 Enrique Lopez Aguilar1*Angeles Del Campo Martinez1Ana Rioscovian Soto1Karen Ayala-Contreras1
Enrique Lopez Aguilar1*Angeles Del Campo Martinez1Ana Rioscovian Soto1Karen Ayala-Contreras1 Marta Zapata-Tarrés2
Marta Zapata-Tarrés2 Miguel Enrique Cuéllar Mendoza2Yadira Betanzos Cabrera1Regina Zevada-Mosti2Sheyla Payán Romo1
Miguel Enrique Cuéllar Mendoza2Yadira Betanzos Cabrera1Regina Zevada-Mosti2Sheyla Payán Romo1 Oscar Omar Esquer Cota1
Oscar Omar Esquer Cota1 Pamela Zazueta Mérida1
Pamela Zazueta Mérida1 Susana Elizabeth Anaya Aguirre1Emmanuel Rolando Rodríguez Cedeño1Maria De Lourdes Gutiérrez Rivera1Jorge Alfonso Martín Trejo1
Susana Elizabeth Anaya Aguirre1Emmanuel Rolando Rodríguez Cedeño1Maria De Lourdes Gutiérrez Rivera1Jorge Alfonso Martín Trejo1 Elvia Yaroslab Mayorga Castillo1Carolina Contreras Camacho1Elio Aaron Reyes Espinoza1Norma Eryca Alatoma Medina1Hector Manuel Tiznado García1
Elvia Yaroslab Mayorga Castillo1Carolina Contreras Camacho1Elio Aaron Reyes Espinoza1Norma Eryca Alatoma Medina1Hector Manuel Tiznado García1 Christian Santillán Ávila1Jose Maria Sepúlveda Núñez1
Christian Santillán Ávila1Jose Maria Sepúlveda Núñez1 Sadya Fuerte Olvera1Lizeth Rodríguez Brindis1Jose Alvaro Parra Salazar1Lilia Adela García Stivalet1Lizette Bojórquez Steffani1Roberto Abraham Betancourt Ortiz1
Sadya Fuerte Olvera1Lizeth Rodríguez Brindis1Jose Alvaro Parra Salazar1Lilia Adela García Stivalet1Lizette Bojórquez Steffani1Roberto Abraham Betancourt Ortiz1 Aurora Treviño1Julio Mercado Castruita1Rocio Aburto Mejia1Adrian Jimenez Salinas1Francisco Javier Valdivia Ibarra1Fabiana Maribel Zepeda Arias1Ana Leticia Figueroa Rosas1Desiree Sagarnaga Durante1Fatima Borrego Perez1Jorge Humberto Urbina Ochoa1Gustavo Ignacio Prieto Torres1Jose De Jesus Chavez Martenez1Juan Gilberto Perez Soltero1
Aurora Treviño1Julio Mercado Castruita1Rocio Aburto Mejia1Adrian Jimenez Salinas1Francisco Javier Valdivia Ibarra1Fabiana Maribel Zepeda Arias1Ana Leticia Figueroa Rosas1Desiree Sagarnaga Durante1Fatima Borrego Perez1Jorge Humberto Urbina Ochoa1Gustavo Ignacio Prieto Torres1Jose De Jesus Chavez Martenez1Juan Gilberto Perez Soltero1 Guillermo Careaga Reyna1Ma. Teresa Cristina Ramos Hernandez1Rocio Cardenas Navarrete1Elsa Fabiola Gonzalez Rosas1Adolfo Pineda Gordillo1Cecilia Ochoa-Drucker2Enrique López Facio1
Guillermo Careaga Reyna1Ma. Teresa Cristina Ramos Hernandez1Rocio Cardenas Navarrete1Elsa Fabiola Gonzalez Rosas1Adolfo Pineda Gordillo1Cecilia Ochoa-Drucker2Enrique López Facio1 Mirna Guadalupe Rios Osuna1
Mirna Guadalupe Rios Osuna1 Claudia Selene Portillo Zavala1
Claudia Selene Portillo Zavala1 Sergio Ruben Cobo Ovando1A. B. Aguilar Román1Brenda Chávez Liñán1Benjamin Arroyo Acosta1Luis E. Bernabe-Gaspar2
Sergio Ruben Cobo Ovando1A. B. Aguilar Román1Brenda Chávez Liñán1Benjamin Arroyo Acosta1Luis E. Bernabe-Gaspar2 A. B. Rivera Ramírez1D. A. Malváez Estrada1E. Ulloa Salaices1V. P. Silva Delfín1G. González Villarreal1M. Estolando Ayón1Aaron Muñoz Flores1E. F. Ortiz de la O1H. J. Ortiz Trujillo1
A. B. Rivera Ramírez1D. A. Malváez Estrada1E. Ulloa Salaices1V. P. Silva Delfín1G. González Villarreal1M. Estolando Ayón1Aaron Muñoz Flores1E. F. Ortiz de la O1H. J. Ortiz Trujillo1 José Luis Moreno Domínguez1Miguel Lopez Suastegui1L. Gallegos Cruz1Celida Duque-Molina1
José Luis Moreno Domínguez1Miguel Lopez Suastegui1L. Gallegos Cruz1Celida Duque-Molina1- 1Coordinación de Atención Oncológica, Instituto Mexicano del Seguro Social, Ciudad de México, Mexico
- 2Coordinación de Investigación, Fundación IMSS, A.C, Ciudad de México, Mexico
Introduction: The Mexican Social Security Institute (IMSS) was created in 1943 as the main public institution in Mexico.
