 Yaxin Jiang
Yaxin Jiang Zimeng Li2
Zimeng Li2 Bizhen Chen
Bizhen Chen- 1Department of Healthcare-Associated Infection Management, The Second Affiliated Hospital of Fujian University of Traditional Chinese Medicine, Fuzhou, China
- 2School of Nursing, Fujian University of Traditional Chinese Medicine, Fuzhou, China
Background: Numerous studies have developed or validated prediction models to estimate the likelihood of postoperative pneumonia (POP) in esophageal cancer (EC) patients. The quality of these models and the evaluation of their applicability to clinical practice and future research remains unknown. This study systematically evaluated the risk of bias and applicability of risk prediction models for developing POP in patients undergoing esophageal cancer surgery.
Methods: PubMed, Embase, Web of Science, Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), China National Knowledge Infrastructure (CNKI), China Science and Technology Journal Database (VIP), WanFang Database and Chinese Biomedical Literature Database were searched from inception to March 12, 2024. Two investigators independently screened the literature and extracted data. The Prediction Model Risk of Bias Assessment Tool (PROBAST) checklist was employed to evaluate both the risk of bias and applicability.
Result: A total of 14 studies involving 23 models were included. These studies were mainly published between 2014 and 2023. The applicability of all studies was good. However, all studies exhibited a high risk of bias, primarily attributed to inappropriate data sources, insufficient sample size, irrational treatment of variables and missing data, and lack of model validation. The incidence of POP in patients undergoing esophageal cancer surgery ranged from 14.60% to 39.26%. The most frequently used predictors were smoking, age, chronic obstructive pulmonary disease(COPD), diabetes mellitus, and methods of thoracotomy. Inter-model discrimination ranged from 0.627 to 0.850, sensitivity ranged between 60.7% and 84.0%, and specificity ranged from 59.1% to 83.9%.
Conclusion: In all included studies, good discrimination was reported for risk prediction models for POP in patients undergoing esophageal cancer surgery, indicating stable model performance. However, according to the PROBAST checklist, all studies had a high risk of bias. Future studies should use the predictive model assessment tool to improve study design and develop new models with larger samples and multicenter external validation.
Systematic review registration: https://www.crd.york.ac.uk/prospero, identifier CRD42024527085.
1 Introduction
Esophageal cancer (EC) is a common malignant tumor of the gastrointestinal tract that originates from the mucosal epithelium of the esophagus. According to data from the National Cancer Center of China, an estimated 224,000 new cases of EC appeared in 2022 (1). Esophagectomy is currently the primary therapeutic option for EC. Despite significant advancements in surgical technology and perioperative care, esophagectomy remains a high-risk procedure, with a postoperative complication rate of 36.2% (2). Among the complications, postoperative pneumonia (POP) is the most common, with an incidence ranging from 8.7% to 28.3% (3). The occurrence of POP prolongs hospitalization and affects patient prognosis and even death. Patients with POP have a higher mortality rate within 1 year than those who do not develop infection after surgery (16.8% vs. 21.6%) (4). Therefore, precise and early assessment of individuals at risk of developing pneumonia after EC, coupled with targeted preventive measures against risk factors, is of utmost importance.
Clinical prediction models combine multiple relevant risk factors to estimate the probability of outcome occurrence so that clinical providers can quickly identify and monitor high-risk patients to avoid adverse events. Recently, numerous predictive models have been developed to predict POP occurrence in patients with EC. These models can be used to identify individuals at high risk of POP; however, there may be contradictions between the results of different studies (5, 6). This poses a major dilemma for surgeons in selecting an appropriate treatment. Therefore, a comprehensive review and overview of existing POP models is necessary to clarify their predictive performance, advantages, and disadvantages, among others, to evaluate the best model with the potential for widespread implementation.
Recent systematic reviews have focused on predictive models for pulmonary complications following esophagectomy (7, 8). However, this is not entirely applicable to identifying people at risk of POP. Our study specifically focused on the population at a high risk of POP following surgery among patients with EC. In this study, we analyzed the existing prediction models for the risk of POP after esophagectomy concerning the reports related to the systematic evaluation of prediction models (9) to provide a reliable assessment tool for preventing and controlling POP.
2 Methods
2.1 search strategy
In order to conduct a comprehensive search, we targeted both Chinese and English databases. Computerized searches the databases included PubMed, Embase, Web of Science, The Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), China Knowledge Network(CNKI), Chinese Science and Technology Journal Database (VIP), Wanfang database, and China Biomedical Literature Database, which were searched from the inception of the databases until March 12, 2024. A combination of subject and free word search was adopted. Search keywords included Esophageal Neoplasms, Esophagectomy, cancer of esophagus, Pneumonia, postoperative pneumonia, lung infection, Risk Assessment, Risk Factors, prediction model, predict*. We also identified additional relevant studies by reviewing the reference lists of the retrieved studies and review articles.
In this systematic review, we employed the PICOTS system recommended by the Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modelling Studies (CHARMS) (10) checklist. This approach aids in formulating the review’s objectives, search strategy, and inclusion/exclusion criteria (5). The essential components of our systematic review are delineated below:
P (Population): patients operated on for EC.
I (Intervention model): development and/or validation of predictive models for the risk of POP in patients operated on for EC.
