 Viktor Grünwald1*
Viktor Grünwald1* Thomas Powles2
Thomas Powles2 Masatoshi Eto3Evgeny Kopyltsov4Sun Young Rha5
Masatoshi Eto3Evgeny Kopyltsov4Sun Young Rha5 Camillo Porta6
Camillo Porta6 Robert Motzer7
Robert Motzer7 Thomas E. Hutson8María José Méndez-Vidal9
Thomas E. Hutson8María José Méndez-Vidal9 Sung-Hoo Hong10
Sung-Hoo Hong10 Eric Winquist11Jeffrey C. Goh12
Eric Winquist11Jeffrey C. Goh12 Pablo Maroto13
Pablo Maroto13 Tomas Buchler14
Tomas Buchler14 Toshio Takagi15Joseph E. Burgents16
Toshio Takagi15Joseph E. Burgents16 Rodolfo Perini17Cixin He18Chinyere E. Okpara19Jodi McKenzie20
Rodolfo Perini17Cixin He18Chinyere E. Okpara19Jodi McKenzie20 Toni K. Choueiri21
Toni K. Choueiri21- 1Clinic for Medical Oncology and Clinic for Urology, University Hospital Essen, Essen, Germany
- 2Barts Cancer Institute and the Royal Free Hospital, Queen Mary University of London, London, United Kingdom
- 3Department of Urology, Kyushu University, Fukuoka, Japan
- 4State Institution of Healthcare Regional Clinical Oncology Dispensary, Omsk, Russia
- 5Department of Internal Medicine, Yonsei Cancer Center, Yonsei University Health System, Seoul, Republic of Korea
- 6Department of Biomedical Sciences and Human Oncology, University of Bari ‘A. Moro’, Bari, Italy
- 7Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, United States
- 8Medical Oncology, Texas Oncology, Dallas, TX, United States
- 9Department of Oncology, Maimonides Institute for Biomedical Research of Córdoba (IMIBIC) Hospital Universitario Reina Sofía, Córdoba, Spain
- 10Department of Urology, Seoul St. Mary’s Hospital, The Catholic University of Korea, Seoul, Republic of Korea
- 11Department of Oncology, University of Western Ontario, London, ON, Canada
- 12ICON Research, South Brisbane & University of Queensland, St Lucia, QLD, Australia
- 13Department of Medical Oncology, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
- 14Department of Oncology, Charles University and Thomayer University Hospital, Prague, Czechia
- 15Department of Urology, Tokyo Women’s Medical University, Tokyo, Japan
- 16Global Clinical Development, Merck & Co., Inc., Rahway, NJ, United States
- 17Clinical Research, Merck & Co., Inc., Rahway, NJ, United States
- 18Biostatistics, Eisai Inc., Nutley, NJ, United States
- 19Clinical Research, Eisai Ltd., Hatfield, United Kingdom
- 20Clinical Research, Eisai Inc., Nutley, NJ, United States
- 21Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, United States
Introduction: The phase 3 CLEAR study demonstrated that lenvatinib plus pembrolizumab significantly improved efficacy versus sunitinib as first-line treatment for patients with advanced renal cell carcinoma (RCC). Prognostic features including presence and/or site of baseline metastases, prior nephrectomy, and sarcomatoid features have been associated with disease and treatment success. This subsequent analysis explores outcomes in patients with or without specific prognostic features.
Methods: In CLEAR, patients with clear cell RCC were randomly assigned (1:1:1) to receive either lenvatinib (20 mg/day) plus pembrolizumab (200 mg every 3 weeks), lenvatinib (18 mg/day) plus everolimus (5 mg/day), or sunitinib alone (50 mg/day, 4 weeks on, 2 weeks off). In this report, progression-free survival (PFS), overall survival (OS), and objective response rate (ORR) were all assessed in the lenvatinib-plus-pembrolizumab and the sunitinib arms, based on baseline features: lung metastases, bone metastases, liver metastases, prior nephrectomy, and sarcomatoid histology.
Results: In all the assessed subgroups, median PFS was longer with lenvatinib-plus-pembrolizumab than with sunitinib treatment, notably among patients with baseline bone metastases (HR 0.33, 95% CI 0.21–0.52) and patients with sarcomatoid features (HR 0.39, 95% CI 0.18–0.84). Median OS favored lenvatinib plus pembrolizumab over sunitinib irrespective of metastatic lesions at baseline, prior nephrectomy, and sarcomatoid features. Of interest, among patients with baseline bone metastases the HR for survival was 0.50 (95% CI 0.30–0.83) and among patients with sarcomatoid features the HR for survival was 0.91 (95% CI 0.32–2.58); though for many groups, median OS was not reached. ORR also favored lenvatinib plus pembrolizumab over sunitinib across all subgroups; similarly, complete responses also followed this pattern.
Conclusion: Efficacy outcomes improved following treatment with lenvatinib-plus-pembrolizumab versus sunitinib in patients with RCC—irrespective of the presence or absence of baseline lung metastases, baseline bone metastases, baseline liver metastases, prior nephrectomy, or sarcomatoid features. These findings corroborate those of the primary CLEAR study analysis in the overall population and support lenvatinib plus pembrolizumab as a standard of care in 1L treatment for patients with advanced RCC.
Clinical trial registration: ClinicalTrials.gov, identifier NCT02811861
1 Introduction
Kidney cancer is one of the most frequently diagnosed cancers in the United States, and the activity of traditional cytotoxic chemotherapy is limited in patients with metastatic renal cell carcinoma (RCC) (1). The phase 3 multicenter, open-label, randomized, CLEAR study (Study 307/KEYNOTE-581) compared the efficacy and safety of lenvatinib plus pembrolizumab or everolimus versus sunitinib as a first-line treatment for patients with advanced RCC (2). In the primary analysis of CLEAR, lenvatinib plus pembrolizumab demonstrated statistically significant and clinically meaningful improvement in efficacy outcomes versus sunitinib (2): median progression-free survival (PFS) was 24 months versus 9 months, respectively (hazard ratio [HR] 0.39; 95% confidence interval [CI] 0.32–0.49; P < 0.001); median overall survival (OS) was not reached for either arm (HR 0.66; 95% CI 0.49–0.88; P = 0.005); and objective response rate (ORR) was 71% versus 36%, respectively (relative risk with lenvatinib plus pembrolizumab versus sunitinib, 1.97; 95% CI 1.69–2.29) (2). The median duration of survival follow-up in the CLEAR study was 26.6 months. The safety profile for the lenvatinib plus pembrolizumab combination was consistent with that of the monotherapies, with no new safety signals.
