 Yimei Ma
Yimei Ma Xiaoxi Lu1,2*
Xiaoxi Lu1,2*- 1Department of Pediatrics, West China Second University Hospital, Sichuan University, Chengdu, China
- 2Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, Chengdu, China
- 3Department of Pediatric Pulmonology and Immunology, West China Second University Hospital, Sichuan University, Chengdu, China
- 4Key Laboratory of Chronobiology (Sichuan University), National Health Commission of China, Chengdu, China
- 5The Joint Laboratory for Lung Development and Related Diseases of West China Second University Hospital, Sichuan University and School of Life Sciences of Fudan University, West China Institute of Women and Children’s Health, West China Second University Hospital, Sichuan University, Chengdu, China
- 6Sichuan Birth Defects Clinical Research Center, West China Second University Hospital, Sichuan University, Chengdu, China
Background: The purpose of this systematic review and meta-analysis was to evaluate the effect of a neutropenic diet and a control diet on infection and mortality rates in oncology patients with neutropenia.
Methods: We searched the following English electronic databases: PubMed, Embase, Cochrane Central Register of Controlled Trials, and Google Scholar Engine. Published studies involving neutropenic diets (study group) and control diets (control group) in oncology patients with neutropenia were searched. The focus of the meta-analysis was on the outcomes of infection and mortality rates. A subgroup analysis was also performed.
Results: A total of 6 studies were included, with a total sample size of 1114 patients. The patients in the study group had a similar infection rate compared with the patients in the control group (P = 0.11). The patients in the study group had a similar mortality rate compared with the patients in the control group (P = 0.74). Another subgroup analysis showed that the incidence of infection was also similar for pediatric (P = 0.74) and adult (P = 0.11) oncology patients between the study and control groups.
Conclusions: Based on the current evidence, this meta-analysis showed that the application of a neutropenic diet cannot reduce the risk of infection and mortality in oncology patients with neutropenia. However, more rigorous randomized controlled trials are needed to confirm this conclusion in the future.
Introduction
In recent years, the long-term survival rate of oncology patients has gradually increased through multimodal treatment, including chemotherapy (1–3) and radiation therapy (4, 5). However, in these patients receiving intensive chemotherapy and radiation therapy, immune function (6, 7) and bone marrow cells are inhibited (8, 9), resulting in long-term neutropenia (10–12). Destruction of the gastrointestinal mucosa also increases the risk of gastrointestinal infections in tumor patients (13, 14). At the same time, it is understood that patients with cancer may experience dysbiosis or an imbalance between potentially beneficial and pathogenic bacteria (15–17) due to exposure to broad-spectrum antibiotics and certain antitumor agents, as well as changes in intestinal peristalsis and integrity (18, 19). Therefore, it also potentially increases the risk of infection in these patients.
A variety of management and treatment protocols have been reported to effectively reduce infections in neutropenia. As previously reported, a “low bacterial diet” or “neutropenic diet” with varying degrees of dietary restriction was implemented to reduce the bacterial load available for infection (20–22). Although there is no evidence of consistency, the “neutropenic diet” is still widely used to treat cancer patients. However, given that malnutrition is a common side effect of cancer patients (23, 24), dietary restrictions may not be well tolerated, and it is also one of the important factors affecting the negative quality of life of patients.
The “neutropenic diet” was initially used as a therapeutic strategy to reduce the risk of acquiring systemic infection in patients with severe immunodeficiency, theoretically limiting patient intake of potential pathogenic microbes (25, 26). Although extensively recommended by oncologists, there are very little clinically relevant data to support this intervention to reduce the effects of chemotherapy-induced leukopenia in cancer patients. To date, a “neutropenic diet” has still no standard definition. Furthermore, to our knowledge, there have been few meta-analyses comparing the “neutrophil diet” and standardized dietary guidelines in leukemia patients with neutropenia, and the benefits and clinical outcomes in oncology patients with neutropenia treatment are unclear.
Thus, we performed a systematic review and meta-analysis and compared the efficacy of neutropenic diets in oncology patients with neutropenia. We hypothesized that (1) the neutropenic diet reduces the incidence of infection and (2) the neutropenic diet reduces the incidence of mortality.
Materials and Methods
Search Strategy
PubMed (1966 to October 2021), Embase (1974 to October 2021), Web of Science (1990 to October 2021), and Central Register of Controlled Trials (October 2021). To search for additional eligible studies, we also used Google Scholar Engine (October 2021). All comparative studies were involved in oncology patients with neutropenia. The following keywords were used: “bone marrow transplant”, “leukemia”, “neutropenic diet”, and “low bacterial diet”. No language and geographic restrictions.
Inclusion Criteria
The meta-analysis used the following inclusion criteria: PICOS (population, intervention, comparator, outcome, study design). (1) Population: the patients were diagnosed with leukemia with neutropenia, including acute lymphoblastic leukemia (AML) and acute myeloid leukemia (ALL); (2) intervention: the intervention was a neutropenic diet (study group); (3) comparison: the comparator was a standardized diet (control group); and (4) results: the incidence of infection and mortality rates. (5) Study design: The study design was a clinical controlled trial. Duplications of published literature, letters, and abstracts were excluded. If the published study was repeated, the study with the largest sample size was retained. All titles and abstracts were independently reviewed by two reviewers. Any discrepancies were resolved by consensus, and if necessary, a third reviewer was consulted.
Assessment of Methodological Quality
The methodological qualities of the included trials were assessed independently by the two reviewers. On the one hand, randomized controlled trials used a specific tool to assess the methodological quality and risk of bias of clinical trials described by the Cochrane Collaboration for Systematic Reviews (27). The seven items of random sequence generation, allocation sequence concealment, blinding of participants and personnel, blinding of the outcome assessment, incomplete outcome data, selective reporting, and other biases contained in the specific tool were meaningful evaluation indices. The overall methodological quality of each included study was evaluated as “Yes” (low risk of bias), “No” (high risk of bias), or “Unclear” (unclear risk of bias). On the other hand, for case–control study, the Newcastle–Ottawa Scale quality assessment scale was selected, which was recommended by the Cochrane nonrandomized studies methods (28).
Data Extraction and Outcome Measures
Two reviewers extracted the results independently from the included studies, including the following information: first author, date of publication, number of participants, type of disease, method of intervention, antibiotic management, and outcome measures. The outcome measures used in this meta-analysis were the infection rate and survival rate between the study group and control group.
