 Francesco Ziglioli1*
Francesco Ziglioli1* Annalisa Patera1Gianmarco Isgrò2
Annalisa Patera1Gianmarco Isgrò2 Davide Campobasso1Giulio Guarino1Umberto Maestroni1
Davide Campobasso1Giulio Guarino1Umberto Maestroni1- 1Department of Urology, University Hospital of Parma, Parma, Italy
- 2Department of Urology, James Cook University Hospital, Middlesbrough, United Kingdom
Introduction: Although prostate cancer (PCa) is one of the most common cancers among men, the impact of modifiable risk and protective factors is still being debated. This review aims to qualitatively summarize the most recent studies related to potential healthy lifestyle factors affecting the development of PCa.
Methods for data acquisition: The literature focusing on modifiable risk factors for prostate cancer was reviewed. Medline and Embase via the Ovid database were searched, and all relevant and inherent articles were analyzed. Non-eligible publications, such as review articles, editorials, comments, guidelines, or case reports, were excluded.
Synthesis of the evidence obtained from data analysis: This review confirms that there is strong evidence that being overweight or obese increases the risk of advanced prostate cancer (assessed by body mass index (BMI), waist circumference, and waist–hip ratio), particularly considering central adiposity and ethnicity as contributing factors. The possible contribution of smoking still seems not entirely clear, while alcohol seems to affect PCa prevention in patients taking 5α-reductase inhibitors (5-ARIs). Dietary fibers may have anti-inflammatory properties and improve insulin sensitivity by reducing IGF bioactivity. In particular, dietary fiber intake like insoluble and legume fibers may be inversely associated with prostate cancer risk. Also, hyperglycemia and hyperinsulinemia, with untreated diabetic fasting blood glucose levels, could be modifiable prostate cancer risk factors. In two studies, aspirin was associated with a lower risk of lethal PCa and overall mortality. Concerning the role of vitamins, despite conflicting and divergent results, serum retinol concentration seems to be associated with an increased risk of prostate cancer and high-grade prostate cancer. Some studies resulted in disagreement about the role of selenium and vitamin E. We found inconsistent and controversial findings about the association between vitamin D and prostate cancer risk.
Conclusion: Far from being conclusive evidence, our findings confirm some strong evidence already found in the previous literature and highlight the need to clarify the role of some risk factors whose role is not yet completely known. This effort would facilitate the cultural and social change that may allow the shift from the treatment of prostate cancer when diagnosed to the real efforts needed for systematic prevention.
1 Introduction
Prostate cancer (PCa) is the most common cancer among men worldwide (1), with the highest incidence and the third highest mortality rate in Europe (2). The advent of prostate-specific antigen (PSA) and its derivatives increased the number of patients being diagnosed with PCa. Non-modifiable risk factors, such as age, ethnicity, and hereditary factors, represent well-established causes underlying the etiology of PCa (3, 4). Nevertheless, the impacts of modifiable risk factors, such as diet, physical activity, obesity, and smoking, remain largely unclear (5).
In 2018, the World Cancer Research Fund (WCRF) and the American Institute for Cancer Research (AICR) presented the Continuous Update Project expert report on prostate with the aim to analyze cancer prevention through diet, nutrition, and physical activity. The recommendations of this report stated evidence on obesity, highlighting that waist circumference and waist–hip ratio are strongly associated with an increased risk of advanced prostate cancer, defined as high-grade PCa (Gleason score ≥7) or stage 3–4 on the American Joint Committee on Cancer (AJCC 1992) classification. Also, there is strong evidence that beta-carotene is unlikely to have a role in the carcinogenesis of PCa. Despite this robust and strongly supported evidence, only limited and inconsistent evidence is reported in the literature about other modifiable risk factors (6, 7).
Considering the impossibility to manage non-modifiable risk factors, a clear analysis of the modifiable and preventable ones appears of utmost importance. In this review, we aimed to summarize the most recent evidence about the impact of diet, habits, physical activity, and other modifiable risk factors on the carcinogenesis of PCa.
2 Methods for data acquisition
2.1 Search strategy
The current review was carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (8).
Medline and Embase via Ovid database were searched using the following keywords (“prostate cancer” OR “prostatic cancer” OR “prostatic tumor” OR “prostatic adenocarcinoma”) AND (“lifestyle” OR “BMI” OR “alcohol intake” OR “prevention” OR “obesity” OR “physical activity” OR “exercise” OR “healthy” OR “smoking” OR “sedentary” OR “pollution” OR “food” OR “diet” OR “nutrition” OR “antioxidant” OR “sex” OR “sexual activity” OR “infections” OR “testosterone” OR “hormones” OR “androgens” OR “nutrients” OR “metabolic syndrome”).
The literature search was performed in February 2023. Only articles published in the last 10 years were considered. Two authors independently selected the articles for inclusion in the review. When there was no agreement between the authors for inclusion/exclusion, a third author was involved in the definitive decision.
The literature search and the selection process are reported in Figure 1.
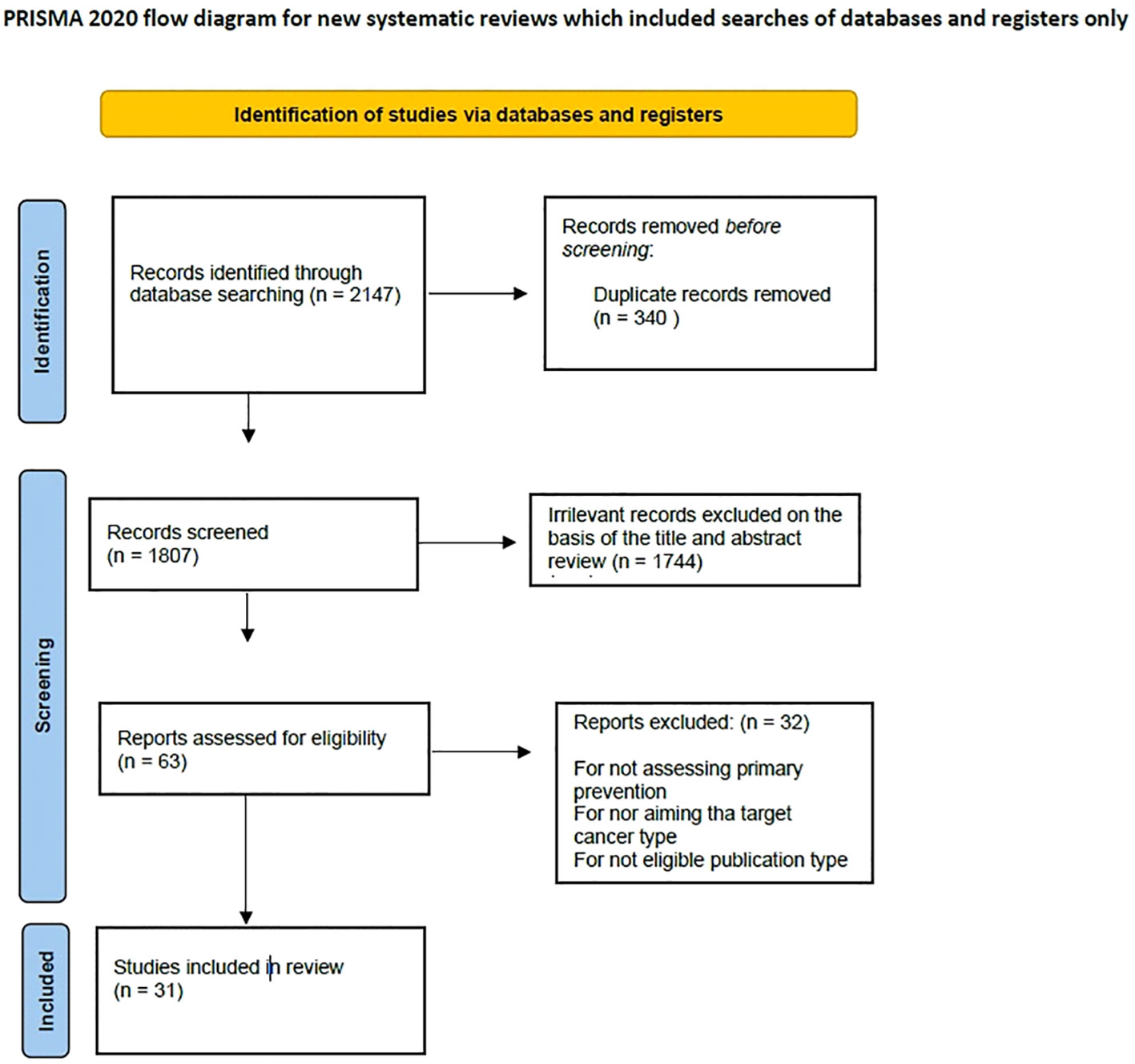
Figure 1 Literature search and selection.
