 Dichitchai Mettarikanon1
Dichitchai Mettarikanon1 Weeratian Tawanwongsri
Weeratian Tawanwongsri- 1Division of Digital Content and Media, School of Informatics, Walailak University, Nakhon Si Thammarat, Thailand
- 2Jigme Dorji Wangchuck National Referral Hospital (JDWNRH), Thimphu, Bhutan
- 3Division of Dermatology, Department of Internal Medicine, School of Medicine, Walailak University, Nakhon Si Thammarat, Thailand
Introduction: Game-based learning (GBL) has gained attention as an innovative approach to patient education, offering interactive and engaging experiences that enhance learning and self-management. In dermatology—where visual recognition and adherence to treatment are particularly important—GBL may offer unique educational advantages.
Methods: This scoping review aimed to map the existing literature on the use of GBL in dermatology patient education and to identify gaps for future investigation. A comprehensive search was conducted across Scopus, Medical Literature Analysis and Retrieval System Online (MEDLINE), and Directory of Open Access Journals (DOAJ), following the Joanna Briggs Institute methodology and the PRISMA-ScR checklist. Eligible studies were peer-reviewed primary research articles, published in English between January 2005 and May 2025, and focused on game-based interventions designed to educate individuals with dermatologic conditions.
Results: Eight studies met the inclusion criteria, addressing a range of conditions including melanoma, atopic dermatitis, cutaneous leishmaniasis, and sun-related skin damage. Interventions featured gamification, serious games, and augmented reality formats. Most studies reported improvements in knowledge, recognition accuracy, treatment adherence, and user satisfaction. However, only three were randomized controlled trials, and the use of validated outcome measures was inconsistent. Digital usability testing was limited, and the majority of the game-based tools were institution-developed and not publicly accessible.
Discussion: GBL shows promise as an engaging and potentially effective method for educating dermatology patients, particularly for conditions that rely heavily on visual learning. Nevertheless, the current body of evidence remains preliminary. Many studies had small sample sizes, varied in methodological quality, and underrepresented older adults and individuals with limited digital literacy. Future research should focus on rigorous study designs, broader participant inclusion, and long-term evaluation to support the integration of GBL into routine dermatologic care.
1 Introduction
Patient education in dermatology is essential for improving clinical outcomes, enhancing self-management capabilities, and increasing overall patient satisfaction (Heratizadeh, 2014; Zirwas and Holder, 2009). Traditional educational methods—including verbal instruction during consultations, written materials like pamphlets, audiovisual resources, and internet information—while widespread, face significant limitations in practice (Alagheband et al., 2015; Feeley et al., 2023; Zhao and Zhang, 2017). These conventional approaches frequently result in low patient engagement and interest, poor information retention over time, and substantial non-adherence rates to recommended treatments (Crawford et al., 2018; Huang and Hwang, 2019). Previous studies demonstrated that up to 50% of patients fail to follow prescribed dermatological treatments, with more than 40% taking medications incorrectly and approximately 80% not adhering to critical lifestyle recommendations such as dietary restrictions or sun protection measures (Allison, 2012; Miller and DiMatteo, 2015). Game-based learning (GBL) represents one of the most promising innovative solutions to these persistent educational challenges by thoughtfully leveraging elements of play, competition, and interactive engagement to enhance the learning experience for patients (Chang et al., 2024). This approach has demonstrated particular value in three key areas: significantly increasing patient engagement and intrinsic motivation through more enjoyable interactive experiences, improving knowledge retention and diagnostic awareness, and enhancing patients’ self-management capabilities and decision-making skills regarding their skin conditions (Chang et al., 2024; Szeto et al., 2021).
The growing interest in GBL approaches in medical education, including dermatology field, is substantiated by compelling evidence demonstrating their effectiveness in enhancing learner engagement, motivation, and educational outcomes (Xu et al., 2023). GBL can assist learners in developing skills such as clinical reasoning, decision-making, and problem-solving. It consists of several distinct pedagogical approaches, each tailored to the specific educational context. GBL, including serious games and gamification, is gaining popularity in medical education. Gamification enhances engagement by incorporating elements such as points, badges, and leaderboards into non-game environments (Cascella et al., 2023; Zadeja and Bushati, 2022; Zhang and Yu, 2022). Serious games prioritize skill development over entertainment, with applications (Cascella et al., 2023; Zadeja and Bushati, 2022). Traditional game-based learning seamlessly integrates educational content with gaming mechanics (Al Fatta et al., 2018). Educational simulations replicate real-world scenarios for practical training purposes, particularly valuable in fields like medicine (Lamb et al., 2018). Edutainment blends educational objectives with entertainment value to create engaging learning experiences through television programs and interactive applications (Al Fatta et al., 2018). Educators can leverage these differentiated approaches by selecting methodologies that best align with their specific pedagogical goals and learning contexts.
Given the promising potential of GBL in patient education, a thorough assessment of its current use in dermatology is crucial for guiding future developments. A scoping review approach was selected to comprehensively map existing evidence, identify knowledge gaps, and explore the breadth and nature of GBL in dermatology patient education—an area where research is still emerging and heterogeneous. By synthesizing current research, this review aims to provide valuable insights for dermatologists, educational technologists, and healthcare systems looking to implement innovative and effective patient education strategies. Additionally, it will highlight areas requiring further study to advance the role of GBL in dermatology education. Therefore, the objective of this scoping review was to map the existing literature on the use of GBL for patient education in dermatology. Specifically, this review addresses the following research question: What are the characteristics, implementation strategies, and reported outcomes of game-based learning interventions used for dermatology patient education?
2 Methods
2.1 Protocol and framework
This scoping review followed the methodological framework recommended by the Joanna Briggs Institute (JBI) and adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) checklist to ensure methodological rigor and transparent reporting (Tricco et al., 2018; Hadie, 2024). Our approach encompassed defining the research question, conducting a comprehensive literature search, selecting studies based on predefined inclusion and exclusion criteria, extracting data using a standardized form, and synthesizing and reporting findings with consideration for practical and research implications. The review protocol was registered with INPLASY (registration number: INPLASY202570068). While registration was completed after data analysis had commenced, this retrospective registration was undertaken to promote transparency and protocol accessibility, in alignment with best practices outlined in the PRISMA-ScR and JBI guidance for scoping reviews.
2.2 Eligibility criteria
This review was guided by the Population–Concept–Context (PCC) framework recommended by the Joanna Briggs Institute (Hadie, 2024). The population of interest included patients diagnosed with various dermatological conditions, including but not limited to acne, eczema, and psoriasis. The concept focused on GBL interventions specifically designed for educational purposes. The context encompassed patient education in dermatology across all healthcare and community settings. To ensure the relevance and currency of the evidence, the review included studies published from January 2005 to May 2025 and limited to English-language publications due to practical constraints. Eligible study designs included randomized controlled trials, experimental studies, and observational research. Only peer-reviewed primary research articles were considered; grey literature, dissertations, conference abstracts, and letters to the editor were excluded to maintain a high standard of evidence quality and ensure the findings were grounded in fully evaluated work. Furthermore, studies focusing exclusively on social media-based interventions or telemedicine approaches without defined game-based elements were excluded to preserve the review’s specific focus on GBL strategies.
