 Ledyane Taynara Marton1Laís Maria Pescinini-e-Salzedas1Maria Eduarda Côrtes Camargo1
Ledyane Taynara Marton1Laís Maria Pescinini-e-Salzedas1Maria Eduarda Côrtes Camargo1 Sandra M. Barbalho1,2,3*Jesselina F. dos Santos Haber1Renata Vargas Sinatora1Claudia Rucco Penteado Detregiachi2Raul J. S. Girio1Daniela Vieira Buchaim1,2Patricia Cincotto dos Santos Bueno1
Sandra M. Barbalho1,2,3*Jesselina F. dos Santos Haber1Renata Vargas Sinatora1Claudia Rucco Penteado Detregiachi2Raul J. S. Girio1Daniela Vieira Buchaim1,2Patricia Cincotto dos Santos Bueno1- 1Department of Biochemistry and Pharmacology, School of Medicine, University of Marília (UNIMAR), Marília, Brazil
- 2Postgraduate Program in Structural and Functional Interactions in Rehabilitation-UNIMAR, Marília, Brazil
- 3Department of Biochemistry, School of Food and Technology of Marilia (FATEC), Marília, Brazil
Diabetes mellitus (DM) is an ensemble of metabolic conditions that have reached pandemic proportions worldwide. Pathology’s multifactorial nature makes patient management, including lifelong drug therapy and lifestyle modification, extremely challenging. Currently, there is growing evidence about the effectiveness of using herbal supplements in preventing and controlling DM. Curcumin is a bioactive component found Curcuma longa, which exhibits several physiological and pharmacological properties such as antioxidant, anti-inflammatory, anticancer, neuroprotective, and anti-diabetic activities. For these reasons, our objective is to systematically review the effects of Curcuma longa or curcumin on DM. Databases such as PUBMED and EMBASE were searched, and the final selection included sixteen studies that fulfilled the inclusion criteria. The results showed that curcumin’s anti-diabetic activity might be due to its capacity to suppress oxidative stress and inflammatory process. Also, it significantly reduces fasting blood glucose, glycated hemoglobin, and body mass index. Nanocurcumin is also associated with a significant reduction in triglycerides, VLDL-c, total cholesterol, LDL-c, HDL-c, serum C reactive protein, and plasma malonaldehyde. Therefore, it can be considered in the therapeutic approach of patients with DM.
Introduction
The International Diabetes Federation has estimated that since 2000, the prevalence of diabetes mellitus (DM), including type 1 (T1DM) and type 2 (T2DM), has increased from 151 million to 463 million in adults aged 20 to 79 years (1). T2DM is the most prevalent chronic metabolic condition characterized by higher blood glucose levels due to the organism’s poor management of insulin. The state of chronic hyperglycemia leads to increased levels of advanced glycation end products (AGEs) that act directly on cells, causing pro-inflammatory effects and oxidative stress (2, 3).
The triggering ways of inflammation in T2DM are still not fully elucidated. The inflammatory process likely contributes to the development of T2DM and may cause insulin resistance which is worsened with hyperglycemia (4). Epidemiologic studies have shown an association between inflammatory biomarkers and the occurrence of T2DM and its complications. Adipose tissue seems to be a significant site of inflammatory biomarkers’ production due to the cross-talk observed between adipocytes, macrophages, and other immune cells that permeate the increased adipose tissue (5, 6).
On the other hand, oxidative stress has a key role in the development of T2DM. Increased oxidative species production and reduced antioxidant capacity have been repeatedly shown in subjects with T2DM (7). Hyperglycemia can contribute to oxidative stress by enhancing the polyol pathway flux, activation of protein kinase C, altering eicosanoid metabolism, and induction of glucose autoxidation that collectively results in increased reactive oxygen species (ROS) generation. ROS can exert numerous detrimental effects that induce and aggravate diabetes, including diminishing glucose transport channels, reducing insulin secretion, protein fragmentation and oxidation, DNA damage, free fatty acid generation, and increased vascular permeability. Moreover, oxidative stress induces the formation of AGEs contributing to endothelial dysfunction and the development of microvascular and macrovascular complications of T2DM (8–10).
Owing to the aforementioned detrimental effects of oxidative stress on the development of T2DM and the progression of its vascular complications, antioxidant therapy has been considered a potentially effective approach (11, 12).
Curcuma longa, the turmeric plant commonly utilized in food preparation as a spice, has been recognized by the scientific community. This plant is characterized by orange tuberous rhizomes and is widely known and cultivated in South East Asia (13). It is used as a natural therapeutic medicine for various pathological conditions in these regions since ancient times. The singular characteristic of this plant is the presence of curcumin, which shows antioxidant and anti-inflammatory properties (14). Besides that, curcumin has a potential role in preventing and treating several diseases due to various actions such as anti-bacterial, anti-diabetic, anti-viral, and anticancer activities (15–17).
Curcuminoids have been shown to improve insulin resistance, decrease glucose and insulin levels, increase adiponectin release, and reduce the levels of leptin, resistin, interleukin (IL)-6 IL-1β, and tumor necrosis factor-α in patients with T2DM (18). These findings suggest that these compounds can affect glucose homeostasis and diabetic complications, and the vascular risk of patients with T2DM (19). Some studies have shown that supplementation of curcuminoids improves the lipid profile and increases the total antioxidant capacity of patients with T2DM (20–22), thus supporting other available evidence on the role of curcuminoids in modifying cardiometabolic risks (23–26). Given the above, this systematic review aimed to investigate the effects of Curcuma longa and its derivatives on DM.
Methods
Focused Question
This review was built to answer the focused question: What are the effects of Curcuma longa on T2DM patients?
Language
Only studies in English were selected.
Databases
This study has included studies in MEDLINE–PubMed (National Library of Medicine, National Institutes of Health), EMBASE, and COCHRANE databases. The descriptors used were Hyperglycemia or Diabetes or Insulin resistance and Curcuma Longa or Curcumin or Curcuminoids. The use of these mesh-terms helped identify studies related to curcumin intake and its beneficial role in metabolic status in T2DM patients. The authors have followed PRISMA (Preferred Reporting Items for a Systematic Review and Meta-Analysis) guidelines (27).
Study Selection
This review included studies that reported Curcuma longa or potential curcumin role to patients with T2DM. This study’s inclusion criteria were Randomized Clinical Trials (RCTs), prospective, double-blind, and placebo-controlled studies. Only full texts were included.
The exclusion criteria were studies with animals, reviews, studies not in English, retrospective studies, case reports, poster presentations, and editorials. Reviews were consulted to build the discussion but were not included.
Data Extraction
This search’s search period included the past five years (January 2016 to December 2020). These studies are described in Table 1.
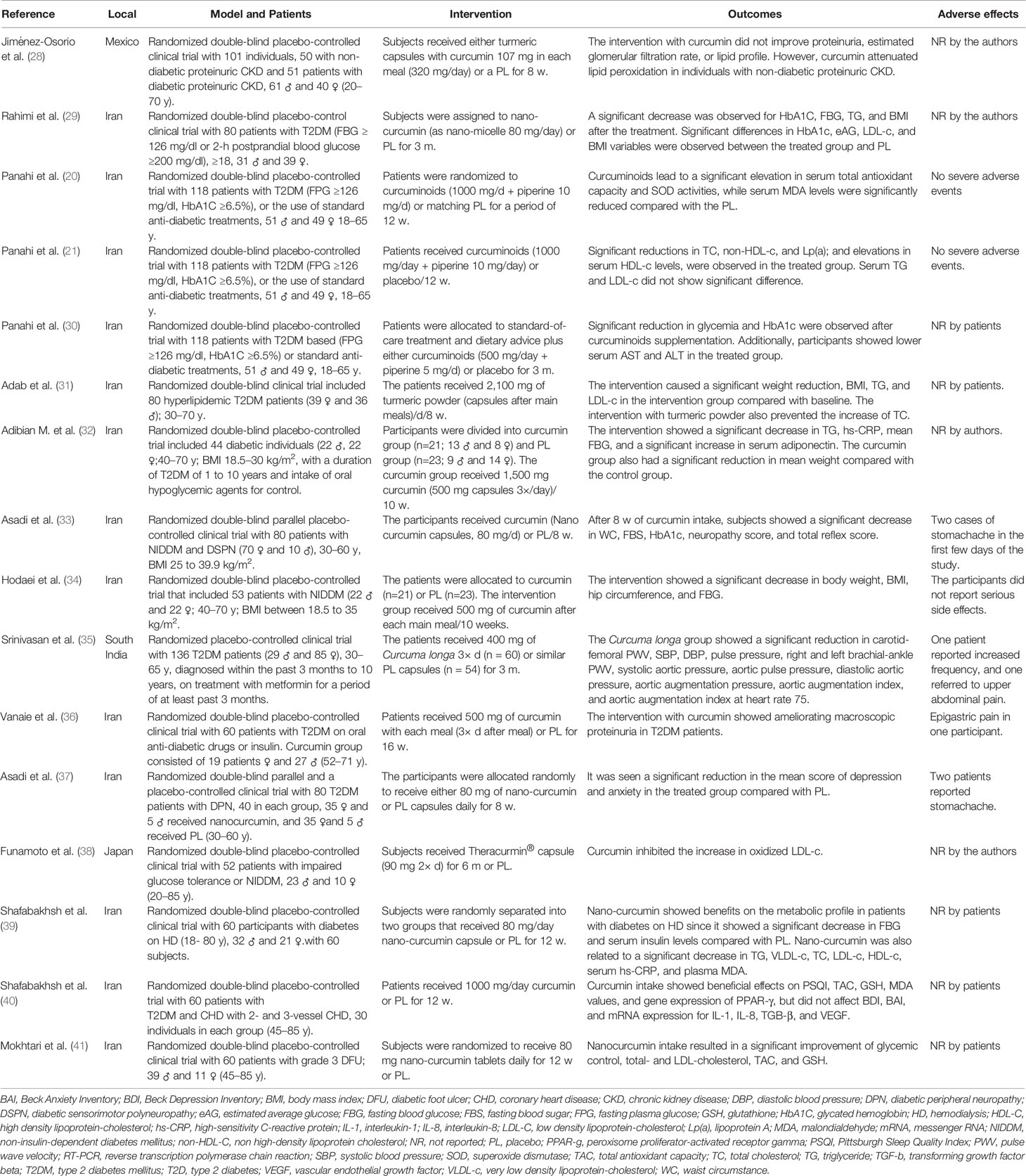
Table 1 Descriptive table of the included studies.
