 Jiajing Zhai
Jiajing Zhai Jiaqi Ou
Jiaqi Ou Jinghong Nie2*
Jinghong Nie2*- 1Film-Television & Communication College, Shanghai Normal University, Shanghai, China
- 2School of Journalism and Communication, Sun Yat-sen University, Guangzhou, Guangdong Province, China
This study investigates how conflicting health evidence shapes cancer-screening information avoidance through the lens of compensatory control theory. We conducted a 5 × 2 between-subjects online experiment (Credamo, China; N = 372, 67% female; Mage = 30.4) in which participants were randomly assigned to read thyroid-screening articles that manipulated evidence conflict (no conflict, statistical conflict, anecdotal conflict, or cross-valence: statistics-support/anecdotes-oppose vs. anecdotes-support/statistics-oppose) and perceived disease control (high vs. low). The dependent variable was health-information avoidance, with message elaboration and ambiguity aversion as mediators. Moderated mediation analyses revealed a clear defensive pathway under low perceived control: conflict increased ambiguity aversion, which in turn increased avoidance (indirect effect = 0.025, 95% CI [0.007, 0.045]). In contrast, the hypothesized engagement pathway via increased elaboration under high control was not supported in the overall model, although a positive relationship between conflict and elaboration was observed in the high-control group. These findings suggest that perceived control shapes whether conflict prompts deeper engagement or defensive withdrawal. Practically, communicators may reduce avoidance by aligning anecdotal and statistical cues—or by embedding control-boosting frames—when targeting low-control audiences.
Introduction
Given the phased evolution of scientific evidence and the incremental updates of clinical guidelines, the emergence of conflicting health information in the news media is both common and consequential (Kaufhold et al., 2020; Zimbres et al., 2021). This is particularly evident in cancer screening, where competing viewpoints and the absence of clear consensus frequently generate contradictory messages (Iles et al., 2022). With the rise of internet platforms and social media, such conflicting information has become more visible and widely disseminated, exposing audiences to inconsistent health messages from public health organizations, news outlets, and lay individuals alike (Gustafson and Rice, 2020).
Prior studies document effects of conflicting health information but rarely distinguish anecdotal–statistical cross-valence conflicts or explain when conflict reduces vs. increases avoidance; “Evidence conflict” refers to the inconsistency between messages that differ in the type or valence of evidence, such as anecdotal (personal stories) versus statistical (probabilistic data) information, or cases where the two types of evidence point to opposing conclusions (Carpenter and Han, 2020). This type of conflict is especially prevalent in cancer communication, where anecdotal narratives often circulate alongside probabilistic evidence. A key outcome of such exposure is information avoidance, or individuals’ tendency to disengage from or resist further health information when faced with conflicting messages (Howell and Shepperd, 2013).
The role of perceived disease control as a boundary condition and elaboration/ambiguity aversion as mechanisms remains untested. Given that reactions to conflicting health information may depend on the type and presentation of such evidence (Carpenter and Han, 2020; Nagler and LoRusso, 2017). Making nuanced distinctions among types of conflicting information can enhance conceptual and theoretical understanding, improve methodological consistency, and facilitate more accurate predictions of audience responses (Gustafson and Rice, 2020). This study addresses these gaps by applying compensatory control theory to investigate how evidence conflict (anecdotal vs. statistical, same-valence vs. cross-valence) influences audience responses to thyroid cancer screening information on social media. Specifically, we examine whether perceived disease control moderates the relationship between evidence conflict and information avoidance, and whether elaboration and ambiguity aversion serve as mediating mechanisms (Figure 1 shows the conceptual model). In doing so, our study advances both theoretical understanding of conflicting health information and practical strategies for reducing its negative impact on health communication.
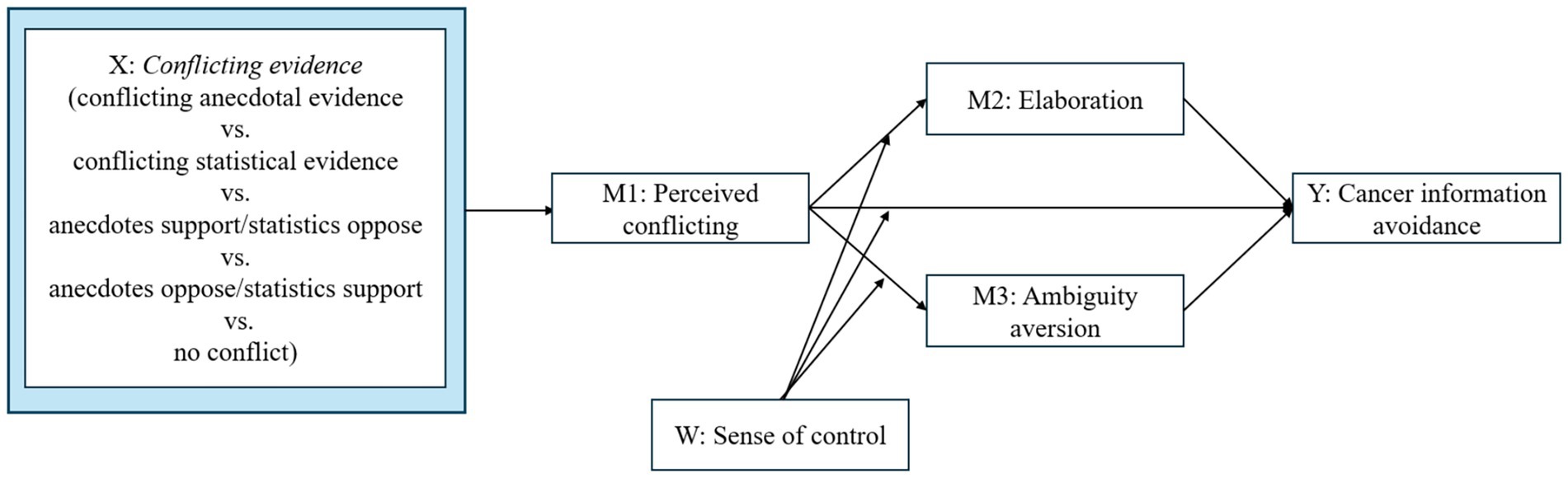
Figure 1. Conceptual model.
Literature review
The nature of evidence conflict and perceived conflict
The public’s encounter with conflicting health information is a common yet challenging experience (Freling et al., 2014). These conflicts often manifest as disagreements between different types of evidence, creating a complex landscape for decision-making. Normative models suggest that individuals should prioritize statistical evidence—valued for its objectivity and scientific robustness derived from large samples (De Wit et al., 2008; Raghubir and Menon, 1996) —over anecdotal evidence. In line with this, presenting statistical information can mitigate the undue influence of anecdotal reasoning (Fagerlin et al., 2005), and anecdotal evidence is generally considered less credible than statistical data in scientific discourse (Chinn and Weeks, 2021).
However, a substantial body of research reveals a pervasive “anecdotal advantage” that contradicts normative models. Cognitive biases, such as the “law of small numbers” (Tversky and Kahneman, 1971), lead individuals to overvalue vivid, concrete anecdotes while undervaluing abstract statistics (Michal et al., 2021). For instance, personal stories that contradict strong statistical evidence can undermine the persuasive power of that evidence and decrease confidence in treatment outcomes (Jaramillo et al., 2019). This effect is particularly potent in health contexts, such as vaccine persuasion (Nissel and Woolley, 2024). These findings suggest that the type of evidence in conflict—whether an anecdote challenges a statistic or vice versa—may modulate the intensity of the public’s response.
Despite these nuances in evidence type, a foundational consensus across the literature is that the mere presence of conflicting information acts as a salient risk cue (Dootson et al., 2022; Li et al., 2020). This perception of conflict can prompt defensive reactions, such as confusion, information overload, fatalism (Jensen et al., 2014; Niederdeppe and Levy, 2007), and a preference for avoiding inconsistent information (Burton et al., 1999). Therefore, while the specific configuration of evidence may influence the degree of response, the primary driver is the existence of conflict itself. Based on this core premise, we hypothesize:
H1: Compared to the non-conflict information group, evidence conflict will increase participants’ perceived level of conflict.
From conflict to avoidance: the dual mediating pathways
The perception of conflict (as posited in H1) does not directly lead to behavioral outcomes like information avoidance; rather, it triggers distinct psychological processes. This study proposes two parallel mediating pathways: one cognitive and one affective.
On one hand, conflicting information can overwhelm an individual’s cognitive capacity. Theories such as the Extended Parallel Process Model (EPPM) and the Carryover Effects Hypothesis indicate that conflict diminishes cognitive engagement. Exposure to conflicting cancer screening information, for example, decreases self-efficacy and response efficacy, reducing the willingness for prevention (Marshall and Comello, 2019). This conflict fosters confusion and skepticism (Nagler, 2014; Nagler et al., 2022), which hampers the integration of new information (D’mello et al., 2014) and can impair cognitive function through heightened concern (Barnwell et al., 2023), ultimately leading to lower levels of information elaboration (Huang et al., 2023).