2.3 Information sources and search strategy
Conducting a preliminary iterative and pilot search of relevant databases informed the development of the final search strategy. The initial set of searches was conducted on April 16, 2025, across major electronic databases, including Scopus, MEDLINE, and the Directory of Open Access Journals (DOAJ), as these databases are widely recognized for publishing research in medical education and dermatology. Given the variability in terminology used to describe dermatological conditions and game-based learning strategies, the search terms were intentionally kept broad during the initial phase to ensure comprehensive coverage of the topic. The authors collaboratively finalized the search terms following detailed consultation with a health sciences librarian. The search strategy incorporated Medical Subject Headings (MeSH) and related keywords such as “dermatological conditions,” “game-based learning,” and “patient education.” These were combined with relevant synonyms and refined using Boolean operators (“AND,” “OR,” and “NOT”) to enhance the precision and relevance of the search results. The final database search was completed on May 5, 2025.
The initial search strategy was developed by the corresponding author and refined in consultation with the review team. The following is an example of a search strategy used in one of the databases (Scopus):
( TITLE-ABS-KEY (“game-based learning” OR “serious games” OR gamification OR “educational games” OR “digital games” OR “interactive learning” OR “educational media” OR animation ) )
AND ( TITLE-ABS-KEY (dermatology OR “skin disease” OR “cutaneous” OR acne OR eczema OR psoriasis OR melanoma OR dermatitis OR leishmaniasis OR “cutaneous malignancies” OR “skin cancer” ) )
AND ( TITLE-ABS-KEY (education OR learning OR awareness OR training ) )
AND ( PUBYEAR > 2004 AND PUBYEAR < 2026 )
AND ( DOCTYPE (ar) )
AND ( LANGUAGE ( english ) )
The complete search strategies for each database are provided in the Supplementary File.
2.4 Study selection
The study selection process involved multiple stages with predefined criteria to minimize selection bias. Initially, two independent reviewers (WT and CE) screened titles and abstracts of all retrieved citations against the eligibility criteria. Articles that potentially met inclusion criteria or where there was uncertainty proceeded to full-text assessment. At the full-text review stage, the same two independent reviewers assessed the complete articles for final inclusion determination. Any disagreements between reviewers at either the title/abstract screening or full-text review stages were resolved through discussion until consensus was reached, with a third reviewer (DM) available to arbitrate when necessary. Reasons for full-text exclusions were documented, and Figure 1 presents the PRISMA-ScR flow diagram detailing the number of studies included and excluded at each stage.
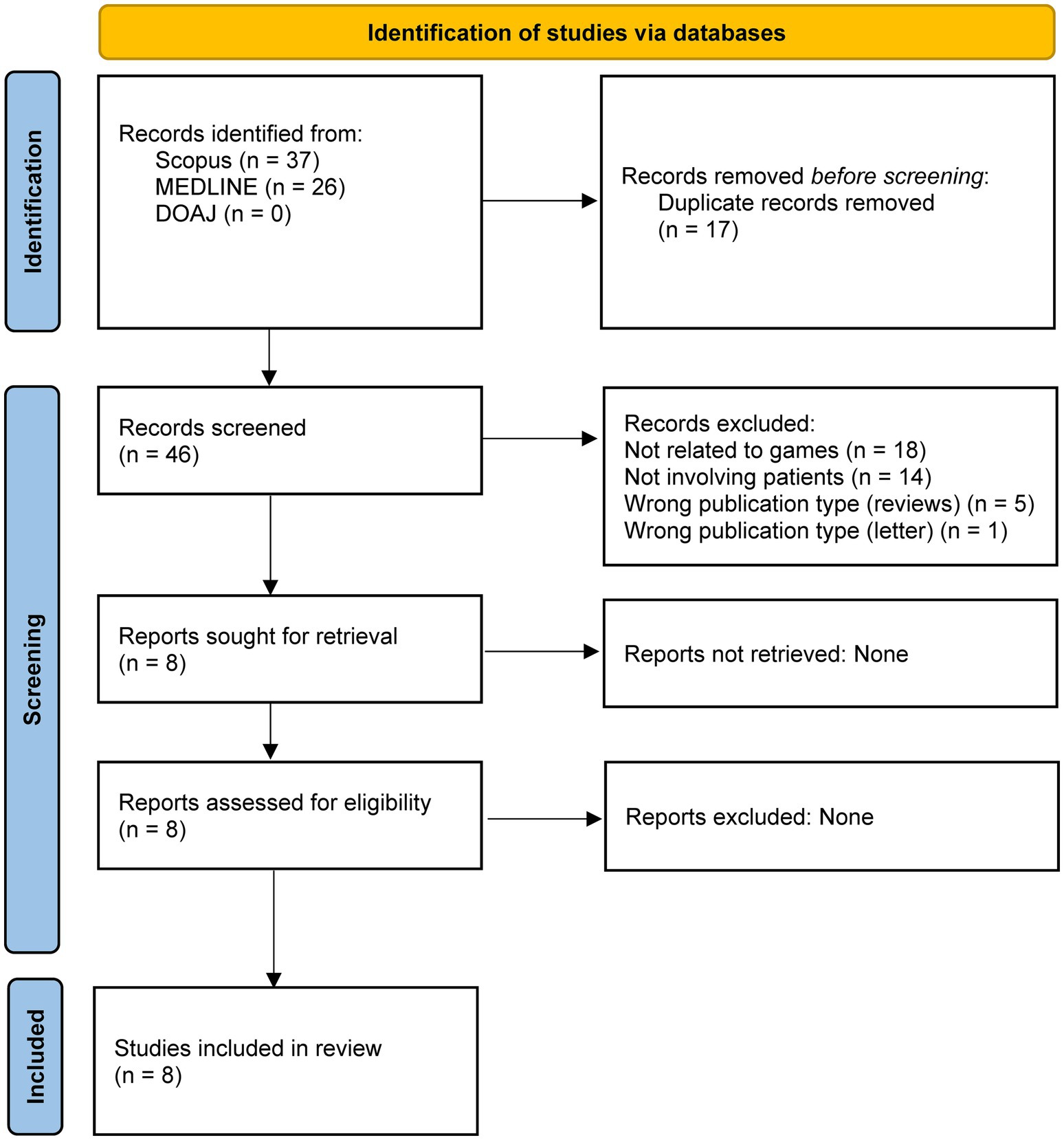
Figure 1. PRISMA-ScR flow diagram illustrating the study selection process for the scoping review. DOAJ, Directory of Open Access Journals; MEDLINE, Medical Literature Analysis and Retrieval System Online.
2.5 Data extraction
After selecting the eligible studies, we systematically extracted relevant data using a standardized manual extraction form. Two reviewers (WT and CE) independently performed the data extraction to ensure accuracy and completeness. Key variables included publication details (year, country, study design, sample size, and follow-up duration), participant characteristics (age, gender, education level, and, where available, socioeconomic status), and specific features of the game-based interventions (type of game, platform used, frequency and duration, and underlying pedagogical approach). The category of game-based patient education was defined in the Supplementary File. We also recorded the dermatological conditions addressed, comparator interventions where applicable, and a range of patient education outcomes, such as knowledge improvement, behavioral change, treatment adherence, self-efficacy, satisfaction, and quality of life. In line with recommendations for basic critical appraisal, we noted whether studies reported digital usability testing—such as user satisfaction, feasibility, or engagement—and whether standardized outcome measures were employed. Where reported, we also documented the theoretical frameworks used to guide intervention development. Any disagreements between reviewers were resolved through discussion, with input from a third reviewer (DM) when needed.
