 Jordi Rubió-Casadevall1*†
Jordi Rubió-Casadevall1*† Beatriz Cirauqui Cirauqui2†
Beatriz Cirauqui Cirauqui2† Javier Martinez Trufero3
Javier Martinez Trufero3 Maria Plana Serrahima4Almudena García Castaño5
Maria Plana Serrahima4Almudena García Castaño5 Alberto Carral Maseda6Lara Iglesias Docampo7Pedro Pérez Segura8Isaac Ceballos Lenza9Vanesa Gutiérrez Calderón10José Fuster Salvà11
Alberto Carral Maseda6Lara Iglesias Docampo7Pedro Pérez Segura8Isaac Ceballos Lenza9Vanesa Gutiérrez Calderón10José Fuster Salvà11 Carolina Pena Álvarez12Irene Hernandez13
Carolina Pena Álvarez12Irene Hernandez13 Edel del Barco Morillo14Manuel Chaves Conde15Joaquina Martínez Galán16Marisa Durán Sánchez17Vanesa Quiroga2Eugenia Ortega3
Edel del Barco Morillo14Manuel Chaves Conde15Joaquina Martínez Galán16Marisa Durán Sánchez17Vanesa Quiroga2Eugenia Ortega3 Ricard Mesia2,17 on behalf of the Spanish Group of Head Neck Cancer Treatment (TTCC), Madrid, Spain
Ricard Mesia2,17 on behalf of the Spanish Group of Head Neck Cancer Treatment (TTCC), Madrid, Spain- 1Medical Oncology Department, Institut Català d’Oncologia Girona, Girona Biomedical Research Institute (IDIBGI), Girona, Spain
- 2Medical Oncology Department, Institut Català d’Oncologia Badalona, B-ARGO Group, IGTP, Badalona, Spain
- 3Medical Oncology Department, Hospital Universitario Miguel Servet, Zaragoza, Spain
- 4Medical Oncology Department, Institut Català d’Oncologia (ICO-Hospitalet), IDIBELL, Hospitalet de Llobregat, Llobregat, Spain
- 5Medical Oncology Department, Hospital Universitario Marqués de Valdecilla, Santander, Spain
- 6Medical Oncology Department, Hospital Universitario Lucus Augusti, Lugo, Spain
- 7Medical Oncology Department, Hospital Universitario 12 de Octubre, Madrid, Spain
- 8Medical Oncology Department, Hospital Clínico San Carlos, IdISSC, Madrid, Spain
- 9Medical Oncology Department, Hospital Universitario de Canarias, San Cristóbal de La Laguna, Spain
- 10UGCI Oncol. Hospital Universitario Regional y Virgen Victoria, IBIMA, Málaga, Spain
- 11Medical Oncology Department, Hospital Universitario Son Espases, Palma de Mallorca, Spain
- 12Medical Oncology Department, Centro Oncológico Galicia, A Coruña, Spain
- 13Medical Oncology Department, Hospital Universitario de Navarra, Instituto de Investigación Sanitaria de Navarra (IdiSNA), Pamplona, Spain
- 14Medical Oncology Department, Hospital Universitario de Salamanca, IBSAL, Salamanca, Spain
- 15Medical Oncology Department, Hospital Universitario Virgen de Valme, Sevilla, Spain
- 16Medical Oncology Department, Hospital Universitario Virgen Nieves, Instituto de Investigación Biosanitaria ibs, Granada, Spain
- 17Spanish Group of Head and Neck Cancer Treatment (TTCC), Madrid, Spain
Objectives: The aim of this study was to confirm the efficacy of the ERBITAX scheme (paclitaxel 80 mg/m2 weekly and cetuximab 400 mg/m2 loading dose, and then 250 mg/m2 weekly) as first-line treatment for patients with recurrent/metastatic squamous cell carcinoma of the head and neck (SCCHN) who are medically unfit for cisplatin-based (PT) chemotherapy.
Materials and methods: This retrospective, non-interventional study involved 16 centers in Spain. Inclusion criteria were to have started receiving ERBITAX regimen from January 2012 to December 2018; histologically confirmed SCCHN including oral cavity, oropharynx, hypopharynx, and larynx; age ≥18 years; and platinum (PT) chemotherapy ineligibility due to performance status, comorbidities, high accumulated dose of PT, or PT refractoriness.
Results: A total of 531 patients from 16 hospitals in Spain were enrolled. The median age was 66 years, 82.7% were male, and 83.5% were current/former smokers. Patients were ineligible to receive PT due to ECOG 2 (50.3%), comorbidities (32%), PT cumulative dose ≥ 225 mg/m2 (10.5%), or PT refractoriness (7.2%). Response rate was 37.7%. Median duration of response was 5.6 months (95% CI: 4.4–6.6). With a median follow-up of 8.7 months (95% CI: 7.7–10.2), median PFS and OS were 4.5 months (95% CI: 3.9–5.0) and 8.9 months (95% CI: 7.8–10.3), respectively. Patients treated with immunotherapy after ERBITAX had better OS with a median of 29.8 months compared to 13.8 months for those who received other treatments. The most common grade ≥ 3 toxicities were acne-like rash in 36 patients (6.8%) and oral mucositis in 8 patients (1.5%). Five (0.9%) patients experienced grade ≥ 3 febrile neutropenia.
Conclusion: This study confirms the real-world efficacy and tolerability of ERBITAX as first-line treatment in recurrent/metastatic SCCHN when PT is not feasible. Immunotherapy after treatment with ERBITAX showed remarkable promising survival, despite potential selection bias.
1 Introduction
Squamous cell carcinoma of the head and neck (SCCHN) is one of the most frequently diagnosed cancers worldwide. More than half of patients diagnosed with locally advanced disease will recur within 5 years (1, 2). Most patients receive platinum-based chemotherapy as first-line treatment for recurrent/metastatic disease, which has a modest impact on survival (3, 4). Recently, the use of immune-checkpoint inhibitors (ICIs) such as nivolumab (5) and pembrolizumab (6) has shown to be effective in the treatment of advanced patients refractory to platinum-based chemotherapy. Likewise, the use of these drugs in the first line can also provide a substantial benefit according to programmed death ligand 1 (PD-L1) combined positive score (CPS) (7).
Recurrent or metastatic SCCHN is challenging because most of the patients have poor performance status, which is accompanied by nutritional disorders, abuse of alcohol or tobacco, or comorbidities (8, 9). Additionally, some patients may have a high accumulated dose of platinum from previous treatments for localized disease or may be considered refractory to platinum. Therefore, many patients are not eligible for platinum-based chemotherapy because they are frail enough to withstand the treatment approach or are expected to not respond to platinum. Although most patients unfit for platinum may have CPS >1, and now can start with a pembrolizumab-based first-line therapy (7), many patients can be CPS < 1 and will not be eligible for this therapeutic approach.
A regimen with the combination of cetuximab (CX) and weekly paclitaxel (PX), named ERBITAX, has shown activity and is well tolerated in patients with SCCHN with poor prognosis, including those for whom platinum is contraindicated (10). Therefore, this is a common option for treating medically unfit or platinum-resistant patients with SCCHN.
The study aimed to describe the real-world characteristics, treatment compliance, safety, and survival outcomes of patients with SCCHN who were unfit to receive platinum and received ERBITAX as first-line treatment for recurrent or metastatic disease in Spain.
2 Patients and methods
2.1 Study design
The TTCC-2019-02 was an observational, retrospective study conducted in 16 hospitals in Spain (Supplementary Data).
This study used secondary data retrieved from medical records. The medical records included all clinical variables required to perform the analysis, and accessing additional sources was not necessary. The assignment of a patient to a specific therapeutic strategy had already been decided in advance by the routine clinical practice of medicine, and the decision to prescribe the ERBITAX scheme was clearly dissociated from the decision to include a patient in the study. No additional interventions different from the standard clinical practice were applied to the patients, either for diagnosis or due to follow-up reasons. Epidemiological methods were used to analyze the data.
The study was conducted according to local regulations, ICH - Good Clinical Practice (R2), and the International Conference on Harmonisation and Declaration of Helsinki. The protocol was approved by the ethics committee of the Hospital Universitari de Bellvitge on 23 October 2020 (IEC code: EPA019/20). The protocol, amendments, and informed consent forms were approved by the institutional review board or ethics committee of each study site before study initiation. All patients were asked to provide written informed consent to participate, although an informed consent exemption was considered in cases when the effort to obtain informed consent was beyond reasonable and feasible (i.e., dead patients).
