 José Mário Matos-Sousa1Victória Santos Chemelo1
José Mário Matos-Sousa1Victória Santos Chemelo1 Deborah Ribeiro Frazão1
Deborah Ribeiro Frazão1 Leonardo Oliveira Bittencourt1
Leonardo Oliveira Bittencourt1 João Daniel Mendonça de Moura1
João Daniel Mendonça de Moura1 Caio Melo Mesquita2
Caio Melo Mesquita2 Guido Marañón-Vásquez3
Guido Marañón-Vásquez3 Nathalia Carolina Fernandes Fagundes4
Nathalia Carolina Fernandes Fagundes4 Luiz Renato Paranhos2
Luiz Renato Paranhos2 Lucianne Cople Maia3
Lucianne Cople Maia3 Marta Chagas Monteiro5
Marta Chagas Monteiro5 Rafael Rodrigues Lima1*
Rafael Rodrigues Lima1*- 1Laboratory of Functional and Structural Biology, Institute of Biological Sciences, Federal University of Pará, Belém-Pará, Brazil
- 2Department of Preventive and Social Dentistry, Faculty of Dentistry, Federal University of Uberlândia, Uberlândia, Minas Gerais, Brazil
- 3Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
- 4School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada
- 5Health Science Institute, Federal University of Pará, Belém-Pará, Brazil
This systematic review aimed to verify whether there is evidence of an association between apical periodontitis and the presence of systemic biomarkers. This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses - PRISMA. For this, the acronym PECO was used; population (P) of adult humans exposed (E) to the presence of apical periodontitis, compared (C) to adult humans without apical periodontitis, and the outcome (O) of the presence of biomarkers was observed. The articles were searched in PubMed, Scopus, Web of Science, LILACS, Cochrane Library, OpenGray, and Google Scholar grey databases. Subsequently, studies were excluded based on title, abstract, and full article reading, following the eligibility criteria. The methodological quality of the selected studies was evaluated using the Newcastle-Ottawa qualifier. After exclusion, 656 studies were identified, resulting in 17 final articles that were divided into case-control, cross-sectional, and cohort studies. Eight studies were considered to have a low risk of bias, one had a medium risk of bias, and eight had a high risk of bias. In addition, 12 articles evaluated biomarkers in blood plasma, four evaluated them in saliva, and only one evaluated them in gingival crevicular fluid. The results of these studies indicated an association between apical periodontitis and the systemic presence of biomarkers. These markers are mainly related to inflammation, such as interleukins IL-1, IL-2, and IL-6, oxidative markers, such as nitric oxide and superoxide anions, and immunoglobulins IgG and IgM.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier (CRD42023493959).
1 Introduction
Because of microbial infection of the root canals, apical periodontitis (AP) is a chronic inflammatory disease that can destroy periradicular tissues (1). AP has microbial factors as its main etiology and is involved in the initiation, development, and persistence of the disease, sustained by a biofilm that can invade periodontal structures (2, 3).
AP development is based on the inflammatory response and bone destruction in periapical tissues related to the microbial location within the root canal, organization of the biofilm, and degree of virulence (3, 4). Microorganisms can cause direct tissue damage and modulate host immune responses by secreting products, including enzymes, immunoglobulins, cytokines, chemokines, the RANK/RANKL/OPG system, and other inflammatory markers (5, 6).
During AP development, acute and chronic inflammatory reactions can develop depending on the intensity of the bacterial infection and the host immune response (6). The large amount and interaction of various inflammatory stimuli can influence and alter disease state and progression (5). The host immune response attempts to localize the infection and prevent its further spread at the expense of disrupting the apical periodontal tissue involving the periodontal ligament, root cementum, and alveolar bone (7).
The periradicular region is modulated by proinflammatory and anti-inflammatory biomarkers. Most of these biomarkers are regulated in response to bacterial infection. The balance between pro- and anti-inflammatory biomarkers controls the host immune response to antigen stimulation during chronic inflammation, triggering the defense process and preventing bone resorption (8, 9).
In apical periodontitis, biomarkers are found in various samples, such as gingival crevicular fluid, plasma, periapical exudate, serum, and saliva. Pro-inflammatory biomarkers are produced mainly by TH1 cells, macrophages, and neutrophils, such as interleukin (IL) -1β, IL-6, interferon (IFN)-γ, and tumor necrosis factor (TNF)-α. In contrast, anti-inflammatory biomarkers are released by TH2 and Treg cells, such as transforming growth factor (TGF)-β and IL-4 (8, 9).
Considering the influence of biomarkers on inflammation and their roles in apical periodontitis, it is important to evaluate the association between apical periodontitis and the presence of biomarkers. Therefore, this systematic review aimed to gather scientific evidence to analyze the association between the presence of systemic biomarkers and apical periodontitis in adult humans.
2 Material and methods
2.1 Register and protocol
This systematic review was registered on the platform responsible for the records and organization of systematic reviews, PROSPERO, under code CRD42023493959. Additionally, this systematic review was conducted according to the Preferred Report Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 version and according to the Conducting Systematic Reviews and Meta-Analyses of Observational Studies of Etiology (COSMOS-E) guideline (10).
2.2 Eligibility criteria and search strategy
This systematic review aimed to determine whether patients with apical periodontitis have different concentrations of biomarkers than healthy patients. We utilized the PECO acrostic to define the eligibility criteria, in which “P” represents the population, “E” the exposure, “C” the comparison, and “O” the outcome. This review used P: human, E: apical periodontitis, C: absence of apical periodontitis, and O: presence of biomarkers. The study included only observational studies and excluded case reports, reviews, opinion articles, animal studies, and in vitro studies. Two examiners (JMMS and VSC) selected the studies by consulting a third examiner (RRL) in cases of disagreement.
The search strategy was performed using MeSH and Entry terms for searching in the following online databases: MEDLINE (PubMed), Scopus (https://www.scopus.com/), Web of Science (https://www.webofscience.com/), Lilacs (BVS), and EMBASE (https://www.embase.com/), using the search string: “Apical Periodontitis” AND “Biomarkers,” as the main meSHs, however, the search key will be presented in Supplementary Table 1. We also searched Google Scholar and OpenGrey (June 2022) using the anonymous guide as the grey literature using the only search string: “Apical Periodontitis” AND “Biomarkers.” There were no restrictions on the language or year of publication. Searches were conducted between January 2022 and January 2023. The studies found in each database were exported in the order of the search to a reference organization application (EndNote®, version X9, Thomson Reuters, Philadelphia, USA).
2.3 Study selection process and data extraction
Two examiners (JMMS and VSC) independently performed the data extraction. A third reviewer was consulted in case of disagreement. This process began with the automatic and manual deletion of duplicates after the articles were imported. Subsequently, studies were evaluated based on their titles and abstracts. These findings were assessed thoroughly. Furthermore, the references of the included studies were manually checked to select all published articles that met the inclusion criteria.
After selecting the final articles, we extracted relevant data for a systematic review. The relevant extracted data were related to the author’s name, year of publication, country, type of study, analysis material, participants (number and mean age of the sample), evaluation of biomarkers (evaluated biomarker and evaluation method), evaluation of apical periodontitis (form of diagnosis, symptomatology, and extent of the lesion), statistical analysis, and results.
2.4 Risk of bias
2.4.1 Quality assessment and risk of bias
Two reviewers (DRF and LOB) used the Newcastle-Ottawa Scale methodology, developed in collaboration between the Universities of Newcastle, Australia, and Ottawa, Canada, to assess the methodological quality and risk of bias of the included studies. This tool was developed to evaluate the quality of nonrandomized research by incorporating quality judgments into the interpretation of meta-analytic findings.
A “star system” was created as part of this protocol. The studies were evaluated by two reviewers from three perspectives: selection of study groups, group comparability, and verification of exposure or outcome of interest for case-control or cohort studies. This checklist aimed to establish an instrument that provides an easy and convenient tool for assessing the quality of nonrandomized studies in a systematic review (12) (Supplementary Table 2).
For cross-sectional investigations, we used Peinado et al.'s (11) adaption of the Newcastle-Ottawa Scale procedure, which still uses the “star system.” After the qualitative assessment, the number of “stars” is used to calculate each study’s risk of bias (Supplementary Table 2).
2.4.2 Evaluation of control statements for possible confounders and bias consideration
This evaluation was based on the results of a previous study by Hemkens et al. (13). All eligible studies were first analyzed for explicit mention of adjustment analyses to control for possible confounders. Studies were excluded if they did not report or if the analyses were unclear. Furthermore, the remaining studies were critically appraised by two independent reviewers (CMM and LRP), and disagreements were resolved by a third reviewer (RRL). Six previously established questions (Table 1) were used to evaluate the abstracts and discussions of each remaining study. The sixth question evaluated the conclusion section; in cases lacking a specific conclusion, the last paragraph of the Discussion section was considered.
