 Marcos Adriano Garcia Campos1*†
Marcos Adriano Garcia Campos1*† Lucas Fernandes Vasques2†
Lucas Fernandes Vasques2† Rafael Goulart de Medeiros2†
Rafael Goulart de Medeiros2† Érico Murilo Monteiro Cutrim1
Érico Murilo Monteiro Cutrim1 Ana Júlia Favarin1Sarah Rebecca Machado Silva1
Ana Júlia Favarin1Sarah Rebecca Machado Silva1 Gyl Eanes Barros Silva3Marcelo Padovani de Toledo Moraes1Mariana Lopes Zanatta1
Gyl Eanes Barros Silva3Marcelo Padovani de Toledo Moraes1Mariana Lopes Zanatta1 Diego Aparecido Rios Queiróz1
Diego Aparecido Rios Queiróz1- 1Department of Internal Medicine, Hospital of Medical School of São Paulo State University, Botucatu, Brazil
- 2Department of Medicine, University of Taubate Faculty of Medicine, Taubaté, Brazil
- 3Laboratory of Immunofluorescence and Electron Microscopy, University Hospital of Federal University of Maranhão, São Luís, Brazil
Clear cell tumors of the lung (CCTL), or “sugar tumors” of lung, are very uncommon lesions and are mostly benign perivascular epithelioid cell (PEC) tumors with no specific morphologic features. Fewer than 100 cases have been reported; the aggressive nature demonstrated in sporadic reports has rarely been described in the literature. Although the course is generally described as benign, eight reported cases showed malignant behavior. We report a case of a PEC with a malignant presentation in a young man, correlating the main characteristics of the tumor with other cases reported in the literature to better elucidate this rare presentation. We also performed a literature review of reports on benign and malignant CCTL cases, with a focus on clinical, imaging, and immunohistochemical differentiation. CCTLs are rare tumors that require histopathological and immunohistochemical confirmation; to date, criteria that can predict malignant evolution are lacking.
Introduction
Clear cell tumors, or “sugar tumors”, are very uncommon lesions (1) and are mostly benign perivascular epithelioid cell (PEC) tumors (2, 3). PEC tumors are a rare group of mesenchymal neoplasms histologically and immunohistochemically distinct from other neoplasms, with an abundance of periodic acid-Schiff (PAS)-positive glycogen (3). They are expressed in the bladder (4), uterus (5), breast (6), ovary (7), vagina (8), kidney (9), prostate (10), pancreas (11), jejunum (12), soft tissues (13) and lung (14). Due to this wide diversity, these tumors lack specific morphologic features (2).
The lungs are an uncommon site for PEC tumors, known as clear cell tumors of lung (CCTL) (15), and such PEC tumors in the lung are usually benign, with malignancy exceedingly rare (9). Although fewer than 100 cases have been reported, sporadic reports have described CCTLs with very rare aggressive nature (3). A silent, indolent, and asymptomatic presentation may pose a diagnostic challenge for pathologists and oncologists (16).
CCTLs exhibit nested histological features similar to other PEC tumors. They consist of uniform round to polygonal epithelioid cells with clear or eosinophilic cytoplasm and well-defined borders. CCTLs are surrounded by prominent thin-walled vascular channels. Although the course of CCTL is typically described as benign, eight cases have shown malignant behavior (17). We present a case of CCTL with a malignant presentation, correlating the main characteristics of the tumor with other cases reported in the literature to better elucidate this rare presentation.
Case description
A 49-year-old man, hypertensive and a smoker, presented to the primary healthcare department with complaints of dyspnea on exertion and daily chest pain for the past year, with gradual worsening in the last three months, in addition to a weight loss of 10 kg. The patient denied coughing, hemoptysis, fever, or a family history of cancer.
Computed tomography (CT) of the chest showed a solid, calcified, upper left paratracheal lesion (191 cm3) with central necrosis in close contact with the ipsilateral subclavian artery without a cleavage plane, in addition to multiple randomly distributed nodules in the lung parenchyma and enlarged lymph nodes in the para-aortic chain and thin left pleural effusion (Figure 1). A lithic image of the T1 vertebral body indicated possible secondary neoplastic involvement; however, bone scintigraphy and positron emission tomography-CT (PET-CT) revealed a low probability of bone metastasis. No secondary lesions were observed in any of the abdominal organs.
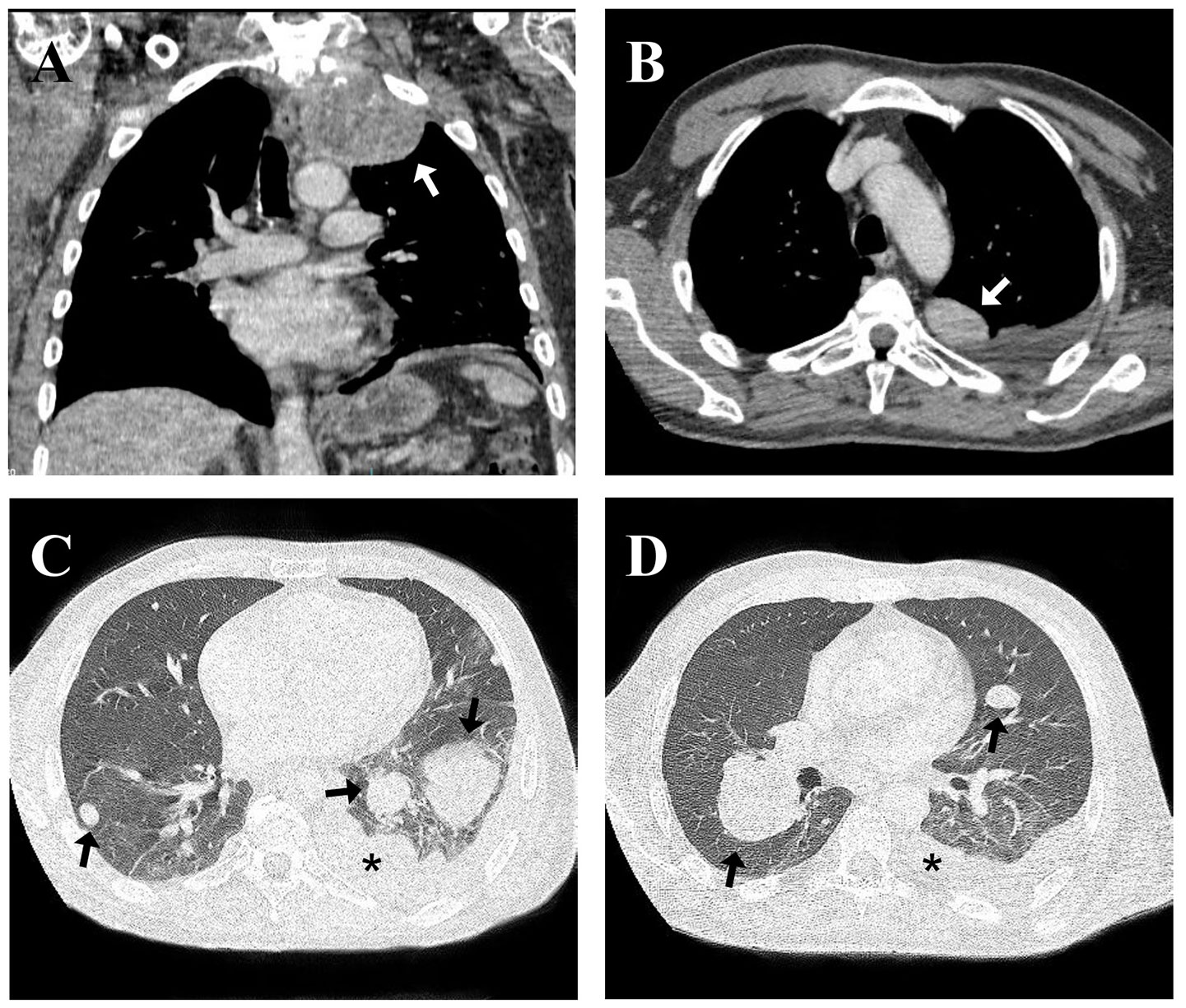
Figure 1 Initial coronal (A) and axial (B) computed tomography pulmonary angiogram reconstruction of the chest performed showing a mass in upper left paratracheal side (white arrow in A, B) associated with multiple randomly distributed nodules in the lung parenchyma (black arrow in C, D), the largest of them in the middle third of the lung right, enlarged lymph nodes in the para-aortic chain and thin left pleural effusion (black asterisk in C, D).