Data Synthesis
The statistical analysis of all eligible studies was performed by RevMan 5 software (Version: 5.3, The Cochrane Collaboration), and a p value of < 0.05 was considered statistically significant. For continuous data, the mean difference and 95% confidence interval (CI) were calculated. For dichotomous data, the risk ratio (RR) and 95% CI were calculated. The meta-analysis assessed statistical heterogeneity using the chi-squared test and I2 statistic. According to the meaning of statistical heterogeneity, the fixed-effects model was selected if the chi-squared test > 0.1 or the I2 < 50%. Otherwise, the random-effects model was used to analyze the pooled data. Publication bias was assessed using a funnel plot of infection rates.
Results
Search Program
Figure 1 shows the flow chart for the inclusion and exclusion of the study. According to the inclusion criteria, 6 studies (20–22, 29–31) were finally included.
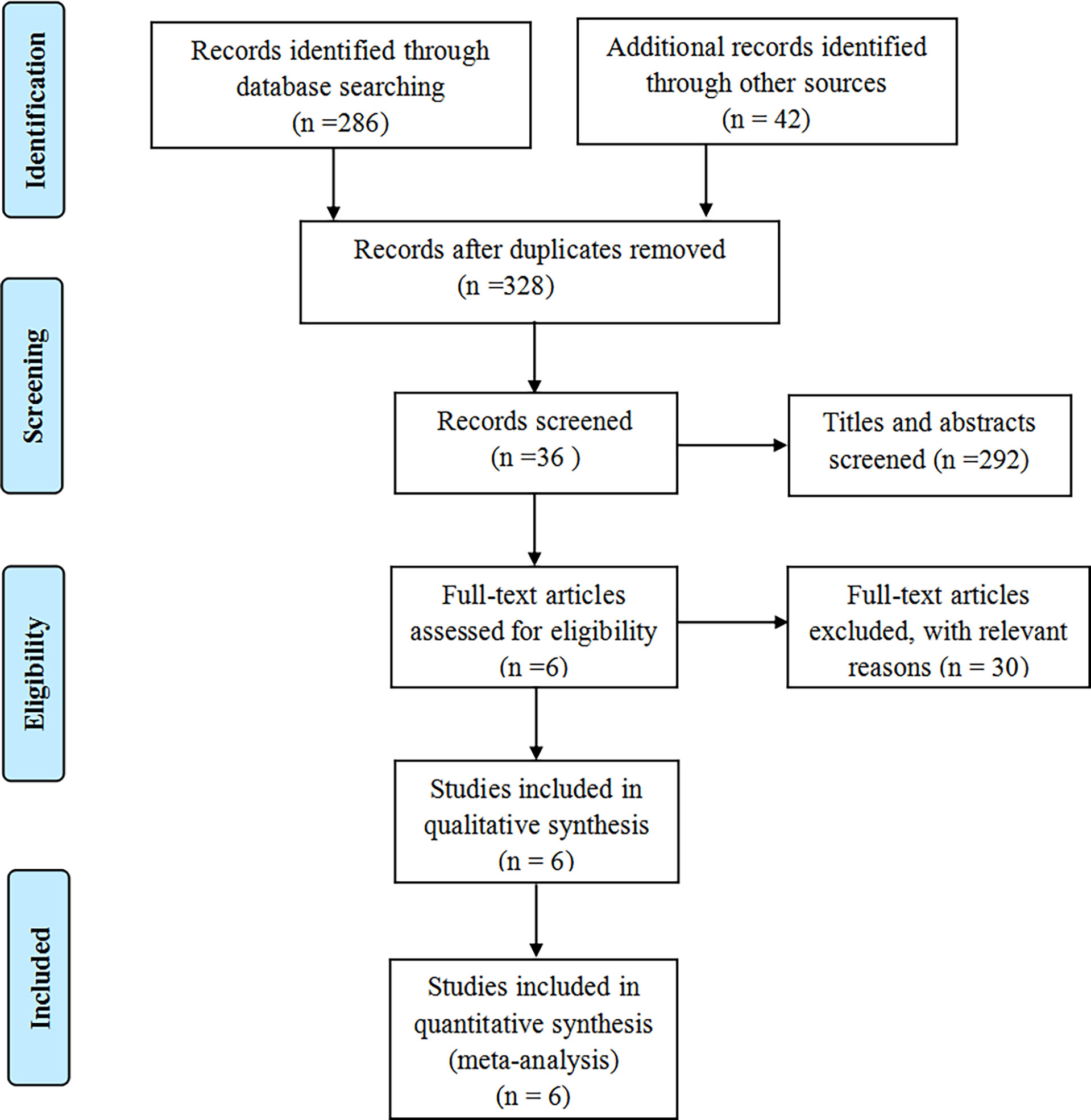
Figure 1 The flow diagram of literature selection.
Study Characteristics and Quality Assessment
The meta-analysis included 562 patients in the study group and 552 patients in the control group. Sample sizes ranged from 9 to 363. All included studies were published between 2007 and 2017. The average age was in the range of 4.1 to 77 years old. Two studies (20, 31) were reported for pediatric oncology patients, and 4 studies (21, 22, 29, 30) were reported for adult oncology patients with neutropenia. The “neutropenic diet” in the included studies has different definitions in various studies, including the elimination of raw fruits and vegetables. The “standardized diet” in the control group was either a “regular hospital diet” or a diet based on the “Food and Drug Administration (FDA)” approved food safety guidelines. The disease types in most studies were AML (21, 22, 29–31) and ALL (20, 21, 29–31). Four studies (21, 22, 29, 30) reported that patients received antibiotics to prevent infection. Table 1 shows the baseline characteristics of all included studies and the Table 2 shows the intervention and the outcome of all included studies.
