 Anne Sauvaget1,2,3*
Anne Sauvaget1,2,3* Benoît Trojak4,5
Benoît Trojak4,5 Samuel Bulteau1,2
Samuel Bulteau1,2 Susana Jiménez-Murcia3,6
Susana Jiménez-Murcia3,6 Fernando Fernández-Aranda3,6
Fernando Fernández-Aranda3,6 Ines Wolz3,6
Ines Wolz3,6 José M. Menchón3,7
José M. Menchón3,7 Sophia Achab5Jean-Marie Vanelle1,2
Sophia Achab5Jean-Marie Vanelle1,2 Marie Grall-Bronnec1,2,8
Marie Grall-Bronnec1,2,8- 1Addictology and Liaison Psychiatry Department, Nantes University Hospital, Nantes, France
- 2Clinical Investigation Unit 18-BALANCED “BehaviorAL AddictioNs and ComplEx Mood Disorders”, University Hospital of Nantes, Nantes, France
- 3Department of Psychiatry, University Hospital of Bellvitge-IDIBELL, Barcelona, Spain
- 4Department of Psychiatry and Addictology, University Hospital of Dijon, Dijon, France
- 5Behavioral Addictions Program, NANT New Addictions New Treatments, Addiction Division, Department of Mental Health and Psychiatry, University Hospital of Geneva, Geneva, Switzerland
- 6CIBER Fisiopatología Obesidad y Nutrición, Instituto de Salud Carlos III, Barcelona, Spain
- 7CIBER Salud Mental, Instituto de Salud Carlos III, Barcelona, Spain
- 8EA 4275 “Biostatistics, Clinical Research and Subjective Measures in Health Sciences”, University of Nantes, Nantes, France
Objectives: Behavioral addictions (BA) are complex disorders for which pharmacological and psychotherapeutic treatments have shown their limits. Non-invasive brain stimulation, among which transcranial direct current stimulation (tDCS), has opened up new perspectives in addiction treatment. The purpose of this work is to conduct a critical and systematic review of tDCS efficacy, and of technical and methodological considerations in the field of BA.
Methods: A bibliographic search has been conducted on the Medline and ScienceDirect databases until December 2014, based on the following selection criteria: clinical studies on tDCS and BA (namely eating disorders, compulsive buying, Internet addiction, pathological gambling, sexual addiction, sports addiction, video games addiction). Study selection, data analysis, and reporting were conducted according to the PRISMA guidelines.
Results: Out of 402 potential articles, seven studies were selected. So far focusing essentially on abnormal eating, these studies suggest that tDCS (right prefrontal anode/left prefrontal cathode) reduces food craving induced by visual stimuli.
Conclusions: Despite methodological and technical differences between studies, the results are promising. So far, only few studies of tDCS in BA have been conducted. New research is recommended on the use of tDCS in BA, other than eating disorders.
Introduction
Substance Use Disorder and Behavioral Addictions
Addictions are complex disorders conventionally represented by substance use disorders (SUDs). Other behaviors without any substance use share many clinical similarities, and are therefore categorized as addictions without drug use,—more commonly called behavioral addictions (BAs) (O'Brien, 2011; Potenza, 2014) -, as evidenced in the recent release of the DSM-5 (American Psychiatric Association, 2013), where gambling disorders now appear in the “substance-related and addictive disorders” category, among other SUDs. Until now, this is the only BA that the task force researchers included into the edited version of the manual. However, for many authors, BAs also encompass video games addiction, Internet addiction, sexual addiction, compulsive buying, sports addiction, and eating disorders (Gearhardt et al., 2011; Farré et al., 2015; Jiménez-Murcia et al., 2015). It has increasingly been suggested that some eating habits, such as the uncontrolled intake of high-calorie food rich in sugar and fat, can also be seen as behavioral addictions and was recently referred to as “food addiction” (Davis and Carter, 2009; Gearhardt et al., 2011; Hebebrand et al., 2014; Schulte et al., 2015).
As in any SUD, one of the key symptoms in BAs is craving, defined as a pressing, urgent, and irrepressible desire to give in to a BA, which results in most cases in a loss of control (Skinner and Aubin, 2010; O'Brien, 2011). The craving contributes to the development, continuation and relapse of an addictive behavior. Although craving is not pathognomonic of addiction, it remains a key symptom in the addictive process, to the point that it is now considered in the DSM-5 as a diagnostic criterion for substance-related and addictive disorders (American Psychiatric Association, 2013). Craving can lead to a loss of control over one's behavior. Executive functions (such as decision making and risk-taking process) and working memory impairments have been found in both SUDs and BAs (Fernández-Serrano et al., 2010; Marazziti et al., 2014). These clinical features suggest that BAs and SUDs may share similar neurophysiopathological abnormalities. Some authors support the idea of common neurochemical and genetic mechanisms involved with both substance and non-substance, addictive behaviors, linked to disturbances of the reward system, so-called “reward deficiency syndrome” (Blum et al., 2014). The central reward pathway involves the dopaminergic system such as the mesolimbic cortical ventral tegmental area and projections to the nucleus accumbens and the prefrontal cortex (Goldstein and Volkow, 2002; García-García et al., 2014). Neuroimanging studies underlined the important function of the prefrontal cortex, especially the dorsolateral prefrontal cortex (DLPFC), in both SUDs and BAs (Goudriaan et al., 2012).
The pharmacological and psychotherapeutic treatments of addictions and of the craving in particular, have shown their limits (Achab and Khazaal, 2011; Marazziti et al., 2014), which indicates the need for new treatment possibilities.
Non-invasive Brain Stimulation, a Promising Treatment for Addictions
More recently, new treatment modalities such as non-invasive brain stimulation (NIBS) have been explored in the field of addiction, such as Transcranial Direct Current Stimulation (tDCS) and repetitive transcranial magnetic stimulation (rTMS) (Jansen et al., 2013; Grall-Bronnec and Sauvaget, 2014). rTMS generates a magnetic field in a coil that is placed on the scalp. The magnetic field induces an electrical current in the brain tissue beneath the coil, resulting in alterations of neural excitability (Ziad, 2002). In addition to its cortical action, TMS may act remotely on deeper structures, via brain circuits and interhemispheric connections (Fox et al., 1997). tDCS is another NIBS method capable of modulating cortical excitability (Feil and Zangen, 2010). tDCS consists in delivering a low intensity electric field (1–2 mA) through the brain between two electrodes. The current enters the brain from the anode, travels through the tissue, and exits out the cathode (Higgins and George, 2009). The anodic stimulation increases cortical excitability, whereas the cathodic stimulation reduces it. The administration of tDCS is relatively easy. Electrodes can be placed anywhere on the scalp and are held in place with an elastic headband (Higgins and George, 2009). In general, one session lasts 10–20 min. Two sessions a day can be given easily if required. Like rTMS (Keck et al., 2002; Hanlon et al., 2013), tDCS showed that it could have remote effects (Chib et al., 2013).
rTMS and tDCS, applied to the DLPFC, may transiently modify decision-making, risk-taking, and impulsivity, processes directly linked to behavioral disorders. It has thus been shown that applying tDCS on prefrontal areas modifies the decision process in sane subjects (Fecteau et al., 2007a,b; Knoch et al., 2008; Boggio et al., 2010), but also in addicted subjects (Fecteau et al., 2014). The decision-making process shares common mechanisms with the impulsive behaviors observed in addictions. By modulating it, we could decrease impulsivity in addicted patients, and, indirectly, act on the craving (Fecteau et al., 2010). Anodal tDCS over the DLPFC may enhance executive function and provide improved cognitive control, and thus reduce the probability of relapse to drug use (da Silva et al., 2013).
Finally, even if the neurophysiological effects behind the effects of tDCS on craving are not completely clarified yet, choosing the DLPFC as a stimulation area is justified by the involvement of frontal areas in the neurobiology of eating disorders, either bulimia, or anorexia nervosa (Kaye et al., 2009; van Kuyck et al., 2009; Frank et al., 2013; Friederich et al., 2013). More precisely, the DLPFC might be involved in the food restriction and cognitive control mechanisms, which are linked with the working memory (von Hausswolff-Juhlin et al., 2015).
rTMS and tDCS applied to the DLPFC may therefore indirectly modulate dopaminergic pathways (Addolorato et al., 2012) and may consequently have an impact on the symptoms of addiction (Keck et al., 2002; Feil and Zangen, 2010). Cognitive control could be improved and/or cravings could be reduced (Jansen et al., 2013). So far, tDCS have proven its efficacy to decrease craving, mainly in SUDs (Jansen et al., 2013; Naim-Feil and Zangen, 2013; Kuo et al., 2014). Moreover, reviews and comprehensive work about tDCS in the field of psychiatry and addictions did not have considered BAs (Feil and Zangen, 2010; Kuo et al., 2014; Tortella et al., 2015).
