 Sridhar Prinitha
Sridhar Prinitha Tony P. Jose
Tony P. Jose- Department of Social Sciences, School of Social Sciences and Languages, Vellore Institute of Technology, Vellore, India
Introduction: In culturally conservative environments, adolescents are more likely to seek sexual health information from the internet, where traditional channels of communication are hindered. However, mere exposure to the internet does not directly translate into knowledge, as this relationship is shaped by critical individual factors, such as adolescents’ self-efficacy and functional digital health literacy.
Objective: The present study investigates the relationship between internet exposure and HIV/AIDS knowledge among Indian adolescents, specifically examining the mediating role of self-efficacy and the moderating role of functional digital health literacy.
Methods: Data for this study were drawn from Wave 2 (2018–19) of the Understanding the Lives of Adolescents and Young Adults (UDAYA) survey. The final sample included 6,103 adolescents (n = 2,159 males; n = 3,944 females). Statistical analyses included Spearman’s rank-order correlation, mediation and moderated mediation analysis using Hayes’ PROCESS macro.
Results: Correlational analysis showed that internet exposure was positively associated with HIV/AIDS knowledge (r = 0.21, p < 0.001). Mediation analysis revealed that self-efficacy significantly mediated this relationship (Bindirect = 0.004, 95% CI: 0.001, 0.007), accounting for 4.8% of the total effect. Moderated mediation analysis further demonstrated that this mediation effect was conditional on functional digital health literacy levels (Index = 0.01, 95% CI: 0.003, 0.02).
Conclusion: The findings indicate that self-efficacy acts as the mediator between internet exposure and HIV/AIDS knowledge, with functional digital health literacy moderating this process. Policymakers should incorporate comprehensive digital health literacy elements and self-efficacy enhancement strategies into current health education modules in order to maximize knowledge acquisition and intervention impact.
1 Introduction
Globally, 85% of adolescents possess personal mobile devices by the age of 14 [International Telecommunication Union (ITU), 2021] and dedicate nearly 6.6 hours daily to non-educational pursuits (Keeley and Little, 2017). Notably, one in every three individuals who use the internet is under the age of 18 (Keeley and Little, 2017), and in India, 50% of smartphone users are students between the ages 15 and 24 (Nielsen, 2018). This widespread digital access has established the internet access, digital literacy, and access to digital devices as digital determinants of health communication (World Health Organization and London School of Economics, 2024).
In India, comprehensive knowledge of HIV remains low. A UNICEF (2021) report states that only 28.2% of males and 18.5% of females aged 15–19 in 2016 have adequate knowledge. However, regional studies reveal a varied landscape. For instance, in one study from Assam, it was found that just over half of the adolescents possess sufficient knowledge (Habib et al., 2024). Another study noted that though the adolescents reported higher levels of knowledge, their attitude toward HIV was low (Khargekar et al., 2024). A longitudinal study using UDAYA data noted that awareness of HIV has increased in recent years, with internet use showing a strong association with this growth (Srivastava et al., 2021). Similarly, a cross-sectional analysis found that social media exposure significantly improved knowledge of sexual and reproductive health, including HIV/AIDS (Saha et al., 2022). However, these studies have primarily focused on establishing this direct association, without exploring the underlying psychological mechanisms that explain how or why internet use facilitates increased knowledge.
While digital platforms offer adolescents unprecedented access to health information, concerns remain regarding the credibility of such content and their capacity for critical evaluation (McKinnon et al., 2020). Although adolescents are often aware of the varying quality of online sources, they frequently lack the comprehensive skills needed to validate the information they encounter (Chereka et al., 2025; Freeman et al., 2018). To address this gap, digital health literacy, defined as the functional capacity to actively seek, comprehend, and evaluate health information from digital sources and apply this knowledge for health management (Norman and Skinner, 2006), constitutes the foundational toolkit for safely navigating the digital health landscape. The Transactional Model of eHealth Literacy outlines four competence levels: functional, communicative, critical, and translational. The present study focuses on the functional level, which reflects participants’ ability to successfully read and write about health using technological devices (Paige et al., 2018).
However, functional digital health literacy skills alone are insufficient; their effective application depends on psychological factors, particularly self-efficacy. Prior research has demonstrated the crucial role of self-efficacy in enhancing information processing and acquisition of health knowledge (Lo et al., 2013). Social Cognitive Theory (SCT) provides a conceptual framework for examining the interaction between internet exposure, self-efficacy, functional digital health literacy and HIV/AIDS knowledge. The theory posits that personal cognitive factors interact with environment to influence behavior (Bandura, 1986). In this framework, self-efficacy, an individual’s belief in their capacity to execute necessary actions to achieve a goal (Bandura, 1997), emerges as a key personal factor. Individuals with high self-efficacy approach challenging content more effectively, engage more readily, persist longer, and are less likely to abandon accurate reasoning prematurely, aided by stronger self-monitoring capabilities (Schunk and Pajares, 2009; Zimmerman, 2000). Therefore, the effectiveness of self-efficacy in health information processing depends on functional digital health literacy, particularly the practical ability to use digital technologies for health-related purposes.
Empirical evidence demonstrates associations between self-efficacy and digital health literacy. Research among Chinese social media users shows that self-efficacy is a key mechanism linking digital health literacy to health intentions (Niu et al., 2021) and a study among Chinese college students confirms self-efficacy’s mediating role between digital health literacy and health self-management behaviors (Zhou et al., 2025), alongside supportive findings from German fourth-graders (Fretian et al., 2020). However, contradictory results from Austrian students revealed no significant relationships (Pendl et al., 2023), suggesting contextual variability in this association. These divergent outcomes highlight a critical gap in the literature, which has predominantly focused on Western and East Asian populations. The present investigation addresses this gap by examining the role of self-efficacy and functional digital health literacy in HIV/AIDS knowledge acquisition among Indian adolescents, where unique sociocultural factors may influence health information behaviors.
