 Alessandro Busca1†‡
Alessandro Busca1†‡ Jon Salmanton-García2,3*†‡
Jon Salmanton-García2,3*†‡ Francesco Marchesi4‡
Francesco Marchesi4‡ Francesca Farina5‡
Francesca Farina5‡ Guldane Cengiz Seval6‡
Guldane Cengiz Seval6‡ Jaap Van Doesum7‡
Jaap Van Doesum7‡ Nick De Jonge8‡
Nick De Jonge8‡ Nathan C. Bahr9‡
Nathan C. Bahr9‡ Johan Maertens10,11‡
Johan Maertens10,11‡ Joseph Meletiadis12‡
Joseph Meletiadis12‡ Nicola S. Fracchiolla13‡Barbora Weinbergerová14‡Luisa Verga15,16‡Zdeněk Ráčil17‡Moraima Jiménez18,19‡
Nicola S. Fracchiolla13‡Barbora Weinbergerová14‡Luisa Verga15,16‡Zdeněk Ráčil17‡Moraima Jiménez18,19‡ Andreas Glenthøj20‡Ola Blennow21‡
Andreas Glenthøj20‡Ola Blennow21‡ Alina Daniela Tanase22
Alina Daniela Tanase22 Martin Schönlein23‡Lucia Prezioso24‡
Martin Schönlein23‡Lucia Prezioso24‡ Nina Khanna25‡
Nina Khanna25‡ Rafael F. Duarte26Pavel Žák27‡Marcio Nucci28‡Marina Machado29‡
Rafael F. Duarte26Pavel Žák27‡Marcio Nucci28‡Marina Machado29‡ Austin Kulasekararaj30,31‡Ildefonso Espigado32‡Elizabeth De Kort33
Austin Kulasekararaj30,31‡Ildefonso Espigado32‡Elizabeth De Kort33 José-María Ribera-Santa Susana34‡Monia Marchetti35‡
José-María Ribera-Santa Susana34‡Monia Marchetti35‡ Gabriele Magliano36‡
Gabriele Magliano36‡ Iker Falces-Romero37‡Osman Ilhan6‡
Iker Falces-Romero37‡Osman Ilhan6‡ Emanuele Ammatuna7‡Sofia Zompi1‡
Emanuele Ammatuna7‡Sofia Zompi1‡ Panagiotis Tsirigotis12‡
Panagiotis Tsirigotis12‡ Anastasia Antoniadou12‡
Anastasia Antoniadou12‡ Giovanni Paolo Maria Zambrotta15,16‡Anna Nordlander21Linda Katharina Karlsson20‡Michaela Hanakova17Giulia Dragonetti38‡
Giovanni Paolo Maria Zambrotta15,16‡Anna Nordlander21Linda Katharina Karlsson20‡Michaela Hanakova17Giulia Dragonetti38‡ Alba Cabirta18‡Caroline Berg Venemyr20‡Stefanie Gräfe2,3‡
Alba Cabirta18‡Caroline Berg Venemyr20‡Stefanie Gräfe2,3‡ Jens Van Praet39‡
Jens Van Praet39‡ Athanasios Tragiannidis40
Athanasios Tragiannidis40 Verena Petzer41‡
Verena Petzer41‡ Alberto López-García42‡Federico Itri43‡Ana Groh44
Alberto López-García42‡Federico Itri43‡Ana Groh44 Eleni Gavriilaki45Michelina Dargenio46‡
Eleni Gavriilaki45Michelina Dargenio46‡ Laman Rahimli2,3‡
Laman Rahimli2,3‡ Oliver A. Cornely2,3,47,48,49‡
Oliver A. Cornely2,3,47,48,49‡ Livio Pagano50‡ and EPICOVIDEHA Consortium
Livio Pagano50‡ and EPICOVIDEHA Consortium- 1Stem Cell Transplant Center, AOU Citta’ della Salute e della Scienza, Turin, Italy
- 2University of Cologne, Faculty of Medicine and University Hospital Cologne, Translational Research, Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), Cologne, Germany
- 3University of Cologne, Faculty of Medicine and University Hospital Cologne, Department I of Internal Medicine, Center for Integrated Oncology Aachen Bonn Cologne Duesseldorf (CIO ABCD) and Excellence Center for Medical Mycology (ECMM), Cologne, Germany
- 4Hematology and Stem Cell Transplant Unit, IRCCS Regina Elena National Cancer Institute, Rome, Italy
- 5IRCCS Ospedale San Raffaele, Milan, Italy
- 6Ankara University, Ankara, Türkiye
- 7University Medical Center Groningen, Groningen, Netherlands
- 8Amsterdam UMC, Amsterdam, Netherlands
- 9University of Kansas Medical Center, Kansas, KS, United States
- 10Department of Microbiology, Immunology, and Transplantation, KULeuven, Leuven, Belgium
- 11Department of Hematology, UZ Leuven, Leuven, Belgium
- 12Clinical Microbiology Laboratory, Medical School, “Attikon” University General Hospital, National and Kapodistrian University of Athens, Athens, Greece
- 13Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy
- 14Department of Internal Medicine - Hematology and Oncology, Masaryk University Hospital Brno, Brno, Czechia
- 15Azienda Ospedaliera San Gerardo - Monza, Monza, Italy
- 16Università Milano-Bicocca, Milan, Italy
- 17Institute of Hematology and Blood Transfusion, Prague, Czechia
- 18Department of Hematology, Vall d’Hebron Hospital Universitari, Experimental Hematology, Vall d’Hebron Institute of Oncology (VHIO), Vall d’Hebron Barcelona Hospital, Barcelona, Spain
- 19Departament de Medicina, Universitat Autònoma de Barcelona, Barcelona, Spain
- 20Department of Hematology, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark
- 21Department of Infectious Diseases, Karolinska University Hospital, Stockholm, Sweden
- 22Fundeni Clinical Institute, University of Medicine and Pharmacy Carol Davila, Bucharest, Romania
- 23Department of Oncology, Hematology and Bone Marrow Transplantation with Section of Pneumology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 24Hospital University of Parma - Hematology and Bone Marrow Unit, Parma, Italy
- 25Division of Infectious Diseases and Hospital Epidemiology, and Department of Clinical Research, University and University Hospital of Basel, Basel, Switzerland
- 26Hospital Universitario Puerta de Hierro, Majadahonda, Spain
- 27University Hospital Hradec Králové, Hradec Králové, Czechia
- 28Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
- 29Clinical Microbiology and Infectious Diseases Department, Hospital General Universitario Gregorio Marañón, Madrid, Spain
- 30King’s College Hospital, London, United Kingdom
- 31King’s College London, London, United Kingdom
- 32Department of Hematology, University Hospital Virgen Macarena - University Hospital Virgen del Rocío, Instituto de Biomedicina de Sevilla (IBIS/CSIC), Universidad de Sevilla (Departamento de Medicina), Seville, Spain
- 33Radboudumc, Nijmegen, Netherlands
- 34Clinical Hematology Department, ICO-Hospital germans Trias i Pujol, Josep Carreras Research Institute, Badalona, Spain