2.6 Risk of Bias and methodological quality assessment
Two investigators (WT and CE) independently assessed the methodological quality and risk of bias of the included studies. Any disagreements were resolved through discussion with a third reviewer (DM). For randomized controlled trials (RCTs), the Cochrane Risk of Bias 2 (RoB 2) tool was used, which evaluates five domains and categorizes the overall risk as low, some concerns, or high (Flemyng et al., 2023). For quasi-experimental or non-randomized studies, the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool was employed, which assesses seven domains and classifies the overall risk as low, moderate, serious, or critical (Jüni et al., 2016).
2.7 Data synthesis
In light of the heterogeneity among study designs, interventions, and outcomes, we employed a narrative synthesis approach guided by a widely used methodological framework (Popay et al., 2006). The synthesis followed four interrelated components. First, we outlined an implicit theory of how game-based interventions support patient education in dermatology—emphasizing mechanisms such as increased engagement, interactive learning, and reinforcement through gameplay. Second, we developed a preliminary synthesis by organizing and summarizing findings from included studies through tabulated data and textual descriptions. Studies were grouped according to dermatological conditions, educational goals, and game formats. Third, to explore relationships within and across studies, we used thematic and content analysis to identify common patterns, such as intervention effectiveness, design features associated with positive outcomes, and variations by target population. Finally, we assessed the robustness of the synthesis by considering factors such as study design, sample size, digital usability testing, and use of standardized outcome measures. This approach enabled a transparent, systematic integration of diverse findings, providing both descriptive and conceptual insights into the role of game-based learning in dermatologic patient education. Findings are presented in both narrative form and summary tables to support interpretation and highlight evidence gaps.
2.8 Ethical considerations
The study was approved by the Walailak University Ethics Committee (WUEC-25-122-01). As this was a scoping review involving the analysis of previously published, publicly accessible data, no new data were collected from human participants, and formal informed consent was not required.
3 Results
This scoping review included eight studies published between 2018 and 2025 that explored the application of game-based learning (GBL) for patient education in dermatology (Table 1). Study designs varied and included three randomized controlled trials, two quasi-experimental studies, one experimental study, and two single-arm feasibility or pre-post studies. Sample sizes ranged from 21 to 1,205 participants. The dermatologic conditions targeted by these interventions included melanoma (n = 4), atopic dermatitis (n = 1), cutaneous leishmaniasis (n = 1), general cutaneous malignancies (n = 1), and sun protection for skin cancer prevention (n = 1). Participants encompassed a wide age range—from school-aged children to older adults—and were recruited from both educational and clinical settings. The risk of bias assessment is summarized in Tables 2, 3.
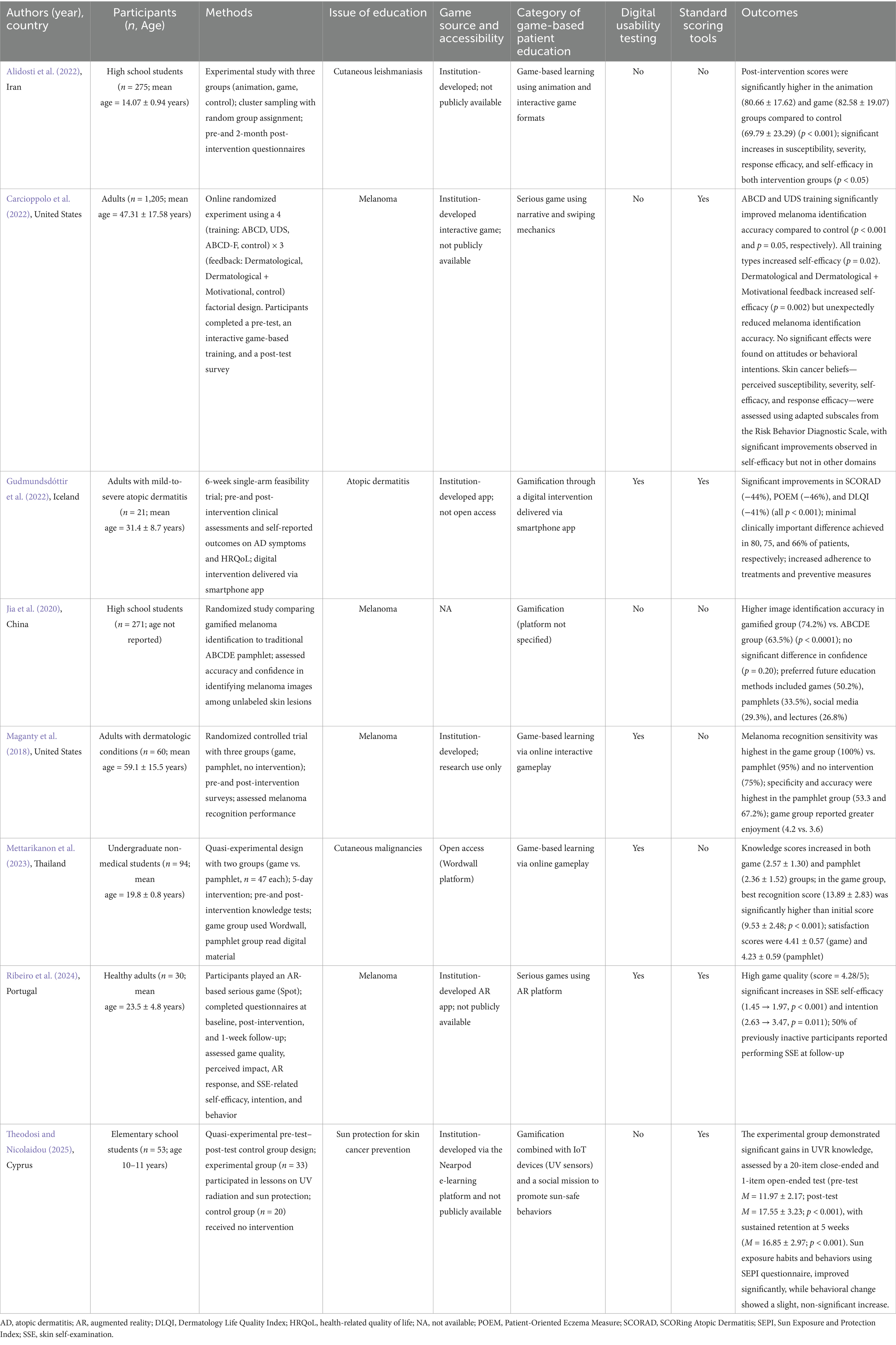
Table 1. Summary of studies on game-based patient education in dermatology.

Table 2. Risk of bias assessment for randomized controlled trials using Cochrane Risk of Bias 2 tool (RoB2).