On the other hand, conflict also triggers an affective-evaluative response rooted in ambiguity aversion. When information is contradictory, the resulting state of ambiguity can lead to pessimistic risk assessments and decision avoidance (Klein et al., 2010). Health conflicts represent a significant source of scientific uncertainty, and communicating such uncertainty heightens risk perception, which in turn elicits a strong aversion to ambiguity (Han et al., 2018; Viscusi et al., 1991). This aversion drives individuals to avoid the ambiguous information altogether.
The moderating role of perceived disease control
We introduce perceived disease control, grounded in Compensatory Control Theory (Kay et al., 2009), as a pivotal moderator that determines which of these two psychological pathways—reduced elaboration or heightened ambiguity aversion—is activated in response to conflict. This theory posits that states of randomness and uncertainty induce psychological stress, motivating efforts to restore order and structure. Individuals with lower perceived control have a greater need for simple, clear explanations and are particularly intolerant of ambiguity (Ma and Kay, 2017).
Conversely, a strong sense of disease control is a vital cognitive resource. It helps ensure that cognitive resources remain available (Skinner, 1995), facilitates beneficial cognitive evaluations (Taylor and Armor, 1996), and promotes active engagement in health behaviors like cancer screening (Henselmans et al., 2010). Individuals with high control are motivated and able to process information more deeply (Briñol et al., 2017; Magee, 2009) and are less averse to ambiguity when they believe they can control the outcome (Stuart et al., 2022). Enhancing perceived control helps mitigate health threats (Goldzweig et al., 2016) and reduces feelings of vulnerability (Lecci and Cohen, 2007).
Therefore, we propose that perceived disease control acts as a switch: it determines whether an individual responds to conflict with engaged processing (the elaboration pathway) or defensive avoidance (the ambiguity aversion pathway).
The present research and hypotheses
Integrating the above, this study examines a moderated mediation model. We propose that the effect of evidence conflict on information avoidance is mediated by either increased elaboration or increased ambiguity aversion, and that the dominant pathway depends on an individual’s level of perceived disease control.
The specific hypotheses are as follows:
H2: Perceived disease control will moderate the effect of perceived conflict on information avoidance, such that the positive effect of perceived conflict on avoidance will be weaker for individuals with high disease control.
H3: For individuals with high disease control, perceived conflict will decrease information avoidance by increasing cognitive elaboration.
H4: For individuals with low disease control, perceived conflict will increase information avoidance by increasing ambiguity aversion.
Method
Procedure and stimulus
Participants, design, and procedure
The experimental protocols were approved by the Sun Yat-sen University Institutional Review Board (IRB) in February 2024. The sample size was predetermined, and a sensitivity power analysis (Faul et al., 2009) indicated that small-to-medium effect sizes could be detected with a power of 0.80. The study employed a 5 × 2 between-subjects design: evidence condition × disease-control prime. A total of 372 adult participants were recruited via Credamo,1 with each receiving a compensation of 5 yuan for participation. Participants (67% female, Mage = 30.4) were randomly assigned to one of ten experimental conditions, corresponding to five types of conflicting evidence (no conflict; statistical evidence conflict; anecdotal evidence conflict; conflict in which statistical evidence supports but anecdotal evidence opposes; conflict in which anecdotal evidence supports but statistical evidence opposes) crossed with two levels of perceived disease control (high vs. low). Randomization was implemented automatically through Credamo’s algorithm. After providing informed consent, participants read a news article discussing the pros and cons of thyroid cancer screening. Those who failed attention checks, provided incomplete responses, or wrote nonsensical answers during the thought-listing task were excluded. The final analytic sample comprised N = 342, with per-cell sample sizes ranging from 32 to 35.
Stimulus
In the no-conflict group, both anecdotal and statistical evidence supported thyroid cancer screening. In the statistical conflict group, there was both supporting and opposing statistical evidence. The anecdotal conflict group featured conflicting anecdotal evidence. The supporting anecdotal evidence emphasized that “thyroid cancer is often asymptomatic, and regular screenings can improve early detection.” The statistical evidence reinforced this by stating that “regular screenings can enhance early detection and cure rates.” In contrast, the opposing anecdotal evidence highlighted that “most thyroid cancers have a low risk of progression, and overdiagnosis can cause psychological distress.” The opposing statistical evidence echoed this concern. Conflicting evidence was presented in a counterbalanced order to minimize order effects (see Table 1). All 10 materials were titled “Is thyroid cancer screening necessary?” and contained 490–500 characters, formatted to resemble the style of “Life Times,” a popular health media outlet in China. The complete stimulus materials are provided in the Supplementary Information.
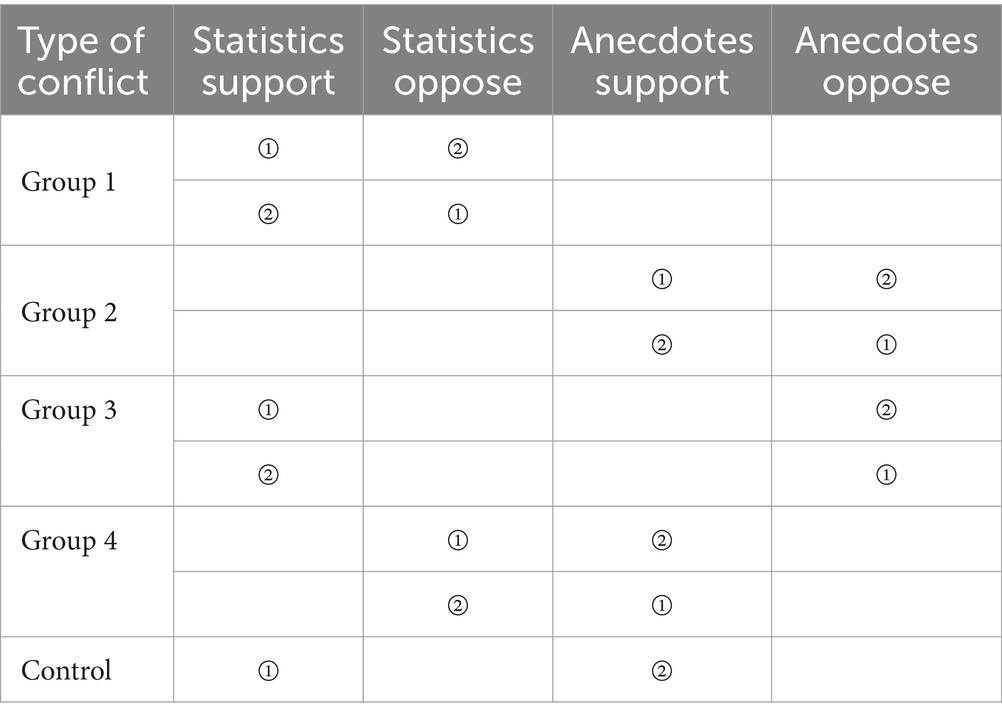
Table 1. Overview of manipulation groups.
The manipulation of disease control was informed by the study conducted by Teachman et al. (2003). In this context, participants in the low control group were presented with materials attributing the primary causes of thyroid cancer to genetic factors and elevated estrogen levels. Conversely, participants in the high control group read materials suggesting that poor personal lifestyle choices and emotional factors are the main contributors to the onset of thyroid cancer, emphasizing that maintaining healthy habits and emotional well-being can serve as preventive measures. Both materials featured the title “Why Do People Develop Thyroid Cancer? The Role of These Two Factors,” with each article comprising a total of 277 characters. Participants in the low disease control group read an article highlighting the potential for lifestyle improvements to prevent thyroid cancer, while those in the high disease control group were exposed to an article asserting that genetic and other uncontrollable factors determine the likelihood of developing thyroid cancer. To enhance the credibility of the manipulation, we structured the prime to indicate that 85.5% of the causes of obesity could be attributed to either environmental and genetic factors or individual behavioral factors, with the remaining 14.5% attributed to other influences.
Variables and measurements
Perceived conflict
This measure was adopted from previous studies (Lee and Shi, 2022; Flemming et al., 2015). Respondents indicated the extent to which they agreed with three statements regarding to the articles on a 1 (“strongly disagree”) to 7 (“strongly agree”) scale. The following statements were included: “There are so many different recommendations about thyroid cancer screening, it is hard to know which one to follow,” “The texts contradict each other,” “After reading the texts, I find it hard to deliver a concluding judgment on whether thyroid cancer screening is necessary” (Cronbach’s α = 0.90).
Elaboration
Following the methodologies employed by previous research (Shen and Dillard, 2009), participants were asked to list any thoughts that came to mind while reading the message in an open-ended format. An index of elaboration was created by summing the number of negative thoughts and positive thoughts that each participant generated. Finally, two coders independently coded 20% of the texts, and after discussion, their inter-coder reliability was established at 0.86, indicating good reliability, which is deemed suitable for coding the remaining content.