The goal of this study is to conduct a systematic review of the efficacy, and of the technical and methodological stakes of applying tDCS to the field of BAs.
Methods
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009).
Search Resources
Two independent reviewers conducted the literature search, including different sources such as electronic databases (PubMed and Science Direct), citations, and reference lists, as well as gray literature. In addition, the reference lists of all included studies were hand searched, limiting the search to articles published in English. To ensure the recency of articles, the search was limited from inception to December, 31st, 2014.
The search terms used were a combination of MESH terms and keywords and included “tDCS” and “addiction,” “anorexia nervosia,” “behavioral addiction,” “bulimia nervosa,” “eating disorders,” “binge eating disorders,” “compulsive buying/shopping,” “craving,” “Dorsolateral prefrontal cortex (DLPFC),” “dependence,” “dopamine,” “eating disorders and not otherwise specified (EDNOS),” “exercise,” “food craving,” “gambling disorder,” “impulsivity,” “Internet addiction,” “pathological gambling,” “risk-taking behavior,” “sex addiction,” and “sports addiction” in the title, abstract, or keywords.
Eligibility Criteria
Studies had to fulfill the following inclusion criteria to be included: the target problem was a BA; the intervention was performed using tDCS; the study was a clinical trial, as defined by the WHO (WHO, 2015)—including randomized controlled trials (RCTs), controlled trials, cohort studies, case-control studies and multiple base-line studies. Exclusion criteria were: clinical studies about tDCS among SUDs; review and didactic articles; physiopathological studies and case reports.
Study Selection
First, all studies were screened based on their titles and abstracts. Second, the two reviewers read the full text of all studies identified in this search process. This work was carried out independently using the same bibliographic search. In the event of a disagreement between the two reviewers, the relevant studies were discussed (see Figure 1 for the study selection flow chart).
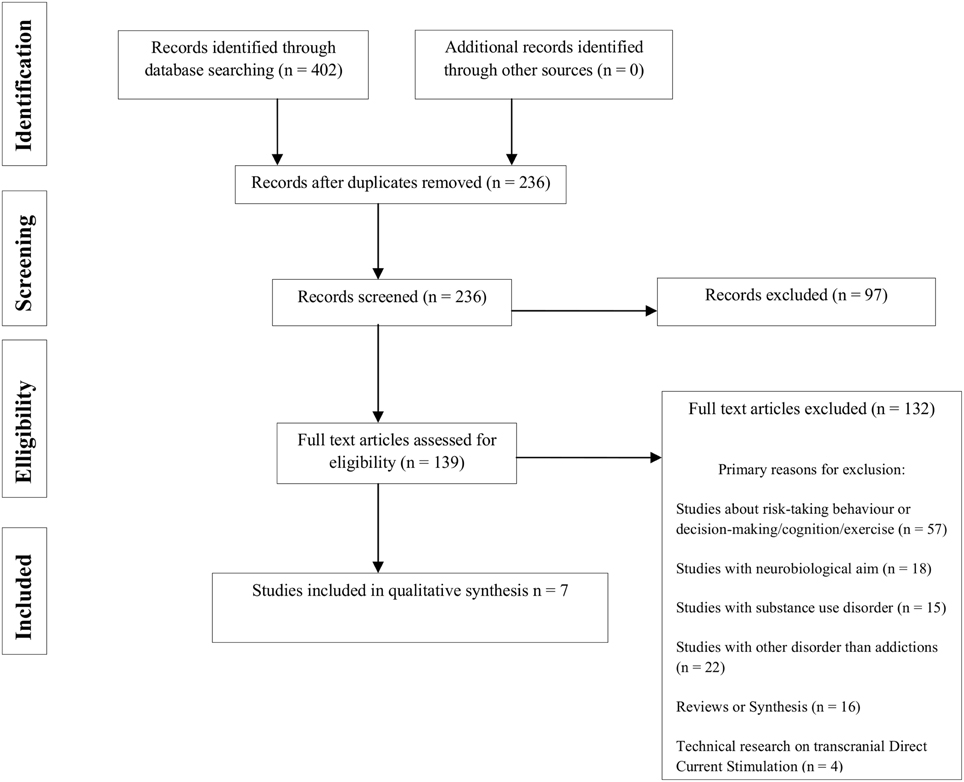
Figure 1. PRISMA flow chart of literature search.
Data Extraction
Extracted data included clinical, methodological, and technical considerations (see Tables 1, 2).
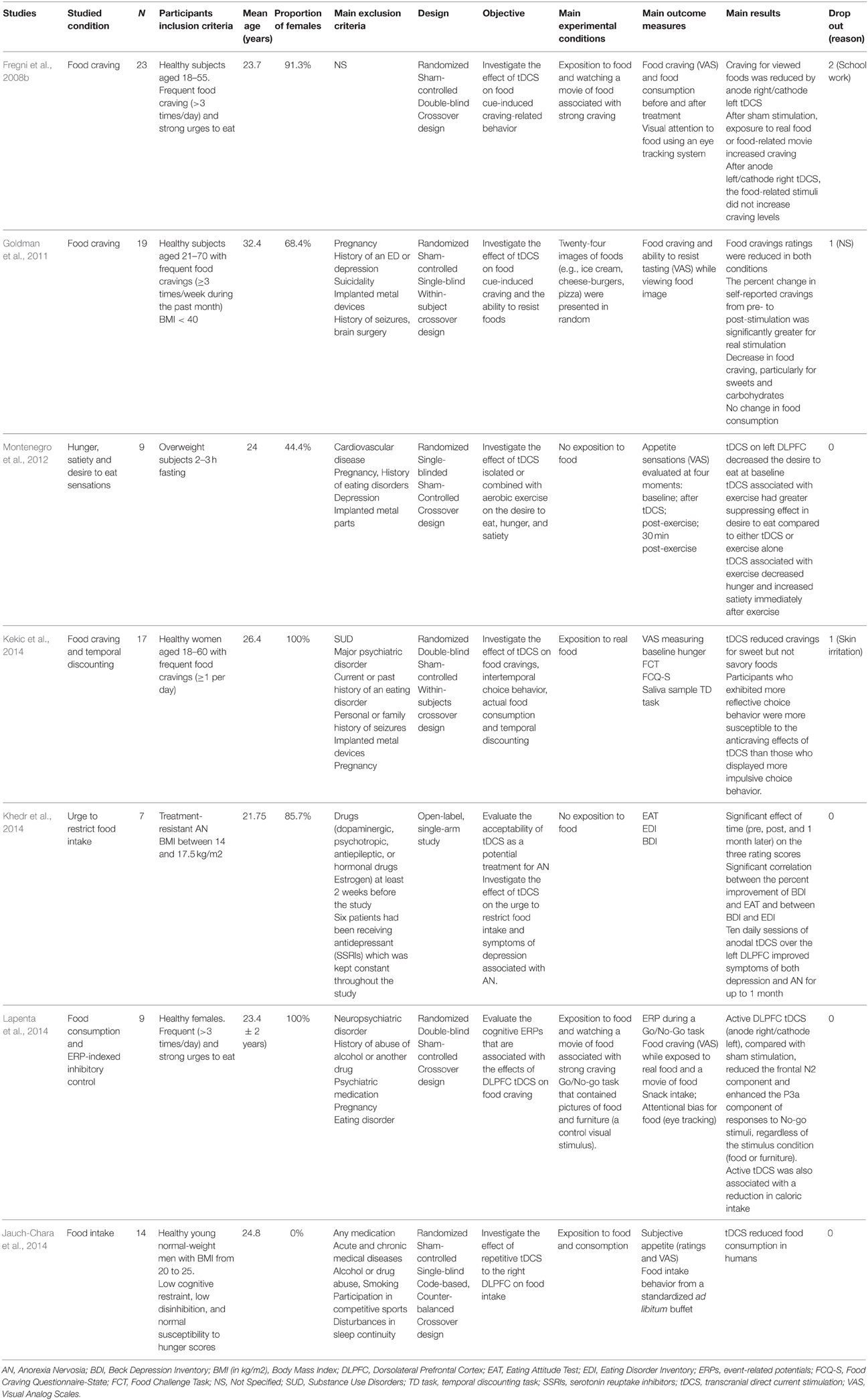
Table 1. Clinical trials of tDCS and behavioral addictions: general and clinical characteristics.