Methods: In 2020, the OncoCREAN (Centros de Referencia Estatal para la Atención del Niño y de la Niña con Cáncer) strategy was established and consists of reference centers of Pediatric Oncology created to provide equitable access to pediatric patients with cancer in Mexico and toimprove the disease survival through standardized immunophenotyping, harmonized diagnosis, homogenized treatment, staff training, and complication response.
Results: At 12 months of follow-up, overall survival is 89.9% in pediatric patients with acute lymphoblastic leukemia; we have no early death, and the main cause of death is still infection.
Discussion: The current procedure in terms of immune molecular diagnosis is to send samples to the first national system of samples reference for the immunological diagnosis of leukemias based on immunophenotyping in the Cytomics Laboratory of the IMSS Research Center in Puebla, as a strong collaborative alliance. We present a narrative description of the strategy as preliminary results.
1 Introduction
The Mexican Social Security Institute (IMSS) was created in 1943 as the main public social institution with more than 80 million beneficiaries, including pediatric patients 18 years old or younger (1, 2). Forty-five percent of Mexican pediatric oncology patients are treated in IMSS, and the rest are treated in other social security institutions and the private system (3, 4). A national strategy was implemented through the IMSS National Oncologic Coordination to achieve equitable access and decreased mortality, regardless of the geographic area where patients live (1).
Pediatric cancer is a complex disease above all in the diagnostic and induction phases when oncological emergencies are more common and fatal. However, in the maintenance phase, patients are more stable, and treatment is generally less toxic. In countries like Chile, the first phase of treatment is given in the capital in a specialized hospital, and the maintenance phase is given in general hospitals closer to the patients’ home. Acute lymphoblastic leukemia (ALL) represents 48% of cancer diagnoses in childhood in Mexico. Overall survival is, on average, 57% in Mexico compared to 80%–90% in developed countries (5). For that reason, the strategy was implemented.
2 The OncoCREAN strategy
In the past, there were four main centers of clinical care for pediatric patients with cancer: two in Mexico City, one in Monterrey, and one in Guadalajara. The current organization involves the maintenance of these four centers with the addition of 32 areas inside pediatric hospitals where patients who already have their oncological diagnosis as well as the initial surgical treatment or induction therapy are treated. The implementation of the 32 centers was gradually carried out in approximately 24 months. Before 2020, the diagnosis of leukemia was done in each hospital when it was possible, or samples were sent to surrogate laboratories. Results in terms of survival toxicity and quality of life were local and not reported as an institutional study. Nowadays, all centers that receive patients with suspected leukemia are approached from the clinical aspect in the OncoCREAN. The bone marrow aspiration, as well as the staining, is done in the OncoCREAN to make the morphological diagnosis. In the same surgical time, the cytometry analysis sample is taken and sent to the West Biomedical Research Center (CIBIOR) located in the central area of Mexico. Samples arrive in less than 24 h via courier and are processed. The current procedure in terms of immune molecular diagnosis is to send samples to the first national system of samples reference for the immunological diagnosis of leukemias based on immunophenotyping in the Cytomics Laboratory of the IMSS Research Center in Puebla, as a strong collaborative alliance with the National Council of Humanities, Sciences, and Technologies (CONAHCYT). Thus, with the financial co-support from CONAHCYT and a new paradigm of research, the Cytomics Laboratory has been responsible for systematic sample preservation and exhaustive studies, for both diagnosis and measurable residual disease (MRD) as established international treatment protocols. Cytogenetics, according to the protocol, considers a DNA index of 1.16 or more and the translocation t (12,21) (ETV6-RUNX1) as provisionally classified as low-risk ALL. Patients with t (9,22) (BCR-ABL1) were considered to suffer from high-risk ALL, and the remaining patients were provisionally classified as having standard-risk (intermediate-risk) ALL.
