 Everardo Josué Díaz-López1,2*
Everardo Josué Díaz-López1,2* Rocio Villar-Taibo1*
Rocio Villar-Taibo1* Gemma Rodriguez-Carnero1,3
Gemma Rodriguez-Carnero1,3 Antia Fernandez-Pombo1,2
Antia Fernandez-Pombo1,2 Roberto Garcia-Peino1Manuel Narciso Blanco-Freire4
Roberto Garcia-Peino1Manuel Narciso Blanco-Freire4 Alberto Pena-Dubra1Teresa Prado-Moraña1,2Irea- Fernández-Xove1Edurne Pérez-Béliz5
Alberto Pena-Dubra1Teresa Prado-Moraña1,2Irea- Fernández-Xove1Edurne Pérez-Béliz5 Jose Manuel Cameselle-Teijeiro5,6Alvaro Hermida-Ameijeiras7Miguel Angel Martinez-Olmos1,8,9
Jose Manuel Cameselle-Teijeiro5,6Alvaro Hermida-Ameijeiras7Miguel Angel Martinez-Olmos1,8,9- 1Division of Endocrinology and Nutrition, University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
- 2Unidad de Enfermedades Tiroideas e Metabólicas (UETeM)-Molecular Pathology Group. Department of Psychiatry, Radiology, Public Health, Nursing and Medicine, Health Research Institute of Santiago de Compostela (IDIS)-Center for Research in Molecular Medicine and Chronic Diseases (CIMUS), University of Santiago de Compostela, Santiago de Compostela, Spain
- 3Division of Epigenomics in Endocrinology and Nutrition Group-Health Research Institute of Santiago de Compostela (IDIS), University of Santiago de Compostela, Santiago de Compostela, Spain
- 4Division of Surgery, University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
- 5Division of Pathology, University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
- 6Medical Faculty, University of Santiago de Compostela, Santiago de Compostela, Spain
- 7Division of Internal Medicine, University Clinical Hospital of Santiago de Compostela, Santiago de Compostela, Spain
- 8Molecular Endocrinology Group-Health Research Institute of Santiago de Compostela (IDIS), University of Santiago de Compostela, Santiago de Compostela, Spain
- 9CIBER Pathophysiology of Obesity and Nutrition (CIBEROBN), Carlos III Health Institute, Madrid, Spain
Severe hypokalaemia causing rhabdomyolysis (RML) in primary aldosteronism (PA) is a rare entity, and only a few cases have been reported over the last four decades. This systematic review and case report aims to gather all published data regarding a hypokalaemic RML as presentation of PA in order to contribute to the early diagnosis of this extremely rare presentation. With the use of PubMed Central, EMBASE, and Google Scholar, a thorough internet-based search of the literature was conducted to identify articles and cases with RML secondary to hypokalaemia due to PA between June 1976 and July 2023. The case study concerns a 68-year-old male patient with hypokalaemic RML at presentation of PA. In the systematic review of the literature, 37 cases of RML secondary to hypokalaemia due to PA have been reported to date. In summary, the median age was 47.5 years, the male/female ratio was 17/21, all patients presented symptoms (weakness and/or myalgia), all the patients were hypertensive, and only four patients had complications with acute kidney injury (AKI). Although PA rarely presents with RML, it should be suspected when marked hypokalaemia and hypertension are also present. Early detection and management are essential to reduce the frequency of manifestations such as AKI.
1 Introduction
Primary aldosteronism (PA), also known as Conn’s syndrome, is the most common and treatable cause of endocrine-related hypertension, with a prevalence of 5%–10% among patients with hypertension in primary care and 20% among patients with resistant hypertension (1). PA results from the excessive production of aldosterone independently of renin and angiotensin II and leads to increased renal tubular resorption of sodium and volume expansion, resulting in increased blood pressure and hypokalaemia.
Although hypokalaemia is common in this disorder, severe hypokalaemia causing rhabdomyolysis (RML) in PA is a rare entity, and only a few cases have been reported over the last four decades (2, 3).
RML is a syndrome characterised by the destruction of striated muscle, which triggers the consequent release of intracellular elements such as electrolytes, myoglobin, creatine kinase (CK), and aldolase (4, 5). The effects are recognised as a clinical syndrome of muscle injury that is associated with the development of myoglobinuria, electrolyte abnormalities, and often acute kidney injury (AKI) (6, 7). RML has been described in patients with electrolyte disorders and endocrine disorders such as hypothyroidism and hyperthyroidism, hyperaldosteronism, diabetes mellitus, and diabetic ketoacidosis (4). One of the most intriguing causes of RML is potassium deficiency (8). The mechanism of hypokalaemia-induced RML is still not clear. Profound hypokalaemia (serum potassium <2.5 mEq/L) might play an important role in muscle damage secondary to i) contraction of capillaries with reduced muscle blood supply and resulting in lysing muscle cells, ii) suppression of synthesis and storage of glycogen, and iii) deranged ion transport across the cell membrane (2, 9).
We present a case report and systematic review aimed at collecting and summarising the published data regarding hypokalaemic RML as a form of presentation of PA in order to contribute to the early diagnosis of this extremely rare presentation.
2 Case report
A 68-year-old man with a history of schizophrenia, type 2 diabetes mellitus, and uncontrolled hypertension of 8 years was evaluated in the emergency department due to a fall after an episode acute of muscle weakness in the lower limbs while walking.
