 Massimo Martino1,2
Massimo Martino1,2 Gaetana Porto1,2Giorgia Policastro1,2
Gaetana Porto1,2Giorgia Policastro1,2 Caterina Alati2,3
Caterina Alati2,3 Barbara Loteta1,2Maria Caterina Micó1,2Clizia Argiró1,2Maria Altomonte2,4Tiziana Moscato1,2Demetrio Labate2,5Vincenzo Dattola2,6
Barbara Loteta1,2Maria Caterina Micó1,2Clizia Argiró1,2Maria Altomonte2,4Tiziana Moscato1,2Demetrio Labate2,5Vincenzo Dattola2,6 Carmelo Massimiliano Rao2,7Francesca Cogliandro1,2
Carmelo Massimiliano Rao2,7Francesca Cogliandro1,2 Filippo Antonio Canale1,2Virginia Naso1,2Gianfranco Filippelli8Antonino Iaria9
Filippo Antonio Canale1,2Virginia Naso1,2Gianfranco Filippelli8Antonino Iaria9 Martina Pitea1,2*
Martina Pitea1,2*- 1Stem Cell Transplantation and Cellular Therapies Unit (CTMO), Department of Hemato-Oncology and Radiotherapy, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli,”, Reggio Calabria, Italy
- 2CAR-T Multidisciplinary Team, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli,”, Reggio Calabria, Italy
- 3Hematology Unit, Department of Hemato-Oncology and Radiotherapy, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, Reggio Calabria, Italy
- 4Pharmacy Unit, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, Reggio Calabria, Italy
- 5ICU Unit, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, Reggio Calabria, Italy
- 6Neurology Unit, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, Reggio Calabria, Italy
- 7Cardiology Unit, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, Reggio Calabria, Italy
- 8Oncology Department, Hospital of Paola, Cosenza, Italy
- 9Oncology Unit, Melito Porto Salvo, Reggio Calabria, Italy
1 Introduction
Chimeric antigen receptor-modified T-cell (CAR-T) is a clinical and technological revolution (1, 2). The more advanced developments that led to the commercialization of the first products, have identified as a target the molecule CD19, expressed in all leukemia acute lymphoblastic leukemia (ALL) (3) and in Non-Hodgkin Lymphoma (NHL) (4), such as diffuse (D) large B-cell lymphoma (LBCL) (5), follicular lymphoma (FL) (6), mantle-cel lymphoma (MCL) (7) and the molecule B-cell maturation antigen (BCMA), expresses in multiple myeloma (MM) (8, 9). This approach has opened a new page in medicine because we have moved from the drug, understood as an active ingredient packaged and ready to be taken, to a highly personalized therapy. Results from CAR-T trials are showing unprecedented outcomes in patients with no other treatment options beyond palliative care (10).
As cellular products, CAR T cells are associated with unique toxicities, and cytokine release syndrome (CRS), immune effector cell-associated neurotoxicity syndrome (ICANS), and cytopenias have been a challenge that has involved a major commitment to the entire scientific community (11). With a growing experience, management of these toxicities is an evolving field, and the current management strategies include continuous monitoring of the patient in the first thirty days post-infusion, rapid detection, and accurate intervention with supportive care, anti-cytokine or corticosteroid therapy. Other toxicities, rarer but described, are an infusion reaction, tumor lysis syndrome, anaphylaxis and immunogenicity, B-cell aplasia and hypogammaglobulinemia, infections and hemophagocytic lymphohistiocytosis/macrophage activation syndrome (12–14).
Data on late toxicities of CAR T cells, including effects on the immune system, such as a new occurrence or exacerbation of neurologic or autoimmune disorders, and secondary malignancies require longer observation periods. The possible development of second cancers is a price to pay for many “lifesaving” treatments, in this setting of patients. The increased risk of second malignancies is related to a combination of factors, including molecular background, host immunological status, genetic predisposition, and chemotherapy administered (15). Second cancers constitute 15 to 20% of all cancer diagnoses in the cancer registries, and the risk of a second cancer is significantly higher than in the general population, between 3- and 10-fold (16).
Although a follow-up of 15 years has been requested as part of the marketing authorization of commercially available CAR T cells, the European Medicines Agency announced on January 12, 2024, that its Pharmacovigilance Risk Assessment Committee has beginning a review of data on secondary malignancies related to T-cells for approved CAR-T therapies (17).
In this paper we evaluated publications pertaining to follow-up updates of clinical trials, specifically presented at the 2023 ASH congress, with a focus on incidence of second cancers (Table 1).