To address this gap, this study leverages a unique conceptualization of self-efficacy available in the secondary data as autonomous decision-making across life domains. This approach contrasts sharply with disease-specific, general, or task-specific measures typically used in previous studies (Lo et al., 2013; Opoku et al., 2022) and provides a novel opportunity to explore how a broader sense of personal agency mediates health information processing. Figure 1 presents the conceptual model guiding this study. The aim is to examine the mediating role of this self-efficacy in the relationship between internet exposure and HIV/AIDS knowledge among Indian adolescents, with functional digital health literacy moderating the self-efficacy-knowledge pathway. By examining this moderated mediation, our findings will inform interventions that cultivate both decision-making autonomy and digital competencies for health empowerment. Accordingly, we propose the following hypotheses:
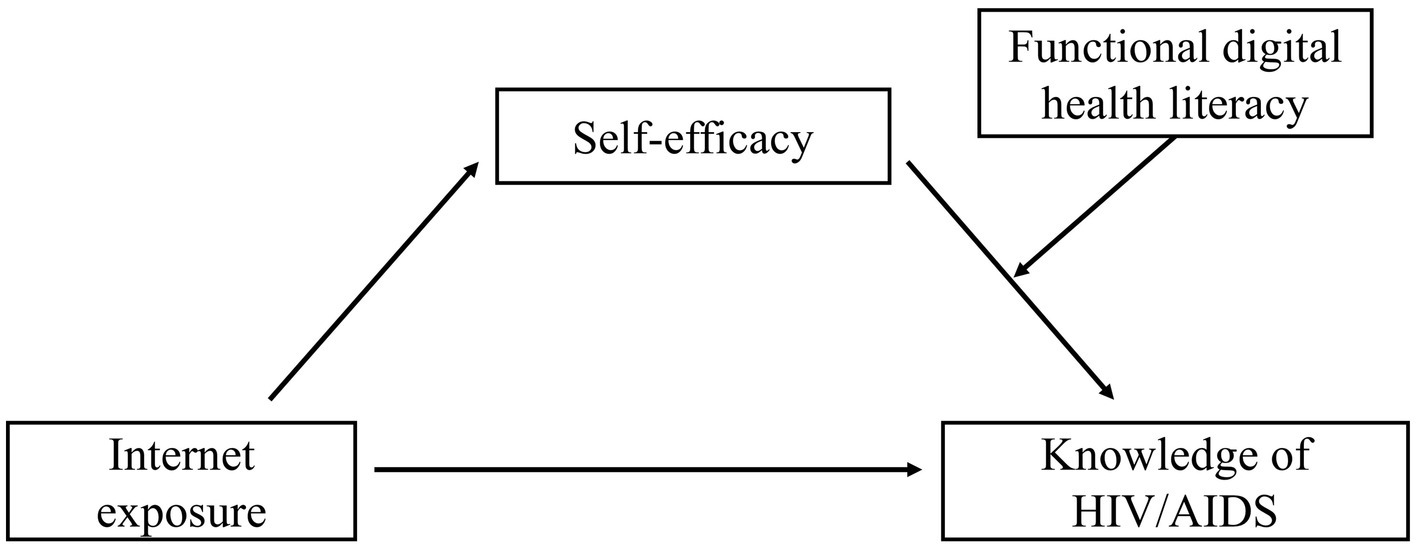
Figure 1. Conceptual model.
H1: Greater internet exposure is associated with higher levels of HIV/AIDS knowledge among adolescents.
H2: Self-efficacy mediates the relationship between internet exposure and HIV/AIDS knowledge among adolescents.
H3: The mediating role of self-efficacy in the relationship between internet exposure and HIV/AIDS knowledge will be moderated by functional digital health literacy. Specifically, the mediation effect will be stronger when functional digital health literacy is high.
2 Methods
2.1 Data source
The data for the current cross-sectional study were derived from the Population Council of India’s “Understanding the Lives of Adolescents and Young Adults (UDAYA)” survey (Santhya et al., 2017). UDAYA is a longitudinal survey focusing on adolescents aged 10 to 19 across the states of Bihar and Uttar Pradesh. The UDAYA survey gathers data on various domains that influence the transition of adolescents to young adults such as knowledge and awareness of sexual and reproductive health matters, exposure to mass media and social media, gender role attitudes, sexual and romantic interests, and health-seeking behavior. The UDAYA survey utilized a systematic and multi-stage stratified sampling approach to independently identify the sampling areas in the selected districts of Bihar and Uttar Pradesh. The 2011 census data served as the sampling framework for this cross-sectional survey. Across the two states, 150 primary sampling units (PSUs) were selected, consisting of villages in rural areas and census wards in urban areas. Within each PSU, systematic sampling technique was employed to choose households. Each PSU was split into two equal segments, one designated for interviews with females and the other for males. A maximum of three respondents were interviewed per household, each representing a different predefined category. In households with multiple respondents within the same category, one respondent was randomly chosen using the Kish table, without replacement. The sample’s uneven gender ratio, with a larger proportion of females, is a result of sampling design. The design included cohorts of unmarried boys and girls as well as a distinct cohort of married girls, but no corresponding cohort for married boys (Santhya et al., 2017).
The UDAYA survey was conducted in two waves. The first wave was conducted between 2015 and 2016 which included 20,594 adolescents, including 5,969 boys and 14,625 girls. The follow-up survey was conducted between 2018 and 2019. Eligible participants included 4,567 male and 12,251 female adolescents who were interviewed again. The factors contributing to the loss to follow-up included participant migration, parental or guardian reluctance to permit re-interview, researchers’ difficulty to locate the household, and participant refusal. 3% of participants with discordant age or education information were excluded from the study. The follow-up survey yielded a sample size of 4,428 teenage boys and 11,864 teenage girls. The second-round survey achieved a response rate of 74% among boys and 81% among girls. Participants in both survey rounds provided their informed consent. The present study comprised 6,103 adolescents, selected from a subgroup of 13,141 adolescents who were aged 15–19 years during Wave 1 and 18–22 years during the follow-up survey, after excluding those with missing data (Santhya et al., 2017). Figure 2 illustrates the sampling criteria applied to achieve the final analytical sample.
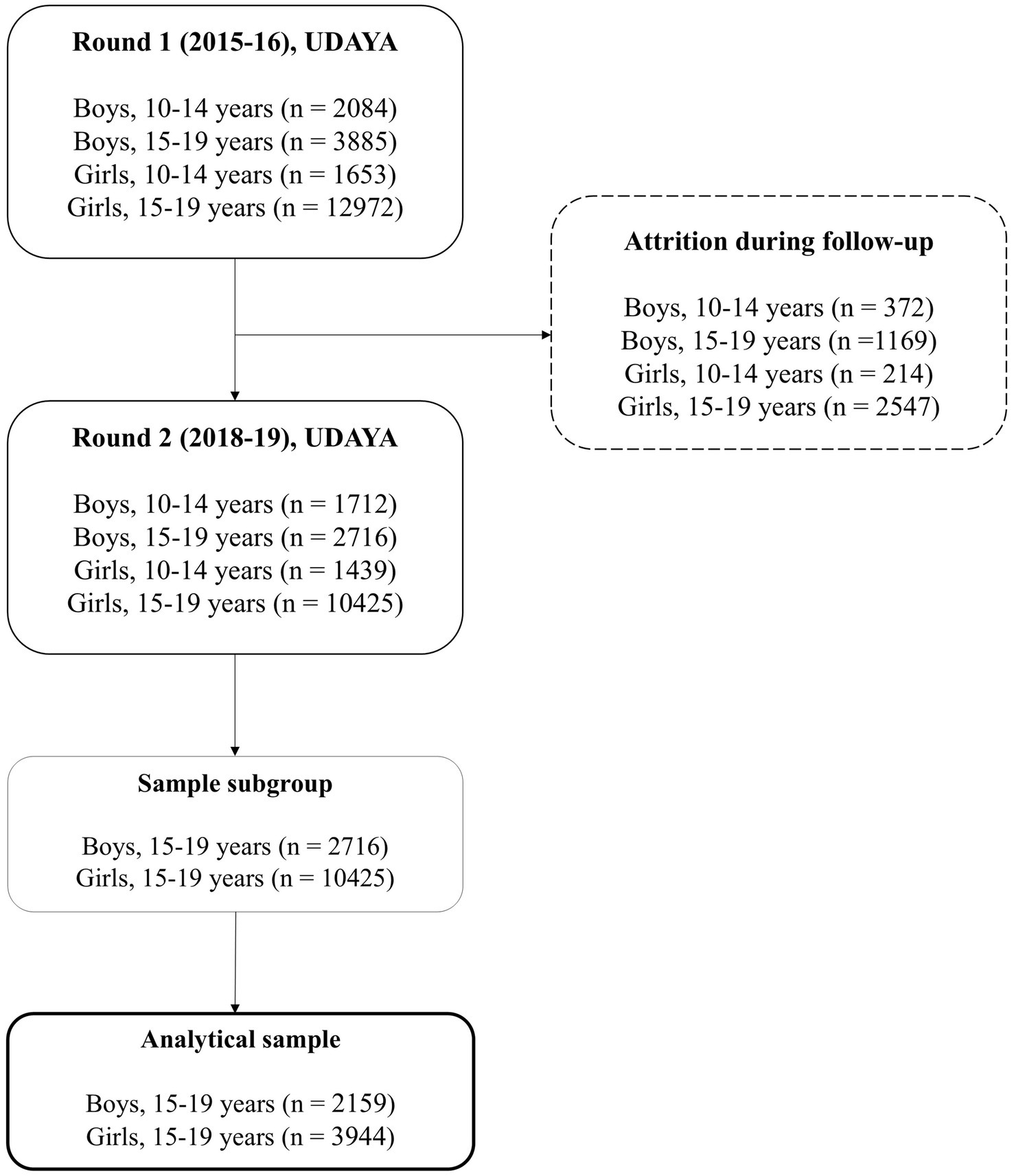
Figure 2. Sampling criteria.