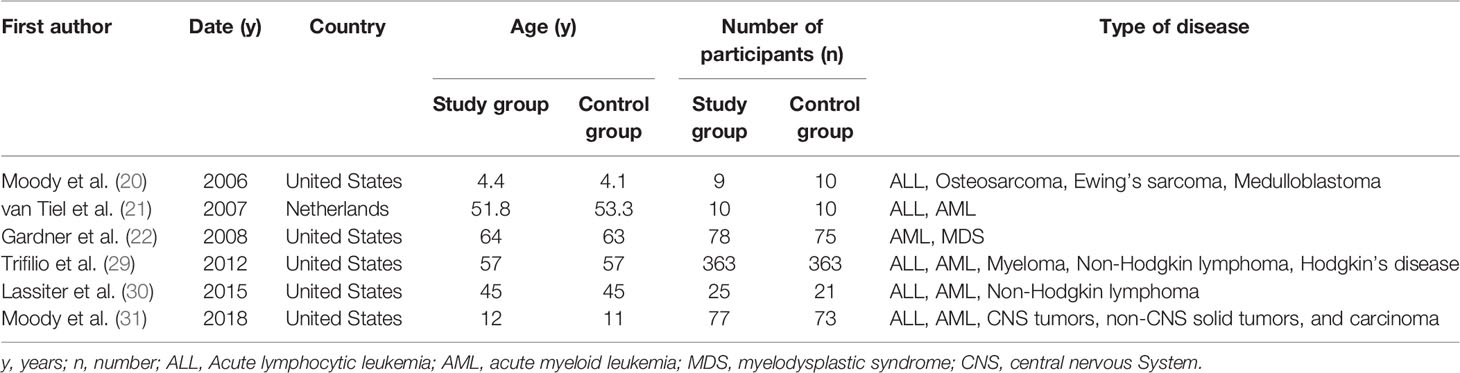
Table 1 The baseline characteristics of all included studies.
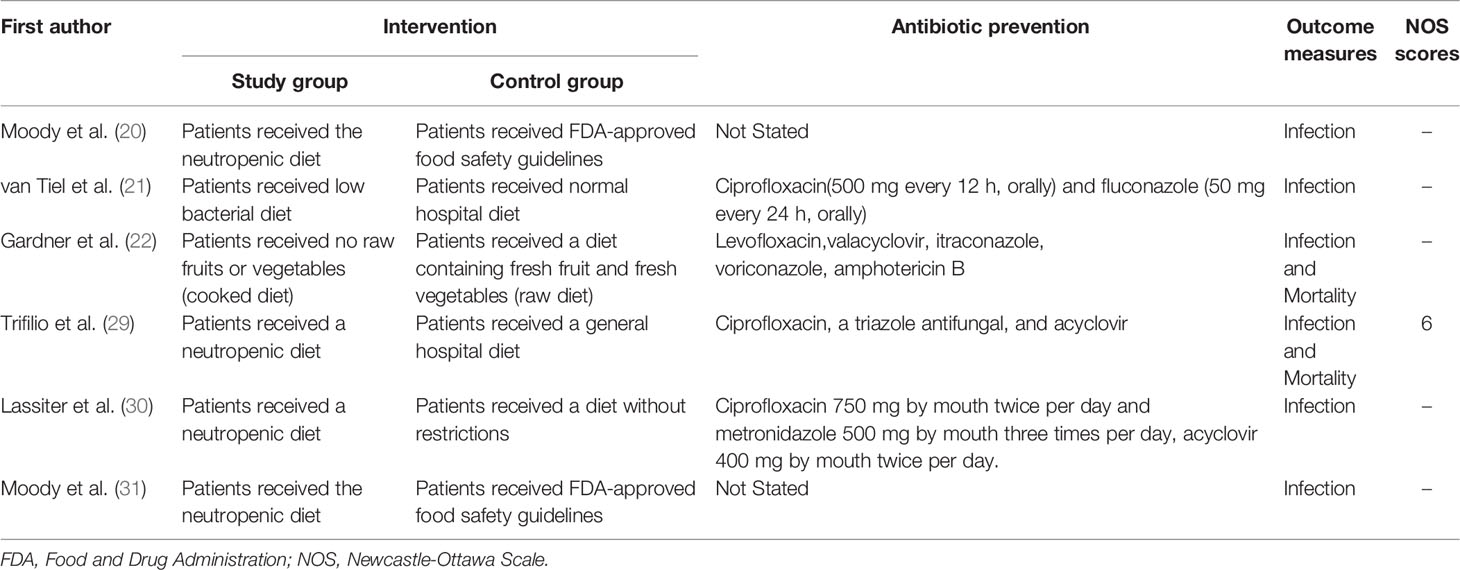
Table 2 The intervention and the outcome of all included studies.
Figure 2 summarizes the methodological quality, and all studies were relatively well designed. Randomized methods were performed in 4 studies (20–22, 31), and 2 randomized controlled trials (20, 31) reported clear blinding. The Newcastle–Ottawa Scale was awarded higher scores, with 6 for the case–control study (29) (Table 2). The meta-analysis independently used funnel plots of the infection rates to assess any publication bias; the plots were generally symmetrical and suggested a low publication bias (Figure 3).