- 35Azienda Ospedaliera Nazionale SS. Antonio e Biagio e Cesare Arrigo, Alessandria, Italy
- 36ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy
- 37La Paz University Hospital, Madrid, Spain
- 38Hematology Unit, Fondazione Policlinico Universitario Agostino Gemelli - IRCCS, Rome, Italy
- 39Department of Nephrology and Infectious diseases, AZ Sint-Jan Brugge-Oostende AV, Brugge, Belgium
- 40Aristotle University of Thessaloniki, Thessaloniki, Greece
- 41Department of Hematology and Oncology, Medical University of Innsbruck, Innsbruck, Austria
- 42Fundacion Jimenez Diaz University Hospital, Health Research Institute IIS-FJD, Madrid, Spain
- 43San Luigi Gonzaga Hospital - Orbassano, Orbassano, Italy
- 44Infektiologie, Universitätsklinikum Frankfurt am Main, Frankfurt am Main, Germany
- 45General Hospital of Thessaloniki “George Papanikolaou”, Thessaloniki, Greece
- 46Hematology and Stem Cell Transplant Unit, Vito Fazzi, Lecce
- 47University of Cologne, Faculty of Medicine and University Hospital Cologne, Clinical Trials Centre Cologne (ZKS Köln), Cologne, Germany
- 48University of Cologne, Faculty of Medicine and University Hospital Cologne, Center for Molecular Medicine Cologne (CMMC), Cologne, Germany
- 49German Centre for Infection Research (DZIF) , Cologne, Germany
- 50Hematology Unit, Università Cattolica del Sacro Cuore, Rome, Italy
Background: The outcome of COVID-19 in allogeneic hematopoietic stem cell transplantation (HSCT) recipients is almost uniformely considered poor. The aim of present study was to retrospectively analyse the outcome and risk factors for mortality in a large series of patients who developed COVID-19 infection after an allogeneic HSCT.
Methods: This multicenter retrospective study promoted by the European Hematology Association – Infections in Hematology Study Working Group, included 326 adult HSCT patients who had COVID-19 between January 2020 and March 2022.
Results: The median time from HSCT to the diagnosis of COVID-19 was 268 days (IQR 86-713; range 0-185 days). COVID-19 severity was mild in 21% of the patients, severe in 39% and critical in 16% of the patients. In multivariable analysis factors associated with a higher risk of mortality were, age above 50 years, presence of 3 or more comorbidities, active hematologic disease at time of COVID-19 infection, development of COVID-19 within 12 months of HSCT, and severe/critical infections. Overall mortality rate was 21% (n=68): COVID-19 was the main or secondary cause of death in 16% of the patients (n=53).
Conclusions: Mortality in HSCT recipients who develop COVID-19 is high and largely dependent on age, comorbidities, active hematologic disease, timing from transplant and severity of the infection.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was recognized in late 2019 and developed into a pandemic with life-threatening disease documented in high-risk groups (1). Allogeneic hematopoietic stem cell transplantation (HSCT) has been increasingly adopted as a curative treatment option for a great variety of hematologic malignancies, however HSCT recipients are vulnerable to viral infections due to neutropenia, immunosuppressive treatments, graft-versus-host disease (GVHD) and incomplete immune reconstitution occurring in the post-transplant period. In this respect, efforts have been made not to postpone transplantation during the pandemic (2). To date, scattered case series of HSCT recipients with coronavirus disease 2019 (COVID-19) have been reported (3–11). Overall, the prognosis of HSCT recipients has been uniformly reported dismal with COVID-19-related mortality ranging between 20 and 39% (5, 6, 12–16), much higher than in the general population. Advanced age, presence of active GVHD and a short time interval from HSCT to COVID-19 were identified as predictors of adverse outcome (3, 5, 14). These findings may be discouraging the treating physicians, fearing for the high fatality rate of HSCT recipients. On the other hand, the use of immunosuppressive agents may potentially mitigate the deleterious systemic inflammatory syndrome secondary to the cytokine storm unleashed by SARS-Cov-2 leading to multiorgan dysfunction and eventually death. According to this observation some studies have reported a lower mortality rate of allogeneic HSCT recipients as compared to non-stem cell transplant patients (18% vs 31%) (3). Hence, aim of our retrospective study was to address the outcome and risk factors for mortality in a large series of patients who developed COVID-19 infection after an allogeneic HSCT.
Patients and methods
Study population
This is retrospective multicenter cohort study promoted by the European Hematology Association – Infections in Hematology Study Working Group (EHA-IDWP; EPICOVIDEHA survey, https://pubmed.ncbi.nlm.nih.gov/34235404/). Data have been collected on all consecutive adult patients who received an allogeneic HSCT and had COVID-19 in more than 150 European centers between January 2020 and March 2022. Only patients for whom allogeneic HSCT represented the last treatment performed were included into the study. Each institutional review board independently approved the study.
Data collection
Researchers at each center collected data using an online questionnaire hosted at www.clinicalsurveys.net, EPICOVIDEHA is registered at http://www.clinicaltrials.gov, with the identifier NCT 04733729. Only de-identified data have been analyzed.
