 Nikola Cihoric
Nikola Cihoric Elena Riggenbach
Elena Riggenbach Paul Martin Putora
Paul Martin Putora Fabio Dennstädt2
Fabio Dennstädt2- 1Department of Radiation Oncology, Inselspital, Bern University Hospital, and the University of Bern, Bern, Switzerland
- 2Department of Radiation Oncology, Kantonsspital St. Gallen, St. Gallen, Switzerland
Background: Digitalization has become integral to healthcare and specifically cancer treatment. Healthcare providers in oncology widely use electronic data collection and management systems in contemporary clinical practice. However, some reports point to severe problems regarding usability, which negatively impact the clinical workforce, as well as safety issues related to electronic health records, which potentially endanger patients. This systematic review aims to evaluate current scientific literature on the usability and safety aspects of electronic health records in oncology.
Methods: We conducted a systematic literature review on PubMed and Scopus to identify articles on the usability and safety aspects of electronic health records and clinical information systems utilized in oncological care. Two authors independently evaluated available literature according to predefined inclusion and exclusion criteria. Finally, we quantitatively analyzed and classified the reported findings.
Results: Our literature research strategy retrieved 1032 articles. We included seven articles for further processing. Three projects focused on the assessment of electronic health record functionality, three projects described the process of user-driven design, and one article described remediation procedures introduced to compensate inability of computer systems to adapt to user requirements.
Conclusion: Literature on the usability and safety of electronic health records in oncology is sparse. It is essential to raise awareness and start systematic activity to promote research on the usability of electronic health records in oncology.
Introduction
Several research groups have recently expressed severe concerns regarding the use of electronic health records. The most frequently reported issues were lack of interoperability (1), lack of standards, poor standards, poor implementation (2), or safety and usability issues (3–5). This directly results in quantifiable problems of data management, where the essential issues from the perspective of the clinician and researcher are duplication of clinical documentation (6), pressure to document negative findings (7), and failure to find data when and where needed, due to missing data or incorrect data entries (8). This situation severely affects healthcare workers and may result in direct patient harm (3, 9). In addition, a high-quality data foundation is a conditio sine qua non for the newest technological approaches, such as machine learning and artificial intelligence. Despite significant data-cleaning investments and other preparation processes, multiple promising technical solutions fell short when applied to broader patient cohorts (10).
The abovementioned investigations and published scientific articles are based primarily on Clinical Information Systems (CIS) and general electronic records and are not specific to oncology. However, oncology is recognized by domain specialists and international standardization groups as a complex clinical domain requiring a specialized information system profile (11–15). The need for such dedicated systems is rooted in the inherent complexity of the oncological clinical environment and the nature of information systems. A comprehensive definition of an information system includes a combination of software, hardware, and telecommunication networks to collect, process, store, and distribute valuable information. Furthermore an information system, per definition, includes formal and sociotechnical aspects of an organization (16). This implies a need for a complex interdisciplinary approach to design and development, including technical and non-technical elements (17–19).
Information systems are designed and developed based on functional and non-functional requirements. Non-functional requirements (NFR) do not relate to the specific functionality of a software system. Instead, NFR describe the system properties as a whole (20). There are six essential types of NFR, namely usability, safety, availability, scalability, effectiveness, and testability (20, 21). From the aspect of the clinicians and other healthcare workers, usability and safety interfere most with clinical routine (4, 5, 15, 22). Therefore, we conducted a systematic literature review to evaluate the current knowledge on the usability and safety of clinical software systems in oncology.
Materials and methods
Formulation of a problem and definition of methodology
To find relevant publications on the usability for clinical work and safety of Oncology Information Systems (OIS), we defined the following question based on the PICO framework (23): “Are there original research articles published in the medical literature analyzing the usability or safety of clinical information systems or electronic health records in oncology?”. To answer this question, we conducted this systematic review according to PRISMA guidelines for systematic reviews and meta-analysis (24).