The final risk status was determined based on the detection of MRD. Patients presenting with an MRD of 1% or more within the bone marrow aspirate on day 19 of remission induction or 0.10% to 0.99% after completion of 6 weeks of induction therapy were considered to have standard-risk ALL. MRD values of 1% or more after the completion of induction therapy indicated high-risk ALL. Immunophenotyping and classification of acute leukemia: BM samples were stained and acquired for flow cytometry analysis according to Euro Flow™ guidelines. First, samples were stained using the Acute Leukemia Orientation Tube (ALOT) to determine the lineage of immature blast cell populations. We classified AL into five review categories according to the affected cell lineage: Pro B-ALL (CD34+ CD19+ cyCD79a+), Pro B–Pre B-ALL (CD34−/+ CD19+ cyCD79a+), Pre B-ALL (CD34− CD19+ cyCD79a+), TALL (cyCD3+ smCD3lo CD7+), and AML (cyMPO+ or CD7+). Once the malignant hematopoietic lineage is identified, complementary antibody panels were applied (BCPALL, T-ALL, and AML). Sample acquisition was conducted using BD FACSCanto II or BD FACSLyric cytometers. Analysis of flow cytometry data was performed using Infinicyt 2.0 software.
When the diagnosis is made, each patient’s results are sent to the OncoCREAN in 24–72 h, the patient is stratified, and the induction therapy is planned and applied in one of the OncoCREAN centers. In January 2022, IMSS OncoCREAN started the implementation of the Total Therapy XV of St. Jude (TTXV) for leukemias that offers total access to and homogenization and decentralization of the treatment at a national level (6). The decision to choose the TTXV St Jude leukemia protocol was supported by the fact that Mexican pediatric oncologists, hematologists, and health professionals have strong experience due to the previous use of the Total XIII St Jude Leukemia protocol at a national level. All patients received the prednisone induction phase. Risk stratification was done as established in the TTXV protocol. Induction ended on day 33, while in this first-line treatment group, no patient received cranial radiotherapy. Toxicity was analyzed according to the National Cancer Institute classification.
The 36 centers have a pediatric oncologist/hematologist, a trained oncological nurse, and the resources to treat these diseases as well as their complications. All centers are connected to the National Coordination, having weekly communication to present new cases and reference stable patients. We are aware that, in the review, surveillance of all aspects of a patient’s life must be implemented, including how we evaluate the diagnosis, the timely treatment, and the presence of complications, nutrition, and psychological support. Pediatric oncologists/hematologists are the only ones responsible for the filing of documentations.
3 Results
So far, follow-up information is only 12 months. There were 809 patients, and the median age was 8.39 years old, with a minimum age of 4 months and a maximum age of 17 years. There were 471 male patients, with 468 being B-cell leukemias; 333 patients were classified as high-risk patients, 3 patients had central nervous system infiltration or mediastinal mass, and 6 patients relapsed. Overall survival is 89.9%; 82 patients died, the leading cause of which is infection. No deaths during the induction phase (early mortality) were reported.
There have been 72 online sessions with a frequency of one per week, in which all OncoCREANs have participated. Training in the protocol, the logistics of transporting samples, and the interpretation of diagnostic tests have been carried out. The current census indicates 91 oncologists and pediatric hematologists.
From CIBIOR, 275 patients were studied. For logistics, the country is divided into four regions (North, Northwest, Central, and South). Most of our patients corresponded to Pro B or Pro B–Pre B cell leukemia as seen in Figure 1.
