 Li Lin
Li Lin Wei Li
Wei Li Chen Chen1
Chen Chen1 Anhua Wei
Anhua Wei Yu Liu
Yu Liu- 1Department of Oncology, Wuhan Asia General Hospital, Wuhan, China
- 2Department of Pharmacy, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Background: The implanted vascular access ports (PORTs) were compared with peripherally inserted central catheters (PICCs) as the administration of chemotherapy regarding different clinical effects and adverse effects. Which is better is debatable. Hence, the current study was conducted to assess the safety and efficacy of these two optimal vascular access strategies.
Methods: The following electronic databases were searched: PubMed, Embase, and the Cochrane Library updated in May 2023. Studies on the differences in complication rates in patients with cancer using either PICC or PORT for chemotherapy were included. Meta-analysis Revman 5.3 software was used for statistical analysis.
Results: A total of 22 articles were retrieved. The results suggested that PORT has a superior safety profile, with lower incidences of overall adverse effects (OR=2.72, 95% CI=1.56–4.72 P=0.0004), catheter-related thrombosis (OR=2.84, 95% CI=1.97–4.11, P<0.00001), and allergic reactions (OR=6.26, 95% CI=1.86–21.09, P=0.003) than typically expected with PICC. Moreover, PICC was non-inferior to the PORT group with respect to DVT (OR=2.00, 95% CI=0.86–4.65, P=0.11) and infection (OR=1.55, 95% CI=0.75–3.22, P=0.24).
Conclusion: PORT achieved safety benefits compared with chemotherapy through PICC. Therefore, PORT is regarded as safe and effective vascular access for the administration of chemotherapy. When considering economic factors and some key elements, more high-quality research would help verify these clinical benefits.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identififier CRD42023421690.
1 Introduction
A central venous device provides safe and reliable access strategy for the central vein and avoids venous toxicities and peripheral venous punctures for chemotherapy delivery.
To date, peripherally inserted central catheters (PICCs) and implanted vascular access ports (PORTs) are two common infusion pathways representing vital developments in nursing technologies for patients receiving chemotherapy (1).
The PICC was replaced with the central venous catheter (CVC) in the 1970s and has been widely used in modern oncology departments (2). Compared with CVC, PICC has been reported to have many advantages, such as avoiding mechanical complications related to CVC, and PICC trained nurse teams have made it quicker and easier to manage in oncology practice (3). A port catheter (PC), the classical route for receiving chemotherapy, was developed to provide deep venous access and allows for iterative perfusion for years.
Recently, concerns have been raised regarding whether PICC or PORT is the optimal vascular access strategy for patients with cancer. All PICCs can be easily implanted and removed but require weekly maintenance, whereas PORTs need monthly maintenance, usually conducted at the end of the chemotherapy infusion. Many oncologists prefer PICCs over PORTs, with the advantages of ease of implantation by nursing teams without a surgical procedure and lower costs (4). Additionally, the device can be easily removed for source control in cases of infection or thrombosis. Nevertheless, previous studies have indicated a higher rate of complications among oncological patients with PICC than those with PORT (5–7).
A meta-analysis by Wang (8) found that PORTs showed favorable influence in reducing the risk of VTE than PICCs in oncologic patients. Meanwhile, some meta-analyses have been carried out to evaluate the safety efficacy of PICCs versus PORTs. However, the pool results had limitations. The research by Wang et al. (8) only explored the incidence of PORT-and PICC-related VTEs in patients with cancer. Baiying Liu’s study (9) only included patients with non-hematological malignancies. The conclusion of another meta-analysis (10) was applicable only to gynecological cancers.
Thus, a systematic, up-to-date assessment with additional trials is needed. We conducted this meta-analysis to identify evidence for differences in the complication rates of PICC versus PORT in patients with cancer who are receiving chemotherapy, including patients with hematological and non-hematological malignancies.
2 Materials and methods
2.1 Search strategy
Two reviewers separately performed literature searches of the PubMed, Embase, and Cochrane databases until May 2023. The literature searching process was conducted with the keywords: “PICC” AND “PORT” AND “cancer” AND “chemotherapy.” Selected Medical Subject Headings were combined with free text terms following Medical Subject Headings (MeSH) terms relating to PICC (peripherally inserted central catheter line insertion, peripheral catheterization, PICC Line Catheterizations), PORT (vascular access device, TIVAD, implantable access port, implantable port catheter, central venous port access system), cancer (tumor, lymphoma, carcinoma, neoplasms, sarcoma), and chemotherapy (chemical, chemo, chemotherapeutic, pharmacotherapies) in PubMed. No limitation was set during the literature search. The references of the eligible studies were checked for additional studies found in the literature search.
2.2 Eligibility criteria
Inclusion criteria were studies relating to the following: (1) patients: studies that enrolled patients with cancer treated with chemotherapy through central venous access devices; (2) design: articles that focused on comparing PICC and PORT; (3) outcomes of interest including the rate of adverse effects, catheter-related thrombosis, deep vein thrombosis, allergic reaction, and infection; and (4) only English texts.
Articles with the following exclusion criteria were eliminated: (1) trials without a comparison group, (2) incompletely reported data that were unable to provide research outcomes, (3) case reports or observational studies, and (4) duplicate previous literature.
2.3 Quality assessment
The risk of bias for each included study was evaluated based on the risk of bias items (ROBI) recommended in The Cochrane Handbook for Systematic Reviews of Interventions. All cohort studies were justified using the Newcastle–Ottawa Scale (11). The process was conducted by two researchers separately, and differences were resolved through discussion. The Newcastle–Ottawa Scale method uses three domains to assess the quality of cohort studies, which include the selection of patients with cancer, comparability between two groups, and assessment of outcomes. Based on the NOS method, four, two, and three points were awarded to the three domains, respectively. Studies with no less than seven points were identified as having high quality; however, those with six points or less were identified as having low quality.
In addition, the Cochrane Collaboration’s “Risk of bias tool for RCT was used (12). The tools for RCT scored a research article according to the descriptions of randomization (two points), blinding (two points), and attrition information (one point). A score of ≥3 points suggests that the study was of “high quality,” and a score of ≤2 points suggests that the study was of “low quality.” To minimize heterogeneity among studies, only high-quality papers were included. The included studies had comparable baseline clinical characteristics without statistically significant differences between the two groups.
2.4 Data extraction
Two reviewers independently extracted information from each article. Disagreements were resolved through discussion. From each of the eligible studies, the following information was collected: author’s name, year of publication, tumor type, type of PORT, date of collection, number of patients, mean age of the patients, and outcome data of interest.