2.2 Measures
2.2.1 Internet exposure
Internet exposure is the predictor variable, which was measured using the following question: “How often do you access the internet on a mobile phone or computer?” (Santhya et al., 2017). One of the following options was provided for participants to choose from: “(1) Almost every day,” “(2) At least once a week,” “(3) At least once a month,” “(4) Rarely,” “(5) Not at all,” and “(6) Not heard of internet” (Santhya et al., 2017). Responses were reverse-coded so that higher values represented greater internet use (i.e., “Almost every day” = 6, “Not heard of internet” = 1). This resulted in a continuous score ranging from 1 to 6, with higher scores indicating greater exposure to the internet.
2.2.2 Knowledge of HIV/AIDS
Knowledge of HIV/AIDS, the outcome variable, was measured using a six-item scale developed for the UDAYA survey to assess participants’ understanding of HIV transmission and prevention (Santhya et al., 2017): (1) mosquito transmission, (2) food sharing, (3) hugging, (4) visual identification of HIV status, (5) monogamy as prevention, and (6) condom use as prevention. For example, one item asked, “Can people get the AIDS virus from mosquito bites?” (Santhya et al., 2017). Responses were recoded in Stata to reflect correct understanding, with accurate responses assigned a score of 1 and incorrect or “do not know” responses assigned a score of 0. A total score was derived by summing the six items. This resulted in scores ranging from 0 to 6, with higher scores signifying greater HIV/AIDS knowledge. The items in the measure demonstrated a reliability coefficient (Cronbach’s alpha) of 0.62.
2.2.3 Self-efficacy
Self-efficacy, the mediating variable, was measured using a six-item scale developed for the UDAYA survey to assess adolescents’ confidence in autonomous decision-making across the following domains (Santhya et al., 2017): (1) discretionary use of time, (2) participation in activities outside the family or school context, (3) income-earning capacity, (4) communication with parents or in-laws about aspirations, (5) clothing choices, and (6) resolution of family conflicts. For example, “How sure are you that you could choose how to spend your free time?” (Santhya et al., 2017). Responses were recorded on a 5-point rating scale from 1 (“Completely sure”) to 5 (“Not at all sure”). The responses were reverse-coded (i.e., 1 was recoded to 5, 2 to 4, and so on), and this recoding was uniformly applied across all 6 items. A total score was obtained by summing the 6 items, which resulted in a continuous self-efficacy measure ranging from 6 to 30, with higher scores indicating greater self-efficacy. The items in the measure demonstrated a reliability coefficient (Cronbach’s alpha) of 0.61.
2.2.4 Functional digital health literacy
Functional digital health literacy is the moderating variable, which was assessed using a single-item measure. Participants were asked, “In the last three years, have you ever used a mobile device to get health information or to check your health and fitness (e.g., blood sugar, blood pressure)?” (Santhya et al., 2017). Responses were recoded into a binary variable, where “Yes” was coded as 1, and both “No” and “Do not Know” were coded as 0.
2.2.5 Control variables
The study included demographic variables such as gender (male, female), age (15–19 years). The education level of participants was categorized as: incomplete education, 1–5 years, 6–10 years, and 11 or more years of formal education. The place of residence of the participants was classified as either urban or rural. The wealth quartile was divided into: Poor, lower-middle, upper-middle, and rich. Finally, peer connection was included as a binary variable (1 = Yes, 0 = No) based on a single item assessing membership in any formal youth group in the last 3 years (Santhya et al., 2017).
2.3 Data analysis
Data analysis was performed using STATA version 14.2 (StataCorp, 2015) and SPSS version 20 (IBM Corp, 2011). Due to the non-normal distribution of a key variable, Spearman’s rank-order correlations were computed to assess bivariate associations. Mediation and moderated mediation analyses were conducted using Hayes’ PROCESS macro in SPSS, employing Model 4 for simple mediation and Model 14 for moderated mediation. This approach uses an ordinary least squares (OLS) regression-based path analysis. A total of 5,000 bootstrap samples were used, and results are shown with 95% bias-corrected confidence intervals (CIs). An indirect effect was considered statistically significant if the CI did not include zero.
3 Results
3.1 Descriptive statistics
The study sample comprised N = 6,103 adolescents, including males (35.48%) and females (64.62%). Participant characteristics are detailed in Table 1. The age distribution was as follows: 19 years (21.09%), 18 years (22.84%), 17 years (20.02%), 16 years (18.43%), and 15 years (17.61%). Regarding education, participants had 11 or more years of schooling (70.77%), 6–10 years (24.59%), 1–5 years (3.93%), or no formal education (0.70%). More participants resided in urban (54.48%) than rural areas (45.52%). The wealth quartile distribution was as follows: upper-middle (49.48%), lower-middle (45.34%), rich (3.67%), and poor (1.51%). Finally, a majority of adolescents reported having a peer connection (91.07%) and functional digital health literacy (76.26%).
