 Vilde Øverlien Dåstøl1,2*
Vilde Øverlien Dåstøl1,2* Kristine Løkås Haftorn1
Kristine Løkås Haftorn1 Hamid Khoshfekr Rudsari1
Hamid Khoshfekr Rudsari1 Piotr Pawel Jaholkowski3,4
Piotr Pawel Jaholkowski3,4 Ketil Størdal5,6Siri Eldevik Håberg7,8
Ketil Størdal5,6Siri Eldevik Håberg7,8 Clarice R. Weinberg9
Clarice R. Weinberg9 Lisa G. Rider10
Lisa G. Rider10 Ole A. Andreassen2,4,11
Ole A. Andreassen2,4,11 Anne Lise Brantsæter12
Anne Lise Brantsæter12 Ida Henriette Caspersen1,7
Ida Henriette Caspersen1,7 Helga Sanner1,13
Helga Sanner1,13- 1Department of Rheumatology, Oslo University Hospital, Oslo, Norway
- 2Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway
- 3Center for Precision Psychiatry, Division of Mental Health and Addiction, Oslo University Hospital, and Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 4KG Jebsen Centre for Neurodevelopmental Disorders, University of Oslo and Oslo University Hospital, Oslo, Norway
- 5Department of Pediatric Research, Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway
- 6Department of Pediatric and Adolescent Medicine, Oslo University Hospital, Oslo, Norway
- 7Centre for Fertility and Health, Norwegian Institute of Public Health, Oslo, Norway
- 8Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway
- 9Biostatistics and Computational Biology Branch, National Institute of Environmental Health Sciences, Research Triangle Park, NC, United States
- 10Environmental Autoimmunity Group, Clinical Research Branch, National Institute of Environmental Health Sciences, National Institutes of Health, Bethesda, MD, United States
- 11Center for Precision Psychiatry, Division of Mental Health and Addiction, Oslo University Hospital, Oslo, Norway
- 12Department of Food Safety and Centre for Sustainable Diets, Norwegian Institute of Public Health, Oslo, Norway
- 13Oslo New University College, Oslo, Norway
Objectives: Juvenile idiopathic arthritis (JIA) originates from a complex interplay between genetic and environmental factors. We investigated the association between seafood intake and dietary contaminant exposure during pregnancy and JIA risk, to identify sex differences and gene-environment interactions.
Methods: We used the Norwegian Mother, Father, and Child Cohort Study (MoBa), a population-based prospective pregnancy cohort (1999–2008). JIA patients were identified through the Norwegian Patient Registry, with remaining mother-child pairs serving as controls. We assessed maternal seafood intake and dietary contaminants typically found in seafood using a food frequency questionnaire completed during pregnancy, mainly comparing high (≥90th percentile, P90) vs low (<P90) intake. Multivariable logistic regression calculated adjusted odds ratios (aOR), including sex-stratification analyses. A polygenic risk score (PRS) for JIA was used in a subsample to assess gene-environment interactions.
Results: We identified 217 JIA patients and 71,884 controls. High vs low maternal intake of lean/semi-oily fish was associated with JIA (aOR 1.51, 95% CI 1.02-2.22), especially among boys (aOR 2.13, 95% CI 1.21-3.75). A significant gene-environment interaction was observed between total fish intake and PRS, with high fish intake associated with JIA primarily in those with low PRS (p<0.03). We found no associations between high vs low exposure to other types of seafood or environmental contaminants and JIA.
Conclusions: We found a modestly increased risk of JIA associated with high intake of lean/semi-oily fish during pregnancy, not explained by estimated exposure to dietary contaminants. Our data suggest a more pronounced association in children with a lower genetic predisposition for JIA.
1 Introduction
Juvenile idiopathic arthritis (JIA), the most common inflammatory rheumatic disease of childhood, manifests as arthritis before the age of 16 years which persists more than six weeks, and without an apparent cause. It consists of seven heterogeneous subgroups, reflecting the complex interplay between genetic predisposition and environmental influences that contribute to the diverse clinical manifestations (1). Known genetic variants are estimated to account for 13-25% of the risk for JIA, while the remaining risk is attributed to environmental factors and their interaction with genetic predisposition (1, 2). Limited high-quality data and modest sample sizes have constrained prior attempts to pinpoint environmental risk and protective factors (3). Furthermore, despite JIA being more prevalent in girls than in boys (4), few studies have investigated this sex disparity, which is important for understanding the underlying pathomechanisms of disease development.
Diet is an example of an environmental factor that remains underexplored in relation to JIA risk (3). Results from a Swedish prospective cohort study showed that fish intake more than once per week during pregnancy and the first year of life was associated with increased risk of JIA, which was mainly attributed to high heavy metal exposure (5).
Among the environmental contributors, heavy metals like mercury and cadmium, and persistent organic pollutants (POPs), have emerged as potential triggers of autoimmunity (6–9). Mercury is associated with subclinical autoimmunity in humans through the production of autoantibodies and cytokines (10–13), while in individuals with a genetic predisposition, cadmium may exacerbate autoimmunity (14) and increase the risk of rheumatoid arthritis (RA) (15, 16). Furthermore, exposure to POPs has also been linked to autoimmune diseases, with research suggesting increased risk of celiac disease, especially in girls (8), and of RA (17).
Diet serves as a major source of these contaminants (18), with seafood being a significant contributor to mercury (19) and shellfish contributing to cadmium exposure (20). Individuals consuming high amounts of seafood are also at greater risk of POPs exposure (21, 22). It has been suggested that diseases with a sex disparity should be investigated for environmental risk factors like contaminant exposure, as differences in vulnerability and susceptibility between the sexes may account for the prevalence disparities (23).
Our primary aim was to explore the association between seafood intake and dietary environmental contaminant exposure during pregnancy and JIA risk. Secondary aims included exploring sex disparities and possible interactions between seafood intake and genetic predisposition to JIA.
2 Material and methods
2.1 Study population and design
We used data from the Norwegian Mother, Father, and Child Cohort Study (MoBa), which was linked by national identification (ID) numbers to the individual records in the following population-based health registers: the Norwegian Patient Registry (NPR) and the Medical Birth Registry of Norway (MBRN).
MoBa is a population-based pregnancy cohort study conducted by the Norwegian Institute of Public Health. Participants were recruited from all over Norway from 1999-2008. Of those invited to participate, 41% of women consented. The cohort includes approximately 114,500 children, 95,200 mothers, and 75,200 fathers. The current study is based on version 12 of the quality-assured data files released for research in 2019 (24). Genotype data was available for a subsample of 51,804 children, which is further described under “Genotyping Data, Polygenic Risk Score (PRS) for JIA”.
Three questionnaires were sent to the mothers during pregnancy, the second being a semi-quantitative food frequency questionnaire (FFQ). The FFQ was distributed in gestational week 22 and covered the average intake of 255 food items and beverages during the first half of pregnancy (25). The MoBa FFQ has been validated and found to be a reliable tool to estimate intake of nutrients and foods during pregnancy, including various types of fish and seafood (26, 27). The FFQ was introduced in March 2002 and all pregnancies recruited between 2002 and 2008 are included in our study. Figure 1 outlines the flow of subject for inclusion in our study from the MoBa cohort.