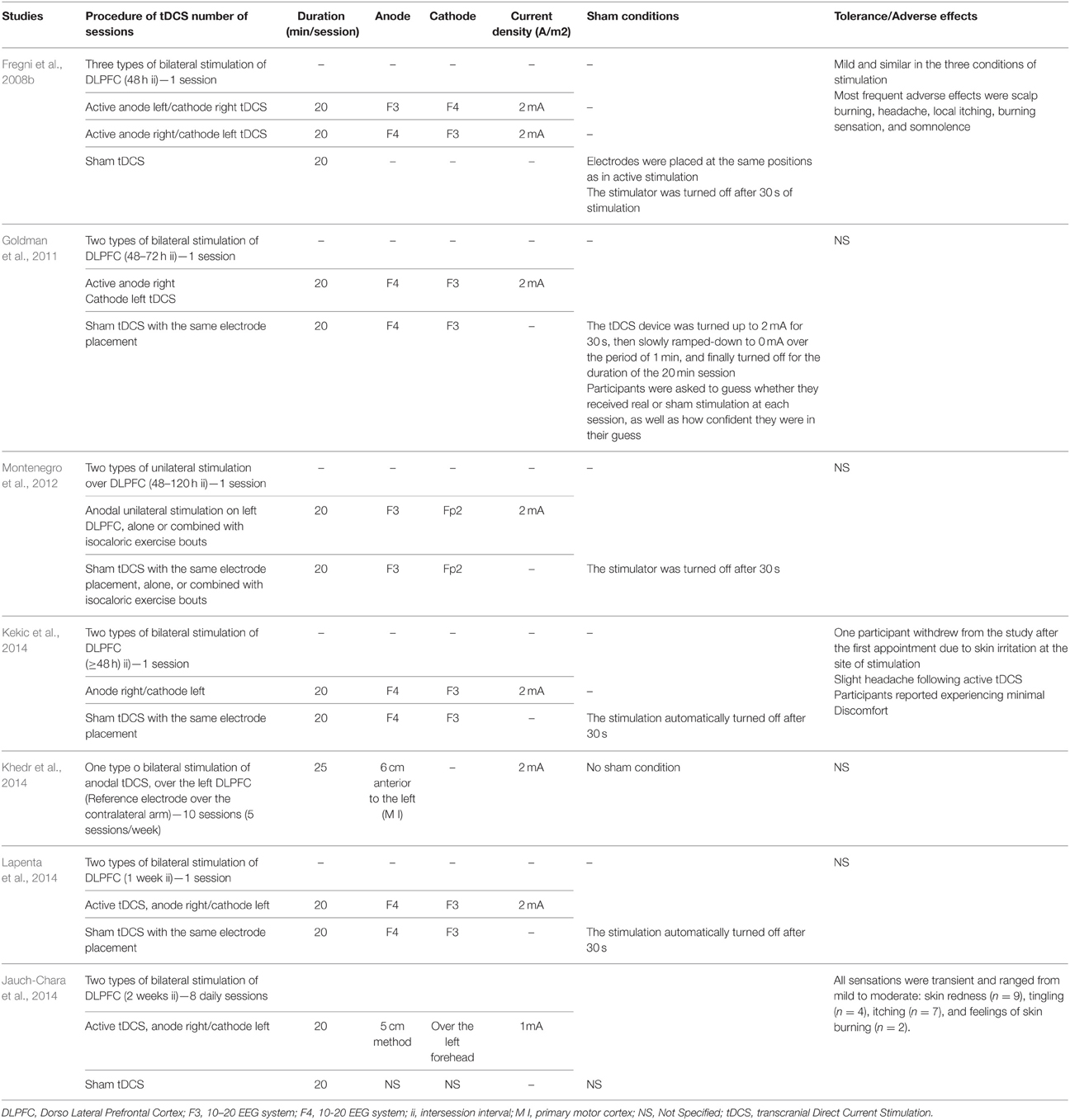
Table 2. Clinical trials of tDCS and behavioral addictions: technical characteristics.
Results
The initial search identified 402 independent articles. Seven articles met the criteria for inclusion. Food craving, in different clinical conditions was the only symptom to be tested. To the best of our knowledge, we found that tDCS has not yet been tested for the following BAs: compulsive buying/shopping, pathological gambling, gambling disorder, Internet addition, video game addiction, sex addiction and sports addiction.
Efficacy of tDCS in Behavioral Addictions
The main characteristics of the studies are summarized in Table 1.
Six out of the seven published studies (Fregni et al., 2008b; Goldman et al., 2011; Montenegro et al., 2012; Jauch-Chara et al., 2014; Kekic et al., 2014; Lapenta et al., 2014) have demonstrated the efficacy of tDCS applied to the DLPFC in reducing food craving. Khedr et al. reported an improvement in anorexic conducts (Khedr et al., 2014). Two of these studies were led by the same team (Fregni et al., 2008b; Lapenta et al., 2014) with the same design. All studies but one (Khedr et al., 2014) were blinded, randomized, and controlled. The used sample sizes vary between 7 (Khedr et al., 2014) and 23 (Fregni et al., 2008b) subjects. The participants were majoritarily women aged less than 30 years old on average, in good health, and with frequent food cravings. Only one study included overweight patients (Montenegro et al., 2012), and only one included anorexic patients (Khedr et al., 2014). In all studies but two (Montenegro et al., 2012; Khedr et al., 2014), the craving was induced visually, either with images, or with real food. The craving was induced through visual stimuli before and after stimulation in four of the seven studies (Fregni et al., 2008b; Goldman et al., 2011; Kekic et al., 2014; Lapenta et al., 2014). One of the studies repeated the induction after half of the stimulation time (Goldman et al., 2011). Three studies used exposure to real, high-calorie food, combined with one or two short movies showing high-calorie foods (Fregni et al., 2008b; Kekic et al., 2014; Lapenta et al., 2014). One study used pictures of high calorie food items to induce craving (Goldman et al., 2011). Both types of craving induction were reported to lead to increased craving. The level of food craving was usually measured before and after stimulation by means of visual analog scales (VAS) with the exception of one study which did not assess craving at all (Khedr et al., 2014). Some studies used additional measures such as eye tracking (Fregni et al., 2008b; Lapenta et al., 2014) or the Food Craving Questionnaire-State (Kekic et al., 2014). Five studies assessed actual food intake after stimulation using a bogus taste test (Fregni et al., 2008b; Goldman et al., 2011; Jauch-Chara et al., 2014; Kekic et al., 2014; Lapenta et al., 2014).
Further assessment methods were also used, either clinical with specific impulsivity scales (Kekic et al., 2014), or physiological like visual attention, measured by eye tracking (Fregni et al., 2008b), salivary cortisol levels (Kekic et al., 2014) or event-related potentials (Lapenta et al., 2014).
tDCS Technical Procedures
The results are summarized in Table 2.
Most studies tested the effect of just one active tDCS session vs. a sham tDCS session (20 min, 2 mA) on food craving. No cortical target other than the DLPFC was tested. Electrodes were most often placed with the anode on the right and the cathode on the left, respectively on F4 and F3 according to the International 10–20 System. Three teams placed them the other way around (cathode on the right and anode on the left) (Fregni et al., 2008b; Montenegro et al., 2012; Khedr et al., 2014). Montenegro and colleagues had two comparing arms (active tDCS and placebo) (Montenegro et al., 2012), whereas Fregni et al. had three comparing arms (anode/right and cathode/left; anode/left and cathode/right; placebo) (Fregni et al., 2008b). The interval between two sessions (active and placebo) ranges from 48 h to a week, to avoid a carry-over effect. The placebo method was described more or less precisely in all studies but one (Jauch-Chara et al., 2014). Tolerance and side effects were reported in 50% of studies (Fregni et al., 2008b; Jauch-Chara et al., 2014; Kekic et al., 2014).