Quality Assessment
To evaluate the risk of biases in the selection, detection, and reporting bias of each.
RCT, we applied the Cochrane Handbook for Systematic Reviews of Interventions. Other risks of biases in the selection of patients, classification of interventions, missing data, and measurement of outcomes were also evaluated.
Results
From the 16 articles selected (Figure 1), 12 were randomized, double-blind placebo-controlled clinical trials, two randomized, double-blind, parallel placebo-controlled clinical trials, one randomized, double-blind clinical trial, and one randomized placebo-controlled clinical trial. A total of 1,309 participants were included, and 1,207 of those were T2DM patients. Five hundred ninety-five were women, and 495 were men. One study did not report the gender of the participants, and 12 studies reported only the gender of the participants who completed the study. The age range was from 18 to 85 years. The studies were performed in different countries (thirteen were from Iran, one from Mexico, one from South Africa, and one from Japan).
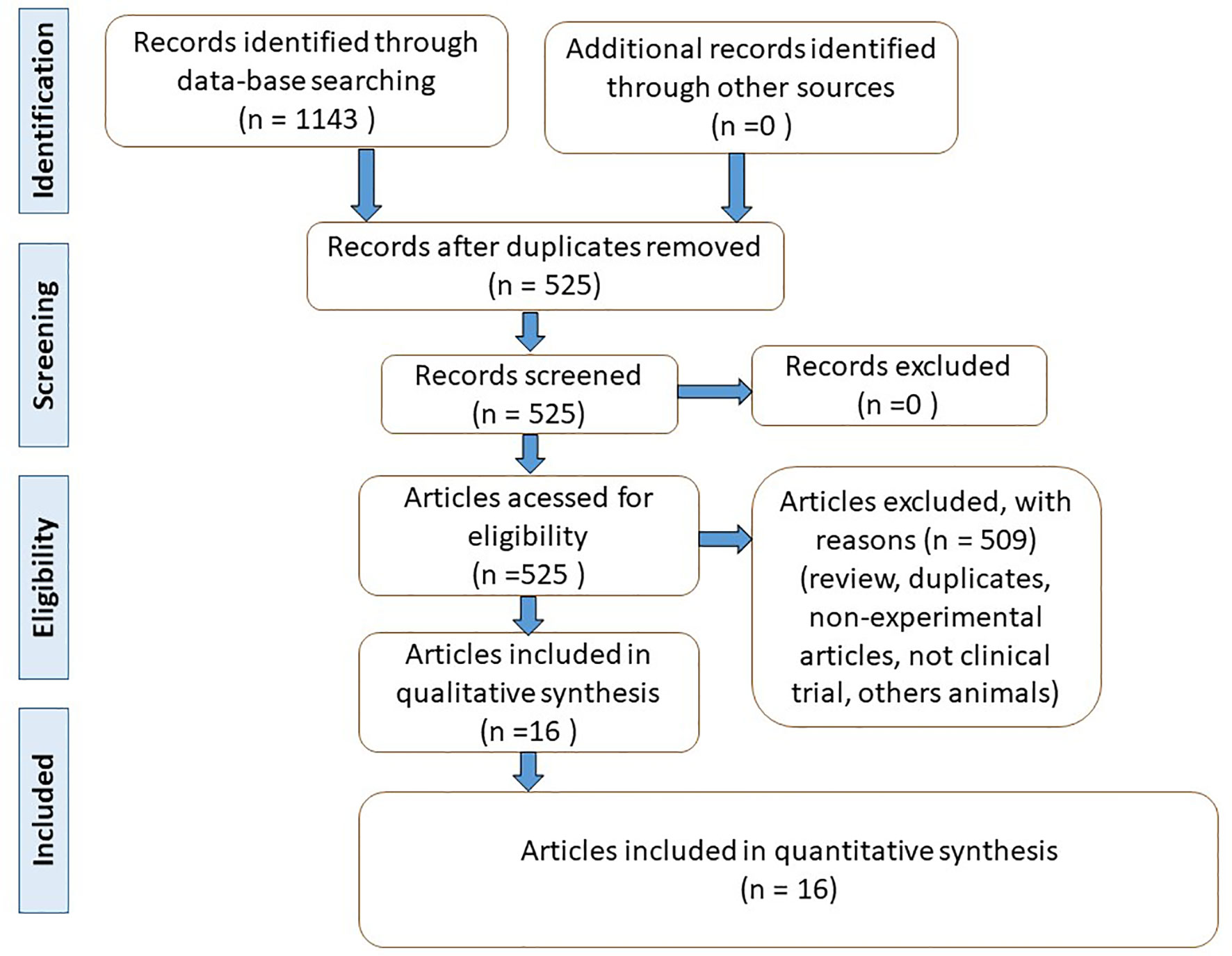
Figure 1 Flow diagram showing the literature search (based on PRISMA, 2009) (27).
Nine of them were performed with T2DM patients, one with T2DM and non-diabetic proteinuric Chronic kidney disease (CKD) patients, one with T2DM and Diabetic Sensorimotor Polyneuropathy (DSPN) patients, one with T2DM and Diabetic Peripheral Neuropathy (DPN) patients, one with Non-Insulin-Dependent Diabetes Mellitus (NIDDM) patients, one with DM on Hemodialysis patients, one with T2DM and coronary heart disease, and one diabetic foot ulcer (DFU). Only one study included patients with type 1 and T2DM.
Five studies used curcumin, five used nano-curcumin, one used Theracurmin®, one Curcuma-longa, one turmeric powder, three curcuminoids associated with piperine. The doses administered had a wide variation range from 80 mg per day to 2,100 mg per day, and the period of intervention ranged from 8 weeks to 16 weeks
The studies showed that the use of Curcuma longa or curcumin (in different formulations) showed significant reduction of lipid peroxidation, fasting blood glucose levels, Glycated hemoglobin (HbA1C), triglycerides, total cholesterol, LDL-c, C-Reactive Protein, systolic and diastolic blood pressure. A significant increase in HDL-c levels and serum antioxidant capacity was also observed. The studies also showed that the use of curcumin could improve depression and anxiety levels. The primary reported adverse effects were epigastric pain and upper abdominal pain (Table 1). Table 2 shows the risk of bias for the included studies.
