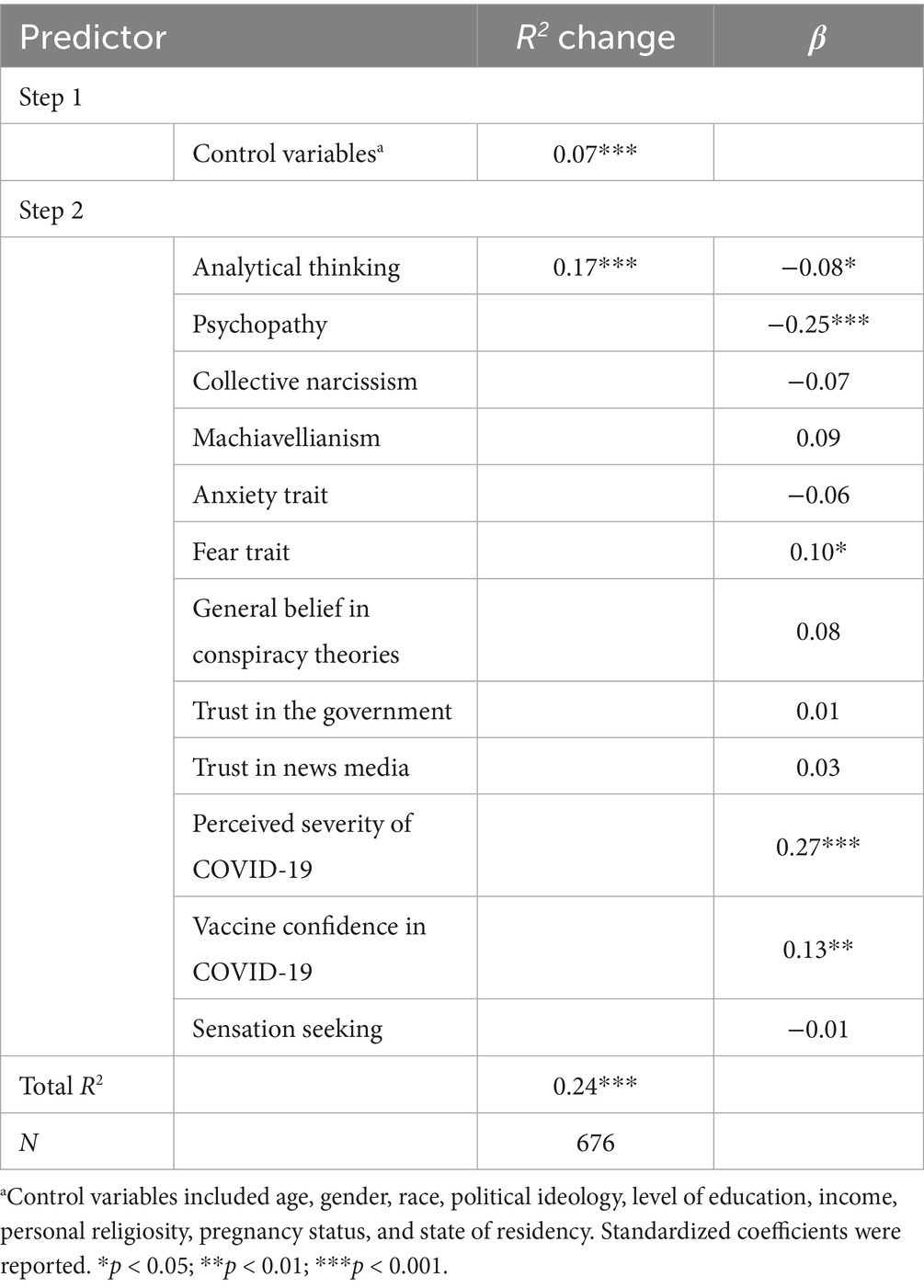
Table 2. Summary of hierarchical regression analysis predicting proactive behaviors.
Second, when it comes to the avoidance behavior, demographic factors such as age, gender, race, political ideology, education, household income, personal religiosity, pregnancy status, and state of residency accounted for a significant amount of the avoidance behavior variance, R2 = 0.10, F(9,663) = 7.90, p < 0.001. After entering the second step, individual-level variables, the model accounted for 32.9% of the variance in avoidance behaviors, F(21,651) = 15.18, p < 0.001. These variables accounted for an additional 23.2% of variance in avoidance behaviors, R2 change = 0.23, F change (12,651) = 18.73. Among them, the perceived severity of COVID-19 was the best individual predictor (β = 0.35, p < 0.001), followed by the trust in the news media (β = 0.21, p < 0.001), sensation seeking (β = −0.14, p < 0.001), and fear trait (β = 0.09, p = 0.02) (see Table 3).