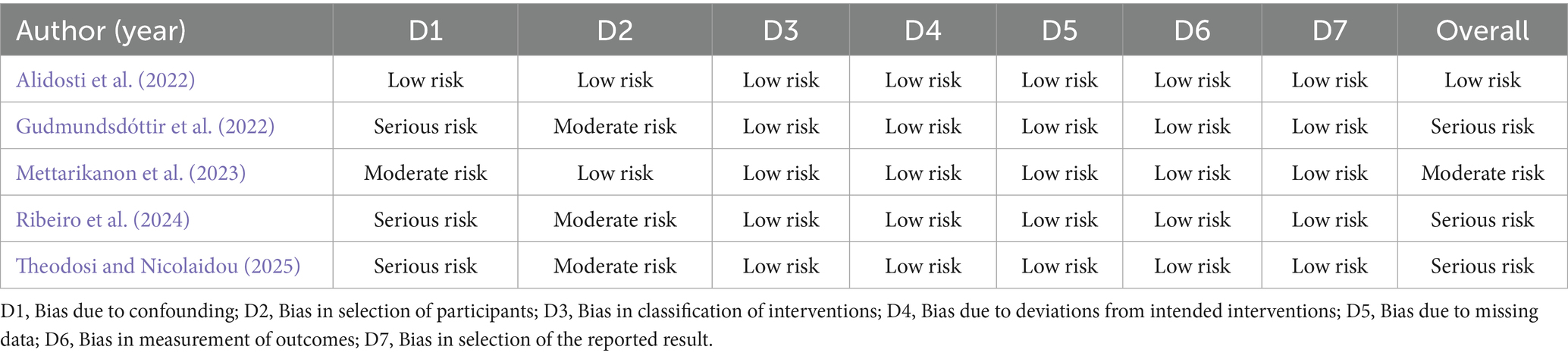
Table 3. Risk of bias assessment for non-randomized controlled trials using Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I).
3.1 Knowledge enhancement and recognition accuracy
Six studies out of a total of eight reported improvements in knowledge acquisition following GBL interventions (Alidosti et al., 2022; Carcioppolo et al., 2022; Jia et al., 2020; Maganty et al., 2018; Mettarikanon et al., 2023; Theodosi and Nicolaidou, 2025). In melanoma-focused studies, participants who engaged with game-based or gamified platforms demonstrated significantly higher image recognition accuracy compared to those receiving traditional pamphlet-based education (Carcioppolo et al., 2022; Jia et al., 2020; Maganty et al., 2018; Ribeiro et al., 2024). Mettarikanon et al. (2023) found that undergraduate students using a game-based tool significantly improved their recognition of cutaneous malignancies compared to those using digital pamphlets. Alidosti et al. (2022) reported increased knowledge scores related to cutaneous leishmaniasis among adolescents after an interactive game-based intervention. Similarly, Theodosi and Nicolaidou (2025) demonstrated significant gains in ultraviolet radiation (UVR) knowledge among elementary school students who participated in a gamified sun protection program.
3.2 Behavioral outcomes and adherence
Behavioral outcomes were reported in three studies. Gudmundsdóttir et al. (2022) observed improved adherence to treatment and preventive measures in patients with atopic dermatitis following engagement with a gamified digital intervention. Ribeiro et al. (2024) reported that 50% of participants who were previously inactive in performing skin self-examinations initiated this behavior after using an augmented reality–based serious game. Theodosi and Nicolaidou (2025) demonstrated significant improvements in sun exposure habits and protection behaviors among elementary school students after participating in a gamified intervention incorporating Internet of Things (IoT) devices, although the observed behavioral change was not statistically significant.
3.3 Clinical outcomes and symptom improvement
Clinical outcomes were reported in one study. Gudmundsdóttir et al. (2022) demonstrated significant reductions in disease severity and quality-of-life impairment among patients with atopic dermatitis following a gamified digital intervention. Specifically, mean scores decreased by 44% for SCORing Atopic Dermatitis (SCORAD), 46% for the Patient-Oriented Eczema Measure (POEM), and 41% for the Dermatology Life Quality Index (DLQI), indicating both clinical and health-related quality-of-life improvements.
3.4 Patient satisfaction and engagement
Two studies evaluated user satisfaction and engagement. Participants in the game-based groups consistently reported greater enjoyment and preference for interactive formats compared to traditional methods (Maganty et al., 2018; Mettarikanon et al., 2023). Preference data from Jia et al. (2020) indicated that 50.2% of participants favored game-based education over lectures, pamphlets, or social media.
Four studies evaluated user satisfaction and engagement with game-based interventions. Participants in the game-based groups consistently reported greater enjoyment and preference for interactive formats compared to traditional educational methods (Maganty et al., 2018; Mettarikanon et al., 2023). Jia et al. (2020) found that 50.2% of participants preferred game-based education over lectures, pamphlets, or social media platforms. Similarly, Ribeiro et al. (2024) reported high ratings for game quality and user engagement following the use of an augmented reality–based serious game, supporting the acceptability of immersive digital formats in patient education.
3.5 Digital usability and standardized tools
Digital usability testing was conducted in five studies, primarily focusing on user satisfaction, feasibility, and perceived impact (Carcioppolo et al., 2022; Gudmundsdóttir et al., 2022; Mettarikanon et al., 2023; Ribeiro et al., 2024; Theodosi and Nicolaidou, 2025). However, only three studies employed validated outcome measures: Gudmundsdóttir et al. (2022) used SCORAD, POEM, and DLQI; Ribeiro et al. (2024) applied standardized self-efficacy scales; and Carcioppolo et al. (2022) utilized adapted subscales from the Risk Behavior Diagnostic Scale. The remaining studies relied on unvalidated or self-developed instruments to assess educational outcomes, limiting comparability across interventions.
3.6 Methodological characteristics and access considerations
The included studies exhibited notable methodological heterogeneity in terms of design, sample size, and outcome evaluation. Three studies employed randomized controlled trials (Carcioppolo et al., 2022; Jia et al., 2020; Maganty et al., 2018), while the remaining five used quasi-experimental (Mettarikanon et al., 2023; Theodosi and Nicolaidou, 2025), experimental (Alidosti et al., 2022), or single-arm feasibility designs (Gudmundsdóttir et al., 2022; Ribeiro et al., 2024). Sample sizes ranged widely, from 21 to 1,205 participants. Most studies utilized pre-and post-intervention assessments to evaluate outcomes related to knowledge acquisition, recognition accuracy, behavioral changes, or clinical improvement. However, the duration, intensity, and structure of the interventions varied considerably across studies. With respect to accessibility, six studies out of a total of eight used institution-developed games that were not publicly available or commercially distributed (Alidosti et al., 2022; Carcioppolo et al., 2022; Gudmundsdóttir et al., 2022; Maganty et al., 2018; Ribeiro et al., 2024; Theodosi and Nicolaidou, 2025). Only one study (Mettarikanon et al., 2023) implemented an open-access platform (Wordwall), offering greater potential for replication and scalability. Notably, none of the included studies utilized commercially available or off-the-shelf educational games.