Data collected included: age at transplantation (dichotomized as <50 years and ≥50 years), sex (male vs female), time from HSCT to the diagnosis of COVID-19, immunosuppression within 6 months of COVID-19 diagnosis, conditioning intensity (myeloablative vs reduced intensity), GVHD prophylaxis, time to engraftment, development of acute or chronic GVHD before COVID-19 diagnosis and immunodeficiency scoring index (ISI) at the time of COVID-19 infection. Clinically significant outcomes (hospital admission and intensive care unit [ICU] admission, vital status) were also evaluated. We did not collect information on treatment strategies of COVID-19.
Definitions
Confirmed cases of COVID-19 were defined by a positive reverse transcription polymerase chain reaction (RT-PCR) assay of a specimen collected on a nasopharyngeal swab.
The severity of COVID-19 at admission is graded according to the China Center for Disease Control and Prevention definitions (17).
Disease status at the time of SARS-CoV-2 detection was defined according to each specific disease’s revised criteria for leukemia, myeloproliferative neoplasm, multiple myeloma, and lymphoma. The ISI was calculated as previously described (4).
Endpoints and statistical analysis
The primary outcome of this analysis was overall survival 30 days after COVID-19 diagnosis.
Categorical variables were summarised in frequencies and percentages and continuous variables with median, interquartile range (IQR) and absolute range. Additionally, to determine which factors were associated to mortality in our sample, we performed a Cox regression, with the backwards Wald method. Those variables with a p value <0.1 in the univariable model were included into the multivariable analysis. A p<0.05 was considered significant. Overall survival probability has been plotted in a Kaplan-Meier survival curve. SPSSv25.0 was employed for statistical analyses (SPSS, IBM Corp., Chicago, IL, United States).
Results
Demographics
Between January 2020 and March 2022, 326 patients receiving an allogeneic HSCT were diagnosed with COVID-19 infection and registered in EPICOVIDEHA.
Baseline transplant characteristics are shown in Table 1. The median age at the time of COVID-19 diagnosis was 51 years (IQR 38-61; range 18-75), 132 patients (41%) were female, and 194 patients (59%) were male. Acute leukemia and myelodysplastic syndromes (MDS) (n=257, 79%) were the most common indications for allogeneic HSCT. Overall, 232 patients (71%) received grafts from alternative donors, including matched unrelated donors in 158 cases (48%) and haploidentical donors in 74 cases (23%). For GVHD prophylaxis, 114 patients (35%) received calcineurin inhibitors-based immunosuppression and 71 patients (22%) received post-transplantation cyclophosphamide (PT/Cy). The majority of the patients (297 out of 326 patients, 91%) were not vaccinated at the time of HSCT.
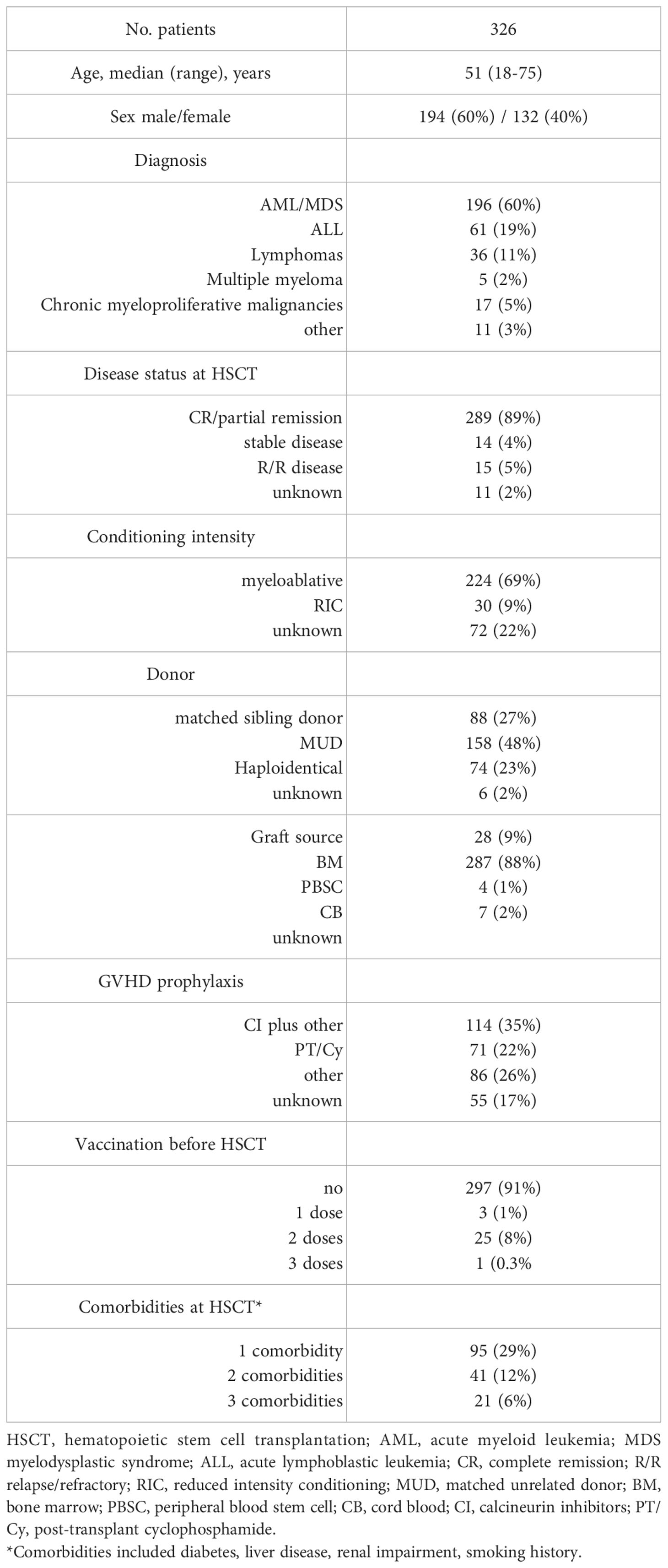
Table 1 Characteristics of HSCT patients with COVID-19 diagnosis.
Clinical characteristics
The median time from HSCT to the diagnosis of COVID-19 was 268 days (IQR 86-713; range 0.185 days). Collectively, 45 patients (14%) received post-HSCT vaccination before COVID-19 diagnosis: 6 patients received one dose, 18 patients two doses, 19 patients three doses and 2 patients four doses.
