 Juan C. Baena1,6*
Juan C. Baena1,6* Juan Sebastián Victoria1,6
Juan Sebastián Victoria1,6 Alejandro Toro-Pedroza1,6Cristian C. Aragón1,2
Alejandro Toro-Pedroza1,6Cristian C. Aragón1,2 Joshua Ortiz-Guzman6,7,16
Joshua Ortiz-Guzman6,7,16 Juan Esteban Garcia-Robledo6,15David Torres6
Juan Esteban Garcia-Robledo6,15David Torres6 Lady J. Rios-Serna4,6Ludwig Albornoz6Joaquin D. Rosales2,6Carlos A. Cañas3,4,6Gustavo Adolfo Cruz-Suarez5,6,8,9
Lady J. Rios-Serna4,6Ludwig Albornoz6Joaquin D. Rosales2,6Carlos A. Cañas3,4,6Gustavo Adolfo Cruz-Suarez5,6,8,9 Felipe Ocampo Osorio5,6,9
Felipe Ocampo Osorio5,6,9 Tania Fleitas12Ivan Laponogov13
Tania Fleitas12Ivan Laponogov13 Alexandre Loukanov6,10,11Kirill Veselkov13,14
Alexandre Loukanov6,10,11Kirill Veselkov13,14- 1Division of Oncology, Department of Medicine, Fundación Valle del Lili, ICESI University, Cali, Colombia
- 2Division of Hematology, Department of Medicine, Fundación Valle del Lili, ICESI University, Cali, Colombia
- 3Division of Rheumatology, Department of Medicine, Fundación Valle del Lili, ICESI University, Cali, Colombia
- 4Universidad Icesi, CIRAT: Centro de Investigación en Reumatología, Autoinmunidad y Medicina Traslacional, Cali, Colombia
- 5Artificial Intelligence Unit, Fundación Valle del Lili, Cali, Colombia
- 6LiliCAR-T Group, Fundación Valle del Lili, ICESI, Cali, Colombia
- 7Director of Clinical Research, Rio Grande Urology, El Paso, TX, United States
- 8Departamento de Salud Pública y Medicina Comunitaria, Universidad ICESI, Cali, Valle del Cauca, Colombia
- 9Centro de Investigaciones Clínicas, Fundación Valle del Lili, Cali, Valle del Cauca, Colombia
- 10Department of Chemistry and Materials Science, National Institute of Technology, Gunma College, Maebashi, Japan
- 11Laboratory of Engineering Nanobiotechnology, University of Mining and Geology "St. Ivan Rilski", Sofia, Bulgaria
- 12Department of Medical Oncology, Hospital Clínico Universitario, INCLIVA, Biomedical Research Institute, University of Valencia, Valencia, Spain
- 13Division of Cancer, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, London, United Kingdom
- 14Department of Environmental Health Sciences, Yale School of Public Health, New Haven, CT, United States
- 15IDC Instituto de Cáncer Hemato Oncólogos, Cali, Colombia
- 16Prodigy Cells Labs, LLC, Doral, Florida, United States
Personalized medicine has redefined cancer treatment by aligning therapies with each patient’s unique biological profile. A key example is chimeric antigen receptor T-cell (CAR-T) therapy, in which a patient’s own T cells are genetically modified to recognize and destroy cancer cells. This approach has delivered remarkable results in hematologic malignancies and is beginning to show promise in solid tumors and autoimmune diseases. However, its broader adoption is limited by major challenges, including complex manufacturing, high costs, limited efficacy in solid tumors, and potentially severe toxicities. Nanotechnology offers exciting possibilities to overcome many of these barriers. Engineered nanoparticles can improve gene delivery, target tumors more precisely, enhance immune cell function, and enable in vivo CAR-T production, reducing the need for labor-intensive ex vivo processes. However, despite this promise, translation into clinical settings remains difficult due to regulatory hurdles, scalability issues, and inconsistent reproducibility in human models. At the same time, artificial intelligence (AI), with its powerful algorithms for data analysis and predictive modeling, is transforming how we design, evaluate, and monitor advanced therapies, including the optimization of manufacturing processes. In the context of CAR-T, AI holds strong potential for better patient stratification, improved prediction of treatment response and toxicity, and faster, more precise design of CAR constructs and delivery systems. Leveraging these three technological pillars, this review introduces the concept of Smart CART Nanosymbionts, an integrated framework in which AI guides the design and deployment of nanotechnology-enhanced CAR-T therapies. We explore how this convergence enables optimization of lipid nanoparticle formulations for mRNA transfection, specific targeting and modification of the tumor microenvironment, real-time monitoring of CAR-T cell behavior and toxicity, and improved in vivo CAR-T generation and overcoming barriers in solid tumors. Finally, it’s important we also address the ethical and regulatory considerations surrounding this emerging interface of living therapies and computational driven systems. The Smart CART Nanosymbionts framework (Figure 1:) represents a transformative step forward, promising to advance personalized cancer treatment toward greater precision, accessibility, and overall effectiveness.
1 Introduction
Personalized medicine is redefining approaches to cancer prevention, diagnosis, and treatment by leveraging each patient’s unique biological profile (1). Among its most significant advancements is CAR-T cell therapy, which involves genetically reprogramming a patient’s own T cells to recognize and eliminate cancer cells expressing specific antigens (2). Since the first approval by the U.S. Food and Drug Administration (FDA) in 2017, CAR-T cell therapy has provided critical treatment options for patients with recurrent leukemias, lymphomas, and myelomas, achieving unprecedented remission rates when conventional treatments have failed (3–6). In the field of autoimmunity, its benefits are beginning to be demonstrated mainly in systemic lupus erythematosus (7).
Despite its successes, several serious challenges impede broader adoption. Reliance on viral vectors for gene delivery introduces risks, including variable transfection efficiency, stringent regulatory requirements, and potential insertional mutagenesis (8–10). Such concerns have prompted regulatory agencies like the FDA to emphasize the urgent need for safer and more precise gene delivery methods (11). Off-target cytotoxicity also remains a major issue, manifesting in severe complications such as cytokine release syndrome (CRS), macrophage activation syndrome (MAS)/hemophagocytic lymphohistiocytosis (HLH), and neurological toxicities. Furthermore, CAR-T therapy is less effective in solid tumors due to immunosuppressive microenvironments and physical barriers that limit T-cell infiltration and function (8, 12, 13). It also comes with high expenses, almost $400,000 per patient and approaching $1 million with associated care (14–16).
Nanotechnology is emerging as a promising solution to these challenges. It enhances CAR-T cell persistence, infiltration, functionality and can provide non-viral gene delivery platforms. It also facilitates real-time monitoring of CAR-T cell activity and supports in vivo CAR-T generation, reducing the need for labor-intensive ex vivo processes (17–21).
Even with this new perspective, there are still cogs in the machine that could be better integrated. AI can streamline manufacturing workflows, automate complex data analyses, and refine the design for nano-driven CAR-T systems, enhancing both efficiency and effectiveness. Defined as the development of systems capable of performing tasks traditionally requiring human intelligence, AI employs advanced algorithms and self-learning models that adapt, identify patterns and make autonomous decisions (22–24). The integration of AI would allow for smart tuning of nanoparticle properties, such as size and surface charge, to optimize delivery efficiency and safety and in the context of CAR-T. Additionally, AI supports CAR-T optimization through predictive tools for patient selection, receptor design, cell classification and quality control, and early toxicity prediction. In this review, we explore how the fusion of nanotechnology and artificial intelligence can help address the current challenges facing CAR-T therapy and describe current AI-models applied to specific problematics. This approach has the potential to revolutionize how CAR-T therapy and nanotechnology come together, signaling a major leap forward in precision in oncology. We introduce a model we call Smart CAR-T Nanosymbionts and combined with the previous Addition by Subtraction model we authors proposed in previous reviews (Figure 1). A model designed to streamline the treatment of patients by reducing inefficiencies, lowering costs, and enhancing therapeutic outcomes through AI-powered nanotech in the context of pathologies targetable with CAR-T. This conceptual framework guides the structure of the review and offers a future-oriented lens for understanding how these technologies can reshape CAR-T innovation (25–28). We have created a glossary (Table 1) at the end of this paper for guidance.
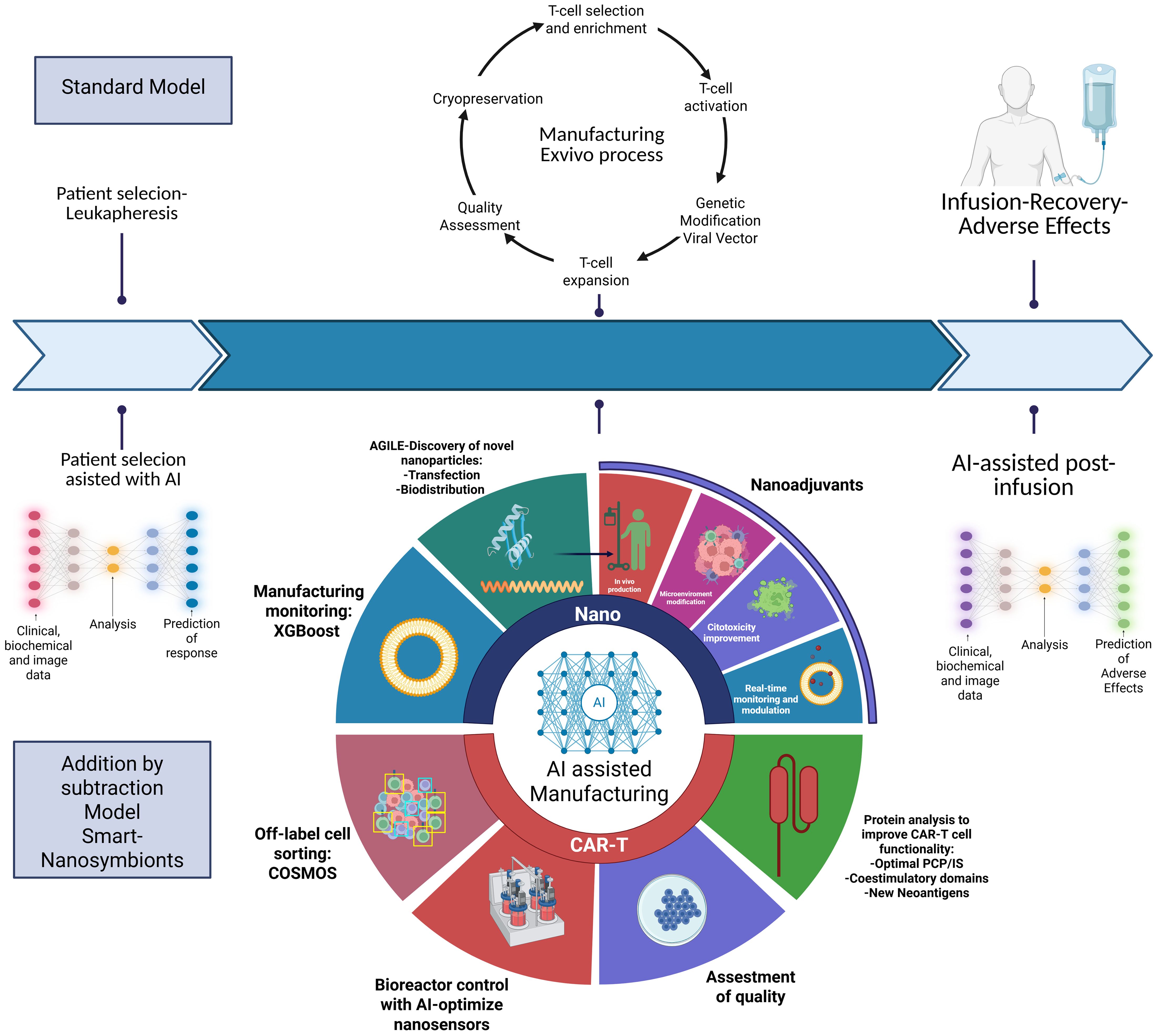
Figure 1. Compares the use of ML and DL in optimizing the production of advanced therapies, such as CAR-T cells and nanoparticles. In the ML section the algorithm can be trained for feature extraction, incorporating clinical data (such as biomarkers and immune responses) and manufacturing data (such as ethanol concentration and total flow rate). These inputs are analyzed to enable early prediction of CRS and ICANS toxicity and to improve the efficiency and quality of nanoparticle production. The DL section presents a more advanced approach using, ANNs, CNNs and GNNs. These technologies analyze proteins, RNA sequences, cellular imaging, and spatial representations. Key applications include the design of nanoparticles with enhanced tumor penetration, the optimization of CAR-T cells with greater cytotoxicity and persistence(CAR-Toner and motifs analysis), and the classification of cells based on their sensitivity or resistance to CAR-T treatment. Additionally, image-based predictions help assess cell sorting (COSMOS), therapeutic response and immune synapse quality. CRS, Cytokine Release Syndrome; ICANS, Immune Effector Cell-Associated Neurotoxicity Syndrome; ANNs, Artificial Neural Networks; GNNs, Graph Neural Networks.
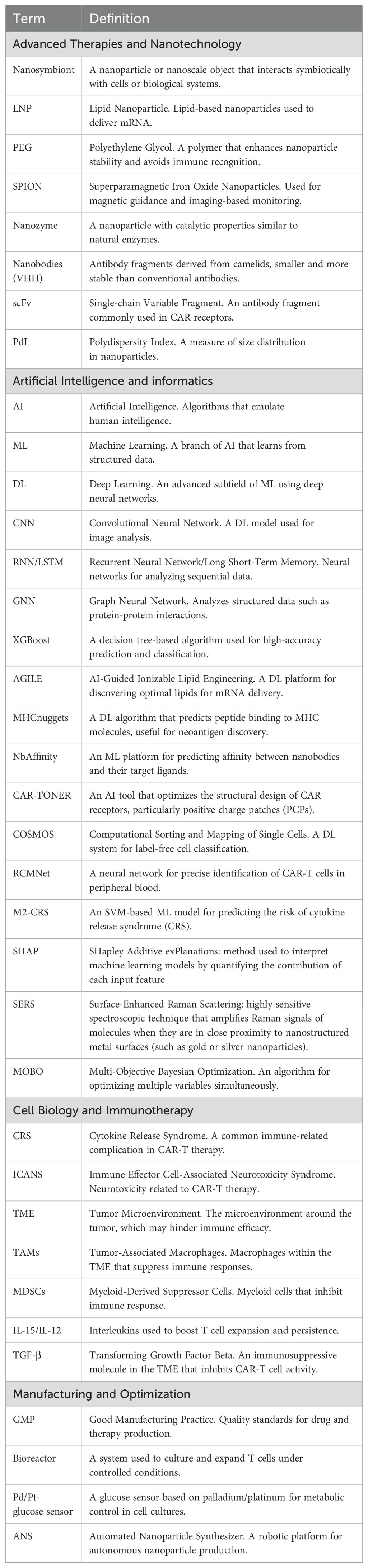
Table 1. Glossary.
2 CAR T-Cell Nanosymbionts: redifying the frontier of cellular immunotherapy with nanotech synergy
A nanosymbiont refers to a nanoscale entity that forms a symbiotic relationship with a host system, typically at the cellular or macromolecular level. These nanosymbionts are often engineered nanoparticles or smarter nano-devices—such as nanomachines and nanorobots—that interact beneficially with biological systems by mimicking or enhancing natural symbiotic functions. These nanosymbionts are often made from lipid-based nanostructures (like liposomes), polymeric nanoparticles, DNA/RNA nanostructures (e.g., nanosnowflakes) (259), Inorganic nanomaterials (e.g., gold or silica nanoparticles) (260).
The discovery of materials exhibiting unique and distinctive properties at the nanoscale (generally defined as structures with dimensions smaller than 100 nanometers) has led to the development of the multidisciplinary field of nanotechnology. This field encompasses the development, synthesis, characterization, and utilization of nanomaterials and nanodevices across various disciplines, including environmental science, electronics, energy, and medicine (261).
Nanoparticles possess a diverse array of tunable properties. These include customizable chemical compositions and internal structures, high surface-to-volume ratios, defined geometries, and distinctive electrical, magnetic, optical, and catalytic behaviors (e.g., nanozymes) (29–32). Their surfaces can be further engineered with functional ligands—such as pH-responsive polymers, polyethylene glycol (PEG), lipids, and biomolecules including antibodies and aptamers, to improve encapsulation efficiency, enhance bioavailability, and enable targeted interactions with biological systems (33–35). These characteristics make nanoparticles especially valuable in biomedical applications, notably for drug delivery. Their small size and surface engineering capabilities enable enhanced permeability and retention (EPR) effects, as well as controlled and sustained drug release. These features have significantly advanced their use in cancer therapy and diagnostics (18, 36–39). Moreover, nanoparticles can be designed to circumvent drug resistance—an obstacle commonly encountered in conventional chemotherapy. By conjugating ligands that selectively bind to receptors overexpressed on cancer cells, nanoparticles can deliver therapeutic agents directly to tumor sites (smart drug delivery systems). This targeted delivery minimizes collateral damage to healthy tissues, improves therapeutic efficacy, and enhances imaging precision (36, 40–44). Consequently, nanotechnology provides innovative strategies to enhance the efficacy, specificity, and safety of cancer treatments, offering potential cost-effective alternatives to traditional methodologies (45, 46). Synthetic nanomachines (nanoconverters, Janus nanomotor, etc.) or nanorobots (ultrasound-propelled biomimetic nanorobot) introduced into cells to perform functions like detoxification, sensing, or energy generation (47–49). Also, nanoparticles that help reprogram immune cells (like CAR-T cells) or interact with microbiota to influence host health.
This field is transforming CAR T-cell design by creating precise, multifunctional platforms that address key therapeutic challenges. For instance, lipid-based and polymer nanoparticles have been developed to deliver mRNA encoding CAR constructs directly into T cells, circumventing safety concerns associated with viral vectors and ensuring efficient delivery with reduced immunogenicity (50, 255). Furthermore, nanotechnology plays a crucial role in developing in vivo CAR T-cell therapies, wherein nanoparticles deliver CAR-encoding materials directly to circulating T cells within patients (51–54). Additionally, nanomachines can selectively target different lymphocyte subtypes via surface-attached antibodies, facilitating precise genetic material delivery. Virus-like nanoparticles engineered for systemic gene therapy demonstrate prolonged circulation time, reduced immunogenicity, and efficient and safe gene delivery to target cells (18).
There are numerous stages in the development of CAR-T cells and aspects of tumor biology where nanotechnology can be effectively integrated. The following are examples of how these two technologies have been successfully combined. The immune synapse (IS) is crucial for car t cell activation, triggering cytotoxic T lymphocytes (CTLs) and CAR-IS shows higher expression of molecules with antiapoptotic and antiproliferative (55, 56). To potentiate this effect, agents like histone deacetylase inhibitors (HDACi), such as panobinostat, can enhance Fas-mediated apoptosis, improving antitumor efficacy (57). Nanocarriers, such as poloxamer 407-based nano-micelles, enhance intracranial delivery of panobinostat in glioma models, increasing therapeutic concentration and tumor response (56).
Precise interaction between the CARs and tumor cell epitopes is essential for CAR T cell function. The scFv fragment, the CAR’s antigen-binding domain, can suffer from misfolding, aggregation, and overstimulation of T cells, leading to early exhaustion. Nanobodies, small, single-domain antibodies derived from camelids, due to their compact size, high stability, and reduced immunogenicity can avoid misfolding and aggregation ensuring a more controlled activation of CAR T cells, preventing the overexpression of cytotoxic signals that could prematurely exhaust the T cells. Nanobodies improve antigen recognition, leading to a stronger and more durable synapse between the CAR T cells and tumor cells. They can also serve as modular structures that facilitate the redirection of universal CAR T cells to target various tumor antigens, further enhancing the precision and adaptability of the therapy (55).
In solid tumors, interferon-γ receptor (IFNγR) signaling is critical for cell adhesion after CAR T cell treatment and its impairment can derive in CAR T cell binding reduction and resistance (58).
SCH-58261-loaded cross-linked multilamellar liposomes with maleimide functionalization on the surface of CAR T cells have been designed in models of ovarian cancer and chronic myelogenous leukemia to target the A2a adenosine receptor (A2aR) inhibitory pathway involved in T cell receptor signaling inhibition and IFNγ production through elevated intracellular cyclic AMP adenosine levels that are increased in the tumor microenvironment. These liposomes enhance the colocalization of nanoparticles in sensitive tumor areas and prolonging tumor growth inhibition by targeting the A2a receptor pathway (59).
To broaden the targeting landscape, aptamers (short, single-stranded nucleic acids capable of binding to target cancer cells with high specificity and affinity) are functionalized with nanocarriers to deliver cytokines, immune checkpoint inhibitors, or cytotoxic agents directly to the tumor site. This expands the antigenic repertoire beyond conventional antibody recognition. The SELEX (Systematic Evolution of Ligands by Exponential Enrichment) technique enables identification of high-affinity aptamers, which, when combined with nanodevices, enhance immune synapse formation and therapeutic delivery (60).
T cell exhaustion, one of the main concerns regarding efficacy and resistance in CAR T cell therapy, occurs due to increased inhibitory signals from molecules such as PD-1, Tim-3, LAG-3, VISTA, CTLA-4, and TIGIT, affecting both tumor cells and T lymphocytes (61). Magnetic nanoclusters, equipped with PD-1 antibodies, utilize a pH-sensitive bond for attachment and bind to effector T cells through PD-1 receptors. In an acidic environment, they release anti PD-L1 antibodies, blocking PD-1 interactions and maintaining CTL functionality above 90% while delaying tumor progression. The treatment also reduced the abundance of Tregs and increased the abundance of CD8+ CTLs in tumor-bearing mice (62). Moreover, the conjugation of liposomes and synthetic nanoparticles with CD8+ T lymphocytes via maleimide-thiol coupling provides continuous pseudoautocrine stimulation of transferred cells. Following this rational, some research groups have developed multilamellar lipid nanoparticle core loaded with IL-15 and IL-21 to release cytokines in very low doses over several days resulting in significantly higher proliferation compared to systemic infusion (63).
