 Raquel Güell-Alonso
Raquel Güell-Alonso Raquel Cabrera-Pérez1,2*
Raquel Cabrera-Pérez1,2* Joaquim Vives
Joaquim Vives- 1Banc de Sang i Teixits, Barcelona, Spain
- 2Vall d’Hebron Research Institute (VHIR), Universitat Autònoma de Barcelona (UAB), Barcelona, Spain
- 3Department of Medicine, Universitat Autònoma de Barcelona (UAB), Barcelona, Spain
The ongoing shortage of cell, tissue, and organ donors has led to prioritizing clinical urgency over optimal immune matching in transplantation, often at the cost of increased reliance on immunosuppressive regimens and their associated adverse effects. Recent advances in the use of Substances of Human Origin (SoHOs), xenotransplantation and emerging cell-, gene-, and tissue-based therapies have enabled the development of tailored cellular therapeutics to enhance engraftment, long-term function, and immunological compatibility. Within this evolving context, artificial intelligence is also increasingly contributing to improve donor–recipient matching through predictive analytics and integrative data modeling, assisting on immune tolerance and the durable integration of transplanted cells into host tissues. In this review, we revisit foundational concepts of immunocompatibility, examine current clinical criteria in organ transplantation, and critically explore the shifting paradigms of donor–recipient matching in the era of personalized medicine. These advances have the potential to redefine clinical strategies in transplantation and regenerative care while ensuring patient access and sustainability.
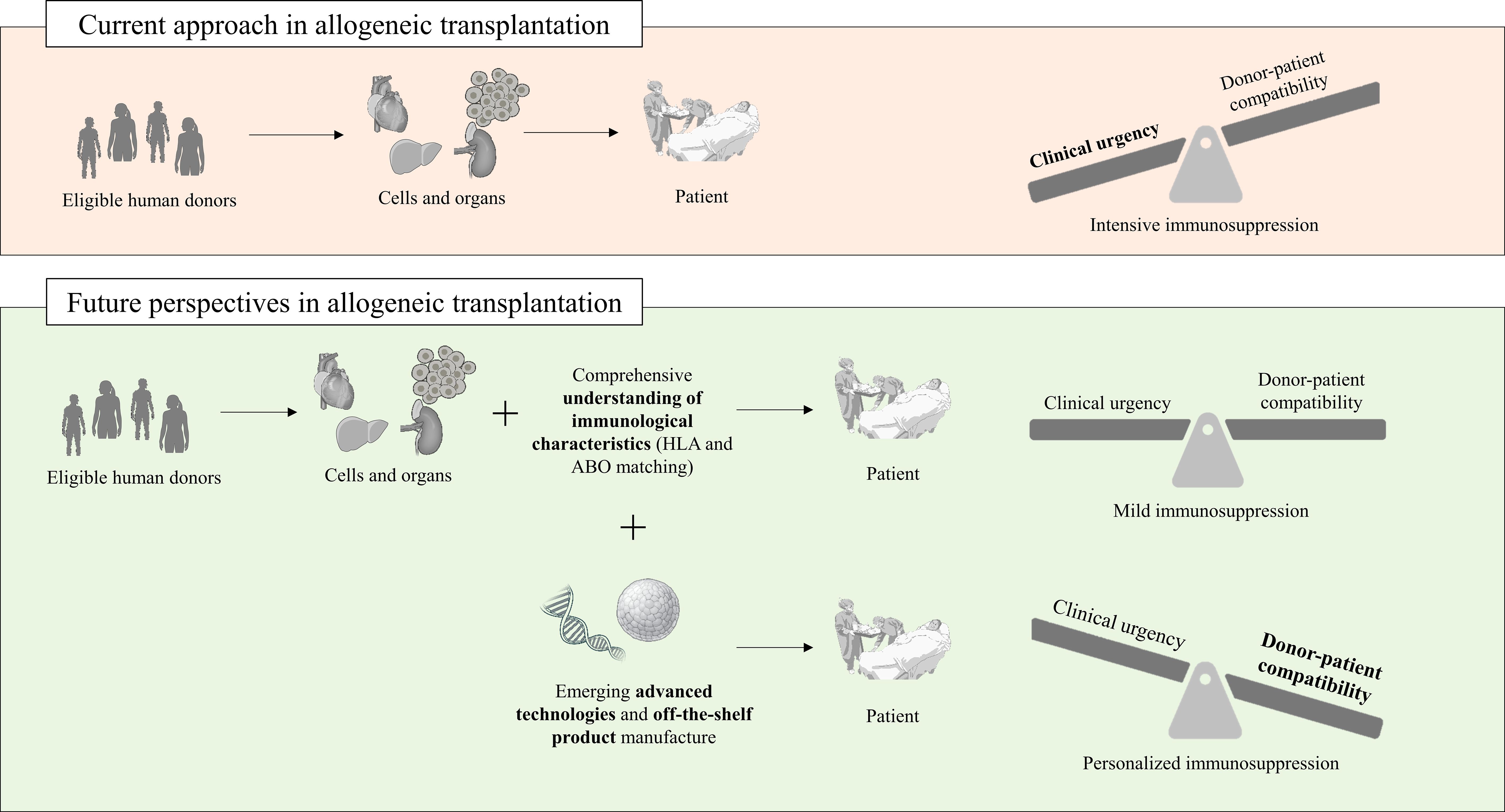
Graphical Abstract. Evolving paradigms in allogeneic transplantation. Part of the figure was designed using images from the NIH BIOART source (https://bioart.niaid.nih.gov/).
1 Introduction
Nowadays, the availability of donated cells, tissues, and organs is still insufficient to meet clinical needs, despite the enormous efforts made at many levels (medical, ethical, regulatory, logistical, health systems, and donation). Such persistent organ, stem cell, and tissue shortages necessitate innovative strategies aimed at the expansion of the donor pool by exploring alternatives while ensuring patient safety. Post-transplant complications such as graft-versus-host disease (GvHD) in hematopoietic stem cell transplantation (HSCT), chronic rejection, donor-specific alloantibody (DSA) formation, and sensitization continue to challenge the field, underscoring the need for ongoing investigation into the critical impact of compatibility issues between donor and recipient. This challenge can be addressed by a combination of emerging therapies and computational tools involving a deeper understanding of the thresholds at which donor-patient disparity can be deemed acceptable, with improved immunosuppressive approaches, thus offering new possibilities for increasing transplantation rates and advancing the frontiers of personalized medicine (1–4).
Herein we aim to introduce the major actors in donor-patient compatibility, understand their role in graft survival and tolerance, and discuss promising strategies aimed at a more accessible, equitable, customized, and sustainable transplantation framework. For clarity, Table 1 includes definitions of terminology used in this article.

Table 1. Definitions.
2 Actors in graft rejection
The immunological rejection of transplanted cells, tissues, and organs is orchestrated by a complex interplay of cellular and humoral immune responses, primarily governed by recognition of non-self antigens.
The major histocompatibility complex (MHC) system, known as the human leukocyte antigen (HLA) in humans, is central to this process and represents the most polymorphic region of the human genome (Figure 1). This high degree of polymorphism makes each individual almost immunogenetically unique, critically determining graft tolerance (5). Classical MHC class I (HLA-A, -B, -C) and class II (HLA-DP, -DQ, -DR) molecules both present alloantigens to recipient T lymphocytes, initiating direct or indirect allorecognition pathways that trigger effector immune responses and contribute to chronic rejection, reduced graft survival, and severe complications. Beyond the classical HLA loci, increasing evidence highlights the role of non-classical MHC-I molecules such as i) HLA-G, which exerts immunomodulatory effects and is implicated in maternal-fetal tolerance; and ii) HLA-E, which interacts with innate and adaptive immune cells leading to both protective and detrimental effects on allograft survival (6–9). Similarly, minor histocompatibility antigens (mHAgs), although less immunogenic than HLA molecules, can also trigger GvHD after HSCT and contribute to late rejection events.