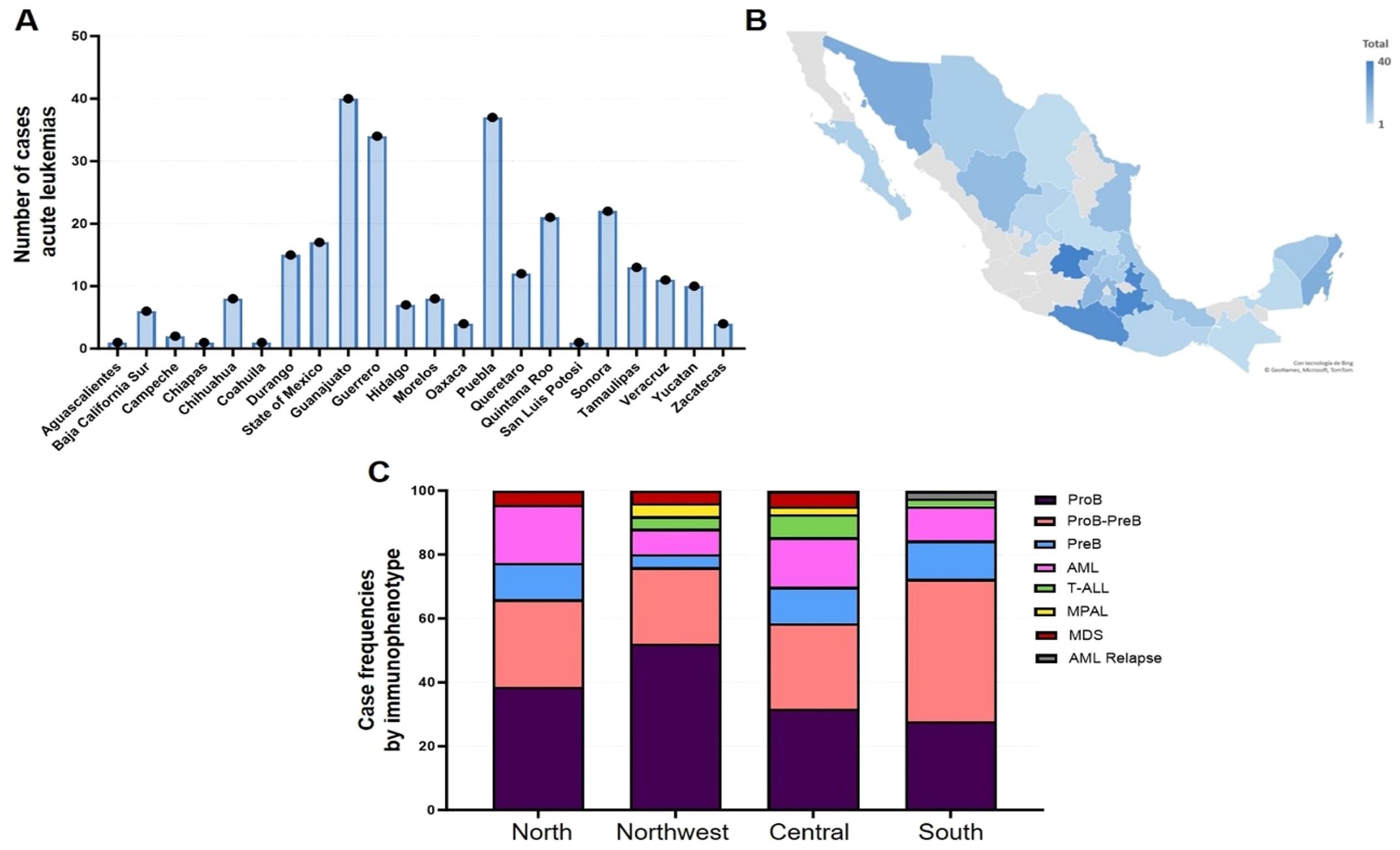
Figure 1. (A, B) represent distribution by states. (C) shows the leukemia by types and regions. AML, acute lymphoblastic leukemia; T-ALL, T-acute lymphoblastic leukemia; MPAL, mixed phenotype acute leukemia; MSD, myelodysplastic syndrome; AML relapse, acute lymphoblastic leukemia relapse.
4 Discussion
In Mexico, this is a historic initiative because it brings patients with cancer equitable access to a standardized care protocol not only in the same care center but also at a national level in all IMSS hospitals. Considering that this has been described as a critical factor contributing to the increased survival of patients with ALL, we are sure that this strategy is changing the prognosis of this disease (7).