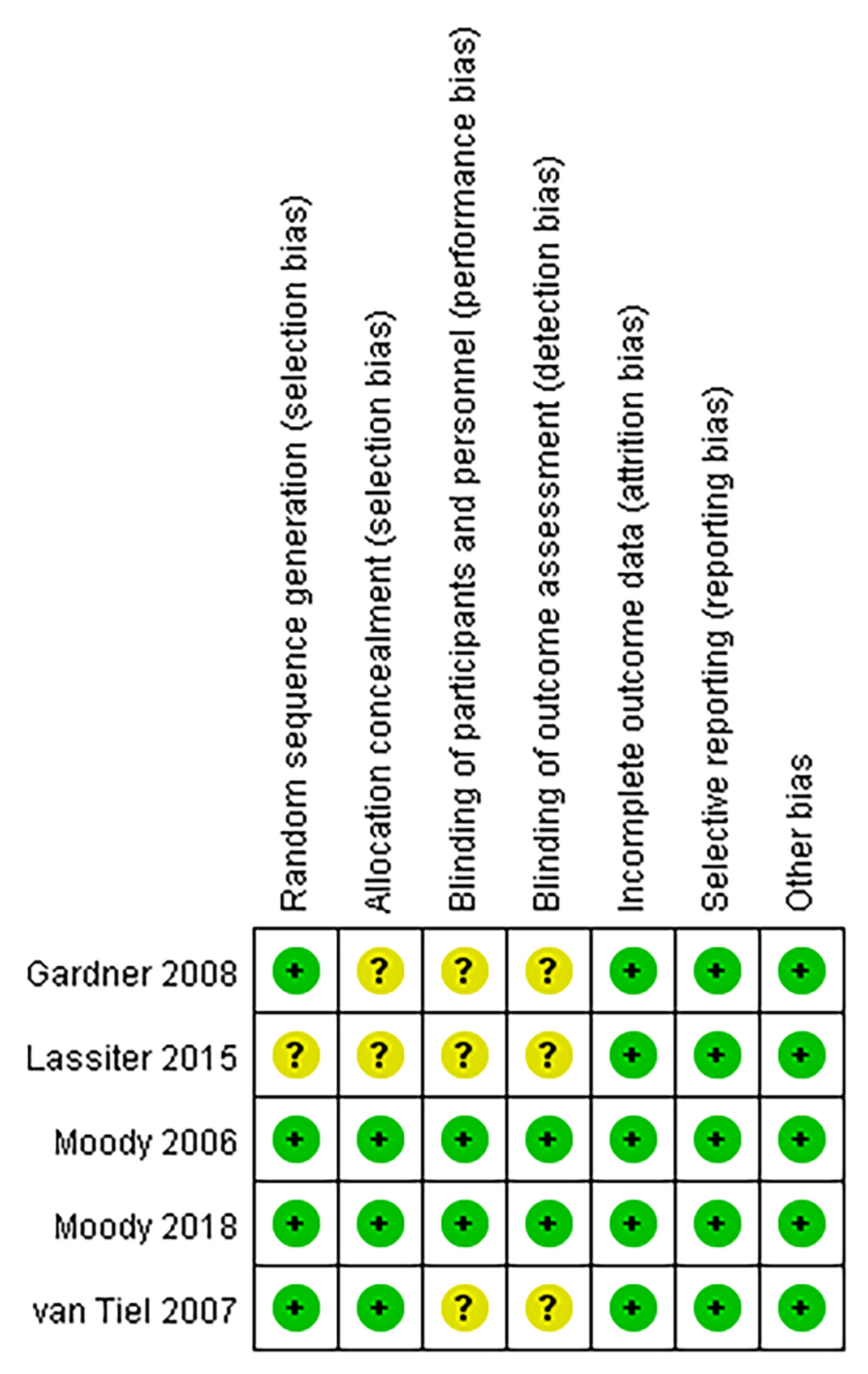
Figure 2 Risk of publication bias summary.
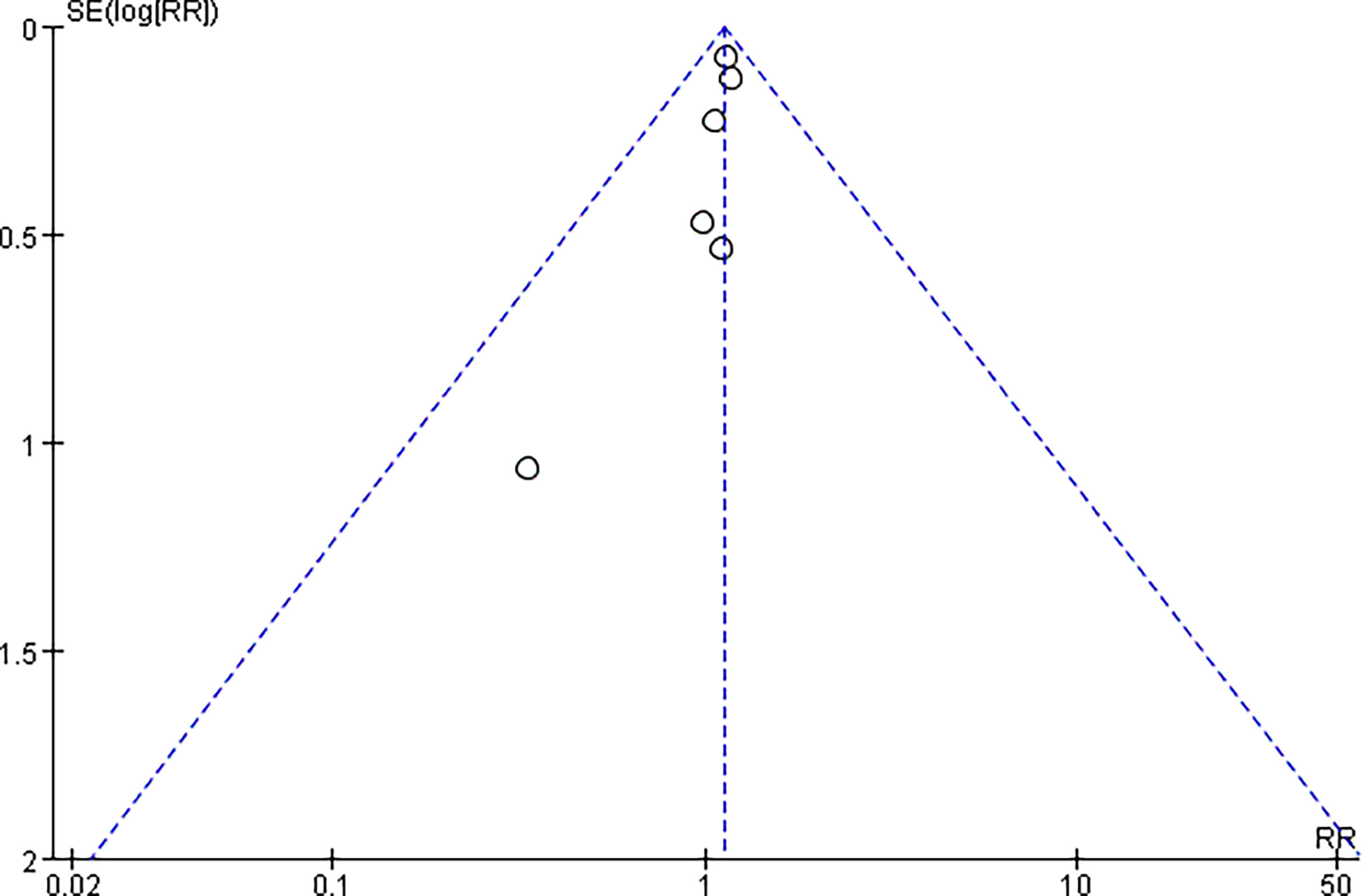
Figure 3 Publication bias of the infection.