He received home antihypertensive treatment with a beta-blocker, mineralocorticoid receptor antagonists (MRAs), and angiotensin-converting enzyme (ACE) inhibitors.
His blood pressure was 183/101 mmHg with a heart rate of 40 beats/minute. He presented a body mass index of 29.8 kg/m2. Laboratory tests showed severe hypokalaemia with serum potassium of 2.1 mmol/L, glycaemia of 459 mg/dL, creatinine of 2.1 mg/dL, myoglobinaemia with serum myoglobin of 10,453 ng/mL, and CK of 3,616 IU/L. An electrocardiogram presented a prolongation of the QT interval.
Four months earlier, he presented with serum potassium of 3.9 mmol/L and creatinine of 0.97 mg/dL.
His clinical records were reviewed, and 4 months earlier, his levels of potassium and creatinine were normal. He also presented a 10-mm right adrenal nodule on an abdominal computed tomography (CT) scan 11 years previously, which was unknown at the time of admission.
With the clinical suspicion of primary hyperaldosteronism, the patient underwent a hormonal analysis, which showed high levels of plasma aldosterone (188.0 ng/dL [upper limit of normal, 39.2 ng/dL]) and low plasma renin activity (0.18 ng/mL/h) with an aldosteronetorenin ratio (ARR) of 1,074.3 ng/dL. His corresponding potassium was 4.1 mmol/L. Plasma cortisol, testosterone, dehydroepiandrosterone sulfate, 24-hour urine cortisol, and metanephrine levels were normal. A new adrenal CT was requested, observing a 27-mm nodule in the right adrenal gland, which showed attenuation of less than 10 Hounsfield units (Figure 1).
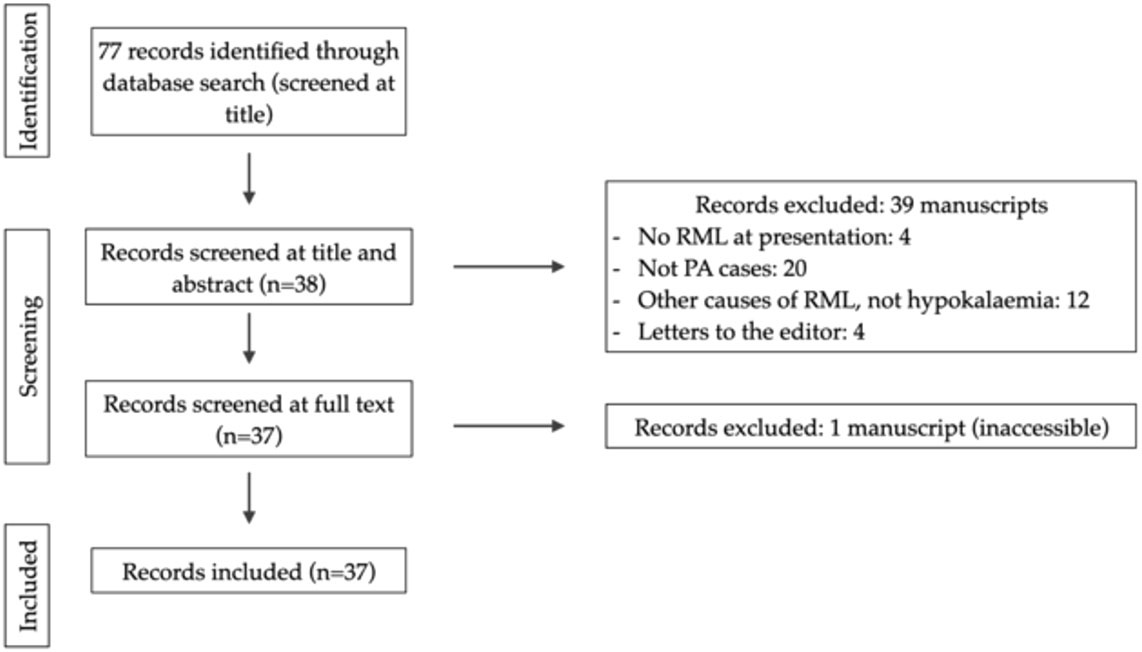
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart for the identification of inclusion and exclusion of studies.
After stabilisation, the decision was taken to discharge the patient due to clinical improvement and normalisation of renal function, serum potassium, CK, and electrocardiogram alterations. Antihypertensives were changed to others that do not interfere with renin and aldosterone measurements in order to request a new hormonal study after 6 weeks.
During follow-up in the outpatient clinic, he presented an ARR of 866.7 ng/dL. Due to the presence of overt PA, no confirmatory studies were deemed necessary since this pattern is not observed in other entities (10).
The patient was evaluated by the Endocrine Tumour Committee at our hospital and scheduled for right posterior retroperitoneoscopic adrenalectomy. An adrenalectomy specimen with abundant adjacent adipose tissue was obtained, weighing 79.7 g and occupying a combined area of 10.8 × 4.2 cm. After the serial cuts, an adrenal gland with conventional characteristics was identified in an area of up to 4.0 × 2.2 cm. The gland included a solid, well-delimited, yellowish nodule measuring 2.6 × 2.3 × 2.0 cm in diameter, compressing the residual adrenal tissue. A diagnosis of cortical adenoma was confirmed, pathologically consistent with aldosterone production. The adjacent adipose tissue did not present notable alterations (Figure 2). A 4.0-cm-diameter cortical adenoma was confirmed, pathologically consistent with aldosterone production. As an incidental finding, the tumour included spironolactone bodies (Figure 3).
