 Jessica L. Krok-Schoen
Jessica L. Krok-Schoen Jill M. Oliveri1
Jill M. Oliveri1- 1Comprehensive Cancer Center, The Ohio State University, Columbus, OH, USA
- 2Division of Cancer Prevention and Control, Department of Internal Medicine, College of Medicine, The Ohio State University, Columbus, OH, USA
- 3Division of Epidemiology, College of Public Health, The Ohio State University, Columbus, OH, USA
Background: Patient navigation (PN) is a patient-centered health-care service delivery model that assists individuals, particularly the medically underserved, in overcoming barriers (e.g., personal, logistical, and system) to care across the cancer care continuum. In 2012, the American College of Surgeons Commission on Cancer (CoC) announced that health-care facilities seeking CoC-accreditation must have PN processes in place starting January 1, 2015. The CoC mandate, in light of the recent findings from centers within the Patient Navigation Research Program and the influx of PN interventions, warrants the present literature review.
Methods: PubMed and Medline were searched for studies published from January 2010 to October 2015, particularly those recent articles within the past 2 years, addressing PN for breast and gynecological cancers, and written in English. Search terms included patient navigation, navigation, navigator, cancer screening, clinical trials, cancer patient, cancer survivor, breast cancer, gynecological cancer, ovarian cancer, uterine cancer, vaginal cancer, and vulvar cancer.
Results: Consistent with prior reviews, PN was shown to be effective in helping women who receive cancer screenings, receive more timely diagnostic resolution after a breast and cervical cancer screening abnormality, initiate treatment sooner, receive proper treatment, and improve quality of life after cancer diagnosis. However, several limitations were observed. The majority of PN interventions focused on cancer screening and diagnostic resolution for breast cancer. As observed in prior reviews, methodological rigor (e.g., randomized controlled trial design) was lacking.
Conclusion: Future research opportunities include testing PN interventions in the post-treatment settings and among gynecological cancer patient populations, age-related barriers to effective PN, and collaborative efforts between community health workers and patient navigators as care goes across segments of the cancer control continuum. As PN programs continue to develop and become a standard of care, further research will be required to determine the effectiveness of cancer PN across the cancer care continuum, and in different patient populations.
Introduction
Profound advances in cancer screening, reductions in the prevalence of risk factors, and development of more effective treatments have positively contributed to increased longevity and quality of life among cancer survivors. Despite these improvements, disparities by race/ethnicity and socioeconomic status remain in cancer prevention, incidence, treatment, and mortality (1, 2). One approach to reduce cancer disparities is through patient navigation (PN). PN is a patient-centered, health-care service delivery model that assists individuals, particularly the medically underserved, in overcoming barriers to care (e.g., personal, logistical, system) across the cancer care continuum. PN is “navigation” in the health-care system compared to outreach, which is in the community and can use lay health advisors, community health workers (CHWs), etc. Typically, CHWs are trusted community members who provide information, support, and encouragement to receive screening tests (3). Previous intervention studies using CHWs to promote cancer screening have reported significantly increased screening rates for breast and cervical cancer (3, 4). CHWs and patient navigators differ in that CHWs work in the community, and their role ends when the patient enters the health-care facility. Patient navigators are typically housed in clinics; however, both the CHW and patient navigator complement each other in that they serve as a bridge between the health-care system and members of underserved communities.
Patient navigation began in 1990 by Harold Freeman who developed a PN program within a public hospital in Harlem, NY, USA to provide assistance to low-income women in need of breast cancer screening and timely follow-up to reduce diagnoses of late-stage breast cancer (5). Due to the promising results from Freeman’s initial PN program and continued evidence of effectiveness, PN has grown nationally as a standard of care (6, 7). PN studies have demonstrated that PN can improve rates of cancer screening (8, 9), ensure follow-up rates after an abnormal screening test (10, 11), and improve cancer care outcomes (i.e., time to treatment, quality of life) (12, 13).
Several recent literature reviews including Robinson-White et al. (14), Paskett et al. (15), and Wells et al. (16) have described the evolution of PN as a model to address cancer disparities. In 2011, a literature review by Paskett et al. (15) provided an update to the 2008 review by Wells et al. (16) on the efficacy of PN for cancer care. Paskett et al. (15) found that within the 3-year window since Wells’ review, the quantity of work in cancer PN literature was comparable to that of the previous years combined. In both reviews, most studies provided evidence for the effectiveness of increasing cancer screening rates including breast and gynecological cancers (15, 16). However, a paucity of research focusing on PN among cancer survivors during and after primary treatment and methodological limitations (i.e., lack of rigorous study design) of PN interventions were noted.
Since the 2011 literature review, many additional PN programs have been implemented especially those within the Patient Navigation Research Program (PNRP), funded by the National Cancer Institute (17) with support from the American Cancer Society (ACS). Active from 2005 to 2010, the PNRP provided funding to 10 institutions nationwide to develop and test interventions for follow-up and the initiation of treatment for four cancers for approved, validated screening tests: breast, cervical, prostate, and colorectal (18). Although any individual could benefit from PN, the PNRP focused efforts to identify and address barriers to care among populations experiencing cancer health disparities.
Breast and gynecological cancers are an optimal arena to use PN because of the known survival benefit of early detection through mammography and Pap tests with prompt follow-up of detected abnormalities. PN is particularly important in women’s cancers because of documented racial and ethnic disparities in cancer care across disease trajectories. In 2015, cervical cancer incidence rates among Hispanic women were the highest of any racial/ethnic group, 50% higher than those among non-Hispanic whites (19). In addition, the death rate for cervical cancer in black women was double than that in non-Hispanic white women (2.0 vs. 4.2 per 100,000, respectively) (19). It is notable that although white women had the highest breast cancer incidence rate, black women had the highest breast cancer mortality rate (19, 20). Thus, PN may be a strategy to help reduce these documented disparities.
