 António Moreira Monteiro
António Moreira Monteiro Diogo Alpuim Costa
Diogo Alpuim Costa Virgínia Mareco
Virgínia Mareco Carla Espiney Amaro
Carla Espiney Amaro- 1Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal
- 2NOVA Medical School, Faculdade de Ciências Médicas, Lisbon, Portugal
- 3Centro de Medicina Subaquática e Hiperbárica (CMSH), Armed Forces Hospital, Lisbon, Portugal
- 4Medical Oncology Department, Hospital de Cascais Dr. José de Almeida, Alcabideche, Portugal
- 5Hematology and Oncology Department, CUF Oncologia, Lisbon, Portugal
- 6Radiotherapy Department, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa Norte, Lisbon, Portugal
Introduction: Despite modern radiotherapy (RT) techniques, radiation-induced proctitis (RIP) remains a significant complication of RT for pelvic organ malignancies. Over the last decades, an enormous therapeutic armamentarium has been considered in RIP, including hyperbaric oxygen therapy (HBOT). However, the evidence regarding the impact of HBOT on RIP is conflicting. This study aims to evaluate the effectiveness and safety of HBOT in the treatment of RIP.
Methods: Ten-year (2013-2023) retrospective analysis of all consecutive patients with RIP treated with HBOT at Centro de Medicina Subaquática e Hiperbárica (CMSH) (Armed Forces Hospital – Lisbon, Portugal). Patients were exposed to 100% oxygen at 2.5 ATA, in a multiplace first-class hyperbaric chamber, for 70-min periods, once daily, five times per week. Fisher’s exact test was performed using SPSS (version 23.0); p<0.05 was accepted as statistically significant.
Results: Of a total of 151 patients with RIP, 88 were included in the final analysis, of whom 38.6% evidenced other concurrent radiation-induced soft tissue lesions. The most reported primary pelvic tumor treated with RT was prostate cancer (77.3%), followed by cervical cancer (10.2%). Hematochezia was the most observed clinical manifestation (86.4%). After a median of 60 HBOT sessions (interquartile range [IQR]: 40-87.5), 62.5% and 31.8% of patients achieved a clinical complete and partial response, respectively, with a hematochezia resolution rate of 93.7% (complete or partial). While partial and complete responses require fewer than 70 sessions of HBOT in terms of overall RIP symptoms (p=0.069), isolated hematochezia tends to require at least 70 sessions (p=0.075). Individuals with at least two concurrent late radiation tissue injuries were associated with a complete response to HBOT (p=0.029). Only about 5.7% of patients did not respond to the treatment. Eighteen patients (20.5%) developed reversible ear barotrauma. The number of HBOT sessions was a predictor of HBOT side effects (odds ratio: 1.010; 95% confidence interval, 1.000-1.020; p=0.047).
Conclusion: The HBOT proved to be an effective and safe treatment for RIP refractory to medical and/or endoscopic treatments. This real-world evidence study adds value to published data on the management of RIP with HBOT.
1 Introduction
Cancer is a foremost cause of global morbidity and mortality (1–4). The International Agency for Research on Cancer predicts a 47% rise in the global cancer burden in 2040 compared to 2020, expecting 28.4 million cancer cases (5). Pelvic organ cancer designates any malignant tumor primarily originating in any pelvic cavity organ (6, 7). Despite the therapeutic avenue innovation, radiotherapy (RT) remains one of the cornerstones for managing malignant tumors, with 50% of patients receiving RT during their course of illness (8–10). Introducing new RT techniques (e.g., three-dimensional conformal radiation therapy and intensity-modulated radiation therapy), it has been possible to eradicate malignant tumor cells with minimal exposure to surrounding tissues (11–13). However, these modern RT approaches are not exempted from side effects, late radiation-induced proctitis (RIP) being one of them (9, 14).
The RIP is defined as an iatrogenic lesion of the mucosa and submucosa of the rectum or rectosigmoid transition following RT for pelvic cancer (8, 10). It can be classified into acute or chronic RIP, considering the time from the end of RT protocol to the onset of RT-related clinical signs and symptoms (8, 15). The incidence rate is estimated from 2 to 39% (16). Proctitis starts with an initial mucosal injury induced by ionizing radiation, and the organism reacts through a chronic inflammatory response leading to fibrosis, obliterative endarteritis, tissue hypoxia and ischemia, and neoangiogenesis (17, 18). Gut microbiota and oxidative stress may also be important in chronic radiation enteritis and colitis (19–21). Different clinical manifestations may develop, including proctalgia, diarrhea, constipation, recurrent ileus, mucus discharge, hematochezia, ulceration/fistulae formation, fecal incontinence/urgency, or a predisposition to a malabsorption syndrome. Patients may also experience other symptoms, such as urinary frequency, dysuria, pelvic pain or discomfort, urinary retention, and hematuria (due to synchronous radiation cystitis [RC]) (22). After a meticulous anamnesis, the clinical diagnostic hypothesis should be confirmed by performing (procto)sigmoidoscopy. Endoscopic images usually reveal an edematous, hyperemic friable mucosa with telangiectasias and possibly areas of ulceration or sloughing (8, 14, 23, 24). Three major therapeutic approaches can be used in RIP – medical, endoscopic, and surgical – and there is no gold standard treatment regimen (8). Among pharmacological regimens, formalin application (4-10%) has been demonstrated to be an effective medical treatment (8, 23, 25–28), as well as sucralfate enemas (6, 23, 29), and metronidazole combined with ciprofloxacin (20, 29). Argon plasma coagulation (APC) is the first-line endoscopic strategy for individuals with hemorrhagic RIP (24, 29–31). Surgery is generally reserved for advanced stages of RIP refractory to optimal medical and endoscopic therapies (8, 30).
Hyperbaric oxygen therapy (HBOT) is another effective and safe intervention for managing RIP (24). It is characterized by inhaling pure oxygen (FiO2 100%) inside a hyperbaric chamber frequently pressurized at 2.0 to 2.8 atmospheres absolute (ATA) for 60 to 120 minutes daily (8, 32, 33). This treatment leads to a series of physiological effects due to increased plasma oxygen concentration and delivery to tissues, contributing to better tissue oxygenation, enhancing microvascularization, and promoting angiogenesis. It also exerts a tumor sensitization effect on RT (34). It might be associated with mild and transient side effects due to pressure and oxygen toxicity, mostly middle ear barotrauma (MEB) (35, 36).
Currently, HBOT represents a primary and complementary standard treatment in several clinical scenarios, including late radiation tissue injuries (LRTIs), namely RIP and RC (type 1 recommendation, level B evidence) (36, 37). However, clinical evidence is still scarce. This retrospective study pretends to evaluate the effectiveness of the HBOT in treating RIP. Secondary objectives include assessing the hematochezia resolution rate; estimation of hematochezia recurrence; evaluation of endoscopic improvement; the correlation between response rates and the number of HBOT sessions; and finally, the evaluation of the HBOT safety level.
2 Materials and methods
2.1 Patients
This retrospective observational single-center study aims to evaluate the effectiveness of HBOT in a group of patients with late RIP treated within the past ten years (from January 2013 to March 2023) at Centro de Medicina Subaquática e Hiperbárica (CMSH), part of the Armed Forces Hospital (Lisbon, Portugal). Figure 1 shows the flowchart of this study. After a preliminary screening, 88 patients were selected according to our inclusion and exclusion criteria and were further analyzed in this study.
