 Zaina Adnan
Zaina Adnan Edmond Sabo2
Edmond Sabo2- 1Department of Endocrinology and Metabolism, Clalit Medical Health Care Services, Haifa and Western Galilee District, Bar-Ilan Faculty of Medicine, Safed, Israel
- 2The Institute of Pathology, Carmel Medical Center, Ruth and Bruce Rappaport Faculty of Medicine, Technion-Institute of Technology, Haifa, Israel
- 3Department of Internal Medicine, Carmel Medical Center, Ruth and Bruce Rappaport Faculty of Medicine, Technion-Institute of Technology, Haifa, Israel
Papillary thyroid carcinoma (PTC) is the most common malignancy of the thyroid gland, typically associated with an indolent course and favourable prognosis. However, although rare, PTC can demonstrate aggressive behaviour, including vascular invasion with extension into major vessels. Intraluminal tumor thrombus involving the great veins, such as the internal jugular vein (IJV), is an uncommon but significant complication. We present the case of a 56-year-old male who was referred to our clinic for evaluation of a right-sided anterior neck mass. Neck ultrasonography revealed a 5.5 x 6.5 cm heterogeneous mass within the right thyroid lobe and a suspected intraluminal thrombus in the right internal jugular vein. Fine-needle aspiration biopsy under ultrasound guidance confirmed the diagnosis of papillary thyroid carcinoma. Subsequent preoperative contrast-enhanced computed tomography (CT) of the neck confirmed the presence of an intraluminal tumours thrombus extending into the right IJV. The patient underwent total thyroidectomy, right modified radical neck dissection, and resection of the involved segment of the IJV. Postoperatively, the patient received radioactive iodine (I-131) ablation therapy. At the one-year follow-up, imaging studies indicated a recurrence of the disease. A review of the literature focusing on vascular involvement in PTC and diagnostic methods for tumours thrombus reveals that, while rare, intraluminal tumor thrombus should be considered in patients with PTC, especially when there is evidence of vascular invasion. Early and accurate preoperative diagnosis using Doppler ultrasonography and/or contrast-enhanced CT is critical for optimal surgical planning and improved prognosis. Given the potential for recurrence, vigilant long-term follow-up is recommended.
Introduction
Papillary thyroid carcinoma (PTC)is common and accounts for approximately 80% of all thyroid malignancies (1). It is well known that some thyroid carcinoma may behave aggressively and tend to cause local invasion, recurrence, and distant metastasis (2). However, microscopic vascular invasion is common in all types of thyroid carcinoma (3). PTC rarely causes extension and growth that may involve the great veins, particularly the internal jugular vein, resulting in intraluminal tumor thrombus (4). In the current article, we present a rare case of metastatic PTC with intraluminal tumor thrombus in the internal jugular vein. We reviewed published data focusing mainly on vascular sites involved with tumor thrombus, diagnosis modalities, and the time of diagnosis preoperative vs. postoperative.
Case presentation
A 56-year-old male was referred to our outpatient endocrinology department in July 2023 with a three-month history of progressive enlargement of a right-sided anterior neck mass. His past medical and family history were unremarkable. Physical examination revealed a firm, non-tender 5 x 5 cm mass within an enlarged right thyroid lobe without palpable lymphadenopathy. Neck ultrasonography identified a 5.5 x 6.5 cm heterogeneous mass in the lateral aspect of the right thyroid lobe, along with a suspected thrombus in the internal jugular vein (IJV). Fine-needle aspiration (FNA) guided by ultrasonography confirmed a diagnosis of papillary thyroid carcinoma (PTC). Preoperative enhanced contrast computed tomography (CT) of the neck and chest demonstrated a heterogeneous 5.5 x 6.5 cm right thyroid mass with hypodense areas and poorly defined margins at the base of the right neck, showing lateral extension. The right internal jugular vein (RIJ) was enlarged and heterogeneous, with an extensive filling defect consistent with an intraluminal tumor thrombus. Additionally, an 8 mm lymph node in the right upper lobe of the lung was noted, raising suspicion for metastasis, though there was no evidence of pericardial or pleural effusion (Figure 1).