Discussion
General Instructions
The initial works on tDCS in BAs are recent, and started around the same period (Fregni et al., 2008b) as studies on tDCS in SUDs (Boggio et al., 2008; Fregni et al., 2008a). However, they have not generated the same intererest overtime, so that the application of tDCS in SUDs has been much more investigated than tDCS in BAs. Works on tDCS in BAs were first and only interested in eating behavior, based on the model of rTMS, which is another NIBS which efficacy in BAs was first tested in eating disorders (Grall-Bronnec and Sauvaget, 2014). Whether through rTMS or tDCS, no study has been conducted to this day on other BAs (pathological gambling, sexual addiction, sports addiction, Internet addiction, compulsive shopping) (Grall-Bronnec and Sauvaget, 2014). Furthermore, although tDCS is a more manageable and less expensive means than rTMS (Brunoni et al., 2013), we observe that fewer studies are conducted with tDCS in the field of BAs and SUD compared to rTMS (Grall-Bronnec and Sauvaget, 2014). The later development of tDCS could explain the smaller number of studies.
tDCS is found effective in reducing craving in BAs in controlled studies comparing stimulation vs. placebo, until now for food craving. These results point in the same direction as those of tDCS for SUDs, which have been consolidated by a recent meta-analysis arguing that applying NIBS to the DLPFC decreases craving levels in substance dependence (Jansen et al., 2013), without any significant difference between rTMS and tDCS. However, the efficacy of tDCS must be discussed in light of methodological and technical considerations. All possible biases have been discussed (see Table 3).
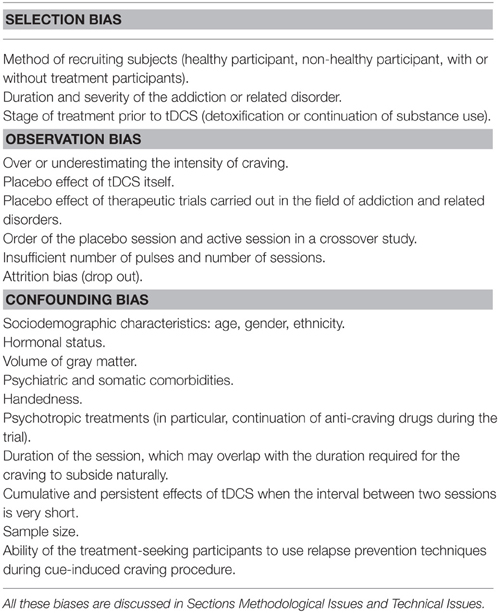
Table 3. Main sources of bias in the studies of tDCS in behavioral addictions.
Methodological Issues
Characteristics of the Participants
Health status of the participants
Patient inclusion criteria can be relatively confusing: indeed, most participants are defined as “healthy” subjects, whereas the study aims at investigating the effect of brain stimulation on food craving, which is a clearly defined disorder from a psychopathological standpoint. The frequency of food craving is relatively low in tDCS studies. It varies, depending on the studies, from 1/day (Kekic et al., 2014) to 3/day (Fregni et al., 2008b; Goldman et al., 2011; Lapenta et al., 2014). Moreover, most patients included in studies on tDCS have a normal weight, apart from one study in obese patients (Montenegro et al., 2012) and another in patients suffering from anorexia nervosa (Khedr et al., 2014). Only Jauch-Chara et al.'s study can be considered as conducted in a physiological condition, since the included subjects had a normal body mass index and no daily food craving (Jauch-Chara et al., 2014). In fact, the studies were more interested in the process of food craving than in full-syndrome eating disorders. Patient morphology could be an important criterion to take into account in configurating tDCS. This precise point is developed in the “Technical Issues” Section.
Age
Participants are rather young (< 40 years old). The age of the studied population is important to interpret results since the clinical expression of craving is likely to evolve with age. Age is also a factor in the variation of cortical excitability (Feil and Zangen, 2010; Clark and Taylor, 2011).
Gender
Apart from Jauch-Chara et al.'s study (2014) in which all subjects are male, the other studies mainly included women, either on purpose (Kekic et al., 2014; Lapenta et al., 2014) or because they were predominant (Fregni et al., 2008b; Goldman et al., 2011; Montenegro et al., 2012; Khedr et al., 2014). A higher prevalence of food craving in women than in men explains the sex-ratio imbalance between patients included in these studies (Mitchison and Hay, 2014). Moreover, the fluctuation of eating behavior throughout the menstrual cycle could affect the result of the studies (Lester et al., 2003). The sexual hormonal variations could also affect the functional cerebral asymmetries (Neufang et al., 2009). The right hemispheric predominance in spatial attention, which seems linked to gender, would disappear under the effect of left anodal tDCS (de Tommaso et al., 2014). Finally, a recent study showed that electric transmission of tDCS is different between men and women, mainly for bone density reasons (Russell et al., 2014).
Handedness
None of the studies analyzed in this review evoked the importance of this parameter in the interpretation of results, conversely to other NIBS works, whether on rTMS (Van den Eynde et al., 2012) or tDCS (Kasuga et al., 2015). Yet, the effects of tDCS could differ according to the handedness of stimulated subjects (Kasuga et al., 2015). The problem of hemispheric dominance remains complex, since the left hemisphere could be the dominant hemisphere in 95–99% of right-handed subjects, and in 70% of left-handed subjects (Corballis, 2014). Moreover, laterality has clinical relevance since left-handers are more at risk of developing addictive disorders (Sperling et al., 2000). Evaluating the hemispheric dominance thanks to a specific questionnaire focused on laterality (Oldfield, 1971) in patients included in studies involving NIBS would allow gathering new data on brain functioning.
Main exclusion criteria
The exclusion criteria are generally mentioned and detailed. Although contra-indications are usually exclusion criteria, in accordance with the literature (Brunoni et al., 2011), the psychiatric and somatic comorbidities can be confounding factors in evaluating the efficacy of tDCS. For example, in eating disorders, the conjoint improvement of depressive symptoms and obsessive-compulsive symptoms on the one hand, and of binge-eating and purging conducts on the other hand, could simply be due to a common physiopathological process rather than to a specific effect of tDCS on the addictive symptoms only (Khedr et al., 2014; Shiozawa et al., 2014). Finally, the use of medication, particularly psychotropic and anticraving drugs, should be considered, as they could interfere with the assessment of craving, but also with the efficacy of tDCS, through their action on cortical excitability. Selective serotonin reuptake inhibitors could indeed aid tDCS response (Nitsche et al., 2009).
Sample size
Among all examined studies, the sample size is always very small, ranging between 7 (Khedr et al., 2014) and 23 subjects (Fregni et al., 2008b). This is probably why all of them, except for two studies (Montenegro et al., 2012; Khedr et al., 2014), adopted a crossover design, to increase the statistical power of their work.
Cortical Excitability
tDCS modifies cortical excitability (Nitsche et al., 2008). The efficacy of tDCS thus depends on numerous factors, which have an influence on cortical excitability, such as age, gender, hormonal status, anxiety levels, lack of sleep, and the use of psychotropic drugs (either legal or illegal). Cortical excitability would also vary according to ethnic origins (Yi et al., 2014). The results of the studies should thus be discussed according to these parameters.
Design
All studies but one (Khedr et al., 2014) were designed following the rules of RCTs, which facilitates comparisons. Although food craving is the main evaluation criterion, some authors have underlined the importance of considering other target symptoms such as impulsivity (Kekic et al., 2014). In their studies, patients with “more reflective choice behavior” are more sensitive to the anti-craving effects of the tDCS than patients with “more impulsive choice behavior.” These results show that the craving involves multiple dimensions that interact with each other, and that can also be modified by tDCS.
The craving induction procedure differs between studies. Although the induction medium (either real or virtual) is most of the time visual, this may vary. Addressing other sense organs like olfaction may increase the external validity of craving induction methods. Although craving is not necessarily related to physiological hunger, food intake before the experimental session may be an important interfering factor. Most studies tried to control this variable, by asking participants to refrain from food intake for a period of time before the session, which varied between 2 and 6 h depending on the study design (Fregni et al., 2008b; Goldman et al., 2011; Montenegro et al., 2012; Jauch-Chara et al., 2014; Lapenta et al., 2014). Some also used a 24 h dietary recall protocol to assess previous food intake (Goldman et al., 2011; Montenegro et al., 2012). One study controlled food intake only by a VAS on hunger (Kekic et al., 2014), and another study did not control this factor at all (Khedr et al., 2014).