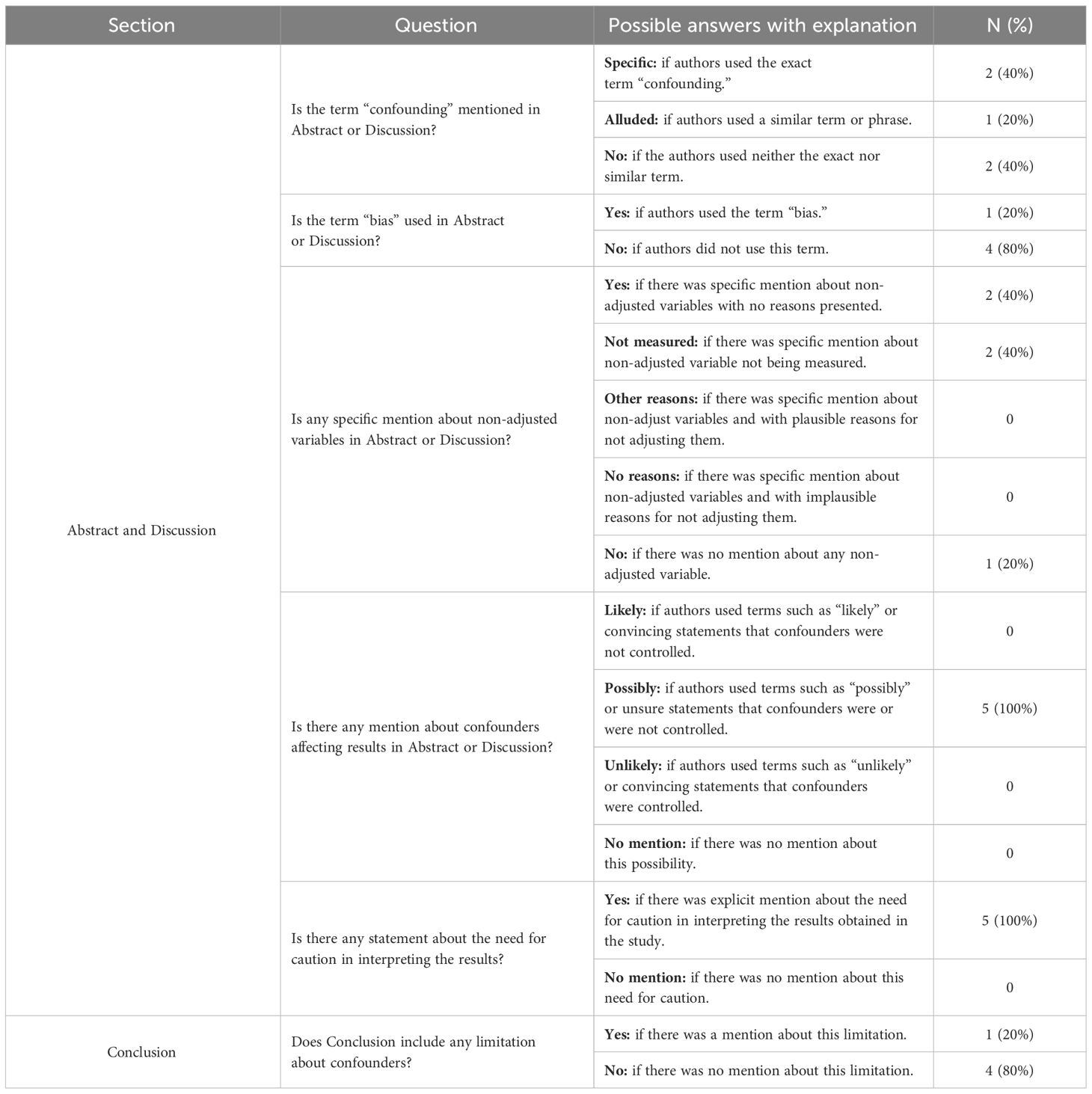
Table 1 Evaluation of control statements for possible confounders and bias consideration.
2.4.3 Assessment of confounding factors
This assessment was based on previous studies by Wallach et al. (14). The remaining studies in the final evaluation was assessed using the Methods and Results section. Assessment of confounding factors was performed by two independent reviewers (CMM and RLP) and a third reviewer (RRL) to resolve conflicts. They identified the variables and confounding domains for each study. The variables were classified into three groups: (1) adjustment (used in multivariate analysis or Poisson regression to control for possible confounders), (2) stratification (used in sample selection to create strata), and (3) matching variables (used to pair known characteristics between study participants or groups).
2.5 Quantitative analysis (meta-analysis)
Quantitative analysis could not be performed since there was a significant divergence in the methodologies of each study, in addition to the diversity of biomarkers evaluated in each study and the different analytical materials.
2.6 Level of evidence (GRADE)
A narrative synthesis of the collected data from the included studies was conducted, including body fluids whose biomarkers were evaluated, target population characteristics, and the type of outcome. The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) was used to compute the absolute expected effect and summary of evidence. The GRADE is a grading system for the evidence level and strength of health recommendations. The mean difference was used as an effect estimate for the Evidence Profile. When serious or extremely serious concerns regarding bias, inconsistency, indirectness, imprecision, and publication bias are identified, the certainty of the evidence drops by one or two. The level of evidence tends to improve when the effect of all plausible confounding factors is minimized or when it suggests a spurious effect.
3 Results
3.1 Characteristics of the included studies
Following the database search, we found a total of 827 studies. After removing duplicates, 535 remained. Following exclusion based on the title and abstract, 31 papers were fully examined. Later, 14 articles were removed because of non-compliance with PECO. For instance, tissue analysis (15–18), absence of a control group (19–22), and non-observational studies (23, 24), treatment analyses (25, 26), microorganism analyses (27) and lack of information (28). Therefore, 17 articles remained in the systematic review (6, 29–44) distributed across cross-sectional, cohort, and case-control studies, as shown in Figure 1.
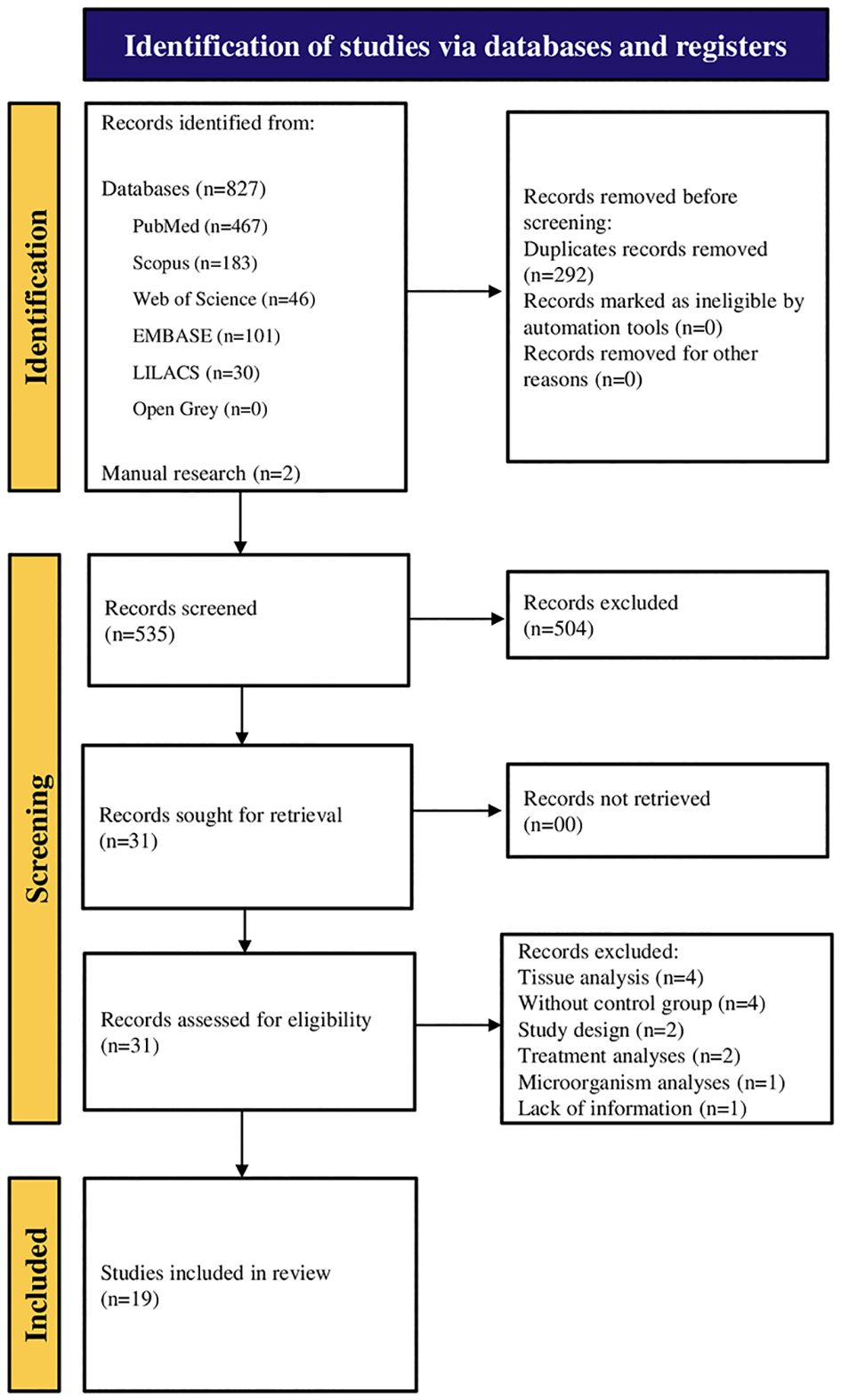
Figure 1 PRISMA flowchart, exclusion process for selecting final articles.
3.2 Results of individual studies
Among the final 17 studies, the majority were case–control studies which included ten articles (6, 32, 34, 35, 38, 40–44). Five cross-sectional studies (30, 31, 33, 36, 39). Finally, two cohort searches (6, 37), as shown in Figure 2.

Figure 2 Graph with results of the evaluated study designs.
The materials analyzed in these studies were blood serum, saliva, and crevicular fluid. Figure 3 shows the ratio of the number of articles for each material. The main material analyzed was blood plasma, with 12 articles (29, 31–35, 37, 38, 40, 41, 41, 2020; 43). Saliva was evaluated in four studies (6, 36, 42, 44), and only one study (30) evaluated the gingival crevicular fluid.
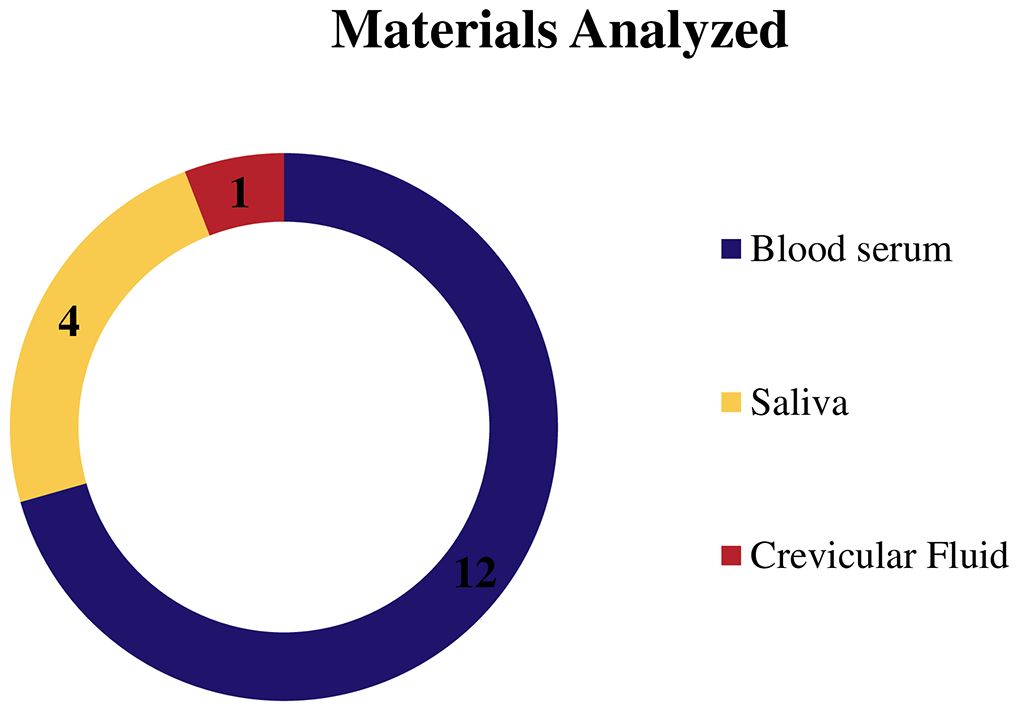
Figure 3 Graph showing the number of articles that evaluated each analysis material.