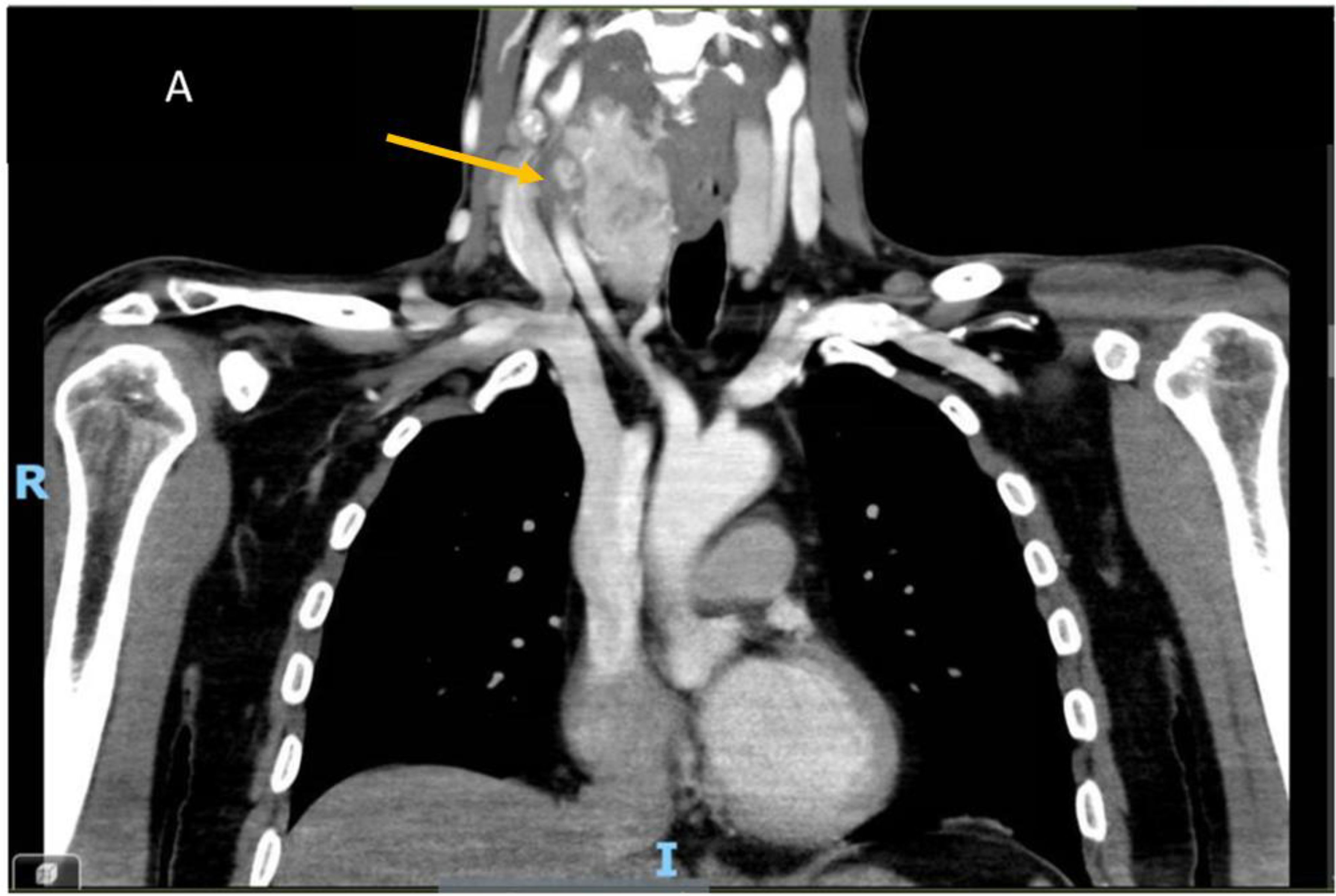
Figure 1. Contrast-enhanced computed tomography (CT) images of the neck and chest reveal a large nodule with areas of cystic degeneration within the right lobe of the thyroid gland. The yellow arrow indicates a tumor thrombus obstructing the right internal jugular vein (IJV).