Epitope spreading arises because of residual dying tumor cells are captured and processed by APCs. This leads to the presentation of novel peptides via MHC class I and II molecules, thereby priming naïve T cells to recognize and attack tumor-associated antigens distinct from those originally targeted by CAR T cells. This secondary immune activation broadens the anti-tumor response beyond the specificity of the initial CAR construct. Tumor cryptic antigens must be presented on MHC Class I molecules, engaging cytotoxic CD8+ T cell responses via cross-presentation, primarily performed by specific APCs (64). Dendritic mesoporous silica nanoparticles (DMSNs), modified with hyaluronic acid and covalently bound to anti-CD3, anti-CD28, and anti-PD-1, facilitate T cell activation and antigen cross-presentation, enhancing IFN-β secretion and MHC upregulation and reducing the likelihood of the cells escaping immune surveillance (65). Additionally, dendritic cell-biomimetic nanoparticles and dendritic cell-mimicking nanovaccines (nanoDCs), fabricated from mature bone marrow-derived DC membranes loaded with TAAs improve CD8+ T cell priming, reduce tumor size, and inhibit metastasis (66, 67). In parallel, other approaches have explored the use of lipopolyplex platforms, in which mRNA molecules are encapsulated within a polymeric polyplex core and subsequently enclosed in a phospholipid bilayer shell. This architecture enables the delivery of mRNA encoding multiple tumor-associated antigens, while concurrently acting as an adjuvant by engaging Toll-like receptor (TLR) signaling in APCs. These nanoconstructs have demonstrated efficiente uptake by dendritic cells, promoting robust antigen presentation, and the bilayer shell effectively prevents nonspecific interactions of the mRNA core with non-target cells, thereby reducing off –target effects and systemic toxicity (68).
Moreover, the tumor microenvironment—through stromal and myeloid cells, angiogenesis, and cytokines like TGF-β—impairs CAR T cell trafficking, infiltration, and cytotoxic function, significantly limiting their efficacy in solid tumors (69). Nano-backpacks utilize T lymphocytes as vehicles to take loaded nanoparticles to tumor microenvironment. Liposomes loading a potent small molecule that works as an inhibitor of the TGF-β receptor I restore granzyme B expression to a higher level than systemic TGF-β inhibitors. Also, these liposomes promoted division and expansion of T cells (70). In line with other backpacking strategies, chemically tethering an interleukin-15 superagonist to T cells via drug-releasing protein nanogels anchored to CD45 has shown enhanced intratumoral expansion. These nanogels are activated upon antigen engagement within the tumor microenvironment, resulting in a 16-fold increase in T cell proliferation compared to systemic cytokine delivery, and over 1,000-fold compared to T cells lacking cytokine support (71).
Other components of TME such as fibrotic stroma and compressed vasculature can be bypassed through photothermal strategies. CAR T cells engineered with indocyanine green nanoparticles (CT-INPs) generate localized heating upon NIR exposure, causing 98% tumor cell death and promoting vasodilation and immune infiltration (72). In addition, vascular-targeted nanorobotics offers a radical approach. DNA origami nanobots loaded with thrombin selectively induce tumor thrombosis by releasing their cargo upon receptor binding, starving the tumor (73).
Strategies currently used by clinicians to follow activity of infused CAR T cells are invasive and do not provide real-time whole-body spatio-temporal distribution of infused T cells. There is a clinical need for a technique that can monitor in vivo performance of CAR T cells in tumors and off-target sites. Ferumoxytol (iron oxide nanoparticles detected by MRI) can be used as a cell marker to monitor real time in vivo CAR T cell in preclinical osteosarcoma model. These CAR T cells are identified through MRI, photoacoustic tomography (PAT), and magnetic particle imaging (MPI). Tumor demonstrates iron enhancement on T2-weighted MRI only in the ferumoxytol-labeled B7-H3 CAR T cell group indicating enhanced infiltration of the T cells in the tumor tissue (20). Similarly, CAR T cells co-expressing CD19 and luciferase can be radiolabeled with gold nanoparticles functionalized with copper-64 and PEG (GNP-64Cu/PEG2000), allowing long-term PET imaging that correlates with bioluminescent signal, confirming the possibility of tracking CAR T cells using positron emitter imaged by PET/CT scanner (21).
Finally, the conventional design of CAR T cells may elicit unpredictable toxicities due to their inherent capacity for expansion, persistence, and recognition of both malignant and non-malignant cells expressing tumor-associated antigens. Reversible control of CAR T activity has been demonstrated using the tyrosine kinase inhibitor dasatinib (DAS), which blocks CD3ζ ITAM phosphorylation, thereby suppressing CAR T effector function and mitigating acute toxicities. However, DAS presents pharmacokinetic limitations, including poor water solubility, pH-dependent absorption, and a short half-life (3–4 h). To address this, a pH-sensitive nanoparticle linking DAS to hyaluronic acid (DAS-HA) enables targeted release in the acidic tumor microenvironment, enhancing intracellular DAS accumulation and improving the safety and efficacy of CAR T modulation (74, 75).
Summary of the applications described in the text are found in Table 2 and Graphical representation in Figure 2:
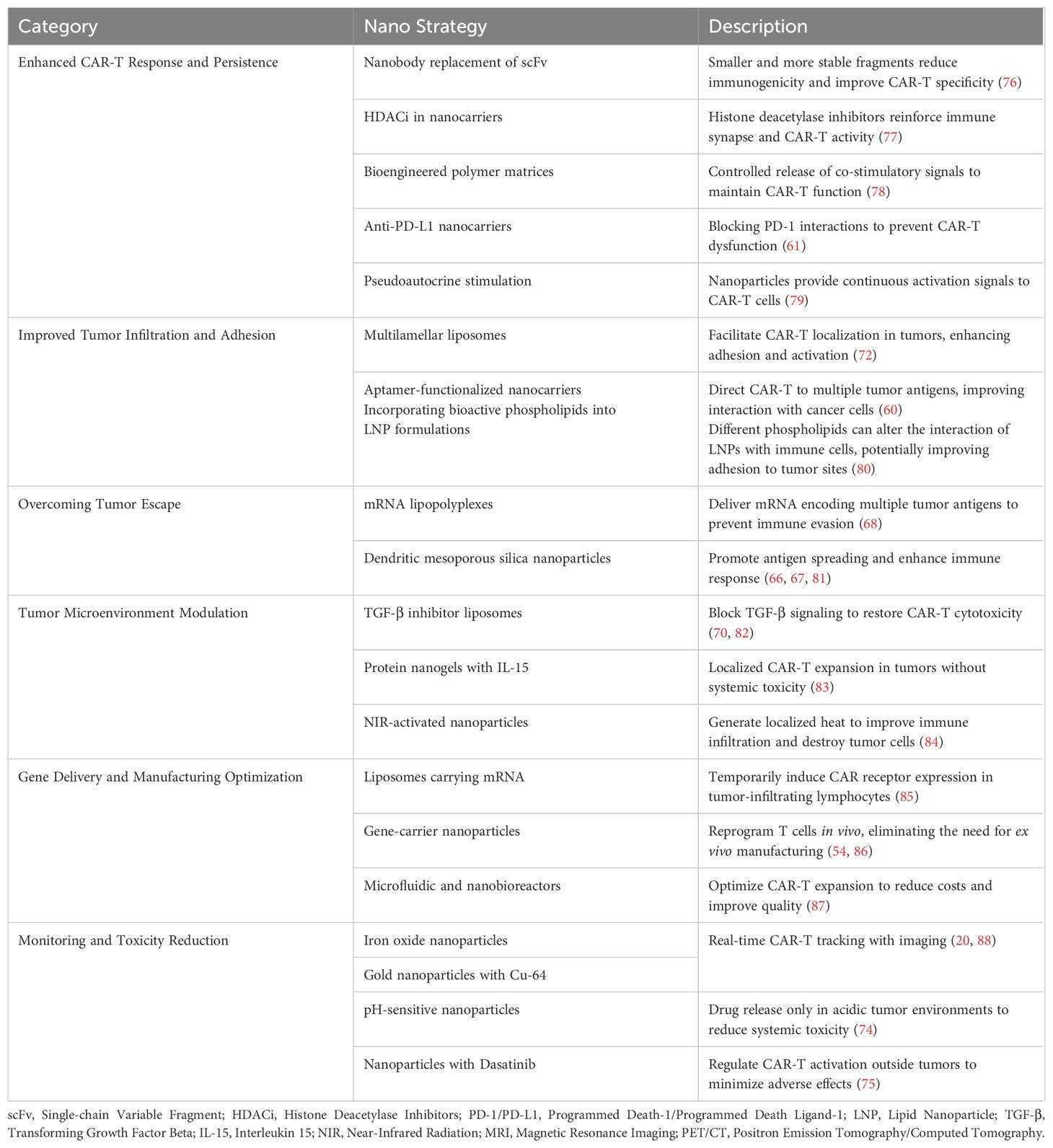
Table 2. Nanotechnology application in CAR-T therapy.
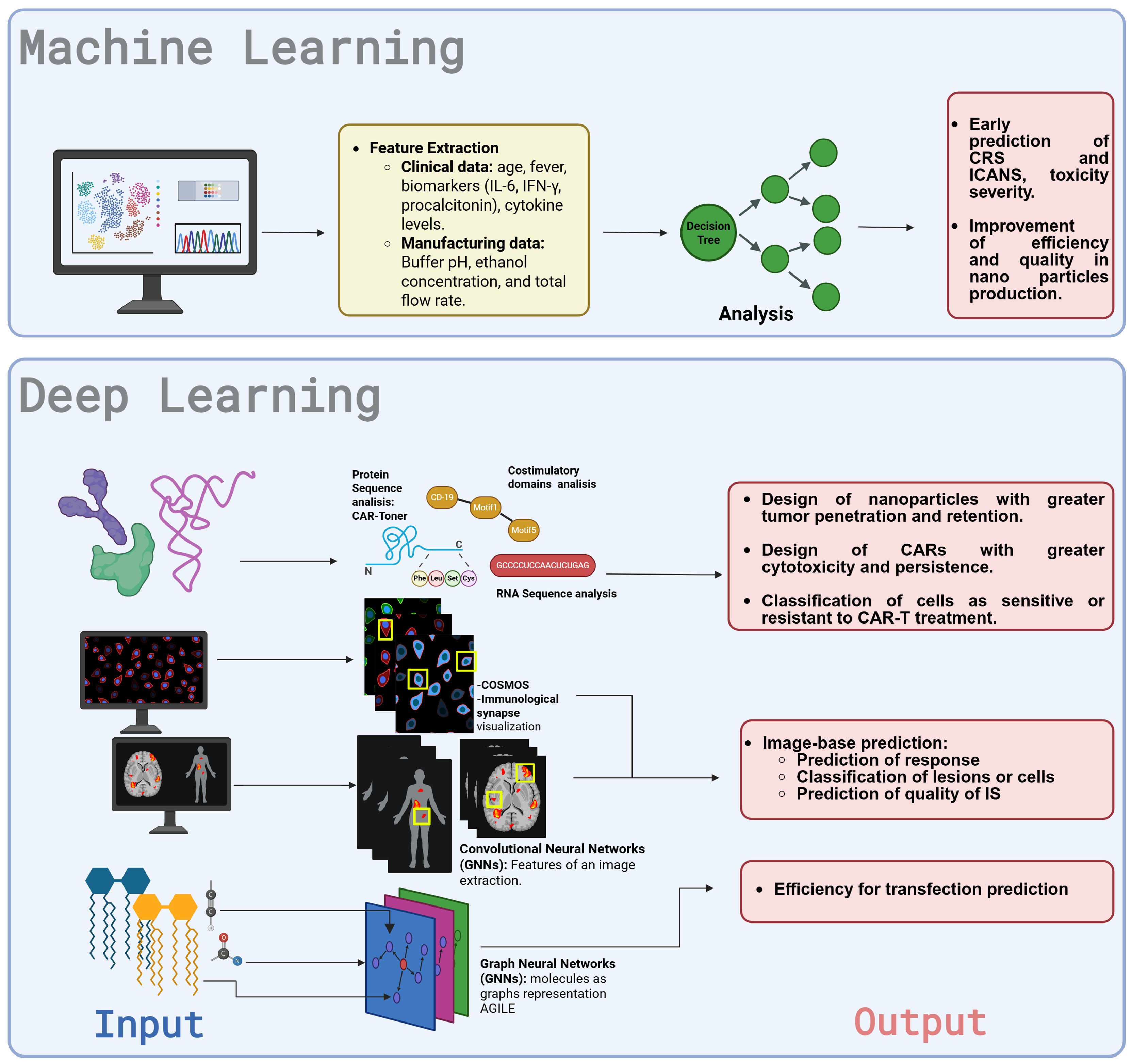
Figure 2. The conventional CAR-T cell manufacturing model involves a complex ex vivo process with multiple steps, including leukapheresis, T-cell selection, genetic modification using viral vectors, expansion, and cryopreservation before infusion, leading to high costs, long production times, and logistical challenges. The “Addition by Subtraction Model: Smart CAR-T Nanosymbionts “ model integrates AI and nanotechnology to streamline production by reducing process steps, replacing viral vectors with non-viral alternatives (e.g., nanoparticles), and leveraging in vivo genetic modification to enhance efficiency. AI-driven patient selection analyzes clinical, biochemical, and imaging data to predict response, while AGILE-based discovery of nanoparticles optimizes transfection and biodistribution for improved CAR-T functionality. AI-enhanced bioreactor control using nanosensors ensures real-time monitoring and quality assessment and technologies like COSMOS helps in label-free sorting cells, refining the final CAR-T product. Additionally, AI-driven protein analysis optimizes CAR structure by improving peptide-CAR interactions, refining co-stimulatory domains, and identifying new neoantigens to enhance efficacy. Post-infusion, AI assists in predicting and managing adverse effects, while nanoadjuvants dynamically regulate CAR-T function, mitigating toxicity, preventing exhaustion, promoting epitope spreading, and strengthening the immunological synapse (IS). This AI- and nanotechnology-driven approach enhances CAR-T therapy by improving safety, reducing costs, and increasing accessibility, marking a significant advancement in cancer immunotherapy. Created with BioRender.com.
3 Machine intelligence in motion: from algorithms to autonomy
AI encompasses a wide range of subfields and methodologies aimed at replicating or augmenting human-like intelligence in machines (89). Rather than representing a single technology, AI consists of a diverse set of interconnected tools and systems with vast potential, particularly in the healthcare domain (90). One of its most prominent branches is machine learning (ML), which focuses on developing systems capable of learning from historical data. These systems leverage algorithms trained on context-specific features within structured datasets to identify patterns and generate predictions, using approaches such as supervised, unsupervised, or reinforcement learning (24, 91). In healthcare, ML is commonly applied to structured medical data for tasks such as early disease detection, prediction of therapeutic responses, and optimization of clinical resource allocation (92, 93). Within ML, deep learning (DL) represents an advanced subcategory that employs artificial neural network-based algorithms to process and analyze large-scale datasets with complex structures (94). Unlike traditional ML techniques, DL excels at uncovering intricate correlations that are often undetectable using conventional methods. One of its core advantages lies in its ability to autonomously perform feature extraction from unstructured data such as medical imaging, genetic sequences, or clinical text, thereby eliminating the need for manual preprocessing. These capabilities have made DL particularly valuable in areas such as drug discovery and the detection of cancerous lesions in radiological images (92, 95, 96).
Among the algorithms encompassed within DL are convolutional neural networks (CNNs) and recurrent neural networks (RNNs), which are designed to replicate biological processes for data analysis. CNNs process visual data by extracting local features at various levels of depth, enabling the identification of complex patterns in images (97, 98). These representations are typically complemented by Multilayer Perceptron (MLP) layers (fully connected neural networks), which are responsible for performing the final classification based on the extracted features (99). In contrast, RNNs—including Long Short-Term Memory (LSTM) networks—capture temporal dependencies in tasks such as language modeling, DNA sequence analysis, and continuous time series prediction, making them valuable for both classification and regression problems (100). These architectures enhance drug–target interaction prediction, pharmacokinetic modeling, and toxicity assessment (101, 102), addressing the high expenses, time demands, and ethical concerns of traditional experimental methods (101, 103). A summary of the current AI-models utilized in healthcare are found in Table 3. Integrating AI with CAR-T therapy and nanotechnology presents remarkable opportunities for enhancing treatment design, delivery, and development, driving advancements in personalized medicine. Current advances in AI for nanotechnology and CAR-T therapy, independently, are shown in Figure 3.
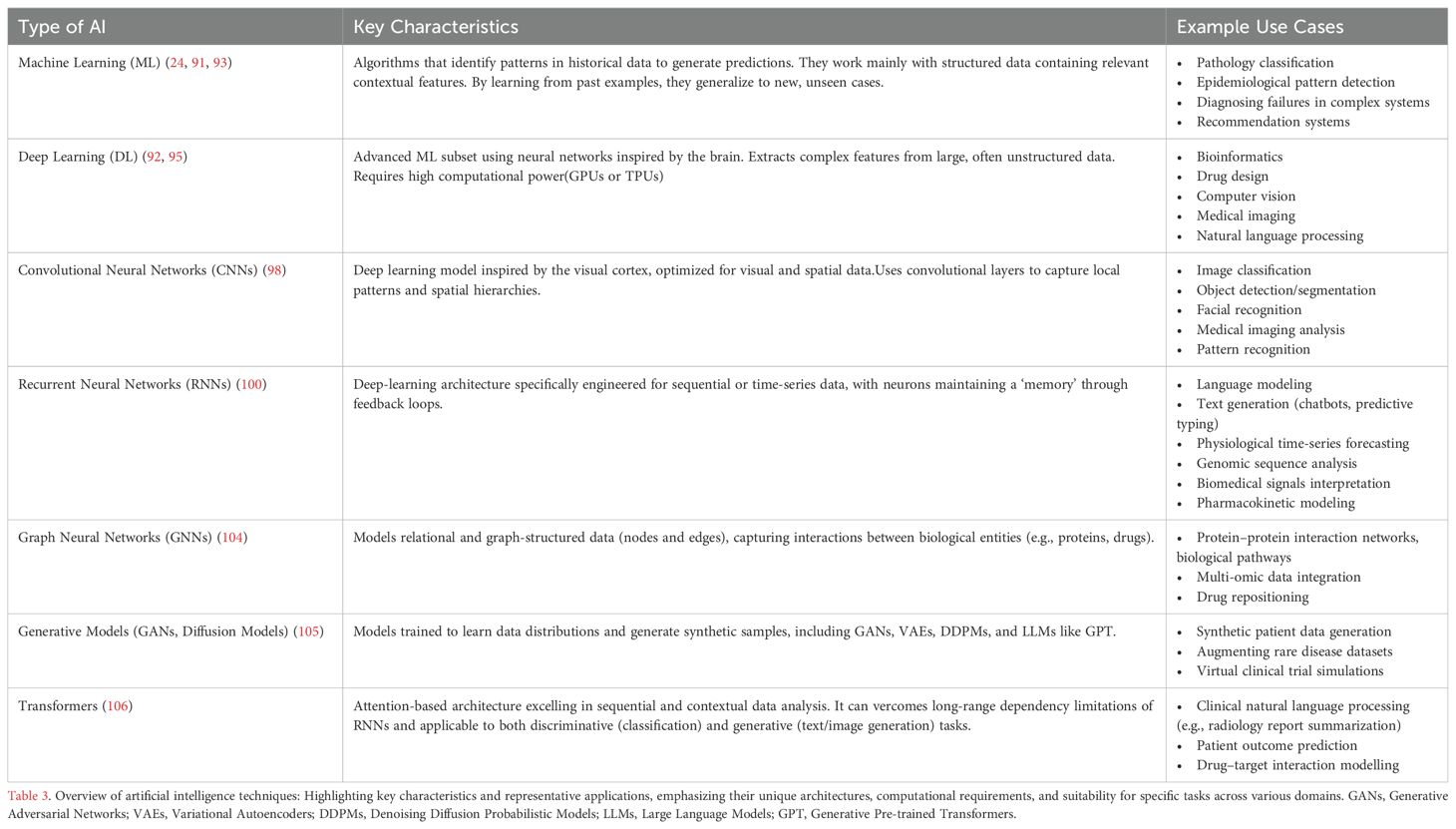
Table 3. Artificial Intelligence types and their applications.
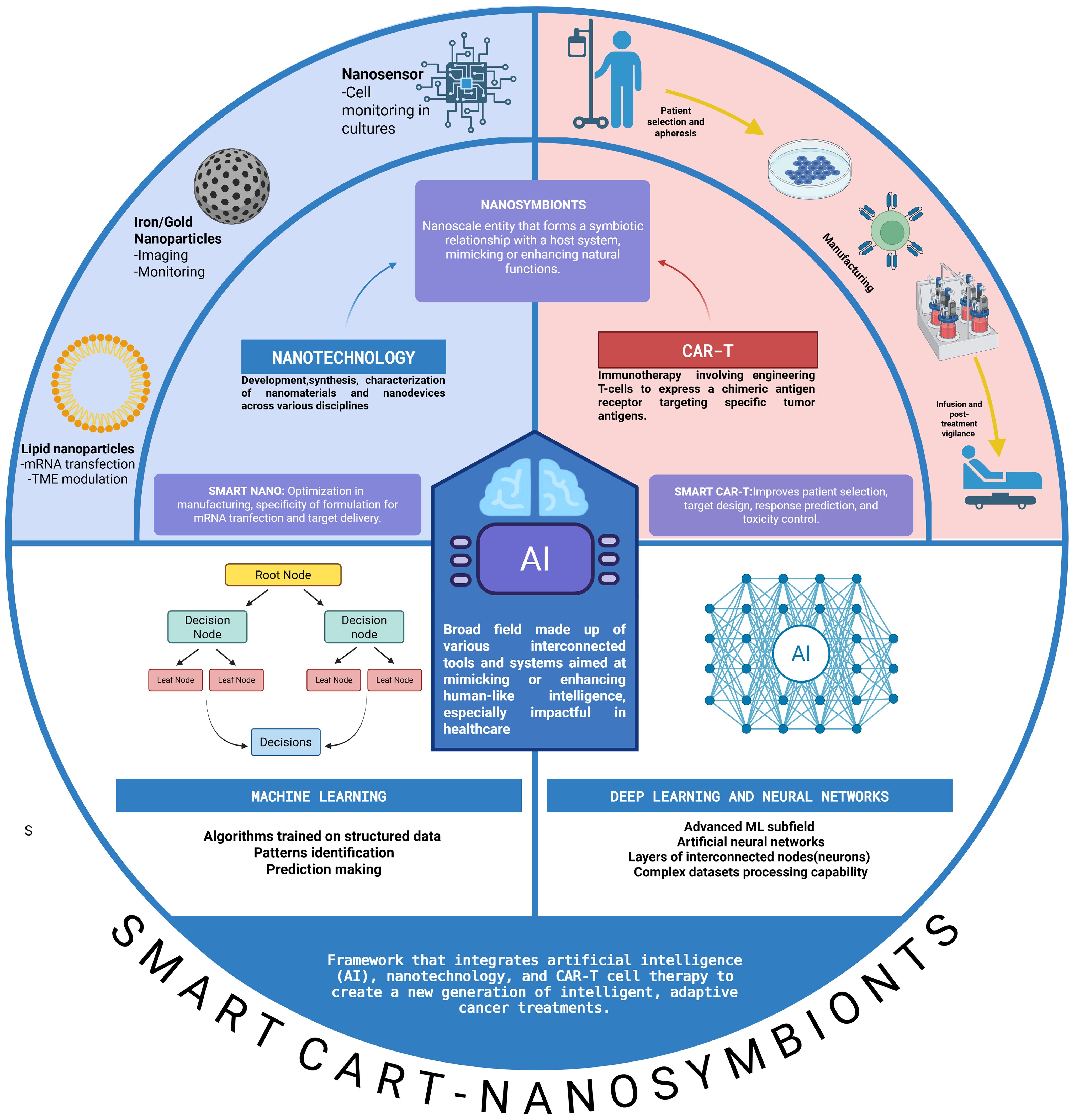
Figure 3. Schematic representation of lipid, polymer, inorganic, and hybrid hydrophobic polymeric nanoparticles (NPs) and the possible advantages of using nanotechnology in CAR T cells (1): Tumor microenvironment remodeling: using indocyanine green nanoparticles plus infrared light irradiation to disrupt the ECM before CAR administration, using targeted nanocarriers with in vitro transcribed mRNA to reprogram TAMs and downregulate PD-L1, and using nanozymes and nanoparticle backpacks. (2) Improving T cell proliferation and lifespan with mesoporous silica micro-rods secreting IL-2, APC cell-membrane mimics, using RNA-LPX to activate T cells, and NPs linking APCs to prime and activate T cells. (3) Improving follow-up and resistance with genetic programming using mRNA nanocarriers for targeted gene expression and NBiTE generation and radiolabeled NPS to track T cells in vivo. APC, antigen-presenting cell; ECM, extracellular matrix; IL-2, interleukin-2; NBiTEs, nano-bispecific T cell engagers; NPs, nanoparticles; PD-L1, programmed cell death ligand-1; TAMs, tumor-associated macrophages. Created with BioRender.com. Taken with permission from: Baena JC, Pérez LM, Toro-Pedroza A, Kitawaki T, Loukanov A. CAR T Cell Nanosymbionts: Revealing the Boundless Potential of a New Dyad. Int J Mol Sci. 2024 Dec 7;25(23):13157. doi: 10.3390/ijms252313157. PMID: 39684867; PMCID: PMC11642191.