C (Comparator): not applicable.
O (Outcome): the primary outcome indicator is the occurrence of POP.
T (Timing): Esophageal cancer after surgery. The prediction was made according to the laboratory indicators and clinical symptoms in the diagnostic criteria of POP.
S (Setting): the intended use of the predictive models is the prediction of the occurrence of POP in patients operated on for EC, to allow for early identification of at-risk populations and targeted preventive measures.
2.2 Inclusion and exclusion criteria
Inclusion criteria:
(1) Patients who have been diagnosed with EC and treated with surgery.
(2) The study is about the construction and/or validation of a prediction model for the risk of pneumonia after surgery for esophageal cancer.
(3) An observational study design.
(4) The predicted outcome is POP.
(5) Studies published in Chinese and English.
Exclusion criteria:
(1) Models consisting of only one predictor (e.g., lung function index, sarcopenia, laboratory tests, etc.).
(2) Studies on risk factors analysis were performed only, without the construction of a complete risk model.
(3) The types of studies were reviews, conference papers, etc.
(4) The full text could not be retrieved despite contacting the authors via email.
(5) Duplicated published studies.
2.3 Study screening
The retrieved literature was imported into the literature management software. Firstly, duplicate studies were manually identified and removed. Second, titles and abstracts of articles were screened. Finally, their full texts were reviewed after applying the inclusion and exclusion criteria. The reference lists of all eligible studies were also checked to ensure the comprehensiveness of the search. Two researchers independently conducted and cross-checked the study’s screening. In case of disagreement, a third researcher was involved in the discussion to solve the problem.
2.4 Data collection
Following the screening process, Data extraction of the identified studies was performed using the CHARMS (10). The information extracted from the selected studies was categorized into two groups: (1) Basic information: first author, year, country, study type, and sample size. (2) Model information: number of models, modeling method, model efficacy, final predictors, selection of variables, model presentation, verification method. Two researchers independently performed and cross-checked data extraction. Any disagreement was resolved with the help of another researcher.
2.5 Assessment of risk of bias and applicability
The risk of bias and applicability of the included studies was evaluated using the Predictive Modeling Risk of Bias Assessment Tool (PROBAST) (11). The risk of bias evaluation included 20 questions in 4 domains: study object, predictor, outcome, and data analysis. The applicability evaluation included three domains: study object, predictor, and outcome. When the results of all domains were “low risk of bias,” the result of the risk of bias assessment was “low risk of bias”; when “high risk of bias” was found in ≥1 domain, the result of the risk of bias assessment was “high risk of bias”; when the result of one domain is “unclear,” and the results of the remaining domains are “low risk of bias,” the risk of bias assessment result is “unclear.” The applicability assessment was similar to the risk of bias assessment. The two researchers carried out the literature assessment, and after the independent assessment, they checked each other’s results. Disagreements, if any, in the above process were resolved through discussion. A third researcher could also be consulted if necessary.
2.6 Descriptive analyses
Results were summarized using descriptive statistics, which was conducted on the included studies, the establishment of prediction models, and the performance of models.
2.7 Patient and public involvement
There was no patient or public involvement in this study.
3 Results
3.1 Process of article screening
The search strategy identified 3508 records, and 1,036 duplicate records were deleted. After title and abstract screening, 2,338 records were excluded. After reviewing the full texts, 120 records were further excluded(108 articles only analyzed risk factors for the development of POP in patients undergoing surgery for EC, three articles were conference papers, five articles had study participants who did not meet the inclusion criteria for this study, 2 duplicated published studies, and two studies only validated the model). Ultimately, 14 articles of literature (12–25) were included in this systematic review. The study selection process is shown in Figure 1.