After an extensive preoperative evaluation, including multidisciplinary consultation with a vascular surgeon team, in October 2023, the patient underwent a total thyroidectomy, right modified lymph node dissection, and resection of the internal jugular vein (IJV). Histopathological examination revealed a multifocal papillary thyroid carcinoma (PTC) measuring up to 7 cm, predominantly displaying a follicular growth pattern. There were cribriform and solid growth areas, with foci consistent with poorly differentiated carcinoma, constituting approximately 10-15% of the tumor volume. Evidence of vascular invasion was observed, including a large vein identified as the IJV containing a tumor thrombus. Invasion of the striated muscle was also noted. Metastatic carcinoma was detected in 3 of 26 lymph nodes, with the largest metastatic focus measuring 4 mm. The left thyroid lobe contained two foci of papillary thyroid microcarcinoma, each up to 5 mm, without extrathyroidal extension or vascular invasion. The IJV showed a tumor thrombus with fragments of PTC (Figure 2).
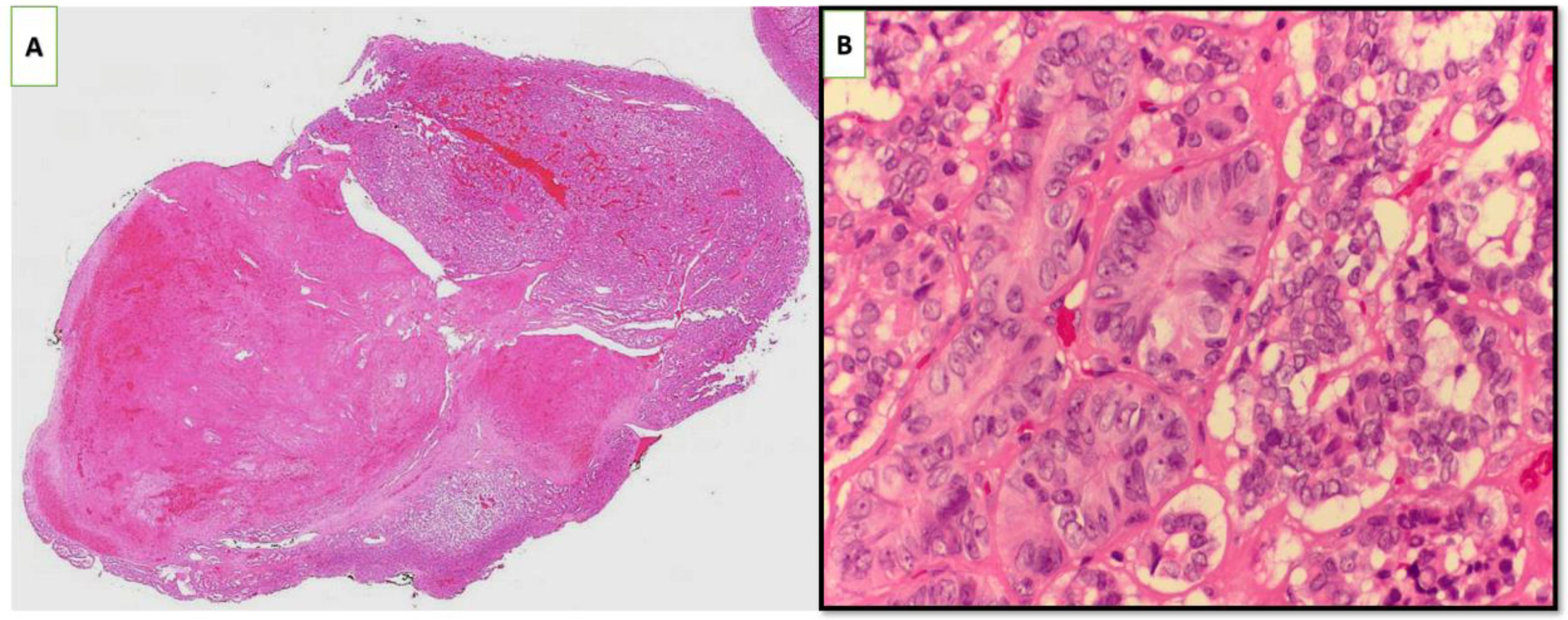
Figure 2. Histopathological examination revealed papillary thyroid carcinoma with a predominantly follicular growth pattern, along with areas consistent with poorly differentiated carcinoma. Vascular invasion was observed in a large vessel identified as the internal jugular vein, which contained a tumor thrombus (H&E staining; (A) ×10 magnification, (B) ×60 magnification).