Regarding outcome measurement, three studies (Carcioppolo et al., 2022; Gudmundsdóttir et al., 2022; Ribeiro et al., 2024) employed validated tools such as SCORAD, POEM, DLQI, or adapted self-efficacy scales. The remaining studies relied on self-developed instruments, which may limit the comparability and rigor of findings. Digital usability testing was conducted in five studies, often focusing on user satisfaction, feasibility, or engagement with the intervention. Overall, these findings underscore the need for greater methodological standardization and consistent use of validated instruments in future research. In addition, the limited accessibility of most game-based tools highlights a critical barrier to widespread implementation. Future efforts should emphasize transparency in design, broader dissemination, and the development of open-access or adaptable formats to support integration into diverse clinical and educational contexts.
4 Discussion
This review provides preliminary evidence supporting the potential of GBL as an engaging educational tool for dermatology patients. Across the eight included studies, game-based interventions—including gamification, serious games, and augmented reality—were associated with improvements in knowledge acquisition, clinical outcomes, and self-management behaviors. Participants often preferred game-based formats over traditional educational methods, highlighting the appeal and acceptability of these approaches. However, these findings must be interpreted with caution due to the limited number of studies, and methodological heterogeneity. In addition, assessments of bias risk in the eight included studies indicated considerable methodological diversity. Of the randomized controlled trials, two out of three studies (Carcioppolo et al., 2022; Maganty et al., 2018) exhibited a low overall risk of bias, thereby enhancing confidence in their results, while one study (Jia et al., 2020) presented concerns due to complications with randomization and attrition. Among the five non-randomized studies, the majority (3 out of 5) (Gudmundsdóttir et al., 2022; Ribeiro et al., 2024; Theodosi and Nicolaidou, 2025) exhibited a significant overall risk of bias, mostly attributable to confounding factors and non-randomized methodologies. Only one non-randomized study Alidosti et al. (2022) demonstrated a low risk, although another research (Mettarikanon et al., 2023) was evaluated as having a moderate risk. These methodological concerns suggest that whereas randomized trials often yield trustworthy information, the results from non-randomized research need careful interpretation due to potential confounding or selection bias affecting good outcomes. This highlights the essential requirement for stringent study designs in forthcoming investigations, emphasizing the importance of randomized trials or strong quasi-experimental studies that explicitly account for confounding variables. It is essential that researchers and educators carefully analyze these findings and implement methodological safeguards to accurately determine intervention efficacy.
The effectiveness of game-based learning in patient education is supported by multiple complementary theoretical frameworks. Behaviorist principles explain how games use reinforcement mechanisms to shape health behaviors through immediate feedback and rewards, while cognitive learning theory illuminates how games structure information in ways that optimize processing and retention (Akl et al., 2013; Gorbanev et al., 2018). The humanistic elements of games foster emotional engagement and self-efficacy that traditional education often lacks, addressing the psychological barriers to treatment adherence that are particularly relevant in chronic dermatological conditions (Kleptsova et al., 2018). Constructivist approaches in game design create environments where patients actively experiment and build understanding through direct experience rather than passive instruction (Koskinen, 2014). This theoretical convergence explains why educational games—particularly those employing cognitive principles—have demonstrated significant advantages in enhancing patient knowledge, motivation, and self-management capabilities beyond conventional educational approaches (Abramson, 2013; Černý, 2023; Mann, 2011; Shandruk et al., 2019). Findings from previous studies support this multidimensional pedagogical approach. Alidosti et al. (2022) demonstrated significant improvements in knowledge and perceived self-efficacy regarding cutaneous leishmaniasis prevention among high school students following both animation-and game-based interventions, underpinned by behaviorist, cognitive, humanistic, and constructivist strategies (Alidosti et al., 2022). Similarly, Gudmundsdóttir et al. (2022) reported clinically meaningful reductions in atopic dermatitis severity scores, along with improved quality of life, following a gamified digital intervention that integrated behavioral and cognitive principles (Gudmundsdóttir et al., 2022). In melanoma education, gamified interventions showed greater accuracy in image recognition (Jia et al., 2020) and higher sensitivity in melanoma detection (Maganty et al., 2018) when compared to traditional pamphlet-based learning. The integration of game elements into digital platforms not only improved learning outcomes but also promoted higher user satisfaction and adherence (Mettarikanon et al., 2023; Ribeiro et al., 2024). These outcomes emphasize the value of embedding diverse pedagogical strategies into game design to address various cognitive and emotional learning needs across different populations and dermatological conditions. Collectively, the evidence underscores the promise of game-based education as a dynamic and patient-centered tool in dermatological health promotion.
To guide the conceptual synthesis of outcomes, this review employed the Kirkpatrick framework—a widely recognized model for evaluating educational interventions across four levels: Reaction, Learning, Behavior, and Results (Moreau, 2017; Alhassan, 2022). Originally developed for workplace training, the model has since been adapted for use in various educational contexts, including patient education and digital learning environments. Among the eight studies included, five (Gudmundsdóttir et al., 2022; Jia et al., 2020; Maganty et al., 2018; Mettarikanon et al., 2023; Ribeiro et al., 2024) addressed the Reaction level, reporting on user satisfaction, engagement, or expressed preferences for game-based approaches. All eight studies contributed to the Learning level by demonstrating gains in knowledge, recognition accuracy, or self-efficacy related to dermatological conditions. At the Behavior level, three studies (Gudmundsdóttir et al., 2022; Ribeiro et al., 2024; Theodosi and Nicolaidou, 2025) reported positive changes, including improved treatment adherence, initiation of skin self-examinations, and healthier sun protection behaviors. However, none of the included studies assessed higher-level outcomes such as long-term clinical impact or integration into healthcare systems, as outlined in the final level of the Kirkpatrick framework. Applying the Kirkpatrick framework highlights a concentration of evidence in early-stage outcomes, with limited insight into sustained or system-level effects. Future research should aim to address this gap by incorporating longer-term follow-up, validated outcome measures, and evaluations of broader healthcare impact. Integrating structured models such as the Kirkpatrick framework from the outset may also enhance methodological rigor and support more meaningful comparisons across studies.
4.1 Unique challenges in dermatology education and how GBL can address these issues
Effective dermatological education necessitates acknowledgment of the discipline’s distinct dependence on visual acuity, the changing expectations of modern learners, and the difficulty of long-term information retention. Furthermore, contemporary technology advancements provide improved access to dermatological information. Dermatology heavily relies on visual recognition for diagnosis, making it a field where visual tools can significantly enhance educational effectiveness (Ko et al., 2019). Most previous studies have focused on cutaneous malignancies, particularly melanoma, as these conditions benefit greatly from visually driven educational approaches. Visual aids often convey clinical information more effectively than text alone, making complex medical concepts more accessible and easier to understand (Paulovich, 2019). This is especially important for patients with low health literacy, where visual tools can significantly enhance comprehension and adherence to medical instructions (Ko et al., 2019). Combining visual content with game-based learning can create a more immersive and effective educational experience. Visuals help simplify complex concepts, while games offer interactive and engaging methods to reinforce learning (Davis et al., 2024). Educational games can be tailored to individual patient needs, enhancing relevance and effectiveness. Additionally, visual content can be customized to match the patient’s level of understanding, ensuring that the information is both accessible and comprehensible (Paulovich, 2019; Martin-Gomez et al., 2021).