4 Synergy of code and cell: AI-powered revolution of CAR-T cell therapies
The integration of AI into CAR-T cell therapies has opened a transformative avenue toward precision oncology, significantly enhancing therapeutic outcomes through optimized patient selection, streamlined manufacturing, CAR design optimization, and accurate prediction of adverse effects. By manipulating advanced computational models and deep learning algorithms, AI addresses critical limitations within current CAR-T cell protocols, such as inconsistent patient responses, complex manufacturing processes, receptor optimization challenges, and treatment-associated toxicities. This section systematically reviews current evidence and applications demonstrating how AI-driven solutions for CAR-T therapy
4.1 Patient selection
Accurate patient selection is essential for the successful implementation of advanced therapies such as CAR-T cell treatment. AI improves patient selection by integrating and analyzing clinical data, such as demographic variables, laboratory results, imaging biomarkers, to identify complex, non-linear correlations that often go unnoticed by conventional statistical methods. By training on large volumes of data, AI models can learn patterns that link specific patient characteristics with therapeutic response or toxicity risk. This enables the stratification of patients based on response or clinical risk, supporting more personalized and evidence-based decision-making (107, 108).
In the pivotal JULIET trial, patients with relapsed or refractory diffuse large B-cell lymphoma (DLBCL) who received a single infusion of Tisagenlecleucel demonstrated a 53% overall response rate (ORR) and a 39% complete response rate (CR). However, significant challenges persisted, evidenced by a median progression-free survival (PFS) of only 2.9 months, with 62% of patients ultimately experiencing disease progression or death. To address these limitations, secondary analyses utilized AI to enhance predictive outcomes and patient stratification. Integrating pre-infusion FDG PET/CT imaging with clinicopathological data, AI models, particularly attention-gated AG-CNNs, were applied to delineate disease foci and improve outcome predictions. The AI analysis revealed that 52.4% of patients exhibited a negative AI signature, and all patients in this group experienced poor outcomes. In contrast, 47.6% had a positive AI signature, of whom 55.6% experienced poor outcomes (109). These findings highlight AI’s ability to classify patients into distinct prognostic groups, particularly those at high risk of poor outcomes.
Similarly, a study on 39 adult B-cell lymphoma patients treated with CD19 CAR-T cells used transfer learning(a deep learning technique) to analyze 770 lymph node lesions. Pre-treatment diagnostic CT (dCT), low-dose CT (lCT) from PET/CT, and FDG-PET images were assessed to predict responses at both lesion and patient levels. Lesion response was defined by size or metabolic activity reduction. Using AlexNet, a pre-trained CNN-MLP, researchers achieved 82% accuracy in lesion-level predictions, outperforming the International Prognostic Index (IPI) in sensitivity, specificity, and accuracy (110).
Beyond imaging-based response prediction, researchers have also applied AI for response prediction using RNA sequencing data. A study of 39 mantle cell lymphoma patient samples (30 sensitive, 9 resistant to CAR-T treatment) employed single-cell RNA sequencing and performed differential gene expression analysis to identify genes that were expressed differently between sensitive and resistant samples. A total of 1,236 different genes were identify. The differentially expressed genes were used as inputs for a MLP. The number of neurons in the input layer corresponds to the number of differentially expressed genes, while the output layer consists of two neurons representing the probability of the patient’s categorical response labels (sensitive or resistant). The model achieved an average accuracy of 90.07% in classifying cells based on the genes expression as sensitive or resistant to therapy (111).
Collectively, these studies highlight AI’s role in improving patient selection and outcome prediction for CAR-T therapy compared to traditional methods and opens new avenues for personalized treatment strategies.
4.2 CAR-T cell extraction, isolation and quality assessment
CAR-T cell production is complex and demands strict quality control to ensure safety and efficacy. As the demand for cell and gene therapies increases, automating manufacturing processes will become critical to achieve enhanced standardization. Innovations that eliminate intermediary steps, such as T cell separation using magnetic beads or nanomatrices coated with anti-CD3 and anti-CD28 antibodies (112), can substantially reduce production timelines, resource usage, and contamination risks inherent to manufacturing processes (113). Traditional flow cytometry (FCM) techniques also play an essential role in assessing cell populations; however, conventional methods involving fluorescent staining with antibodies and chemical reagents may compromise cell function, introduce toxicity, and reduce viability (114). Additionally, meeting Good Manufacturing Practice (GMP) standards necessitates specialized personnel, further increasing costs and operational variability (115, 116). These factors hinder the efficient scale-up of CAR-T cell production.
AI-driven sorting systems like ghost cytometry (GC), introduced by K. Sugimoto et al., offer a label-free alternative to antibody-based cell sorting. With this tool developed in 2020, cells are illuminated during imaging to produce distinct optical signatures and waveforms, reflecting various aspects of cell morphology and behavior. ML analyzes these aspects, enabling high-speed sorting when integrated with microfluidics. By training ML classifier with temporal and frequency-domain features extracted from the specific waveforms generated by each cell, allowing the capture of relevant morphological information, GC accurately distinguishes live from dead cells and identifies CD3-positive T cells in peripheral blood mononuclear cells (PBMC) populations (117). By 2024, label-free GC (LF-GC) further improved precision, differentiating live vs. apoptotic cells, T cells vs. non-T cells, and detecting particulate impurities. These advancements enhance real-time cell monitoring and quality control in cell therapy manufacturing without the need for surface markers or stains (118).
Other approaches like COSMOS (Computational Sorting and Mapping of Single Cells), combines high-resolution imaging, DL, and microfluidics for real-time, label-free cell sorting. Using brightfield microscopy, it captures cellular images and analyzes size, shape, and structures. Using deep learning with CNNs and MLPs, it classifies cells by mapping their features into a representation space, enabling accurate and real-time identification (119). Other AI-enhanced systems like DeepCell integrate high-content imaging with neural networks to predict cell identity and function in real time. These platforms enable morphological profiling without staining and support cloud-connected analytics for remote QC, offering potential scalability for GMP-compliant CAR-T production (120).
Computer vision plays a fundamental role in enhancing these image-based sorting technologies by enabling the automated extraction of detailed morphological and structural features from high-resolution cellular images. This field within deep learning allows for accurate, real-time classification without the need for chemical staining, significantly improving throughput, consistency, and viability in CAR-T cell manufacturing. This integration accelerates decision-making and ensures greater standardization in cell quality assessment (121).
4.3 CAR design and optimization of T cell function
A key goal is engineering T-cell phenotypes that enhance cytotoxicity while maintaining a stem-like state for long-term persistence, which its traditionally made on trial-and-error methods (110). Neural networks can expedite CAR development by analyzing large datasets that integrate receptor structures with therapeutic outcomes.
One study constructed a library of costimulatory domains by recombining 13 signaling motifs, generating 2,379 unique combinations with distinct phenotypic traits. For instance, the 4-1BB domain enhances persistence, while CD28 boosts cytotoxicity but reduces longevity (122). ML models analyzed these motif interactions and generated diverse T-cell phenotypes, including separate cytotoxicity and stemness traits not typically observed with natural domains. This predictive approach significantly expands exploration of receptor combinations, potentially advancing the development of precise and potent cellular therapies (123).
Costimulatory domains also influence IS quality, directly affecting CAR-T activation and cytotoxicity. Unlike conventional T cells, CAR-T cells form disorganized IS structures, initiating rapid signaling via Lck/ZAP70 and exhibiting “serial killer” activity (17, 55, 56, 124–126). Traditional prediction methods, such as flow cytometry and in vivo models, are resource-intensive and inconsistent (127). In response to these challenges, researchers developed a DL tool that improves IS analysis using clinical trial data. They employed a segmentation neural network to accurately delineate kappa-CAR-T cells within the images, followed by a classification network that predicted therapeutic response based on the morphological analysis of the immunological synapse. This approach proved effective even in low-contrast images, accurately distinguishing between treatment responders and non-responders (128). Other approaches use the images obtained by optical diffraction tomography (ODT) combined with DL, which allows automated 3D IS tracking by segmentation and classification, further refining CAR-T assessments (129).
Beyond IS dynamics, tonic signaling is crucial for CAR-T function. This baseline signaling, independent of antigen engagement, must be carefully regulated—too little weakens persistence, while excessive signaling induces exhaustion (130–132). CAR antigen-binding domains with positive charge patches (PCPs) promote clustering, influencing tonic signaling (130). AI-driven tools like CAR-Toner leverage structural data from (Protein Data Bank)PDB and AlphaFold to optimize PCP scores, improving CAR-T expansion and reducing exhaustion. This method was validated in camelid single-domain nanobody (VHH)-based CARs targeting CLL1 in acute myeloid leukemia, identifying an optimal PCP score range (43–52, 255) that correlates with superior CAR-T function (133).
4.4 Adverse effect prediction
CAR-T therapies represent a breakthrough in cancer treatment but carry risks such as Cytokine Release Syndrome (CRS), Immune Effector Cell-Associated Neurotoxicity Syndrome (ICANS), and On-Target, Off-Tumor Toxicity (OTOT).These toxicities significantly impact clinical outcomes, requiring effective management strategies and early detection of this complications often rely on clinical observation, scoring and are often subjective and time-intensive (134, 135). CRS, the most common complication, affects 30%–100% of patients, with severe cases (grade ≥3) occurring in 10%–30% (136, 137). It results from excessive cytokine release and endothelial activation, leading to increased vascular permeability, hypoperfusion, coagulopathy, and potential multi-organ dysfunction (138–141).
To enhance early detection, ML models like M2-CRS have been developed. This meta-analysis-informed ML approach integrates statistical data from clinical studies with ten predictive cytokine biomarkers, including IL-2, IL-6, IFN-γ, and GM-CSF. By leveraging a robust Knowledge Base (KB) of cytokine interactions, M2-CRS addresses data scarcity while maintaining high interpretability. The model, based on Support Vector Machines, consistently achieves accuracy and precision above 90%, making it a promising tool for CRS risk stratification and timely intervention. To further enhance interpretability, SHapley Additive exPlanations(SHAP) values were applied, allowing the identification of the most influential features within the model. This analysis revealed IFN-γ and IL-10 as the most relevant proteins contributing to CRS risk prediction in acute myeloid leukemia and B cell Lymphomas (142).
ICANS, another significant CAR-T toxicity, affects 30%–50% of patients, with severe cases in 12%–30% (143). It arises from cerebral endothelial activation, blood-brain barrier disruption, and cytokine-induced astrocyte and pericyte dysfunction, leading to cerebral edema, thrombosis, hemolysis, and disseminated intravascular coagulation (DIC). Logistic regression model can analyze longitudinal patient data faster, predicting ICANS onset and severity with accuracy of 77%. By identifying key risk factors such as age, fever, IL-6 levels, and procalcitonin, ML can forecast ICANS progression up to three days in advance. This predictive capability enhances clinical decision-making, optimizing resource allocation, hospitalization planning, and early therapeutic interventions (144).
5 Smart CAR-T Nanosymbionts: AI-nanotech interface empowering living CAR-T therapeutics
The features of nanotechnology and artificial intelligence, previously applied independently in CAR-T therapy, can be seamlessly integrated, offering transformative potential throughout CAR-T design and functionality. Our interface “Smart CAR-T Nanosymbionts” represents an advanced AI-nanotechnology boundary designed to optimize many aspects of CAR-T therapy, including manufacturing, in vivo efficacy, and patient monitoring. This model enhances scalability and precision in nanoparticle formulation, facilitates structural modeling and simulations for CAR engineering, and provides real-time monitoring capabilities. Additionally, it proactively detects and manages adverse effects, creating a comprehensive system that maximizes therapeutic performance
5.1 AI-Driven optimization of CAR-T cell and nanoparticle manufacturing: from mRNA Delivery to antigen targeting
CAR-T cell and nanoparticle production are interdependent biotechnological processes, requiring precise control for consistency and efficacy. Nanoparticles are essential for mRNA-based CAR expression, facilitating gene delivery to T cells, but large-scale manufacturing faces challenges in maintaining size, charge, and composition. Batch variability affects cellular uptake and gene transfer, making precise formulation critical (145, 146). Similarly, CAR-T cell production demands careful monitoring of viability and expansion in bioreactors.
Integrating real-time monitoring with ML can optimize synthesis parameters, reducing variability and enhancing scalability in both nanoparticle formulation and CAR-T manufacturing (147, 148). Lipid nanoparticles (LNPs) are currently the most widely utilized carriers for mRNA delivery, comprising ionizable lipids, phospholipids, cholesterol, and PEG-lipids (149–151). Ionizable lipids facilitate protein expression, while nanoparticle size and charge critically influence cellular uptake, immune responses, and delivery efficiency; therefore is essential to ensure consistent and effective large-scale production (152–155). XGBoost is a gradient boosting algorithm based on decision trees, known for its high predictive accuracy and computational efficiency in structured data. It builds models iteratively, adding new trees to correct previous errors while balancing accuracy and complexity through regularization. In the context of nanoparticle production, XGBoost has demonstrated significant effectiveness in optimizing nanoparticle production. Sato et al. used XGBoost to predict key parameters in the manufacturing of lipid LNPs, such as particle size, polydispersity index (encapsulation efficiency (EE Independent regression models were built using process variables such as total flow rate, pH, and concentrations of lipids, ethanol, mRNA, and buffer. The models demonstrated high accuracy, with correlation coefficients of 0.998 for particle size, 0.990 for PdI, and 0.977 for EE (156).
Other notable advancement is presented by Amirreza Mottafegh et al. Introducing an autonomous platform for rapidly synthesizing drug-loaded nanoparticles, such as liposomes and polymeric nanoparticles. Their system features an Automated Nanoparticle Synthesizer (ANS) using nanoprecipitation to precisely control flow rates and reactant concentrations. It also incorporates a ML-driven multi-objective Bayesian optimization (MOBO) algorithm, which dynamically adjusts parameters based on real-time feedback. This innovation reduces production time from hours or days to just 20 minutes while ensuring high reproducibility and quality (157). AI-driven optimization in nanoparticle manufacturing can enhance CAR-T therapy by boosting initial production and improving efficiency.
Our proposed AI-revolution could also extend to cell manufacturing with smart bioreactors equipped with nanosensors enabling precise, real-time monitoring and adaptive control of culture conditions. These advanced systems integrate thin-film nanosensors—such as iridium oxide for pH, platinum-based for oxygen, and graphene-coated for glucose—capable of detecting even subtle environmental changes (158–161). For example, a Pd/Pt-functionalized glucose sensor on graphene ensures continuous nutrient monitoring, preventing both starvation and overfeeding. When paired with wireless electronics, these sensors provide continuous feedback, allowing automated adjustments to optimize culture conditions, reduce costs, and enhance scalability without compromising quality (160). AI analytics further enhance this approach by enabling the interpretation of complex, high-dimensional nanosensor data. In the work by Herpin et al., MLP network was employed to disentangle overlapping infrared spectral signals from proteins, lipids, nucleotides, and peptides, enabling real-time monitoring of dynamic molecular interactions with high accuracy (162, 163). Similarly, Leong et al. demonstrated the use of CNNs to analyze multiplexed Surface-Enhanced Raman Scattering (SERS) spectra, achieving over 86.8% classification accuracy in distinguishing small-molecule metabolites such as ATP, glucose, and lactate in complex biological environments. These deep learning models transform intricate biochemical signatures into interpretable and actionable insights, paving the way for real-time diagnostics and precise metabolite monitoring at the point of need (164).
In bioreactors, AI models analyze cell growth, nutrient levels, and environmental fluctuations, dynamically adjusting conditions to optimize expansion. For example, in the work by Grzesik et al. regression models (including Elastic Net and Random Forest) were trained on donor-specific data to predict T cell viability and expansion with high accuracy (R² > 0.92, RMSE < 1.5). These models enabled the in-silico design of optimized culture media, which were experimentally validated and outperformed traditional regression approaches, illustrating how machine learning can streamline media optimization and enhance bioprocess robustness (165, 166).
Beyond manufacturing, it’s important to look at the molecular level to integrate innovative approaches aimed at enhancing CAR-T therapy. Initially, it is key to optimize mRNA delivery for CAR-T therapy success. Within the acidic environment of endosomes, lipid cores become charged, facilitating endosomal escape—a crucial step for successful nucleic acid delivery (167, 168). However, not all nanoparticle formulations perform equally well. Some formulations may accumulate within sub-endosomal membranes, impeding efficient release and consequently reducing transfection efficiency (169). While nanoparticles show great potential, optimizing their performance through conventional trial-and-error methods remains challenging (170).
DL is a powerful tool for overcoming these bottlenecks, enabling the analysis of molecular patterns, deciphering chemical structures, and predicting the behavior of novel substances. Computational models can simulate cationic polymer behavior within endosomes, facilitating the design of more efficient gene delivery systems (171). This significantly reduces the time and cost involved in developing new platforms. AI-driven models also allow detailed study of ion channel physiology and genomics, supporting the design of systems that promote enhanced endosomal and lysosomal escape (96, 172–174). AI can also evaluate critical factors like cargo fusion rates after internalization, optimizing vectors for better performance (26, 175). In this context, multimodal neural networks (which integrate heterogeneous data sources such as chemical structure, physicochemical descriptors, biological response profiles, and imaging data) are emerging as advanced tools for optimizing nanoparticle design. By jointly analyzing multiple modalities, these models offer a more holistic understanding of how structural and functional features interact, allowing for more precise prediction of mRNA transfection outcomes and nanoparticle behavior across complex biological environments (176).
A prominent example of AI’s potential in gene delivery is the AGILE platform, developed by Yue Xu and colleagues. AGILE uses DL, combining combinatorial chemistry with high-throughput screening (HTS), to rapidly discover ionizable lipids optimized for mRNA delivery. At the core of AGILE is a multimodal deep learning model that integrates two complementary inputs: molecular graphs and calculated descriptors. The graph encoder, based on graph neural networks (GNNs), encodes the structural topology of lipid molecules, while a molecular descriptor encoder processes physicochemical features derived from each compound. Initially, the GNN is pre-trained in a self-supervised manner on a vast dataset of small molecules to capture generalizable structural patterns. It is then fine-tuned with experimental data from 1.200 synthesized lipids formulated into lipid nanoparticles (LNPs) and assessed for mRNA transfection potency (mTP) in specific cell lines. This refined, multimodal model predicts the mTP of new lipid candidates, enabling the prioritization and selection of high-performing structures for experimental validation. AGILE identified H9 and R6, ionizable lipids optimized for mRNA delivery to muscle cells and macrophages, respectively. H9 outperformed industry-standard lipids like ALC-0315 (used in Pfizer’s COVID-19 vaccine) in muscle tissue, minimizing liver off-target effects, while R6 exhibited superior transfection efficiency in macrophages (175). By rapidly screening extensive lipid libraries, AI-driven platforms like AGILE can optimize ionizable lipids for T-cell mRNA transfection, improving CAR expression, T-cell expansion, and addressing critical factors for broader clinical adoption.
Optimizing nanoparticle formulations is essential for effective mRNA delivery; however, identifying optimal targets for immune recognition is equally crucial for successful CAR-T therapies. Neoantigens—tumor-specific antigens generated by cancer cell mutations—are fundamental to CAR-T therapy design. Integrating AI into this process can boost neoantigen discovery, significantly improving therapeutic precision and safety. Traditional neoantigen prediction tools primarily assess peptide-MHC binding strengths to identify potential epitopes. While mouse models utilize in vivo and ex vivo methods to assess immunogenicity, equivalent approaches for humans remain unavailable (177, 178). Additionally, predicted neoantigens often exceed experimentally validated immunogenic peptides, highlighting the need for advanced computational tools capable of accurately predicting neoantigen immunogenicity (179, 180). Here, bioinformatics plays a key role by enabling the integration and interpretation of multi-omic data (such as transcriptomic, proteomic, and genomic profiles) to uncover biologically relevant patterns. When enhanced with AI, especially deep learning, these bioinformatic pipelines become powerful tools capable of modeling complex immune interactions, improving the prediction of truly immunogenic neoantigens and accelerating the design of personalized immunotherapies (181).