At the time of COVID-19 diagnosis, active grade II-IV acute GVHD (aGVHD) was present in 15 patients (5%), and 32 patients (10%) had evidence of moderate to severe chronic GVHD (cGVHD). Overall, 199 patients (61%) were on systemic immunosuppressive treatments during the last 6 months before COVID-19 diagnosis. Only a minority of patients was neutropenic (ANC ≤500/mm3) or lymphocytopenic (ALC ≤200/mm3) at the time of COVID-19 diagnosis (6% and 10% respectively).
COVID-19 severity was mild in 21% of the patients, severe in 39% and critical in 16% of the patients; 79 patients (24%) had asymptomatic infection.
Among the 184 patients who were hospitalized, 51 patients (28%) were admitted to ICU, and 34 patients required mechanical ventilation.
Patient characteristics at the time of COVID-19 diagnosis are summarized in Table 2.
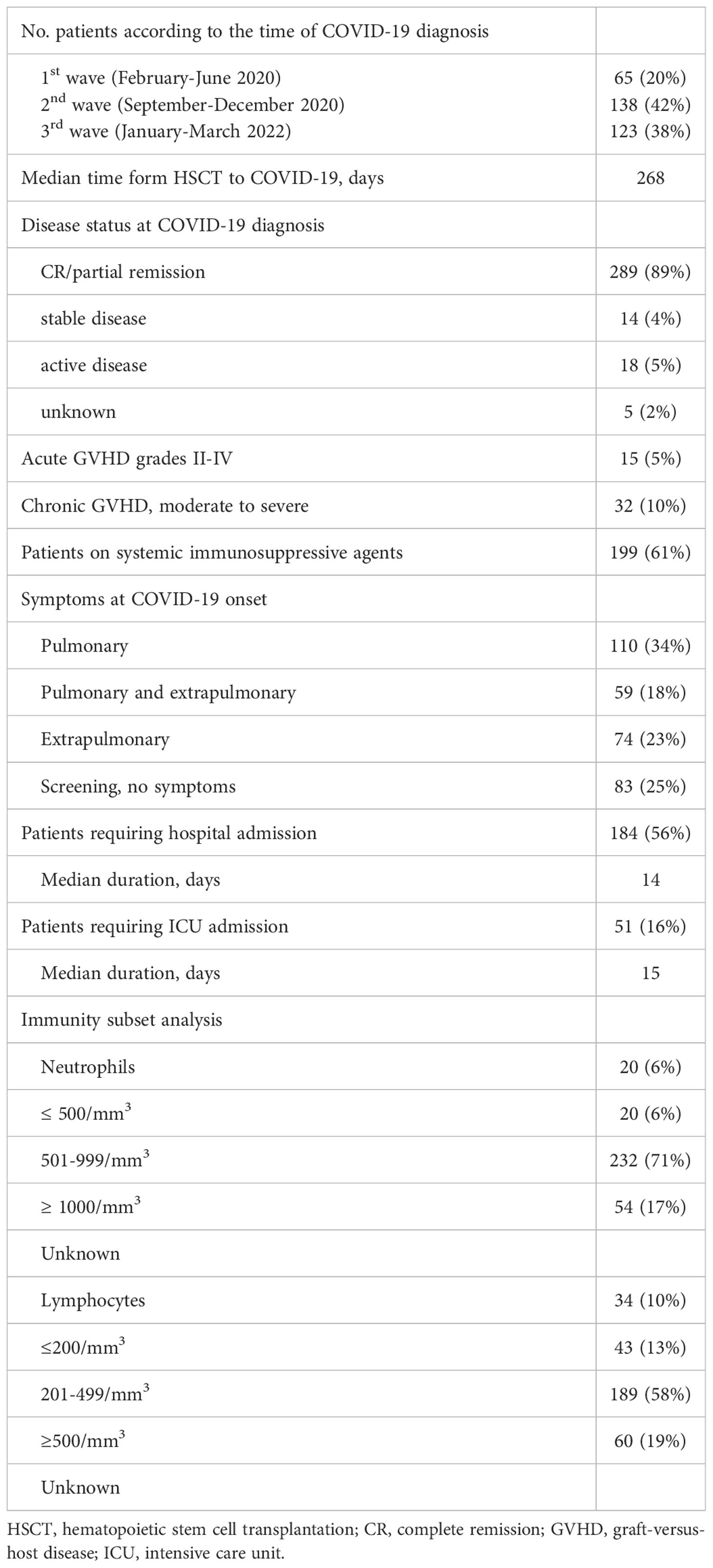
Table 2 Patient Characteristics at diagnosis of COVID-19.
Factors associated with mortality and outcome of COVID-19 infection
The results of Cox regression analysis for factors associated with mortality after COVID-19 diagnosis in allogeneic HSCT recipients are shown in Table 3.