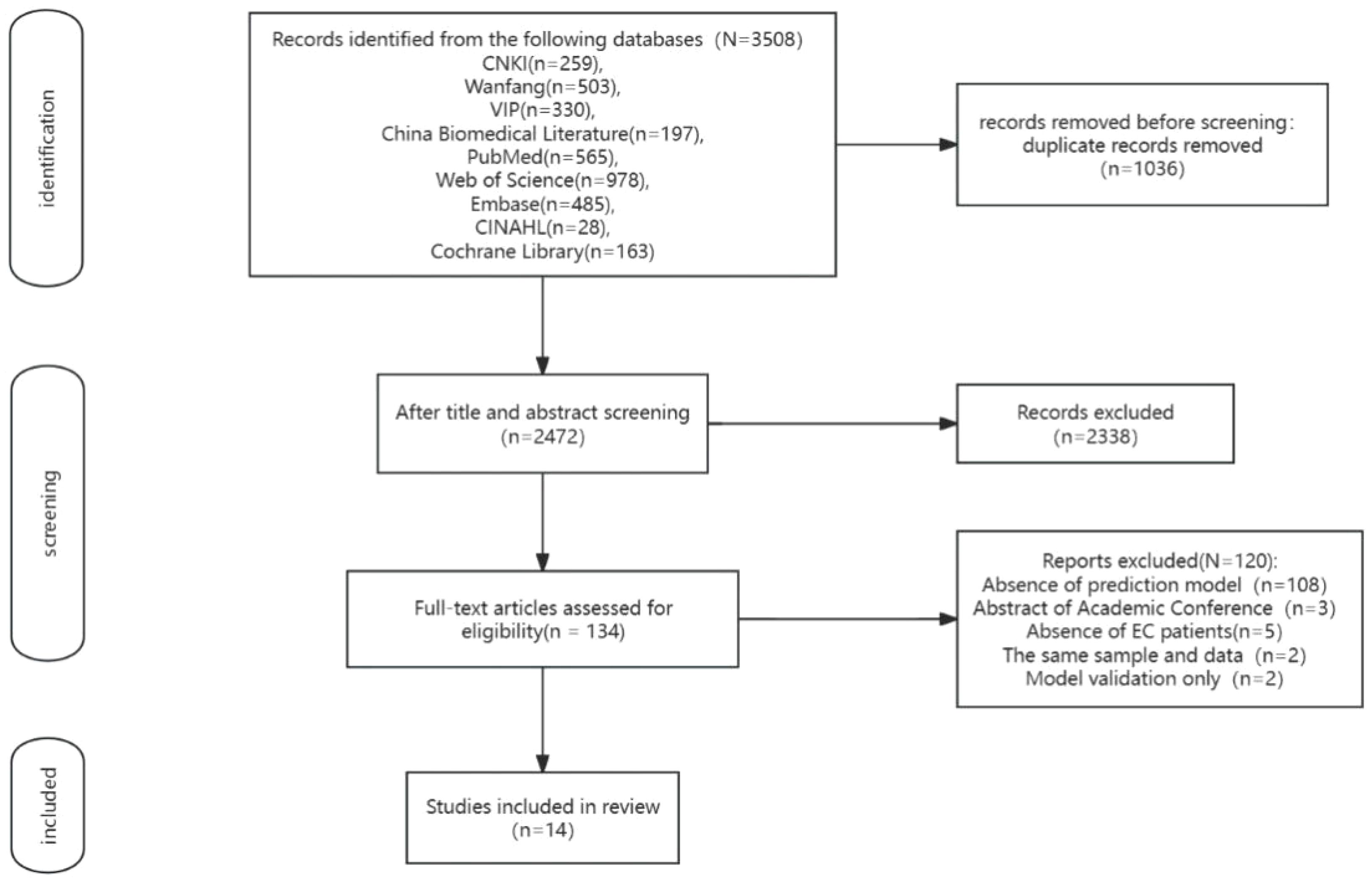
Figure 1 Process of study selection.
3.2 Study characteristics
The year of publication of the 14 included studies was primarily between 2014 and 2023. Twelve were conducted in China (14–25) (nine studies published in Chinese), one from the Netherlands (12) and one from Japan (13). The majority (n=11, 78.57%) of the included studies were retrospective. One Japanese study (13) involved multiple centers, while the others were conducted at single centers. Regarding the study population, two studies (14, 15) focused on EC patients aged 60 years or older. The specific characteristics of the included studies are summarized in Table 1.
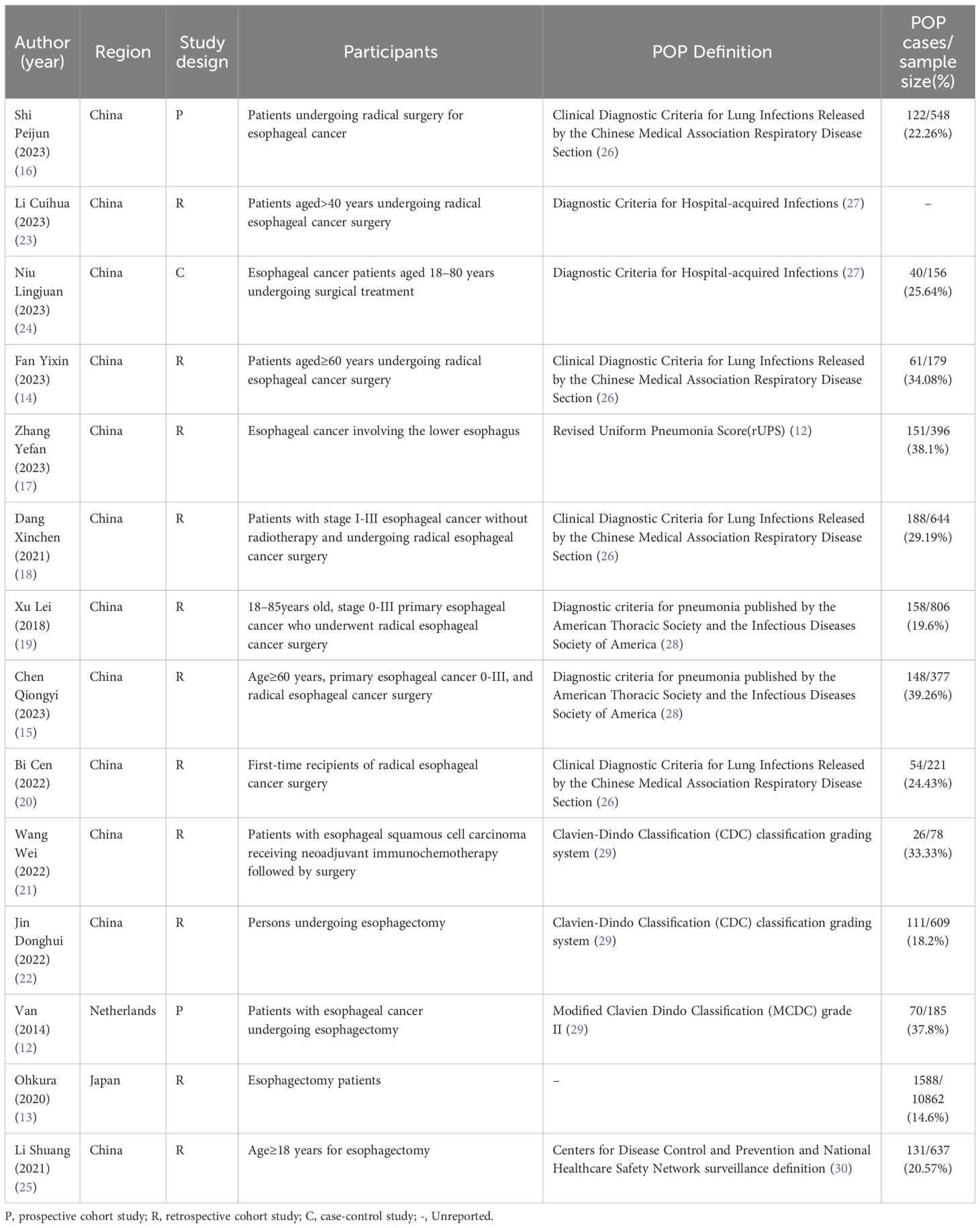
Table 1 General characteristics of the included studies (n =14).
3.3 Basic features of prediction model
Most included studies developed only one model, while four studies (12, 13, 15, 16) developed more than one model, resulting in 30. Notably, the study by Ohkura contributed eight models (13). However, our