Technical Issues
General Considerations
The tDCS procedure is generally well-described and detailed, which allows for a better comparison between studies. Teams that consecutively conduct several studies tend to replicate the same protocol (Fregni et al., 2008b; Lapenta et al., 2014).
Stimulation Site
Only the DLPFC drew the researchers' attention, most often in the following setting: anode on the right DLPFC (excitation) and cathode on the left DLPFC (inhibition). The results of Lapenta et al.'s team suggest that stimulating the DLPFC could facilitate the inhibitory response and modify the connections between the cortical and subcortical structures (Lapenta et al., 2014).
The positive results both in overeating with the “anode on the right DLPFC and cathode on the left DLPFC” scheme and in food restriction with the “anode on the left DLPFC and cathode on the right DLPFC” scheme argue in favor of a different hemispheric functioning in eating disorders. In the case of overeating and obesity, increasing the activity of the right DLPFC and inhibiting the left DLPFC would help reducing the induced food craving. This could decrease appetite and restore food control mechanisms, in line with the “right brain hypothesis for obesity” theory (Alonso-Alonso and Pascual-Leone, 2007; Alonso-Alonso, 2013). In the case of food restriction, the hypothesis of an imbalanced interhemispheric balance (with hyperactive right frontal regions) combined with anorexia nervosa (Hecht, 2010) has been partly confirmed by Khedr's work (Khedr et al., 2014). The possible predominance of the right hemisphere in the genesis of an eating disorder has also been evoked in a post-lesional context (Uher and Treasure, 2005). These results are consistent with the works on rTMS that put forward the respective roles of the right and left DLPFC in the control of craving. Whereas, the left DLPFC seems to have a role in the control of craving (Hayashi et al., 2013), the right DLPFC seems to play a part in the inhibitory control of emotional impulses (Pripfl et al., 2013).
However, the studies published to this day do not all have the same methodology, clinical populations or objectives. The results they put forward are still at a very preliminary stage and do not allow concluding on a hemispheric specialization in eating disorders and in BAs generally speaking. Besides switching electrodes between the two hemispheres to test the two conditions (excitatory or inhibitory) (McClelland et al., 2013), it would be interesting to stimulate other cortical regions, such as the parietal cortex, which is a cerebral region that seems to be involved in body image (Gaudio and Quattrocchi, 2012).
The choice of the stimulation site must also take into account the neural loops involved in the studied BA. It seems more pertinent to choose the stimulation site based on the neural loops involved in the studied behavioral addiction, rather than sticking to a given cortical region.
General Design of the Sessions and tDCS Parameters
Apart from two studies (Jauch-Chara et al., 2014; Khedr et al., 2014), the included studies only tested the effects of one tDCS session. It can be assumed that repeating sessions could increase and sustain efficacy on craving and other eating disorder symptoms, as reported in studies on the treatment of depressive disorders (Shiozawa et al., 2014) and SUDs (Feil and Zangen, 2010; Tortella et al., 2015).
tDCS is generally described as easier to implement than rTMS. However, this should not overshadow the importance of some tDCS parameters, which might have an influence on the results (Horvath et al., 2014).
Indeed, beside the optimal position of the electrodes, current intensity, and stimulation duration, other parameters should be taken into account, such as hair thickness, sweat (Horvath et al., 2014), but also electrode size (Russell et al., 2014; Nasseri et al., 2015), with individual differences (Russell et al., 2013). The location of the reference electrode may also have an impact on tDCS effects (Nasseri et al., 2015). The electric current in tDCS is not relayed in the same way by the different anatomical structures it passes through (Shahid et al., 2014). For example, regarding adipose tissue, Truong et al. have showed that, based on the MRI analysis of five patients' adipose tissue, that tissue could influence the intensity of tDCS electric current in the brain (Truong et al., 2013). Furthermore, patients suffering from eating disorders could present changes in gray matter and its thickness (Frank et al., 2013). Consequently, the transmission of tDCS electric current could be altered, and the results could differ from the intended target.
Sham Procedure
The placebo conditions, as described more or less precisely in all studies are similar, and follow a validated method (Gandiga et al., 2006). The placebo tDCS method seems more reliable and easier to implement than the rTMS placebo method, thus limiting the interpretation biases (Grall-Bronnec and Sauvaget, 2014). However, some authors have evidenced that sham tDCS was not as reliable as it seemed (Horvath et al., 2014).
Safety and Tolerance
When reported (Fregni et al., 2008; Jauch-Chara et al., 2014), the side effects were similar to those found in literature (Brunoni et al., 2011). Indeed, tDCS is generally known as a safe technique with mild and transient adverse effects (Brunoni et al., 2011). Even though seizures induced by tDCS are very rare (Ekici, 2015), subjects suffering from substance use addiction present an increased risk of seizures, especially during the alcohol or benzodiazepine withdrawal periods (Leach et al., 2012). The tDCS techniques could be tolerated better by patients suffering from BAs, as they are less likely to have seizures than patients with a SUD.
Conclusion and Future Perspectives
The application field of tDCS in BAs is for now restricted to the study of food craving, mainly in so-called “sane” participants, i.e., who do not fulfill the diagnostic criteria of characterized eating disorders. These studies show that stimulating the right DLPFC and inhibiting the left DLPFC reduces the induced food craving.
Therefore, there is a clinical interest in having a symptomatic treatment of craving, by considering tDCS as a complementary therapy to the standard treatment of eating disorder. On a neuroscientific level, tDCS could reduce inter-hemispheric imbalance, since data report overactivity in the frontal area of the right hemisphere in anorexia nervosa, as ventured by Hecht in 2010 (Hecht, 2010), and recently comforted by Khedr et al.'s work (2014). Also, other therapeutic effects could be observed with tDCS, especially on food restriction (Jauch-Chara et al., 2014).
The rationale of expanding tDCS work to other behavioral addictions is justified by its positive effect in sane subjects on their decision-making process (improved) and on their risk-taking (reduced) (Fecteau et al., 2007a,b), both strongly linked to addictive issues. Indeed, the recent works on tDCS in the field of cognition and impulsivity (Feil and Zangen, 2010; Elmasry et al., 2015) demonstrate promising therapeutic prospects for tDCS.
The tDCS techniques offer many undeniable advantages in treating BAs: they are non-invasive, well-tolerated, implemented through a portable, and compact device, and relatively cheap compared to other techniques (such as rTMS). Thus, tDCS could be implemented in outpatient structures specialized in addictions.
Several research avenues must be explored, in line with the research conducted with rTMS. The effects of tDCS in other BAs could be explored, like pathological gambling, sports addiction, sexual addictions, or video games. It would also be particularly interesting to evaluate the effects of tDCS in the longer term, whether on craving or on other BA symptoms, such as maintained abstinence.
Finally, combining neuroimaging and electrophysiology studies (Val-Laillet et al., 2015; Wolz et al., 2015) to tDCS studies should be considered, to understand better the pathophysiological mechanisms involved in BAs, and allow for a better identification of targets and stimulation parameters.
In summary, the main goals of tDCS application in BAs are all at once therapeutic, by modulating craving, impulsivity, executive functions and physiopathological, by enhancing the knowledge of neurophysiological basis of BAs.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to thank warmly A. F. Goalic for her assistance in the literature search and Hélène Henderson for language editing. This manuscript was partially supported by grants from Instituto Salud Carlos III (PI14/290 and CIBERobn) and Fondo Europeo de Desarrollo Regional (FEDER), but also PROMOSAM (PSI2014-56303-REDT), Spain. IW was supported by a predoctoral grant of AGAUR (2014FI_B 00372). CIBERobn and CIBERsam are both initiatives of ISCIII.