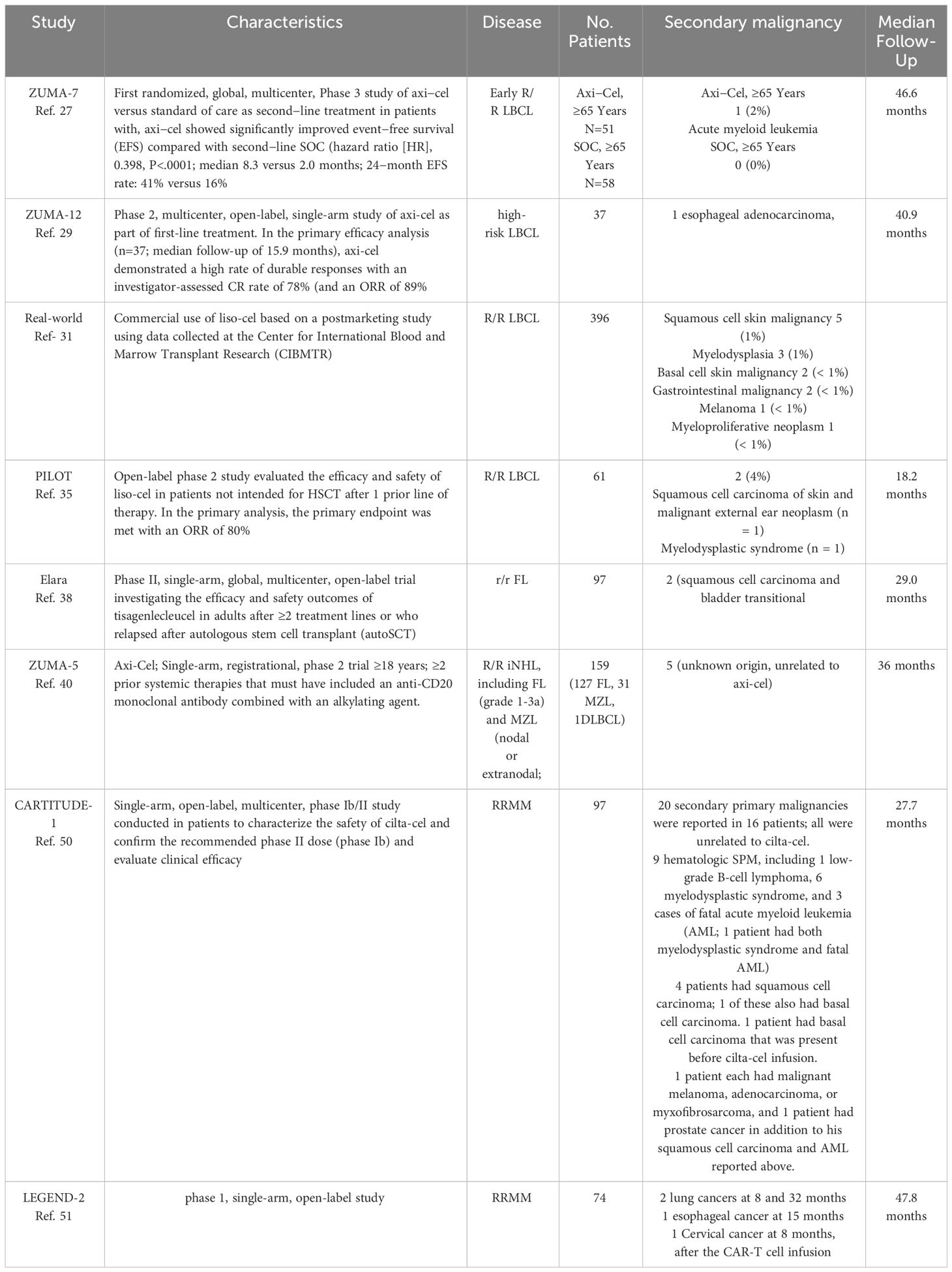
Table 1 Description of second malignancies in studies with updated follow-up.
1.1 ALL
Anti-CD19 CAR-T cell therapy is approved for patients up to 25 years of age and for adult affect by ALL based on the ELIANA (tisagenlecleucel-tisa-cel) (18) and ZUMA-3 trial (brexucabtagene autoleucel – brex-cel) (19). Most trials of CAR-T cells in relapsed/refractory (RR) ALL demonstrate impressive response rates, with >70% of patients achieving complete remission (CR) (20). Given the poor prognosis, there appears to be no evidence of secondary malignancy in this setting, where we emphasize there are no therapeutic alternatives.
1.2 LBCL
Anti-CD19 CAR-Ts, axicabtagene ciloleucel (axi-cel) (21), tisa-cel (22), and lisocaptagene maraleucel (liso-cel) (23), showed impressive activity in the third and higher treatment line in a non-comparative clinical trial.
ZUMA−1 is a multicenter, single−arm, registrational phase 1/2 study of axi−cel in patients with refractory LBCL after ≥2 lines of therapy (24). Long−term results from ZUMA−1 demonstrated sustained overall survival (OS), with a median of 25.8 months and a 5−year estimate of 43%. Initial assessments in ZUMA−1 suggested axi−cel may be curative for a subset of patients (25, 26).
In the primary analysis of the pivotal JULIET trial of tisa-cel, the best ORR was 52% and the CR rate was 40% in adult patients with RR LBCL (22). At a median follow-up of 40.3 months, tisa-cel continued to show durable activity (27). The safety profile analysis did not show any secondary tumor, and no deaths were attributed to tisa-cel.
Liso-cel demonstrated significant efficacy with a manageable safety profile as third-line or later treatment in patients with RR LBCL (23). After 2-year follow-up, the ORR was 73% and CR rate was 53% with no new safety signals (28).
Axi-cel and liso-cel showed a significant improvement in PFS and a strong trend in OS in two phase III clinical studies in high-risk RR LBCL compared with salvage therapy (ST) followed by autologous stem cell transplantation (ASCT) (29–32). Kersten et al. reported an updated efficacy and safety results from the primary OS analysis among ZUMA-7 patients aged ≥65 and ≥70 years (33). No new treatment-related deaths occurred. One patient died for an acute myeloid leukemia.
ZUMA-12 is a phase 2, multicenter, single-arm study of axi-cel as part of first-line treatment in patients with high-risk LBCL (34). In the updated analysis with a median follow-up of ≥40 months (35), axi-cel confirmed a high rate of durable responses and no new safety signals. There were 8 deaths due to progressive disease (n=5) and other causes not related to axi-cel (1 COVID-19, 1 esophageal adenocarcinoma, 1 septic shock on Days 350, 535, and 287 post axi-cel infusion, respectively). Two of the 8 deaths (1 progressive disease and 1 esophageal adenocarcinoma) occurred after the primary analysis.
Current guidelines indicate that CAR-T is the standard of care in DLBCL patients with refractory disease, early relapse after first-line chemotherapy, and in third line of treatment (36).
