 Pengcheng Wei
Pengcheng Wei Chen Lo
Chen Lo Jie Gao
Jie Gao Jiye Zhu
Jiye Zhu Xin Sun
Xin Sun Zhao Li
Zhao Li- 1Department of Hepatobiliary Surgery, Peking University People’s Hospital, Beijing, China
- 2Beijing Key Surgical Basic Research Laboratory of Liver Cirrhosis and Liver Cancer, Peking University People’s Hospital, Beijing, China
- 3Peking University Center of Liver Cancer Diagnosis and Treatment, Peking University People’s Hospital, Beijing, China
- 4Peking University Institute of Organ Transplantation, Peking University People’s Hospital, Beijing, China
- 5Musculoskeletal Tumor Center and Beijing Key Laboratory of Musculoskeletal Tumor, Peking University People’s Hospital, Beijing, China
Solitary fibrous tumor of the liver (SFTL) is an exceptionally rare mesenchymal tumor, with only 117 cases reported in the literature. While most SFTs are benign, some exhibit malignant behavior, including local recurrence and metastasis. This report presents two cases of SFTL with systemic metastases, both involving prior intracranial tumors. The first case, a 52-year-old woman, discovered a liver mass incidentally during a routine physical exam. Subsequent investigations revealed potential bone metastasis, and biopsy confirmed SFT. She received two TACE procedures, anlotinib targeted therapy, and radiotherapy for the iliac bone lesion, resulting in stable disease with reduction in lesion size. The second case, a 46-year-old man, presented with multiple liver, pelvic, and lung lesions following pelvic tumor resection, with pathology confirming SFT. He was treated with long-term anlotinib therapy, CyberKnife for hepatic, lung, and pelvic lesions, and radiofrequency ablation for hepatic lesions. Postoperative recovery was uneventful, with no tumor progression on follow-up. SFTL presents with atypical clinical and imaging features, and diagnosis requires pathological and genetic confirmation. Radical resection is preferred for solitary tumors, while comprehensive treatment, including surgery and long-term follow-up, is essential for cases with recurrence or metastasis.
1 Introduction
Solitary fibrous tumor (SFT), first identified by Klemperer and Rabin in 1931, is a rare tumor originating from fibroblastic mesenchymal tissues, comprising spindle cells and collagen (1). SFT affects a broad age range, including young adults and the elderly, with no significant gender disparity, though some reports indicate a slight female predominance (1, 2). SFT has a relatively low incidence compared to other systemic tumors, typically occurring in serosal-lined organs like the pleura, peritoneum, and retroperitoneum, as well as in non-serosal sites like the central nervous system, orbits, lungs, and mediastinum (3). Solitary fibrous tumor of the liver (SFTL) is exceedingly rare, with only 117 cases documented in medical literature to date. While most SFTLs follow a benign clinical course, they possess malignant potential, with approximately 10-20% categorized as malignant, capable of local recurrence and metastasis (4).
Most SFTL patients exhibit no clear symptoms, though some may have an abdominal mass or mild discomfort, typically found incidentally during exams for other conditions (5). When large, the tumor can pressure nearby liver structures, leading to vague right upper abdominal pain, intermittent dull pain, and right subcostal pressure. SFTL lacks distinctive imaging characteristics, making ultrasound, CT, and MRI non-specific for diagnosing it. Differential diagnosis includes hepatocellular carcinoma, focal nodular hyperplasia (FNH), and vascular ectodermal cell neoplasm, among others. A definitive diagnosis relies on distinct histopathological and immunohistochemical features. Treatment for SFTL varies with the tumor’s characteristics, size, and the patient’s general health. For localized lesions, surgical resection is preferred (6). Additionally, radiotherapy, chemotherapy, interventional therapy, ablation therapy, and targeted immunotherapy are effective treatment options.
However, in-depth research on the clinical diagnosis and treatment of SFTL is lacking. This article summarizes and analyzes the clinicopathological features and prognosis of two SFTL cases at our center, along with previous literature reports, aiming to offer a foundation and reference for SFTL diagnosis and treatment to guide clinical practice.
2 Case presentation
2.1 Case 1
A 52-year-old female patient was found to have a hepatic space-occupying lesion during a physical examination two weeks ago and reported mild abdominal discomfort. She had a history of an intracranial tumor, with surgery performed many years ago. Pathology suggested a possible hemangiopericytoma. She had no history of liver disease, no family history of genetic disorders, and no family history of tumors. Physical examination revealed stable vital signs and normal cardiopulmonary function. The abdomen was soft, without tenderness or rebound pain, and the liver and spleen were not palpable below the rib margin. Laboratory tests showed normal results for blood, urine, and fecal routine examinations, as well as normal biochemistry. Hepatitis B and C tests were negative, and tumor markers were within normal limits.
An MRI enhancement scan of the upper abdomen, performed prior to hospital admission, revealed multiple liver parenchymal lesions of varying sizes, displaying long T1 and T2 signals. The lesions exhibited uneven signals and inhomogeneous high intensity on DWI. The largest lesion, measuring approximately 10.4×7.8×10.4 cm, protruded significantly from beneath the liver and showed progressive, inhomogeneous, and marked enhancement. Low-density, non-enhancing necrotic areas were observed in the centers of the larger lesions, while smaller lesions showed more uniform enhancement. FDG PET/CT imaging further indicated multiple foci of increased FDG metabolism in the liver, sacrum, T8 vertebrae, and left ilium, suggesting multiple metastatic malignant tumors, with the primary origin possibly in the liver. Some liver foci were poorly demarcated from the inferior vena cava, raising the possibility of tumor thrombus. Scattered solid nodules were also observed in both lungs, raising concerns about potential lung metastasis.
The patient was admitted to the hospital and underwent an ultrasound-guided hepatic biopsy. Pathology revealed tumor invasion in a small liver tissue sample, characterized by spindle-shaped and ovoid tumor cells with mild to moderate atypia. Rare schizonts were observed, along with prominent luminal-like components, an interstitium rich in thin-walled blood vessels, and areas of interstitial hyalinized fibrosis. Immunohistochemistry results were as follows: CK (-), Hepatocyte (-), Arg1 (-), CD31 (+), CD34 (+), ERG (+), CD117 (-), DOG1 (-), PDGFR (-), and Ki-67 (10%+), consistent with a tumor of mesenchymal origin. Refer to Figure 1. Further NGS-506 genetic testing identified NAB2-STAT6 fusion, consistent with solitary fibrous tumor (SFT). Refer to Table 1.
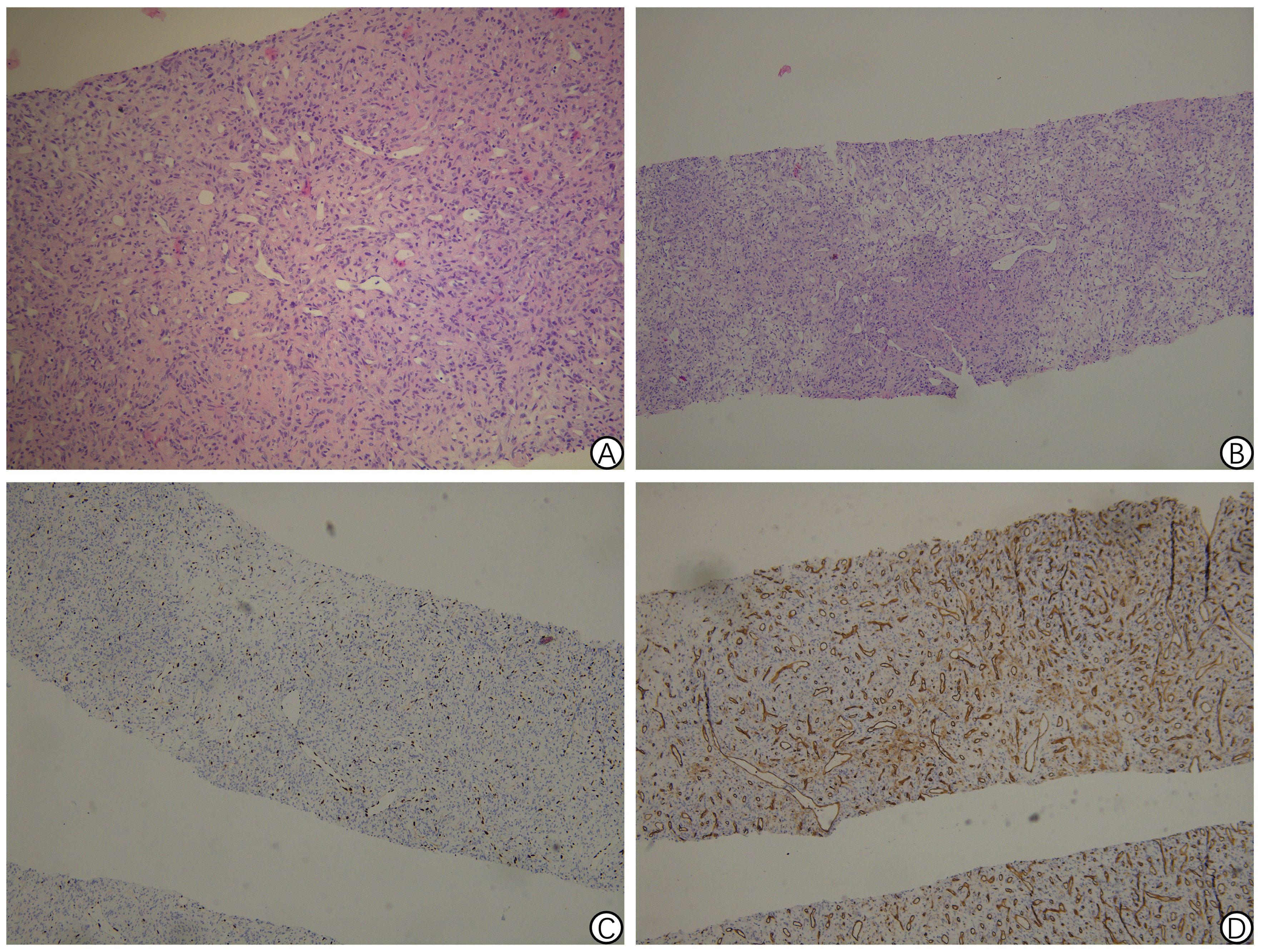
Figure 1. Pathology findings of solitary fibrous tumor of hepatic puncture biopsy in Case 1. (A) Proliferation of spindle cells randomly arranged in the abundant stromal collagen (hematoxylin and eosin staining, 200 × magnification); (B) Immunohistochemical staining revealing the positive ERG staining in the tumor cells (100 × magnification); (C) Immunohistochemical staining showing the positive CD34 staining in the tumor cells (100 × magnification); (D) Ki-67 Labeling index of 10%-15% (100 × magnification).