While CLEAR showed statistically significant and clinically meaningful efficacy in the overall population, some clinical characteristics of patients with RCC can impact disease status and may play a role in physicians’ treatment decisions and patient outcomes. Such characteristics include the presence/location of metastases (specifically lung, bone, and liver), whether or not patients had a nephrectomy prior to treatment, and the presence or absence of sarcomatoid features, and these may all be considered prognostic indicators of the disease (3–5). The most common sites of metastasis in patients with RCC are lung, bone, lymph nodes, and liver (3, 6, 7). The lung is the most common site of metastasis in patients with clear cell RCC (3, 8); these patients often have more promising OS durations (median 25.1 months, 95% CI 24.1–26.0) than patients who have RCC with metastases to other sites (3, 8). Bone metastases are associated with skeletal-related events (ie, fractures, spinal cord compression, hypercalcemia, and bone pain) that impair quality of life and can lead to lower rates of survival (9–11). In a characterization of metastatic sites in patients with RCC that accessed data from more than 11000 patients from the International mRCC Database Consortium, median OS among patients with bone metastases was 19.4 months (95% CI 18.1–20.5) (3). While liver metastases are less common than bone or lung metastases, prognoses and OS rates are poor among patients with liver metastases (median OS 17.6 months; 95% CI 16.0–19.2) (3, 12).
Although localized RCC is initially treated by nephrectomy, with adjuvant pembrolizumab treatment depending on disease state and/or histology (7), 25% to 30% of patients develop metastatic disease following nephrectomy (13, 14); until recently, cytoreductive nephrectomy was widely used in the case of metastatic disease (15). While partial nephrectomy can be preferred to radical nephrectomy, it is generally considered not suitable for patients with advanced tumors (7). Sarcomatoid features can occur in most histologic subtypes of RCC (5, 16). Patients who have RCC with a sarcomatoid component (in approximately 20% of tumors from patients with advanced RCC) have a poor prognosis and low 5-year survival rate compared with patients without sarcomatoid features (5, 12, 16, 17), and treatment options for these patients is an important unmet need (18).
This analysis explored efficacy outcomes in subgroups of patients with or without specific baseline features (ie, lung metastases, bone metastases, liver metastases, prior nephrectomy, and sarcomatoid histology) using data from the lenvatinib plus pembrolizumab and sunitinib arms of CLEAR.
2 Methods
2.1 Patients
In CLEAR, patients were randomly assigned (1:1:1) to receive either lenvatinib 20 mg orally once daily plus pembrolizumab 200 mg intravenously once every 3 weeks; lenvatinib 18 mg plus everolimus 5 mg orally once daily; or sunitinib 50 mg orally once daily (4 weeks on/2 weeks off). Key eligibility criteria included: advanced RCC with no prior systemic therapy; at least 1 measurable lesion per Response Evaluation Criteria In Solid Tumors version 1.1 (RECIST v1.1); and a Karnofsky performance-status score ≥ 70. Additional eligibility criteria have been published (2). Randomization was stratified by geographic region (ie, Western Europe and North America or rest of the world) and by Memorial Sloan Kettering Cancer Center prognostic risk group (ie, favorable, intermediate, or poor risk).
2.2 Study design
CLEAR was a multicenter, open-label, randomized study that compared efficacy and safety of lenvatinib plus pembrolizumab or everolimus versus sunitinib in patients with RCC. The primary endpoint was PFS, as assessed by an independent review committee (IRC) using RECIST v1.1. Key secondary endpoints included OS, and ORR as assessed by IRC using RECIST v1.1. Results of the primary and key secondary endpoints have been published (2).
The trial was conducted in accordance with the International Council for Harmonisation Good Clinical Practice Guidelines and the principles of the 2013 Declaration of Helsinki. Institutional review boards or independent ethics committees approved the protocol and appropriate related documents; all patients provided written informed consent. Safety and efficacy data were monitored by an independent data and safety monitoring committee.
2.3 Statistics
Median PFS and OS for the lenvatinib-plus-pembrolizumab and sunitinib arms were estimated using the Kaplan–Meier method; HR and 95% CIs comparing lenvatinib-plus-pembrolizumab versus sunitinib arms were estimated by a stratified Cox model. If a stratification factor was itself a subgroup, this factor was removed from the stratified analysis. The subgroups/strata with sample size less than 5% of the treatment group are not displayed. Odds ratios were used to compare ORRs for the lenvatinib-plus-pembrolizumab and sunitinib arms. This preplanned subgroup analysis compared PFS, OS, and ORR in the lenvatinib-plus-pembrolizumab arm versus the sunitinib arm, based on selected baseline features comprising lung metastases, bone metastases, liver metastases, prior nephrectomy, and sarcomatoid histology. Patients could be included in multiple categories simultaneously. Programmed cell death ligand-1 (PD-L1) status may be another prognostic factor that can inform clinical decisions; however, data on PD-L1 status have previously been published (2) and are not included here. Data by International Metastatic Renal Cell Carcinoma Database Consortium risk group and Memorial Sloan Kettering Cancer Center risk group are included for reference. All results of this subgroup analysis are descriptive.
3 Results
3.1 Patients
Of the 1069 patients randomly assigned to treatment in CLEAR, 355 were randomly assigned to receive lenvatinib plus pembrolizumab and 357 to receive sunitinib (2). Baseline characteristics of patients in these 2 arms have previously been published (2), and are summarized in Table 1. Among patients in the lenvatinib-plus-pembrolizumab arm, 249 (70.1%) had lung metastases, 85 (23.9%) had bone metastases, and 60 (16.9%) had liver metastases. In the sunitinib arm, 239 (66.9%) patients had lung metastases, 97 (27.2%) had bone metastases, and 61 (17.1%) had liver metastases. Of the patients who had bone metastases (85 patients in the lenvatinib-plus-pembrolizumab arm and 97 patients in the sunitinib arm), 11 (12.9% of patients with bone metastasis in the lenvatinib-plus-pembrolizumab arm) and 21 (21.6% of patients with bone metastasis in the sunitinib arm), received concomitant bone-targeting treatment. Most patients (262 [73.8%] in the lenvatinib-plus-pembrolizumab arm and 275 [77.0%] in the sunitinib arm) had undergone a prior nephrectomy (2). Sarcomatoid features were observed in 28 (7.9%) patients in the lenvatinib-plus-pembrolizumab arm and in 21 (5.9%) patients in the sunitinib arm (2). The number of patients with MSKCC and International Metastatic RCC Database Consortium (IMDC) favorable/intermediate/poor risk in the lenvatinib-plus-pembrolizumab arm (MSKCC: 96 [27.0%]/227 [63.9%]/32 [9.0%]; IMDC: 110 [31.0%]/210 [59.2%]/33 [9.3%]) and sunitinib arm (MSKCC: 97 [27.2%]/228 [63.9%]/32 [9.0%]; IMDC: 124 [34.7%]/192 [53.8%]/37 [10.4%]) have been previously reported (2). Data for these groups are included for reference (Table 1; Figures 1–3; Supplementary Table 1) throughout.