In February 2024, the patient underwent radioiodine ablation therapy with a dose of 150 mCi and was prescribed levothyroxine at 200 mcg daily. Laboratory results showed suppressed thyroid-stimulating hormone (TSH) levels and undetectable thyroglobulin (Tg) levels with normal thyroglobulin antibodies (TgAbs).
At the one-year follow-up in July 2024, a neck ultrasound revealed a suspicious right lymph node measuring 11 x 6.5 x 5 mm at level 3. Positron emission tomography/computed tomography (PET/CT) demonstrated pathological FDG uptake in a 10 mm lymph node in the right mid-neck, along with pulmonary nodules suggestive of lung metastasis. Fine-needle aspiration (FNA) indicated the lymph node was suspicious for metastatic PTC. In August 2024, the patient underwent resection of the lymph node and a left modified neck dissection. The histological findings revealed a 1.3 cm lymph node at level 3 on the right side, which was almost totally replaced by papillary metastatic carcinoma of a poorly differentiated variant. Focally extranodal tumor extension less than 1 mm was also seen. Examination of the excised lymph node at level 3 on the left neck disclosed fragments of lymph node tissue and surrounding fibro-fatty tissues infiltrated by metastatic poorly differentiated thyroid carcinoma variant. The other 13 dissected lymph nodes at this level were free of tumor involvement. At level 2, nine lymph nodes were dissected and found to be free of tumor. At level 4, one lymph node measuring 3 mm out of eight lymph nodes revealed metastatic thyroid carcinoma. no extranodal extension was observed. Postoperatively, a detectable Tg of 9.4 mcg/L with normal TgAbs was observed. Therefore, the patient was referred to the oncology department for further evaluation, ongoing follow-up, and treatment.
Discussion
Tumour thrombosis of large vessels is commonly observed in angio-invasive malignancies, such as hepatocellular carcinoma and renal cell carcinoma, which frequently involve the portal vein, hepatic veins, renal veins, and the inferior vena cava (5, 6). In contrast, papillary thyroid carcinoma (PTC) typically spreads via the lymphatic system, with hematogenous dissemination leading to distant metastasis being rare (1). Microinvasion of cervical veins has been well documented in thyroid follicular and Hürthle cell carcinomas (2).
In this case report, we demonstrated the presence of an internal jugular vein (IJV) thrombus preoperatively. Reviewing the literature, we identified 50 cases of thyroid carcinoma associated with vascular tumor thrombus (Table 1). Among these patients, 34 were female, with a mean age of 56.8 years (range: 26–84 years). Most reports consist of case reports (34 cases) and case series (16 cases). Caudal extension of the thrombus was frequently observed, involving the brachiocephalic veins, superior vena cava, and, in some cases, propagation to the right atrium and tricuspid valve (7–44).