2.2 Study selection
There was no restriction on the type of study (retrospective or prospective), but only clinical trials and randomized controlled trials were considered, excluding non-eligible publication types, such as review articles, comments, guidelines, editorials, and case reports.
A total of 2,147 articles were identified and screened through the evaluation of the title and the abstract to exclude irrelevant studies. When the abstract clearly showed that the related article did not focus on the objective of the present review, it was excluded. In case of doubt, the article was studied for potential inclusion. Subsequently, full-text assessment was performed for all articles included. Articles were excluded when results did not achieve statistical significance and/or when statistical analysis was not robust. Duplicates (defined as articles clearly reporting the same series) and irrelevant articles, which would not contribute to the review, were excluded. Only articles in English were considered.
At the end of the selection process, 31 articles were included in the review (Table 1).
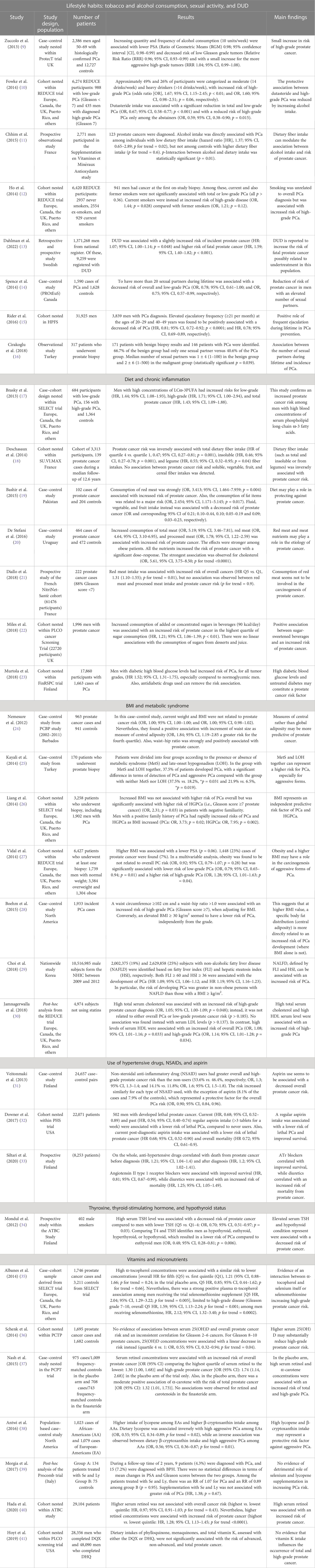
Table 1 Synthesis of the evidence about the association between modifiable risk factors and prostate cancer.
2.3 Data extraction
Two authors extracted the following data from the included articles: year of publication, type of the study, funding, patients’ characteristics, and results.
As quantitative analysis was not possible due to the very high heterogeneity among the included studies, only qualitative analysis was carried out.
2.4 Studies included
All studies included were published between 2012 and 2023. A total of 21 studies were nested case–control (NCC), three studies were observational, and seven were case–control studies.
The cohort was nested within the following trials:
◼ The Selenium and Vitamin E Cancer Prevention Trial (SELECT): a randomized placebo-controlled trial that tested the role of selenium and vitamin E in reducing prostate cancer risk (the USA, Puerto Rico, and Canada) (42).
◼ The Prostate Testing for cancer and Treatment (ProtecT) study: a multicenter randomized controlled trial (UK) (43).
◼ The Alpha-Tocopherol, Beta-Carotene Cancer Prevention (ATBC) Study: a randomized, double-blind, placebo-controlled trial on the effects of supplementation with α-tocopherol and β-carotene on cancer incidence (USA and Finland) (44).
◼ The Reduction by Dutasteride of Prostate Cancer Events (REDUCE) study: a multicenter, randomized, double-blind, placebo-controlled study comparing dutasteride with placebo (Europe, Canada, UK, Puerto Rico, and others) (45).
◼ The Prostate Cancer Prevention Trial (PCPT): a randomized, placebo-controlled trial testing the role of 5α-reductase inhibitor in the prevention of prostate cancer (USA) (46).
◼ The Supplementation en Vitamines et Minéraux Antioxydants (SU.VI.MAX) cohort: a randomized, double-blind, placebo-controlled trial assessing the effect of daily supplementation of antioxidants on the incidence of cardiovascular diseases and cancers (France) (47).
◼ The Physicians’ Health Study (PHS I): a randomized, placebo-controlled trial on aspirin and β-carotene for the prevention of cardiovascular disease and cancer (USA) (48).
◼ The Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial: a large, prospective, randomized, multi-site study (USA) investigating the effects of cancer screening on cancer mortality (49).
◼ The Finnish Randomized Study of Screening for Prostate Cancer (FinRSPC), the largest component of the multinational European Randomized Study of Screening for Prostate Cancer (ERSPC), whose main goal was to find out if systematic screening can decrease prostate cancer mortality (50).
◼ The NutriNet-Santé study was an ongoing web-based cohort launched in France in 2009 with the aim to study the association between nutrition and health (51).