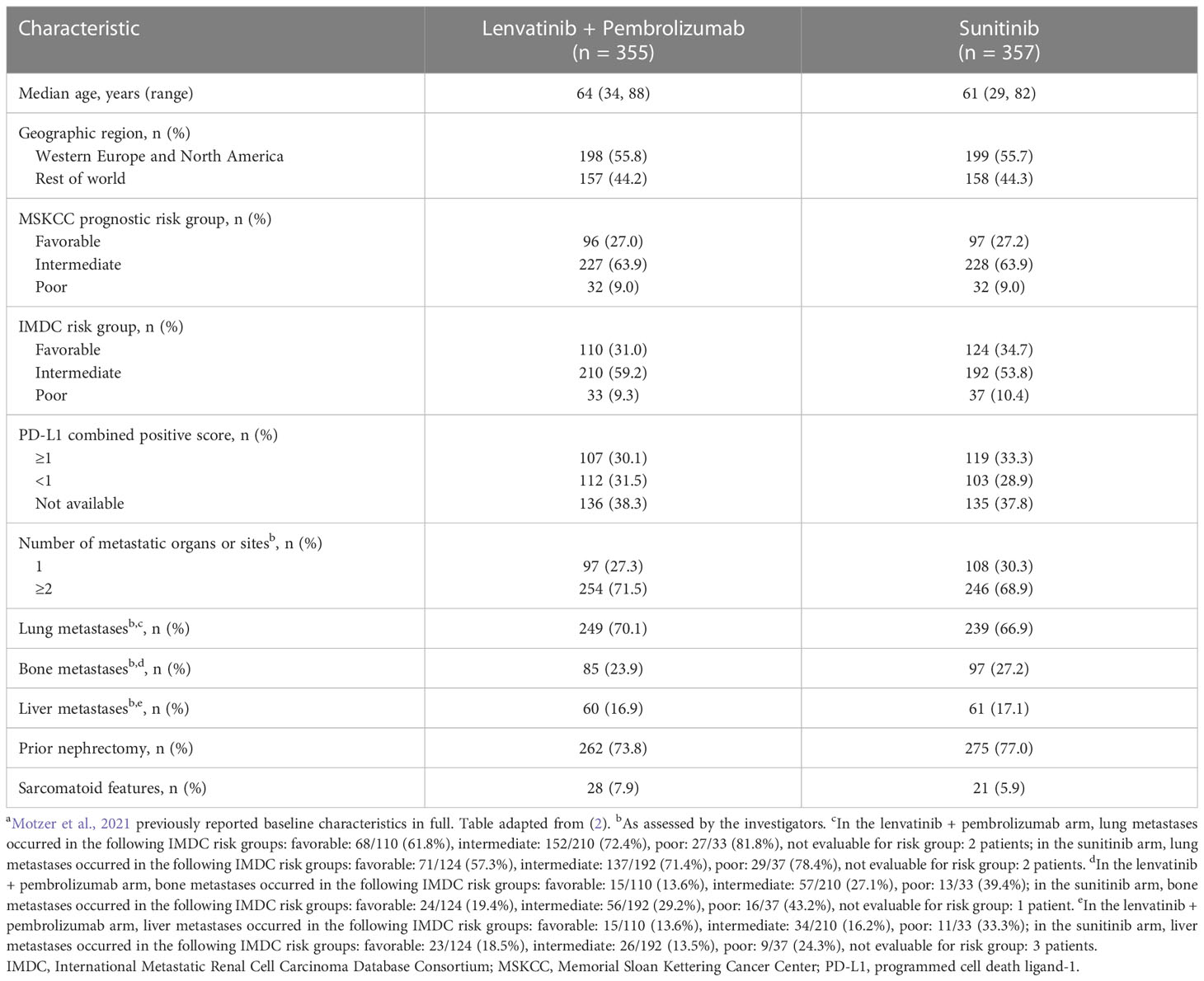
Table 1 Patient demographics and characteristics of the lenvatinib + pembrolizumab and sunitinib arms in CLEARa.
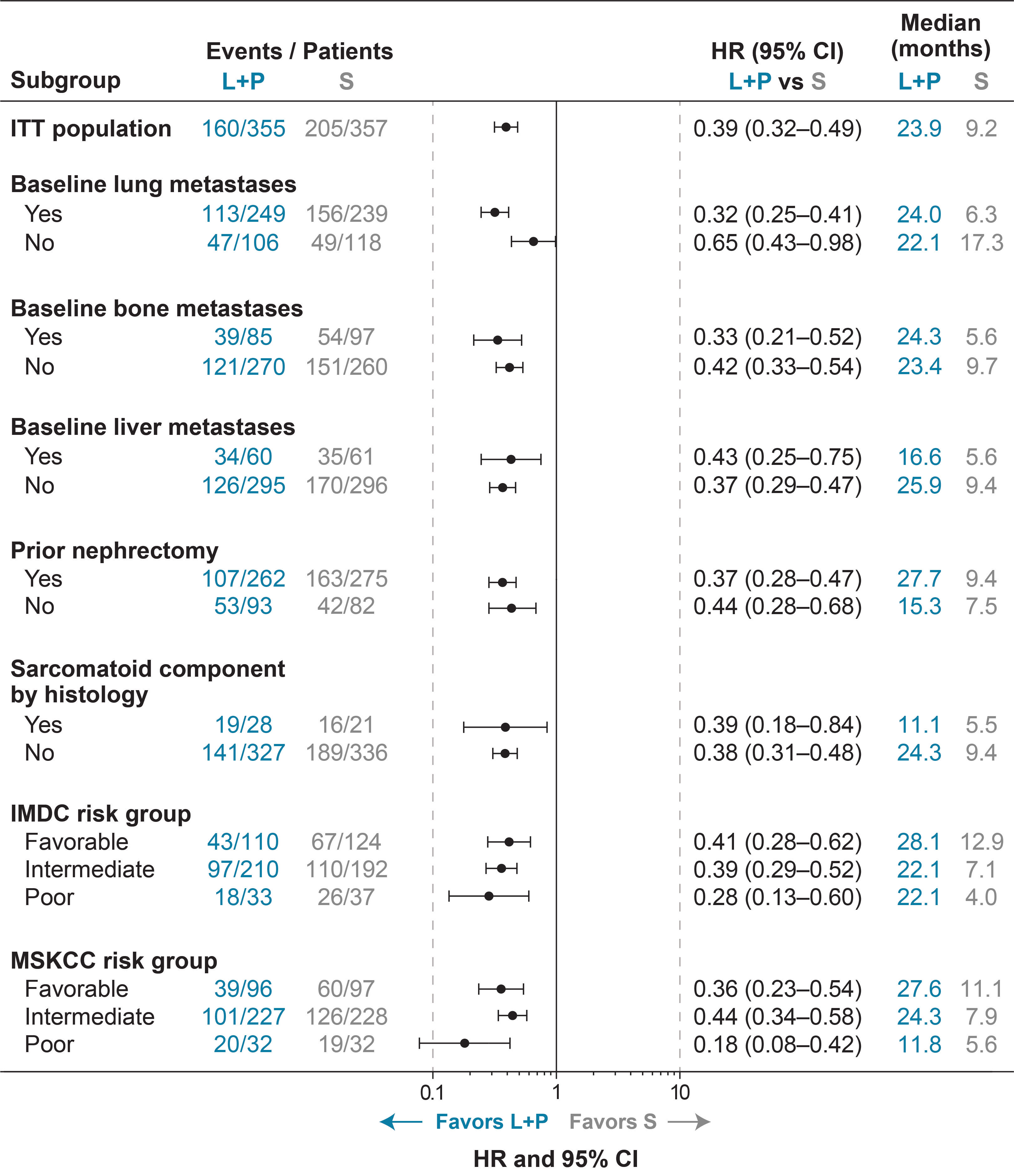
Figure 1 Forest Plot of PFS for Lenvatinib + Pembrolizumab Versus Sunitinib Treatment by IRC per RECIST v1.1. CI, confidence interval; HR, hazard ratio; IMDC, International Metastatic Renal Cell Carcinoma Database Consortium; IRC, independent review committee; ITT, intention to treat; L+P, lenvatinib + pembrolizumab; MSKCC, Memorial Sloan Kettering Cancer Center; PFS, progression-free survival; RECIST v1.1, Response Evaluation Criteria In Solid Tumors version 1.1; S, sunitinib.