2.5 Data synthesis and analysis
I2 and chi-square tests were used to assess the heterogeneity of the studies (13). Studies with I2≥50% were considered as high degree of heterogeneity, and I2<50% suggested low heterogeneity (14). A fixed-effects model was used when heterogeneity among the studies was of low degree. A random-effects model was used when the degree of heterogeneity was uncertain (I2>50%). Statistical significance was set at P<0.05. significant. Review Manager version 5.3 software (Revman; The Cochrane Collaboration, Oxford, United Kingdom) was used for statistical analysis. Our results are shown in forest plots, and publication bias was evaluated using funnel plots.
3 Results
3.1 Study selection
A total of 376 publications were retrieved. During the review of abstracts and titles, 27 studies were evaluated through reading the full articles; however, five were excluded based on the inclusion criteria. Finally, 22 studies were further eliminated (15–36). Figure 1 illustrates the search process in detail. Figure 2 presented the summary of the quality assessment process of the RCTs. Table 1 describes the primary characteristics of the eligible studies in detail.
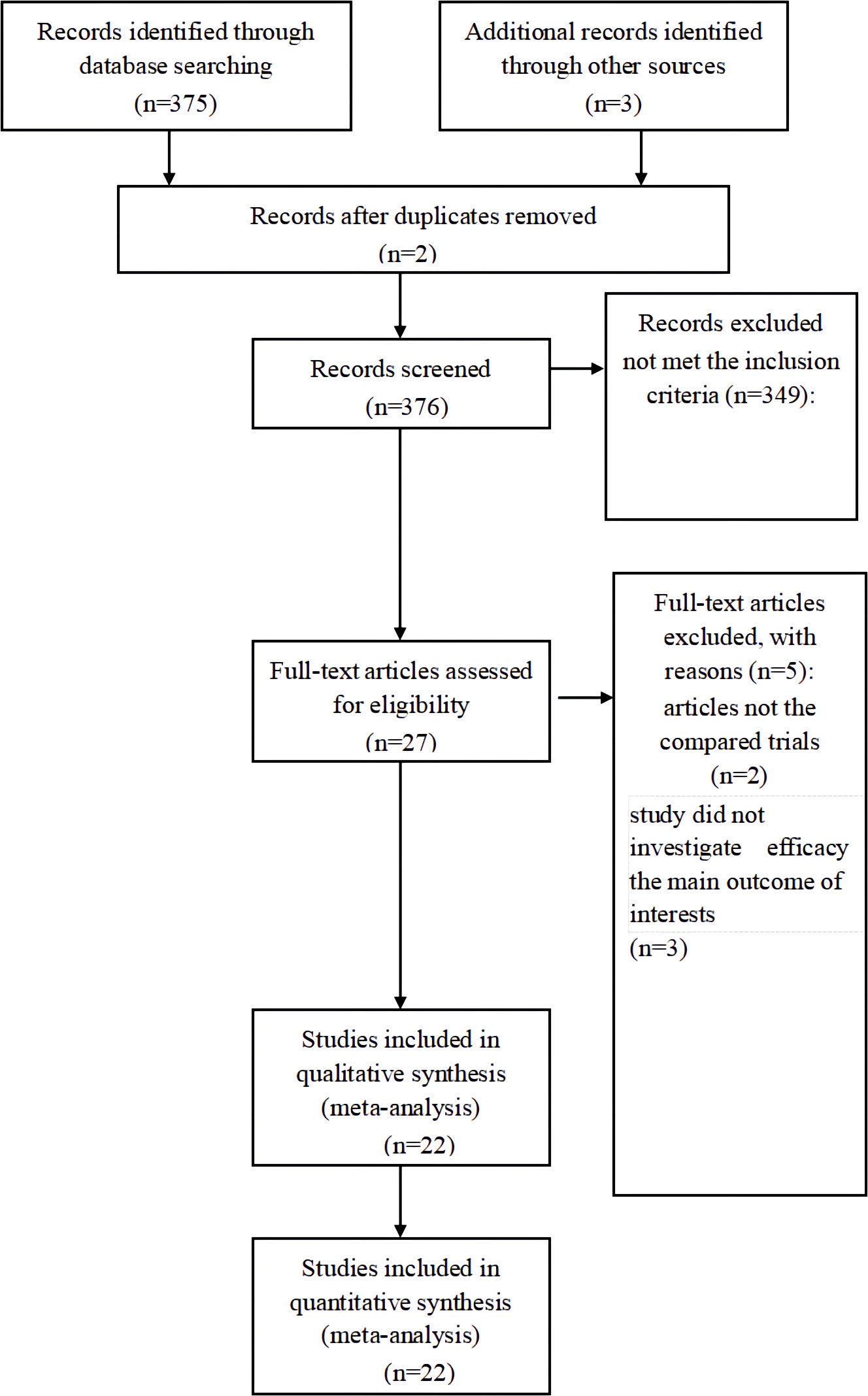
Figure 1 PRISMA flow chart of selection process to identify studies eligible for pooling.