In terms of geographical distribution, many studies were multicentric randomized studies including patients from the USA, the UK, Europe, Canada, and Puerto Rico, with a small contribution from Finland, France, Pakistan, Uruguay, Turkey, Korea, and Italy.
The results of the studies included are summarized in Table 1.
3 Synthesis of the evidence obtained from data analysis
3.1 Lifestyle habits
3.1.1 Tobacco consumption
Cigarette smoking is considered a major public health concern worldwide due to its consequences in terms of mortality and morbidity. Despite the correlation between smoking and several solid tumors, the relationship between smoking and PCa remains a matter of debate (52). The REDUCE trial offered an opportunity to evaluate the relationship between cigarette smoking and prostate cancer. Ho et al. (12) conducted a logistic regression to test the association between smoking and cancer on the first on-study biopsy in REDUCE. Among men with high PSA levels and negative biopsy in REDUCE, smoking was unrelated to overall prostate or low-grade PCa. However, smoking was found to be associated with an increased risk of high-grade PCa.
3.1.2 Alcohol consumption
Concerning alcohol consumption, most of the evidence in the literature confirms a correlation with the increased risk of high-grade prostate cancer, with a smaller influence on the overall risk. In particular, alcohol consumption among moderate and heavy drinkers (estimated at least 10 units/week) appears to increase the risk of high-grade PCa (9). Fowke et al. (10) confirmed that alcohol affects PCa in patients on 5α-reductase inhibitors (5-ARIs). Dutasteride was assumed to be associated with a significantly reduced risk of high-grade PCa among alcohol abstainers, suggesting that alcohol intake represents an unfavorable risk factor in those taking phosphodiesterase inhibitors. However, it is reported that the intake of a high amount of dietary fiber represents a protective factor among alcohol consumers (11).
3.1.3 Sexual habits/activity
The role of sexual activity as a modifiable risk factor in PCa prevention is still being debated. The main studies in the literature focused on ejaculatory frequency, number of sexual partners, and age of the first intercourse. Sexually transmitted infections (STIs) have also been investigated. However, it was not possible to unequivocally clarify the correlation with the carcinogenesis of prostate cancer (53). Spence et al. (14) carried out a case–control study, finding a reduction in the risk of overall and low-grade PCa among men with multiple female sexual partners during their lifetime (more than 20). In contrast, men with multiple male sexual partners had a slightly increased risk, with an apparent association with a higher risk of STIs. Frequent sexual intercourse may lead to a potentially increased exposure to sexually transmitted diseases (STDs) and is associated with higher androgen function and higher PCa risk (54). Indeed, Cirakoglu et al. (16) found a positive association between the number of sexual partners during a lifetime and the incidence of PCa. In addition, Rider et al. (15) supported the “prostate stagnation hypothesis”, as they reported a positive role of frequent ejaculation during a lifetime (more equal than 20 per month) in preventing prostate cancer. This can be related to the decrease of carcinogenic molecules within prostatic fluid due to frequent ejaculation.
3.2 Diet and chronic inflammation
Dietary fiber intake is associated with anti-inflammatory properties through a decreased oxidation of lipids and better control of glucose serum levels, which are known for decreasing proinflammatory cytokines like plasma interleukins (55). Chronic inflammation contributes to several forms of cancers, and it is well known that this can stimulate prostate carcinogenesis (56, 57). Deschasaux et al. confirmed that high dietary fiber is inversely associated with PCa risk, especially for insoluble and legume fiber intake. However, the authors found no association between prostate cancer risk and soluble, cereal, vegetable, and fruit fiber intakes.
Phospholipid long-chain ω-3 fatty acids represent serum biomarkers of fatty acid intake, whose role in prostate cancer carcinogenesis has been recently suggested (58).
Brasky et al. (17) investigated the association between plasma LCω-3PUFA and PCa, confirming an increased prostate cancer risk.
3.2.1 Meat
The International Agency for Research on Cancer (WHO-IARC) classified processed meat intake as “carcinogenic to humans” and consumption of red meat as “probably carcinogenic to humans” (59). The carcinogenic role of processed and red meat was confirmed also in two case–control studies (19, 20), in which increased consumption was directly associated with increased risk of PCa, with a significant dose–response rate. Moreover, Bashir et al. (19) found a decreased risk association with fluid, vegetable, and fruit intake. Nevertheless, Diallo et al. (21) observed no correlation between red or processed meat intake and PCa but found that meat intake is involved in carcinogen-induced tumors such as colorectal cancer.
3.2.2 Diabetes
Glucose metabolism and chronic inflammation may have a role in PCa development (60), modulating signaling pathways and promoting uncontrolled cell proliferation and oxidative stress (61). Murtola et al. (23) evaluated prostate cancer risk in relation to normal and elevated serum glucose levels in diabetic patients. Diabetic patients with high blood glucose levels have an increased risk of overall PCa. The use of antidiabetic drugs and glucose level normalization is reported to contribute to decreasing the risk of PCa.
Miles et al. (22) studied its relationship with concentrated dietary sugar intake. Increased consumption of added or concentrated sugar-sweetened beverages (in the highest quartile) is related to an increased risk of PCa. There is a non-linear association instead with sugar intake from juices and desserts, suggesting a role of low glycemic index food selection in the prevention.
3.2.3 Body mass index and metabolic syndrome
The relationship between obesity, body mass index (BMI), and PCa has been extensively investigated in literature and was confirmed by the WCRF/AICR recommendations in 2018. In particular, obesity is related to lower concentrations of free testosterone and a decreased risk of localized/low-grade PCa and with an increased risk of advanced/high-grade PCa (62, 63). In two nested case–control studies from the SELECT and REDUCE trials (26, 27), increased BMI was found to be associated with a higher risk of high-grade PCa (Gleason score ≥7) in patients uninformed about PCa.
Nemesure et al. (24), in a case–control study on the Barbados population, found that a major correlation between waist size and waist–hip ratio is a measure of central adiposity and adiposity distribution, and prostate cancer risk. These results were confirmed also in another case–control study carried out by Boehm et al. (28). This suggests that body fat distribution may be more directly related to an increased high-grade risk PCa than BMI alone.
Abdominal obesity is closely related to metabolic syndrome (MetS), including insulin resistance, hypertension, impaired glucose tolerance, and lipid profile (64). According to some authors, late-onset hypogonadism (LOH), defined as the decrease of androgen levels, should be considered part of the MetS (65, 66). Kayali et al. (25) published a case–control study on the Turkish population subdividing patients into groups according to the presence of MetS and LOH. The authors found that the group with both MetS and LOH had an increased risk of prostate cancer, especially with aggressive histologic features.
In addition, the altered hepatic metabolism in non-alcoholic fatty liver disease (NAFLD), which is associated with metabolic syndrome, determines a suppression of the hepatic glucose leading to hyperglycemia, hypertriglyceridemia, and hyperinsulinemia (27, 67). Choi et al. (29) analyzed the correlation with PCa, suggesting that NAFLD is directly associated with an increased risk of prostate cancer, especially in non-obese patients with NAFLD.