The purpose of this review is to: (a) provide a summary of the recent literature (2010–2015) on PN and breast and gynecologic cancers from screening through treatment along the cancer care continuum; and (b) highlight research challenges and opportunities of PN that impact women’s health.
Methods
PubMed and Medline were searched for studies published from January 2010 to October 2015, particularly those recent articles within the past 2 years, addressing PN for breast and gynecological cancers and written in English. Only original studies reporting quantitative, qualitative, or mixed methods results regarding PN that dealt with cancer screening, diagnosis, treatment, clinical trials, or survivorship were included in this review. Editorials, abstracts, anecdotal reports, literature reviews, and articles lacking data from original research were excluded, as were articles that included non-breast/non-gynecological cancers and/or men in the analyses. Search terms included patient navigation, navigation, navigator, cancer screening, clinical trials, cancer patient, cancer survivor, breast cancer, gynecological cancer, ovarian cancer, uterine cancer, vaginal cancer, and vulvar cancer.
A total of 209 articles referencing PN in women’s cancers were found, of which 180 did not meet the inclusion criteria, resulting in 29 articles that met the criteria for inclusion in this review. Several notable PNRP articles were excluded because they included non-breast/non-gynecological cancer and men in their analyses (21–25). The 29 articles were then divided into categories along the cancer care continuum (screening, diagnostic resolution, and after primary diagnosis). The articles were reviewed and summarized by one study author (Jessica L. Krok-Schoen). Questions regarding inclusion were resolved by consensus among the other two authors (Jill M. Oliveri and Electra D. Paskett). Each article was reviewed, and the results presented are organized by placement along the cancer care continuum described above. Table 1 comprises a summary of published cancer PN studies (N = 29).
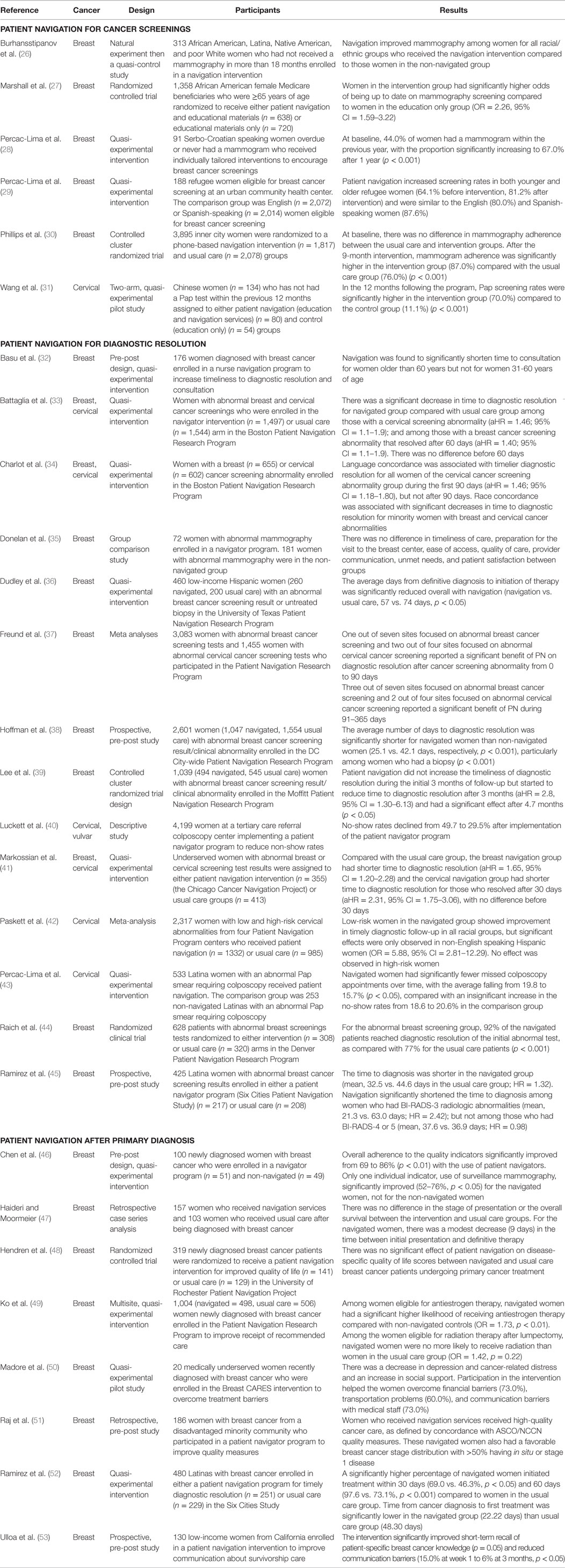
Table 1. Summary of published cancer patient navigation studies: 2010–2015.
Results
PN for Cancer Screening
The literature on PN interventions to increase breast cancer screening included five studies (26–30), with two randomized controlled trials (RCTs) (27, 30). In a large RCT with 3,895 inner city women, Phillips et al. (30) found no statistical difference in mammography adherence between the control (usual care) and PN intervention groups at baseline. After the 9-month intervention, mammogram adherence was significantly higher in the PN intervention group compared to the control group (87 vs. 76%, respectively, p < 0.001). Marshall et al. (27) implemented a RCT to increase breast cancer screening among 1,905 older African American Medicare beneficiaries. Women in the intervention group who received educational materials and PN services had significantly higher odds of being within guidelines for mammography screening at the end of the 2-year follow-up period compared to women in the control group who received only educational material [odds ratio (OR) = 2.26, 95% confidence interval (CI) = 1.59–3.22].