The average sample size was ± 94.56, with a combination of males and women. The form of biomarker evaluation was primarily verified by the ELISA test in nine of the selected studies (6, 29–31, 33, 38, 39, 41, 44), with the remaining eight alternating between spectrophotometrically, system cadmium-copper reagent, glomax luminomete (35); enzyme immunoassay (EIA) kits (36 and 32); Biological antioxidant potential (BAP) test and d-ROMs test (37); Gauging system (40); Agilent 5977B interfaced to the GC 7890B (42), radioimmunodiffusion (43) and immunoassay customized kits (34).
Among the biomarkers examined, interleukins were found in 9 research (29, 30, 32, 31, 33, 34, 36, 39, 41), followed by oxidative markers in 5 studies (30, 35, 37, 40, 44), also C-reactive protein (CRP) in 5 articles each (33, 34, 36, 38, 41) with the same number of articles are analyzed TNF-a (30–32, 34, 41), and immunoglobulins in 4 articles (6, 33, 38, 43) in addition, matrix metalloproteinase, lipoproteins, lipids, were found, as shown on Figure 4. Table 2 displays all the individual qualities.
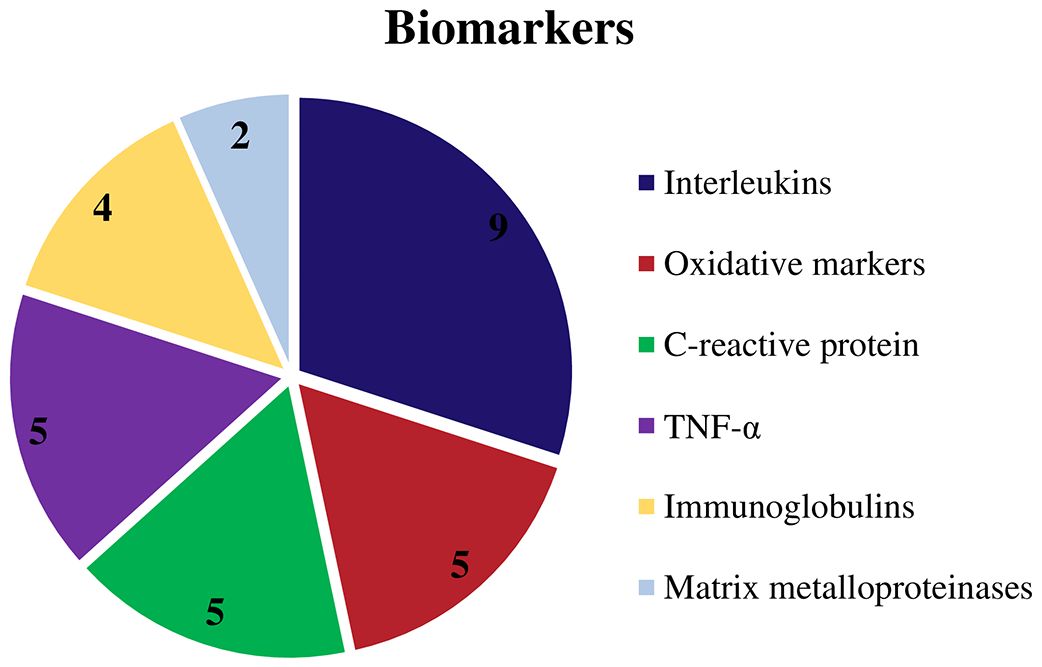
Figure 4 Graphic showing the biomarkers evaluated by the authors.
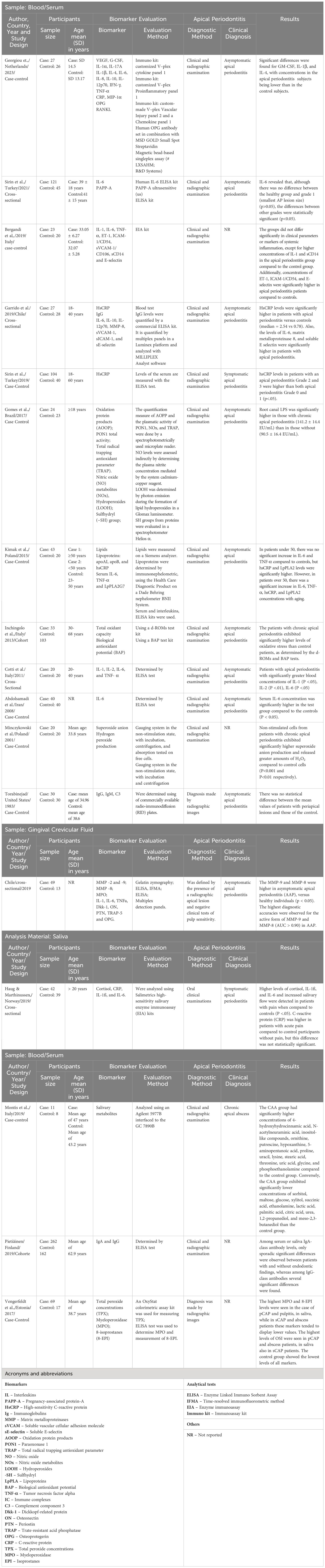
Table 2 Summary of the characteristics and results of the included studies.
Furthermore, in all of the 17 evaluated studies, apical periodontitis was diagnosed by a combination of clinical and radiographic tests (6, 29–44.).
Regarding clinical diagnosis, 11 studies specifically diagnosed asymptomatic AP (29–31, 33–35, 37, 39, 41, 43, 44). Some studies have specified the diagnosis of symptomatic apical periodontitis (36, 38), acute apical abscess (44), and chronic apical abscess (42). Additionally, three studies did not specify a diagnosis other than periapical lesions (6, 32, 40), as shown in Figure 5.

Figure 5 Graphic showing the clinical diagnosis of the studies.
In terms of lesion extent, 12 articles were not specific (6, 29, 31, 32, 34–36, 38, 39, 41–43), three observed lesions >3 mm (30, 33, 40), and two observed lesions <2 cm (37, 44).
Biomarker concentrations in individuals with apical periodontitis versus healthy patients were analyzed in 12 studies (6, 29–33, 35, 37–40, 44), revealing significant differences. However, the remaining four studies reported different outcomes. Rethnam Haug et al. (36) found a substantial increase in interleukins in the exposed group, but there was no significant difference in CRP concentration. Kimak et al. (41) showed that patients under 50 did not have a significant increase in TNF-α but a significant increase in LpPLA2 and HsCRP, while patients over 50 years had significant changes in all biomarkers tested. In addition, Georgiou (34) found a difference in the concentration of biomarkers with reduced levels of anti-inflammatory interleukins in the group with AP. Finally, Montis et al. (42) observed a significant difference in the concentrations of 76 salivary metabolites, some of which were identified at higher concentrations and others at lower concentrations, compared with the control group. Furthermore, Torabinejad et al. (43) found no significant differences in group comparisons (Figure 6).
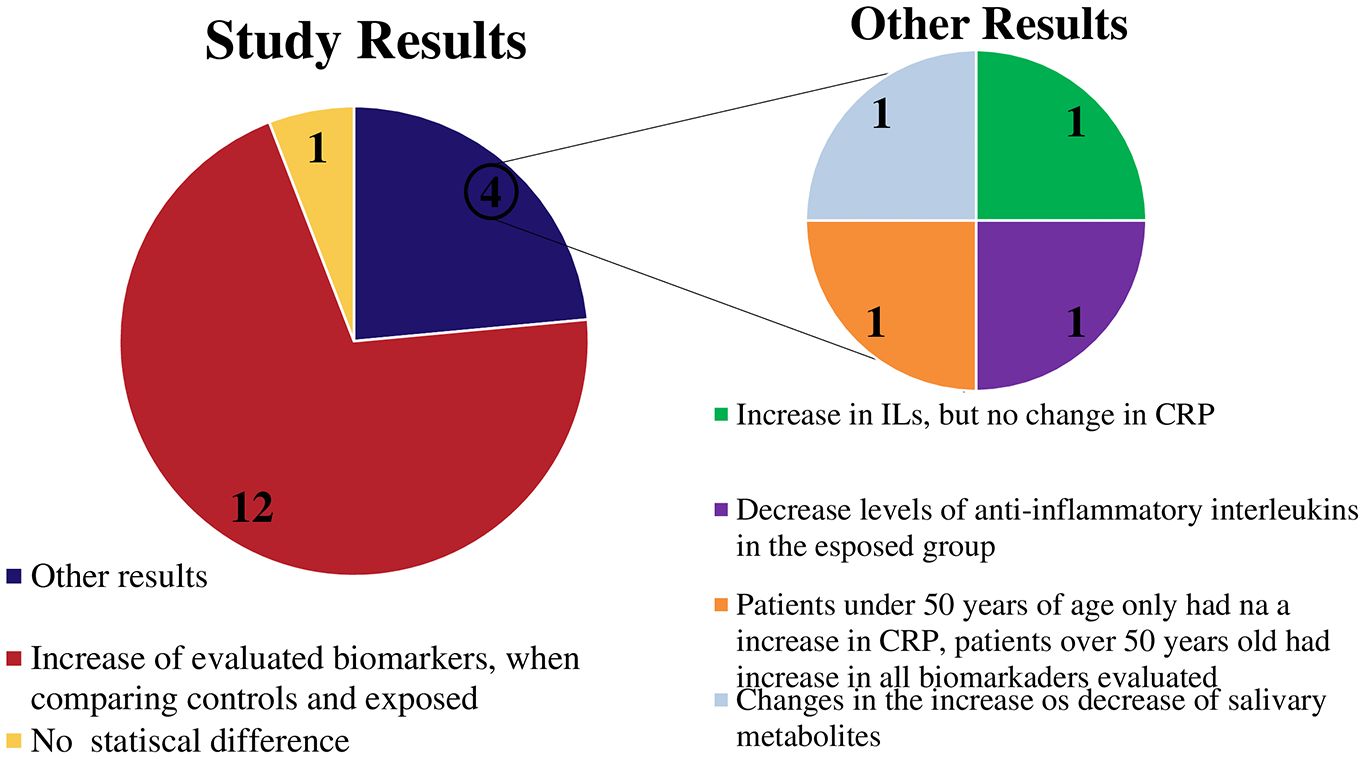
Figure 6 Graphic showing the main results of the studies.