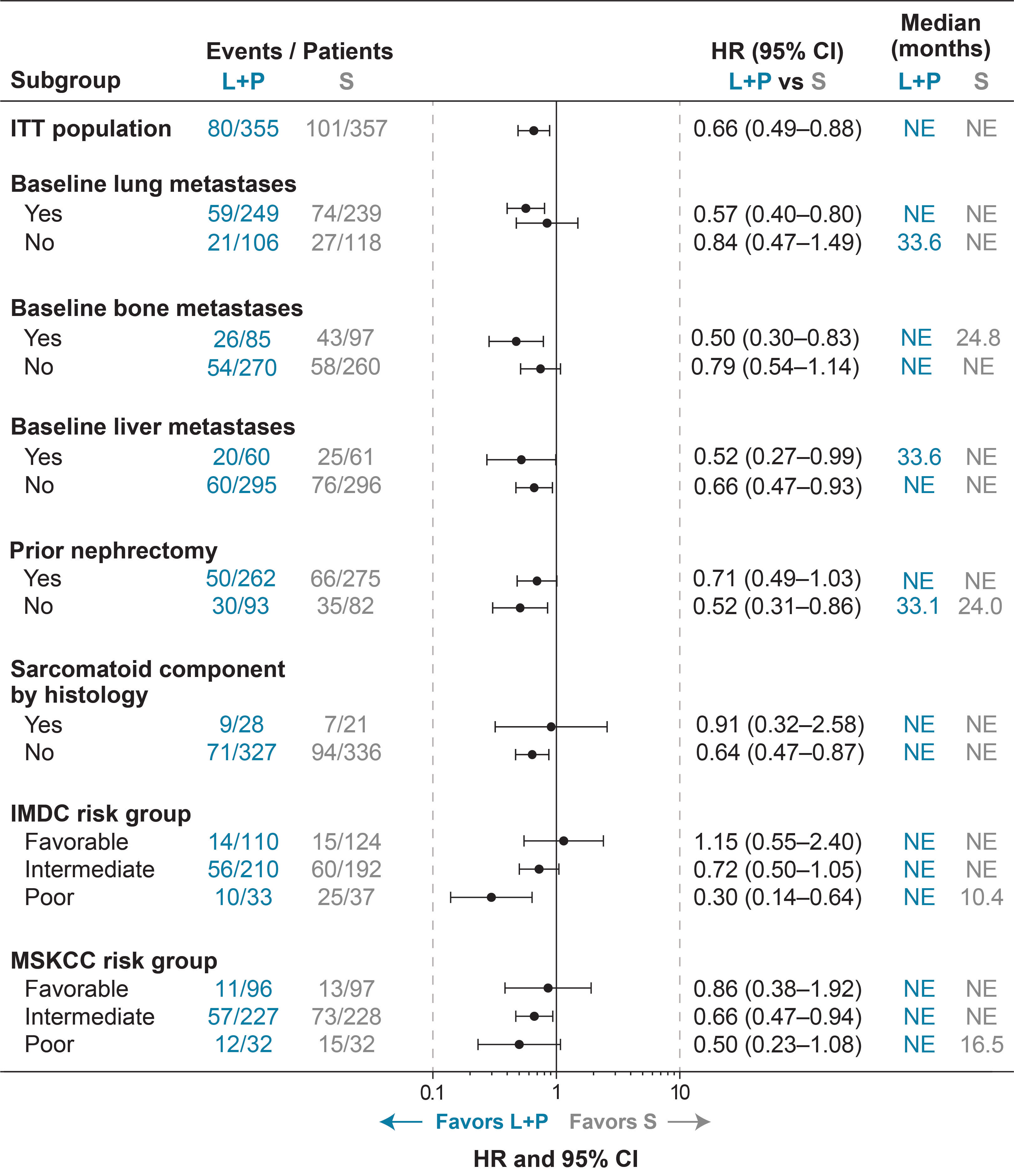
Figure 2 Forest Plot of OS for Lenvatinib + Pembrolizumab Versus Sunitinib Treatment. CI, confidence interval; HR, hazard ratio; IMDC, International Metastatic Renal Cell Carcinoma Database Consortium; ITT, intention to treat; L+P, lenvatinib + pembrolizumab; MSKCC, Memorial Sloan Kettering Cancer Center; NE, not estimable; OS, overall survival; S, sunitinib.
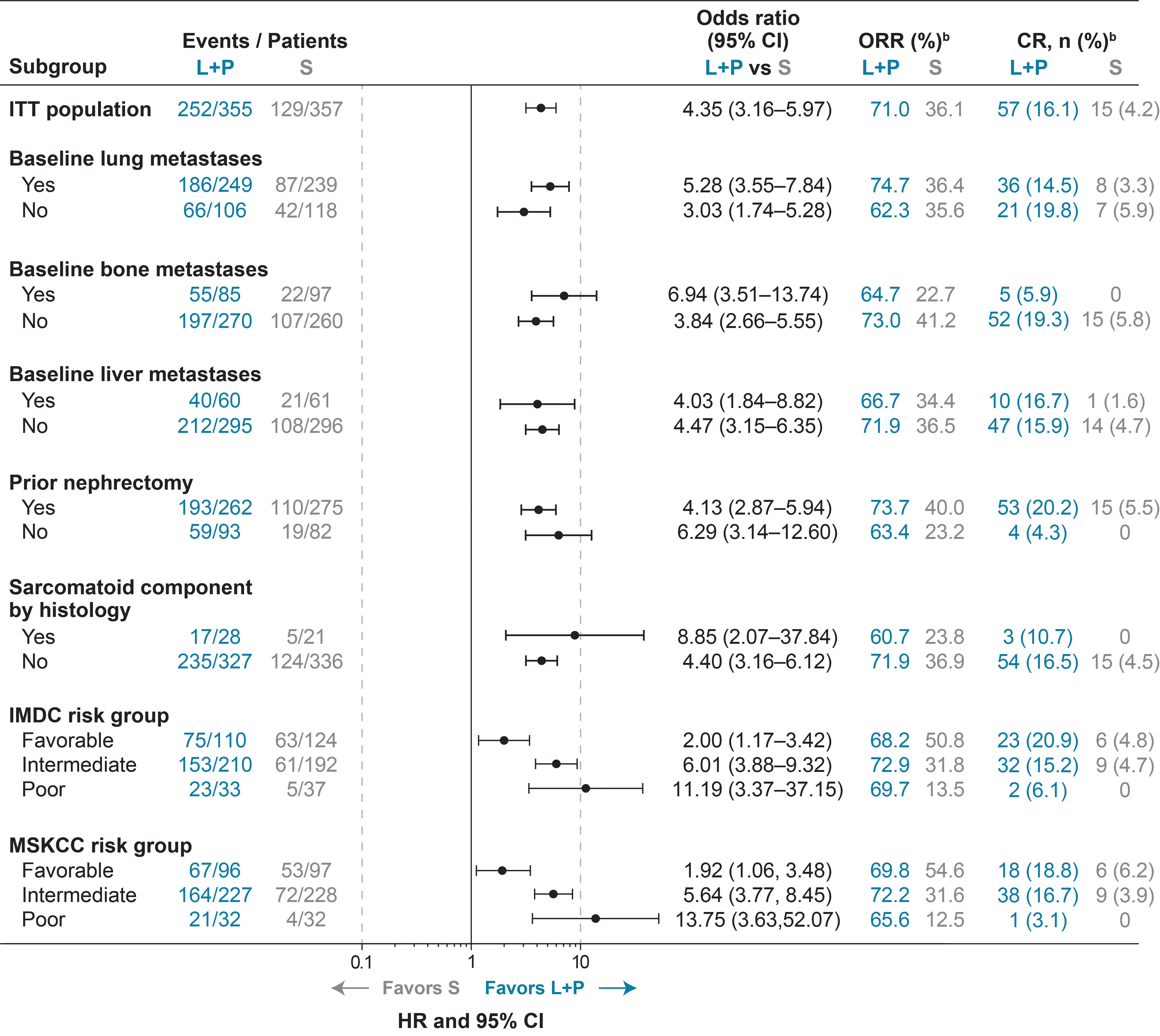
Figure 3 ORRa and Odds Ratios for Lenvatinib + Pembrolizumab Versus Sunitinib Treatment in Subgroups of Interest. aAs assessed by IRC per RECIST v1.1. bPercents were calculated based on listed subgroups. CI, confidence interval; CR, complete response; IMDC, International Metastatic Renal Cell Carcinoma Database Consortium; IRC, independent review committee; ITT, intention to treat; L+P, lenvatinib + pembrolizumab; MSKCC, Memorial Sloan Kettering Cancer Center; ORR, objective response rate; RECIST v1.1, Response Evaluation Criteria In Solid Tumors version 1.1; S, sunitinib.