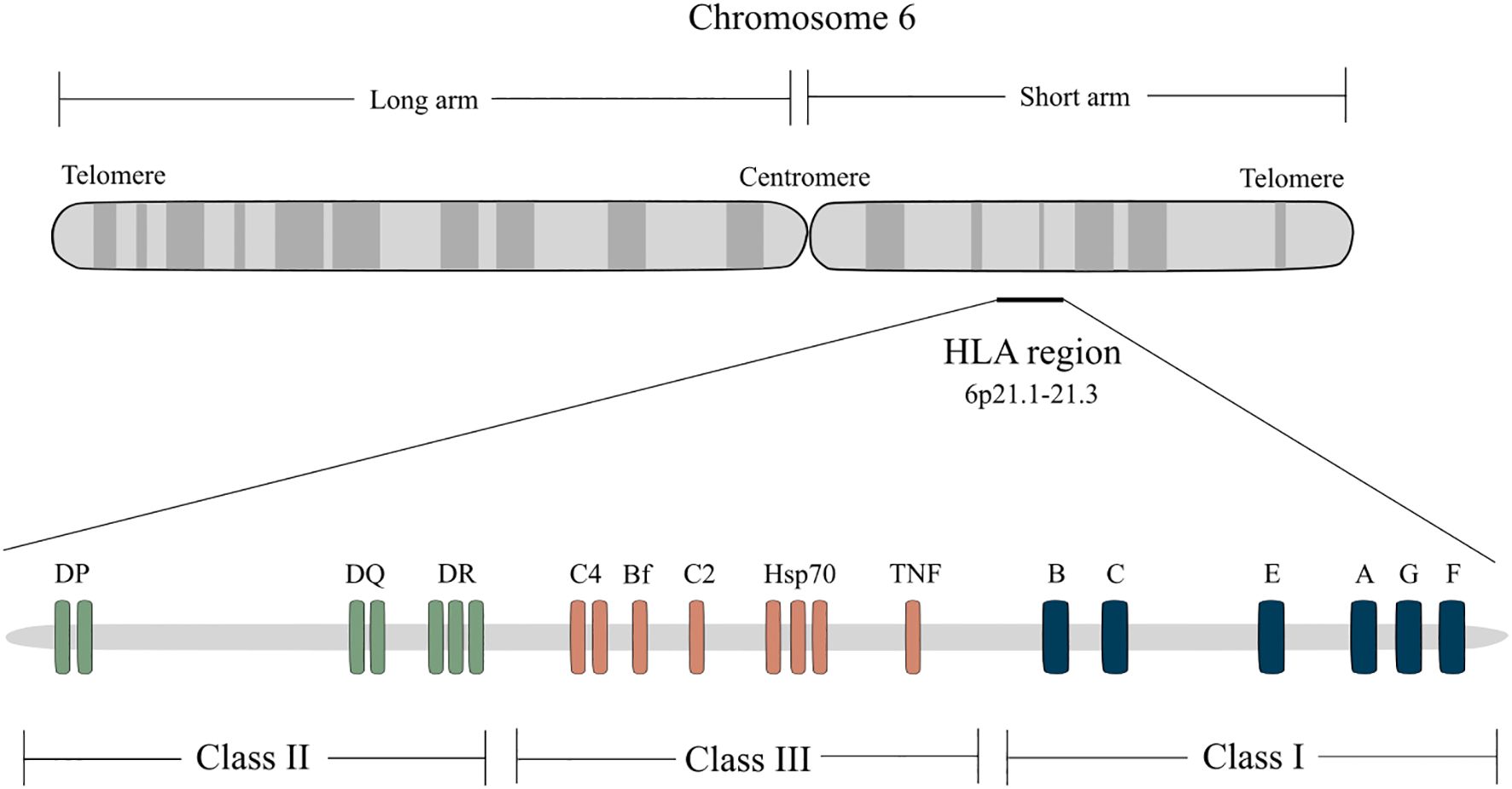
Figure 1. Classical and non-classical HLA loci. The human major histocompatibility complex (MHC) is called the HLA (human leukocyte antigen) and is located on the short arm of chromosome 6 (6p21.1-21.3). The class I region contains the classical HLA-A, HLA-B, and HLA-C genes that encode the heavy chains of class I molecules, which present antigens to CD8+effector T cells, and the non-classical HLA-E, HLA-F, and HLA-G, which interact with NK cells. The class II region consists of a series of subregions, namely DR, DQ, and DP, each containing A and B genes encoding α and β chains, respectively. Class II reactive T cells are usually CD4+ helper cells. HLA class I molecules are expressed on the surface of almost all nucleated cells while class II molecules are expressed only on B lymphocytes, APCs (monocytes, macrophages, and dendritic cells), and activated T lymphocytes. The class III region does not encode HLA molecules but other important genes, including C’ (complement genes), HSP (heat shock protein) and TNF (tumor necrosis factor).
Traditional HLA matching has largely focused on major immunogenic HLA loci, namely HLA-A, -B, and -DR. Matching at the HLA-DR locus has been shown to have the most pronounced effect on allograft survival and long-term graft function (10). However, mismatches in HLA-DP and -DQ are also relevant, especially in highly sensitized patients or those undergoing multiple transplants.
The ABO blood group also represents another key immunological barrier, particularly in solid organ transplantation, where naturally occurring antibodies against non-self ABO antigens can mediate hyperacute rejection and graft dysfunction in incompatible settings. The ABO gene encodes for a glycosyltransferase that modifies oligosaccharides on the surface of the red blood cells (RBC), vascular endothelium, and other tissues (11). Variations in the sequence of ABO are responsible for the major blood group phenotypes (A, B, AB, and O). Interestingly, more than 300 RBC antigens belonging to 36 blood group systems have been officially reported in humans by the International Society of Blood Transfusion (ISBT) so far (12). ABO-incompatible transplantation is feasible but requires desensitization and intensification of immunosuppression to prevent allograft rejection (11).
Additionally, a number of immune cell types participate in graft acceptance or failure. Antigen-presenting cells (APCs), including dendritic cells, macrophages, and B cells, play an initiating role by processing and presenting alloantigens to naïve T cells, thus bridging innate and adaptive immunity. Effector CD8+ cytotoxic T cells and CD4+ helper T cells, along with natural killer (NK) cells, plasma cells, and memory B cells, perpetuate graft rejection via direct cytotoxicity, cytokine release, and alloantibody production (13).
Finally, the interplay between these actors is further shaped by the inflammatory milieu, the immune status of the recipient (e.g., pre-sensitization), and the immunogenicity of the graft itself, which are all important factors in innovative cell-based therapies, tissue-engineering, and xenogeneic applications. As transplantation strategies evolve toward precision immunomodulation, a better understanding of these actors at the cellular, molecular, and epitope-specific levels becomes imperative to predict and prevent rejection, tailor immunosuppression and, ultimately, enhance long-term graft survival.
3 Compatibility in transplantation
Stringent HLA matching is often balanced against the urgency of transplantation and donor availability. The entire lifespan of an organ transplant recipient relies on efforts to maintain the delicate balance between the risk of rejection on the one hand, and on the other, the risk of infection and malignancy later on. Although the current intensive immunosuppressive protocols reduce the occurrence of severe acute rejections (ARs) to a minimum, patients with functioning organs may later die of severe infections or malignancies instead. In the following sections, we present current evidence on the minimal HLA donor-recipient match requirements as well as the influence of ABO blood types for successful outcomes across major organs and tissues (summarized in Table 2 and Figure 2).
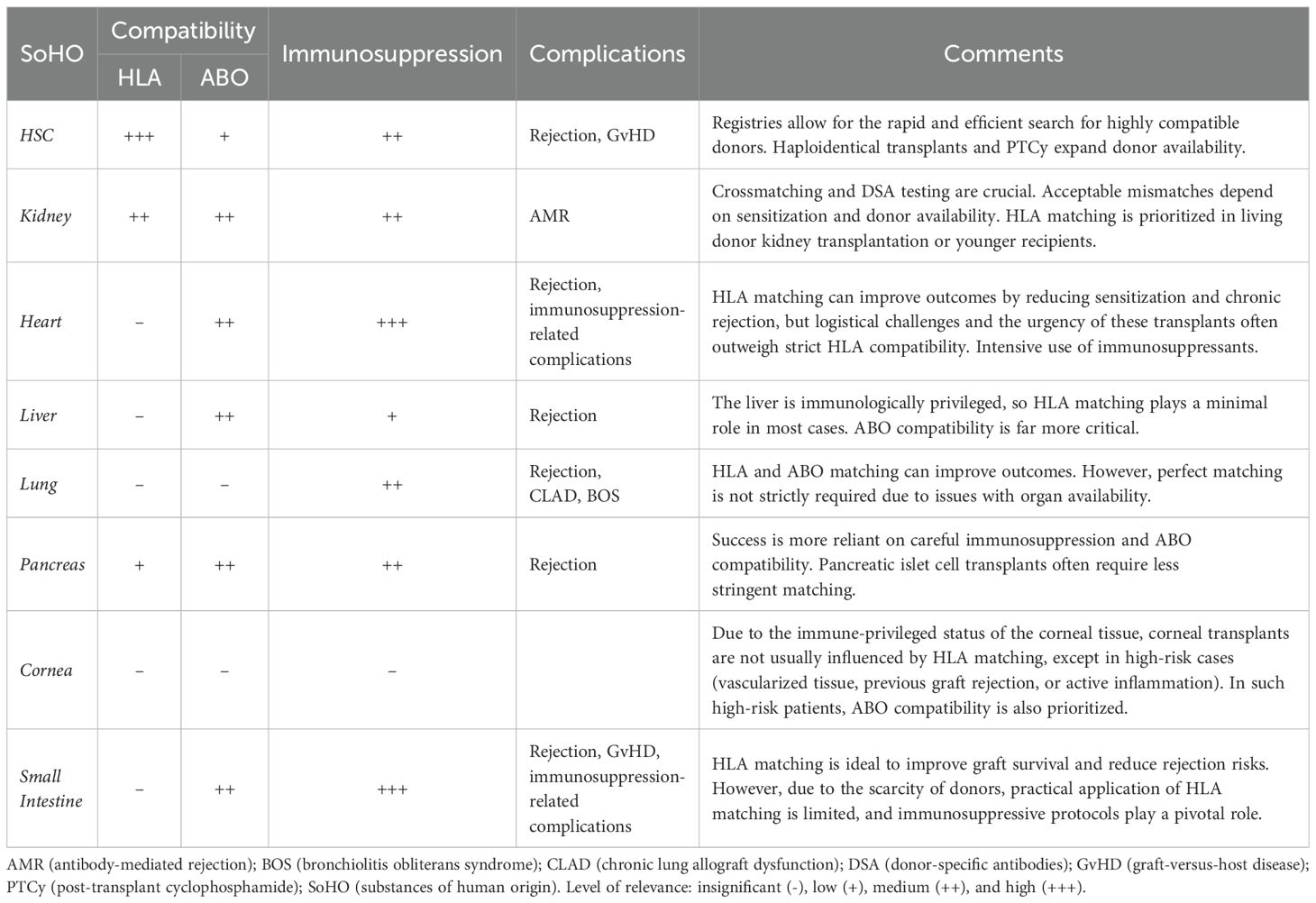
Table 2. Current criteria on HLA and ABO compatibility considerations in major organ transplantation. .