A study made by Fabiana Perna et al. demonstrated computational discovery of potential antigens by identifying acute myeloid leukemia (AML) targets—ADGRE2, CCR1, CD70, and LILRB2—via surface proteomics and transcriptomics. These antigens showed high AML cell expression with minimal presence in normal tissues (182). AI-based methods could enhance such processes further by rapidly analyzing data and detecting complex protein expression patterns, significantly improving prediction accuracy and speed (183, 184). ML algorithms like Random Forest and XGBoost effectively predict immunogenic peptide responses. In one study, researchers trained models on a dataset of immunogenic and non-immunogenic peptides, analyzing characteristics like hydrophobicity, peptide size, and amino acid preferences. This allowed the models to predict peptide immunogenicity efficiently, accelerating antigen discovery for immunotherapy (184).
Similarly, the DL-based tool MHCnuggets employs Long Short-Term Memory (LSTM) neural networks to predict peptide binding to MHC class I and II molecules. Its adaptable architecture handles variable-length peptides and integrates both binding affinity measurements and mass spectrometry-derived data, substantially improving prediction performance. The model supports both regression, estimating continuous IC50 binding affinity values, and classification, identifying binders versus non-binders from immunopeptidomic (HLAp) datasets. MHCnuggets rapidly analyzes millions of peptide-MHC interactions, identifying immunogenic mutations across various cancer types. Although CAR-T therapies do not directly rely on MHC molecules, adapting similar approaches could help identify highly specific surface antigens, enriching overall immune responses and enhancing therapy effectiveness (185). Likewise, nanotechnology addresses challenges in neoantigen stability and immunogenicity, improving antigen spreading and delivery. Zhao et al. Showed myeloperoxidase nanovaccines capable of inducing immunogenic cell death (ICD), triggering an immune response cascade, enhancing neoantigen delivery to lymph nodes, and promoting a pro-inflammatory tumor microenvironment. Integrating AI tools like MHCnuggets could optimize this process further by rapidly prioritizing immunogenic neoantigens for personalized cancer immunotherapy (186–188).
It’simportant to mention that, besides the discovery of neoantigens, the quest for highly specific and effective targeting mechanisms leads us to explore alternative binders: Nbs present a promising alternative to traditional scFvs in CAR-T therapy. Due to their smaller size, enhanced stability, reduced immunogenicity, and ability to target unique epitopes, nanobody-based CAR-T cells hold significant potential to improve cancer treatments (76). CAR-Toner has demonstrated that nanobodies-based CARs exhibit optimal positive charge patch (PCP) scores, correlating with improved CAR-T cell functionality (133). Accelerating the discovery of high-affinity nanobodies enables more precise and effective therapeutic interventions. Artificial intelligence further enhances this process, notably through the ML-driven platform NbAffinity, which predicts nanobody-target binding affinity by analyzing critical molecular interactions such as hydrogen bonding, aromatic stacking, and ionic interactions. NbAffinity integrates advanced algorithms—including Random Forest (RF), Rotation Forest (RotF), and Support Vector Machines (SVMs)—to efficiently analyze extensive structural data. Trained on a comprehensive dataset of 991 nanobody-ligand complexes supplemented by 444 protein-protein interaction pairs, NbAffinity achieves robust, generalizable predictions.On the test set, SVM reached an accuracy of 75.87%, reflecting a strong ability to classify affinitive versus non-affinitive nanobodies based on structural interaction features (189).
Building on the precision offered by AI-driven nanobody discovery, it becomes clear that understanding and enhancing dynamic interactions within the tumor microenvironment is equally crucial for advancing CAR-T therapies. Predicting real-time interactions between CAR-T cells, nanoparticles, and tumor cells remains a complex challenge. Emerging technologies like digital twins and virtual patient models are poised to improve cancer treatment by leveraging computational methodologies, including quantitative systems pharmacology (QSP) and physiologically based pharmacokinetics (PBPK), to simulate complex biological processes (190–194). Digital twins provide real-time, personalized tumor replicas, capturing distinct biological and physical attributes. In contrast, virtual patient models incorporate population-level variability, offering valuable insights into diverse subgroup responses (195). These models integrate multi-omics data, predicting tumor dynamics, immune interactions, and therapeutic outcomes, thus enhancing targeting accuracy and minimizing off-target effects (196–198). Such approaches significantly improve simulation of interactions within the CAR-T cell-nanoparticle-tumor axis, optimizing tumor targeting and delivery efficiency (199–202).
Integrating AI further amplifies these capabilities by analyzing tumor morphology, metabolism, and pharmacokinetic profiles (200). This data-driven approach refines tumor microenvironment simulations, optimizing CAR-T cell and nanoparticle design and administration. Platforms such as TumorScopePredict illustrate practical applications by generating dynamic 3D tumor models and accurately predicting therapeutic responses from pre-treatment imaging data processed via CNNs, simulating tumor behavior, drug sensitivity, and resistance (203, 204). The adaptive nature of AI ensures these models remain at the forefront of cancer research, continuously evolving with new data (205, 206).
5.2 Precision remodeling of the solid tumor microenvironment: the role of AI-guided nanotechnology in CAR-T cell therapy and vivo manufacturing
One significant challenge for CAR-T therapy in solid tumors is overcoming physical and immunosuppressive barriers within the tumor microenvironment (TME). Unlike hematologic malignancies, solid tumors present dense extracellular matrices (ECM) and aberrant vasculature, impeding T-cell migration. Additionally, immunosuppressive cells such as tumor-associated macrophages (TAMs), regulatory T cells (Tregs), and myeloid-derived suppressor cells (MDSCs) create a hostile environment, limiting T-cell effectiveness through cytokine secretion and checkpoint inhibition (207–213).
Nanotechnology addresses these challenges by remodeling the TME, degrading ECM, and reprogramming immunosuppressive cells like TAMs. It also facilitates targeted delivery of supportive cytokines (e.g., IL-12, IL-15) and immune checkpoint inhibitors (e.g., anti-PD-1) to enhance CAR-T cell performance. Additionally, nanoparticles address antigen escape via multi-antigen targeting and epitope spreading (17, 64, 84, 84, 214, 215). However, clinical translation remains limited due to poor delivery efficiency (DE), with only ~0.67% of nanoparticles reaching the tumor, while the remainder accumulates off-target, primarily in the liver, spleen, and lungs (216–221). This challenge highlights the necessity for improved nanoparticle design to enhance tumor targeting while minimizing systemic distribution.
AI-driven approaches can significantly enhance nanoparticle design, optimizing physicochemical properties to improve tumor targeting and reduce systemic distribution. A DNN utilizing the Nano-Tumor Database (534 tumor datasets, 1972 tissue datasets) accurately predicted nanoparticle DE in tumors and key organs based on nanoparticle properties and therapy strategies. This AI-driven approach identified core materials as critical determinants of DE and provided a web-based tool, Nano-AI-QSAR, facilitating nanoparticle optimization (222). Other organ-specific studies have used AI to optimized brain-targeted nanoparticle delivery, identifying influential factors such as release rate and molecular weight, enhancing nanoparticle effectiveness (223). Additionally, AI-driven optimization of mRNA nanovaccines demonstrated significant improvements in transfection efficiency and lymphatic delivery, successfully activating the stimulator of interferon genes (STING) pathway and boosting antitumor immunity in vivo (224). Given the high dimensionality, heterogeneity, and non-linear relationships within biological and physicochemical data, deep learning models are increasingly favored for their capacity to capture complex patterns and interactions that traditional models may overlook (225).
Based on the foundation of AI-optimized nanoparticle design for improved delivery efficiency (DE), an exciting frontier lies in magnetically guided nanoparticles, a strategy ripe for further refinement through AI-driven models. Certain nanoparticles possess magnetic properties that facilitate their targeted redirection to tumor sites—a strategy that can be refined through AI-driven models. Yasmeen Akhtar et al. developed computational simulations integrating factors like magnetic field strength, blood flow, and chemical dynamics to optimize delivery efficiency (DE) and minimize off-target accumulation. Pulsatile flow experiments revealed that stronger magnetic fields enhance nanoparticle retention, while pulsatile conditions improve tumor penetration (62, 226).
Such AI-driven magnetic guidance methodologies hold considerable promise for CAR-T therapy, especially since magnetic control has already demonstrated potential for directing T-cell migration. This suggests substantial opportunities to further apply AI techniques to optimize these processes. Innovative strategies, such as CAR-T-cell-based microrobots (M-CAR Ts), which incorporate immunomagnetic beads onto CAR-T cells, facilitate precise targeting and deep tumor infiltration through sequential magnetic-acoustic actuation, markedly increasing T-cell accumulation and therapeutic efficacy (227). Similarly, CAR-T cells functionalized with superparamagnetic iron oxide nanoparticles (SPIONs) can be magnetically guided to tumor sites, enhancing localized cytolytic activity while simultaneously reducing systemic cytokine release and associated toxicities (228). Integrating AI-driven predictive modeling with advanced nanoparticle engineering can actualize the therapeutic potential of nanotechnology for solid tumors. AI can overcome critical barriers in CAR-T therapy by optimizing nanoparticle properties for superior delivery efficiency, precision targeting, and incorporating complementary approaches such as magnetic guidance to achieve robust and targeted therapeutic outcomes.
Now that the key components for precise and efficient targeted delivery are in place—including AI-optimized nanoparticles and advanced TME-modulating strategies—the prospect of in vivo CAR-T cell generation could be within reach. Current CAR T-cell production involves leukapheresis to isolate patient T cells, activation with cytokines and co-stimulatory molecules, genetic modification via lentiviral or γ-retroviral vectors to introduce CAR genes, and subsequent cell expansion into therapeutic doses. This complex and costly procedure requires specialized facilities and trained personnel (14, 229). In contrast, the proposed in vivo CAR T-cell production, involving direct in-patient delivery of CAR genes and activation signals, simplifies manufacturing, reduces costs, and enhances accessibility. Preclinical studies in mouse models have shown comparable antitumor efficacy between in vivo-produced and ex vivo-engineered CAR-T cells (53, 54, 230).
Successful in vivo CAR-T cell therapy must meet several critical criteria: high gene-editing efficiency, precise T cell targeting, the ability to overcome solid tumor barriers, sustained functionality and persistence of CAR-T cells, and minimal toxicity (51, 231). CAR T cells face major barriers in the tumor microenvironment (TME), including physical, chemical, and immunological obstacles. To overcome these, nanoparticles are being developed not just for drug delivery but also to modulate the TME and create a “theranostic window” where tumors are both treatable and detectable. These particles (10–200 nm) accumulate in tumors via the EPR effect and can be functionalized with ligands targeting tumor or stromal cells. They can also carry enzymes like collagenase to degrade the ECM, enhancing T cell infiltration and nanoparticle penetration. Additionally, they can deliver siRNA, miRNA, or inhibitors (e.g., TGF-β, IDO, checkpoint blockers) to reprogram the immunosuppressive TME. The Smart CAR-T Nanosymbionts interface exemplifies this advancement, integrating functionalities for precise targeting, enhanced persistence, and minimized toxicity by leveraging the advanced technologies discussed in this paper. Furthermore, AI-driven platforms such as AGILE are being employed to optimize the design of ionizable lipids, significantly enhancing the transfection efficiency of gene delivery systems. This ensures robust CAR expression in T cells, further supporting the development of effective in vivo CAR-T therapies (175).
Additionally, AI-guided nanoparticle design improves tumor-specific targeting, minimizing off-target accumulation, facilitating extracellular matrix degradation for improved tumor infiltration, delivering targeted immunomodulatory agents (e.g., IL-12, anti-PD-1), and enabling efficient mRNA delivery into T cells (222). Advanced targeting strategies like magnetically guided M-CAR Ts and SPION-functionalized CAR-T cells enhance tumor localization and deep tissue penetration as necessary (228). Maintaining CAR-T cell functionality involves localized cytokine delivery facilitated by nanotechnology, complemented by AI-driven optimization tools such as CAR-Toner, which refine tonic signaling, and computational approaches optimizing co-stimulatory domains (CD28, 4-1BB) to balance T-cell activation and memory formation directly within the patient (55–60). Finally, addressing potential toxicity necessitates a comprehensive strategy incorporating precise targeting, tumor-specific neoantigen prediction, and controlled-release systems for cytokines and checkpoint inhibitors, collectively ensuring both safety and therapeutic efficacy (232–234). Figure 4 represents the congregation of these technologies in the “In vivo Smart CAR-T Nanosymbionts manufacturing”.
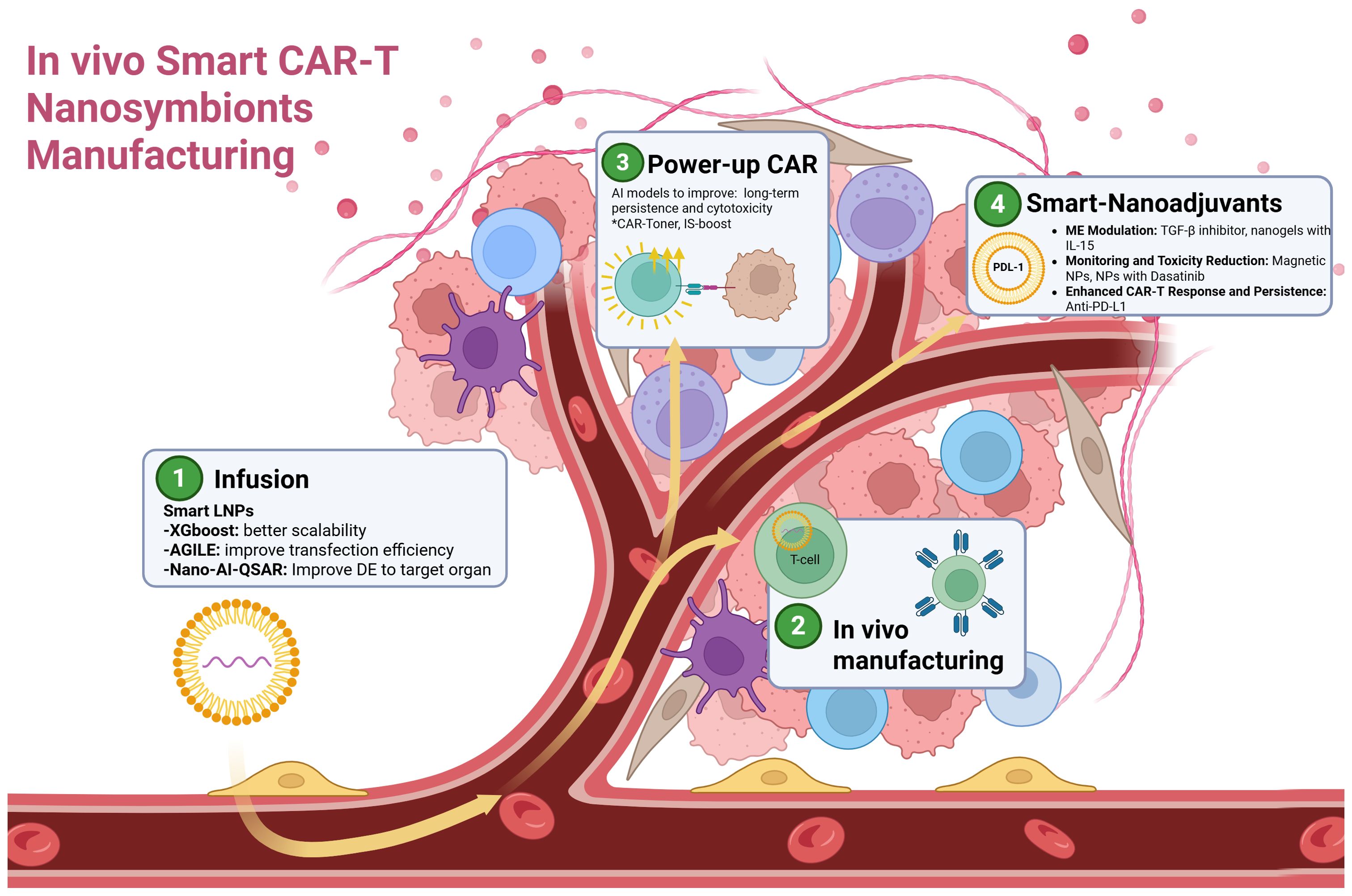
Figure 4. Illustrative schematic of the In Vivo Smart CAR-T Manufacturing, highlighting four key phases in targeted cancer therapy: 1. Infusion: Administration of smart lipid nanoparticles optimized with artificial intelligence models such as XGBoost for improved scalability, AGILE for enhanced transfection efficiency, and Nano-AI-QSAR to optimize delivery and gene expression in target organs. 2. In vivo manufacturing: Direct conversion of T cells into CAR-T cells within the patient, eliminating the need for ex vivo manipulation, reducing production time and costs. 3. CAR-T enhancement: Implementation of AI models to improve CAR-T cell persistence and cytotoxicity through strategies like CAR-Toner to prevent exhaustion, and AI-improved IS + costimulatory domain to enhance cytotoxicity and memory formation. 3. Smart nano-adjuvants: Finally, independent strategies for solid tumors can further be improve with AI(like target delivery) to act in key factors such as; Modulation of the tumor microenvironment using TGF-β inhibitors and IL-15 nanogels, target monitoring and toxicity control with magnetic nanoparticles and Dasatinib, and enhanced CAR-T response and persistence with PD-L1 inhibitors. Created with: Biorender.com. Abbreviations:.
5.3 Clinical applications of AI-enhanced monitoring of CAR-T: imaging, tracking, and toxicity detection
AI-driven image analysis has the potential to revolutionize cancer imaging by shifting from qualitative interpretation to objective, quantitative evaluations. This transformation facilitates earlier detection, precise lesion characterization, and improved monitoring of disease progression and treatment responses (235). In CAR-T therapy specifically, multimodal network models integrating imaging and clinical data have successfully predicted treatment outcomes (109, 110).
Iron and gold nanoparticles have emerged as powerful contrast agents for magnetic resonance (MR), computed tomography (CT), and positron emission tomography (PET) imaging, significantly enhancing the resolution and visibility of both solid tumors and hematological malignancies. These advancements not only improve diagnostic accuracy but also reduce imaging duration and resource utilization (236–239). When combined with AI-driven innovations in biodistribution and targeted delivery, nanoparticles further amplify tumor contrast, enabling precise lesion delineation and superior assessment of therapeutic responses. CNNs trained on nanoparticle-enhanced imaging data refine tumor characterization and support real-time clinical decision-making, fostering automated and precise cancer monitoring (240). Additionally, in vivo tracking of CAR-T cell distribution with contrast agents enhances persistence and tumor targeting. This enables real-time response assessment and better lesion characterization (228). The previously mentioned CNN-based approach could further improve non-invasive CAR-T tracking methods, such as ferumoxytol-enhanced MRI for iron oxide- or gold-labeled CAR-T cells, optimizing the evaluation of therapy distribution and effectiveness (20, 21, 88).
Besides imaging monitoring, tracking CAR-T cells in peripheral blood is critical for assessing therapy efficacy and ensuring patient safety, particularly in blood malignancies like acute leukemia (241). Traditional identification methods are limited due to the similarities between CAR-T cells and other immune cells. However, the RCMNet model, which integrates CNN-MLP trained on Peripheral Blood Cells (PBC) datasets, achieves a top-1 accuracy of 99.63%, revolutionizing CAR-T cell identification in blood samples. This approach alleviates manual evaluation burdens, provides real-time automated analysis, and markedly improves diagnostic accuracy (242). Transformers, originally developed for natural language processing, rely on self-attention mechanisms that allow the model to weigh the importance of different input features relative to one another (243). In this context, they enhance the model’s ability to focus on subtle, context-dependent cellular traits that differentiate CAR-T cells from other immune populations.
While monitoring therapeutic responses is crucial, it is equally vital to detect adverse effects such as cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) at an early stage. Nanoelectronics biosensors, such as silicon nanowire field-effect transistors (SiNW FETs), provide highly sensitive, real-time detection capabilities that surpass traditional methods like ELISA (244, 245). These nanosensors enable precise tracking of cytokines and toxicity markers, facilitating rapid clinical intervention—all of which can be further optimized and enhanced through AI-driven models (246). The detailed data generated by these biosensors can strengthen AI-driven predictive models, such as M2-CRS, facilitating early toxicity predictions and personalized treatment management. Additionally, machine learning algorithms, particularly Random Forest (RF), can integrate nanoparticle physicochemical properties—such as size, shape, surface coating, and zeta potential—along with exposure conditions like dose, duration, and tissue type to accurately predict nanoparticle-induced toxicity. Such predictive models improve safety assessments, enabling proactive risk management and tailored therapeutic adjustments (247).
6 Technological convergence in CAR-T therapies: challenges, limitations, and future directions
The convergence of CAR-T therapy with AI and nanotechnology marks a turning point in personalized oncology. These technologies offer complementary advantages: AI enables data-driven prediction and adaptation, while nanotechnology facilitates controlled delivery and improved CAR-T functionality. Yet, this synergy introduces multilayered challenges that span scientific, ethical, and regulatory domains.
At the scientific frontier, multiple ML and DL models have been integrated across CAR-T development stages, from receptor design to toxicity prediction. CNNs support high-resolution classification and three-dimensional immunological synapse analysis (119, 129); support vector machines (e.g., M2-CRS) can predict cytokine release syndrome (142); MLPs aid signal separation (162); and hybrid models like RCMNet blend CNNs with transformers to identify CAR-T cells in blood samples (242). Platforms such as AGILE combine GNNs and MLPs for lipid discovery in mRNA transfection (175), while LSTM models like MHCnuggets predict peptide–MHC binding (185). However, none of these approaches have yet reached a level of technological maturity suitable for commercial implementation (TRL ≤ 5), and at the time of writing this paper, there is no clinical trials are on the way. A summary of ML/DL models applied to CAR-T therapy can be found at Table 4.