Meta-Analysis of the Incidence of Infection
All the included studies (20–22, 29–31) reported relevant data on the incidence of infection (562 and 552 patients in the study and control groups, respectively). The meta-analysis found that patients in the study group had similar results for the incidence of infection compared with the patients in the control group (risk ratio, 1.13; 95% CI, 0.97 to 1.31; P = 0.11). The fixed effects model was adopted in the meta-analysis since the pooled data did not show statistical heterogeneity (P = 0.90, I2 = 0%) (Figure 4).
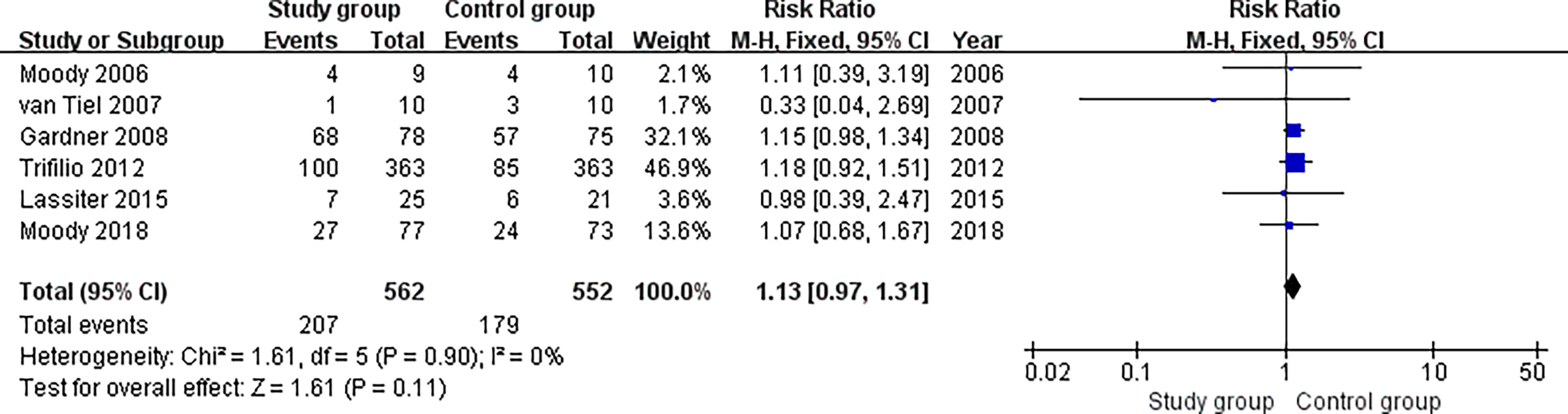
Figure 4 Meta-analysis of the incidence of infection.
Subgroup Analysis for Pediatric and Adult Oncology Patients With Neutropenia
Two studies (20, 31) reported relevant data on the incidence of infection for pediatric oncology patients (86 and 83 patients in the study and control groups, respectively). The subgroup analysis found that patients in the study group had similar results for the incidence of infection compared with the patients in the control group (risk ratio, 1.07; 95% CI, 0.71 to 1.62; P = 0.74). The fixed effects model was adopted in the meta-analysis since the pooled data did not show statistical heterogeneity (P = 0.94, I2 = 0%) (Figure 5).
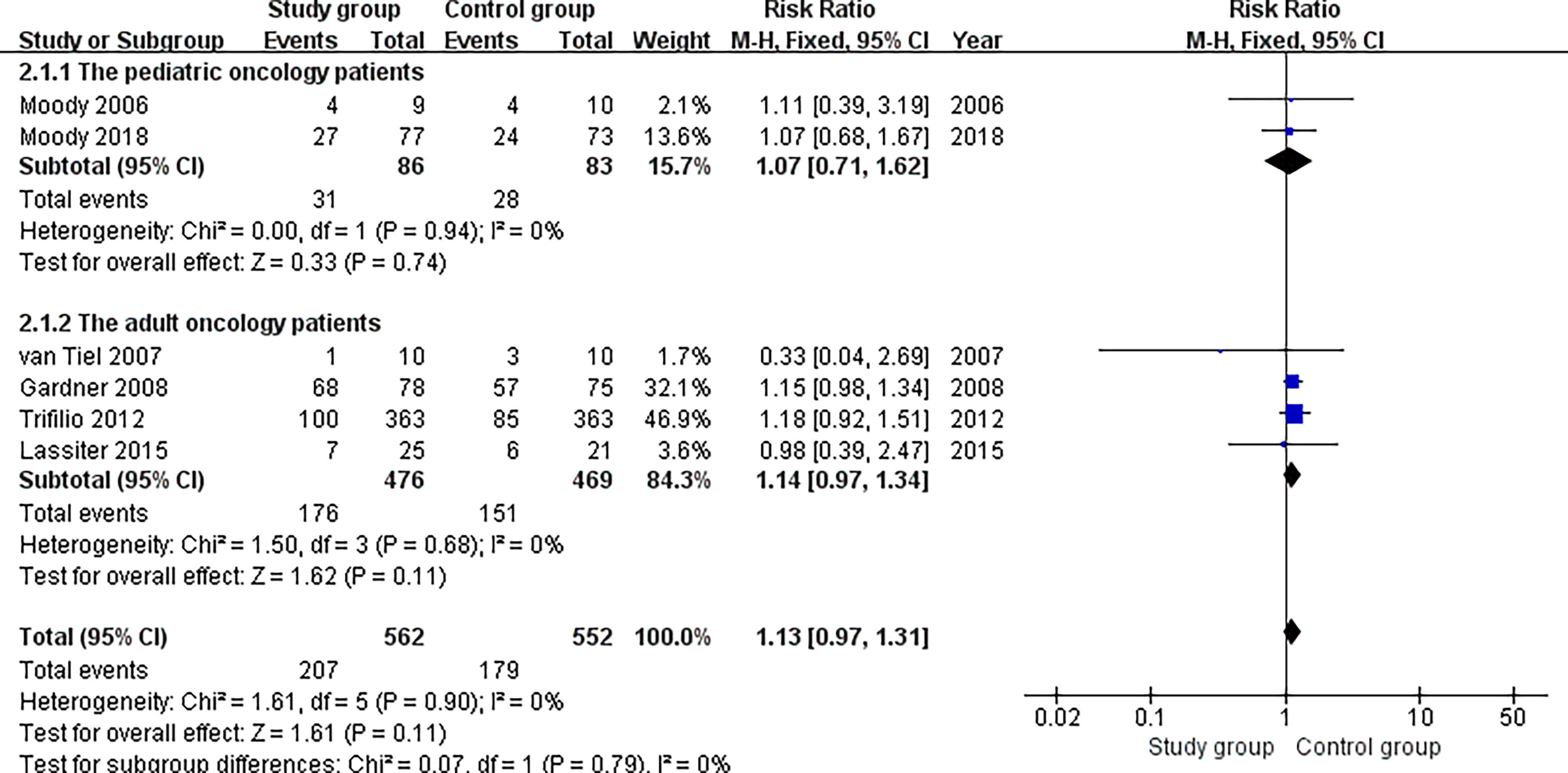
Figure 5 Subgroup analysis for pediatric and adult oncology patients.