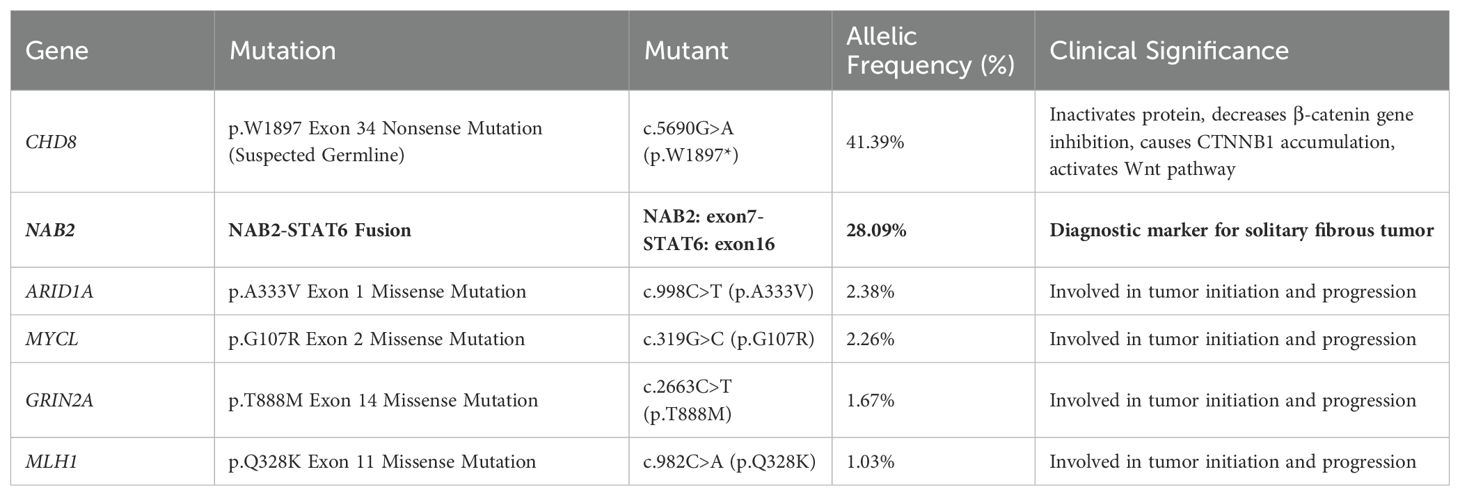
Table 1. The results of the Next-Generation Sequencing (NGS) analysis of 506 relevant genes from the liver biopsy specimen in Case 1.
A follow-up thoracic, abdominal, and pelvic CT enhancement scan revealed scattered nodular and lamellar hypodense shadows in the liver, with marked circumferential enhancement. The largest lesion, located in the right posterior lobe, measured approximately 10 × 8.2 cm. Bone destruction was observed on the left side of the sacrum, accompanied by a lamellar soft-tissue mass measuring approximately 5.0 × 4.6 cm, showing marked inhomogeneous enhancement. A ground-glass nodule was detected in the lower lobe of the left lung, with the nature yet to be determined. Scattered small solid nodules in both lungs were considered benign and old lesions. Refer to Figure 2. An MR enhancement scan of the pelvis revealed bone destruction on the left side of the sacrum, with an associated soft tissue mass measuring approximately 5.8 × 3.8 × 5.5 cm. The lesion exhibited uneven signals, with high signal intensity on DWI and marked uneven enhancement on the enhancement scan. The lesion involved the adjacent left pyriform muscle, with increased signal intensity on fat-suppressed images. Bone destruction was also noted in the adjacent left iliac bone, with localized patches of high signal on fat-suppressed images.
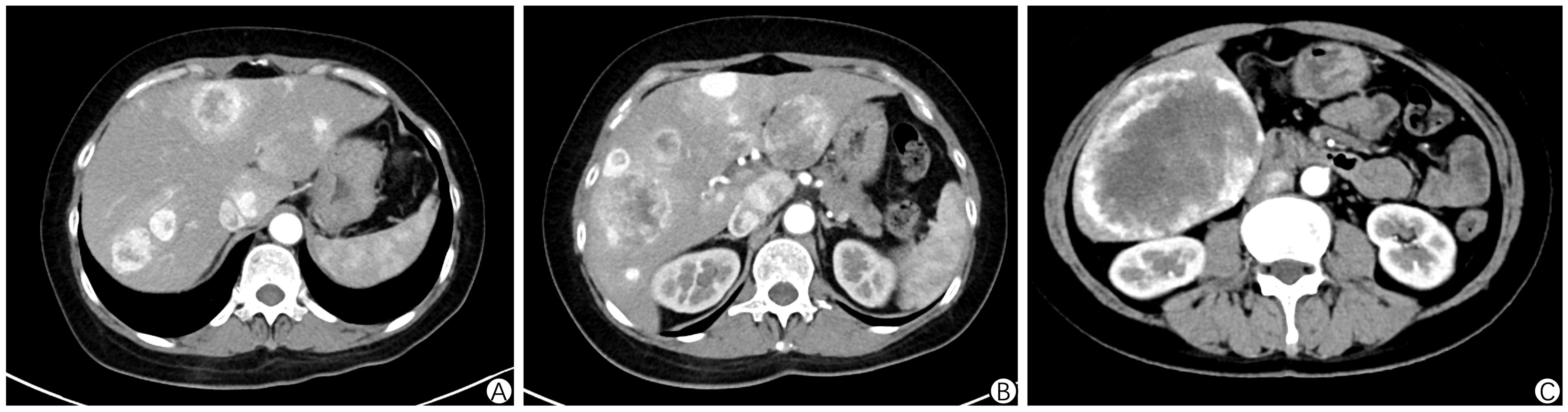
Figure 2. Abdominal enhanced CT in Case 1. (A-C) shows scattered nodular and patchy slightly low-density areas in the liver, with prominent ring-shaped enhancement. The largest lesion, located in the right posterior lobe, measures approximately 10 × 8.2 cm.
After a multidisciplinary team (MDT) discussion, it was concluded that the tumor might originate from the sacrum, and a further puncture biopsy was recommended to determine the pathological nature. The patient subsequently underwent a puncture biopsy of the sacral lesion, with pathological results revealing ovoid, short spindle-shaped tumor cells exhibiting mild to moderate heterogeneity. These cells were arranged in bundles and grew diffusely, with visible dilated thin-walled small blood vessels. The histomorphology was consistent with SFT. Immunohistochemistry results were as follows: CK (-), EMA (-), CD34 (focal +), STAT6 (+), CD117 (-), DOG-1 (-), PDGFR (-), Desmin (-), SOX10 (-), Vimentin (+), INI1 (+), S-100 (focal +), PR (-), CD31 (-), ERG (-), TLE1 (focal +), SDHB (+), p16 (focal +), MDM2 (focal +), CDK4 (-), and Ki-67 (approximately 15%+).
The patient underwent the first hepatic artery embolization, which involved superselective cannulation of the right hepatic artery and transcatheter injection of super-liquefied iodized oil and Embosphere microsphere particles (100-300 µm) for arterial embolization. Postoperatively, the patient started on anlotinib targeted therapy and received a total of 24 sessions of radiotherapy to the iliac lesion during the treatment period. During this period, the patient experienced lumbosacral pain, soreness, and abdominal distension, but no other significant abnormalities. Follow-up imaging after treatment showed a decrease in liver tumor enhancement. The patient then underwent a second hepatic artery embolization, with superselective cannulation of the left and right hepatic arteries for continued arterial embolization therapy. Follow-up imaging revealed shrinkage of the iliac lesion, which was evaluated as stable disease (SD). Refer to Figure 3.

Figure 3. Timeline of the patient’s medical history in Case 1.
2.2 Case 2
A 46-year-old male patient had a history of metastatic liver tumors for over two years. The patient had previously undergone surgery for an intracranial tumor with titanium plate implantation. Postoperative pathology suggested hemangiopericytoma, followed by local radiotherapy to the brain. Subsequent imaging revealed lesions in the pelvis, lungs, and liver, leading to pelvic tumor resection. Postoperative pathology and genetic testing confirmed SFT. The patient received long-term anlotinib treatment, along with CyberKnife therapy for liver, lung, and pelvic lesions. The patient had chronic hepatitis B, controlled and stabilized with oral entecavir. The patient had no family history of genetic diseases or tumors. Physical examination revealed stable vital signs, normal cardiopulmonary function, a soft abdomen without tenderness or rebound pain, and no palpable liver or spleen. Laboratory tests showed normal blood, urine, and fecal results, normal biochemistry, and negative tumor markers.
Pathological examination of the pelvic tumor resection specimen revealed infiltrative growth of tumor tissue into the bone and surrounding soft tissues. The tumor consisted of ovoid and short spindle-shaped cells with heterogeneous nuclei and nuclear schizogony, arranged in bundles. Features included vitreous degeneration, ossification, and antler-like branching blood vessels, with no evidence of necrosis. Immunohistochemistry results were as follows: CK (-), EMA (-), Vimentin (+), CD99 (+), NKX2.2 (-), BCOR (partially +), WT1 (-), Ki-67 (15% +), CD34 (focal weak +), STAT6 (+), SMA (-), S-100 (-), Desmin (-), TLE1 (-), SATB2 (-), and WT1 (-).Comparing the current specimen with the patient’s previous intracranial tumor pathology slides revealed similar morphology, suggesting recurrent intracranial SFT metastasis. Refer to Figure 4. Subsequent genetic testing identified a NAB2-STAT6 fusion, confirming the diagnosis of SFT. Refer to Figure 5 and Table 2.