review focuses only on the most relevant models (POP). Ultimately, our systematic review evaluates 23 models. The sample size across all studies ranged from 78 to 10,862 patients. Only six studies (12, 15, 17–20) reported the number of missing sample cases and addressed them through direct exclusion. In terms of model development, the methodologies used by most studies were logistic regression. Additionally, five studies (16–18, 21, 22) utilized R software for constructing their models, and only 1 study developed a predictive model using machine learning techniques (15). For predictors, the final number of predictors obtained ranged from 2 to 17, with the five most frequently occurring predictors being smoking, age, chronic obstructive pulmonary disease(COPD), diabetes, and open chest surgery method. The basic features information in the prediction model is summarized in Table 2.
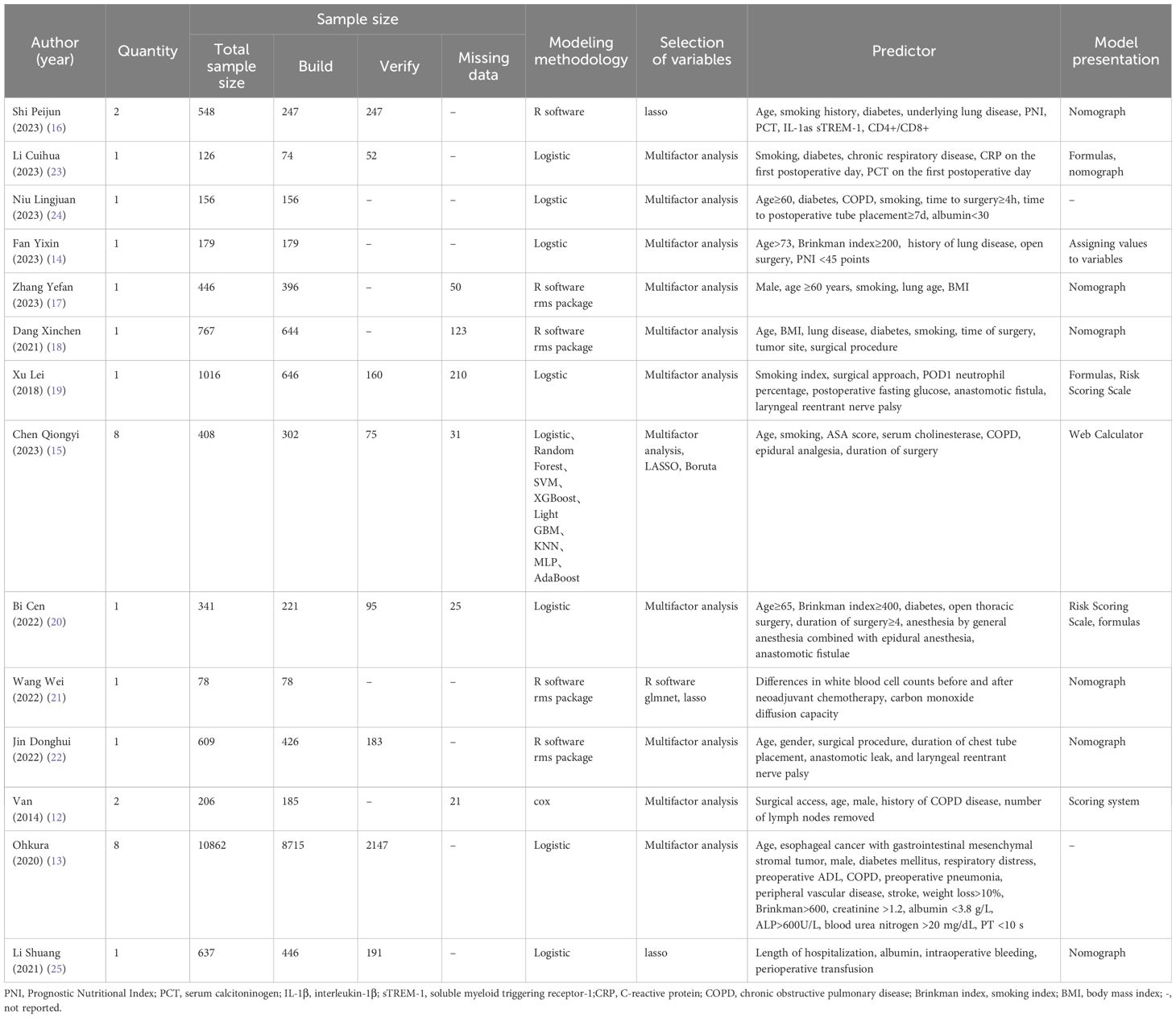
Table 2 Establishment of a POP risk prediction model in patients with esophageal cancer(n =14).