Four studies (21, 22, 29, 30) reported relevant data on the incidence of infection for adult oncology patients (476 and 469 patients in the study and control groups, respectively). The subgroup analysis found that patients in the study group had similar results for the incidence of infection compared with the patients in the control group (risk ratio, 1.14; 95% CI, 0.97 to 1.34; P = 0.11). The fixed effects model was adopted in the meta-analysis since the pooled data did not show statistical heterogeneity (P = 0.68, I2 = 0%) (Figure 5).
Meta-Analysis of the Incidence of Mortality
Two studies (22, 29) reported relevant data on the incidence of mortality (441 and 438 patients in the study and control groups, respectively). The meta-analysis found that patients in the study group had similar results for the incidence of mortality compared with the patients in the control group (risk ratio, 1.06; 95% CI, 0.76 to 1.48; P = 0.74). The random effects model was adopted in the meta-analysis since the pooled data did not show statistical heterogeneity (P = 0.64, I2 = 29%) (Figure 6).

Figure 6 Meta-analysis of the incidence of mortality.
Discussion
This is a systematic review and meta-analysis to demonstrate whether neutropenic diets in oncology patients with neutropenia can reduce infection compared to a standardized diet. The meta-analysis found that a “neutropenic diet” did not reduce the incidence of infection and mortality in patients compared with a standardized diet. In addition, a subgroup analysis found no difference in the incidence of infection for neutropenia diets between children and adults.
Oncology patients with neutropenia who are affected by myelosuppressive chemotherapy cause neutropenia and are often instructed to follow “neutropenic diets” to reduce the risk of target infection and death (22, 29). However, “neutropenic diets” often interfere with patient food choices and may result in inadequate nutrient intake during chemotherapy. Previous studies (20, 21, 29, 31) have been extensively published on the application of a “neutropenic diet” in leukemia patients, and it has produced inconsistent clinical results. A randomized controlled trial (31) involving 150 patients who had AML, ALL or a malignant solid tumor and will undergo a period of myelosuppressive chemotherapy indicated that patients receiving a “neutropenic diet” showed no difference in the prevention of infection in pediatric oncology patients compared with those who received FDA-approved food safety guidelines (33% vs. 35%, P = 0.78). Similarly, another randomized controlled trial (20) of 19 patients comparing patients who received a neutropenic diet versus an FDA diet in pediatric oncology patients receiving myelosuppressive chemotherapy indicated that both a neutropenic diet and an FDA diet were similar in preventing infection (44% vs. 40%). In contrast, Trifilio et al. (29) showed an increased risk of infection in patients with a “neutropenic diet” and a higher risk of developing diarrhea and urinary tract infections. This may be a change in the microbiota and normal gut flora following the use of a “neutropenic diet”, as these infections have been shown to be associated with changes in bacterial volume.
The meta-analysis also raises questions about whether neutropenic patients have restricted diets, and this is especially important for cancer patients who have important problems with cachexia and anorexia (32). Fresh vegetables and fruits are an important source of dietary fiber, and fiber is important for improving intestinal transport and reducing constipation. Therefore, if these fibrous diets are excluded, they are harmful to the body to some extent. The results of this meta-analysis showed that the infection rate of patients with a neutropenic diet was similar to that of the FDA-approved food safety guidelines, which may suggest that oncologists should reconsider whether a neutropenic diet should be treated as a routine treatment.
The subgroup analysis in the meta-analysis also showed that in oncology patients with neutropenia in pediatric patients and adults, a “neutropenic diet” does not reduce the risk of infection. This is important for children and adults with cancer, as food restrictions can have a negative impact on their quality of life. Therefore, a standardized diet rather than a “neutropenic diet” is preferred because it is less restrictive, making it easier for them to meet calorie and survival needs. In addition, previously published studies (29, 31) have shown that standardized diets are more likely to freely access food than neutropenic diets and are also beneficial in saving the cost of medical care for inpatients.
However, it is still unclear whether reducing food restrictions increases the quality of life of cancer patients. Moody et al. (20) used the Peds QL Quality of Life Inventory Core Module and Cancer Module to measure health-related quality of life and found that the average score for the baseline core module was 73 for patients in the food safety group and 55 for patients in the neutropenia diet group. This difference was statistically significant in both groups, indicating poor quality of life in patients fed a neutropenia diet. However, Hamada et al. (33) showed that the management of dietary restrictions did not directly reduce the quality of life in patients with hematological malignancies. Although the diets in the two groups are still controversial, studies on cancer patients in adults and children have shown that dietary intake is an important factor in quality of life and is closely related to physical health. Therefore, proper diet management and selection require further research to identify the best program to improve the quality of life of patients.
Another interesting question is whether granulocyte colony stimulating factor (GCSF) can affect the incidence of infection. We reviewed 6 studies and found that a total of 3 studies reported the use of GCSF. Gardner et al. (22) reported CGSF, but there was no exact number of reports used. Moody et al. (20) reported CGSF in the study group (4/9) and the control group (5/10), but the infection results were not significantly different. Moody et al. (31) reported CGSF in the study group (43/77) and the control group (40/73), and the infection was not significantly different. Although we wanted to use a meta-analysis to assess the impact of GCSF use on infection outcomes in this study, it could not be included in the meta-analysis calculation considering that not all patients were using GCSF. However, in terms of infection rates in each study, the use of GCSF seems to have little impact on infection rates, but it is still necessary to verify the results of many samples in the future due to the limited sample size.