3.3 Analyses of risk of bias
3.3.1 Quality assessment and risk of bias
Table 3 summarizes the findings of the methodological quality and bias risk assessments. As a result, ten studies were rated as high quality, with a low risk of bias (6, 29, 32, 34, 35, 38, 41–44); 1 as fair quality and medium risk of bias (43); and six as low quality with a high risk of bias (31, 33, 36, 37, 39, 40). The main issues found in the studies with a high risk of bias were the verification of exposure and non-response rates. Flaws in the adequate definition of cases, sample size, and ascertainment of exposure were observed in studies with a moderate risk of bias.
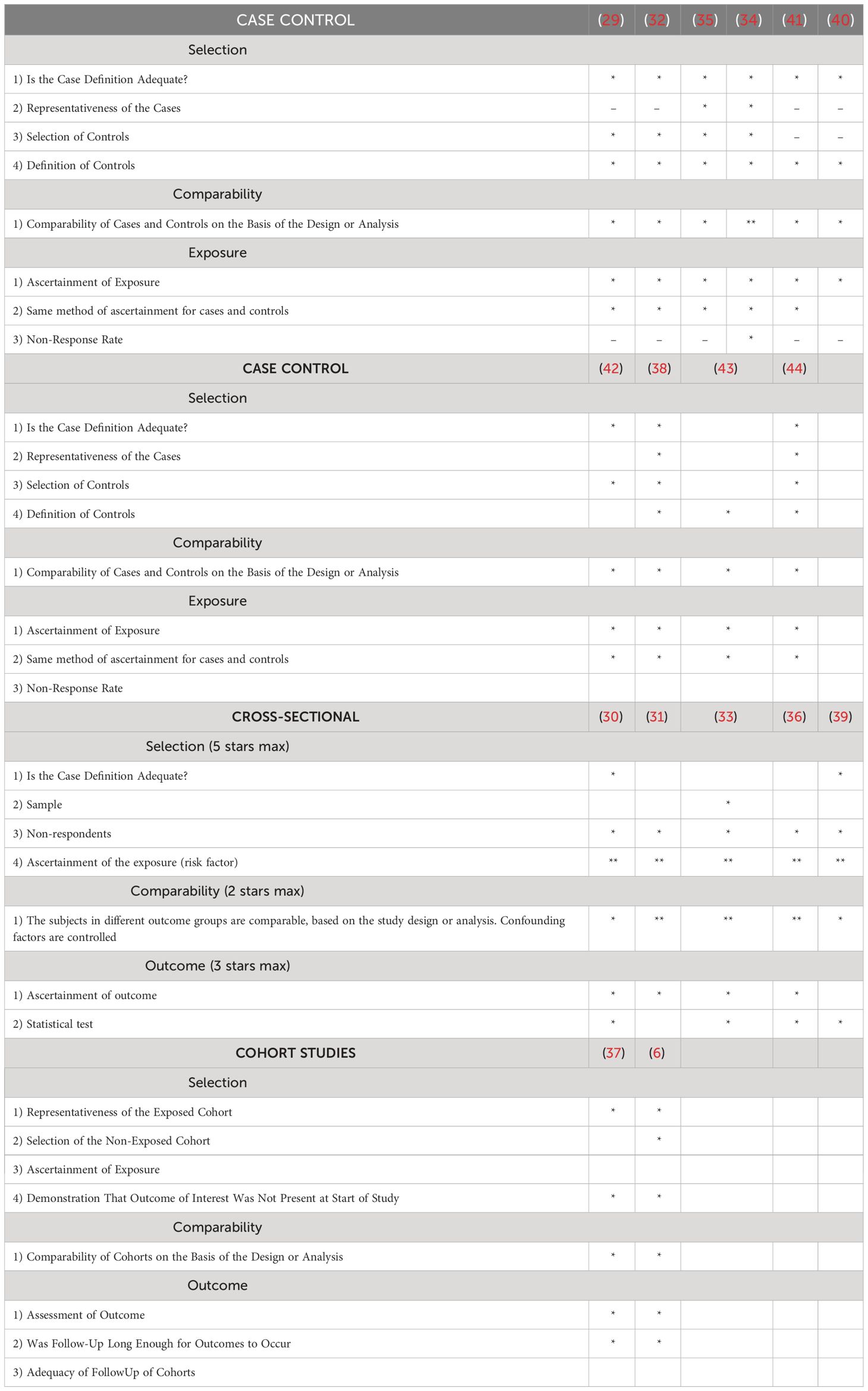
Table 3 Quality assessment and risk of bias.
3.3.2 Evaluation of control statements for possible confounders and bias consideration
Eight eligible studies (29, 32, 34, 37, 39, 40, 43, 44) had not performed adjusment analysis and four studies (31, 38, 41, 42) were unclear about the conducting or reporting of their confounding control analyses. Therefore, only five eligible studies (6, 30, 33, 35, 36) were selected to be critically appraised in further steps.
Two studies (6, 33) made a specific mention of the term “confounding,” and one study (35) alluded to it. Only one study (33) used the term “bias.” Two studies (30, 36) mentioned non-adjusted variables: gingival crevicular fluid in chronic periodontitis and asymptomatic apical periodontitis (30) and severity of stress among groups (36). Two other studies (6, 35) mentioned non-adjusted variables, such as uric acid and xanthine oxidase (35), intracanal bacterial samples, and serum cross-reactive antibodies (6). All five studies (6, 30, 33, 35, 36) mentioned that their results may be affected by confounders and stated the need for caution when interpreting their results. Only one study (30) had limitations regarding confounders in their conclusions. The results of the evaluation of the control statements for possible confounders and bias considerations are summarized in Table 1.
3.3.3 Assessment of confounding factors
A total of 145 variables were identified in selected studies. There were 98 variables used in multivariate analysis to control possible confounders. No studies performed sample stratification. Only one study (36) used matching variables, which were “age” and “sex.”
Six confounding domains were identified in the selected studies: (1) biomarkers; (2) oral health-related domains; (3) body and comorbidities; (4) sociodemographic and socioeconomic status; (5) quality of life; and (6) analysis. The confounding domains identified in each study are listed in Table 4.
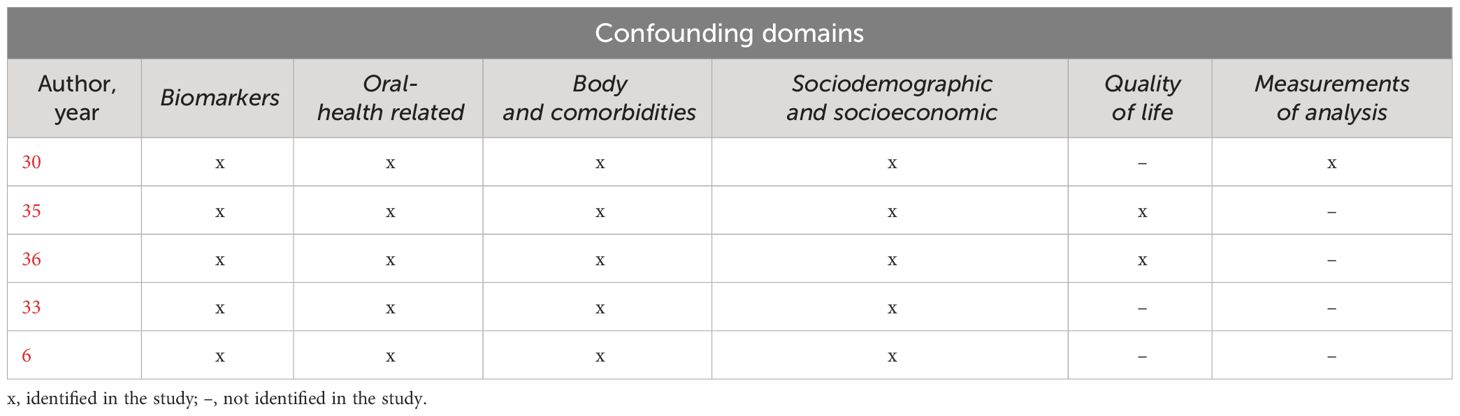
Table 4 Confounding domains identified in selected studies.
The “Biomarkers” domain was the most explored, with a total of 45 variables, whereas both the “quality of life” and “measurements of analysis” domains were the least explored, with seven variables in each of them. Descriptions and examples of the variables identified in each domain are provided in Supplementary Table 3. The results of the analysis of confounding factors in the five eligible articles (6, 30, 33, 35, 36) are shown in Figure 7.