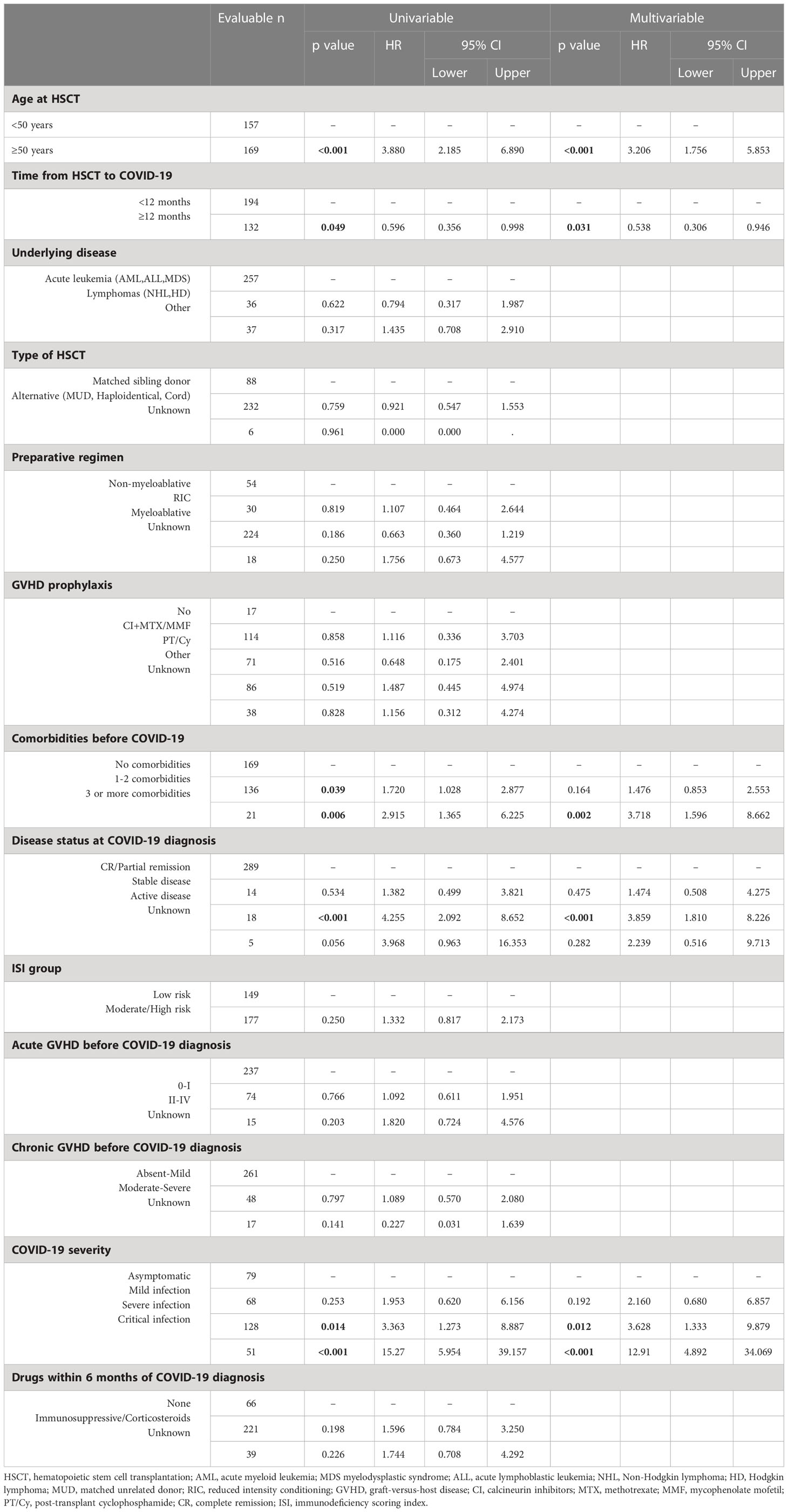
Table 3 Univariate and multivariate analysis for risk factors associated with COVID-19 mortality.
In multivariable analysis factors associated with a higher risk of mortality were, age 50 years or older, presence of 3 or more comorbidities, active hematologic disease at time of COVID-19 infection, development of COVID-19 within 12 months of HSCT, and severe/critical infections. The type of HSCT, the intensity of preparative regimen, the presence of aGVHD and cGVHD before COVID-19 infection and ISI group were not associated with increased mortality.
Vaccination and the number of doses (one, two or more doses) administered did not have an impact on the outcome of the patients.
At the time of last follow-up, 258 patients (79%) are alive: from the diagnosis of COVID-19, the median follow of survivors was 126 days (IQR 32-339; range 0-643 days). The Kaplan-Meier overall survival estimate is shown in Figure 1. Overall, 68 patients (21%) had died after a median follow-up post COVID-19 of 26 days (IQR 12-56; range 0-379 days). Causes of death were COVID-19 infection in 42 cases (13%), COVID-19 in parallel to recurrence of the underlying hematologic malignancy in 11 cases (3%), and hematologic malignancy +/- other reasons in 15 cases (5%).
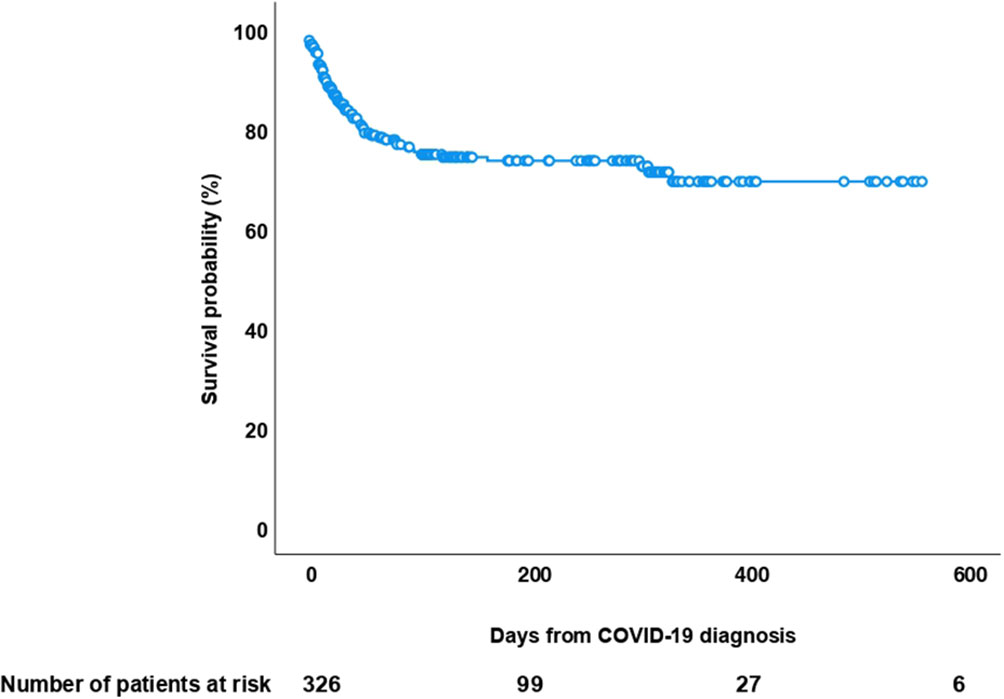
Figure 1 Kaplan-Meier overall survival curve after diagnosis of COVID-19 infection in 326 allogeneic HSCT recipients.