The other three studies (26, 28, 29) examined the effectiveness of PN interventions to increase breast cancer screening among diverse populations, including African American, Latina, Native American (26), immigrant (28, 29), and refugee (28, 29) women. Burhansstipanov et al. (26) implemented an education-based PN intervention to facilitate mammography screening for African American, Latina, Native American, and poor white women in the Greater Denver Metropolitan area. Statistically significant associations were found between having received the PN intervention and reporting a mammogram screening for all racial/ethnic groups (p < 0.05). A study by Percac-Lima et al. (28) implemented an educational, language concordant PN program for Serbo-Croatian refugees and immigrants to overcome barriers to breast cancer screening and support them in scheduling a mammogram. They found that, at baseline, 44% of women had a mammogram within the previous year, with the proportion increasing to 67% after 1-year (p = 0.001) of receiving the education-based PN intervention. Lastly, another study by Percac-Lima et al. (29) found that an education-based PN intervention to overcome barriers to breast cancer screening and information on how to obtain mammogram screening when needed among Somali, Arabic, or Serbo-Croatian refugee women improved mammography rates and significantly decreased disparities in screening rates between refugee and English- and Spanish-speaking women receiving care at the same health center.
One study in our review examined the impact of PN on screening rates for gynecological cancers. Wang et al. (31) found Chinese women in need of a Pap test reported significantly higher Pap test screening rates for those who received the PN intervention (education and PN services) compared to the control group (education only) (70 vs. 11.1%, respectively, p < 0.001).
PN for Diagnostic Resolution
Six studies (32, 35, 36, 38, 39, 45) were identified that focused on PN interventions to reduce time from abnormal breast cancer screening to diagnostic resolution. Of the six studies, one RCT by Lee et al. (39) examined the efficacy of PN among medically underserved populations in Tampa, FL, USA. Results showed a lagged effect of PN; PN did not increase the timeliness of diagnostic resolution during the initial 3 months of follow-up [adjusted hazard ratio (aHR) = 0.85, 95% CI = 0.64–1.13], but reduced the time to diagnostic resolution after 3 months (aHR = 2.8395% CI = 1.30–6.13) and had a significant effect (p < 0.05) after 4.7 months. Several quasi-experimental studies (32, 36, 38, 45) on PN and diagnostic resolution for abnormal breast cancer screening reported that PN significantly shortened time to diagnostic resolution compared to women who did not receive PN. One cohort study (35) exploring patient perspectives of clinical care and PN in follow-up of abnormal mammography reported no differences in the timeliness of care, preparation for the visit to the breast center, ease of access, quality of care, provider communication, unmet needs, and patient satisfaction between navigated and non-navigated groups.
Three studies, a meta-analysis (42), descriptive study (40), and quasi-experimental study (43), were published during the time period reviewed that examined PN for diagnostic resolution of an abnormal cervical cancer screening result. A recent meta-analysis by Paskett et al. (42) examined the effectiveness of PN for diagnostic resolution of an abnormal cervical cancer screening among four PNRP centers. Within these centers, low-risk women in the navigated group showed improvement in timely diagnostic follow-up in all racial groups, but statistically significant effects were only observed in non-English speaking Hispanic women (OR = 5.88, 95% CI = 2.81–12.29). No effect was observed in high-risk women. A pre-post study (40) implemented a PN program to reduce no-show rates at a colposcopy center. After implementation, no-show rates for abnormal Pap test follow-up declined from 49.7 to 29.5% (p < 0.0001). In another quasi-experimental study (43) focused on Latinas in need of abnormal Pap test follow-up, navigated women had significantly fewer missed colposcopy appointments over time (i.e., reduction from 19.8 to 15.7%; p = 0.02) compared with an insignificant increase in no-show rates from 18.6 to 20.6% in the comparison group.
Three studies (33, 34, 41) explored PN interventions with regard to diagnostic resolution after an abnormal breast or cervical cancer screening test. A study by Markossian et al. (41) reported PN for abnormal breast cancer screening was associated with shorter time to diagnostic resolution (aHR = 1.65, 95% CI = 1.20–2.28, p = 0.002). However, there was a lag in the effectiveness of PN regarding diagnostic resolution for abnormal cervical cancer screening. In the first 30 days, the difference between those in the PN arm vs. those in the comparison group was not significant. But, from days 31 to 365, women in the PN group experienced a shorter time to diagnostic resolution compared with those women who received usual care (aHR = 2.31, 95% CI = 1.75–3.06, p < 0.001). A similar trend was noted by Battaglia et al. (33) among participants with an abnormal breast and cervical cancer screening test. Conversely, Charlot et al. (34) found a language concordance PN intervention was associated with timelier resolution for the cervical cancer screening abnormalities group during the first 90 days (aHR = 1.46, 95% CI = 1.18–1.80), but not after 90 days. No significant difference was found between the navigated and non-navigated breast cancer screening abnormality groups throughout the course of the study.
The PNRP studies included other cancers (colorectal and prostate), but the majority of the cancers were breast and cervical. A meta-analysis by Freund et al. (37) assessed the timeliness of diagnostic resolution for an abnormal breast and cervical cancer screening result across the PNRP. The results of the meta-analysis found little benefit during the first 90 days of care as only one of the seven sites focusing on breast cancer screening and two of the four sites focusing on cervical cancer screening observed a positive effect of PN on time to diagnostic resolution (p < 0.05). Greater benefit from navigation was seen from 91 to 365 days for diagnostic resolution among three of the seven sites focused on breast cancer screening and two of the four sites focused on cervical cancer screening (p < 0.05). Meta-regression revealed that navigation had its greatest benefits within centers with the greatest delays in follow-up under usual care.