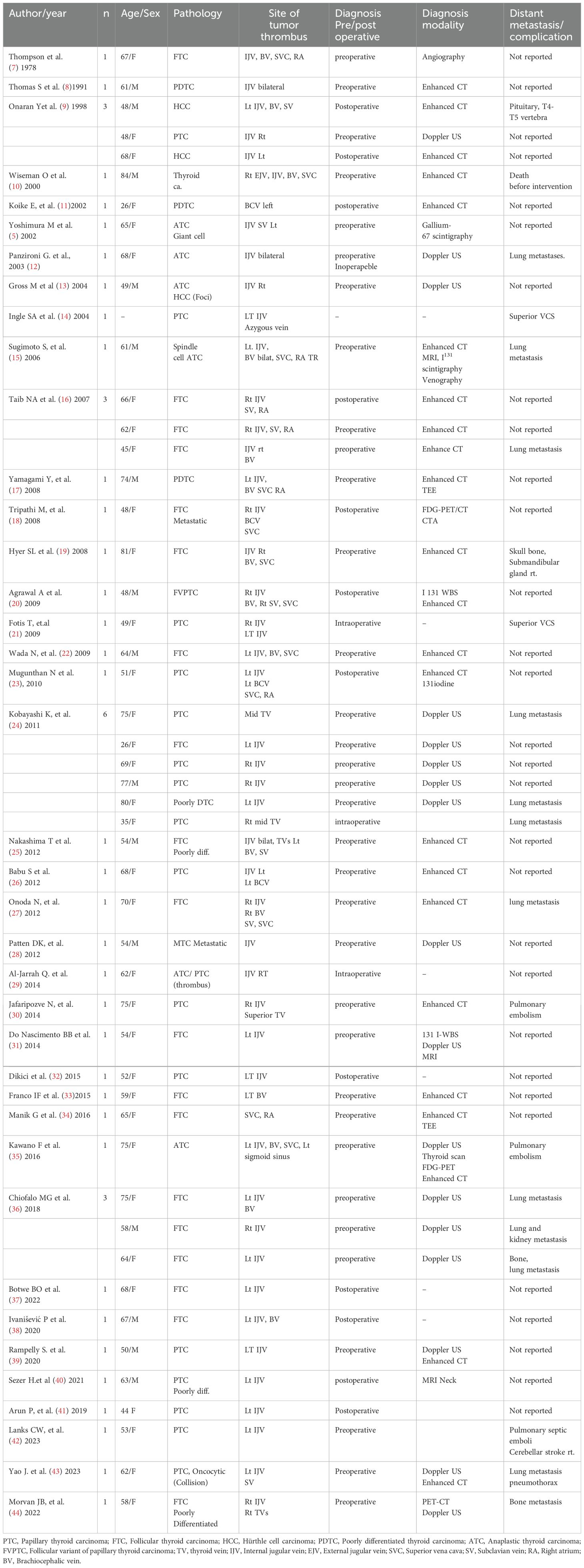
Table 1. Characteristics of patients with thyroid carcinoma and vascular tumor thrombus.
In contrast, proximal extension was rare, with only one case reporting involvement of the sigmoid sinus. Additionally, distant metastases to uncommon sites, including the vertebrae, pituitary gland, and skull bones, were reported (Table 1). Complications such as superior vena cava syndrome, pulmonary embolism, metastasis to different sites, and mortality were extensively reported in our manuscript.
Diagnosing vascular tumor thrombus can be clinically challenging and is highly dependent on the location and extent of the thrombus. However, dilated neck veins, upper limb edema, or extensive involvement of large vessels such as the jugular vein, subclavian vein, and superior vena cava should raise suspicion of tumor thrombus in this patient population. As highlighted in our case, preoperative imaging modalities, including Doppler ultrasonography (US) and contrast-enhanced computed tomography (CT), are essential for accurate diagnosis and surgical planning. Doppler US and contrast-enhanced CT were the most commonly used techniques to detect vascular tumor thrombus in the reviewed cases (Table 1). Contrast-enhanced CT is generally preferred due to its reliability, whereas the US is more operator-dependent, potentially limiting its accuracy.
Conclusions
Tumor thrombus is rare among patients with PTC. However, this entity should be considered, particularly in patients with signs of vascular involvement. Preoperative diagnosis using Doppler US and/or enhanced contrast CT is mandatory for a favorable outcome.