Contemporary learners, particularly from Generation Y and Z, frequently perceive conventional teaching techniques as tedious and misaligned with their learning preferences, as they inherently choose interactive and technology-enhanced educational experiences (Kliesener et al., 2024). Generation Z learners exhibit a pronounced preference for pedagogical methods that integrate technology with experiential involvement, as research indicates that learners demonstrate significantly higher engagement levels during lectures utilizing tools such as audience response clickers in contrast to traditional lecture formats (Hampton et al., 2020) The disparity between conventional pedagogical methods and contemporary student expectations engenders a significant mismatch, frequently leading to diminished motivation and engagement in the classroom (Ali et al., 2017). Previous studies indicate that GBL presents an effective approach, with significant outcomes such as heightened student engagement, enhanced material retention, and the robust development of critical thinking abilities (Riyandi et al., 2023). Educational games often operate through three fundamental strategies that engage learners: delivering rapid feedback to learners, presenting prizes and successes that incentivize ongoing involvement, and establishing clear progression pathways that illustrate learners’ growth. Effective GBL environments typically integrate recognizable components such as leaderboards that promote friendly rivalry, badges that acknowledge achievements, point systems that monitor progress, and leveling mechanisms that offer a feeling of progression. Research consistently demonstrates that integrating game-like features into education markedly enhances student engagement; however, educators and researchers acknowledge the necessity for more comprehensive studies to thoroughly comprehend the specific effects of these gaming elements on student learning and information retention.
Knowledge retention is a considerable challenge in education, including dermatology. One of the most critical factors influencing knowledge retention is the choice of teaching methods. Conventional lectures and GBL have demonstrated similar short-term effectiveness in improving material retention among learners (Riyandi et al., 2023). However, GBL frequently outperforms traditional lectures in enhancing long-term information retention. A prior study shown significantly enhanced long-term retention in participants involved in a board game seminar compared to those attending traditional lectures, particularly in assessments conducted 14 days post-intervention (Karbownik et al., 2016). Another study indicated that learners employing game-based computer programs had superior long-term recall relative to those participating in lecture-based sessions (Hu et al., 2022). A meta-analysis confirmed comparable results, indicating that serious games enhance learning outcomes and retention, while they do not consistently surpass traditional methods in terms of learner motivation (Wouters et al., 2013). GBL markedly improves information acquisition by increasing learner involvement and engagement within the classroom environment. Enhancing information retention in dermatological education necessitates a comprehensive approach that integrates interactive, technology-driven learning approaches, regular assessment techniques, and ongoing faculty development (Mahmood, 2024; Watchmaker et al., 2019). By employing these varied strategies, educators can significantly enhance learners’ capacity to retain and apply dermatological knowledge over time.
In the digital age, learners increasingly favor education that is available at any time and place, enabling them to learn at their own speed, in their preferred manner, and under their chosen circumstances (Singh, 2016). GBL effectively utilizes digital technologies and internet platforms to enhance information dissemination beyond conventional approaches like brochures or verbal instruction. Nevertheless, certain educational resources remain inaccessible to the public, limiting options for learners seeking information about similar or identical clinical conditions. Making these materials openly accessible can significantly improve knowledge dissemination, enabling learners with similar clinical presentations to easily obtain relevant information. Moreover, the internet provides flexible learning options, allowing individuals who cannot attend traditional educational settings to access content remotely and at their convenience. Thus, publicly available online platforms and digital resources substantially enhance information distribution and broaden educational accessibility (Steyaert, 2005).
4.2 Review limitations and future directions
This scoping review has several limitations. First, the included studies employed diverse designs—such as randomized controlled trials, quasi-experimental designs, and single-arm pre-post interventions—which may introduce methodological inconsistencies, selection bias, and a lack of control conditions, thereby affecting the internal validity of findings. Second, most studies featured short follow-up periods, limiting the ability to assess long-term knowledge retention, sustained behavior change, or the durability of clinical benefits over time. Third, there was considerable heterogeneity in the game-based learning approaches utilized, including gamification, serious games, and digital simulations. This variability, combined with differences in educational objectives and dermatologic conditions, complicates cross-study comparisons and generalization of findings. Fourth, the use of non-standardized outcome measures in several studies led to inconsistencies in evaluating the effectiveness of game-based learning. Only a minority employed validated instruments, which limits the comparability and reliability of reported outcomes. Fifth, although most studies reported favorable results, the generalizability of these findings is limited due to small sample sizes, varying levels of methodological rigor, and a predominant focus on younger adults or student populations. Older adults and individuals with limited digital literacy were underrepresented, despite being important target groups in dermatology. Furthermore, six out of the eight interventions were institutionally developed and not publicly accessible, which restricts opportunities for replication, broader implementation, and external validation in diverse settings. Sixth, several barriers to implementation should be acknowledged. Challenges such as limited digital literacy, age-related difficulties with technology use, and unequal access to mobile devices may hinder the scalability and inclusivity of GBL interventions. Additionally, ensuring cultural and linguistic relevance is essential for engaging diverse patient populations. Privacy and ethical considerations surrounding the collection and use of health-related data on digital platforms also warrant careful attention. To promote equitable adoption in clinical practice, educational games must be designed to be inclusive, user-friendly, secure, and adaptable to various patient needs. Finally, although this review focuses on dermatology, its findings may have broader implications for other visually dependent specialties, such as ophthalmology and radiology, where patient education and diagnostic accuracy also rely heavily on visual recognition. Furthermore, certain pedagogical strategies used in GBL—such as interactive simulations—may also enhance medical education for clinicians, particularly in developing diagnostic reasoning and decision-making skills. These limitations should be considered when interpreting the results. Future research should prioritize rigorous, multicenter randomized controlled trials involving diverse and representative populations. In addition, studies should evaluate long-term outcomes, compare GBL with other digital education modalities (e.g., virtual reality), and explore the integration of AI-driven personalization and adaptive learning technologies to enhance engagement and optimize individual learning experiences.
5 Conclusion
GBL represents a promising and innovative approach to patient education in dermatology, particularly for visually oriented conditions such as melanoma and atopic dermatitis. Preliminary evidence suggests that GBL interventions may enhance patient knowledge, support self-management, and improve adherence to treatment recommendations through engaging and interactive formats. By incorporating visually rich and interactive content, these tools can help simplify complex dermatological information and make learning more patient-centered. However, given the limited number of available studies, methodological variability, and underrepresentation of diverse populations, these findings should be interpreted with caution. The current evidence base remains preliminary, and high-quality research is needed to assess long-term clinical outcomes, sustained behavior change, and real-world implementation. Studies should also prioritize methodological rigor—employing validated outcome measures, longer-term follow-up, and robust strategies to minimize bias. Additionally, extending the use of GBL to a wider array of dermatologic conditions and incorporating advanced features, including AI-driven personalization, may further improve learning outcomes and support equitable access to education.