Crombie et. presented the results of patients who were followed in the CIBMTR Cellular Therapy Registry after infusion with commercial liso-cel for the treatment of R/R LBCL (37). Of the 396 patients evaluated, 14 patients developed a second malignancy (5 squamous cell skin malignancy; 3 myelodysplasia; 2 basal cell skin malignancy; 2 a gastrointestinal malignancy; 1 melanoma; 1 myeloproliferative neoplasm, respectively.
In LBCL patients not intended to receive ASCT after failure of first-line therapy outcomes have been poor (38, 39). The phase 2 PILOT study evaluated the efficacy and safety of liso-cel in this setting (40). Sehgal et al. reported the final analysis after 24 months of follow-up or study discontinuation (41). There were no new safety signals. Two patients developed a second primary malignancy (squamous cell carcinoma of skin and malignant external ear neoplasm, n = 1; myelodysplastic syndrome, n = 1).
Ghilardi et al. reported a T cell lymphoma occurring 3 months after CAR-T infusion for non-Hodgkin B cell lymphoma (42). The T cell clone was identified at low levels in the blood before CAR T infusion and in lung cancer. Moreover, the authors evaluated the risk of secondary primary malignancy after commercial CAR-T therapy in 449 patients treated in a cancer center in the United States. Sixty-teen patients (3.6%) had a secondary primary malignancy, and the 5-year incidence was 2.3% for hematological malignancies, and 15.2% for solid tumor. Overall, one case of T cell lymphoma was observed, suggesting a very low risk of this disease after CAR T.
1.3 FL
Tisa-cel is approved for adults with R/R FL in the ≥3 rd-line setting (43). The primary analysis of the Phase II ELARA trial reported high response rates and excellent safety profile in extensively pretreated patients with r/r FL (44). Findings from a longer-term update of the ELARA trial continue to demonstrate high response rates and durable remissions with a favorable safety profile (45). No new safety signals were reported. Two patients experienced a secondary malignancy during this longer-term follow-up (squamous cell carcinoma and bladder transitional cell carcinoma). Additionally, 3 new deaths occurred during this updated 2-year follow-up period (progressive disease, n=1; serious adverse events, n=2 (urothelial bladder carcinoma and graft-vs-host disease following allogeneic SCT). None of the malignancies or deaths were considered related to study treatment.
Beyond the potential efficacy of CAR-T in FL, axi-cel results in a high number of durable responses in the third and higher treatment line in a non-comparative clinical trial (46). Axi−cel was tested on the ZUMA−5 multicenter, single−arm, Phase 2 study, in patients with R/R indolent non−Hodgkin lymphoma (NHL), including FL and marginal zone lymphoma (MZL) (47). After a median follow−up of ≥3 years, median PFS was 40.2 months in patients with FL and not reached in those with MZL (25). After ≥4 years median follow−up in ZUMA−5, axi−cel demonstrated continued durable responses and long−term survival in patients with RR iNHL (47). After the 3-year data cutoff date, 1 patient with FL developed a myelodysplastic syndrome, and 1 patient with MZL an acute myeloid leukemia.
1.4 MCL
Brexu-cel is an autologous anti-CD19 CAR T-cell therapy approved in adults with R/R MCL following ≥2 prior therapies, including ibrutinib a BTKi (48). After three years in ZUMA-2, brexu-cel demonstrated an ORR of 91%, and a CR rate of 68%. ZUMA-18 is an expanded access study of brexu-cel for the treatment of patients with R/R MCL, including BTKi-naive patients who received ≥ 1 prior therapy following ZUMA-2 enrollment completion. Goy et al. reported the primary analysis of ZUMA-18 and the 4-year follow-up of ZUMA-2 (49). Consistent with ZUMA-2 findings, brexu-cel demonstrated a high level of efficacy, with an ORR of 87%.
1.5 MM
Newer treatment options for patients with triple-class RRMM include classes of drugs targeting BCMA, among which are the CAR-T cells idecabtagene vicleucel (ide-cel) and ciltacabtagene autoleucel (cilta-cel) (50).
The first commercially available CAR-T therapy was ide-cel, approved for patients with RR disease after at ‗three lines of therapies, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 antibody (51, 52). In the phase 2 KarMMa trial, at a median follow-up of 24.8 months, patients who received ide-cel showed an ORR of 73% and a CR or better rate of 33% (53). The phase III KarMMa-3 randomized controlled trial results were published comparing ide-cel with SOC (54). No second cancers have been reported.
Cilta-cel was the second CAR-T cell therapy to enter the market for MM and was approved by the FDA and the EMA for the same indications as ide-cel (54–57). At the 28-month median follow-up, a total of 20 secondary tumors had occurred in CARTITUDE-1 and were all considered unrelated to cilta-cel. Six cases of skin cancers were reported, including squamous cell carcinoma (n = 4) and basal cell carcinoma (n = 2). Ten cases of hematologic secondary tumors were reported in ten patients, including low-grade B-cell lymphoma (n = 1), myelodysplastic syndrome (n = 6), and l acute myeloid leukemia (n = 3). One case each of prostate cancer, malignant melanoma, adenocarcinoma, and myxofibrosarcoma also occurred. The accumulation of late-onset malignancies is not unexpected with long-term follow-up of patients with RR MM, many of whom have received subsequent anti-myeloma therapy. Initially referred to as LCAR-B38M, this construct was first studied in humans in a phase I trial (58). Four-year follow-up results were recently published, representing the most extended follow-up to date of any CAR-T therapy for MM. Second primary malignancies occurred in 4 patients [lung cancer (n = 2) and 1 case each of esophageal and cervical cancer].