Author contributions
ZA: Conceptualization, Writing – original draft, Writing – review & editing. ES: Writing – original draft, Writing – review & editing. SK: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Prete A, Borges de Souza P, Censi S, Muzza M, Nucci N, Sponziello M. Update on fundamental mechanisms of thyroid cancer. Front Endocrinol (Lausanne). (2020) 11:102. doi: 10.3389/fendo.2020.00102
2. Baloch ZW, Asa SL, Barletta JA, Ghossein RA, Juhlin CC, Jung CK, et al. Overview of the 2022 WHO classification of thyroid neoplasms. Endocr Pathol. (2022) 33:27–63. doi: 10.1007/s12022-022-09707-3
3. Fonseca L, Borges Duarte D, Brandão JR, Alves Pereira C, Amado A, Gouveia P, et al. Papillary thyroid carcinoma: the impact of histologic vascular invasion. Minerva Endocrinol (Torino). (2024) 49:69–75. doi: 10.23736/S2724-6507.22.03749-6
4. Gui Y, Wang JY, Wei XD. Middle thyroid vein tumor thrombus in metastatic papillary thyroid microcarcinoma: A case report and review of literature. World J Clin Cases. (2022) 10:3213–21. doi: 10.12998/wjcc.v10.i10.3213
5. Yoshimura M, Kawamoto A, Nakasone K, Kakizaki D, Tsutsui H, Serizawa H, et al. Gallium-67 accumulation to the tumor thrombus in anaplastic thyroid cancer. Ann Nucl Med. (2003) 17:689–91. doi: 10.1007/BF02984976
6. Khan AR, Wei X, Xu XJ. Portal vein tumor thrombosis and hepatocellular carcinoma - the changing tides. Hepatocell Carcinoma. (2021) 8:1089–115. doi: 10.2147/JHC.S318070
7. Thompson NW, Brown J, Orringer M, Sisson J, Nishiyama R. Follicular carcinoma of the thyroid with massive angioinvasion: extension of tumor thrombus to the heart. Surgery. (1978) 83:451–7.
8. Thomas S, Sawhney S, Kapur BM. Case report: bilateral massive internal jugular vein thrombosis in carcinoma of the thyroid: CT evaluation. Clin Radiol. (1991) 43:433–4. doi: 10.1016/s0009-9260(05)80580-x
9. Onaran Y, Terzioğlu T, Oğuz H, Kapran Y, Tezelman S. Great cervical vein invasion of thyroid carcinoma. Thyroid. (1998) 8:59–61. doi: 10.1089/thy.1998.8.59
10. Wiseman O, Preston PG, Clarke JM. Presentation of thyroid carcinoma as a thrombosed external jugular vein, with intraluminal tumour thrombus in the great veins. Eur J Surg Oncol. (2000) 26:816–7. doi: 10.1053/ejso.2000.1011
11. Koike E, Yamashita H, Watanabe S, Yamashita H, Noguchi S. Brachiocephalic vein thrombus of papillary thyroid cancer: report of a case. Surg Today. (2002) 32:59–62. doi: 10.1007/s595-002-8114-7
12. Panzironi G, Rainaldi R, Ricci F, Casale A, De Vargas Macciucca M. Gray-scale and color Doppler findings in bilateral internal jugular vein thrombosis caused by anaplastic carcinoma of the thyroid. J Clin Ultrasound. (2003) 31:111–5. doi: 10.1002/jcu.0132
13. Gross M, Mintz Y, Maly B, Pinchas R, Muggia-Sullam M. Internal jugular vein tumor thrombus associated with thyroid carcinoma. Ann Otol Rhinol Laryngol. (2004) 113:738–40. doi: 10.1177/000348940411300912
14. Ingle SA, Karnik ND, Pradhan NN, Ranadive NU, Dhurde A, Kotalwar M. Papillary carcinoma of thyroid presenting as posterior mediastinal mass with superior vena cava syndrome. J Assoc Physicians India. (2004) 52:1004–5.