Author contributions
DM: Methodology, Validation, Formal analysis, Investigation, Writing – review & editing, Writing – original draft. CE: Investigation, Supervision, Writing – review & editing, Formal analysis. WT: Methodology, Data curation, Investigation, Conceptualization, Writing – review & editing, Visualization, Writing – original draft, Project administration, Formal analysis, Validation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. This manuscript was edited with the assistance of a generative AI tool (ChatGPT, GPT-4 model, OpenAI), which was used solely for language improvement and formatting. All content, including data interpretation, analysis, and conclusions, was generated and verified by the authors.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2025.1636364/full#supplementary-material
References
Abramson, C. I. (2013). Problems of teaching the behaviorist perspective in the cognitive revolution. Behav. Sci. 3, 55–71. doi: 10.3390/bs3010055
Akl, E. A., Kairouz, V. F., Sackett, K. M., Erdley, W. S., Mustafa, R. A., Fiander, M., et al. (2013). Educational games for health professionals. Cochrane Database Syst. Rev. 2013:CD006411. doi: 10.1002/14651858.CD006411.pub4
Al Fatta, H., Maksom, Z., and Zakaria, M. H. (2018). Game-based learning and gamification: searching for definitions. Int. J. Simulat. Syst. Sci. Technol. 19, 41.1–41.5. doi: 10.5013/IJSSST.a.19.06.41
Alagheband, S. J., Miller, J. J., and Clarke, J. T. (2015). Individualizing patient education for greater patient satisfaction. Cutis 95, 291–292
Alhassan, A. I. (2022). Implementing faculty development programs in medical education utilizing Kirkpatrick’s model. Adv. Med. Educ. Pract. 13, 945–954. doi: 10.2147/AMEP.S372652
Ali, R., Jamil, N. I., Ahmad, S. N. D., Mohamed, N., and Yaacob, N. A. (2017). The impact of Xrace game board as an experiential learning approach. Adv. Sci. Lett. 23, 10648–10651. doi: 10.1166/asl.2017.10122
Alidosti, M., Shahnazi, H., Heidari, Z., and Zamani-Alavijeh, F. (2022). Design and evaluation of two educational media in the form of animation and games to promote the cutaneous leishmaniasis prevention behaviors in adolescent female. BMC Public Health 22:2288. doi: 10.1186/s12889-022-14772-8
Allison, K. (2012). Adherence through education: a call to clinicians to educate all patients on medication use. Ment. Health Clin. 2, 83–85. doi: 10.9740/mhc.n117761
Carcioppolo, N., Kim, S., Sanchez, M., Mao, B., Malova, E., and Ryan, A. (2022). Evaluating a game-based randomized experiment to increase melanoma identification among adults living in the US. Soc. Sci. Med. 310:115281. doi: 10.1016/j.socscimed.2022.115281
Cascella, M., Cascella, A., Monaco, F., and Shariff, M. N. (2023). Envisioning gamification in anesthesia, pain management, and critical care: basic principles, integration of artificial intelligence, and simulation strategies. J. Anesth. Analg. Crit. Care 3:33. doi: 10.1186/s44158-023-00118-2
Černý, M. (2023). “Theoretical background of education and research in IVR” in Learning and teaching in virtual reality: possibilities and limits of collaborative immersive virtual environments (Brno: Masarykova univerzita).
Chang, Y. I., Kovalchuk, I., Savytska, M., and Zayachkivska, O. (2024). Building active learning in medical education: how to bridge vision with real practice? Proceedings of the Shevchenko scientific society. Medical sciences, 76.
Crawford, T., Roger, P., and Candlin, S. (2018). Supporting patient education using schema theory: a discourse analysis. Collegian 25, 501–507. doi: 10.1016/j.colegn.2017.12.004
Davis, K., Gowda, A. S., Thompson-Newell, N., Maloney, C., Fayyaz, J., and Chang, T. (2024). Gamification, serious games, and simulation in health professions education. Pediatr. Ann. 53, e401–e407. doi: 10.3928/19382359-20240908-06
Feeley, T. H., Keller, M., and Kayler, L. (2023). Using animated videos to increase patient knowledge: a meta-analytic review. Health Educ. Behav. 50, 240–249. doi: 10.1177/10901981221116791
Flemyng, E., Moore, T. H., Boutron, I., Higgins, J. P., Hróbjartsson, A., Nejstgaard, C. H., et al. (2023). Using risk of Bias 2 to assess results from randomised controlled trials: guidance from Cochrane. BMJ Evid. Based Med. 28, 260–266. doi: 10.1136/bmjebm-2022-112102
Gorbanev, I., Agudelo-Londoño, S., González, R. A., Cortes, A., Pomares, A., Delgadillo, V., et al. (2018). A systematic review of serious games in medical education: quality of evidence and pedagogical strategy. Med. Educ. Online 23:1438718. doi: 10.1080/10872981.2018.1438718
Gudmundsdóttir, S. L., Ballarini, T., Ámundadóttir, M. L., Mészáros, J., Eysteinsdóttir, J. H., Thorleifsdóttir, R. H., et al. (2022). Clinical efficacy of a digital intervention for patients with atopic dermatitis: a prospective single-center study. Dermatol. Ther. 12, 2601–2611. doi: 10.1007/s13555-022-00821-y
Hadie, S. N. H. (2024). ABC of a scoping review: a simplified JBI scoping review guideline. Educ. Med. J. 16, 185–197. doi: 10.21315/eimj2024.16.2.14
Hampton, D., Welsh, D., and Wiggins, A. T. (2020). Learning preferences and engagement level of generation Z nursing students. Nurse Educ. 45, 160–164. doi: 10.1097/NNE.0000000000000710
Heratizadeh, A. (2014). Therapeutic patient education. Curr. Treat. Options Allergy 1, 358–364. doi: 10.1007/s40521-014-0033-x
Hu, H., Liu, Z., and Li, H. (2022). Teaching disaster medicine with a novel game-based computer application: a case study at Sichuan University. Disaster Med. Public Health Prep. 16, 548–554. doi: 10.1017/dmp.2020.309
Huang, H., and Hwang, G. J. (2019). Facilitating inpatients’ family members to learn: a learning engagement-promoting model to develop interactive e-book systems for patient education. Educ. Technol. Soc. 22, 74–87.
Jia, J. L., Shen, A., Tabata, M. M., and Sarin, K. Y. (2020). Gamification improves melanoma visual identification among high school students: results from a randomized study. Pediatr. Dermatol. 37, 752–753. doi: 10.1111/pde.14158
Jüni, P., Loke, Y., Pigott, T., Ramsay, C., Regidor, D., Rothstein, H., et al. (2016). Risk of bias in non-randomized studies of interventions (ROBINS-I): detailed guidance. Br. Med. J. 355:i4919.
Karbownik, M. S., Wiktorowska-Owczarek, A., Kowalczyk, E., Kwarta, P., Mokros, L., and Pietras, T. (2016). Board game versus lecture-based seminar in the teaching of pharmacology of antimicrobial drugs-a randomized controlled trial. FEMS Microbiol. Lett. 363:fnw045. doi: 10.1093/femsle/fnw045
Kleptsova, E. Y., Kleptsov, N. N., Mishutinskaya, E. A., Shubnitsyna, T. V., and Tsvetkova, N. V. (2018). Psychological structure of humane interpersonal relations among the subjects of educational activity. J. Pharm. Sci. Res. 10, 1844–1848.