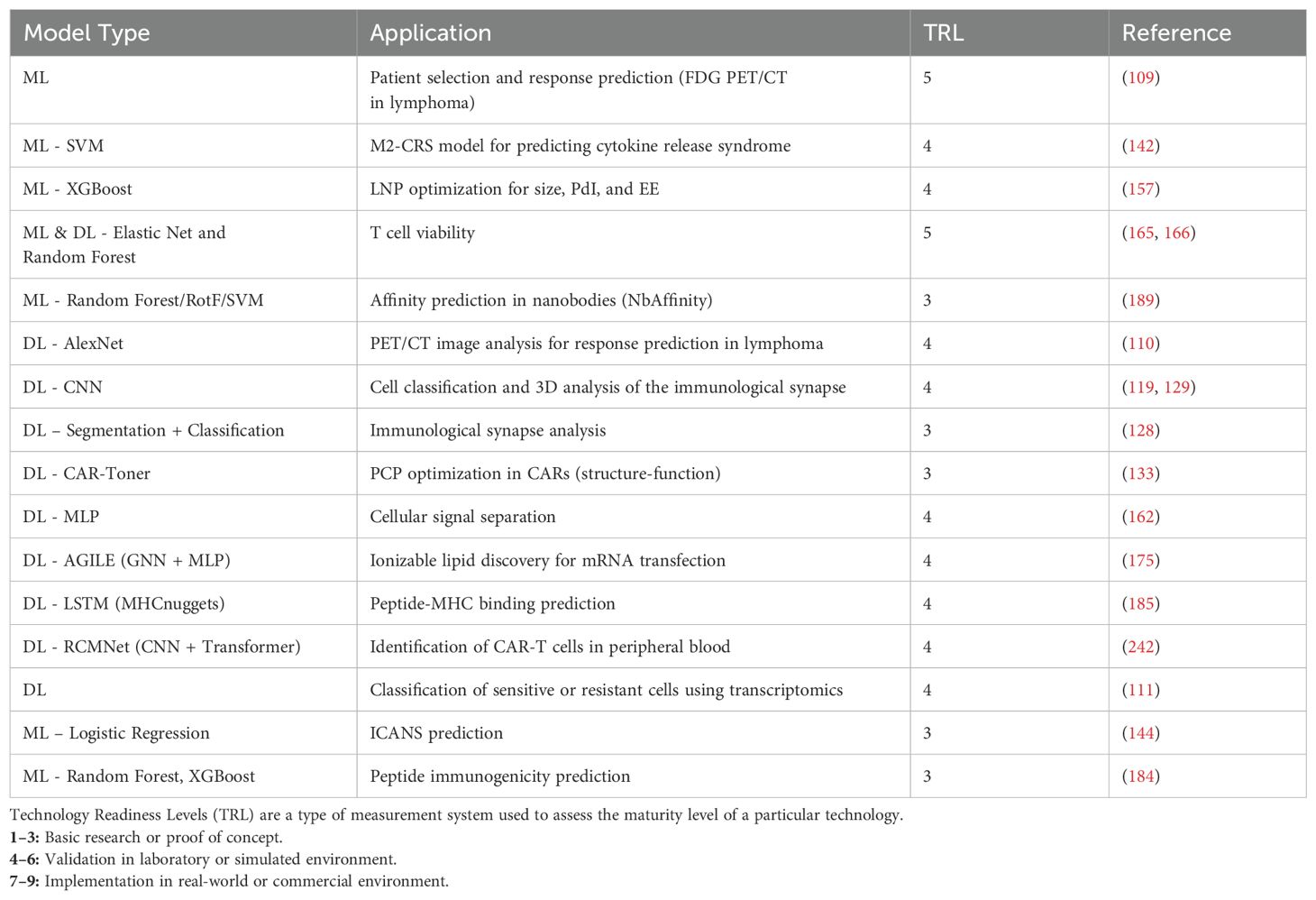
Table 4. Summary of ML/DL models applied to CAR-T therapy: applications, and TRL.
A central concern is data integrity. Biased or incomplete datasets can skew AI outputs, introducing disparities in therapeutic prediction or patient stratification. Algorithmic bias—driven by unbalanced training data or non-generalizable architectures—threatens equity across population subgroups (248). Moreover, the probabilistic nature of AI decisions challenges established paradigms of clinical accountability and informed consent. Interpretability tools have emerged to audit these models (93), and explainable AI is gaining regulatory traction (249), yet the gap between computational abstraction and clinical utility remains.
To improve system robustness, data preprocessing, outlier detection via unsupervised learning, and synthetic data generation (e.g., augmentation) are actively explored. Still, generalization in low-data settings remains a core limitation. This demands interoperable clinical databases and the use of synthetic sampling or generative AI to enrich training sets (250). Standardization of model documentation and traceability is essential to harmonize with emerging governance standards and enable consistent model retraining in non-stationary biological environments.
At the nanoscale, delivery systems unlock new routes for CAR-T engineering. Nanoparticle platforms enable the potential for in vivo generation of CAR-T cells, bypassing the need for centralized manufacturing. However, unresolved concerns around long-term biocompatibility, off-target immune effects, and pharmacokinetic variability persist. Efficiency of delivery to solid tumors remains a major bottleneck, necessitating novel chemistries, adaptive functionalization, and ligand-directed targeting to increase specificity while minimizing systemic exposure (251).
The fusion of these technologies disrupts traditional regulatory classification. CAR-T therapies enhanced by nanodevices and AI systems defy existing frameworks, which were not designed to evaluate dynamic, self-learning systems or hybrid constructs that combine genetically modified cells, synthetic vectors, and algorithmic decision layers. While they may theoretically qualify as combination products, the lack of harmonized guidance across nanoparticle characterization, AI validation, and cell-processing protocols hinders regulatory review. Existing pathways cannot adjudicate how these components interact to affect dosing, targeting, and real-time decision-making.
Compounding this, there is a dearth of standardized protocols for validating AI-governed nanoparticle formulations under physiological stress, particularly in immunologically diverse populations. The absence of nano-toxicological assays capable of modeling long-term safety profiles further constrains clinical translation. In this context, regulatory frameworks established for mRNA vaccines—already approved and deployed in humans—could serve as a foundational reference to streamline the evaluation of lipid-based delivery systems and accelerate safe clinical adoption. Without robust retraining strategies, AI systems are prone to model drift and loss of predictive performance/failure modes that could compromise patient safety in real-world settings.
Ethical and translational risks are also something to address. As algorithms increasingly guide critical interventions, from patient selection to adaptive dosing, they raise concerns about equity, transparency, and liability. The opacity of high-dimensional models challenges informed consent, while layered technological mediation complicates assignment of clinical responsibility. Regulatory bodies currently lack the tools to evaluate how these algorithmic and biological elements co-evolve, necessitating novel oversight structures that ensure longitudinal monitoring, auditability, and preservation of clinician agency.
Moving forward, three strategic priorities must be addressed to realize the promise of Smart CAR-T Nanosymbionts:
First, AI tools must be developed for generalization in data-scarce, heterogeneous clinical environments. Centralized, standardized repositories and controlled access to interoperable datasets are foundational. Data augmentation techniques and generative models can mitigate sampling limitations (250), but interpretability remains vital. All outputs must be benchmarked against clinical criteria to ensure trust and biomedical validity (252).
Second, nanoparticle platforms require enhanced specificity and safety. Efficient tumor targeting, high-fidelity gene transfection, and reduced immunogenicity are prerequisites for in vivo CAR-T generation. These aspects require mechanistic insight into how nanoparticle properties influence cell activation, exhaustion, and biodistribution. Standardized assays correlating particle chemistry with toxicity and organ accumulation are essential.
Third, interdisciplinary integration is paramount. Teams spanning AI, nanomedicine, immunology, and clinical oncology must co-develop scalable protocols and shared data infrastructures. Regulatory harmonization should evolve in parallel to support transparency, patient safety, and equitable access as these technologies transition to clinical settings (253, 254).
In summary, the integration of AI and nanotechnology into CAR-T therapy represents a technological opportunity. Despite this, only through ethical, scientifically rigorous, and regulatory-aware frameworks can these multilayered platforms move from conceptual models to safe, effective, and accesible next-generation therapies.
7 Conclusions
CAR-T therapy has revolutionized modern oncology, but its large-scale application faces significant challenges, including complex manufacturing processes, high costs, limited efficacy in solid tumors, and potentially severe toxicities. Emerging technologies such as nanotechnology and AI offer innovative tools to address these limitations, greatly enhancing therapeutic precision and scalability. While both have demonstrated individual promise, their full potential can only be realized through strategic and synergistic integration. The Smart CAR-T Nanosymbionts framework represents a paradigm shift in this direction. It is designed to converge the capabilities of AI and nanotechnology into a unified therapeutic interface that enhances every stage of CAR-T therapy, from design and engineering of CAR constructs to their delivery, in vivo behavior, and monitoring. By incorporating AI-driven modeling and optimization, this approach enables dynamic adjustments to manufacturing conditions, personalized antigen targeting, and real-time monitoring of patient-specific responses. Simultaneously, the use of nanotechnology allows for non-viral gene delivery, tumor-specific modulation of the microenvironment, and spatially controlled release of cytokines and inhibitors that enhance CAR-T cell persistence and reduce immune-related toxicities. Moreover, the Smart CAR-T Nanosymbionts challenge boundaries by introducing the possibility of in vivo CAR-T generation. This vision leverages AI-optimized lipid nanoparticles to deliver CAR constructs directly into patient T cells, bypassing the need for ex vivo manipulation. Such a system could radically simplify production, reduce timelines and costs, and expand access to cell-based therapies, particularly in low-resource settings.
As a complementary conceptual tool, our group has previously developed the Addition by Subtraction model, an operational philosophy aimed at amplifying therapeutic outcomes by systematically eliminating inefficiencies, redundancies, and sources of toxicity across biological and technological layers (17). Although originally proposed in a different context, this model aligns with the foundational goals of Smart CAR-T Nanosymbionts and serves as a guiding principle for integrating innovation in a way that is both scalable and clinically actionable (Figure 5; Table 5).
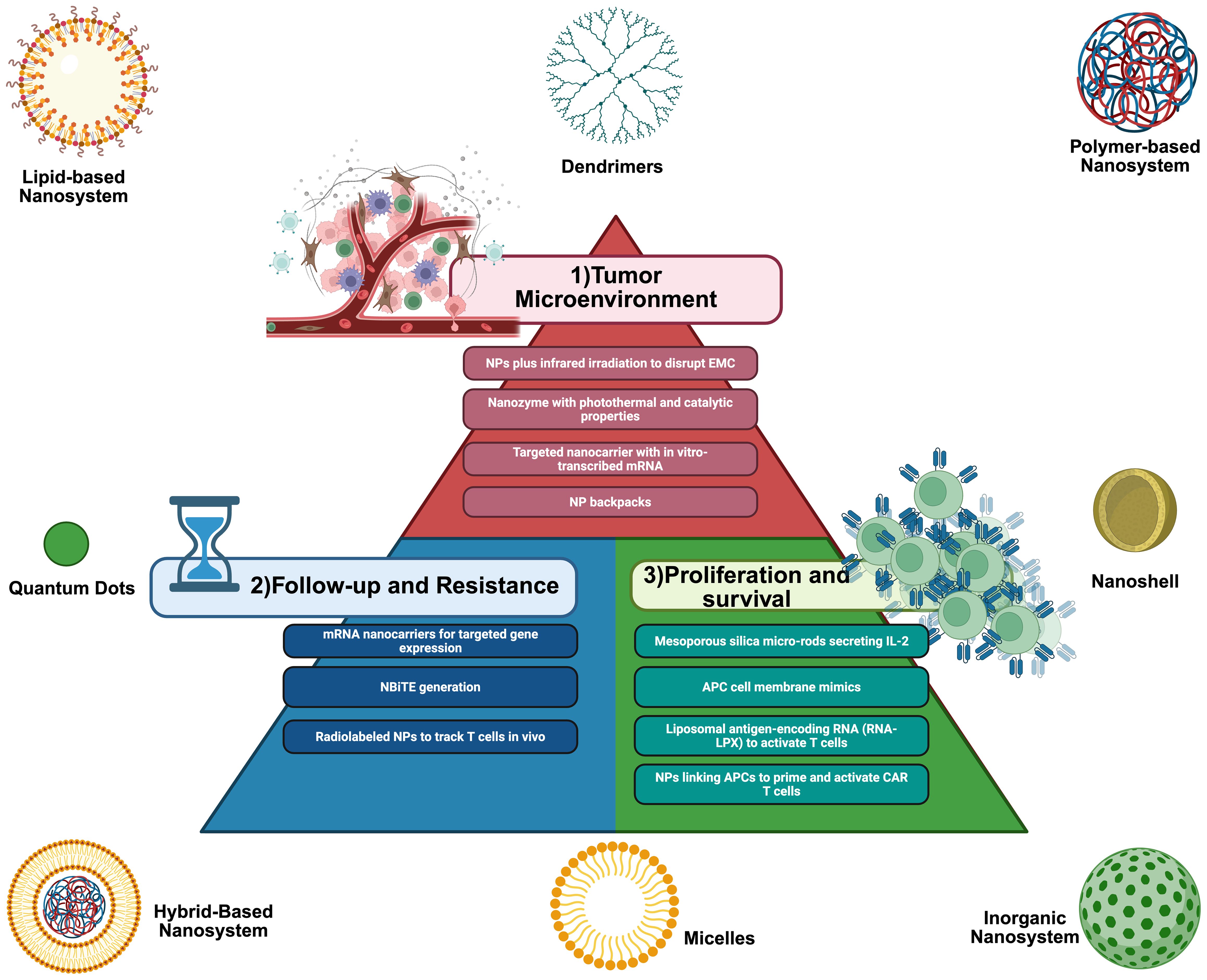
Figure 5. Graphical Abstract of Addition by Subtraction: Smart CART Nanosymbionts: AI serves as the central integrative engine, leveraging machine learning and deep learning algorithms to drive decision-making, pattern recognition, and predictive modeling. This AI-driven framework enhances the design, function and specificity of nanoparticles—such as lipid and -based nanoparticles—and improves CAR-T cell therapy by optimizing patient selection, target specificity, response prediction, and toxicity control. Together, these elements enable the development of intelligent, adaptive, and personalized cancer treatments.
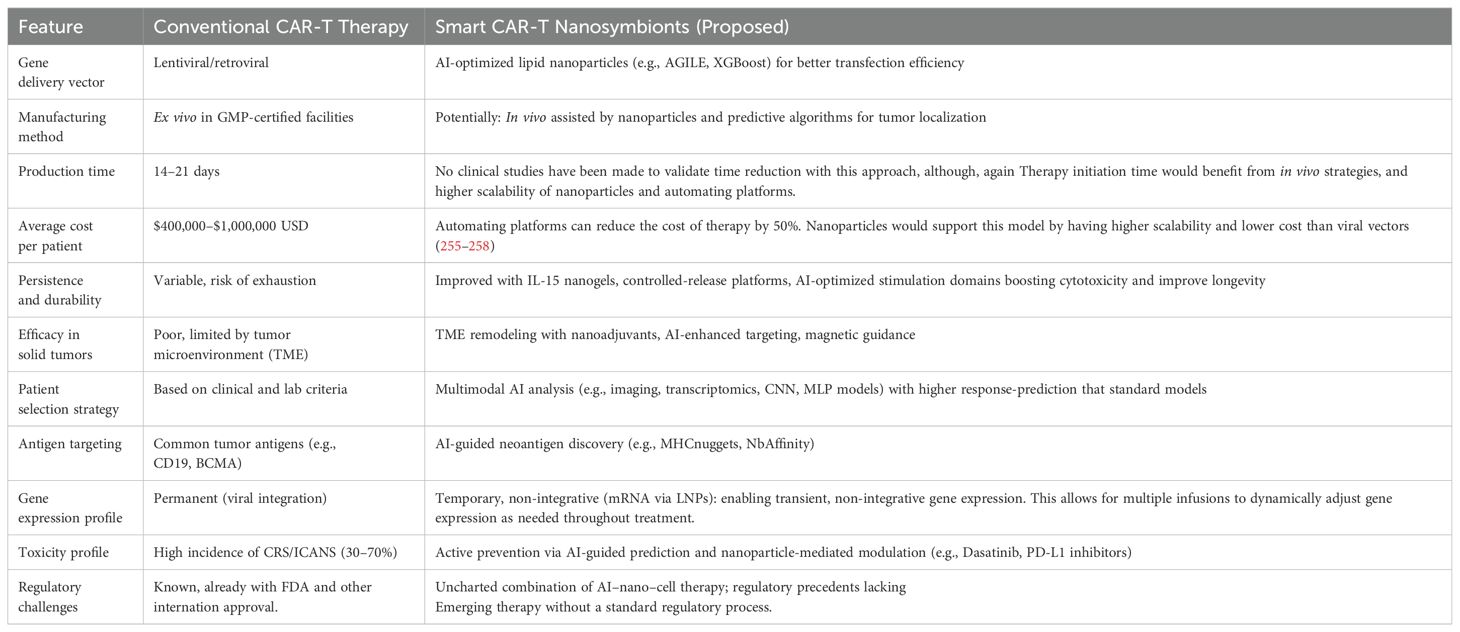
Table 5. Comparison between conventional CAR-T therapy and smart CAR-T nanosymbionts.
Ultimately, the integration of AI, nanotechnology, and CAR-T therapy holds the promise of transforming cancer care by enabling truly adaptive, intelligent, and personalized treatments. However, realizing this vision requires not only scientific advancement, but also regulatory evolution, ethical vigilance, and interdisciplinary collaboration. Future research must prioritize the development of robust translational pipelines, real-time monitoring systems, and equitable frameworks to ensure that these next-generation therapies are safe, accessible, and impactful across global health systems.
To clearly illustrate the transformative potential of this integrated approach, we present a comparative framework between conventional CAR-T therapy and the Smart CAR-T Nanosymbionts model. This side-by-side analysis highlights how the convergence of artificial intelligence and nanotechnology can address critical limitations in manufacturing, safety, cost, and clinical scalability.
Author contributions
JB: Visualization, Writing – original draft, Conceptualization, Methodology, Supervision, Project administration, Investigation, Validation, Writing – review & editing, Data curation. JV: Conceptualization, Validation, Supervision, Methodology, Project administration, Investigation, Writing – review & editing, Resources, Visualization, Formal analysis, Writing – original draft. AT-P: Writing – review & editing, Writing – original draft, Formal analysis, Visualization, Investigation, Project administration, Validation, Conceptualization, Methodology, Supervision. CA: Validation, Data curation, Writing – review & editing, Supervision, Investigation, Writing – original draft, Visualization, Funding acquisition, Formal analysis. JO-G: Validation, Formal analysis, Project administration, Supervision, Conceptualization, Writing – original draft, Writing – review & editing, Investigation. JG-R: Validation, Visualization, Formal analysis, Supervision, Writing – review & editing, Conceptualization, Writing – original draft, Investigation. DT: Writing – review & editing, Supervision, Writing – original draft, Visualization, Data curation, Investigation, Validation, Conceptualization. LR-S: Supervision, Formal analysis, Funding acquisition, Software, Writing – original draft, Investigation, Writing – review & editing, Conceptualization, Validation, Visualization. LA: Conceptualization, Supervision, Writing – review & editing, Investigation, Writing – original draft, Validation, Visualization. JR: Validation, Writing – review & editing, Formal analysis, Supervision, Investigation, Data curation, Visualization, Writing – original draft, Conceptualization. CC: Visualization, Writing – original draft, Formal analysis, Software, Conceptualization, Validation, Writing – review & editing, Supervision. GC-A: Writing – original draft, Validation, Visualization, Writing – review & editing, Supervision, Investigation, Conceptualization. FO: Writing – original draft, Visualization, Conceptualization, Data curation, Supervision, Formal analysis, Writing – review & editing, Validation, Investigation. TF: Visualization, Investigation, Validation, Conceptualization, Supervision, Writing – original draft, Writing – review & editing. IL: Supervision, Writing – review & editing, Software, Conceptualization, Visualization, Writing – original draft, Formal analysis, Validation. AL: Conceptualization, Visualization, Investigation, Validation, Funding acquisition, Formal analysis, Writing – original draft, Supervision, Data curation, Writing – review & editing. KV: Writing – original draft, Data curation, Visualization, Conceptualization, Investigation, Validation, Funding acquisition, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
Author JO-G is the founder and CEO of Prodigy Cells Labs, LLC.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. We used generative AI as a tool to improve redaction.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Personalized Medicine. Available online at: https://www.genome.gov/genetics-glossary/Personalized-Medicine (Accessed March 21, 2025).
2. Alnefaie A, Albogami S, Asiri Y, Ahmad T, Alotaibi SS, Al-Sanea MM, et al. Chimeric antigen receptor T-cells: an overview of concepts, applications, limitations, and proposed solutions. Front Bioeng Biotechnol. (2022) 10:797440. doi: 10.3389/fbioe.2022.797440
3. Commissioner O of the FDA. FDA approves CAR-T cell therapy to treat adults with certain types of large B-cell lymphoma(2020). Available online at: https://www.fda.gov/news-events/press-announcements/fda-approves-car-t-cell-therapy-treat-adults-certain-types-large-b-cell-lymphoma (Accessed March 28, 2025).
4. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med. (2018) 378:439–48. doi: 10.1056/NEJMoa1709866
5. Westin J and Sehn LH. CAR T cells as a second-line therapy for large B-cell lymphoma: a paradigm shift? Blood. (2022) 139:2737–46. doi: 10.1182/blood.2022015789
6. Zhang X, Zhu L, Zhang H, Chen S, and Xiao Y. CAR-T cell therapy in hematological Malignancies: current opportunities and challenges. Front Immunol. (2022) 13:927153. doi: 10.3389/fimmu.2022.927153
7. Zhou J, Lei B, Shi F, Luo X, Wu K, Xu Y, et al. CAR T-cell therapy for systemic lupus erythematosus: current status and future perspectives. Front Immunol. (2024) 15:1476859. doi: 10.3389/fimmu.2024.1476859
8. Srivastava S and Riddell SR. CAR T cell therapy: challenges to bench-to-bedside efficacy. J Immunol Baltim Md 1950. (2018) 200:459–68. doi: 10.4049/jimmunol.1701155
9. Srivastava A, Mallela KMG, Deorkar N, and Brophy G. Manufacturing challenges and rational formulation development for AAV viral vectors. J Pharm Sci. (2021) 110:2609–24. doi: 10.1016/j.xphs.2021.03.024
10. WebMD. CAR T-cell therapy: managing costs and finding financial assistance. Available online at: https://www.webmd.com/cancer/lymphoma/features/navigate-finances-car-t-cell-therapy (Accessed April 3, 2025).