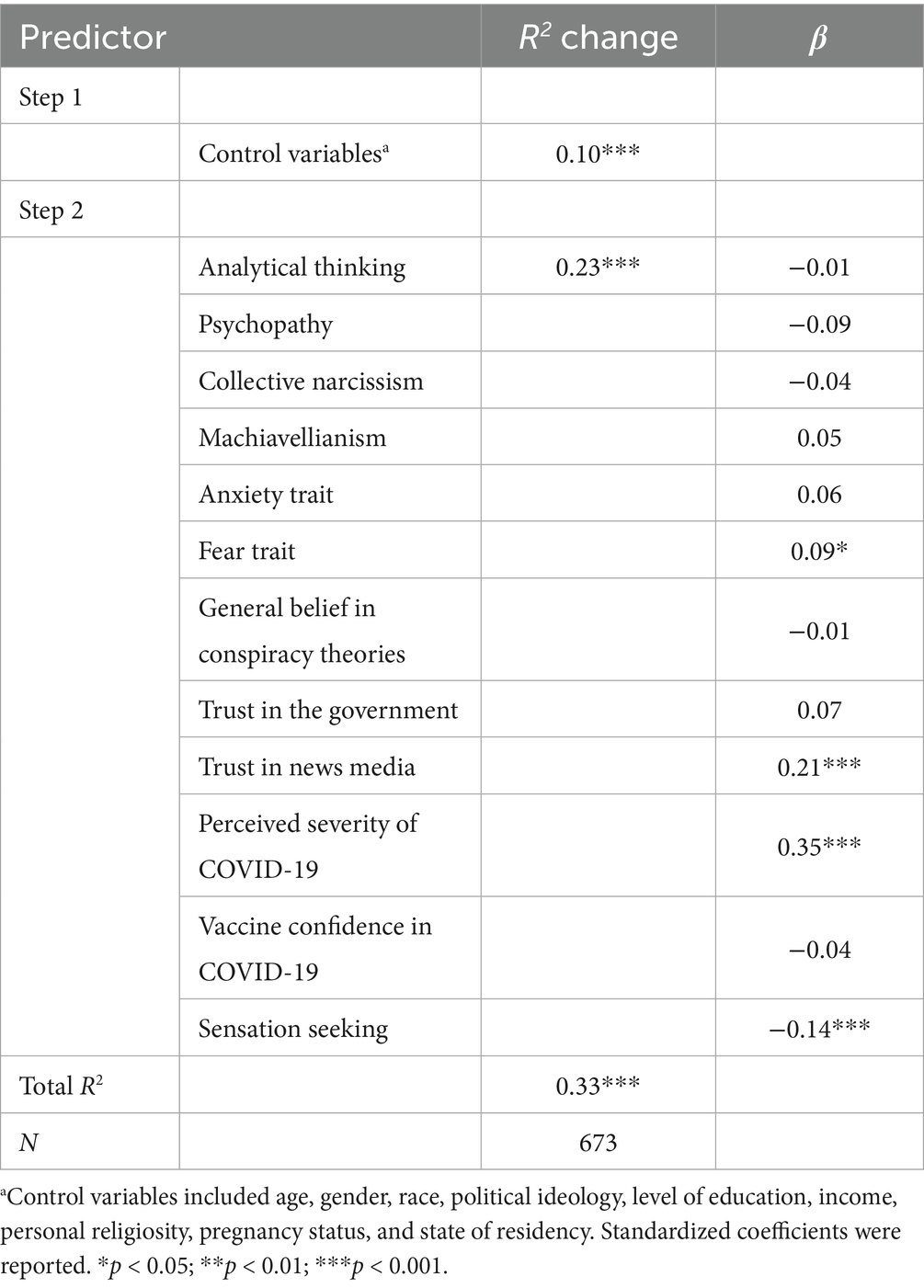
Table 3. Summary of hierarchical regression analysis predicting avoidance behavior.
Third, in terms of one’s actual vaccination behavior, demographic factors accounted for a significant amount of variance, R2 = 0.04, F(9,668) = 3.15, p < 0.001. After entering analytical thinking, psychopathy, collective narcissism, Machiavellianism, general belief in CTs, trust in the government, trust in news media, perceived severity of COVID-19, vaccine confidence in COVID-19, sensation seeking, anxiety trait, and fear trait, the model accounted for 9.5% of the variance in actual vaccination behavior, F(21,656) = 3.29, p < 0.001. The second step, individual-level variables accounted for an additional 5.5% of variance in actual vaccination behavior, R2 change = 0.06, F change (12,656) = 3.30. When controlling for demographic factors, confidence in the COVID-19 vaccine was the best predictor for one’s actual vaccination behavior (β = 0.21, p < 0.001). Additionally, collective narcissism was positively associated with actual vaccination (β = 0.12, p = 0.02). Trust in news media (β = −0.11, p = 0.04) and sensation seeking (β = −0.10, p = 0.04) were negatively associated with one’s actual vaccination behavior (see Table 4).2
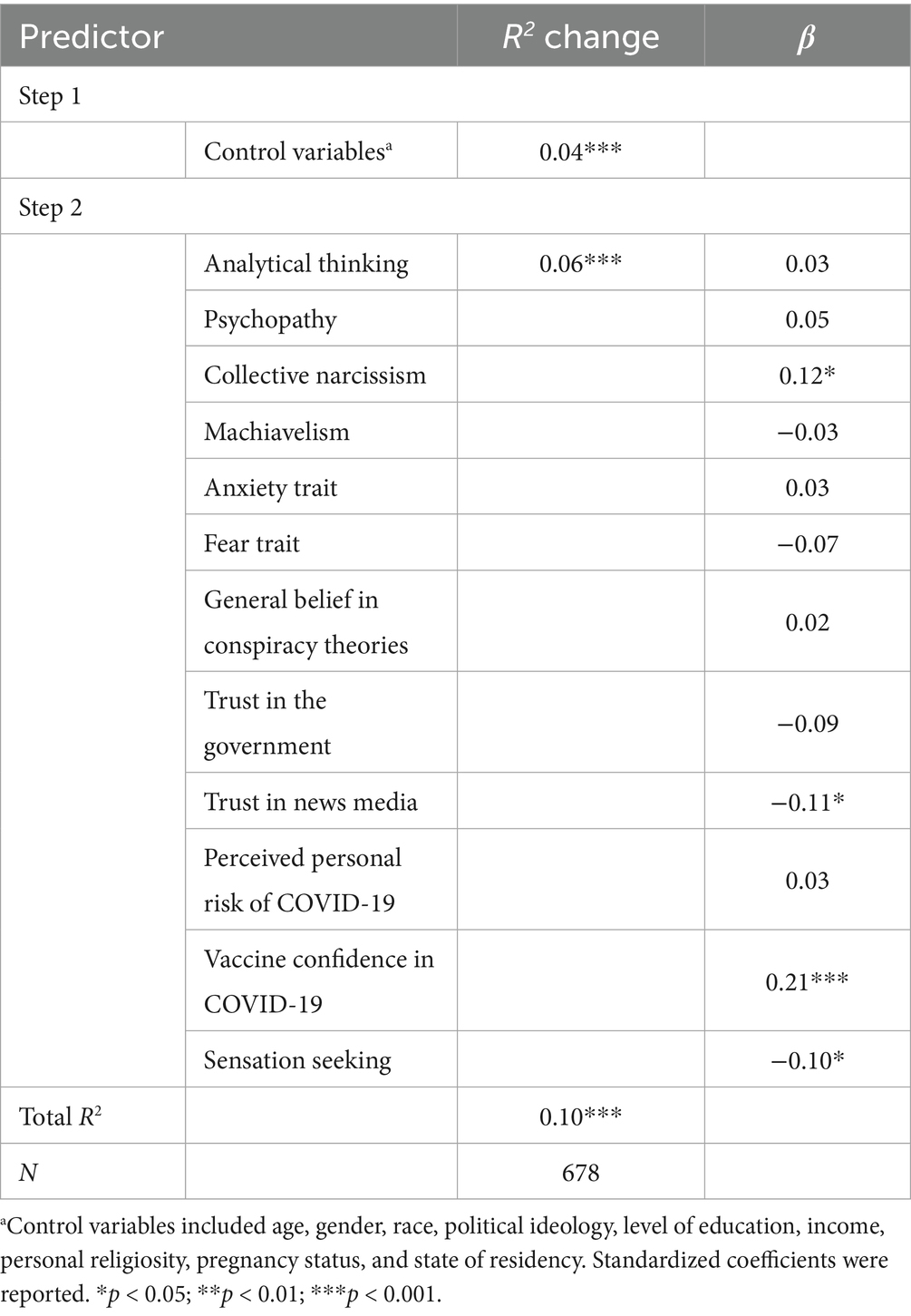
Table 4. Summary of hierarchical regression analysis predicting actual vaccination behavior.
Based on the results of RQ2, the strongest predictor of belief in COVID-19 CTs was the belief in other CTs (i.e., general CTs). RQ3 sought to investigate whether and how the beliefs in COVID-19 CTs mediate the relationship between belief in general CTs and health-related behaviors. The linear regression with the PROCESS macro model 4 was used to analyze how belief in general CTs influences proactive behavior, avoidance behavior, and actual vaccination behavior, respectively, through belief in COVID-19 CTs. The demographic factors, including age, sex, race, education, household income, political ideology, personal religiosity, pregnancy status, and state of residency, were controlled for. There was no significant direct effect of belief in general CTs. However, belief in COVID-19 CTs served as a significant predictor of avoidance behavior (b = −0.17, p < 0.001). We found a significant indirect effect of belief in general CTs on avoidance behavior through belief in COVID-19 CTs [point estimate = −0.15, BootSE = 0.04, Boot95% CI = (−0.23, −0.07)]. The relationship between belief in general CTs and avoidance behavior was fully mediated by belief in COVID-19 CTs (see Figure 1). Also, no significant mediation was detected on either the relationship between belief in general CTs and proactive behavior [point estimate = 0.01, BootSE = 0.03, Boot95% CI = (−0.05, 0.07)] or the relationship between belief in general CTs and actual vaccination behavior [point estimate = 0.00, BootSE = 0.02, Boot95% CI = (−0.03, 0.04)].