The anatomopathological examination of the transbronchial biopsy showed the presence of neoplasia caused by epithelioid cells with abundant clear and granular cytoplasm, well-defined cell borders, and round and hyperchromatic nuclei, without the presence of prominent nucleoli (Figure 2). There were mild cellular atypia and foci of hemorrhage, necrosis, and absence of significant mitotic activity. Immunohistochemical (IHC) analysis revealed negativity for pan-cytokeratin (AE1, AE3, TTF1, RCC, MiTF, S-100, CK7, CK8, CK20, and desmin) and positivity for muscle markers and melanocyte antibodies (HMB-45, smooth actin muscle, CD10, and Melan-A) and Cathepsin K. These findings were indicative of a CCTL.
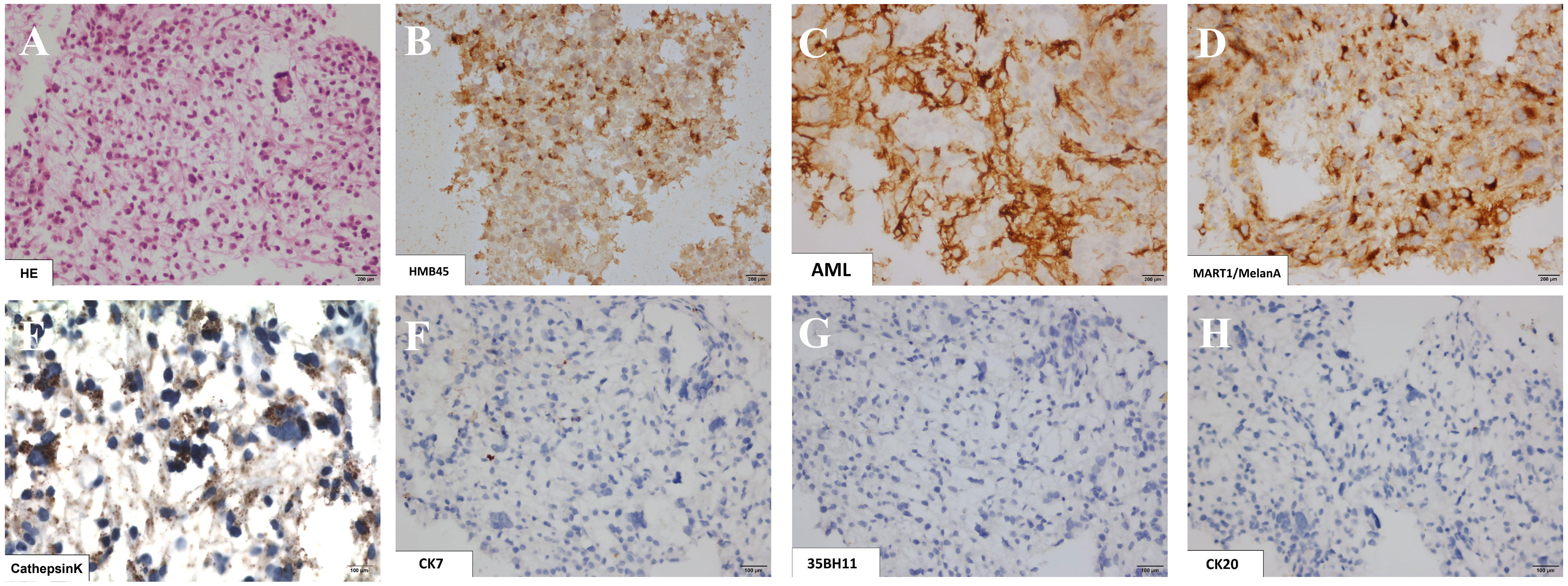
Figure 2 Histological sections of lung biopsy showing in hematoxylin-eosin staining the presence of clear cell tumors represented by epithelioid cells with abundant clear and granular cytoplasm, with well-delimited cell borders and round and hyperchromatic nuclei, discreet cell atypia and absence of significant mitotic activity (A). The immunohistochemical study revealed co-expression of markers: HMB45 (B), smooth muscle actin (C), Melan-A (D) and Cathepsin K (E), and negativity for cytokeratins CK7, CK8 and CK20 (F, G, H, respectively).
The challenges of verifying diagnosis and scheduling medical appointments, combined with suboptimal patient adherence, led to delayed treatment initiation. Only, five months after the biopsy, the patient underwent 2000 cGy doses of radiotherapy targeting the left lung in five fractions over one week and three cycles of doxorubicin 75 mg/m2 within three months. However, owing to his compromised performance status and the presence of multiple nodules, surgical resection could not be performed. He presented with deterioration of the clinical picture and progression of pulmonary nodules in number and size two months after starting treatment, in addition to an increase in mediastinal lymph nodes and bilateral pleural effusion.
One month later, the patient was admitted to the emergency room with dyspnea, desaturation, and severe chest pain. Additionally, he had mild respiratory alkalosis associated with microcytic and hypochromic anemia without leukocytosis or normal platelet levels. He had normal electrolyte and renal function, increase in transaminase levels by about three times the upper normal value, and slight hypoalbuminemia, without changes in bilirubin or coagulogram. C-reactive protein was 8.9 mg/dl (reference value, < 1 mg/dl), with no reports of infectious symptoms. Serological tests for hepatitis, HIV and syphilis were negative. Chest radiography and CT revealed a significant progression of the lung masses (Figure 3). There was no evidence of other complications such as massive pleural effusion, pulmonary embolism, or pneumothorax, which would justify respiratory worsening in addition to the progression of tumor masses. Owing to the rapid progression of his condition, the patient underwent palliative sedation and died approximately 48 h after admission. A timeline specifying the entire clinical evolution of the patient is shown in Figure 4.