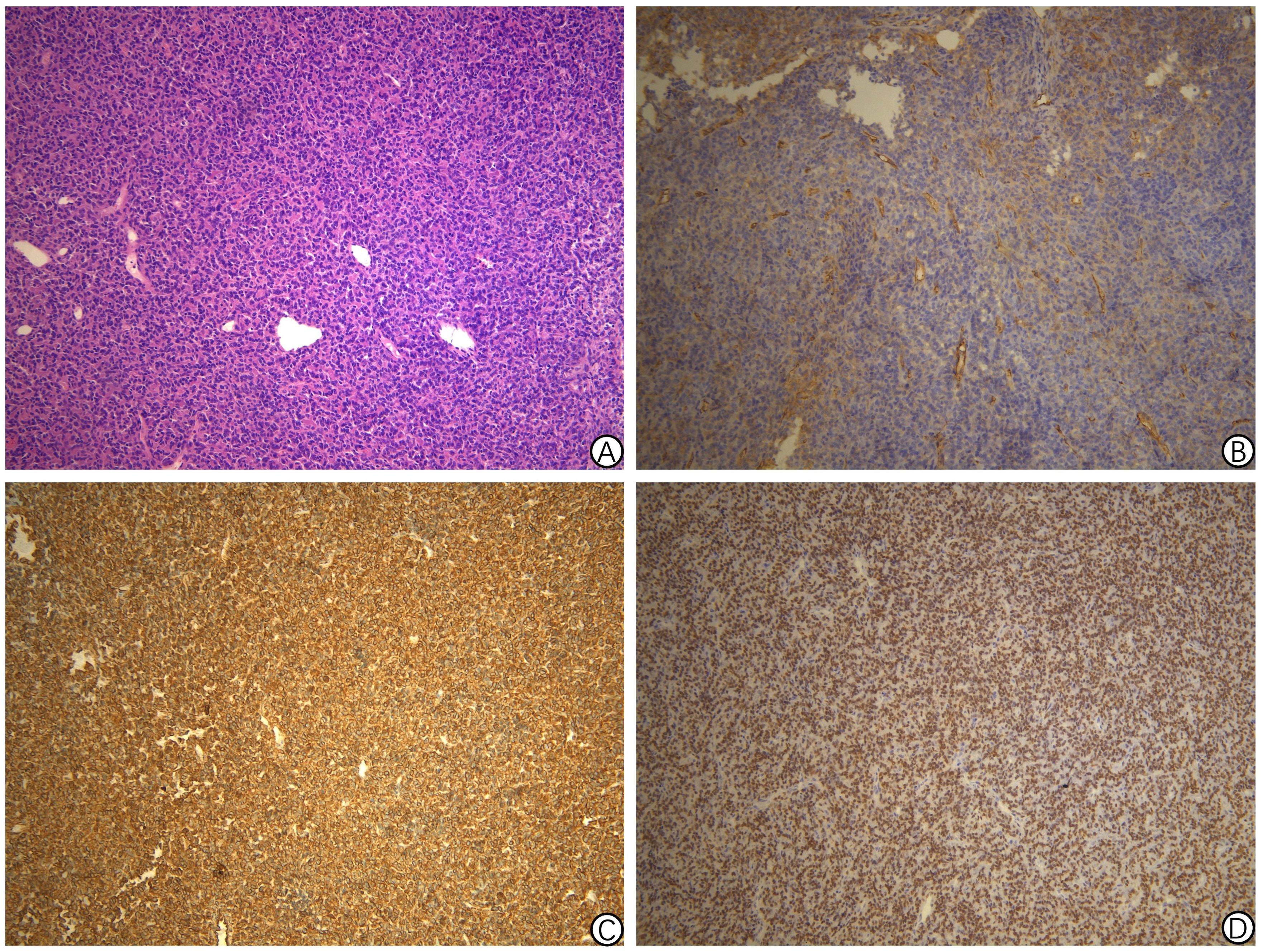
Figure 4. Pathology findings of solitary fibrous tumor of pelvic tumor resection specimen in Case 2. (A) Proliferation of spindle cells randomly arranged in the abundant stromal collagen (hematoxylin and eosin staining, 200 × magnification); (B) Immunohistochemical staining revealing the positive CD34 staining in the tumor cells (200 × magnification); (C) Immunohistochemical staining revealing the positive CD99 staining in the tumor cells (200 × magnification); (D) Immunohistochemical staining showing a strong STAT6 expression in the nucleus (200 × magnification).
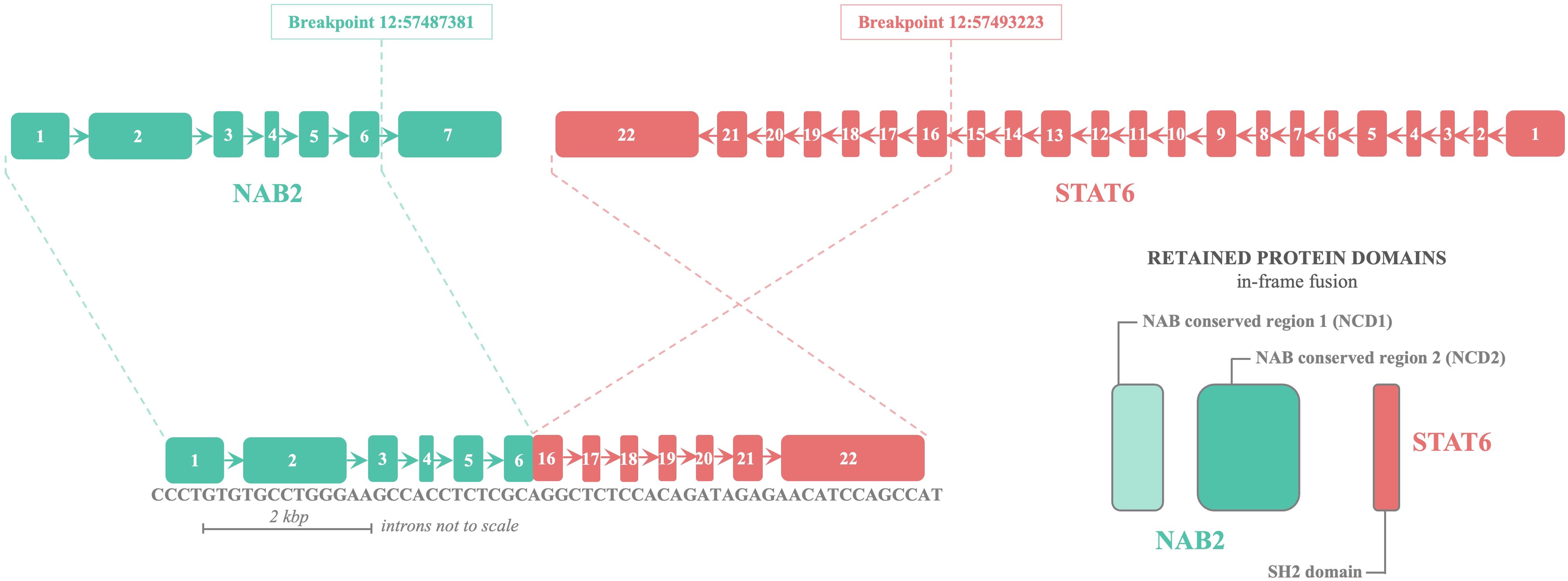
Figure 5. Schematic representation of NAB2–STAT6 fusion in Case 2.
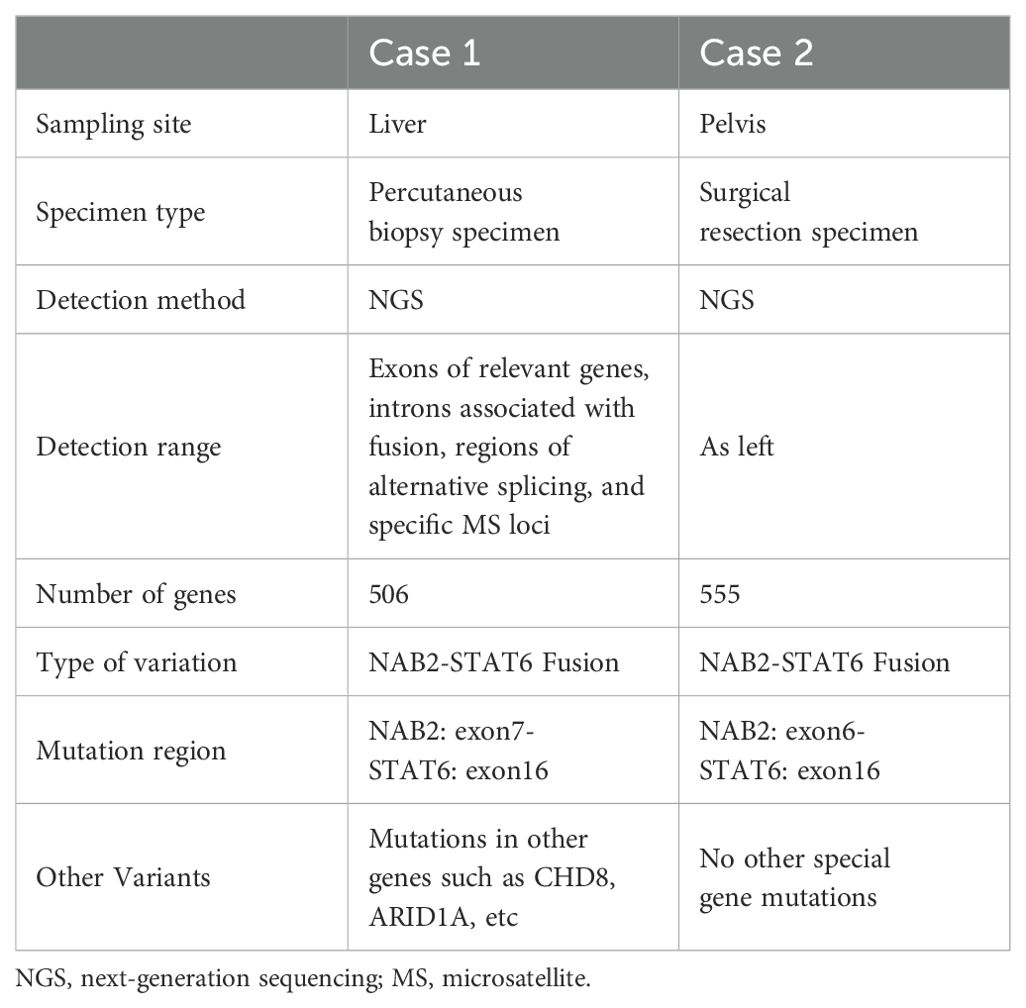
Table 2. Comparison of genetic test results between two cases.
Prior to hospital admission, an MRI enhancement scan of the upper abdomen revealed scattered round nodules in the liver with long T1 and T2 signals. The largest nodule, located in the left lobe, measured approximately 2.5×2.1 cm and showed a high signal on DWI. Most enhancement scans showed ring enhancement, while some arterial phases displayed significant enhancement in the form of small nodules, and portal phases exhibited isointense enhancement. Multiple liver metastases were considered, with the S7 segment lesion appearing smaller than before, showing a slight increase in enhancement. Other lesions were noted to have enlarged compared to previous scans. Refer to Figure 6. After admission, a CT enhancement scan of the cervicothoracic, abdominal, and pelvic regions showed rounded non-enhancing low-density shadows in the liver’s S6 and S4b segments, along with scattered rounded low-enhancing density shadows in the S5 and S6 segments, the largest measuring approximately 1.4×1.0 cm. A lesion in the dorsal segment of the lower lobe of the left lung was noted, raising suspicion of tumor metastasis, and sacral metastasis was considered at the S2-3 level.