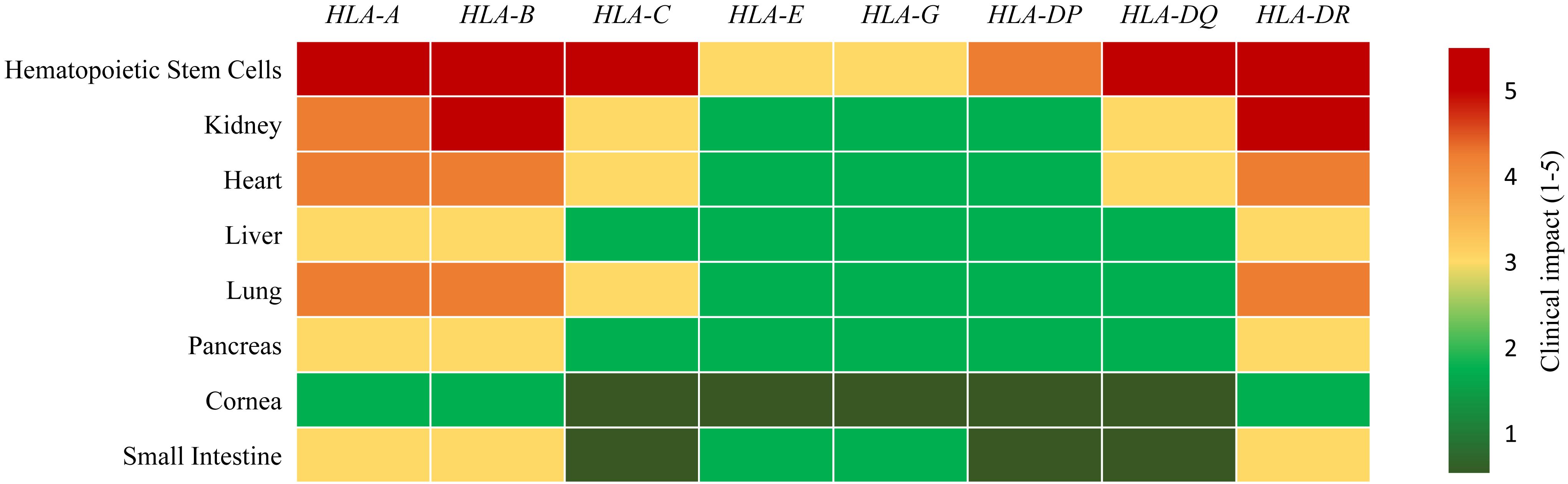
Figure 2. Relevance of donor-recipient HLA loci compatibility in organ transplant success. A higher score (5, shown in red) indicates that matching at the given HLA locus is critically important for transplant success, whereas a lower score (1, shown in dark green) indicates lower clinical impact in current transplant settings in combination with immunosuppressive agents.
3.1 Hematopoietic stem cells
HSCT is indicated for hematologic malignancies, non-malignant blood disorders, primary immunodeficiencies, severe autoimmune diseases, and congenital metabolic disorders, serving as a curative or life-extending therapy by replacing dysfunctional hematopoietic and immune systems (14). In HSCT, HLA matching (especially at HLA-A, -B, -C, and -DR) is paramount to prevent graft failure, GvHD, and other complications. A 10/10 match (for both alleles of HLA-A, -B, -C, -DR, and -DQ) is preferred for unrelated donor transplants, while mismatches at a single locus (e.g., 9/10) are acceptable but increase the risk of GvHD. It is worth noting that having national and international registries enables highly compatible donors to be identified rapidly and efficiently. Patients lacking HLA-identical donors can be treated with haploidentical transplants that allow the use of HSC from an allogeneic half-matched donor (5/10 match), who is typically a family member. However, they often require additional interventions to mitigate risks, such as T-cell depletion or post-transplant immunomodulation. HLA-C and HLA-DP matching has also been shown to improve outcomes in HSCT (15).
3.2 Kidney
Kidney transplantation is indicated for patients with end-stage renal disease (ESRD) or advanced chronic kidney disease (CKD) who present irreversible loss of kidney function, requiring renal replacement therapy to improve survival and quality of life. Cross-matching and DSA testing are crucial adjuncts to HLA matching for kidney transplants. Acceptable mismatches depend on sensitization and availability of donors. HLA-A, -B and -DR matching has a direct impact on long-term graft survival, while HLA-DR mismatches tend to be the most immunogenic and impactful. HLA-B mismatches also carry a strong risk due to high polymorphism. HLA-A mismatches are important but generally considered less immunogenic than -DR or -B. Patients with higher HLA matches require less immunosuppression and have a reduced risk of AMR. HLA matching is often prioritized in living donor kidney transplantation or for younger recipients where longevity of the graft is critical (16).
Interestingly, ABO antigens are expressed on kidney endothelial and epithelial surfaces, and their presence on allograft tissue can lead to higher short-term hyperacute or acute AMR, although with good management, long-term outcomes can approach those of compatible transplants. It is worth noting that blood group B kidney recipients experience longer waiting times than other ABO groups prior to transplantation (17). The prevalence of group B is higher in African Americans and Asian Americans and thus these ethnic minorities are the most affected populations within the group B cohort (18).
Apart from HLA/ABO matching, the effect of other factors on post-transplant outcomes, including viral serology, age and size mismatch, mismatch in other HLA antigens (e.g. HLA-C and HLA-DQ), and eplet matching, has become increasingly recognized. Of note, kidney transplant recipients who experience rejection can return to dialysis, a situation that is not paralleled in other transplantation settings.
3.3 Heart
Heart transplantation is indicated for patients with end-stage heart failure due to conditions such as dilated or ischemic cardiomyopathy, congenital heart disease, or refractory ventricular arrhythmias, who have severe symptoms despite medical, surgical, or device-based therapies and meet criteria for irreversible hemodynamic compromise. Although, where feasible, HLA-A, -B, and -DR matching is considered, primarily to reduce the risk of sensitization in re-transplantation cases, no specific HLA match requirement is universally mandatory given that transplantation may not be delayed due to clinical urgency. Consequently, immunosuppression protocols are heavily relied upon in heart transplants, much more than in kidney transplantation, since graft rejection is usually fatal (19). This may explain why no further decline in the organ survival rate was found as the number of HLA mismatches increased from three to six (19, 20). As a consequence of intensive immunosuppressive treatment, high rates of malignant lymphomas are reported in heart transplant patients (21).
Transplantation of hearts from ABO-incompatible donors is contraindicated because of the risk of hyperacute rejection. This contraindication may not apply to infants younger than 2 years, who do not yet produce antibodies against T-cell-independent antigens. However, use of donors with minor ABO mismatches is also a safe and feasible option in older children and adult patients (22–24).
3.4 Liver
Liver transplantation is indicated for patients with end-stage liver disease, acute liver failure, or metabolic disorders affecting hepatic function due to conditions such as cirrhosis, hepatocellular carcinoma within transplant criteria, or genetic liver diseases, when no alternative treatment can prevent life-threatening complications or hepatic decompensation. In liver transplantation, no stringent HLA matching is required since the liver is considered immunologically privileged compared to other organs due to its inherent tolerogenic properties. Of note, ABO compatibility is more critical than HLA matching for liver transplants (25–27).
3.5 Lung
Lung transplantation is indicated for patients with end-stage pulmonary disease, such as chronic obstructive pulmonary disease (COPD), idiopathic pulmonary fibrosis, cystic fibrosis, or pulmonary arterial hypertension, who have severe respiratory failure and reduced life expectancy. Matching at HLA-A, -B, and -DR may improve long-term outcomes, particularly chronic lung allograft dysfunction (CLAD) and bronchiolitis obliterans syndrome (BOS). However, issues related to organ availability mean that perfect matching is not strictly required. High levels of pre-transplant sensitization increase the risk of rejection. Opelz and collaborators analyzed a large series of lung transplant procedures followed up on for 5 years, demonstrating that a high number of HLA mismatches or, surprisingly, zero mismatches, unfavorably impacts graft survival rates (28). Recently, HLA-C mismatches have been described as beneficial in lung transplantation due to a reduced incidence of CLAD in recipients with HLA-C mismatching (29).