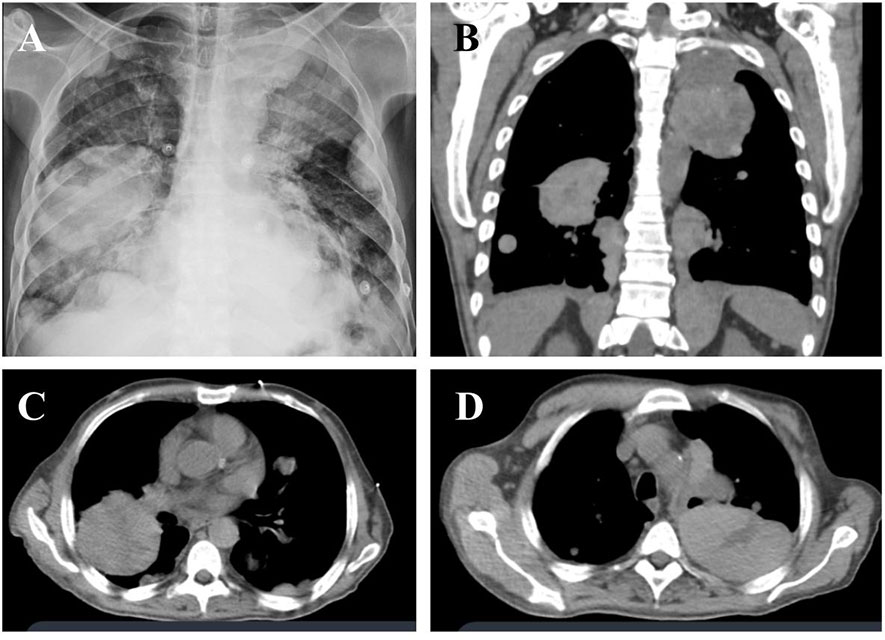
Figure 3 Radiographic images showing extensive pulmonary masses on chest X-ray (A) and computed tomography of the chest in coronal (B) and axial planes (C, D), suggesting disease progression. A solid tumor, calcified upper left parasternal lesion with central necrosis, close contact with ipsilateral subclavian artery, without a cleavage plane and a tumor with similar characteristics on the lower right.
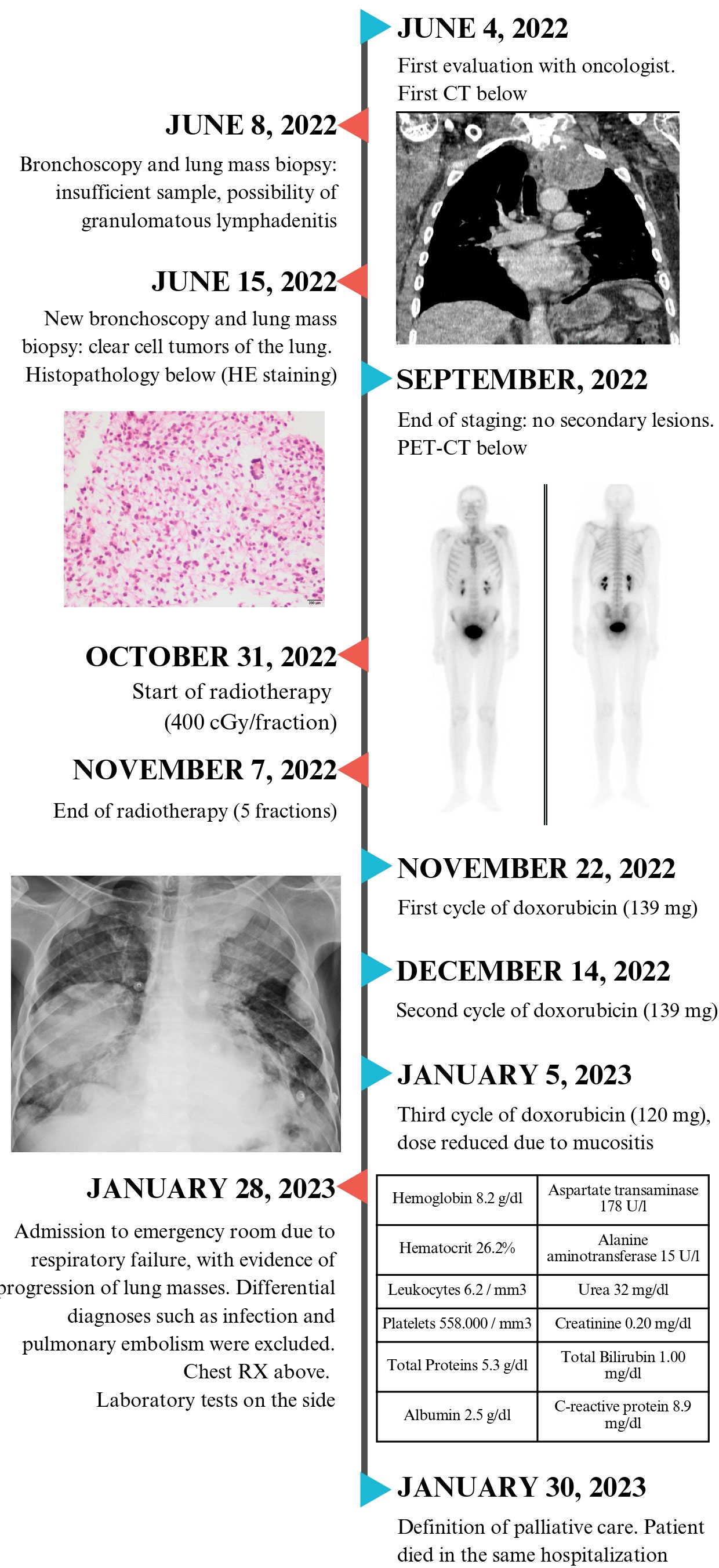
Figure 4 Timeline from the initial clinical presentation and tests performed for the diagnosis of clear cell tumors of the lung. The time of chemotherapy, radiotherapy and hospitalization until the outcome of the case are also specified.
Discussion
Herein, we present a rare case of malignant CCTL. It is an uncommon and usually benign neoplasm composed of uniform round to polygonal epithelioid cells with clear or eosinophilic cytoplasm, well-defined borders, and prominent thin-walled vascular channels (1), as observed in our case. Throughout the clinical and imaging evaluation, the malignant presentation of the patient was clear.
CCTL has no established epidemiology, clinical characteristics, diagnoses, or treatments. It is commonly confused with lung carcinoma or metastases from clear-cell carcinoma of the kidney (18). Patients are usually > 50 years old, but cases from 9 to 75 years of age have been reported (15, 19), with a similar prevalence between the sexes (20).
Among the benign manifestations of CCTL, an asymptomatic condition with an accidental diagnosis is common. However, as the size of this neoplasm can vary from several millimeters to approximately 16 cm (15), symptoms such as chest pain, cough, shortness of breath, hemoptysis, or fever may be observed in larger masses, especially if the size exceeds 2.2 cm (21–24).