11. Suran M. FDA adds boxed warning to CAR T-cell therapies, but says benefits outweigh risks of secondary cancers. JAMA. (2024) 331:818–20. doi: 10.1001/jama.2024.1011
12. Bailey SR, Berger TR, Graham C, Larson RC, and Maus MV. Four challenges to CAR T cells breaking the glass ceiling. Eur J Immunol. (2023) 53:e2250039. doi: 10.1002/eji.202250039
13. Mikhael J, Fowler J, and Shah N. Chimeric antigen receptor T-cell therapies: barriers and solutions to access. JCO Oncol Pract. (2022) 18:800–7. doi: 10.1200/OP.22.00315
14. Cliff ERS, Kelkar AH, Russler-Germain DA, Tessema FA, Raymakers AJN, Feldman WB, et al. High cost of chimeric antigen receptor T-cells: challenges and solutions. Am Soc Clin Oncol Educ Book. (2023) 43):e397912. doi: 10.1200/EDBK_397912
15. Potnis KC, Di M, Isufi I, Gowda L, Seropian SE, Foss FM, et al. Cost-effectiveness of chimeric antigen receptor T-cell therapy in adults with relapsed or refractory follicular lymphoma. Blood Adv. (2023) 7:801–10. doi: 10.1182/bloodadvances.2022008097
16. Chen T, Wang M, Chen Y, and Liu Y. Current challenges and therapeutic advances of CAR-T cell therapy for solid tumors. Cancer Cell Int. (2024) 24:133. doi: 10.1186/s12935-024-03315-3
17. Baena JC, Pérez LM, Toro-Pedroza A, Kitawaki T, and Loukanov A. CAR T cell nanosymbionts: revealing the boundless potential of a new dyad. Int J Mol Sci. (2024) 25:13157. doi: 10.3390/ijms252313157
18. Bao CJ, Duan JL, Xie Y, Feng XP, Cui W, Chen SY, et al. Bioorthogonal engineered virus-like nanoparticles for efficient gene therapy. Nano-Micro Lett. (2023) 15:197. doi: 10.1007/s40820-023-01153-y
19. Parayath NN, Stephan SB, Koehne AL, Nelson PS, and Stephan MT. In vitro-transcribed antigen receptor mRNA nanocarriers for transient expression in circulating T cells in vivo. Nat Commun. (2020) 11:6080. doi: 10.1038/s41467-020-19486-2
20. Rivera-Rodriguez A, Hoang-Minh LB, Chiu-Lam A, Sarna N, Marrero-Morales L, Mitchell DA, et al. Tracking adoptive T cell immunotherapy using magnetic particle imaging. Nanotheranostics. (2021) 5:431–44. doi: 10.7150/ntno.55165
21. Bhatnagar P, Li Z, Choi Y, Guo J, Li F, Lee DY, et al. Imaging of genetically engineered T cells by PET using gold nanoparticles complexed to Copper-64. Integr Biol Quant Biosci Nano Macro. (2013) 5:231–8. doi: 10.1039/c2ib20093g
22. Genesereth MR and Nilsson NJ. Logical Foundations of Artificial Intelligence. Palo Alto, CA: Morgan Kaufmann (2012). 427 p.
23. Ertel W. Introduction to Artificial Intelligence. Springer International Publishing AG 2017 (2018). 365 p.
24. Holzinger A, Langs G, Denk H, Zatloukal K, and Müller H. Causability and explainability of artificial intelligence in medicine. WIREs Data Min Knowl Discov. (2019) 9:e1312. doi: 10.1002/widm.1312
25. Wang L, Ding J, Pan L, Cao D, Jiang H, and Ding X. Artificial intelligence facilitates drug design in the big data era. Chemom Intell Lab Syst. (2019) 194:103850. doi: 10.1016/j.chemolab.2019.103850
26. Paul D, Sanap G, Shenoy S, Kalyane D, Kalia K, and Tekade RK. Artificial intelligence in drug discovery and development. Drug Discov Today. (2021) 26:80–93. doi: 10.1016/j.drudis.2020.10.010
27. Das KP JC. Nanoparticles and convergence of artificial intelligence for targeted drug delivery for cancer therapy: Current progress and challenges. Front Med Technol. (2022) 4:1067144. doi: 10.3389/fmedt.2022.1067144
28. Bäckel N, Hort S, Kis T, Nettleton DF, Egan JR, Jacobs JJL, et al. Elaborating the potential of Artificial Intelligence in automated CAR-T cell manufacturing. Front Mol Med. (2023) 3:1250508/full. doi: 10.3389/fmmed.2023.1250508/full
29. Loukanov A, Chichova M, Filipov C, Shkodrova M, Mishonova M, Mladenova K, et al. Photo-oxidase carbon dot-based nanozyme for breast cancer theranostics under normoxia condition. J Photochem Photobiol Chem. (2023) 439:114632. doi: 10.1016/j.jphotochem.2023.114632
30. Loukanov A. Carbon nanodots chelated with metal ions as efficient electrocatalysts for enhancing performance of microbial fuel cell based on sulfate reducing bacteria. Colloids Surf Physicochem Eng Asp. (2019) 1:4. Available online at: https://www.academia.edu/85690271/Carbon_nanodots_chelated_with_metal_ions_as_efficient_electrocatalysts_for_enhancing_performance_of_microbial_fuel_cell_based_on_sulfate_reducing_bacteria (Accessed May 1, 2025).
31. Loukanov A, Mladenova P, Toshev S, Karailiev A, Ustinovich E, and Nakabayashi S. Real time monitoring and quantification of uptake carbon nanodots in eukaryotic cells. Microsc Res Tech. (2018) 81:1541–7. doi: 10.1002/jemt.23161
32. Loukanov A, Kuribara A, Nikolova S, and Saito M. Light-activated oxidize-mimicking nanozyme for inhibition of pathogenic Escherichia coli. Microsc Res Tech. (2022) 85:1949–55. doi: 10.1002/jemt.24056
33. Loukanov A and Emin S. Biotinylated vanadium and chromium sulfide nanoparticles as probes for colocalization of membrane proteins. Microsc Res Tech. (2016) 79:799–805. doi: 10.1002/jemt.22701
34. Loukanov A and Emin S. Quantum dots for detection, identification and tracking of single biomolecules in tissue and cells. Intell Nanomater. (2012) 649–77. doi: 10.1002/9781118311974.ch17
35. Loukanov AR and Gagov H. High-resolution subunit detection of glutamate receptor by ultrasmall gold nanoparticles. Microsc Res Tech. (2012) 75:1159–64. doi: 10.1002/jemt.22043
36. Loukanov A, Kuribara A, Filipov C, and Nikolova S. Theranostic nanomachines for cancer treatment. Pharmacia. (2022) 69:285–93. doi: 10.3897/pharmacia.69.e80595
37. Mi J, Ye Q, and Min Y. Advances in nanotechnology development to overcome current roadblocks in CAR-T therapy for solid tumors. Front Immunol. (2022) 13:849759. doi: 10.3389/fimmu.2022.849759
38. Nam J, Son S, Park KS, Zou W, Shea LD, and Moon JJ. Cancer nanomedicine for combination cancer immunotherapy. Nat Rev Mater. (2019) 4:398–414. doi: 10.1038/s41578-019-0108-1
39. Krishnan N, Fang RH, and Zhang L. Cell membrane-coated nanoparticles for the treatment of cancer. Clin Transl Med. (2023) 13:e1285. doi: 10.1002/ctm2.1285
40. Loukanov A, Nikolova S, Filipov C, and Nakabayashi S. Nanomaterials for cancer medication: from individual nanoparticles toward nanomachines and nanorobots. Pharmacia. (2019) 66:147–56. doi: 10.3897/pharmacia.66.e37739
41. Lan H, Jamil M, Ke G, and Dong N. The role of nanoparticles and nanomaterials in cancer diagnosis and treatment: a comprehensive review. Am J Cancer Res. (2023) 13:5751–84.
42. Yao Y, Zhou Y, Liu L, Xu Y, Chen Q, Wang Y, et al. Nanoparticle-based drug delivery in cancer therapy and its role in overcoming drug resistance. Front Mol Biosci. (2020) 7:193. doi: 10.3389/fmolb.2020.00193
43. Al-Thani AN, Jan AG, Abbas M, Geetha M, and Sadasivuni KK. Nanoparticles in cancer theragnostic and drug delivery: A comprehensive review. Life Sci. (2024) 352:122899. doi: 10.1016/j.lfs.2024.122899
44. Elabed S, Sheirf A, and Ali M. Nanostructures for cancer therapeutics and diagnostics: Recent advances and future outlook. Radiat Phys Chem. (2025) 226:112295. doi: 10.1016/j.radphyschem.2024.112295
45. Kang X, Mita N, Zhou L, Wu S, Yue Z, Babu RJ, et al. Nanotechnology in advancing chimeric antigen receptor T cell therapy for cancer treatment. Pharmaceutics. (2024) 16:1228. doi: 10.3390/pharmaceutics16091228
46. Wang B, Hu S, Teng Y, Chen J, Wang H, Xu Y, et al. Current advance of nanotechnology in diagnosis and treatment for Malignant tumors. Signal Transduct Target Ther. (2024) 9:1–65. doi: 10.1038/s41392-024-01889-y
47. Loukanov AR, Basnakian AG, Kawamura R, Udono H, Filipov CK, Savenka AV, et al. Light-powered nanoconverters cytotoxic to breast cancer cells. J Phys Chem C. (2018) 122:7916–24. doi: 10.1021/acs.jpcc.7b11779
48. Loukanov A. Light-triggered Janus nanomotor for targeting and photothermal lysis of pathogenic bacteria. Microsc Res Tech. (2021) 84:967–75. doi: 10.1002/jemt.23657
49. Toshev S and Loukanov A. Ultrasound-propelled biomimetic nanorobot for targeting and isolation of pathogenic bacteria from diverse environmental media. J Min. Geol Sci. (2020) 63:105–7.
50. Pinto IS, Cordeiro RA, and Faneca H. Polymer- and lipid-based gene delivery technology for CAR T cell therapy. J Controlled Release. (2023) 353:196–215. doi: 10.1016/j.jconrel.2022.11.038
51. Bui TA, Mei H, Sang R, Ortega DG, and Deng W. Advancements and challenges in developing in vivo CAR T cell therapies for cancer treatment. eBioMedicine. (2024) 106:4. Available online at: https://www.thelancet.com/journals/ebiom/article/PIIS2352-3964%2824%2900302-5/fulltext.
52. Smith TT, Stephan SB, Moffett HF, McKnight LE, Ji W, Reiman D, et al. In situ programming of leukaemia-specific T cells using synthetic DNA nanocarriers. Nat Nanotechnol. (2017) 12:813–20. doi: 10.1038/nnano.2017.57
53. Zhou JE, Sun L, Jia Y, Wang Z, Luo T, Tan J, et al. Lipid nanoparticles produce chimeric antigen receptor T cells with interleukin-6 knockdown in vivo. J Control Release Off J Control Release Soc. (2022) 350:298–307. doi: 10.1016/j.jconrel.2022.08.033
54. Rurik JG, Tombácz I, Yadegari A, Méndez Fernández PO, Shewale SV, Li L, et al. CAR T cells produced in vivo to treat cardiac injury. Science. (2022) 375:91–6. doi: 10.1126/science.abm0594
55. Dustin ML and Long EO. Cytotoxic immunological synapses. Immunol Rev. (2010) 235:24–34. doi: 10.1111/j.0105-2896.2010.00904.x
56. Davenport AJ, Cross RS, Watson KA, Liao Y, Shi W, Prince HM, et al. Chimeric antigen receptor T cells form nonclassical and potent immune synapses driving rapid cytotoxicity. Proc Natl Acad Sci. (2018) 115:E2068–76. doi: 10.1073/pnas.1716266115
57. Upadhyay R, Boiarsky JA, Pantsulaia G, Svensson-Arvelund J, Lin MJ, Wroblewska A, et al. A critical role for fas-mediated off-target tumor killing in T-cell immunotherapy. Cancer Discov. (2021) 11:599–613. doi: 10.1158/2159-8290.CD-20-0756
58. Larson RC, Kann MC, Bailey SR, Haradhvala NJ, Llopis PM, Bouffard AA, et al. CAR T cell killing requires the IFNγR pathway in solid but not liquid tumours. Nature. (2022) 604:563–70. doi: 10.1038/s41586-022-04585-5
59. Lappas CM, Rieger JM, and Linden J. A2A adenosine receptor induction inhibits IFN-gamma production in murine CD4+ T cells. J Immunol Baltim Md 1950. (2005) 174:1073–80. doi: 10.1038/s41586-022-04585-5
60. Wong KY, Wong MS, and Liu J. Aptamer-functionalized liposomes for drug delivery. BioMed J. (2024) 47:100685. doi: 10.1016/j.bj.2023.100685
61. Fraietta JA, Lacey SF, Orlando EJ, Pruteanu-Malinici I, Gohil M, Lundh S, et al. Determinants of response and resistance to CD19 chimeric antigen receptor (CAR) T cell therapy of chronic lymphocytic leukemia. Nat Med. (2018) 24:563–71. doi: 10.1038/s41591-018-0010-1
62. Nie W, Wei W, Zuo L, Lv C, Zhang F, Lu GH, et al. Magnetic nanoclusters armed with responsive PD-1 antibody synergistically improved adoptive T-cell therapy for solid tumors. ACS Nano. (2019) 13:1469–78. doi: 10.1021/acsnano.8b07141
63. Stephan MT, Moon JJ, Um SH, Bershteyn A, and Irvine DJ. Therapeutic cell engineering using surface-conjugated synthetic nanoparticles. Nat Med. (2010) 16:1035–41. doi: 10.1038/nm.2198
64. Heckler M and Dougan SK. Unmasking pancreatic cancer: epitope spreading after single antigen chimeric antigen receptor T-cell therapy in a human phase I trial. Gastroenterology. (2018) 155:11–4. doi: 10.1053/j.gastro.2018.06.023
65. Lu J, Choi E, Tamanoi F, and Zink JI. Light-activated nanoimpeller-controlled drug release in cancer cells. Small Weinh Bergstr Ger. (2008) 4:421–6. doi: 10.1002/smll.200700903
66. Li Y, Tang K, Zhang X, Pan W, Li N, and Tang B. A dendritic cell-like biomimetic nanoparticle enhances T cell activation for breast cancer immunotherapy. Chem Sci. (2021) 13:105–10. doi: 10.1039/D1SC03525H
67. Zhang J, Fan B, Cao G, Huang W, Jia F, Nie G, et al. Direct presentation of tumor-associated antigens to induce adaptive immunity by personalized dendritic cell-mimicking nanovaccines. Adv Mater. (2022) 34:2205950. doi: 10.1002/adma.202205950
68. Persano S, Guevara ML, Li Z, Mai J, Ferrari M, Pompa PP, et al. Lipopolyplex potentiates anti-tumor immunity of mRNA-based vaccination. Biomaterials. (2017) 125:81–9. doi: 10.1016/j.biomaterials.2017.02.019
69. Burga RA, Thorn M, Point GR, Guha P, Nguyen CT, Licata LA, et al. Liver myeloid-derived suppressor cells expand in response to liver metastases in mice and inhibit the anti-tumor efficacy of anti-CEA CAR-T. Cancer Immunol Immunother CII. (2015) 64:817–29. doi: 10.1007/s00262-015-1692-6
70. Wrzesinski SH, Wan YY, and Flavell RA. Transforming growth factor-beta and the immune response: implications for anticancer therapy. Clin Cancer Res Off J Am Assoc Cancer Res. (2007) 13:5262–70. doi: 10.1158/1078-0432.CCR-07-1157
71. Chada NC and Wilson JT. Jump-starting chimeric antigen receptor-T cells to go the extra mile with nanotechnology. Curr Opin Biotechnol. (2024) 89:103179. doi: 10.1016/j.copbio.2024.103179
72. Siriwon N, Kim YJ, Siegler E, Chen X, Rohrs JA, Liu Y, et al. CAR-T cells surface-engineered with drug-encapsulated nanoparticles can ameliorate intratumoral T-cell hypofunction. Cancer Immunol Res. (2018) 6:812–24. doi: 10.1158/2326-6066.CIR-17-0502
73. Li S, Jiang Q, Liu S, Zhang Y, Tian Y, Song C, et al. A DNA nanorobot functions as a cancer therapeutic in response to a molecular trigger in vivo. Nat Biotechnol. (2018) 36:258–64. doi: 10.1038/nbt.4071
74. Chu S, Shi X, Tian Y, and Gao F. pH-responsive polymer nanomaterials for tumor therapy. Front Oncol. (2022) 12:855019. doi: 10.3389/fonc.2022.855019
75. Zhang Y, Zeng X, Wang H, Fan R, Hu Y, Hu X, et al. Dasatinib self-assembled nanoparticles decorated with hyaluronic acid for targeted treatment of tumors to overcome multidrug resistance. Drug Deliv. (2021) 28:670–9. doi: 10.1080/10717544.2021.1905751
76. Safarzadeh Kozani P, Naseri A, Mirarefin SMJ, Salem F, Nikbakht M, Evazi Bakhshi S, et al. Nanobody-based CAR-T cells for cancer immunotherapy. biomark Res. (2022) 10:24. doi: 10.1186/s40364-022-00371-7
77. Tu B, Zhang M, Liu T, and Huang Y. Nanotechnology-based histone deacetylase inhibitors for cancer therapy. Front Cell Dev Biol. (2020) 8:400/full. doi: 10.3389/fcell.2020.00400/full
78. Stephan SB, Taber AM, Jileaeva I, Pegues EP, Sentman CL, and Stephan MT. Biopolymer implants enhance the efficacy of adoptive T-cell therapy. Nat Biotechnol. (2015) 33:97–101. doi: 10.1038/nbt.3104
79. Dinauer N, Balthasar S, Weber C, Kreuter J, Langer K, and von Briesen H. Selective targeting of antibody-conjugated nanoparticles to leukemic cells and primary T-lymphocytes. Biomaterials. (2005) 26:5898–906. doi: 10.1016/j.biomaterials.2005.02.038
80. Chen SP, Wang S, Liao S, and Blakney AK. Exploring the effects of incorporating different bioactive phospholipids into messenger ribonucleic acid lipid nanoparticle (mRNA LNP) formulations. ACS Bio Med Chem Au. (2025) 5:154–65. doi: 10.1021/acsbiomedchemau.4c00085
81. Wauters AC, Scheerstra JF, Vermeijlen IG, Hammink R, Schluck M, Woythe L, et al. Artificial antigen-presenting cell topology dictates T cell activation. ACS Nano. (2022) 16:15072–85. doi: 10.1021/acsnano.2c06211
82. Zheng Y, Tang L, Mabardi L, Kumari S, and Irvine DJ. Enhancing adoptive cell therapy of cancer through targeted delivery of small-molecule immunomodulators to internalizing or noninternalizing receptors. ACS Nano. (2017) 11:3089–100. doi: 10.1021/acsnano.7b00078
83. Tang L, Zheng Y, Melo MB, Mabardi L, Castaño AP, Xie YQ, et al. Enhancing T cell therapy through TCR-signaling-responsive nanoparticle drug delivery. Nat Biotechnol. (2018) 36:707–16. doi: 10.1038/nbt.4181
84. Chen Z, Pan H, Luo Y, Yin T, Zhang B, Liao J, et al. Nanoengineered CAR-T biohybrids for solid tumor immunotherapy with microenvironment photothermal-remodeling strategy. Small Weinh Bergstr Ger. (2021) 17:e2007494. doi: 10.1002/smll.202007494
85. Fang J, Sawa T, and Maeda H. Factors and mechanism of “EPR” Effect and the enhanced antitumor effects of macromolecular drugs including SMANCS. In: Maeda H, Kabanov A, Kataoka K, and Okano T, editors. Polymer Drugs in the Clinical Stage: Advantages and Prospects. Springer US, Boston, MA (2003). p. 29–49. doi: 10.1007/0-306-47932-X_2
86. Nawaz W, Xu S, Li Y, Huang B, Wu X, and Wu Z. Nanotechnology and immunoengineering: How nanotechnology can boost CAR-T therapy. Acta Biomater. (2020) 109:21–36. doi: 10.1016/j.actbio.2020.04.015
87. Cheung AS, Zhang DKY, Koshy ST, and Mooney DJ. Scaffolds that mimic antigen-presenting cells enable ex vivo expansion of primary T cells. Nat Biotechnol. (2018) 36:160–9. doi: 10.1038/nbt.4047
88. Kiru L, Zlitni A, Tousley AM, Dalton GN, Wu W, Lafortune F, et al. In vivo imaging of nanoparticle-labeled CAR T cells. Proc Natl Acad Sci U.S.A. (2022) 119:e2102363119. doi: 10.1073/pnas.2102363119
89. Alowais SA, Alghamdi SS, Alsuhebany N, Alqahtani T, Alshaya AI, Almohareb SN, et al. Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC Med Educ. (2023) 23:689. doi: 10.1186/s12909-023-04698-z
90. Khanna NN, Maindarkar MA, Viswanathan V, Fernandes JFE, Paul S, Bhagawati M, et al. Economics of Artificial Intelligence in Healthcare: Diagnosis vs. Treatment. Healthc Switz. (2022) 10:6. Available online at: http://www.scopus.com/inward/record.url?scp=85144668904&partnerID=8YFLogxK.
91. Nilius H, Tsouka S, Nagler M, and Masoodi M. Machine learning applications in precision medicine: Overcoming challenges and unlocking potential. TrAC Trends Anal Chem. (2024) 179:117872. doi: 10.1016/j.trac.2024.117872
92. Quazi S. Artificial intelligence and machine learning in precision and genomic medicine. Med Oncol Northwood Lond Engl. (2022) 39:120. doi: 10.1007/s12032-022-01711-1
93. Ocampo Osorio F, Alzate-Ricaurte S, Mejia Vallecilla TE, and Cruz-Suarez GA. The anesthesiologist’s guide to critically assessing machine learning research: a narrative review. BMC Anesthesiol. (2024) 24:452. doi: 10.1186/s12871-024-02840-y
94. Robinson MC, Glen RC, and Lee AA. Validating the validation: reanalyzing a large-scale comparison of deep learning and machine learning models for bioactivity prediction. J Comput Aided Mol Des. (2020) 34:717–30. doi: 10.1007/s10822-019-00274-0
95. Davenport T and Kalakota R. The potential for artificial intelligence in healthcare. Future Healthc J. (2019) 6:94. doi: 10.7861/futurehosp.6-2-94
96. Ongsulee P. Artificial intelligence, machine learning and deep learning. 2017 15th Int Conf ICT Knowl Eng ICTKE. (2017) 1–6. doi: 10.1109/ICTKE.2017.8259629
97. Gawehn E, Hiss JA, and Schneider G. Deep learning in drug discovery. Mol Inform. (2016) 35:3–14. doi: 10.1002/minf.201501008
98. LeCun Y, Bengio Y, and Hinton G. Deep learning. Nature. (2015) 521:436–44. doi: 10.1038/nature14539
99. Desai M and Shah M. An anatomization on breast cancer detection and diagnosis employing multi-layer perceptron neural network (MLP) and Convolutional neural network (CNN). Clin EHealth. (2021) 4:1–11. doi: 10.1016/j.ceh.2020.11.002
100. Chen H, Engkvist O, Wang Y, Olivecrona M, and Blaschke T. The rise of deep learning in drug discovery. Drug Discov Today. (2018) 23:4. doi: 10.1016/j.drudis.2018.01.039
101. Suresh N, Kumar NCA, Subramanian S, and Srinivasa G. Memory augmented recurrent neural networks for de-novo drug design. PloS One. (2022) 17:e0269461. doi: 10.1371/journal.pone.0269461
102. Naik GG and Jagtap VA. Two heads are better than one: Unravelling the potential Impact of Artificial Intelligence in nanotechnology. Nano TransMed. (2024) 3:100041. doi: 10.1016/j.ntm.2024.100041
103. Sharma B, Chenthamarakshan V, Dhurandhar A, Pereira S, Hendler JA, Dordick JS, et al. Accurate clinical toxicity prediction using multi-task deep neural nets and contrastive molecular explanations. Sci Rep. (2023) 13:4908. doi: 10.1038/s41598-023-31169-8
104. Zhou J, Cui G, Hu S, Zhang Z, Yang C, Liu Z, et al. Graph neural networks: A review of methods and applications. arXiv. (2021). Available online at: http://arxiv.org/abs/1812.08434.