2.2 Study population
Patients aged ≥18 years with histologically confirmed recurrent or metastatic SCCHN, including the oral cavity, oropharynx, hypopharynx, and larynx; considered unfit for standard platinum-based chemotherapy; and who received at least one dose of weekly paclitaxel (starting dose of 80 mg/m2) and cetuximab (loading dose of 400 mg/m2, followed by 250 mg/m2) as first-line treatment in the recurrent or metastatic setting were eligible. Paclitaxel was administered weekly (i.e., days 1, 8, 15, 21…). Cetuximab could have been switched to biweekly during the maintenance phase. The included patients had to have started the ERBITAX regimen between January 2012 and December 2018. Unfit criteria for platinum included the following: poor Eastern Cooperative Oncology Group performance status (ECOG PS), comorbidities, and high accumulated dose of platinum or platinum refractoriness, defined as early disease progression (less than 6 months) to previous platinum-based chemotherapy in locally advanced setting (11, 12). Patients with unknown primary tumor, nasopharyngeal cancer, and non-squamous head and neck tumor, or ECOG >2 were excluded from the study.
Once the patients who had received at least one complete cycle of ERBITAX were identified, all cases from each center were included to avoid selection bias.
2.3 Objectives
The primary objective was to estimate the progression-free survival (PFS) in patients treated with ERBITAX as the first-line treatment for recurrent and/or metastatic SCCHN.
The secondary objectives were to determine the efficacy of ERBITAX measured by the best overall response (BOR), objective response rate (ORR), disease control rate (DCR), duration of response (DoR), and overall survival (OS); to establish potential prognostic factors associated with survival; and to characterize the safety profile by means of treatment compliance and toxicities.
2.4 Endpoints
Descriptive baseline characteristics to define the study population included demographic (i.e., age, sex, and ECOG PS), habits (i.e., smoking and enolic habit), HPV status (through p16 IHQ and DNA-HPV analysis), and pathological (i.e., stage and location) endpoints.
The primary endpoint, PFS, was defined as the time from the start of the study treatment to the date of progression or death, whichever occurred first. Patients without a PFS event were censored on the date of the last radiological evaluation or on the date of the last study treatment if the tumor response was not evaluated later. If no PFS event was observed prior to the start of second-line treatment, the patient was censored at the date of second-line treatment.
Secondary endpoints for efficacy included the following: BOR, classified as complete response (CR), partial response (PR), standard disease (SD), or progressive disease (PD) according to RECIST 1.1; ORR, defined as the proportion of patients with CR or PR; DCR, defined as the proportion of patients with CR, PR or SD; DoR, defined as the time from the first occurrence of response until PD or death, whichever occurs first; and OS, defined as time from the start of the study treatment until the date of death due to any cause. For alive patients, the OS time was censored at the last date known to be alive. Long-term survivors for stratified analysis of OS were considered those who were alive and disease-free 2 years after the start of the study treatment. Stratified analysis of subgroups according to baseline characteristics was used to determine the potential prognostic factors for efficacy.
Treatment compliance was measured using relative dose intensity (RDI), defined as the amount of drug administered per unit of time expressed as the fraction of that established in the standard regimen, rate of dose interruptions, modifications, and discontinuations. RDI was calculated as follows: RDI = 100*(DTD/STD) where DTD (Delivered Total Dose) is the total amount of drug actually administered over chemotherapy course in mg/m2 and STD (Standard Total Dose) is the total standard amount of drug for administration over chemotherapy course in mg/m2.
Secondary endpoints for safety included the rate of adverse events (AEs) that fulfilled any of the following criteria: AEs that were grade ≥3, led to discontinuation or dosage reduction of paclitaxel and/or cetuximab, or met criteria for serious AE (SAE). AEs were classified and graded according to the National Cancer Institute Common Toxicity Criteria for Adverse Events (NCI CTCAE) version 5.0.
The frequency of assessments followed the standard clinical practice. Preventive measures to identify patient duplicates were implemented, including cross-checking of variables such as birth date, sex, center, or diagnosis. We consider death as a cause of treatment interruption when the progression has not been objectified or clearly reflected in the clinical reports, although it is possible it would have occurred, and it is understood that the treatment does not have to be the cause of death.
2.5 Statistical analysis
Descriptive statistics and frequency tables were provided for all baseline, efficacy, and safety variables as appropriate. Continuous variables were summarized using mean, standard deviation, range, and median values. Frequency counts and percentages of participants within each category were provided for categorical data. The response percentages were estimated by binomial proportion using 95% confidence intervals (CIs) or full-range intervals. The time-to-event endpoints were estimated using the Kaplan–Meier method and log-rank test was used to obtain the median, CIs. Cox regression analysis was used to statistically compare between patient subgroups. Patients without documented progression or death at the time of analysis were censored on the last date of tumor evaluation. Logistic regression and Cox regression models were used to analyze the association between baseline characteristics, the treatment and disease outcomes. Multivariate models were used to estimate the hazard ratios (HR) for OS. All statistical analyses were performed using R (version 3.6.3 [2020-02-29] “Holding the Windsock,” The R Foundation for Statistical Computing, Vienna, Austria). Figures and tables were generated using RStudio (Version 1.2.5033 2009-2019 RStudio, Inc., Boston, MA, USA). All statistical tests were two-tailed with an alpha of 0.05.
The sample size calculation was based on the estimated number of patients with recurrent and/or metastatic SCCHN who were treated with ERBITAX in the first-line setting in Spain. The study planned to enroll at least 500 patients, which was considered a representative sample for the population of patients with SCCHN treated with ERBITAX. Assuming a total of 500 evaluable patients for PFS, and a censoring rate of 20%, the width (precision) of the 95% CI is 0.032 when the estimated hazard rate was 0.165 (95% CI: 0.1492–0.1816). The corresponding 95% CI for an estimated median PFS of 4.2 months is 3.8–4.6 months, which provides a considerably more precise estimate of the median PFS than previous reports (10).
3 Results
3.1 Patient disposition
A total of 531 patients were enrolled in this study between December 2020 and September 2021 (Figure 1). The number exceeded the minimum planned sample size by approximately 5% to allow inclusion of all patients treated in each center, thus avoiding biasing. All patients who met the eligibility criteria and received at least one dose of ERBITAX were evaluable for the study.
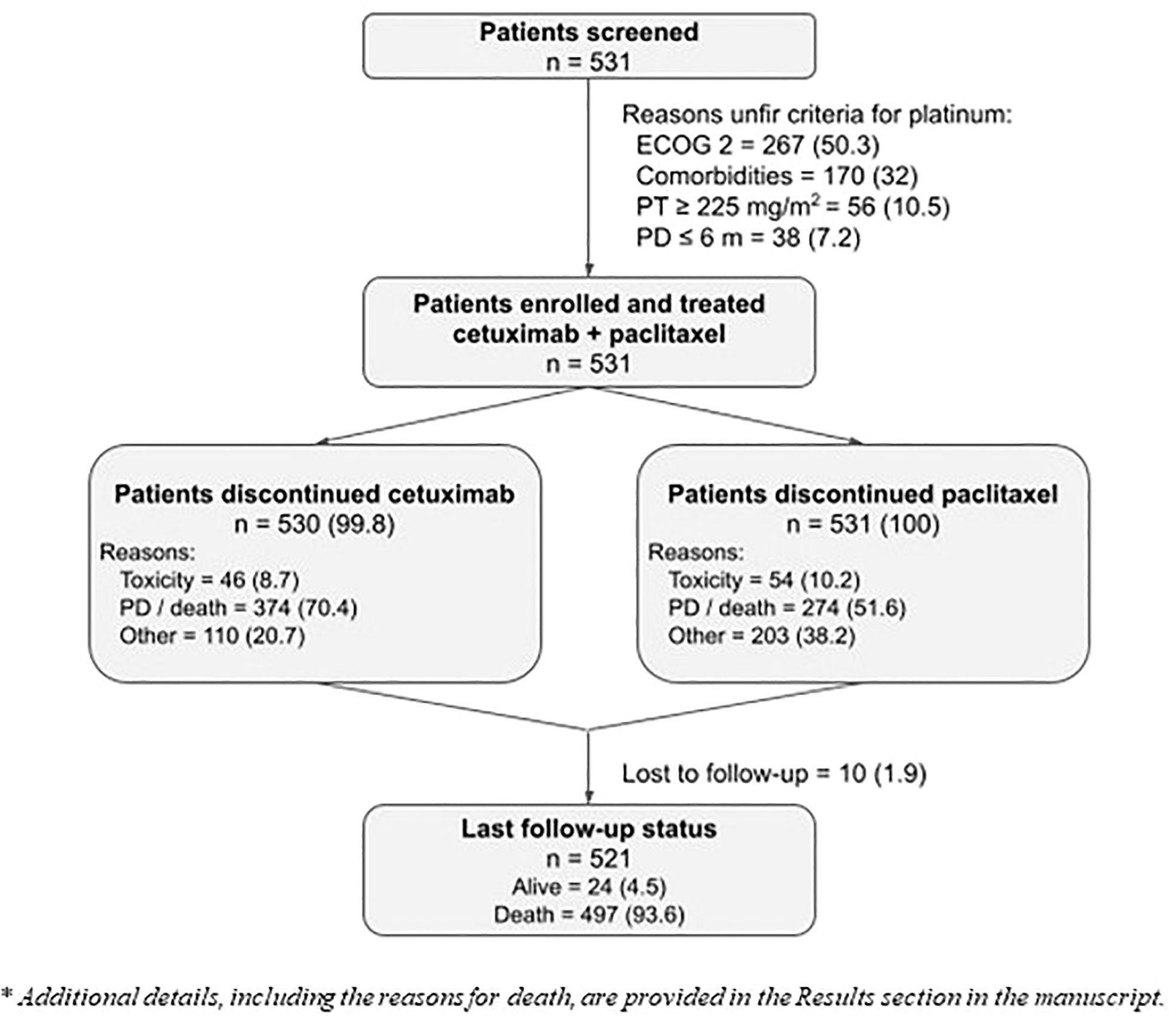
Figure 1 Patient disposition. Numbers are expressed as number of patients and percentage; n (%). The reasons for unfit criteria were ranked with ECOG 2 being the first evaluated, comorbidities second, and platinum ineligibility due to high accumulated dose or refractoriness as third.