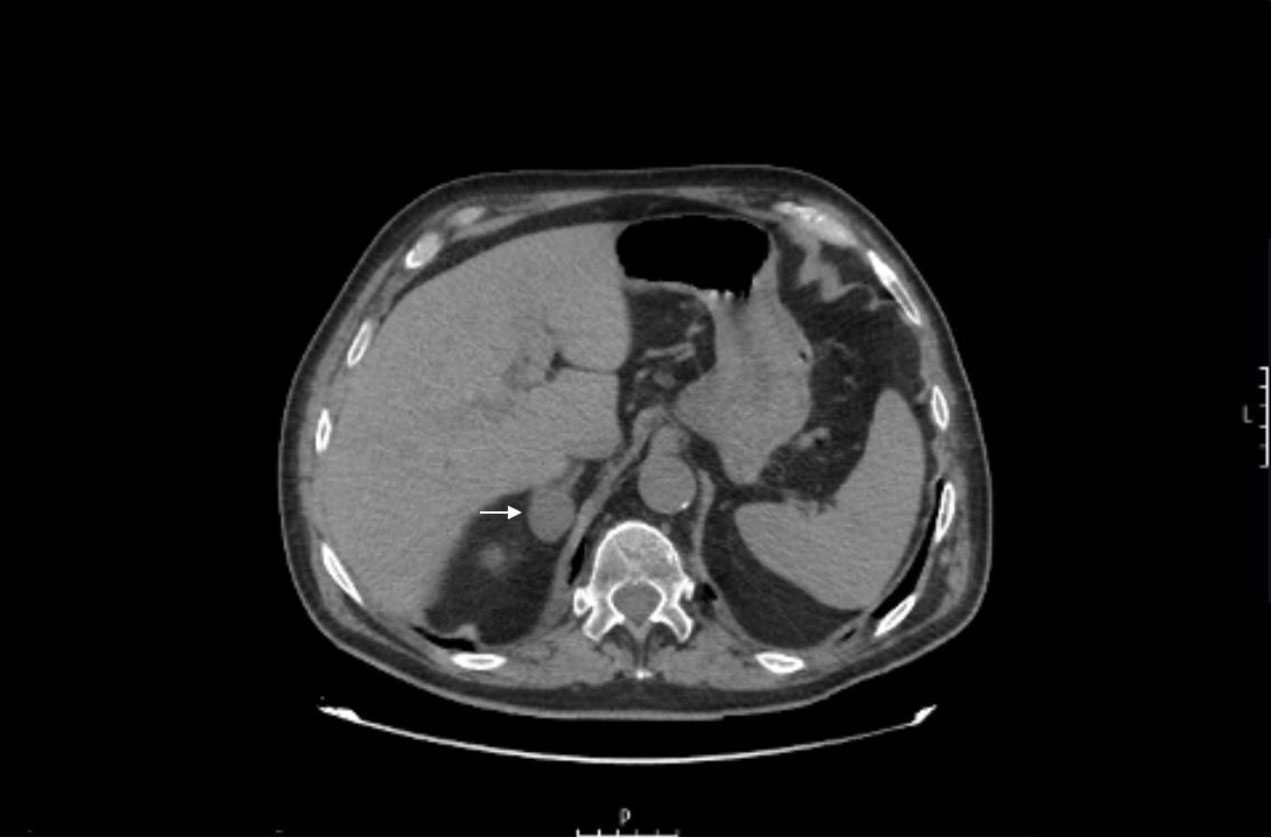
Figure 2 Adrenal computed tomography of the case study. White arrow showing a 27-mm nodule in the right adrenal gland.

Figure 3 Aldosterone-producing adrenal cortical adenoma. The tumour is a solid, yellowish nodule that is well-demarcated by a thin rim of normal adrenal cortex.
Fifteen days after surgery, there was a clinical improvement in strength, and antihypertensive treatment (only with amlodipine 5 mg) was reduced due to good control of blood pressure. Potassium and aldosterone levels normalised without the need for oral potassium supplementation. The patient is currently fully recovered and is being monitored in primary care.
3 Research design and methods
3.1 Literature search and screening
The reported systematic review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The protocol was registered on PROSPERO International Prospective Register of Systematic Reviews, with registration ID CRD42023439678.
With the use of PubMed Central, EMBASE, and Google Scholar, a thorough internet-based search of the literature was carried out to identify articles and cases with RML secondary to hypokalaemia due to PA between June 17, 1976, and July 2, 2023. The search strategy was as follows: [(rhabdomyolysis) OR (hypokalaemia) OR (hypokalaemic rhabdomyolysis) OR (primary aldosteronism AND (hypokalaemia OR rhabdomyolysis)] OR (hypokalaemic rhabdomyolysis) OR (Conn’s syndrome).