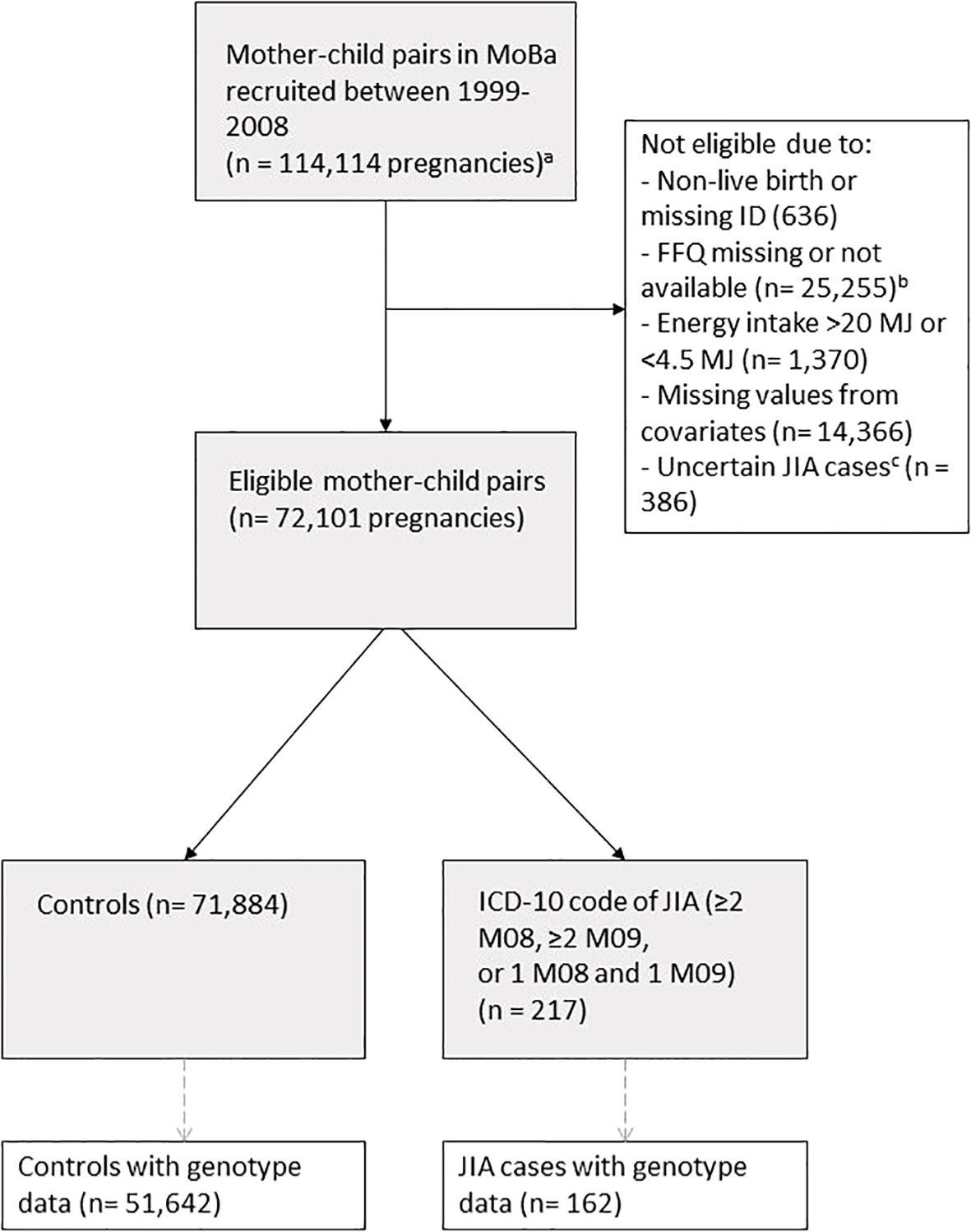
Figure 1. Flowchart of study population with exclusion criteria. a This number includes siblings. b The MoBa FFQ was introduced in 2002. c We excluded all controls with a single ICD-10 code (M08 or M09) to rule out potential JIA cases, except for those who received their first code in 2021. For these cases, we accepted a single relevant ICD-10 code, acknowledging that they might have had only one doctor visit before our latest NPR update in 2022.
2.2 Outcome
The Norwegian Patient Registry (NPR) contains data with personal ID numbers from all Norwegian public hospitals and specialists with public funding from 2008. We defined a JIA case as having at least two International Classification of Diseases (ICD)-10 codes (≥2 M08, ≥2 M09, or 1 M08 and 1 M09). We recently validated this case definition and have found a positive predictive value of 93.4% (28). For cases where the child received their first ICD-10 code in 2021, we accepted a single relevant ICD-10 code (M08 or M09), recognizing that there might have been only one doctor visit before we received our latest updates from NPR in December 2021. Controls were defined as live births that were non-JIA cases. We excluded children with only one registration of ICD-10 code M08 or M09 between 2008-2020 because they might have JIA.
2.3 Exposure variables: intake of seafood and environmental contaminants
We estimated maternal seafood intake and the exposure to dietary contaminants by the FFQ that was developed and validated for pregnant women in MoBa (25).
Food frequencies reported in the FFQ were converted to food amounts (grams/day) using FoodCalc and the Norwegian food table (26). Seafood intake was allocated into five variables, of which three were strictly related to fish intake: 1) oily fish (more than 8% fat, such as herring, mackerel, salmon), 2) lean/semi-oily fish (up to 8% fat, such as cod, haddock, saithe), and 3) total fish (total amount of oily fish and lean/semi-oily fish). In addition, we included 4) shellfish intake (capturing crab, shrimp, and mussels), and 5) total seafood (total fish and shellfish, including fish liver, roe, and fish liver/roe spread). We converted these continuous variables (grams/day) into categorical variables in the following way:
We categorized the seafood variables into high intake, defined as equal to or exceeding the 90th percentile (≥P90) of the population, and low intake, defined as less than 90th percentile (<P90). In secondary analyses, the five seafood variables were also divided into quintiles with the lowest group serving as reference. Lastly, because the Norwegian Directorate of Health recommends between 300-450 grams of fish each week (29), an exposure variable was also set at ≥300 grams of fish per week, which was compared to intake <300 grams/week.
The exposure to dietary environmental contaminants was estimated by combining consumption data from the FFQ with concentrations of contaminants in Norwegian food, based on data across various Nordic studies and databases, with the mean or median values from these studies used for the estimation of dietary contaminant exposure. The food contamination data spans several years, corresponding with the period when the FFQ was completed, and is described elsewhere (30, 31). Dietary contaminant exposure was categorized into two main groups: 1) heavy metals and 2) persistent organic pollutants (POPs). Heavy metals included a) mercury, and b) cadmium, while POPs included c) dioxins and dioxin-like (dl) compounds, and d) non-dioxin-like (non-dl) polychlorinated biphenyls (using PCB-153 as a proxy). The exposure to dioxins and dl-compounds is expressed as toxic equivalents (TEQ) when assessing their combined effect (32). The dietary contaminant variables were calculated per kilogram of pre-pregnancy body weight (kg bw), which was self-reported. We analyzed high vs. low intake and across quintiles as defined above.
2.4 Covariates and confounders
Potential confounding factors included maternal education, and parity (categorical variables); maternal age, pre-pregnancy BMI, daily energy intake (continuous variables); and maternal history of inflammatory rheumatic disease (see definition below), parental smoking status, and maternal supplement use during pregnancy (e.g., fish oil, vitamin D, folate) as dichotomous variables (yes/no). Associations with lean/semi-oily and oily fish were mutually adjusted due to their correlated intake.
When analyzing dietary environmental contaminants, we included the child’s birth year from the Medical Birth Registry as a possible confounder because contaminant levels in fish may have varied over the years, and because the cumulative risk of JIA increases with the child’s age. Information about region of birth was also obtained from the Medical Birth Registry.
Mother’s history of inflammatory rheumatic diseases was obtained via linkage to NPR and included following ICD-10 codes: M05, M06, M07, M08, M09, M30, M31, M32, M33, M34, M35, M45, M46, and L94.
2.5 Genotyping data, polygenic risk score for JIA
In MoBa, umbilical cord blood samples were collected at birth and DNA was stored at the Norwegian Institute of Public Health (33). Genotyping was carried out over several years through various research projects (34). MoBaPsychGen genotype quality control (QC) pipeline was developed to manage the complex relationships within the cohort. This pipeline includes steps for pre-imputation QC, phasing, imputation, and post-imputation QC, and it accounts for array and batch effects (35).
We focused on individuals of European ancestry, identified by visually comparing the first seven genetic principal components (PCs) to those from unrelated samples in the 1000 Genomes phase 1 project (35). Related individuals with a kinship coefficient >0.05 had one member excluded, prioritizing the retention of JIA cases, with other exclusions made randomly.
To estimate the genetic risk for JIA, we calculated PRSs using data from a genome-wide association study (GWAS) of JIA (36). The calculation was done using PRSice version 2.3.3 (37), applying different P-value thresholds as 5E-8, 1E-6, 1E-5, 1E-4, 1E-3, 1E-2, 5E-2, 1E-1, 5E-1, and 1. We then extracted the first PC of PRSs across all P-value thresholds, following a widely used method (38). The standardized PRS was then converted into a binary variable with cut-off at 0, of which the PRS <0 was regarded as “low”, whereas the PRS ≥0 was regarded as “high”.