Death due to toxicity continues to be a determining factor, which is why in developing countries, such adaptations to chemotherapy protocols are made (7). It is imperative to intensify medical and nursing training of all OncoCREANs, emphasizing Golden Hour Pediatric Early Warning Score (PEWS) and the vascular line manual, which are strategies focused on early care of complications associated with treatment toxicity.
From 1950 to date, we have seen how systematization in treating patients with cancer has positively impacted survival. Despite this, we know that there are still global disparities in access to high-quality treatment for children with cancer (8). This work can be the beginning of a later analysis of how including patients with ALL in a standardized treatment protocol can allow us to make an individualized treatment according to the assigned risk and decrease the treatment’s long-term effects (6–10).
It would be the first time in Mexico that an institutional treatment strategy implemented at a national level is followed up with two main objectives: assistance and information generation for future research. In the IMSS, successful cooperation, central registration, precision, and quality of diagnosis and prognosis tests are changing the epidemiology of pediatric acute leukemias as well as the work organization. Analyzing the very preliminary information we have, early mortality is controlled probably due to the very close supervision of these patients in all the sections of health centers (emergency room, hospitalization, and outpatient clinic).
Considering the scalability of the strategy, we must consider the human infrastructure that at this moment at IMSS consists of 217 pediatric oncologists and 142 hematologists. On the other hand, cases of ALL were 800 per year with the number of cases increasing. The OncoCREAN system is designed to give attention to patients in the maintenance phase in which complications are less common to appear. This strategy has the advantage of patients being close to their homes; thus, the abandonment rate is decreasing (data not shown). Quality of life and school attendance must be studied in the future as social indicators of patient follow-up.
A formal survival analysis including all the variables associated with survival of patients with pediatric ALL was carried out and will be reported in a future study.
5 Conclusion
Implementing strategies to provide standardized diagnosis, prognosis, and treatment to patients with ALL are essential to improve survival (11). Moreover, training in support therapies for the care of complications secondary to treatment toxicity is indispensable. In review, OncoCREAN’s strategy in Mexico based on care and scientific research is bringing precision oncology closer to our pediatric population suffering from leukemia. This project has its share of challenges: this is one of the first attempts by IMSS to make a cooperative project at the national level at different centers, the time for the referral of samples at the CIBIOR, and the standardization of sample sending data. The strengths of this program include the fact that a national referral center for molecular diagnosis was made at the CIBIOR and the standardization of TTXV for the clinical centers.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
ELA: Conceptualization, Formal Analysis, Writing – original draft, Writing – review & editing, Data curation, Investigation, Methodology, Project administration, Software, Supervision, Visualization. ADC: Conceptualization, Formal Analysis, Writing – original draft, Data curation, Investigation, Methodology, Project administration, Supervision. ARS: Conceptualization, Data curation, Investigation, Methodology, Supervision, Validation, Writing – original draft. KAC: Data curation, Investigation, Formal Analysis, Writing – original draft. MZT: Conceptualization, Writing – review & editing, Formal Analysis, Writing – original draft. MC: Data curation, Formal Analysis, Investigation, Writing – original draft. YB: Investigation, Conceptualization, Writing – review & editing. RZM: Data curation, Software, Writing – original draft. SP: Data curation, Writing – review & editing. OE: Data curation, Writing – review & editing. PZ: Data curation, Writing – review & editing. SA: Data curation, Writing – review & editing. ERC: Data curation, Writing – review & editing. MG: Data curation, Writing – review & editing. JMT: Data curation, Writing – review & editing. EM: Data curation, Writing – review & editing. CC: Data curation, Writing – review & editing. ERE: Data curation, Writing – review & editing. NA: Data curation, Writing – review & editing. HT: Data curation, Writing – review & editing. CS: Data curation, Writing – review & editing. JS: Data curation, Writing – review & editing. SF: Writing – review & editing, Data curation. LR: Writing – review & editing, Data curation. JAPS: Writing – review & editing, Data curation. LGS: Writing – review & editing, Data curation. LBS: Data curation, Writing – review & editing. RB: Data curation, Writing – review & editing. AT: Data curation, Writing – review & editing. JMC: Data curation, Writing – review & editing. RA: Data curation, Writing – review & editing. AJ: Data curation, Writing – review & editing. FV: Data curation, Writing – review & editing. FZ: Data curation, Writing – review & editing. AF: Data curation, Writing – review & editing. DS: Data curation, Writing – review & editing. FB: Data curation, Writing – review & editing. JU: Data curation, Writing – review & editing. GP: Data curation, Writing – review & editing. JC: Data curation, Writing – review & editing. JGPS: Data curation, Writing – review & editing. GC: Data curation, Writing – review & editing. MRH: Data curation, Writing – review & editing. RC: Data curation, Writing – review & editing. EG: Data curation, Writing – review & editing. AP: Data curation, Writing – review & editing. COD: Data curation, Investigation, Writing – original draft, Writing – review & editing. EL: Data curation, Writing – review & editing. MRO: Data curation, Writing – review & editing. CP: Data curation, Writing – review & editing. SC: Data curation, Writing – review & editing. AA: Data curation, Writing – review & editing. BC: Data curation, Writing – review & editing. BA: Data curation, Writing – review & editing. LBG: Data curation, Writing – review & editing. AR: Data curation, Writing – review & editing. DM: Data curation, Writing – review & editing. EU: Data curation, Writing – review & editing. VS: Data curation, Writing – review & editing. GG: Data curation, Writing – review & editing. ME: Data curation, Writing – review & editing. AM: Data curation, Writing – review & editing. EO: Data curation, Writing – review & editing. HO: Data curation, Writing – review & editing. JMD: Data curation, Writing – review & editing. ml: Data curation, Writing – review & editing. LGC: Data curation, Writing – review & editing. CD-M: Data curation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was co-supported by the National Council of Humanities, Science, and Technology (CONAHCYT), Grant FORDECYT-PRONACES 302994 to RP, and by the Translational Research Program, Coordinación de Investigación en Salud, Instituto Mexicano del Seguro Social. For publication fees, Servier provide funding. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer JF declared a shared affiliation with the authors to the handling editor at the time of review.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Pérez-Cuevas R, Doubova SV, Zapata-Tarrés M, Flores-Hernández S, Frazier L, Rodríguez-Galindo C, et al. Scaling up cancer care for children without medical insurance in developing countries: The case of Mexico. Pediatr Blood Cancer. (2013) 60:196–203. doi: 10.1002/pbc.24265
2. Gómez Dantes O, Sesma S, Becerrril VM, Knaul FM, Arreola H, and Frenk J. Sistema de salud de México Vol. 53. Salud Publica Mex (2011) p. s220–32.
3. Oncología pediátrica (2023). Available online at: http://www.imss.gob.mx/oncologia-pediatrica (Accessed March 04, 2023).
4. El IMSS busca alcanzar 90 por ciento de sobre vida en niños con cáncer (2023). Available online at: https://www.imss.gob.mx/prensa/archivo/202202/078 (Accessed March 04, 2023).