References
Achab, S., and Khazaal, Y. (2011). Psychopharmacological treatment in pathological gambling: a critical review. Curr. Pharm. Des. 17, 1389–1395. doi: 10.2174/138161211796150774
Addolorato, G., Leggio, L., Hopf, F. W., Diana, M., and Bonci, A. (2012). Novel therapeu-tic strategies for alcohol and drug addiction: focus on GABA, ion channels andtranscranial magnetic stimulation. Neuropsychopharmacology 37, 163–177. doi: 10.1038/npp.2011.216
Alonso-Alonso, M. (2013). Translating tDCS into the field of obesity: mechanism-driven approaches. Front. Hum. Neurosci. 7:512. doi: 10.3389/fnhum.2013.00512
Alonso-Alonso, M., and Pascual-Leone, A. (2007). The right brain hypothesis for obesity. JAMA 297, 1819–1822. doi: 10.1001/jama.297.16.1819
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Washington, DC: Association AP, 947 p.
Blum, K., Febo, M., McLaughlin, T., Cronjé, F. J., Han, D., and Gold, S. M. (2014). Hatching the behavioral addiction egg: Reward Deficiency Solution System (RDSS)™ as a function of dopaminergic neurogenetics and brain functional connectivity linking all addictions under a common rubric. J. Behav. Addict. 3, 149–156. doi: 10.1556/JBA.3.2014.019
Boggio, P. S., Campanhã, C., Valasek, C. A., Fecteau, S., Pascual-Leone, A., and Fregni, F. (2010). Modulation of decision-making in a gambling task in older adults with transcranial direct current stimulation. Eur. J. Neurosci. 31, 593–597. doi: 10.1111/j.1460-9568.2010.07080.x
Boggio, P. S., Sultani, N., Fecteau, S., Merabet, L., Mecca, T., Pascual-Leone, A., et al. (2008). Prefrontal cortex modulation using transcranial DC stimulation reduces alcohol craving: a double-blind, sham-controlled study. Drug Alcohol Depend. 92, 55–60. doi: 10.1016/j.drugalcdep.2007.06.011
Brunoni, A. R., Amadera, J., Berbel, B., Volz, M. S., Rizzerio, B. G., and Fregni, F. (2011). A systematic review on reporting and assessment of adverse effects associated with transcranial direct current stimulation. Int. J. Neuropsychopharmacol. 14, 1133–1145. doi: 10.1017/S1461145710001690
Brunoni, A. R., Boggio, P. S., Ferrucci, R., Priori, A., and Fregni, F. (2013). Transcranial direct current stimulation: challenges, opportunities, and impact on psychiatry and neurorehabilitation. Front. Psychiatry 4:19. doi: 10.3389/fpsyt.2013.00019
Chib, V. S., Yun, K., Takahashi, H., and Shimojo, S. (2013). Noninvasive remote activation of the ventral midbrain by transcranial direct current stimulation of prefrontal cortex. Transl. Psychiatry 3:e268. doi: 10.1038/tp.2013.44
Clark, B. C., and Taylor, J. L. (2011). Age-related changes in motor cortical properties and voluntary activation of skeletal muscle. Curr. Aging Sci. 4, 192–199. doi: 10.2174/1874609811104030192
Corballis, M. C. (2014). Left brain, right brain: facts and fantasies. PLoS Biol. 12:e1001767. doi: 10.1371/journal.pbio.1001767
da Silva, M. C., Conti, C. L., Klauss, J., Alves, L. G., do Nascimento Cavalcante, H. M., Fregni, F., et al. (2013). Behavioral effects of transcranial direct current stimulation (tDCS) induced dorsolateral prefrontal cortex plasticity in alcohol dependence. J. Physiol. Paris 107, 493–502. doi: 10.1016/j.jphysparis.2013.07.003
Davis, C., and Carter, J. C. (2009). Compulsive overeating as an addiction disorder. A review of theory and evidence. Appetite 53, 1–8. doi: 10.1016/j.appet.2009.05.018
de Tommaso, M., Invitto, S., Ricci, K., Lucchese, V., Delussi, M., Quattromini, P., et al. (2014). Effects of anodal TDCS stimulation of left parietal cortex on visual spatial attention tasks in men and women across menstrual cycle. Neurosci. Lett. 574, 21–25. doi: 10.1016/j.neulet.2014.05.014
Ekici, B. (2015). Transcranial direct current stimulation-induced seizure: analysis of a case. Clin. EEG Neurosci. 46, 169. doi: 10.1177/1550059414540647
Elmasry, J., Loo, C., and Martin, D. (2015). A systematic review of transcranial electrical stimulation combined with cognitive training. Restor. Neurol. Neurosci. 33, 263–278. doi: 10.3233/RNN-140473
Farré, J. M., Fernández-Aranda, F., Granero, R., Aragay, N., Mallorquí-Bague, N., Ferrer, V., et al. (2015). Sex addiction and gambling disorder: similarities and differences. Compr. Psychiatry 56, 59–68. doi: 10.1016/j.comppsych.2014.10.002
Fecteau, S., Agosta, S., Hone-Blanchet, A., Fregni, F., Boggio, P., Ciraulo, D., et al. (2014). Modulation of smoking and decision-making behaviors with transcranial direct current stimulation in tobacco smokers: a preliminary study. Drug Alcohol Depend. 140, 78–84. doi: 10.1016/j.drugalcdep.2014.03.036
Fecteau, S., Fregni, F., Boggio, P. S., Camprodon, J. A., and Pascual-Leone, A. (2010). Neuromodulation of decision-making in the addictive brain. Subst. Use Misuse 45, 1766–1786. doi: 10.3109/10826084.2010.482434
Fecteau, S., Knoch, D., Fregni, F., Sultani, N., Boggio, P., and Pascual-Leone, A. (2007a). Diminishing risk-taking behavior by modulating activity in the prefrontal cortex: a direct current stimulation study. J. Neurosci. 27, 12500–12505. doi: 10.1523/JNEUROSCI.3283-07.2007
Fecteau, S., Pascual-Leone, A., Zald, D. H., Liguori, P., Théoret, H., Boggio, P. S., et al. (2007b). Activation of prefrontal cortex by transcranial direct current stimulation reduces appetite for risk during ambiguous decision making. J. Neurosci. 27, 6212–6218. doi: 10.1523/JNEUROSCI.0314-07.2007
Feil, J., and Zangen, A. (2010). Brain stimulation in the study and treatment of addiction. Neurosci. Biobehav. Rev. 34, 559–574. doi: 10.1016/j.neubiorev.2009.11.006
Fernández-Serrano, M. J., Pérez-García, M., Perales, J. C., and Verdejo-García, A. (2010). Prevalence of executive dysfunction in cocaine, heroin and alcohol usersenrolled in therapeutic communities. Eur. J. Pharmacol. 626, 104–112 doi: 10.1016/j.ejphar.2009.10.019
Fox, P., Ingham, R., George, M. S., Mayberg, H., Ingham, J., Roby, J., et al. (1997). Imaging human intra-cerebral connectivity by PET during TMS Neuroreport 8, 2787–2791. doi: 10.1097/00001756-199708180-00027
Frank, G. K., Shott, M. E., Hagman, J. O., and Mittal, V. A. (2013). Alterations in brain structures related to taste reward circuitry in ill and recovered anorexia nervosa and in bulimia nervosa. Am. J. Psychiatry 170, 1152–1160. doi: 10.1176/appi.ajp.2013.12101294
Fregni, F., Liguori, P., Fecteau, S., Nitsche, M. A., Pascual-Leone, A., and Boggio, P. S. (2008a). Cortical stimulation of the prefrontal cortex with transcranial direct current stimulation reduces cue-provoked smoking craving: a randomized, sham-controlled study. J. Clin. Psychiatry 69, 32–40. doi: 10.4088/JCP.v69n0105
Fregni, F., Orsati, F., Pedrosa, W., Fecteau, S., Tome, F. A. M., Nitsche, M. A., et al. (2008b). Transcranial direct current stimulation of the prefrontal cortex modulates the desire for specific foods. Appetite 51, 34–41. doi: 10.1016/j.appet.2007.09.016
Friederich, H. C., Wu, M., Simon, J. J., and Herzog, W. (2013). Neurocircuit function in eating disorders. Int. J. Eat. Disord. 46, 425–432. doi: 10.1002/eat.22099