We performed a literature review of the cases of benign and malignant CCTL (Table 1). Cases of CCTL with malignant behavior during the course of the disease and its outcomes have been reported sporadically. Certain characteristics, such as diameter greater than 2.5-3.0 cm, presence of symptoms, metastases, extensive necrosis, and abundant mitoses, are associated with a malignant presentation (24). Of the 76 benign occurrences found, necrosis was present in only 6.5% of the cases and mitotic activity was present in 4.0%. The largest mean mass diameter was 2.8 cm. In malignant cases, necrosis and mitotic activity were significantly more frequent, occurring in 50% and 12.5% respectively, and the mean diameter of the mass was 6.7 cm, which is 2.3 times greater than that of benign masses.
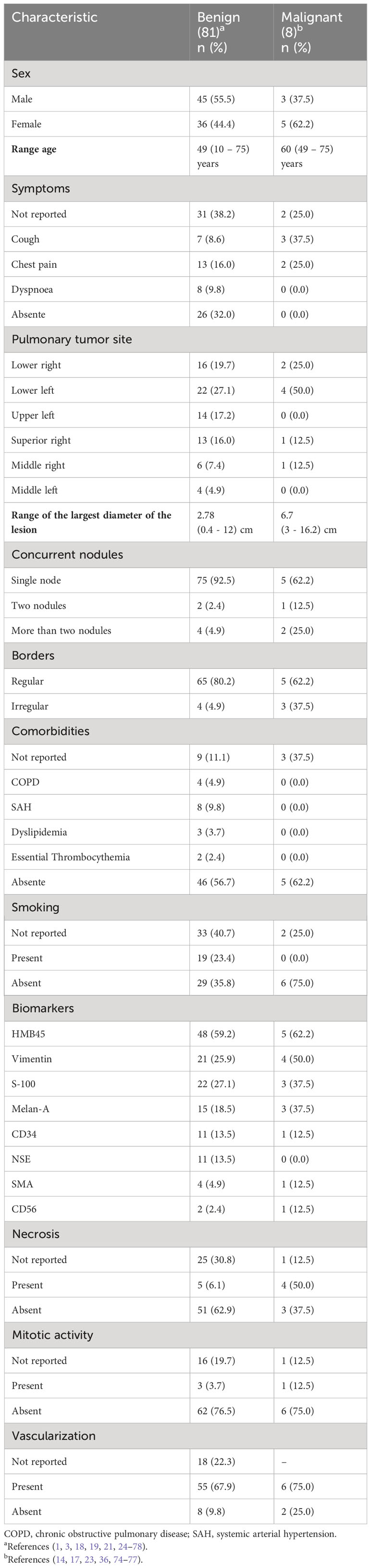
Table 1 Comparison of features between benign and malignant cases of perivascular epithelioid cells (PEC) tumors.
The site that was most affected by the primary nodule was the lower lobe of the lung. In this case, an extensive lesion was observed in the left upper lobe, characterized by necrosis and abundant vascularization, in addition to other scattered nodules in the parenchyma.
CCTL has already been associated with other diseases, such as tuberous sclerosis complex (79), Birt-Hogg-Dube Syndrome, and essential thrombocythemia (26, 27). However, in the malignant cases, it was not possible to determine the presence of risk factors strongly related to CCTL (Table 2).
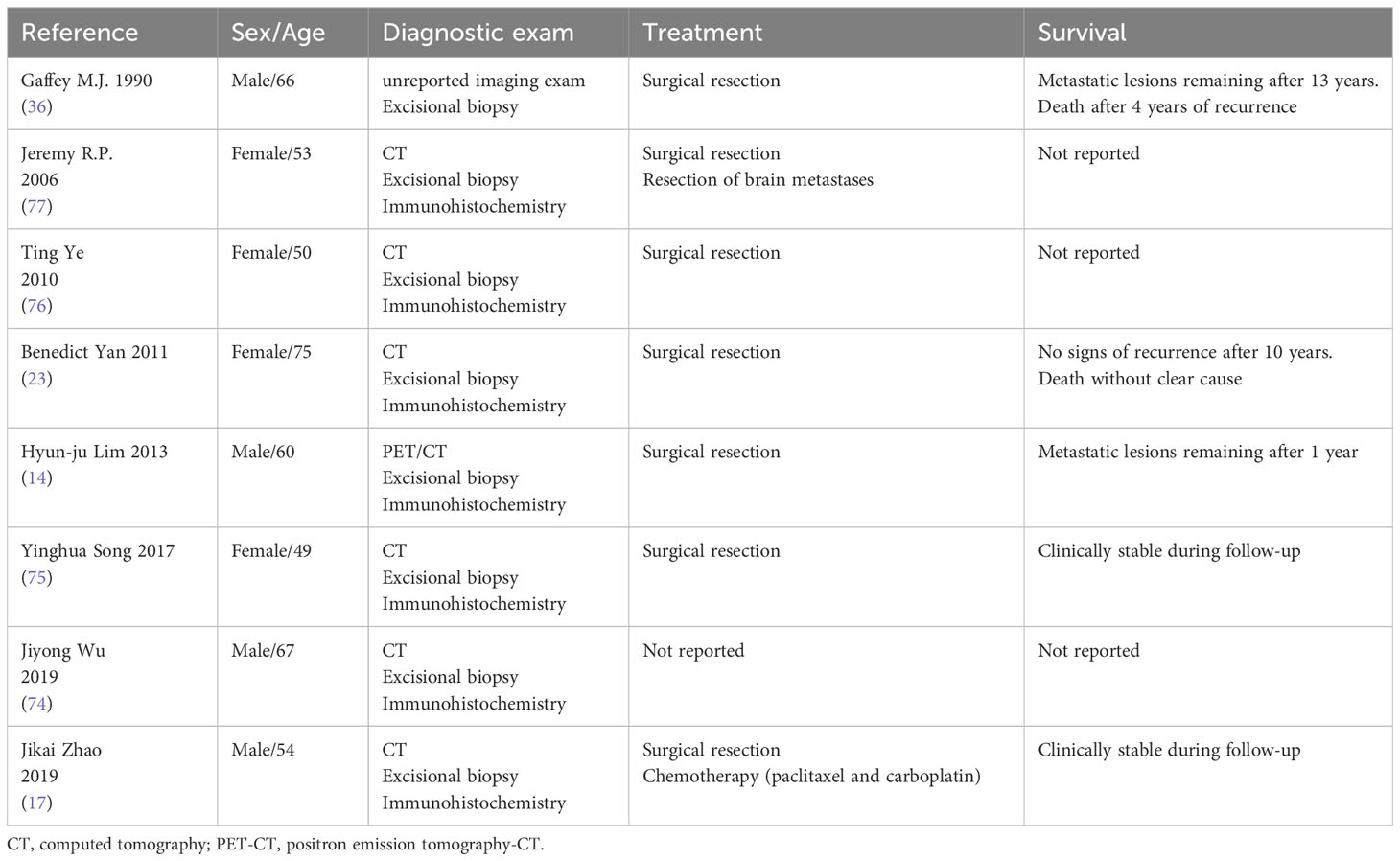
Table 2 Malignant cases of perivascular epithelioid cells (PEC) tumors reported in literature.