Kliesener, T., Jandek, M., Navarini, A., Brandt, O., and Müller, S. (2024). Dermatology teaching for undergraduate medical students in clinical routine—a structured four-week curriculum. BMC Med. Educ. 24:116. doi: 10.1186/s12909-023-04921-x
Ko, C. J., Braverman, I., Sidlow, R., and Lowenstein, E. J. (2019). Visual perception, cognition, and error in dermatologic diagnosis: key cognitive principles. J. Am. Acad. Dermatol. 81, 1227–1234. doi: 10.1016/j.jaad.2018.10.082
Koskinen, H. I. (2014). From constructivism to realism: a new approach to see teaching and learning in natural sciences. Int. J. Sci. Math. Technol. Learn. 20, 51–59. doi: 10.18848/2327-7971/CGP/v20i01/49025
Lamb, R. L., Annetta, L., Firestone, J., and Etopio, E. (2018). A meta-analysis with examination of moderators of student cognition, affect, and learning outcomes while using serious educational games, serious games, and simulations. Comput. Hum. Behav. 80, 158–167. doi: 10.1016/j.chb.2017.10.040
Maganty, N., Ilyas, M., Zhang, N., and Sharma, A. (2018). Online, game-based education for melanoma recognition: a pilot study. Patient Educ. Couns. 101, 738–742. doi: 10.1016/j.pec.2017.11.003
Mahmood, M. N. (2024). Dermatopathology rotation and education for residents: the art and science of traditional and innovative pedagogic methods. Skinmed 22, 332–338
Mann, K. V. (2011). Theoretical perspectives in medical education: past experience and future possibilities. Med. Educ. 45, 60–68. doi: 10.1111/j.1365-2923.2010.03757.x
Martin-Gomez, A., Hill, C., Lin, H. Y., Fotouhi, J., Han-Oh, S., Wang, K. K. H., et al. (2021). Towards exploring the benefits of augmented reality for patient support during radiation oncology interventions. Comput. Methods Biomech. Biomed. Engin. Imaging Vis. 9, 322–329. doi: 10.1080/21681163.2020.1835547
Mettarikanon, D., Tawanwongsri, W., Wanchai, A., and Chookerd, N. (2023). Comparison of the efficacy between game-based learning and pamphlet on enhancing recognition of common cutaneous malignancies in Thai younger adults. Contemporary. Educ. Technol. 15:ep419. doi: 10.30935/cedtech/13013
Miller, T. A., and Dimatteo, M. R. (2015). Patient adherence to health care regimens. Int. Encycl. Soc. Behav. Sci. 17, 598–602. doi: 10.1016/B978-0-08-097086-8.14113-3
Moreau, K. A. (2017). Has the new Kirkpatrick generation built a better hammer for our evaluation toolbox? Med. Teach. 39, 999–1001. doi: 10.1080/0142159X.2017.1337874
Paulovich, B. (2019). “Communicating health information to patients: a collaborative visual communication design approach” in Learning to see: the meanings, modes and methods of visual literacy. eds. M. Heitkemper-Yates and K. Kaczmarczyk (Leiden, The Netherlands: Brill).
Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., et al. (2006). Guidance on the conduct of narrative synthesis in systematic reviews. A product from the Esrc methods programme Version, 1, b92.
Ribeiro, N., Tavares, P., Ferreira, C., and Coelho, A. (2024). Melanoma prevention using an augmented reality-based serious game. Patient Educ. Couns. 123:108226. doi: 10.1016/j.pec.2024.108226
Riyandi, M. A. O., Santoso, H. B., and Putra, P. O. H. (2023). The application of game mechanics and technological trend in game-based learning: a review of the research. J. Resti 7, 774–781. doi: 10.29207/resti.v7i4.4928
Shandruk, S. I., Smirnova, L. L., Cherednichenko, N. Y., Lysenko, L. O., Kapitan, T. A., Chernionkov, Y. A., et al. (2019). Future human development from the standpoint of dominant philosophical concepts of the United States pedagogical education. Astra Salvensis 7, 323–333.
Singh, R. (2016). Learner and learning in digital era: some issues and challenges. Int. Educ. Res. J. 2, 92–94.
Steyaert, J. (2005). Web-based higher education: the inclusion/exclusion paradox. J. Technol. Hum. Serv. 23, 67–78. doi: 10.1300/J017v23n01_05
Szeto, M. D., Strock, D., Anderson, J., Sivesind, T. E., Vorwald, V. M., Rietcheck, H. R., et al. (2021). Gamification and game-based strategies for dermatology education: narrative review. JMIR Dermatol. 4:e30325. doi: 10.2196/30325
Theodosi, S., and Nicolaidou, I. (2025). How can we help children adopt healthy sun protection habits? A quasi-experiment using internet of things (IoT), gamification, and a social mission. Educ. Inf. Technol. 30, 11583–11604. doi: 10.1007/s10639-024-13240-7
Tricco, A. C., Lillie, E., Zarin, W., O’brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 169, 467–473. doi: 10.7326/M18-0850
Watchmaker, J., Gonzales, E. C., and Larson, A. R. (2019). Interactive teaching and repeat exposure maximize medical student satisfaction but do not promote long-term retention of dermatologic knowledge. Dermatol. Online J. 25:13030/qt04w1t6dc. doi: 10.5070/D3259045507
Wouters, P., Van Nimwegen, C., Van Oostendorp, H., and Van Der Spek, E. D. (2013). A meta-analysis of the cognitive and motivational effects of serious games. J. Educ. Psychol. 105, 249–265. doi: 10.1037/a0031311
Xu, M., Luo, Y., Zhang, Y., Xia, R., Qian, H., and Zou, X. (2023). Game-based learning in medical education. Front. Public Health 11:1113682. doi: 10.3389/fpubh.2023.1113682
Zadeja, I., and Bushati, J. Gamification and serious games methodologies in education. International symposium on graphic engineering and design, (2022). 599–605.
Zhang, Q., and Yu, Z. (2022). Investigating and comparing the effects on learning achievement and motivation for gamification and game-based learning: a quantitative study employing Kahoot. Educ. Res. Int. 2022:9855328. doi: 10.1155/2022/1519880
Zhao, Y., and Zhang, J. (2017). Consumer health information seeking in social media: a literature review. Health Info. Libr. J. 34, 268–283. doi: 10.1111/hir.12192
Keywords: educational technology, patient education, dermatology, health knowledge, digital health education, game-based learning
Citation: Mettarikanon D, Eden C and Tawanwongsri W (2025) The role of game-based learning in dermatology: a scoping review on patient education. Front. Commun. 10:1636364. doi: 10.3389/fcomm.2025.1636364
Edited by:
Nashwa Ismail, Imperial College London, United KingdomReviewed by:
Ruano Juan, Hospital Universitario Reina Sofía, SpainMaosen Xu, Sichuan University, China
Mariela Bellotti, National University of Río Negro, Argentina
Copyright © 2025 Mettarikanon, Eden and Tawanwongsri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weeratian Tawanwongsri, d2VlcmF0aWFuLnRhQGdtYWlsLmNvbQ==