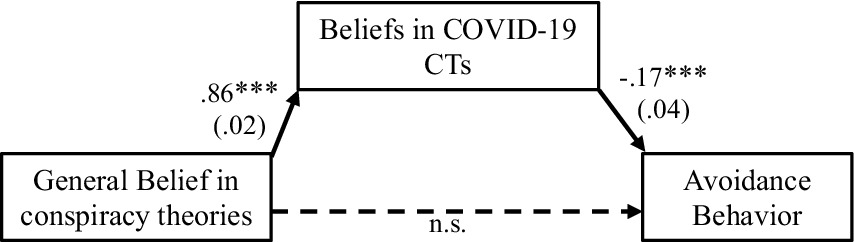
Figure 1. Mediation model with unstandardized coefficients. N = 880. Age, gender, race, education, household income, political ideology, personal religiosity, pregnancy status, and state of residency are included as exogenous variables and controlled in the model. However, the results associated with these variables are not included here in the Figure in the interest of presentation parsimony. Significant paths are presented with solid lines. Non-significant paths are presented with dotted lines. *p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study comprehensively examined individual-level predictors of COVID-19 conspiracy beliefs and related health behaviors in a national sample of U.S. adults. Skepticism can be productive and useful for democratic societies. Political philosophers argue that a skeptical way of believing is “an intellectual prerequisite of democracy” (p. 16) as it allows us to challenge the opinions of others, while demanding responsibility to consult reason and evidence when producing political judgments (Talisse, 2008). However, regular monitoring of the work of elites (e.g., through investigative journalism) and a healthy dose of civic suspicion toward the motives of those who hold positions of power differ from conspiratorial thinking, which tends to explain all social phenomena through the lens of grand conspiracies. Individuals engaged in this line of thinking exit the realm of skepticism to enter dogmatism, which avoids sources of disconfirmation in an attempt to preserve a preferred worldview. In these instances, CTs proper, as Baden and Sharon (2021) call them, become dangerous mutilations of ascertained knowledge. Such mutilations can saturate extremist and populist political discourses and gain pathological and paranoid qualities. This study showed the importance of studying conspiratorial beliefs in assessing new health communication phenomena, such as information disorders associated with COVID-19. According to Sellnow et al. (2019), information disorders are “intentionally and verifiably false” claims strategically distributed to broad audiences, resulting in disrupted public communication based on factual information and the normal discourse of renewal in risk and crises. They further cited that information disorders encompass “rumors, CTs and fabricated information” that, through digital connectivity, are broadly distributed and noticed due to their “shock value” (Wardle and Derakhshan, 2017, p. 10).