PEC tumors can manifest in the bladder, uterus, breast, ovary, vulva, vagina, kidney, prostate, pancreas, jejunum and soft tissues, often with benign behavior (2, 14). PEC tumors originating in soft tissues and gynecological have some findings suggestive of malignancy (8), being indicative in the presence of 2 or more criteria: > 5 cm, infiltration, high-grade atypia, necrosis, vascular invasion, mitoses > 1/50 high power fields. Some authors (80) suggest greater specificity for PEC tumors of gynecological origin with at least 4 or more of these characteristics. But WHO followed the guidance of at least 3 criteria for malignancy (81).
There are currently no well-defined diagnostic methods for malignant CCTL. Zhao et al. proposed major and minor criteria for differentiating between benign and malignant manifestations (17). Imaging characteristics are nonspecific, and the tumor can appear in any lobe (although more commonly in the bilateral lower lobes) with a well-demarcated nodule without cavitation or calcification (24). The presence of a single and intraparenchymal pulmonary nodule is common to several diseases in addition to CCTL, such as bronchogenic carcinoma and oat cell carcinoma, others tumors such as angiomyolipoma, and with metastases from clear cell carcinoma of the kidney, breast, liver, ovary, uterus and cervix, adrenal and melanoma (28, 82). Due to the nonspecificity of the image, histopathological and immunohistochemical is highly recommended for the CCTL characterization (19)
At optical microscopy the CCTL cells are round or oval, have clear cytoplasm strongly stained by PAS due to the presence of glycogen, mild nuclear pleomorphism and a characteristic plexus of prominent sinusoidal vessels, but mitotic activity and necrosis are absent (19, 24). This characteristic pattern helps to differentiate CCTL from other conditions, such as angiomyolipoma and adrenal carcinoma (28, 82).
Tumor cells show reactivity for HMB-45 in about 90% of cases, similar to most mesenchymal tumors, and do not express cytokeratins (AE1/AE3, CK7, CK8 and CK20) and epithelial membrane antigen (EMA) in 90% of cases, a fact that facilitates differentiation from other types of tumors (18, 19, 28), as observed in our case. The immunoreactivity of renal cell carcinoma to EMA, cytokeratins, CD10 and RCC are useful for the differentiation of CCTL, despite having vimentin as a positive marker in common. However, in the case of atypical melanomas, positivity to HMB-45 and S-100 present in both, does not allow elucidation of the diagnosis (28). Cathepsin K, the main marker for differentiating PEC tumors from other neoplasms, was diffusely positive in 5 cases of CCTL described in the literature (82), demonstrating the superiority of this marker over HMB-45 in differentiating CCTL from other lung tumors. Thus, the co-expression of HMB-45 and cathepsin K markers ensures a more accurate diagnosis.
Furthermore, other markers such as S-100, vimentin, CD34, Melan-A, microphthalmia factor, neuron-specific enolase, cathepsin B, and CD1a can be expressed (18, 20, 28). CD10 may be expressed in other types of non-pulmonary PEComas (83, 84). Our patient tested positive for HMB-45, Melan-A, smooth muscle actin, and CD10, and tested negative for cytokeratins.
Complete surgical resection is probably the most effective therapeutic method at present (85). Radiotherapy may be considered for patients with surgical contraindications (20). Chemotherapy should be administered for malignant manifestations, as in the reported case. CCTLs upregulate the mammalian target of rapamycin (mTOR) signaling pathway; therefore, mTOR inhibitors can be used in such cases (86, 87).
Despite being described in the literature, mitotic activity and some biomarkers may not differ between malignant and benign CCTLs. Except for lesion size, clinical characteristics and complementary examinations cannot predict a worse development. Close follow-up can identify when CCTL cases may exhibit unexpected and malignant behaviors.
Conclusion
Herein, we report the clinical evolution of a patient with malignant CCTL. Although this form of presentation is extremely rare in the literature, it is not yet possible to establish clinical, immunohistochemical, or histopathological criteria to predict the prognosis and possible malignant evolution. Although described in some studies, mitotic activity does not differentiate between benign and malignant tumors. The size of the initial lesion, presence of multiple lesions, and patient’s clinical evolution seem to be the only comparative parameters.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the proxy for the patient described in the manuscript.
Author contributions
MC: Conceptualization, Methodology, Writing – review & editing. LV: Data curation, Formal Analysis, Investigation, Writing – original draft. RM: Data curation, Formal Analysis, Investigation, Writing – original draft. ÉM: Conceptualization, Methodology, Writing – original draft. AF: Conceptualization, Methodology, Writing – original draft. SS: Conceptualization, Methodology, Writing – original draft. GS: Supervision, Visualization, Writing – review & editing. MM: Data curation, Visualization, Writing – review & editing. MZ: Data curation, Investigation, Visualization, Writing – review & editing. DQ: Conceptualization, Investigation, Supervision, Writing – review & editing.
Acknowledgments
Medical School of São Paulo State University (Unesp), Botucatu Campus
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Liebow AA, Castleman B. Benign clear cell (“sugar”) tumors of the lung. Yale J Biol Med (1971) 43:213–22.
2. Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. The 2015 world health organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer (2015) 10:1243–60. doi: 10.1097/JTO.0000000000000630
3. Shen L, Lin J, Ren Z, Wang B, Liu Y, Yuan J, et al. Clear cell tumor of the lung could be aggressive: a case report and review of the literature. J Cardiothorac Surg (2020) 15:177. doi: 10.1186/s13019-020-01224-w
4. Pann CC, Yu IT, Yang AH, Chiang H. Clear cell myomelanocytic tumor of the urinary bladder. Am J Surg Pathol (2003) 27(5):689-92. doi: 10.1097/00000478-200305000-00013
5. Vang R, Kempson RL. Perivascular epithelioid cell tumor ('PEComa’) of the uterus: a subset of HMB-45-positive epithelioid mesenchymal neoplasms with an uncertain relationship to pure smooth muscle tumors. Am J Surg Pathol (2002) 26:1–13. doi: 10.1097/00000478-200201000-00001