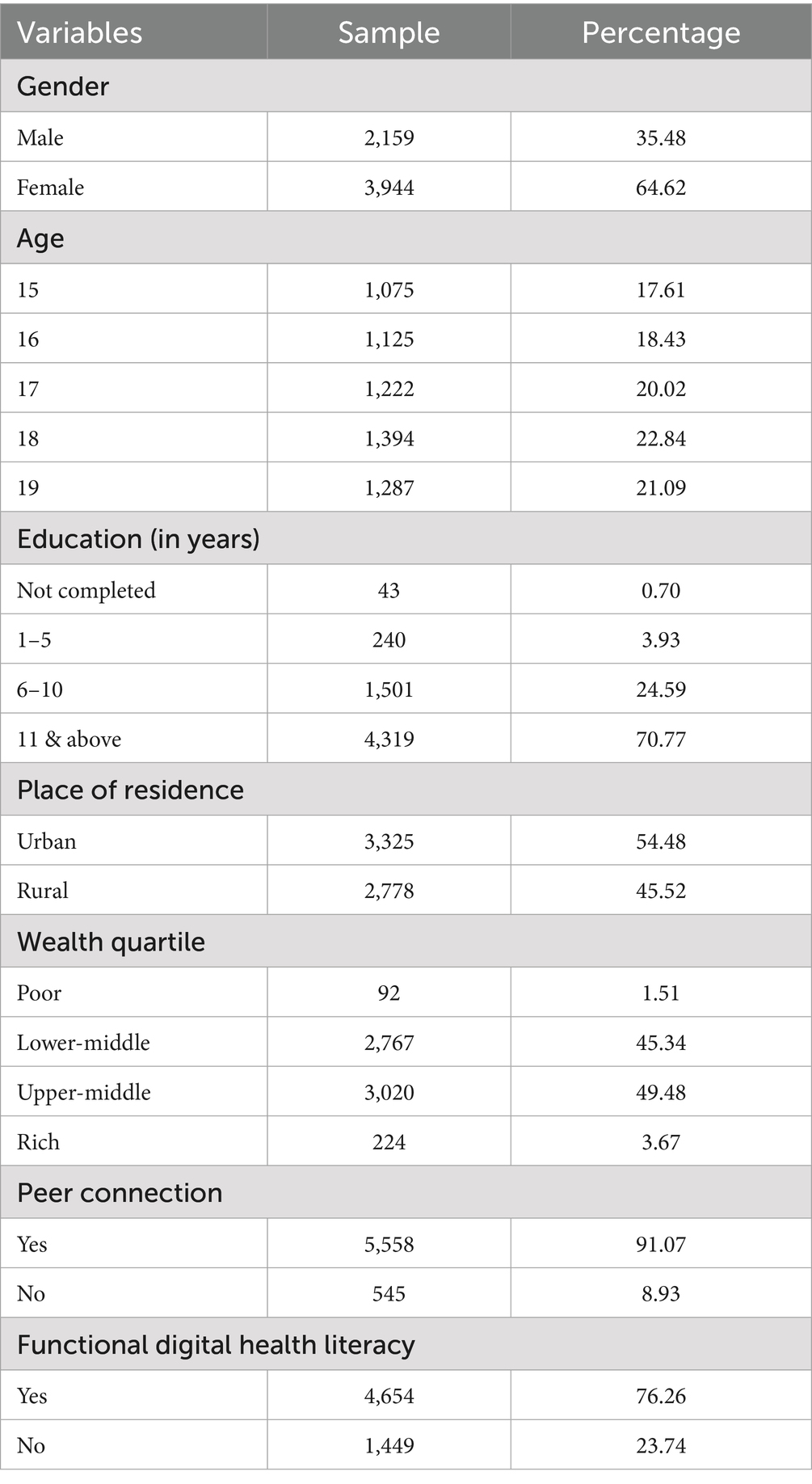
Table 1. Demographic characteristics of the study sample.
3.2 Correlation analysis
Table 2 presents the correlations between the continuous variables under study. The means were as follows: internet exposure score (M = 4.57, SD = 1.74), self-efficacy (M = 25.87, SD = 3.37), and knowledge of HIV/AIDS (M = 3.99, SD = 1.64). Internet exposure showed a small but positive correlation with self-efficacy (r = 0.20, p < 0.001) and knowledge of HIV/AIDS (r = 0.21, p < 0.001), explaining approximately 4 and 4.4% of the variance, respectively. Additionally, self-efficacy demonstrated a small significant association with HIV/AIDS knowledge (r = 0.11, p < 0.001), accounting for 1.2% of the variance. This result provides statistical support for Hypotheses 1, confirming the hypothesized positive association between internet exposure and HIV/AIDS knowledge.

Table 2. Spearman’s rank-order correlations among the continuous variables examined in the study.
3.3 Mediation analysis
Table 3 presents the mediation analysis of self-efficacy in the relationship between internet exposure and knowledge of HIV/AIDS. To investigate the mediating role of self-efficacy in the relationship between internet exposure and HIV/AIDS knowledge, a Model 4 mediation analysis was conducted using the bootstrapping method recommended by Hayes (2018). The direct and indirect effects were evaluated using 5,000 bootstrap resamples with 95% bias-corrected confidence intervals. The analysis controlled for gender, age, education, place of residence, wealth quartile, and peer connection.
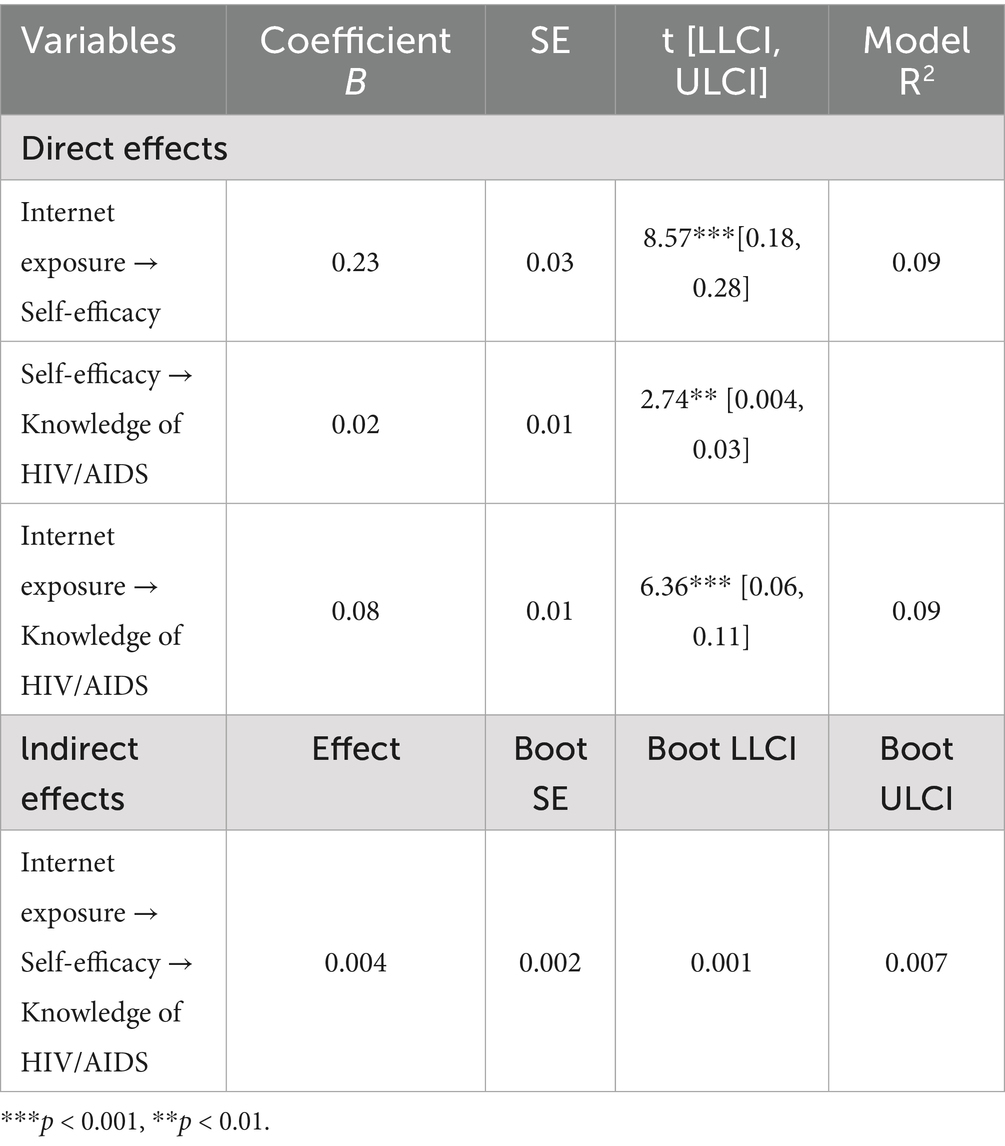
Table 3. Mediation analysis of self-efficacy in the association between internet exposure and knowledge of HIV/AIDS.