Formulation of definition and search criteria
For this work, we defined software usability as “the quality of a user’s experience when interacting with products or systems” and safety as “freedom from those conditions that can cause death, injury, occupational illness, damage to or loss of information or data”. In addition, we defined oncology as a clinical field involving specialties and subspecialties focused on the prevention, screening, diagnosis, treatment, and follow-up of patients with neoplastic diseases. Furthermore, we defined an OIS as an information system developed for collecting, processing, storing, and distributing information for oncological clinical practice. Under this definition, we included all software for the general collection and management of patient data within routine clinical practice, such as electronic health records (EHR) or CIS (25). Finally, for the sake of discussion, we will consider a syntagm OIS as a synonym for both EHR and CIS. We conducted literature research without limitation to any time frame.
Eligibility criteria
Our eligibility criteria for the selection of relevant articles were as follows:
Inclusion criteria
● Original research articles evaluating or quantifying the usability of OIS for clinical work.
● Original research articles evaluating or quantifying safety issues of OIS.
● Original research articles describing the development of OIS or isolated OIS features with a focus on safety or usability.
● Original research articles about the implementation of measures intended to solve usability or safety issues of OIS.
● Only articles published in peer-reviewed journals were accepted.
● Only original research article published in English.
Exclusion criteria
● Another type of article than the original research article.
● Articles focusing on patient-oriented information systems (Electronic Patient-Reported Outcome Measures PROMs and similar).
● Articles focusing on documentation systems not intended for use in daily-clinical life (such as cancer registries).
● Articles not (or not primarily) addressing documentation of medical data from cancer patients.
● Reports analyzing IT solutions not strictly fulfilling the abovementioned definition of an OIS (e.g., software not intended for recording of data, but for processing/utilizing data recorded in EHRs (such as Clinical Decision Support Systems externally integrated into a pre-existing EHR)).
● Articles focusing on aspects other than clinical usability or safety of an OIS (including analyses of a specific data set regarding completeness or accuracy).
● Evaluation of a single feature of an OIS (e.g., Dose Prescription of Chemotherapy or radiation therapy).
Literature search
We conducted a literature search on two bibliographic platforms, PubMed and Scopus. Based on predefined definition and criteria, we executed the following query to search for publications containing keywords in the title or abstract published within the last ten years:
(“health record”[Title/Abstract] OR “oncology information system”[Title/Abstract] OR “clinical information system”[Title/Abstract]) AND (“usability”[Title/Abstract] OR “useful”[Title/Abstract] OR “safety”[Title/Abstract] OR “safe”[Title/Abstract] OR “security”[Title/Abstract] OR “quality”[Title/Abstract] OR “qualitative”[Title/Abstract]) AND (oncology[Title/Abstract] OR cancer[Title/Abstract]) AND (y_10[Filter]).
We executed the literature search on 20th of January 2023.
Selection process
Review of eligible articles was done from 20 January 2023 to 10 March 2023 by two authors (NC and FD). Articles were first screened by assessing the title and the abstract for relevance to the topic based on the eligibility mentioned above criteria. Afterward, we analyzed the full text of the preselected articles. Finally, the two authors (NC and FD) discussed the eligibility of articles in cases of discrepancies or doubt.
Results
The initial search strategy retrieved 475 articles from the PubMed database and 1017 within Scopus. After deleting duplicate records, we selected 1302 abstracts for a title and abstract screening. The title and abstract selection process revealed 64 articles eligible for full-text review. After a full-text review, the authors selected seven publications for inclusion in the study. We presented details of the selection process in Figure 1.