6. Kim H, Kim J, Lee SK, Cho EY, Cho SY. TFE3-expressing perivascular epithelioid cell tumor of the breast. J Pathol Transl Med (2019) 53:62–5. doi: 10.4132/jptm.2018.08.30
7. Anderson AE, Yang X, Young RH. Epithelioid angiomyolipoma of the ovary: a case report and literature review. Int J Gynecol Pathol Off J Int Soc Gynecol Pathol (2002) 21:69–73. doi: 10.1097/00004347-200201000-00013
8. Folpe AL, Mentzel T, Lehr H-A, Fisher C, Balzer BL, Weiss SW. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol (2005) 29:1558–75. doi: 10.1097/01.pas.0000173232.22117.37
9. Martignoni G, Pea M, Reghellin D, Zamboni G, Bonetti F. PEComas: the past, the present and the future. Virchows Arch Int J Pathol (2008) 452:119–32. doi: 10.1007/s00428-007-0509-1
10. Pan C-C, Yang A-H, Chiang H. Malignant perivascular epithelioid cell tumor involving the prostate. Arch Pathol Lab Med (2003) 127:e96–8. doi: 10.5858/2003-127-e96-MPECTI
11. Zamboni G, Pea M, Martignoni G, Zancanaro C, Faccioli G, Gilioli E, et al. Clear cell “Sugar” Tumor of the pancreas: A novel member of the family of lesions characterized by the presence of perivascular epithelioid cells. Am J Surg Pathol (1996) 20:722. doi: 10.1097/00000478-199606000-00010
12. Yanai H, Matsuura H, Sonobe H, Shiozaki S, Kawabata K. Perivascular epithelioid cell tumor of the jejunum. Pathol - Res Pract (2003) 199:47–50. doi: 10.1078/0344-0338-00353
13. Mai KT, Belanger EC. Perivascular epithelioid cell tumour (PEComa) of the soft tissue. Pathol (Phila) (2006) 38:415–20. doi: 10.1080/00313020600922504
14. Lim H, Lee HY, Han J, Choi YS, Lee KS. Uncommon of the uncommon: Malignant perivascular epithelioid cell tumor of the lung. Korean J Radiol (2013) 14:692–6. doi: 10.3348/kjr.2013.14.4.692
15. Tazelaar HD, Batts KP, Srigley JR. Primary extrapulmonary sugar tumor (PEST): a report of four cases. Mod Pathol Off J U S Can Acad Pathol Inc (2001) 14:615–22. doi: 10.1038/modpathol.3880360
16. Chakrabarti A, Bandyopadhyay M, Purkayastha B. Malignant perivascular epitheloid cell tumour (PEComa) of the lung – a rare entity. Innov Surg Sci (2017) 2:39–42. doi: 10.1515/iss-2016-0032
17. Zhao J, Teng H, Zhao R, Ding W, Yu K, Zhu L, et al. Malignant perivascular epithelioid cell tumor of the lung synchronous with a primary adenocarcinoma: one case report and review of the literature. BMC Cancer (2019) 19:235. doi: 10.1186/s12885-019-5383-0
18. Olivencia-Yurvati AH, Rodriguez AE. Clear cell “Sugar” Tumor of the lung: benign or Malignant? Int Surg (2015) 100:924–6. doi: 10.9738/INTSURG-D-14-00021.1
19. Tsilimigras DI, Bakopoulos A, Ntanasis-Stathopoulos I, Gavriatopoulou M, Moris D, Karaolanis G, et al. Clear cell “sugar tumor” of the lung: Diagnostic features of a rare pulmonary tumor. Respir Med Case Rep (2018) 23:52–4. doi: 10.1016/j.rmcr.2017.12.001
20. Ntanasis-Stathopoulos I, Kyriazoglou A, Tsilimigras DI, Tzanninis IG, Liontos M, Dimopoulos MA, et al. Clear cell sugar tumor of the lung; a systematic review for a rare entity. J BUON Off J Balk Union Oncol (2021) 26:17–32.
21. Gora-Gebka M, Liberek A, Bako W, Szumera M, Korzon M, Jaskiewicz K. The “sugar” clear cell tumor of the lung—clinical presentation and diagnostic difficulties of an unusual lung tumor in youth. J Pediatr Surg (2006) 41:e27–9. doi: 10.1016/j.jpedsurg.2006.02.035
22. Zarbis N, Barth TFE, Blumstein NM, Schelzig H. Pecoma of the lung: a benign tumor with extensive 18F-2-deoxy-d-glucose uptake. Interact Cardiovasc Thorac Surg (2007) 6:676–8. doi: 10.1510/icvts.2007.154039
23. Yan B, Yau EX, Petersson F. Clear cell ‘sugar’ tumour of the lung with Malignant histological features and melanin pigmentation – the first reported case. Histopathology (2011) 58:498–500. doi: 10.1111/j.1365-2559.2011.03773.x
24. Wang G, Zhang D, Diao X, Wen L. Clear cell tumor of the lung: a case report and literature review. World J Surg Oncol (2013) 11:247. doi: 10.1186/1477-7819-11-247
25. Gupta I, Bhalla AS, Mallick S, Mohan A, Jain D. An enigma of a rare pulmonary neoplasm in bronchial brushings. Cytopathol Off J Br Soc Clin Cytol (2021) 32:534–7. doi: 10.1111/cyt.12971
26. Yazak V, Sargin G, Yavasoglu I, Kadikoylu G, Tataroglu C, Bozkurt G, et al. Lung clear “Sugar” Cell tumor and JAK V617F positive essential thrombocythemia: a simple coincidence? Mediterr J Hematol Infect Dis (2013) 5:e2013021. doi: 10.4084/MJHID.2013.021
27. Sen S, Senturk E, Kuman NK, Pabuscu E, Kacar F. PEComa (Clear cell “Sugar” Tumor) of the lung: A benign tumor that presented with trombocytosis. Ann Thorac Surg (2009) 88:2013–5. doi: 10.1016/j.athoracsur.2009.05.041
28. Policarpio-Nicolas ML, Covell J, Bregman S, Atkins K. Fine needle aspiration cytology of clear cell “sugar” tumor (PEComa) of the lung: Report of a case. Diagn Cytopathol (2008) 36:89–93. doi: 10.1002/dc.20647
29. Becker NH, Soifer I. Benign clear cell tumor (“sugar tumor”) of the lung. Cancer (1971) 27:712–9. doi: 10.1002/1097-0142(197103)27:3<712::aid-cncr2820270330>3.0.co;2-b
30. Hoch WS, Patchefsky AS, Takeda M, Gordon G. Benign clear cell tumor of the lung. ultrastructural study. Cancer (1974) 33:1328–36. doi: 10.1002/1097-0142(197405)33:5<1328::aid-cncr2820330518>3.0.co;2-j
31. Harbin WP, Mark GJ, Greene RE. Benign clear-cell tumor (“Sugar” Tumor) of the lung: a case report and review of the literature. Radiology (1978) 129:595–6. doi: 10.1148/129.3.595
32. Makek M, Rüttner JR. Benigner hellzelliger lungentumor (≫Sugar tumor≪). Langenbecks Arch Für Chir (1979) 348:177–81. doi: 10.1007/BF01239445
33. Andrion A, Mazzucco G, Gugliotta P, Monga G. Benign clear cell (‘Sugar’) tumor of the lung A light microscopic, histochemical, and ultrastructural study with a review of the literature. Cancer (1985) 56:2657–63. doi: 10.1002/1097-0142(19851201)56:11<2657::AID-CNCR2820561121>3.0.CO;2-U
34. Nakanishi K, Kawai T, Suzuki M. Benign clear cell tumor of the lung a histopathologic study. Pathol Int (1988) 38:515–22. doi: 10.1111/j.1440-1827.1988.tb02324.x
35. Termeer A, Arkenbout PM, Lacquet LK, Cox AL. Benign clear cell tumour of the lung–intermediate filament typing as a tool in differential diagnosis. Eur Respir J (1988) 1:288–90. doi: 10.1183/09031936.93.01030288
36. Gaffey MJ, Mills SE, Askin FB, Ross GW, Sale GE, Kulander BG, et al. Clear cell tumor of the lung. A clinicopathologic, immunohistochemical, and ultrastructural study of eight cases. Am J Surg Pathol (1990) 14:248–59. doi: 10.1097/00000478-199003000-00006
37. Mishina T, Suzuki I, Fujino M, Watanabe N, Akita H, Narita Y, et al. A benign clear cell tumor of the lung that grew gradually over five years. Nihon Kyobu Shikkan Gakkai Zasshi (1995) 33:765–70.