Discussion
To our knowledge, the present study includes the largest series of allogeneic HSCT recipients with COVID-19. The aim of our analysis was to evaluate the outcome of COVID-19 in a cohort of patients particularly susceptible to infectious complications and to investigate risk factors that may impact on mortality. Patients were at high risk for severe disease and adverse outcome from COVID-19: a large proportion of patients (70%) received HSCT from alternative donors, 16% had critical infection and required ICU admission. Even more importantly, the median time from HSCT to COVID-19 infection was 268 days, remarkably shorter when compared to other reports (474-790 days) (3, 4, 12, 14). This finding might mirror the adoption of less stringent measures of stewardship among transplant centers after the 1st and 2nd COVID-19 wave. In fact, it should be recognized that one third of the patients had COVID-19 infection diagnosed during the 3rd wave.
Our study demonstrated that COVID-19 infection is a severe complication in allogeneic HSCT recipients with an attributable mortality of 16%. Our results are roughly superimposable to those reported from other recent studies. The CIBMTR reported a COVID-19-related mortality rate of 20% in 184 allogeneic HSCT recipients (14), Piñana et al. analyzed the outcome of COVID-19 in 65 allogeneic HSCT patients and reported a mortality of 18% (3). An EBMT (European Society for Blood and Marrow Transplantation) and GETH (Spanish Group of Hematopoietic Stem Cell Transplantation) prospective study reported an overall mortality rate of 28% among 236 allogeneic HSCT recipients (12). Other smaller series documented similar mortality rates ranging from 20 to 25% (5–7, 9). It is worthwhile recalling that mortality in the general population declined over the 2nd and 3rd waves: this observation should be considered when we consider that only 20% of our patients were diagnosed with COVID-19 during the first wave.
Multivariable analysis showed that age, comorbidities, active disease, and severe/critical infection have been associated with higher mortality, consistent with previous studies (3, 4, 12, 14). Nevertheless, it should be noted that a consistent number of comorbidities and demographic characteristics (i.e. diabetes, BMI, race) potentially influencing the outcome of the patients were not available Similarly, time from HSCT to COVID-19 diagnosis of less than 12 months was a factor significantly associated with fatal outcome. Surprisingly, GVHD at the time of COVID-19 diagnosis did not impact on the outcome of our patients, however it should be underscored that only 5% of the patients had grade II-IV acute GVHD and 10% had moderate/severe chronic GVHD; in addition, data on the cumulative dose of steroids and the different immunosuppressive agents used were not available.
Likewise, mortality was not influenced by the use of immunosuppressive drugs and steroids during the 6 months preceding COVID-19 diagnosis, notwithstanding the number of patients on treatment was extremely high. Whether the administration of two to three doses of vaccine in 20% of the patients might have contributed to dampen the severity of the disease as documented in some studies (18, 19), remains speculative. Regrettably, we do not have data on patient seroconversion and B-cell reconstitution underpinning the effectiveness of vaccination.
ISI did not result as an independent risk factor for poor outcome as shown by Ljungman et al, however several variables included in the ISI (ANC and ALC, GVHD) were poorly represented in our study group. Two studies including a small number of patients reported a favorable outcome of patients receiving PT/Cy as GVHD prophylaxis, since cytokine release syndrome (CRS) associated with haploidentical HSCT and COVID-19 share similar pathophysiology (10, 11). It is well known that a dysregulated, excessive immune response with increased pro-inflammatory cytokines levels during the later phases of COVID-19 infection may lead to multiorgan failure (20). Cy is an alkylating agent largely used in the setting of haploidentical HSCT due to its capacity of depleting rapidly proliferating T-cells while sparing regulatory-T cells (21). According to these observations, it has been postulated a potential effect of Cy in mitigating the COVID-19 infection (22), however in our cohort, we did not find any significant relationship between the type of GVHD prophylaxis and mortality, including PT/Cy in 22% of the cases. ANC and ALC at the time of COVID-19 diagnosis did not result as significant factors for disease severity as shown in other studies (3, 5), however a minority of our patients were neutropenic or had low ALC.
We recognize limitations of our study inherent to the retrospective design. We cannot exclude a possible selection bias in the registration of the patients among such a large number of centers. Our study presents a significant heterogeneity in terms of different variants of concern, namely wild type, delta and omicron variants, each with distinctive transmission rates and infection associated mortality. Information on the treatment of COVID-19 were not available and the management of patients with COVID-19 across centers may differ profoundly, potentially influencing clinical outcome.
Conclusion
Our study on a large number of patients who developed COVID-19 infection following HSCT, shows a high mortality rate compared to the general population. In this respect, it is of upmost relevance to see whether vaccination of patients after HSCT and the availability of pre- and post-exposure prophylactic measures effectively mitigates the severity of the disease in this vulnerable group of patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by EPICOVIDEHA was approved by the local ethics committee of the Fondazione Policlinico Universitario Agostino Gemelli - IRCCS, Università Cattolica del Sacro Cuore of Rome, Italy (Study ID: 3226). The patients/participants provided their written informed consent to participate in this study.
A list of EPICOVIDEHA Collaborators members
Juergen Prattes, Malgorzata Mikulska, Gustavo-Adolfo Méndez, Tobias Lahmer, Pavel Jindra, Anna Guidetti, Rita Fazzi, Maria Ilaria Del Principe, Cristina De Ramón, Maria Calbacho, Zlate Stojanoski, Andrés Soto, Alexandra Serris, Irati Ormazabal-Vélez, Ali S. Omrani, Milan Navrátil, Sonia Martín-Pérez, Joyce Marques De Almeida, Sylvain Lamure, Martin Kolditz, Ozren Jaksic, Martin Hoenigl, Carolina Garcia-Vidal, Noemí Fernández, Shaimaa El-Ashwah, Natasha Čolović, Martin Čerňan, Caterina Buquicchio, Valentina Bonuomo, Josip Batinić, Murtadha Al-Khabori, Tatjana Adžić-Vukičević, Juan-Alberto Martín-González, Maria Vittoria Sacchi, María-Josefa Jiménez-Lorenzo, Dominik Wolf, Maria Vehreschild, Raul Cordoba, Ramón García-Sanz, Toni Valković, Miloš Mladenović, Nicole García-Poutón, Ziad Emarah, Julio Dávila-Valls
Author contributions
AB, JS-G, FM, OC and LiP contributed to study design, study supervision, and data interpretation and wrote the paper. AB, JS-G and LiP did the statistical plan. JS-G performed the analysis and AB, JS-G and LiP interpreted the data. All authors recruited participants and collected and interpreted data, contributed to manuscript writing and review of the manuscript, agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved and have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
EPICOVIDEHA has received funds from Optics COMMITTM (COVID-19 Unmet Medical Needs and Associated Research Extension) COVID-19 RFP program by GILEAD Science, United States (Project 2020-8223). The funder of the study had no role in study design, data analysis, interpretation, or writing of the report. All authors had full access to the data and had final responsibility for the decision to submit for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zhang Y, Xu J, Li H, Cao B. A novel coronavirus (COVID-19) outbreak: A call for action. Chest. (2020) 157:e99–e101. doi: 10.1016/j.chest.2020.02.014
2. EBMT COVID-19 guidelines . Available at: https://www.ebmt.org/sites/default/files/2021-06/EBMT%20COVID-19%20guidelines%20v.%2016.03.pdf.