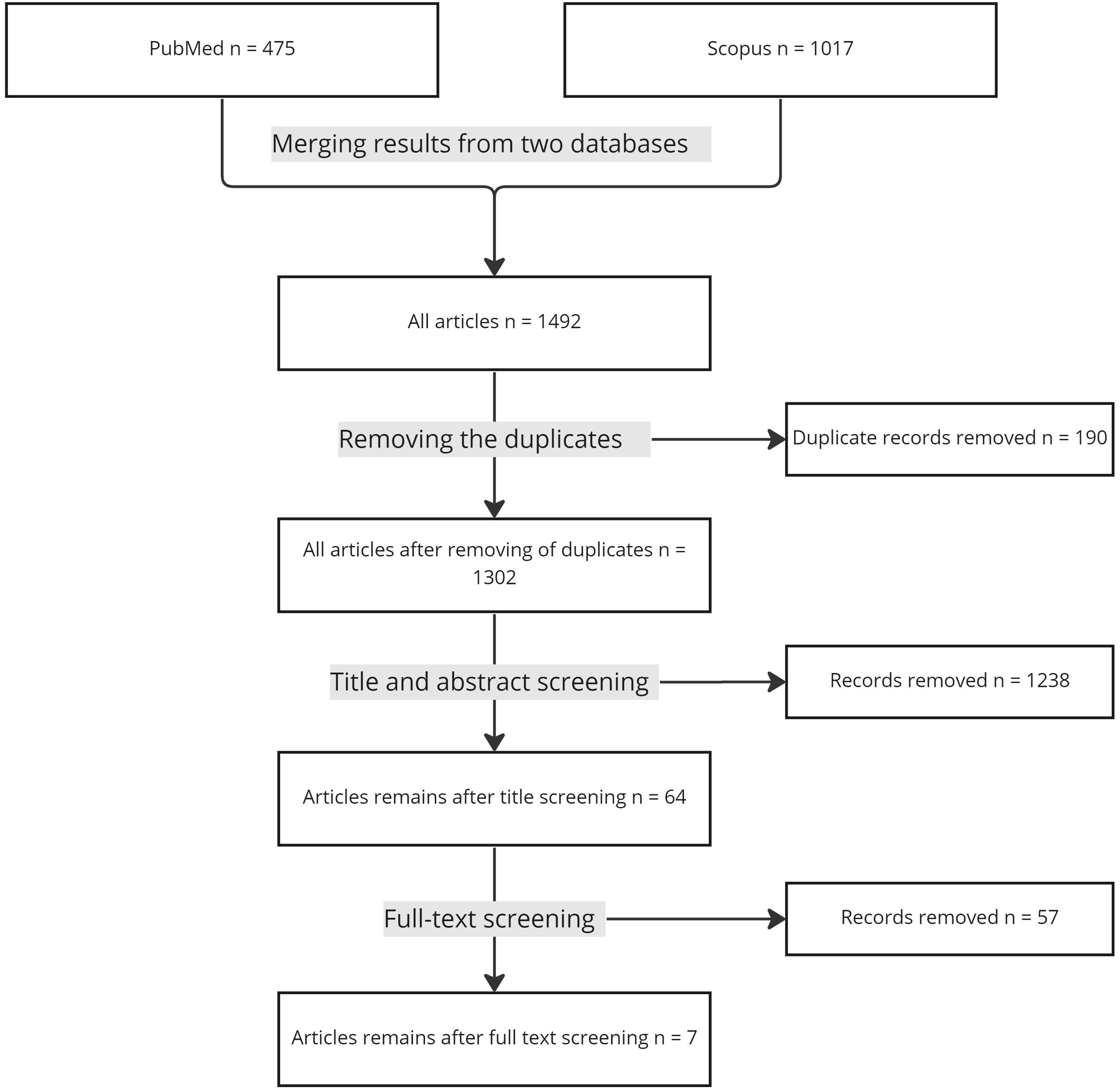
Figure 1. PRISMA Flowchart of the included studies.
Selected articles were published in the period from 2013 to 2022. The authors of five articles focused on evaluating the usability of electronic systems. One was focused on the enhancement of safety, and one was on the enhancement of usability. All of the five publications evaluating the usability of electronic systems used a survey methodology for examining the user experience. Four of them furthermore used some sort of time measurement methodology for evaluating usefulness and practicability. One publication included the percentage of medical consultations with filled clinical notes as indicator for documentation and system usage.
Two author groups described the information systems from an ear, nose, throat (ENT) cancer center perspective, two from a general oncology perspective, one focused on breast cancer, one on pediatric oncology, and one on supportive care.
The software domain (as defined by the authors) was EHR in 4 publications. The domain of the other three publications were defined as CIS, training software and presentation dashboard.