105. Goodfellow IJ, Pouget-Abadie J, Mirza M, Xu B, Warde-Farley D, Ozair S, et al. Generative adversarial networks. arXiv. (2014). Available online at: http://arxiv.org/abs/1406.2661 (Accessed April 15, 2025).
106. Vaswani A, Shazeer N, Parmar N, Uszkoreit J, Jones L, Gomez AN, et al. Attention is all you need. arXiv. (2023). Available online at: http://arxiv.org/abs/1706.03762 (Accessed April 15, 2025).
107. Boretti A. Improving chimeric antigen receptor T-cell therapies by using artificial intelligence and internet of things technologies: A narrative review. Eur J Pharmacol. (2024) 974:176618. doi: 10.1016/j.ejphar.2024.176618
108. Bhattamisra SK, Banerjee P, Gupta P, Mayuren J, Patra S, and Candasamy M. Artificial intelligence in pharmaceutical and healthcare research. Big Data Cognit Comput. (2023) 7:10. doi: 10.3390/bdcc7010010
109. Jak M, van der Velden BHM, de Keizer B, Elias SG, Minnema MC, and Gilhuijs KGA. Prediction of poor outcome after tisagenlecleucel in patients with relapsed or refractory diffuse large B cell lymphoma (DLBCL) using artificial intelligence analysis of pre-infusion PET/CT. Blood. (2022) 140:1919–20. doi: 10.1182/blood-2022-158543
110. Tong Y, Udupa JK, Chong E, Winchell N, Sun C, Zou Y, et al. Prediction of lymphoma response to CAR T cells by deep learning-based image analysis. PloS One. (2023) 18:e0282573. doi: 10.1371/journal.pone.0282573
111. Yan F, Jiang VC, Liu Y, Li Y, Che Y, Jain P, et al. Predicting CAR-T response in mantle cell lymphoma using deep neural network models on single-cell RNA sequencing data. Blood. (2023) 142:4377. doi: 10.1182/blood-2023-187544
112. Ceja MA, Khericha M, Harris CM, Puig-Saus C, and Chen Y. CAR-T cell manufacturing: Major process parameters and next-generation strategies. J Exp Med. (2024). Available online at: https://www.semanticscholar.org/paper/CAR-T-cell-manufacturing%3A-Major-process-parameters-Ceja-Khericha/4cc1766c8d2b7769aaf4edcb5fba9ef144c4313a.
113. Molina SA, Davies SJ, Sethi D, Oh S, Durand N, Scott M, et al. Particulates are everywhere, but are they harmful in cell and gene therapies? Cytotherapy. (2022) 24:1195–200. doi: 10.1084/jem.20230903
114. Andrzejewska A, Jablonska A, Seta M, Dabrowska S, Walczak P, Janowski M, et al. Labeling of human mesenchymal stem cells with different classes of vital stains: robustness and toxicity. Stem Cell Res Ther. (2019) 10:187. doi: 10.1186/s13287-019-1296-8
115. Cossarizza A, Chang HD, Radbruch A, Acs A, Adam D, Adam-Klages S, et al. Guidelines for the use of flow cytometry and cell sorting in immunological studies (second edition). Eur J Immunol. (2019) 49:1457–973. doi: 10.1002/eji.201970107
116. Campbell JDM and Fraser AR. Flow cytometric assays for identity, safety and potency of cellular therapies. Cytometry B Clin Cytom. (2018) 94:725–35. doi: 10.1002/cyto.b.21735
117. Sugimoto K. Machine learning-driven label-free cell sorting for CAR-T cell manufacturing. Cytotherapy. (2019) 21:S39. doi: 10.1016/j.jcyt.2019.03.376
118. Teranishi K, Wagatsuma K, Toda K, Nomaru H, Yanagihashi Y, Ochiai H, et al. Label-free ghost cytometry for manufacturing of cell therapy products. Sci Rep. (2024) 14:21848. doi: 10.1038/s41598-024-72016-8
119. Salek M, Li N, Chou HP, Saini K, Jovic A, Jacobs KB, et al. COSMOS: a platform for real-time morphology-based, label-free cell sorting using deep learning. Commun Biol. (2023) 6:1–11. doi: 10.1038/s42003-023-05325-9
120. Mavropoulos A, Johnson C, Lu V, Nieto J, Schneider EC, Saini K, et al. Artificial intelligence-driven morphology-based enrichment of Malignant cells from body fluid. Mod Pathol Off J U S Can Acad Pathol Inc. (2023) 36:100195. doi: 10.1016/j.modpat.2023.100195
121. Shaban M, Bai Y, Qiu H, Mao S, Yeung J, Yeo YY, et al. MAPS: pathologist-level cell type annotation from tissue images through machine learning. Nat Commun. (2024) 15:28. doi: 10.1038/s41467-023-44188-w
122. Kawalekar OU, O’Connor RS, Fraietta JA, Guo L, McGettigan SE, Posey AD, et al. Distinct signaling of coreceptors regulates specific metabolism pathways and impacts memory development in CAR T cells. Immunity. (2016) 44:380–90. doi: 10.1016/j.immuni.2016.01.021
123. Daniels KG, Wang S, Simic MS, Bhargava HK, Capponi S, Tonai Y, et al. Decoding CAR T cell phenotype using combinatorial signaling motif libraries and machine learning. Science. (2022) 378:1194–200. doi: 10.1126/science.abq0225
124. Huppa JB and Davis MM. T-cell-antigen recognition and the immunological synapse. Nat Rev Immunol. (2003) 3:973–83. doi: 10.1038/nri1245
125. Liu D, Badeti S, Dotti G, Jiang Jg, Wang H, Dermody J, et al. The role of immunological synapse in predicting the efficacy of chimeric antigen receptor (CAR) immunotherapy. Cell Commun Signal. (2020) 18:134. doi: 10.1186/s12964-020-00617-7
126. Cassioli C, Patrussi L, Valitutti S, and Baldari CT. Learning from TCR signaling and immunological synapse assembly to build new chimeric antigen receptors (CARs). Int J Mol Sci. (2022) 23:14255. doi: 10.3390/ijms232214255
127. Xiong W, Chen Y, Kang X, Chen Z, Zheng P, Hsu YH, et al. Immunological synapse predicts effectiveness of chimeric antigen receptor cells. Mol Ther. (2021) 29:1349–51. doi: 10.1016/j.ymthe.2021.01.025
128. Naghizadeh A, Tsao Wc, JH C, Xu H, Mohamed M, Li D, et al. In vitro machine learning-based CAR T immunological synapse quality measurements correlate with patient clinical outcomes. PloS Comput Biol. (2022) 18:e1009883. doi: 10.1371/journal.pcbi.1009883
129. Lee M, Lee YH, Song J, Kim G, Jo Y, Min H, et al. Deep-learning-based three-dimensional label-free tracking and analysis of immunological synapses of CAR-T cells. eLife. (2020) 9:e49023. doi: 10.7554/eLife.49023
130. Chen J, Qiu S, Li W, Wang K, Zhang Y, Yang H, et al. Tuning charge density of chimeric antigen receptor optimizes tonic signaling and CAR-T cell fitness. Cell Res. (2023) 33:341–54. doi: 10.1038/s41422-023-00789-0
131. Wang H, Huang Y, and Xu C. Charging CAR by electrostatic power. Immunol Rev. (2023) 320:138–46. doi: 10.1111/imr.13232
132. Wang H, Song X, Shen L, Wang X, and Xu C. Exploiting T cell signaling to optimize engineered T cell therapies. Trends Cancer. (2022) 8:123–34. doi: 10.1016/j.trecan.2021.10.007
133. Qiu S, Chen J, Wu T, Li L, Wang G, Wu H, et al. CAR-Toner: an AI-driven approach for CAR tonic signaling prediction and optimization. Cell Res. (2024) 34:386–8. doi: 10.1038/s41422-024-00936-1
134. Gust J, Hay KA, Hanafi LA, Li D, Myerson D, Gonzalez-Cuyar LF, et al. Endothelial activation and blood-brain barrier disruption in neurotoxicity after adoptive immunotherapy with CD19 CAR-T cells. Cancer Discov. (2017) 7:1404–19. doi: 10.1158/2159-8290.CD-17-0698
135. Gust J, Finney OC, Li D, Brakke HM, Hicks RM, Futrell RB, et al. Glial injury in neurotoxicity after pediatric CD19-directed chimeric antigen receptor T cell therapy. Ann Neurol. (2019) 86:42–54. doi: 10.1002/ana.25502
136. Frey N and Porter D. Cytokine release syndrome with chimeric antigen receptor T cell therapy. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant. (2019) 25:e123–7. doi: 10.1016/j.bbmt.2018.12.756
137. Gudiol C, Lewis RE, Strati P, and Kontoyiannis DP. Chimeric antigen receptor T-cell therapy for the treatment of lymphoid Malignancies: is there an excess risk for infection? Lancet Haematol. (2021) 8:e216–28. doi: 10.1016/S2352-3026(20)30376-8
138. Park JH, Rivière I, Gonen M, Wang X, Sénéchal B, Curran KJ, et al. Long-term follow-up of CD19 CAR therapy in acute lymphoblastic leukemia. N Engl J Med. (2018) 378:449–59. doi: 10.1056/NEJMoa1709919
139. Fajgenbaum DC and June CH. Cytokine storm. N Engl J Med. (2020) 383:2255–73. doi: 10.1056/NEJMra2026131
140. Giavridis T, van der Stegen SJC, Eyquem J, Hamieh M, Piersigilli A, and Sadelain M. CAR T cell-induced cytokine release syndrome is mediated by macrophages and abated by IL-1 blockade. Nat Med. (2018) 24:731–8. doi: 10.1038/s41591-018-0041-7
141. Kang S, Tanaka T, Inoue H, Ono C, Hashimoto S, Kioi Y, et al. IL-6 trans-signaling induces plasminogen activator inhibitor-1 from vascular endothelial cells in cytokine release syndrome. Proc Natl Acad Sci U.S.A. (2020) 117:22351–6. doi: 10.1073/pnas.2010229117
142. Bogatu A, Wysocka M, Wysocki O, Butterworth H, Pillai M, Allison J, et al. Meta-analysis informed machine learning: Supporting cytokine storm detection during CAR-T cell Therapy. J BioMed Inform. (2023) 142:104367. doi: 10.1016/j.jbi.2023.104367
143. Hayden PJ, Roddie C, Bader P, Basak GW, Bonig H, Bonini C, et al. Management of adults and children receiving CAR T-cell therapy: 2021 best practice recommendations of the European Society for Blood and Marrow Transplantation (EBMT) and the Joint Accreditation Committee of ISCT and EBMT (JACIE) and the European Haematology Association (EHA). Ann Oncol Off J Eur Soc Med Oncol. (2022) 33:259–75. doi: 10.1016/j.annonc.2021.12.003
144. Amidi Y, Eckhardt CA, Quadri SA, Malik P, Firme MS, Jones DK, et al. Forecasting immune effector cell-associated neurotoxicity syndrome after chimeric antigen receptor t-cell therapy. J Immunother Cancer. (2022) 10:e005459. doi: 10.1136/jitc-2022-005459
145. Khairnar SV, Pagare P, Thakre A, Nambiar AR, Junnuthula V, Abraham MC, et al. Review on the scale-up methods for the preparation of solid lipid nanoparticles. Pharmaceutics. (2022) 14:1886. doi: 10.3390/pharmaceutics14091886
146. Mülhopt S, Diabaté S, Dilger M, Adelhelm C, Anderlohr C, Bergfeldt T, et al. Characterization of nanoparticle batch-to-batch variability. Nanomaterials. (2018) 8:311. doi: 10.3390/nano8050311
147. Silveira RF, Lima AL, Gross IP, Gelfuso GM, Gratieri T, and Cunha-Filho M. The role of artificial intelligence and data science in nanoparticles development: a review. Nanomed. (2024) 19:1271–83. doi: 10.1080/17435889.2024.2359355
148. Jiang Y, Salley D, Sharma A, Keenan G, Mullin M, and Cronin L. An artificial intelligence enabled chemical synthesis robot for exploration and optimization of nanomaterials. Sci Adv. (2022) 8:eabo2626. doi: 10.1126/sciadv.abo2626
149. Tenchov R, Bird R, Curtze AE, and Zhou Q. Lipid nanoparticles─From liposomes to mRNA vaccine delivery, a landscape of research diversity and advancement. ACS Nano. (2021) 15:16982–7015. doi: 10.1021/acsnano.1c04996
150. Hassett KJ, Benenato KE, Jacquinet E, Lee A, Woods A, Yuzhakov O, et al. Optimization of lipid nanoparticles for intramuscular administration of mRNA vaccines. Mol Ther Nucleic Acids. (2019) 15:1–11. doi: 10.1016/j.omtn.2019.01.013
151. Kauffman KJ, Dorkin JR, Yang JH, Heartlein MW, DeRosa F, Mir FF, et al. Optimization of lipid nanoparticle formulations for mRNA delivery in vivo with fractional factorial and definitive screening designs. Nano Lett. (2015) 15:7300–6. doi: 10.1021/acs.nanolett.5b02497
152. Nakamura T, Kawai M, Sato Y, Maeki M, Tokeshi M, and Harashima H. The effect of size and charge of lipid nanoparticles prepared by microfluidic mixing on their lymph node transitivity and distribution. Mol Pharm. (2020) 17:944–53. doi: 10.1021/acs.molpharmaceut.9b01182
153. Cui L, Hunter MR, Sonzini S, Pereira S, Romanelli SM, Liu K, et al. Mechanistic studies of an automated lipid nanoparticle reveal critical pharmaceutical properties associated with enhanced mRNA functional delivery in vitro and in vivo. Small Weinh Bergstr Ger. (2022) 18:e2105832. doi: 10.1002/smll.202105832
154. Hassett KJ, Higgins J, Woods A, Levy B, Xia Y, Hsiao CJ, et al. Impact of lipid nanoparticle size on mRNA vaccine immunogenicity. J Control Release Off J Control Release Soc. (2021) 335:237–46. doi: 10.1016/j.jconrel.2021.05.021
155. FDA- Liposome Drug Products, Chemistry, Manufacturing, and Controls, Human Pharmacokinetics and Bioavailability, Labeling Documentation. Guidance for Industry, and Pharmaceutical Quality/CMC. U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). New Hampshire: Food and Drug Administration (2018).
156. Sato S, Sano S, Muto H, Kubara K, Kondo K, Miyazaki T, et al. Understanding the manufacturing process of lipid nanoparticles for mRNA delivery using machine learning. Chem Pharm Bull (Tokyo). (2024) 72:529–39. doi: 10.1248/cpb.c24-00089
157. Mottafegh A, Joo JU, Na GS, Sharma V, and Kim DP. AI-assisted autonomous manufacturing of tailored drug-loaded nanoparticles by multi-step continuous-flow platform. Chem Eng J. (2024) 500:157454. doi: 10.1016/j.cej.2024.157454
158. Amor H, Kouki A, Marsh P, Kim K, and Cao H. Development of a novel miniaturized LTCC-based wireless pH sensing system. IEEE Sensors. (2016) 2025:1 p. doi: 10.1109/ICSENS.2016.7808853
159. Huang WD, Cao H, Deb S, Chiao M, and Chiao JC. A flexible pH sensor based on the iridium oxide sensing film. Sens Actuators Phys. (2011) 169:1–11. doi: 10.1016/j.sna.2011.05.016
160. Jia H, Chang G, Shu H, Xu M, Wang X, Zhang Z, et al. Pt nanoparticles modified Au dendritic nanostructures: Facile synthesis and enhanced electrocatalytic performance for methanol oxidation. Int J Hydrog Energy. (2017) 42:22100–7. doi: 10.1016/j.ijhydene.2017.01.218
161. Xie W, Zhang F, Wang Z, Yang M, Xia J, Gui R, et al. Facile preparation of PtPdPt/graphene nanocomposites with ultrahigh electrocatalytic performance for methanol oxidation. J Electroanal Chem. (2016) 761:55–61. doi: 10.1016/j.jelechem.2015.12.007
162. John-Herpin A, Kavungal D, von Mücke L, and Altug H. Infrared metasurface augmented by deep learning for monitoring dynamics between all major classes of biomolecules. Adv Mater. (2021) 33:2006054. doi: 10.1002/adma.202006054
163. Leong SX, Leong YX, Koh CSL, Tan EX, Nguyen LBT, Chen JRT, et al. Emerging nanosensor platforms and machine learning strategies toward rapid, point-of-need small-molecule metabolite detection and monitoring. Chem Sci. (2022) 13:11009–29. doi: 10.1039/D2SC02981B
164. Li JQ, Dukes PV, Lee W, Sarkis M, and Vo-Dinh T. Machine learning using convolutional neural networks for SERS analysis of biomarkers in medical diagnostics. J Raman Spectrosc. (2022) 53:2044–57. doi: 10.1002/jrs.6447
165. Hort S, Herbst L, Bäckel N, Erkens F, Niessing B, Frye M, et al. Toward rapid, widely available autologous CAR-T cell therapy - artificial intelligence and automation enabling the smart manufacturing hospital. Front Med. (2022) 9:913287. doi: 10.3389/fmed.2022.913287
166. Grzesik P and Warth SC. One-time optimization of advanced T cell culture media using a machine learning pipeline. Front Bioeng Biotechnol. (2021) 9:614324. doi: 10.3389/fbioe.2021.614324
167. Billingsley MM, Singh N, Ravikumar P, Zhang R, June CH, and Mitchell MJ. Ionizable lipid nanoparticle-mediated mRNA delivery for human CAR T cell engineering. Nano Lett. (2020) 20:1578–89. doi: 10.1021/acs.nanolett.9b04246
168. Hou X, Zaks T, Langer R, and Dong Y. Lipid nanoparticles for mRNA delivery. Nat Rev Mater. (2021) 6:1078–94. doi: 10.1038/s41578-021-00358-0
169. Paramasivam P, Franke C, Stöter M, Höijer A, Bartesaghi S, Sabirsh A, et al. Endosomal escape of delivered mRNA from endosomal recycling tubules visualized at the nanoscale. J Cell Biol. (2022) 221:e202110137. doi: 10.1083/jcb.202110137
170. Han X, Zhang H, Butowska K, Swingle KL, Alameh MG, Weissman D, et al. An ionizable lipid toolbox for RNA delivery. Nat Commun. (2021) 12:7233. doi: 10.1038/s41467-021-27493-0
171. Freeman EC, Weiland LM, and Meng WS. Modeling the proton sponge hypothesis: examining proton sponge effectiveness for enhancing intracellular gene delivery through multiscale modeling. J Biomater Sci Polym Ed. (2013) 24:398–416. doi: 10.1080/09205063.2012.690282
172. Foret L, Dawson JE, Villaseñor R, Collinet C, Deutsch A, Brusch L, et al. A general theoretical framework to infer endosomal network dynamics from quantitative image analysis. Curr Biol CB. (2012) 22:1381–90. doi: 10.1016/j.cub.2012.06.021
173. Gautreau A, Oguievetskaia K, and Ungermann C. Function and regulation of the endosomal fusion and fission machineries. Cold Spring Harb Perspect Biol. (2014) 6:a016832. doi: 10.1101/cshperspect.a016832
174. Price E and Gesquiere AJ. An in vitro assay and artificial intelligence approach to determine rate constants of nanomaterial-cell interactions. Sci Rep. (2019) 9:13943. doi: 10.1038/s41598-019-50208-x
175. Xu Y, Ma S, Cui H, Chen J, Xu S, Gong F, et al. AGILE platform: a deep learning powered approach to accelerate LNP development for mRNA delivery. Nat Commun. (2024) 15:6305. doi: 10.1038/s41467-024-50619-z
176. Wu K, Wang Z, Yang X, Chen Y, Han Z, Zhang J, et al. TransMA: an explainable multi-modal deep learning model for predicting properties of ionizable lipid nanoparticles in mRNA delivery. arXiv. (2024). Available online at: http://arxiv.org/abs/2407.05736 (Accessed May 14 & 15, 2025).