Ambiguity aversion
The variable of perceived ambiguity aversion, as experienced by participants while reading the article, was assessed using a seven-point Likert scale based on established measurement instruments (McLain, 2009). Participants were asked to express their views on statements such as “I find it difficult to tolerate ambiguous recommendations regarding thyroid cancer screening,” “I dislike ambiguous recommendations about thyroid cancer screening,” and “I prefer recommendations that present a clear ‘best’ solution for thyroid cancer screening.” The scale consisted of five items (1 = strongly disagree, 7 = strongly agree), and it demonstrated an internal consistency reliability of 0.90.
Cancer screening information avoidance
The variable measuring participants’ willingness to avoid health information after reading the article was adapted from the scale of Howell and Shepperd (2013). Participants’ views were assessed using a seven-point Likert scale, which included statements such as “I would rather not know about thyroid cancer screening,” “I would avoid learning about thyroid cancer screening,” “Even if it will upset me, I want to know about thyroid cancer screening (R).” “I want to know about thyroid cancer screening. (R)” “It is important to know about thyroid cancer screening (R).” and “Even if the results might upset me, I still want to know about thyroid cancer screening (R).” The scale consisted of five items (1 = strongly disagree, 7 = strongly agree), with a Cronbach’s α of 0.85.
Results
To test H1 and H2, we conducted OLS regression models with preregistered predictors and controls. To test the indirect effect hypothesized in H3 and H4, we used PROCESS Model 4 (Hayes, 2018) with 5,000 bootstrap resamples. All variables, hypotheses, and analytic procedures were specified in advance to ensure transparency and replicability.
Manipulation checks
Drawing on methodologies from prior studies on information conflict, we implemented a comprehension check after participants completed the evidence conflict article. This check consisted of one item that assessed participants’ understanding of the manipulated evidence conflict. Participants were presented with five options: “There is statistical evidence supporting thyroid cancer screening, but also statistical evidence opposing it,” “There is statistical evidence supporting thyroid cancer screening, but anecdotal evidence against it,” “There is anecdotal evidence supporting thyroid cancer screening, but statistical evidence opposing it,” “There is anecdotal evidence supporting thyroid cancer screening, but also anecdotal evidence against it,” and “Both statistical and anecdotal evidence support thyroid cancer screening.” Participants passed the manipulation check only if their selection exactly matched their assigned condition—a binary (correct/incorrect) coding based on the accurate identification of the evidence conflict. This check was passed by 99.3% of participants, confirming a successful manipulation.
To assess the manipulation of perceived cancer control, we adapted the approach of Teachman et al. (2003). Following their reading of the article designed to manipulate perceptions of cancer control, participants were asked, “What do you believe are the primary causes of cancer?” Their open-ended responses were then coded to indicate whether the reported factors were perceived as controllable or uncontrollable (e.g., lifestyle choices versus genetic factors). Participants who provided responses consistent with the intended manipulation passed the check, with a correct response rate of 98.3%, indicating successful manipulation.
Cancer information avoidance (dependent variable)
This study employed a univariate analysis of variance (ANOVA) to examine the effects of evidence conflict (five conditions: no conflict group, anecdotal conflict group, anecdotal support with statistical opposition group, statistical support with anecdotal opposition group, and statistical conflict group) and perceived control (two levels: low perceived control and high perceived control) on participants’ willingness to avoid health information. The results indicate a significant main effect of evidence conflict on the willingness to avoid health information [F(4, 336) = 4.94, p < 0.001]. Additionally, the main effect of perceived control was significant [F(1, 336) = 10.75, p < 0.001]. Furthermore, the interaction between evidence conflict and perceived control significantly influenced the willingness to avoid health information [F(4, 336) = 3.16, p < 0.05] (Figure 2).
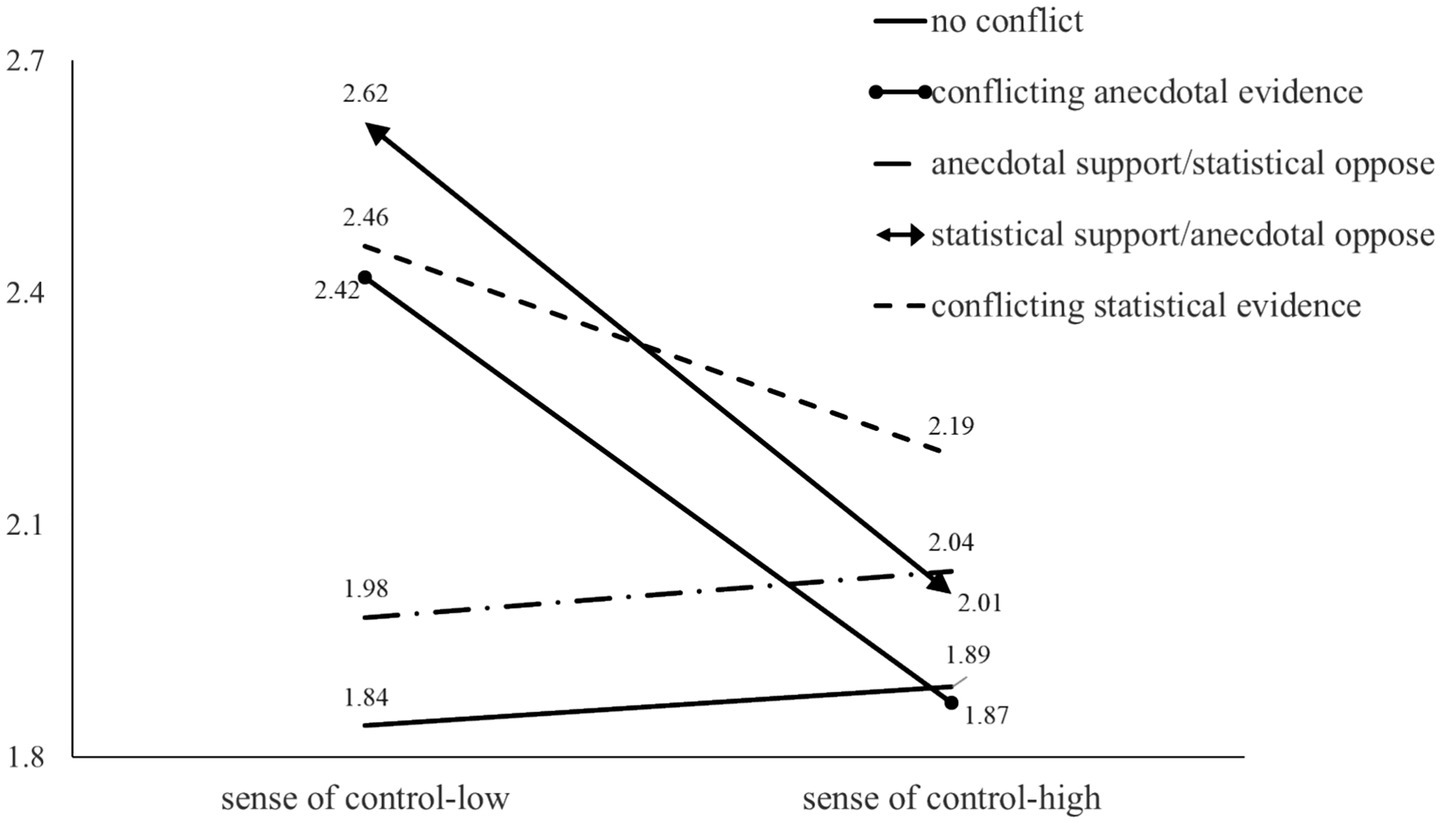
Figure 2. The impact of evidence conflict and perceived control on information avoidance willingness.
The simple effects analysis revealed that, under conditions of low perceived control, participants demonstrated a higher willingness to avoid health information in the anecdotal conflict group (M_anecdotal conflict = 2.42, SD_anecdotal conflict = 1.21, p < 0.01), the statistical support but anecdotal opposition group (M_statistical support but anecdotal opposition = 2.62, SD_statistical support but anecdotal opposition = 0.12, p < 0.001), and the statistical conflict group (M_statistical conflict = 2.46, SD_statistical conflict = 0.12, p < 0.001) compared to the no conflict group (M_no conflict = 1.84, SD_no conflict = 0.13). However, there was no significant difference in willingness to avoid health information between the no conflict group and the anecdotal support but statistical opposition group (M_anecdotal support but statistical opposition = 1.98, SD_anecdotal support but statistical opposition = 1.21, p = 0.41).