One study (44) reported on the difference in time to diagnostic resolution between those in the PN intervention vs. control groups. A RCT from the Denver PNRP center evaluated the effectiveness of PN programs for increasing rates of diagnostic resolution for abnormal breast cancer screening. Raich et al. (44) found PN shortened time to resolution in the navigated group (p < 0.001) compared to the usual care group. Specifically, PN improved diagnostic resolution for patients presenting with mammographic BIRADS 0 and 3, but not BIRADS 4/5 or abnormal breast examinations.
PN after Diagnosis
The results of the literature review for PN after cancer diagnosis resulted in eight studies (46–53), including one RCT (48), reporting effects on various outcomes among cancer patients including start of treatment, receipt of recommended care, completion of treatment, quality of life and depressive symptoms, communication with physicians, and quality measures. Hendren et al. (48) found no significant effect of PN on disease-specific quality of life scores between navigated and usual care breast cancer patients from baseline to 3 months. Other studies suggest that PN had no effect on time to completion of primary cancer treatment, satisfaction with cancer-related care, or psychological distress, and they attributed the non-significant findings to the open eligibility criteria (all patients) instead of targeting those with shown need, as seen in other effective interventions (49, 51, 52).
A study by Ramirez et al. (52) sought to examine the effectiveness of PN in reducing time from breast cancer diagnosis to initiation of treatment among Hispanic/Latino women. Compared to control patients, there was a significantly higher percentage of navigated women who initiated treatment within 30 days (69.0 vs. 46.3%, p < 0.05, intervention vs. control, respectively) and 60 days (97.6 vs. 73.1%, p < 0.001, intervention vs. control, respectively) from diagnosis. Also, time from breast cancer diagnosis to first treatment was significantly lower in the navigated group (22.22 days) than among women in the control group (48.30 days).
In a large, multisite study, Ko et al. (49) sought to improve the receipt of recommended care for newly diagnosed breast cancer patients, and the findings varied based on the type of treatment received by the patients. Among women eligible for antiestrogen therapy, navigated participants were more likely to receive antiestrogen therapy compared with usual care participants (OR = 1.73, p = 0.004). Among women eligible for radiation therapy after lumpectomy, navigated participants were no more likely to receive radiation than usual care participants (OR = 1.42, p = 0.22).
Barriers to Care and PN
Several studies have conducted secondary analyses to understand the association between barriers to care and clinical outcomes, particularly within the PNRP. A 2015 study by Ramachandran et al. (54) explored the association among number of barriers to care, type of barriers, and timeliness of diagnostic resolution among women with abnormal cancer screening results. They found that 74% of breast cancer screening participants and 55% of cervical cancer screening participants reported at least one barrier to diagnostic resolution. Navigated women with barriers resolved cancer screening abnormalities at a slower rate compared with navigated women with no barriers. Another study by Ramachandran et al. (55) using Boston PNRP data, found the odds of timely diagnostic resolution reduced as the number of barriers increased (one barrier, aHR = 0.81, 95% CI = 0.56–1.17, p = 0.26; two barriers, aHR = 0.55, 95% CI = 0.37–0.81, p = 0.0025; three or more barriers, aHR = 0.31, 95% CI = 0.21–0.46, p < 0.0001). Lastly, Katz et al. (56) examined the effect of having barriers to diagnostic resolution and time to resolution among participants in the PN intervention arm with a breast or cervical cancer abnormality in the PNRP. They found that 63.7% of breast abnormality and 46.6% of cervical abnormality participants had at least one barrier resulting in longer time to diagnostic resolution among breast (aHR = 0.74, 95% CI = 0.67–0.83, p < 0.01) and cervical (aHR = 0.79, 95% CI = 0.70–0.90, p < 0.01) participants vs. those with no reported barriers.
Specific types of barriers patients report were described by several studies (57–59). Korber et al. (57) found the most common barriers to cancer treatment were patient-provider communication and knowledge of patient resources. Other studies found location of health-care facility (59), transportation problems (58), not speaking English (55), no insurance (56), financial concerns (58, 60), lack of social/practical support (58, 59), and lack of information about the abnormality (57) as the most prevalent barriers to cancer care among patients enrolled in PN interventions.
Some studies have attempted to determine which variables are associated with having a barrier to cancer care to identify women most in need of PN. Several studies (55, 60–62) found that women with barriers to cancer care were more likely to be racial and ethnic minorities (55, 60), unmarried (62), part-time employed/unemployed (60, 62), non-English language speakers (55, 61), and have public/no health insurance (55, 60) compared to women without any barriers to care.
Discussion
As evidenced in this literature review, PN has been shown to help women receive cancer screenings, receive more timely diagnostic resolution after a breast and cervical cancer screening abnormality, initiate treatment sooner, receive proper treatment, and improve quality of life among cancer patients. Also, it was shown that PN eliminates barriers to care. PNRP demonstrated: (1) who has barriers; (2) that barriers delay the receipt of care; and (3) types of numbers of barriers that impact time to treatment (54–56).
Several trends emerged from this review. PN programs have been implemented among diverse populations specifically focused on reducing health disparities in racial and ethnic minorities and/or underserved populations. It is important to note that each study population and setting was unique, thus generalizability of these findings may be limited. Another trend noted was the limited effectiveness for certain groups receiving PN, alluding to the possibility that PN is not equally effective for all groups. Results found significant differences in PN effectiveness with regard to age (32), ethnicity (42), location of care (37), type of screening test (38), and type of treatment (49). Although relevant for all populations, use of a “one-size-fits all” approach to PN may not be the best approach. The original intent of PN is to improve the experience of care among patients with the greatest needs by tailoring actions to an individual’s barriers to care (63). If implementation across the patient population is too demanding on resources, especially due to the fact that the American College of Surgeons Commission on Cancer (CoC)’s accreditation mandates are currently unfunded, targeting PN implementation may be a possible solution. By identifying those most likely to need PN, scarce resources can be diverted to women in most need and most likely to delay or not receive prompt, appropriate care (64).