We summarized the results of the review in Table 1.
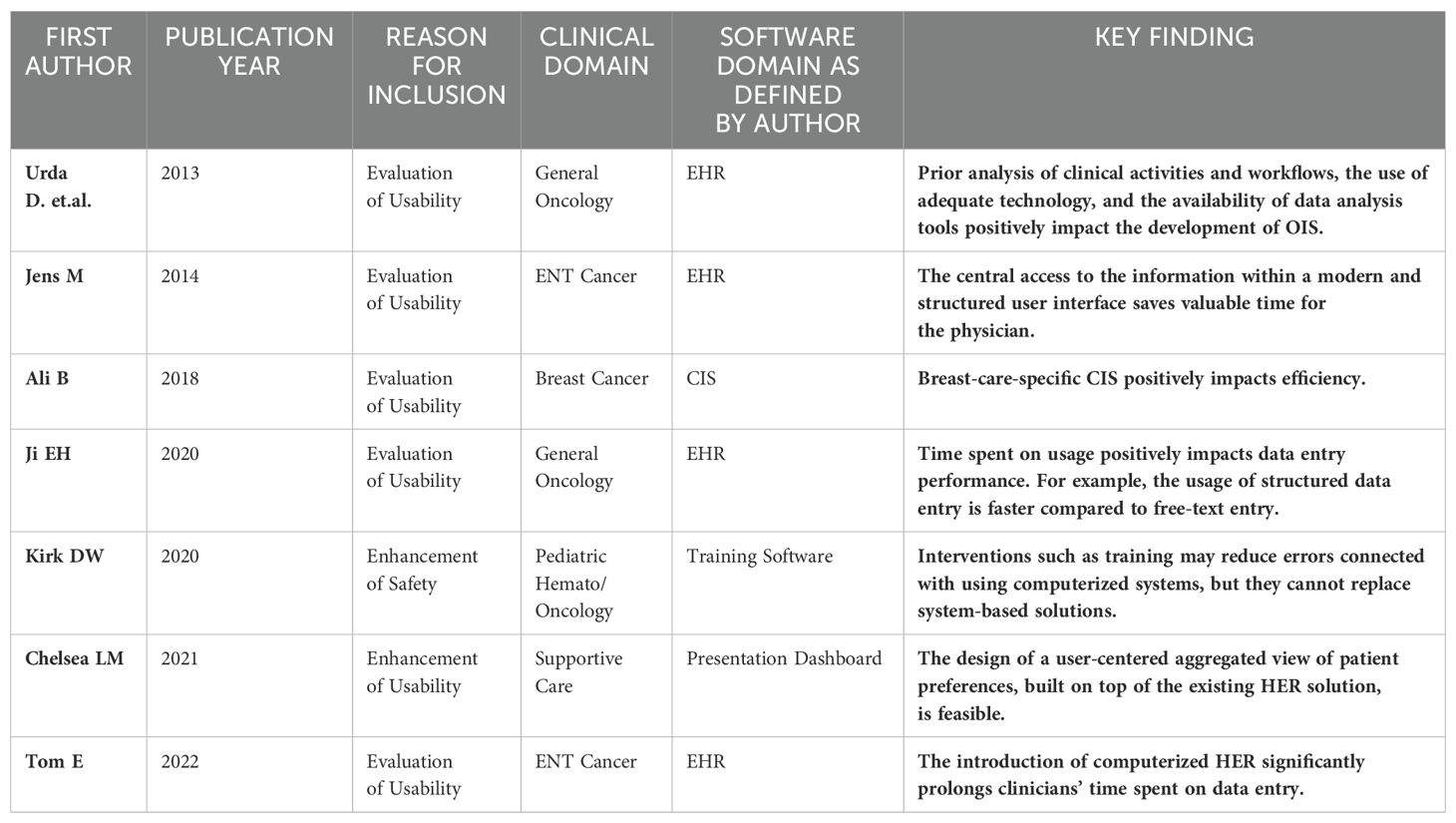
Table 1. Summary of the systematic review.