3.4 Model predictive performance
Regarding model performance, the reported discrimination in the model development research ranged from 0.627 to 0.850. Four studies evaluated the models using internal validation (13, 15, 20, 22), and four carried out external validation (16, 19, 23, 25). In the validation model studies, the area under the curve (AUC) values of the model validation groups exceeded 0.7, except for Jin’s model (22), which had an AUC value below 0.7. Although the discriminability of the model was not reported in van’s study (12), internal and external validation of the model was conducted by Weijs (31) and Seesing (32), and the mean value of the AUC was 0.94, which suggests that the model validation performance was stable. Wang (21) and Jin (22) reported only the calibration method of the model, while the study by Niu (24) and Fan (14) focused only on the sensitivity and specificity of the model. Notably, six studies (15–18, 21, 22) used calibration curves to assess the consistency between actual and predicted data, and three studies (15, 19, 20) chose the Hosmer-Lemeshow (H-L) goodness-of-fit test to assess model calibration. The risk prediction model performance is shown in Table 3.
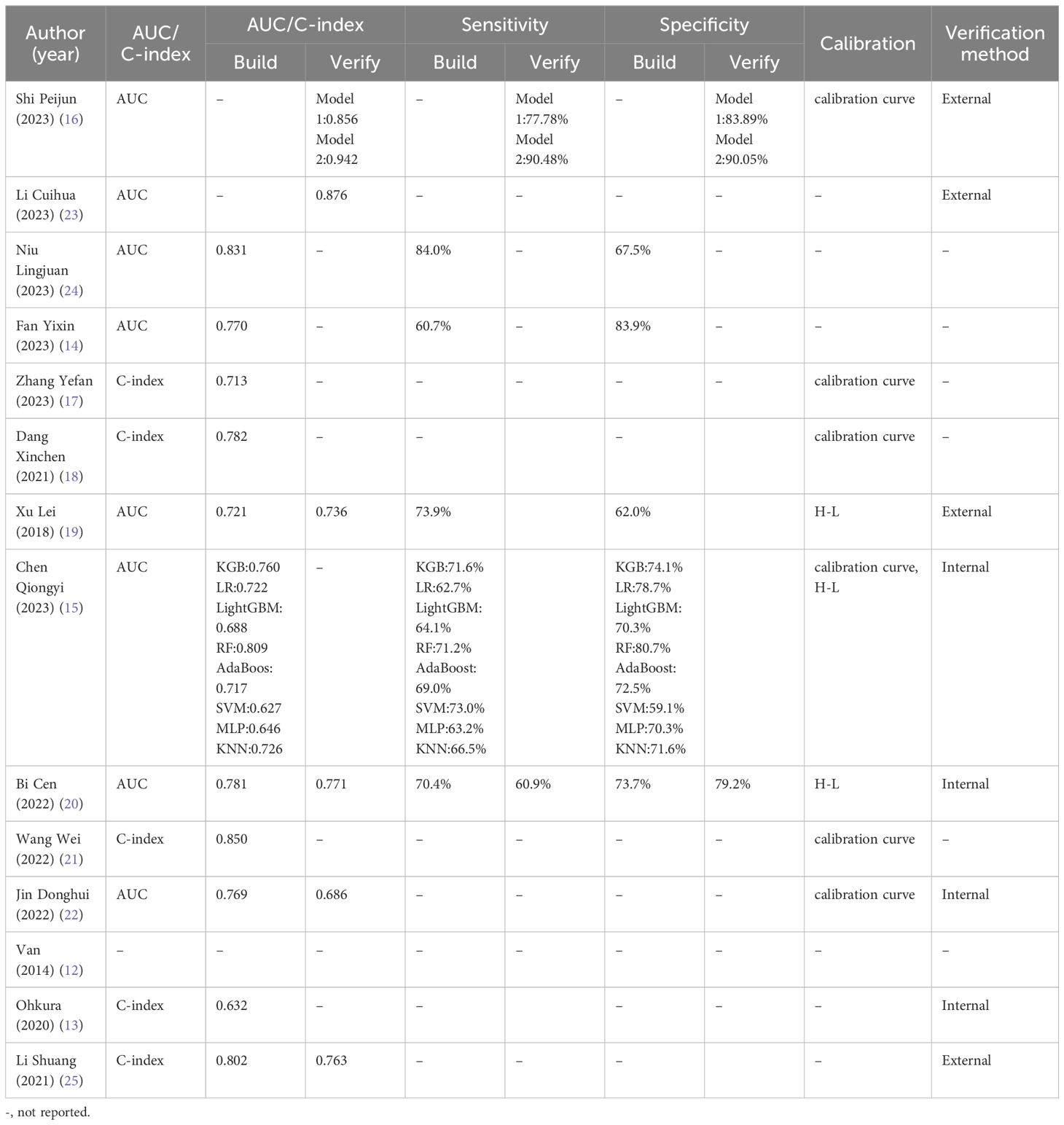
Table 3 Performance of POP risk prediction model for EC (n=14).