Finally, although there is evidence of the potential of PN to improve outcomes related to cancer screening and diagnostic resolution, many studies have utilized less robust designs (i.e., quasi-experimental and descriptive studies), as mentioned by previous reviews (14–16). A notable difference between this review and the prior reviews is an increase in the number of studies evaluating PN on cancer screening and treatment outcomes. Another difference between this and previous reviews was inclusion of studies that evaluated the association of PN with reported outcomes during cancer treatment and post-treatment. Yet, there was great heterogeneity among the studied outcomes (e.g., quality of life, proper treatment), and therefore, cumulative evidence, as seen in PN interventions on cancer screening and diagnostic resolution, is lacking.
Research Opportunities in PN and Women’s Health
Due to the increased prevalence of PN in health-care systems, there are growing research opportunities in PN and women’s health. One area that is ripe for researchers is PN in cancer survivorship, particularly among post-treatment cancer survivors. Increases in the number of individuals diagnosed with cancer each year, as well as improving survival rates, have led to an ever-increasing number of cancer survivors (20). As evidenced by this review, implementation of PN interventions among post-treatment cancer survivors is lacking. Future research should not only explore adherence to post-treatment surveillance behaviors but also treatment outcomes that can affect the physical and psychological well-being of women.
The PN literature on women’s cancers is growing; however, it is limited in that researchers have primarily focused on breast cancer (as seen in the literature on PN after diagnosis). Although cervical cancer incidence and mortality rates have steadily decreased, it is estimated that in 2015, 12,900 new cases of invasive cervical cancer occurred and 4,100 died from this disease (19). There is a wide racial and socioeconomic disparity in the incidence and mortality rates from cervical cancer. Underlying these disparities are often education, language, geographic, and trust factors (65). As evidenced by this review, the few studies that have explored PN in gynecological cancers showed promising results. Thus, researchers should make gynecological cancers a focus for their PN interventions to maximize the positive impact on this survivor population. Important yet understudied subpopulations, such as women with increased genetic risk, should be considered. PN can provide education, support, and guidance within the clinical setting for these women to receive appropriate screenings, genetic testing and counseling, prompt diagnosis, and proper treatment.
Women may also benefit from PN during cancer care that is tailored to specific family-related barriers, such as child care and transportation. Women often assume the role of caregivers and income-earners and may need more assistance in caregiving for others while receiving cancer care for themselves. PN can link them to resources that offer emotional (i.e., support groups) and tangible support (i.e., house cleaning, child care) and has the potential to improve quality of life and psychosocial outcomes for both women with cancer and women who are caregivers.
Navigators should consider the age of the female patient and their stage in life during PN interventions. For example, younger women often face very different challenges and complications than older women, including concerns about becoming a mother; caring for children when faced with a life-threatening illness; premature menopause leading to loss of fertility; sudden onset of vasomotor symptoms; long-term consequences of early ovarian decline; body image and sexuality; and career and work concerns related to productivity and job security (66). For older adults, age-related concerns may include spousal caregiving; lack of social support; quality vs. quantity of life; comorbidities; risk of polypharmacy; mobility challenges; housing and transportation needs; and declining cognitive function and information processing (67, 68). Navigators from the PNRP used a standardized, structured list and an open-ended approach that captured barriers to care identified by participants. Future studies should utilize this approach to collect information on barriers to care and explore age-related differences in reported barriers to address individual needs accordingly.
The similarity of patient navigators to the participants is important for the success of PN interventions. For example, patient navigator race and language concordance improved the timeliness of care in a minority population (34). Likeness to the patient population is already a typical characteristic of CHWs, who work within a target community to improve community awareness and adherence to cancer screenings, and thus, this successful strategy should be extended to navigators. Since the CHWs’ role is to connect underserved populations from the community with screening services, PN programs should work with CHWs to assist women across the entire cancer care spectrum from cancer prevention to post-treatment. Future research should explore the effect of a combined CHW and PN intervention to increase community engagement, improve access to preventive health services, facilitate timely diagnosis and treatment, and ultimately improve the health of women in underserved areas.
Author Contributions
JK-S was responsible for the planning, literature review, writing, editing, and submitting the manuscript. JO was responsible for the planning, literature review, writing, and editing the manuscript. EP was responsible for the planning, writing, and editing the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ward E, Jemal A, Cokkinides V, Singh GK, Cardinez C, Ghafoor A, et al. Cancer disparities by race/ethnicity and socioeconomic status. CA Cancer J Clin (2004) 54:78–93. doi: 10.3322/canjclin.54.2.78
2. Gehlert S, Colditz GA. Cancer disparities: unmet challenges in the elimination of disparities. Cancer Epidemiol Biomarkers Prev (2011) 20:1809–14. doi:10.1158/1055-9965.EPI-11-0628
3. Paskett ED, McLaughlin JM, Lehman AM, Katz ML, Tatum CM, Oliveri JM. Evaluating the efficacy of lay health advisors for increasing risk-appropriate Pap test screening: a randomized controlled trial among Ohio Appalachian women. Cancer Epidemiol Biomarkers Prev (2011) 20:835–43. doi:10.1158/1055-9965.EPI-10-0880
4. Russell KM, Champion VL, Monahan PO, Millon-Underwood S, Zhao Q, Spacey N, et al. Randomized trial of a lay health advisor and computer intervention to increase mammography screening in African American women. Cancer Epidemiol Biomarkers Prev (2010) 19:201–10. doi:10.1158/1055-9965.EPI-09-0569
5. Freeman HP, Muth BJ, Kerner JF. Expanding access to cancer screening and clinical follow-up among the medically underserved. Cancer Pract (1995) 3:19–30.