15. Sugimoto S, Doihara H, Ogasawara Y, Aoe M, Sano S, Shimizu N. Intraatrial extension of thyroid cancer: a case report. Acta Med Okayama. (2006) 60:135–40. doi: 10.18926/AMO/30734
16. Taib NA, Hisham AN. Follicular thyroid carcinoma with direct tumour extension into the great cervical veins and right atrium: is transcervical thrombectomy a safe option? Asian J Surg. (2007) 30:216–9. doi: 10.1016/s1015-9584(08)60025-1
17. Yamagami Y, Tori M, Sakaki M, Ohtake S, Nakahara M, Nakao K. Thyroid carcinoma with extensive tumor thrombus in the atrium. Gen Thorac Cardiovasc Surg. (2008) 56:555–8. doi: 10.1007/s11748-008-0307-y
18. Tripathi M, Sharma R, Jaimini A, Singh N, Saw SK, Mishra AK, et al. Metastatic follicular carcinoma of the thyroid with tumor thrombus in the superior vena cava and right brachiocephalic and internal jugular veins: FDG-PET/CT findings. Clin Nucl Med. (2008) 33:426–8. doi: 10.1097/RLU.0b013e318170d508
19. Hyer SL, Dandekar P, Newbold K, Haq M, Wechalakar K, Thway K, et al. Thyroid cancer causing obstruction of the great veins in the neck. World J Surg Oncol. (2008) 6:36. doi: 10.1186/1477-7819-6-36
20. Agrawal A, Agrawal R, Asopa R. Detection of metastases to internal jugular vein and superior vena cava on 131-I scan. Clin Nucl Med. (2009) 34:934–5. doi: 10.1097/RLU.0b013e3181bed1aa
21. Fotis T, Konstantinou E, Mariolis-Sapsakos T, Mitsos A, Restos S, Katsenis K, et al. Solitary internal jugular vein invasion by thyroid carcinoma: resection and reconstruction. J Vasc Nurs. (2009) 27:46–7. doi: 10.1016/j.jvn.2009.02.001
22. Wada N, Masudo K, Hirakawa S, Woo T, Arai H, Suganuma N, et al. Superior vena cava (SVC) reconstruction using autologous tissue in two cases of differentiated thyroid carcinoma presenting with SVC syndrome. World J Surg Oncol. (2009) 7:75. doi: 10.1186/1477-7819-7-75
23. Mugunthan N, Kumar AR, Thomas P. Tumor thrombus in the great veins from papillary carcinoma of the thyroid: 131I scan findings. J Clin Endocrinol Metab. (2010) 95:2527–8. doi: 10.1210/jc.2009-2031
24. Kobayashi K, Hirokawa M, Yabuta T, Fukushima M, Kihara M, Higashiyama T, et al. Tumor thrombus of thyroid Malignancies in veins: importance of detection by ultrasonography. Thyroid. (2011) 21:527–31. doi: 10.1089/thy.2010.0099
25. Nakashima T, Nakashima A, Murakami D, Toh S, Shiratsuchi H, Yasumatsu R, et al. Follicular carcinoma of the thyroid with massive invasion into the cervical and mediastinum great veins: our own experience and literature review. Laryngoscope. (2012) 122:2855–7. doi: 10.1002/lary.23690
26. Babu S, Salih S, Kumar V, Satheeshan B. Intravenous tumour thrombus from papillary carcinoma of thyroid- a case report & review of literature. Indian J Surg Oncol. (2012) 3:206–7. doi: 10.1007/s13193-012-0126-6
27. Onoda N, Nakamura M, Hosono M, Sasaki Y, Kawajiri H, Takashima T, et al. Successful surgical treatment of advanced follicular thyroid carcinoma with tumor thrombus infiltrating the superior vena cava: report of a case. Surg Today. (2012) 42:185–90. doi: 10.1007/s00595-011-0033-4
28. Patten DK, Flora R, Tolley N, Palazzo F. Sporadic medullary thyroid carcinoma with a pedunculated intraluminal internal jugular vein recurrence: A case report and literature review. Int J Surg Case Rep. (2012) 3:92–6. doi: 10.1016/j.ijscr.2011.11.005
29. Al-Jarrah Q, Abou-Foul A, Heis H. Intravascular extension of papillary thyroid carcinoma to the internal jugular vein: A case report. Int J Surg Case Rep. (2014) 5:551–3. doi: 10.1016/j.ijscr.2014.06.005
30. Ataiekhorasgani M, Jafaripozve N. Acute pulmonary emboli due to internal jugular vein thrombosis in papillary thyroid carcinoma, a case report and literature review. Adv BioMed Res. (2014) 3:27. doi: 10.4103/2277-9175.124676