3.6 Pancreas and pancreatic islets
Pancreas and pancreatic islet transplantation are indicated for patients with type 1 diabetes mellitus experiencing severe glycemic instability, recurrent hypoglycemia unawareness syndrome, or secondary complications, particularly when simultaneous kidney transplantation is required due to ESRD or when intensive insulin therapy fails to achieve metabolic control. HLA-A, -B, and -DR matching is ideal in pancreas transplantation but is not always feasible. According to the results published by Rudolph et al., the risk of acute rejection increases significantly at four or more mismatches, especially when they involve the HLA-B or -DR locus (30). In contrast, recent results suggest that HLA matching is not associated with improved graft survival or a reduction in acute rejection (31).
Interestingly, success in pancreas transplantation is more reliant on careful immunosuppression and ABO compatibility. Despite this, there have been successful cases of ABO-incompatible pancreas transplantation, particularly in simultaneous pancreas-kidney (SPK) procedures. These cases usually involve intensive immunosuppressive regimens and pre-transplant antibody removal strategies (e.g., plasmapheresis, rituximab) to lower the risk of rejection.
Pancreatic islet cell transplants often require less stringent matching due to i) advances in immunosuppressive options, and ii) the infusion of a small amount of islets into the liver via the portal vein. In this context, a recent study suggests that recipients with HLA-DR matching, excluding diabetogenic HLA-DR3 and -DR4 alleles, maintained higher rates of insulin independence 5 years after transplantation compared to those with mismatching (32). Of note, the purity of islet preparations has a direct impact on rejection due to contamination with pancreatic exocrine tissue components and acinar tissue expressing ABH antigens (33). Additionally, certain HLA-DQ antigens have been associated with improved graft survival (34).
3.7 Cornea
Corneal transplantation, also known as keratoplasty, can be complete (penetrating keratoplasty) or partial (endothelial keratoplasty) and is indicated for patients with corneal opacification, thinning, or structural damage due to conditions such as keratoconus, corneal dystrophies, infections, trauma, or scarring, when visual rehabilitation or ocular integrity cannot be achieved through other interventions. Although no HLA matching is typically required for low-risk corneal transplants due to the immune-privileged status of the corneal tissue (characterized by avascularity, low expression of HLA antigens, and presence of immunomodulatory molecules), HLA-A, -B, and -DR matching can reduce the risk of rejection in high-risk cases (e.g., vascularized tissue, previous graft rejection, or active inflammation) (35–37). In such high-risk patients, ABO compatibility is also prioritized.
3.8 Small intestine
Small bowel transplantation, which is a relatively infrequent procedure, is indicated for patients with irreversible intestinal failure who are unable to maintain adequate nutrition and hydration through parenteral nutrition due to life-threatening complications such as liver failure, recurrent sepsis, or loss of central venous access. The small intestine is highly immunogenic and has one of the highest rates of acute rejection among all solid organ transplants (38). HLA-A, HLA-B, and, particularly, HLA-DR matching is ideal to improve graft survival and reduce the risk of rejection (39). However, due to the paucity of donors, practical application of HLA matching is limited, and immunosuppressive protocols play a pivotal role (38). These factors place patients at increased risk of developing immunosuppression-related complications, namely cellular rejection and AMR, infection, kidney disease, lymphoproliferative disorders, and GvHD.
ABO compatibility is usually mandatory, except for pediatric patients under 1 year old. Nevertheless, ABO-incompatible transplants could be feasible with the appropriate management of blood type antibodies and the use of adequate immunosuppression in the early period (40).
4 Impact of emerging technologies
The notion of immunocompatibility in transplantation is being redefined by a convergence of biomedical innovations, such as advances in molecular diagnostics, gene editing, and regenerative medicine, which go beyond traditional HLA and ABO matching paradigms. These technologies have begun to reshape not only how compatibility is assessed but also how immune risk is managed and donor availability is expanded. Broadly, three strategic frameworks have emerged: i) tools to increase compatibility precision; ii) modalities to broaden donor resources; and iii) interventions to mitigate adverse immune reactions. While their application varies across transplant settings, these strategies reflect a shift toward dynamic, tailored approaches in clinical transplantation.
4.1 Enhancing compatibility precision
A first group of technologies focuses on refining histocompatibility assessment and improving donor–recipient matching at molecular and functional levels. On the one hand, RNA-based next-generation sequencing (NGS) and advanced bioinformatics pipelines now enable allele-specific HLA expression profiling, providing deeper insight into immune compatibility, informing donor selection more accurately, and improving predictive modelling for transplant outcomes. These techniques are especially relevant in HSCT (14).Similarly, high-resolution typing and eplet analysis have advanced compatibility beyond antigen-level matching. Algorithms such as HLA-Matchmaker, PIRCHE, and HLA-EMMA analyze amino acid polymorphisms and antigen-presenting peptide predictions to quantify mismatches more precisely, enabling clinicians to stratify risk at the molecular interface of HLA. These tools are particularly valuable in heart transplantation, where nuanced HLA compatibility influences graft survival and immunosuppression needs (18).
Additionally, artificial intelligence (AI) and machine learning (ML) have revolutionized donor matching and risk stratification. In HSCT, predictive models integrate HLA typing with clinical parameters such as patient comorbidities, disease stage, and immunogenetic factors to identify optimal donors (41). In kidney transplantation, AI and ML tools -including Chatbot- assist throughout the transplant process, from donor selection to postoperative monitoring (42). Other quantitative tools such as the Living Kidney Donor Profile Index (LKDPI) empirically compares potential living donors across multiple factors (viral serology, age, eplet matching) to more precisely characterize donor-recipient incompatibilities and improve long-term graft survival (43). In liver transplantation, ML models can be used to identify patients at high risk for developing GvHD and to predict graft failure (44–46). For lung transplantation, InsightTx employs XGBoost algorithms to predict outcomes based on ex vivo lung perfusion (EVLP) data (46, 47). Similarly, pancreas transplantation has benefited from Naive Bayesian Classifier and Support Vector Machine-based models to estimate rejection probability in simultaneous pancreas–kidney recipients (48). In corneal transplants, AI applications utilizing Optical Coherence Tomography (OCT) imaging have also demonstrated remarkable accuracy in evaluating graft rejection (49).
Finally, gene editing technologies also serve compatibility goals by directly modifying donor organs or cells to enhance compatibility at the genetic level. CRISPR/Cas9 tools allow targeted disruption of immunogenic loci (e.g., HLA, T cell receptor TCRα), insertion of safety or regulatory transgenes (e.g., suicide switches, cytokine modulators), and overexpression of immunotolerance-associated molecules (e.g., HLA-E, CD47). These interventions are being explored in heart and lung transplantation. In this field, Figueiredo and collaborators proposed silencing donor MHC molecules via shRNAs to reduce immunogenicity, while CRISPR/Cas technologies hold promise for generating universal blood type lungs (50–52).
4.2 Expanding the donor pool
While compatibility precision improves outcomes, donor scarcity remains a fundamental constraint, especially for time-sensitive organs. To address this, a spectrum of strategies has emerged to expand transplantable resources without compromising immunological feasibility.
In this context, xenotransplantation has made significant strides, particularly with porcine donors genetically modified to silence xenoantigens involved in hyperacute rejection (synthesizing α-1,3-galactosyltransferase, GGTA1; and β-1,4-N-acetyl-galactosaminyltransferase 2, B4GALNT2), and synthesizing N-glycolylneuraminic acid (CMAH)) and express human transgenic proteins that regulate immune response (CD47 and heme oxygenase 1), coagulation (human thrombomodulin, hTBM), and complement activation (CD39, CD46 and CD55). Proof-of-concept transplants of porcine kidney, heart, and liver into human recipients have shown early success, suggesting that compatibility can be manufactured, rather than matched (53–56).
Bioengineering and regenerative medicine approaches, such as tissue engineering and 3D bioprinting, are also expanding alternatives to traditional organ replacement while enabling the development of personalized therapies through the creation of functional organ substitutes. These strategies reduce dependence on donor availability and enable HLA-compatible solutions. Scaffolds from decellularized organs repopulated with human stem or allogeneic progenitor cells (such as in kidney and heart bioengineering) preserve the native extracellular matrix while removing immunogenic antigens, promoting regeneration and reducing immune rejection (57–60). Kidney and liver organoids mimicking native tissue architecture are also being developed to increase graft availability (61–63). Intestinal organoids derived from adult stem cells or iPSCs show promise for treating conditions like inflammatory bowel disease, celiac disease, and short bowel syndrome by restoring barrier integrity, modulating immune response, and supporting nutrient absorption. In mice, transplanted epithelial organoids integrate and promote mucosal healing, with some studies using hydrogels or decellularized scaffolds to engineer functional intestinal tissue (64–67). In pancreatic transplantation, alginate encapsulation of islets has been explored to reduce immune rejection, even without immunosuppression, in both allo- and xenotransplantation settings (68–72). In the kidney, 3D bioprinting technologies aim to recreate nephron-like structures for future renal replacement therapies (57, 73), while similar strategies in the liver and lung are used to fabricate transplantable hepatic tissue or airway structures, respectively (62, 74).