6. American College of Surgeons. National Accrediation Program for Breast Centers Breast Center Components. Chicago, IL: American College of Surgeons (2010).
7. National Comprehensive Cancer Network. The Case Manager or Patient Navigator: Providing Support for Cancer Patients During Treatment and Beyond. Fort Washington, PA: National Comprehensive Cancer Network (2014).
8. Clark CR, Baril N, Kunicki M, Johnson N, Soukup J, Ferguson K, et al. Addressing social determinants of health to improve access to early breast cancer detection. J Womens Health (2009) 18:677–90. doi:10.1089/jwh.2008.0972
9. Fang CY, Ma GX, Tan Y, Chi N. A multifaceted intervention to increase cervical cancer screening among underserved Korean women. Cancer Epidemiol Biomarkers Prev (2007) 16:1298–302. doi:10.1158/1055-9965.EPI-07-0091
10. Battaglia TA, Roloff K, Posner MA, Freund KM. Improving follow-up to abnormal breast cancer screening in an urban population. Cancer (2007) 109:S359–67. doi:10.1002/cncr.22354
11. Ell K, Vourlekis B, Lee PJ, Xie B. Patient navigation and case management following an abnormal mammogram: a randomized clinical trial. Prev Med (2008) 44:26–33. doi:10.1016/j.ypmed.2006.08.001
12. Ell K, Vourlekis B, Xie B, Nedjat-Haiem FR, Lee PJ, Muderspach L, et al. Cancer treatment adherence among low-income women with breast or gynecologic cancer: a randomized controlled trial of patient navigation. Cancer (2009) 115:4606–15. doi:10.1002/cncr.24500
13. Schwaderer KA, Proctor JW, Martz EF, Slack RJ, Ricci E. Evaluation of patient navigation in a community radiation oncology center involved in disparities studies: a time-to-completion-of-treatment study. J Oncol Pract (2008) 4: 220–4. doi:10.1200/JOP.0852001
14. Robinson-White S, Conroy B, Slavish KH, Rosenzweig M. Patient navigation in breast cancer: a systematic review. Cancer Nurs (2010) 33(2):127–40. doi:10.1097/NCC.0b013e3181c40401
15. Paskett ED, Harrop JP, Wells KJ. Patient navigation: an update on the state of the science. CA Cancer J Clin (2011) 61(4):237–49. doi:10.3322/caac.20111
16. Wells KJ, Battaglia TA, Dudley DJ, Garcia R, Greene A, Calhoun E, et al. Patient navigation: state of the art or is it science? Cancer (2008) 113(8):1999–2010. doi:10.1002/cncr.23815
17. Simard S, Thewes B, Humphris G, Dixon M, Hayden C, Mireskandari S, et al. Fear of cancer recurrence in adult cancer survivors: a systematic review of quantitative studies. J Cancer Surviv (2013) 7(3):300–22. doi:10.1007/s11764-013-0272-z
18. Freund KM, Battaglia TA, Calhoun E, Dudley DJ, Fiscella K, Paskett E, et al. National cancer institute patient navigation research program. Cancer (2008) 113:3391–9. doi:10.1002/cncr.23960
19. American Cancer Society. Cancer Facts and Figures, 2015. Atlanta, GA: American Cancer Society (2015).
20. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin (2014) 64:9–29. doi:10.3322/caac.21208
21. Paskett ED, Katz ML, Post DM, Pennell ML, Young GS, Seiber EE, et al. The Ohio patient navigation research program: does the American cancer society patient navigation model improve time to resolution in patients with abnormal screening tests? Cancer Epidemiol Biomarkers Prev (2012) 21(10):1620–8. doi:10.1158/1055-9965.EPI-12-0523
22. Warren-Mears V, Dankovchik J, Patil M, Fu R. Impact of patient navigation on cancer diagnostic resolution among northwest tribal communities. J Cancer Educ (2013) 28(1):109–18. doi:10.1007/s13187-012-0436-y
23. Wells KJ, Lee JH, Calcano ER, Meade CD, Rivera M, Fulp WJ, et al. A cluster randomized trial evaluating the efficacy of patient navigation in improving quality of diagnostic care for patients with breast or colorectal cancer abnormalities. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1664–72. doi:10.1158/1055-9965.EPI-12-0448
24. Fiscella K, Whitley E, Hendren S, Raich P, Humiston S, Winters P, et al. Patient navigation for breast and colorectal cancer treatment: a randomized trial. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1673–81. doi:10.1158/1055-9965.EPI-12-0506
25. Wagner EH, Ludman EJ, Aiello Bowles EJ, Penfold R, Reid RJ, Rutter CM, et al. Nurse navigators in early cancer care: a randomized, controlled trial. J Clin Oncol (2014) 32:12–8. doi:10.1200/JCO.2013.51.7359
26. Burhansstipanov L, Dignan MB, Schumacher SA, Krebs LU, Alfonsi G, Apodaca CC. Breast screening navigator programs within three settings that assist underserved women. J Cancer Educ (2010) 25:247–52. doi:10.1007/s13187-010-0071-4
27. Marshall JK, Mbah OM, Ford JG, Phelan-Emrick D, Ahmed S, Bone L, et al. Effect of patient navigation on breast cancer screening among African American Medicare beneficiaries: a randomized controlled trial. J Gen Intern Med (2015) 31(1):68–76. doi:10.1007/s11606-015-3484-2