177. Colli LM, Machiela MJ, Myers TA, Jessop L, Yu K, and Chanock SJ. Burden of nonsynonymous mutations among TCGA cancers and candidate immune checkpoint inhibitor responses. Cancer Res. (2016) 76:3767–72. doi: 10.1158/0008-5472.CAN-16-0170
178. Thorsson V, Gibbs DL, Brown SD, Wolf D, Bortone DS, Ou Yang TH, et al. The immune landscape of cancer. Immunity. (2018) 48:812–830.e14. doi: 10.1016/j.immuni.2018.03.023
179. Saito R, Smith CC, Utsumi T, Bixby LM, Kardos J, Wobker SE, et al. Molecular subtype-specific immunocompetent models of high-grade urothelial carcinoma reveal differential neoantigen expression and response to immunotherapy. Cancer Res. (2018) 78:3954–68. doi: 10.1158/0008-5472.CAN-18-0173
180. Smith CC, Chai S, Washington AR, Lee SJ, Landoni E, Field K, et al. Machine-learning prediction of tumor antigen immunogenicity in the selection of therapeutic epitopes. Cancer Immunol Res. (2019) 7:1591–604. doi: 10.1158/2326-6066.CIR-19-0155
181. Jamialahmadi H, Khalili-Tanha G, Nazari E, and Rezaei-Tavirani M. Artificial intelligence and bioinformatics: a journey from traditional techniques to smart approaches. Gastroenterol Hepatol Bed Bench. (2024) 17:241–52. doi: 10.22037/ghfbb.v17i3.2977
182. Perna F, Berman SH, Soni RK, Mansilla-Soto J, Eyquem J, Hamieh M, et al. Integrating proteomics and transcriptomics for systematic combinatorial chimeric antigen receptor therapy of AML. Cancer Cell. (2017) 32:506–519.e5. doi: 10.1016/j.ccell.2017.09.004
183. Mann M, Kumar C, Zeng WF, and Strauss MT. Artificial intelligence for proteomics and biomarker discovery. Cell Syst. (2021) 12:759–70. doi: 10.1016/j.cels.2021.06.006
184. Bhinder B, Gilvary C, Madhukar NS, and Elemento O. Artificial intelligence in cancer research and precision medicine. Cancer Discov. (2021) 11:900–15. doi: 10.1158/2159-8290.CD-21-0090
185. Shao XM, Bhattacharya R, Huang J, Sivakumar IKA, Tokheim C, Zheng L, et al. High-throughput prediction of MHC Class i and II neoantigens with MH cnuggets. Cancer Immunol Res. (2020) 8:396–408. doi: 10.1158/2326-6066.CIR-19-0464
186. Sterner RC and Sterner RM. CAR-T cell therapy: current limitations and potential strategies. Blood Cancer J. (2021) 11:1–11. doi: 10.1038/s41408-021-00459-7
187. Jogalekar MP, Rajendran RL, Khan F, Dmello C, Gangadaran P, and Ahn BC. CAR T-Cell-Based gene therapy for cancers: new perspectives, challenges, and clinical developments. Front Immunol. (2022) 13:925985. doi: 10.3389/fimmu.2022.925985
188. Zhao X, Zhang J, Chen B, Ding X, Zhao N, and Xu FJ. Rough nanovaccines boost antitumor immunity through the enhancement of vaccination cascade and immunogenic cell death induction. Small Methods. (2023) 7:e2201595. doi: 10.1002/smtd.202201595
189. Feng H, Sun X, Li N, Xu Q, Li Q, Zhang S, et al. Machine learning-driven methods for nanobody affinity prediction. ACS Omega. (2024) 9:47893–902. doi: 10.1021/acsomega.4c09718
190. Wang H, Arulraj T, Ippolito A, and Popel AS. From virtual patients to digital twins in immuno-oncology: lessons learned from mechanistic quantitative systems pharmacology modeling. NPJ Digit Med. (2024) 7:1–6. doi: 10.1038/s41746-024-01188-4
191. Stahlberg EA, Abdel-Rahman M, Aguilar B, Asadpoure A, Beckman RA, Borkon LL, et al. Exploring approaches for predictive cancer patient digital twins: Opportunities for collaboration and innovation. Front Digit Health. (2022) 4:1007784/full. doi: 10.3389/fdgth.2022.1007784/full
192. Katsoulakis E, Wang Q, Wu H, Shahriyari L, Fletcher R, Liu J, et al. Digital twins for health: a scoping review. NPJ Digit Med. (2024) 7:1–11. doi: 10.1038/s41746-024-01073-0
193. Moingeon P, Chenel M, Rousseau C, Voisin E, and Guedj M. Virtual patients, digital twins and causal disease models: Paving the ground for in silico clinical trials. Drug Discov Today. (2023) 28:103605. doi: 10.1016/j.drudis.2023.103605
194. Wu C, Jarrett AM, Zhou Z, Elshafeey N, Adrada BE, Candelaria RP, et al. MRI-based digital models forecast patient-specific treatment responses to neoadjuvant chemotherapy in triple-negative breast cancer. Cancer Res. (2022) 82:3394–404. doi: 10.1158/0008-5472.CAN-22-1329
195. Cheng Y, Straube R, Alnaif AE, Huang L, Leil TA, and Schmidt BJ. Virtual populations for quantitative systems pharmacology models. Methods Mol Biol Clifton NJ. (2022) 2486:129–79. doi: 10.1007/978-1-0716-2265-0_8
196. Sové RJ, Jafarnejad M, Zhao C, Wang H, Ma H, and Popel AS. QSP-IO: A quantitative systems pharmacology toolbox for mechanistic multiscale modeling for immuno-oncology applications. CPT Pharmacomet Syst Pharmacol. (2020) 9:484–97. doi: 10.1002/psp4.12546
197. Jafarnejad M, Gong C, Gabrielson E, Bartelink IH, Vicini P, Wang B, et al. A computational model of neoadjuvant PD-1 inhibition in non-small cell lung cancer. AAPS J. (2019) 21:79. doi: 10.1208/s12248-019-0350-x
198. Ma H, Wang H, Sove RJ, Jafarnejad M, Tsai CH, Wang J, et al. A quantitative systems pharmacology model of T cell engager applied to solid tumor. AAPS J. (2020) 22:85. doi: 10.1208/s12248-020-00450-3
199. Joslyn LR, Huang W, Miles D, Hosseini I, and Ramanujan S. Digital twins elucidate critical role of Tscm in clinical persistence of TCR-engineered cell therapy. NPJ Syst Biol Appl. (2024) 10:1–12. doi: 10.1038/s41540-024-00335-7
200. Applied Clinical Trials. A digital twin on CAR-T cytokine release syndrome (CRS) patients with standard of care measured by CRS distribution by grade. Available online at: https://www.appliedclinicaltrialsonline.com/view/a-digital-twin-on-car-t-cytokine-release-syndrome-crs-patients-with-standard-of-care-measured-by-crs-distribution-by-grade (Accessed April 5, 2025).
201. Goraya SA, Ding S, Miller RC, Arif MK, Kong H, and Masud A. Modeling of spatiotemporal dynamics of ligand-coated particle flow in targeted drug delivery processes. Proc Natl Acad Sci. (2024) 121:e2314533121. doi: 10.1073/pnas.2314533121
202. Shabbir F, Mujeeb AA, Jawed SF, Khan AH, and Shakeel CS. Simulation of transvascular transport of nanoparticles in tumor microenvironments for drug delivery applications. Sci Rep. (2024) 14:1764. doi: 10.1038/s41598-024-52292-0
203. Howard FM, He G, Peterson JR, Pfeiffer JR, Earnest T, Pearson AT, et al. Highly accurate response prediction in high-risk early breast cancer patients using a biophysical simulation platform. Breast Cancer Res Treat. (2022) 196:57–66. doi: 10.1007/s10549-022-06722-0
204. Peterson JR, Cole JA, Pfeiffer JR, Norris GH, Zhang Y, Lopez-Ramos D, et al. Novel computational biology modeling system can accurately forecast response to neoadjuvant therapy in early breast cancer. Breast Cancer Res BCR. (2023) 25:54. doi: 10.1186/s13058-023-01654-z
205. Holford NH, Kimko HC, Monteleone JP, and Peck CC. Simulation of clinical trials. Annu Rev Pharmacol Toxicol. (2000) 40:209–34. doi: 10.1146/annurev.pharmtox.40.1.209
206. Madabushi R, Seo P, Zhao L, Tegenge M, and Zhu H. Review: role of model-informed drug development approaches in the lifecycle of drug development and regulatory decision-making. Pharm Res. (2022) 39:1669–80. doi: 10.1007/s11095-022-03288-w
207. Newick K, O’Brien S, Moon E, and Albelda SM. CAR T cell therapy for solid tumors. Annu Rev Med. (2017) 68:139–52. doi: 10.1146/annurev-med-062315-120245
208. Ma S, Li X, Wang X, Cheng L, Li Z, Zhang C, et al. Current progress in CAR-T cell therapy for solid tumors. Int J Biol Sci. (2019) 15:2548–60. doi: 10.7150/ijbs.34213
209. Lo A, Wang LCS, Scholler J, Monslow J, Avery D, Newick K, et al. Tumor-promoting desmoplasia is disrupted by depleting FAP-expressing stromal cells. Cancer Res. (2015) 75:2800–10. doi: 10.1158/0008-5472.CAN-14-3041
210. Walker C, Mojares E, and Del Río Hernández A. Role of extracellular matrix in development and cancer progression. Int J Mol Sci. (2018) 19:3028. doi: 10.3390/ijms19103028
211. Gobert M, Treilleux I, Bendriss-Vermare N, Bachelot T, Goddard-Leon S, Arfi V, et al. Regulatory T cells recruited through CCL22/CCR4 are selectively activated in lymphoid infiltrates surrounding primary breast tumors and lead to an adverse clinical outcome. Cancer Res. (2009) 69:2000–9. doi: 10.1158/0008-5472.CAN-08-2360
212. Aparicio C, Belver M, Enríquez L, Espeso F, Núñez L, Sánchez A, et al. Cell therapy for colorectal cancer: the promise of chimeric antigen receptor (CAR)-T cells. Int J Mol Sci. (2021) 22:11781. doi: 10.3390/ijms222111781
213. Bardhan K, Anagnostou T, and Boussiotis VA. The PD1:PD-L1/2 pathway from discovery to clinical implementation. Front Immunol. (2016) 7:550. doi: 10.3389/fimmu.2016.00550
214. Li F, Wang Y, Chen D, and Du Y. Nanoparticle-based immunotherapy for reversing T-cell exhaustion. Int J Mol Sci. (2024) 25:1396. doi: 10.3390/ijms25031396
215. El-Baz N, Nunn BM, Bates PJ, and O’Toole MG. The impact of PEGylation on cellular uptake and in vivo biodistribution of gold nanoparticle MRI contrast agents. Bioengineering. (2022) 9:766. doi: 10.3390/bioengineering9120766
216. Anselmo AC and Mitragotri S. Nanoparticles in the clinic: An update. Bioeng Transl Med. (2019) 4:e10143. doi: 10.1002/btm2.10143
217. Cheng YH, He C, Riviere JE, Monteiro-Riviere NA, and Lin Z. Meta-analysis of nanoparticle delivery to tumors using a physiologically based pharmacokinetic modeling and simulation approach. ACS Nano. (2020) 14:3075–95. doi: 10.1021/acsnano.9b08142
218. Chen Q, Yuan L, Chou WC, Cheng YH, He C, Monteiro-Riviere NA, et al. Meta-analysis of nanoparticle distribution in tumors and major organs in tumor-bearing mice. ACS Nano. (2023) 17:19810–31. doi: 10.1021/acsnano.3c04037
219. Price LSL, Stern ST, Deal AM, Kabanov AV, and Zamboni WC. A reanalysis of nanoparticle tumor delivery using classical pharmacokinetic metrics. Sci Adv. (2020) 6:eaay9249. doi: 10.1126/sciadv.aay9249
220. Wilhelm S, Tavares AJ, Dai Q, Ohta S, Audet J, Dvorak HF, et al. Analysis of nanoparticle delivery to tumours. Nat Rev Mater. (2016) 1:1–12. doi: 10.1038/natrevmats.2016.14
221. Dogra P, Butner JD, Ruiz Ramírez J, Chuang Y, Noureddine A, Jeffrey Brinker C, et al. A mathematical model to predict nanomedicine pharmacokinetics and tumor delivery. Comput Struct Biotechnol J. (2020) 18:518–31. doi: 10.1016/j.csbj.2020.02.014
222. Mi K, Chou WC, Chen Q, Yuan L, Kamineni VN, Kuchimanchi Y, et al. Predicting tissue distribution and tumor delivery of nanoparticles in mice using machine learning models. J Controlled Release. (2024) 374:219–29. doi: 10.1016/j.jconrel.2024.08.015
223. Yousfan A, Al Rahwanji MJ, Hanano A, and Al-Obaidi H. A comprehensive study on nanoparticle drug delivery to the brain: application of machine learning techniques. Mol Pharm. (2024) 21:333–45. doi: 10.1021/acs.molpharmaceut.3c00880
224. Zhou L, Yi W, Zhang Z, Shan X, Zhao Z, Sun X, et al. STING agonist-boosted mRNA immunization via intelligent design of nanovaccines for enhancing cancer immunotherapy. Natl Sci Rev. (2023) 10:nwad214. doi: 10.1093/nsr/nwad214
225. Hwang H, Jeon H, Yeo N, and Baek D. Big data and deep learning for RNA biology. Exp Mol Med. (2024) 56:1293–321. doi: 10.1038/s12276-024-01243-w
226. Akhtar Y, Ahmad S, Khalid F, Junjua M ud D, Aryanfar Y, Hendy AS, et al. Machine learning- a new paradigm in nanoparticle-mediated drug delivery to cancerous tissues through the human cardiovascular system enhanced by magnetic field. Sci Rep. (2024) 14:22048. doi: 10.1038/s41598-024-72629-z
227. Tang X, Yang Y, Zheng M, Yin T, Huang G, Lai Z, et al. Magnetic–acoustic sequentially actuated CAR T cell microrobots for precision navigation and in situ antitumor immunoactivation. Adv Mater. (2023) 35:2211509. doi: 10.1002/adma.202211509
228. Pfister F, Carnell LR, Löffler L, Boosz P, Schaft N, Dörrie J, et al. Loading of CAR-T cells with magnetic nanoparticles for controlled targeting suppresses inflammatory cytokine release and switches tumor cell death mechanism. MedComm. (2025) 6:e70039. doi: 10.1002/mco2.70039
229. Short L, Holt RA, Cullis PR, and Evgin L. Direct in vivo CAR T cell engineering. Trends Pharmacol Sci. (2024) 45:406–18. doi: 10.1016/j.tips.2024.03.004
230. Kheirolomoom A, Kare AJ, Ingham ES, Paulmurugan R, Robinson ER, Baikoghli M, et al. In situ T-cell transfection by anti-CD3-conjugated lipid nanoparticles leads to T-cell activation, migration, and phenotypic shift. Biomaterials. (2022) 281:121339. doi: 10.1016/j.biomaterials.2021.121339
231. Michels A, Ho N, and Buchholz CJ. Precision medicine: In vivo CAR therapy as a showcase for receptor-targeted vector platforms. Mol Ther J Am Soc Gene Ther. (2022) 30:2401–15. doi: 10.1016/j.ymthe.2022.05.018
232. Weber EW, Lynn RC, Sotillo E, Lattin J, Xu P, and Mackall CL. Pharmacologic control of CAR-T cell function using dasatinib. Blood Adv. (2019) 3:711–7. doi: 10.1182/bloodadvances.2018028720
233. McHugh MD, Park J, Uhrich R, Gao W, Horwitz DA, and Fahmy TM. Paracrine co-delivery of TGF-β and IL-2 using CD4-targeted nanoparticles for induction and maintenance of regulatory T cells. Biomaterials. (2015) 59:172–81. doi: 10.1016/j.biomaterials.2015.04.003
234. Eskandari SK, Sulkaj I, Melo MB, Li N, Allos H, Alhaddad JB, et al. Regulatory T cells engineered with TCR signaling-responsive IL-2 nanogels suppress alloimmunity in sites of antigen encounter. Sci Transl Med. (2020) 12:eaaw4744. doi: 10.1126/scitranslmed.aaw4744
235. Koh DM, Papanikolaou N, Bick U, Illing R, Kahn CE, Kalpathi-Cramer J, et al. Artificial intelligence and machine learning in cancer imaging. Commun Med. (2022) 2:1–14. doi: 10.1038/s43856-022-00199-0
236. Israel LL, Galstyan A, Holler E, and Ljubimova JY. Magnetic iron oxide nanoparticles for imaging, targeting and treatment of primary and metastatic tumors of the brain. J Control Release Off J Control Release Soc. (2020) 320:45–62. doi: 10.1016/j.jconrel.2020.01.009
237. Li J, Cha R, Zhang Y, Guo H, Long K, Gao P, et al. Iron oxide nanoparticles for targeted imaging of liver tumors with ultralow hepatotoxicity. J Mater Chem B. (2018) 6:6413–23. doi: 10.1039/C8TB01657G
238. Luo D, Wang X, Burda C, and Basilion JP. Recent development of gold nanoparticles as contrast agents for cancer diagnosis. Cancers. (2021) 13:1825. doi: 10.3390/cancers13081825
239. Aghighi M, Pisani LJ, Sun Z, Klenk C, Madnawat H, Fineman SL, et al. Speeding up PET/MR for cancer staging of children and young adults. Eur Radiol. (2016) 26:4239–48. doi: 10.1007/s00330-016-4332-4
240. Oumano M and Yu H. A deep learning approach to gold nanoparticle quantification in computed tomography. Phys Med PM Int J Devoted Appl Phys Med Biol Off J Ital Assoc BioMed Phys AIFB. (2021) 87:83–9. doi: 10.1016/j.ejmp.2021.05.036
241. Fridberg G, Horn G, Globerson Levin A, Benisty D, Kay S, Glait-Santar C, et al. The clinical significance of circulating lymphocytes morphology in diffuse large B-cell lymphoma as determined by a novel, highly sensitive microscopy. Cancers. (2023) 15:5611. doi: 10.3390/cancers15235611
242. Zhang R, Han X, Lei Z, Jiang C, Gul I, Hu Q, et al. RCMNet: A deep learning model assists CAR-T therapy for leukemia. Comput Biol Med. (2022) 150:106084. doi: 10.1016/j.compbiomed.2022.106084
243. Islam S, Elmekki H, Elsebai A, Bentahar J, Drawel N, Rjoub G, et al. A comprehensive survey on applications of transformers for deep learning tasks. Expert Syst Appl. (2024) 241:122666. doi: 10.1016/j.eswa.2023.122666
244. Chen KI, Li BR, and Chen YT. Silicon nanowire field-effect transistor-based biosensors for biomedical diagnosis and cellular recording investigation. Nano Today. (2011) 6:131–54. doi: 10.1016/j.nantod.2011.02.001
245. Nguyen-Le TA, Bartsch T, Wodtke R, Brandt F, Arndt C, Feldmann A, et al. Nanosensors in clinical development of CAR-T cell immunotherapy. Biosens Bioelectron. (2022) 206:114124. doi: 10.1016/j.bios.2022.114124
246. Ayadi N, Lale A, Hajji B, Launay J, and Temple-Boyer P. Machine learning-based modeling of pH-sensitive silicon nanowire (SiNW) for ion sensitive field effect transistor (ISFET). Sensors. (2024) 24:8091. doi: 10.3390/s24248091
247. Ahmadi M, Ayyoubzadeh SM, and Ghorbani-Bidkorpeh F. Toxicity prediction of nanoparticles using machine learning approaches. Toxicology. (2024) 501:153697. doi: 10.1016/j.tox.2023.153697
248. Gray M, Samala R, Liu Q, Skiles D, Xu J, Tong W, et al. Measurement and mitigation of bias in artificial intelligence: A narrative literature review for regulatory science. Clin Pharmacol Ther. (2024) 115:687–97. doi: 10.1002/cpt.3117
249. Sadeghi Z, Alizadehsani R, Cifci MA, Kausar S, Rehman R, Mahanta P, et al. A review of Explainable Artificial Intelligence in healthcare. Comput Electr Eng. (2024) 118:109370. doi: 10.1016/j.compeleceng.2024.109370
250. Qiu Y and Hu Z. Data governance and open sharing in the fields of life sciences and medicine: A bibliometric analysis. Digit Health. (2025) 11:20552076251320302. doi: 10.1177/20552076251320302
251. Capella MP and Esfahani K. A review of practice-changing therapies in oncology in the era of personalized medicine. Curr Oncol. (2024) 31:1913–9. doi: 10.3390/curroncol31040143
252. Nasarian E, Alizadehsani R, Acharya UR, and Tsui KL. Designing interpretable ML system to enhance trust in healthcare: A systematic review to proposed responsible clinician-AI-collaboration framework. Inf Fusion. (2024) 108:102412. doi: 10.1016/j.inffus.2024.102412
253. Souto EB, Blanco-Llamero C, Krambeck K, Kiran NS, Yashaswini C, Postwala H, et al. Regulatory insights into nanomedicine and gene vaccine innovation: Safety assessment, challenges, and regulatory perspectives. Acta Biomater. (2024) 180:1–17. doi: 10.1016/j.actbio.2024.04.010
254. Palaniappan K, Lin EYT, Vogel S, and Lim JCW. Gaps in the global regulatory frameworks for the use of artificial intelligence (AI) in the healthcare services sector and key recommendations. Healthcare. (2024) 12:1730. doi: 10.3390/healthcare12171730
255. Khawar MB, Afzal A, Si Y, and Sun H. Steering the course of CAR T cell therapy with lipid nanoparticles. J Nanobiotechnology. (2024) 22:380. doi: 10.1186/s12951-024-02630-1
256. Becker J. Logistics for Cell and Gene Therapies: Challenges and Strategies for Scaling Personalized Medicine. Rochester, NY: Social Science Research Network (2025). Available online at: https://papers.ssrn.com/abstract=5270904 (Accessed March 27, 2025).
257. Wang Y, Barrett A, and Hu Q. Nanotechnology-assisted CAR-T-cell therapy for tumor treatment. WIREs Nanomedicine Nanobiotechnology. (2024) 16:e2005. doi: 10.1002/wnan.2005
258. Prazeres PHDM, Ferreira H, Costa PAC, da Silva W, Alves MT, Padilla M, et al. Delivery of plasmid DNA by ionizable lipid nanoparticles to induce CAR expression in T cells. Int J Nanomedicine. (2023) 18:5891–904. doi: 10.2147/IJN.S424723
259. Loukanov A, Arahangelova V, Emin S, and Filipov C. Engineering of functional nanosnowflakes from gold nanocarriers capped with amino-modified DNA oligonucleotides. Microsc Res Tech. (2023) 86:1169–76. doi: 10.1002/jemt.24390
260. Loukanov A, Kamasawa N, Danev R, Shigemoto R, and Nagayama K. Immunolocalization of multiple membrane proteins on a carbon replica with STEM and EDX. Ultramicroscopy. (2010) 110:366–74. doi: 10.1016/j.ultramic.2010.01.016
Keywords: CAR-T therapy, nanotechnology, artificial intelligence, machine learning, deep learning, immunotherapy, manufacturing, personalized medicine
Citation: Baena JC, Victoria JS, Toro-Pedroza A, Aragón CC, Ortiz-Guzman J, Garcia-Robledo JE, Torres D, Rios-Serna LJ, Albornoz L, Rosales JD, Cañas CA, Adolfo Cruz-Suarez G, Osorio FO, Fleitas T, Laponogov I, Loukanov A and Veselkov K (2025) Smart CAR-T Nanosymbionts: archetypes and proto-models. Front. Immunol. 16:1635159. doi: 10.3389/fimmu.2025.1635159
Received: 26 May 2025; Accepted: 01 July 2025;
Published: 12 August 2025.
Edited by:
Rohit Kumar Tiwari, Sharda University, IndiaReviewed by:
Dr. Adil Husain, Babu Banarasi Das University, IndiaTabrez Faruqui, Era University, India
Copyright © 2025 Baena, Victoria, Toro-Pedroza, Aragón, Ortiz-Guzman, Garcia-Robledo, Torres, Rios-Serna, Albornoz, Rosales, Cañas, Adolfo Cruz-Suarez, Osorio, Fleitas, Laponogov, Loukanov and Veselkov. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan C. Baena, anVhbi5iYWVuYUBmdmwub3JnLmNvbQ==