The mediation analysis showed that while all paths were statistically significant, the magnitudes of the key effects on HIV/AIDS knowledge were modest. Specifically, the direct effects of internet exposure (B = 0.08, SE = 0.01, 95% CI: 0.06, 0.11) and self-efficacy (B = 0.02, SE = 0.01, 95% CI: 0.004, 0.03) on HIV/AIDS knowledge were small. More importantly, the indirect effect analysis revealed that self-efficacy was a statistically significant mediator (Bindirect = 0.004, SE = 0.002, 95% CI: 0.001, 0.007). However, its contribution was small, accounting for only 4.8% of the total effect of internet exposure on HIV/AIDS knowledge. Therefore, Hypothesis 2 is supported, with self-efficacy serving as a mediator in this relationship.
3.4 Moderated mediation analysis
Table 4 presents the moderated mediation analysis for knowledge of HIV/AIDS outcome. To test whether the indirect effect of internet exposure on HIV/AIDS knowledge through self-efficacy was conditional on levels of functional digital health literacy, a Model 14 analysis was conducted using PROCESS (Hayes, 2018). Direct, indirect, and conditional indirect effects were estimated with 5,000 bootstrap resamples and 95% bias-corrected confidence intervals. The analysis controlled for gender, age, education, place of residence, wealth quartile, and peer connection.
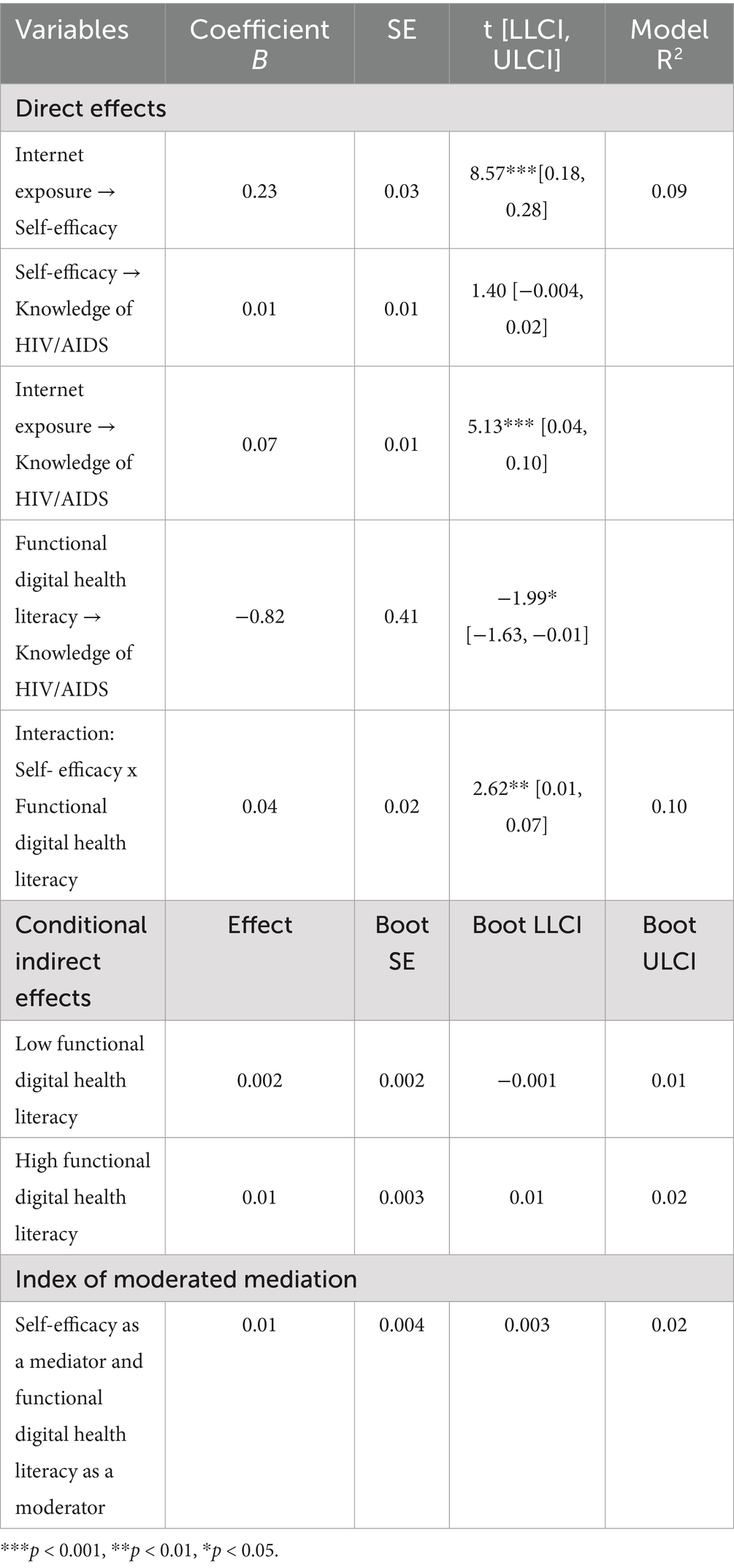
Table 4. Moderated mediation analysis for knowledge of HIV/AIDS outcome.
The direct effects indicated that internet exposure was significantly associated with self-efficacy (B = 0.23, SE = 0.03, 95% CI: 0.18, 0.28) and showed a small but significant association with HIV/AIDS knowledge (B = 0.07, SE = 0.01, 95% CI: 0.04, 0.10). However, self-efficacy was not significantly related to HIV/AIDS knowledge (B = 0.01, SE = 0.01, 95% CI: −0.004, 0.02). In contrast, functional digital health literacy had a negative association with knowledge (B = −0.82, SE = 0.41, 95% CI: −1.63, −0.01), suggesting that digital literacy alone may be insufficient or potentially counterproductive without adequate self-efficacy to effectively process health information. Notably, functional digital health literacy significantly moderated the association between self-efficacy and HIV/AIDS knowledge (B = 0.04, SE = 0.02, 95% CI: 0.01, 0.07). This moderation effect is illustrated in Figure 3. The conditional indirect effects demonstrated that the mediating pathway through self-efficacy was modest but significant at higher levels of functional digital health literacy (Bindirect = 0.01, SE = 0.003, 95% CI: 0.01, 0.02), but was non-significant at lower levels (Bindirect = 0.002, SE = 0.002, 95% CI: −0.001, 0.01). The overall model was further supported by a significant index of moderated mediation (Index = 0.01, SE = 0.004, 95% CI: 0.003, 0.02). Collectively, the predictors explained 9% (R2 = 0.09) of the variance in self-efficacy and 10% (R2 = 0.10) of the variance in HIV/AIDS knowledge. Therefore, Hypothesis 3 is supported, indicating that the indirect effect of internet exposure on HIV/AIDS knowledge through self-efficacy is conditional on adolescents’ functional digital health literacy.