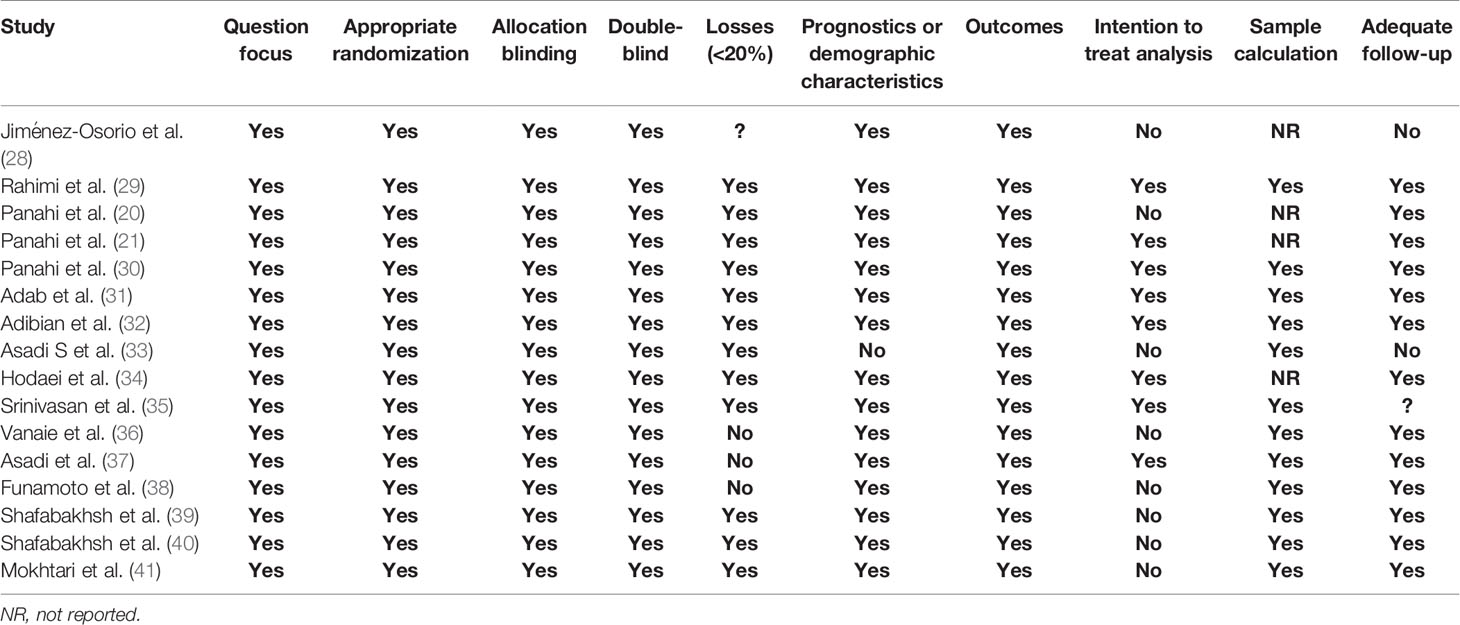
Table 2 Descriptive table of the biases of the included randomized clinical trials.
Discussion
Type II Diabetes Mellitus in a Nutshell
T2DM is a prevalent chronic disorder characterized by high blood sugar levels representing 80% of DM patients. This condition has a multifactorial nature, triggered by several genetic and environmental factors, with a critical mechanism of progressive loss of β-cell insulin secretion (42–44). As long as the patient β-cells can compensate for insulin resistance, the normoglycemia is preserved. However, the natural disease progression is hyperglycemia (43, 45).
The chronic hyperglycemic state contributes to oxidative stress by increasing levels of AGEs and ROS (46), increasing the risk of development of microvascular (retinopathy, nephropathy, and neuropathy), and macrovascular complications (congestive heart failure, stroke, coronary heart disease, myocardial infarction, and peripheral vascular disease) (42, 47). These consequences result in a reduction in quality of life and life expectancy by even ten years among diabetic patients (42, 48).
Arterial hypertension, dyslipidemia, older age, sedentary lifestyle, and abdominal obesity are key risk factors for T2DM (43, 48) since the adipose tissue secretes several biomarkers, such as resistin, TNF-α, and IL-6, which can induce a chronic inflammatory state and insulin resistance. Moreover, in obese patients, low adiponectin levels and a leptin-resistance state are commonly seen (42).
The natural progression of DM is hyperglycemia, which contributes to oxidative stress, and pro-inflammatory markers, which lead to lipid peroxidation, increase the oxidative stress scenario, resulting in inflammation and increased VEGF, ICAM-1, VCAM-1, endothelial dysfunction, and apoptosis. These processes increase the risk of micro and macrovascular complications (49–51). Figure 2 summarizes the pathophysiology of DM.
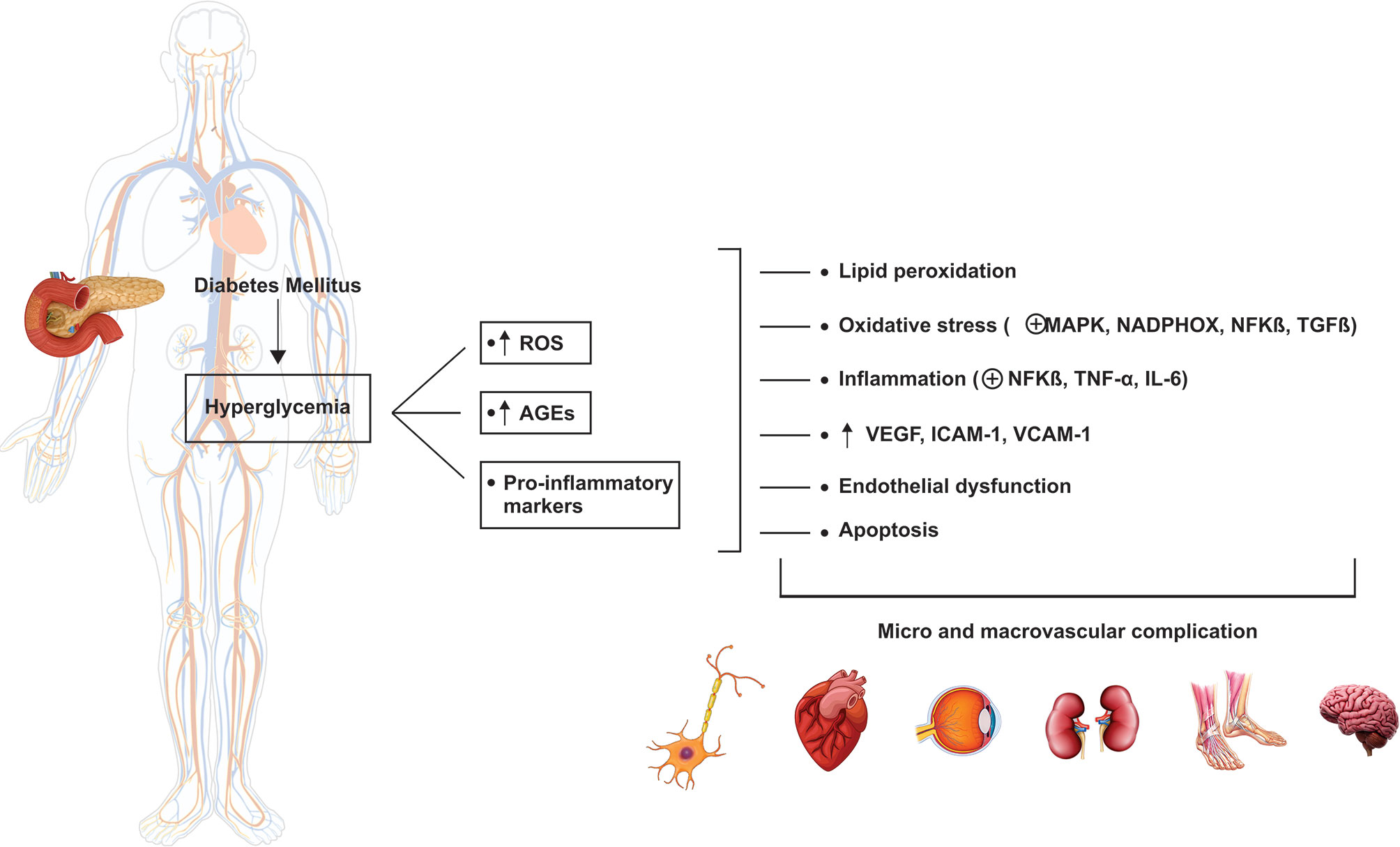
Figure 2 Pathophysiology of diabetes mellitus. The hyperglycemic state leads to the increase in ROS and pro-inflammatory biomarkers related to the complications associated with diabetes. ROS, reactive oxygen species; AGEs, advanced glycation end-products; MAPK, mitogen-activated protein kinase; NADPHOX, nicotinamide adenine dinucleotide phosphate oxidase; NFKβ, nuclear factor-kappa β; TGF-β, transforming growth factor β; TNF-α, tumor necrosis factor α; IL-6, interleukin-6; VEGF, vascular endothelial growth factor; ICAM-1, intercellular adhesion molecule 1; VCAM-1, vascular cell adhesion protein.