Lastly, Jamnagerwalla et al. (30) found that high total serum cholesterol and high serum HDL are associated with an increased risk of high-grade PCa, thus confirming the importance of metabolic syndrome in the predisposition to PCa.
3.3 Use of drugs and vitamins
3.3.1 Use of hypertensive drugs
The use of hypertensive drugs is reported to increase the risk of mortality among patients diagnosed with prostate cancer. In particular, in a Finnish cohort of patients, Siltari et al. (33) found that ACE inhibitors and ATr blockers correlate with improved survival, while diuretics correlate with decreased survival.
Similarly, in a UK longitudinal cohort, Cardwell et al. reported that ACE inhibitors and ATr blockers decreased the risk of cancer-specific mortality (68).
The mechanism related to the role of ACE inhibitors and ATr blockers is unclear but probably involves the activity of angiotensin-II in mediating cell proliferation and fibrosis (69)
3.3.2 Use of aspirin and NSAIDs
Whereas regular aspirin administration probably protects from some malignancies, its exact role in the carcinogenesis of overall PCa and lethal PCa is still unclear. Downer et al. (32) found out that current and previous regular aspirin use (more than 200 mg per week) is associated with a lower lethal prostate cancer risk, especially compared to never users. In this study, the administration of aspirin after diagnosis had an impact on overall mortality. In a Finnish case–control study, Veitonmäki et al. (31) tested the association between non-steroidal anti-inflammatory drugs (NSAIDs) and PCa and found that NSAID users had an increased high-grade and all-grade PCa. This was similar for all types of NSAIDs tested, except for aspirin, which acted as a protective factor for overall prostate cancer risk.
3.3.3 Thyroxine, thyroid-stimulating hormone, and hypothyroid status
Triiodothyronine (T3) and thyroxine (T4) are thought to promote carcinogenesis through cell differentiation and development (54, 70). Mondul et al. (34) explored the relationship between circulating thyroid hormones, thyroid status, and prostate cancer risk. Compared with euthyroid men, the patients with high thyroid-stimulating hormone (TSH) and hypothyroidism had a decreased risk of PCa.
3.3.4 Vitamin and micronutrients
Vitamins are essential nutrients for human metabolism, and they play an important role as coenzymes in the normal functioning of the body as well as in many vital processes. In recent years, it has become clear that vitamins are essential for health and human disease (21, 70), thanks to several studies examining this correlation. However, according to Cancer Research UK, there is no reliable evidence that dietary supplements can help prevent cancer. Evidence in the literature is inconclusive and conflicting, with positive or no reported associations.
The 2018 WCRF/AICR recommendation downgraded lycopene and selenium supplementation from “may reduce prostate cancer risk” to “limited—inconclusive” (7). In fact, Morgia et al. (39) studied the incidence of PCa in a group of patients treated with selenium and lycopene in the previous Procomb study, but the evidence did not support a significant role for supplements in affecting prostate cancer risk. Conversely, Antwi et al. (38) carried out a case–control study among African American (AA) and European-American (EA) men from North America. They observed a higher intake of lycopene among EAs and a higher intake of beta-cryptoxanthin among AAs. Dietary lycopene and beta-cryptoxanthin have an indirect relationship with the development of high-grade PCa among EAs and AAs.
Vitamin E reduces DNA damage, enhances DNA repair, affects cellular responses to oxidative stress, inhibits cell proliferation, enhances immune responses, and reduces cellular testosterone levels (71). Albanes et al. (35) investigated the role of pre-supplementation of plasma α-tocopherol or γ-tocopherol in the development of high-grade (Gleason score 7–10) prostate cancer. Men with higher concentrations of α-tocopherol had a similar risk if compared to men with lower concentrations. Nevertheless, the authors found a strong positive association between plasma α-tocopherol and the risk of developing PCa in men receiving selenomethionine supplementation.
Retinol has been reported to promote cell differentiation and apoptosis. It increases the level of other antioxidants and regulates DNA transcription (63). Nash et al. (37) presented a nested case–control study evaluating the association of serum retinol and carotenoids with overall PCa risk. The authors found that serum retinol levels were associated with an increased risk of all grades of prostate cancer. Even in the placebo group, α-carotene was moderately positively associated with the risk of all grades of prostate cancer. In addition, Hada et al. (40), in 2015, prospectively investigated serum retinol and the overall risk of PCa as well as the role of α-tocopherol and β-carotene in overall PCa prevention. After multivariable adjustment, they concluded that high serum retinol was not associated with overall cancer risk but was associated with an increased risk of prostate cancer (72–74).
Vitamin D metabolites regulate cell growth and differentiation. The administration of vitamin D analogs suppresses prostate cancer progression in animal models and phase II studies (36, 37, 74). Schenk et al. (36) conducted a case–cohort study using data from the PCPT and found that high levels of serum 25(OH)-vitamin D slightly increased the risk of high-grade PCa and could reduce the risk of low-grade PCa.
Hoyt et al. (41) evaluated the relationship between dietary intake of phylloquinone, menaquinone, total vitamin K, and prostate cancer risk. The authors reported clear evidence of the role of vitamin K in the development of prostate cancer. In this study, the authors concluded that vitamin K intake affects the incidence of overall and advanced prostate cancer.
3.4 Drug use disorder
Drug use disorder (DUD) is reported to increase the risk of fatal prostate cancer. According to Dahlman et al. (13), DUD gives rise to a little increase in incident prostate cancer, but more interestingly, it is a statistically significant predictor of fatal prostate cancer. The authors hypothesize that in this group of patients, the underlying cause is the more advanced stage at diagnosis due to a delay in the diagnosis and treatment. This study is retrospective and based on the Swedish population.
In a previous study, Chhatre et al. reported that substance use disorders, including prescription drugs and recreational or non-legal substances, are related to an increase in mortality in patients diagnosed with advanced prostate cancer, particularly in patients with mental and behavioral disorders (75).
Similar results are reported by Jayadevappa et al. in a larger longitudinal cohort (76).
4 Discussion
In accordance with the latest World Cancer Research Fund International Continuous Update Project report on prostate 2018, a systematic and global analysis of the scientific research on prostate cancer, the present review shed more light on modifiable risk factors of prostate cancer, including diet, micronutrients, obesity, and metabolic syndrome, but may topics remain a matter of debate and controversial (54).
In the last years, many articles have been published on the refinements in the diagnosis of PCa (77) as well as on the algorithms for predicting the risk of recurrence after cutting-edge techniques for the treatment of this disease (78), but no comparable effort has been made in order to implement the strategies to prevent PCa.
Although not conclusive, our review contributes to clarifying potentially modifiable risk factors for the development of PCa and focuses on the role of some biochemical mechanisms not yet fully understood in the pathogenesis of PCa.
One of the major limitations of this review is its failure to quantify the risk for each risk factor considered. Unfortunately, different studies on a specific risk factor use different statistical analyses, so the results are often not comparable. If we found many studies obtaining appreciable results, it was not possible to achieve a cumulative result. As a consequence, for many risk factors, the results of our review could not be conclusive.