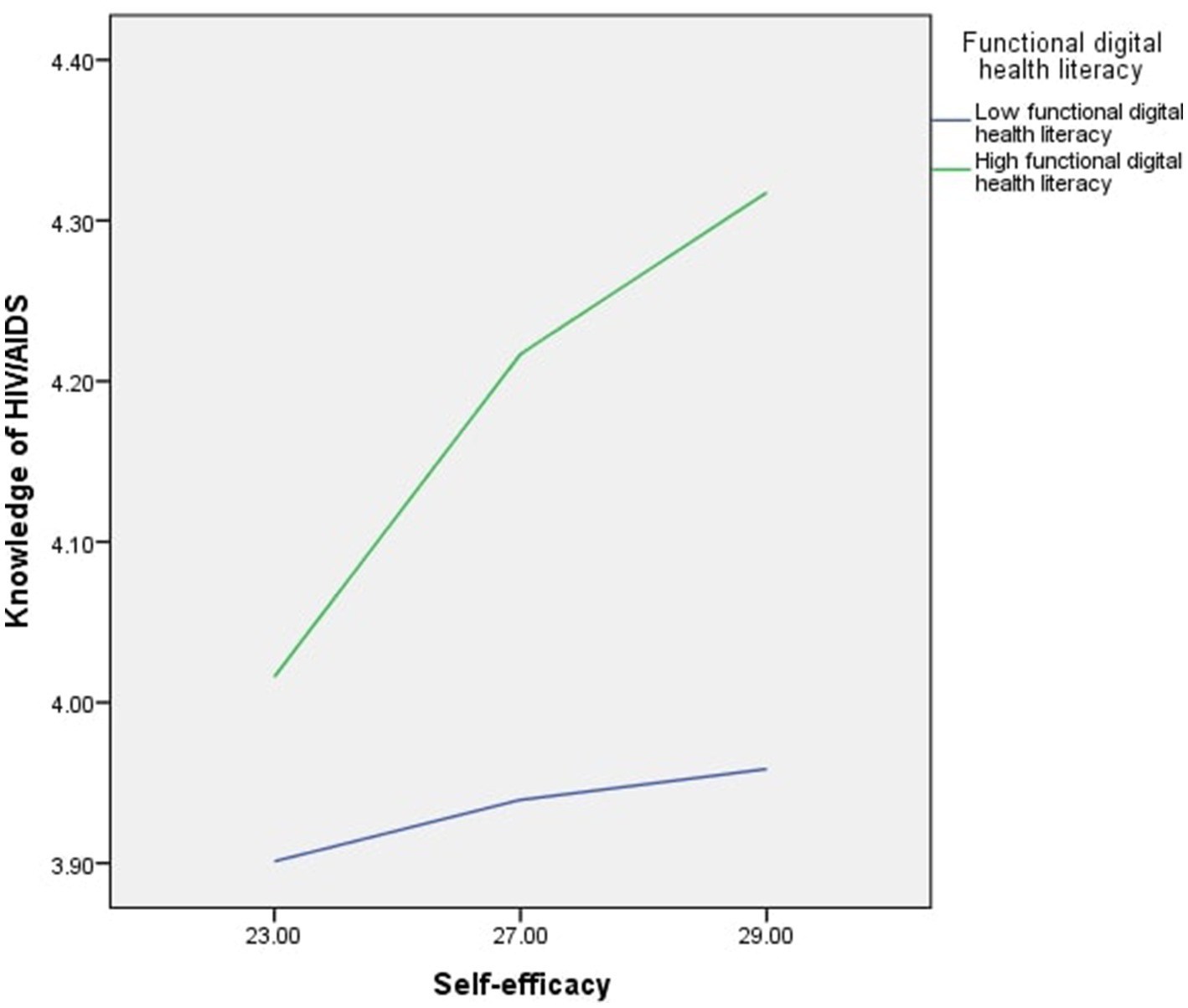
Figure 3. Moderating role of functional digital health literacy on the relationship between self-efficacy and HIV/AIDS knowledge.
4 Discussion
Formal and familial communication about sexuality in India, hindered by embarrassment, discomfort, and personal inhibitions, drives adolescents toward the internet for its promise of privacy and anonymity (Byers et al., 2021; Likith, 2024; Pandey and Rao, 2023). This reliance on digital resources is critical, as national data indicates that adolescents’ knowledge about HIV/AIDS is low. The National Family Health Survey (NFHS) reveals that among adolescents, only 21.71% of girls and 33.56% of boys are sufficiently informed (Barnwal and Hussain, 2025; Bhattacharyya et al., 2023). While the internet is a key source of information, the factors that translate online exposure into actual knowledge are not well understood. Therefore, the study examines the mediating role of self-efficacy in the relationship between internet exposure and HIV/AIDS knowledge. The study further investigates the moderating role of functional digital health literacy on the pathway between self-efficacy and HIV/AIDS knowledge.
The findings validate that the internet serves as an important channel for health information. The findings revealed a statistically significant, though modest (r = 0.21), positive correlation between internet exposure and knowledge about HIV/AIDS. This aligns with a body of research establishing media as an information source for adolescents. For instance, mass media exposure has been associated with greater HIV-related knowledge in a large-scale survey carried out in Uganda (Bago and Lompo, 2019), and similar small but significant associations between media exposure and knowledge have been reported in Nigeria (r = 0.23) (Hamid et al., 2020). This implies that mere exposure is insufficient, and rather suggests mediating factors that facilitate the translation of exposure into knowledge.
The present study found a modest but significant positive correlation between HIV/AIDS knowledge and self-efficacy, a finding consistent with research in Ghana (Opoku et al., 2022) and among Nepalese adolescents (Mahat and Pradhan, 2012). Although previous Indian work has also found associations among the variables (Saha et al., 2022; Srivastava et al., 2021), the key contribution of this work is the establishment of the psychological mechanism linking them. The mediation model revealed that self-efficacy partially mediates the impact of internet exposure on HIV/AIDS knowledge. Although the mediating effect is modest, accounting for approximately 4.8% of the total impact, it remains meaningful both theoretically and practically. From a theoretical perspective, it transcends associations to describe how exposure on the internet is translated into knowledge. This is complemented by an Indonesian study, where self-efficacy mediates the effects of sexual education programs on adolescents’ protective behaviors (Nindrea and Darma, 2024). By unraveling this psychological process, this study provides an essential addition to the formation of a more integral description of functional digital health literacy.
However, the extended analysis reveals a modest, conditional effect in which the mediating role of self-efficacy is contingent upon functional digital health literacy, as the indirect pathway to knowledge is significant only for adolescents with high literacy levels. Research indicates a positive correlation between self-efficacy and health literacy (Ceylan et al., 2022). However, a crucial discrepancy often exists between adolescents’ highly perceived and actual digital health literacy skills. This gap is largely attributed to a lack of critical health literacy, as the effect of self-efficacy is contingent upon an individual’s digital health literacy (Taba et al., 2022).
While the mediating role of self-efficacy aligns with the tenets of Social Cognitive Theory, the analysis shows this interplay is incomplete without considering the critical moderating role of functional digital health literacy. This evidence, backed by other studies (Kisaakye et al., 2023; Opoku et al., 2022), suggests a more dynamic process. This implies a virtuous process where online exposure creates initial awareness, which raises self-efficacy. When this heightened self-efficacy is armed with functional digital health literacy, it then encourages more competent information seeking and, ultimately, greater knowledge acquisition.