3.2 Efficacy
3.2.1 Progression-free survival
The data cutoff date for the primary analysis of CLEAR was August 28, 2020 (2). Median PFS, as assessed by IRC per RECIST v1.1, was longer with lenvatinib-plus-pembrolizumab versus sunitinib treatment across baseline-characteristic subgroups of interest (Figure 1). Among patients with baseline lung metastases, those in the lenvatinib-plus-pembrolizumab arm had a median PFS of 24.0 months and those in the sunitinib arm had a median PFS of 6.3 months (HR 0.32; 95% CI 0.25–0.41). Patients with no baseline lung metastases had median PFS of 22.1 months in the lenvatinib-plus-pembrolizumab arm and 17.3 months in the sunitinib arm (HR 0.65; 95% CI 0.43–0.98). Patients with bone metastases had a median PFS of 24.3 months versus 5.6 months in the lenvatinib-plus-pembrolizumab versus sunitinib arms, respectively (HR 0.33; 95% CI 0.21–0.52); those without bone metastases had a median PFS of 23.4 months in the lenvatinib-plus-pembrolizumab arm and 9.7 months in the sunitinib arm (HR 0.42; 95% CI 0.33–0.54). Patients with liver metastases had a median PFS of 16.6 months in the lenvatinib-plus-pembrolizumab arm and 5.6 months in the sunitinib arm (HR 0.43; 95% CI 0.25–0.75); those without liver metastases had a median PFS of 25.9 months in the lenvatinib-plus-pembrolizumab arm and 9.4 months in the sunitinib arm (HR 0.37; 95% CI 0.29–0.47).
In patients with prior nephrectomy, PFS outcomes also favored lenvatinib plus pembrolizumab (median 27.7 months) versus sunitinib (median 9.4 months) (HR 0.37; 95% CI 0.28–0.47); similarly, in those without prior nephrectomy, median PFS was 15.3 versus 7.5 months, respectively (HR 0.44; 95% CI 0.28–0.68; Figure 1). In patients with sarcomatoid features, median PFS was 11.1 months in the lenvatinib-plus-pembrolizumab arm versus 5.5 months in the sunitinib arm (HR 0.39; 95% CI 0.18–0.84), and in those without sarcomatoid features median PFS was 24.3 months in patients in the lenvatinib-plus-pembrolizumab arm versus 9.4 months in the sunitinib arm (HR 0.38; 95% CI 0.31–0.48).
3.2.2 Overall survival
While median OS was not reached in most groups, OS results also generally favored lenvatinib-plus-pembrolizumab versus sunitinib treatment across baseline-characteristic subgroups of interest (Figure 2). Lenvatinib-plus-pembrolizumab treatment was favored over sunitinib treatment in patients who had baseline lung metastases (HR 0.57; 95% CI 0.40–0.80), and was favored in patients who did not have baseline lung metastases (HR 0.84; 95% CI 0.47–1.49). In patients with bone metastases, lenvatinib plus pembrolizumab was favored over sunitinib (HR 0.50; 95% CI 0.30–0.83); in patients without bone metastases, median OS was not reached in either arm (HR 0.79; 95% CI 0.54–1.14). Lenvatinib plus pembrolizumab was favored over sunitinib whether patients had liver metastases (HR 0.52; 95% CI 0.27–0.99) or not (HR 0.66; 95% CI 0.47–0.93).
Median OS favored lenvatinib-plus-pembrolizumab over sunitinib treatment both in patients with prior nephrectomy (median not reached in either group; HR 0.71; 95% CI 0.49–1.03) and without prior nephrectomy (median 33.1 versus 24.0 months, respectively; HR 0.52; 95% CI 0.31–0.86; Figure 2). Median OS was not reached in either treatment arm in patients with (HR 0.91; 95% CI 0.32–2.58) or without sarcomatoid features (HR 0.64; 95% CI 0.47–0.87).
3.2.3 Objective response
ORR results favored lenvatinib-plus-pembrolizumab versus sunitinib treatment across subgroups of interest (ie, lung metastases, bone metastases, liver metastases, prior nephrectomy, and sarcomatoid features) (Figure 3, Supplementary Table 1). In patients with lung metastases, ORR was 74.7% in the lenvatinib-plus-pembrolizumab arm and 36.4% in the sunitinib arm (odds ratio 5.28; 95% CI 3.55–7.84). In patients without lung metastases, ORR was 62.3% in the lenvatinib-plus-pembrolizumab arm and 35.6% in the sunitinib arm (odds ratio 3.03; 95% CI 1.74–5.28). In patients with bone metastases, ORR was 64.7% in the lenvatinib-plus-pembrolizumab arm and 22.7% in the sunitinib arm (odds ratio 6.94; 95% CI 3.51–13.74). In patients without bone metastases, ORR was 73.0% in the lenvatinib-plus-pembrolizumab arm and 41.2% in the sunitinib arm (odds ratio 3.84; 95% CI 2.66–5.55). ORR was 66.7% in patients with liver metastases in the lenvatinib-plus-pembrolizumab arm and 34.4% in patients with liver metastases in the sunitinib arm (odds ratio 4.03; 95% CI 1.84–8.82). In patients without liver metastases, ORR was 71.9% and 36.5% in the lenvatinib-plus-pembrolizumab and sunitinib arms, respectively (odds ratio 4.47; 95% 3.15–6.35).