2.6 Statistical analysis
Stata V.17.0 statistical software (StataCorp) and R version 4.2.3 (39) were used to conduct all statistical analyses. Characteristics of high vs low consumers of fish were reported as mean (SD) or median (IQR), as appropriate for continuous variables and by distribution differences (counts and percentages) for categorical variables. We used multiple logistic regression to examine the associations between seafood intake, dietary environmental contaminant exposure and risk of JIA. All associations are reported as odds ratios (OR) with 95% confidence intervals (CI), and as adjusted ORs (aOR) when adjusted for possible confounding factors listed above. The number of subjects with missing values on covariates was low for both cases (n=40, 18%) and controls (n=14,366, 20%), and all estimates are therefore based on complete case analyses. All analyses were further stratified by sex. In a sensitivity analysis, we included the region of birth (South-East, West, Middle and North), and thus presumably the region where the pregnancy took place, as a possible confounder because research shows a two-fold increased incidence of JIA in northern compared to southern Norway (28) and reports of geographical variations in fish intake (40).
To assess potential interactions between fish intake and genetic predisposition to JIA, we conducted multiple logistic regression analyses with an interaction term between fish intake and PRS. We included the same variables as in the main model except maternal history of inflammatory rheumatic disease to avoid over-adjustment. The Wald test was used to assess statistical significance of an interaction, and a p-value <0.05 was regarded as significant. We further investigated the interaction between fish intake and PRS by calculating the products of fish intake and dummy variables of each PRS group and replacing the interaction term in the multiple logistic regression with those products. This allowed us to estimate the association between fish intake and JIA in the low and high PRS groups separately. We used this model to visualize the relationship between fish intake and JIA in both groups predicting JIA risk in a simulated dataset of n = 200. As an additional test for interactions, we applied a case-only analysis by testing for associations between seafood intake and PRS in the cases only (41).
3 Results
3.1 Study sample characteristics
Our final analytical sample included 72,110 mother-child pairs; 217 children with JIA were identified (Figure 1). Of JIA cases, there were 139 (64.1%) girls and 78 (35.9%) boys. The median weekly maternal fish intake was 218 grams. Baseline characteristics categorized by high (≥P90) vs. low (<P90) total fish intake are shown in Table 1.
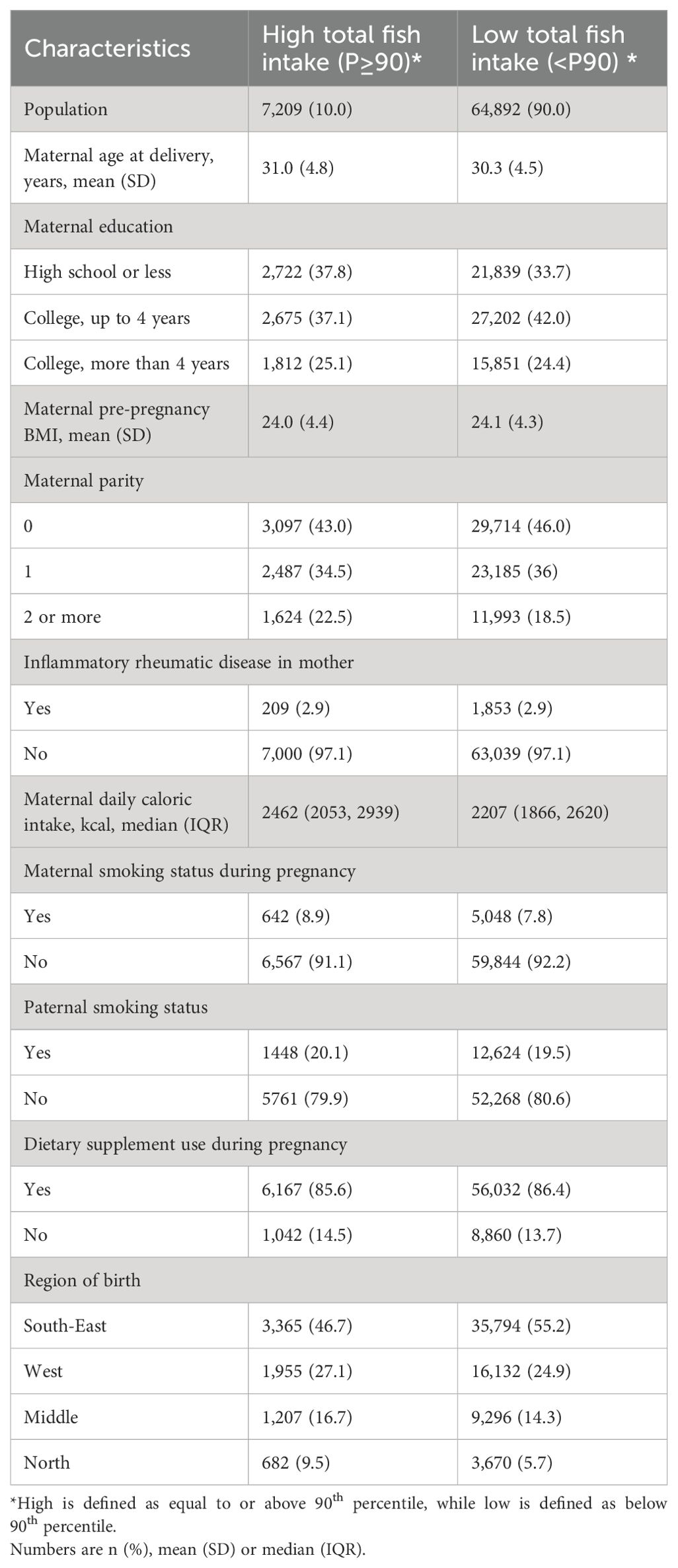
Table 1. Baseline characteristics categorized by high and low total fish intake in 72,101 MoBa participants 2002-2008.
3.2 Seafood intake and JIA
High vs low intake of lean/semi-oily fish during pregnancy was associated with JIA (aOR 1.51, 95% CI 1.02-2.22) (Table 2). After adjusting for region of birth, the confidence interval included 1 (aOR 1.45, 95% CI 0.99-2.18) (Supplementary Table 1). Additional results with region of birth as a covariate are presented in Supplementary Table 1-Supplementary Table 2. We found no other evidence of associations between high vs low intake of other seafood variables and JIA risk (Table 2).