1.6 Genotoxicity and secondary malignancies
The use of retroviral and lentiviral vectors for lymphocyte transduction results in the so-called risk of insertional mutagenesis (59–61).
Although this risk, no genotoxicity of gene transfer into differentiated cells, including T cells, has been reported, and. no vectors-related transformational events in more than 500 cumulative follow-up years of patients treated with engineered T cells have been observed (62). Pre-existing mutations in patients receiving CAR-T cell therapies can result in secondary malignancies in some cases (63). A recently published study showed a clonal hematopoiesis before treatment in 86% of patients receiving CAR-T cells, among those with prolonged cytopenias (64).
The risk of second malignancies in the context of CAR-T therapies needs to be evaluated against other available therapeutic approaches (65). The development of secondary malignancies is demonstrated after radiotherapy and/or chemotherapy treatment. The genotoxicity of these treatments is a well-known long-term side that results in a predisposition to the development of neoplasms (66).
Increased risk of second cancer after stem cell transplantation (SCT) ranges from 8 to 28% (67). Incidence correlates with the type of therapy given before and after SCT, the age of the patient, and the type of transplantation. Most of these secondary malignancies are myeloid-derived.
2 Discussion
CAR-Ts have revolutionized the treatment of some hematologic cancers. The development of a second cancer was considered a significant potential risk at the time of approval and is included in the risk management plan. Close monitoring was provided, with a requirement to conduct long-term follow-up studies on safety and efficacy and to submit safety update reports. The reported incidence of second cancers is negligible given the global number of people worldwide who have received CAR-T therapy. It should not be forgotten that the alternative to CAR-Ts is chemotherapy combined with cytotoxic agents with non-negligible secondary malignancy rates (16, 68–72). The true nature and frequency of secondary malignancies are yet to be confirmed. Important patient characteristics such as age, prior immune status, whether the CAR gene is present in the tumor, the landscape of genetic mutations carried by patients in these cases, and other clinical features such as the time from CAR T infusion to the development of T cell lymphoma, are unknown. Only expanded use in thousands of people can give us an accurate estimate of the risks. However, we must be cautious not to over-emphasize standard practice and not to create alarmism about therapies that save many lives. Indeed, it should be remembered that there have been very few cases of secondary cancers compared with thousands of patients treated and who had no other treatment options. The concern is related to genetically modifying T cells taken from the patient. We use a viral vector that carries a gene inside the T cell to prepare CAR-T cells. The virus integrates into the DNA in only a partially controlled way, so there is a risk that it could damage genes crucial for cell proliferation and differentiation. These genes, when altered, can generate tumor development. This potential risk, known as insertional mutagenesis (73), is therefore linked to the very fact of genetically modifying a cell and has already been observed in other gene therapies, for example, in the treatment of immunodeficiencies (74). The regulator’s website states that the EMA is thoroughly investigating the content of some reports of T-cell neoplasms in patients previously treated with CAR-T cells. The initial approvals of CAR-Ts were subject to the fulfillment of post-marketing requirements, which require observational safety studies to be conducted to calculate the risk of treatment-related adverse events; thus, these are safety-focused trials to be conducted on an expanded cohort of people and include an assessment of the risk of secondary malignancies occurring. It is now well known that patients receiving CAR-Ts will need to continue to be monitored within follow-up programs because the occurrence of new, potentially severe adverse events can also be realized over the long term. Nonetheless, it should be noted that correlation with treatment must be proven beyond reasonable doubt, and this is a process that takes time and effort. It must be ascertained that other factors are not contributing and that the disease is not related, instead, to the heavy chemotherapy regimens or frail state of the treated cancer patients. For this reason, extreme caution is needed, both in analyzing reports and communicating their results, to avoid generating unfounded fears to fuel mistrust of therapies now considered lifesaving.
Author contributions