28. Percac-Lima S, Milosavljevic B, Oo SA, Marable D, Bond B. Patient navigation to improve breast cancer screening in Bosnian refugees and immigrants. J Immigr Minor Health (2012) 14:727–30. doi:10.1007/s10903-011-9539-5
29. Percac-Lima S, Ashburner JM, Bond B, Oo SA, Atlas SJ. Decreasing disparities in breast cancer screening in refugee women using culturally tailored patient navigation. J Gen Intern Med (2013) 28(11):1463–8. doi:10.1007/s11606-013-2491-4
30. Phillips CE, Rothstein JD, Beaver K, Sherman BJ, Freund KM, Battaglia TA. Patient navigation to increase mammography screening among inner city women. J Gen Intern Med (2011) 26(2):123–9. doi:10.1007/s11606-010-1527-2
31. Wang X, Fang C, Tan Y, Liu A, Ma GX. Evidence-based intervention to reduce access barriers to cervical cancer screening among underserved Chinese American women. J Womens Health (2010) 19(3):463–9. doi:10.1089/jwh.2009.1422
32. Basu M, Linebarger J, Gabram SG, Patterson SG, Amin M, Ward KC. The effect of nurse navigation on timeliness of breast cancer care at an academic comprehensive cancer center. Cancer (2013) 119(14):2524–31. doi:10.1002/cncr.28024
33. Battaglia TA, Bak SM, Heeren T, Chen CA, Kalish R, Tringale S, et al. Boston patient navigation research program: the impact of navigation on time to diagnostic resolution after abnormal cancer screening. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1645–54. doi:10.1158/1055-9965.EPI-12-0532
34. Charlot M, Santana MC, Chen CA, Bak S, Heeren TC, Battaglia TA, et al. Impact of patient and navigator race and language concordance on care after cancer screening abnormalities. Cancer (2015) 121(9):1477–83. doi:10.1002/cncr.29221
35. Donelan K, Mailhot JR, Dutwin D, Barnicle K, Oo SA, Hobrecker K, et al. Patient perspectives of clinical care and patient navigation in follow-up of abnormal mammography. J Gen Intern Med (2011) 26(2):116–22. doi:10.1007/s11606-010-1436-4
36. Dudley DJ, Drake J, Quinlan J, Holden A, Saegert P, Karnard A, et al. Beneficial effects of a combined navigator/promotora approach for Hispanic women diagnosed with breast abnormalities. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1639–44. doi:10.1158/1055-9965.EPI-12-0538
37. Freund KM, Battaglia TA, Calhoun E, Darnell JS, Dudley DJ, Fiscella K, et al. Impact of patient navigation on timely cancer care: the patient navigation research program. J Natl Cancer Inst (2014) 106(6):dju115. doi:10.1093/jnci/dju115
38. Hoffman HJ, LaVerda NL, Young HA, Levine PH, Alexander LM, Brem R, et al. Patient navigation significantly reduces delays in breast cancer diagnosis in the District of Columbia. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1655–63. doi:10.1158/1055-9965.EPI-12-0479
39. Lee JH, Fulp W, Wells KJ, Meade CD, Calcano E, Roetzheim R. Patient navigation and time to diagnostic resolution: results for a cluster randomized trial evaluating the efficacy of patient navigation among patients with breast cancer screening abnormalities, Tampa, FL. PLoS One (2013) 8(9):e74542. doi:10.1371/journal.pone.0074542
40. Luckett R, Pena N, Vitonis A, Bernstein MR, Feldman S. Effect of patient navigator program on no-show rates at an academic referral colposcopy clinic. J Womens Health (2015) 24(7):608–15. doi:10.1089/jwh.2014.5111
41. Markossian TW, Darnell JS, Calhoun EA. Follow-up and timeliness after an abnormal cancer screening among underserved, urban women in a patient navigation program. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1691–700. doi:10.1158/1055-9965.EPI-12-0535
42. Paskett ED, Dudley DJ, Young GS, Brewer B, Wells KJ, Calhoun E, et al. Impact of patient navigation interventions on timely diagnostic follow-up for abnormal cervical cancer screening. J Womens Health (2016) 25:15–21. doi:10.1089/jwh.2014.5094
43. Percac-Lima S, Benner CS, Liu R, Aldrich LS, Oo SA, Regan N, et al. The impact of a culturally tailored patient navigator program on cervical cancer prevention in Latina women. J Womens Health (2013) 22(5):426–31. doi:10.1089/jwh.2012.3900
44. Raich PC, Whitley EM, Thorland W, Valverde P, Fairclough D. Patient navigation improves cancer diagnostic resolution: an individually randomized clinical trial in an underserved population. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1629–38. doi:10.1158/1055-9965.EPI-12-0513
45. Ramirez AG, Perez-Stable EJ, Penedo FJ, Talavera GA, Carrillo JE, Fernandez ME, et al. Navigating Latinas with breast screen abnormalities to diagnosis: the six cities study. Cancer (2013) 119(7):1298–305. doi:10.1002/cncr.27912
46. Chen F, Mercado C, Yermilov I, Puig M, Ko CY, Kahn KL, et al. Improving breast cancer quality of care with the use of patient navigators. Am Surg (2010) 76(10):1043–6.