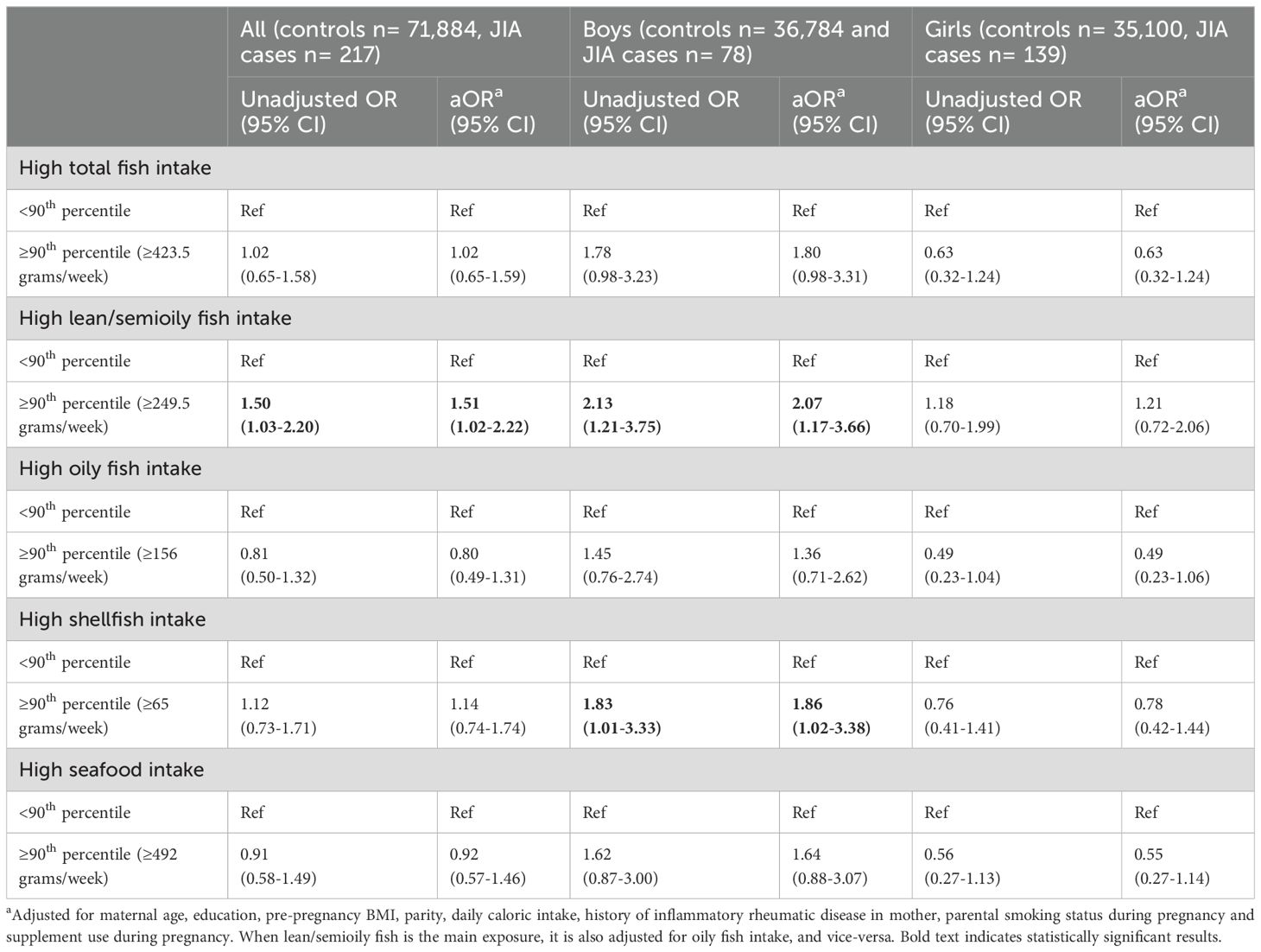
Table 2. Overall and sex-stratified associations between high vs. low seafood intake and JIA.
After sex-stratification, we found an association with lean/semi-oily fish intake among boys (aOR 2.07, 95% CI 1.17-3.66), but not in girls (Table 2 and Supplementary Table 1). Similarly, high shellfish intake was associated with increased risk among boys (aOR 1.86, 95% CI 1.02-3.38), but not girls (Table 2). Additionally, consuming fish ≥300 vs. <300 grams/week during pregnancy, regardless of fat content, was linked to higher odds of JIA in boys (aOR 1.92, 95% CI: 1.22-3.04), but not in girls (Supplementary Table 3). When analyzing by quintiles, no other convincing evidence of associations were observed (Supplementary Table 4).
3.3 Interactions between fish intake and polygenic risk score
The following results are based on a smaller sample than our main analyses (controls n= 51,642, JIA case n= 162) due to lack of genetic data on all observations. To account for this, we ran the main analyses on the smaller dataset as a sensitivity analysis, with the results provided in Supplementary Table 5.
We found evidence of an interaction between total fish intake and PRS (aOR 0.33, 95% CI 0.12-0.90, p-value 0.03), but not with the other seafood variables (Supplementary Table 6). The association between total fish intake and JIA was only apparent in the low PRS group (aOR 2.26, 95% CI 1.08-4.71) (Table 3 and Figure 2). Furthermore, we also found an association between lean/semi-oily fish and JIA in the low PRS group (aOR 2.23, 95% CI 1.06-4.66), but not with the other seafood variables (Table 3 and Supplementary Figure 1-Supplementary Figure 2). A case-only design was used to test the interaction between fish intake and PRS, which further confirmed the findings from the case-control analyses: the high total fish intake was negatively associated with PRS in the cases, whereas none of the other seafood variables reached statistical significance (Supplementary Table 7).
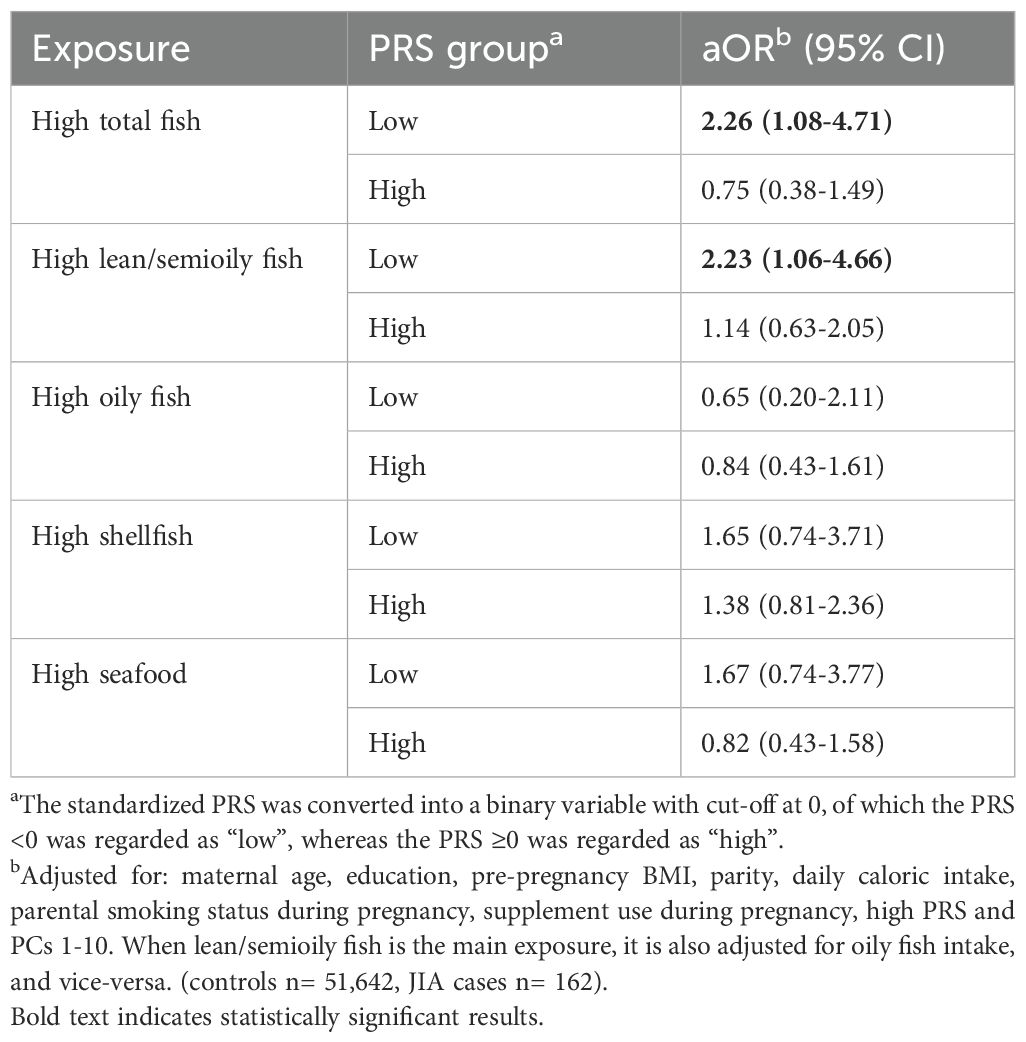
Table 3. Associations between high seafood intake and JIA risk in groups of high or low genetic risk (PRS of JIA).