MMa: Investigation, Supervision, Writing – original draft, Writing – review & editing. GaP: Investigation, Writing – original draft. GiP: Investigation, Writing – original draft. CAl: Investigation, Writing – original draft. BL: Investigation, Methodology, Writing – original draft. MMi: Investigation, Methodology, Writing – original draft. CAr: Investigation, Writing – original draft. MA: Investigation, Writing – original draft. TM: Investigation, Writing – original draft. DL: Supervision, Writing – original draft. VD: Methodology, Supervision, Writing – original draft. MR: Methodology, Supervision, Visualization, Writing – review & editing. FCo: Methodology, Supervision, Visualization, Writing – original draft. FCa: Investigation, Supervision, Writing – original draft. VN: Investigation, Supervision, Writing – review & editing. GF: Methodology, Supervision, Writing – original draft. AI: Supervision, Visualization, Writing – review & editing. MP: Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Joy R, Phair K, O'Hara R, Brady D. Recentadvances and current challenges in CAR-T cell therapy. Biotechnol Lett. (2024) 46:115–26. doi: 10.1007/s10529-023-03461-0
2. Abbasi S, Totmaj MA, Abbasi M, Hajazimian S, Goleij P, Behroozi J, et al. (CAR-T) cells: Novelcell therapy for hematologicalmalignancies. Cancer Med. (2023) 12:7844–58. doi: 10.1002/cam4.5551
3. Martino M, Alati C, Canale FA, Musuraca G, Martinelli G, Cerchione CA. Review of Clinical Outcomes of CAR T-Cell Therapies for B-Acute LymphoblasticLeukemia. Int J Mol Sci. (2021) 22:2150. doi: 10.3390/ijms22042150
4. Martino M, Canale FA, Naso V, Porto G, Gerace D, Allegra A. Do CAR-T and AllogeneicStem Cell TransplantBothHave a Place in LymphoidNeoplasms? Int J Mol Sci. (2023) 24:1045. doi: 10.3390/ijms24021045
5. Martino M, Canale FA, Porto G, Verduci C, Utano G, Policastro G, et al. Integrating CAR-T cell therapy into the management of DLBCL: whatwe are learning. Expert OpinBiolTher. (2023) 23:1277–85. doi: 10.1080/14712598.2023.2292634
6. Testa U, D'Alò F, Pelosi E, Castelli G, Leone G. CAR-T Cell Therapy for FollicularLymphomas. Mediterr J HematolInfectDis. (2024) 16:e2024012. doi: 10.4084/MJHID.2024.012
7. Benevolo Savelli C, Clerico M, Botto B, Secreto C, Cavallo F, Dellacasa C, et al. Chimeric Antigen Receptor-T Cell Therapy for Lymphoma: New Settings and Future Directions. Cancers (Basel). (2023) 16:46. doi: 10.3390/cancers16010046
8. Martino M, Canale FA, Alati C, Vincelli ID, Moscato T, Porto G, et al. CART-Cell Therapy: Recent Advances and New Evidence in Multiple Myeloma. Cancers (Basel). (2021) 13:2639. doi: 10.3390/cancers13112639
9. Martino M, Paviglianiti A. An update on B-cell maturation antigen-targeted therapies in Multiple Myeloma. Expert Opin Biol Ther. (2021) 21:1025–34. doi: 10.1080/14712598.2021.1872540
10. Kim SJ, Yoon SE, Kim WS. Current Challenges in Chimeric Antigen Receptor T-cell Therapy in Patients With B-cell Lymphoid Malignancies. Ann Lab Med. (2024) 44:210–21. doi: 10.3343/alm.2023.0388
11. Schubert ML, Schmitt M, Wang L, Ramos CA, Jordan K, Müller-Tidow C, et al. Side-effect management of chimeric antigen receptor (CAR) T-cell therapy. Ann Oncol. (2021) 32:34–48. doi: 10.1016/j.annonc.2020.10.478
12. Howard SC, Trifilio S, Gregory TK, Baxter N, McBride A. Tumor lysis syndrome in the era of novel and targeted agents in patients with hematologic malignancies: a systematic review. Ann Hematol. (2016) 95:563–73. doi: 10.1007/s00277-015-2585-7
13. Cruz CR, Hanley PJ, Liu H, Torrano V, Lin YF, Arce JA, et al. Adverse events following infusion of T cells for adoptive immunotherapy: a 10-year experience. Cytotherapy. (2010) 12:743–9. doi: 10.3109/14653241003709686
14. Kochenderfer JN, Dudley ME, Feldman SA, Wilson WH, Spaner DE, Maric I, et al. B-cell depletion and remissions of malignancy along with cytokine-associated toxicity in a clinical trial of anti-CD19 chimeric-antigen-receptor-transduced T cells. Blood. (2012) 119:2709–20. doi: 10.1182/blood-2011-10-384388
15. Tadmor T, Liphshitz I, Silverman B, Polliack A. Incidence and epidemiology of non-Hodgkin lymphoma and risk of second malignancy among 22 466 survivors in Israel with 30 years of follow-up. Hematol Oncol. (2017) 35:599–607. doi: 10.1002/hon.2302
16. Demoor-Goldschmidt C, de Vathaire F. Review of risk factors of secondary cancers among cancer survivors. Br J Radiol. (2019) 92:20180390. doi: 10.1259/bjr.20180390
17. . Available online at: https://www.ema.europa.eu/en/news/meeting-highlights-pharmacovigilance-risk-assessment-committee-prac-8-11-january-2024.
18. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N Engl J Med. (2018) 378:439–48. doi: 10.1056/NEJMoa1709866
19. Shah BD, Ghobadi A, Oluwole OO, Logan AC, Boissel N, Cassaday RD, et al. KTE-X19 for relapsed or refractory adult B-cell acute lymphoblastic leukaemia: phase 2 results of the single-arm, open-label, multicentre ZUMA-3 study. Lancet. (2021) 398:491–502. doi: 10.1016/S0140-6736(21)01222-8