47. Haideri NA, Moormeier JA. Impact of patient navigation from diagnosis to treatment in an urban safety net breast cancer population. J Cancer (2011) 2:467–73. doi:10.7150/jca.2.467
48. Hendren S, Griggs JJ, Epsitein R, Humiston S, Jean-Pierre P, Winters P, et al. Randomized controlled trial of patient navigation for newly diagnosed cancer patients: effects on quality of life. Cancer Epidemiol Biomarkers Prev (2012) 21:1682–90. doi:10.1158/1055-9965.EPI-12-0537
49. Ko NY, Darnell JS, Calhoun E, Freund KM, Wells KJ, Shapiro CL, et al. Can patient navigation improve receipt of recommended breast cancer care? Evidence from the national patient navigation research program. J Clin Oncol (2014) 32(25):2758–64. doi:10.1200/JCO.2013.53.6037
50. Madore S, Kilbourn K, Valverde P, Borrayo E, Raich P. Feasibility of a psychosocial and patient navigation intervention to improve access to treatment among underserved breast cancer patients. Support Care Cancer (2014) 22(8):2085–93. doi:10.1007/s00520-014-2176-5
51. Raj A, Ko N, Battaglia TA, Chabner BA, Moy B. Patient navigation for underserved patients diagnosed with breast cancer. Oncologist (2012) 17:1027–31. doi:10.1634/theoncologist.2012-0191
52. Ramirez A, Perez-Stable E, Penedo F, Talavera G, Carrillo JE, Fernandez M, et al. Reducing time-to-treatment in underserved Latinas with breast cancer: the six cities study. Cancer (2014) 120(5):752–60. doi:10.1002/cncr.28450
53. Ulloa JG, Hemmelgarn M, Viveros L, Odele P, Feldman NR, Ganz PA, et al. Improving breast cancer survivors’ knowledge using a patient-centered intervention. Surgery (2015) 158(3):669–75. doi:10.1016/j.surg.2015.03.056
54. Ramachandran A, Snyder FR, Katz ML, Darnell JS, Dudley DJ, Patierno SR, et al. Barriers to health care contribute to delays in follow-up among women with abnormal cancer screening: data from the patient navigation research program. Cancer (2015) 121:4016–24. doi:10.1002/cncr.29607
55. Ramachandran A, Freund KM, Bak SM, Heeren TC, Chen CA, Battaglia TA. Multiple barriers delay care among women with abnormal cancer screening despite patient navigation. J Womens Health (Larchmt) (2015) 24(1):30–6. doi:10.1089/jwh.2014.4869
56. Katz ML, Young GS, Reiter PL, Battaglia TA, Wells KJ, Sanders M, et al. Barriers reported among patients with breast and cervical abnormalities in the patient navigation research program: impact on timely care. Womens Health Issues (2014) 24(1):e155–62. doi:10.1016/j.whi.2013.10.010
57. Korber SF, Padula C, Gray J, Powell M. A breast navigator program: barriers, enhancers, and nursing interventions. Oncol Nurs Forum (2011) 38(1):44–50. doi:10.1188/11.ONF.44-50
58. Carroll JK, Humiston SG, Meldrum SC, Salamone CM, Jean-Pierre P, Epstein RM, et al. Patients’ experiences with navigation for cancer care. Patient Educ Couns (2010) 80:241–7. doi:10.1016/j.pec.2009.10.024
59. Koh C, Nelson JM, Cook PF. Evaluation of a patient navigation program. Clin J Oncol Nurs (2011) 15(1):41–8. doi:10.1188/11.CJON.41-48
60. Primeau SW, Freund KM, Ramachandran A, Bak SM, Heeren T, Chen CA, et al. Social service barriers delay care among women with abnormal cancer screening. J Gen Intern Med (2014) 29(1):169–75. doi:10.1007/s11606-013-2615-x
61. Karlinger KS, Ma L, Hofmann M, Kerlikowske K. Language barriers, location of care and delays in follow-up of abnormal mammograms. Med Care (2012) 50:171–8. doi:10.1097/MLR.0b013e31822dcf2d
62. Hendren S, Chin N, Fisher S, Winters P, Griggs J, Mohile S, et al. Patients’ barriers to receipt of cancer care, and factors associated with needing more assistance from a patient navigator. J Natl Med Assoc (2011) 103(8):701–10. doi:10.1016/S0027-9684(15)30409-0
63. Freeman HP. The origin, evolution, and principles of patient navigation. Cancer Epidemiol Biomarkers Prev (2012) 21(10):1614–7. doi:10.1158/1055-9965.EPI-12-0982
64. Krok-Schoen JL, Brewer B, Young GS, Weier RC, Tatum CM, DeGraffinreid CR, et al. Participants’ barriers to diagnostic resolution and factors associated with needing patient navigation. Cancer (2015) 121:2757–64. doi:10.1002/cncr.29414
65. Natale-Pereira A, Enard KR, Nevarez L, Jones LA. The role of patient navigators in eliminating health disparities. Cancer (2011) 117(Suppl 15):3543–52. doi:10.1002/cncr.26264
66. Manuel JC, Burwell SR, Crawford SL, Lawrence RH, Farmer DF, Hege A, et al. Younger women’s perceptions of coping with breast cancer. Cancer Nurs (2007) 30:85–94. doi:10.1097/01.NCC.0000265001.72064.dd
67. Posma ER, van Weert JCM, Jansen J, Bensing JM. Older cancer patients’ information and support needs surrounding treatment: an evaluation trough the eyes of patients, relatives and professionals. BMC Cancer (2009) 8:1–15. doi:10.1186/1472-6955-8-1
Keywords: patient navigation, breast cancer, cervical cancer, gynecological cancers, women’s health, cancer disparities
Citation: Krok-Schoen JL, Oliveri JM and Paskett ED (2016) Cancer Care Delivery and Women’s Health: The Role of Patient Navigation. Front. Oncol. 6:2. doi: 10.3389/fonc.2016.00002
Received: 09 November 2015; Accepted: 03 January 2016;
Published: 28 January 2016
Edited by:
Sarah M. Temkin, National Cancer Institute, USAReviewed by:
Reuven Reich, Hebrew University of Jerusalem, IsraelBrigitte Mlineritsch, Private Medical University Clinic Salzburg, Austria
Copyright: © 2016 Krok-Schoen, Oliveri and Paskett. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica L. Krok-Schoen, amVzc2ljYS5rcm9rQG9zdW1jLmVkdQ==