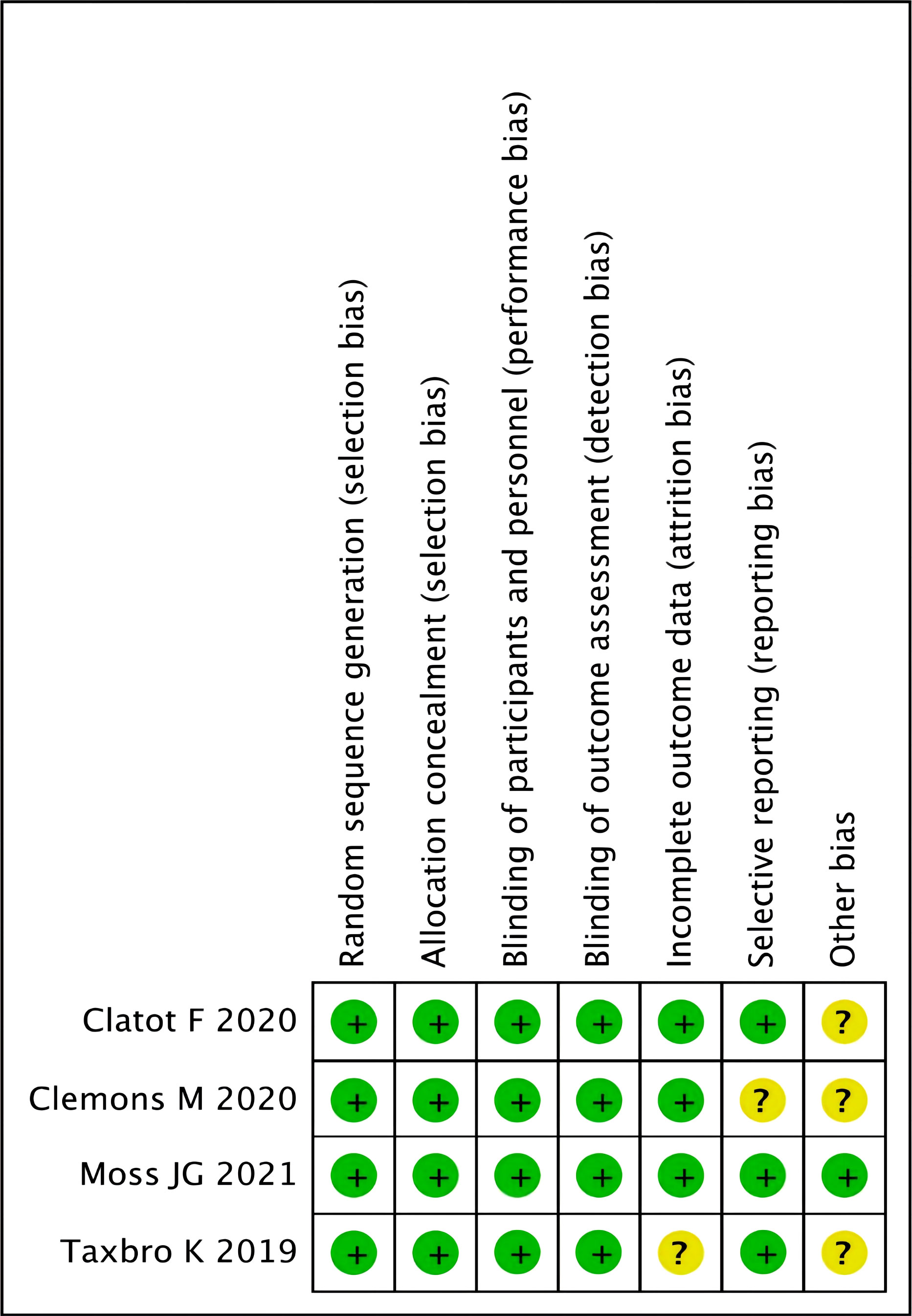
Figure 2 Methodological quality assessment for each RCT study.

Table 1 The primary characteristics of the eligible studies in more detail.
The number of participants with PICC recruited varied among the 22 studies, ranging from 10 to 1433. In addition, the number of participants recruited with PORT ranged from 27 to 4080.
The quality of the included studies was assessed using the NOS method; 18 studies scored at least seven points and thus were of high quality. All the included publications were based on moderate-quality evidence (Table 1).
3.2 Clinical and methodological heterogeneity
3.2.1 Overall adverse effects
Heterogeneity among the 11 studies was high (I2 = 88%, P<0.00001). For the AEs, a significant difference was observed between PICC and PORT with the random-effects model (OR=2.72, 95% CI=1.56–4.72 P=0.0004) (Figure 3).
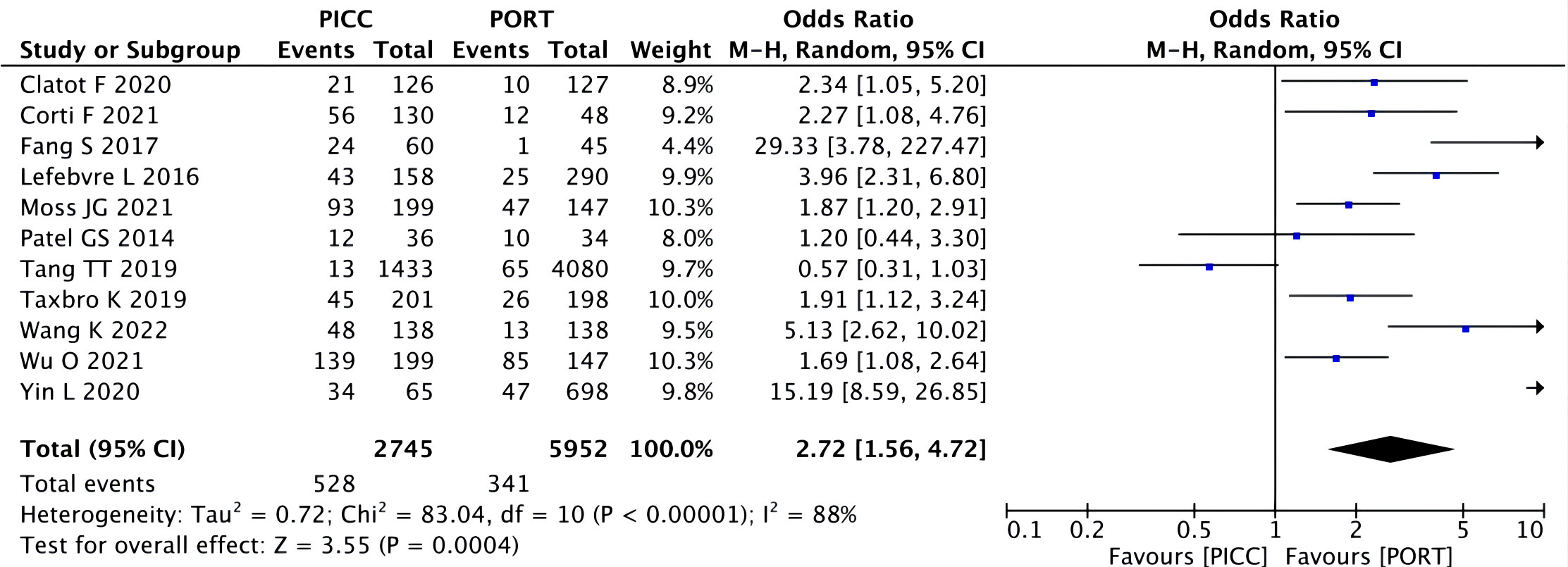
Figure 3 Pooled analysis of overall adverse effects comparing PICC with PORT.
3.2.2 Complications by access type
3.2.2.1 Catheter-related and deep vein thrombosis
A fixed-effects model was used to pool the thrombosis data because heterogeneity across the included studies was low. The pooled data showed the catheter-related thrombosis to be more frequent in patients with a PICC (OR=2.84, 95% CI=1.97–4.11, P<0.00001) (Figure 4), while the rate of the DVT did not reach a statistically significant level (OR=2.00, 95% CI=0.86–4.65, P=0.11) (Figure 5).