The current DM treatment strategies are based on a multifactorial approach, targeting all risk factors rather than glucose control alone, resulting in a decrease or delay in its progression and improving the overall life quality (42, 48). However, there is no cure for diabetes so far, and none of the large numbers of the drug classes that are used modifies the progressive decline in β-cell function over time (42, 43). Therefore, researchers have been searching for evidence about herbal therapy’s effectiveness in preventing and controlling DM.
Curcuma longa
The genus Curcuma (Zingiberaceae) includes perennial rhizomatous plants native to subtropical to tropical regions. Curcuma cultivation is extensively found in tropical and subtropical regions of Asia, Australia, and South America (52). Since ancient times in India and China, it has been considered to treat illnesses such as dermatologic diseases, infection, stress, and depression (53–55).
The main part of the plant is the rhizomes, and the most prevalent active components are the curcuminoids (curcumin, demethoxycurcumin, and bisdemethoxycurcumin) (53, 56, 57). Curcuminoids are nontoxic polyphenolic that exerts a wide range of biological activities (58, 59), such as the production of significant immunosuppressants that inhibit the production of IL-2 and IL-12. This compound inhibits the expression of iNOS (inducible nitric oxide synthase), COX-2 (cyclooxygenase-2), lipoxygenase-5, and many other pro-inflammatory cytokines, such as TNF-α, IL-1, IL-6, and IL-8 (60–62).
Curcuminoids can also regulate apoptosis and suppress neurotoxic factors in macrophages and alveolar monocytes stimulated by lipopolysaccharides. Besides, it inhibits phosphorylation and degradation of IκBα (nuclear factor of kappa light polypeptide gene enhancer in B-cells inhibitor, alpha) and activates the γ receptor mechanism activated by peroxisome proliferator, reducing inflammation pattern induced by NF-κB pathway (62–64).
The peculiar characteristics that attract scientists’ attention are the antioxidant and anti-inflammatory activities and the safety of its pharmacological profile (14, 15, 65, 66). The mechanism of action in several molecular pathways is due to curcumin’s particular chemical structure, capable of having many molecular targets. The biological effects may include the inhibition of reactive oxygen species (ROS) production, playing a fundamental role, particularly for diseases related to oxidative stress and inflammation, such as DM (67, 68). Figure 3 shows some systemic effects of curcumin.
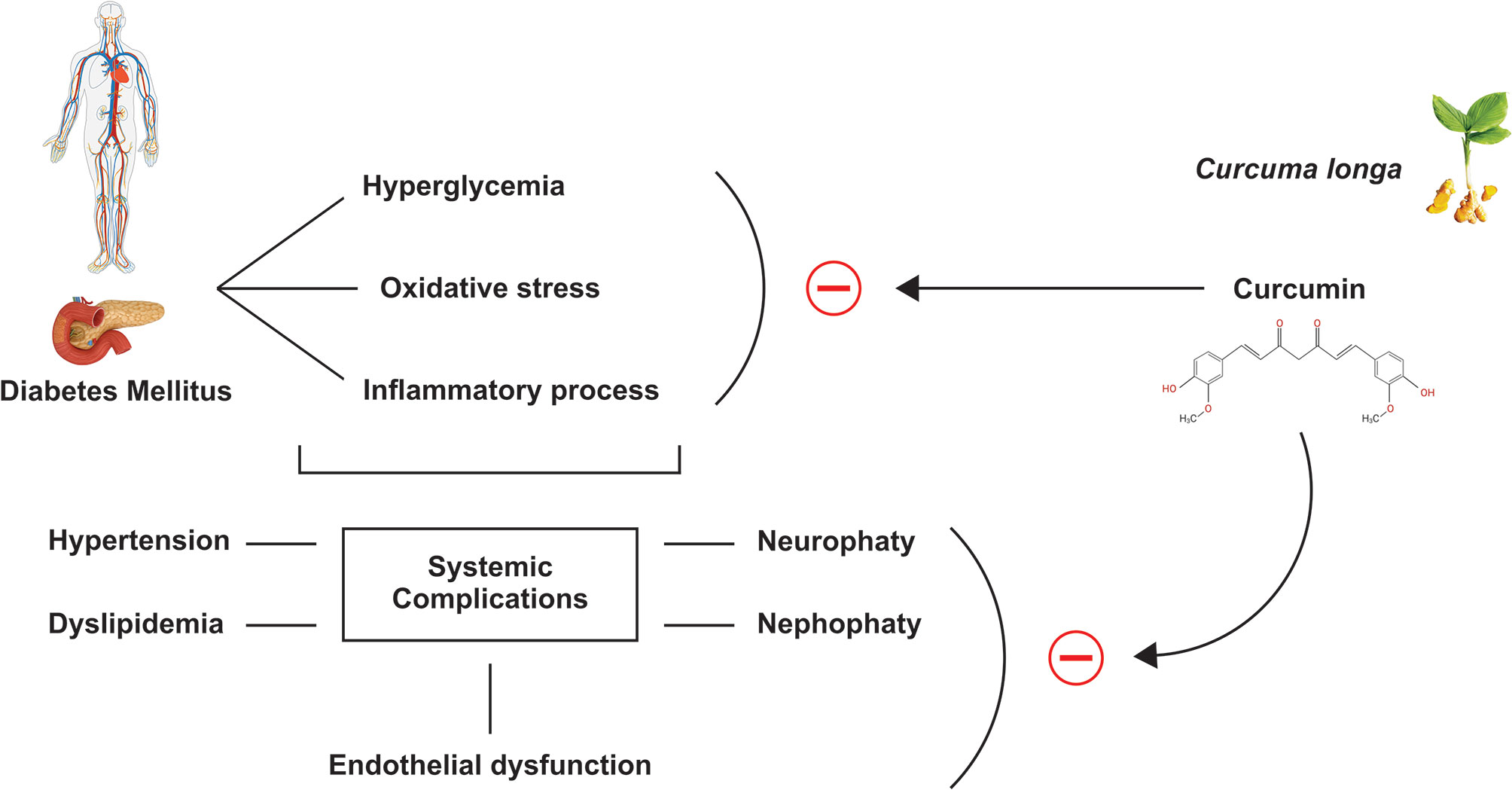
Figure 3 Effects of curcumin. Curcumin can inhibit hyperglycemia, oxidative stress, and the inflammatory processes caused by Diabetes Mellitus, in addition, and consequently inhibits the systemic complications of this disease, such as hypertension, dyslipidemia, neuropathy, nephropathy, and endothelial dysfunction.
As seen above, curcumin can exhibit a huge range of therapeutic possibilities; however, it presents low solubility and rapid metabolism limiting its absorption in the gastrointestinal tract and resulting in weak bioavailability. The weak bioavailability has been associated to its insolubility in the water and the increased degradation in alkaline solutions or crystallization in acidic environments (69–71). Significant changes occur in its degradation time according to the pH, at pH> 7 if it degrades in about 30 min, already in acidic conditions, the degradation is much slower, with less than 20% of the total curcumin decomposed in 1 h. When ingested orally, the bioavailability of curcumin can be influenced by the food matrix, like lipids and proteins. Most of it is excreted in the feces, and only a small part will be absorbed in the intestine, which still undergoes a fast metabolism in the liver and the plasma. A high conjugation rate via glucuronidation and sulfation is also largely converted to its water-soluble metabolites (sulfates and glucuronides) that are excreted in the urine, explaining its concentration has a very low level in the blood (72–74).
The low bioavailability leads to reduced serum concentrations, reducing the possibilities of producing positive health effects. Due to these reasons, in the last few years, several delivery methods have been developed to improve oral curcumin bioavailability (75, 76). Some pharmaceutical technologies, and combinations with other compounds, such as piperine or lecithin, are being considered as they increase curcumin´s solubility, extend its residence in plasma, and improve the pharmacokinetic profile and cell absorption. Different new delivery systems, such as solid lipid particles, micellar systems, or hydrophilic nanoparticles, can increase curcumin concentration up to 15 to 20 times. Therefore, there is an improved curcumin solubility, bioavailability, transmembrane permeability, prolonged plasma half‐life, long‐term stability, target‐specific delivery, and upgraded therapeutic effects (77, 78).
According to studies that explored the safety of turmeric, standardized powder and extract of turmeric and curcumin are safe for human use, even in high doses of 6 g/day for seven weeks. Moreover, endovenous use of curcumin is safe if used if the dose administered is lower than that used orally. In pregnant animals, curcumin showed to be safe, but further studies are needed to confirm its safety in pregnant women (79, 80). Curcumin is also a nontoxic, non-mutagenic, non-carcinogenic, non-photo toxic agent and considered safe at lower doses than oral doses in intravenous administration in humans.