3.2 Study selection and data management
Regarding study selection, data from the retrieved articles (title, authors, date of publication, journal, abstract, and keywords) were gathered from the major scientific platforms and transferred into Zotero (www.zotero.org) to identify and eliminate duplicate articles. Two independent reviewers (EJDL and RVT) initially screened the eligibility of studies based on the title/abstract content of each study identified. Studies that clearly did not satisfy the inclusion criteria were discarded with any disagreements being resolved by consensus or, if necessary, via consultation with a third reviewer (GRC). When no agreement was reached, a third reviewer (GRC) was involved to make the final decision.
All potentially eligible articles from this screening were downloaded as full text and distributed to the reviewers for verification that they fulfilled all the inclusion criteria and none of the exclusion criteria. Only cases or case series with hypokalaemic RML as presentation of PA were considered. Cases with no RML as presentation or other causes of RML not related to hypokalaemia were excluded. No restrictions on language or search period were included. In addition to the relevant articles, the articles referenced in the retrieved publications were also manually scrutinised.
General information from each article, such as first author or year of publication, was noted. Specific epidemiological data were also registered, including age and sex. The following clinical and biochemical variables were recorded: initial symptoms, antihypertensive drugs, presence of AKI, serum potassium (mmol/L), and creatinine (u/L). The treatment for PA and the anatomopathological diagnosis were also recorded.
Written informed consent was obtained from the patient for the publication of this article.
4 Results of the systematic review
In the systematic review of the literature, 37 cases of RML secondary to hypokalaemia due to PA reported to date were identified. The flow chart of studies included is presented in Figure 4.
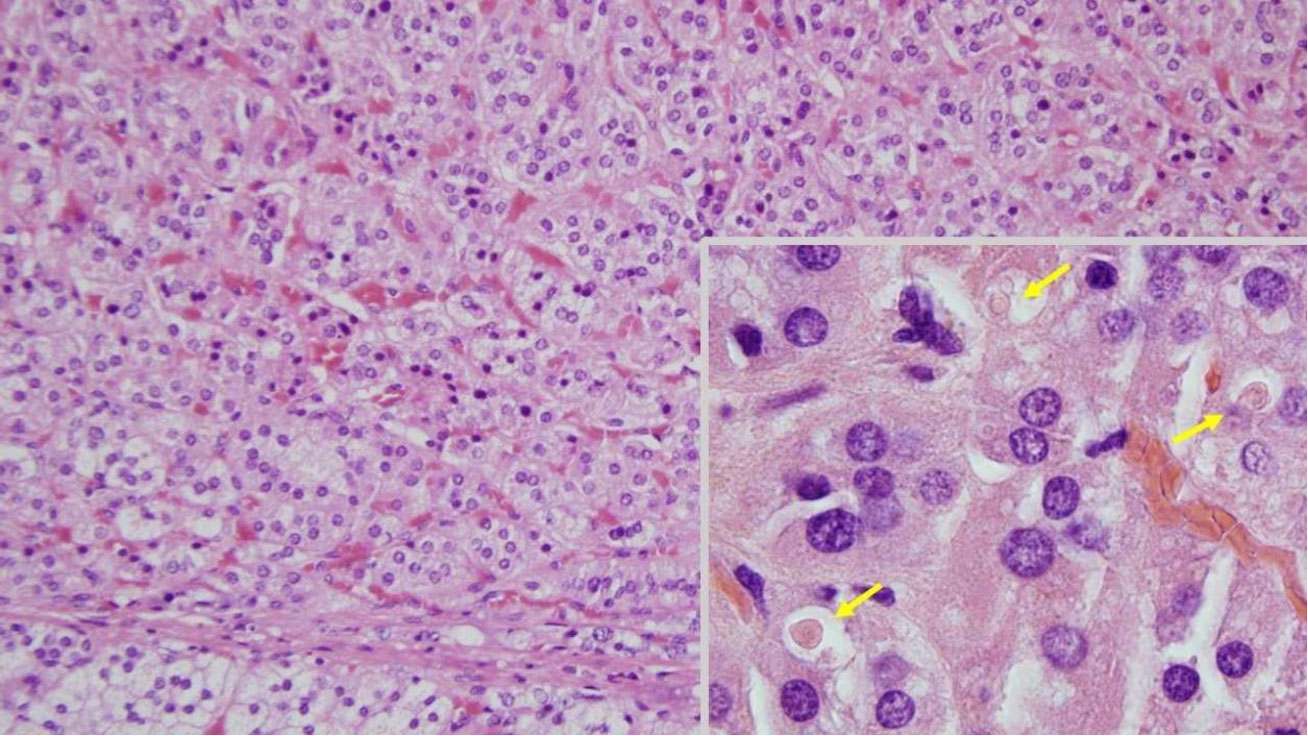
Figure 4 Adrenal histology of the case study. The adenoma is well-vascularised and composed of trabeculae of monomorphic cells with weakly eosinophilic cytoplasm, which contrasts with the clearer appearance of the cytoplasm of adjacent normal cells (bottom). At higher magnification (inset), spironolactone bodies can be seen (arrows); (hematoxylin and eosin, ×200; inset, ×1,000).
Clinical features, diagnosis data, treatment, and outcomes of all cases (including our patient) are presented in Table 1. In summary, the median age was 47.5 years, the male/female ratio was 17/21, all patients presented symptoms (weakness and/or myalgia), all the patients were hypertensive, and only four patients had complications with AKI.