3.2 Demographic and baseline clinical characteristics
The median age of our sample was 66 years (range: 35–92). Most patients were male (82.7%), were smokers or former smokers (83.5%), had an ECOG score of 2 (50.3%), and had stage IVa-b disease at diagnosis (58.9%). The most common primary tumor sites were oral cavity (36.2%), larynx (30.9%), oropharynx (19.2%) and hypopharynx (13.7%). Previous systemic chemotherapy before recurrent/metastatic setting was administered to 333 (62.7%) patients (Table 1). Previous taxanes during induction were administered to 139 (26.2%) patients. Regarding the ineligibility criteria for PT, the distribution of patients was as follows: ECOG 2, 267 patients (50.3%); comorbidities, 170 patients (32%); PT cumulative dose ≥ 225 mg/m2, 56 patients (10.5%); PT refractoriness, 38 patients (7.2%).
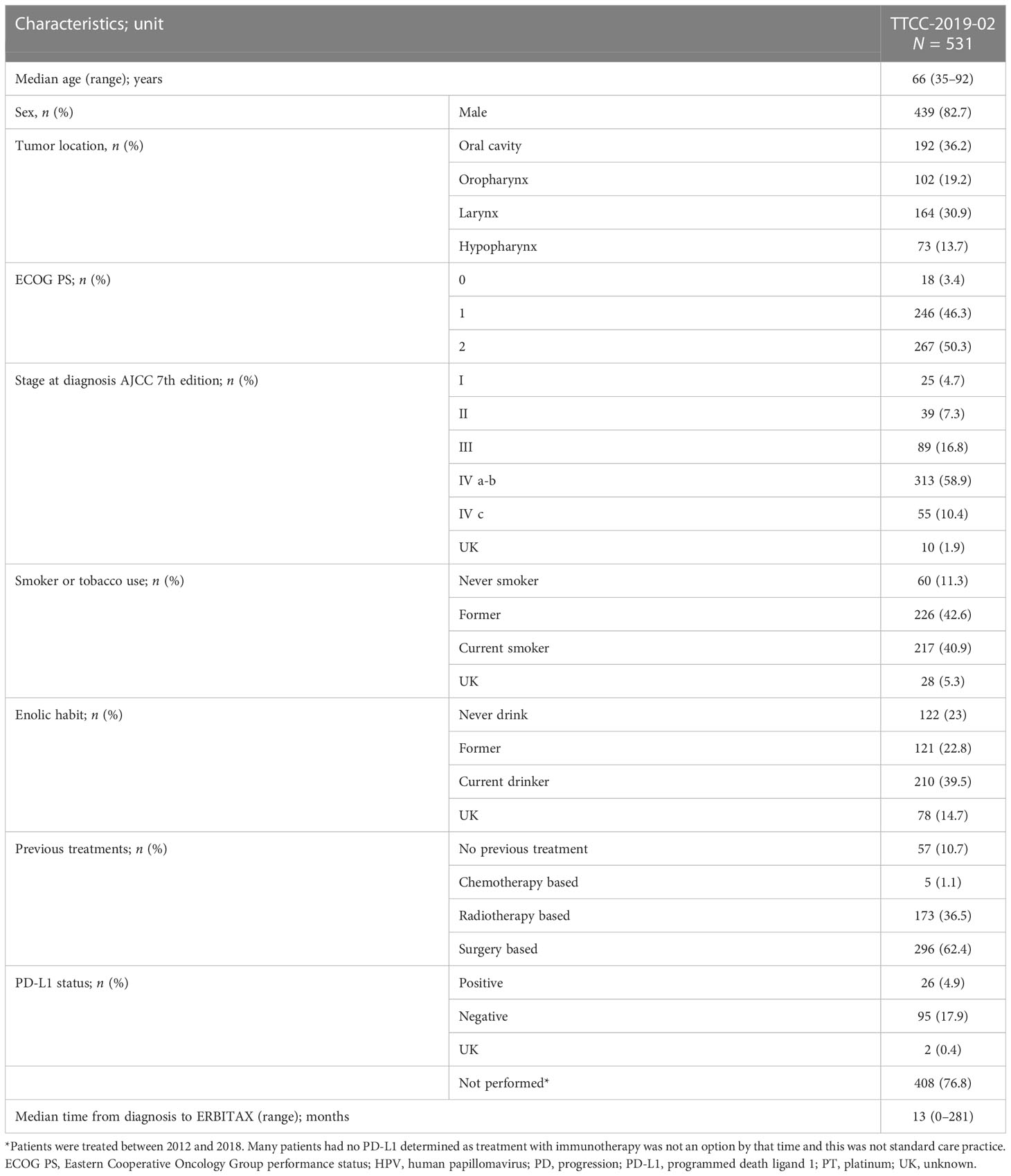
Table 1 Baseline characteristics.
3.3 Treatment compliance
At the data cutoff, most patients discontinued the study treatment, only 1 patient continued treatment with cetuximab, and none with paclitaxel (Figure 1). The most common cause of permanent discontinuation was disease progression (59% for CX and 41.1% for PX; percentages vary between treatments due to patients who progressed during cetuximab maintenance monotherapy). Cetuximab and paclitaxel were discontinued due to toxicity in 8.7% and 10.2% of patients, respectively (Figures 2A, B). Some patients discontinued one or both drugs due to medical decisions, generally after a long period of treatment, to avoid future toxicities, such as neurotoxicity in the case of PX. Some patients refused to continue with the treatment with absence of adverse events or other documented reasons that would have led to treatment discontinuation. The median duration of treatment with cetuximab was 3.5 months (95% CI: 3.0–4.1) and that with paclitaxel was 2.8 months (95% CI: 2.7–3.2). Dose reductions and temporary interruptions of cetuximab (6.6% and 13.9%) and paclitaxel (7.7% and 13.6%) were required to manage treatment-emergent toxicities. Overall, 219 (41.4%) patients did not achieve 100% RDI for cetuximab, and 66 (12.4%) patients did not achieve 100% RDI for paclitaxel (Figure 2C).