The results indicated that belief in other CTs best predicted whether an individual would be likely to believe that COVID-19 has been a product of a secret group of malevolent actors that pursues a hidden plot with the intent to secure or strengthen its own power. This variable emerged as the most important even when an entire set of other individual-level variables were entered into the equation, including demographics, psychopathological variables, emotion traits, cognitive variables, trust perceptions, and health-related variables. The predictive power of the model was high, as it explained significant 73% of variance in belief in COVID-19 CTs. Our research supports the findings of previous studies that people who believe in one CT are more likely to believe in another (e.g., Bruder et al., 2013; Dyrendal et al., 2021), which indicates a conspiracy spillover effect.
In addition, our results showed that the belief in COVID-19 CTs leads to lower avoidance behaviors such as social distancing, possibly because some CTs discourage this behavior. These findings not only support the findings of previous studies about congruency between attitudes and behaviors (see Ajzen and Sexton, 1999) but could also show a stronger general tendency to utilize CT as a generic explanation for social phenomena, including health-related ones. It also might suggest that a belief in CTs might be path-dependent, persisting alongside evidence that falsifies it. It might be that certain mental conspiratorial models are formed that are transferred and applied to explanations of the majority of social phenomena, especially the ones that are novel and thus subject to a plentitude of interpretations. The danger of possible path dependency in conspiratorial beliefs lies in the possibility that the dogmatic logic of explaining all phenomena by a conspiracy leaves no room for falsification. These findings underscore the complexity of the relationship between CTs and health behaviors and highlight how easily skepticism can devolve into harmful CTs that threaten public well-being.
Traditional approaches to correcting health misinformation may be insufficient to address the conspiracy theory spillover effect consistent with our study’s findings. Our results suggest that among U.S. adults, beliefs in other/general CTs lead to beliefs in specific CTs about one focal health issue (COVID-19). Further research should examine if this chain reaction of misbeliefs is true in other areas of health information. Additionally, given that most health misinformation correction focuses on correcting misperception (e.g., van der Meer and Jin, 2020), how to elevate misinformation correction at the misbelief management level needs to be further addressed by health communication scholars and practitioners. To prevent and/or contain the CT spillover effect as detected in our study, and to remove belief-system created obstacles in accurate health information dissemination, health agencies and public health information officers might consider implementing more proactive health literacy education, with an increased emphasis on debunking general CTs before new health issues emerge and intertwine with new specific CTs, prohibiting protective action taking. Interventions should aim to promote healthy skepticism that encourages critical thinking and informed decision-making in a democracy, while simultaneously combating the spread of dangerous CTs.
Our results further indicate that the perceived severity of COVID-19 was the best individual predictor for proactive health behavior, which included washing one’s hands appropriately and more often and covering one’s sneezes, as well as for avoidance behaviors, which included a range of COVID-19 avoidance measures, such as avoiding close contact with people who are sick and avoiding dining out. This indicates that among the large number of individual-level variables, perceived severity of a potentially deadly disease will outweigh all other factors in predicting some health-related behaviors. In other words, if individuals consider that a disease is severe and dangerous, regardless of their other psychopathological, emotional, cognitive, or trust characteristics, they are more likely to engage in a set of behavioral measures that would prevent such an outcome. Perceptions of disease threat are often closely compared to fear traits in predicting behavioral outcomes in health and medicine. Our findings indicate that fear traits were positively associated with predicting both proactive and avoidance behaviors, suggesting that individuals who are generally more fearful would engage more often in behaviors considered to help protect them from COVID-19. Although there is a considerable and impressive body of research in the area of health psychology that predicts health behaviors, perceptions of illness threat are one of the important factors of social-cognition models that examine various aspects of an individual’s cognitions to predict future health-related behaviors and outcomes (for review see Conner and Norman, 2005). Our study supports those claims for proactive and avoidance behavior regarding COVID-19. However, for actual vaccination behavior, our study found that confidence in COVID-19 vaccines was a better predictor. This finding aligns with the vaccine hesitation literature, which warned that misinformation about vaccines (e.g., false claims about the link between MMR and vaccine autism; false claims about the HPV vaccine) can impact immunization behavior (e.g., Chen et al., 2021; Gross, 2009). Further studies are needed to distinguish between possible singularity of willingness to vaccinate from other health-related behaviors and its connection to vaccines-related CTs.