Nevertheless, some adverse effects are related to its consumption, such as dyspepsia, nausea, flatulence, and diarrhea. It was also demonstrated that turmeric could interact with some medications; it affects cytochromes P450, and the pharmacokinetics of some conventional drugs such as anticoagulants, antibiotics, antidiabetics, cardiovascular drugs, anticancer drugs, and antidepressants are influenced by curcuminoids (52, 80–82).
Effects of Curcuma longa and Curcumin on Type 2 Diabetes Mellitus
Several studies have investigated the effects of curcumin on diabetes. These studies are shown in Table 1 and discussed below.
A Pilot Study performed in Mexico (28) showed evidence that dietary supplementation with curcumin can reduce oxidative stress in patients with non-diabetic or diabetic proteinuric CKD. Curcumin significantly improved the elimination of free radicals activity in individuals with non-diabetic proteinuric CKD and reduced the plasma levels of malondialdehyde (MDA). However, its effects were limited; patients with diabetic proteinuric CKD treated with placebo showed a significant reduction in MDA content after the intervention. Also, no significant differences were observed in glutathione disulfide (GSSG) content or glutathione (GSH)/GSSG ratio between groups or with relation to sampling. Curcumin treatment did not modify the antioxidant activity of glutathione peroxidase, glutathione reductase, erythrocyte superoxide dismutase (SOD), and erythrocyte catalase, or to increase nuclear factor (erythroid-derived 2)-like 2 (Nrf2) activation in both patients with non-diabetic and diabetic proteinuric CKD. A study with a higher dose and longer follow-up is necessary to confirm these findings.
Another study, which investigated the effect of nano-curcumin in T2DM individuals, was adequately randomized, with no significant loss of participants, and even with a dose that the authors considered low, the effects of curcumin were positive. The fasting blood glucose (FBG), Hemoglobin A1c (HbA1C), body mass index (BMI), Estimated Average Glucose (eAG), total cholesterol (TC), LDL-c, HDL-c, and triglyceride (TG) were compared between the two groups after the intervention. Curcumin improved FBG, HbA1c, BMI, and eAG, but did not affect LDL-c, HDL-c, TG, and TC (29).
The results of Panahi et al. (20) showed an antioxidant effect of curcuminoid supplementation in patients with T2DM since supplementation promoted a significant increase in total antioxidant capacity and serum SOD activities, while MDA amounts were significantly decreased compared to the placebo group. Future studies may assess the impact of these antioxidant effects on diabetic complications and cardiovascular outcomes.
The treatment of T2DM patients with curcuminoid plus piperine resulted in a reduction in serum Lp (a) and an increase in HDL-c concentrations. These results are important because, until very recently, the possibilities of influencing Lp (a) were extremely limited. Serum concentrations of lipids including TC, LDL-c, HDL-c, TG, lipoprotein (a) (Lp(a)), and non-HDL-c were investigated at the beginning and at the end of the trial and revealed significant reductions in serum TC, non-HDL-c, and Lp (a) levels, and increase in serum HDL-c levels in the curcuminoid group compared to the placebo. Therefore, curcuminoids plus piperine may be a useful supplement in treating dyslipidemia in patients with T2DM (21).
The trial results performed by Panahi et al. (30) also revealed a beneficial effect of curcuminoids plus piperine supplementation on glycemic and hepatic parameters but not on hs-CRP levels in T2DM patients. However, this study has insufficient information regarding standard-of-care treatment that may be involved in the lack of curcuminoid efficacy on some parameters measured, particularly hs-CRP. Second, dietary intake and physical activity were not assessed; nevertheless, by randomization, it is expected that these characteristics were distributed similarly in the study groups minimizing the risk of bias. Finally, the trial duration was short, and it would help assess the efficacy of curcuminoids in long-term trials.
Positive effects of curcumin were also found by Adab et al. (31) in hyperlipidemic T2DM patients who received turmeric powder daily for eight weeks. BMI, TC, TG, LDL-c, HDL-c, insulin, HbA1C, FBG, fasting serum insulin, Apolipoprotein A1 and B were evaluated at the beginning and after the period of intervention. The authors concluded that this intervention could be used as an adjunct therapy to reduce diabetes complications, atherosclerosis, and overweight. The limitations of this trial may include a short intervention duration and low sample size.
The trial performed by Adibian et al. (32) with T2DM patients showed that the intervention with 1,500 mg daily of curcumin for ten weeks might reduce diabetes complications by decreasing indicators of inflammation. However, the authors suggest that higher sample sizes, longer duration, and different curcumin doses could lead to better outcomes.
In the trial performed by Asadi et al. (33), supplementation with nano-curcumin in patients with T2DM improved and reduced the severity of DSPN. The study also showed a reduction in glycemia after 2 h (Bs2hp), weight, and body mass index; however, these modifications were not significant. Meanwhile, the authors recognize some limitations: a short duration of follow-up, a single-dose trial, and low male participation.
The randomized, double-blind placebo-controlled trial performed in Iran by Hodaei et al. (34) indicated that the daily administration of a high dose of curcumin for ten weeks in NIDDM patients had positive effects on inflammatory indicators. However, this intervention had no effects on oxidative stress, serum insulin levels, IR, and HbA1c. The authors recognize that the study had a short duration of intervention and showed significant loss of patients.
Srinivasan et al. (35) showed that intervention with Curcuma longa produced a significant reduction in arterial stiffness in T2DM patients. The carotid-femoral pulse wave velocity (PWV), left brachial-ankle PWV, aortic augmentation pressure, aortic augmentation index, and aortic augmentation index decrease significantly. The authors attributed the lack of statistical reduction in endothelial dysfunction markers as adiponectin, leptin, ICAM, and VCAM due to methodological analysis limitations.
In the trial performed by Vanaie et al. (36), curcumin’s oral administration showed benefit on renal function by significantly decreasing albuminuria, therefore being considered a promising alternative therapy for T2DM patients with a mild decrease in glomerular filtration rate (GFR). The authors recognized some study limitations, such as small sample size and short intervention time.
The treatment of patients with T2DM with nano-curcumin capsules showed a beneficial effect on depression and anxiety. Moreover, curcumin was safe and well-tolerated during the study (37). However, these effects were minor, and no significant effect was observed for stress. The authors considered that the intervention might show better effects in the long term or higher supplementation doses.
Funamoto et al. (38) showed that the oral intervention with Theracurmin® in patients with impaired glucose tolerance or non-insulin-dependent diabetes mellitus could increase adiponectin expression, resulting in antiatherosclerotic action. Besides, the authors noticed that leptin demonstrated a decreasing trend after administration of Theracurmin. However, this trial’s limitations were the small sample size and the short duration of the intervention.
The results of Shafabakhsh et al. (39) revealed that the intervention with nano-curcumin in T2DM significantly decreased fasting plasma glucose and insulin levels and decreased the plasma lipids. Also, nano-curcumin intake upregulated gene expression of PPAR-γ and LDLR in PBMCs and increased total nitrite and total antioxidant capacity (TAC) levels without affecting GSH levels and gene expression of TGF-β. The authors concluded that this supplementation showed anti-inflammatory and antioxidant effects; however, they recognized some limitations in the trial, since they did not check compliance to nano-curcumin intake, and they were also unable to determine the effects of the administration on other biomarkers of oxidative stress and inflammation.
Another clinical trial developed by Shafabakhsh et al. (40) showed that curcumin intake upregulated PPAR-gamma in peripheral blood mononuclear cells of T2DM subjects with coronary heart disease (CHD). Furthermore, it was able to improve Pittsburgh Sleep Quality Index (PSQI) score. The authors considered that this is the first analysis of curcumin’s effects on psychological symptoms, inflammatory factors, oxidative status, and gene expression related to metabolic profiles in patients with T2DM and CHD. These findings suggest that curcumin can improve the psychological status, metabolic disorders, and patients’ quality of life. The study’s limitations include the short period of intervention, small sample size, lack of examinations for other metabolic and genetic biomarkers of inflammation, and oxidative damage.
The clinical trial developed by Mokhtari et al. (41) showed that the oral intervention with nano-curcumin in patients with diabetic foot ulcer (DFU) resulted in a significant improvement of FPG, insulin levels, the homeostasis model of assessment-insulin resistance (HOMA-IR), the quantitative insulin sensitivity check index (QUICKI), LDL-c, TAC and total glutathione (GSH) levels, but did not affect ulcer size, HbA1c, lipid profile, markers of inflammation, and oxidative stress. Therefore, the study revealed strengths, such as the first study that evaluated the effects of nano-curcumin on wound healing parameters and metabolic control in DFU patients. As DFU patients are susceptible to insulin resistance and cardiometabolic disorders, there was a good rationale for this project. However, the trial had few limitations, including the small sample size and the short intervention period. Furthermore, the authors could not assess the effects of curcumin supplementation on gene expression related to insulin resistance, lipid homeostasis, and inflammation in patients with DFU.