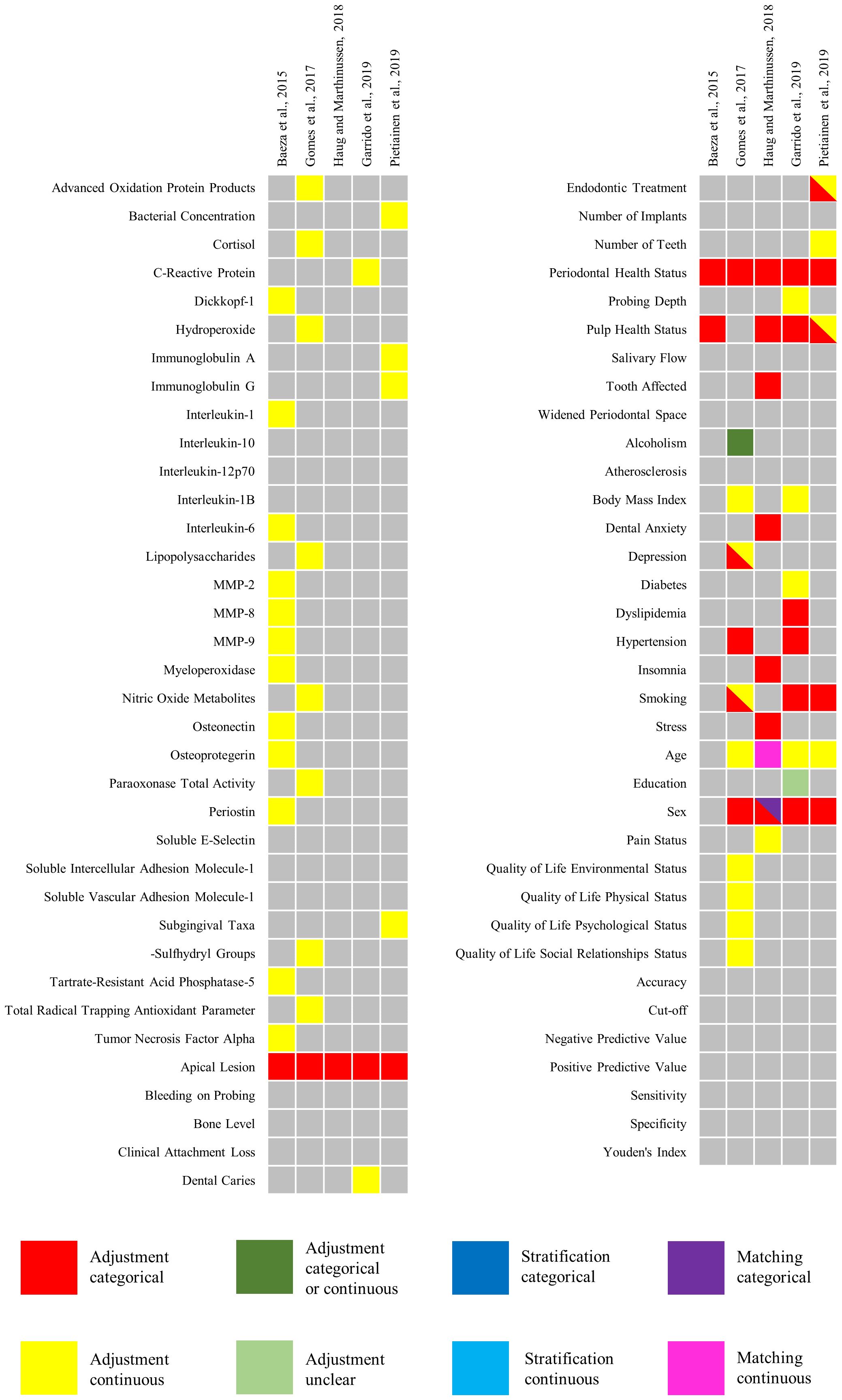
Figure 7 The results of the analysis of confounding factors in the eligible articles.
3.4 Level of evidence (GRADE tool)
The GRADE narrative analysis was used to assess the quality of evidence regarding changes in biomarker levels in the blood/serum, gingival crevicular fluid, and saliva in apical periodontitis (Table 5). The observational studies included in the analysis provided evidence of moderate certainty regarding the three outcomes. However, some issues were identified in some of the studies. Three studies (41, 43) reported problems with sample selection in the assessment of changes in blood and serum biomarkers. Comparability issues across groups have been reported for changes in gingival crevicular fluid biomarkers. Similarly, all four studies (6, 36, 42, 44) that assessed the changes in salivary biomarkers had comparability issues across groups.
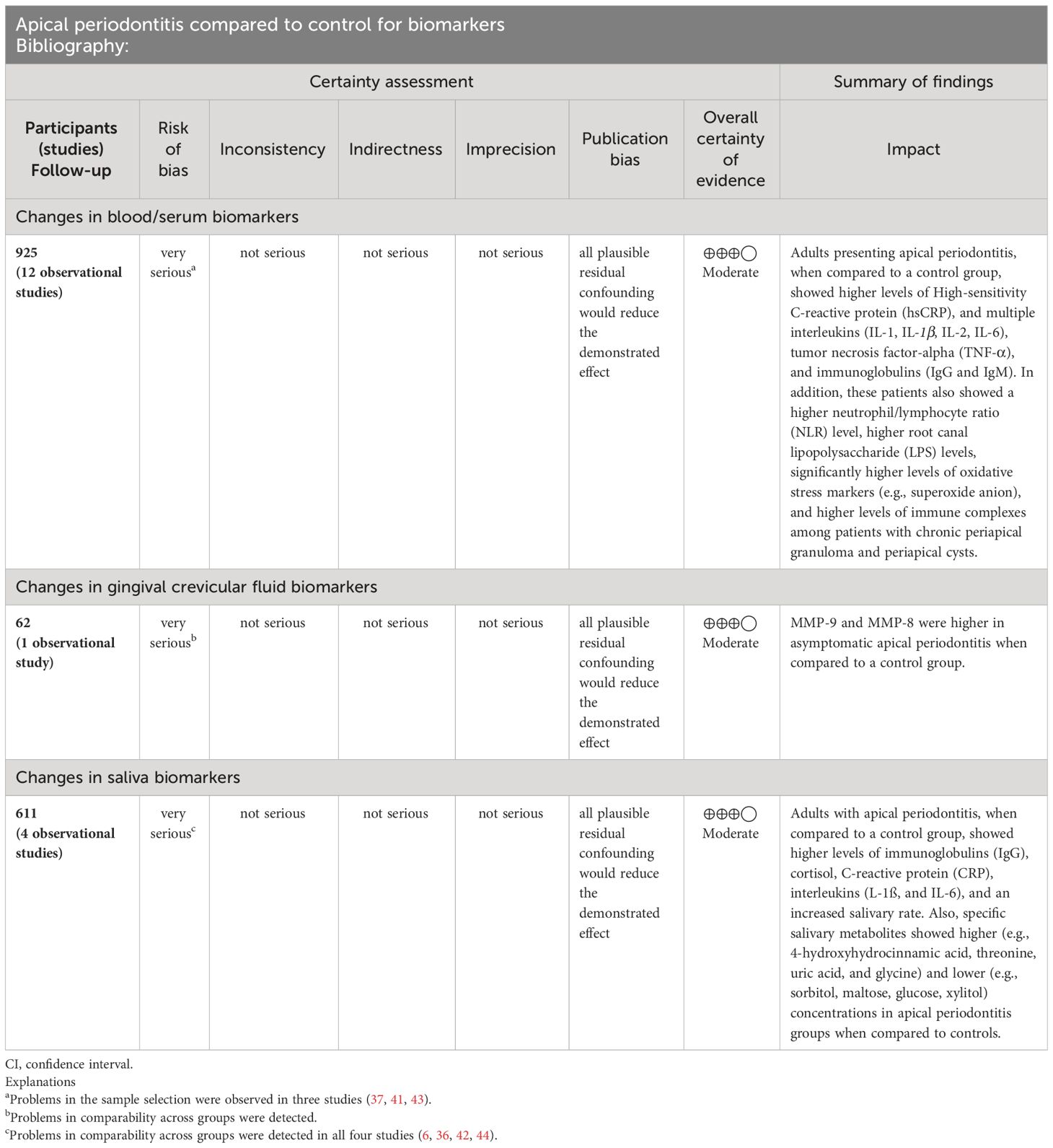
Table 5 The certainty of evidence: association between biomarkers and apical periodontitis.
4 Discussion
This systematic review revealed significant differences in the presence of biomarkers between patients with apical periodontitis compared to healthy individuals. This association was observed in 12 papers (6, 29–33, 35, 37–40, 44) included in this review, showing that systemic alterations may be triggered or aggravated in the presence of endodontic infection (45).
To consider systemic factors, only studies that evaluated biomarkers in body fluids were included because of recent advancements in the development of new methods for diagnosing and monitoring diseases by analyzing biomarkers in body fluids (46). Body fluids have a broad range of secretomes and various cell types that contribute to the analysis systems, increasing the spectrum of fluid-based analysis systems (47). Out of the 17 studies, 12 evaluated biomarkers in blood samples (29, 31–35, 37, 38, 39 40, 41, 41, 43), which are generally considered the best fluid to evaluate systemic processes through biomarkers (48, 49). Additionally, four studies evaluated biomarkers in saliva samples (6, 36, 42, 44). Saliva has become an alternative fluid to blood since salivary components are derived from both glands and blood owing to the high vascularity of salivary glands. Therefore, biomarkers in the saliva may reflect those in the blood (48). In addition, Baeza et al. (30) analyzed gingival crevicular fluid samples, which in a healthy state are considered a serum transudate as fluid from the surrounding capillaries that passes into the gingival sulcus and has a protein concentration similar to that of the interstitial fluid. However, in an inflamed state, it is considered an exudate with a protein concentration resembling to that of the serum (50).
All included studies had only clinical diagnoses available because they performed only radiographic examinations and clinical tests; however, a definitive diagnostic differentiation of the actual periapical status can only be attained by histopathology (51). In this review, 17 studies (6, 29–44.) diagnosed apical periodontitis by combining clinical and radiographic tests. This highlights the lack of adequate control for confounders in studies seeking an association between apical periodontitis and the systemic inflammatory burden.
Regarding the clinical diagnosis, most of studies included in this review specifically diagnosed asymptomatic apical periodontitis, which is a common type of periapical disease (29–31, 33–35, 37, 39, 41, 43, 44). However, other studies have focused on other types of periapical diseases such as symptomatic apical periodontitis (36, 38), acute apical abscess (44), and chronic apical abscess (42). In contrast, three studies did not specify a diagnosis other than “periapical lesion.”
Identifying the type of periapical disease is important, as it can affect the presentation of symptoms and the level of systemic involvement. For example, symptomatic infections occur when bacteria invade the periradicular tissues, leading to more noticeable symptoms (52). In contrast, asymptomatic apical periodontitis may not present with any symptoms. Additionally, different types of periapical diseases may lead to different levels of systemic involvement as endodontic infections can contribute to the overall oral infectious burden or lead to bacteremia stemming from endodontic treatment or acute abscesses. In addition, immunoglobulin levels can differ among different types of periapical lesions, with cysts exhibiting higher immunoglobulin levels than granulomas (53). Therefore, the specific diagnosis of periapical disease can play an important role in determining appropriate biomarkers to evaluate and interpret the results.