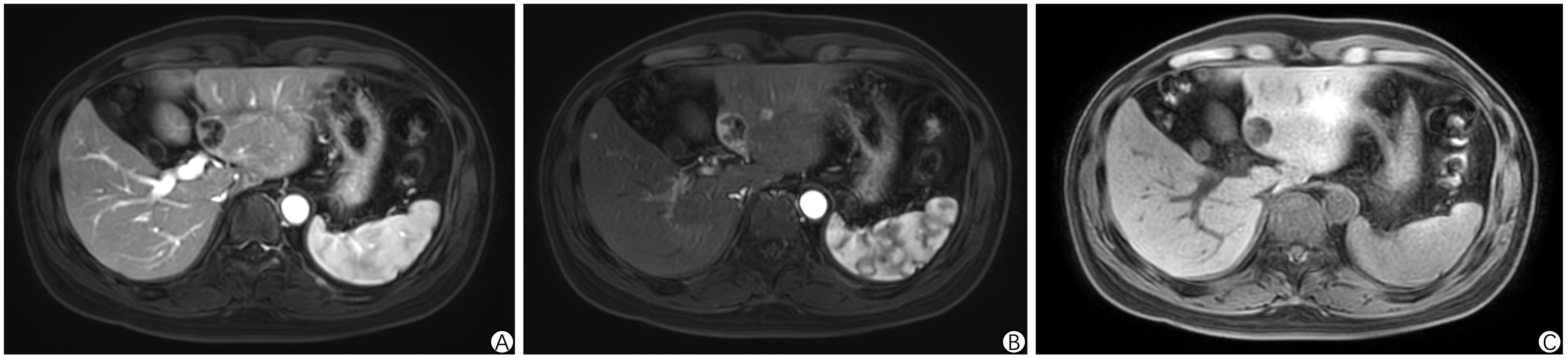
Figure 6. Abdominal enhanced MRI in Case 2. (A-C) demonstrates scattered round nodules in the liver with prolonged T1 and T2 signals. The largest nodule, located in the left lobe, measures approximately 2.5 × 2.1 cm and shows a pronounced high signal on DWI. Most nodules exhibit ring-shaped enhancement, with some displaying significant enhancement during the arterial phase and generally isointense enhancement in the portal phase.
The patient was admitted to the hospital and underwent radiofrequency ablation of hepatic lesions, targeting a total of 5 tumors in both the right and left lobes of the liver. Two days after the procedure, the patient developed persistent epigastric pain. CT indicated free pneumoperitoneum, raising the suspicion of gastrointestinal perforation. The patient subsequently underwent repair of a duodenal bulb ulcer perforation. Postoperative recovery was uneventful, and regular follow-up was conducted after discharge. Repeat enhanced CT of the chest, abdomen, and pelvis showed no evidence of tumor progression. Refer to Figure 7.
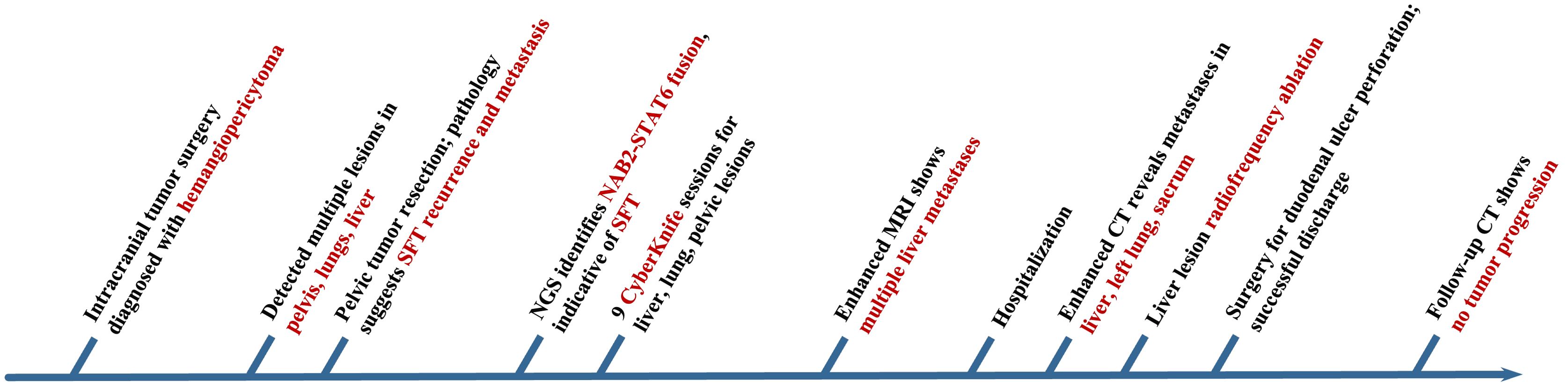
Figure 7. Timeline of the patient’s medical history in Case 2.
3 Discussion
SFT is a rare tumor originating from mesenchymal tissue, commonly found in the chest. A clear familial inheritance pattern or association with syndromes has not been widely reported, and most SFTs are considered sporadic (1, 7). SFTL, an extremely rare subtype of SFT, affects both the young and elderly with minimal gender incidence disparity. SFTL diagnosis is challenging due to its typically asymptomatic nature, manifesting only as an abdominal mass or mild discomfort. Since 1958, only 117 cases of SFTL have been reported in the international literature, with 92 cases showing intrahepatic solitary metastases (Table 3). Systemic multiple metastases were observed in 27 cases, including the 2 cases reported in this study (Table 4).
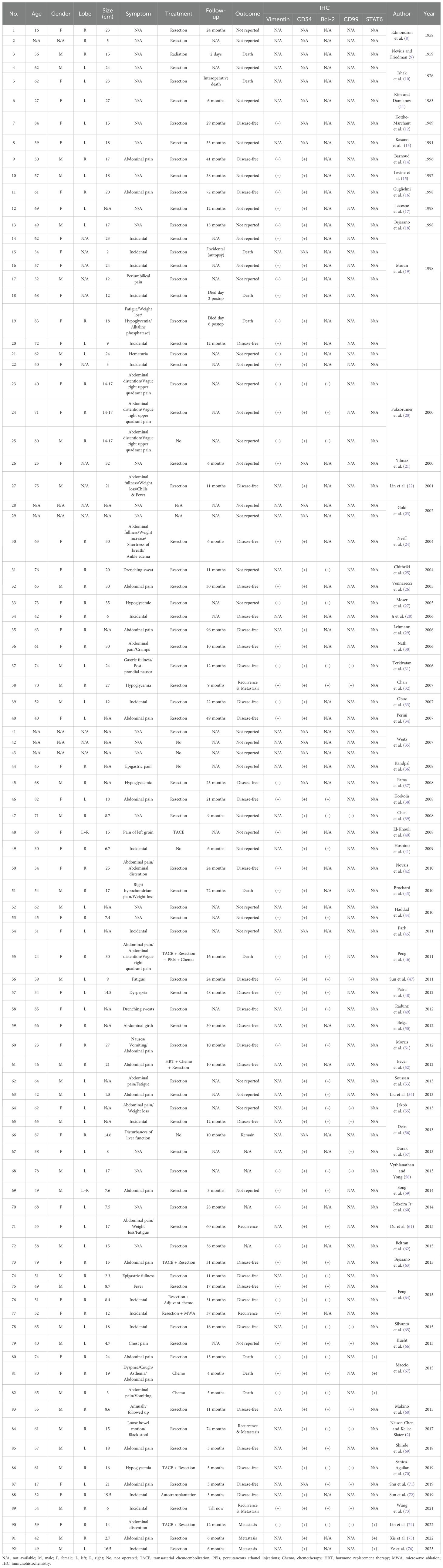
Table 3. 92 cases of solitary fibrous tumor of the liver (SFTL) found in the literature.
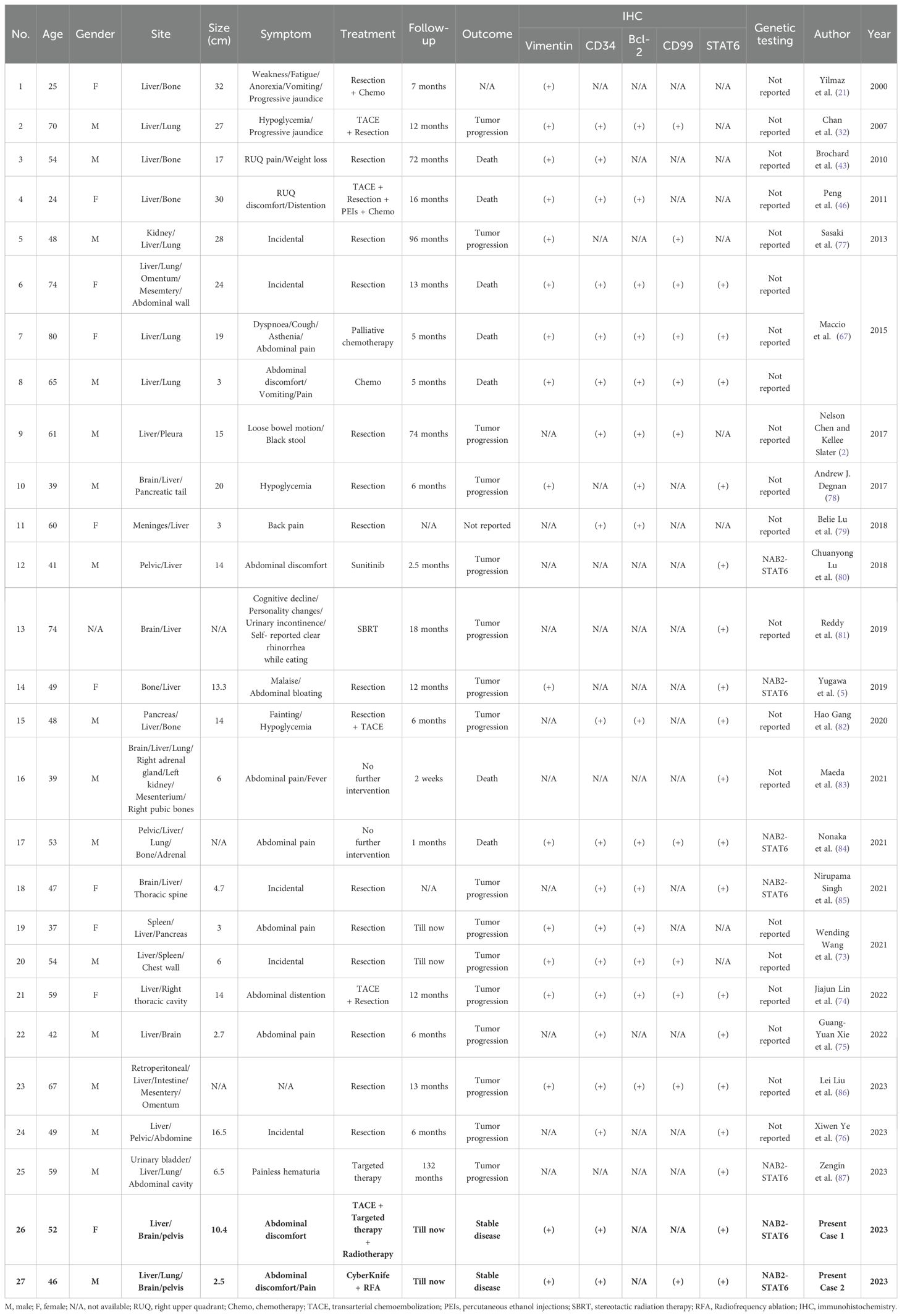
Table 4. 27 cases of solitary fibrous tumor of the liver (SFTL) with malignant features, local recurrence or metastatic disease found in the literature, including the present cases.