In practice, these findings have important public health implications. Our results indicate that successful digital health interventions need to go beyond providing access alone, by simultaneously strengthening adolescents’ self-efficacy and digital health literacy. Government-initiated platforms like the Saathiya Salah mobile application and the Just Ask AI chatbot hold great promise for embedding interactive modules involving peer success stories, goal-setting activities, and skill-building exercises in evaluating credible health information. For wider population-level impact, these interventions can be integrated into the Rashtriya Kishor Swasthya Karyakram (RKSK) platform, particularly through Adolescent Friendly Health Clinics (AFHC), to create synergy between face-to-face counseling and on-demand online support. Pilot implementation in selected states, evaluated through outcomes such as health-seeking behavior and improvements in digital literacy, offers a practical pathway for scaling these interventions within India’s adolescent health system.
It should be noted that the correlations found were small (r ≤ 0.21), and the model accounted for a small proportion of the variance in knowledge about HIV/AIDS. First, the study’s large sample (N = 6,103) provides ample statistical power such that our estimates of these small effects are precise and not the product of statistical artifacts. Second, as Funder and Ozer (2019) comment, most established findings in psychological science tend to yield similarly small correlations. For that reason, we embrace the interpretive stance they suggest: our results represent effects that are “very small for the explanation of single events but potentially consequential in the not-very-long run (Funder and Ozer, 2019, p. 156).” This potential impact is especially noteworthy in the Indian context. With millions of teenagers going online for health information, this statistically significant pathway is an opportunity for interventions that, taken in aggregate across a large population, could affect a considerable absolute number of adolescents. However, replication in the future will be required to firmly ascertain the strength of this small but potentially significant effect.
5 Limitations
The research has certain limitations. First, its cross-sectional nature precludes inferring causality. Although self-efficacy was modeled as the mediator, a reverse pathway where gained knowledge enhances self-efficacy, which is also likely a process moderated by functional digital health literacy, cannot be ruled out. Second, the reliance on self-reported information introduces the possibility of recall bias and social desirability bias. Third, the measurement of variables could be refined. Functional digital health literacy was captured using a single-item indicator, which does not assess the full spectrum of skills, while our measure for internet exposure quantified access frequency but not intent of use. Fourth, the data were gathered pre-pandemic (2018–19), which constrains timeliness but offers a vital baseline from the era of India’s swift internet development. Finally, while the study has a specific geographic focus and modest effect sizes, the findings hold significant theoretical and practical value. The focus on two states, Uttar Pradesh and Bihar, while not nationally representative, covers a substantial portion of India’s youth demographic. Furthermore, the small effect sizes are best interpreted in the context of population-level impact, where such effects can be highly consequential when aggregated across millions of individuals. Therefore, the key contribution of this research is not its predictive power for any single event, but its identification of the interplay of self-efficacy and digital health literacy that can inform the design of more impactful digital health interventions for a large and vulnerable population.
6 Conclusion
The findings suggest that interventions should employ a multi-faceted approach: promoting internet exposure, enhancing self-efficacy and digital health literacy skills. The moderated mediation model suggests internet exposure influences HIV/AIDS knowledge through self-efficacy, with this pathway being moderated by functional digital health literacy.
This study’s contribution shows that while internet exposure has a direct effect on HIV/AIDS knowledge, the indirect path through self-efficacy is significant as well. The interaction between functional digital health literacy and self-efficacy suggests that enhancing digital competencies helps individuals to translate self-efficacy into the acquisition of knowledge effectively.
Future research needs to explore: (1) longitudinal development of these abilities, (2) multi-pathway intervention strategies that target these mechanisms simultaneously, (3) qualitative studies exploring the practical significance of these relationships, and (4) cross-cultural validation of these pathways.
This model has potential applications to other adolescent health issues beyond HIV/AIDS, particularly in digital health communication contexts. While the individual pathway effects are modest, the practical implication is significant. Comprehensive approaches that address multiple pathways, including internet access, self-efficacy building, and digital health literacy enhancement, are needed to achieve meaningful health communication outcomes in adolescent populations.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://dataverse.harvard.edu/file.xhtml?fileId=4163718. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the ethical review board of the Population Council of India, New Delhi. The studies were conducted in accordance with local legislation and institutional requirements. Informed consent was obtained from all participants, including parental or guardian consent for unmarried minors (ages 10–17). To preserve participant confidentiality, signing the consent form was optional for all respondents and parents/guardians. However, interviewers were required to sign documentation confirming that they had explained the consent form content and procedures to each participant or parent/guardian, as approved by the ethics committee.
Author contributions
SP: Writing – original draft. TJ: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
This research is based on data from the Population Council’s UDAYA study, which was funded by the Bill and Melinda Gates Foundation and the David and Lucile Packard Foundation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bago, J. L., and Lompo, M. L. (2019). Exploring the linkage between exposure to mass media and HIV awareness among adolescents in Uganda. Sex. Reprod. Healthc. 21, 1–8. doi: 10.1016/J.SRHC.2019.04.004
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Englewood Cliffs, New Jersey: Prentice Hall.
Barnwal, J., and Hussain, D. (2025). Factors influencing HIV knowledge among Indian men: a cross-sectional study. PLoS One 20, 1–14. doi: 10.1371/journal.pone.0327411
Bhattacharyya, A., Chakraborty, R., Raj, T., Padhi, B. K., Khubchandani, J., Satapathy, P., et al. (2023). Comprehensive knowledge about HIV/AIDS among women of reproductive age in India. Epidemiologia 4, 492–504. doi: 10.3390/epidemiologia4040041
Byers, E. S., O’Sullivan, L. F., Mitra, K., and Sears, H. A. (2021). Parent-adolescent sexual communication in India: responses of middle class parents. J. Fam. Issues 42, 762–784. doi: 10.1177/0192513X20930343
Ceylan, D., Çelen, F. N. A., Özkan, S., and Aycan, Z. (2022). Promoting adolescent health: health literacy, self-efficacy and internet use. Turk. J. Pediatr. 64, 110–121. doi: 10.24953/turkjped.2021.1264
Chereka, A. A., Butta, F. W., Demsash, A. W., Kassie, S. Y., Shibabaw, A. A., Dubale, A. T., et al. (2025). Examining internet use for health information seeking and influencing factors among undergraduate health science students in Southwest Ethiopia. Heliyon 11:e41545. doi: 10.1016/J.HELIYON.2024.E41545
Freeman, J. L., Caldwell, P. H. Y., Bennett, P. A., and Scott, K. M. (2018). How adolescents search for and appraise online health information: a systematic review. J. Pediatr. 195, 244–255.e1. doi: 10.1016/j.jpeds.2017.11.031
Fretian, A., Bollweg, T. M., Okan, O., Pinheiro, P., and Bauer, U. (2020). Exploring associated factors of subjective health literacy in school-aged children. Int. J. Environ. Res. Public Health 17. doi: 10.3390/ijerph17051720
Funder, D. C., and Ozer, D. J. (2019). Evaluating effect size in psychological research: sense and nonsense. Adv. Methods Pract. Psychol. Sci. 2, 156–168. doi: 10.1177/2515245919847202
Habib, A., Goswami, K., Ojah, J., and Bharali, M. D. (2024). Knowledge and attitudes about HIV/AIDS among adolescent students in 15-19 years age group based on the adolescent education programme: a cross-sectional study conducted in Kamrup (metro), Assam. Cureus 16:e62122. doi: 10.7759/cureus.62122
Hamid, M. A., Tamam, E., and Osman, M. N. b. (2020). Relationships between media exposure and knowledge, attitude, and practice on HIV/AIDS: a cross-sectional survey of adolescent Islamiyya girls in Nigeria. Health Commun. 35, 419–429. doi: 10.1080/10410236.2018.1564960
Hayes, A. F. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. 2nd Edn. New York: Guilford Press.