3.5 Risk of bias and applicability evaluation
All included studies had good applicability regarding the study population, predictors, and outcome domains. However, the overall risk of bias was high, indicating methodological issues in either the development or validation of the model. For risk of bias assessment, In the participant domain, 11 studies (13–15, 17–23, 25) were identified as having a high risk of bias, primarily due to their reliance on retrospective data. In the domain of predictor variables, all included studies were rated at low risk of bias. In the outcome domain, five studies (12, 17, 23–25) had uncertain forecast times. In addition, Ohkura Y (13) did not report diagnostic criteria for POP. In the area of analyses, two studies (13, 22) evaluated the results as having an unclear risk of bias, and the rest of the studies were assessed as having a high risk of bias in this area. The model risk of bias and applicability evaluations are shown in Table 4.
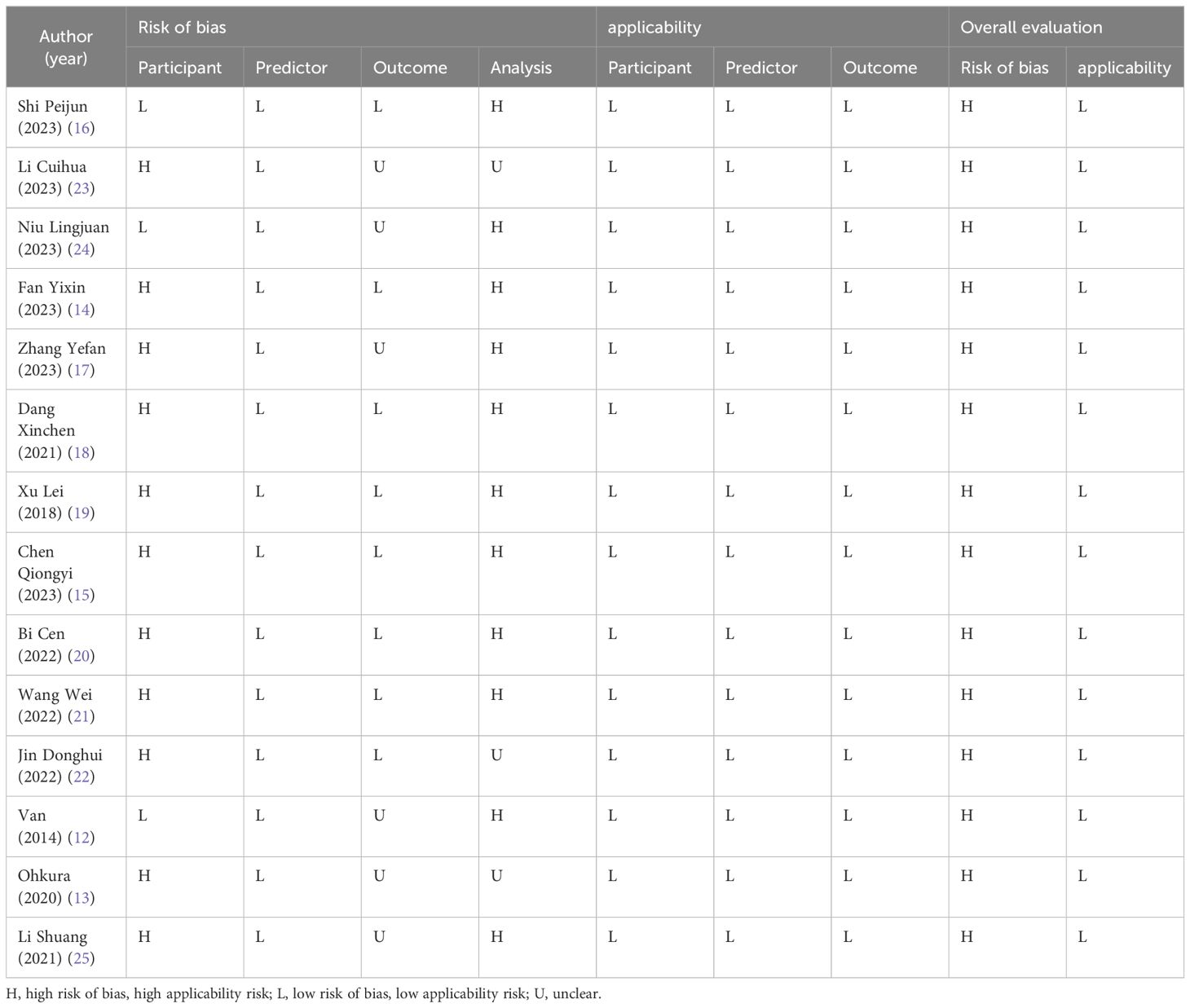
Table 4 Evaluations of the bias risk and applicability of the included models (n=14).