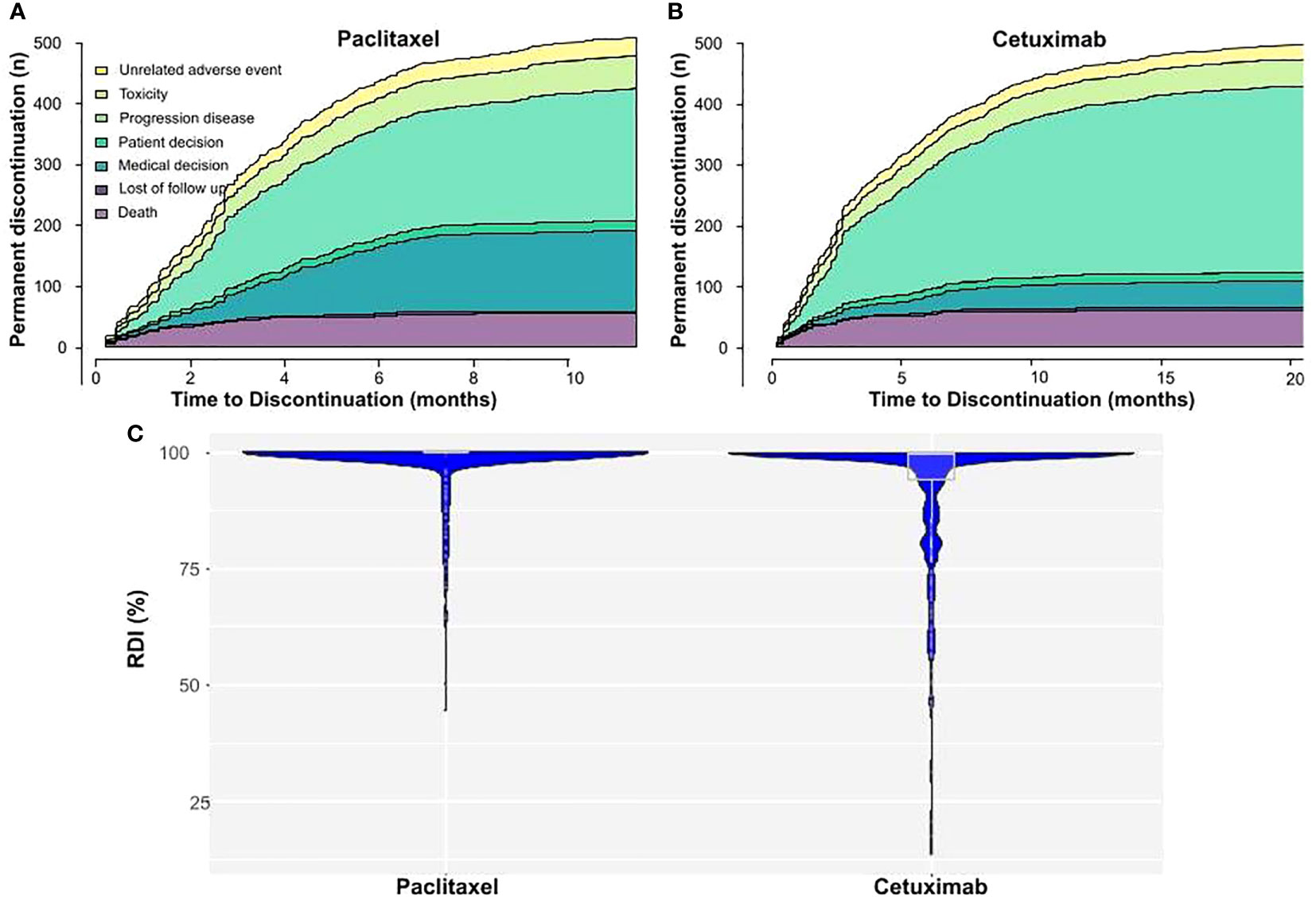
Figure 2 Cetuximab and paclitaxel treatment compliance. (A) Cetuximab and (B) Paclitaxel permanent discontinuations through time. The number of discontinuations is coloured according to the cause of discontinuation. (C) Relative dose intensity (RDI) for cetuximab and paclitaxel. The width of the plot in the X axis represents the number of patients with those RDI levels.
3.4 Efficacy
The locally assessed ORR was 37.7% (95% CI: 33.5–41.9); 37 (7%) patients achieved CR, 163 (30.7%) achieved PR, 90 (17%) achieved stable disease, 118 (22.2%) progressed, and 123 (23%) patients were not radiologically evaluated. DCR was 54.6% (95% CI: 50.3–58.9). The median DoR for the 200 patients who experienced a response was 5.6 months (95% CI: 4.8–6.6). The median duration of SD was 3.2 months (95% CI: 2.4–3.8).
The median follow-up was 8.7 months (range: 0.1–104.1). The median PFS was 4.5 months (95% CI: 3.9–5), with a 1-year PFS rate of 14.9% (95% CI: 12.1–18.4) (Figure 3A).
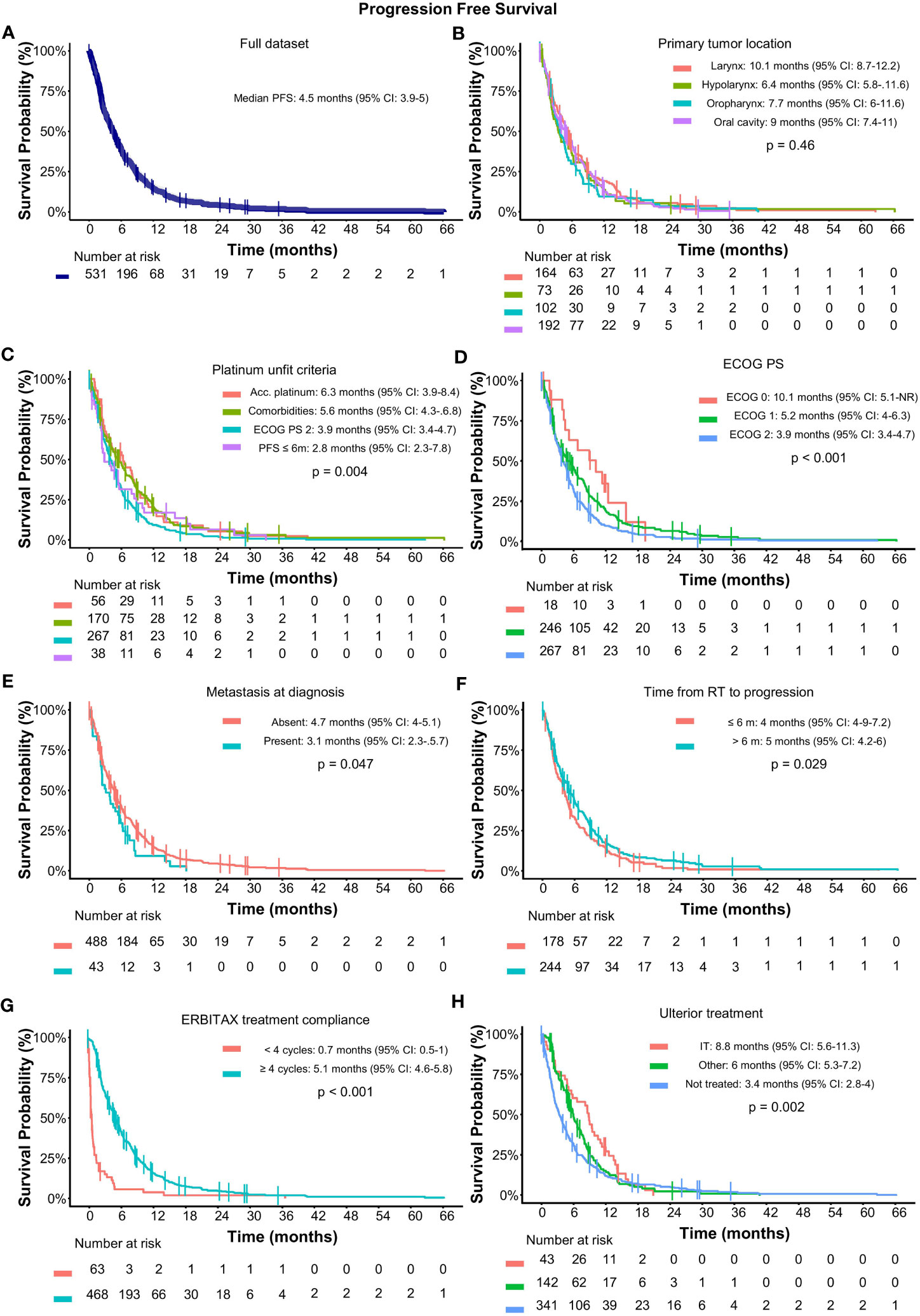
Figure 3 Progression-free survival in SCCHN treated with cetuximab and paclitaxel as first-line treatment. (A) PFS for the full dataset; Subgroup analysis of PFS according to (B) primary tumor location; (C) unfit criteria; (D) ECOG PS; (E) metastatic status at diagnosis; (F) time from radiotherapy; (G) ERBITAX treatment compliance; and (H) ulterior treatment. Median PFS and significance by cox model are displayed within the graphics. Acc, accumulated; CI, confidence interval; ECOG PS, Eastern cooperative oncology group performance status; IT, immunotherapy; RT, radiotherapy; PFS, progression-free survival.
Subgroup analysis according to primary tumor location showed similar PFS regardless of tumor origin (Figure 3B). Patients who were considered unfit for platinum due to comorbidities or accumulated doses of platinum had better prognosis than those with ECOG 2 or platinum refractoriness, with a median PFS of 6.3 and 5.6 months versus, 3.9, and 2.8 months, respectively; p-value = 0.004) (Figure 3C). Accordingly, ECOG PS was correlated with prognosis and showed a median PFS of 10.1, 5.2, and 3.9 months for ECOG 0 to 2, respectively (p-value < 0.001) (Figure 3D). Patients who presented with metastatic disease at baseline, treatment compliance, and more than 6 months from the end of radiotherapy also correlated with the prognosis (Figures 3E–G).
No differences in PFS were observed regarding previous local treatment based on surgery (4.8 months) or radiotherapy (3.6 months, p = 0.147) or the use of taxanes or not in induction treatment (4.7 vs. 4.0 months, p = 0.627). Patients who received ICI in any subsequent treatment line had a median PFS of 8.8 months (95% CI: 5.6–11.3) while patients who received subsequent treatments different than ICI had a median PFS of 6 months (95% CI: 2.8–4) (p-value = 0.002) (Figure 3H).