The trials that met the eligibility criteria for this review showed that curcumin significantly improves insulin resistance, serum glucose levels, HbA1c, lipid profile, and inflammatory biomarkers in patients with T2DM. However, in low doses and a short period of use, it may not interfere with the disease’s symptoms. Despite this, as T2DM remains incurable, understanding the role of curcumin in this pathology may represent a new therapeutic target.
Conclusion
T2DM has a multifactorial pathology and affects thousands of people worldwide. Its treatment consists of lifestyle changes, diet, physical activity, and therapies with medications for the rest of life. Curcumin is a natural anti-inflammatory and anti-diabetic agent representing a safe and low-cost alternative for this condition’s therapeutic approach, although it is still necessary to know its effective dose. We suggest that more robust and rigorous randomized controlled clinical trials are carried out to establish the role of curcumin in the therapeutics of T2DM.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author Contributions
All the authors contributed equally to the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
2. Patergnani S, Bouhamida E, Leo S, Pinton P, Rimessi A. Mitochondrial Oxidative Stress and “Mito-Inflammation”: Actors in the Diseases. Biomedicines (2021) 9(2):216. doi: 10.3390/biomedicines9020216
3. Ghorbani Y, Schwenger KJP, Allard JP. Manipulation of Intestinal Microbiome as Potential Treatment for Insulin Resistance and Type 2 Diabetes. Eur J Nutr (2021) 1–19. doi: 10.1007/s00394-021-02520-4
4. Wittwer J, Bradley D. Clusterin and Its Role in Insulin Resistance and the Cardiometabolic Syndrome. Front Immunol (2021) 12:612496. doi: 10.3389/fimmu.2021.612496
5. Snelson M, de Pasquale C, Ekinci EI, Coughlan MT. Gut Microbiome, Prebiotics, Intestinal Permeability and Diabetes Complications. Best Pract Res Clin Endocrinol Metab (2021) 101507. doi: 10.1016/j.beem.2021.101507
6. Zhang P, Sun X, Jin H, Zhang FL, Guo ZN, Yang Y. Association Between Obesity Type and Common Vascular and Metabolic Diseases: A Cross-Sectional Study. Front Endocrinol (2019) 10:900. doi: 10.3389/fendo.2019.00900
7. Sousa RAL, Improta-Caria AC, Souza BSF. Exercise-Linked Irisin: Consequences on Mental and Cardiovascular Health in Type 2 Diabetes. Int J Mol Sci (2021) 22(4):2199. doi: 10.3390/ijms22042199
8. Adams JA, Uryash A, Lopez JR, Sackner MA. The Endothelium as a Therapeutic Target in Diabetes: A Narrative Review and Perspective. Front Physiol (2021) 12:638491. doi: 10.3389/fphys.2021.638491
9. Shen CY, Lu CH, Wu CH, Li KJ, Kuo YM, Hsieh SC, et al. The Development of Maillard Reaction, and Advanced Glycation End Product (Age)-Receptor for AGE (Rage) Signaling Inhibitors as Novel Therapeutic Strategies for Patients With AGE-Related Diseases. Molecules (Basel Switzerland) (2020) 25(23):5591. doi: 10.3390/molecules25235591
10. Salvatore T, Pafundi PC, Galiero R, Rinaldi L, Caturano A, Vetrano E, et al. Can Metformin Exert as an Active Drug on Endothelial Dysfunction in Diabetic Subjects? Biomedicines (2021) 9(1):3. doi: 10.3390/biomedicines9010003
11. Tafrihi M, Imran M, Tufail T, Gondal TA, Caruso G, Sharma S, et al. The Wonderful Activities of the Genus Mentha: Not Only Antioxidant Properties. Molecules (Basel Switzerland) (2021) 26(4):1118. doi: 10.3390/molecules26041118
12. Asbaghi O, Kashkooli S, Mardani M, Rezaei Kelishadi M, Fry H, Kazemi M, et al. Effect of Green Coffee Bean Extract Supplementation on Liver Function and Inflammatory Biomarkers: A Meta-Analysis of Randomized Clinical Trials. Complement Therapies Clin Pract (2021) 43:101349. doi: 10.1016/j.ctcp.2021.101349
13. Matias JN, Achete G, Campanari G, Guiguer É L, Araújo AC, Buglio DS, et al. A Systematic Review of the Antidepressant Effects of Curcumin: Beyond Monoamines Theory. Aust New Z J Psychiatry (2021) 4867421998795. doi: 10.1177/0004867421998795
14. Kunnumakkara AB, Bordoloi D, Padmavathi G, Monisha J, Roy NK, Prasad S, et al. Curcumin, the Golden Nutraceutical: Multitargeting for Multiple Chronic Diseases. Br J Pharmacol (2017) 174:1325–48. doi: 10.1111/bph.13621
15. Perrone D, Ardito F, Giannatempo G, Dioguardi M, Troiano G, Lo Russo L, et al. Biological and Therapeutic Activities, and Anticancer Properties of Curcumin. Exp Ther Med (2015) 10:1615–23. doi: 10.3892/etm.2015.2749
16. Turmeric. Drugs and Lactation Database (Lactmed). Bethesda (MD: National Library of Medicine (US (2006).
17. Sultana S, Munir N, Mahmood Z, Riaz M, Akram M, Rebezov M, et al. Molecular Targets for the Management of Cancer Using Curcuma Longa Linn. Phytoconstituents: A Review. Biomed Pharmacother = Biomed Pharmacother (2021) 135:111078. doi: 10.1016/j.biopha.2020.111078
18. Hajavi J, Momtazi AA, Johnston TP, Banach M, Majeed M, Sahebkar A. Curcumin: A Naturally Occurring Modulator of Adipokines in Diabetes. J Cell Biochem (2017) 118:4170–82. doi: 10.1002/jcb.26121
19. Katsiki N, Mikhailidis DP, Banach M. Leptin, Cardiovascular Diseases and Type 2 Diabetes Mellitus. Acta Pharmacol Sin (2018) 39:1176–88. doi: 10.1038/aps.2018.40
20. Panahi Y, Khalili N, Sahebi E, Namazi S, Karimian MS, Majeed M, et al. Antioxidant Effects of Curcuminoids in Patients With Type 2 Diabetes Mellitus: A Randomized Controlled Trial. Inflammopharmacology (2017) 25:25–31. doi: 10.1007/s10787-016-0301-4
21. Panahi Y, Khalili N, Sahebi E, Namazi S, Reiner Ž, Majeed M, et al. Curcuminoids Modify Lipid Profile in Type 2 Diabetes Mellitus: A Randomized Controlled Trial. Complement Therapies Med (2017) 33:1–5. doi: 10.1016/j.ctim.2017.05.006
22. Altobelli E, Angeletti PM, Marziliano C, Mastrodomenico M, Giuliani AR, Petrocelli R. Potential Therapeutic Effects of Curcumin on Glycemic and Lipid Profile in Uncomplicated Type 2 Diabetes-A Meta-Analysis of Randomized Controlled Trial. Nutrients (2021) 13(2):404. doi: 10.3390/nu13020404
23. Cicero AFG, Colletti A, Bajraktari G, Descamps O, Djuric DM, Ezhov M, et al. Lipid-Lowering Nutraceuticals in Clinical Practice: Position Paper From an International Lipid Expert Panel. Nutr Rev (2017) 75:731–67. doi: 10.1093/nutrit/nux047
24. Johnston TP, Korolenko TA, Pirro M, Sahebkar A. Preventing Cardiovascular Heart Disease: Promising Nutraceutical and non-Nutraceutical Treatments for Cholesterol Management. Pharmacol Res (2017) 120:219–25. doi: 10.1016/j.phrs.2017.04.008
25. Ward N, Sahebkar A, Banach M, Watts G. Recent Perspectives on the Role of Nutraceuticals as Cholesterol-Lowering Agents. Curr Opin Lipidol (2017) 28:495–501. doi: 10.1097/MOL.0000000000000455
26. Sahebkar A. Curcuminoids for the Management of Hypertriglyceridaemia. Nat Rev Cardiol (2014) 11:123. doi: 10.1038/nrcardio.2013.140-c1
27. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ (Clin Res ed) (2009) 339:b2700. doi: 10.1136/bmj.b2700
28. Jiménez-Osorio AS, García-Niño WR, González-Reyes S, Álvarez-Mejía AE, Guerra-León S, Salazar-Segovia J, et al. The Effect of Dietary Supplementation With Curcumin on Redox Status and Nrf2 Activation in Patients With Nondiabetic or Diabetic Proteinuric Chronic Kidney Disease: A Pilot Study. J Renal Nutr: Off J Council Renal Nutr Natl Kidney Foundation (2016) 26:237–44. doi: 10.1053/j.jrn.2016.01.013
29. Rahimi HR, Mohammadpour AH, Dastani M, Jaafari MR, Abnous K, Ghayour Mobarhan M, et al. The Effect of Nano-Curcumin on HbA1c, Fasting Blood Glucose, and Lipid Profile in Diabetic Subjects: A Randomized Clinical Trial. Avicenna J Phytomed (2016) 6(5):567–77.