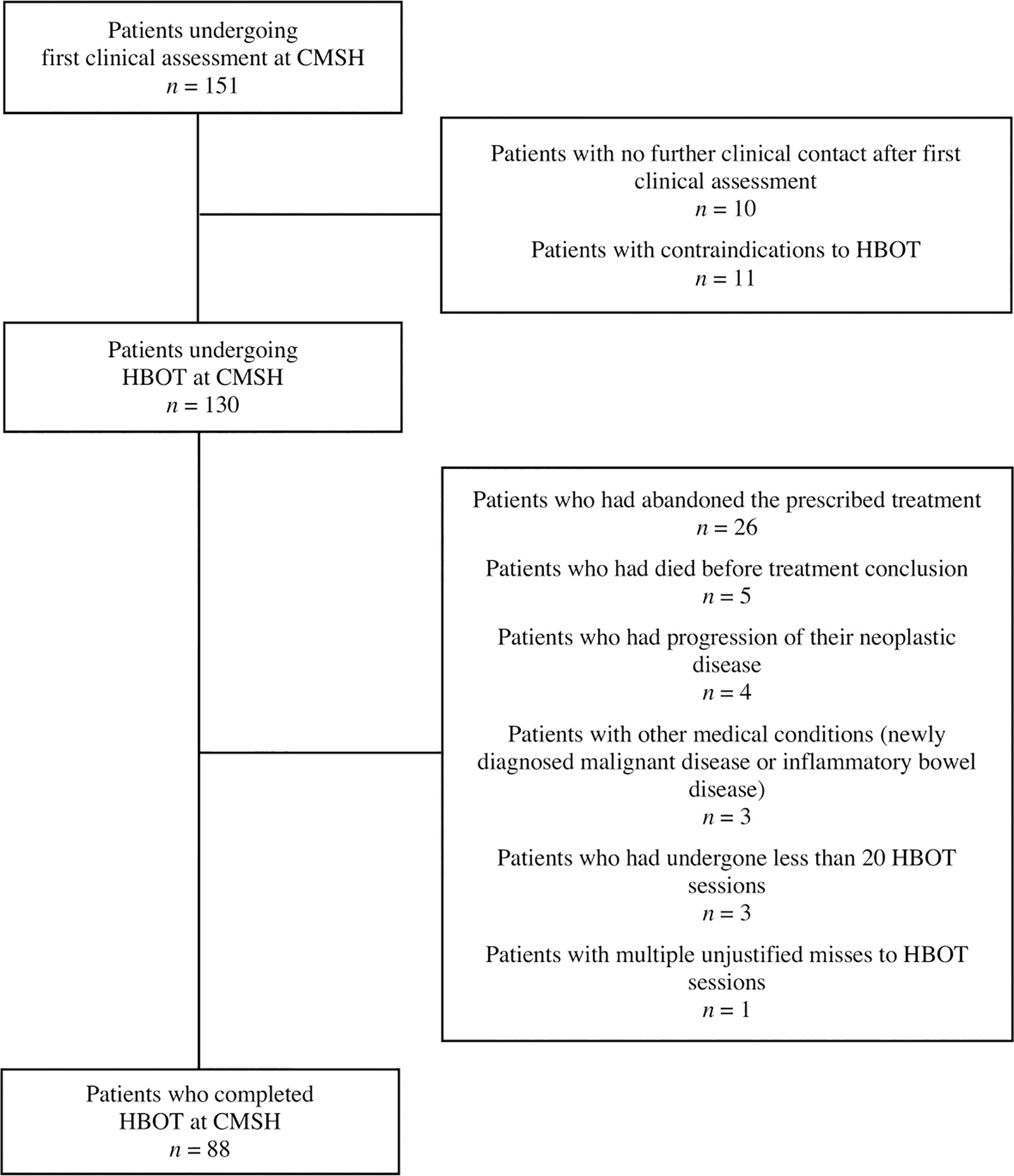
Figure 1 Flowchart exhibiting individuals eligible for this study and all excluded patients. After a preliminary screening, 88 patients were selected according to our inclusion and exclusion criteria and were further analyzed in this study. CMSH, Centro de Medicina Subaquática e Hiperbárica; HBOT, hyperbaric oxygen therapy.
This patient subgroup comprises individuals aged at least 18 years of age who have undergone RT as a curative treatment for pelvic cancer, considering multiple primary pelvic malignancies (e.g., colorectal, prostate, cervical, and uterine). The enrolled patients presented with clinical and/or radiological and/or histological evidence of RIP, including chronic diarrhea/constipation, abdominal cramp, proctalgia, lower gastrointestinal (GI) bleeding/hematochezia, obstruction, tenesmus, fecal urgency/incontinence, proliferative mucosal telangiectasias, ulceration, or development of fistulae. Patients with concurrent clinical manifestations resulting from other LRTIs (e.g., [entero]colitis, RC, and urethritis) were also included. Patients eligible for the study had a previous endoscopic examination with a diagnosis of rectal lesion. Also, eligible patients have failed at least one previous conservative treatment (pharmacological or endoscopic). Exclusion criteria included a number of HBOT sessions inferior to 20; patients who have refused/abandoned the post-HBOT follow-up period; patients with medical conditions that may justify a similar clinical presentation as LRTIs (e.g., inflammatory bowel disease, colorectal cancer); and patients with contraindications for HBOT (e.g., uncontrolled epilepsy, pneumothorax, severe claustrophobia, a recent episode of barotrauma).
To evaluate the effectiveness of HBOT, we establish the complete, partial, and overall response rates, as well as the non-response rate. The total resolution of symptoms defines a complete response; a partial response is characterized by a reduction of frequency and/or severity of symptoms; and non-response means the maintenance of symptoms as presented at the time of diagnosis or even its aggravation. Patients were considered improved in their RIP-related symptomatology if they have demonstrated a complete or partial response to HBOT. Our analysis also assessed the percentage of patients who had developed HBOT side effects and compliance with the proposed treatment protocol.
The Armed Forces Hospital ethics committee approved this study. Due to its retrospective nature and the fact that the clinical data could not identify the enrolled patients, informed consent was not required. Nevertheless, all clinical data were analyzed under confidentiality for the sole purpose of this study.
2.2 Treatment protocol
The HBOT was performed at CMSH, part of the Armed Forces Hospital (Lisbon, Portugal). Patients were treated inside a multiplace first class hyperbaric chamber, where they were breathing 100% oxygen administered at 2.5 ATA, for 70-min periods (total duration of 100-min, considering descending, a 5-minute air-break, and ascending), once daily, 5 times a week, as shown in Figure 2. After the conclusion of an initial treatment course of 20 sessions, patients were evaluated to assess if there was an improvement in clinical signs and symptoms. The treatment ended if patients were revealed to be asymptomatic (mostly considering hematochezia). On the other hand, if patients remained symptomatic, the treatment protocol’s total duration might be extended to several weeks until a clinical and/or endoscopic best clinical response was obtained. Once treatment was concluded, patients were re-evaluated and referred to the attending physician, who had initially reported the case to our center and was responsible for the patient’s follow-up. In case of recurrence of symptoms, the patient had to be referred again to our center for further evaluation.