Overall, 497 (93.6%) patients died. The most common cause of death was inexorable progression of the disease (82.3%). One patient died due to lung infection and another due to sepsis, both secondary to treatment toxicity. The median OS was 8.9 months (95% CI: 7.8–10.3), with a 1-year OS rate of 38.2% (95% CI: 34.2–42.6) (Figure 4A). As happened for PFS, patients who were considered unfit for platinum due to comorbidities or accumulated doses of platinum had better OS than those with ECOG 2 or platinum refractoriness (Figure 4B).
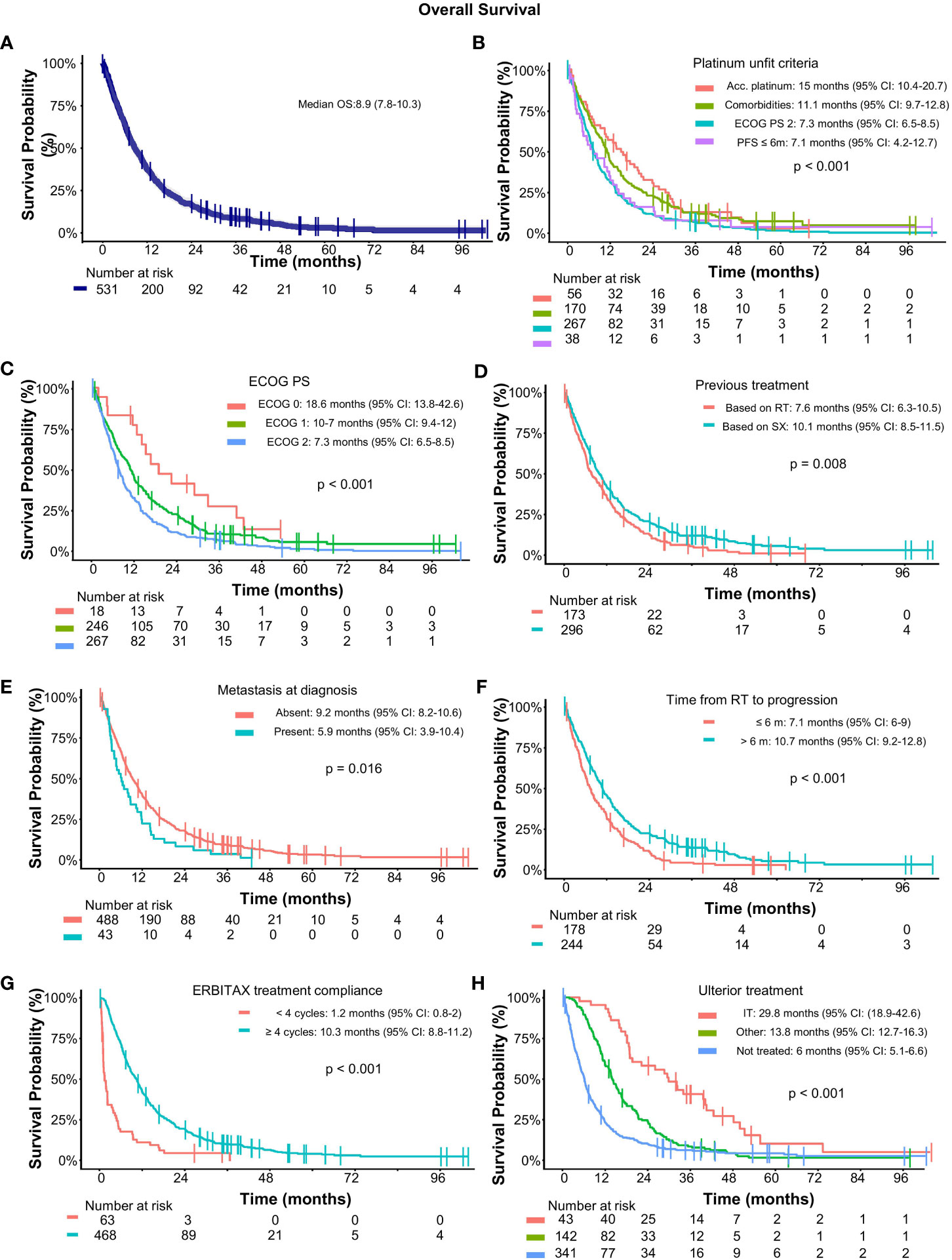
Figure 4 Overall survival in SCCHN treated with cetuximab and paclitaxel as first-line treatment. (A) OS for the full dataset; Subgroup analysis of OS according to (B) pundit criteria; (C) ECOG PS; (D) Previoous treatments; (E) metastatic status at diagnosis; (F) time from radiotherapy; (G) ERBITAX treatment compliance; and (H) ulterior treatment. Median OS and significance by cox model are displayed within the graphics. Acc, accumulated; CI, confidence interval; ECOG PS, Eastern cooperative oncology group performance status; IT, immunotherapy; RT, radiotherapy.
A subgroup of 11 (2.1%) long-term survivors were disease-free and alive >2 years after the start of study treatment. Only 3 of them underwent subsequent treatments. Multivariate and log-rank analysis revealed that patients with better ECOG performance status, with absence of metastasis at diagnosis, and who are compliant with treatments (Figures 4C–G) had better OS. The use of taxanes in induction was not significant for OS.
Patients treated with ICI (nivolumab) in subsequent lines also had better survival with a median OS of 29.8 months (95% CI: 18.9–42.6) and 13.8 months (95% CI: 12.7–16.3) for immunotherapy and other treatments, respectively (p-value < 0.001) (Figure 4H). After ERBITAX, the median duration of response was 6.9 months (95% CI: 5.3–9.8) for patients who were subsequently treated with ICI and 4.6 months (95% CI: 3.7–6.5) for other treatments (p = 0.04).
Patients who received subsequent immunotherapy had significantly better ECOG performance and outcomes to ERBITAX than those who received other ulterior therapies (Table 2). Those patients had a good median PFS of 3.2 months (95% CI: 2.2–11.8) when receiving immunotherapy as second line or 5.6 months (95% CI: 4.2–16.1) even in third-line therapy (p = 0.197) (Figure 5). Patients treated with other drugs instead of ICI mainly received schemes based on carboplatin (43%) or methotrexate (43%). PDL1 determination was performed in few patients (Table S1) since the indication for nivolumab was independent of its result. Its approval by the regulatory agencies in our country was in 2017.
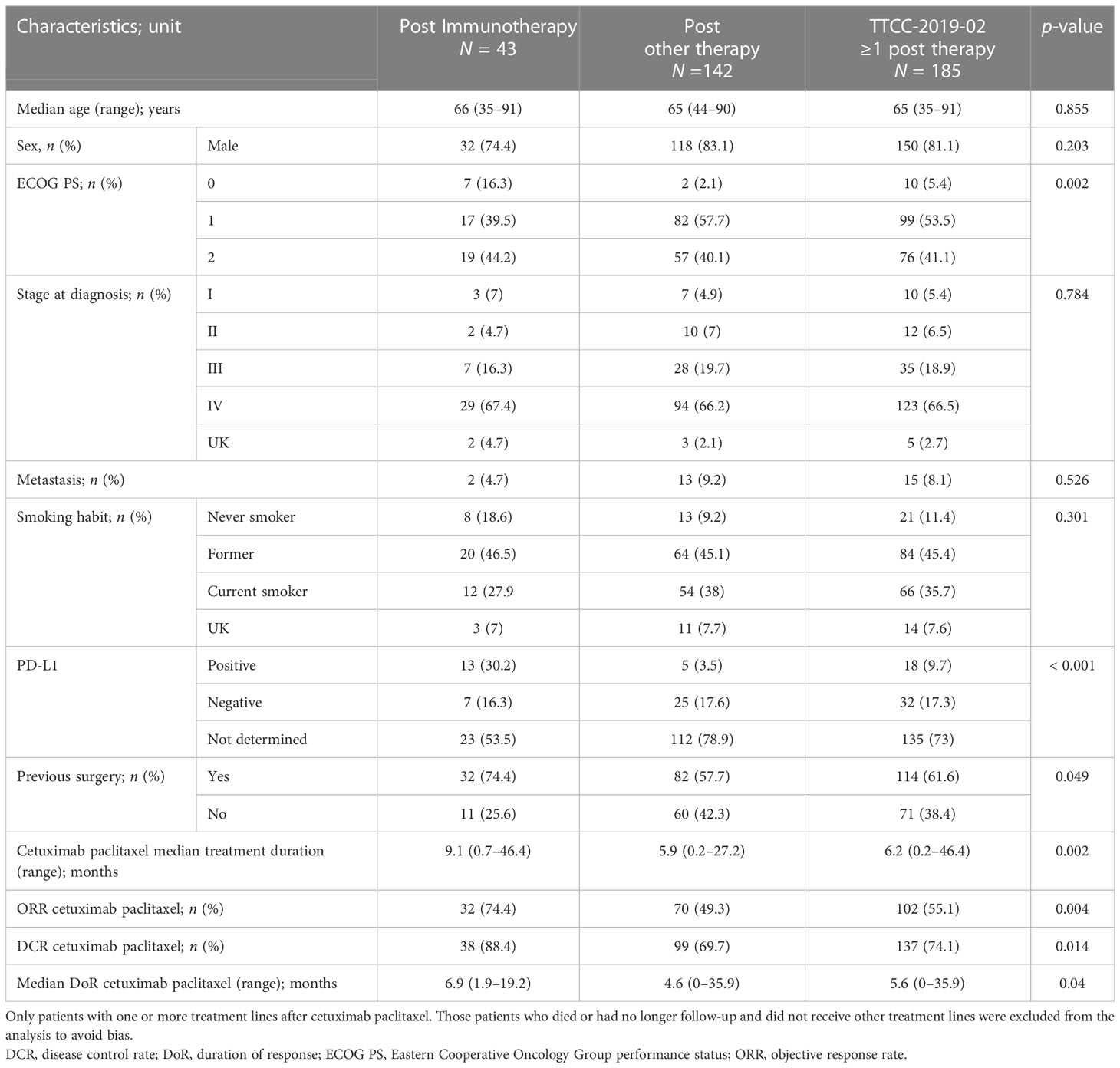
Table 2 Baseline characteristics for patients who received ulterior immunotherapies or other treatments.