The meta-analysis also has some limitations. First, the main limitation is its methodological quality. Randomized controlled trials are the most effective and reliable study to evaluate clinical outcomes in meta-analysis, but we included a case–control study that may produce quality bias and affect the results. Therefore, more carefully and scientifically designed randomized controlled trials are needed in the future to further confirm and compare the differences between neutropenic diets and standardized diets. The second limitation of this study is the sample size. A larger sample is needed and will be able to answer whether it is safe to reduce the diet that limits neutropenia and follow the food safety guidelines for patients with neutropenia.
Conclusion
Based on the current evidence, this meta-analysis showed that the application of a neutropenic diet does not reduce the risk of infection and mortality in oncology patients with neutropenia. However, more rigorous randomized controlled trials are needed to confirm this conclusion in the future.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Author Contributions
YM collects data and writes manuscript. XL conducted statistical analysis and designed experiments. HL designed experiments and revised manuscripts. All authors contributed to the article and approved the submitted version.
Funding
The study was supported by the Science and Technology Department of Sichuan Province (2017FZ0056), and it was supported by the West China Second University Hospital of Sichuan University (KX144).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bakogeorgos M, Georgoulias V. Risk-Reduction and Treatment of Chemotherapy-Induced Peripheral Neuropathy. Expert Rev Anticancer Ther (2017) 17(11):1045–60. doi: 10.1080/14737140.2017.1374856
2. Soularue E, Cohen R, Tournigand C, Zaanan A, Louvet C, Bachet JB, et al. Efficacy and Safety of Trastuzumab in Combination With Oxaliplatin and Fluorouracil-Based Chemotherapy for Patients With HER2-Positive Metastatic Gastric and Gastro-Oesophageal Junction Adenocarcinoma Patients: A Retrospective Study. B Cancer (2015) 102(4):324–31. doi: 10.1016/j.bulcan.2014.08.001
3. Kondoh C, Kadowaki S, Komori A, Narita Y, Taniguchi H, Ura T, et al. Salvage Chemotherapy With the Combination of Oxaliplatin, Leucovorin, and 5-Fluorouracil in Advanced Gastric Cancer Refractory or Intolerant to Fluoropyrimidines, Platinum, Taxanes, and Irinotecan. Gastric Cancer: Off J Int Gastric Cancer Assoc Jpn Gastric Cancer Assoc (2018) 21(6):1050–7. doi: 10.1007/s10120-018-0825-y
4. Specht L, Yahalom J, Illidge T, Berthelsen AK, Constine LS, Eich HT, et al. Modern Radiation Therapy for Hodgkin Lymphoma: Field and Dose Guidelines From the International Lymphoma Radiation Oncology Group (ILROG). Int J Radiat Oncol (2014) 89(4):854–62. doi: 10.1016/j.ijrobp.2013.05.005
5. Robin TP, Goodman KA. Radiation Therapy in the Management of Pancreatic Adenocarcinoma: Review of Current Evidence and Future Opportunities. Chin Clin Oncol (2017) 6(3):28. doi: 10.21037/cco.2017.06.12
6. Tallet AV, Dhermain F, Le Rhun E, Noel G, Kirova YM. Combined Irradiation and Targeted Therapy or Immune Checkpoint Blockade in Brain Metastases: Toxicities and Efficacy. Ann Oncol (2017) 28(12):2962–76. doi: 10.1093/annonc/mdx408
7. Manyam B, Garsa AA, Chin RI, Reddy CA, Gastman B, Vidimos AT, et al. A Multi-Institutional Comparison of Outcomes of Immunosuppressed and Immunocompetent Patients Treated With Surgery and Radiation Therapy for Cutaneous Squamous Cell Carcinoma of the Head and Neck. Int J Radiat Oncol (2016) 96(2):S159–S60. doi: 10.1016/j.ijrobp.2016.06.386
8. Zeng T, Li Y, Zhang CL, Yu LH, Zhu ZP, Zhao XL, et al. Garlic Oil Suppressed the Hematological Disorders Induced by Chemotherapy and Radiotherapy in Tumor-Bearing Mice. J Food Sci (2013) 78(6):H936–42. doi: 10.1111/1750-3841.12137
9. Kalbasi A, Komar C, Tooker GM, Liu MG, Lee JW, Gladney WL, et al. Tumor-Derived CCL2 Mediates Resistance to Radiotherapy in Pancreatic Ductal Adenocarcinoma. Clin Cancer Res (2017) 23(1):137–48. doi: 10.1158/1078-0432.CCR-16-0870
10. Vioral AN, Wentley D. Managing Oncology Neutropenia and Sepsis in the Intensive Care Unit. Crit Care Nurs Q (2015) 38(2):165–74. doi: 10.1097/CNQ.0000000000000058
11. Family L, Li YL, Chen LH, Page JH, Klippel ZK, Chao C. A Study of Novel Febrile Neutropenia Risk Factors Related to Bone Marrow or Immune Suppression, Barrier Function, and Bacterial Flora. J Natl Compr Canc Ne (2018) 16(10):1201–8. doi: 10.6004/jnccn.2018.7051
12. Alenzi EO, Kelley GA. The Association of Hyperglycemia and Diabetes Mellitus and the Risk of Chemotherapy-Induced Neutropenia Among Cancer Patients: A Systematic Review With Meta-Analysis. J Diabetes Complicat (2017) 31(1):267–72. doi: 10.1016/j.jdiacomp.2016.09.006
13. Abdel-Rahman O, ElHalawani H, Essam-Eldin S. S-1-Based Regimens and the Risk of Oral and Gastrointestinal Mucosal Injury: A Meta-Analysis With Comparison to Other Fluoropyrimidines. Expert Opin Drug Saf (2016) 15(1):5–20. doi: 10.1517/14740338.2016.1105959
14. Liu D, Jiang XY, Zhou LS, Song JH, Zhang X. Effects of Probiotics on Intestinal Mucosa Barrier in Patients With Colorectal Cancer After Operation Meta-Analysis of Randomized Controlled Trials. Medicine (2016) 95(15):e3342. doi: 10.1097/MD.0000000000003342
15. Khan ID. Outbreak of Prototheca Wickerhamii Algaemia and Sepsis in a Tertiary Care Chemotherapy Oncology Unit. Int J Infect Dis (2016) 45:195–. doi: 10.1016/j.ijid.2016.02.452
16. Kowalska-Krochmal B, Chaber R, Jermakow K, Hurkacz M, Piatkowska E, Gosciniak G, et al. Frequency of Isolation and Drug Susceptibility of Bacterial Strains Isolated From Child Oncohematological Patients 2011-2014: A Single Center Study. Adv Clin Exp Med (2018) 27(9):1201–9. doi: 10.17219/acem/69003
17. Inoue D, Nagai Y, Mori M, Nagano S, Takiuchi Y, Arima H, et al. Fulminant Sepsis Caused by Bacillus Cereus in Patients With Hematologic Malignancies: Analysis of its Prognosis and Risk Factors. Leukemia Lymphoma (2010) 51(5):860–9. doi: 10.3109/10428191003713976
18. Kim JC, Yang SS, Jang TY, Kwak JY, Yun MJ, Lim SB. Open Versus Robot-Assisted Sphincter-Saving Operations in Rectal Cancer Patients: Techniques and Comparison of Outcomes Between Groups of 100 Matched Patients. Int J Med Robot Comp (2012) 8(4):468–75. doi: 10.1002/rcs.1452
19. Di Carlo I, Toro A, Pannofino O, Pulvirenti EPE. Laparoscopic Versus Open Restoration of Intestinal Continuity After Hartmann Procedure. Hepato-Gastroenterol (2010) 57(98):232–5.