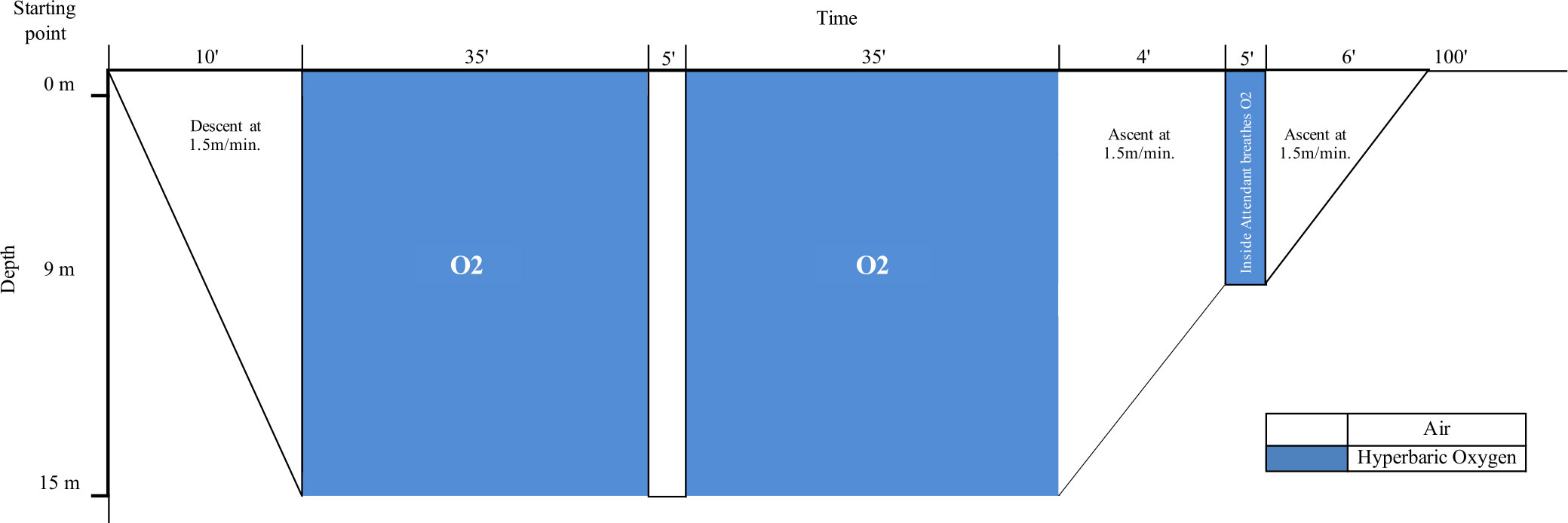
Figure 2 Treatment protocol for RIP at Centro de Medicina Subaquática e Hiperbárica (CMSH). Patients were treated inside a multiplace first class hyperbaric chamber, where they breathed 100% oxygen administered at 2.5 ATA, for 70-min periods (total duration of 100-min, considering descending, a 5-minute air-break, and ascending), once daily, 5 times a week. ATA, atmospheres absolute; RIP, radiation-induced proctitis.
Patients were submitted to a prior clinical evaluation to assess their eligibility to initiate the treatment protocol, ruling out significant contraindications to HBOT. Before the initiation of HBOT, it was also mandatory to perform: a chest radiologic examination (to exclude pneumothorax, pulmonary blebs or bullae, or other relevant pulmonary diseases), a standard 12-lead electrocardiogram (to exclude major cardiac pathology), and a tympanogram (to exclude Eustachian tube dysfunction). Those individuals also received indications from the nursing team about the precautions to take prior to and after each treatment session to avoid complications.
2.3 Data collection
All clinical data were retrospectively collected and analyzed by revisiting the patients’ medical records archived at CMSH installations. The accessed clinical data include the type, time of diagnosis, and corresponding treatment of the pelvic organ cancer; clinical manifestations, time of diagnosis, and previous treatments of RIP and other synchronous LRTIs; and all the relevant data related to the response and compliance to HBOT.
2.4 Statistical analysis
The data analysis was performed in Microsoft Excel and Statistical Package for the Social Sciences (IBM® SPSS® Statistics 23.0) software.
In addition to descriptive statistics, Chi-square or Fisher exact tests were used to compare categorical data; the Mann-Whitney U or Kruskal-Wallis tests to compare continuous/ordinal data between two or more groups of a nominal independent variable, respectively; the Spearman’s correlation analysis to relate continuous/ordinal data to each other; and logistic regression to predict binary or multinomial outcomes given a set of independent continuous/ordinal variables. Normal distribution for all continuous variables was tested using the Kolmogorov-Smirnov test. A p-value <0.05 was considered to indicate statistical significance (two-tailed).
3 Results
3.1 Sample characterization
A total of 151 patients with RIP were referred to CMSH to be treated with HBOT. Twenty-one of them did not start the treatment because there was no further clinical contact after the first clinical assessment (n=10) or because the HBOT was contraindicated due to active neoplastic disease (n=6), major cardiac pathology (n=2), a recent episode of barotrauma/pathologic tympanogram (n=1), pulmonary blebs (n=1), or relevant cognitive impairment conditioning the compliance to HBOT (n=1). Additionally, 42 patients were excluded after HBOT initiation. This subgroup comprised patients who had abandoned the prescribed treatment/failed additional HBOT prescribed sessions (n=26); patients who had died before treatment conclusion (n=5); patients who had documented progression of their neoplastic disease (n=4); patients with other medical conditions that were the actual cause of GI bleeding (e.g., newly diagnosed malignant disease [n=2] and inflammatory bowel disease [n=1]); patients who had undergone less than 20 HBOT sessions (n=3); and a patient who had multiple unjustified misses to HBOT sessions (n=1).
Thus, after excluding 63 patients, this retrospective study analyzed 88 patients undergoing complete treatment with HBOT for RIP from January 2013 to March 2023, as shown in Figure 1.
Considering the population evaluated in this study, 83% of them were male patients (n=73) and 17% female patients (n=15), with a median age of 69.5 (interquartile range [IQR]: 64-75). The primary tumor most frequently reported justifying the need for RT was prostate cancer in 77.3% (n=68), and the second most frequent malignancy was cervix uteri cancer, with 10.2% incidence (n=9). Also, 78.4% of patients had undergone external beam radiation therapy (n=69), 10.2% brachytherapy (n=9), and 11.4% both RT approaches (n=10). Nevertheless, 52.3% had at least performed another oncological treatment, namely surgery, androgen deprivation therapy, and chemotherapy. Furthermore, 61.4% of patients had received the diagnosis of RIP with not having other synchronous LRTIs (n=54). The second most common diagnosis combined RIP and RC, representing 30.7% of the analyzed population (n=27). Table 1 describes demographic and clinical data related to the primary tumor, type of RT, patient’s clinical presentation, and previous therapeutic approaches for RIP.
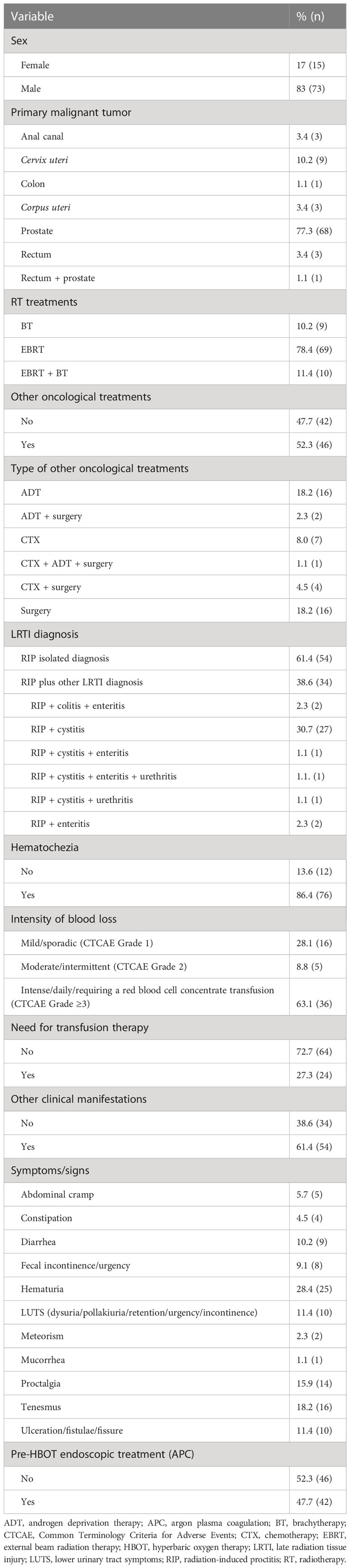
Table 1 Sample characterization, considering patient’s sex, type of primary malignant tumor, implemented oncological treatments, LRTI diagnosis (other than RIP), patient’s clinical presentation at our first clinical assessment, and previous therapeutic approaches for RIP.