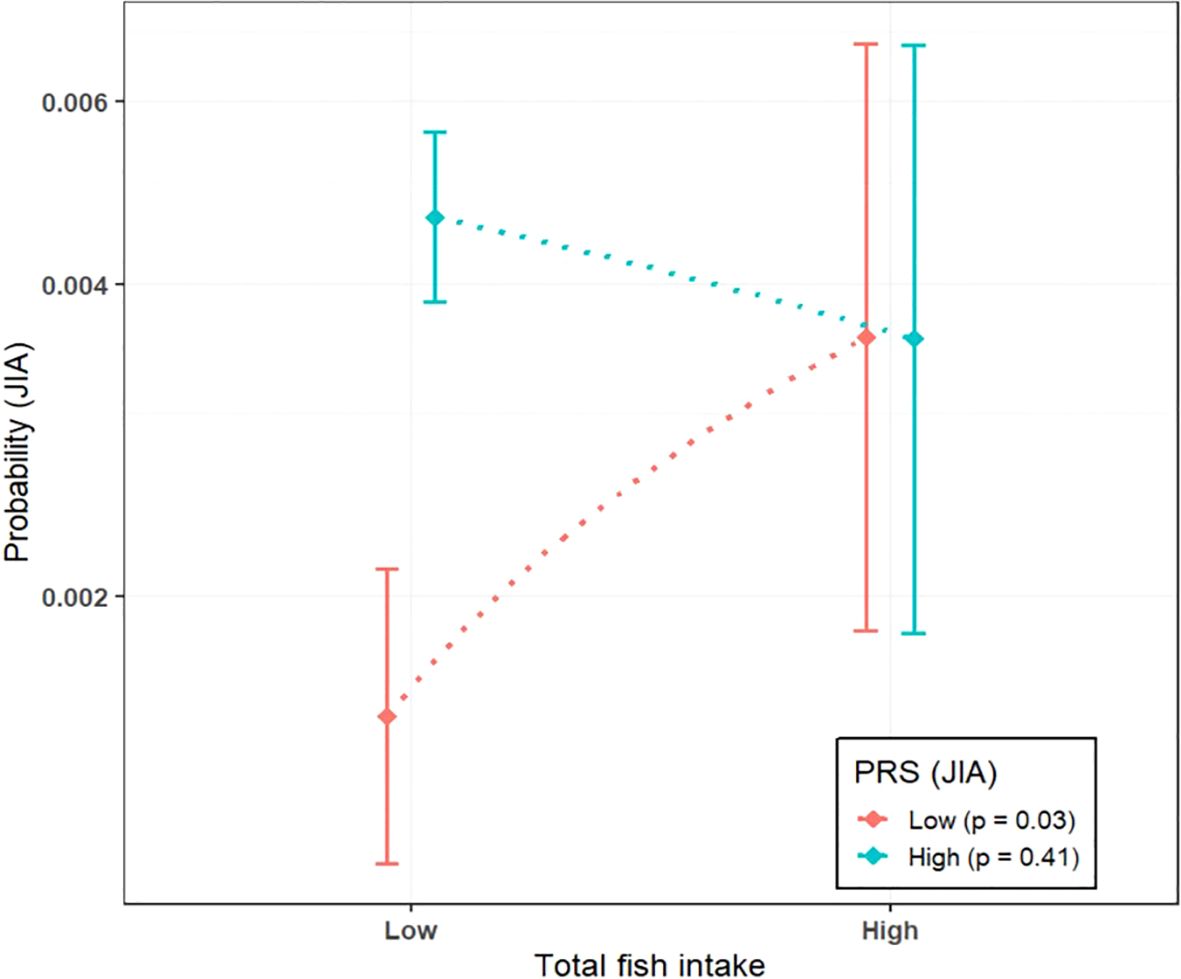
Figure 2. Association between total fish intake and JIA risk grouped by high (=>0) and low (<0) polygenic risk score (PRS) for JIA. P-values indicate the significance of the associations between fish intake and JIA risk within each PRS group.
3.4 Estimated environmental contaminants and JIA
We found no evidence of associations between estimated dietary intake of environmental contaminants and risk of JIA, whether analyzed by high vs. low intake (Table 4) or by quintiles (Supplementary Table 8).
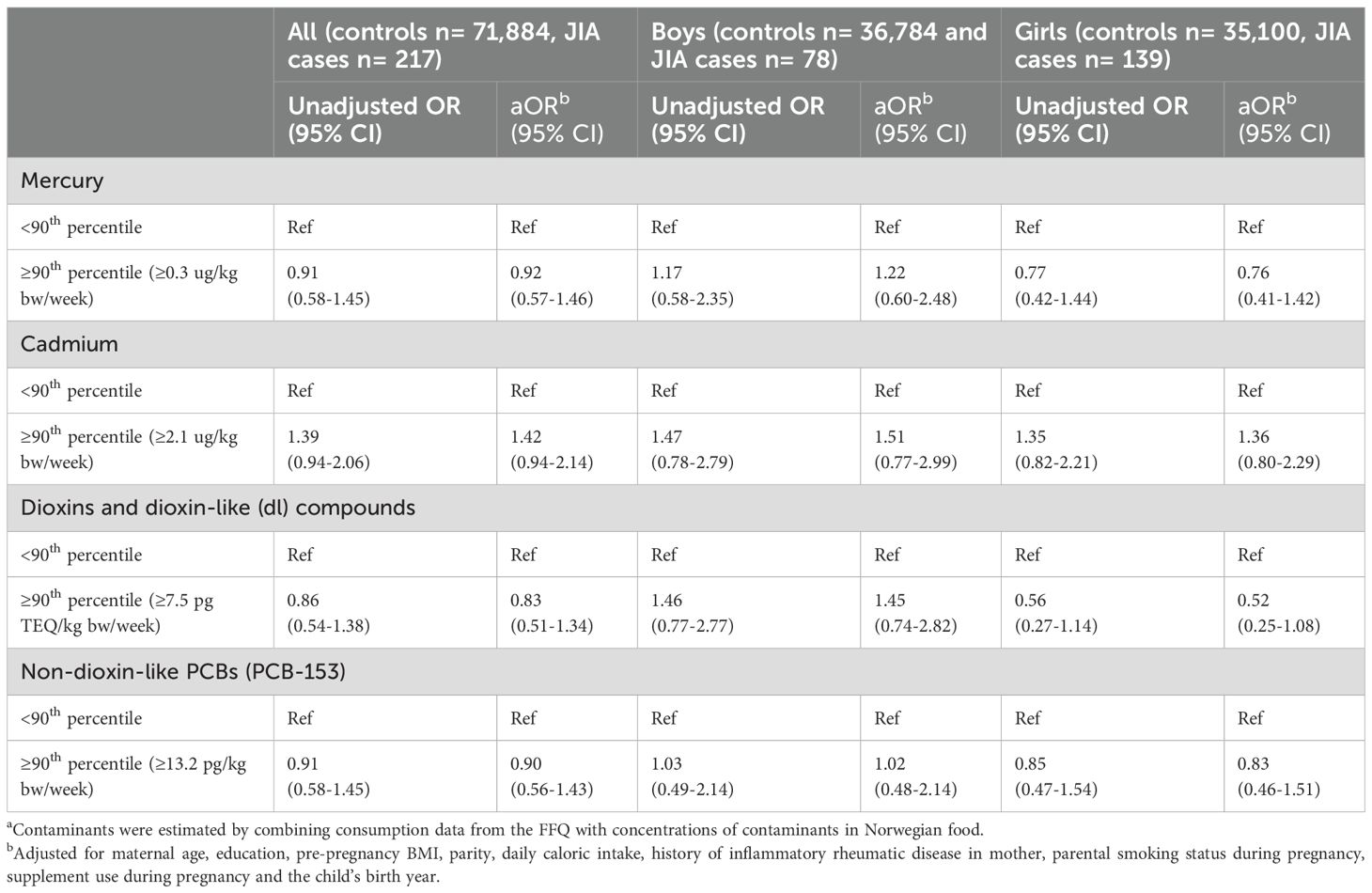
Table 4. Overall and sex-stratified associations between high vs. low dietary contaminant exposurea and JIA.
After sex-stratification, we found a positive association between non-dl PCBs and JIA in boys (aOR 2.24, 95% CI 1.03-4.86), when comparing a dietary exposure corresponding to the 4th quintile to the 1st quintile (Supplementary Table 8). Among girls, being in the 5th quintile of either dl-compound or non-dl PCB intake, was negatively associated with risk of JIA (aOR 0.40, 95% CI 0.20-0.79 and aOR 0.44, 95% CI 0.23-0.83; Supplementary Table 8).