In contrast, under conditions of high perceived control, no significant differences were found in willingness to avoid health information between the no conflict group and the anecdotal conflict group (M_anecdotal conflict = 1.87, SD_anecdotal conflict = 1.42, p = 0.19), the anecdotal support but statistical opposition group (M_anecdotal support but statistical opposition = 1.87, SD_anecdotal support but statistical opposition = 1.42, p = 0.18), the statistical support but anecdotal opposition group (M_statistical support but anecdotal opposition = 2.01, SD_statistical support but anecdotal opposition = 0.13, p = 0.18), or the statistical conflict group (M_statistical conflict = 2.19, SD_statistical conflict = 0.13, p = 0.18).
Perceived conflict (first mediator)
H1 predicted a positive relationship between conflicting evidence and perceived conflict. The results indicate that, with the exception of the anecdotal support but statistical opposition conflict, all other types of conflicting information significantly enhanced perceived conflict compared to the no conflict group [F(4, 336) = 5.08, p < 0.01]. Post-hoc tests revealed no significant difference in willingness to avoid health information between the no conflict group (M_no conflict = 1.87, SD_no conflict = 0.57) and the anecdotal support but statistical opposition group (M_anecdotal support but statistical opposition = 2.01, SD_anecdotal support but statistical opposition = 0.65; p = 0.26). In contrast, the willingness to avoid health information in the other groups was significantly higher than that of the no conflict group (M_statistical conflict = 2.34, SD_statistical conflict = 0.69; M_anecdotal support but statistical opposition = 2.19, SD_anecdotal support but statistical opposition = 0.92; M_anecdotal conflict = 1.87, SD_anecdotal conflict = 0.57; M_statistical support but anecdotal opposition = 2.33, SD_statistical support but anecdotal opposition = 0.91; p < 0.05). Thus, hypothesis H1 receives partial support.
Elaboration (second mediator)
This study employed the SPSS PROCESS Model 1 to examine the effects of perceived conflict and perceived control on elaboration levels. The analysis revealed that the impact of perceived conflict on elaboration was not statistically significant (β = −0.10, p = 0.36). However, the interaction between perceived conflict and perceived control significantly influenced elaboration (β = 0.25, p < 0.001).
Spotlight analyses indicated that high perceived conflict (defined as being more than one standard deviation above the mean) notably enhanced elaboration levels under conditions of high perceived control (elaboration: 1.92 vs. 3.34, β = 0.43, SE = 0.09, t = 4.77, p < 0.0001, CI = [0.25, 0.60]). In contrast, low perceived conflict did not result in a significant difference in cognitive processing levels under conditions of low perceived control (elaboration: 1.96 vs. 2.48, β = −0.02, SE = 0.09, t = −0.20, p = 0.84, CI = [−0.19, 0.16]) (Figure 3).
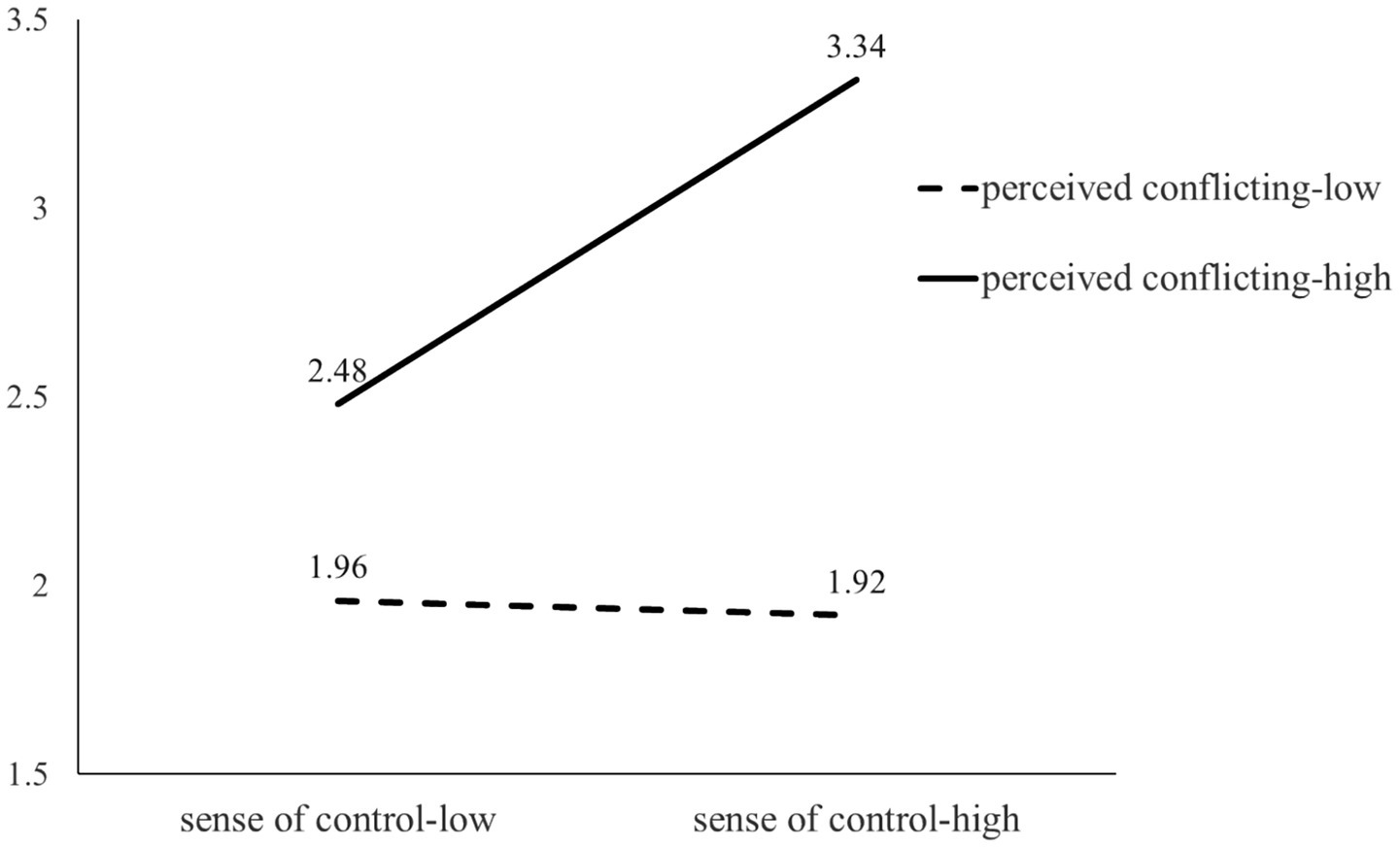
Figure 3. The impact of perceived conflict and disease control on elaboration. “Low perceived control” is defined as being below one standard deviation from the mean, while “high perceived conflict” is characterized as being above one standard deviation from the mean.
Ambiguity aversion (third mediator)
The data analysis results indicate that perceived conflict significantly affects ambiguity aversion (β = 0.58, p < 0.001), and the interaction between perceived conflict and perceived control also has a significant impact on ambiguity aversion (β = −0.22, p < 0.01).
Spotlight analysis results reveal that perceived control can mitigate ambiguity aversion to some extent. High perceived conflict (one standard deviation above the mean) significantly increases ambiguity aversion levels under low perceived control conditions (ambiguity aversion: 4.07 vs. 5.34, β = 0.34, SE = 0.10, t = −3.41, p < 0.001, CI = [−0.54, −0.15]). In contrast, there are no significant differences in ambiguity aversion levels under high perceived control conditions regardless of perceived conflict (ambiguity aversion: 4.17 vs. 4.66, β = 0.05, SE = 0.10, t = 0.53, p = 0.60, CI = [−0.15, 0.25]) (Figure 4).