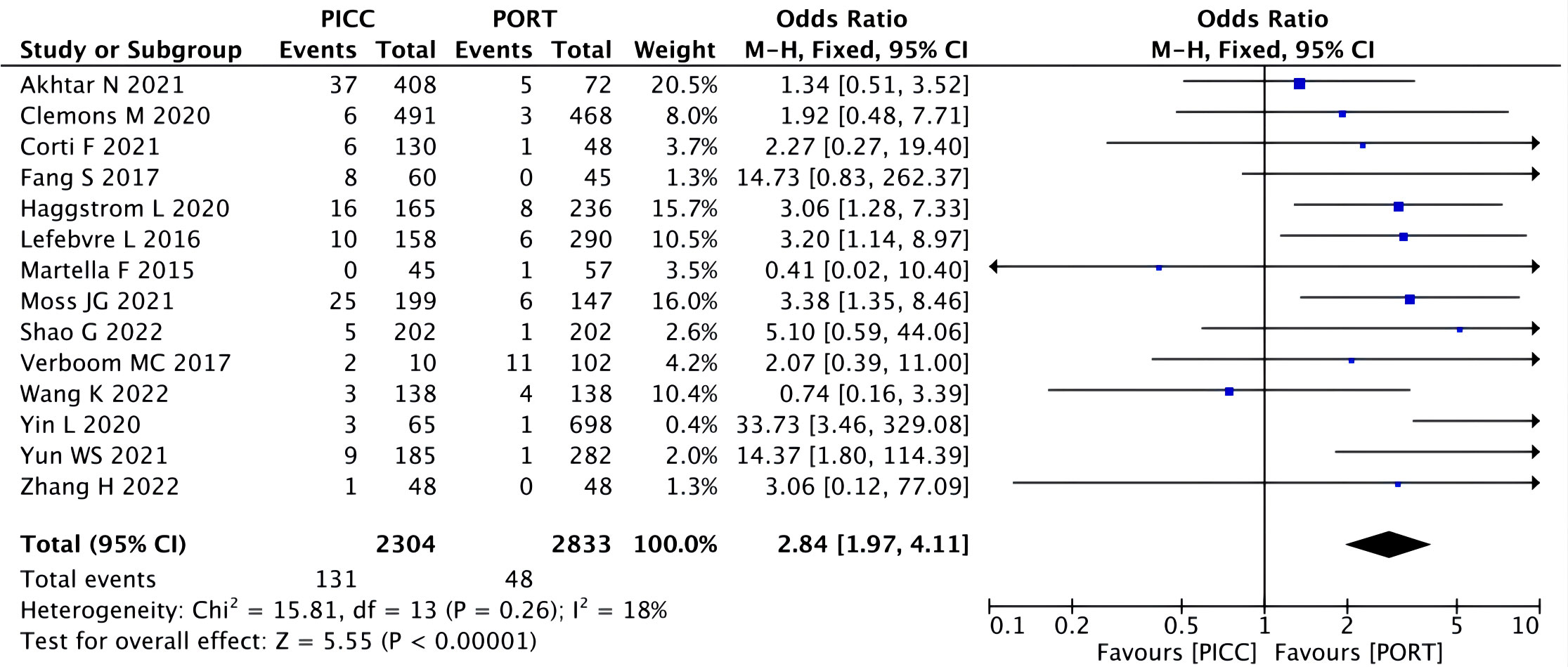
Figure 4 Pooled analysis of catheter-related thrombosis comparing PICC with PORT.
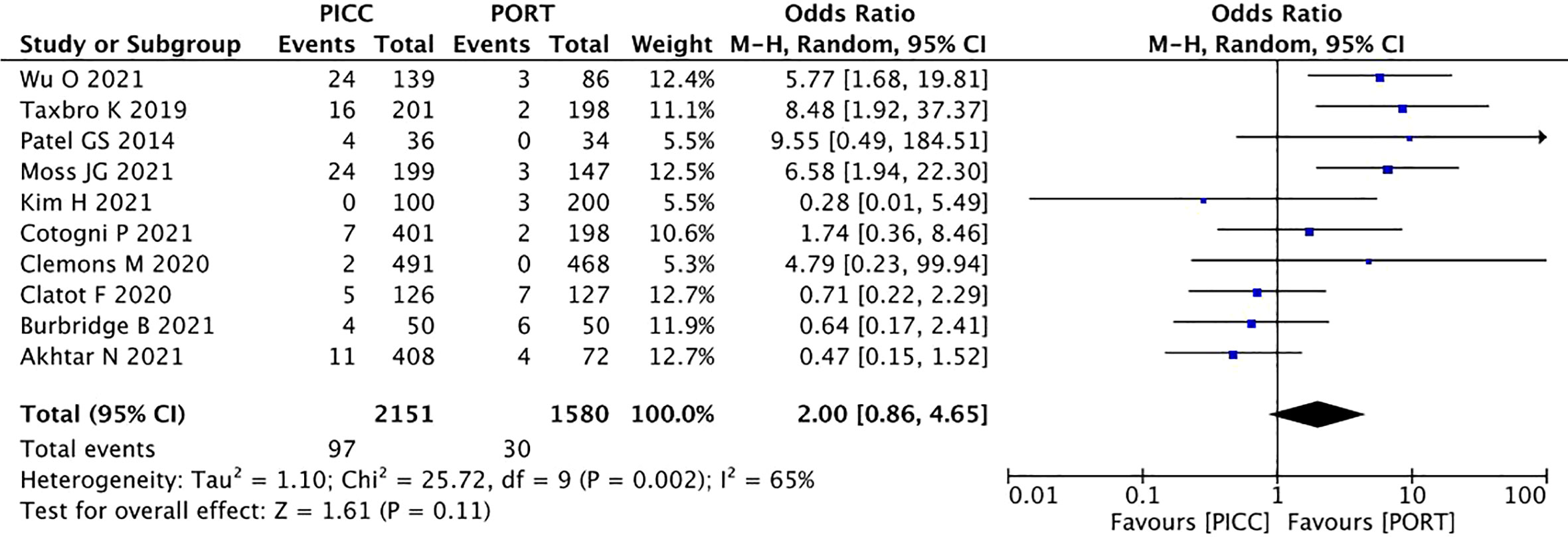
Figure 5 Pooled analysis of DVT comparing PICC with PORT.