4 Discussion
In this large population-based study, we found a modestly increased risk of JIA associated with high maternal intake of lean/semi-oily fish (approximately 250 grams or more per week) during pregnancy. No clear associations were found between JIA and overall maternal intake of fish, oily fish, shellfish, or seafood intake. Sex-stratified analyses suggested a stronger positive association between high maternal seafood intake and JIA risk in boys. For instance, an intake of >300 grams of fish per week as recommended by the Norwegian Directorate of Health (29), was linked to increased risk of JIA in boys but not in girls. We observed no clear associations with estimated maternal dietary contaminant exposures. The risk associated with total fish intake depended on genetic predisposition: high fish intake significantly affected JIA risk only in individuals with a low genetic predisposition to JIA.
Our results are partly in line with a Swedish study (5), which found positive associations between fish intake of more than once per week during pregnancy and JIA risk, although our effect sizes were of substantially lower magnitude. The Swedish study did not specify portion sizes, complicating direct comparisons. Furthermore, our study specifically associates lean/semi-oily fish with increased JIA risk, while the Swedish study identified the strongest association with total fish intake without distinguishing between fish varieties (5).
We found no evidence of robust associations between exposure to dietary environmental contaminants and risk of JIA. This differs from the Swedish study which attributed the heightened risk of JIA to increased heavy metal exposure, including mercury, through fish intake (5), and another study showing that prenatal exposure to environmental contaminants can alter the cord serum metabolome, potentially increasing the risk of immune-mediated diseases such as JIA (42). Despite seafood accounting for 88% of total dietary mercury exposure – with lean fish contributing to more than half of this - as well as being a considerable source of other contaminants (20, 43, 44), we found no evidence that it contributed to JIA risk in MoBa. In fact, our sex-stratified analyses show an inverse relationship between exposure to POPs and JIA in girls. Unlike the Swedish study, which measured blood concentrations, our study relies on self-reported dietary data, but includes a much larger sample size (217 vs. 41 JIA cases) (5).
JIA is more prevalent in girls than boys (4), yet our study suggests that high seafood intake is more strongly associated with JIA risk in boys. Sex-stratified analyses showed no indication of increased risk of JIA when comparing high vs low intake of seafood and contaminant exposure (except lean/semi-oily fish and cadmium) in girls, on the contrary, estimates indicated a lower risk of JIA with high intake. In contrast, for boys, all associations indicated an increased risk of JIA.
Most studies on sex disparities in pediatric illnesses do not explore underlying causes (45), making our sex-stratified analyses valuable for addressing this knowledge gap. Although estrogen levels are often suggested as a cause for the higher prevalence of autoimmunity in women, the low and stable levels during childhood suggest other mechanisms (4). The varying patterns of JIA risk between boys and girls with seafood intake may be due to lack of statistical power given the sample size (girls, n = 139, boys, n = 78), and the results should be interpreted cautiously. The inverse relationship between POP exposure and JIA risk in girls observed in our study may not be directly linked to POPs, but could reflect a spurious association with oily fish, which was estimated to have a protective association in girls. This protective association may be related to nutrients in oily fish rather than POPs. A study on diabetes type 1 observed similar findings (46). A separate MoBa study on prenatal exposure to POPs showed immunosuppressive effects (32), which could potentially explain a protective association in girls. Inherent biological differences may also influence these sex-specific trends.
Gene-environment interaction analyses suggest that genetic predisposition modifies the effect of fish intake on JIA risk, and vice versa. Specifically, fish intake had a stronger estimated association with JIA risk in individuals with low genetic predisposition, while its impact was estimated as less pronounced in those with a high genetic risk. Our previous findings show that the PRS is more strongly associated with JIA in girls than in boys, with a higher proportion of female JIA cases having a standardized PRS >0 (submitted for publication)1. This might explain why we observe a stronger association between fish intake and JIA risk in boys, as male JIA cases, on average, have a lower genetic risk of JIA.
Our study’s strengths include its prospective design, comprehensive data collection with genetic liability, a large study population, and linkage to national registries, ensuring minimal loss to follow-up. A significant and novel strength is the incorporation of a PRS within a subset of our cohort, enabling us to study gene-environment interactions in JIA. By sex-stratification, we discerned variations in risk estimates between boys and girls. To our knowledge, this is the largest population-based prospective cohort study exploring environmental risk factors for JIA, identifying 217 cases.
While including more JIA cases than in previous studies, the sample size remains the main limitation of the study, as it reduces the power to detect small effects, especially in stratified analyses and for the subset with genotype data. We also lack data on JIA subtypes, which is important given the disease’s heterogeneity; different subtypes may have distinct pathomechanisms or vulnerabilities. We did not exclude controls with other systemic autoimmune diseases, potentially diluting the observed effects. Additionally, while the recruitment into MoBa was population-based, the cohort is not fully representative of the general population (47). For instance, the homogenous ethnic background of MoBa participants (48) may limit the generalizability of our findings to more diverse populations. The self-reported dietary data may result in exposure misclassification as the FFQ provide rough estimates, even though it has been validated (26). We cannot study exact dietary intake for the second half of the pregnancy as the FFQ was completed in week 22, however, we assume consistent dietary patterns throughout the pregnancy. Additionally, we lack measured blood concentration of contaminants. Our contamination estimates rely on broader Nordic averages rather than location-specific data, so this approach may not adequately capture exposure differences across Norway, especially in areas of higher contamination, highlighting the need for future research to measure blood concentrations. Although we adjusted for potential confounders, residual confounding cannot be ruled out due to the observational nature of the study. Lastly, since NPR data begins in 2008, JIA cases diagnosed and in remission between 2002-2008 may be missing. Some of the older-diagnosed JIA cases are also missing, because follow up ended in 2021.
In conclusion, we observed an increased risk of JIA in children whose mothers consumed high amounts of lean/semi-oily fish during pregnancy, particularly in boys. Despite lean fish being an important source of dietary mercury exposure, the heightened JIA risk was not explained by contaminant exposure in our study. Our findings also suggest a stronger association between fish intake and JIA in those with a low genetic predisposition to JIA. Further studies are warranted to explore the underlying mechanisms of seafood and JIA, as definitive causation cannot be inferred. This includes more precise assessments of contaminant exposure via blood samples, and the need to clarify the observed sex differences and genetic interactions.
Data availability statement
Data from the Norwegian Mother, Father and Child Cohort Study and the Medical Birth Registry of Norway used in this study are managed by the national health register holders in Norway (Norwegian Institute of public health) and can be made available to researchers, provided approval from the Regional Committees for Medical and Health Research Ethics (REC), compliance with the EU General Data Protection Regulation (GDPR) and approval from the data owners. The consent given by the participants does not open for storage of data on an individual level in repositories or journals. Researchers who want access to data sets for replication should apply through helsedata.no. Access to data sets requires approval from The Regional Committee for Medical and Health Research Ethics in Norway and an agreement with MoBa.
Ethics statement
The establishment of MoBa and initial data collection was based on a license from the Norwegian Data Protection Agency and approval from The Regional Committees for Medical and Health Research Ethics. The MoBa cohort is currently regulated by the Norwegian Health Registry Act. The current study, part of the MoBaRheuma project, was approved by The Regional Committees for Medical and Health Research Ethics (REK), which includes linkages with NPR and MBRN. REK ref. nr. 2019/1222.
Author contributions
VD: Writing – original draft, Writing – review & editing, Conceptualization, Formal analysis, Methodology, Visualization. KH: Conceptualization, Formal analysis, Methodology, Validation, Visualization, Writing – review & editing. HR: Formal analysis, Methodology, Validation, Writing – review & editing. PJ: Formal analysis, Methodology, Supervision, Writing – review & editing. KS: Methodology, Writing – review & editing. SH: Conceptualization, Methodology, Resources, Writing – review & editing. CW: Methodology, Writing – review & editing. LR: Methodology, Writing – review & editing. OA: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review & editing. AB: Conceptualization, Methodology, Resources, Writing – original draft, Writing – review & editing. IC: Conceptualization, Formal analysis, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. HS: Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Our work has been financed through several public sources: Foundation DAM (grant number 2023/FO426544), South-Eastern Norway Regional Health Authority (grant number HSO/2023070) and Norwegian Rheumatology Association. LR and CW were supported by the intramural research program of the National Institute of Environmental Health Sciences, National Institutes of Health. The study was partly funded by the Research Council of Norway through its Centres of Excellence funding scheme (project No 262700).