Relevant findings of selected papers
Urda D et al. described developing a web-based oncology information system designed and developed for the medical oncology department at the “Hospital Universitario Virgen de la Victoria” in Málaga, Spain, with subsequent evaluation by the users (26). The most important findings in the post-implementation review were increased data accessibility and patient progress updates. Additionally, medical practitioners perceived that OIS improved the quality of care. However, those findings contrast other objectively measured studies on general EHR, which reported adverse impacts on the patient-physician relationship to some extent. The most frequently reported problems were increased doctor computer preoccupation (27–29), affected communication flow, and challenges in verbal communication (27, 30, 31).
Meier et al. (32), from Leipzig, Germany, described developing and evaluating an EHR for data management in the ENT cancer domain called Oncoflow. A team established a set of development goals with a focus on usability. Authors compared Oncoflow on several parameters considering usability with an existing system based on the SAP(r) software. Although documentation time in Oncoflow was slightly longer, users’ evaluation reveals high satisfaction with functionalities, meeting expectations, and satisfaction with anamnesis and clinical examination modules.
Ali B at al (33). from Sydney, Australia, reported the development of a CIS specialized in breast cancer care driven by the clinical community based on agile methodology. Implementation teams set a focus of development on usability, efficiency, and adaptability. Post-implementation evaluation revealed an overall time-saving gain of 30% compared with existing enterprise EMR (Type and manufacturer not mentioned in the manuscript).
Ji EH et al. (34) from Asan Medical Center, Seoul, Republic of Korea, reported on developing structured templates for routine data collection during regular clinical care and evaluated the time and effort needed for data collection. A central finding was overall excess in the time required for documentation at the beginning, up to 70%. However, as users become more efficient after a learning period, this resulted in time gains from 1 minute and 23 seconds up to five minutes for data entry of a pathology report.
Kirk DW et al. (35), Mayo Clinic, United States, implemented a simulation-based environment with the goal of remediation of potential serious medical mistakes during a computerized order entry of chemotherapy in pediatric oncology. The study was motivated by the inability of a software vendor to adapt and change an implemented solution. Within a study, eight participants identified and mitigated an average of 5.5 out of 10 safety risks during the initial simulation and 7.4 out of 10 during a follow-up simulation.
Chelsea LM et al. (36) from Memorial Sloan Kettering Cancer Center and Weill Cornell Graduate School of Medical Science aimed to develop a usability and accessibility-focused EHR feature to enhance access to information about patient’s values and preferences. As stated by the authors, it was the first study to use a design methodology for addressing patient values for all stages of cancer care.
Tom E. et al. (37) from Radboud University Medical Center, Nijmegen, and Antoni van Leeuwenhoek Department of Head and Neck Surgery Amsterdam, Netherlands, conducted a study to quantify the time and effort spent on the EHR in ENT cancer. The authors used a cross-sectional, time-motion methodology. The results indicate significant time investment in EHR-related tasks, where 44% of initial oncological consultation and 31% of follow-up consultation duration was spent on EHR-related tasks.
Discussion
The two most critical non-functional requirements of computer systems, usability and safety, directly impact the daily work of all stakeholders of the oncology enterprise. Despite the importance of the topic and its direct implication on patient safety, health workers’ well-being, and rising healthcare costs, the data on the usability and safety of OIS is scarce. Understanding problems encountered by the clinical workforce may help shape future-oriented information systems in oncology and other clinical disciplines.
Literature on the safety and usability of EHR is scarce. There are several possible reasons for this situation. A possible consequence of the gap in evidence is a lack of appropriate methodologies, challenges in developing relevant metrics, and prohibitive licensing rules of software providers (“gag clauses” (38).) For example, a review by Rawani et al., published in 2016, reveals a general lack of data and awareness in the clinical and scientific community (4). The cited work of Rawani et al. motivated a multi-centric study, which confirmed the hypothesis of limited usability and safety of EHRs in the ambulatory emergency medicine domain (5). A recent Swiss publication on the efficiency and safety of electronic health records, directly motivated by the work of Rawani et al., tested two EHR systems where the scenarios included internal medicine specialists engaged in clinical oncology (3). The results reveal that it is basically impossible for practicing clinicians to finish their tasks error-free. However, the major drawback of the cited papers is a one-sighted view of the clinical practitioners and their interaction with computerized systems. The authors conducted the studies from the perspective of one practician and one clinical setting. It is common sense to argue that the situation in oncology is more complex and requires specific considerations. Diagnostic requires integration of a data form multiple sources (clinical imaging, pathology, laboratory, specialists investigations). Treatment requires frequently combination of surgery, radiation therapy, and medical oncology, were significant effort must be invested in organization and management. Moreover, the most crucial decision is usually made within multidisciplinary rounds.