4 Discussion
4.1 Efficacy of a prediction model for the POP in patients with EC and risk of bias analysis
This systematic review ultimately included 14 relevant studies reporting 23 models. The included models performed well in terms of applicability assessment and model differentiation. The mean AUC of model differentiation was 0.741.
However, the included studies also showed significant limitations in the evaluation of risk of bias, primarily attributable to the following reasons:(1) Inappropriate data sources: 78.57% of the studies in this review used a retrospective study design, and relevant factors, such as patients’ social support status, education level, and knowledge of the disease, could not be included, which resulted in an incomplete prediction factor prone to bias. (2) Insufficient sample size: In model development studies, 13 studies (12–22, 24, 25) had an event per variable (EPV) <20, and a low EPV can lead to overfitting of the model (11). In model external validation studies, the assessment of model performance may be overestimated when the outcome event (number of POP cases occurring) is <100 (33). However, in the external model validation, we found that only the study by Xu (19) fulfilled the sample size requirement. (3) Inappropriate treatment of continuous variables: three studies (14, 19, 20) converted predictors of continuous variables into categorical variables in model construction and did not state the basis for categorization. (4) Inappropriate treatment of missing data: Six studies (12, 15, 17–20) used the direct exclusion method to deal with missing data, which may lead to the researchers ignoring the potential predictor variables in the excluded subjects, thus affecting the final data quality. (5) Incomplete assessment of model performance: Six studies (12–14, 23–25) did not report the calibration of the model, which may not be able to assess the actual prediction accuracy of the model and cause bias. (6) Only four studies (13, 15, 20, 22) performed internal validation and four studies (16, 19, 23, 25) performed external validation; the lack of internal validation makes the problem of overfitting easy to be ignored (34); furthermore, it is detrimental to the clinical promotion of the model’s application.
At present, there is still a problem of heavy development but light validation in the field of predictive model construction, and some studies only perform model construction and ignore the importance of the actual clinical application of predictive models. To improve reporting and study quality, the PROBAST (11) assessment criteria can be useful. In terms of study design, prospective or randomized controlled studies should be conducted according to these assessment criteria, and a sufficiently large study sample size should be selected to reduce the difference between the study population and the actual population. In terms of data processing, variables and missing data should be treated rigorously. Commonly used methods for processing missing data include interpolation, deletion, and weighting (35), which are reasonable methods for accurately reflecting the characteristics of the population at risk. Furthermore, the use of objective tools is necessary to assess model performance, validate the model internally and externally to ensure the model’s practicability and popularization in clinical application, enhance the persuasiveness and accuracy of the study, and reduce the risk of bias.
4.2 Predictor analysis of a predictive model for POP risk in patients with EC
Because of differences in the diagnosis of POP, the predictive variables included, and research organizations, the risk factors that induce POP are both different and common across studies.In this study, the five most frequent predictor variables of risk for POP in patients with esophageal cancer were found to be: smoking, age, respiratory disease (COPD), diabetes mellitus, and surgical procedure (Open chest surgery).
Elderly individuals are one of the populations most affected by POP, and with age, there are degenerative changes in body functions. One study (36) found that the risk of POP was 2.68 times higher in the older population than in those aged <60 years. In older adults, lung tissue defenses are lower. Furthermore, immunity declines with age. The immune response reduces alveolar macrophage function, which can lead to the development of lung infections (18). Smoking contributes to the development of respiratory symptoms, and the risk of respiratory symptoms is proportional to the duration and amount of smoking (37). Harmful substances in tobacco irritate the respiratory tract, damage the respiratory mucosa, and affect the cilia’s ability to clean, resulting in excessive mucus secretion that cannot be cleared by lung tissues, thus increasing the risk of lung infections (38). Guidelines (39) recommend that patients undergoing esophagectomy should quit smoking for at least 4 weeks before surgery to reduce the incidence of lung disease. Furthermore, healthcare professionals should encourage perioperative patients to quit smoking and perform respiratory exercises to prevent POP. Moreover, patients with chronic obstructive pulmonary disease, emphysema, and other chronic respiratory diseases before surgery have high amounts of secretions in the respiratory tract that are not easy to cough up, which increases the risk of POP to a certain extent (15). Patients with diabetes mellitus should actively control their blood glucose levels before surgery, and a hyperglycemic environment is conducive to bacterial reproduction and induces infection (16). Relevant guidelines (39) recommend minimally invasive luminal surgery as the primary treatment modality for patients undergoing EC surgery. Compared with minimally invasive luminal surgery, traditional surgery is traumatic, and postoperative patients often do not dare to cough due to wound pain; therefore, they cannot expel sputum in time, thus inducing POP (20). Clinical staff should pay attention to the perioperative assessment of elderly patients, preoperative patients with underlying lung diseases and diabetes mellitus, and smoking patients and efficiently identify high-risk groups. For high-risk patients, healthcare professionals should provide detailed perioperative education, supervise patients to quit smoking, and control blood glucose levels to improve the patient’s awareness of the risk of lung infection and select the optimal surgical treatment plan according to the patient’s condition.