Lastly, ex vivo organ perfusion platforms such as normothermic machine perfusion (NMP) and EVLP extend the viability of marginal grafts and enable functional rejuvenation. These systems also act as delivery routes for immunomodulatory agents (e.g., MSCs) and gene vectors, thereby minimizing off-target effects and vector-induced inflammation and transforming preservation into a therapeutic window. Applied in kidney, heart, lung, and liver transplantation, perfusion technologies help bridge immunological gaps and optimize graft readiness (75–78).
4.3 Mitigating immune adverse effects
When HLA or ABO compatibility cannot be strictly achieved, technological advances aim to neutralize immunological consequences and promote tolerance. Innovation in immunosuppressive regimens includes post-transplant cyclophosphamide (PTCy), costimulatory blockade, monoclonal antibodies targeting memory B and T cells, and targeted drug delivery. In HSCT, PTCy has gained prominence as a cost-effective method with strong GvHD prevention capacity, significantly expanding the use of haploidentical donors and redefining donor selection criteria (79). In lung, upregulation of interleukin-10 (IL-10) in models of acute rejection and CLAD has been shown to reduce inflammation and improve graft tolerance (80, 81). In intestinal transplantation, therapies targeting key inflammatory mediators, such as monoclonal antibodies against TNF-α and integrins, proteasome inhibitors and purine analogs, and modulation of the intestinal microbiome through selective antibiotics or probiotics reduce rejection while minimizing systemic toxicity (82).
Besides pharmacological approaches, cell-based immunomodulation is nowadays at the forefront. Regulatory T cells (Tregs) are increasingly used in HSC, kidney, liver, pancreas, and small intestine transplantation to prevent rejection and promote immune adaptation (82–87). Moreover, mesenchymal stromal cells (MSCs) exhibit immunosuppressive and anti-inflammatory properties, with therapeutic use spanning HSC, liver, lung (where a first-in-human study showed a slower decline in lung function in patients with advanced CLAD after MSCs infusion), and small intestine transplants (84, 86, 88–91). Additionally, regulatory dendritic cells have also shown promise in liver immunoregulation (92) and, recently, PRDM16-dependent APCs have been described to induce tolerance to gut antigens, offering new insights into developing therapeutic strategies for intestinal transplant tolerance (93). Chimerism-based strategies have been also tested, promoting immune adaptation through the co-transplantation of donor HSCs, as demonstrated in kidney and liver transplantation (94, 95). Finally, CAR-engineered immune cells, including CAR-T and CAR-NK, are under investigation in HSCT for their dual role in eliminating residual disease and modulating post-transplant immunity (83, 84, 96). AI-assisted monitoring complements these interventions. Tools analyzing gene expression profiles (e.g., AlloMap), donor cfDNA levels, and longitudinal patient data help detect early signs of rejection and guide immunosuppression tapering, thus allowing real-time adaptation and adjusting drug regimens dynamically to avoid over- or under-immunosuppression (42, 97–102).
These converging innovations indicate a shift from rigid antigen matching toward a functional and personalized approach to immunocompatibility. By integrating molecular precision, regenerative capacity, and predictive analytics, emerging technologies offer viable pathways to reconcile immunological complexity with therapeutic feasibility in modern transplantation.
5 Final remarks and outlook
Transplantation medicine has entered a transformative phase where immunocompatibility is no longer governed by a one-size-fits-all framework. In HSCT and kidney transplantation, compatibility-enhancing platforms are already reshaping donor selection. These fields will likely remain at the forefront of high-resolution typing, algorithmic matching, and integration of gene-edited therapies. In contrast, heart and pancreas grafts, constrained by urgency and donor scarcity, may benefit more from immune engineering, scaffolded tissues, and xenogeneic sources. Although the liver is more immunotolerant, these innovations also offer complementary solutions where donor availability is limited. In lung and intestinal transplantation, technologies mitigating immune aggression (such as EVLP-based gene delivery, PRDM16-dependent tolerance, and MSC infusions) are addressing the limitations of conventional matching. Meanwhile, corneal transplantation and pancreatic islets, both involving immune-privileged or compartmentalized sites, exemplify how bioengineered constructs and smart encapsulation can circumvent systemic immune triggers.
Looking ahead, compatibility may become a design feature rather than a selection criterion. Organoids, bioprinted tissues, and modular graft systems could be engineered with specific immune profiles, built to engage host defenses intelligently or resist them entirely. AI-driven dashboards might one day manage graft–host communication proactively, guiding immunomodulation not by static protocols but by continuous biological feedback. In this landscape, HLA and ABO matching remain foundational, but no longer absolute. Compatibility is expanding beyond genetic coincidence to include dynamic tolerability, functional resilience, and engineered neutrality. The goal is not perfect alignment, but sustainable integration: building transplant systems that adapt, persist, and heal across the immunological spectrum.
By embracing this new paradigm, transplantation can move from the constraints of biological inheritance toward the possibilities of biomedical design, where the immune system is not an obstacle to be overcome, but a partner to be engaged through technology, insight, and innovation.
Author contributions
RG-A: Validation, Methodology, Writing – original draft, Formal analysis, Data curation, Visualization, Writing – review & editing, Conceptualization, Investigation. RC-P: Project administration, Formal analysis, Validation, Methodology, Visualization, Data curation, Conceptualization, Writing – original draft, Writing – review & editing. JV: Methodology, Conceptualization, Writing – original draft, Supervision, Data curation, Visualization, Writing – review & editing, Funding acquisition, Resources.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. JV’s laboratory is a member of the Red Española de Terapias Avanzadas (RICORS-TERAV/TERAV+, file nos. RD21/0017/0022 and RD24/0014/0037, PI: JV), funded by the Instituto de Salud Carlos III (ISCiii) in the context of NextGenerationEU Recovery, Transformation and Resilience Plan. The joint BST-VHIR Musculoskeletal Tissue Engineering Group is a Consolidated Research Group accredited by the Agència de Gestió d’Ajuts Universitaris i de Recerca (AGAUR) of the Generalitat de Catalunya (file no. 2021-SGR-00877). RG-A is recipient of a PhD fellowship from the VHIR PhD call funded by Vall Hebron Research Institute (VHIR) - Amics del VHIR.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. During the preparation of this work, the authors used ChatGPT in order to improve the clarity and linguistic accuracy of the manuscript. Then, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rampersad C, Ahn C, Callaghan C, Dominguez-Gil B, Ferreira GF, Kute V, et al. Organ donation and transplantation registries across the globe: A review of the current state. Transplantation. (2024) 108:e321–e6. doi: 10.1097/TP.0000000000005043
2. Knoedler L, Dean J, Diatta F, Thompson N, Knoedler S, Rhys R, et al. Immune modulation in transplant medicine: a comprehensive review of cell therapy applications and future directions. Front Immunol. (2024) 15:1372862. doi: 10.3389/fimmu.2024.1372862
3. Al Moussawy M, Lakkis ZS, Ansari ZA, Cherukuri AR, and Abou-Daya KI. The transformative potential of artificial intelligence in solid organ transplantation. Front Transpl. (2024) 3:1361491. doi: 10.3389/frtra.2024.1361491