Consequently, physicians must coordinate numerous substeps, which follow after centralized decision-making. In addition, they must report on changes to the agreed protocol and register the overall patient state and specific outcome of clinical interventions. Moreover, this relates not only to acute or subacute care but to more than 50% of patients on longitudinal care, which frequently spans decades after the treatment (39). Undoubtfully, such an environment adds a layer of complexity to the usability and safety of computerized systems.
Based on the result of the review, we may derive several hypotheses and actionable points. First, all selected articles within the discussion pointed to the necessity of closer involvement of users in the planning, design, and implementation of computerized systems for oncology. Second, flexibility and the possibility to continuously evaluate systems for usability and safety and implement changes are necessary. Third, there is very little data on the interdisciplinary aspects of software design, development, and evaluation in oncology.
Study limitations
We conducted a literature review on two bibliographic databases. Additional articles may be available through other sources. However, the two utilized databases cover the most relevant journals and reports with the most relevant publications. As in any review article, inclusion and exclusion criteria are a potential source of bias. To reduce this bias, we narrowly define our inclusion criteria and broadly define what should not be included. Such a strategy helps us to focus on one particular domain. Furthermore, an inherent bias is caused by the naming convention of the software utilized to manage clinical data. Focus on OIS has potentially excluded some articles assessing general EHR/CIS solutions, also covering the oncology domain to some extent. However, as stated in the introduction, we believe that the nature of oncological care requires dedicated systems, and it has specific usability and safety requirements.
Conclusion
This review shows a lack of specific data about OIS usability and safety in oncology. The results of our systematic review did not generate sufficient evidence for best practices and guidance on future development. However, the review is valuable for raising awareness about this critical topic, as the findings of individual publications indicate considerable issues regarding usability and safety of IT systems. Further research with systematic evaluation of EHRs and CIS is needed to better understand and overcome the existing issues of impaired safety and usability.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
NC: Conceptualization, Writing – original draft. ER: Data curation, Writing – review & editing. PP: Methodology, Writing – review & editing. FD: Methodology, Data curation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CIS, Clinical Information System; CMS, Centers for Medicare & Medicaid Services; HER, Electronic Health Record; ENT, ear, nose, throat; NFR, Non-functional requirement; OIS, Oncology Information System; PICO, Problem, Intervention, Comparison, Outcome; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
References
1. Bernstam EV, Warner JL, Krauss JC, Ambinder E, Rubinstein WS, Komatsoulis G, et al. Quantitating and assessing interoperability between electronic health records. J Am Med Inform Assoc. (2022) 29:753–60. doi: 10.1093/jamia/ocab289
2. Carter AB, de Baca ME, Luu HS, Campbell WS, Stram MN. Use of LOINC for interoperability between organisations poses a risk to safety. Lancet Digit Health. (2020) 2:e569. doi: 10.1016/S2589-7500(20)30244-2
3. Fischer S, Schwappach DLB. Efficiency and safety of electronic health records in Switzerland-A comparative analysis of 2 commercial systems in hospitals. J Patient Saf. (2022) 18:645–51. doi: 10.1097/PTS.0000000000001009
4. Ratwani R, Fairbanks T, Savage E, Adams K, Wittie M, Boone E, et al. Mind the Gap. A systematic review to identify usability and safety challenges and practices during electronic health record implementation. Appl Clin Inform. (2016) 7:1069–87.