Limitations and future directions
There are several limitations of the current study to be addressed in future studies. First, we collected data in October and November 2021, at one specific point in time, only during the ongoing, prolonged COVID-19 pandemic. Before and after the data collection time period, there have been informational, perceptual, and behavioral fluctuations among individuals and their responses to health communication messages. Longitudinal studies and/or temporal comparisons on how different clusters of factors impacting general and COVID-19-specific CTs and health-related behaviors will shed further light on the evolving pattern of CT spillover. Second, the current study was conducted among U.S. adults. Given the prevalence of CTs and their impacts across countries and contingents, the extent to which the strongest predictors of conspiratorial beliefs function and how the CT spillover effect mutates in different cultural and socio-economic contexts is yet to be fully examined. Third, the timing of the recruitment occurred after the vaccines were widely available and often mandated. In addition, our screener questions resulted in having predominantly those who have received two doses of vaccines (90.4%), while those who received one dose (4.3%) and unvaccinated individuals (5.3%) were in the minority. While those screener questions might have contributed to the avoidance of the ceiling effect in data and overrepresentation of those holding extreme views on COVID-19-related issues, they might have led to skewed results in the model with actual vaccination behavior. The results of this study regarding the actual vaccination model should thus be interpreted with this limitation in mind. Fourth, the sample of our study includes some demographic biases: Republicans (23.2%), Democrats (49.8%), and Independents (3.6%) relative to the U.S. population. Gallup data for 2021 showed that 27% of Americans declared themselves as Republicans, 42% as Independents, and 29% as Democrats (Gallup, 2024). Having in mind the smaller discrepancy between data for Republicans than between the data for Democrats and Independents, it is possible that in that particular point in time, in the peak of the COVID-19 crisis, and high political polarization in the country, more Independents were likely to proclaim themselves as Democrats possibly to side with Democrats’ policies on COVID-19. Although our study did not use political affiliation as a predictor variable, and has controlled for political affiliation to minimize bias, the authors acknowledge that the answers given to the questions in this study might have been painted overly by Democratic perspectives on COVID-19. However, it must be noted that the percentage of Independents in the US population has been relatively stable since 2011 (from 39 to 43%). The demographic profile of our study might indicate that in times of highly contentious public topics (such as COVID-19), the US population might shift toward expressing polarized opinions rather than nuanced reflection. Future studies should include meta-analyses of COVID-19 data to examine whether such polarization has been pronounced in other studies during the pandemic and provide a clear interpretation of the data. Finally, the cross-sectional survey data do not allow for the establishment of causal relationships. This study only identified correlations between independent and dependent variables. The authors limited potential response biases by question ordering in the actual survey (making sure that demographics go at the end, preceded by dependent variables), and by using adequate statistical analyses to control for a set of demographic variables, while examining the effects of independent variables on predictor variables. To establish robust casualty, future studies could use models with longitudinal data or an experimental design.
Data availability statement
The raw data supporting the conclusions of this article will be made available upon request from the authors.
Ethics statement
The studies involving humans were approved by University of Georgia Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
IP: Conceptualization, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. LK: Data curation, Writing – original draft. WZ: Formal analysis, Methodology, Visualization, Writing – original draft. XL: Formal analysis, Methodology, Visualization, Writing – original draft. YJ: Funding acquisition, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study has been supported by the funds from the Grady College of Journalism and Mass Communication, University of Georgia.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^Some participants declined to answer some of the questions in the survey, leading to a varied sample size across different variables. The sample size for each variable was shown alongside the measurement.
2. ^As a side analysis, we coded the results of our open-ended question which asked the participants to indicate the reason for which they vaccinated. The results indicated that most of them did it for prevention purposes – to protect themselves and their loved ones (54.7%), because they had a underlying health condition (11.2%), because they were forced to do so (7.1%), or because it was a smart thing to do and they trusted science (6.5%).
References
Ahmed, W., Vidal-Alaball, J., Downing, J., and Seguí, F. L. (2020). COVID-19 and the 5G conspiracy theory: social network analysis of twitter data. J. Med. Internet Res. 22:458. doi: 10.2196/19458
Ajzen, I., and Sexton, J. (1999). “Depth of processing, belief congruence, and attitude–behavior correspondence” in Dual-process theories in social psychology. eds. S. Chaiken and Y. Trope (New York, NY: Guilford Press), 117–138.
Allington, D., Duffy, B., Wessely, S., Dhavan, N., and Rubin, J. (2021). Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 51, 1763–1769. doi: 10.1017/S003329172000224X
Andrade, G. E., and Hussain, A. (2018). Polio in Pakistan: political, sociological, and epidemiological factors. Cureus 10:3502. doi: 10.7759/cureus.3502
Baden, C., and Sharon, T. (2021). Blinded by the lies? Toward an integrated definition of conspiracy theories. Commun. Theory 31, 82–106. doi: 10.1093/ct/qtaa023