38. Takanami I, Kodaira S, Imamura T. The use of transbronchial lung biopsy to establish a diagnosis of benign clear cell tumor of the lung: Report of a case. Surg Today (1998) 28:985–7. doi: 10.1007/s005950050268
39. Hashimoto T, Oka K, Hakozaki H, Kuraoka S, Otani S, Kawano H, et al. Benign clear cell tumor of the lung. Ultrastruct Pathol (2001) 25:479–83. doi: 10.1080/019131201753343511
40. Kula* Ö, Bekçi* TT, Şenol* T, Pazarli* P. Akciğerin iyi huylu clear cell tümörü. Turk Klin Arch Lung (2002) 3:67–9.
41. Masur Y, Becker HP, Fackeldey V. [Sugar tumor. Rare differential diagnosis of pulmonary clear cell tumor after renal carcinoma]. Urol Ausg A (2003) 42:1250–4. doi: 10.1007/s00120-003-0376-6
42. Santana ANC, Nunes FS, Ho N, Takagaki TY. A rare cause of hemoptysis: benign sugar (clear) cell tumor of the lung. Eur J Cardiothorac Surg (2004) 25:652–4. doi: 10.1016/j.ejcts.2004.01.022
43. Drebber U, Ortmann M, Kasper HU, Kern MA, Fischer UM, Nemat AT, et al. Klarzelltumor der lunge. Pathol (2005) 26:378–82. doi: 10.1007/s00292-005-0755-4
44. Jordá Aragón C, Froufe Sánchez A, Padilla Alarcón J. Benign clear cell tumor of the lung. Arch Bronconeumol (2005) 41:59. doi: 10.1016/s1579-2129(06)60396-0
45. Adachi Y, Kitamura Y, Nakamura H, Taniguchi Y, Miwa K, Horie Y, et al. Benign clear (sugar) cell tumor of the lung with CD1a expression. Pathol Int (2006) 56:453–6. doi: 10.1111/j.1440-1827.2006.01988.x
46. Kavunkal AM, Pandiyan MS, Philip MA, Parimelazhagan KN, Manipadam MT, Cherian VK. Large clear cell tumor of the lung mimicking Malignant behavior. Ann Thorac Surg (2007) 83:310–2. doi: 10.1016/j.athoracsur.2006.04.038
47. Ayadi-Kaddour A, Ben Slama S, Braham E, Abid L, Djilani H, Ismail O, et al. Clear cell tumor of the lung. A case report with review of the literature. Rev Pneumol Clin (2006) 62:395–8. doi: 10.1016/s0761-8417(06)75474-8
48. Shiran M, Tan G, Arunachalam N, Sabariah A, Pathmanathan R. Clear cell “sugar” tumour of the lung: a case report. Malays J Pathol (2006) 28:113–6.
49. Hirata T, Otani T, Minamiguchi S. Clear cell tumor of the lung. Int J Clin Oncol (2006) 11:475–7. doi: 10.1007/s10147-006-0604-3
50. Edelweiss M, Gupta N, Resetkova E. Preoperative diagnosis of clear cell “sugar” tumor of the lung by computed tomography-guided fine-needle biopsy and core-needle biopsy. Ann Diagn Pathol (2007) 11:421–6. doi: 10.1016/j.anndiagpath.2006.12.015
51. Kim WJ, Kim SR, Choe YH, Lee KY, Park SJ, Lee HB, et al. Clear cell “Sugar” Tumor of the lung: A well-enhanced mass with an early washout pattern on dynamic contrast-enhanced computed tomography. J Korean Med Sci (2008) 23:1121–4. doi: 10.3346/jkms.2008.23.6.1121
52. Nehra D, Vagefi PA, Chang H, Louissaint A, Mino-Kenudson M, Ryan DP. Clear cell sugar tumor of the lung masquerading as tuberculosis in a pediatric patient. J Thorac Cardiovasc Surg (2010) 139:e108–9. doi: 10.1016/j.jtcvs.2009.03.037
53. Mizobuchi T, Masahiro N, Iwai N, Kohno H, Okada N, Nakada S. Clear cell tumor of the lung: surgical and immunohistochemical findings. Gen Thorac Cardiovasc Surg (2010) 58:243–7. doi: 10.1007/s11748-009-0513-2
54. Vijayabhaskar R, Mehta SS, Deodhar KK, Pramesh CS, Mistry RC. PEComa of the lung. J Cancer Res Ther (2010) 6:109–11. doi: 10.4103/0973-1482.63548
55. Han B, Jiang G, Wang H, He W, Liu M, Song N. Benign clear cell tumor of the lung. Ann Thorac Surg (2010) 89:2012–4. doi: 10.1016/j.athoracsur.2009.10.017
56. Kalkanis A, Trianti M, Psathakis K, Mermigkis C, Kalkanis D, Karagkiouzis G, et al. A clear cell tumor of the lung presenting as a rapidly growing coin lesion: is it really a benign tumor? Ann Thorac Surg (2011) 91:588–91. doi: 10.1016/j.athoracsur.2010.07.043
57. Neri S, Ishii G, Aokage K, Hishida T, Yoshida J, Nishimura M, et al. Multiple perivascular epithelioid cell tumors: clear cell tumor of the lung accompanied by angiomyolipoma of the liver. Ann Thorac Cardiovasc Surg Off J Assoc Thorac Cardiovasc Surg Asia (2014) 20 Suppl:453–6. doi: 10.5761/atcs.cr.12.02179
58. Sanai Raggad S, Zouaoui A, Mehiri N, Cherif J, Zakhama H, Kchir MN, et al. [Sugar tumor]. Tunis Med (2011) 89:202–5.
59. Das S, Cherian SV, Das N, Hamarneh WA, Singh Garcha A, Preet Singh P, et al. A 52-year-old smoker with an incidental pulmonary nodule. Chest (2012) 141:1346–50. doi: 10.1378/chest.11-2242
60. Xu Q, Lu C, Li L, Xu K. Clear cell tumor of the lung. Med (Baltimore) (2016) 95:e4492. doi: 10.1097/MD.0000000000004492
61. Gunji-Niitsu Y, Kumasaka T, Kitamura S, Hoshika Y, Hayashi T, Tokuda H, et al. Benign clear cell “sugar” tumor of the lung in a patient with Birt-Hogg-Dubé syndrome: a case report. BMC Med Genet (2016) 17:85. doi: 10.1186/s12881-016-0350-y
62. Chang M, Lim D, Genovesi M. Clear cell “sugar” tumor of the lung: a case report and review of the literature. AME Case Rep (2018) 2:40. doi: 10.21037/acr.2018.08.03
63. Yeon EK, Kim JI, Won KY, Lee HN. Growth pattern change of a benign clear cell “sugar” tumor of the lung: Serial imaging surveillance over seven years. Oncol Lett (2018) 15:8652–4. doi: 10.3892/ol.2018.8391
64. Sjniari M, Miele E, Stati V, Di Cristofano C, Diso D, Pecoraro Y, et al. Early clear cell “sugar” lung cancer management: A case report and a brief literature review. Thorac Cancer (2019) 10:1289–94. doi: 10.1111/1759-7714.13077
65. Page S, Yong MS, Sinha A, Saxena P. Clear cell sugar tumour: a rare tumour of the lung. ANZ J Surg (2020) 90:E54–6. doi: 10.1111/ans.15218
66. Onorati I, Kambouchner M, Martinod E. A pigmented lung perivascular epithelioid cell tumor. Am J Respir Crit Care Med (2021) 203:1023–4. doi: 10.1164/rccm.202004-1358IM
67. Yu S, Zhai S, Gong Q, Hu X, Yang W, Liu L, et al. Perivascular epithelioid cell tumor of the lung: A case report and literature review. Thorac Cancer (2022) 13:2542–53. doi: 10.1111/1759-7714.14583
68. Donato UM, Ferguson K. Perivascular epithelioid cell tumor (PEComa) of the lung in a 56-year-old female patient: a case report. Cureus (2022) 14:e29246. doi: 10.7759/cureus.29246
69. Buero A, Tchercansky A, Olivera Lopez S, Pankl LG, Chimondeguy DJ, Lyons GA, et al. PEComa pulmonar. Med BAires (2022) 82(6):963–6.