3.2.2.2 Allergic reaction
A significant heterogeneity was noted among the three studies (I2 =53%, P=0.06). The pooling allergic reaction data showed statistical significance in the PICC group (OR=6.26, 95% CI=1.86–21.09, P=0.003). Thus, the PICC regimen was associated with a higher rate of allergic reactions (Figure 6).
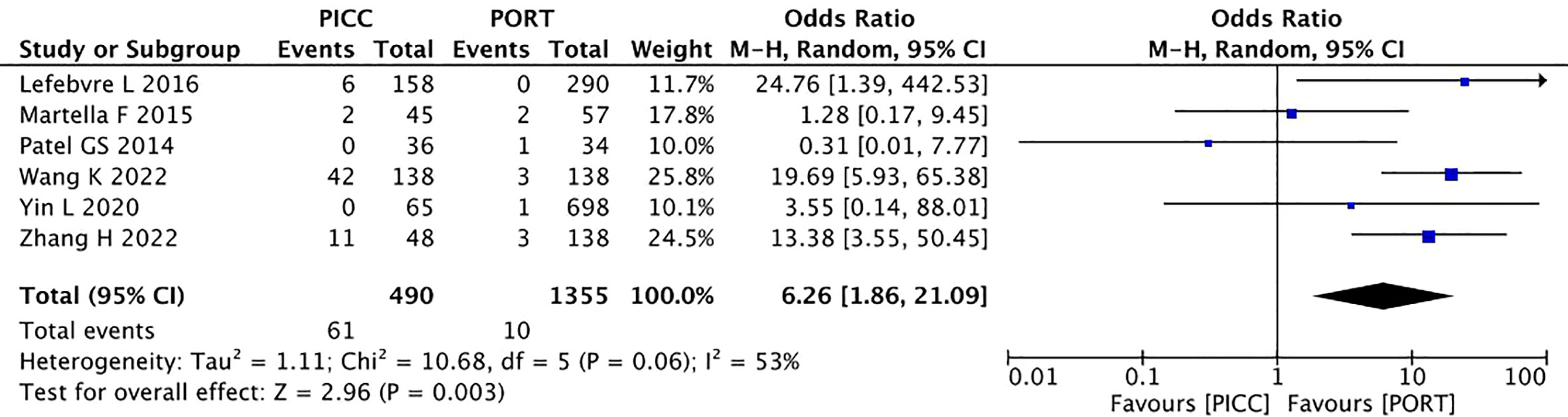
Figure 6 Pooled analysis of allergic reaction comparing PICC with PORT.
3.2.2.3 Infection
In terms of infection, a random-effects model was used, causing low heterogeneity across the included studies (I2 =78%, P<0.00001). The pooled result showed that PICC was non-inferior to the PORT group (OR=1.55, 95% CI=0.75–3.22, P=0.24) (Figure 7).
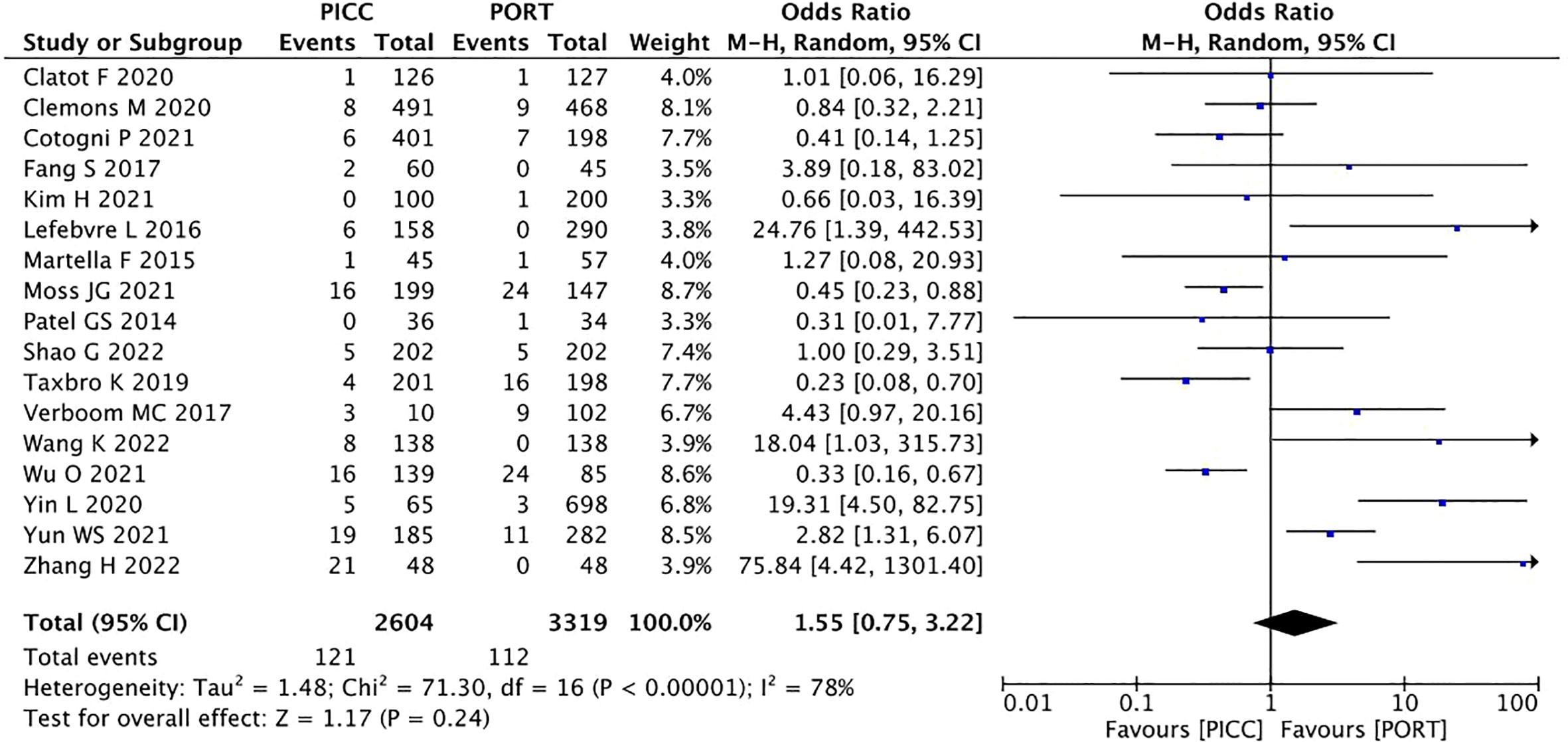
Figure 7 Pooled analysis of infection comparing PICC with PORT.