4. Geneugelijk K and Spierings E. PIRCHE-II: an algorithm to predict indirectly recognizable HLA epitopes in solid organ transplantation. Immunogenetics. (2020) 72:119–29. doi: 10.1007/s00251-019-01140-x
5. Tambur AR. Human leukocyte antigen matching in organ transplantation: what we know and how can we make it better (Revisiting the past, improving the future). Curr Opin Organ Transplant. (2018) 23:470–6. doi: 10.1097/MOT.0000000000000538
6. Rohn H and Rebmann V. Is HLA-E with its receptors an immune checkpoint or an antigenic determinant in allo-HCT? Best Pract Res Clin Haematol. (2024) 37:101560. doi: 10.1016/j.beha.2024.101560
7. Zhuang B, Shang J, and Yao Y. HLA-G: an important mediator of maternal-fetal immune-tolerance. Front Immunol. (2021) 12:744324. doi: 10.3389/fimmu.2021.744324
8. Pabón MA, Navarro CE, Osorio JC, Gómez N, Moreno JP, Donado AF, et al. Impact of human leukocyte antigen molecules E, F, and G on the outcome of transplantation. Transplant Proc. (2014) 46:2957–65. doi: 10.1016/j.transproceed.2014.07.010
9. de Miranda BLM, Gelmini GF, Risti M, Hauer V, da Silva JS, Roxo V, et al. HLA-E genotyping and its relevance in kidney transplantation outcome. Hla. (2020) 95:457–64. doi: 10.1111/tan.13806
10. Zachary AA and Leffell MS. HLA mismatching strategies for solid organ transplantation - A balancing act. Front Immunol. (2016) 7:575. doi: 10.3389/fimmu.2016.00575
11. Joseph A, Murray CJ, Novikov ND, Velliquette RW, Vege S, Halls JBL, et al. ABO Genotyping finds more A2 to B kidney transplant opportunities than lectin-based subtyping. Am J Transplant. (2023) 23:512–9. doi: 10.1016/j.ajt.2022.12.017
12. Raud L, Férec C, and Fichou Y. From genetic variability to phenotypic expression of blood group systems. Transfus Clin Biol. (2017) 24:472–5. doi: 10.1016/j.tracli.2017.06.011
13. Jiang H and Jiang J. Balancing act: the complex role of NK cells in immune regulation. Front Immunol. (2023) 14:1275028. doi: 10.3389/fimmu.2023.1275028
14. Passweg JR, Baldomero H, Chabannon C, Basak GW, de la Cámara R, Corbacioglu S, et al. Hematopoietic cell transplantation and cellular therapy survey of the EBMT: monitoring of activities and trends over 30 years. Bone Marrow Transpl. (2021) 56:1651–64. doi: 10.1038/s41409-021-01227-8
15. Johansson T, Partanen J, and Saavalainen P. HLA allele-specific expression: Methods, disease associations, and relevance in hematopoietic stem cell transplantation. Front Immunol. (2022) 13:1007425. doi: 10.3389/fimmu.2022.1007425
16. Lozano-Suárez N, García-López A, Gómez-Montero A, and Girón-Luque F. Relación entre la compatibilidad del HLA y la pérdida del injerto en trasplante renal de donante cadavérico: Un análisis por propensity score matching en Colombia. Rev Colombiana Cirugía. (2024) 39:268–79. doi: 10.30944/20117582.2491
17. Subramanian V, Ramachandran S, Klein C, Wellen JR, Shenoy S, Chapman WC, et al. ABO-incompatible organ transplantation. Int J Immunogenet. (2012) 39:282–90. doi: 10.1111/j.1744-313X.2012.01101.x
18. Kasiske BL, Neylan JF 3rd, Riggio RR, Danovitch GM, Kahana L, Alexander SR, et al. The effect of race on access and outcome in transplantation. N Engl J Med. (1991) 324:302–7. doi: 10.1056/NEJM199101313240505
19. Opelz G and Wujciak T. The influence of HLA compatibility on graft survival after heart transplantation. Collab Transplant Study N Engl J Med. (1994) 330:816–9. doi: 10.1056/NEJM199403243301203
20. Opelz G. Strength of HLA-A, HLA-B, and HLA-DR mismatches in relation to short- and long-term kidney graft survival. Collaborative Transplant Study. Transplant Int: Off J Eur Soc Organ Transpl. (1992) 5 Suppl 1:S621–4. doi: 10.1007/978-3-642-77423-2_182
21. Opelz G and Henderson R. Incidence of non-hodgkin lymphoma in kidney and heart transplant recipients. Lancet. (1993) 342:1514–6. doi: 10.1016/S0140-6736(05)80084-4
22. Neves C, Prieto D, Sola E, and Antunes MJ. Heart transplantation from donors of different ABO blood type. Transplant Proc. (2009) 41:938–40. doi: 10.1016/j.transproceed.2009.01.061
23. Urschel S, Ballweg JA, Cantor RS, Koehl DA, Reinhardt Z, Zuckerman WA, et al. Clinical outcomes of children receiving ABO-incompatible versus ABO-compatible heart transplantation: a multicentre cohort study. Lancet Child Adolesc Health. (2021) 5:341–9. doi: 10.1016/S2352-4642(21)00023-7
24. West LJ, Pollock-Barziv SM, Dipchand AI, Lee KJ, Cardella CJ, Benson LN, et al. ABO-incompatible heart transplantation in infants. N Engl J Med. (2001) 344:793–800. doi: 10.1056/NEJM200103153441102
25. Bricogne C, Halliday N, Fernando R, Tsochatzis EA, Davidson BR, Harber M, et al. Donor-recipient human leukocyte antigen A mismatching is associated with hepatic artery thrombosis, sepsis, graft loss, and reduced survival after liver transplant. Liver Transplant. (2022) 28:1306–20. doi: 10.1002/lt.26458
26. Abrol N, Jadlowiec CC, and Taner T. Revisiting the liver’s role in transplant alloimmunity. World J Gastroenterol. (2019) 25:3123–35. doi: 10.3748/wjg.v25.i25.3123
27. Kok G, Ilcken EF, Houwen RHJ, Lindemans CA, Nieuwenhuis EES, Spierings E, et al. The effect of genetic HLA matching on liver transplantation outcome: A systematic review and meta-analysis. Ann Surg Open: Perspect Surg History Educ Clin Approaches. (2023) 4:e334. doi: 10.1097/AS9.0000000000000334
28. Opelz G, Süsal C, Ruhenstroth A, and Döhler B. Impact of HLA compatibility on lung transplant survival and evidence for an HLA restriction phenomenon: A collaborative transplant study report. Transplantation. (2010) 90:912–7. doi: 10.1097/TP.0b013e3181f2c981
29. Hiho SJ, Levvey BJ, Diviney MB, Brooks AG, Holdsworth R, Snell GI, et al. HLA-C mismatching improves outcomes following lung transplantation. Hla. (2024) 103:e15544. doi: 10.1111/tan.15544
30. Rudolph EN, Dunn TB, Mauer D, Noreen H, Sutherland DE, Kandaswamy R, et al. HLA-A, -B, -C, -DR, and -DQ matching in pancreas transplantation: effect on graft rejection and survival. Am J Transpl. (2016) 16:2401–12. doi: 10.1111/ajt.13734
31. Nabulsi S, Otunla A, Salciccioli J, Marshall D, Villani V, Shanmugarajah K, et al. O236: the impact of HLA matching on pancreas and simultaneous pancreas-kidney (SPK) transplantation outcomes. Br J Surg. (2024) 111. doi: 10.1093/bjs/znae046.015
32. Ballou C, Barton F, Payne EH, Berney T, Villard J, Meier RPH, et al. Matching for HLA-DR excluding diabetogenic HLA-DR3 and HLA-DR4 predicts insulin independence after pancreatic islet transplantation. Front Immunol. (2023) 14:1110544. doi: 10.3389/fimmu.2023.1110544
33. Verhoeff K, Cuesta-Gomez N, Albers P, Pawlick R, Marfil-Garza BA, Jasra I, et al. Evaluating the potential for ABO-incompatible islet transplantation: expression of ABH antigens on human pancreata, isolated islets, and embryonic stem cell-derived islets. Transplantation. (2023) 107:e98–e108. doi: 10.1097/TP.0000000000004347
34. Forbes S, Halpin A, Lam A, Grynoch D, Parker R, Hidalgo L, et al. Islet transplantation outcomes in type 1 diabetes and transplantation of HLA-DQ8/DR4: results of a single-centre retrospective cohort in Canada. EClinicalMedicine. (2024) 67:102333. doi: 10.1016/j.eclinm.2023.102333
35. Sachdeva GS, Cabada JP, Karim SS, Kahandawa DL, Thomas KA, Kumar A, et al. Effectiveness of matching human leukocyte antigens (HLA) in corneal transplantation: a systematic review protocol. Syst Rev. (2021) 10:150. doi: 10.1186/s13643-021-01704-7
36. van Essen TH, Roelen DL, Williams KA, and Jager MJ. Matching for Human Leukocyte Antigens (HLA) in corneal transplantation - to do or not to do. Prog Retinal Eye Res. (2015) 46:84–110. doi: 10.1016/j.preteyeres.2015.01.001
37. Armitage WJ, Goodchild C, Griffin MD, Gunn DJ, Hjortdal J, Lohan P, et al. High-risk corneal transplantation: recent developments and future possibilities. Transplantation. (2019) 103:2468–78. doi: 10.1097/TP.0000000000002938
38. Kesseli S and Sudan D. Small bowel transplantation. Surg Clinics North America. (2019) 99:103–16. doi: 10.1016/j.suc.2018.09.008