6. Pui CH, Campana D, Pei D, Bowman WP, Sandlund JT, Kaste SC, et al. Treating childhood acute lymphoblastic leukemia without cranial irradiation. N Engl J Med. (2009) 360:2730–41. doi: 10.1056/NEJMoa0900386
7. Lam CG, Howard SC, Bouffet E, and Pritchard-Jones K. Science and health for all children with cancer. Science. (2019) 363:1182–6. doi: 10.1126/science.aaw4892
8. Pritchard-Jones K, Pieters R, Reaman GH, Hjorth L, Downie P, Calaminus G, et al. Sustaining innovation and improvement in the Treatment of childhood cancer: lessons from high-income countries. Lancet Oncol. (2013) 14:e95–e103. doi: 10.1016/S1470-2045(13)70010-X
9. Hunger SP, Sung L, and Howard SC. Treatment Strategies and regimens of graduated intensity for Childhood ALL in LIC: a proposal. Pediatr Blood Cancer. (2009) 52:559–65. doi: 10.1002/pbc.21889
10. Strahlendorf C, Pole JD, Barber R, Dix D, Kulkarni K, Martineau E, et al. Enrolling children with acute lymphoblastic leukemia on a Clinical Trial Improves event-free Survival: A Population-based study. Br J Cancer. (2018), 1–6. doi: 10.1038/bjc.2017.462
Keywords: leukemia, Mexico, acute lymphoblastic leukemia, middle income countries (MIC), pediatric cancer
Citation: Lopez Aguilar E, Del Campo Martinez A, Rioscovian Soto A, Ayala-Contreras K, Zapata-Tarrés M, Cuéllar Mendoza ME, Betanzos Cabrera Y, Zevada-Mosti R, Payán Romo S, Esquer Cota OO, Zazueta Mérida P, Anaya Aguirre SE, Rodríguez Cedeño ER, Gutiérrez Rivera ML, Martín Trejo JA, Mayorga Castillo EY, Contreras Camacho C, Reyes Espinoza EA, Alatoma Medina NE, Tiznado García HM, Santillán Ávila C, Sepúlveda Núñez JM, Fuerte Olvera S, Rodríguez Brindis L, Parra Salazar JA, García Stivalet LA, Bojórquez Steffani L, Betancourt Ortiz RA, Treviño A, Mercado Castruita J, Aburto Mejia R, Jimenez Salinas A, Valdivia Ibarra FJ, Zepeda Arias FM, Figueroa Rosas AL, Sagarnaga Durante D, Borrego Perez F, Urbina Ochoa JH, Prieto Torres GI, Chavez Martenez JJ, Perez Soltero JG, Careaga Reyna G, Ramos Hernandez MTC, Cardenas Navarrete R, Gonzalez Rosas EF, Pineda Gordillo A, Ochoa-Drucker C, López Facio E, Rios Osuna MG, Portillo Zavala CS, Cobo Ovando SR, Aguilar Román AB, Chávez Liñán B, Arroyo Acosta B, Bernabe-Gaspar LE, Rivera Ramírez AB, Malváez Estrada DA, Ulloa Salaices E, Silva Delfín VP, González Villarreal G, Estolando Ayón M, Muñoz Flores A, Ortiz de la O EF, Ortiz Trujillo HJ, Moreno Domínguez JL, Lopez Suastegui M, Gallegos Cruz L and Duque-Molina C (2025) Equitable access to a personalized treatment with the OncoCREAN national strategy in pediatric patients with acute lymphoblastic leukemia from the Mexican Social Security Institute. Front. Oncol. 14:1304640. doi: 10.3389/fonc.2024.1304640
Received: 29 September 2023; Accepted: 07 August 2024;
Published: 10 September 2025.
Edited by:
Mario Ernesto Cruz-Munoz, Autonomous University of the State of Morelos, MexicoReviewed by:
Concetta Micalizzi, Giannina Gaslini Institute (IRCCS), ItalyJulio de la Torre, Comillas Pontifical University, Spain
Janet Flores Lujano, Mexican Social Security Institute, Mexico
Copyright © 2025 Lopez Aguilar, Del Campo Martinez, Rioscovian Soto, Ayala-Contreras, Zapata-Tarrés, Cuéllar Mendoza, Betanzos Cabrera, Zevada-Mosti, Payán Romo, Esquer Cota, Zazueta Mérida, Anaya Aguirre, Rodríguez Cedeño, Gutiérrez Rivera, Martín Trejo, Mayorga Castillo, Contreras Camacho, Reyes Espinoza, Alatoma Medina, Tiznado García, Santillán Ávila, Sepúlveda Núñez, Fuerte Olvera, Rodríguez Brindis, Parra Salazar, García Stivalet, Bojórquez Steffani, Betancourt Ortiz, Treviño, Mercado Castruita, Aburto Mejia, Jimenez Salinas, Valdivia Ibarra, Zepeda Arias, Figueroa Rosas, Sagarnaga Durante, Borrego Perez, Urbina Ochoa, Prieto Torres, Chavez Martenez, Perez Soltero, Careaga Reyna, Ramos Hernandez, Cardenas Navarrete, Gonzalez Rosas, Pineda Gordillo, Ochoa-Drucker, López Facio, Rios Osuna, Portillo Zavala, Cobo Ovando, Aguilar Román, Chávez Liñán, Arroyo Acosta, Bernabe-Gaspar, Rivera Ramírez, Malváez Estrada, Ulloa Salaices, Silva Delfín, González Villarreal, Estolando Ayón, Muñoz Flores, Ortiz de la O, Ortiz Trujillo, Moreno Domínguez, Lopez Suastegui, Gallegos Cruz and Duque-Molina. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Enrique Lopez Aguilar, ZWxvcGV6YWd1aWxhckBob3RtYWlsLmNvbQ==