3.2.3 Publication bias
Forest plots were used to present publication bias. Figure 8 shows funnel plots of the overall adverse effects (A), catheter-related thrombosis (B), deep vein thrombosis (C), allergic reaction (D), and infection (E).
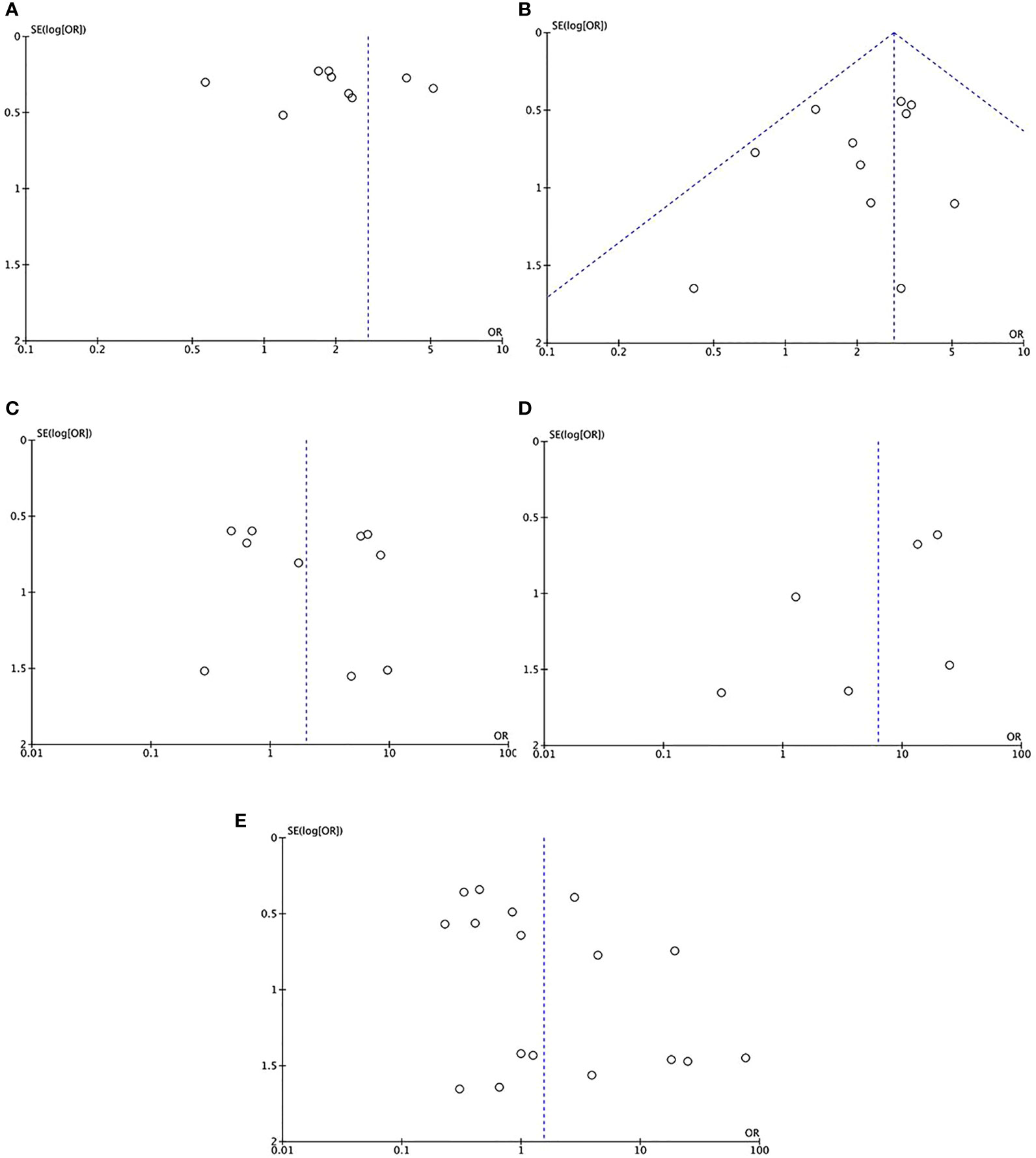
Figure 8 The funnel plots of the overall adverse effects (A), catheter-related thrombosis (B), deep vein thrombosis (C), allergic reaction (D), and infection (E).
4 Discussion
Despite an important management decision in clinical practice, little is known regarding the benefits and relative risks of the various methods of venous access in patients with cancer receiving chemotherapy. CVCs are associated with a high budgetary impact on cancer patients and place patients at risk of complications associated with catheters that could differ between PICCs and PORTs (19).
Today is an era that focuses on safety and raising cost awareness. Owing to the limited cost evidence, our meta-analysis only compared the complication rates of port catheters and PICC. The results indicated that PICCs were associated with a higher risk of catheter-related complications than PORTs, revealing that PICCs are an independent risk factor for device-related complications.
Consistent with previous studies (4, 5, 37), a higher rate of thrombosis and allergic reactions with PICC than with PORT was found in our study. Thrombosis was the most common complication. The pathogenesis of CR thrombosis is multifactorial and involves several risk factors (38, 39). Vascular injury, blood stasis, hypercoagulability related to cancer, and the catheter itself are considered classic contributors (Virchow’s triad) to venous thrombosis. Compared with PORT, PICCs are inserted into smaller-diameter veins and longer catheters. Therefore, this increased contact between the PICC and the vascular wall leads to vascular endothelium damage and blood flow reduction (17). However, the deep vein thrombosis did not reach statistical significance. Some elements, such as the study location and type of PICC-inserting provider, have been reported to be associated with the risk of vein thrombosis. A meta-analysis by Wang et al. (8) reported that PICC increased the risk of vein thrombosis compared with PORT in non-Asian countries, and no significant difference was observed in Asian countries. In addition, differences in the type of PICC-inserting provider and pooled results may affect the risk of vein thrombosis between the two groups. Considering the limitations of the included studies, limited data could not be obtained to explore the subtype elements affecting the interpretation of the results. Further investigation of vein thrombosis based on specific subtypes may help in making informed treatment decisions while maintaining a manageable safety profile.
With regard to the incidence of infection, the pooled results showed that PICC was non-inferior to PORT. To the best of our knowledge, this result may have been an underestimate. The extremities of a PICC remain outside the body and can increase the risk of bacterial infection on the outer edge of the catheter compared with implantable ports. Weekly maintenance inhibits cutaneous infectious side effects at the insertion site, whereas repeated handling and flushing may be associated with bacteremia (17). Some studies have shown that all nurses received relevant education in maintenance of PICC, and professional nurses and nurse education in aftercare led to a decrease in the rate of PICC complications in their clinical work (40).