20. Mohty M, Gautier J, Malard F, Aljurf M, Bazarbachi A, Chabannon C, et al. CD19 chimeric antigen receptor-T cells in B-cell leukemia and lymphoma: current status and perspectives. Leukemia. (2019) 33:2767–78. doi: 10.1038/s41375-019-0615-5
21. Locke FL, Ghobadi A, Jacobson CA, Miklos DB, Lekakis LJ, Oluwole OO, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol. (2019) 20:31–42. doi: 10.1016/S1470-2045(18)30864-7
22. Schuster SJ, Bishop MR, Tam CS, Waller EK, Borchmann P, McGuirk JP, et al. Tisagenlecleucel in adult relapsed or refractory diffuse large B-cell lymphoma. N Engl J Med. (2019) 380:45–56. doi: 10.1056/NEJMoa1804980
23. Abramson JS, Palomba ML, Gordon LI, Lunning MA, Wang M, Arnason J, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. (2020) 396:839–52. doi: 10.1016/S0140-6736(20)31366-0
24. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Miklos DB, Jacobson CA, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. N Engl J Med. (2017) 377:2531–44. doi: 10.1056/NEJMoa1707447
25. Neelapu SS, Jacobson CA, Ghobadi A, Miklos DB, Lekakis LJ, Oluwole OO, et al. Five-year follow-up of ZUMA-1 supports the curative potential of axicabtagene ciloleucel in refractory large B-cell lymphoma. Blood. (2023) 141:2307–15. doi: 10.1182/blood.2022018893
26. Neelapu SS, Jacobson CA, Ghobadi A, Miklos DB, Lekakis LJ, Spooner C, et al. Curative Potential of Axicabtagene Ciloleucel (Axi-Cel): An Exploratory Long-Term Survival Assessment in Patients with Refractory Large B-Cell Lymphoma from ZUMA-1. Blood. (2023) 142:4864. doi: 10.1182/blood-2023-174288
27. Schuster SJ, Tam CS, Borchmann P, Worel N, McGuirk JP, Holte H, et al. Long-term clinical outcomes of tisagenlecleucel in patients with relapsed or refractory aggressive B-cell lymphomas (JULIET): a multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. (2021) 22:1403–15. doi: 10.1016/S1470-2045(21)00375-2
28. Abramson JS, Palomba ML, Gordon LI, Lunning MA, Wang ML, Arnason JE, et al. Two-year follow-up of lisocabtagene maraleucel in relapsed or refractory large B-cell lymphoma in TRANSCEND NHL 001. Blood. (2023) 143(5):404–16. doi: 10.1182/blood.2023020854
29. Locke FL, Jacobson C, Perales MA, Kersten MJ, Westin JR. Primary analysis of ZUMA−7: a phase 3 randomized trial of axicabtagene ciloleucel (Axi-Cel) versus standard−of−care therapy in patients with relapsed/refractory large B-cell lymphoma. Blood. (2021) 138:2. doi: 10.1182/blood-2021-148039
30. Kamdar M, Solomon SR, Arnason JE, Johnston PB, Glass B, Bachanova V, et al. Lisocabtagene maraleucel (liso-cel), a CD19-directed chimeric antigen receptor (CAR) T cell therapy, versus standard of care (SOC) with salvage chemotherapy (CT) followed by autologous stem cell transplantation (ASCT) as second-line (2L) treatment in patients (Pts) with relapsed or refractory (R/R) large B-cell lymphoma (LBCL): results from the randomized phase 3 transform study. Blood. (2021) 138:91. doi: 10.1182/blood-2021-147913
31. Locke FL, Miklos DB, Jacobson CA, Perales MA, Kersten MJ, Oluwole OO, et al. Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. N Engl J Med. (2022) 386:640–54. doi: 10.1056/NEJMoa2116133
32. Westin JR, Locke FL, Dickinson M, Ghobadi A, Elsawy M, van Meerten T, et al. Safety and Efficacy of Axicabtagene Ciloleucel versus Standard of Care in Patients 65 Years of Age or Older with Relapsed/Refractory Large B-Cell Lymphoma. Clin Cancer Res. (2023) 29:1894–905. doi: 10.1158/1078-0432.CCR-22-3136
33. Kersten MJ, Farooq U, Rapoport AP, Locke FL, Leslie LA, Ghobadi A, et al. Improved Overall Survival with AxicabtageneCiloleucel Vs Standard of Care in Second-Line Large B-Cell LymphomaAmong the Elderly: A Subgroup Analysis of ZUMA-7. Blood. (2023) 142:1761. doi: 10.1182/blood-2023-173873
34. Neelapu SS, Dickinson M, Munoz J, Ulrickson ML, Thieblemont C, Oluwole OO, et al. Axicabtageneciloleucel as first-line therapy in high-risk large B-cell lymphoma: the phase 2 ZUMA-12 trial. NatMed. (2022) 28:735–42. doi: 10.1038/s41591-022-01731-4
35. Chavez JC, Dickinson M, Munoz JL, Ulrickson ML, Thieblemont C, Oluwole OO, et al. 3-Year Analysis of ZUMA-12: A Phase 2 Study of AxicabtageneCiloleucel (Axi-Cel) As First-Line Therapy in Patients with High-Risk Large B-Cell Lymphoma (LBCL). Blood. (2023) 142:894. doi: 10.1182/blood-2023-174510
36. Snowden JA, Sánchez-Ortega I, Corbacioglu S, Basak GW, Chabannon C, de la Camara R, et al. Indications for haematopoietic cell transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe, 2022. Bone Marrow Transplant. (2022) 57:1217–39. doi: 10.1038/s41409-022-01691-w
37. Crombie JL, Nastoupil LJ, Andreadis C, Isufi I, Hunter B, Winter A. Multicenter, Real-World Study in Patients with R/R Large B-Cell Lymphoma (LBCL) Who Received Lisocabtagene Maraleucel (liso-cel) in the United States (US). Blood. (2023) 142:104. doi: 10.1182/blood-2023-180242
38. Crump M, Neelapu SS, Farooq U, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. (2017) 130:1800–8. doi: 10.1182/blood-2017-11-817775