31. do Nascimento BB, de Sá Camargo Etchebehere EC, Montalli Assumpção LV, Tincani AJ, de Oliveira Santos A, Baracat J, et al. Follicular thyroid carcinoma metastasis to the internal jugular vein demonstrated by 131I SPECT/CT. Clin Nucl Med. (2014) 39:e270–3. doi: 10.1097/RLU.0b013e3182952959
32. Dikici AS, Yıldırım O, Er ME, Kılıç F, Tutar O, Kantarcı F, et al. A rare complication of the thyroid Malignancies: jugular vein invasion. Pol J Radiol. (2015) 80:360–3. doi: 10.12659/PJR.894057
33. Franco IF, Gurrado A, Lissidini G, Di Meo G, Pasculli A, Testini M. Floating left innominate vein neoplastic thrombus: a rare case of mediastinal extension of follicular thyroid carcinoma. Phlebology. (2015) 30:140–4. doi: 10.1177/0268355513515209
34. Manik G, Jose J, Hygriv Rao B. Follicular thyroid carcinoma with tumour thrombus extending into superior vena cava and right atrium - A case report. Indian Heart J. (2016) 68:S146–7. doi: 10.1016/j.ihj.2016.05.016
35. Kawano F, Tomita M, Tanaka H, Nagahama H, Tashiro K, Nakao H, et al. Thyroid carcinoma with extensive tumor thrombus in the superior vena cava: A case report. Int J Surg Case Rep. (2016) 29:25–9. doi: 10.1016/j.ijscr.2016.10.037
36. Chiofalo MG, D'Anna R, Di Gennaro F, Setola SV, Marotta V. Great veins invasion in follicular thyroid cancer: single-centre study assessing prevalence and clinical outcome. Endocrine. (2018) 62:71–5. doi: 10.1007/s12020-018-1622-4
37. Mayeden RN, Dzefi-Tettey K, Botwe BO. Follicular thyroid carcinoma with internal jugular vein tumour thrombus. Ghana Med J. (2022) 56:42–5. doi: 10.4314/gmj.v56i1.7
38. Čolović Z, Ivanišević P, Bulat C, Barić A, Kontić M, Punda H, et al. Treatment approach to follicular thyroid carcinoma tumor thrombus in the internal jugular vein and brachiocephalic vein. Acta Clin Croat. (2020) 59:149–52. doi: 10.20471/acc.2020.59.s1.20
39. Rampelly S, Goel V, Pawar S. Internal jugular vein and sternocleidomastoid muscle invasion by papillary carcinoma thyroid. Indian J Otolaryngol Head Neck Surg. (2022) 74:1917–19. doi: 10.1007/s12070-020-01901-1
40. Sezer H, Yazıcı D, Tezelman S, Demirkol MO, Ünal ÖF, Dilege Ş, et al. Concomittant occurence of well-differentiated thyroid carcinoma metastasis and chronic lymphocytic leukemia in the same lymph node along with internal jugular vein thrombus: a case report. Indian J Pathol Microbiol. (2021) 64:149–51. doi: 10.4103/IJPM.IJPM_537_20
41. Jain PV, Sharan R, Manikantan K, Biswas G, Ray S, Arun P. Unusual loco-regional presentation in papillary carcinoma of thyroid: A case series. Indian J Cancer. (2019) 56:325–29. doi: 10.4103/ijc.IJC_368_18
42. Im DCS, Sridhar V, Lanks CW. Lemierre's syndrome associated with papillary thyroid cancer and cerebellar stroke. cureus. (2023) 15:e38889. doi: 10.7759/cureus.38889
43. Liu F, Han F, Lu L, Chang J, Bian Z, Yao J. Thyroid collision tumour with pulmonary metastases treated effectively with nedaplatin and paclitaxel chemotherapy: A case report. J Int Med Res. (2023) 51:3000605231208602. doi: 10.1177/03000605231208602
Keywords: case report, papillary thyroid carcinoma, tumor thrombus, distant metastasis, jugular vein, enhanced CT
Citation: Adnan Z, Sabo E and Kassem S (2025) Metastatic papillary thyroid carcinoma with internal jugular vein tumor thrombus - A case report and review of the literature. Front. Endocrinol. 16:1505800. doi: 10.3389/fendo.2025.1505800
Received: 03 October 2024; Accepted: 07 January 2025;
Published: 29 January 2025.
Edited by:
Alessio G. Morganti, University of Bologna, ItalyReviewed by:
Kyriakos Vamvakidis, Henry Dunant Hospital, GreeceCopyright © 2025 Adnan, Sabo and Kassem. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zaina Adnan, emFpbmFfYWRuYW5AeWFob28uY29t
†ORCID: Zaina Adnan, orcid.org/0000-0001-7482-3104