IBM Corp. (2011). IBM SPSS statistics for windows, version 20.0 [computer software]. Available online at: https://www.ibm.com/products/spss-statistics
International Telecommunication Union (ITU) (2021) Measuring digital development: Facts and figures 2021 Available online at: https://www.itu.int/en/ITU-D/Statistics/Documents/facts/FactsFigures2021.pdf
Keeley, B., and Little, C. (2017) The state of the world's children 2017: Children in a digital world Available online at: https://www.unicef.org/reports/state-worlds-children-2017
Khargekar, N., Takke, A., Athalye, S., Panale, P., Rajamani, N., and Banerjee, A. (2024). Exploring factors influencing the perspective regarding HIV transmission and prevention among college students in India. J. Family Med. Prim. Care 13, 1467–1472. doi: 10.4103/jfmpc.jfmpc_1756_23
Kisaakye, P., Bukuluki, P., Wandiembe, S. P., Kiwujja, V., Kajungu, C., Mugwanya, W., et al. (2023). How self-efficacy and agency influence risky sexual behavior among adolescents in northern Uganda. Adolescents 3, 404–415. doi: 10.3390/adolescents3030028
Likith, R. S. (2024). Exploring factors influencing parent-adolescent communication on sexual and reproductive health (SRH)—a qualitative study from Bengaluru, India. J. Psychosexual Health 6, 235–241. doi: 10.1177/26318318241265822
Lo, V. H., Wei, R., and Su, H. (2013). Self-efficacy, information-processing strategies, and acquisition of health knowledge. Asian J. Commun. 23, 54–67. doi: 10.1080/01292986.2012.725175
Mahat, G., and Pradhan, G. (2012). HIV/AIDS knowledge and self-efficacy among late adolescents in Nepal. Res. Theory Nurs. Pract. 26, 205–215. doi: 10.1891/1541-6577.26.3.205
McKinnon, K. A., Caldwell, P. H. Y., and Scott, K. M. (2020). How adolescent patients search for and appraise online health information: a pilot study. J. Paediatr. Child Health 56, 1270–1276. doi: 10.1111/jpc.14918
Nielsen. (2018). Average Indian smartphone user spends 4x time on online activities as compared to offline activities [press release]. Available online at: https://www.nielsen.com/in/en/press-releases/2018/average-indian-smartphone-user-spends-4x-time-on-online-activities-as-compared-to-offline-activities/
Nindrea, R. D., and Darma, I. Y. (2024). Self-efficacy mediates the relationship between sexual education and prevention of sexually-transmitted diseases awareness among secondary school students in Padang City, Indonesia. Afr. J. Infect. Dis. 19, 57–63. doi: 10.21010/Ajidv19i1.7
Niu, Z., Willoughby, J., and Zhou, R. (2021). Associations of health literacy, social media use, and self-efficacy with health information-seeking intentions among social media users in China: cross-sectional survey. J. Med. Internet Res. 23:e19134. doi: 10.2196/19134
Norman, C. D., and Skinner, H. A. (2006). Ehealth literacy: essential skills for consumer health in a networked world. J. Med. Internet Res. 8, 1–10. doi: 10.2196/jmir.8.2.e9
Opoku, M. P., Agyei-Okyere, E., Nketsia, W., Torgbenu, E. L., and Kumi, E. O. (2022). Perceived self-efficacy of students and its influence on attitudes and knowledge about HIV/AIDS in Ghana. Int. J. Health Plann. Manag. 37, 755–769. doi: 10.1002/hpm.3371
Paige, S. R., Stellefson, M., Krieger, J. L., Anderson-Lewis, C., Cheong, J., and Stopka, C. (2018). Proposing a transactional model of eHealth literacy: concept analysis. J. Med. Internet Res. 20:e10175. doi: 10.2196/10175
Pandey, M. K., and Rao, T. S. S. (2023). Sexuality education in India yet remains a taboo—an attempt to dust-off. J. Psychosex. Health 5, 11–12. doi: 10.1177/26318318231155993
Pendl, D., Maitz, K. M., and Gasteiger-Klicpera, B. (2023). Examining the relationship between health literacy and individual and sociodemographic factors in secondary school students. J. Public Health 32, 531–542. doi: 10.1007/s10389-023-01836-1
Saha, R., Paul, P., Yaya, S., and Banke-Thomas, A. (2022). Association between exposure to social media and knowledge of sexual and reproductive health among adolescent girls: evidence from the UDAYA survey in Bihar and Uttar Pradesh, India. Reprod. Health 19:178. doi: 10.1186/s12978-022-01487-7
Santhya, K. G., Acharya, R., Pandey, N., Singh, S. K., Rampal, S., Zavier, A. J., et al., (2017). Understanding the lives of adolescents and young adults (UDAYA) in Bihar, India. Population Council. Available online at: https://www.popcouncil.org/uploads/pdfs/2017PGY_UDAYA-BiharReport.pdf
Schunk, D. H., and Pajares, F. (2009). Self-efficacy theory. In K. R. Wentzel and A. Wigfield (Eds.), Handbook of motivation at school (pp. 35–53). New York: Routledge.
Srivastava, S., Chauhan, S., Patel, R., and Kumar, P. (2021). A study of awareness on HIV/AIDS among adolescents: a longitudinal study on UDAYA data. Sci. Rep. 11:22841. doi: 10.1038/s41598-021-02090-9
Taba, M., Allen, T. B., Caldwell, P. H. Y., Skinner, S. R., Kang, M., McCaffery, K., et al. (2022). Adolescents' self-efficacy and digital health literacy: a cross-sectional mixed methods study. BMC Public Health 22, 1–13. doi: 10.1186/s12889-022-13599-7
UNICEF (2021) Global and regional trends 2021. Available online at: https://data.unicef.org/topic/hivaids/global-regional-trends/
World Health Organization and London School of Economics. (2024)New WHO and London School of Economics study identifies key digital factors affecting health [news release]. Available online at: https://www.who.int/europe/news/item/02-12-2024-new-who-and-london-school-of-economics-study-identifies-key-digital-factors-affecting-health
Zhou, Y., Xu, J., Wang, R., and Guan, X. (2025). Understanding how digital health literacy affects health self-management behaviors: the mediating role of self-efficacy in college students. Sci. Rep. 15, 27230–27211. doi: 10.1038/s41598-025-12726-9
Keywords: digital health communication, internet exposure, self-efficacy, HIV/AIDS knowledge, functional digital health literacy
Citation: Prinitha S and Jose TP (2025) Internet exposure and knowledge of HIV/AIDS among adolescents in India: exploring the mediating role of self-efficacy using UDAYA data. Front. Commun. 10:1648383. doi: 10.3389/fcomm.2025.1648383
Edited by:
Vsevolod Konstantinov, Penza State University, RussiaReviewed by:
Anindita Banerjee, Indian Council of Medical Research (ICMR), IndiaWahyu Rahardjo, Gunadarma University, Indonesia
Copyright © 2025 Prinitha and Jose. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tony P. Jose, dG9ueS5qb3NlQHZpdC5hYy5pbg==