39. Nowakowski GS, Blum KA, Kahl BS, Friedberg JW, Baizer L, Little RF. Beyond RCHOP: A Blueprint for Diffuse Large B Cell Lymphoma Research. J Natl Cancer Inst. (2016) 108:djw257. doi: 10.1093/jnci/djw257
40. Sehgal A, Hoda D, Riedell PA, Ghosh N, Hamadani M, Hildebrandt GC, et al. Lisocabtagene maraleucel as second-line therapy in adults with relapsed or refractory large B-cell lymphoma who were not intended for haematopoietic stem cell transplantation (PILOT): an open-label, phase 2 study. Lancet Oncol. (2022) 23:1066–77. doi: 10.1016/S1470-2045(22)00339-4
41. Sehgal AR, Hoda D, Riedell PA, Ghosh N, Hamadani M, Hildebrandt G, et al. Lisocabtagene Maraleucelas Second-Line Therapy for R/R Large B-Cell Lymphoma in Patients Not Intended for Hematopoietic Stem Cell Transplant: Final Analysis of the Phase 2 PILOT Study. Blood. (2023) 142:105. doi: 10.1182/blood-2023-180952
42. Ghilardi G, Fraietta JA, Gerson JN, Van Deerlin VM, Morrissette JJD, Caponetti GC, et al. T cell lymphoma and secondary primary malignancy risk after commercial CAR T cell therapy. Nat Med. (2024) 30(4):984–9. doi: 10.1038/s41591-024-02826-w
43. Fowler NH, Dickinson M, Dreyling M, Martinez-Lopez J, Kolstad A, Butler J, et al. Tisagenlecleucel in adultrelapsed or refractoryfollicularlymphoma: the phase 2 ELARA trial. NatMed. (2022) 28(2):325–32. doi: 10.1038/s41591-021-01622-0
44. Schuster SJ, Dickinson M, Dreyling M, Martinez-Lopez J, Kolstad A, Butler J, et al. IBCL-195: Primaryanalysis of the phase 2 ELARA trial: Tisagenlecleucelefficacy and safety in adultpatients with relapsed/refractoryfollicularlymphoma (r/r FL). ClinLymphomaMyelomaLeuk. (2021) 21:S403–4. doi: 10.1016/S2152-2650(21)01911-X
45. Dreyling M, Fowler NH, Dickinson M, Martínez-López J, Kolstad A, Butler J, et al. Durable Response After Tisagenlecleucel in Adults With Relapsed/Refractory Follicular Lymphoma: ELARA Trial Update. Blood. (2024). doi: 10.1182/blood.2023021567
46. Jacobson CA, Chavez JC, Sehgal A, William BM, Munoz J, Salles GA, et al. Outcomes in ZUMA-5 with axicabtagene ciloleucel (axi-cel) in patients (pts) with relapsed/refractory (R/R) indolent non-Hodgkin lymphoma (iNHL) who had the high-risk feature of progression within 24 months from initiation of first anti-CD20–containing chemoimmunotherapy (POD24). J Clin Oncol. (2021) 39:7515–. doi: 10.1200/JCO.2021.39.15_suppl.7515
47. Jacobson CA, Chavez JC, Sehgal AR, William BM, Munoz J, Salles G, et al. Axicabtagene ciloleucel in relapsed or refractory indolent non-Hodgkin lymphoma (ZUMA-5): a single-arm, multicentre, phase 2 trial. Lancet Oncol. (2022) 23:91–103. doi: 10.1016/S1470-2045(21)00591-X
48. Wang M, Munoz J, Goy A, Locke FL, Jacobson CA, Hill BT, et al. Three-Year Follow-Up of KTE-X19 in Patients With Relapsed/Refractory Mantle Cell Lymphoma, Including High-Risk Subgroups, in the ZUMA-2 Study. J Clin Oncol. (2023) 41:555–67. doi: 10.1200/JCO.21.02370
49. Goy A, Jacobson CA, Flinn IW, Hill BT, Weng W-K. Outcomes of Patients with Relapsed/Refractory Mantle Cell Lymphoma Treated with BrexucabtageneAutoleucel in ZUMA-2 and ZUMA-18, an Expanded Access Study. Blood. (2023) 142:106. doi: 10.1182/blood-2023-174273
50. Martin TG, Madduri D, Pacaud L, Usmani SZ. Cilta-cel, a BCMA-targeting CAR-T therapy for heavily pretreated patients with relapsed/refractory multiple myeloma. Future Oncol. (2023) 19:2297–311. doi: 10.2217/fon-2022-1317
51. Celgene Corporation, a Bristol-Myers Squibb Company. ABECMA® (idecabtagene vicleucel) prescribing information). Available online at: https://packageinserts.bms.com/pi/ (Accessed 10 October 2022).
52. Bristol-Myers Squibb Pharma. ABECMA® (idecabtagene vicleucel) Summary of Product Characteristics). Available online at: https://www.ema.europa.eu/en/documents/product-information/abecma-epar-product-information_en.pdf (Accessed 10 October 2022).
53. Anderson LD Jr, Munshi N, Shah N, Jagannath S, Berdeja JG, Lonial S, et al. Idecabtagene vicleucel (ide-cel, bb2121), a BCMA-directed CAR T therapy, in relapsed and refractory multiple myeloma: updated KarMMa results. J Clin Oncol. (2021) 39:8016. doi: 10.1200/JCO.2021.39.15_suppl.8016
54. Rodriguez-Otero P, Ailawadhi S, Arnulf B, Patel K, Cavo M, Nooka AK, et al. Ide-cel or standard regimens in relapsed and refractory multiple myeloma. N Engl J Med. (2023) 388:1002–14. doi: 10.1056/NEJMoa2213614
55. Janssen Biotech, Inc and Legend Biotech. CARVYKTI® (ciltacabtagene autoleucel) prescribing information). Available online at: https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/CARVYKTI-pi.pdf (Accessed 10 October 2022).
56. Janssen Biotech, Inc and Legend Biotech. CARVYKTI® (ciltacabtagene autoleucel) Summary of Product Characteristics). Available online at: https://www.ema.europa.eu/en/documents/product-information/carvykti-epar-product-information_en.pdf (Accessed 10 October 2022).