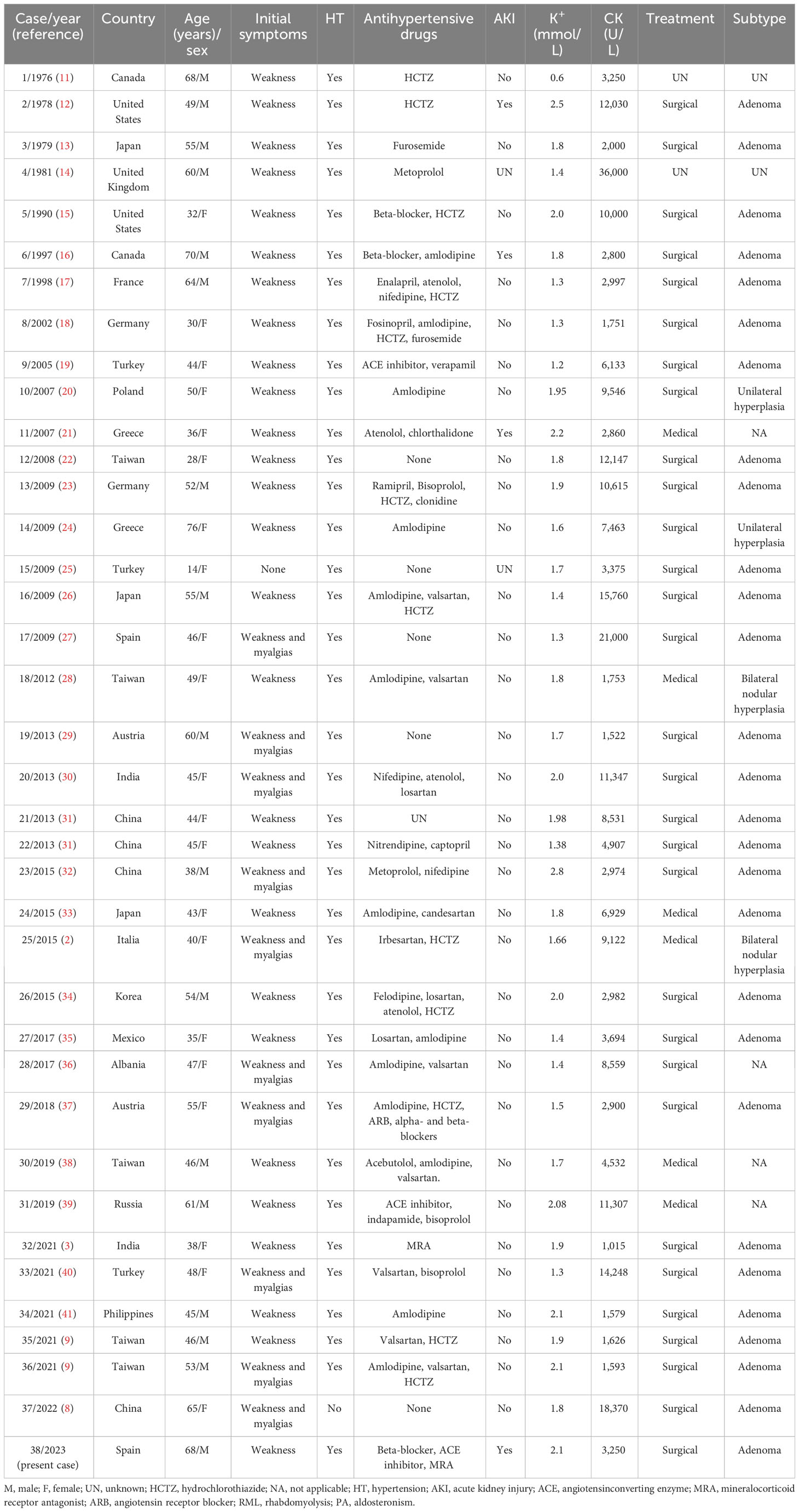
Table 1 Clinical features, diagnosis data, treatment, and outcomes of all cases with hypokalaemic RML due to PA as a form of presentation.
5 Discussion
Here, we present a patient who was suspected of having RML secondary to PA due to the presence of resistant hypertension and hypokalaemia, although this is a very rare presentation of PA, and it is more common for patients with RML to present hyperkalaemia due to the release of intracellular metabolites (potassium, phosphates, and urate) and intracellular proteins to the extracellular space and circulation (42).
The diagnosis of RML was based on the clinical presentation and the very high levels of CK and myoglobin. The myoglobinuria was detected by the presence of dark-coloured urine, with a positive urine dipstick test for blood without evidence of red blood cells on microscopy. This is a clue to the presence of RML, as myoglobin will also react with the orthotolidine test reagent (7).
A confirmatory test for PA was not required in this patient considering that current guidelines suggest bypassing such tests in patients with a particularly severe clinical phenotype (overt PA), i.e., patients with hypokalaemia, undetectable plasma renin, and plasma aldosterone concentrations higher than 20 ng/dL (555 pmol/L) (43).