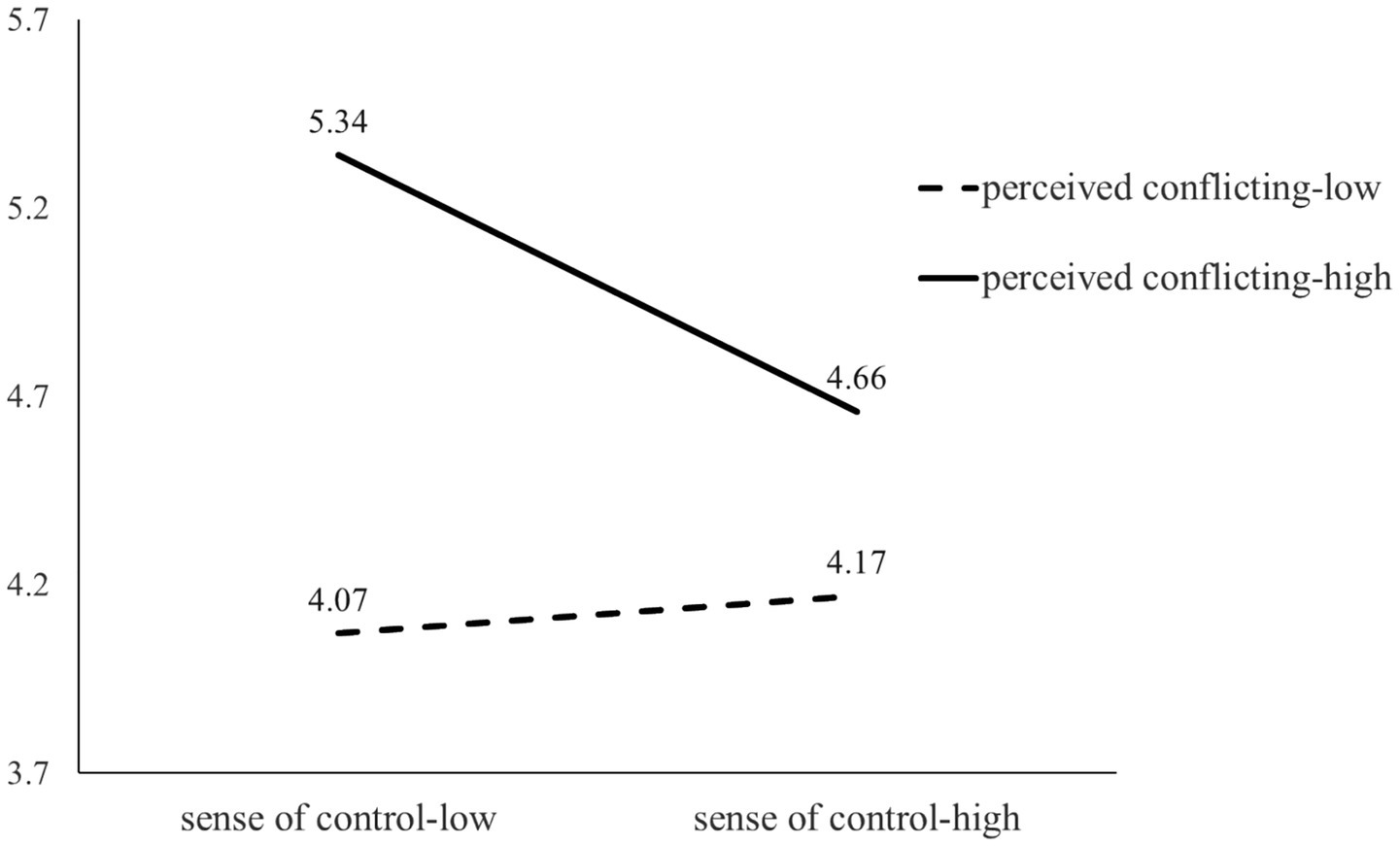
Figure 4. The impact of perceived conflict and disease control on ambiguity aversion.
Moderated serial mediation analysis
The results of the moderated serial mediation analysis are illustrated in Figure 5 and summarized in Table 2. The data indicate that perceived conflict has a significant and positive effect on ambiguity aversion (β = 0.49, CI [0.24, 0.74]). Furthermore, elaboration has a significant and negative effect on cancer information avoidance (β = −0.07, CI [−0.13, −0.01]). The direct effects of the variables on cancer information avoidance were partially significant: for anecdotal conflict (βconflicting anecdotal evidence = 0.73, CI conflicting anecdotal evidence [−0.03, 1.49]), anecdotal support with statistical opposition (βanecdotal support with statistical opposition = −0.13, CI anecdotal support with statistical opposition [−0.87, 0.61]), statistical support with anecdotal opposition (βstatistical support with anecdotal opposition = 1.12, CI statistical support with anecdotal opposition [0.37, 1.86]), and statistical conflict (β statistical conflict = 0.65, CI statistical conflict [−0.09, 1.39]). However, the indirect effects of encountering conflicting evidence on cancer information avoidance through elaboration were not significant, leading to the conclusion that Hypothesis 3 was not supported.
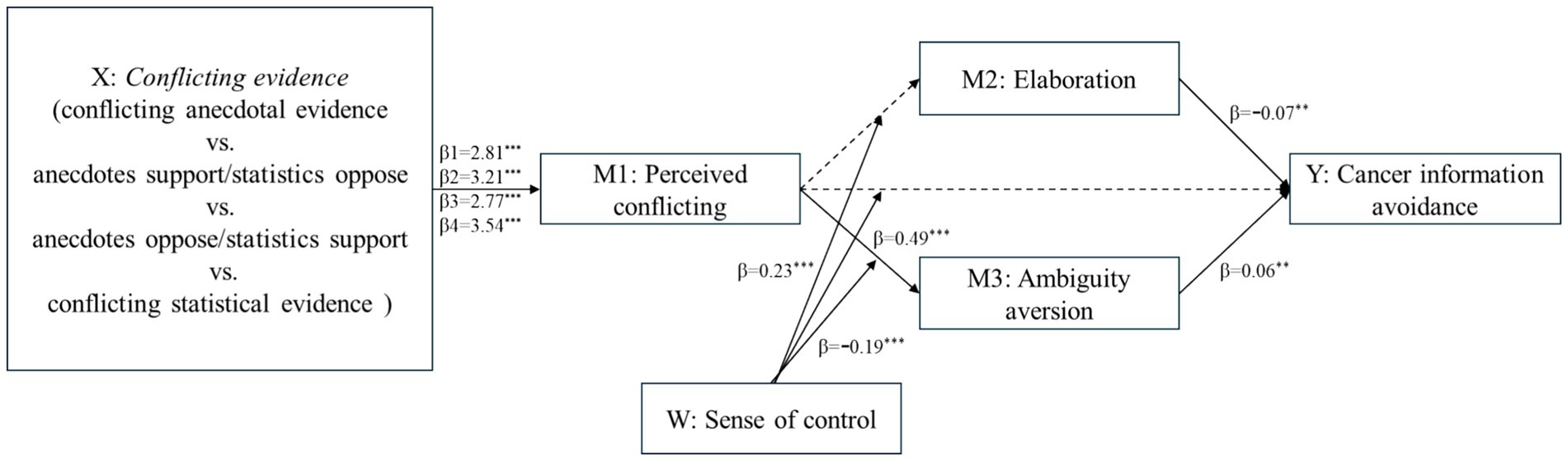
Figure 5. Result of moderated serial mediation analysis. *p < 0.05, **p < 0.01, ***p < 0.001.
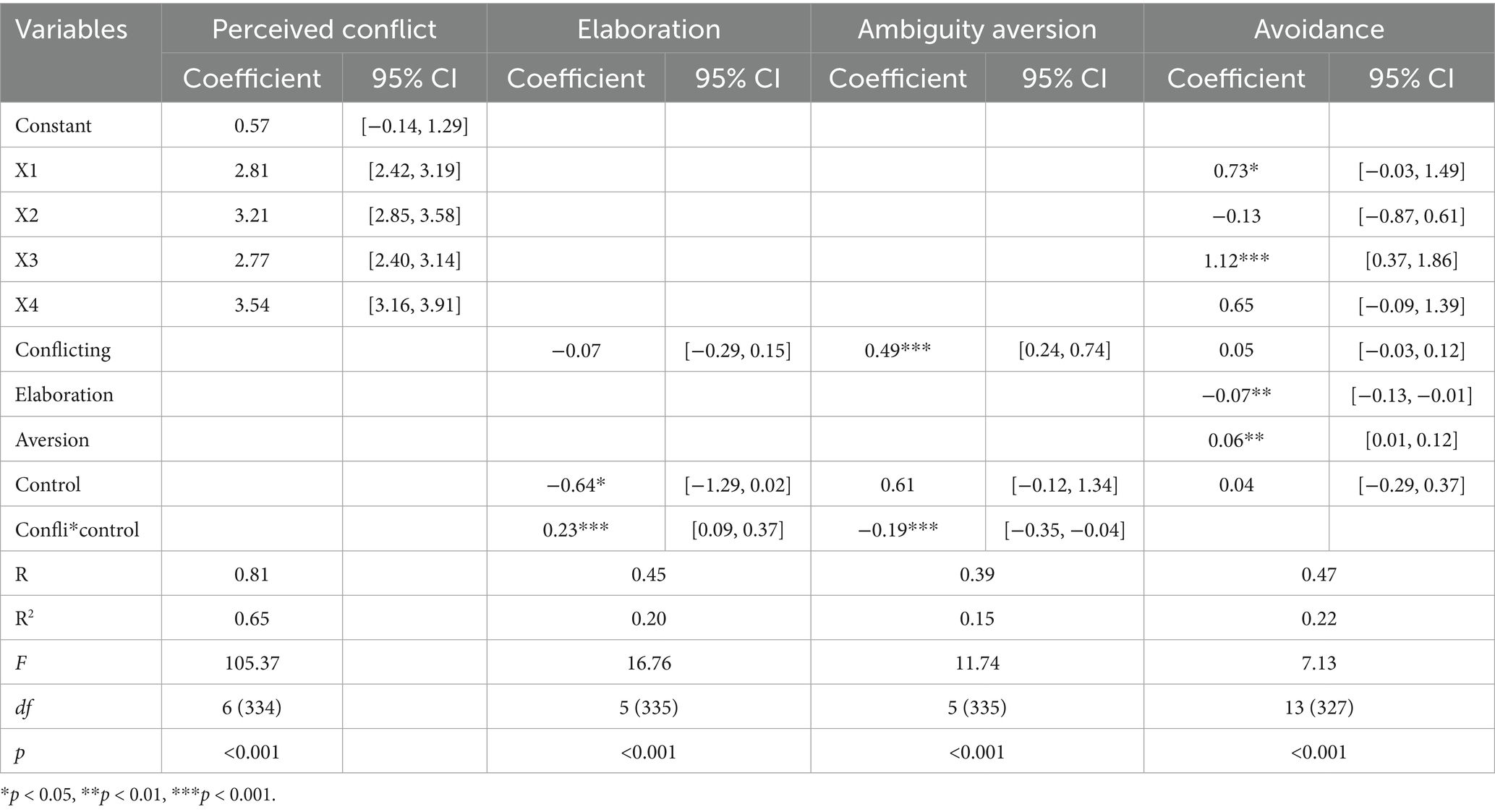
Table 2. Results of moderated serial mediation analysis.