Pool analysis uses a well-maintained and updated database. However, the retrospective nature of all the included studies may have influenced the comparison of catheter-related outcomes. Additionally, publication bias led to heterogeneity among the included studies. All studies in our meta-analysis used a wide range of malignancies and variations in specific methods of catheterization, catheter material, and catheter maintenance methods. Moreover, our study did not evaluate the cost efficiency between the two groups. Cost effectiveness should also be considered when adopting central access devices for patients with cancer.
5 Conclusion
This study found that patients with PICC had a higher rate of overall adverse events than those with PORT. The results provide practitioners with a better knowledge of adverse events between the two CVCs and will be of assistance when choosing an appropriate CVC for the administration of chemotherapy for cancer patients. When making clinical decisions, the safety of venous access and optimal patient satisfaction must be prioritized.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Author contributions
YL and AW contributed to study design. LL and WL conducted the literature search, acquired the data and performed data analysis. LL wrote the article. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Pu YL, Li ZS, Zhi XX, Shi YA, Meng AF, Cheng F, et al. Complications and costs of peripherally inserted central venous catheters compared with implantable port catheters for cancer patients: a meta-analysis. Cancer Nurs (2020) 43(6):455–67. doi: 10.1097/NCC.0000000000000742
2. Kelly L. A practical guide to safe PICC placement. Br J Nurs (2013) 22(8):S13–4, S16, S18-9. doi: 10.12968/bjon.2013.22.Sup5.S13
3. Liu Y, Gao Y, Wei L, Chen W, Ma X, Song L. Peripherally inserted central catheter thrombosis incidence and risk factors in cancer patients: a double-center prospective investigation. Ther Clin Risk Manag (2015) 11:153–60. doi: 10.2147/TCRM.S73379
4. Johansson E, Hammarskjöld F, Lundberg D, Heibert Arnlind M. A survey of the current use of peripherally inserted central venous catheter (PICC) in Swedish oncology departments. Acta Oncol (2013) 52(6):1241–2. doi: 10.3109/0284186X.2013.806820
5. Chopra V, Anand S, Hickner A, Buist M, Rogers MA, Saint S, et al. Risk of venous thromboembolism associated with peripherally inserted central catheters: a systematic review and meta-analysis. Lancet (2013) 382(9889):311–25. doi: 10.1016/S0140-6736(13)60592-9
6. Saber W, Moua T, Williams EC, Verso M, Agnelli G, Couban S, et al. Risk factors for catheter-related thrombosis (CRT) in cancer patients: a patient-level data (IPD) meta-analysis of clinical trials and prospective studies. J Thromb Haemost (2011) 9(2):312–9. doi: 10.1111/j.1538-7836.2010.04126.x
7. Cheong K, Perry D, Karapetis C, Koczwara B. High rate of complications associated with peripherally inserted central venous catheters in patients with solid tumours. Intern Med J (2004) 34(5):234–8. doi: 10.1111/j.1444-0903.2004.00447.x
8. Wang P, Soh KL, Ying Y, Liu Y, Huang X, Huang J. Risk of VTE associated with PORTs and PICCs in cancer patients: a systematic review and meta-analysis. Thromb Res (2022) 213:34–42. doi: 10.1016/j.thromres
9. Liu B, Wu Z, Lin C, Li L, Kuang X. Applicability of TIVAP versus PICC in non-hematological malignancies patients: a meta-analysis and systematic review. PloS One (2021) 16(8):e0255473. doi: 10.1371/journal.pone.0255473
10. Capozzi VA, Monfardini L, Sozzi G, Armano G, Butera D, Scarpelli E, et al. Peripherally inserted central venous catheters (PICC) versus totally implantable venous access device (PORT) for chemotherapy administration: a meta-analysis on gynecological cancer patients. Acta BioMed (2021) 92(5):e2021257. doi: 10.23750/abm.v92i5.11844
11. Cook DA, Reed DA. Appraising the quality of medical education research methods: the medical education research study quality instrument and the Newcastle-Ottawa scale-education. Acad Med (2015) 90(8):1067–76. doi: 10.1097/ACM.0000000000000786
12. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. Cochrane bias methods group; cochrane statistical methods group. the cochrane collaboration's tool for assessing risk of bias in randomised trials. BMJ (2011) 343:d5928. doi: 10.1136/bmj.d5928
13. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med (2002) 21(11):1539–58. doi: 10.1002/sim.1186
14. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ (2003) 327(7414):557–60. doi: 10.1136/bmj.327.7414.557
15. Martella F, Salutari V, Marchetti C, Pisano C, Di Napoli M, Pietta F, et al. A retrospective analysis of trabectedin infusion by peripherally inserted central venous catheters: a multicentric Italian experience. Anticancer Drugs (2015) 26(9):990–4. doi: 10.1097/CAD.0000000000000275
16. Taxbro K, Hammarskjöld F, Thelin B, Lewin F, Hagman H, Hanberger H, et al. Clinical impact of peripherally inserted central catheters vs implanted port catheters in patients with cancer: an open-label, randomised, two-centre trial. Br J Anaesth (2019) 122(6):734–41. doi: 10.1016/j.bja.2019.01.038
17. Lefebvre L, Noyon E, Georgescu D, Proust V, Alexandru C, Leheurteur M, et al. Port catheter versus peripherally inserted central catheter for postoperative chemotherapy in early breast cancer: a retrospective analysis of 448 patients. Support Care Cancer (2016) 24(3):1397–403. doi: 10.1007/s00520-015-2901-8
18. Clemons M, Stober C, Kehoe A, Bedard D, MacDonald F, Brunet MC, et al. A randomized trial comparing vascular access strategies for patients receiving chemotherapy with trastuzumab for early-stage breast cancer. Support Care Cancer (2020) 28(10):4891–9. doi: 10.1007/s00520-020-05326-y
19. Patel GS, Jain K, Kumar R, Strickland AH, Pellegrini L, Slavotinek J, et al. Comparison of peripherally inserted central venous catheters (PICC) versus subcutaneously implanted port-chamber catheters by complication and cost for patients receiving chemotherapy for non-haematological malignancies. Support Care Cancer (2014) 22(1):121–8. doi: 10.1007/s00520-013-1941-1
20. Fang S, Yang J, Song L, Jiang Y, Liu Y. Comparison of three types of central venous catheters in patients with malignant tumor receiving chemotherapy. Patient Prefer Adherence (2017) 11:1197–204. doi: 10.2147/PPA.S142556
21. Clatot F, Fontanilles M, Lefebvre L, Lequesne J, Veyret C, Alexandru C, et al. Randomised phase II trial evaluating the safety of peripherally inserted catheters versus implanted port catheters during adjuvant chemotherapy in patients with early breast cancer. Eur J Cancer (2020) 126:116–24. doi: 10.1016/j.ejca.2019.11.022
22. Yun WS, Yang SS. Comparison of peripherally inserted central catheters and totally implanted venous access devices as chemotherapy delivery routes in oncology patients: a retrospective cohort study. Sci Prog (2021) 104(2):1–12. doi: 10.1177/00368504211011871. 368504211011871.