70. Sale GF, Kulander BG. Benign clear cell tumor of lung with necrosis. Cancer (1976) 37:2355–8. doi: 10.1002/1097-0142(197605)37:5<2355::aid-cncr2820370527>3.0.co;2-4
71. Arafah MA, Raddaoui E, Alsheikh A, Hajjar WM, Alyousef F. Mimicry of sugar tumor and minute pulmonary meningothelial-like nodule to metastatic lung deposits in a patient with rectal adenocarcinoma. Ann Saudi Med (2013) 33:400–3. doi: 10.5144/0256-4947.2013.400
72. Fernandez A, Jatene FB, Zamboni M. Diagnóstico e estadiamento do câncer de pulmão. J Pneumol (2002) 28:219–28. doi: 10.1590/S0102-35862002000400006
73. Wang B, Xu X, Zhao Z. Clear cell “sugar” tumor of the lung: Diagnostic characteristics of a rare pulmonary tumor: A case report and review of literature. Med (Baltimore) (2023) 102:e33035. doi: 10.1097/MD.0000000000033035
74. Wu J, Jiang L, Zhang F, Huang Y, Wang H. Malignant perivascular epithelioid cell tumor of lung on FDG PET/CT. Clin Nucl Med (2019) 44:469–71. doi: 10.1097/RLU.0000000000002505
75. Song Y, Chen F, Zhang C, Lin X. Spindle cell subtype of pulmonary clear cell tumor with prominent calcification and Malignant potential. Thorac Cancer (2017) 8:530–4. doi: 10.1111/1759-7714.12457
76. Ye T, Chen H, Hu H, Wang J, Shen L. Malignant clear cell sugar tumor of the lung: patient case report. J Clin Oncol Off J Am Soc Clin Oncol (2010) 28:e626–628. doi: 10.1200/JCO.2010.29.6939
77. Parfitt JR, Keith JL, Megyesi JF, Ang LC. Metastatic PEComa to the brain. Acta Neuropathol (Berl) (2006) 112:349–51. doi: 10.1007/s00401-006-0105-5
78. Papla B, Demczuk S, Malinowski E. Benign clear-cell “sugar” tumor of the lung–a case report. Pol J Pathol Off J Pol Soc Pathol (2003) 54:183–5.
79. Flieder DB, Travis WD. Clear cell “sugar” tumor of the lung: association with lymphangioleiomyomatosis and multifocal micronodular pneumocyte hyperplasia in a patient with tuberous sclerosis. Am J Surg Pathol (1997) 21:1242–7. doi: 10.1097/00000478-199710000-00017
80. Schoolmeester JK, Howitt BE, Hirsch MS, Dal Cin P, Quade BJ, Nucci MR. Perivascular epithelioid cell neoplasm (PEComa) of the gynecologic tract: clinicopathologic and immunohistochemical characterization of 16 cases. Am J Surg Pathol (2014) 38:176–88. doi: 10.1097/PAS.0000000000000133
81. Bennett JA, Braga AC, Pinto A, Van de Vijver K, Cornejo K, Pesci A, et al. Uterine PEComas: A morphologic, immunohistochemical, and molecular analysis of 32 tumors. Am J Surg Pathol (2018) 42:1370–83. doi: 10.1097/PAS.0000000000001119
82. Caliò A, Mengoli MC, Cavazza A, Rossi G, Ghimenton C, Brunelli M, et al. Cathepsin K expression in clear cell “sugar” tumor (PEComa) of the lung. Virchows Arch (2018) 473:55–9. doi: 10.1007/s00428-018-2325-1
83. Ueberschaar S, Goebeler M, Kneitz H. CD10-positive cutaneous PEComa: an extremely rare skin tumour. Case Rep Dermatol (2020) 12:192–8. doi: 10.1159/000510718
84. Armah HB, Parwani AV. Malignant perivascular epithelioid cell tumor (PEComa) of the uterus with late renal and pulmonary metastases: a case report with review of the literature. Diagn Pathol (2007) 2:45. doi: 10.1186/1746-1596-2-45
85. Eldessouki I, Gaber O, Riaz MK, Wang J, Abdel Karim N. Clinical presentation and treatment options for clear cell lung cancer: university of cincinnati A case series and literature review of clear cell lung cancer. Asian Pac J Cancer Prev APJCP (2018) 19:2373–6. doi: 10.22034/APJCP.2018.19.9.2373
86. Sanfilippo R, Jones RL, Blay J-Y, Le Cesne A, Provenzano S, Antoniou G, et al. Role of chemotherapy, VEGFR inhibitors, and mTOR inhibitors in advanced perivascular epithelioid cell tumors (PEComas). Clin Cancer Res Off J Am Assoc Cancer Res (2019) 25:5295–300. doi: 10.1158/1078-0432.CCR-19-0288
Keywords: PEComa, sugar tumor, pulmonary cancer, cathepsin K, HMB-45
Citation: Campos MAG, Vasques LF, Medeiros RGd, Monteiro Cutrim ÉM, Favarin AJ, Silva SRM, Silva GEB, Moraes MPdT, Zanatta ML and Queiróz DAR (2023) Malignant lung PEComa (clear cell tumor): rare case report and literature review. Front. Oncol. 13:1260844. doi: 10.3389/fonc.2023.1260844
Received: 18 July 2023; Accepted: 30 August 2023;
Published: 20 September 2023.
Edited by:
Paolo Graziano, IRCCS Casa Sollievo della Sofferenza Hospital, ItalyReviewed by:
Anna Caliò, University of Verona, ItalyPietro Bertoglio, IRCCS Azienda Ospedaliero Universitaria di Bologna, Italy
Copyright © 2023 Campos, Vasques, Medeiros, Monteiro Cutrim, Favarin, Silva, Silva, Moraes, Zanatta and Queiróz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcos Adriano Garcia Campos, Z3lsZWFuZXNAYWx1bW5pLnVzcC5icg==
†These authors have contributed equally to this work and share first authorship