3. Piñana JL, Martino R, García-García I, Parody R, Morales MD, Benzo G, et al. Risk factors and outcome of COVID-19 in patients with hematological malignancies. Exp Hematol Oncol (2020) 9:21. doi: 10.1186/s40164-020-00177-z
4. Shah GL, DeWolf S, Lee YJ, Tamari R, Dahi PB, Lavery JA, et al. Favorable outcomes of COVID-19 in recipients of hematopoietic cell transplantation. J Clin Invest (2020) 130(12):6656–67. doi: 10.1172/JCI141777
5. Varma A, Kosuri S, Ustun C, Ibrahim U, Moreira J, Bishop MR, et al. COVID-19 infection in hematopoietic cell transplantation: Age, time from transplant and steroids matter. Leukemia (2020) 34(10):2809–12. doi: 10.1038/s41375-020-01019-x
6. Coll E, Fernàndez-Ruiz M, Sánchez-Álvarez JE, Martínez-Fernández JR, Crespo M, Gayoso J, et al. COVID-19 in transplant recipients: The Spanish experience. Am J Transplant (2021) 21:1825–37. doi: 10.1111/ajt.16369
7. Mushtaq MU, Shahzad M, Chaudhary SG, Luder M, Ahmed N, Abdelhakim H, et al. Impact of SARS-CoV-2 in hematopoietic stem cell transplantation and chimeric antigen receptor T cell therapy recipients. Transplant Cell Ther J (2021) 27(9):796.e1–7. doi: 10.1016/j.jtct.2021.07.005
8. Altuntas F, Ata N, Yigenoglu TN, Bascı S, Dal MS, Korkmaz S, et al. COVID-19 in hematopoietic cell transplant recipients. Bone Marrow Transplant (2021) 56:952–5. doi: 10.1038/s41409-020-01084-x
9. Camargo JF, Mendoza MA, Lin R, Moroz IV, Anderson AD, Morris MI, et al. Clinical presentation and outcomes of COVID-19 following hematopoietic cell transplantation and cellular therapy. Wiley Periodicals (2021) 23(4):e13625. doi: 10.1111/tid.13625
10. Abid MB, Hamadani M, Szabo A, Hari PN, Graham MB, Frank MO, et al. Severity of cytokine release syndrome and its association with infections after T cell-replete haploidentical related donor transplantation. Biol Blood Marrow Transplant (2020) 26:1670–8.
11. Abid MB, Mughal M, Abid MA. Coronavirus disease 2019 (COVID-19) and immune-engaging cancer treatment. JAMA Oncol (2020) 6:1529–30.
12. Ljungman P, de la Cámara R, Mikulska M, Tridello G, Aguado B, Zahrani MA, et al. COVID-19 and stem cell transplantation; results from an EBMT and GETH multicenter prospective survey. Leukemia (2021) 35(10):2885–94. doi: 10.1038/s41409-021-01302-5
13. Passamonti F, Cattaneo C, Arcaini L, Bruna R, Cavo M, Merli F, et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: A retrospective, multicentre, cohort study. Lancet Hematol (2020) 7(10):e737–45. doi: 10.1016/S2352-3026(20)30251-9
14. Sharma A, Bhatt NS, St Martin A, Abid MB, Bloomquist J, Chemaly RF, et al. Clinical characteristics and outcomes of COVID-19 in haematopoietic stem-cell transplantation recipients: An observational cohort study. Lancet Haematol (2021) 8:e185–93. doi: 10.1016/S2352-3026(20)30429-4
15. Pagano L, Salmanton-García J, Marchesi F, Busca A, Corradini P, Hoenigl M, et al. COVID-19 infection in adult patients with hematological malignancies: a European hematology association survey (EPICOVIDEHA). J Hematol Oncol (2021) 14(1):168. doi: 10.1186/s13045-021-01177-0
16. Salmanton-García J, Busca A, Cornely OA, Corradini P, Hoenigl M, Klimko N, et al. EPICOVIDEHA: A ready to use platform for epidemiological studies in hematological patients with COVID-19. Hemasphere (2021) 5(7):e612. doi: 10.1097/HS9.0000000000000612
17. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese center for disease control and prevention. JAMA (2020) 323:1239.
18. Abid MB, Rubin M, Ledeboer N, Szabo A, Longo W, Mohan M, et al. Efficacy of a third SARS-CoV-2 mRNA vaccine dose among hematopoietic cell transplantation, CAR T cell, and BiTE recipients. Cancer Cell (2022) 40(4):340–2. doi: 10.1016/j.ccell.2022.02.010
19. Maillard A, Redjoul R, Klemencie M, Labussière Wallet H, Le Bourgeois A, D'Aveni M, et al. Antibody response after 2 and 3 doses of SARS-CoV-2 mRNA vaccine in allogeneic hematopoietic cell transplant recipients. Blood. (2022) 139(1):134–7. doi: 10.1182/blood.2021014232
20. Channappanavar R, Perlman S. Human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin Immunopathol (2017) 39:529–39.
21. Luznik I, O’Donnell PV, Fuchs EJ. Post-transplantation cyclophosphamide for tolerance induction in HLA-haploidentical bone marrow transplantation. Semin Oncol (2012) 39:683–93.