3.2 Clinical presentation
The median time between the end of RT and RIP-related symptomatology initiation was 12 months (IQR: 7.25-24). Hematochezia represents the most common clinical manifestation of RIP in this group of patients, emerging in 86.4% of the patients (n=76). Among the 13.6% of individuals whose most preeminent clinical manifestation was not hematochezia (n=12), only 25% received the isolated diagnosis of RIP (n=3), presenting other nonspecific GI symptoms. Regarding the intensity of GI blood loss, 28.1% of patients developed mild/sporadic hematochezia (CTCAE Grade 1), 8.8% experienced moderate/intermittent hematochezia (CTCAE Grade 2), and 63.1% developed intense/daily hematochezia or severe anemia requiring transfusion support (CTCAE Grade ≥3). Considering the total number of patients, around 30% had required at least one red blood cell concentrate transfusion (n=24). About other clinical manifestations, the most frequently reported were hematuria in 28.4% of cases, tenesmus (18.2%), proctalgia (15.9%), and the development of ulceration/fistulae/fissure (11.4%).
It is also important to reinforce that most patients (91%) had documented a previous endoscopic examination confirming the RIP diagnosis (only 8 clinical records did not have registered any information concerning pre-HBOT endoscopic evaluation). All patients tried at least one last conservative treatment modality (pharmacological or endoscopic treatments) that was revealed to be ineffective. Almost half of the patients (47.7%) underwent at least one APC treatment session before starting HBOT. Although only 35 clinical registries confirmed the attempt to treat RIP with medical treatment at the beginning, some pharmacological treatment has been carried out as it is classically the first line treatment to be applied in the management of RIP.
3.3 Response to hyperbaric oxygen therapy
The median time between installing RIP-related symptomatology and initiating HBOT was 8 months (IQR: 3.25-14). Patients completed a median of 60 HBOT sessions (IQR: 40-87.5) during a median time of 5.82 months (IQR: 3.07-11.24). An overall response rate of 94.3% was revealed – 62.5% of patients had a complete clinical response with full resolution of symptoms, and 31.8% had a partial clinical response with a reduction of frequency or severity of symptoms (e.g., patients reported the occurrence of less frequency and quantity of GI blood loss to isolated episodes of hematochezia, with no hemodynamic repercussions). The registered hematochezia resolution rate was 93.7% (considering both complete and partial resolution). Individuals with at least two concomitant LRTIs (e.g., RIP and RC) were associated with a complete response to HBOT (p=0.029). Response to HBOT showed no differences according to gender, age, primary tumor, type of RT, whether other cancer treatments were performed or not, the initial symptoms, the time between the end of RT and the onset of symptoms, the time between symptoms and HBOT, and the need for blood transfusions or treatments prior to HBOT. Only about 5.7% of patients did not respond to the treatment, maintaining refractory hematochezia (6.3%) or the other initial symptoms. Also, 34.1% of patients performed a post-HBOT endoscopic evaluation, and 83.3% showed endoscopic improvement of RIP, as shown in Figure 3. The time between the end of RT and the onset of hematochezia was inversely associated with the number of HBOT sessions. Although, the relationship is weak because Spearman’s rho (ρ) correlation coefficient is between -0.20 and -0.29 (ρ: -0.259; p=0.036).

Figure 3 Pre- and post-HBOT endoscopic findings of one patient. Left side (pre-HBOT): just-anal rectal mucosae bleeding actively, compatible with RIP secondary to BT; APC was performed to control bleeding telangiectasias. Right side (post-HBOT): visualization of 3cm-superficial ulceration on the just-anal rectal mucosae, with friability and cicatricial areas, after 60 HBOT sessions. APC, argon plasma coagulation; BT, brachytherapy; HBOT, hyperbaric oxygen therapy; RIP, radiation-induced proctitis.
Sample characterization considering refractory symptoms, post-HBOT endoscopic findings, clinical response to HBOT and its related side effects, hematochezia relapse, and the need to perform a surgical procedure for symptomatic control are listed in Table 2. It is also important to note that in about 21.6% (n=19) of cases there were minor complications related to HBOT, and the most frequently reported adverse event was treatable MEB (20.5%; n=18). Only one case of reversible myopia was reported, and no other side effects were observed during or after the treatment protocol conclusion. The number of HBOT sessions was a statistically significant predictor of HBOT side effects (odds ratio= 1.010; 95% confidence interval, 1.000-1.020; p=0.047).

Table 2 Sample characterization considering clinical response rates, refractory symptoms, post-HBOT endoscopic exam results, side effects development, hematochezia recurrence, and the necessity to perform a surgical procedure for symptomatic control.
The estimated hematochezia recurrence rate was 14.8% (n=13), considering the progression of the disease. In 5.7% of cases, a surgical procedure to achieve symptomatic control or fistulae formation resolution was needed (n=5). The average follow-up time at our center was 1.8 months. Considering hematochezia as the most prevalent clinical manifestation (86.4%), we further analyzed in detail the exclusive relationship between hematochezia resolution rate and refractory hematochezia rate with the other most relevant variables, both categorical (sex, primary tumor, type of radiation-induced soft tissue lesions, need for transfusion support, pre-HBOT APC treatment, post-HBOT endoscopic results) and continuous (time between RT and symptoms onset, the time between symptoms onset and HBOT initiation, number of HBOT sessions and total duration of HBOT). No statistically significant relations were found, as specified in Table 3; however, there is a trend to achieve hematochezia resolution (complete or partial) after completing at least 70 HBOT sessions (p=0.075, applying Fisher’s exact test). While partial and complete responses require fewer than 70 sessions of HBOT in terms of overall RIP symptoms (p=0.069), isolated hematochezia tends to require at least 70 sessions by Fisher’s exact test.