In the systematic review, 21 out of 38 of the cases presented in women (55%), the majority of the patients (30/38) were younger than 60 years, and all the patients manifested symptoms (weakness and/or myalgias). In the Chinese biomedical literature database, 13 cases have been reported of PA being related to hypokalaemic RML. In this series, the epidemiological characteristics of the patients were similar, with a predominance of cases in women (69%), most of whom were under 60 years of age (84.6%). All 13 patients had a history of hypertension and weakness and/or myalgias. Twelve out of 13 patients had blood potassium lower than 2.5 mmol/L, 11 had adrenal adenoma, and none had renal failure (8). In a review of the English literature, 22 cases of PA related to hypokalaemic RML were summarised. Among these cases, nine patients were male and 13 were female (59%), five were 60 years of age or older and 17 were younger, 21 had symptoms of fatigue, and 20 had hypertension (2).
Regarding the levels of hypokalaemia related to RML occurrence, severe muscle weakness or RML usually occurs if serum potassium is below 2.5 mmol/L (44). In this review of cases, there are 35 patients who developed rhabdomyolysis with serum potassium below 2.1 mmol/L.
In the cases described, acute renal injury was very rare, being observed in only four patients (12, 16, 21). It was intensively managed with fluid therapy and intravenous potassium, with rapid clinical and analytical improvement. Intravenous fluids should be initiated as soon as possible, preferably within the first 6 hours after muscle injury (45).
In this review, 85% of the patients received surgery as the treatment for PA. The pathological diagnosis was adrenal adenomas in 93% of the cases. Of those who received definitive medical treatment (n = 5), three patients did not accept surgery, and two did not meet the criteria due to bilateral nodular hyperplasia. As an incidental finding, in our case, spironolactone bodies were detected. The incidence of spironolactone bodies within the adrenal gland in patients taking spironolactone or eplerenone is unknown. Patel et al., in a retrospective study, detected inclusions in only 33% of patients with PA treated with spironolactone and/or eplerenone (46). In this review, there were no cases other than our case describing this finding.
In conclusion, after reviewing the cases published in the literature, it can be concluded that hypokalaemic RML due to PA is a rare condition. It presents mostly in young patients (<60 years of age) with a certain predominance among women. It should be suspected in subjects with hypertension and mild hypokalaemia. Early diagnosis and management can lead to a better evolution of the patient, reducing the frequency of RML and complications such as AKI.
Author contributions
ED-L: Conceptualization, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. RV-T: Conceptualization, Methodology, Supervision, Writing – review & editing. GR-C: Conceptualization, Writing – review & editing. AF-P: Supervision, Writing – review & editing. RG-P: Writing – review & editing. MB-F: Writing – review & editing. AP-D: Writing – review & editing. TP-M: Writing – review & editing. IF-X: Writing – review & editing. EP-B: Writing – review & editing. JC-T: Writing – review & editing. AH-A: Supervision, Writing – review & editing. MM-O: Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article. AF-P receives funding from the Fundació;n Alfonso Martí;n Escudero.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Parra Ramí;rez P, Rojas-Marcos PM, Paja Fano M, González Boillos M, Pascual-Corrales E, Garcí;a-Cano A, et al. Differences in the presentation and evolution of primary aldosteronism in elderly (≥65 years) and young patients (<65 years)(2022). Available at: https://ec.bioscientifica.com/view/journals/ec/11/6/EC-22-0169.xml (Accessed 2023 Jun 17).
2. Zavatto A, Concistrè A, Marinelli C, Zingaretti V, Umbro I, Fiacco F, et al. Hypokalemic rhabdomyolysis: a rare manifestation of primary aldosteronism. Eur Rev Med Pharmacol Sci (2015) 19(20):3910–6.
3. Kollipara S, Ravindra S, Pai K, Shetty S. Quadriplegia and rhabdomyolysis as a presenting feature of Conn’s syndrome. BMJ Case Rep (2021) 14(1):e234686. doi: 10.1136/bcr-2020-234686
4. Młynarska E, Krzemińska J, Wronka M, Franczyk B, Rysz J, Rhabdomyolysis-Induced AKI. (RIAKI) including the role of COVID-19. Int J Mol Sci (2022) 23(15):8215. doi: 10.3390/ijms23158215
5. Baeza-Trinidad R. Rhabdomyolysis: A syndrome to be considered(2022). Available at: https://linkinghub.elsevier.com/retrieve/pii/S2387020622000961 (Accessed 2023 Apr 10).
6. Gupta A, Thorson P, Penmatsa KR, Gupta P. Rhabdomyolysis: revisited. Ulster Med J (2021) 90(2):61–9.
7. Zimmerman JL, Shen MC. Rhabdomyolysis(2013). Available at: https://linkinghub.elsevier.com/retrieve/pii/S0012369213606261 (Accessed 2023 Jun 4).
8. Han R, Jiang X. Hypokalemia-induced rhabdomyolysis as the first symptom of primary aldosteronism: a case report and literature review. Ann Palliat Med (2022) 11(8):2778–84. doi: 10.21037/apm-21-3010
9. Chen CT, Wang YC, Lin CM. Hypokalemia-induced rhabdomyolysis caused by adrenal tumor-related primary aldosteronism: A report of 2 cases. Am J Case Rep (2021) 22:e929758. doi: 10.12659/AJCR.929758
10. Araujo-Castro M, Parra-Ramí;rez P. Diagnó;stico del hiperaldosteronismo primario(2022). Available at: https://linkinghub.elsevier.com/retrieve/pii/S0025775321006564 (Accessed 2023 Jun 16).