Acknowledgments
The Norwegian Mother, Father and Child Cohort Study is supported by the Norwegian Ministry of Health and Care Services and the Ministry of Education and Research. We are grateful to all the participating families in Norway who take part in this on-going cohort study and the registries (MBRN and NPR) for making data available. We thank the Norwegian Institute of Public Health (NIPH) for generating high-quality genomic data. This research is part of the HARVEST collaboration, supported by the Research Council of Norway (#229624). We also thank the NORMENT Centre for providing genotype data, funded by the Research Council of Norway (#223273), South East Norway Versjon 7.03 Health Authorities and Stiftelsen Kristian Gerhard Jebsen. We further thank the Center for Diabetes Research, the University of Bergen for providing genotype data and performing quality control and imputation of the data funded by the ERC AdG project SELECTionPREDISPOSED, Stiftelsen Kristian Gerhard Jebsen, Trond Mohn Foundation, the Research Council of Norway, the Novo Nordisk Foundation, the University of Bergen, and the Western Norway Health Authorities. We would also like to thank Professor Håkon K. Gjessing for valuable discussions and guidance regarding the gene-environment interaction analyses. Part of this work was presented as an oral abstract at the EULAR Annual European Congress of Rheumatology conference in Vienna 2024 (49).
Conflict of interest
OA has received consulting fees from Cortechs.ai and Precision Health AS and declares future stock options with Cortechs.ai and Precision Health AS. OA has also received speaker fees from Lundbeck, Janssen, Otsuka, and Sunovion.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. ChatGPT was solely used to improve the language clarity and precision, as English is not the primary language of the authors. It was not used for data analysis or any other purpose beyond improving language.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2024.1523990/full#supplementary-material
Footnotes
- ^ 1Haftorn KL, Rudsari HK, Jaholkowski PP, Dåstøl VØ, Hestetun SV, Andreassen OA, et al. Nonlinearity and sex differences in the performance of a polygenic risk score for juvenile idiopathic arthritis. (2024).
References
1. Martini A, Lovell DJ, Albani S, Brunner HI, Hyrich KL, Thompson SD, et al. Juvenile idiopathic arthritis. Nat Rev Dis Primers. (2022) 8:5. doi: 10.1038/s41572-021-00332-8
2. Horton DB, Shenoi S. Review of environmental factors and juvenile idiopathic arthritis. Open Access Rheumatol. (2019) 11:253–67. doi: 10.2147/OARRR.S165916
3. Clarke SLN, Mageean KS, Maccora I, Harrison S, Simonini G, Sharp GC, et al. Moving from nature to nurture: a systematic review and meta-analysis of environmental factors associated with juvenile idiopathic arthritis. Rheumatol (Oxford). (2022) 61:514–30. doi: 10.1093/rheumatology/keab627
4. Cattalini M, Soliani M, Caparello MC, Cimaz R. Sex differences in pediatric rheumatology. Clin Rev Allergy Immunol. (2019) 56:293–307. doi: 10.1007/s12016-017-8642-3
5. Kindgren E, Guerrero-Bosagna C, Ludvigsson J. Heavy metals in fish and its association with autoimmunity in the development of juvenile idiopathic arthritis: a prospective birth cohort study. Pediatr Rheumatol Online J. (2019) 17:33. doi: 10.1186/s12969-019-0344-3
6. Pollard KM, Cauvi DM, Mayeux JM, Toomey CB, Peiss AK, Hultman P, et al. Mechanisms of environment-induced autoimmunity. Annu Rev Pharmacol Toxicol. (2021) 61:135–57. doi: 10.1146/annurev-pharmtox-031320-111453
7. Pollard KM, Christy JM, Cauvi DM, Kono DH. Environmental xenobiotic exposure and autoimmunity. Curr Opin Toxicol. (2018) 10:15–22. doi: 10.1016/j.cotox.2017.11.009
8. Gaylord A, Trasande L, Kannan K, Thomas KM, Lee S, Liu M, et al. Persistent organic pollutant exposure and celiac disease: A pilot study. Environ Res. (2020) 186:109439. doi: 10.1016/j.envres.2020.109439
9. Kharrazian D. Exposure to environmental toxins and autoimmune conditions. Integr Med (Encinitas). (2021) 20:20–4.
10. Alves MF, Fraiji NA, Barbosa AC, De Lima DS, Souza JR, Dórea JG, et al. Fish consumption, mercury exposure and serum antinuclear antibody in Amazonians. Int J Environ Health Res. (2006) 16:255–62. doi: 10.1080/09603120600734147
11. Nyland JF, Fillion M, Barbosa F Jr., Shirley DL, Chine C, Lemire M, et al. Biomarkers of methylmercury exposure immunotoxicity among fish consumers in Amazonian Brazil. Environ Health Perspect. (2011) 119:1733–8. doi: 10.1289/ehp.1103741
12. Crowe W, Allsopp PJ, Watson GE, Magee PJ, Strain JJ, Armstrong DJ, et al. Mercury as an environmental stimulus in the development of autoimmunity - A systematic review. Autoimmun Rev. (2017) 16:72–80. doi: 10.1016/j.autrev.2016.09.020
13. Somers EC, Ganser MA, Warren JS, Basu N, Wang L, Zick SM, et al. Mercury exposure and antinuclear antibodies among females of reproductive age in the United States: NHANES. Environ Health Perspect. (2015) 123:792–8. doi: 10.1289/ehp.1408751
14. Popov Aleksandrov A, Mirkov I, Tucovic D, Kulas J, Zeljkovic M, Popovic D, et al. Immunomodulation by heavy metals as a contributing factor to inflammatory diseases and autoimmune reactions: Cadmium as an example. Immunol Lett. (2021) 240:106–22. doi: 10.1016/j.imlet.2021.10.003
15. Chen L, Sun Q, Peng S, Tan T, Mei G, Chen H, et al. Associations of blood and urinary heavy metals with rheumatoid arthritis risk among adults in NHANES, 1999-2018. Chemosphere. (2022) 289:133147. doi: 10.1016/j.chemosphere.2021.133147
16. Joo SH, Lee J, Hutchinson D, Song YW. Prevalence of rheumatoid arthritis in relation to serum cadmium concentrations: cross-sectional study using Korean National Health and Nutrition Examination Survey (KNHANES) data. BMJ Open. (2019) 9:e023233. doi: 10.1136/bmjopen-2018-023233
17. Lee DH, Steffes M, Jacobs DR. Positive associations of serum concentration of polychlorinated biphenyls or organochlorine pesticides with self-reported arthritis, especially rheumatoid type, in women. Environ Health Perspect. (2007) 115:883–8. doi: 10.1289/ehp.9887
18. Costa LG. Contaminants in fish: risk-benefit considerations. Arh Hig Rada Toksikol. (2007) 58:367–74. doi: 10.2478/v10004-007-0025-3
19. Mahaffey KR, Clickner RP, Bodurow CC. Blood organic mercury and dietary mercury intake: National Health and Nutrition Examination Survey, 1999 and 2000. Environ Health Perspect. (2004) 112:562–70. doi: 10.1289/ehp.6587
20. Ferrari P, Arcella D, Heraud F, Cappé S, Fabiansson S. Impact of refining the assessment of dietary exposure to cadmium in the European adult population. Food Addit Contam Part A Chem Anal Control Expo Risk Assess. (2013) 30:687–97. doi: 10.1080/19440049.2013.777161
21. Kovner K. Persistent organic pollutants: A global issue, A global response. Washington, DC, USA: United States ENvironmental Protection Agency (EPA (2002). Available at: https://www.epa.gov/international-cooperation/persistent-organic-pollutants-global-issue-global-response (Accessed March 14, 2024).
22. (WHO) WHO. Food safety: Persistent organic pollutants (POPs). Geneva, Switzerland: Nutrition and Food Safety (NFS)WHO (2020). Available at: https://www.who.int/news-room/questions-and-answers/item/food-safety-persistent-organic-pollutants-(pops) (Accessed March 15, 2024).