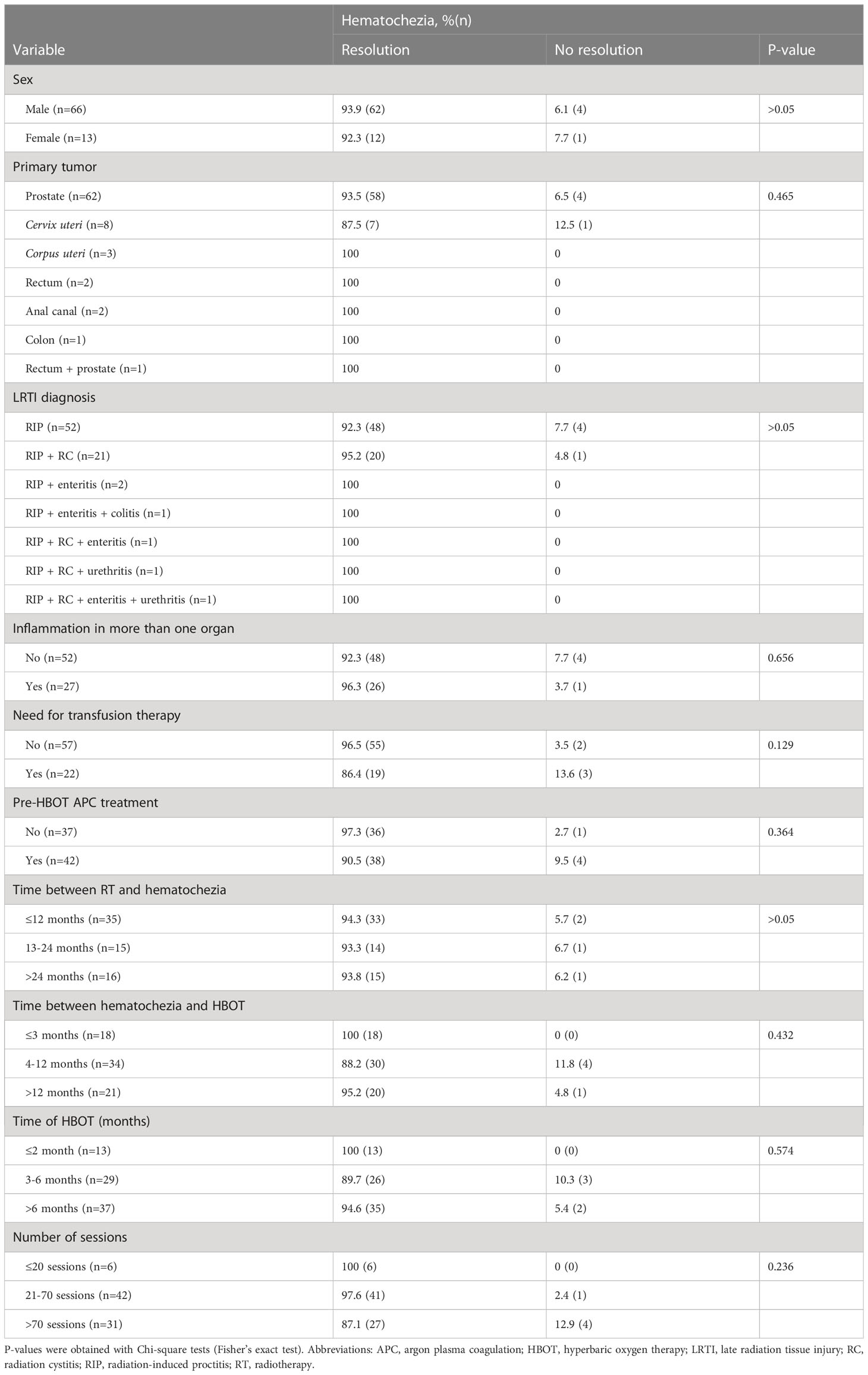
Table 3 Relationship between hematochezia resolution rates versus other categorical and continuous variables (after categorization).
4 Discussion
Consistent guidelines are not currently available for the management of RIP (24). Generally, patients are treated empirically on a tailored basis according to patient comorbidities, the severity of the clinical condition, and medical and institutional expertise (6, 8, 16, 24).
The HBOT is used in several clinical conditions as well as in professional and military training (8, 37, 38). As a result of the 10th European Consensus Conference on Hyperbaric Medicine, HBOT was recommended for the treatment of soft tissue radionecrosis, namely, RIP and RC (type 1 recommendation, level B evidence) (36). The first cutting-edge case report in this setting was conducted by Charneau J et al. (1991). It revealed the utility of HBOT in treating a 74-year-old male patient with a history of transfusion-dependent hemorrhagic RIP refractory to medical treatment. This patient achieved a complete response after 82 HBOT sessions (2.5 ATA, for 90 min, twice daily), with the clinical response remaining for at least 9 months, avoiding colostomy (39). Afterward, it was the motto for several case reports and small series, retrospective studies, clinical trials, reviews, and meta-analyses published in the last three decades (40–68).
In a Cochrane systematic review, Bennett M et al. (2016) reviewed 14 studies that showed moderate-quality evidence of HBOT in the management of LRTIs, including RIP (40). Another earlier systematic review conducted by Feldmeier J and Hampson NB (2002) considered 74 publications (including 14 on RIP and radiation enteritis), in which all but seven reported a positive outcome. Thus, based on the consistency of these findings, HBOT was considered “Likely to be Beneficial” for the treatment of patients with RIP and radiation enteritis (41).
We report real-world evidence of HBOT effectiveness in a large cohort of patients (n= 88) with RIP over a significant period of time (10 years).
Achieving an overall clinical response and hematochezia resolution rates of 94.3% and 93.7%, respectively, we can state that HBOT proved effective in managing RIP. These numbers reinforce the importance of this study compared to others, although positive, have less statistical robustness (40–46). The HOT2 clinical trial was an exception, which controversially demonstrated that HBOT was ineffective in treating chronic bowel dysfunction following pelvic RT (44). However, several limitations were pointed out for this study, such as the small sample size for a phase 3 trial, the predefined follow-up duration of only 12 months or even the exclusion of patients with grade 3 symptoms of LENT-SOMA score (including severe fecal incontinence and transfusion-dependent RIP) (8).
Generally, there is an underestimation of RIP mild symptoms, either by patients or physicians (8, 46). As expected, hematochezia represented our series’ most common clinical manifestation of RIP. The reason for this is possibly related to the fact that hematochezia is the most appreciated symptom and the primary manifestation of RIP, as it is an alarming symptom for the doctor-patient binomial. This information is consistent with data from previous studies, including that by Clarke RH et al. (2008), with the majority of patients presenting lower GI hemorrhage and other chronic symptoms such as diarrhea, constipation, ulceration, and pain (47). Additionally, our study showed a higher hematochezia resolution rate (complete and partial) when compared to other studies, such as that by Dall’Era MA et al. (2006) and Oliai C et al. (2012) with 76% and 75%, respectively (49, 50).
Furthermore, some patients have experienced symptoms other than GI as a result of RT damage to surrounding healthy tissues (22). Tolerance to irradiation of pelvic structures varies from specific organ to another. Normal tissues of the vagina, cervix, and uterus can withstand high radiation doses and recover quickly from RT lesions (51, 52). On the opposite side, the bladder, sigmoid, rectosigmoid, and rectum are more prone to radiation toxicity. Utmost point doses of 75 and 70 Gy are acceptable for the bladder and rectum, respectively (51, 53, 54). This supports that RIP and RC are two commonly reported LRTIs, possibly arising concurrently (51, 54–56). In fact, the combination of RIP and RC was our second most common LRTI diagnosis. A previous study conducted by Ribeiro de Oliveira T et al. (2015) evaluating hemorrhagic RC response to HBOT pointed to 23.9% of patients with LRTIs other than RC (namely RIP and enteritis) (55). Our data showed that individuals with at least two concurrent LRTIs were associated with complete response to HBOT, probably because other LRTIs require fewer HBOT sessions to achieve a complete clinical resolution and, consequently, are easier to treat when compared to RIP. Furthermore, previous studies investigating the efficacy of HBOT in treating RC, such as that by Oscarsson N et al. (2019), demonstrated that 30 HBOT sessions were associated with clinically relevant improvement in RC (57). Ribeiro de Oliveira T et al. (2015) also showed that 89.6% of patients achieved complete resolution of hematuria after an average of 37 sessions (55). Similarly, Degener S et al. (2012) presented an 80% complete resolution of hematuria after 30 sessions for a 35-month follow-up (58). Therefore, we believe that this treatment modality should be specially considered as a first-line treatment for patients who develop more than one LRTI (55, 59).
Patients eligible for our study tried at least one last conservative treatment modality (medical or endoscopic) that proved to be ineffective in treating RIP-associated symptomatology. Besides only 35 clinical records confirm the attempt to treat RIP initially with medical treatment, we believe that some pharmacological treatment has been performed globally as it is classically the first-line treatment to be applied in the management of RIP (8, 23, 29, 69). Sucralfate and mesalamine enemas were the most frequently prescribed treatments; less common options included metronidazole, vitamin A, and corticosteroid enemas. About 50% of patients underwent APC treatment before starting HBOT. Álvaro-Villegas JC et al. (2011) found that APC and HBOT were equally effective in treating RIP with regard to controlling rectal bleeding, the need for transfusions, and the impact on tissue toxicity. However, APC was associated with faster and higher responses at baseline (60). One of the relevant aspects of our series is that we have a heavily treated population in which HBOT played an important role in its subsequent control.