Keywords: allogeneic HSCT, COVID-19 infection, immunocompromised patients, SARS-CoV-2, hematological malignances
Citation: Busca A, Salmanton-García J, Marchesi F, Farina F, Seval GC, Van Doesum J, De Jonge N, Bahr NC, Maertens J, Meletiadis J, Fracchiolla NS, Weinbergerová B, Verga L, Ráčil Z, Jiménez M, Glenthøj A, Blennow O, Tanase AD, Schönlein M, Prezioso L, Khanna N, Duarte RF, Žák P, Nucci M, Machado M, Kulasekararaj A, Espigado I, De Kort E, Ribera-Santa Susana JM, Marchetti M, Magliano G, Falces-Romero I, Ilhan O, Ammatuna E, Zompi S, Tsirigotis P, Antoniadou A, Zambrotta GPM, Nordlander A, Karlsson LK, Hanakova M, Dragonetti G, Cabirta A, Berg Venemyr C, Gräfe S, Van Praet J, Tragiannidis A, Petzer V, López-García A, Itri F, Groh A, Gavriilaki E, Dargenio M, Rahimli L, Cornely OA, Pagano L and EPICOVIDEHA Consortium (2023) Outcome of COVID-19 in allogeneic stem cell transplant recipients: Results from the EPICOVIDEHA registry. Front. Immunol. 14:1125030. doi: 10.3389/fimmu.2023.1125030
Received: 15 December 2022; Accepted: 01 February 2023;
Published: 24 February 2023.
Edited by:
David Allan, Ottawa Hospital Research Institute (OHRI), CanadaReviewed by:
Guillermo José Ruiz-Argüelles, Clínica Ruiz, MexicoMuhammad Bilal Abid, Medical College of Wisconsin, United States
Copyright © 2023 Busca, Salmanton-García, Marchesi, Farina, Seval, Van Doesum, De Jonge, Bahr, Maertens, Meletiadis, Fracchiolla, Weinbergerová, Verga, Ráčil, Jiménez, Glenthøj, Blennow, Tanase, Schönlein, Prezioso, Khanna, Duarte, Žák, Nucci, Machado, Kulasekararaj, Espigado, De Kort, Ribera-Santa Susana, Marchetti, Magliano, Falces-Romero, Ilhan, Ammatuna, Zompi, Tsirigotis, Antoniadou, Zambrotta, Nordlander, Karlsson, Hanakova, Dragonetti, Cabirta, Berg Venemyr, Gräfe, Van Praet, Tragiannidis, Petzer, López-García, Itri, Groh, Gavriilaki, Dargenio, Rahimli, Cornely, Pagano and EPICOVIDEHA Consortium. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jon Salmanton-García, am9uLnNhbG1hbnRvbi1nYXJjaWFAdWsta29lbG4uZGU=
†These authors share first authorship
‡ORCID: Alessandro Busca, orcid.org/0000-0001-5361-5613
Jon Salmanton-García, orcid.org/0000-0002-6766-8297
Francesco Marchesi, orcid.org/0000-0001-6353-2272
Francesca Farina, orcid.org/0000-0002-5124-6970
Guldane Cengiz Seval, orcid.org/0000-0001-9433-2054
Jaap Van Doesum, orcid.org/0000-0003-0214-3219
Nick De Jonge, orcid.org/0000-0002-9901-0887
Nathan C. Bahr, orcid.org/0000-0002-9431-8938
Johan Maertens, orcid.org/0000-0003-4257-5980
Joseph Meletiadis, orcid.org/0000-0002-8869-1509
Nicola S. Fracchiolla, orcid.org/0000-0002-8982-8079
Barbora Weinbergerová, orcid.org/0000-0001-6460-2471
Luisa Verga, orcid.org/0000-0002-0868-3358
Zdeněk Ráčil, orcid.org/0000-0003-3511-4596
Moraima Jiménez, orcid.org/0000-0003-1444-8562
Andreas Glenthøj, orcid.org/0000-0003-2082-0738
Ola Blennow, orcid.org/0000-0002-7167-7882
Martin Schönlein, orcid.org/0000-0002-1010-0975
Lucia Prezioso, orcid.org/0000-0003-1660-4960
Nina Khanna, orcid.org/0000-0002-2642-419x
Pavel Žák, orcid.org/0000-0003-4465-5343
Marcio Nucci, orcid.org/0000-0003-4867-0014
Marina Machado, orcid.org/0000-0002-8370-2248
Austin Kulasekararaj, orcid.org/0000-0003-3180-3570
Ildefonso Espigado, orcid.org/0000-0002-4043-6613
José-María Ribera-Santa Susana, orcid.org/0000-0003-1042-6024
Monia Marchetti, orcid.org/0000-0001-7615-0572
Gabriele Magliano, orcid.org/0000-0002-9129-1530
Iker Falces-Romero, orcid.org/0000-0001-5888-7706
Osman Ilhan, orcid.org/0000-0003-1665-372x
Emanuele Ammatuna, orcid.org/0000-0001-8247-4901
Sofia Zompi, orcid.org/0000-0002-4075-8727
Panagiotis Tsirigotis, orcid.org/0000-0002-3522-3680
Anastasia Antoniadou, orcid.org/0000-0003-0991-9198
Giovanni Paolo Maria Zambrotta, orcid.org/0000-0002-8612-2994
Linda Katharina Karlsson, orcid.org/0000-0003-3317-7550
Giulia Dragonetti, orcid.org/0000-0003-1775-6333
Alba Cabirta, orcid.org/0000-0001-7198-8894
Caroline Berg Venemyr, orcid.org/0000-0003-2461-5395
Stefanie Gräfe, orcid.org/0000-0001-7678-0179
Jens Van Praet, orcid.org/0000-0002-7125-7001
Verena Petzer, orcid.org/0000-0002-9205-1440
Alberto López-García, orcid.org/0000-0002-5354-5261
Federico Itri, orcid.org/0000-0002-3532-5281
Michelina Dargenio, orcid.org/0000-0003-0924-4629
Laman Rahimli, orcid.org/0000-0003-2266-445x
Oliver A. Cornely, orcid.org/0000-0001-9599-3137
Livio Pagano, orcid.org/0000-0001-8287-928x