Thus, examining the biomarkers present in a systemic manner can help in the differential diagnosis of a specific type of periapical disease, as the cells and cytokines present tend to have a different predominance according to the type of lesion (5). Thus, the literature shows that the presence of T helper 2 (Th2) cells, Interleukin-1 (IL-1) and TNF-α, is more pronounced in periapical cysts, while T helper 1 (Th1) cells, Interleukin-10 (IL-10) and FoxP3 are more associated with the diagnosis of periapical granulomas (54, 55). In addition, IL-6, due to its pro-inflammatory character, is present in the earliest stages of development of symptomatic apical periodontitis (56). Furthermore, Interleukin-17 (IL-17) acts in the stimulation of Interleukin-8 (IL-8) production, which in turn aggravates the inflammatory process of apical periodontitis, and in the production of RANKL - which acts in the process of osteoclastogenesis, aggravating bone resorption; it is found mainly in cases of chronic apical periodontitis (57–59).
Biomarkers play a crucial role in providing valuable information regarding the status of periapical lesions, severity, degree of inflammation, and immune response within a clinical context. These biomarkers can be assessed in specimens such as blood, saliva, or tissue, offering insights into specific biological processes and distinguishing between the active and chronic stages of periapical lesions (60). Biomarkers linked to acute inflammation, such as proinflammatory interleukins (IL-1, IL-6, and IL-8) and C-reactive protein (CRP), are indicative of recent periapical lesions. Elevated levels of these biomarkers may suggest heightened and severe inflammation, providing valuable information about the severity of the lesion and the degree of the acute inflammatory response (61). Conversely, biomarkers associated with chronic inflammation can offer insight into persistent and long-standing periapical lesions. Elevated concentrations of pro-inflammatory cytokines, including interleukins and TNF-α, may signify intensified and active inflammation in these chronic lesions (62). The presence of heightened levels of immunoglobulins, such as IgG and IgA, indicates an adaptive immune response against chronic infection, potentially playing a role in immune defense mechanisms aimed at combating persistent inflammation (63). To substantiate these observations, comprehensive research involving the analysis of biomarker profiles in patients with varying stages of periapical lesions combined with clinical data and imaging assessments is warranted.
In this context, although the lesion size is not commonly considered in studies that evaluate correlations between endodontic disease and the presence of systemic damage, it is essential to assess this factor. Among the selected studies, 12 articles were not specific (6, 29, 31, 32, 34–36, 38, 39, 41–43), three observed lesions >3 mm (30, 33, 40), and two observed lesions <2 cm (37, 44). Matsuo et al. (64) evaluated the exudates collected from lesions and observed that the levels of IgG and IgA were directly proportional to the periapical lesion size. Although the selected studies did not directly evaluate the material collected from the lesion, this may indicate that lesion size can systemically interfere with biomarkers.
The presence of pro-inflammatory biomarkers, such as interleukins (e.g., IL-6 and IL-1β), in the bloodstream is positively correlated with the occurrence and intensity of systemic inflammation (39). The release of these pro-inflammatory cytokines indicates an activated immune response throughout the body in response to infections or chronic inflammatory conditions (5, 39). Elevated levels of systemic inflammatory markers like C-reactive protein (CRP) and tumor necrosis factor-alpha (TNF-α), are associated with the degree of systemic inflammation and may reflect the activity and severity of inflammation (5, 25). The presence of inflammatory biomarkers such as interleukins (e.g., IL-8), is positively correlated with the occurrence and intensity of local inflammation in saliva. These cytokines may indicate an inflammatory response at the site of origin, such as in oral infections or periodontal conditions (36, 65). Elevated levels of oxidative markers in the saliva, such as total peroxide concentration (TPX), myeloperoxidase (MPO), and 8-isoprostanes (8-EPI), suggest increased production of reactive oxygen species (ROS) and imply more intense and extensive inflammation associated with apical lesions (66). Conversely, the presence of immunoglobulins (IgA and IgG) in the saliva is associated with versatile adaptive immune responses against both local bacterial and host derived (6). Immunosuppressive biomarkers, like interleukin-10 (IL-10), show an inverse relationship with the severity of both systemic and local inflammations when detected in blood and saliva (36, 65). Higher IL-10 levels may signify an anti-inflammatory response and the modulation of the immune system (6).
In the presence of periapical infection, T cells, macrophages, and other cells produce chemicals that increase osteoclast production (RANKL expression). Proinflammatory cytokines (such as TNF-α, IL-6, IL-11, IL-17, and IL-1β) and chemical mediators (prostaglandins and bradykinins) are released. These substances accumulate at high concentrations in the bone and decrease osteoprotegerin expression in bone marrow stromal cells (59, 67). Among the selected studies, these and other biomarkers involved in periapical lesion pathogenesis were identified among the selected studies. Interleukins were found in nine studies (29–34, 36, 39, 41), followed by oxidative markers in five studies (30, 35, 37, 40, 44), immunoglobulins in four articles (6, 33, 38, 43), C-reactive protein in five articles each (33, 34, 36, 38, 41), and TNF-α in five studies (30–32, 34, 41) in addition to matrix metalloproteinase, lipoproteins, and lipids.
The limitations of the observational design of the eligible studies should be acknowledged. First, observational studies may be influenced by confounding factors, which can be mitigated by controlling known confounders using multivariate analyses (68). However, unknown confounders that are not controlled can significantly affect data interpretation, limiting the ability to make cause-and-effect statements from observational studies (10). Therefore, it is important to explicitly conduct and report adjustment analyses in the critical appraisal of eligible studies, and other steps serve as tools for analyzing the remaining studies (6, 30, 33, 35, 36).
While all the studies that remained in the analysis (6, 30, 33, 35, 36) mentioned the need for caution when interpreting their results, three studies (6, 33, 36) did not explicitly state this. This lack of explicit mention may result in a misinterpretation of the feasibility and generalizability of the study for the average reader. Although some studies (33, 35) have the aforementioned limitations, it is common for readers to focus solely on the final section. Therefore, it is important to include brief limitations and cautions in the study conclusions to provide a more complete understanding of the results.
There was a good proportion of controlled variables in the critically appraised studies (98/145), however, three identified domains were almost unexplored: “sociodemographic and socioeconomic,” “quality of life,” and “measurements of analysis.” Although these studies focused on sample analyses for biomarkers, these samples were collected from study participants and may have indirect or direct effects on the environmental factors of daily living. Additionally, laboratory tests have different aspects depending on the test used and the conditions under which they were performed. This supports the need to explicitly acknowledge more variables within the unexplored domains, which does not necessarily invalidate the results of each study. Notably, there can also be more confounding domains that are not yet identifiable, highlighting the need for caution when interpreting observational study results.
The quality of evidence for the association between biomarkers and apical periodontitis can be considered moderate using the GRADE approach, which implies that there are some limitations to the available evidence. This review included a substantial number of studies that showed significant differences in the presence of biomarkers between patients with and without apical periodontitis. However, there are some limitations, such as the reliance on clinical diagnosis rather than histopathology, which may have influenced the accuracy of the diagnosis. Moreover, these studies used different fluids to measure biomarkers, which may have affected the consistency of the results. Therefore, while describing the quality of evidence, it is important to provide a balanced assessment and highlight any limitations that could affect the interpretation of results.
Moreover, based on the findings of this systematic review, it is recommended for further research involves stratifying patients into those with apical periodontitis and those without. By comparing biomarker levels in these two groups separately, researchers can elucidate whether the observed associations are specific to apical periodontitis or if they are influenced by the presence of others concurrent oral disease, such as periodontal disease. This approach would improve the precision and validity of future investigations into the systemic impact of apical periodontitis. Additionally, to address the observed heterogeneity in the selected studies regarding biomarker types and sample sources (blood plasma, saliva, gingival crevicular fluid), future studies should adopt standardized methodologies to enhance result comparability and generalizability.
Furthermore, a recommendation to conduct studies comparing the levels of biomarkers before and after endodontic treatment can provide valuable insights into the systemic effects of this dental procedure. By assessing biomarker levels before the initiation of endodontic treatment and comparing them with post-treatment levels, researchers can evaluate the impact of the treatment on systemic inflammation and overall health. This comparison can help determine whether endodontic treatment leads to changes in systemic biomarker levels, indicating potential systemic benefits or risks associated with the procedure. Additionally, such studies can contribute to a better understanding of the systemic implications of endodontic treatment and guide clinical decision-making to optimize patient outcomes and overall health.
5 Conclusion
The reviewed studies demonstrate a correlation between the presence of biomarkers in systemic fluids and apical periodontitis. Biomarkers associated with inflammation, such as IL-1, IL-2, and IL-6, as well as oxidative markers, including nitric oxide, superoxide anions, and immunoglobulins IgG and IgM, have been identified during the disease. Nonetheless, there was considerable diversity in the methodologies and materials employed for analysis between the studies. Therefore, further clinical investigations with standardized evaluation parameters are necessary to provide more accurate knowledge of the association between biomarkers and apical periodontitis.
Nevertheless, although our review finds a non-causal association between AP and elevated systemic biomarker levels, it is crucial to acknowledge the interrelationship between oral health and general health. Apical periodontitis, as part of the oral inflammatory burden, may impact systemic health, particularly when concurrent with other oral inflammatory conditions such as periodontal disease. Therefore, we underscore the importance of implementing effective preventive and therapeutic strategies for periodontal diseases and AP, aiming not only at oral health but also at mitigating the risk of systemic complications arising from oral inflammation.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
JM-S: Conceptualization, Investigation, Methodology, Software, Writing – original draft. VC: Conceptualization, Investigation, Methodology, Software, Writing – original draft. DF: Conceptualization, Formal analysis, Investigation, Software, Supervision, Writing – review & editing. LB: Conceptualization, Formal analysis, Supervision, Validation, Visualization, Writing – review & editing. JM: Conceptualization, Formal analysis, Investigation, Supervision, Validation, Visualization, Writing – review & editing. CM: Investigation, Methodology, Software, Writing – review & editing. GM-V: Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – review & editing. NF: Conceptualization, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – review & editing. LP: Formal analysis, Methodology, Software, Supervision, Validation, Visualization, Writing – review & editing. LM: Conceptualization, Data curation, Formal analysis, Investigation, Software, Supervision, Validation, Visualization, Writing – review & editing. MM: Data curation, Formal analysis, Methodology, Supervision, Validation, Visualization, Writing – review & editing. RL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. RL is a Conselho Nacional de Desenvolvimento Cientifico e Tecnológico (CNPq) researcher who has earned grants numbered 312275/2021-8. This study was financed in part by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brazil (CAPES) – Finance Code 001. The APC was supported by the Federal University of Pará’s Pró-Reitoria de Pesquisa e Pós-graduaço (PROPESP-UFPA).