20. Moody K, Finlay J, Mancuso CO, Charlson M. Feasibility and Safety of a Pilot Randomized Trial of Infection Rate: Neutropenic Diet Versus Standard Food Safety Guidelines. J Pediat Hematol Onc (2006) 28(3):126–33. doi: 10.1097/01.mph.0000210412.33630.fb
21. van Tiel FH, Harbers MM, Terporten PHW, van Boxtel RTC, Kessels AG, Voss GBWE, et al. Normal Hospital and Low-Bacterial Diet in Patients With Cytopenia After Intensive Chemotherapy for Hematological Malignancy: A Study of Safety. Ann Oncol (2007) 18(6):1080–4. doi: 10.1093/annonc/mdm082
22. Gardner A, Mattiuzzi G, Faderl S, Borthakur G, Garcia-Manero G, Pierce S, et al. Randomized Comparison of Cooked and Noncooked Diets in Patients Undergoing Remission Induction Therapy for Acute Myeloid Leukemia. J Clin Oncol (2008) 26(35):5684–8. doi: 10.1200/JCO.2008.16.4681
23. Shaw C, Fleuret C, Pickard JM, Mohammed K, Black G, Wedlake L. Comparison of a Novel, Simple Nutrition Screening Tool for Adult Oncology Inpatients and the Malnutrition Screening Tool (MST) Against the Patient-Generated Subjective Global Assessment (PG-SGA). Support Care Cancer (2015) 23(1):47–54. doi: 10.1007/s00520-014-2319-8
24. Sanz EA, Siles MG, Fernandez LR, Roldan RV, Dominguez AR, Abiles J. Nutritional Risk and Malnutrition Rates at Diagnosis of Cancer in Patients Treated in Outpatient Settings: Early Intervention Protocol. Nutrition (2019) 57:148–53. doi: 10.1016/j.nut.2018.05.021
25. Casewell M, Phillips I. Food as a Source of Klebsiella Species for Colonization and Infection of Intensive Care Patients. J Clin Pathol (1978) 31(9):845–9. doi: 10.1136/jcp.31.9.845
26. Ball S, Brown TJ, Das A, Khera R, Khanna S, Gupta A. Effect of Neutropenic Diet on Infection Rates in Cancer Patients With Neutropenia: A Meta-Analysis of Randomized Controlled Trials. Am J Clin Oncol (2019) 42(3):270–4. doi: 10.1097/COC.0000000000000514
27. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ (2011) 343:d5928. doi: 10.1136/bmj.d5928
28. Luchini C, Stubbs B, Solmi M, Veronese N. Assessing the Quality of Studies in Meta-Analyses: Advantages and Limitations of the Newcastle Ottawa Scale. World J Meta-Anal (2017) 5(4):80–4. doi: 10.13105/wjma.v5.i4.80
29. Trifilio S, Helenowski I, Giel M, Gobel B, Pi J, Greenberg D, et al. Questioning the Role of a Neutropenic Diet Following Hematopoetic Stem Cell Transplantation. Biol Blood Marrow Tr (2012) 18(9):1385–90. doi: 10.1016/j.bbmt.2012.02.015
30. Lassiter M, Schneider SM. A Pilot Study Comparing the Neutropenic Diet to a non-Neutropenic Diet in the Allogeneic Hematopoietic Stem Cell Transplantation Population. Clin J Oncol Nurs (2015) 19(3):273–8. doi: 10.1188/15.CJON.19-03AP
31. Moody KM, Baker RA, Santizo RO, Olmez I, Spies JM, Buthmann A, et al. A Randomized Trial of the Effectiveness of the Neutropenic Diet Versus Food Safety Guidelines on Infection Rate in Pediatric Oncology Patients. Pediatr Blood Cancer (2018) 65(1):e26711. doi: 10.1002/pbc.26711
32. Bozzetti F. Nutritional Support of the Oncology Patient. Crit Rev Oncol Hemat (2013) 87(2):172–200. doi: 10.1016/j.critrevonc.2013.03.006
Keywords: neutropenic diet, infection, mortality, meta-analysis, oncology
Citation: Ma Y, Lu X and Liu H (2022) Neutropenic Diet Cannot Reduce the Risk of Infection and Mortality in Oncology Patients With Neutropenia. Front. Oncol. 12:836371. doi: 10.3389/fonc.2022.836371
Received: 15 December 2021; Accepted: 08 February 2022;
Published: 09 March 2022.
Edited by:
Chi-kong Li, The Chinese University of Hong Kong, ChinaReviewed by:
Mohamed Mahmoud Moussa, Ain Shams University, EgyptAli Aycicek, Cam Sakura Pediatric Hematology Oncology, Turkey
Copyright © 2022 Ma, Lu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hanmin Liu, bGl1aG1Ac2N1LmVkdS5jbg==; Xiaoxi Lu, bHVfaGVsZW5hQHNpbmEuY29t