11. Crawhall JC, Tolis G, Roy D. Elevation of serum creatine kinase in severe hypokalemic hyperaldosteronism. Clin Biochem (1976) 9(5):237–40. doi: 10.1016/S0009-9120(76)80067-7
12. Dominic JA, Koch M, Guthrie GP, Galla JH. Primary aldosteronism presenting as myoglobinuric acute renal failure. Arch Intern Med (1978) 138(9):1433–4. doi: 10.1001/archinte.1978.03630340099036
13. Atsumi T, Ishikawa S, Miyatake T, Yoshida M. Myopathy and primary aldosteronism: electronmicroscopic study. Neurology. (1979) 29(10):1348–53. doi: 10.1212/WNL.29.10.1348
14. SChady W, Yuill GM. Myopathy and primary hyperaldosteronism. Neurology. (1981) 31(2):225–6. doi: 10.1212/WNL.31.2.225-b
15. Mahdyoon H, Mermiges DN, Wisgerhof M. Conn’s syndrome with rhabdomyolysis mimicking deep vein thrombophlebitis. South Med J (1990) 83(3):346–7. doi: 10.1097/00007611-199003000-00024
16. Chow CP, Symonds CJ, Zochodne DW. Hyperglycemia, lumbar plexopathy and hypokalemic rhabdomyolysis complicating Conn’s syndrome. Can J Neurol Sci J Can Sci Neurol (1997) 24(1):67–9. doi: 10.1017/S0317167100021132
17. Mourad JJ, Milliez P, Blacher J, Safar M, Girerd X. [Conn adenoma manifesting as reversible tetraparesis and rhabdomyolysis]. Rev Med Interne. (1998) 19(3):203–5. doi: 10.1016/S0248-8663(97)80722-9
18. Ozgür B, Kürsat S. Hypokalemic rhabdomyolysis aggravated by diuretics complicating Conn’s syndrome without acute renal failure. Clin Nephrol. (2002) 57(1):89–91. doi: 10.5414/cnp57089
19. Kaşifoğlu T, Korkmaz C, Paşaoğlu O. Conn’s syndrome (primary hyperaldosteronism) simulating polymyositis. Rheumatol Int (2005) 25(2):133–4. doi: 10.1007/s00296-004-0462-0
20. Gonerska-Szadkowska A, Wittych-Długosz J, Makarewicz J, Szmidt M, Lewiński A. Rhabdomyolysis following severe hypokalemia caused by Conn’s syndrome. Arch Med Sci (2007) 3(3):274–7.
21. Petidis K, Douma S, Aslanidis S, Papaefthimiou P, Kartali N, Zamboulis C. Hypertension associated with rhabdomyolysis. J Clin Hypertens Greenwich Conn. (2007) 9(1):60–2. doi: 10.1111/j.1524-6175.2007.05811.x
22. Chuang TH, Wang CH, Tseng BY, Hsu YH, Tsai JP, Hsu BG, et al. syndrome with an unusual presentation of rhabdomyolysis secondary to severe hypokalemia. Conn’s (2008) (Accessed 2023 May 29).
23. Etgen T, Gräbert C. Tetraparesis with hypertensive crisis: hypokalemic rhabdomyolysis in primary hyperaldosteronism. Nervenarzt. (2009) 80(6):717–9. doi: 10.1007/s00115-009-2676-6
24. Kotsaftis P, Savopoulos C, Agapakis D, Ntaios G, Tzioufa V, Papadopoulos V, et al. Hypokalemia induced myopathy as first manifestation of primary hyperaldosteronism - an elderly patient with unilateral adrenal hyperplasia: a case report. cases J (2009) 2:6813. doi: 10.4076/1757-1626-2-6813
25. Karagüzel G, Bahat E, Imamoğlu M, Ahmetoğlu A, Yildiz K, Okten A. An unusual case of an aldosterone-producing adrenocortical adenoma presenting with rhabdomyolysis. J Pediatr Endocrinol Metab JPEM. (2009) 22(11):1087–90. doi: 10.1515/jpem.2009.22.11.1087
26. Goto A, Takahashi Y, Kishimoto M, Minowada S, Aibe H, Hasuo K, et al. Primary aldosteronism associated with severe rhabdomyolysis due to profound hypokalemia. Intern Med Tokyo Jpn (2009) 48(4):219–23. doi: 10.2169/internalmedicine.48.1444
27. Martí;nez JJA, Oliveira CL, Meneses AL, Rodrí;guez SA, Corrales PP, Ló;pez AH, et al. Rhabdomyolysis due to primary hyperaldosteronism(2009) (Accessed 2023 May 29).
28. Tsai WT, Chen YL, Yang WS, Lin HD, Chien CC, Lin CL. Primary aldosteronism associated with severe hypokalemic rhabdomyolysis. Horm Athens Greece. (2012) 11(4):505–6. doi: 10.14310/horm.2002.1385
29. Finsterer J, Lässer S. Severe hypokalemic paralysis as a manifestation of a mitochondrial disorder. Tohoku J Exp Med (2013) 231(1):9–12. doi: 10.1620/tjem.231.9
30. Cooray MSA, Bulugahapitiya US, Peiris DN. Rhabdomyolysis: A rare presentation of aldosterone-producing adenoma. Indian J Endocrinol Metab (2013) 17(Suppl 1):S237–239. doi: 10.4103/2230-8210.119583
31. Wen Z, Chuanwei L, Chunyu Z, Hui H, Weimin L. Rhabdomyolysis presenting with severe hypokalemia in hypertensive patients: a case series. BMC Res Notes. (2013) 6:155. doi: 10.1186/1756-0500-6-155
32. Yao B, Qin Z, Tan Y, He Y, Yan J, Liang Q, et al. Rhabdomyolysis in primary aldosteronism: A case report and review of the literature(2015) (Accessed 2023 May 29).