23. Tang TT, Liu L, Li CX, Li YT, Zhou T, Li HP, et al. Which is better for patients with breast cancer: totally implanted vascular access devices (TIVAD) or peripherally inserted central catheter (PICC)? World J Surg (2019) 43(9):2245–9. doi: 10.1007/s00268-019-05022-x
24. Moss JG, Wu O, Bodenham AR, Agarwal R, Menne TF, Jones BL, et al. CAVA trial group. central venous access devices for the delivery of systemic anticancer therapy (CAVA): a randomised controlled trial. Lancet (2021) 398(10298):403–15. doi: 10.1016/S0140-6736(21)00766-2
25. Wang K, Zhou Y, Huang N, Lu Z, Zhang X. Peripherally inserted central catheter versus totally implanted venous port for delivering medium- to long-term chemotherapy: a cost-effectiveness analysis based on propensity score matching. J Vasc Access (2022) 23(3):365–74. doi: 10.1177/1129729821991360
26. Shao G, Zhou X, Zhang S, Wu S, Dong Y, Dong Z. Cost-utility analysis of centrally inserted totally implanted access port (PORT) vs. peripherally inserted central catheter (PICC) in the oncology chemotherapy. Front Public Health (2022) 10:942175. doi: 10.3389/fpubh.2022.942175
27. Akhtar N, Lee L. Utilization and complications of central venous access devices in oncology patients. Curr Oncol (2021) 28(1):367–77. doi: 10.3390/curroncol28010039
28. Zhang H, Li Y, Zhu N, Li Y, Fu J, Liu J. Comparison of peripherally inserted central catheters (PICCs) versus totally implantable venous-access ports in pediatric oncology patients, a single center study. Sci Rep (2022) 12(1):3510. doi: 10.1038/s41598-022-07584-8
29. Corti F, Brambilla M, Manglaviti S, Di Vico L, Pisanu MN, Facchinetti C, et al. Comparison of outcomes of central venous catheters in patients with solid and hematologic neoplasms: an Italian real-world analysis. Tumori (2021) 107(1):17–25. doi: 10.1177/0300891620931172
30. Haggstrom L, Parmar G, Brungs D. Central venous catheter thrombosis in cancer: a multi-centre retrospective study investigating risk factors and contemporary trends in management. Clin Med Insights Oncol (2020) 14:1179554920953097. doi: 10.1177/1179554920953097
31. Yin L, Li J. Central venous catheter insertion in colorectal cancer patients, PICC or PC? Cancer Manag Res (2020) 12:5813–8. doi: 10.2147/CMAR.S250410
32. Cotogni P, Mussa B, Degiorgis C, De Francesco A, Pittiruti M. Comparative complication rates of 854 central venous access devices for home parenteral nutrition in cancer patients: a prospective study of over 169,000 catheter-days. JPEN J Parenter Enteral Nutr (2021) 45(4):768–76. doi: 10.1002/jpen.1939
33. Burbridge B, Lim H, Dwernychuk L, Le H, Asif T, Sami A, et al. Comparison of the quality of life of patients with breast or colon cancer with an arm vein port (TIVAD) versus a peripherally inserted central catheter (PICC). Curr Oncol (2021) 28(2):1495–506. doi: 10.3390/curroncol28020141
34. Kim H, Kwon S, Son SM, Jeong E, Kim JY. Tailored approach to the choice of long-term vascular access in breast cancer patients. PloS One (2021) 16(7):e0255004. doi: 10.1371/journal.pone.0255004
35. Wu O, McCartney E, Heggie R, Germeni E, Paul J, Soulis E, et al. Venous access devices for the delivery of long-term chemotherapy: the CAVA three-arm RCT. Health Technol Assess (2021) 25(47):1–126. doi: 10.3310/hta25470
36. Verboom MC, Ouwerkerk J, Steeghs N, Lutjeboer J, Martijn Kerst J, van der Graaf WTA, et al. Central venous access related adverse events after trabectedin infusions in soft tissue sarcoma patients; experience and management in a nationwide multi-center study. Clin Sarcoma Res (2017) 7:2. doi: 10.1186/s13569-017-0066-6
37. Pikwer A, Åkeson J, Lindgren S. Complications associated with peripheral or central routes for central venous cannulation. Anaesthesia (2012) 67(1):65–71. doi: 10.1111/j.1365-2044.2011.06911.x
38. Geerts W. Central venous catheter-related thrombosis. Hematol Am Soc Hematol Educ Program (2014) 2014(1):306–11. doi: 10.1182/asheducation-2014.1.306
39. Chopra V, Kaatz S, Conlon A, Paje D, Grant PJ, Rogers MAM, et al. The Michigan risk score to predict peripherally inserted central catheter-associated thrombosis. J Thromb Haemost (2017) 15(10):1951–62. doi: 10.1111/jth.13794
Keywords: PICC, PORT, cancer, central venous access, meta-analysis
Citation: Lin L, Li W, Chen C, Wei A and Liu Y (2023) Peripherally inserted central catheters versus implantable port catheters for cancer patients: a meta-analysis. Front. Oncol. 13:1228092. doi: 10.3389/fonc.2023.1228092
Received: 07 June 2023; Accepted: 30 June 2023;
Published: 14 July 2023.
Edited by:
Luigi Marano, University of Siena, ItalyReviewed by:
Apurva Patel, Gujarat Cancer & Research Institute, IndiaGianmario Edoardo Poto, University of Siena, Italy
Copyright © 2023 Lin, Li, Chen, Wei and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anhua Wei, YWh3ZWkwNzE2QDE2My5jb20=; Yu Liu, MTM4NzEzODIzMjZAMTI2LmNvbQ==
†These authors have contributed equally to this work