Literature review and this study’s cases reveal a median patient age of 57 years (range 16-87 years). The gender distribution was balanced (53 males, 59 females, 7 unknown). Single liver tumors were distributed evenly, with 34 in the left liver, 43 in the right, 2 in both, and 13 unknown. SFTL with systemic metastases developed not only in the liver but also in the pelvis, meninges, spine, lung, pancreas, and kidney, with metastases in the bone (10 cases), lung (8), brain (7), and other sites (13). The median tumor diameter was 16.0 cm (range 1.5-35 cm). Refer to Table 5.
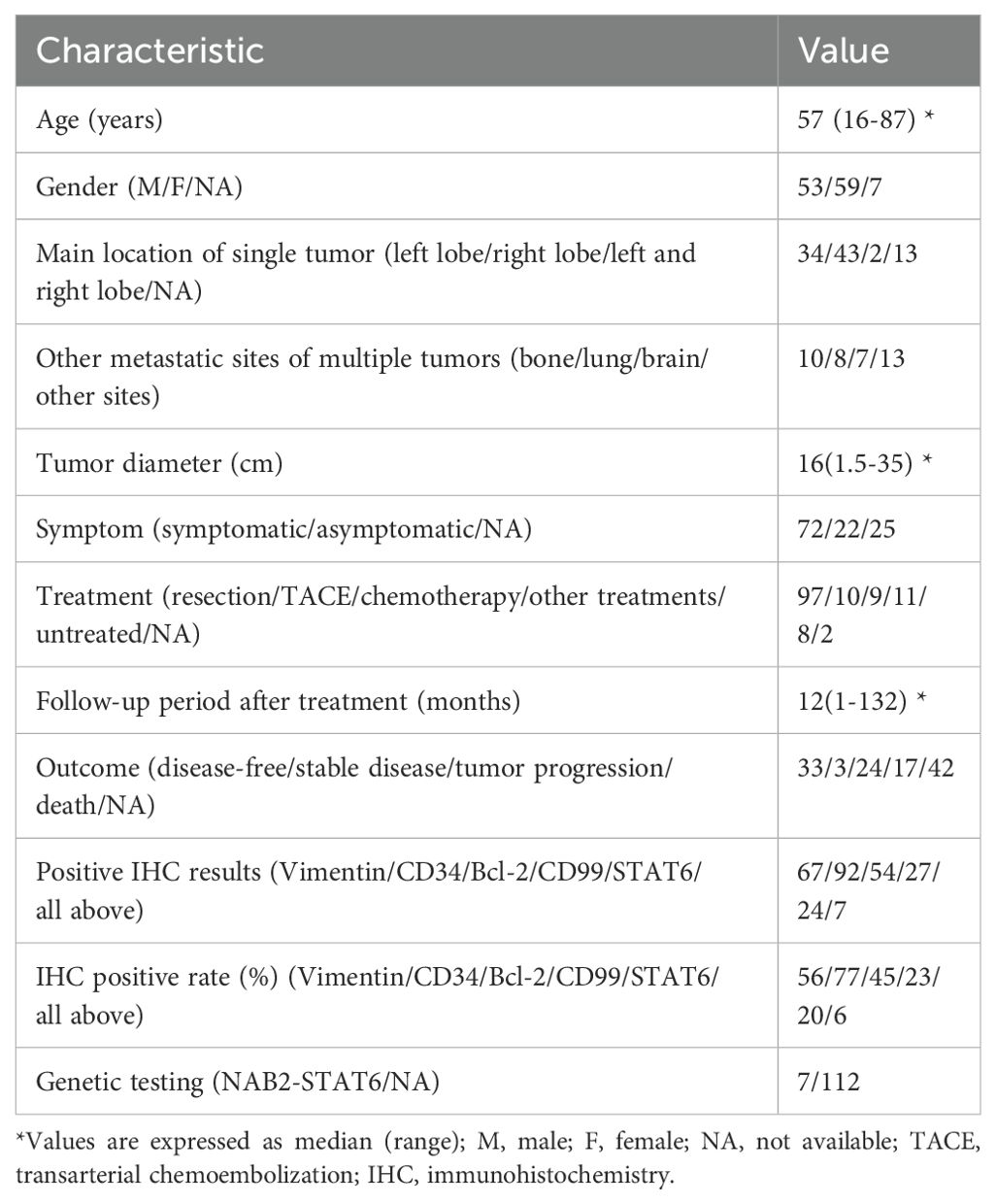
Table 5. Clinical summary of 119 cases of solitary fibrous tumor of the liver (SFTL).
This study’s two patients reported mild abdominal discomfort or pain. According to the literature, 72 cases presented with symptoms such as abdominal pain, distension, weight loss, malaise, and hypoglycemia, while 22 were asymptomatic, and the symptom status of 25 cases remains unknown. The nonspecific nature of SFTL’s clinical symptoms means that most cases are discovered incidentally during examinations. When symptoms do manifest, they are primarily due to the tumor’s mass effect or associated paraneoplastic syndromes. A few patients may exhibit Doege-Potter syndrome, characterized by non-islet-cell tumor hypoglycemia (NICTH), although this condition is rare (88). The association between SFT and hypoglycemia is attributed to abnormally high levels of insulin-like growth factor (IGF)-II in the tumor. This factor can bind to insulin and IGF-I receptors, mimicking endogenous insulin effects, increasing glucose uptake by tissues, and inhibiting growth hormone secretion and its hypoglycemia regulatory response, resulting in hypoglycemia and, in severe cases, epilepsy (89).
Notably, both patients in this study had a history of intracranial tumor surgery and subsequently developed systemic metastases, including to the liver, bone, and lungs. During follow-up, we reviewed the postoperative pathological findings from the intracranial tumor resections performed at an outside hospital. In Case 1, the pathology suggested atypical hemangiopericytoma. Immunohistochemistry results showed AE1/AE3 (+), CD31 (+), CD34 (+), CD68 (+), EMA (partially +), GFAP (-), Ki-67 (15% +), NF (-), S-100 (+), and Vimentin (+). In Case 2, the pathology suggested anaplastic hemangiopericytoma. Immunohistochemistry results revealed CD34 (+), S-100 (-), GFAP (-), PR (-), STAT-6 (+), SSTR-2 (-), Bcl-2 (partially +), CD99 (+), EMA (-), Vimentin (+), and Ki-67 (20%+). Reviewing the pathology of both patients, it is evident that their postoperative diagnoses initially considered hemangiopericytoma, and their immunohistochemistry profiles shared features characteristic of mesenchymal tumors. Similarly, a patient with SFTL and multiple systemic metastases, reported by Xie et al. in 2022, exhibited a similar disease progression (75). This patient had previously undergone intracranial tumor resection, with an initial pathology diagnosis of hemangiopericytoma, followed by liver metastases, and a final diagnosis of SFTL after surgical resection. Interestingly, as research progressed, hemangiopericytoma and SFT were found to significantly overlap in histologic features and molecular characteristics. Consequently, in the 2013 WHO Classification of Tumors of Soft Tissue and Bone, hemangiopericytoma is no longer classified as a separate tumor type but is grouped with SFT (90). This underscores the importance of considering similar patient histories, such as previous intracranial tumors, to enhance diagnostic sensitivity for SFTL in clinical practice.
SFTL’s imaging characteristics are non-specific; however, ultrasound, CT, and MRI remain the primary diagnostic modalities. Abdominal ultrasound may reveal a non-uniform mass with distinct borders, which may or may not include calcifications (71). CT scans commonly reveal heterogeneous lesion densities, displaying soft tissue density in solid components and hypodensity in cystic necrotic areas, with calcification and hemorrhage being infrequent. In enhanced CT, the solid tumor component exhibits uneven and marked enhancement during the arterial phase, with progressive or sustained enhancement in the venous and delayed phases. The characteristic “fast-in-slow-out” pattern in multiphase or dynamic scans is a hallmark of SFT (6). MRI reveals that SFTL generally displays low to medium signal intensity on T1-weighted images (T1WI) and heterogeneous, mixed low to high signal intensity on T2-weighted images (T2WI) (91). For Case 1 in this study, diagnosing SFTL based solely on imaging was challenging until pathological results were obtained, indicating the absence of typical imaging characteristics for SFTL. Furthermore, in cases of SFT with systemic metastases, PET-CT can identify intensely hypermetabolic malignant metastatic lesions, aiding in the detection of the tumor and its spread.
A definitive diagnosis of SFTL relies on histopathological and immunohistochemical analysis. HE staining reveals spindle or ovoid tumor cells, irregularly arranged and fasciculated, interspersed with abundant collagen fibers and staghorn blood vessels, featuring scant cytoplasm and an ovoid nucleus. SFT is classified as malignant if it is hypercellular and mitotically active (≥ 4 mitoses per 10 HPF) and exhibits cytologic atypia, tumor necrosis, or infiltrative margins (92). Immunohistochemistry frequently identifies SFT through positive staining for Vimentin, CD34, Bcl-2, and CD99, with CD34 serving as a critical marker to differentiate SFT from other spindle cell tumors. Nonetheless, a minor subset of SFT patients may exhibit negative immunohistochemical staining for CD34 (5). Moreover, recent research has established STAT6 as a potential key protein and a specific marker for SFT, playing a significant role in its immunohistochemical diagnosis (93). This study, combined with prior reports, found immunohistochemical positivity rates for Vimentin at 56% (67/119), CD34 at 77% (92/119), Bcl-2 at 45% (54/119), CD99 at 23% (27/119), and STAT6 at 20% (24/119). Only 6% (7/119) of patients were positive for all mentioned markers. These findings underscore the importance of these immunohistochemical markers in diagnosing SFTL.