In addition, as many authors have highlighted, risk factors are often correlated with each other, thus making it much more difficult, or even impossible, to quantify the role of a single risk factor in the prevention of PCa. In this respect, we argue that policies for the prevention of PCa should not be addressed to a single risk factor, even if important in public health, but to a number of risk factors together, especially when working on lifestyle, diet, and sexual habits.
Noteworthy, major risk factors, such as tobacco, alcohol consumption, and DUD, are risk factors for many other diseases, like lung, liver, and bladder cancers, with well-established evidence in the literature showing that reducing these modifiable risk factors dramatically results in a decrease of the prevalence of these tumors.
Other risk factors concerning lifestyle, diet, and sexual habits are not strictly related to a specific pathology, especially when the reduction of these risk factors is not planned in the scenario of wider prevention policies aiming to improve the general health status. A policy aiming to improve the general health status of patients, through a reduction of modifiable risk factors concerning lifestyle, diet, and sexual habits, would lead to an improvement in quality of life and general health and in turn a decrease in the risk of developing cancer and other non-tumoral pathologies. In this view, PCa would be one of the targets of this policy.
Further studies are needed to reach proper evidence in the perspective that prevention may be effective in limiting the number of patients not undergoing treatment. In this view, the prevention of PCa may improve the quality of life due to the burden of complications and side effects of active treatment, such as surgery, radiotherapy, chemotherapy, and androgen deprivation, which are known for their negative impact on the quality of life.
Last but not least, preventing men from developing prostate cancer would be much more cost-effective for the healthcare systems of the majority of countries. All the efforts to facilitate the shift from the paradigm of treatment of PCa to the paradigm of its prevention (which has been called the “paradigm shift”) would be beneficial, and a deeper insight into the modifiable risk factors of this disease is of the utmost importance to plan policies for systematic prevention (77).
There is common agreement in the literature about the effectiveness of early diagnosis as a policy for cancer prevention. Although a tumor-specific marker for prostate cancer is not available as yet, the advent of PSA and its derivatives, like PSA-IgM, as well as other markers, like PCA-3, has been investigated with the aim to support the early diagnosis of prostate cancer (79–81). Multiparametric MRI has also revolutionized the detection of prostate cancer in its earliest stage (82–85). Unfortunately, overtreatment remains a matter of fact, with many men needing therapy for side effects related to treatment. For this reason, the policies aiming to prevent PCa should focus not only on detecting prostate cancer as early as possible but also on more efforts to the prevention of modifiable risk factors in order to achieve a decrease in the prevalence of prostate cancer and a consequent decrease of the side effects of treatment. This is particularly important when considering the overall costs of PCa.
It goes without saying that this concept of prevention is strictly related to education and cultural environment, which may be different in different countries. In this view, the policies to prevent modifiable risk factors for PCa may be different from country to country and should be made known early to patients.
The present review shows a number of modifiable risk factors that should be known and understood for the implementation of health policies, as well as for counseling patients as regards prostate cancer, particularly those who are at risk due to non-modifiable risk factors, such as familiarity, race, or genetics.
5 Conclusion
Prostate cancer is a major issue in men’s health, with an increased number of patients being diagnosed and treated due to the refinements in detection techniques in the last two decades. This led to overtreatment in some cases, unnecessary costs for the health systems, and the need to treat the side effects related to the treatment.
The implementation of policies of prevention may lead to less incidence of PCa. Due to the impossibility to act on non-modifiable risk factors, there is still the chance to apply policies able to decrease the impact of modifiable risk factors.
The present review of the literature showed that many risk factors are fit as targets of prevention policies. Unfortunately, we were not able to quantify the role of every single risk factor due to the fragmentation of the literature or even the presence of conflicting results in some cases. However, focusing on a wide range of risk factors allowed a deeper insight into the mechanisms of nutrients, lifestyle, habits, and drugs in preventing or facilitating PCa. This may support proper patient counseling as well as inform policies for prostate cancer prevention.
Author contributions
Study concept and design: FZ, UM. Data search and collection: AP, GI. Writing: AP, GG. Editing: AP, DC. Revision: AP, DC, FZ. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2018) 68::394–424. doi: 10.3322/caac.21492
3. Eeles RA, Al Olama AA, Benlloch S, Saunders EJ, Leongamornlert DA, Tymrakiewicz M, et al. Identification of 23 new prostate cancer susceptibility loci using the iCOGS custom genotyping array. Nat Genet (2013) 45:385–91. doi: 10.1038/ng.2560
4. Tan SH, Petrovics G, Srivastava S. Prostate cancer genomics: recent advances and the prevailing underrepresentation from racial and ethnic minorities. Int J Mol Sci (2018) 19:1255. doi: 10.3390/ijms19041255
5. Ballon-Landa E, Parsons JK. Nutrition, physical activity, and lifestyle factors in prostate cancer prevention. Curr Opin Urol (2018) 28:55–61. doi: 10.1097/MOU.0000000000000460
6. Clinton SK, Giovannucci EL, Hursting SD. The world cancer research fund/american institute for cancer research third expert report on diet, nutrition, physical activity, and cancer: impact and future directions. J Nutr (2020) 150:663–71. doi: 10.1093/jn/nxz268
7. World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective (2018). Continuous Update Project. Available at: http://dietandcancerreport.org (Accessed 14 February 2023).