In contrast, the indirect effects of encountering conflicting evidence on cancer information avoidance through ambiguity aversion were significant when the sense of cancer control was low: the pathway from conflicting evidence type to perceived conflict to ambiguity aversion to cancer information avoidance yielded positive effects for anecdotal conflict (Effect = 0.05, CI [0.14, 0.10]), anecdotal support with statistical opposition (Effect = 0.06, CI [0.02, 0.12]), anecdotal opposition with statistical support (Effect = 0.05, CI [0.01, 0.10]), and conflicting statistical evidence (Effect = 0.07, CI [0.02, 0.13]).
Notably, these indirect effects were not significant when the sense of cancer control was high: the pathway from conflicting evidence type to perceived conflict to ambiguity aversion to cancer information avoidance resulted in negligible effects for anecdotal conflict (Effect = 0.02, CI [−0.01, 0.05]), anecdotal support with statistical opposition (Effect = 0.02, CI [−0.01, 0.06]), anecdotal opposition with statistical support (Effect = 0.02, CI [−0.01, 0.05]), and conflicting statistical evidence (Effect = 0.02, CI [−0.01, 0.07]).
The indexes of moderated mediation for the indirect effects of conflicting evidence type through perceived conflict and ambiguity aversion were significant: for anecdotal conflict (Index = −0.04, CI [−0.08, −0.01]), anecdotal support with statistical opposition (Index = −0.04, CI [−0.09, −0.01]), anecdotal opposition with statistical support (Index = −0.03, CI [−0.08, −0.01]), and conflicting statistical evidence (Index = −0.04, CI [−0.10, −0.01]). These findings support the indirect effects of conflicting evidence types on cancer information avoidance through perceived conflict and ambiguity aversion, particularly under varying levels of perceived control.
To further probe these effects, we conducted moderated mediation analyses (PROCESS, Model 7, 5,000 bootstraps) with perceived conflict as the predictor, information avoidance as the outcome, and ambiguity aversion/elaboration as mediators, moderated by perceived control. Under high perceived control, perceived conflict increased elaboration (β = 0.39, p < 0.001), which in turn negatively predicted avoidance (β = −0.10, p < 0.01). The indirect effect via elaboration was significant (indirect = −0.038, 95% CI [−0.075, −0.006]). In contrast, under low control, perceived conflict heightened ambiguity aversion (β = 0.36, p < 0.001; interaction β = −0.22, p < 0.01), which significantly increased avoidance (β = 0.07, p < 0.05). The indirect effect via ambiguity aversion was significant (indirect = 0.025, 95% CI [0.007, 0.045]).
Robustness check
To address potential concerns about individual differences, we added education and income as covariates in the moderated mediation model (PROCESS, Model 7, 5,000 bootstraps). Results indicated that both education (B = 0.19, p = 0.028) and income (B = −0.05, p = 0.021) were significantly associated with information avoidance. However, including these controls did not alter the significance of the focal effects. Specifically, the conditional indirect effect of conflicting evidence on avoidance via ambiguity aversion remained stronger when perceived control was low (effect = 0.03, 95% CI [0.007, 0.049]) than when perceived control was high (effect = 0.02, 95% CI [0.002, 0.026]; index of moderated mediation = −0.015, 95% CI [−0.035, −0.001]). Likewise, the conditional indirect effect via elaboration remained significant (low control: effect = −0.014, 95% CI [−0.033, −0.002]; high control: effect = −0.037, 95% CI [−0.072, −0.007]). These findings demonstrate that the moderated mediation effects are robust to the inclusion of covariates.
Discussion
This study investigated how exposure to conflicting evidence about cancer screening influences individuals’ information behaviors through both cognitive and affective mechanisms. Specifically, we examined perceived conflict as the proximal response to conflicting information, with elaboration and ambiguity aversion serving as parallel mediators that shape downstream avoidance. We further tested perceived control as a moderator of these processes.
Dual-pathway mechanisms of conflict processing
Consistent with prior research suggesting that the same evidence can be processed differently across contexts (Baillon et al., 2012; Einhorn and Hogarth, 1985; Visschers, 2017), our findings show that perceived conflict does not exert uniform effects on health information behaviors but instead operates through two distinct psychological pathways. When individuals reported low disease control, perceived conflict heightened ambiguity aversion, which in turn increased their tendency to avoid cancer-related information. Conversely, while the moderated mediation effect through elaboration was not statistically significant, the pattern of results suggested a potential pathway where higher disease control may encourage more elaborate processing of conflicting information. This pattern aligns with the theoretical proposition that a sense of agency can foster cognitive engagement, and its role as a mechanism for reducing avoidance warrants further investigation in future research. These findings extend prior work that has often treated conflict as uniformly detrimental (e.g., Nagler et al., 2019; Ahn and Kahlor, 2022) by specifying its dual and opposing potential consequences.
Boundary conditions and process explanation
The moderating role of perceived control suggests that conflict does not automatically trigger avoidance. Instead, when individuals feel a sense of agency over their health, conflict may be less threatening and therefore less likely to produce disengagement. This aligns with prior research grounded in rational action and uncertainty reduction theories, which suggests that negative consequences of conflicting information can be mitigated when individuals engage in increased cognitive processing, thereby reducing health information avoidance (Jensen et al., 2014; Niederdeppe and Levy, 2007; Miles et al., 2008; Chatterjee et al., 2005; Zimbres et al., 2021; Mateos et al., 2018). Conversely, when control is low, conflicting evidence may amplify uncertainty and avoidance, consistent with findings in other health decision-making contexts.
Theoretical implications
This study makes three theoretical contributions. First, building on compensatory control theory, we advance a novel account of why and when individuals either succumb to or overcome the challenges of conflicting information. This explanation deepens the field’s understanding of the mechanisms underlying health information avoidance. When people’s fundamental need for control is threatened, they are more likely to react with heightened ambiguity aversion, as external certainty serves as a substitute source of order. In contrast, when individuals feel a sufficient sense of control, they can reframe conflict as an opportunity for elaboration, thereby mitigating avoidance. This study extends compensatory control theory by showing that perceived control restores psychological equilibrium through two distinct mechanisms: reducing the negative affective response of ambiguity aversion and enhancing the cognitive response of elaboration. This dual-pathway account advances prior work by specifying how control moderates the consequences of conflict.
Second, our work clarifies longstanding contradictions in the evidence on the consequences of conflict. Previous studies have reported mixed findings, with some suggesting that conflict discourages engagement (Han et al., 2007; Viscusi and Chesson, 1999) while others highlight its potential to stimulate deeper processing. We reconcile these inconsistencies by identifying perceived control as a boundary condition: conflict is harmful under low control—leading to avoidance via ambiguity aversion—but beneficial under high control, where it fosters elaboration and reduces avoidance. This explanation aligns with broader research showing that higher personal control promotes confidence and risk taking (Kouchaki et al., 2014; Chan et al., 2014).
Third, our study contributes to conceptual clarity in the literature on conflicting health information. We distinguish between perceived conflict (a subjective psychological appraisal) and objective conflict (a structural property of information). Our findings highlight that perceptions, rather than information structure alone, are the proximal drivers of avoidance. Future research should also differentiate between cross-valence conflict (contradictory positive vs. negative cues) and univalent conflict (contradictions within the same valence), as these forms may involve distinct psychological processes.
Practical implications
Beyond theoretical contributions, our findings carry practical relevance for cancer communication. Conflicting messages are likely to continue proliferating in digital environments, but their detrimental effects can be buffered by strengthening individuals’ sense of control. Campaigns should not only aim to reduce message inconsistency but also actively enhance perceived control—for instance, by emphasizing actionable steps, clarifying the rationale behind guidelines, or highlighting areas of certainty amid uncertainty. By fostering a sense of agency, communicators may encourage advice seeking and engagement rather than avoidance.