Acknowledgments
We would like to thank the Brazilian National Council for Scientific and Technological Development (CNPq) and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1366954/full#supplementary-material
References
1. Nair PR. Pathogenesis of apical periodontitis and the causes of endodontic failures. Crit Rev Oral Biol Med. (2004) 15:348–81. doi: 10.1177/154411130401500604
2. Segura-Egea JJ, Martín-González J, Castellanos-Cosano L. Endodontic medicine: connections between apical periodontitis and systemic diseases. Int Endodontic J. (2015) 48:933–51. doi: 10.1111/iej.12507
3. Peddis N, Musu D, Ideo F, Rossi-Fedele G, Cotti E. Interaction of biologic therapy with apical periodontitis and periodontitis: a systematic review. Aust Dental J. (2019) 64:122–34. doi: 10.1111/adj.12684
4. Nair PNR. On the causes of persistent apical periodontitis: a review. Int endodontic J. (2006) 39:249–81. doi: 10.1111/j.1365-2591.2006.01099.x
5. Braz-Silva PH, Bergamini ML, Mardegan AP, De Rosa CS, Hasseus B, Jonasson P. Inflammatory profile of chronic apical periodontitis: a literature review. Acta Odontol Scandinavica. (2019) 77:173–80. doi: 10.1080/00016357.2018.1521005
6. Pietiäinen M, Liljestrand JM, Akhi R, Buhlin K, Johansson A, Paju S, et al. Saliva and serum immune responses in apical periodontitis. J Clin Med. (2019) 8:889. doi: 10.3390/jcm8060889
7. Hernández-Ríos P, Pussinen PJ, Vernal R, Hernández M. Oxidative stress in the local and systemic events of apical periodontitis. Front Physiol. (2017) 8:869. doi: 10.3389/fphys.2017.00869
8. Dessaune Neto N, Porpino M, Antunes H, Rodrigues R, Perez AR, Pires FR, et al. Pro-inflammatory and anti-inflammatory cytokine expression in post-treatment apical periodontitis. J Appl Oral sci: Rev FOB. (2018) 26:e20170455. doi: 10.1590/1678-7757-2017-0455
9. Georgiou AC, Crielaard W, Armenis I, de Vries R, van der Waal SV. Apical periodontitis is associated with elevated concentrations of inflammatory mediators in peripheral blood: a systematic review and meta-analysis. J endodontics. (2019) 45:1279–95. doi: 10.1016/j.joen.2019.07.017
10. Dekkers OM, Vandenbroucke JP, Cevallos M, Renehan AG, Altman DG, Egger M. COSMOS-E: guidance on conducting systematic reviews and meta-analyses of observational studies of etiology. PloS Med. (2019) 16:e1002742. doi: 10.1371/journal.pmed.1002742
11. Peinado BRR, Frazão DR, Bittencourt LO, de Souza-Rodrigues RD, Vidigal MTC, da Silva DT, et al. Is obesity associated with taste alterations? a systematic review. Front Endocrinol. (2023) 14:1167119. doi: 10.3389/fendo.2023.1167119
12. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-analyses. Ottawa, Ontario, Canada: Ottawa Health Research Institute (2009).
13. Hemkens LG, Ewald H, Naudet F, Ladanie A, Shaw JG, Sajeev G, et al. Interpretation of epidemiologic studies very often lacked adequate consideration of confounding. J Clin Epidemiol. (2018) 93:94–102. doi: 10.1016/j.jclinepi.2017.09.013
14. Wallach JD, Serghiou S, Chu L, Egilman AC, Vasiliou V, Ross JS, et al. Evaluation of confounding in epidemiologic studies assessing alcohol consumption on the risk of ischemic heart disease. BMC Med Res Method. (2020) 20:1–10. doi: 10.1186/s12874-020-0914-6
15. Chen J, Chen Z, Zhang L. Zhonghua kou qiang yi xue za zhi = Zhonghua kouqiang yixue zazhi. Chin J stomatol. (1998) 33:155–7.
16. Brekalo Pršo I, Kocjan W, Simić H, Brumini G, Pezelj-Ribarić S, Borcić J, et al. Tumor necrosis factor-alpha and interleukin 6 in human periapical lesions. Mediators Inflammation. (2007) 2007:38210. doi: 10.1155/2007/38210
17. Araujo-Pires AC, Francisconi CF, Biguetti CC, Cavalla F, Aranha AM, Letra A, et al. Simultaneous analysis of T helper subsets (Th1, Th2, Th9, Th17, Th22, Tfh, Tr1 and Tregs) markers expression in periapical lesions reveals multiple cytokine clusters accountable for lesions activity and inactivity status. J Appl Oral sci: Rev FOB. (2014) 22:336–46. doi: 10.1590/1678-775720140140
18. Toledo AON, Couto AMD, Madeira MFM, Caldeira PC, Queiroz-Junior CM, Aguiar MCF. Cytokines and chemokines associated with Treg/Th17 response in chronic inflammatory periapical disease. Braz Oral Res. (2019) 33:e093. doi: 10.1590/1807-3107bor-2019.vol33.0093
19. Burgener B, Ford AR, Situ H, Fayad MI, Hao JJ, Wenckus CS, et al. Biologic markers for odontogenic periradicular periodontitis. J endodontics. (2010) 36:1307–10. doi: 10.1016/j.joen.2010.04.018
20. Dezerega A, Madrid S, Mundi V, Valenzuela MA, Garrido M, Paredes R, et al. Pro-oxidant status and matrix metalloproteinases in apical lesions and gingival crevicular fluid as potential biomarkers for asymptomatic apical periodontitis and endodontic treatment response. J Inflammation. (2012) 9:1–9. doi: 10.1186/1476-9255-9-8
21. Vidal F, Fontes TV, Marques TV, Gonçalves LS. Association between apical periodontitis lesions and plasmatic levels of C-reactive protein, interleukin 6 and fibrinogen in hypertensive patients. Int endodontic J. (2016) 49:1107–15. doi: 10.1111/iej.12567
22. Nunez N, Erdogan O, Casey SM, Hernandez R, Tan S, Gibbs JL. Elevated cytokine levels in gingival crevicular fluid of teeth with apical periodontitis. J endodontics. (2023) 49:657–63. doi: 10.1016/j.joen.2023.03.010
23. Mundi Burgos V, Dezerega Piwonka A, Osorio Alfaro C, Dutzan Muñoz N, Franco Martínez ME, Ortega Pinto AV, et al. Inmunodetección de metaloproteinasas de matriz extracelular (MMPs)-2, -9, -13 y -14 en lesiones apicales asociadas con periodontitis apical asintomática. Rev clínica periodoncia implantol y rehabilitación Oral. (2011) 4:17–21. doi: 10.4067/S0719-01072011000100004
24. Brosco RE. Análise comparativa dos níveis de proteína C-reativa altamente sensível entre indivíduos portadores e não portadores de lesão periapical crônica. Doctoral dissertation, Universidade de São Paulo (2009).