33. Eguchi T, Miyauchi S. A case of primary aldosteronism with secondary hyperparathyroidism and bilateral adrenal tumors. Endocrinol Diabetes Metab Case Rep (2015) 2015:15–0029. doi: 10.1530/EDM-15-0029
34. Lee JH, Kim E, Chon S. Hypokalemia-induced rhabdomyolysis by primary aldosteronism coexistent with sporadic inclusion body myositis. Ann Rehabil Med (2015) 39(5):826–32. doi: 10.5535/arm.2015.39.5.826
35. Martí;nez-Ruiz EE, Paz-Manifacio S, Sánchez-Dí;az S, Cruz E. Rhabdomyolysis due to hypokalemia: an atypical manifestation of Conn’s syndrome. Med Interna Mex. (2017) 33:826–34. doi: 10.24245/mim.v33i6.1417
36. Dyrmishi B, Olldashi T, Rista E, Fureraj T, Ylli D, Ylli A. Severe Hypokalemia Induced Rhabdomyolysis By Primary Hyperaldosteronism Coexistent With Recurrent Bilateral Renal Calculi. Acta Endocrinol Buchar Rom 2005. (2017) 13(2):228–31. doi: 10.4183/aeb.2017.228
37. Pecnik P, Müller P, Vrabel S, Windpessl M. Two cases of hypokalaemic rhabdomyolysis: same but different(2018) (Accessed 2023 Apr 10).
38. Wang SC, Chiu KY. Primary hyperaldosteronism manifested by rhabdomyolysis. Open J Clin Med Case Rep (2019) 5(3):1519.
39. Skaletsky K, Kosmacheva E, Kizhvatova N, Porhanov V. Primary aldosteronism complicated by hypokalemic rhabdomyolysis (2019) (Accessed 2023 May 29).
40. Sirkeci O, Sirkeci EE, Kucukciloglu Y. Severe hypokalemia and rhabdomyolysis caused by conn syndrome. Clin Ter. (2021) 172(5):407–9. doi: 10.32322/jhsm.844053
41. Maung AC, Kerwen AK, Ching LP. Hypokalaemic rhabdomyolysis as initial presentation of primary aldosteronism. J R Coll Physicians Edinb. (2021) 51(2):149–52. doi: 10.4997/jrcpe.2021.211
42. Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med (2009) 361(1):62–72. doi: 10.1056/NEJMra0801327
43. Burrello J, Amongero M, Buffolo F, Sconfienza E, Forestiero V, Burrello A, et al. Development of a prediction score to avoid confirmatory testing in patients with suspected primary aldosteronism. J Clin Endocrinol Metab (2021) 106(4):e1708–16. doi: 10.1210/clinem/dgaa974
44. Maung AC, Kerwen AK, Ching LP. Hypokalaemic rhabdomyolysis as initial presentation of primary aldosteronism (Accessed 2023 Apr 10).
45. Scharman EJ, Troutman WG. Prevention of kidney injury following rhabdomyolysis: a systematic review. Ann Pharmacother. (2013) 47(1):90–105. doi: 10.1345/aph.1R215
Keywords: rhabdomyolysis, hypokalaemia, hypokalaemic rhabdomyolysis, primary aldosteronism, acute kidney injury
Citation: Díaz-López EJ, Villar-Taibo R, Rodriguez-Carnero G, Fernandez-Pombo A, Garcia-Peino R, Blanco-Freire MN, Pena-Dubra A, Prado-Moraña T, Fernández-Xove I, Pérez-Béliz E, Cameselle-Teijeiro JM, Hermida-Ameijeiras A and Martinez-Olmos MA (2023) Should we suspect primary aldosteronism in patients with hypokalaemic rhabdomyolysis? A systematic review. Front. Endocrinol. 14:1257078. doi: 10.3389/fendo.2023.1257078
Received: 11 July 2023; Accepted: 28 August 2023;
Published: 22 September 2023.
Edited by:
Piotr Glinicki, Centre of Postgraduate Medical Education, PolandReviewed by:
Takao Ando, Nagasaki University Hospital, JapanLakshmi Kannan, University of Pikeville Kentucky College of Osteopathic Medicine, United States
Copyright © 2023 Díaz-López, Villar-Taibo, Rodriguez-Carnero, Fernandez-Pombo, Garcia-Peino, Blanco-Freire, Pena-Dubra, Prado-Moraña, Fernández-Xove, Pérez-Béliz, Cameselle-Teijeiro, Hermida-Ameijeiras and Martinez-Olmos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Everardo Josué Díaz-López, ZXZlcmFyZG9kaWF6MkBnbWFpbC5jb20=; Rocio Villar-Taibo, cm90YWlibzIyQGdtYWlsLmNvbQ==