Gandiga, P. C., Hummel, F. C., and Cohen, L. G. (2006). Transcranial DC stimulation (tDCS): a tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 117, 845–850. doi: 10.1016/j.clinph.2005.12.003
García-García, I., Horstmann, A., Jurado, M. A., Garolera, M., Chaudhry, S. J., Margulies, D. S., et al. (2014). Reward processing in obesity, substance addiction and non-substance addiction. Obes. Rev. 15, 853–869. doi: 10.1111/obr.12221
Gaudio, S., and Quattrocchi, C. C. (2012). Neural basis of a multidimensional model of body image distortion in anorexia nervosa. Neurosci. Biobehav. Rev. 36, 1839–1847. doi: 10.1016/j.neubiorev.2012.05.003
Gearhardt, A. N., White, M. A., and Potenza, M. N. (2011). Binge eating disorder and food addiction. Curr. Drug Abuse Rev. 4, 201–207. doi: 10.2174/1874473711104030201
Goldman, R. L., Borckardt, J. J., Frohman, H. A., O'Neil, P. M., Madan, A., Campbell, L. K., et al. (2011). Prefrontal cortex transcranial direct current stimulation (tDCS) temporarily reduces food cravings and increases the self-reported ability to resist food in adults with frequent food craving. Appetite 56, 741–746. doi: 10.1016/j.appet.2011.02.013
Goldstein, R. Z., and Volkow, N. D. (2002). Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am. J. Psychiatry 159, 1642–1652. doi: 10.1176/appi.ajp.159.10.1642
Goudriaan, A. E., de Ruiter, M. B., van den Brink, W., Oosterlaan, J., and Veltman, D. J. (2012). Brain activation patterns associated with cue reactivity and craving in abstinent problem gamblers, heavy smokers and healthy controls: an fMRI study. Addict. Biol. 15, 491–503. doi: 10.1111/j.1369-1600.2010.00242.x
Grall-Bronnec, M., and Sauvaget, A. (2014). The use of repetitive transcranial magnetic stimulation for modulating craving and addictive behaviours: a critical literature review of efficacy, technical and methodological considerations. Neurosci. Biobehav. Rev. 47C, 592–613. doi: 10.1016/j.neubiorev.2014.10.013
Hanlon, C. A., Canterberry, M., Taylor, J. J., DeVries, W., Li, X., Brown, T. R., et al. (2013). Probing the frontostriatal loops involved in executive and limbic processing via interleaved TMS and functional MRI at two prefrontal locations: a pilot study. PLoS ONE 8:e67917. doi: 10.1371/journal.pone.0067917
Hayashi, T., Ko, J. H., Strafella, A. P., and Dagher, A. (2013). Dorsolateral prefrontal and orbitofrontal cortex interactions during self-control of cigarette craving. Proc. Natl. Acad. Sci. U.S.A. 110, 4422–4427. doi: 10.1073/pnas.1212185110
Hebebrand, J., Albayrak, Ö., Adan, R., Antel, J., Dieguez, C., de Jong, J., et al. (2014). “Eating addiction”, rather than “food addiction,” better captures addictive-like eating behavior. Neurosci. Biobehav. Rev. 47, 295–306. doi: 10.1016/j.neubiorev.2014.08.016
Hecht, D. (2010). Transcranial direct current stimulation in the treatment of anorexia. Med. Hypotheses 74, 1044–1047. doi: 10.1016/j.mehy.2009.12.032
Higgins, E. S., and George, M. S. (2009). Brain Stimulation Therapies for Clinicians. 1st Edn. Arlington, TX: APPI.
Horvath, J. C., Carter, O., and Forte, J. D. (2014). Transcranial direct current stimulation: five important issues we aren't discussing (but probably should be). Front. Syst. Neurosci. 8:2. doi: 10.3389/fnsys.2014.00002
Jansen, J. M., Daams, J. G., Koeter, M. W. J., Veltman, D. J., van den Brink, W., and Goudriaan, A. E. (2013). Effects of non-invasive neurostimulation on craving: a meta-analysis. Neurosci. Biobehav. Rev. 37, 2472–2480. doi: 10.1016/j.neubiorev.2013.07.009
Jauch-Chara, K., Kistenmacher, A., Herzog, N., Schwarz, M., Schweiger, U., and Oltmanns, K. M. (2014). Repetitive electric brain stimulation reduces food intake in humans. Am. J. Clin. Nutr. 100, 1003–1009. doi: 10.3945/ajcn.113.075481
Jiménez-Murcia, S., Granero, R., Moragas, L., Steiger, H., Israel, M., Aymamí, N., et al. (2015). Differences and similarities between bulimia nervosa, compulsive buying and gambling disorder. Eur. Eat. Disord. Rev. 23, 111–118.
Kasuga, S., Matsushika, Y., Kasashima-Shindo, Y., Kamatani, D., Fujiwara, T., Liu, M., et al. (2015). Transcranial direct current stimulation enhances mu rhythm desynchronization during motor imagery that depends on handedness. Laterality 20, 453–468. doi: 10.1080/1357650X.2014.998679
Kaye, W. H., Fudge, J. L., and Paulus, M. (2009). New insights into symptoms and neurocircuit function of anorexia nervosa. Nat. Rev. Neurosci. 10, 573–584. doi: 10.1038/nrn2682
Keck, M. E., Welt, T., Müller, M. B., Erhardt, A., Ohl, F., Toschi, N., et al. (2002). Repetitive transcranial magnetic stimulation increases the release of dopamine in the mesolimbic and mesostriatal system. Neuropharmacology 43, 101–109. doi: 10.1016/S0028-3908(02)00069-2
Kekic, M., McClelland, J., Campbell, I., Nestler, S., Rubia, K., David, A. S., et al. (2014). The effects of prefrontal cortex transcranial direct current stimulation (tDCS) on food craving and temporal discounting in women with frequent food cravings. Appetite 78, 55–62. doi: 10.1016/j.appet.2014.03.010
Khedr, E. M., Elfetoh, N. A., Ali, A. M., and Noamany, M. (2014). Anodal transcranial direct current stimulation over the dorsolateral prefrontal cortex improves anorexia nervosa: a pilot study. Restor. Neurol. Neurosci. 32, 789–797. doi: 10.3233/RNN-140392
Knoch, D., Nitsche, M. A., Fischbacher, U., Eisenegger, C., Pascual-Leone, A., and Fehr, E. (2008). Studying the neurobiology of social interaction with transcranial direct current stimulation–the example of punishing unfairness. Cereb. Cortex 18, 1987–1990. doi: 10.1093/cercor/bhm237
Kuo, M.-F., Paulus, W., and Nitsche, M. A. (2014). Therapeutic effects of non-invasive brain stimulation with direct currents (tDCS) in neuropsychiatric diseases. Neuroimage 85(Pt 3), 948–960. doi: 10.1016/j.neuroimage.2013.05.117
Lapenta, O. M., Sierve, K., de Macedo, E. C., Fregni, F., and Boggio, P. S. (2014). Transcranial direct current stimulation modulates ERP-indexed inhibitory control and reduces food consumption. Appetite 83, 42–48. doi: 10.1016/j.appet.2014.08.005
Leach, J. P., Mohanraj, R., and Borland, W. (2012). Alcohol and drugs in epilepsy: pathophysiology, presentation, possibilities, and prevention. Epilepsia 53(Suppl. 4), 48–57. doi: 10.1111/j.1528-1167.2012.03613.x
Lester, N. A., Keel, P. K., and Lipson, S. F. (2003). Symptom fluctuation in bulimia nervosa: relation to menstrual-cycle phase and cortisol levels. Psychol. Med. 33, 51–60. doi: 10.1017/S0033291702006815
Marazziti, D., Presta, S., Baroni, S., Silvestri, S., and Dell'Osso, L. (2014). Behavioral addictions: a novel challenge for psychopharmacology. CNS Spectr. 19, 486–495. doi: 10.1017/S1092852913001041
McClelland, J., Bozhilova, N., Campbell, I., and Schmidt, U. (2013). A systematic review of the effects of neuromodulation on eating and body weight: evidence from human and animal studies. Eur. Eat. Disord. Rev. 21, 436–455. doi: 10.1002/erv.2256
Mitchison, D., and Hay, P. J. (2014). The epidemiology of eating disorders: genetic, environmental, and societal factors. Clin. Epidemiol. 6, 89–97. doi: 10.2147/CLEP.S40841