With advancements in molecular testing, genetic testing has become increasingly valuable in diagnosing SFTL. Park et al.’s study demonstrated that the NAB2-STAT6 gene fusion, involving Nerve growth factor-induced gene A binding protein (NAB) 2 and signal transducer and activator of transcription (STAT) 6, offers better sensitivity and specificity for diagnosing SFT than traditional immunohistochemical markers (94). Originating from an inversion at the 12q13 locus, the NAB2-STAT6 fusion gene triggers the expression of the early growth response pathway, with its transcripts identifiable in 55-100% of SFT cases (95). In this study, combined with literature reviews, genetic testing revealed the NAB2-STAT6 gene fusion in seven SFTL patients, offering insights for molecular-level diagnosis of SFTL.
Recent advancements have been made in prediction models for the clinical diagnosis and treatment of SFT, marking a significant trend in the evolution of clinical diagnostics. Demicco et al.’s clinical prediction model integrates factors such as patient age, tumor size, mitotic activity, and extent of tumor necrosis to predict SFT metastasis risk, offering a comprehensive assessment of the tumor state to enhance diagnostic and therapeutic strategies (96). Zhang et al.’s recent comprehensive risk prediction model for SFT incorporates tumor mitotic counts, Ki-67(+) and CD163(+) cell densities, and MTOR mutations. This model aims to pinpoint therapeutic targets and risk factors, suggesting that a combination of immunotherapy and targeted therapy could benefit SFT patients. It heralds progress in refining SFT’s risk prediction models and developing therapeutic strategies (97).
Most SFTs exhibit benign biological behavior and have a favorable survival prognosis. Prognosis is influenced by treatment choices, as well as factors like tumor size, location, and histological characteristics. The primary treatment for SFTL involves comprehensive management centered around surgical resection. The 5-year survival rate after radical resection of SFT ranges from 59% to 100%, with a 10-year survival rate between 40% and 89%, and a recurrence rate of 5% to 20% (6). Additional treatment options include transarterial chemoembolization (TACE), chemotherapy, radiotherapy, and ablation therapy. Jin’s study summarized the effects of TACE in treating SFT, highlighting its efficacy as a locoregional treatment for some cases of SFTL (98). Gou et al.’s study, which included 42 SFT patients, demonstrated the positive role of postoperative radiotherapy in prolonging survival and achieving local control (99). Ablative therapy achieved good local tumor control in three patients with liver metastases of SFT, as reported by Krendl et al., and played a key role in multidisciplinary treatment strategies (100). Additionally, several clinical studies have employed multi-targeted tyrosine kinase inhibitors (e.g., sunitinib, sorafenib, pazopanib) for the treatment of invasive SFT, with favorable outcomes in some cases (1, 101). According to previous literature, this study reported 97 SFTL cases underwent surgical resection, 10 received TACE, 9 underwent chemotherapy, 11 received other treatments, 8 were untreated, and the treatment for 2 cases was unknown. Furthermore, two patients in this study, unable to undergo surgical resection for SFTL due to widespread metastases, received comprehensive treatment including TACE, radiotherapy, targeted therapy, and ablation therapy for systemic SFT, resulting in favorable outcomes and improved survival prognosis.
Given the unpredictable nature of SFT’s biological behavior, continuous long-term follow-up is crucial. This study’s median follow-up duration was 12 months, with outcomes as follows: 33 disease-free, 3 stable disease, 24 tumor progression, 17 deceased, and 42 unknown. Additionally, the study indicated median disease-free survival (DFS) and overall survival (OS) of 126.5 and 138.8 months (102), respectively, for SFT patients, with those undergoing surgical resection generally experiencing better long-term outcomes compared to those receiving alternative treatments. If complete tumor resection is unfeasible, combination therapy may extend survival. In addition, prognostic data on SFT with concomitant metastases are limited. In this study, 27 cases of SFTL with systemic metastases were summarized. Most patients experienced tumor recurrence and progression after treatment, likely due to the highly malignant nature of SFT. However, the prognosis for SFT patients with concomitant metastases is gradually improving with advancements in diagnosis and treatment, as well as increased focus on monitoring and follow-up. Lin et al. reported a case of giant SFTL with multiple metastases (74). The patient underwent TACE combined with surgical resection after MDT discussion. One year after surgery, no tumor recurrence was observed. In this study, two patients with SFTL and multiple metastases achieved stable disease (SD) status through effective treatment and regular long-term follow-up. Thus, a comprehensive approach involving surgical resection, consistent imaging, and extended follow-up is key to enhancing SFTL patients’ survival prognosis.
In summary, SFTL, a rare tumor, often presents no typical early symptoms. Larger lesions, however, can lead to abdominal pain, distension, and potentially hypoglycemia. Clinical symptoms and imaging features of SFTL are nonspecific. Histopathology and immunohistochemistry remain the diagnostic gold standards, while genetic testing offers further diagnostic clarification. Radical resection is preferred for solitary tumors. Malignant tumors with recurrence or metastasis risk typically require combination therapy following surgical resection, with regular follow-up being crucial for enhancing patient prognosis. This study’s two cases offer insights into diagnosing and treating SFTL with systemic metastases. As more cases accumulate, it is anticipated that SFTL diagnosis and treatment strategies will evolve, subsequently improving patient long-term prognosis.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by The Ethics Committee of Peking University People’s Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
PW: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. CL: Conceptualization, Data curation, Investigation, Writing – original draft. JG: Conceptualization, Supervision, Writing – review & editing. JZ: Conceptualization, Writing – review & editing. XS: Conceptualization, Investigation, Supervision, Writing – review & editing. ZL: Conceptualization, Investigation, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Capital Health Research and Development of Special Fund (2022-2-4084).
Acknowledgments
The authors would like to extend their deepest gratitude to Prof. Zhao Li and Prof. Xin Sun for their invaluable guidance and mentorship throughout the course of this research. Additionally, we wish to thank all the colleagues at Peking University People’s Hospital who participated in and supported this work. Their contributions were instrumental in the completion of this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Martin-Broto J, Mondaza-Hernandez JL, Moura DS, Hindi N. A Comprehensive Review on Solitary Fibrous Tumor: New Insights for New Horizons. Cancers (Basel). (2021) 13(12):2913. doi: 10.3390/cancers13122913
2. Chen N, Slater K. Solitary fibrous tumour of the liver-report on metastasis and local recurrence of a Malignant case and review of literature. World J Surg Oncol. (2017) 15:27. doi: 10.1186/s12957-017-1102-y
3. Rouy M, Guilbaud T, Birnbaum DJ. Liver solitary fibrous tumor: a rare incidentaloma. J Gastrointest Surg. (2021) 25:852–3. doi: 10.1007/s11605-020-04701-8
4. Fu Z, Henderson-Jackson EB, Centeno BA, Lauwers GY, Druta M, Anaya DA, et al. A case of hepatic Malignant solitary fibrous tumor: A case report and review of the literature. Case Rep Pathol. (2023) 2023:2271690. doi: 10.1155/2023/2271690
5. Yugawa K, Yoshizumi T, Mano Y, Kurihara T, Yoshiya S, Takeishi K, et al. Solitary fibrous tumor in the liver: case report and literature review. Surg Case Rep. (2019) 5:68. doi: 10.1186/s40792-019-0625-6
6. Davanzo B, Emerson RE, Lisy M, Koniaris LG, Kays JK. Solitary fibrous tumor. Transl Gastroenterol Hepatol. (2018) 3:94. doi: 10.21037/tgh.2018.11.02
7. Alghamdi ZM, Othman SA, Al-Yousef MJ, AlFadel BZ. Intrapulmonary location of benign solitary fibrous tumor. Ann Thorac Med. (2020) 15(2):98–101. doi: 10.4103/atm.ATM_14_20
8. BLANC WA. Tumors of the Liver and Intrahepatic Bile Ducts. . Pediatrics. (1958) 22(6):1109–9. doi: 10.1542/peds.22.6.1109
9. NEVIUS DB, FRIEDMAN NB. Mesotheliomas and extraovarin thecomas with hypoglycemic and nephrotic syndromes. Cancer. (1959) 12:1263–9. doi: 10.1002/1097-0142(195911/12)12:6<1263::aid-cncr2820120620>3.0.co;2-4
10. Ishak KG. Mesenchymal tumors of the liver. In: Okusa K, Peters RL, editors. Hepatocellular carcinoma. New York: John Wiley and Sons (1976). p. 247–307.
11. Kim H, Damjanov I. Localized fibrous mesothelioma of the liver. report of a giant tumor studied by light and electron microscopy. Cancer. (1983) 52(9):1662–5. doi: 10.1002/1097-0142(19831101)52:9<1662::aid-cncr2820520919>3.0.co;2-b
12. Kottke-Marchant K, Hart WR, Broughan T. Localized fibrous tumor (localized fibrous mesothelioma) of the liver. Cancer. (1989) 64(5):1096–102. doi: 10.1002/1097-0142(19890901)64:5<1096::aid-cncr2820640521>3.0.co;2-0
13. Kasano Y, Tanimura H, Tabuse K, Nagai Y, Mori K, Minami K. Giant fibrous mesothelioma of the liver. Am J Gastroenterol (1991) 86(3):379–80.
14. Barnoud R, Arvieux C, Pasquier D, Pasquier B, Letoublon C. Solitary fibrous tumour of the liver with CD34 expression. Histopathology. (1996) 28(6):551–4. doi: 10.1046/j.1365-2559.1996.d01-468.x
16. Guglielmi A, Frameglia M, Iuzzolino P, et al. Solitary fibrous tumor of the liver with CD 34 positivity and hypoglycemia. J Hepatobiliary Pancreat Surg (1998) 5(2):212–6. doi: 10.1007/s005340050036
17. Lecesne R, Drouillard J, Le Bail B, Saric J, Balabaud C, Laurent F. Localized fibrous tumor of the liver: imaging findings. Eur Radiol (1998) 8(1):36–8. doi: 10.1007/s003300050333
18. Bejarano PA, Blanco R and Hanto DW. Solitary fibrous tumor of the liver. a case report, river of the literature and differential diagnosis of spindle cell lesions of the liver. Int J Surg Pathol (1998) 6:93–100. doi: 10.1177/106689699800600206
19. Moran CA, Ishak KG, Goodman ZD. Solitary fibrous tumor of the liver: a clinicopathologic and immunohistochemical study of nine cases. Ann Diagn Pathol (1998) 2(1):19–24. doi: 10.1016/s1092-9134(98)80031-2
20. Fuksbrumer MS, Klimstra D, Panicek DM. Solitary fibrous tumor of the liver: imaging findings. AJR Am J Roentgenol. (2000) 175(6):1683–7. doi: 10.2214/ajr.175.6.1751683
21. Yilmaz S, Kirimlioglu V, Ertas E, et al. Giant solitary fibrous tumor of the liver with metastasis to the skeletal system successfully treated with trisegmentectomy. Dig Dis Sci (2000) 45(1):168–74. doi: 10.1023/a:1005438116772
22. Lin YT, Lo GH, KH L, et al. Solitary fibrous tumor of the liver. Zhonghua Yi Xue Za Zhi (Taipei). (2001) 64(5):305–9.
23. Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. (2002) 94(4):1057–68.
24. Neeff H, Obermaier R, Technau-Ihling K, et al. Solitary fibrous tumour of the liver: case report and review of the literature. Langenbecks Arch Surg (2004) 389(4):293–8. doi: 10.1007/s00423-004-0488-5
25. Chithriki M, Jaibaji M, Vandermolen R. Solitary fibrous tumor of the liver with presenting symptoms of hypoglycemic coma. Am Surg (2004) 70(4):291–3.
26. Vennarecci G, GM E, Giovannelli L, et al. Solitary fibrous tumor of the liver. J Hepatobiliary Pancreat Surg (2005) 12(4):341–4. doi: 10.1007/s00534-005-0993-0
27. Moser T, TS N, Neuville A, et al. Delayed enhancement pattern in a localized fibrous tumor of the liver. AJR Am J Roentgenol. (2005) 184(5):1578–80. doi: 10.2214/ajr.184.5.01841578
28. Ji Y, Fan J, Xu Y, Zhou J, HY Z, Tan YS. Solitary fibrous tumor of the liver. Hepatobiliary Pancreat Dis Int (2006) 5(1):151–3.
29. Lehmann C, Mourra N, JM T, Arrivé L. Tumeur fibreuse solitaire du foie [Solitary fibrous tumor of the liver]. J Radiol (2006) 87:139–42. doi: 10.1016/s0221-0363(06)73986-5
30. Nath DS, Rutzick AD, Sielaff TD. Solitary fibrous tumor of the liver. AJR Am J Roentgenol (2006) 187:W187–90. doi: 10.2214/AJR.05.0294
31. Terkivatan T, Kliffen M, de Wilt JH, van Geel AN, Eggermont AM, Verhoef C. Giant solitary fibrous tumour of the liver. World J Surg Oncol (2006) 4:81. doi: 10.1186/1477-7819-4-81
32. Chan G, Horton PJ, Thyssen S, et al. Malignant transformation of a solitary fibrous tumor of the liver and intractable hypoglycemia. J Hepatobiliary Pancreat Surg (2007) 14(6):595–9. doi: 10.1007/s00534-007-1210-0
33. Obuz F, Secil M, Sagol O, Karademir S, Topalak O. Ultrasonography and magnetic resonance imaging findings of solitary fibrous tumor of the liver. Tumori. (2007) 93(1):100–2. doi: 10.1177/030089160709300118
34. Perini MV, Herman P, D'Albuquerque LA, Saad WA. Solitary fibrous tumor of the liver: report of a rare case and review of the literature. Int J Surg (2008) 6(5):396–9. doi: 10.1016/j.ijsu.2007.10.004
35. Weitz J, Klimstra DS, Cymes K, et al. Management of primary liver sarcomas. Cancer. (2007) 109(7):1391–6. doi: 10.1002/cncr.22530
36. Kandpal H, Sharma R, Gupta SD, Kumar A. Solitary fibrous tumour of the liver: a rare imaging diagnosis using MRI and diffusion-weighted imaging. Br J Radiol (2008) 81(972):e282–6. doi: 10.1259/bjr/98393711
37. Famà F, Le Bouc Y, Barrande G, et al. Solitary fibrous tumour of the liver with IGF-II-related hypoglycaemia. A Case Rep Langenbecks Arch Surg (2008) 393(4):611–6. doi: 10.1007/s00423-008-0329-z
38. Korkolis DP, Apostolaki K, Aggeli C, et al. Solitary fibrous tumor of the liver expressing CD34 and vimentin: a case report. World J Gastroenterol (2008) 14(40):6261–4. doi: 10.3748/wjg.14.6261
39. Chen JJ, SL O, Richards C, et al. Inaccuracy of fine-needle biopsy in the diagnosis of solitary fibrous tumour of the liver. Asian J Surg (2008) 31(4):195–8. doi: 10.1016/S1015-9584(08)60085-8
40. El-Khouli RH, Geschwind JF, Bluemke DA, Kamel IR. Solitary fibrous tumor of the liver: magnetic resonance imaging evaluation and treatment with transarterial chemoembolization. J Comput Assist Tomogr. (2008) 32(5):769–71. doi: 10.1097/RCT.0b013e3181557453
41. Hoshino M, Nakajima S, Futagawa Y, Fujioka S, Okamoto T, Yanaga K. A solitary fibrous tumor originating from the liver surface. Clin J Gastroenterol (2009) 2(4):320–4. doi: 10.1007/s12328-009-0097-5
42. Novais P, Robles-Medranda C, Pannain VL, Barbosa D, Biccas B, Fogaça H. Solitary fibrous liver tumor: is surgical approach the best option? J Gastrointestin Liver Dis (2010) 19(1):81–4.
43. Brochard C, Michalak S, Aubé C, et al. A not so solitary fibrous tumor of the liver. Gastroenterol Clin Biol (2010) 34(12):716–20. doi: 10.1016/j.gcb.2010.08.004
44. Haddad A, Karras R, Fraiman M, Mackey R. Solitary fibrous tumor of the liver... Am Surg (2010) 76(7):E78–9.
45. Park HS, Kim YK, Cho BH, Moon WS. Pedunculated hepatic mass. Liver Int (2011) 31(4):541. doi: 10.1111/j.1478-3231.2010.02318.x
46. Peng L, Liu Y, Ai Y, Liu Z, He Y, Liu Q. Skull base metastases from a malignant solitary fibrous tumor of the liver. A Case Rep literature review. Diagn Pathol (2011) 6:127. doi: 10.1186/1746-1596-6-127
47. Sun K, Lu JJ, Teng XD, Ying LX, Wei JF. Solitary fibrous tumor of the liver: a case report. World J Surg Oncol (2011) 9:37. doi: 10.1186/1477-7819-9-37
48. Patra S, Vij M, Venugopal K, Rela M. Hepatic solitary fibrous tumor: report of a rare case. Indian J Pathol Microbiol (2012) 55(2):236–8. doi: 10.4103/0377-4929.97892
49. Radunz S, Baba HA, Sotiropoulos GC. Large tumor of the liver and hypoglycemic shock in an 85-year-old patient. Gastroenterology. (2012) 142(2):e10–1. doi: 10.1053/j.gastro.2011.02.072
50. Belga S, Ferreira S, Lemos MM. A rare tumor of the liver with a sudden presentation. Gastroenterology. (2012) 143(3):e14–5. doi: 10.1053/j.gastro.2012.02.045
51. Morris R, McIntosh D, Helling T, Martin JN Jr.. Solid fibrous tumor of the liver: a case in pregnancy. J Matern Fetal Neonatal Med (2012) 25(6):866–8. doi: 10.3109/14767058.2011.596958
52. Beyer L, Delpero JR, Chetaille B, et al. Solitary fibrous tumor in the round ligament of the liver: a fortunate intraoperative discovery. Case Rep Oncol (2012) 5(1):187–94. doi: 10.1159/000338616
53. Soussan M, Felden A, Cyrta J, Morère JF, Douard R, Wind P. Case 198: solitary fibrous tumor of the liver. Radiology. (2013) 269(1):304–8. doi: 10.1148/radiol.13121315
54. Liu Q, Liu J, Chen W, Mao S, Guo Y. Primary solitary fibrous tumors of liver: a case report and literature review. Diagn Pathol (2013) 8:195. doi: 10.1186/1746-1596-8-195
55. Jakob M, Schneider M, Hoeller I, Laffer U, Kaderli R. Malignant solitary fibrous tumor involving the liver. World J Gastroenterol (2013) 19(21):3354–7. doi: 10.3748/wjg.v19.i21.3354
56. Debs T, Kassir R, Amor IB, Martini F, Iannelli A, Gugenheim J. Solitary fibrous tumor of the liver: report of two cases and review of the literature. Int J Surg (2014) 12(12):1291–4. doi: 10.1016/j.ijsu.2014.10.037
57. Güray Durak M, Sağol Ö, Tuna B, et al. Cystic solitary fibrous tumor of the liver: a case report. Turk Patoloji Derg. (2013) 29(3):217–20. doi: 10.5146/tjpath.2013.01173
58. Vythianathan M, Yong J. A rare primary malignant solitary fibrous tumour of the liver. Pathology (2013) 45:S86–7. doi: 10.1097/01.PAT.0000426954.68370.26
59. Song L, Zhang W, Zhang Y. (18)F-FDG PET/CT imaging of malignant hepatic solitary fibrous tumor. Clin Nucl Med (2014) 39(7):662–4. doi: 10.1097/RLU.0000000000000431
60. Teixeira F Jr, de Freitas Perina AL, de Oliveira Mendes G, de Andrade AB, da Costa FP. Fibrous solitary tumour of the liver. J Gastrointest Cancer. (2014) 45 Suppl 1:216–7. doi: 10.1007/s12029-014-9635-6
61. Du EH, Walshe TM, Buckley AR. Recurring rare liver tumor presenting with hypoglycemia. Gastroenterology. (2015) 148(2):e11–3. doi: 10.1053/j.gastro.2014.09.036
62. Beltrán MA. Solitary fibrous tumor of the liver: a review of the current knowledge and report of a new case. J Gastrointest Cancer. (2015) 46(4):333–42. doi: 10.1007/s12029-015-9769-1
63. Bejarano-González N, García-Borobia FJ, Romaguera-Monzonís A, et al. Solitary fibrous tumor of the liver. case report and review of the literature. Rev Esp Enferm Dig. (2015) 107(10):633–9. doi: 10.17235/reed.2015.3676/2014
64. Feng LH, Dong H, Zhu YY, Cong WM. An update on primary hepatic solitary fibrous tumor: An examination of the clinical and pathological features of four case studies and a literature review. Pathol Res Pract (2015) 211(12):911–7. doi: 10.1016/j.prp.2015.09.004
65. Silvanto A, Karanjia ND, Bagwan IN. Primary hepatic solitary fibrous tumor with histologically benign and malignant areas. Hepatobiliary Pancreat Dis Int (2015) 14(6):665–8. doi: 10.1016/s1499-3872(15)60365-4
66. Kueht M, Masand P, Rana A, Cotton R, Goss J. Concurrent hepatic hemangioma and solitary fibrous tumor: diagnosis and management. J Surg Case Rep (2015) 2015(7):rjv089. doi: 10.1093/jscr/rjv089
67. Maccio L, Bonetti LR, Siopis E, Palmiere C. Malignant metastasizing solitary fibrous tumors of the liver: a report of three cases. Pol J Pathol (2015) 66(1):72–6. doi: 10.5114/pjp.2015.51156
68. Makino Y, Miyazaki M, Shigekawa M, et al. Solitary fibrous tumor of the liver from development to resection. Intern Med (2015) 54(7):765–70. doi: 10.2169/internalmedicine.54.3053
69. Shinde RS, Gupta A, Goel M, Patkar S. Solitary fibrous tumor of the liver - an unusual entity: A case report and review of literature. Ann Hepatobiliary Pancreat Surg (2018) 22(2):156–8. doi: 10.14701/ahbps.2018.22.2.156
70. De Los Santos-Aguilar RG, Chávez-Villa M, Contreras AG, et al. Successful multimodal treatment of an IGF2-producing solitary fibrous tumor with acromegaloid changes and hypoglycemia. J Endocr Soc (2019) 3(3):537–43. doi: 10.1210/js.2018-00281
71. Shu Q, Liu X, Yang X, Guo B, Huang T, Lei H, et al. Malignant solitary fibrous tumor of the liver: a case report. Int J Clin Exp Pathol. (2019) 12(6):2305–10.