Additionally, our data showed that the time between RT and the onset of hematochezia was inversely associated with the number of HBOT sessions required. Therefore, it can be inferred that patients with a longer time until the clinical manifestation of hematochezia may have a better prognosis. After completing a median of 60 sessions, the overall response to HBOT tended to be inversely associated with the number of sessions, possibly because patients with a better response to HBOT needed fewer sessions. However, there was a trend for hematochezia resolution after completing at least 70 HBOT sessions. In general, the number of sessions performed in our study was higher than in other studies that present a full course treatment with an average of 40 sessions (42, 49, 61). This higher number of prescribed sessions may be explained by the fact that we treat more severe cases of RIP, as patients come to us in later phases and, consequently, with more refractory symptoms. Hence, due to our institutional experience, we anticipate the need for a more prolonged treatment, frequently surpassing 40 sessions.
Although rare and usually non-severe, HBOT has known potential adverse events. In a retrospective analysis of 1.5 million treatments, only 0.68% were associated with a side effect, being barotrauma and confinement anxiety the most reported events (62). The incidence of MEB varies according to the series and ranges from 0.37 to 84% in non-ventilated patients versus 94% in ventilated patients (38, 63, 64). Our data align with published data and showed that the number of HBOT sessions was a predictor of side effects, mainly MEB.
Lastly, our retrospective study is not exempted from limitations. The current analysis is limited by several factors, including its retrospective nature, the single institution source of data, and the quality of our medical and supervisor records compromised by the lack of complete clinical information. Once patients turned asymptomatic (mainly in relation to hematochezia) and completed the treatment course, they were referred to the attending physician. One of the limitations is the short follow-up period and the loss of follow-up of treated patients after referral to the attending physician. These facts may have prevented more reliable monitoring of symptoms or even their relapse. Moreover, it may even influence the evaluation of the hematochezia recurrence rate. The lack of grading of adverse events based on a validated classification did not allow for drawing more robust conclusions, configuring another important limitation of our study. The missed information about the different RT protocols administered (total dose and fractionation) and comprehensive information related to pre-HBOT medical treatment conditioned our analysis of the potential relationship between different variables and the clinical response to HBOT. Also, the inexistence of a more detailed characterization of the post-HBOT clinical picture limited us from assessing the remaining symptoms.
In this cohort of HBOT-treated refractory RIP patients (the largest reported to date), the overall clinical response rate was 94.3% (including 62.5% complete responses) after a median of 60 HBOT sessions. Furthermore, HBOT proved to be a safe treatment when patients are previously studied and the correct protocol is applied. This real-world evidence study adds value to published data on the management of RIP with HBOT.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by Armed Forces Hospital Ethics Committee - Armed Forces Hospital, Lisbon, Portugal. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
The present manuscript is the result of the original work by the authors. AMM and DAC conceived and designed the study. AMM performed the consultation of medical records. AMM, DAC, and VM performed the analysis and interpretation of the data; all the authors approved manuscript draft. DAC, VM, and CEA performed the manuscript supervision.
Acknowledgments
We thank Professor Elisabete Fernandes from the Faculdade de Medicina (Universidade de Lisboa) for collaborating on the statistical analysis. We also thank all the staff of the Centro de Medicina Subaquática e Hiperbárica (Armed Forces Hospital, Lisbon) for facilitating the consultation of the archived medical records.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Cancer. World Health Organization (2022). Available at: https://www.who.int/news-room/fact-sheets/detail/cancer.
2. Cancer fact sheets - All cancers. The Global Cancer Observatory - International Agency for Research on Cancer (2020). Available at: https://gco.iarc.fr/today/data/factsheets/cancers/39-All-cancers-fact-sheet.pdf.
3. Óbitos por algumas causas de morte (%). PORDATA - Estatísticas Sobre Portugal E Europa (2022). Available at: https://www.pordata.pt/portugal/obitos+por+algumas+causas+de+morte+(percentagem)-758-235710.
4. Population fact sheets - Portugal. The Global Cancer Observatory - International Agency for Research on Cancer (2021). Available at: https://gco.iarc.fr/today/data/factsheets/populations/620-portugal-fact-sheets.pdf.
5. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J Clin (2021) 71(3):209–49. doi: 10.3322/caac.21660
6. van de Wetering FT, Verleye L, Andreyev HJN, Maher J, Vlayen J, Pieters BR, et al. Non-surgical interventions for late rectal problems (proctopathy) of radiotherapy in people who have received radiotherapy to the pelvis. Cochrane library (2016) 2016(4). doi: 10.1002/14651858.CD003455.pub2
7. Marchetti C, Felice D, Perniola G, Lecce F, Vertechy L, Monti M, et al. Screening program in ovarian cancer: A logical step in clinical management? A meta-analysis. Curr Problems Cancer (2018) 42(2):235–40. doi: 10.1016/j.currproblcancer.2017.12.005
8. Alpuim Costa D, Espiney Amaro C, Nunes A, Cardoso JFMF, Daniel PM, Rosa IMD, et al. Hyperbaric oxygen therapy as a complementary treatment for radiation proctitis: Useless or useful? – A literature review. World J Gastroenterol (2021) 27(27):4413–28. doi: 10.3748/wjg.v27.i27.4413
9. De Ruysscher D, Niedermann G, Burnet NG, Siva S, Lee AWM, Hegi-Johnson F. Radiotherapy toxicity. Nat Rev Dis Primers (2019) 5(1). doi: 10.1038/s41572-019-0064-5
10. Baskar R, Lee KH, Yeo R, Yeoh KW. Cancer and radiation therapy: Current advances and future directions. Int J Med Sci (2012) 9(3):193–9. doi: 10.7150/ijms.3635
11. Maani EV, Maani C. Radiation therapy. StatPearls - NCBI Bookshelf (2022). Available at: https://www.ncbi.nlm.nih.gov/books/NBK537036/.
12. Chen AP, Kuo MT. Improving radiotherapy in cancer treatment: Promises and challenges. Oncotarget (2017) 8(37):62742–58. doi: 10.18632/oncotarget.18409
13. Baumann MH, Krause M, Overgaard J, Debus J, Bentzen SM, Daartz J, et al. Radiation oncology in the era of precision medicine. Nat Rev Cancer (2016) 16(4):234–49. doi: 10.1038/nrc.2016.18
14. Kichloo A, Tuma F, Aljadah M, Wani F. Radiation proctitis and management strategies. Clin Endosc (2021) 55(1):22–32. doi: 10.5946/ce.2020.288
15. Types of radiation therapy. New Jersey: National Institutes of Health - National Cancer Institute. 40: 2016. Available at: https://training.seer.cancer.gov/treatment/radiation/types.html.