30. Panahi Y, Khalili N, Sahebi E, Namazi S, Simental-Mendía LE, Majeed M, et al. Effects of Curcuminoids Plus Piperine on Glycemic, Hepatic and Inflammatory Biomarkers in Patients With Type 2 Diabetes Mellitus: A Randomized Double-Blind Placebo-Controlled Trial. Drug Res (2018) 68:403–9. doi: 10.1055/s-0044-101752
31. Adab Z, Eghtesadi S, Vafa MR, Heydari I, Shojaii A, Haqqani H, et al. Effect of Turmeric on Glycemic Status, Lipid Profile, hs-CRP, and Total Antioxidant Capacity in Hyperlipidemic Type 2 Diabetes Mellitus Patients. Phytother Research: PTR (2019) 33:1173–81. doi: 10.1002/ptr.6312
32. Adibian M, Hodaei H, Nikpayam O, Sohrab G, Hekmatdoost A, Hedayati M. The Effects of Curcumin Supplementation on High-Sensitivity C-reactive Protein, Serum Adiponectin, and Lipid Profile in Patients With Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Phytother Research: PTR (2019) 33:1374–83. doi: 10.1002/ptr.6328
33. Asadi S, Gholami MS, Siassi F, Qorbani M, Khamoshian K, Sotoudeh G. Nano Curcumin Supplementation Reduced the Severity of Diabetic Sensorimotor Polyneuropathy in Patients With Type 2 Diabetes Mellitus: A Randomized Double-Blind Placebo- Controlled Clinical Trial. Complement Therapies Med (2019) 43:253–60. doi: 10.1016/j.ctim.2019.02.014
34. Hodaei H, Adibian M, Nikpayam O, Hedayati M, Sohrab G. The Effect of Curcumin Supplementation on Anthropometric Indices, Insulin Resistance and Oxidative Stress in Patients With Type 2 Diabetes: A Randomized, Double-Blind Clinical Trial. Diabetol Metab Syndrome (2019) 11:41. doi: 10.1186/s13098-019-0437-7
35. Srinivasan A, Selvarajan S, Kamalanathan S, Kadhiravan T, Prasanna Lakshmi NC, Adithan S. Effect of Curcuma Longa on Vascular Function in Native Tamilians With Type 2 Diabetes Mellitus: A Randomized, Double-Blind, Parallel Arm, Placebo-Controlled Trial. Phytother Research: PTR (2019) 33:1898–911. doi: 10.1002/ptr.6381
36. Vanaie A, Shahidi S, Iraj B, Siadat ZD, Kabirzade M, Shakiba F, et al. Curcumin as a Major Active Component of Turmeric Attenuates Proteinuria in Patients With Overt Diabetic Nephropathy. J Res Med Sci: Off J Isfahan Univ Med Sci (2019) 24:77. doi: 10.4103/jrms.JRMS_1055_18
37. Asadi S, Gholami MS, Siassi F, Qorbani M, Sotoudeh G. Beneficial Effects of Nano-Curcumin Supplement on Depression and Anxiety in Diabetic Patients With Peripheral Neuropathy: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Phytother Research: PTR (2020) 34:896–903. doi: 10.1002/ptr.6571
38. Funamoto M, Shimizu K, Sunagawa Y, Katanasaka Y, Miyazaki Y, Kakeya H, et al. Effects of Highly Absorbable Curcumin in Patients With Impaired Glucose Tolerance and Non-Insulin-Dependent Diabetes Mellitus. J Diabetes Res (2019) 2019:8208237. doi: 10.1155/2019/8208237
39. Shafabakhsh R, Asemi Z, Reiner Z, Soleimani A, Aghadavod E, Bahmani F. The Effects of Nano-curcumin on Metabolic Status in Patients With Diabetes on Hemodialysis, a Randomized, Double Blind, Placebo-Controlled Trial. Iranian J Kidney Dis (2020) 14(4):290–9.
40. Shafabakhsh R, Mobini M, Raygan F, Aghadavod E, Ostadmohammadi V, Amirani E, et al. Curcumin Administration and the Effects on Psychological Status and Markers of Inflammation and Oxidative Damage in Patients With Type 2 Diabetes and Coronary Heart Disease. Clin Nutr ESPEN (2020) 40:77–82. doi: 10.1016/j.clnesp.2020.09.029
41. Mokhtari M, Razzaghi R, Momen-Heravi M. The Effects of Curcumin Intake on Wound Healing and Metabolic Status in Patients With Diabetic Foot Ulcer: A Randomized, Double-Blind, Placebo-Controlled Trial. Phytother Research: PTR (2020) 35(4):2099–107. doi: 10.1002/ptr.6957
42. Artasensi A, Pedretti A, Vistoli G, Fumagalli L. Type 2 Diabetes Mellitus: A Review of Multi-Target Drugs. Molecules (Basel Switzerland) (2020) 25(8):1987. doi: 10.3390/molecules25081987
43. Eizirik DL, Pasquali L, Cnop M. Pancreatic β-Cells in Type 1 and Type 2 Diabetes Mellitus: Different Pathways to Failure. Nat Rev Endocrinol (2020) 16:349–62. doi: 10.1038/s41574-020-0355-7
44. Li N, Wang LJ, Jiang B, Li XQ, Guo CL, Guo SJ, et al. Recent Progress of the Development of Dipeptidyl Peptidase-4 Inhibitors for the Treatment of Type 2 Diabetes Mellitus. Eur J Medicinal Chem (2018) 151:145–57. doi: 10.1016/j.ejmech.2018.03.041
45. Guthrie RA, Guthrie DW. Pathophysiology of Diabetes Mellitus. Crit Care Nurs Q (2004) 27:113–25. doi: 10.1097/00002727-200404000-00003
46. Taylor JJ, Preshaw PM, Lalla E. A Review of the Evidence for Pathogenic Mechanisms That may Link Periodontitis and Diabetes. J Clin Periodontol (2013) 40(Suppl 14):S113–34. doi: 10.1111/jcpe.12059
47. Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium Glucose Cotransporter 2 Inhibitors in the Treatment of Diabetes Mellitus: Cardiovascular and Kidney Effects, Potential Mechanisms, and Clinical Applications. Circulation (2016) 134:752–72. doi: 10.1161/CIRCULATIONAHA.116.021887
48. Scheen AJ. Sodium-Glucose Cotransporter Type 2 Inhibitors for the Treatment of Type 2 Diabetes Mellitus. Nat Rev Endocrinol (2020) 16:556–77. doi: 10.1038/s41574-020-0392-2
49. Jain A, Saxena S, Khanna VK, Shukla RK, Meyer CH. Status of Serum VEGF and ICAM-1 and its Association With External Limiting Membrane and Inner Segment-Outer Segment Junction Disruption in Type 2 Diabetes Mellitus. Mol Vision (2013) 19:1760–8.