39. Wu G, Liu C, Zhou X, Zhao L, Zhang W, Wang M, et al. Living donor intestinal transplantation: recipient outcomes. Ann Surg. (2022) 276:e444–e9. doi: 10.1097/SLA.0000000000005659
40. Fan DM, Zhao QC, Wang WZ, Shi H, Wang M, Chen DL, et al. Successful ABO-incompatible living-related intestinal transplantation: a 2-year follow-up. Am J Transpl. (2015) 15:1432–5. doi: 10.1111/ajt.13121
41. Logan BR, Maiers MJ, Sparapani RA, Laud PW, Spellman SR, McCulloch RE, et al. Optimal donor selection for hematopoietic cell transplantation using Bayesian machine learning. JCO Clin Cancer Inf. (2021) 5:494–507. doi: 10.1200/CCI.20.00185
42. Garcia Valencia OA, Thongprayoon C, Jadlowiec CC, Mao SA, Miao J, and Cheungpasitporn W. Enhancing kidney transplant care through the integration of chatbot. Healthc (Basel Switzerland). (2023) 11. doi: 10.3390/healthcare11182518
43. Jackson KR and Segev DL. Rethinking incompatibility in kidney transplantation. Am J Transpl. (2022) 22:1031–6. doi: 10.1111/ajt.16826
44. Cooper JP, Perkins JD, Warner PR, Shingina A, Biggins SW, Abkowitz JL, et al. Acute graft-versus-host disease after orthotopic liver transplantation: predicting this rare complication using machine learning. Liver Transplant. (2022) 28:407–21. doi: 10.1002/lt.26318
45. Bhat M, Rabindranath M, Chara BS, and Simonetto DA. Artificial intelligence, machine learning, and deep learning in liver transplantation. J Hepatol. (2023) 78:1216–33. doi: 10.1016/j.jhep.2023.01.006
46. Lau L, Kankanige Y, Rubinstein B, Jones R, Christophi C, Muralidharan V, et al. Machine-learning algorithms predict graft failure after liver transplantation. Transplantation. (2017) 101:e125–e32. doi: 10.1097/TP.0000000000001600
47. Liu X, Chen W, Du W, Li P, and Wang X. Application of artificial intelligence and machine learning in lung transplantation: a comprehensive review. Front Digital Health. (2025) 7:1583490. doi: 10.3389/fdgth.2025.1583490
48. Vigia E, Ramalhete L, Ribeiro R, Barros I, Chumbinho B, Filipe E, et al. Pancreas rejection in the artificial intelligence era: new tool for signal patients at risk. J Pers Med. (2023) 13. doi: 10.3390/jpm13071071
49. Shanthi S, Aruljyothi L, Balasundaram MB, Janakiraman A, Nirmaladevi K, and Pyingkodi M. Artificial intelligence applications in different imaging modalities for corneal topography. Survey Ophthalmol. (2022) 67:801–16. doi: 10.1016/j.survophthal.2021.08.004
50. Deuse T, Hu X, Gravina A, Wang D, Tediashvili G, De C, et al. Hypoimmunogenic derivatives of induced pluripotent stem cells evade immune rejection in fully immunocompetent allogeneic recipients. Nat Biotechnol. (2019) 37:252–8. doi: 10.1038/s41587-019-0016-3
51. Figueiredo C, Carvalho Oliveira M, Chen-Wacker C, Jansson K, Höffler K, Yuzefovych Y, et al. Immunoengineering of the vascular endothelium to silence MHC expression during normothermic ex vivo lung perfusion. Hum Gene Ther. (2019) 30:485–96. doi: 10.1089/hum.2018.117
52. Wang A, Ribeiro RVP, Ali A, Brambate E, Abdelnour-Berchtold E, Michaelsen V, et al. Ex vivo enzymatic treatment converts blood type A donor lungs into universal blood type lungs. Sci Transl Med. (2022) 14:eabm7190. doi: 10.1126/scitranslmed.abm7190
53. Montgomery RA, Stern JM, Lonze BE, Tatapudi VS, Mangiola M, Wu M, et al. Results of two cases of pig-to-human kidney xenotransplantation. N Engl J Med. (2022) 386:1889–98. doi: 10.1056/NEJMoa2120238
54. Yang C, Wei Y, Li X, Xu K, Huo X, Chen G, et al. Production of four-gene (GTKO/hCD55/hTBM/hCD39)-edited donor pigs and kidney xenotransplantation. Xenotransplantation. (2024) 31:e12881. doi: 10.1111/xen.12881
55. Griffith BP, Goerlich CE, Singh AK, Rothblatt M, Lau CL, Shah A, et al. Genetically modified porcine-to-human cardiac xenotransplantation. N Engl J Med. (2022) 387:35–44. doi: 10.1056/NEJMoa2201422
56. Tao KS, Yang ZX, Zhang X, Zhang HT, Yue SQ, Yang YL, et al. Gene-modified pig-to-human liver xenotransplantation. Nature. (2025) 641:1029–36. doi: 10.1038/s41586-025-08799-1
57. Ali M, Pr AK, Yoo JJ, Zahran F, Atala A, and Lee SJ. A photo-crosslinkable kidney ECM-derived bioink accelerates renal tissue formation. Adv Healthc Mater. (2019) 8:e1800992. doi: 10.1002/adhm.201800992
58. Ott HC, Matthiesen TS, Goh SK, Black LD, Kren SM, Netoff TI, et al. Perfusion-decellularized matrix: using nature’s platform to engineer a bioartificial heart. Nat Med. (2008) 14:213–21. doi: 10.1038/nm1684
59. Prat-Vidal C, Rodriguez-Gomez L, Aylagas M, Nieto-Nicolau N, Gastelurrutia P, Agusti E, et al. First-in-human PeriCord cardiac bioimplant: Scalability and GMP manufacturing of an allogeneic engineered tissue graft. EBioMedicine. (2020) 54:102729. doi: 10.1016/j.ebiom.2020.102729
60. Bayes-Genis A, Gastelurrutia P, Monguió-Tortajada M, Cámara ML, Prat-Vidal C, Cediel G, et al. Implantation of a double allogeneic human engineered tissue graft on damaged heart: insights from the PERISCOPE phase I clinical trial. EBioMedicine. (2024) 102:105060. doi: 10.1016/j.ebiom.2024.105060
61. Lawlor KT, Vanslambrouck JM, Higgins JW, Chambon A, Bishard K, Arndt D, et al. Cellular extrusion bioprinting improves kidney organoid reproducibility and conformation. Nat Mater. (2021) 20:260–71. doi: 10.1038/s41563-020-00853-9
62. Yang H, Sun L, Pang Y, Hu D, Xu H, Mao S, et al. Three-dimensional bioprinted hepatorganoids prolong survival of mice with liver failure. Gut. (2021) 70:567–74. doi: 10.1136/gutjnl-2019-319960
63. Hu H, Gehart H, Artegiani B, LÖpez-Iglesias C, Dekkers F, Basak O, et al. Long-term expansion of functional mouse and human hepatocytes as 3D organoids. Cell. (2018) 175:1591–606 e19. doi: 10.1016/j.cell.2018.11.013
64. Watanabe S, Kobayashi S, Ogasawara N, Okamoto R, Nakamura T, Watanabe M, et al. Transplantation of intestinal organoids into a mouse model of colitis. Nat Protoc. (2022) 17:649–71. doi: 10.1038/s41596-021-00658-3
65. Watanabe S, Ogasawara N, Kobayashi S, Kirino S, Inoue M, Hiraguri Y, et al. Organoids transplantation as a new modality to design epithelial signature to create a membrane-protective sulfomucin-enriched segment. J Gastroenterol. (2023) 58:379–93. doi: 10.1007/s00535-023-01959-y
66. Nakanishi A, Toyama S, Onozato D, Watanabe C, Hashita T, Iwao T, et al. Effects of human induced pluripotent stem cell-derived intestinal organoids on colitis-model mice. Regen Ther. (2022) 21:351–61. doi: 10.1016/j.reth.2022.08.004
67. Sugimoto S, Kobayashi E, Fujii M, Ohta Y, Arai K, Matano M, et al. An organoid-based organ-repurposing approach to treat short bowel syndrome. Nature. (2021) 592:99–104. doi: 10.1038/s41586-021-03247-2
68. Wang Q, Huang YX, Liu L, Zhao XH, Sun Y, Mao X, et al. Pancreatic islet transplantation: current advances and challenges. Front Immunol. (2024) 15:1391504. doi: 10.3389/fimmu.2024.1391504
69. Mallett AG and Korbutt GS. Alginate modification improves long-term survival and function of transplanted encapsulated islets. Tissue Eng Part A. (2009) 15:1301–9. doi: 10.1089/ten.tea.2008.0118
70. Alagpulinsa DA, Cao JJL, Driscoll RK, Sîrbulescu RF, Penson MFE, Sremac M, et al. Alginate-microencapsulation of human stem cell-derived β cells with CXCL12 prolongs their survival and function in immunocompetent mice without systemic immunosuppression. Am J Transpl. (2019) 19:1930–40. doi: 10.1111/ajt.15308
71. Chen T, Yuan J, Duncanson S, Hibert ML, Kodish BC, Mylavaganam G, et al. Alginate encapsulant incorporating CXCL12 supports long-term allo- and xenoislet transplantation without systemic immune suppression. Am J Transpl. (2015) 15:618–27. doi: 10.1111/ajt.13049
72. Gazda LS, Vinerean HV, Laramore MA, Hall RD, Carraway JW, and Smith BH. No evidence of viral transmission following long-term implantation of agarose encapsulated porcine islets in diabetic dogs. J Diabetes Res. (2014) 2014:727483. doi: 10.1155/2014/727483
73. Pichler R, Rizzo L, Tröndle K, Bühler M, Brucker H, Müller AL, et al. Tuning the 3D microenvironment of reprogrammed tubule cells enhances biomimetic modeling of polycystic kidney disease. Biomaterials. (2022) 291:121910. doi: 10.1016/j.biomaterials.2022.121910
74. Barreiro Carpio M, Dabaghi M, Ungureanu J, Kolb MR, Hirota JA, and Moran-Mirabal JM. 3D bioprinting strategies, challenges, and opportunities to model the lung tissue microenvironment and its function. Front Bioeng Biotechnol. (2021) 9:773511. doi: 10.3389/fbioe.2021.773511
75. Zeng Z, Xu L, Xu Y, Ruan Y, Liu D, Li J, et al. Normothermic ex vivo heart perfusion with mesenchymal stem cell-derived conditioned medium improves myocardial tissue protection in rat donation after circulatory death hearts. Stem Cells Int. (2022) 2022:8513812. doi: 10.1155/2022/8513812
76. Li J, Peng Q, Yang R, Li K, Zhu P, Zhu Y, et al. Application of mesenchymal stem cells during machine perfusion: an emerging novel strategy for organ preservation. Front Immunol. (2021) 12:713920. doi: 10.3389/fimmu.2021.713920
77. Sage AT, Donahoe LL, Shamandy AA, Mousavi SH, Chao BT, Zhou X, et al. A machine-learning approach to human ex vivo lung perfusion predicts transplantation outcomes and promotes organ utilization. Nat Commun. (2023) 14:4810. doi: 10.1038/s41467-023-40468-7
78. Niroomand A, Hirdman G, Olm F, and Lindstedt S. Current status and future perspectives on machine perfusion: A treatment platform to restore and regenerate injured lungs using cell and cytokine adsorption therapy. Cells. (2021) 11. doi: 10.3390/cells11010091
79. Arcuri LJ, Ribeiro AAF, Hamerschlak N, and Kerbauy MN. Posttransplant cyclophosphamide beyond haploidentical transplantation. Ann Hematol. (2024) 103:1483–91. doi: 10.1007/s00277-023-05300-8
80. Oishi H, Okada Y, Kikuchi T, Hoshikawa Y, Sado T, Noda M, et al. Transbronchial human interleukin-10 gene transfer reduces acute inflammation associated with allograft rejection and intragraft interleukin-2 and tumor necrosis factor-alpha gene expression in a rat model of lung transplantation. J Heart Lung Transpl: Off Publ Int Soc Heart Transpl. (2010) 29:360–7. doi: 10.1016/j.healun.2009.10.002
81. Boehler A, Chamberlain D, Xing Z, Slutsky AS, Jordana M, Gauldie J, et al. Adenovirus-mediated interleukin-10 gene transfer inhibits post-transplant fibrous airway obliteration in an animal model of bronchiolitis obliterans. Hum Gene Ther. (1998) 9:541–51. doi: 10.1089/hum.1998.9.4-541
82. Dogra H and Hind J. Innovations in immunosuppression for intestinal transplantation. Front Nutr. (2022) 9:869399. doi: 10.3389/fnut.2022.869399
83. Blazar BR, Hill GR, and Murphy WJ. Dissecting the biology of allogeneic HSCT to enhance the GvT effect whilst minimizing GvHD. Nat Rev Clin Oncol. (2020) 17:475–92. doi: 10.1038/s41571-020-0356-4
84. Pashkina E, Blinova E, Bykova M, Aktanova A, and Denisova V. Cell therapy as a way to increase the effectiveness of hematopoietic stem cell transplantation. Cells. (2024) 13. doi: 10.3390/cells13242056
85. Martin-Moreno PL, Tripathi S, and Chandraker A. Regulatory T cells and kidney transplantation. Clin J Am Soc Nephrol. (2018) 13:1760–4. doi: 10.2215/CJN.01750218
86. Detry O, Vandermeulen M, Delbouille MH, Somja J, Bletard N, Briquet A, et al. Infusion of mesenchymal stromal cells after deceased liver transplantation: A phase I-II, open-label, clinical study. J Hepatol. (2017) 67:47–55. doi: 10.1016/j.jhep.2017.03.001
87. Battaglia M, Stabilini A, Draghici E, Gregori S, Mocchetti C, Bonifacio E, et al. Rapamycin and interleukin-10 treatment induces T regulatory type 1 cells that mediate antigen-specific transplantation tolerance. Diabetes. (2006) 55:40–9. doi: 10.2337/diabetes.55.01.06.db05-0613
88. Chambers DC, Enever D, Lawrence S, Sturm MJ, Herrmann R, Yerkovich S, et al. Mesenchymal stromal cell therapy for chronic lung allograft dysfunction: results of a first-in-man study. Stem Cells Transl Med. (2017) 6:1152–7. doi: 10.1002/sctm.16-0372
89. Levitte S, Zhang KY, Guevara-Tique AA, Ganguly A, Dulken BW, Nilkant R, et al. Mesenchymal stem cell-derived extracellular vesicles for the treatment of acute rejection in pediatric and adult bowel transplant. Am J Transplant. (2023) 24. doi: 10.1016/j.ajt.2023.10.019
90. Perez-Torres Lobato M, Benitez-Carabante MI, Alonso L, Torrents S, Castillo Flores N, Uria Oficialdegui ML, et al. Mesenchymal stromal cells in the treatment of pediatric hematopoietic cell transplantation-related complications (graft vs. host disease, hemorrhagic cystitis, graft failure and poor graft function): a single center experience. Front Pediatr. (2024) 12:1375493. doi: 10.3389/fped.2024.1375493
91. Vives J and Mirabel C. Multipotent mesenchymal stromal cells from bone marrow for current and potential clinical applications. In: Reis RL, editor. Encyclopedia of Tissue Engineering and Regenerative Medicine. Academic Press, Oxford (2019). p. 503–12.
92. Zhou Y, Shan J, Guo Y, Li S, Long D, Li Y, et al. Effects of adoptive transfer of tolerogenic dendritic cells on allograft survival in organ transplantation models: an overview of systematic reviews. J Immunol Res. (2016) 2016:5730674. doi: 10.1155/2016/5730674
93. Fu L, Upadhyay R, Pokrovskii M, Chen FM, Romero-Meza G, Griesemer A, et al. PRDM16-dependent antigen-presenting cells induce tolerance to gut antigens. Nature. (2025) 642:756–65. doi: 10.1038/s41586-025-08982-4
94. Little CJ, Kim SC, Fechner JH, Post J, Coonen J, Chlebeck P, et al. Early allogeneic immune modulation after establishment of donor hematopoietic cell-induced mixed chimerism in a nonhuman primate kidney transplant model. Front Immunol. (2024) 15:1343616. doi: 10.3389/fimmu.2024.1343616
95. Donckier V, Troisi R, Le Moine A, Toungouz M, Ricciardi S, Colle I, et al. Early immunosuppression withdrawal after living donor liver transplantation and donor stem cell infusion. Liver Transpl: Off Publ Am Assoc Study Liver Dis Int Liver Transplant Society. (2006) 12:1523–8. doi: 10.1002/lt.20872
96. Huang R and Zhang X. Exploration and practice: New integration of cellular therapy and hematopoietic stem cell transplantation. Chin Med J (Engl). (2025) 138:1261–5. doi: 10.1097/CM9.0000000000003558
97. Borkowski P, Singh N, and Borkowska N. Advancements in heart transplantation: donor-derived cell-free DNA as next-generation biomarker. Cureus. (2024) 16:e54018. doi: 10.7759/cureus.54018
98. Deng MC. The AlloMap™ genomic biomarker story: 10 years after. Clin Transplant. (2017) 31. doi: 10.1111/ctr.12900
99. Piening BD, Dowdell AK, Zhang M, Loza BL, Walls D, Gao H, et al. Whole transcriptome profiling of prospective endomyocardial biopsies reveals prognostic and diagnostic signatures of cardiac allograft rejection. J Heart Lung Transpl: Off Publ Int Soc Heart Transpl. (2022) 41:840–8. doi: 10.1016/j.healun.2022.01.1377
100. Naruka V, Arjomandi Rad A, Subbiah Ponniah H, Francis J, Vardanyan R, Tasoudis P, et al. Machine learning and artificial intelligence in cardiac transplantation: A systematic review. Artif Organs. (2022) 46:1741–53. doi: 10.1111/aor.14334
101. Kampaktsis PN, Siouras A, Doulamis IP, Moustakidis S, Emfietzoglou M, Van den Eynde J, et al. Machine learning-based prediction of mortality after heart transplantation in adults with congenital heart disease: A UNOS database analysis. Clin Transpl. (2023) 37:e14845. doi: 10.1111/ctr.14845
Keywords: ABO, emerging therapies, HLA match, immunosupression, personalized medicine, rejection, tolerance, transplantation
Citation: Güell-Alonso R, Cabrera-Pérez R and Vives J (2025) Immunocompatibility in transplantation: adapting to a changing therapeutic landscape. Front. Immunol. 16:1648534. doi: 10.3389/fimmu.2025.1648534
Received: 17 June 2025; Accepted: 15 August 2025;
Published: 09 September 2025.
Edited by:
Aurore Saudemont, Xap Therapeutics, United KingdomReviewed by:
Stanislaw Stepkowski, University of Toledo, United StatesAnna Christina Dragon, Hannover Medical School, Germany
Copyright © 2025 Güell-Alonso, Cabrera-Pérez and Vives. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Cabrera-Pérez, cmNhYnJlcmFAYnN0LmNhdA==; Joaquim Vives, anZpdmVzQGJzdC5jYXQ=