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J. Clin. Epidemiol. 62, 1006–1012. doi: 10.1016/j.jclinepi.2009.06.005
Montenegro, R. A., Okano, A. H., Cunha, F. A., Gurgel, J. L., Fontes, E. B., and Farinatti, P. T. V. (2012). Prefrontal cortex transcranial direct current stimulation associated with aerobic exercise change aspects of appetite sensation in overweight adults. Appetite 58, 333–338. doi: 10.1016/j.appet.2011.11.008
Naim-Feil, J., and Zangen, A. (2013). Addiction. Handb. Clin. Neurol. 116, 613–630. doi: 10.1016/B978-0-444-53497-2.00049-8
Nasseri, P., Nitsche, M. A., and Ekhtiari, H. (2015). A framework for categorizing electrode montages in transcranial direct current stimulation. Front. Hum. Neurosci. 9:54. doi: 10.3389/fnhum.2015.00054
Neufang, S., Specht, K., Hausmann, M., Güntürkün, O., Herpertz-Dahlmann, B., Fink, G. R., et al. (2009). Sex differences and the impact of steroid hormones on the developing human brain. Cereb. Cortex 19, 464–473. doi: 10.1093/cercor/bhn100
Nitsche, M. A., Cohen, L. G., Wassermann, E. M., Priori, A., Lang, N., Antal, A., et al. (2008). Transcranial direct current stimulation: state of the art 2008. Brain Stimul. 1, 206–223. doi: 10.1016/j.brs.2008.06.004
Nitsche, M. A., Kuo, M.-F., Karrasch, R., Wächter, B., Liebetanz, D., and Paulus, W. (2009). Serotonin affects transcranial direct current-induced neuroplasticity in humans. Biol. Psychiatry 66, 503–508. doi: 10.1016/j.biopsych.2009.03.022
O'Brien, C. (2011). Addiction and dependence in DSM-V. Addiction 106, 866–867. doi: 10.1111/j.1360-0443.2010.03144.x
Oldfield, R. C. (1971). The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9, 97–113. doi: 10.1016/0028-3932(71)90067-4
Potenza, M. N. (2014). Non-substance addictive behaviors in the context of DSM-5. Addict. Behav. 39, 1–2. doi: 10.1016/j.addbeh.2013.09.004
Pripfl, J., Neumann, R., Köhler, U., and Lamm, C. (2013). Effects of transcranial direct current stimulation on risky decision making are mediated by “hot” and “cold” decisions, personality, and hemisphere. Eur. J. Neurosci. 38, 3778–3785. doi: 10.1111/ejn.12375
Russell, M., Goodman, T., Wang, Q., Groshong, B., and Lyeth, B. G. (2014). Gender differences in current received during transcranial electrical stimulation. Front. Psychiatry 5:104. doi: 10.3389/fpsyt.2014.00104
Russell, M. J., Goodman, T., Pierson, R., Shepherd, S., Wang, Q., Groshong, B., et al. (2013). Individual differences in transcranial electrical stimulation current density. J. Biomed. Res. 27, 495–508. doi: 10.7555/JBR.27.20130074
Schulte, E. M., Avena, N. M., and Gearhardt, A. N. (2015). Which foods may be addictive? The roles of processing, fat content, and glycemic load. PLoS ONE 10:e0117959. doi: 10.1371/journal.pone.0117959
Shahid, S., Wen, P., and Ahfock, T. (2014). Assessment of electric field distribution in anisotropic cortical and subcortical regions under the influence of tDCS. Bioelectromagnetics 35, 41–57. doi: 10.1002/bem.21814
Shiozawa, P., Fregni, F., Benseñor, I. M., Lotufo, P. A., Berlim, M. T., Daskalakis, J. Z., et al. (2014). Transcranial direct current stimulation for major depression: an updated systematic review and meta-analysis. Int. J. Neuropsychopharmacol. 17, 1443–1452. doi: 10.1017/S1461145714000418
Skinner, M. D., and Aubin, H.-J. (2010). Craving's place in addiction theory: contributions of the major models. Neurosci. Biobehav. Rev. 34, 606–623. doi: 10.1016/j.neubiorev.2009.11.024
Sperling, W., Frank, H., Martus, P., Mader, R., Barocka, A., Walter, H., et al. (2000). The concept of abnormal hemispheric organization in addiction research. Alcohol Alcohol. 35, 394–399. doi: 10.1093/alcalc/35.4.394
Tortella, G., Casati, R., Aparicio, L. V. M., Mantovani, A., Senço, N., D'Urso, G., et al. (2015). Transcranial direct current stimulation in psychiatric disorders. World J. Psychiatry 5, 88–102. doi: 10.5498/wjp.v5.i1.88
Truong, D. Q., Magerowski, G., Blackburn, G. L., Bikson, M., and Alonso-Alonso, M. (2013). Computational modeling of transcranial direct current stimulation (tDCS) in obesity: impact of head fat and dose guidelines. Neuroimage Clin. 2, 759–766. doi: 10.1016/j.nicl.2013.05.011
Uher, R., and Treasure, J. (2005). Brain lesions and eating disorders. J. Neurol. Neurosurg. Psychiatr. 76, 852–857. doi: 10.1136/jnnp.2004.048819
Val-Laillet, D., Aarts, E., Weber, B., Ferrari, M., Quaresima, V., Stoeckel, L., et al. (2015). Neuroimaging and neuromodulation approaches to study eating behavior and prevent and treat eating disorders and obesity. Neuroimage Clin. 8, 1–31. doi: 10.1016/j.nicl.2015.03.016
Van den Eynde, F., Broadbent, H., Guillaume, S., Claudino, A., Campbell, I. C., and Schmidt, U. (2012). Handedness, repetitive transcranial magnetic stimulation and bulimic disorders. Eur. Psychiatry 27, 290–293. doi: 10.1016/j.eurpsy.2010.08.015
van Kuyck, K., Gérard, N., van Laere, K., Casteels, C., Pieters, G., Gabriëls, L., et al. (2009). Towards a neurocircuitry in anorexia nervosa: evidence from functional neuroimaging studies. J. Psychiatr. Res. 43, 1133–1145. doi: 10.1016/j.jpsychires.2009.04.005
von Hausswolff-Juhlin, Y., Brooks, S. J., and Larsson, M. (2015). The neurobiology of eating disorders–a clinical perspective. Acta Psychiatr. Scand. 131, 244–255. doi: 10.1111/acps.12335
WHO. (2015). WHO. Available online at: http://www.who.int/topics/research/en/ (Retrieved May 24, 2015).
Wolz, I., Fagundo, A. B., Treasure, J., and Fernández-Aranda, F. (2015). The processing of food stimuli in abnormal eating: a systematic review of electrophysiology. Eur. Eat. Disord. Rev. 23, 251–261. doi: 10.1002/erv.2366
Yi, X., Fisher, K. M., Lai, M., Mansoor, K., Bicker, R., and Baker, S. N. (2014). Differences between Han Chinese and Caucasians in transcranial magnetic stimulation parameters. Exp. Brain Res. 232, 545–553. doi: 10.1007/s00221-013-3763-2
Keywords: transcranial direct current stimulation, neuromodulation, behavioral addiction, craving, eating disorders, food craving, non-invasive brain stimulation
Citation: Sauvaget A, Trojak B, Bulteau S, Jiménez-Murcia S, Fernández-Aranda F, Wolz I, Menchón JM, Achab S, Vanelle J-M and Grall-Bronnec M (2015) Transcranial direct current stimulation (tDCS) in behavioral and food addiction: a systematic review of efficacy, technical, and methodological issues. Front. Neurosci. 9:349. doi: 10.3389/fnins.2015.00349
Received: 24 July 2015; Accepted: 14 September 2015;
Published: 09 October 2015.
Edited by:
Antonio Oliviero, Hospital Nacional de Parapléjicos, SpainReviewed by:
Andre R. Brunoni, Universidade de São Paulo, BrazilLaura Mordillo-Mateos, Hospital Nacional de Parapléjicos, Spain
Copyright © 2015 Sauvaget, Trojak, Bulteau, Jiménez-Murcia, Fernández-Aranda, Wolz, Menchón, Achab, Vanelle and Grall-Bronnec. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anne Sauvaget, Cappa Jacques Prevert, Addictology and Liaison-Psychiatry Department, Hôtel Dieu 3éme Nord, 1 Place Alexis-Ricordeau, 44000 Nantes, France,YW5uZS5zYXV2YWdldEBjaHUtbmFudGVzLmZy