16. Jhingran A. Chapter 23 - Complications of radiation oncology. In: Principles of Gynecologic Oncology Surgery. Philadelphia, PA: Elsevier (2018). p. 318–29. doi: 10.1016/B978-0-323-42878-1.00023-7
17. Grodsky MB, Sidani SM. Radiation proctopathy. Clinics Colon Rectal Surg (2015) 28(2):103–11. doi: 10.1055/s-0035-1547337
18. Moussa L, Usunier B, Demarquay C, Benderitter M, Tamarat R, Semont A, et al. Bowel radiation injury: Complexity of the pathophysiology and promises of cell and tissue engineering. Cell Transplantation (2016) 25(10):1723–46. doi: 10.3727/096368916X691664
19. Liu L, Chen C, Liu X, Bingcheng C, Ding C, Liang J. Altered gut microbiota associated with hemorrhage in chronic radiation proctitis. Front Oncol (2021) 11:637265. doi: 10.3389/fonc.2021.637265
20. Jian YP, Zhang D, Liu M, Wang Y, Xu Z. The impact of gut microbiota on radiation-induced enteritis. Front Cell Infection Microbiol (2021) 11:586392. doi: 10.3389/fcimb.2021.586392
21. Kumagai T, Rahman F, Smith AM. The microbiome and radiation induced-bowel injury: Evidence for potential mechanistic role in disease pathogenesis. Nutrients (2018) 10(10):1405. doi: 10.3390/nu10101405
22. Villeirs L, Tailly T, Ost P, Waterloos M, Decaestecker K, Fonteyne V, et al. Hyperbaric oxygen therapy for radiation cystitis after pelvic radiotherapy: Systematic review of the recent literature. Int J Urol (2020) 27(2):98–107. doi: 10.1111/iju.14130
23. Paquette IM, Vogel JD, Abbas MA, Feingold DL, Steele SR, Surgeons R. The american society of colon and rectal surgeons clinical practice guidelines for the treatment of chronic radiation proctitis. Dis Colon Rectum. (2018) 61(10):1135–40. doi: 10.1097/DCR.0000000000001209
24. Tabaja L, Sidani SM. Management of radiation proctitis. Digestive Dis Sci (2018) 63(9):2180–8. doi: 10.1007/s10620-018-5163-8
25. Bowen JM, Gibson RJ, Coller JK, Blijlevens NMA, Bossi P, Al-Dasooqi N, et al. Systematic review of agents for the management of cancer treatment-related gastrointestinal mucositis and clinical practice guidelines. Supportive Care Cancer (2019) 27(10):4011–22. doi: 10.1007/s00520-019-04892-0
26. Ramakrishnaiah VPN, Javali T, Dharanipragada K, Rajender RK, Krishnamachari S. Formalin dab, the effective way of treating haemorrhagic radiation proctitis: a randomized trial from a tertiary care hospital in South India. Colorectal Disease (2012) 14(7):876–82. doi: 10.1111/j.1463-1318.2012.03008.x
27. Tsujinaka S, Baig MMFA, Gornev R, de la Garza C, Hwang JK, Sands DR, et al. Formalin instillation for hemorrhagic radiation proctitis. Surg Innovation (2005) 12(2):123–8. doi: 10.1177/155335060501200209
28. Sharma B, Gupta M, Sharma R, GA K, Sharma N, Sharma M, et al. Four percent formalin application for the management of radiation proctitis in carcinoma cervix patients: An effective, safe, and economical practice. J Cancer Res Ther (2018) 15(1):92–5. doi: 10.4103/jcrt.JCRT_393_17
29. Weiner JA, Wong A, Schwartz DA, Martínez M, Aytaman A, Schreiber D. Endoscopic and non-endoscopic approaches for the management of radiation-induced rectal bleeding. World J Gastroenterol (2016) 22(31):6972. doi: 10.3748/wjg.v22.i31.6972
30. Wu X, Liu X, Katz S, Shen B. Pathogenesis, diagnosis, and management of ulcerative proctitis, chronic radiation proctopathy, and diversion proctitis. Inflamm Bowel Dis (2015) 21(3):703–15. doi: 10.1097/MIB.0000000000000227
31. Laranjo A, Ferriani MDGC, Rei A, Veloso N, Medeiros I. The effect of hyperbaric oxygen therapy on rectal ulcers after argon plasma coagulation. GE Portuguese J Gastroenterol (2021) 28(4):288–91. doi: 10.1159/000510792
32. Cooper JS, Hanley M. Hyperbaric treatment of radiation proctitis. Treasure Island, FL: StatPearls Publishing (2022). Available at: https://www.ncbi.nlm.nih.gov/books/NBK537343/.
33. Fernández E, Morillo V, Salvador MD, Santafé A, Beato I, Rodríguez MA, et al. Hyperbaric oxygen and radiation therapy: a review. Clin Trans Oncol (2021) 23(6):1047–53. doi: 10.1007/s12094-020-02513-5
34. Bennett MJ, Feldmeier JJ, Smee R, Milross C. Hyperbaric oxygenation for tumour sensitisation to radiotherapy. Cochrane Lib (2018) 2018(7). doi: 10.1002/14651858.CD005007.pub4
35. Mechem C, Manaker S. Hyperbaric oxygen therapy [Internet] (2023). Available at: https://www.uptodate.com/contents/hyperbaric-oxygen-therapy.
36. Mathieu D, Marroni A, Kot J. Tenth European Consensus Conference on Hyperbaric Medicine: recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving Hyperbaric Med (2017) 47(1):24–32. doi: 10.28920/dhm47.1.24-32
37. HBO indications - Undersea & Hyperbaric Medical Society. Undersea & Hyperbaric Medical Society. Available at: https://www.uhms.org/resources/hbo-indications.
38. Costa D, Ganilha JS, Barata PC, Guerreiro FG. Seizure frequency in more than 180,000 treatment sessions with hyperbaric oxygen therapy – a single centre 20-year analysis. Diving Hyperbaric Med (2019) 49(3):167–74. doi: 10.28920/dhm49.3.167-174
39. Charneau J, Bouachour G, Person B, Burtin P, Ronceray J, Boyer J. Severe hemorrhagic radiation proctitis advancing to gradual cessation with hyperbaric oxygen. Digestive Dis Sci (1991) 36:373–5. doi: 10.1007/BF01318212
40. Bennett MJ, Feldmeier JJ, Hampson NB, Smee R, Milross C. Hyperbaric oxygen therapy for late radiation tissue injury. New Jersey: The Cochrane Library (2016). doi: 10.1002/14651858.CD005005.pub4
41. Feldmeier JJ, Hampson NB. A systematic review of the literature reporting the application of hyperbaric oxygen prevention and treatment of delayed radiation injuries: an evidence based approach. Undersea Hyperbaric Med: J Undersea Hyperbaric Med Soc (2002) 29(1):4–30.
42. Gaio-Lima C, Castedo J, Cruz M, Candeias M, Camacho Ó. The role of hyperbaric oxygen therapy in the treatment of radiation lesions. Clin Trans Oncol (2022) 24(12):2466–74. doi: 10.1007/s12094-022-02892-x
43. Andren J, Bennett MJ. An observational trial to establish the effect of hyperbaric oxygen treatment on pelvic late radiation tissue injury due to radiotherapy. Diving Hyperbaric Med (2020) 50(3):250–5. doi: 10.28920/dhm50.3.250-255
44. Glover M, Smerdon GR, Andreyev HJN, Benton B, Bothma P, Firth O, et al. Hyperbaric oxygen for patients with chronic bowel dysfunction after pelvic radiotherapy (HOT2): a randomised, double-blind, sham-controlled phase 3 trial. Lancet Oncol (2016) 17(2):224–33. doi: 10.1016/S1470-2045(15)00461-1
45. Tahir A, Westhuyzen J, Dass J, Collins MJ, Webb RM, Hewitt S, et al. Hyperbaric oxygen therapy for chronic radiation-induced tissue injuries: Australasia’s largest study. Asia-pacific J Clin Oncol (2015) 11(1):68–77. doi: 10.1111/ajco.12289
46. Girnius S, Cersonsky N, Gesell L, Cico S, Barrett W. Treatment of refractory radiation-induced hemorrhagic proctitis with hyperbaric oxygen therapy. Am J Clin Oncol (2006) 29(6):588–92. doi: 10.1097/01.coc.0000236004.95384.5b
47. Friedman LS, Hong TS. Radiation proctitis: Clinical manifestations, diagnosis and management (2023). Available at: https://www.uptodate.com/contents/radiation-proctitis-clinical-manifestations-diagnosis-and-management.