25. Bakhsh A, Moyes D, Proctor G, Mannocci F, Niazi SA. The impact of apical periodontitis, non-surgical root canal retreatment and periapical surgery on serum inflammatory biomarkers. Int Endodontic J. (2022) 55:923–37. doi: 10.1111/iej.13786
26. Janani K, Teja KV, AjithA P, Sandhya R. Assessment of sCD14 levels in patients with endodontic pathology requiring root canal treatment. Braz dent Sci. (2022) 25:1–5. doi: 10.4322/bds.2022.e2809
27. Matsushita K, Tajima T, Tomita K, Abeyama K, Maruyama I, Takada H, et al. Inflammatory cytokine production and specific antibody responses against possible causative bacteria in patients with multilesional periapical periodontitis. J endodontics. (1998) 24:817–21. doi: 10.1016/S0099-2399(98)80009-5
28. Stys LPA, Böttcher DE, Scarparo RK, Gonçalves Waltrick SB, de Figueiredo JAP, Gomes MS, et al. Serum levels of inflammatory markers and HbA1c in patients with type 2 diabetes and apical periodontitis: Preliminary findings. Aust endodontic J. (2022) 48:105–15. doi: 10.1111/aej.12569
29. Abdolsamadi HR, Vahedi M, Esmaeili F, Nazari S, Abdollahzadeh S. Serum interleukin-6 as a serologic marker of chronic periapical lesions: a case-control study. J Dental Res Dental Clinics Dental Prospects. (2008) 2:43. doi: 10.5681/joddd.2008.009
30. Baeza M, Garrido M, Hernández-Ríos P, Dezerega A, García-Sesnich J, Strauss F, et al. Diagnostic accuracy for apical and chronic periodontitis biomarkers in gingival crevicular fluid: an exploratory study. J Clin periodontol. (2016) 43:34–45. doi: 10.1111/jcpe.12479
31. Cotti E, Dessì C, Piras A, Flore G, Deidda M, Madeddu C, et al. Association of endodontic infection with detection of an initial lesion to the cardiovascular system. J endodontics. (2011) 37:1624–9. doi: 10.1016/j.joen.2011.09.006
32. Bergandi L, Giuggia B, Alovisi M, Comba A, Silvagno F, Maule M, et al. Endothelial Dysfunction Marker Variation in Young Adults with Chronic Apical Periodontitis before and after Endodontic Treatment. J endodontics. (2019) 45:500–6. doi: 10.1016/j.joen.2019.01.018
33. Garrido M, Cárdenas AM, Astorga J, Quinlan F, Valdés M, Chaparro A, et al. Elevated systemic inflammatory burden and cardiovascular risk in young adults with endodontic apical lesions. J endodontics. (2019) 45:111–5. doi: 10.1016/j.joen.2018.11.014
34. Georgiou AC, Twisk JWR, Crielaard W, Ouwerling P, Schoneveld AH, van der Waal SV. The influence of apical periodontitis on circulatory inflammatory mediators in peripheral blood: A prospective case-control study. Int endodontic J. (2023) 56:130–45. doi: 10.1111/iej.13854
35. Gomes C, Martinho FC, Barbosa DS, Antunes LS, Póvoa HCC, Baltus THL, et al. Increased root canal endotoxin levels are associated with chronic apical periodontitis, increased oxidative and nitrosative stress, major depression, severity of depression, and a lowered quality of life. Mol Neurobiol. (2018) 55:2814–27. doi: 10.1007/s12035-017-0545-z
36. Rethnam Haug S, Cuida Marthinussen M. Acute dental pain and salivary biomarkers for stress and inflammation in patients with pulpal or periapical inflammation. J Oral Facial Pain Headache. (2019) 33:227–33. doi: 10.11607/ofph.2007
37. Inchingolo F, Marrelli M, Annibali S, Cristalli MP, Dipalma G, Inchingolo AD, et al. Influence of endodontic treatment on systemic oxidative stress. Int J Med Sci. (2014) 11:1. doi: 10.7150/ijms.6663
38. Sirin DA, Ozcelik F, Uzun C, Ersahan S, Yesilbas S. Association between C-reactive protein, neutrophil to lymphocyte ratio and the burden of apical periodontitis: a case-control study. Acta Odontol Scandinavica. (2019) 77:142–9. doi: 10.1080/00016357.2018.1522447
39. Sirin DA, Ozcelik F, Ersahan S, Pence HH. The importance of inflammatory biomarkers, IL-6 and PAPP-A, in the evaluation of asymptomatic apical periodontitis. Odontology. (2021) 109:250–8. doi: 10.1007/s10266-020-00534-8
40. Minczykowski A, Woszczyk M, Szczepanik A, Lewandowski L, Wysocki H. Hydrogen peroxide and superoxide anion production by polymorphonuclear neutrophils in patients with chronic periapical granuloma, before and after surgical treatment. Clin Oral investig. (2001) 5:6–10. doi: 10.1007/s007840000095
41. Kimak A, Strycharz-Dudziak M, Bachanek T, Kimak E. Lipids and lipoproteins and inflammatory markers in patients with chronic apical periodontitis. Lipids Health Dis. (2015) 14:1–8. doi: 10.1186/s12944-015-0156-5
42. Montis N, Cotti E, Noto A, Fattuoni C, Barberini L. Salivary metabolomics fingerprint of chronic apical abscess with sinus tract: A pilot study. TheScientificWorldJournal. (2019) 2019:3162063. doi: 10.1155/2019/3162063
43. Torabinejad M, Theofilopoulos AN, Ketering JD, Bakland LK. Quantitation of circulating immune complexes, immunoglobulins G and M, and C3 complement component in patients with large periapical lesions. Oral Surg Oral Med Oral Pathol. (1983) 55:186–90. doi: 10.1016/0030-4220(83)90177-9
44. Vengerfeldt V, Mändar R, Saag M, Piir A, Kullisaar T. Oxidative stress in patients with endodontic pathologies. J Pain Res. (2017) 10:2031–40. doi: 10.2147/JPR.S141366
45. Cintra LTA, Gomes MS, da Silva CC, Faria FD, Benetti F, Cosme-Silva L, et al. Evolution of endodontic medicine: a critical narrative review of the interrelationship between endodontics and systemic pathological conditions. Odontology. (2021) 109:741–69. doi: 10.1007/s10266-021-00636-x
46. Broza YY, Zhou X, Yuan M, Qu D, Zheng Y, Vishinkin R, et al. Disease detection with molecular biomarkers: from chemistry of body fluids to nature-inspired chemical sensors. Chem Rev. (2019) 119:11761–817. doi: 10.1021/acs.chemrev.9b00437
47. Properzi F, Logozzi M, Fais S. Exosomes: the future of biomarkers in medicine. Biomarkers Med. (2013) 7:769–78. doi: 10.2217/bmm.13.63
48. Williamson S, Munro C, Pickler R, Grap MJ, Elswick RK. Comparison of biomarkers in blood and saliva in healthy adults. Nurs Res Pract. (2012) 2012. doi: 10.1155/2012/246178
49. Bellagambi FG, Petersen C, Salvo P, Ghimenti S, Franzini M, Biagini D, et al. Determination and stability of N-terminal pro-brain natriuretic peptide in saliva samples for monitoring heart failure. Sci Rep. (2021) 11:1–9. doi: 10.1038/s41598-021-92488-2
50. Papagerakis P, Zheng L, Kim D, Said R, Ehlert AA, Chung KKM, et al. Saliva and gingival crevicular fluid (GCF) collection for biomarker screening. Odontogenesis. (2019), 549–62. doi: 10.1007/978-1-4939-9012-2_41
51. Ricucci D, Rôças IN, Hernández S, Siqueira JF Jr. “True” Versus “Bay” Apical cysts: clinical, radiographic, histopathologic, and histobacteriologic features. J Endodontics. (2020) 46:1217–27. doi: 10.1016/j.joen.2020.05.025
52. Siqueira JF, Rôças IN. Present status and future directions: Microbiology of endodontic infections. Int Endodontic J. (2021) 55(Suppl 3):512–30. doi: 10.1111/iej.13677
53. Pulver WH, Taubman MA, Smith DJ. Immune components in human dental periapical lesions. Arch Oral Biol. (1978) 23:435–43. doi: 10.1016/0003-9969(78)90074-2
54. Fukada SY, Silva TA, Garlet GP, Rosa AL, Da Silva JS, Cunha FDQ. Factors involved in the T helper type 1 and type 2 cell commitment and osteoclast regulation in inflammatory apical diseases. Oral Microbiol Immunol. (2009) 24:25–31. doi: 10.1111/j.1399-302X.2008.00469.x
55. Francisconi CF, Vieira AE, Biguetti CC, Glowacki AJ, Trombone APF, Letra A, et al. Characterization of the protective role of regulatory T cells in experimental periapical lesion development and their chemoattraction manipulation as a therapeutic tool. J endodontics. (2016) 42:120–6. doi: 10.1016/j.joen.2015.09.022
56. Suzuki T, Kumamoto H, Ooya K, Motegi K. Immunohistochemical analysis of CD1a-labeled Langerhans cells in human dental periapical inflammatory lesions–correlation with inflammatory cells and epithelial cells. Oral Dis. (2001) 7:336–43. doi: 10.1034/j.1601-0825.2001.00722.x
57. Čolić M, Lukić A, Vučević D, Milosavljević P, Majstorović I, Marjanović M, et al. Correlation between phenotypic characteristics of mononuclear cells isolated from human periapical lesions and their in vitro production of Th1 and Th2 cytokines. Arch Oral Biol. (2006) 51:1120–30. doi: 10.1016/j.archoralbio.2006.05.003
58. Naufel AO, Aguiar MCF, Madeira FM, Abreu LG. Treg and Th17 cells in inflammatory periapical disease: a systematic review. Braz Oral Res. (2017) 31. doi: 10.1590/1807-3107bor-2017.vol31.0103
59. Bracks IV, Armada L, Gonçalves LS, Pires FR. Distribution of mast cells and macrophages and expression of interleukin-6 in periapical cysts. J Endodontics. (2014) 40:63–8. doi: 10.1016/j.joen.2013.09.037
60. Ebersole JL, Nagarajan R, Akers D, Miller CS. Targeted salivary biomarkers for discrimination of periodontal health and disease (s). Front Cell infect Microbiol. (2015) 5:62. doi: 10.3389/fcimb.2015.00062
61. Ansar W, Ghosh S, Ansar W, Ghosh S. Inflammation and inflammatory diseases, markers, and mediators: Role of CRP in some inflammatory diseases. Biol C react Protein Health Dis. (2016), 67–107. doi: 10.1007/978-81-322-2680-2_4
62. Kany S, Vollrath JT, Relja B. Cytokines in inflammatory disease. Int J Mol Sci. (2019) 20:6008. doi: 10.3390/ijms20236008
63. Hansen IS, Baeten DL, den Dunnen J. The inflammatory function of human IgA. Cell Mol Life Sci. (2019) 76:1041–55. doi: 10.1007/s00018-018-2976-8
64. Matsuo T, Nakanishi T, Ebisu S. Immunoglobulins in periapical exudates of infected root canals: correlations with the clinical findings of the involved teeth. Dental Traumatol. (1995) 11:95–9. doi: 10.1111/j.1600-9657.1995.tb00466.x
65. Hajishengallis G, Chavakis T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat Rev Immunol. (2021) 21:426–40. doi: 10.1038/s41577-020-00488-6
66. Georgiou AC, Ulloa PC, Van Kessel GMH, Crielaard W, Van der Waal SV. Reactive oxygen species can be traced locally and systemically in apical periodontitis: A systematic review. Arch Oral Biol. (2021) 129:105167. doi: 10.1016/j.archoralbio.2021.105167
67. Zupan J, Jeras M, Marc J. Osteoimmunology and the influence of pro-inflammatory cytokines on osteoclasts. Biochem Med. (2013) 23:43–63. doi: 10.11613/BM.2013.007
Keywords: apical periodontitis, biomarkers, inflammatory markers, systemic biomarkers, and endodontic infection
Citation: Matos-Sousa JM, Chemelo VS, Frazão DR, Bittencourt LO, Moura JDM, Mesquita CM, Marañón-Vásquez G, Fagundes NCF, Paranhos LR, Maia LC, Monteiro MC and Lima RR (2024) Is there any association between the presence of biomarkers and apical periodontitis? A systematic review. Front. Immunol. 15:1366954. doi: 10.3389/fimmu.2024.1366954
Received: 07 January 2024; Accepted: 15 April 2024;
Published: 22 May 2024.
Edited by:
Francisco W. G. Paula-Silva, University of São Paulo, BrazilReviewed by:
Krzysztof Guzik, Jagiellonian University, PolandNadya Marouf, Hamad Medical Corporation, Qatar
Copyright © 2024 Matos-Sousa, Chemelo, Frazão, Bittencourt, Moura, Mesquita, Marañón-Vásquez, Fagundes, Paranhos, Maia, Monteiro and Lima. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafael Rodrigues Lima, cmFmYWxpbWFAdWZwYS5icg==