ORR was 73.7% and 40.0% in patients who had a prior nephrectomy in the lenvatinib-plus-pembrolizumab and sunitinib arms, respectively (odds ratio 4.13; 95% CI 2.87–5.94); and 63.4% and 23.2%, respectively, in patients who had not had a prior nephrectomy (odds ratio 6.29; 95% CI 3.14–12.60) (Figure 3, Supplementary Table 1). In patients with sarcomatoid features, ORR was 60.7% and 23.8% in the lenvatinib-plus-pembrolizumab arm and the sunitinib arm, respectively (odds ratio 8.85; 95% CI 2.07–37.84). In patients without sarcomatoid features, ORR was 71.9% in the lenvatinib-plus-pembrolizumab arm and 36.9% in the sunitinib arm (odds ratio 4.40; 95% CI 3.16–6.12). The rate of patients with complete responses (CR) was generally higher across subgroups of interest in the lenvatinib-plus-pembrolizumab arm versus the sunitinib arm (Figure 3). As expected, the rates of CRs were higher in patients without baseline bone metastases, and in patients who had a prior nephrectomy. CR rates were similar irrespective of whether or not patients had baseline liver metastases. Among patients with bone metastases, 5 patients in the lenvatinib-plus-pembrolizumab arm had a CR and, of those, 2 patients had received bone-targeting agents.
4 Discussion
In this exploratory subgroup analysis of prognostic factors in patients with advanced RCC, efficacy outcomes favored lenvatinib-plus-pembrolizumab versus sunitinib treatment, regardless of presence of baseline lung metastases, bone metastases, liver metastases, prior nephrectomy, or sarcomatoid histology. These findings across PFS, OS, and ORR outcomes are consistent with the efficacy outcomes observed in the intention-to-treat population, in which the efficacy of lenvatinib plus pembrolizumab was superior to that of sunitinib in patients with advanced RCC (2).
Other trials have assessed immune checkpoint inhibitor (ICI)-based combination therapies in patients with advanced RCC (19–22). In the CheckMate 9ER study, with a median follow-up time for OS of 18.1 months, nivolumab plus cabozantinib was superior to sunitinib for PFS (HR 0.51; 95% CI 0.41–0.64), OS (HR 0.60; 98.89% CI 0.40–0.89), and ORR (difference 28.6%) (19). Nivolumab plus cabozantinib was favored over sunitinib for PFS and OS whether or not patients had baseline bone metastases. Nivolumab plus cabozantinib was also favored over sunitinib for PFS irrespective of whether patients had a prior nephrectomy, and was favored over sunitinib for OS among patients who had a prior nephrectomy (19). The CheckMate 214 study, at a median follow-up time of 25.2 months, demonstrated that nivolumab plus ipilimumab was superior to sunitinib for OS (HR 0.63; 99.8% CI 0.44–0.89) and ORR (42% versus 27%, P < 0.001) (20). Nivolumab plus ipilimumab was favored over sunitinib for OS, for most subgroups, including patients who did not have bone metastases, patients irrespective of liver metastases, patients with lung metastases, and patients regardless of prior nephrectomy (20). Avelumab plus axitinib was superior to sunitinib for PFS (stratified HR 0.69; 95% CI, 0.56–0.84) and ORR (stratified odds ratio 3.10; 95% CI 2.30–4.15) in the JAVELIN Renal 101 study (21), with a median follow-up for OS of 12.0 months and 11.5 months, respectively. Avelumab plus axitinib was favored over sunitinib for PFS among patients who had a prior nephrectomy, and numerically favored among those patients without a prior nephrectomy, though the patient numbers were low (21). While care should be taken in comparing clinical trial data, and relevant biomarker data for prediction of ICI efficacy are limited (23), these results are all from phase 3 trials in patients with advanced RCC that utilize sunitinib as a comparator. Those factors provide some support for cross-trial comparison, and indicate that ICI-based combination treatments often have superior efficacy over sunitinib; this efficacy extends to patients with certain baseline prognostic features (19–21). The results from assessment of prognostic groups within the CLEAR study indicate that lenvatinib plus pembrolizumab showed superior efficacy over sunitinib in subgroups of interest.
This analysis of data from CLEAR was limited as patient numbers were small for some subgroups, particularly the subgroup with sarcomatoid features (ie, n = 28 patients in the lenvatinib-plus-pembrolizumab arm and 21 patients in the sunitinib arm). Small patient numbers and low numbers of events led to wide CIs, especially in the OS analysis. In addition, not all subgroups were stratification factors, though patient numbers were generally similar between treatment arms. These findings are based on the prespecified subgroup analyses in the statistical analysis plan. Another limitation is that they are exploratory in nature and not statistically powered for individual subgroups (24). Because of the limitation of multiple comparisons, the validity of these findings needs to be confirmed in prospective clinical trials.
Despite limitations inherent to subgroup analyses, these analyses can provide valuable information for treatment customization for patients with RCC. The American Society for Clinical Oncology guidelines suggest ICI-based treatments could be considered for patients with RCC with sarcomatoid features (11), as recent data may indicate that tumors with sarcomatoid features could be especially responsive to ICI-based therapies (25). This recommendation is supported by a molecular analysis of renal cancer tumors, which found that tumors with sarcomatoid features were characterized by low angiogenesis and higher immune presence, which could present mechanistic support for use of ICIs in this subgroup of patients (17). The CheckMate 9ER trial found that among patients with bone metastases, nivolumab plus cabozantinib was more efficacious than sunitinib (19). The data in this analysis demonstrate that lenvatinib plus pembrolizumab was also effective in patients with bone metastases. Among patients with bone metastases, median PFS (HR 0.33, 95% CI 0.21–0.52), median OS (HR 0.50, 95% CI 0.30–0.83), and ORR (odds ratio 6.94, 95% CI 3.51–13.74) were all superior with lenvatinib plus pembrolizumab compared with sunitinib; moreover, of the 85 patients with bone metastases in the lenvatinib-plus-pembrolizumab arm, 5 patients had a best overall response of CR by RECIST v1.1.
The primary results (2) of the phase 3 CLEAR study in patients with RCC supported the combination of lenvatinib plus pembrolizumab as a first-line treatment option for patients with advanced RCC. This further analysis of the prognostic factors of baseline lung, bone, or liver metastases, and of prior nephrectomy and sarcomatoid features, indicates that the superior efficacy of lenvatinib plus pembrolizumab is consistent across multiple important subgroups of patients with advanced RCC.
Data availability statement
The datasets presented in this article are not readily available because of commercial confidentiality. Requests to access the datasets should be directed to Eisai Oncology Medical Information (ZXNpX29uY21lZGluZm9AZWlzYWkuY29t).
Ethics statement
The trial involving human participants was conducted in accordance with the International Council for Harmonisation Good Clinical Practice Guidelines and the principles of the 2013 Declaration of Helsinki. Institutional review boards or independent ethics committees approved the protocol and appropriate related documents. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Study concept and design: VG, RP, CH, CO, JM, TKC. Data acquisition: all authors. Data analysis: JEB, RP, CH, JM, CO. Data interpretation: all authors. Review of the manuscript drafts, approval of the final version for submission: all authors.