48. Clarke RH, Tenorio LMC, Hussey JR, Toklu AS, Cone DL, Hinojosa JA, et al. Hyperbaric oxygen treatment of chronic refractory radiation proctitis: A randomized and controlled double-blind crossover trial with long-term follow-up. Int J Radiat Oncol Biol Physics (2008) 72(1):134–43.e15. doi: 10.1016/j.ijrobp.2007.12.048
49. Dall’Era MA, Hampson NB, Hsi RA, Madsen B, Corman JM. Hyperbaric oxygen therapy for radiation induced proctopathy in men treated for prostate cancer. J Urol (2006) 176(1):87–90. doi: 10.1016/S0022-5347(06)00491-5
50. Oliai C, Fisher B, Jani A, Wong MH, Poli J, Brady LW, et al. Hyperbaric oxygen therapy for radiation-induced cystitis and proctitis. Int J Radiat Oncol Biol Phys (2012) 84(3):733–40. doi: 10.1016/j.ijrobp.2011.12.056
51. Yashar C. 23 – basic principles in gynecologic radiotherapy. In: Clinical Gynecologic Oncology, 9th ed. Philadelphia, PA: Elsevier (2018). p. 586–605. doi: 10.1016/B978-0-323-40067-1.00023-1
52. D’Souza DP, Rumble RB, Fyles A, Yaremko B, Warde P. Intensity-modulated radiotherapy in the treatment of Gynaecological cancers. Clin Oncol (2012) 24(7):499–507. doi: 10.1016/j.clon.2012.05.005
53. Do N, Nagle D, Poylin V. Radiation proctitis: Current strategies in management. Gastroenterol Res Practice (2011) 2011:1–9. doi: 10.1155/2011/917941
54. Denton AS, Andreyev J, Forbes A, Maher J. Non surgical interventions for late radiation proctitis in patients who have received radical radiotherapy to the pelvis. Cochrane Database Systematic Rev (2002). doi: 10.1002/14651858.CD001773
55. Ribeiro De Oliveira TF, Romão C, Guerreiro F, Lopes T. Hyperbaric oxygen therapy for refractory radiation-induced hemorrhagic cystitis. Int J Urol (2015) 22(10):962–6. doi: 10.1111/iju.12857
56. Denton AS, Clarke NW, Maher J. Non-surgical interventions for late radiation cystitis in patients who have received radical radiotherapy to the pelvis. Cochrane Lib (2002) 2022(1). doi: 10.1002/14651858.CD003455
57. Oscarsson N, Müller B, Rosén A, Lodding P, Mölne J, Giglio D, et al. Radiation-induced cystitis treated with hyperbaric oxygen therapy (RICH-ART): a randomised, controlled, phase 2–3 trial. Lancet Oncol (2019) 20(11):1602–14. doi: 10.1016/S1470-2045(19)30494-2
58. Degener S, Strelow H, Pohle A, Lazica DA, Windolf J, Zumbé J, et al. [Hyperbaric oxygen in the treatment of hemorrhagic radiogenic cystitis after prostate cancer]. Der Urologe Ausg A (2012) 51(12):1735–40. doi: 10.1007/s00120-012-3036-x
59. Safra T, Gutman G, Fishlev G, Soyfer V, Gall N, Lessing JB, et al. Improved quality of life with hyperbaric oxygen therapy in patients with persistent pelvic radiation-induced toxicity. Clin Oncol (2008) 20(4):284–7. doi: 10.1016/j.clon.2007.12.005
60. Alvaro-Villegas JC, Sobrino-Cossío S, Tenorio-Téllez LC, de la Mora-Levy JG, Hernández-Guerrero A, Alonso-Lárraga JO, et al. Argon plasma coagulation and hyperbaric oxygen therapy in chronic radiation proctopathy, effectiveness and impact on tissue toxicity. Rev Espanola Enfermedades Digestivas (2011) 103(11):576–81. doi: 10.4321/s1130-01082011001100004
61. Oscarsson N, Arnell P, Lodding P, Ricksten SE, Seeman-Lodding H. Hyperbaric oxygen treatment in radiation-induced cystitis and proctitis: A prospective cohort study on patient-perceived quality of recovery. Int J Radiat Oncol Biol Physics (2013) 87(4):670–5. doi: 10.1016/j.ijrobp.2013.07.039
62. Jokinen-Gordon H, Barry RC, Watson B, Covington DS. A retrospective analysis of adverse events in hyperbaric oxygen therapy (2012-2015): lessons learned from 1.5 million treatments. Adv Skin Wound Care (2017) 30(3):125–9. doi: 10.1097/01.ASW.0000508712.86959.c9
63. Alpuim Costa D, Sampaio-Alves M, Netto E, Fernandez G, Oliveira E, Teixeira A, et al. Hyperbaric oxygen therapy as a complementary treatment in glioblastoma-A scoping review. Front Neurol (2022) 13:886603. doi: 10.3389/fneur.2022.886603
64. Miyazawa T, Ueda H, Yanagita N. Eustachian tube function and middle ear barotrauma associated with extremes in atmospheric pressure. Ann Otology Rhinology Laryngol (1996) 105(11):887–92. doi: 10.1177/000348949610501109
65. Warren DC, Feehan P, Slade JB, Cianci PE. Chronic radiation proctitis treated with hyperbaric oxygen. Undersea Hyperbaric Med - J Undersea Hyperbaric Med Soc (1997) 24(3):181–4.
66. Woo TC, Joseph D, Oxer HF. Hyperbaric oxygen treatment for radiation proctitis. Int J Radiat Oncol Biol Physics (1997) 38(3):619–22. doi: 10.1016/s0360-3016(97)00017-5
67. Gouëllo JP, Bouachour G, Person B, Ronceray J, Cellier P, Alquier P. Intérêt de l’oxygènothérapie hyperbare dans la pathologie digestive post-radique. 36 observations [The role of hyperbaric oxygen therapy in radiation-induced digestive disorders. 36 cases]. Presse Médicale (1999) 28(20):1053–7.
68. Geldof NI, Hulst V, Ridderikhof ML, Teguh DN. Hyperbaric oxygen treatment for late radiation-induced tissue toxicity in treated gynaecological cancer patients: a systematic review. Radiat Oncol (2022) 17(1). doi: 10.1186/s13014-022-02067-6
69. Sahakitrungruang C, Patiwongpaisarn A, Kanjanasilp P, Malakorn S, Atittharnsakul P. A randomized controlled trial comparing colonic irrigation and oral antibiotics administration versus 4% formalin application for treatment of hemorrhagic radiation proctitis. Dis Colon Rectum (2012) 55(10):1053–8. doi: 10.1097/DCR.0b013e318265720a
Keywords: radiotherapy, radiation injury, late radiation tissue injury, radiation-induced proctitis, radiation proctitis, hyperbaric oxygenation, hyperbaric oxygen, hyperbaric oxygen therapy
Citation: Moreira Monteiro A, Alpuim Costa D, Mareco V and Espiney Amaro C (2023) The effectiveness of hyperbaric oxygen therapy for managing radiation-induced proctitis – results of a 10-year retrospective cohort study. Front. Oncol. 13:1235237. doi: 10.3389/fonc.2023.1235237
Received: 05 June 2023; Accepted: 07 July 2023;
Published: 11 August 2023.
Edited by:
David Pasquier, Oscar Lambret Centre, FranceReviewed by:
Guillaume Vogin, Centre François Baclesse (CFB), LuxembourgAngel Montero, HM Madrid Hospital, Spain
Copyright © 2023 Moreira Monteiro, Alpuim Costa, Mareco and Espiney Amaro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: António Moreira Monteiro, YW50b25pby1tb250ZWlyb0BjYW1wdXMudWwucHQ=; Diogo Alpuim Costa, ZGlvZ29hbHB1aW1jb3N0YUBnbWFpbC5jb20=
†These authors have contributed equally to this work