23. Butter ME. Are women more vulnerable to environmental pollution? J Hum Ecol. (2006) 20:221–6. doi: 10.31901/24566608.2006/20.03.12
24. Magnus P, Birke C, Vejrup K, Haugan A, Alsaker E, Daltveit AK, et al. Cohort profile update: the norwegian mother and child cohort study (MoBa). Int J Epidemiol. (2016) 45:382–8. doi: 10.1093/ije/dyw029
25. Meltzer HM, Brantsaeter AL, Ydersbond TA, Alexander J, Haugen M. Methodological challenges when monitoring the diet of pregnant women in a large study: experiences from the Norwegian Mother and Child Cohort Study (MoBa). Matern Child Nutr. (2008) 4:14–27. doi: 10.1111/j.1740-8709.2007.00104.x
26. Brantsaeter AL, Haugen M, Alexander J, Meltzer HM. Validity of a new food frequency questionnaire for pregnant women in the Norwegian Mother and Child Cohort Study (MoBa). Matern Child Nutr. (2008) 4:28–43. doi: 10.1111/j.1740-8709.2007.00103.x
27. Vejrup K, Brandlistuen RE, Brantsæter AL, Knutsen HK, Caspersen IH, Alexander J, et al. Prenatal mercury exposure, maternal seafood consumption and associations with child language at five years. Environ Int. (2018) 110:71–9. doi: 10.1016/j.envint.2017.10.008
28. Hestetun SV, Rudsari HK, Jaholkowski P, Shadrin A, Haftorn KL, Andersen S, et al. Incidence and genetic risk of juvenile idiopathic arthritis in Norway by latitude. Arthritis & rheumatology (Hoboken, N.J.) (2024). doi: 10.1002/art.43040
29. Helsedirektoratet. Kostrådene. Fisk til middag to til tre ganger i uken (2016). Available online at: https://www.helsedirektoratet.no/faglige-rad/kostradene-og-naeringsstoffer/kostrad-for-befolkningenfisk-til-middag-to-til-tre-ganger-i-uken-praktisk-informasjon (Accessed March 19, 2024).
30. Jenssen MT, Brantsæter AL, Haugen M, Meltzer HM, Larssen T, Kvalem HE, et al. Dietary mercury exposure in a population with a wide range of fish consumption–self-capture of fish and regional differences are important determinants of mercury in blood. Sci Total Environ. (2012) 439:220–9. doi: 10.1016/j.scitotenv.2012.09.024
31. Kvalem HE, Knutsen HK, Thomsen C, Haugen M, Stigum H, Brantsaeter AL, et al. Role of dietary patterns for dioxin and PCB exposure. Mol Nutr Food Res. (2009) 53:1438–51. doi: 10.1002/mnfr.200800462
32. Stølevik SB, Nygaard UC, Namork E, Haugen M, Meltzer HM, Alexander J, et al. Prenatal exposure to polychlorinated biphenyls and dioxins from the maternal diet may be associated with immunosuppressive effects that persist into early childhood. Food Chem Toxicol. (2013) 51:165–72. doi: 10.1016/j.fct.2012.09.027
33. (NIPH) NIoPH. Protocols for the norwegian mother, father and child cohort study (MoBa). Norwegian Institute of Public Health: Norwegian Institute of Public Health (2019) (Oslo, Norway). Available at: https://www.fhi.no/en/publ/2012/protocols-for-moba/ (Accessed May 20, 2024).
34. Høgåsen G. MoBa genetics (2024). Available online at: https://github.com/folkehelseinstituttet/mobagen (Accessed May 20, 2024).
35. Corfield E, Shadrin A, Frei O, Rahman Z, Lin A, Athanasiu L, et al. Genetic profile of the norwegian mother, father, and child cohort study (Moba): results from the mobapsychgen pipeline. Eur Neuropsychopharmacol. (2022) 63:e292–e3. doi: 10.1016/j.euroneuro.2022.07.517
36. López-Isac E, Smith SL, Marion MC, Wood A, Sudman M, Yarwood A, et al. Combined genetic analysis of juvenile idiopathic arthritis clinical subtypes identifies novel risk loci, target genes and key regulatory mechanisms. Ann Rheum Dis. (2021) 80:321–8. doi: 10.1136/annrheumdis-2020-218481
37. Choi SW, O’Reilly PF. PRSice-2: Polygenic Risk Score software for biobank-scale data. Gigascience. (2019) 8. doi: 10.1093/gigascience/giz082
38. Coombes BJ, Ploner A, Bergen SE, Biernacka JM. A principal component approach to improve association testing with polygenic risk scores. Genet Epidemiol. (2020) 44:676–86. doi: 10.1002/gepi.22339
39. R Core Team. R. A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2022).
40. Stabell C. Hvem spiser fisk, in: Statistisk sentralbyrå: Statistisk sentralbyrå (2017). Available online at: https://www.ssb.no/helse/artikler-og-publikasjoner/hvem-spiser-fisk (Accessed May 13, 2024).
41. Piegorsch WW, Weinberg CR, Taylor JA. Non-hierarchical logistic models and case-only designs for assessing susceptibility in population-based case-control studies. Stat Med. (1994) 13:153–62. doi: 10.1002/sim.4780130206
42. Karthikeyan BS, Hyötyläinen T, Ghaffarzadegan T, Triplett E, Orešič M, Ludvigsson J. Prenatal exposure to environmental contaminants and cord serum metabolite profiles in future immune-mediated diseases. J Expo Sci Environ Epidemiol. (2024) 34:647–58. doi: 10.1038/s41370-024-00680-z
43. Vejrup K, Brantsæter AL, Knutsen HK, Magnus P, Alexander J, Kvalem HE, et al. Prenatal mercury exposure and infant birth weight in the Norwegian Mother and Child Cohort Study. Public Health Nutr. (2014) 17:2071–80. doi: 10.1017/S1368980013002619
44. Ho QT, Frantzen S, Nilsen BM, Nøstbakken OJ, Azad AM, Duinker A, et al. Congener-specific accumulation of persistent organic pollutants in marine fish from the Northeast Atlantic Ocean. J Hazard Mater. (2023) 457:131758. doi: 10.1016/j.jhazmat.2023.131758
45. Piccini P, Montagnani C, de Martino M. Gender disparity in pediatrics: a review of the current literature. Ital J Pediatr. (2018) 44:1. doi: 10.1186/s13052-017-0437-x
46. Rignell-Hydbom A, Elfving M, Ivarsson SA, Lindh C, Jönsson BA, Olofsson P, et al. A nested case-control study of intrauterine exposure to persistent organochlorine pollutants in relation to risk of type 1 diabetes. PloS One. (2010) 5:e11281. doi: 10.1371/journal.pone.0011281
47. Nilsen RM, Vollset SE, Gjessing HK, Skjaerven R, Melve KK, Schreuder P, et al. Self-selection and bias in a large prospective pregnancy cohort in Norway. Paediatr Perinat Epidemiol. (2009) 23:597–608. doi: 10.1111/j.1365-3016.2009.01062.x
48. Corfield EC, Frei O, Shadrin AA, Rahman Z, Lin A, Athanasiu L, et al. The Norwegian Mother, Father, and Child cohort study (MoBa) genotyping data resource: MoBaPsychGen pipeline v. 1. bioRxiv. (2022) 2022:06.23.496289. doi: 10.1101/2022.06.23.496289
Keywords: juvenile idiopathic arthritis (JIA), MoBa, fish, contaminants, heavy metals, polygenic risk score, gene-environment interaction, sex differences
Citation: Dåstøl VØ, Haftorn KL, Rudsari HK, Jaholkowski PP, Størdal K, Håberg SE, Weinberg CR, Rider LG, Andreassen OA, Brantsæter AL, Caspersen IH and Sanner H (2025) Maternal seafood intake, dietary contaminant exposure, and risk of juvenile idiopathic arthritis: exploring gene-environment interactions. Front. Immunol. 15:1523990. doi: 10.3389/fimmu.2024.1523990
Received: 06 November 2024; Accepted: 16 December 2024;
Published: 14 January 2025.
Edited by:
Esther Erdei, University of New Mexico Health Sciences Center, United StatesReviewed by:
Justyna Roszkiewicz, Medical University of Lodz, PolandLillemor Berntson, Uppsala University, Sweden
Copyright © 2025 Dåstøl, Haftorn, Rudsari, Jaholkowski, Størdal, Håberg, Weinberg, Rider, Andreassen, Brantsæter, Caspersen and Sanner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vilde Øverlien Dåstøl, dmlsZGUuZGFzdG9sQGdtYWlsLmNvbQ==