5. Ratwani RM, Savage E, Will A, Arnold R, Khairat S, Miller K, et al. A usability and safety analysis of electronic health records: a multi-center study. J Am Med Inform Assoc. (2018) 25:1197–201. doi: 10.1093/jamia/ocy088
6. Steinkamp J, Kantrowitz JJ, Airan-Javia S. Prevalence and sources of duplicate information in the electronic medical record. JAMA Netw Open. (2022) 5:e2233348. doi: 10.1001/jamanetworkopen.2022.33348
7. Kuhn T, Basch P, Barr M, Yackel T. Medical Informatics Committee of the American College of P: Clinical documentation in the 21st century: executive summary of a policy position paper from the American College of Physicians. Ann Intern Med. (2015) 162:301–3. doi: 10.7326/M14-2128
8. Agency EM. GUIDELINE ON MISSING DATA IN CONFIRMATORY CLINICAL TRIALS. Brussels, Belgium: USE CFMPFH. Internet: European Medicines Agency (2009).
9. Jha AK, Iliff A, Chaoui AA, Defossez S, Bombaugh MC, Miller YR. A crisis in health care: a call to action on physician burnout. Waltham, MA: Massachusetts Medical Society, MHaHA, Harvard TH Chan School of Public Health, and Harvard Global Health Institute (2019).
10. Sohn E. The reproducibility issues that haunt health-care AI. Nature. (2023) 613:402–3. doi: 10.1038/d41586-023-00023-2
12. Clauser SB, Wagner EH, Aiello Bowles EJ, Tuzzio L, Greene SM. Improving modern cancer care through information technology. Am J Prev Med. (2011) 40:S198–207. doi: 10.1016/j.amepre.2011.01.014
13. Kabukye JK, de Keizer N, Cornet R. Elicitation and prioritization of requirements for electronic health records for oncology in low resource settings: A concept mapping study. Int J Med Inform. (2020) 135:104055. doi: 10.1016/j.ijmedinf.2019.104055
14. Osterman TJ, Terry M, Miller RS. Improving cancer data interoperability: the promise of the minimal common oncology data elements (mCODE) initiative. JCO Clin Cancer Inform. (2020) 4:993–1001. doi: 10.1200/CCI.20.00059
15. Hassett MJ. Usability considerations in oncology electronic medical records. J Oncol Pract. (2017) 13:539–41. doi: 10.1200/JOP.2017.024745
16. Wood-Harper AT, Antill L, Avison DE. Information systems definition: The multiview approach. Brussels, Belgium: Blackwell Scientific Publications, Ltd (1985).
17. Tang T, Lim ME, Mansfield E, McLachlan A, Quan SD. Clinician user involvement in the real world: Designing an electronic tool to improve interprofessional communication and collaboration in a hospital setting. Int J Med Inform. (2018) 110:90–7. doi: 10.1016/j.ijmedinf.2017.11.011
18. Kaplan B, Harris-Salamone KD. Health IT success and failure: recommendations from literature and an AMIA workshop. J Am Med Inform Assoc. (2009) 16:291–9. doi: 10.1197/jamia.M2997
19. Park SY, Chen Y. (2012). Adaptation as design: learning from an EMR deployment study, in: Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, , Vol. 2012. pp. 2097–106.
20. Lau F, Kuziemsky C eds. Handbook of eHealth Evaluation: An Evidence-based Approach. Victoria (BC): University of Victoria (2017).
21. Farzandipour M, Meidani Z, Nabovati E, Sadeqi Jabali M, Dehghan Banadaki R. Technical requirements framework of hospital information systems: design and evaluation. BMC Med Inform Decis Mak. (2020) 20:61. doi: 10.1186/s12911-020-1076-5
22. Lee Y, Bahn S, Shin GW, Jung MY, Park T, Cho I, et al. Development of safety and usability guideline for clinical information system. Med (Baltimore). (2021) 100:e25276. doi: 10.1097/MD.0000000000025276
23. Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. (2007) 7:16. doi: 10.1186/1472-6947-7-16
24. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. (2021) 134:103–12. doi: 10.1016/j.jclinepi.2021.02.003
25. Electronic Health Records . Available online at: https://www.cms.gov/Medicare/E-Health/EHealthRecords. (accessed January, 5 2023).