Bernstein, D. A., and Allen, G. J. (1969). Fear survey schedule (II): normative data and factor analyses based upon a large college sample. Behav. Res. Ther. 7, 403–407. doi: 10.1016/0005-7967(69)90072-2
Bertin, P., Nera, K., and Delouvée, S. (2020). Conspiracy beliefs, rejection of vaccination, and support for hydroxychloroquine: a conceptual replication-extension in the COVID-19 pandemic context. Front. Psychol. 11:565128. doi: 10.3389/fpsyg.2020.565128
Betsch, C., and Böhm, R. (2016). Detrimental effects of introducing partial compulsory vaccination: experimental evidence. Eur J Public Health 26, 378–381. doi: 10.1093/eurpub/ckv154
Bierwiaczonek, K., Kunst, J. R., and Pich, O. (2020). Belief in COVID-19 conspiracy theories reduces social distancing over time. Appl. Psychol. Health Well Being 12, 1270–1285. doi: 10.1111/aphw.12223
Bogart, L. M., and Bird, S. T. (2003). Exploring the relationship of conspiracy beliefs about HIV/AIDS to sexual behaviors and attitudes among African-American adults. J. Natl. Med. Assoc. 95, 1057–1065
Brotherton, R., and French, C. C. (2014). Belief in conspiracy theories and susceptibility to the conjunction fallacy. Appl. Cogn. Psychol. 28, 238–248. doi: 10.1002/acp.2995
Brotherton, R., French, C. C., and Pickering, A. D. (2013). Measuring belief in conspiracy theories: the generic Conspiracist beliefs scale. Front. Psychol. 4:279. doi: 10.3389/fpsyg.2013.00279
Bruder, M., Haffke, P., Neave, N., Nouripanah, N., and Imhoff, R. (2013). Measuring individual differences in generic beliefs in conspiracy theories across cultures: conspiracy mentality questionnaire. Front. Psychol. 4:225. doi: 10.3389/fpsyg.2013.00225
Callaghan, T., Motta, M., Sylvester, S., Trujillo, K. L., and Blackburn, C. C. (2019). Parent psychology and the decision to delay childhood vaccination. Soc. Sci. Med. 238:112407. doi: 10.1016/j.socscimed.2019.112407
Chen, L., Zhang, Y., Young, R., Wu, X., and Zhu, G. (2021). Effects of vaccine-related conspiracy theories on Chinese young adults’ perceptions of the HPV vaccine: an experimental study. Health Commun. 36, 1343–1353. doi: 10.1080/10410236.2020.1751384
Cheruvu, V. K., Bhatta, M. P., and Drinkard, L. N. (2017). Factors associated with parental reasons for “no-intent” to vaccinate female adolescents with human papillomavirus vaccine: National Immunization Survey—teen 2008–2012. BMC Pediatr. 17:52. doi: 10.1186/s12887-017-0804-1
Chou, W. Y. S., and Budenz, A. (2020). Considering emotion in COVID-19 vaccine communication: addressing vaccine hesitancy and fostering vaccine confidence. Health Commun. 35, 1718–1722. doi: 10.1080/10410236.2020.1838096
Cillizza, C. (2022). Fact checking a strange new Covid conspiracy theory: athletes dying from vaccines. CNN. Available online at: https://www.cnn.com/2022/01/27/politics/ron-johnson-john-stockton-covid-comments
Conner, M., and Norman, P. (2005). Predicting health behaviour: Research and practice with social cognition models. 2nd Edn. Maidenhead, England: Open University Press.
Dahling, J. J., Whitaker, B. G., and Levy, P. E. (2009). The development and validation of a new Machiavellianism scale. J. Manag. 35, 219–257. doi: 10.1177/0149206308318618
de Zavala, A. G., Cichocka, A., Eidelson, R., and Jayawickreme, N. (2009). Collective narcissism and its social consequences. J. Pers. Soc. Psychol. 97, 1074–1096. doi: 10.1037/a0016904
de Zavala, A. G., Federico, C. M., Sedikides, C., Guerra, R., Lantos, D., Mroziński, B., et al. (2020). Low self-esteem predicts out-group derogation via collective narcissism, but this relationship is obscured by in-group satisfaction. J. Pers. Soc. Psychol. 119, 741–764. doi: 10.1037/pspp0000260
Dickson, E. J. (2020). Anti-vax doctor promotes conspiracy theory that death certificates falsely cite COVID-19. Rolling Stone. Available online at: https://www.rollingstone.com/culture/culture-features/anti-vax-doctor-covid-19-death-certificates-984407/
Dye, J. (2014). Pfizer confronts surge of lawsuits over Lipitor. Reuters. Available online at: https://www.reuters.com/article/us-pfizer-lipitor-lawsuits-insight/pfizer-confronts-surge-of-lawsuits-over-lipitor-idUSKBN0G80E520140808\
Dyer, C. (1988). Judge “not satisfied” that whooping cough vaccine causes permanent brain damage. Br. Med. J. 296, 1189–1190. doi: 10.1136/bmj.296.6630.1189
Dyrendal, A., Kennair, L. E. O., and Bendixen, M. (2021). Predictors of belief in conspiracy theory: the role of individual differences in schizotypal traits, paranormal beliefs, social dominance orientation, right wing authoritarianism and conspiracy mentality. Personal. Individ. Differ. 173:110645. doi: 10.1016/j.paid.2021.110645
Enders, A. M., Uscinski, J. E., Klofstad, C., and Stoler, J. (2020). The different forms of COVID-19 misinformation and their consequences. Harvard Kennedy School Misinform Rev. 1:48. doi: 10.37016/mr-2020-48
Ernst, E. (2019). Alternative medicine: A critical assessment of 150 modalities. Cham, Switzerland: Springer.
Frankovic, K. (2021). Why won’t Americans get vaccinated? YouGov. Available online at: https://today.yougov.com/politics/articles/37052-why-wont-americans-get-vaccinated-poll-data
Frenkel, S., Decker, B., and Alba, D. (2020). How the ‘Plandemic’ movie and its falsehoods spread widely online. The New York Times.
Gallup. (2024). Party affiliation. Gallup Historical Trends. Available online at: https://news.gallup.com/poll/15370/party-affiliation.aspx
Gharpure, R., Hunter, C. M., Schnall, A. H., Barrett, C. E., Kirby, A. E., Kunz, J., et al. (2020). Knowledge and practices regarding safe household cleaning and disinfection for COVID-19 prevention—United States, may 2020. Am. J. Transplant. 20, 2946–2950. doi: 10.1111/ajt.16300
Goertzel, T. (2010). Conspiracy theories in science: conspiracy theories that target specific research can have serious consequences for public health and environmental policies. EMBO Rep. 11, 493–499. doi: 10.1038/embor.2010.84
Gross, L. (2009). A broken trust: lessons from the vaccine–autism wars. PLoS Biol. 7:e1000114. doi: 10.1371/journal.pbio.1000114
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York, NY (Hayes) and Cham, Switzerland (Hellinger): Guilford Press.
Hellinger, D. C. (2019). Conspiracies and conspiracy theories in the age of trump : Palgrave Macmillan.
Hornsey, M. J., Finlayson, M., Chatwood, G., and Begeny, C. T. (2020). Donald Trump and vaccination: the effect of political identity, conspiracist ideation and presidential tweets on vaccine hesitancy. J. Exp. Soc. Psychol. 88:103947. doi: 10.1016/j.jesp.2019.103947
Hoyle, R. H., Stephenson, M. T., Palmgreen, P., Lorch, E. P., and Donohew, R. L. (2002). Reliability and validity of a brief measure of sensation seeking. Personal. Individ. Differ. 32, 401–414. doi: 10.1016/S0191-8869(01)00032-0
Hughes, S., and Machan, L. (2021). It’s a conspiracy: COVID-19 conspiracies link to psychopathy, Machiavellianism and collective narcissism. Personal. Individ. Differ. 171:110559. doi: 10.1016/j.paid.2020.110559
Imhoff, R., and Lamberty, P. (2020). A bioweapon or a hoax? The link between distinct conspiracy beliefs about the coronavirus disease (COVID-19) outbreak and pandemic behavior. Soc. Psychol. Personal. Sci. 11, 1110–1118. doi: 10.1177/1948550620934692
Jolley, D., and Douglas, K. M. (2014). The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS One 9:e89177. doi: 10.1371/journal.pone.0089177
Kang, S. J., and Jung, S. I. (2020). Age-related morbidity and mortality among patients with COVID-19. Infect Chemother 52, 154–164. doi: 10.3947/ic.2020.52.2.154
Knight, P. (2013). Conspiracy theories in the United States: An encyclopedia. New York, NY: Routledge.
Kohring, M., and Matthes, J. (2007). Trust in news media: development and validation of a multidimensional scale. Commun. Res. 34, 231–252. doi: 10.1177/0093650206298071
Levenson, M., Kiehl, K., and Fitzpatrick, C. (1995). Assessing psychopathic attributes in a noninstitutionalized population. J. Pers. Soc. Psychol. 68, 151–158. doi: 10.1037/0022-3514.68.1.151
Lukito, J. (2020). Coordinating a multi-platform disinformation campaign: internet research agency activity on three U.S. social media platforms, 2015 to 2017. Polit. Commun. 37, 238–255. doi: 10.1080/10584609.2019.1661889
Mannan, D. K. A., and Farhana, K. M. (2020). Knowledge, attitude and acceptance of a COVID-19 vaccine: a global cross-sectional study. Int Res J Bus Soc Sci 6, 1–23. doi: 10.2139/ssrn.3763373
Marinthe, G., Brown, G., Delouvée, S., and Jolley, D. (2020). Looking out for myself: exploring the relationship between conspiracy mentality, perceived personal risk, and COVID-19 prevention measures. Br. J. Health Psychol. 25, 957–980. doi: 10.1111/bjhp.12449
Mills, E., Jadad, A., Ross, C., and Wilson, K. (2005). Systematic review of qualitative studies exploring parental beliefs and attitudes toward childhood vaccination identifies common barriers to vaccination. J. Clin. Epidemiol. 58, 1081–1088. doi: 10.1016/j.jclinepi.2005.09.002
Mitchell, A., Jurkowitz, M., Oliphant, B., and Shearer, E. (2020) “Three months in, many Americans see exaggeration, conspiracy theories and partisanship in COVID-19 news.” Pew Research Center’s Journalism Project. Available online at: www.pewresearch.org/journalism/2020/06/29/three-months-in-many-americans-see-exaggeration-conspiracy-theories-and-partisanship-in-covid-19-news/.
Motta, M., Stecula, D., and Farhart, C. (2020). How right-leaning media coverage of COVID-19 facilitated the spread of misinformation in the early stages of the pandemic in the U.S. Can. J. Polit. Sci. 53, 335–342. doi: 10.1017/S0008423920000396
Natoli, E. E., and Marques, M. D. (2021). The antidepressant hoax: conspiracy theories decrease health-seeking intentions. Br. J. Soc. Psychol. 60, 902–923. doi: 10.1111/bjso.12426
Nowak, G. J., Cacciatore, M. A., and Len-Ríos, M. E. (2018). Understanding and increasing influenza vaccination acceptance: insights from a 2016 National Survey of U.S. adults. Int. J. Environ. Res. Public Health 15:711. doi: 10.3390/ijerph15040711
Oliver, J. E., and Wood, T. J. (2014). Conspiracy theories and the paranoid style(s) of mass opinion. Am. J. Polit. Sci. 58, 952–966. doi: 10.1111/ajps.12084
Pennycook, G., McPhetres, J., Zhang, Y., Lu, J. G., and Rand, D. G. (2020). Fighting COVID-19 misinformation on social media: experimental evidence for a scalable accuracy-nudge intervention. Psychol. Sci. 31, 770–780. doi: 10.1177/0956797620939054
Pluviano, S., Della Sala, S., and Watt, C. (2020). The effects of source expertise and trustworthiness on recollection: the case of vaccine misinformation. Cogn. Process. 21, 321–330. doi: 10.1007/s10339-020-00974-8
Pluviano, S., Watt, C., and Della Sala, S. (2017). Misinformation lingers in memory: failure of three pro-vaccination strategies. PLoS One 12:640. doi: 10.1371/journal.pone.0181640
Popken, B. (2016). Mylan CEO’S pay rose over 600 percent as EpiPen price rose 400 percent. NBC News. Available online at: https://www.nbcnews.com/business/consumer/mylan-execs-gave-themselves-raises-they-hiked-epipen-prices-n636591
Roisman, J. (2006). The rhetoric of conspiracy in ancient Athens. Berkeley, CA (Roisman) and Washington, DC (Schaeffer): University of California Press.
Romer, D., and Jamieson, K. H. (2020). Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc. Sci. Med. 263:113356. doi: 10.1016/j.socscimed.2020.113356
Rouan, R. (2021). Fact check: CDC is not inflating the COVID-19 death count. USA Today. Available online at: https://www.usatoday.com/story/news/factcheck/2021/02/16/fact-check-cdc-not-inflating-covid-19-deaths/6764078002/
Schaeffer, K. (2020). A look at the Americans who believe there is some truth to the conspiracy theory that COVID-19 was planned : Pew Research Center.
Sellnow, T. L., Parrish, A., and Semenas, L. (2019). From hoax as crisis to crisis as hoax: fake news and information disorder as disruptions to the discourse of renewal. J Int Crisis Risk Commun 2, 121–142. doi: 10.30658/jicrcr.2.1.6
Simione, L., Vagni, M., Gnagnarella, C., Bersani, G., and Pajardi, D. (2021). Mistrust and beliefs in conspiracy theories differently mediate the effects of psychological factors on propensity for COVID-19 vaccine. Front. Psychol. 12:683684. doi: 10.3389/fpsyg.2021.683684
Sun, R., Wang, X., Lin, L., Zhang, N., Li, L., and Zhou, X. (2021). The impact of negative emotional reactions on parental vaccine hesitancy after the 2018 vaccine event in China: a cross-sectional survey. Hum. Vaccin. Immunother. 17, 3042–3051. doi: 10.1080/21645515.2021.1907149
Sunstein, C. R., and Vermeule, A. (2009). Conspiracy theories: causes and cures. J. Polit. Philos. 17, 202–227. doi: 10.1111/j.1467-9760.2008.00325.x
Talisse, R. B. (2008). Skepticism and the democratic ideal. Think 6, 7–18. doi: 10.1017/S1477175600002359
Tomljenovic, H., Bubic, A., and Erceg, N. (2020). It just doesn’t feel right – the relevance of emotions and intuition for parental vaccine conspiracy beliefs and vaccination uptake. Psychol. Health 35, 538–554. doi: 10.1080/08870446.2019.1673894
University of Bristol and King’s College London (2021). Coronavirus conspiracies and views of vaccination. Available online at: https://www.kcl.ac.uk/policy-institute/assets/coronavirus-conspiracies-and-views-of-vaccination.pdf
Uscinski, J. E., and Parent, J. M. (2014). American conspiracy theories. New York, NY: Oxford University Press.
van der Linden, S., Roozenbeek, J., Maertens, R., Basol, M., Kácha, O., Rathje, S., et al. (2021). How can psychological science help counter the spread of fake news? Span. J. Psychol. 24:e25. doi: 10.1017/SJP.2021.23
van der Meer, T. G. L. A., and Jin, Y. (2020). Seeking formula for misinformation treatment in public health crises: the effects of corrective information type and source. Health Commun. 35, 560–575. doi: 10.1080/10410236.2019.1573295
van Mulukom, V., Pummerer, L. J., Alper, S., Bai, H., Čavojová, V., Farias, J., et al. (2022). Antecedents and consequences of COVID-19 conspiracy beliefs: a systematic review. Soc. Sci. Med. 301:114912. doi: 10.1016/j.socscimed.2022.114912
Vijaykumar, S., Jin, Y., Rogeson, D., Lu, X., Sharma, S., Maughan, A., et al. (2021). How shades of truth and age affect responses to COVID-19 (mis)information: randomized survey experiment among WhatsApp users in UK and Brazil. Humanities and Social Sciences Communications 8:88. doi: 10.1057/s41599-021-00749-0
Von Rueden, C., and Van Vugt, M. (2015). Leadership in small-scale societies: some implications for theory, research, and practice. Leadersh. Q. 26, 978–990. doi: 10.1016/j.leaqua.2015.10.004
Wardle, C., and Derakhshan, H. (2017). Information disorder: Toward an interdisciplinary framework for research and policymaking. Strasbourg, France: Council of Europe.
Webb, G. (2019). Dark alliance: The CIA, the contras, and the cocaine explosion. New York, NY: Seven Stories Press.
Wood, M. J., and Douglas, K. M. (2015). Online communication as a window to conspiracist worldviews. Front. Psychol. 6:836. doi: 10.3389/fpsyg.2015.00836
Zhao, X., and Tsang, S. J. (2022). Self-protection by fact-checking: how pandemic information seeking and verifying affect preventive behaviors. J Contingenc Crisis Manage 30, 171–184. doi: 10.1111/1468-5973.12372
Keywords: conspiracy theories, COVID-19, health behaviors, spillover effect, public health
Citation: Pjesivac I, Klein L, Zhao W, Lu X and Jin Y (2025) Examining conspiracy theory spillover in the health communication arena: factors that impact COVID-19 conspiratorial beliefs and health-related behaviors. Front. Commun. 10:1548575. doi: 10.3389/fcomm.2025.1548575
Edited by:
Christopher McKinley, Montclair State University, United StatesReviewed by:
Yi Luo, Montclair State University, United StatesEnzo Loner, University of Trento, Italy
Copyright © 2025 Pjesivac, Klein, Zhao, Lu and Jin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ivanka Pjesivac, aXZhbmthQHVnYS5lZHU=