Limitations and future research
Several limitations should be acknowledged. First, the conflict manipulations were intentionally subtle and participants were exposed to the stimuli only once. While this approach ensured experimental control and internal validity, it may have constrained participants’ opportunity to engage in more extended message processing. In real-world settings, exposure to conflicting health information tends to be repeated and cumulative, which may elicit deeper cognitive elaboration over time. Future research could employ multi-exposure or longitudinal designs to capture how elaboration develops dynamically.
Second, the present findings indicate that ambiguity aversion exerted stronger effects than elaboration, suggesting that people may react more readily on an affective rather than a deliberative level when confronted with conflicting evidence. Future studies could further investigate this emotional–cognitive asymmetry by incorporating richer measures of both response types or by testing interventions that encourage deeper information engagement.
Finally, the generalizability of the results may be shaped by the Chinese cultural and informational context in which the study was conducted. High baseline trust in public health authorities (Steinhardt, 2011), a collectivistic orientation toward social responsibility (Du et al., 2015), and relatively low perceived personal control over systemic risks (Cheng et al., 2013) could have influenced how participants interpreted and responded to evidence conflict. These contextual features may moderate the role of compensatory control processes in other cultures. Cross-cultural replications that vary the framing of individual control and trust cues would help clarify the boundary conditions of the observed effects.
Conclusion
In sum, this study highlights the central role of perceived conflict and perceived control in shaping responses to conflicting cancer screening information. While conflicting evidence can undermine engagement by heightening ambiguity aversion, enhancing perceived control enables individuals to reframe conflict as an opportunity for elaboration and deeper processing. These insights provide both theoretical refinement and practical guidance for designing health communication strategies that minimize avoidance and foster informed engagement.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Review Board of the School of Journalism and Communication, Sun Yat-sen University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JZ: Conceptualization, Formal analysis, Software, Writing – original draft, Writing – review & editing. JO: Investigation, Methodology, Writing – original draft. JN: Funding acquisition, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2025.1590787/full#supplementary-material
Footnotes
References
Ahn, J., and Kahlor, L. A. (2022). When experts offer conflicting information: a study of perceived ambiguity, information insufficiency, trustworthiness and risk information behaviors. Health Commun. 38, 3276–3286. doi: 10.1080/10410236.2022.2146033
Baillon, A., Cabantous, L., and Wakker, P. P. (2012). Aggregating imprecise or conflicting beliefs: an experimental investigation using modern ambiguity theories. J. Risk Uncertain. 44, 115–147. doi: 10.1007/s11166-012-9140-x
Barnwell, P. V., Rattigan, J. A., Brennan, K. T., Fedorenko, E. J., and Contrada, R. J. (2023). Exposure to conflicting COVID-19 information in undergraduates: implications for pandemic-related information-seeking and concern, attention, and cognitive workload. J. Am. Coll. Heal. 73, 311–322. doi: 10.1080/07448481.2023.2220409
Briñol, P., Petty, R. E., Durso, G. R., and Rucker, D. D. (2017). Power and persuasion: Processes by which perceived power can influence evaluative judgments. Rev. Gen. Psychol., 21, 223–241.
Burton, A. K., Waddell, G., Tillotson, K. M., and Summerton, N. (1999). Information and advice to patients with back pain can have a positive effect: a randomized controlled trial of a novel educational booklet in primary care. Spine 24, 2484–2491. doi: 10.1097/00007632-199912010-00010
Carpenter, D. M., and Han, P. K. (2020). “Conflicting health information” in The Wiley encyclopedia of health psychology, In S. B. Gulliver, L. M. Cohen (Eds.), (Hoboken, NewJersey, USA: John Wiley & Sons) 47–53.
Chan, K. Q., Tong, E. M. W., and Tan, Y. L. (2014). Taking a leap of faith: reminders of god lead to greater risk taking. Soc. Psychol. Personal. Sci. 5, 901–909. doi: 10.1177/1948550614537309
Chatterjee, S., Kang, Y. S., and Mishra, D. P. (2005). Market signals and relative preference: the moderating effects of conflicting information, decision focus, and need for cognition. J. Bus. Res. 58, 1362–1370. doi: 10.1016/j.jbusres.2004.07.001
Cheng, C., Cheung, S. F., Chio, J. H. M., and Chan, M. P. S. (2013). Cultural meaning of perceived control: a meta-analysis of locus of control and psychological symptoms across 18 cultural regions. Psychol. Bull. 139, 152–188. doi: 10.1037/a0028596
Chinn, S., and Weeks, B. E. (2021). Effects of competing statistical and testimonial evidence in debates about science. Environ. Commun. 15, 353–368. doi: 10.1080/17524032.2020.1837900
D’Mello, S., Lehman, B., Pekrun, R., and Graesser, A. (2014). Confusion can be beneficial for learning. Learn. Instr. 29, 153–170. doi: 10.1016/j.learninstruc.2012.05.003
De Wit, J. B., Das, E., and Vet, R. (2008). What works best: objective statistics or a personal testimonial? An assessment of the persuasive effects of different types of message evidence on risk perception. Health Psychol. 27, 110–115. doi: 10.1037/0278-6133.27.1.110
Dootson, P., Kuligowski, E., Greer, D. A., Miller, S. A., and Tippett, V. (2022). Consistent and conflicting information in floods and bushfires impact risk information seeking, risk perceptions, and protective action intentions. Int. J. Disaster Risk Reduct. 70:102774. doi: 10.1016/j.ijdrr.2021.102774
Du, H., Li, X., Lin, D., and Tam, C. C. (2015). Collectivistic orientation, acculturative stress, cultural self-efficacy, and depression: a longitudinal study among Chinese internal migrants. Community Ment. Health J. 51, 239–248. doi: 10.1007/s10597-014-9785-9
Einhorn, H. J., and Hogarth, R. M. (1985). Ambiguity and uncertainty in probabilistic inference. Psychol. Rev. 92, 433–461. doi: 10.1037/0033-295X.92.4.433
Fagerlin, A., Wang, C., and Ubel, P. A. (2005). Reducing the influence of anecdotal reasoning on people’s health care decisions: is a picture worth a thousand statistics? Med. Decis. Mak. 25, 398–405. doi: 10.1177/0272989X05278931
Faul, F., Erdfelder, E., Buchner, A., and Lang, A. G. (2009). Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods, 41, 1149–1160.
Flemming, D., Feinkohl, I., Cress, U., and Kimmerle, J. (2015). Individual uncertainty and the uncertainty of science: the impact of perceived conflict and general self-efficacy on the perception of tentativeness and credibility of scientific information. Front. Psychol. 6:1859. doi: 10.3389/fpsyg.2015.01859
Freling, T., Saini, R., and Yang, Z. (2014). “Involved but inaccurate: when high-stakes lead to anecdotal bias.” In Harvard Center for Risk Analysis Risk, Perception, and Response Conference Paper. Available at: http://www.hsph.harvard.edu/hcra/risk-perception-and-response-conference/conference-agenda-and-papers/
Goldzweig, G., Hasson-Ohayon, I., Alon, S., and Shalit, E. (2016). Perceived threat and depression among patients with cancer: the moderating role of health locus of control. Psychol. Health Med. 21, 601–607. doi: 10.1080/13548506.2016.1140902
Gustafson, A., and Rice, R. E. (2020). A review of the effects of uncertainty in public science communication. Public Underst. Sci. 29, 614–633. doi: 10.1177/0963662520942122
Han, P. K., Moser, R. P., and Klein, W. M. (2007). Perceived ambiguity about cancer prevention recommendations: associations with cancer-related perceptions and behaviours in a US population survey. Health Expect. 10, 321–336. doi: 10.1111/j.1369-7625.2007.00456.x
Han, P. K., Zikmund-Fisher, B. J., Duarte, C. W., Knaus, M., Black, A., Scherer, A. M., et al. (2018). Communication of scientific uncertainty about a novel pandemic health threat: ambiguity aversion and its mechanisms. J. Health Commun. 23, 435–444. doi: 10.1080/10810730.2018.1461961
Hayes, A. F. (2018). Partial, conditional, and moderated moderated mediation: Quantification, inference, and interpretation. Commun. Monogr, 85, 4–40.