Funding
This work was supported by Eisai Inc., Nutley, NJ, USA, and Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. Medical writing support was provided by Oxford PharmaGenesis Inc., Newtown, PA, USA, and was funded by Eisai Inc., Nutley, NJ, USA, and Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. Patients treated at Memorial Sloan Kettering Cancer Center were supported in part by Memorial Sloan Kettering Cancer Center Support Grant/Core Grant (P30 CA008748).
Conflict of interest
VG: Invited Speaker: AstraZeneca, Astellas, BMS, EISAI, Ipsen, Janssen-Cilag, Merck, MSD, Pfizer, ONO Pharmaceutical, Novartis/AAA; Advisory Board: Apogepha, BMS, EISAI, EUSA Pharm, Cureteq, Debiopharm, Gilead, Janssen-Cilag, Merck, MSD, Pfizer, Novartis, Oncorena, PCI Biotech; Stocks/Shares: AstraZeneca, BMS, MSD, SeaGen; Steering Committee Member: BMS, EISAI, Ipsen, Novartis, PharmaMar; Travel support: AstraZeneca, Ipsen, Merck, Janssen, Pfizer. Non-Financial Interests: Membership: ASCO, ESMO, German medical Oncology and Hematology Society; Advisory role: German Cancer Society; Leadership role: Working Group medical oncology (AIO). TP: reports research funding from Astellas Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, Exelixis, Ipsen, Johnson & Johnson, Merck, Merck Serono, MSD, Novartis, Pfizer, Roche, and Seattle Genetics; consulting fees from Astellas Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, Exelixis, Incyte, Ipsen, Johnson & Johnson, Merck, Merck Serono, MSD, Novartis, Pfizer, Roche, and Seattle Genetics; support for attending meetings or travel from Astra Zeneca, Ipsen, MSD, Pfizer, and Roche. ME: reports research funding from Kissei, Sanofi, Astellas, ONO, Takeda, and Bayer; and payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from MSD, ONO, Chugai, Novartis, Pfizer, Bristol Myers Squibb, Takeda, Janssen, and Merck. SYR: reports grants or contracts from Amgen, Merck, Bristol Myers Squibb, MSD, Lilly, Daiichi Sankyo, Beigene, Eisai, and AstraZeneca; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Amgen, Lilly, Bristol Myers Squibb, MSD, and Eisai; and participation on a data safety monitoring board or advisory board from Amgen, MSD, Bristol Myers Squibb, Merck, Indivumed, Beigene, Eisai, and Daiichi Sankyo. CP: reports consulting fees from Angelini Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, Ipsen, and MSD; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Angelini Pharma, AstraZeneca, Bristol Myers Squibb, Eisai, General Electric, Ipsen, and MSD; and participation on a data safety monitoring board or advisory board for Bristol Myers Squibb, Eisai, MSD, the European Society of Medical Oncology, and the Italian Association for Medical Oncology. RM: reports research funding, paid to their institution from Bristol Myers Squibb, Eisai, Exelixis, Genentech/Roche, Merck, Pfizer, and Aveo Pharmaceuticals and consulting fees from AstraZeneca, Aveo Pharmaceuticals, Eisai, EMD Serono, Exelixis, Genentech/Roche, Incyte, Lilly, Merck, Novartis, Pfizer, and Takeda. TEH: reports grants or contracts, paid to their institution, from Bristol Myers Squibb, Eisai, Exelixis, Johnson & Johnson, and Pfizer; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Astellas Pharma, Bristol Myers Squibb, Eisai, Exelixis, Johnson & Johnson, and Pfizer; and participation on a data safety monitoring board or advisory board for Astellas Pharma, Bayer/Onyx, Bristol Myers Squibb, Exelixis, Johnson & Johnson, Novartis, and Pfizer. MJM-V: reports consulting fees from Astellas Pharma, Bristol Myers Squibb, EUSA Pharma, Ipsen, Eisai, Janssen-Cilag, Novartis, Pfizer, Roche, and Sanofi; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Astellas Pharma, Bristol Myers Squibb, Ipsen, EUSA Pharma, Janssen-Cilag, Pfizer, and Roche; and support for attending meetings or travel from Astellas Pharma, Bristol Myers Squibb, Ipsen, Janssen-Cilag, Pfizer, and Roche. EW: reports research support, paid to their institution from Ayala Pharmaceuticals, Eisai, Merck, Pfizer, and Roche/Genentech; honoraria from Amgen, Bayer, Eisai, Merck, and Roche. JCG: reports consulting fees for an advisory board meeting from MSD Australia, Bristol Myers Squibb, and GlaxoSmithKline; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Janssen–Cilag, Ipsen, MSD Australia, and AstraZeneca Australia; and support for attending meetings or travel from AstraZeneca Australia, GlaxoSmithKline, and Pfizer. PM: reports research support, paid to their institution from Roche. TB: reports institutional research support from AstraZeneca, Roche, Bristol Myers Squibb, Exelixis, Merck, and Novartis; consulting fees from Bristol Myers Squibb, Astellas, Janssen, and Sanofi/Aventis; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Ipsen, Bristol Myers Squibb, Servier, and Pfizer; and institutional receipt of equipment, materials, drugs, medical writing, gifts, or other services from Bristol Myers Squibb, AstraZeneca, Roche, and Servier. TT: reports honoraria from Bristol Myers Squibb, Eisai, and Ono Pharmaceutical. JEB: employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. RP: employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. CH: employee of Eisai Inc. CO: employee of Eisai Ltd. JM: employee of Eisai Inc. TKC: reports institutional and/or personal, paid and/or unpaid support for research, advisory boards, consultancy, and honoraria from: Alkermes, AstraZeneca, Aravive, Aveo, Bayer, Bristol Myers Squibb, Calithera, Circle Pharma, Eisai, EMD Serono, Exelixis, GlaxoSmithKline, Gilead, IQVA, Infinity, Ipsen, Jansen, Kanaph, Lilly, Merck, Nikang, Nuscan, Novartis, Pfizer, Roche, Sanofi/Aventis, Scholar Rock, Surface Oncology, Takeda, Tempest, Up-To-Date, CME events Peerview, OncLive, MJH and others, outside the submitted work. Institutional patents filed on molecular alterations and immunotherapy response/toxicity, and ctDNA. Equity: Tempest, Pionyr, Osel, Precede Bio, CureResponse. Committees: NCCN, GU Steering Committee, ASCO/ESMO, ACCRU, KidneyCan. Medical writing and editorial assistance support may have been funded by Communications companies in part. No speaker’s bureau. Mentored several non-US citizens on research projects with potential funding in part from non-US sources/Foreign Components. The institution Dana-Farber Cancer Institute may have received additional independent funding of drug companies or/and royalties potentially involved in research around the subject matter. TKC is supported in part by the Dana-Farber/Harvard Cancer Center Kidney SPORE 2P50CA101942-16 and Program 5P30CA006516-56, the Kohlberg Chair at Harvard Medical School and the Trust Family, Michael Brigham, Pan Mass Challenge, Hinda and Arthur Marcus Fund and Loker Pinard Funds for Kidney Cancer Research at DFCI.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1223282/full#supplementary-material
References
1. Choueiri TK, Motzer RJ. Systemic therapy for metastatic renal-cell carcinoma. N Engl J Med (2017) 376:354–66. doi: 10.1056/NEJMra1601333
2. Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med (2021) 384:1289–300. doi: 10.1056/NEJMoa2035716
3. Dudani S, de Velasco G, Wells JC, Gan CL, Donskov F, Porta C, et al. Evaluation of clear cell, papillary, and chromophobe renal cell carcinoma metastasis sites and association with survival. JAMA Netw Open (2021) 4:e2021869. doi: 10.1001/jamanetworkopen.2020.21869
4. Wei H, Miao J, Cui J, Zheng W, Chen X, Zhang Q, et al. The prognosis and clinicopathological features of different distant metastases patterns in renal cell carcinoma: analysis based on the SEER database. Sci Rep (2021) 11:17822. doi: 10.1038/s41598-021-97365-6
5. Hahn AW, Lebenthal J, Genovese G, Sircar K, Tannir NM, Msaouel P. The significance of sarcomatoid and rhabdoid dedifferentiation in renal cell carcinoma. Cancer Treat Res Commun (2022) 33:100640. doi: 10.1016/j.ctarc.2022.100640
6. Bianchi M, Sun M, Jeldres C, Shariat SF, Trinh QD, Briganti A, et al. Distribution of metastatic sites in renal cell carcinoma: a population-based analysis. Ann Oncol (2012) 23:973–80. doi: 10.1093/annonc/mdr362
7. National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Kidney Cancer. Available at: https://www.nccn.org/professionals/physician_gls/PDF/kidney.pdf (Accessed April 31, 2023).