72. Sun Z, Ding Y, Jiang Y, et al. Ex situ hepatectomy and liver autotransplantation for a treating giant solitary fibrous tumor: A case report. Oncol Lett (2019) 17(1):1042–52. doi: 10.3892/ol.2018.9693
73. Wang W, Bao B, Hu A, Zhu X, Chen Q. Two case reports of rare diseases occurring in rare parts: splenic vein solitary fibrous tumor and liver solitary fibrous tumor. AME Case Rep (2021) 5:17. doi: 10.21037/acr-20-142
74. Lin J, Huang S, Wang J, Cai Z. Multidisciplinary collaboration for the successful treatment of a giant hepatic solitary fibrous tumor protruding into the thorax: A case report. Exp Ther Med. (2022) 24:461. doi: 10.3892/etm.2022.11388
75. Xie G-Y, Zhu H-B, Jin Y, Li B-Z, Yu Y-Q, Li J-T. Solitary fibrous tumor of the liver: A case report and review of the literature. World J Clin Cases. (2022) 10:7097–104. doi: 10.12998/wjcc.v10.i20.7097
76. Ye X, Tang X, Li F, Lin Y. A giant malignant solitary fibrous tumor in the liver: A case report. Asian J Surg (2023) 46(9):3920–3. doi: 10.1016/j.asjsur.2023.03.178
77. Sasaki H, Kurihara T, Katsuoka Y, et al. Distant metastasis from benign solitary fibrous tumor of the kidney. Case Rep Nephrol Urol. (2013) 3(1):1–8. doi: 10.1159/000346850
78. Andrew J, Degnan Degnan AJ, KK L, Minervini MI, Borhani AA. Metastatic extrapleural malignant solitary fibrous tumor presenting with hypoglycemia (Doege-potter syndrome). Radiol Case Rep (2016) 12(1):113–9. doi: 10.1016/j.radcr.2016.10.014
79. Lu B, Lu Q, Huang B, Yuan H, Li C. Contrast enhanced imaging features of liver metastasis from a meningeal solitary fibrous tumor: a case report. Med Ultrason. (2018) 20(3):392–5. doi: 10.11152/mu-1472
80. Lu C, Alex D, Benayed R, Rosenblum M, Hameed M. Solitary fibrous tumor with neuroendocrine and squamous dedifferentiation: a potential diagnostic pitfall. Hum Pathol (2018) 77:175–80. doi: 10.1016/j.humpath.2017.12.024
81. Reddy S, Plitt A, Raisanen J, et al. Intracranial anaplastic hemangiopericytoma presenting with simultaneous extra-cranial metastases: A case report and review of the literature. Surg Neurol Int (2019) 10:148. doi: 10.25259/SNI_111_2019
82. Geng H, Ye Y, Jin Y, et al. Malignant solitary fibrous tumor of the pancreas with systemic metastasis: A case report and review of the literature. World J Clin Cases. (2020) 8(2):343–52. doi: 10.12998/wjcc.v8.i2.343
83. Maeda M, Fukuda T, Miyake M, Takahashi H, Ikegami M. Extracranial metastatic solitary fibrous tumor/hemangiopericytoma expressing g-CSF and its receptor. Neuropathology. (2021) 41(4):288–92. doi: 10.1111/neup.12734
84. Nonaka H, Kandori S, Nitta S, et al. Case report: Molecular characterization of aggressive malignant retroperitoneal solitary fibrous tumor: A case study. Front Oncol (2021) 11:736969. doi: 10.3389/fonc.2021.736969
85. Singh N, Collingwood R, Eich ML, et al. NAB2-STAT6 gene fusions to evaluate Primary/Metastasis of Hemangiopericytoma/Solitary fibrous tumors. Am J Clin Pathol (2021) 156(5):906–12. doi: 10.1093/ajcp/aqab045
86. Liu L, Chen S, Wang L. Retroperitoneal malignant solitary fibrous tumor with second recurrence and lymphatic metastases: A case report. Oncol Lett (2022) 25(2):57. doi: 10.3892/ol.2022.13643
87. Zengin HB, McCabe M, Yildiz B, et al. Malignant solitary fibrous tumor of the urinary bladder progressing to widespread metastases and death: a rare case report and literature review. Int J Clin Exp Pathol (2023) 16(9):243–51.
88. Taliente F, De Rose AM, Ardito F, Giuliante F. Solitary fibrous tumor of the liver with Doege-Potter syndrome: An exceptional finding. Discovering the role of blood glucose levels and insulin growth factor II. Clin Res Hepatol Gastroenterol. (2022) 46:102051. doi: 10.1016/j.clinre.2022.102051
89. Gomez FD, Robin L, Jakubowicz D, Sillou S, Lab JP, Balian C. Solitary fibrous tumor of the retroperitoneum with urinary symptoms revealing a Doege-Potter’s syndrome. Prog Urol. (2019) 29:136–7. doi: 10.1016/j.purol.2019.02.004
90. Yamashita D, Suehiro S, Kohno S, Ohue S, Nakamura Y, Kouno D, et al. Intracranial anaplastic solitary fibrous tumor/hemangiopericytoma: immunohistochemical markers for definitive diagnosis. Neurosurg Rev. (2021) 44:1591–600. doi: 10.1007/s10143-020-01348-6
91. Esteves C, Maia T, Lopes JM, Pimenta M. Malignant solitary fibrous tumor of the liver: AIRP best cases in radiologic-pathologic correlation. Radiographics. (2017) 37:2018–25. doi: 10.1148/rg.2017160200
92. O’Neill AC, Tirumani SH, Do WS, Keraliya AR, Hornick JL, Shinagare AB, et al. Metastatic patterns of solitary fibrous tumors: A single-institution experience. AJR Am J Roentgenol. (2017) 208:2–9. doi: 10.2214/AJR.16.16662
93. Huang S-C, Huang H-Y. Solitary fibrous tumor: An evolving and unifying entity with unsettled issues. Histol Histopathol. (2019) 34:313–34. doi: 10.14670/HH-18-064
94. Park HK, Yu DB, Sung M, Oh E, Kim M, Song J-Y, et al. Molecular changes in solitary fibrous tumor progression. J Mol Med (Berl). (2019) 97:1413–25. doi: 10.1007/s00109-019-01815-8
95. Chmielecki J, Crago AM, Rosenberg M, O’Connor R, Walker SR, Ambrogio L, et al. Whole-exome sequencing identifies a recurrent NAB2-STAT6 fusion in solitary fibrous tumors. Nat Genet. (2013) 45:131–2. doi: 10.1038/ng.2522
96. Demicco EG, Wagner MJ, Maki RG, Gupta V, Iofin I, Lazar AJ, et al. Risk assessment in solitary fibrous tumors: validation and refinement of a risk stratification model. Mod Pathol. (2017) 30:1433–42. doi: 10.1038/modpathol.2017.54
97. Zhang R, Yang Y, Hu C, Huang M, Cen W, Ling D, et al. Comprehensive analysis reveals potential therapeutic targets and an integrated risk stratification model for solitary fibrous tumors. Nat Commun. (2023) 14:7479. doi: 10.1038/s41467-023-43249-4
98. Jin K, Zhong S, Lin L, Wu J, Wang Y, Cui W, et al. Targeting-intratumoral-lactic-acidosis transcatheter-arterial-chemoembolization for non-islet cell tumor hypoglycemia secondary to a liver metastatic solitary fibrous tumor: A case report and literature review. Front Endocrinol (Lausanne). (2022) 13:955687. doi: 10.3389/fendo.2022.955687
99. Gou Q, Xie Y, Ai P. Intracranial solitary fibrous tumor/hemangiopericytoma: Role and choice of postoperative radiotherapy techniques. Front Oncol. (2022) 12:994335. doi: 10.3389/fonc.2022.994335
100. Krendl FJ, Messner F, Laimer G, Djanani A, Seeber A, Oberhuber G, et al. Multidisciplinary treatment of liver metastases from intracranial SFTs/HPCs: A report of three consecutive cases. Curr Oncol. (2022) 29:8720–41. doi: 10.3390/curroncol29110687
101. Riedel RF. Anti-angiogenic therapy for Malignant solitary fibrous tumour: validation through collaboration. Lancet Oncol. (2019) 20:14–5. doi: 10.1016/S1470-2045(18)30745-9
Keywords: solitary fibrous tumor, liver tumor, mesenchymal neoplasms, malignancy, metastasis
Citation: Wei P, Lo C, Gao J, Zhu J, Sun X and Li Z (2024) Systemic metastasis in malignant solitary fibrous tumor of the liver: two case reports and literature review. Front. Oncol. 14:1418547. doi: 10.3389/fonc.2024.1418547
Received: 16 April 2024; Accepted: 06 September 2024;
Published: 02 October 2024.
Edited by:
Alberto Brolese, APSS, ItalyReviewed by:
Naonori Kawakubo, Kyushu University, JapanAbdul Qahar Khan Yasinzai, University of Florida, United States
Copyright © 2024 Wei, Lo, Gao, Zhu, Sun and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhao Li, Z29vZGxpemhhb0BzaW5hLmNvbQ==; Xin Sun, eGluc3VuMTk4MUBob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship