 Shuaiwei Wang1Hao Fu1,2Xiaoqing Li1,3Hongrui Xu1Yu Bai1Wenjun Jiang1Xiaozhe Cheng1Na Chen1,4
Shuaiwei Wang1Hao Fu1,2Xiaoqing Li1,3Hongrui Xu1Yu Bai1Wenjun Jiang1Xiaozhe Cheng1Na Chen1,4 Yijie Zhang1,5
Yijie Zhang1,5 Wei Li1*
Wei Li1*- 1Sepsis Laboratory, Center for Translational Medicine, The Second College of Clinical Medicine, Henan University, Kaifeng, Henan, China
- 2Department of Endocrine and Metabolic Diseases, The Fifth Affiliated Hospital of Zunyi Medical University, Zhuhai, Guangdong, China
- 3Clinical Laboratory, The First People’s Hospital, Shangqiu, Henan, China
- 4Department of Pulmonary and Critical Care Medicine, The Second College of Clinical Medicine, Henan University, Kaifeng, Henan, China
- 5Department of Clinical Medicine, Luohe Medical College, Luohe, Henan, China
A Correction on
Plasma polymeric immunoglobulin receptor exacerbates lung injury in Klebsiella pneumoniae-induced pneumosepsis
By Wang S, Fu H, Li X, Xu H, Bai Y, Jiang W, Cheng X, Chen N, Zhang Y and Li W (2025) Plasma polymeric immunoglobulin receptor exacerbates lung injury in Klebsiella pneumoniae-induced pneumosepsis. Front. Immunol. 16:1624014. doi: 10.3389/fimmu.2025.1624014
There was a mistake in the caption of Figure 2B as published The symbol (&) needs to be removed. The corrected caption of Figure 2B appears below.
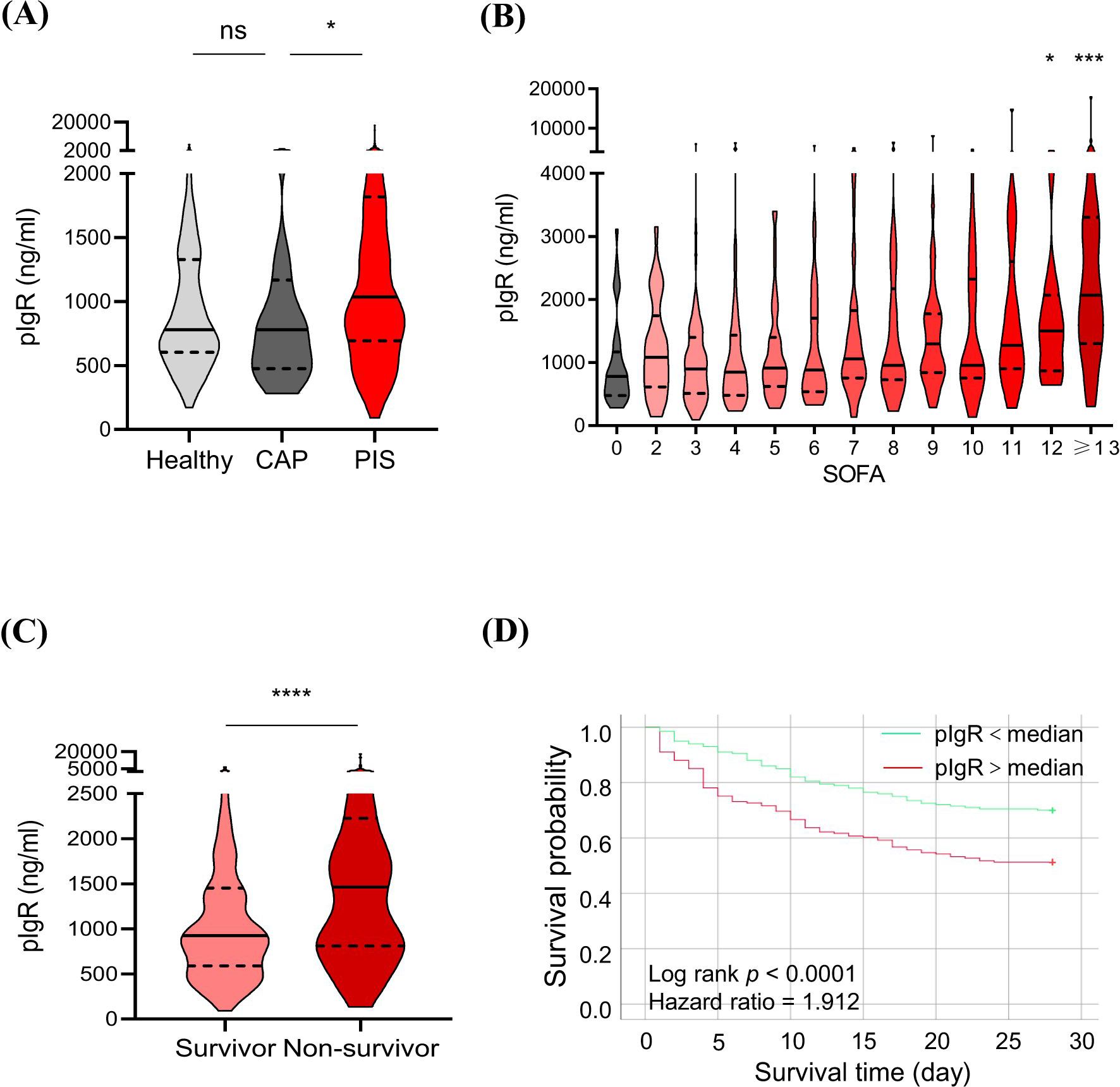
Figure 2. Association of plasma polymeric immunoglobulin receptor (pIgR) with the occurrence and prognosis of sepsis. (A) Comparisons of pIgR concentrations in plasma from healthy (n = 129), community-acquired pneumonia (CAP, n = 33) and pneumonia-induced sepsis (PIS, n = 449) subjects. Mann Whitney test was used to calculate p values. nsp > 0.05; *p < 0.05. (B) Comparisons of pIgR concentrations in CAP subjects (SOFA = 0, n = 33) with PIS subjects with different degrees of organ dysfunctions (SOFA scores). The n values are 29, 69, 48, 43, 40, 39, 25, 35, 33, 20, 22 and 46 for SOFA groups 2 to ≥ 13, respectively. Kruskal-Wallis test was used to calculate p values. *p < 0.05; ***p < 0.001. (C) A comparison of pIgR concentrations between PIS subjects that did (Survivor, n = 248) and did not (Non-survivor, n = 163) survive 28 days of hospitalization. *p < 0.05; ***p < 0.001. (D) Log-rank (Mantel-Cox) test of Kaplan-Meier survival curves of PIS patients with a higher (> median, n = 225, red line) and those with a lower (< median, n = 224, green line) levels of plasma pIgR. ****p < 0.0001. Variables in (A-C) are presented as median ± interquartile ranges.
“(B) Comparisons of pIgR concentrations in CAP subjects (SOFA = 0, n = 33) with PIS subjects with different degrees of organ dysfunctions (SOFA scores). The n values are 29, 69, 48, 43, 40, 39, 25, 35, 33, 20, 22 and 46 for SOFA groups 2 to ≥ 13, respectively. Kruskal-Wallis test was used to calculate p values. *p < 0.05; ***p < 0.001”.
Also, there was an error in the article text, during the typographical process, an ampersand (&) was added to the body text of the article. A correction has been made to 3 Results, 3.2 Elevation of plasma pIgR is associatedwith sepsis mortality, Paragraph 3.
The corrected sentence appears below:
“The median concentrations of pIgR were 779.76, 780.27 and 1041.87 ng/mL in healthy, CAP and PIS subjects, respectively (Figure 2A). pIgR concentrations were not different between healthy and CAP subjects (p = 0.47), but 34% higher in PIS group (p = 0.01, Figure 2A). Among PIS subjects, only those with multiple organ failures (SOFA score > 12) had a significantly higher level of pIgR than CAP subjects (SOFA = 0, Figure 2B). In addition, pIgR concentration was higher in PIS patients that were destined to die (1463 ng/ml) than those survived 28 days of hospitalization (924 ng/ml, p <0.0001, Figure 2C). Consistent with the TMT-MS results, higher pIgR concentrations (> median) were associated with increased risk of death (hazard ratio = 1.912, p < 0.0001, Figure 2D)”.
Lastly, there was another error in the published article. The word ‘not’ is missing from the body text of the article. A correction has been made to 4 Discussion, 4.3 AT2-targeting by plasma pIgR, Paragraph 6.
“KP infection causes widespread injuries of alveolar epithelial cells, such as AT1 and AT2, as indicated by the marked reduction in GP36, SPA and SPC in KPS mouse lungs. The significant impacts of r_pIgR and pIgR_Ab on SPA and SPC, but not GP36, suggest that AT2 are preferentially targeted by plasma pIgR. This notion is consistent with the virtually exclusive localization of pIgR immunoreactivity in AT2, among all alveolar cells, in KPS mouse lungs. Since AT2 do not express endogenous pIgR under physiological conditions or after bacterial infection (9, 11), the emergence of pIgR immunoreactivity likely results from a binding of extracellular pIgR. Indeed, pIgR was not detectable in primary AT2 cells before and after LPS treatment, but was evident after an exposure to r_pIgR. The further increase in pIgR in LPS-treated cells suggests that an infection by Gram-negative bacteria, such as KP, can augment the pIgR-binding capacity of AT2”.
The original article has been updated.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Keywords: sepsis, polymeric immunoglobulin receptor, Klebsiella pneumoniae, alveolar type 2 epithelial cells, pyroptosis, caspase-11
Citation: Wang S, Fu H, Li X, Xu H, Bai Y, Jiang W, Cheng X, Chen N, Zhang Y and Li W (2025) Correction: Plasma polymeric immunoglobulin receptor exacerbates lung injury in Klebsiella pneumoniae-induced pneumosepsis. Front. Immunol. 16:1678276. doi: 10.3389/fimmu.2025.1678276
Received: 02 August 2025; Accepted: 11 August 2025;
Published: 22 August 2025.
Edited and reviewed by:
Mariana Araújo-Pereira, Gonçalo Moniz Institute (IGM), BrazilCopyright © 2025 Wang, Fu, Li, Xu, Bai, Jiang, Cheng, Chen, Zhang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Li, MTAyMjAwMzhAdmlwLmhlbnUuZWR1LmNu