Henselmans, I., Fleer, J., de Vries, J., Baas, P. C., Sanderman, R., and Ranchor, A. V. (2010). The adaptive effect of personal control when facing breast cancer: cognitive and behavioural mediators. Psychol. Health 25, 1023–1040. doi: 10.1080/08870440902935921
Howell, J. L., and Shepperd, J. A. (2013). Reducing health-information avoidance through contemplation. Psychol. Sci. 24, 1696–1703. doi: 10.1177/0956797613478616
Huang, Q., Mao, B., Jia, X., and Peng, W. (2023). COVID-19 information overload mediated the effects of cross-channel information differences on health information elaboration. J. Health Commun. 28, 401–411. doi: 10.1080/10810730.2023.2217097
Iles, I. A., Gillman, A. S., O'Connor, L. E., Ferrer, R. A., and Klein, W. M. (2022). Understanding responses to different types of conflicting information about cancer prevention. Soc. Sci. Med. 311:115292. doi: 10.1016/j.socscimed.2022.115292
Jaramillo, S., Horne, Z., and Goldwater, M. (2019). The impact of anecdotal information on medical decision-making. PsyArXiv. doi: 10.31234/osf.io/r5pmj
Jensen, J. D., Carcioppolo, N., King, A. J., Scherr, C. L., Jones, C. L., and Niederdeppe, J. (2014). The Cancer information overload (CIO) scale: establishing predictive and discriminant validity. Patient Educ. Couns. 94, 90–96. doi: 10.1016/j.pec.2013.09.016
Kaufhold, M. A., Rupp, N., Reuter, C., and Habdank, M. (2020). Mitigating information overload in social media during conflicts and crises: design and evaluation of a cross-platform alerting system. Behav. Inform. Technol. 39, 319–342. doi: 10.1080/0144929X.2019.1620334
Kay, A. C., Whitson, J. A., Gaucher, D., and Galinsky, A. D. (2009). Compensatory control: achieving order through the mind, our institutions, and the heavens. Curr. Dir. Psychol. Sci. 18, 264–268. doi: 10.1111/j.1467-8721.2009.01649.x
Klein, W. M., Cerully, J. L., Monin, M. M., and Moore, D. A. (2010). Ability, chance, and ambiguity aversion: revisiting the competence hypothesis. Judgm. Decis. Mak. 5, 192–199. doi: 10.1017/S1930297500001078
Kouchaki, M., Oveis, C., and Gino, F. (2014). Guilt enhances the sense of control and drives risky judgments. J. Exp. Psychol. Gen. 143, 2103–2110. doi: 10.1037/a0037932
Lecci, L., and Cohen, D. (2007). Altered processing of health threat words as a function of hypochondriacal tendencies and experimentally manipulated control beliefs. Cognit. Emot. 21, 211–224. doi: 10.1080/02699930600625248
Lee, S. F., and Shi, J. (2022). Examining the roles of fatalism, stigma, and risk perception on cancer information seeking and avoidance among Chinese adults in Hong Kong. J. Psychosoc. Oncol. 40, 425–440. doi: 10.1080/07347332.2021.1957061
Li, J. Y., Wen, J., Kim, J., and McKeever, R. (2020). Applying the theory of motivated information management to the context of conflicting online health information: implications for childhood vaccination communication with parents. Int. J. Strateg. Commun. 14, 330–347. doi: 10.1080/1553118X.2020.1817030
Ma, A., and Kay, A. C. (2017). Compensatory control and ambiguity intolerance. Organ. Behav. Hum. Decis. Process. 140, 46–61. doi: 10.1016/j.obhdp.2017.04.001
Magee, J. C. (2009). Seeing power in action: the roles of deliberation, implementation, and action in inferences of power. J. Exp. Soc. Psychol. 45, 1–14. doi: 10.1016/j.jesp.2008.06.010
Marshall, L. H., and Comello, M. L. (2019). Stymied by a wealth of health information: how viewing conflicting information online diminishes cancer screening. J. Commun. Healthc. 12, 4–12. doi: 10.1080/17538068.2019.1580064
Mateos, M., Martín, E., Cuevas, I., Villalón, R., Martínez, I., and González-Lamas, J. (2018). Improving written argumentative synthesis by teaching the integration of conflicting information from multiple sources. Cogn. Instr. 36, 119–138. doi: 10.1080/07370008.2018.1425300
McLain, D. L. (2009). Evidence of the properties of an ambiguity tolerance measure: the multiple stimulus types ambiguity tolerance scale–II (MSTAT–II). Psychol. Rep. 105, 975–988. doi: 10.2466/PR0.105.3.975-988
Michal, A. L., Zhong, Y., and Shah, P. (2021). When and why do people act on flawed science? Effects of anecdotes and prior beliefs on evidence-based decision-making. Cogn. Res. Princip. Implicat. 6:28. doi: 10.1186/s41235-021-00293-2
Miles, A., Voorwinden, S., Chapman, S., and Wardle, J. (2008). Psychologic predictors of cancer information avoidance among older adults: the role of cancer fear and fatalism. Cancer Epidemiol. Biomarkers Prev. 17, 1872–1879. doi: 10.1158/1055-9965.EPI-08-0074
Nagler, R. H. (2014). Adverse outcomes associated with media exposure to contradictory nutrition messages. J. Health Commun. 19, 24–40. doi: 10.1080/10810730.2013.798384
Nagler, R. H., and LoRusso, S. M. (2017). “Conflicting information and message competition in health and risk messaging” in ed. Powers, M. Oxford research encyclopedia of communication.
Nagler, R. H., Vogel, R. I., Gollust, S. E., Yzer, M. C., and Rothman, A. J. (2022). Effects of prior exposure to conflicting health information on responses to subsequent unrelated health messages: results from a population-based longitudinal experiment. Ann. Behav. Med. 56, 498–511. doi: 10.1093/abm/kaab069
Nagler, R. H., Yzer, M. C., and Rothman, A. J. (2019). Effects of media exposure to conflicting information about mammography: results from a population-based survey experiment. Ann. Behav. Med. 53, 896–908. doi: 10.1093/abm/kay098
Niederdeppe, J., and Levy, A. G. (2007). Fatalistic beliefs about cancer prevention and three prevention behaviors. Cancer Epidemiol. Biomarkers Prev. 16, 998–1003. doi: 10.1158/1055-9965.EPI-06-0608
Nissel, J., and Woolley, J. D. (2024). Anecdata: children’s and adults’ evaluation of anecdotal and statistical evidence. Front. Dev. Psychol. 2:1324704. doi: 10.3389/fdpys.2024.1324704
Raghubir, P., and Menon, G. (1996). Asking sensitive questions: the effects of type of referent and frequency wording in counterbiasing methods. Psychol. Mark. 13, 633–652. doi: 10.1002/(SICI)1520-6793(199610)13:7<633::AID-MAR1>3.0.CO;2-I
Shen, L., and Dillard, J. P. (2009). Message frames interact with motivational systems to determine depth of message processing. Health Commun. 24, 504–514. doi: 10.1080/10410230903104897
Steinhardt, H. C. (2011). How is high trust in China possible? Comparing the origins of generalized trust in three Chinese societies. Polit. Stud. 60, 434–454. doi: 10.1111/j.1467-9248.2011.00909.x
Stuart, J. O. R., Windschitl, P. D., Miller, J. E., Smith, A. R., Zikmund-Fisher, B. J., and Scherer, L. D. (2022). Attributions for ambiguity in a treatment-decision context can create ambiguity aversion or seeking. J. Behav. Decis. Mak. 35:e2249. doi: 10.1002/bdm.2249
Taylor, S. E., and Armor, D. A. (1996). Positive illusions and coping with adversity. J. Pers. 64, 873–898. doi: 10.1111/j.1467-6494.1996.tb00947.x
Teachman, B. A., Gapinski, K. D., Brownell, K. D., Rawlins, M., and Jeyaram, S. (2003). Demonstrations of implicit anti-fat bias: the impact of providing causal information and evoking empathy. Health Psychol. 22, 68–78. doi: 10.1037/0278-6133.22.1.68
Tversky, A., and Kahneman, D. (1971). Belief in the law of small numbers. Psychol. Bull. 76, 105–110. doi: 10.1037/h0031322
Viscusi, W. K., and Chesson, H. (1999). Hopes and fears: the conflicting effects of risk ambiguity. Theor. Decis. 47, 157–184. doi: 10.1023/A:1005173013606
Viscusi, W. K., Magat, W. A., and Huber, J. (1991). Communication of ambiguous risk information. Theor. Decis. 31, 159–173. doi: 10.1007/BF00132991
Visschers, V. H. (2017). Judgments under uncertainty: evaluations of univocal, ambiguous and conflicting probability information. J. Risk Res. 20, 237–255. doi: 10.1080/13669877.2015.1043569
Keywords: evidence conflict, compensatory control, ambiguity aversion, health information avoidance, elaboration
Citation: Zhai J, Ou J and Nie J (2025) How evidence conflict affects willingness to avoid health information: from the perspective of compensatory control theory. Front. Commun. 10:1590787. doi: 10.3389/fcomm.2025.1590787
Edited by:
Grant McGeechan, Teesside University, United KingdomReviewed by:
Jiankun Gong, University of Malaya, MalaysiaJudith Eberhardt, Teesside University, United Kingdom
Copyright © 2025 Zhai, Ou and Nie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinghong Nie, bHBzbmpoQG1haWwuc3lzdS5lZHUuY24=