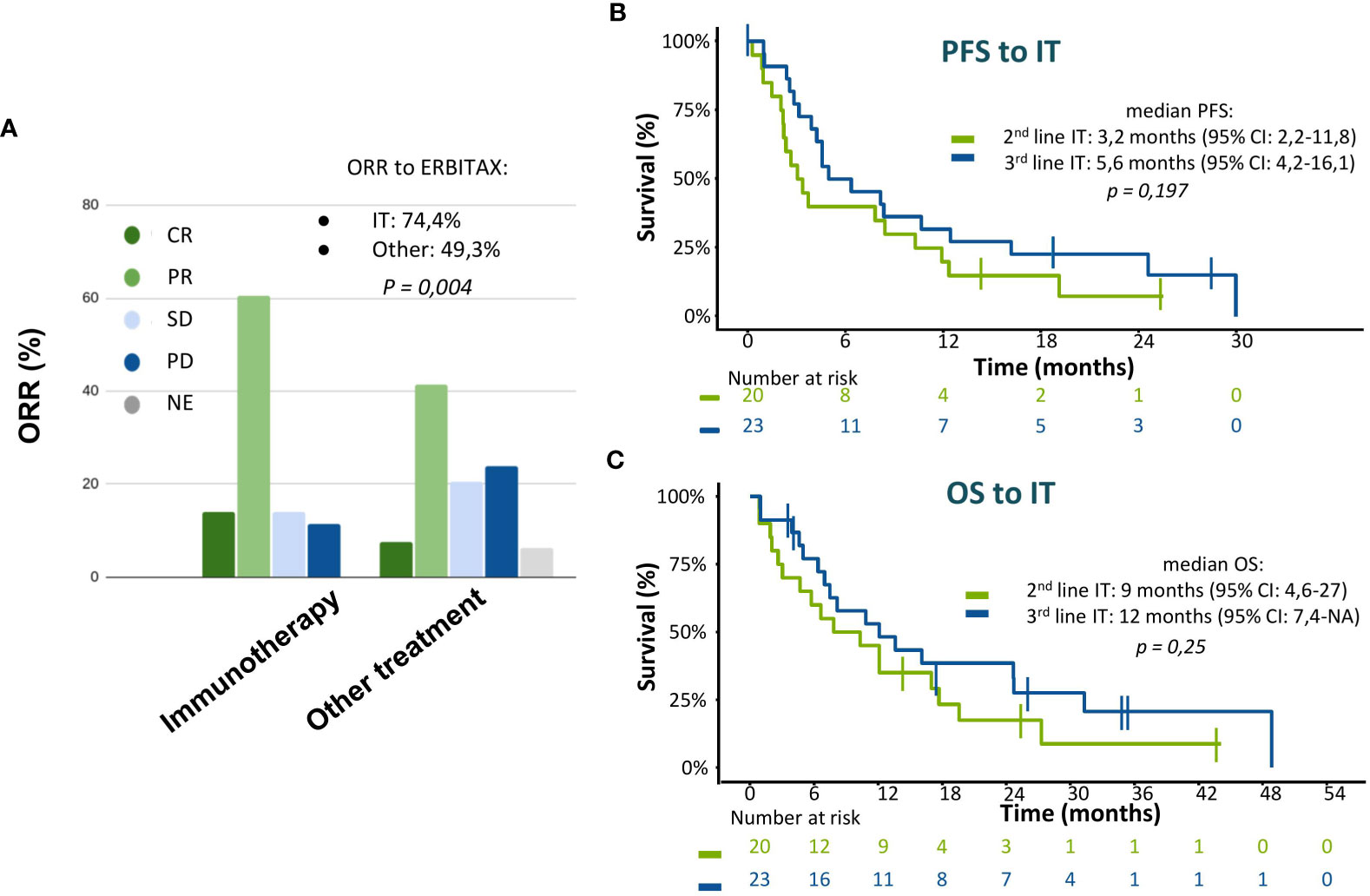
Figure 5 Efficacy of immunotherapy after a first line with ERBITAX regimen. (A) ORR to ERBITAX scheme with patients stratified according to ulterior treatment. (B) PFS to immunotherapy treatment stratified by treatment line, patients who were treated with immunotherapy as second line vs third line. (C) OS to immunotherapy treatment stratified by treatment line, patients who were treated with immunotherapy as second line vs third line. CI, confidence interval; IT, immunotherapy; ORR, objective response rate; OS, overall survival; PFS, progression-free survival.
3.5 Safety
The study collected only those AEs that were grade ≥ 3 or led to discontinuation or dose reduction of paclitaxel and/or cetuximab or met criteria for serious AE (SAE). Ninety-four (17.7%) patients experienced grade ≥ 3 treatment-related AEs (toxicities). The most common grade ≥ 3 toxicities were acne-like rash in 36 patients (6.8%) and oral mucositis in 8 patients (1.5%) (Table 3). Five (0.9%) patients experienced grade ≥ 3 febrile neutropenia and three (0.6%) had grade ≥ 3 hypomagnesemia, all of whom were properly managed with dose temporary interruptions or reductions. Three patients experienced grade ≥ 3 neurotoxic effects, including paresthesia in two (0.4%) patients and peripheral sensory neuropathy in one (0.2%). Regarding those AEs that led to discontinuation of the regimen, skin rash in 18 patients (3.4%) was the main one.
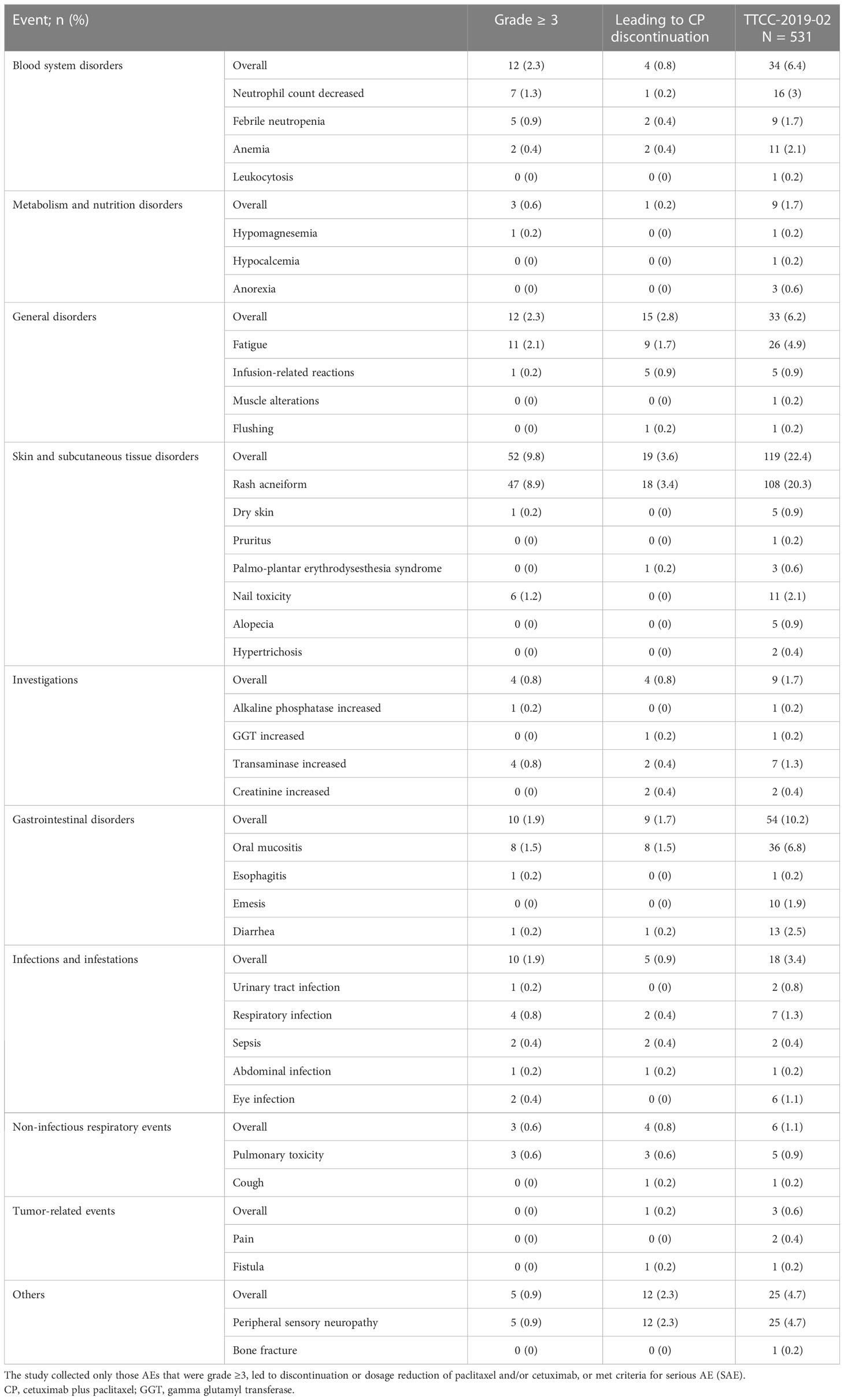
Table 3 Toxicities (treatment-related AEs) to cetuximab plus paclitaxel treatment.
4 Discussion
The TTCC-2019-02 study showed that ERBITAX regimen is an active first-line treatment option in routine clinical practice for patients with recurrent or metastatic SCCHN who are considered ineligible for platinum-based regimens. The real-world efficacy outcomes agreed with the previous trial that tested ERBITAX (10), in which median PFS and OS were 4.2 and 8.1 months, respectively. Despite the limitations of indirect comparison, the ORR reported in our study was similar to that of first-line platinum/5-FU with cetuximab in the EXTREME trial (37.7% vs. 36%, respectively), in line with the survival outcomes (3). As in a previous report, ERBITAX showed efficacy regardless of previous treatment (10). Treatment compliance was also associated with better outcomes, even though we could not discard bias due to the presence of patients with the worst prognosis among those who had early treatment discontinuation. Twelve percent of patients received less than 4 weeks of ERBITAX, some of whom may be poorly selected to receive chemotherapy. In those who received more than 3 weeks of ERBITAX, a median PFS greater than 5 months was obtained.
The results are especially encouraging considering that a high proportion of patients had an ECOG PS of 2 (50.3%), which is considered a poor prognostic factor associated with inferior OS (13, 14). Having comorbidities or high accumulated doses of platinum as the primary reason for platinum ineligibility showed a significant benefit in survival compared to other platinum unfit criteria, suggesting that the ERBITAX scheme as a first-line treatment should be specially considered for those patient profiles. Similar results have been reported in other retrospective studies (14, 15).
Recently, immunotherapy has changed the paradigm of advanced or metastatic SCCHN. Nivolumab and pembrolizumab in mostly pretreated patients showed an ORR of 13.3% and 14.6% and a median OS of 7.5 and 8.4 months, respectively (5, 6, 16). We observed a remarkably prolonged PFS and OS from the diagnosis of advanced or metastatic disease in patients who received immunotherapy after ERBITAX, even in patients ECOG PS 2, who were not included in the immunotherapy trials.
Real-world studies of immunotherapy after platinum-based chemotherapy reported similar activity to that of phase 3 trials, with a median OS that ranged from 6.5 to 8.7 months (17, 18). Only one previous real-world study with SCCHN patients who received immunotherapy as second-line therapy reported a prolonged median OS of 22.1 months in line with our results (19). DoR and survival were substantially longer in those who received immunotherapy after first-line chemotherapy, suggesting a potential boosting effect of previous chemotherapy (19). Despite their poor prognosis, we achieve that a percentage of patients, although low, can benefit from subsequent lines and improve survival.
The baseline characteristics of the patients who received ulterior immunotherapy suggested a potential selection bias. This may explain the good result of these subsequent lines of treatment. Patients with better outcomes with ERBITAX received immunotherapy in the standard clinical practice. We could not discard the potential conditioning effect of the first-line treatment as already reported in other studies that combine taxanes and cetuximab (4). Retrospective studies propose to explore what is the best combination strategy between schemes with ICI and with cetuximab (20), also given the current positioning of ICI as a first-line treatment for advanced SCCHN.
Regarding tolerability, the rate of permanent discontinuation due to toxicity for cetuximab (8.7%) and paclitaxel (10.2%) was amenable, in line with previous reports (4.6%–13%) (10, 15), and lower than that reported for the EXTREME scheme (20%) (3). The median duration of ERBITAX was shorter than that in the previous clinical trial (6 months) (10) or patients who received the EXTREME scheme (4.5 months) (3, 21), which may indicate that real-world patients discontinue earlier and for reasons other than toxicity. The toxicity profile was similar to that of other clinical trials, with acneiform rash being the most common event (10, 15).
The study is based on the data collected in the clinical reports in the routine practice; thus, the AEs may be under-reported, especially those of low grade. Indirect comparisons of the frequencies of any-grade AEs with previous clinical trials were not feasible as the study only collected AEs leading to treatment discontinuation, those with grade ≥ 3, or those considered serious. The rate of grade ≥ 3 toxicities (17.7%) was much lower than that reported in previous trials (65%) (10). Hypomagnesemia and febrile neutropenia were less frequent than previously reported (10, 15). Two deaths were related to infection processes secondary to the study medication.
The main limitation of this study was its retrospective design, which may have led to an increased rate of missing data, which did not compromise the interpretation of our results. The greatest missing data were reported for smoking habits (5.3%) or stage at diagnosis (1.9%).
Some patients initially with bad performance status due to tumor effect were able to benefit from the response to ERBITAX, improve it, and receive carboplatin-based regimens at next disease progression.
The therapeutic scenario at the time in which the study patients were treated was different from the current one. Some refractory patients or those with contraindications to platinum and positive CPS can now benefit from first-line immunotherapy. Given the good tolerance and effectiveness of ERBITAX, this scheme could be placed in the treatment after progression to chemo-immunotherapy or for those patients who, being refractory to cisplatin, need a fast response.
5 Conclusion
Our trial demonstrates that the ERBITAX scheme is feasible as a first-line treatment for advanced SCCHN patients unfit for platinum-based chemotherapy. Treatment with ICI in subsequent lines after ERBITAX implies an important benefit in survival.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethic Commitee of each participating institution. The patients/participants provided their written informed consent to participate in this study.
Author contributions
JR-C, BCC and RM were the coordinators of the project and responsible for the final writing of the manuscript. MD was the data coordinator at Spanish Group of Head and Neck Cancer Treatment (TTCC). All authors contributed to study design, patient data acquisition and to the analysis and interpretation of the study results. All authors corrected and approved the final manuscript.
Funding
This work was sponsored by the Grupo Español de Tumores de Cabeza y Cuello (TTCC). The authors declare that this study received funding from Merck S.L.U. Madrid, Spain, an affiliate of Merck KGaA (Funder ID: 10.13039/100009945). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
We acknowledge MFAR Clinical Research staff for their assistance with the development of this study. Pau Doñate, Ph.D., and Jordi Curto, M.Sc., both from MFAR Clinical Research (Barcelona, Spain), contributed to the medical writing and statistical analysis, respectively.
Conflict of interest
JR-C: Advisory role: Sanofi, Novartis and Merck. BCC: Support for this manuscript from Merck through TTCC Group. Speaker on behalf of BMS, MSD, and Merck. Meeting support from BMS and MSD. Member of TTCC Group unpaid. MP: Speaker on behalf of BMS. Meeting support from MSD Oncology. AG: Advisory board from MSD and Bristol Myers Squibb. AC: Speaker on behalf of Merck. Meeting support from Merck. LI: Speaker on behalf of Merck, MSD, Roche, Bayer, Eisai. Meeting support from Merck and MSD. Advisory board from Merck MSD, Roche, Lilly, and Ipsen. PP: Received grants from BMS, Merck, and MSD. Consulting fees from BMS, Merck, and MSD. Speaker on behalf of BMS, Merck, and MSD. Meeting support from BMS, Merck, and MSD. Member of TTCC Group. IC: Speaker on behalf of MSD, Merck, Roche, BMS, Seagen, and Pfizer. Meeting support in Pfizer, MSD, and Merck. CP: Speaker on behalf of Novartis, Merck, and MSD. Meeting support from Novartis, Merck, and MSD. IH: Speaker on behalf of Pierre Fabre educational event and Merck lecture. Meeting support from Merck support for an event and AztraZeneca support for educational expertise. MC: Participated in and received equipment for clinical trials from the institution. Speaker on behalf of MSD and Merck. Meeting support from MSD and Merck. EO: Speaker on behalf of GSK, AstraZeneca, Clovis, Merck, Pharmamar, and MSD. Expert testimony for GSK. Meeting support from Merck and MSD. Advisory board for Eisai. RM: Support for this manuscript from Merck for medical writing and article processing charges. Speaker on behalf of MSD and Merck. Meeting support from BMS, Merck, and MSD. Advisory board for MSD, Merck, Boehringer, Bayer, Roche, Nanobiotics and Sigean.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2023.1226939/full#supplementary-material
Abbreviations
AEs, Adverse events; BOR, Best overall response; CI, Confidence interval; HR, Hazard ratio; OS, Overall survival; PFS, Progression-free survival; RDI, Relative dose intensity; SCCHN, Squamous cell carcinoma of the head and neck; SEOM, Society of Medical; CR, Complete response; DCR, Disease control rate; DoR, Duration of response; GGT, Gamma glutamyl transferase; ORR, Objective response rate; PD, Progressive disease; PR, Partial response; SD, Standard disease.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. Machiels J-P, René Leemans C, Golusinski W, Grau C, Licitra L, Gregoire V, et al. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol (2020) 31(11):1462–75. doi: 10.1016/j.annonc.2020.07.011
3. Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med (2008) 359(11):1116–27. doi: 10.1056/NEJMoa0802656
4. Guigay J, Aupérin A, Fayette J, Saada-Bouzid E, Lafond C, Taberna M, et al. Cetuximab, docetaxel, and cisplatin versus platinum, fluorouracil, and cetuximab as first-line treatment in patients with recurrent or metastatic head and neck squamous-cell carcinoma (GORTEC 2014-01 TPExtreme): a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol (2021) 22(4):463–75. doi: 10.1016/S1470-2045(20)30755-5
5. Ferris RL, Blumenschein G Jr., Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med (2016) 375(19):1856–67. doi: 10.1056/NEJMoa1602252
6. Cohen EEW, Soulières D, Le Tourneau C, Dinis J, Licitra L, Ahn M-J, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet (2019) 393(10167):156–67. doi: 10.1016/S0140-6736(18)31999-8
7. Burtness B, Harrington KJ, Greil R, Soulières D, Tahara M, de Castro G, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet (2019) 394(10212):1915–28. doi: 10.1016/S0140-6736(19)32591-7
8. Olshan AF. Epidemiology, pathogenesis, and prevention of head and neck cancer Vol. 1. . New York, NY: Springer, Publishers (2010).
9. Hashibe M, Brennan P, Chuang S-C, Boccia S, Castellsague X, Chen C, et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: pooled analysis in the international head and neck cancer epidemiology consortium. Cancer Epidemiol Biomarkers Prev (2009) 18(2):541–50. doi: 10.1158/1055-9965.EPI-08-0347
10. Hitt R, Irigoyen A, Cortes-Funes H, Grau JJ, Garcia-Sáenz JA, Cruz-Hernandez JJ, et al. Phase II study of the combination of cetuximab and weekly paclitaxel in the first-line treatment of patients with recurrent and/or metastatic squamous cell carcinoma of head and neck. Ann Oncol (2012) 23(4):1016–22. doi: 10.1093/annonc/mdr367
11. Porceddu SV, Scotté F, Aapro M, Salmio S, Castro A, Launay-Vacher V, et al. Treating patients with locally advanced squamous cell carcinoma of the head and neck unsuitable to receive cisplatin-based therapy. Front Oncol (2020) 9:1522. doi: 10.3389/fonc.2019.01522
12. Falco A, Bueno de Oliveira T, Cacicedo J, Ospina AV, Ticona MA, Galindo H, et al. Ibero-American expert consensus on squamous cell carcinoma of the head and neck treatment in patients unable to receive cisplatin: recommendations for clinical practice. Cancer Manag Res (2021) 13:6689–703. doi: 10.2147/CMAR.S322411
13. Pogorzelski M, Hilser T, Ting SC, Kansy B, Gauler TC, Stuschke M, et al. Identification of a prognostic clinical score for patients with recurrent or metastatic squamous cell carcinoma of the head and neck treated with systemic therapy including cetuximab. Front Oncol (2021) 11:635096. doi: 10.3389/fonc.2021.635096
14. Naruse T, Yanamoto S, Otsuru M, Yamakawa N, Kirita T, Shintani Y, et al. Multicenter retrospective study of weekly cetuximab plus paclitaxel for recurrent or metastatic oral squamous cell carcinoma. Anticancer Res (2021) 41(11):5785–91. doi: 10.21873/anticanres.15395
15. Enokida T, Okano S, Fujisawa T, Ueda Y, Uozumi S, Tahara M. Paclitaxel plus cetuximab as 1st line chemotherapy in platinum-based chemoradiotherapy-refractory patients with squamous cell carcinoma of the head and neck. Front Oncol (2018) 8:339. doi: 10.3389/fonc.2018.00339
16. Gillison ML, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Long-term outcomes with nivolumab as first-line treatment in recurrent or metastatic head and neck cancer: subgroup analysis of CheckMate 141. Oncologist (2022) 27(2):e194–8. doi: 10.1093/oncolo/oyab036
17. Vasiliadou I, Breik O, Baker H, Leslie I, Ren Sim V, Hegarty G, et al. Safety and treatment outcomes of nivolumab for the treatment of recurrent or metastatic head and neck squamous cell carcinoma: retrospective multicenter cohort study. Cancers (Basel) (2021) 13(6):1413. doi: 10.3390/cancers13061413
18. Singh P, McDonald L, Waldenberger D, Welslau M, von der Heyde E, Gauler T, et al. Pooled analysis of nivolumab treatment in patients with recurrent/metastatic squamous cell carcinoma of the head and neck in the United States and Germany. Head Neck (2021) 43(11):3540–51. doi: 10.1002/hed.26853
19. Even C, Torossian N, Ibrahim T, Martin N, Mayache Badis L, Ferrand FR, et al. First-line versus second-line immunotherapy in recurrent/metastatic squamous cell carcinoma of the head and neck. Ann Oncol (2019) 30(5):v462. doi: 10.1093/annonc/mdz252.030
20. Park JC, Durbeck J, Clark JR, Faden DL. Treatment sequence of cetuximab and immune checkpoint inhibitor in head and neck squamous cell carcinoma differentially affects outcomes. Oral Oncol (2020) 111:105024. doi: 10.1016/j.oraloncology.2020.105024
21. Sano D, Fujisawa T, Tokuhisa M, Shimizu M, Sakagami T, Hataro T, et al. Real-world treatment outcomes of the EXTREME regimen as first-line therapy for Recurrent/Metastatic squamous cell carcinoma of the head and neck: a multi-center retrospective cohort study in Japan. Anticancer Res (2019) 39(12):6819–27. doi: 10.21873/anticanres.13898
Keywords: squamous cell carcinoma of head and neck, cetuximab, paclitaxel, platinum ineligible, frail patients
Citation: Rubió-Casadevall J, Cirauqui Cirauqui B, Martinez Trufero J, Plana Serrahima M, García Castaño A, Carral Maseda A, Iglesias Docampo L, Pérez Segura P, Ceballos Lenza I, Gutiérrez Calderón V, Fuster Salvà J, Pena Álvarez C, Hernandez I, del Barco Morillo E, Chaves Conde M, Martínez Galán J, Durán Sánchez M, Quiroga V, Ortega E and Mesia R (2023) TTCC-2019-02: real-world evidence of first-line cetuximab plus paclitaxel in recurrent or metastatic squamous cell carcinoma of the head and neck. Front. Oncol. 13:1226939. doi: 10.3389/fonc.2023.1226939
Received: 22 May 2023; Accepted: 27 June 2023;
Published: 01 August 2023.
Edited by:
Tomoya Yokota, Shizuoka Cancer Center, JapanReviewed by:
Shinya Suzuki, National Cancer Center Hospital East, JapanMaria Cossu Rocca, European Institute of Oncology (IEO), Italy
Copyright © 2023 Rubió-Casadevall, Cirauqui Cirauqui, Martinez Trufero, Plana Serrahima, García Castaño, Carral Maseda, Iglesias Docampo, Pérez Segura, Ceballos Lenza, Gutiérrez Calderón, Fuster Salvà, Pena Álvarez, Hernandez, del Barco Morillo, Chaves Conde, Martínez Galán, Durán Sánchez, Quiroga, Ortega and Mesia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jordi Rubió-Casadevall, anJ1YmlvQGljb25jb2xvZ2lhLm5ldA==
†These authors have contributed equally to this work