8. Liberati A, Altman DG, Tetzlaff J, Murlow C, Gotzsche P, Joannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PloS Med (2009) 6(7):e1000100. doi: 10.1371/journal.pmed.1000100
9. Zuccolo L, Lewis SJ, Donovan JL, Hamdy FC, Neal DE, Davey Smith G, et al. Alcohol consumption and PSA-detected prostate cancer risk–a case-control nested in the ProtecT study. Int J Cancer (2013) 132:2176–85. doi: 10.1002/ijc.27877
10. Fowke JH, Howard L, Andriole GL, Freedland SJ. Alcohol intake increases high-grade prostate cancer risk among men taking dutasteride in the REDUCE trial. Eur Urol (2014) 66:1133–8. doi: 10.1016/j.eururo.2014.01.037
11. Chhim AS, Fassier P, Latino-Martel P, Zelek L, Duverger L, Hercberg S, et al. Prospective association between alcohol intake and hormone-dependent cancer risk: modulation by dietary fiber intake. Am J Clin Nutr (2015) 102:182–9. doi: 10.3945/ajcn.114.098418
12. Ho T, Howard LE, Vidal AC, Gerber L, Moreira D, McKeever M, et al. Smoking and risk of low- and high-grade prostate cancer: results from the REDUCE study. Clin Cancer Res (2014) 20:5331–8. doi: 10.1158/1078-0432
13. Dahlman D, Li X, Crump C, Sundquist J, Sundquist K. Drug use disorder and risk of incident and fatal prostate cancer in Swedish men: a nationwide epidemiological study. Cancer Causes Contr (2022) 33:313–22. doi: 10.1007/s10552-021-01513-2
14. Spence AR, Rousseau MC, Parent ME. Sexual partners, sexually transmitted infections, and prostate cancer risk. Cancer Epidemiol (2014) 38:700–7. doi: 10.1016/j.canep.2014.09.005
15. Rider JR, Wilson KM, Sinnott JA, Kelly RS, Mucci LA, Giovannucci EL. Ejaculation frequency and risk of prostate cancer: updated results with an additional decade of follow-up. Eur Urol (2016) 70:974–82. doi: 10.1016/j.eururo.2016.03.027
16. Cirakoglu A, Benli E, Yuce A. Polygamy, sexual behavior in a population under risk for prostate cancer diagnostic: an observational study from the Black Sea Region in Turkey. Int Braz J Urol (2018) 44:704–8. doi: 10.1590/S1677-5538
17. Brasky TM, Darke AK, Song X, Tangen CM, Goodman PJ, Thompson IM, et al. Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst (2013) 105:1132–41. doi: 10.1093/jnci/djt174
18. Deschasaux M, Pouchieu C, His M, Hercberg S, Latino-Martel P, Touvier M. Dietary total and insoluble fiber intakes are inversely associated with prostate cancer risk. J Nutr (2014) 144:504–10. doi: 10.3945/jn.113.189670
19. Bashir MN, Malik MA. Case-control study of diet and prostate cancer in a rural population of Faisalabad, Pakistan. Asian Pac J Cancer Prev (2015) 16:2375–8. doi: 10.7314/apjcp.2015.16.6.2375
20. Stefani ED, Boffetta PL, Ronco A, Deneo-Pellegrini H. Meat consumption, related nutrients, obesity and risk of prostate cancer: a case-control study in uruguay. Asian Pac J Cancer Prev (2016) 17:1937–45. doi: 10.7314/apjcp.2016.17.4.1937
21. Diallo A, Deschasaux M, Latino-Martel P, Hercberg S, Galan P, Fassier P, et al. Red and processed meat intake and cancer risk: results from the prospective NutriNet-Santé cohort study. Int J Cancer (2018) 142:230–7. doi: 10.1002/ijc.31046
22. Miles FL, Neuhouser ML, Zhang ZF. Concentrated sugars and incidence of prostate cancer in a prospective cohort. Br J Nutr (2018) 120:703–10. doi: 10.1017/S0007114518001812
23. Murtola TJ, Vihervuori VJ, Lahtela J, Talala K, Taari K, Tammela TL, et al. Fasting blood glucose, glycemic control and prostate cancer risk in the Finnish randomized study of screening for prostate cancer. Br J Cancer (2018) 118:1248–54. doi: 10.1038/s41416-018-0055-4
24. Nemesure B, Wu SY, Hennis A, Leske MC. Prostate Cancer in a Black Population (PCBP) study group. Central adiposity and prostate cancer in a black population. Cancer Epidemiol Biomarkers Prev (2012) 21:851–8. doi: 10.1158/1055-9965
25. Kayali M, Balci M, Aslan Y, Bilgin O, Guzel O, Tuncel A, et al. The relationship between prostate cancer and presence of metabolic syndrome and late-onset hypogonadism. Urology (2014) 84:1448–52. doi: 10.1016/j.urology.2014.07.015
26. Liang Y, Ketchum NS, Goodman PJ, Klein EA, Thompson IM Jr. Is there a role for body mass index in the assessment of prostate cancer risk on biopsy? J Urol (2014) 192:1094–9. doi: 10.1016/j.juro.2014.04.015
27. Vidal AC, Howard LE, Moreira DM, Castro-Santamaria R, Andriole GL Jr, Freedland SJ, et al. Obesity increases the risk for high-grade prostate cancer: results from the REDUCE study. Cancer Epidemiol Biomarkers Prev (2014) 23:2936–42. doi: 10.1158/1055-9965
28. Boehm K, Sun M, Larcher A, Blanc-Lapierre A, Schiffmann J, et al. Waist circumference, waist-hip ratio, body mass index, and prostate cancer risk: results from the North-American case-control study Prostate Cancer and Environment Study. Urol Oncol (2015) 33:494.e1–7. doi: 10.1016/j.urolonc.2015.07.006
29. Choi YJ, Lee DH, Han KD, Yoon H, Shin CM, Park YS, et al. Is nonalcoholic fatty liver disease associated with the development of prostate cancer? A nationwide study with 10,516,985 Korean men. PloS One (2018) 13:e0201308. doi: 10.1371/journal.pone.0201308
30. Jamnagerwalla J, Howard LE, Allott EH, Vidal AC, Moreira DM, Castro-Santamaria R, et al. Serum cholesterol and risk of high-grade prostate cancer: results from the REDUCE study. Prostate Cancer Prostatic Dis (2018) 21:252–59. doi: 10.1038/s41391-017-0030-9
31. Veitonmäki T, Tammela TL, Auvinen A, Murtola TJ. Use of aspirin, but not other non-steroidal anti-inflammatory drugs is associated with decreased prostate cancer risk at the population level. Eur J Cancer (2013) 49:938–45. doi: 10.1016/j.ejca.2012.09.030
32. Downer MK, Allard CB, Preston MA, Gaziano JM, Stampfer MJ, Mucci LA, et al. Regular Aspirin use and the risk of lethal prostate cancer in the Physicians' Health Study. Eur Urol (2017) 72:821–27. doi: 10.1016/j.eururo.2017.01.044
33. Siltari A, Murtola TJ, Talala K, Taari K, Tammela TLJ, Auvinen A. Antihypertensive drug use and prostate cancer-specific mortality in Finnish men. PloS One (2020) 15:e0234269. doi: 10.1371/journal.pone.0234269
34. Mondul AM, Weinstein SJ, Bosworth T, Remaley AT, Virtamo J, Albanes D. Circulating thyroxine, thyroid-stimulating hormone, and hypothyroid status and the risk of prostate cancer. PloS One (2012) 7:e47730. doi: 10.1371/journal.pone.0047730