8. Yue G, Deyu L, Lianyuan T, Fengmin S, Mei G, Yajun H, et al. Clinical features and prognostic factors of patients with metastatic renal cell carcinoma stratified by age. Aging (Albany NY) (2021) 13:8290–305. doi: 10.18632/aging.202637
9. Chen SC, Kuo PL. Bone metastasis from renal cell carcinoma. Int J Mol Sci (2016) 17:987. doi: 10.3390/ijms17060987
10. Coleman R, Hadji P, Body JJ, Santini D, Chow E, Terpos E, et al. Bone health in cancer: ESMO Clinical Practice Guidelines. Ann Oncol (2020) 31:1650–63. doi: 10.1016/j.annonc.2020.07.019
11. Rathmell WK, Rumble RB, Van Veldhuizen PJ, Al-Ahmadie H, Emamekhoo H, Hauke RJ, et al. Management of metastatic clear cell renal cell carcinoma: ASCO guideline. J Clin Oncol (2022) 40:2957–95. doi: 10.1200/JCO.22.00868
12. Hamada S, Ito K, Kuroda K, Sato A, Asakuma J, Horiguchi A, et al. Clinical characteristics and prognosis of patients with renal cell carcinoma and liver metastasis. Mol Clin Oncol (2015) 3:63–8. doi: 10.3892/mco.2014.432
13. Leibovich BC, Blute ML, Cheville JC, Lohse CM, Frank I, Kwon ED, et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. Cancer (2003) 97:1663–71. doi: 10.1002/cncr.11234
14. Bottiglieri A, Sepe P, Stellato M, Pircher C, Fotia G, Leone AG, et al. Optimal choice of adjuvant treatment for renal cell carcinoma following nephrectomy. Cancer Manag Res (2022) 14:3071–81. doi: 10.2147/CMAR.S360441
15. Culp SH, Tannir NM, Abel EJ, Margulis V, Tamboli P, Matin SF, et al. Can we better select patients with metastatic renal cell carcinoma for cytoreductive nephrectomy? Cancer (2010) 116:3378–88. doi: 10.1002/cncr.25046
16. Gong J, Maia MC, Dizman N, Govindarajan A, Pal SK. Metastasis in renal cell carcinoma: biology and implications for therapy. Asian J Urol (2016) 3:286–92. doi: 10.1016/j.ajur.2016.08.006
17. Motzer RJ, Banchereau R, Hamidi H, Powles T, McDermott D, Atkins MB, et al. Molecular subsets in renal cancer determine outcome to checkpoint and angiogenesis blockade. Cancer Cell (2020) 38:803–17.e4. doi: 10.1016/j.ccell.2020.10.011
18. Choueiri TK, Atkins MB, Bakouny Z, Carlo MI, Drake CG, Jonasch E, et al. Summary from the first kidney cancer research summit, September 12-13, 2019: A focus on translational research. J Natl Cancer Inst (2021) 113:234–43. doi: 10.1093/jnci/djaa064
19. Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med (2021) 384:829–41. doi: 10.1056/NEJMoa2026982
20. Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med (2018) 378:1277–90. doi: 10.1056/NEJMoa1712126
21. Motzer RJ, Penkov K, Haanen J, Rini B, Albiges L, Campbell MT, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med (2019) 380:1103–15. doi: 10.1056/NEJMoa1816047
22. Braun DA, Bakouny Z, Hirsch L, Flippot R, Van Allen EM, Wu CJ, et al. Beyond conventional immune-checkpoint inhibition - novel immunotherapies for renal cell carcinoma. Nat Rev Clin Oncol (2021) 18:199–214. doi: 10.1038/s41571-020-00455-z
23. Van Allen EM, Choueiri TK. Dissecting the immunogenomic biology of cancer for biomarker development. Nat Rev Clin Oncol (2021) 18:133–4. doi: 10.1038/s41571-020-00461-1
24. Burke JF, Sussman JB, Kent DM, Hayward RA. Three simple rules to ensure reasonably credible subgroup analyses. BMJ (2015) 351:h5651. doi: 10.1136/bmj.h5651
Keywords: renal cell carcinoma, lenvatinib, pembrolizumab, sunitinib, bone metastases, liver metastases, lung metastases, sarcomatoid histology
Citation: Grünwald V, Powles T, Eto M, Kopyltsov E, Rha SY, Porta C, Motzer R, Hutson TE, Méndez-Vidal MJ, Hong S-H, Winquist E, Goh JC, Maroto P, Buchler T, Takagi T, Burgents JE, Perini R, He C, Okpara CE, McKenzie J and Choueiri TK (2023) Phase 3 CLEAR study in patients with advanced renal cell carcinoma: outcomes in subgroups for the lenvatinib-plus-pembrolizumab and sunitinib arms. Front. Oncol. 13:1223282. doi: 10.3389/fonc.2023.1223282
Received: 15 May 2023; Accepted: 11 July 2023;
Published: 16 August 2023.
Edited by:
Umang Swami, The University of Utah, United StatesReviewed by:
Fabio Calabro', San Camillo Forlanini Hospital, Italy; Hamid Emamekhoo, University of Wisconsin-Madison, United StatesCopyright © 2023 Grünwald, Powles, Eto, Kopyltsov, Rha, Porta, Motzer, Hutson, Méndez-Vidal, Hong, Winquist, Goh, Maroto, Buchler, Takagi, Burgents, Perini, He, Okpara, McKenzie and Choueiri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viktor Grünwald, VmlrdG9yLkdydWVud2FsZEB1ay1lc3Nlbi5kZQ==