57. Martin T, Usmani SZ, Berdeja JG, Agha M, Cohen AD, Hari P, et al. Ciltacabtagene autoleucel, an anti-B-cell maturation antigen chimeric antigen receptor T-cell therapy, for relapsed/refractory multiple myeloma: CARTITUDE-1 2 years follow-up. J Clin Oncol. (2023) 41:1265–74. doi: 10.1200/JCO.22.00842
58. Zhao W-H, Wang B-Y, Chen L-J, Fu W-J, Xu J, Liu J, et al. Four-year follow-up of LCAR-B38M in relapsed or refractory multiple myeloma: a phase I, single-arm, open-label, multicenter study in China (LEGEND-2). J Hematol Oncol. (2022) 15:86. doi: 10.1186/s13045-022-01301-8
59. Hacein-Bey-Abina S, von Kalle C, Schmidt M, Le Deist F, Wulffraat N, McIntyre E, et al. A serious adverse event after successful gene therapy for X-linked severe combined immunodeficiency. N Engl J Med. (2003) 348:255–6. doi: 10.1056/NEJM200301163480314
60. Astrakhan A, Sather BD, Ryu BY, Khim S, Singh S, Humblet-Baron S, et al. Ubiquitous high-level gene expression in hematopoietic lineages provides effective lentiviral gene therapy of murine Wiskott-Aldrich syndrome. Blood. (2012) 119:4395–407. doi: 10.1182/blood-2011-03-340711
61. Schwarzwaelder K, Howe SJ, Schmidt M, Brugman MH, Deichmann A, Glimm H, et al. Gammaretrovirus-mediated correction of SCID-X1 is associated with skewed vector integration site distribution in vivo. Clin Invest. (2007) 117(8):2241–9. doi: 10.1172/JCI31661
62. Cornetta K, Duffy L, Turtle CJ, Jensen M, Forman S, Binder-Scholl G, et al. Absence of Replication-Competent Lentivirus in the Clinic: Analysis of Infused T Cell Products. Mol Ther. (2018) 26:280–8. doi: 10.1016/j.ymthe.2017.09.008
63. Lamble AJ, Myers RM, Taraseviciute A, John S, Yates B, Steinberg SM, et al. Preinfusion factors impacting relapse immunophenotype following CD19 CAR T cells. Blood Adv. (2023) 7:575–85. doi: 10.1182/bloodadvances.2022007423
64. Hamilton MP, Sworder B, Alig S, Good Z, Boegeholz J, Schroers-Martin J, et al. CAR19 Therapy Drives Expansion of Clonal Hematopoiesis and Associated Cytopenias. Transplant Cell Ther. (2024) 30:S3–4. doi: 10.1016/j.jtct.2023.12.023
65. Levine BL, Pasquini MC, Connolly JE, Porter DL, Gustafson MP, Boelens JJ, et al. Unanswered questions following reports of secondary malignancies after CAR-T cell therapy. Nat Med. (2024) 30:338–41. doi: 10.1038/s41591-023-02767-w
66. Meadows AT, Friedman DL, Neglia JP, Mertens AC, Donaldson SS, Stovall M, et al. Second neoplasms in survivors of childhood cancer: findings from the Childhood Cancer Survivor Study cohort. J Clin Oncol. (2009) 27:2356–62. doi: 10.1200/JCO.2008.21.1920
67. Brown JR, Yeckes H, Friedberg JW, Neuberg D, Kim H, Nadler LM, et al. Increasing incidence of late second malignancies after conditioning with cyclophosphamide and total-body irradiation and autologous bone marrow transplantation for non-Hodgkin's lymphoma. J Clin Oncol. (2005) 23:2208–14. doi: 10.1200/JCO.2005.05.158
68. Swerdlow AJ, Higgins CD, Smith P, Cunningham D, Hancock BW, Horwich A, et al. Second cancer risk after chemotherapy for Hodgkin’s lymphoma: a collaborative British cohort study. J Clin Oncol. (2011) 29:4096–104. doi: 10.1200/JCO.2011.34.8268
69. Davies SM. Therapy-related leukemia associated with alkylating agents. Med Pediatr Oncol. (2001) 36:536–40. doi: 10.1002/mpo.1126
70. Morton LM, Onel K, Curtis RE, Hungate EA, Armstrong GT. The rising incidence of second cancers: patterns of occurrence and identification of risk factors for children and adults. Am Soc Clin Oncol Educ Book. (2014) 34:e57–67. doi: 10.14694/EdBook_AM.2014.34.e57
71. Tukenova M, Diallo I, Hawkins M, Guibout C, Quiniou E, Pacquement H, et al. Long-term mortality from second malignant neoplasms in 5-year survivors of solid childhood tumors: temporal pattern of risk according to type of treatment. Cancer Epidemiol Biomarkers Prev. (2010) 19:707–15. doi: 10.1158/1055-9965.EPI-09-1156
72. Gilbert ES, Curtis RE, Hauptmann M, Kleinerman RA, Lynch CF, Stovall M, et al. Stomach cancer following hodgkin lymphoma, testicular cancer and cervical cancer: a pooled analysis of three international studies with a focus on radiation effects. Radiat Res. (2017) 187:186–95. doi: 10.1667/RR14453.1
73. Baum C. Insertional mutagenesis in gene therapy and stem cell biology. Curr Opin Hematol. (2007) 14:337–42. doi: 10.1097/MOH.0b013e3281900f01
Keywords: car-t, follow-up, second cancer, malignancies, therapy
Citation: Martino M, Porto G, Policastro G, Alati C, Loteta B, Micó MC, Argiró C, Altomonte M, Moscato T, Labate D, Dattola V, Rao CM, Cogliandro F, Canale FA, Naso V, Filippelli G, Iaria A and Pitea M (2024) Effectiveness of CAR-T treatment toward the potential risk of second malignancies. Front. Immunol. 15:1384002. doi: 10.3389/fimmu.2024.1384002
Received: 08 February 2024; Accepted: 24 April 2024;
Published: 02 May 2024.
Edited by:
Marcos De Lima, The Ohio State University, United StatesReviewed by:
Kotaro Miyao, Anjo Kosei Hospital, JapanCopyright © 2024 Martino, Porto, Policastro, Alati, Loteta, Micó, Argiró, Altomonte, Moscato, Labate, Dattola, Rao, Cogliandro, Canale, Naso, Filippelli, Iaria and Pitea. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martina Pitea, bWFydGluYS5waXRlYUBvc3BlZGFsZXJjLml0