35. Albanes D, Till C, Klein EA, Goodman PJ, Mondul AM, Weinstein SJ, et al. Plasma tocopherols and risk of prostate cancer in the Selenium and Vitamin E Cancer Prevention Trial (SELECT). Cancer Prev Res (Phila) (2014) 7:886–95. doi: 10.1158/1940-6207.CAPR-14-0058
36. Schenk JM, Till CA, Tangen CM, Goodman PJ, Song X, Torkko KC, et al. Serum 25-hydroxyvitamin D concentrations and risk of prostate cancer: results from the Prostate Cancer Prevention Trial. Cancer Epidemiol Biomarkers Prev (2014) 23:1484–93. doi: 10.1158/1055-9965
37. Nash SH, Till C, Song X, Lucia MS, Parnes HL, Thompson IM Jr, et al. Serum Retinol and Carotenoid concentrations and prostate cancer risk: results from the Prostate Cancer Prevention Trial. Cancer Epidemiol Biomarkers Prev (2015) 24:1507–15. doi: 10.1158/1055-9965
38. Antwi SO, Steck SE, Su LJ, Hebert JR, Zhang H, Craft NE, et al. Carotenoid intake and adipose tissue carotenoid levels in relation to prostate cancer aggressiveness among African-American and European-American men in the North Carolina-Louisiana prostate cancer project (PCaP). Prostate (2016) 76:1053–66. doi: 10.1002/pros.23189
39. Morgia G, Voce S, Palmieri F, Gentile M, Iapicca G, Giannantoni A, et al. Association between selenium and lycopene supplementation and incidence of prostate cancer: Results from the post-hoc analysis of the procomb trial. Phytomedicine (2017) 34:1–5. doi: 10.1016/j.phymed.2017.06.008
40. Hada M, Mondul AM, Weinstein SJ, Albanes D. Serum retinol and risk of overall and site-specific cancer in the ATBC Study. Am J Epidemiol (2020) 189:532–42. doi: 10.1093/aje/kwz226
41. Hoyt M, Reger M, Marley A, Fan H, Liu Z, Zhang J, et al. Vitamin K intake and prostate cancer risk in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial. Am J Clin Nutr (2019) 109:392–401. doi: 10.1093/ajcn/nqy251
42. Klein EA, Thompson IM Jr, Tangen CM, Crowley JJ, Scott Lucia M, Goodman PJ, et al. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). Jama (2011) 306:1549–56. doi: 10.1001/jama.2011.1437
43. Lane JA, Hamdy FC, Martin RM, Turner EL, Niel DE, Donovan JL. Latest results from the UK trials evaluating prostate cancer screening and treatment: the CAP and ProtecT studies. Eur J Cancer (2010) 46:3095–101. doi: 10.1016/j.ejca.2010.09.016
44. The alpha-tocopherol, beta-carotene lung cancer prevention study: design, methods, participant characteristics, and compliance. The ATBC Cancer Prevention Study Group. Ann Epidemiol (1994) 4:1–10. doi: 10.1016/1047-2797(94)90036-1
45. Andriole GL, Bostwick DG, Brawley OW, Gomella LG, Margerger M, Montorsi F, et al. Effect of dutasteride on the risk of prostate cancer. N Engl J Med (2010) 362:1192–202. doi: 10.1056/NEJMoa0908127
46. Thompson IM, Goodman PJ, Tangen CM, Scott Lucia M, Miller GJ, Ford LG, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med (2003) 349:215–24. doi: 10.1056/NEJMoa030660
47. Hercberg S, Galan P, Preziosi P, Mennen L, Malvy D, Roussel A-M, et al. The SU.VI.MAX Study: a randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch Intern Med (2004) 164:2335–42. doi: 10.1001/archinte.164.21.2335
48. Steering Committee of the Physicians’ Health Study Research Group. Final report on the aspirin component of the ongoing Physicians' Health Study. N Engl J Med (1989) 321:129–35. doi: 10.1056/NEJM198907203210301
49. Prorok PC, Andriole GL, Bresalier RS, Buys SS, Chia D, Crawford ED, et al. Design of the Prostate, Lung, Colorectal and Ovarian (PLCO) cancer screening trial. Control Clin Trials (2000) 21:273s–309s. doi: 10.1016/S0197-2456(00)00098-2
50. Kilpeläinen TP, Tammela TL, Malila N, Hakama M, Santti H, Maattanan L, et al. Prostate cancer mortality in the Finnish randomized screening trial. J Natl Cancer Inst (2013) 105:719–25. doi: 10.1093/jnci/djt038
51. Hercberg S, Castetbon K, Czernichow S, Malon A, Mejean C, Kesse E, et al. The Nutrinet-Santé Study: a web-based prospective study on the relationship between nutrition and health and determinants of dietary patterns and nutritional status. BMC Public Health (2010) 10:242. doi: 10.1186/1471-2458-10-242
52. Brookman-May SD, Campi R, Henríquez JDS, Klatte T, Langenhuijsen JF, Brausi M, et al. Latest evidence on the impact of smoking, sports, and sexual activity as modifiable lifestyle risk factors for prostate cancer incidence, recurrence, and progression: a systematic review of the literature by the European Association of Urology Section of Oncological Urology (ESOU). Eur Urol Focus (2019) 5:756–87. doi: 10.1016/j.euf.2018.02.007
53. Jian Z, Ye D, Chen Y, Li H, Wang K. Sexual activity and risk of prostate cancer: a dose-response meta-analysis. J Sex Med (2018) 15:1300–09. doi: 10.1016/j.jsxm.2018.07.004
54. Shaneyfelt T, Husein R, Bubley G, Mantzoros CS. Hormonal predictors of prostate cancer: a meta-analysis. J Clin Oncol (2000) 18:847–53. doi: 10.1200/JCO.2000.18.4.847
55. Ma Y, Griffith JA, Chasan-Taber L, Olendzki BC, Jackson E, Stanek EJ 3rd, et al. Association between dietary fiber and serum C-reactive protein. Am J Clin Nutr (2006) 83:760–6. doi: 10.1093/ajcn/83.4.760
56. Sfanos KS, De Marzo AM. Prostate cancer and inflammation: the evidence. Histopathology (2012) 60:199–215. doi: 10.1111/j.1365-2559.2011.04033.x
57. Touvier M, Fezeu L, Ahluwalia N, Julia C, Charnaux N, Sutton A, et al. Association between prediagnostic biomarkers of inflammation and endothelial function and cancer risk: a nested case-control study. Am J Epidemiol (2013) 177:3–13. doi: 10.1093/aje/kws359
58. Brasky TM, Till C, White E, Neuhouser ML, Song X, Goodman P, et al. Serum phospholipid fatty acids and prostate cancer risk: results from the prostate cancer prevention trial. Am J Epidemiol (2011) 173:1429–39. doi: 10.1093/aje/kwr027
59. Bouvard V, Loomis D, Guyton KZ, Grosse Y, Ghissassi FE, Benbrahim-Tallaa L, et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol (2015) 16:1599–600. doi: 10.1016/S1470-2045(15)00444-1
60. Murtola TJ, Wahlfors T, Haring A, Taari K, Stenman UH, Tammela TL, et al. Polymorphisms of genes involved in glucose and energy metabolic pathways and prostate cancer: interplay with metformin. Eur Urol (2015) 68:1089–97. doi: 10.1016/j.eururo.2015.03.026