26. Urda D, Ribelles N, Subirats JL, Franco L, Alba E, Jerez JM. Addressing critical issues in the development of an Oncology Information System. Int J Med Inform. (2013) 82:398–407. doi: 10.1016/j.ijmedinf.2012.08.001
27. Greatbatch D, Heath C, Campion P, Luff P. How do desk–top computers affect the doctor–patient interaction? Fam Pract. (1995) 12:32–6.
28. Booth N, Robinson P. Interference with the patient–doctor relationship–the cultural gap? Lessons from observation. Stud Health Technol Inform. (2002) 87:6–9.
29. Booth A, Lecouteur A, Chur–Hansen A. The impact of the desktop computer on rheumatologist–patient consultations. Clin Rheumatol. (2013) 32:391–3. doi: 10.1007/s10067-012-2140-z
30. Als AB. The desk–top computer as a magic box: patterns of behavior connected with the desk–top computer, GPs’ and patients’ perceptions. Fam Pract. (1997) 14:17–23. doi: 10.1093/fampra/14.1.17
31. Shachak A, Hadas–Dayagi M, Ziv A, Reis S. Primary care physicians’ use of an electronic medical record system: a cognitive task analysis. J Gen Intern Med. (2009) 24:341–8. doi: 10.1007/s11606-008-0892-6
32. Meier J, Boehm A, Kielhorn A, Dietz A, Bohn S, Neumuth T. Design and evaluation of a multimedia electronic patient record “oncoflow” with clinical workflow assistance for head and neck tumor therapy. Int J Comput Assist Radiol Surg. (2014) 9:949–65. doi: 10.1007/s11548-014-0988-x
33. Besiso A, Patrick JD, Dip G, Ho V, Cheng Y. The impact of an enterprise electronic medical record (EEMR) model vs a clinical information system (CIS) model on usability, efficiency, and adaptability. AMIA Annu Symp Proc. (2018) 2018:242–51.
34. Hwang JE, Seoung BO, Lee SO, Shin SY. Implementing structured clinical templates at a single tertiary hospital: survey study. JMIR Med Inform. (2020) 8:e13836. doi: 10.2196/13836
35. Wyatt KD, Freedman EB, Arteaga GM, Rodriguez V, Warad DM. Computer–based simulation to reduce EHR–related chemotherapy ordering errors. Cancer Med. (2020) 9:8844–51. doi: 10.1002/cam4.v9.23
36. Michael CL, Mittelstaedt H, Chen Y, Desai AV, Kuperman GJ. Applying user–centered design in the electronic health record (EHR) to facilitate patient–centered care in oncology. AMIA Annu Symp Proc. (2020) 2020:833–9.
37. Ebbers T, Kool RB, Smeele LE, Takes RP, van den Broek GB, Dirven R. Quantifying the electronic health record burden in head and neck cancer care. Appl Clin Inform. (2022) 13:857–64. doi: 10.1055/s-0042-1756422
38. Ratwani RM, Hodgkins M, Bates DW. Improving electronic health record usability and safety requires transparency. JAMA. (2018) 320:2533–4. doi: 10.1001/jama.2018.14079
Keywords: electronic health record, usability, safety, oncology, oncology information systems
Citation: Cihoric N, Riggenbach E, Putora PM and Dennstädt F (2024) Safety and usability of oncology information systems – a systematic review. Front. Oncol. 14:1231757. doi: 10.3389/fonc.2024.1231757
Received: 02 June 2023; Accepted: 07 November 2024;
Published: 28 November 2024.
Edited by:
Olgun Elicin, University Hospital Bern, SwitzerlandReviewed by:
Joaquim Carreras, Tokai University, JapanDavid Schwartz, University of Tennessee Health Science Center (UTHSC), United States
Copyright © 2024 Cihoric, Riggenbach, Putora and Dennstädt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nikola Cihoric, bmlrb2xhLmNpaG9yaWNAZ21haWwuY29t