50. Giacco F, Brownlee M. Oxidative Stress and Diabetic Complications. Circ Res (2010) 107:1058–70. doi: 10.1161/CIRCRESAHA.110.223545
51. Folli F, Corradi D, Fanti P, Davalli A, Paez A, Giaccari A, et al. The Role of Oxidative Stress in the Pathogenesis of Type 2 Diabetes Mellitus Micro- and Macrovascular Complications: Avenues for a Mechanistic-Based Therapeutic Approach. Curr Diabetes Rev (2011) 7:313–24. doi: 10.2174/157339911797415585
52. Dosoky NS, Setzer WN. Chemical Composition and Biological Activities of Essential Oils of Curcuma Species. Nutrients (2018) 10(9):1196. doi: 10.3390/nu10091196
53. Kocaadam B, Sanlier N. Curcumin, an Active Component of Turmeric (Curcuma Longa), and its Effects on Health. Crit Rev Food Sci Nutr (2017) 57:2889–95. doi: 10.1080/10408398.2015.1077195
54. Ayati Z, Ramezani M, Amiri MS, Moghadam AT, Rahimi H, Abdollahzade A, et al. Ethnobotany, Phytochemistry and Traditional Uses of Curcuma Spp. and Pharmacological Profile of Two Important Species (C. Longa and C. Zedoaria): A Review. Curr Pharm Design (2019) 25:871–935. doi: 10.2174/1381612825666190402163940
55. Mazieiro R, Frizon RR, Barbalho SM, Goulart RA. Is Curcumin a Possibility to Treat Inflammatory Bowel Diseases? J Medicinal Food (2018) 21:1077–85. doi: 10.1089/jmf.2017.0146
56. Jena S, Ray A, Banerjee A, Sahoo A, Nasim N, Sahoo S, et al. Chemical Composition and Antioxidant Activity of Essential Oil From Leaves and Rhizomes of Curcuma Angustifolia Roxb. Natural Product Res (2017) 31:2188–91. doi: 10.1080/14786419.2017.1278600
57. Lobo R, Prabhu KS, Shirwaikar A, Shirwaikar A. Curcuma Zedoaria Rosc. (White Turmeric): A Review of its Chemical, Pharmacological and Ethnomedicinal Properties. J Pharm Pharmacol (2009) 61:13–21. doi: 10.1211/jpp/61.01.0003
58. Itokawa H, Shi Q, Akiyama T, Morris-Natschke SL, Lee KH. Recent Advances in the Investigation of Curcuminoids. Chin Med (2008) 3:11. doi: 10.1186/1749-8546-3-11
59. Srivilai J, Phimnuan P, Jaisabai J, Luangtoomma N, Waranuch N, Khorana N, et al. Curcuma Aeruginosa Roxb. Essential Oil Slows Hair-Growth and Lightens Skin in Axillae; a Randomised, Double Blinded Trial. Phytomed Int J phytother Phytopharmacol (2017) 25:29–38. doi: 10.1016/j.phymed.2016.12.007
60. Seo EJ, Fischer N, Efferth T. Phytochemicals as Inhibitors of NF-κb for Treatment of Alzheimer’s Disease. Pharmacol Res (2018) 129:262–73. doi: 10.1016/j.phrs.2017.11.030
61. Cunha Neto F, Marton LT, de Marqui SV, Lima TA, Barbalho SM. Curcuminoids From Curcuma Longa: New Adjuvants for the Treatment of Crohn’s Disease and Ulcerative Colitis? Crit Rev Food Sci Nutr (2019) 59:2136–43. doi: 10.1080/10408398.2018.1456403
62. Baliga MS, Joseph N, Venkataranganna MV, Saxena A, Ponemone V, Fayad R. Curcumin, an Active Component of Turmeric in the Prevention and Treatment of Ulcerative Colitis: Preclinical and Clinical Observations. Food Funct (2012) 3:1109–17. doi: 10.1039/c2fo30097d
63. Hanai H, Sugimoto K. Curcumin has Bright Prospects for the Treatment of Inflammatory Bowel Disease. Curr Pharm Design (2009) 15:2087–94. doi: 10.2174/138161209788489177
64. Hatcher H, Planalp R, Cho J, Torti FM, Torti SV. Curcumin: From Ancient Medicine to Current Clinical Trials. Cell Mol Life Sci: CMLS (2008) 65:1631–52. doi: 10.1007/s00018-008-7452-4
65. Pivari F, Mingione A, Brasacchio C, Soldati L. Curcumin and Type 2 Diabetes Mellitus: Prevention and Treatment. Nutrients (2019) 11(8):1837. doi: 10.3390/nu11081837
66. Pulido-Moran M, Moreno-Fernandez J, Ramirez-Tortosa C, Ramirez-Tortosa M. Curcumin and Health. Molecules (Basel Switzerland) (2016) 21:264. doi: 10.3390/molecules21030264
67. Stanić Z. Curcumin, a Compound From Natural Sources, a True Scientific Challenge - A Review. Plant Foods for Human Nutrition (Dordrecht. Netherlands) (2017) 72:1–12. doi: 10.1007/s11130-016-0590-1
68. Liang Y, Zhu B, Li S, Zhai Y, Yang Y, Bai Z, et al. Curcumin Protects Bone Biomechanical Properties and Microarchitecture in Type 2 Diabetic Rats With Osteoporosis Via the Tgfβ/Smad2/3 Pathway. Exp Ther Med (2020) 20:2200–8. doi: 10.3892/etm.2020.8943
69. Saffarionpour S, Diosady LL. Curcumin, a Potent Therapeutic Nutraceutical and its Enhanced Delivery and Bioaccessibility by Pickering Emulsions. Drug Delivery Trans Res (2021) 1–34. doi: 10.1007/s13346-021-00936-3
70. Rodrigues FC, Kumar NA, Thakur G. The Potency of Heterocyclic Curcumin Analogues: An Evidence-Based Review. Pharmacol Res (2021) 105489. doi: 10.1016/j.phrs.2021.105489
71. Dei Cas M, Ghidoni R. Dietary Curcumin: Correlation Between Bioavailability and Health Potential. Nutrients (2019) 11(9):2147. doi: 10.3390/nu11092147
72. Kotha RR, Luthria DL. Curcumin: Biological, Pharmaceutical, Nutraceutical, and Analytical Aspects. Molecules (Basel Switzerland) (2019) 24(16):2930. doi: 10.3390/molecules24162930
73. Lopresti AL. The Problem of Curcumin and Its Bioavailability: Could its Gastrointestinal Influence Contribute to Its Overall Health-Enhancing Effects? Adv Nutr (Bethesda Md) (2018) 9:41–50. doi: 10.1093/advances/nmx011
74. Tsuda T. Curcumin as a Functional Food-Derived Factor: Degradation Products, Metabolites, Bioactivity, and Future Perspectives. Food Funct (2018) 9:705–14. doi: 10.1039/C7FO01242J
75. Liu W, Zhai Y, Heng X, Che FY, Chen W, Sun D, et al. Oral Bioavailability of Curcumin: Problems and Advancements. J Drug Targeting (2016) 24:694–702. doi: 10.3109/1061186X.2016.1157883
76. Šudomová M, Hassan STS. Nutraceutical Curcumin With Promising Protection Against Herpesvirus Infections and Their Associated Inflammation: Mechanisms and Pathways. Microorganisms (2021) 9(2):292. doi: 10.3390/microorganisms9020292
77. Meghwal M, Goswami TK. Piper Nigrum and Piperine: An Update. Phytother Research: PTR (2013) 27:1121–30. doi: 10.1002/ptr.4972
78. Jude S, Amalraj A, Kunnumakkara AB, Divya C, Löffler BM, Gopi S. Development of Validated Methods and Quantification of Curcuminoids and Curcumin Metabolites and Their Pharmacokinetic Study of Oral Administration of Complete Natural Turmeric Formulation (Cureit™) in Human Plasma Via UPLC/ESI-Q-TOF-MS Spectrometry. Molecules (Basel Switzerland) (2018) 23(10):2415. doi: 10.3390/molecules23102415
79. Tossetta G, Fantone S, Giannubilo SR, Marzioni D. The Multifaced Actions of Curcumin in Pregnancy Outcome. Antioxid (Basel Switzerland) (2021) 10(1):126. doi: 10.3390/antiox10010126
80. Soleimani V, Sahebkar A, Hosseinzadeh H. Turmeric (Curcuma Longa) and its Major Constituent (Curcumin) as Nontoxic and Safe Substances: Review. Phytother Research: PTR (2018) 32:985–95. doi: 10.1002/ptr.6054
81. Goulart RA, Barbalho SM, Rubira CJ, Araújo AC, Lima VM, Rogerio Leoni B, et al. Curcumin Therapy for Ulcerative Colitis Remission: Systematic Review and Meta-Analysis. Expert Rev Gastroenterol Hepatol (2020) 14:1171–9. doi: 10.1080/17474124.2020.1808460
Keywords: Curcuma longa, curcumin, curcuminoids, diabetes, type 2 diabetes mellitus
Citation: Marton LT, Pescinini-e-Salzedas LM, Camargo MEC, Barbalho SM, Haber JFdS, Sinatora RV, Detregiachi CRP, Girio RJS, Buchaim DV and Cincotto dos Santos Bueno P (2021) The Effects of Curcumin on Diabetes Mellitus: A Systematic Review. Front. Endocrinol. 12:669448. doi: 10.3389/fendo.2021.669448
Received: 18 February 2021; Accepted: 08 April 2021;
Published: 03 May 2021.
Edited by:
Alberto Battezzati, University of Milan, ItalyReviewed by:
Somasundaram Arumugam, National Institute of Pharmaceutical Education and Research, Kolkata, IndiaBharat B. Aggarwal, University of Texas MD Anderson Cancer Center, United States
Copyright © 2021 Marton, Pescinini-e-Salzedas, Camargo, Barbalho, Haber, Sinatora, Detregiachi, Girio, Buchaim and Cincotto dos Santos Bueno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandra M. Barbalho, c21iYXJiYWxob0BnbWFpbC5jb20=