61. Arthur R, Møller H, Garmo H, Holmberg L, Stattin P, Malmstrom H, et al. Association between baseline serum glucose, triglycerides and total cholesterol, and prostate cancer risk categories. Cancer Med (2016) 5:1307–18. doi: 10.1002/cam4.665
62. Freedland SJ, Bañez LL, Sun LL, Fitzsimons NJ, Moul JW. Obese men have higher-grade and larger tumors: an analysis of the duke prostate center database. Prostate Cancer Prostatic Dis (2009) 12:259–63. doi: 10.1038/pcan.2009.11
63. Endogenous Hormones and Prostate Cancer Collaborative Group, Roddam AW, Allen NE, Appleby P, Key TJ. Endogenous sex hormones and prostate cancer: a collaborative analysis of 18 prospective studies. J Natl Cancer Inst (2008) 100:170–83. doi: 10.1093/jnci/djm323
64. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome. An American Heart Association/ National Heart, Lung, and Blood Institute Scientific Statement. Circulation (2005) 112:2735–52. doi: 10.1161/CIRCULATIONAHA.105.169404
65. Laaksonen DE, Niskanen L, Punnonen K, Nyyssönen K, Tuomainen TP, Salonen R, et al. Sex hormones, inflammation and the metabolic syndrome: a population based study. Eur J Endocrinol (2003) 149:601–8. doi: 10.1530/eje.0.1490601
66. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer statistics, 2008. CA Cancer J Clin (2008) 58:71–96. doi: 10.3322/CA.2007.0010
67. European Association for the Study of the Liver, European Association for the Study of Diabetes, European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Obes facts (2016) 9:65–90. doi: 10.1159/000443344
68. Cardwell CR, Coleman HG, Murray LJ, O'Sullivan JM, Powe DG. Beta-blocker usage and prostate cancer survival: a nested case-control study in the UK Clinical Practice Research Datalink cohort. Cancer Epidemiol (2014) 38:279–85. doi: 10.1016/j.canep.2014.03.011
69. Atlas SA. The renin-angiotensin aldosterone system: pathophysiological role and pharmacologic inhibition. J Manag Care Pharm (2007) 13(8 Suppl B):9–20. doi: 10.18553/jmcp.2007.13.s8-b.9
70. Gaziano JM, Sesso HD, Christen WG, Bubes V, Smith JP, MacFadyen J, et al. Multivitamins in the prevention of cancer in men: the Physicians' Health Study II randomized controlled trial. JAMA (2012) 308:1871–80. doi: 10.1001/jama.2012.14641
71. Chan JM, Darke AK, Penney KL, Tangen CM, Goodman PJ, Lee GM, et al. Selenium- or Vitamin E-related gene variants, interaction with supplementation, and risk of high-grade prostate cancer in SELECT. Cancer Epidemiol Biomarkers Prev (2016) 25:1050–8. doi: 10.1158/1055-9965.EPI-16-0104
72. Nemesure B, Wu SY, Hennis A, Leske MC, Barbados Eye Studies Group, et al. Nine-year incidence of obesity and overweight in an African-origin population. Int J Obes (Lond) (2008) 32:329–35. doi: 10.1038/sj.ijo.0803721
73. Barrington WE, Schenk JM, Etzioni R, Arnold KB, Neuhouser ML, Thompson IM Jr, et al. Difference in association of obesity wth prostate cancer risk between US African American and Non-Hispanic white men in the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA Oncol (2015) 1:342–9. doi: 10.1001/jamaoncol.2015.0513
74. Gilbert R, Metcalfe C, Fraser WD, Donovan J, Hamdy F, Neal DE, et al. Associations of circulating retinol, vitamin E, and 1,25-dihydroxyvitamin D with prostate cancer diagnosis, stage, and grade. Cancer Causes Control (2012) 23:1865–73. doi: 10.1007/s10552-012-0052-5
75. Chhatre S, Metzger DS, Malkowicz SB, Woody G, Jayadevappa R. Substance use disorder and its efects on outcomes in men with advanced-stage prostate cancer. Cancer (2014) 120:3338–45. doi: 10.1002/cncr.28861
76. Jayadevappa R, Chhatre S. Association between age, substance use, and outcomes in Medicare enrollees with prostate cancer. J Geriatr Oncol (2016) 7:444–52. doi: 10.1016/j.jgo.2016.06.007
77. Ziglioli F, Granelli G, Cavalieri D, Bocchialini T, Maestroni U, et al. What chance do we have to decrease prostate cancer overdiagnosis and overtreatment? A narrative review. Acta BioMed (2019) 90:423–6. doi: 10.23750/abm.v90i4.9070
78. Maestroni U, Morandin F, Ferretti S, Dinale F, Ziglioli F, et al. Recurrence of prostate cancer after HIFU. Proposal of a novel predictive index. Acta BioMed (2018) 89:220–6. doi: 10.23750/abm.v89i2.6730
79. Gallotta A, Ziglioli F, Ferretti S, Maestroni U, Moretti M, Aloe R, et al. A novel algorithm for the prediction of prostate cancer in clinically suspected patients. Cancer biomark (2013) 13(4):227–34. doi: 10.3233/CBM-130357
80. Maestroni U, Cavalieri DM, Campobasso D, Guarino G, Ziglioli F. PSA-IgM and iXip in the diagnosis and management of prostate cancer: clinical relevance and future potential. A review Acta Biomed (2022) 92(6):e2021344. doi: 10.23750/abm.v92i6.12058
81. Freedland SJ. Screening, risk assessment, and the approach to therapy in patients with prostate cancer. Cancer (2011) 117:1123–35. doi: 10.1002/cncr.25477
82. Rouvière O, Puech P, Renard-Penna R, Claudon M, Roy C, Mège-Lechevallier F, et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRIFIRST): a prospective, multicentre, paired diagnostic study. Lancet Oncol (2019) 20:100–9. doi: 10.1016/S1470-2045(18)30569-2
83. Ziglioli F, Maestroni U, Manna C, Negrini G, Granelli G, Greco V, et al. Multiparametric MRI in the management of prostate cancer: an update-a narrative review. Gland Surg (2020) 9(6):2321–30. doi: 10.21037/gs-20-561
84. Schirò S, Milanese G, Maddalo M, Ziglioli F, Maestroni UV, Manna C, et al. MR-based simplified extraprostatic extension evaluation: comparison of performances of different predictive models. Eur Radiol (2023) 33(4):2975–84. doi: 10.1007/s00330-022-09240-1
Keywords: prostate cancer, risk factors, prevention, lifestyle, prevention policy
Citation: Ziglioli F, Patera A, Isgrò G, Campobasso D, Guarino G and Maestroni U (2023) Impact of modifiable lifestyle risk factors for prostate cancer prevention: a review of the literature. Front. Oncol. 13:1203791. doi: 10.3389/fonc.2023.1203791
Received: 11 April 2023; Accepted: 06 July 2023;
Published: 08 September 2023.
Edited by:
Andrea Venerando, University of Udine, ItalyReviewed by:
Giorgio Cozza, University of Padua, ItalyJordi Vilardell Vila, Autonomous University of Barcelona, Spain
Copyright © 2023 Ziglioli, Patera, Isgrò, Campobasso, Guarino and Maestroni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Ziglioli, ZnppZ2xpb2xpQGFvLnByLml0