Note that most risk prediction studies have neglected the potential impact of perioperative laboratory indicators. The laboratory indicator that appeared most frequently in the studies included in this article was albumin, and only three studies (13, 24, 25) have reported that a decrease in the body’s albumin levels not only caused a decrease in the patient’s immunity but also was accompanied by a decrease in plasma osmolality, which induces lung infection (25). Note that Xu (19) identified the significance of postoperative fasting blood glucose levels ≥7.1 in predicting POP development. Most studies have primarily focused on history of diabetes mellitus as a crucial risk factor for POP, often overlooking the harmful effects of transient hyperglycemia. Transient hyperglycemia is not diabetes mellitus; it may indicate stress-induced hyperglycemia, which compromises leukocyte bactericidal capacity and elevates the risk of POP (40). Therefore, perioperative laboratory indicators are also important predictors of the occurrence of POP in patients with EC; however, they have been ignored by researchers because of limited data acquisition caused by differences in the types of studies and medical equipment. Relevant risk factors should be comprehensively and systematically included in the future, aiming to prevent the occurrence of POP to the greatest extent possible.
4.3 Future trends and challenges in the predictive modeling of POP risk in patients with EC
Research on POP risk prediction models for patients with EC started late, and there has been a rapid development trend in the past 2 years; however, the effectiveness of these models varies. External validation studies on most developed models are limited. Among the models included in this study, only 28.57% of the studies (16, 19, 23, 25) conducted external validation. Weijs (31) and Seesing (32) performed internal and external validation of van’s scoring system with outstanding predictive results (12), offering novel insights for the clinical diagnosis of POP. However, note that this validation was limited to the United States and the Netherlands, necessitating further investigation into the applicability of the model in other regions. Ohkura conducted a multicenter study using data from the Japanese National Clinical Data Bank (13); however, because of a lack of standardized surgical teams, the model exhibited poor predictive efficacy. The nomogram prediction model of Shi had good model efficacy in external validation (16), which contained nine predictive entries; however, serological indicators, such as PCT, IL-1β, sTREM-1, and CD4+/CD8+, among the predictors under study, were difficult to obtain and expensive, which was not conducive to the generalization of the predictive factors in clinical practice. The model of Li (25) contained four predictive entries: hospitalization time, albumin, intraoperative bleeding, and perioperative transfusion, which are relatively easy to obtain in clinical work and are more likely to be adopted by healthcare professionals. However, Li’s model was only externally validated, and external validation is required to strengthen the stability and persuasiveness of the model based on internal validation. Chen (15) and Fan (14) analyzed the risk factors of vulnerable populations by constructing a POP risk prediction model for elderly patients with EC, suggesting that future researchers should consider conducting risk prediction modeling studies for different target populations. With the rise of big data applications, researchers have begun to attempt developing modeling techniques. Chen (15) constructed eight models based on machine learning methods; however, the model lacked external validation to assess its accuracy, which encourages future researchers to try new modeling techniques based on machine learning to build models with stronger predictive capabilities.
Six diagnostic criteria for POP exist for the studies included in this study. Fortunately, We found commonalities in these diagnostic criteria based on authoritative, evidence-based evidence. These diagnostic criteria are based on the clinical signs of infection, such as increased leukocyte count, increased sputum in the respiratory tract, increased body temperature, and imaging tests. We remain hopeful that in the future, there will be a globally recognized and uniform diagnostic standard for POP that will facilitate the predictive power and generalizability of inter-model comparisons.
4.4 Recommendations for future research
Currently, the predictive variables of POP risk among patients undergoing EC surgery are not well unified. In the future, studies can be conducted based on the risk factors for POP occurrence in different surgical procedures or special populations; more high-quality models can be constructed; and multicenter and large-sample internal and external validation can be conducted to improve the persuasiveness and accuracy of the models. Furthermore, researchers must consider the feasibility and simplicity of models in clinical practice, identify potential problems in model application early, and improve them. The perioperative training of healthcare workers is also an issue that should not be ignored. Understanding the acceptability and workload of healthcare workers and encouraging them to propose limitations of model application and improve them will enhance the trust of clinical workers on the theoretical basis and facilitate the practical application of the model.
5 Conclusion
In conclusion, the 14 studies of POP risk prediction models for patients with EC included in this study had high model efficacy and applicability; however, the overall risk of bias was high, different predictor variables among different studies were not quantitatively analyzed, and most models were not externally validated, resulting in poor model generalization. Future studies may adopt prospective, randomized controlled methods for model construction and internal and external validation. Multicenter and large-sample validation studies based on existing models should be conducted to enhance the generalizability of the models in clinical applications. The use of machine learning and other emerging technologies must be considered to develop predictive models with good predictive performance, high accuracy, and ease of operation, to provide a theoretical basis for their clinical applications.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
YJ: Writing – original draft, Writing – review & editing. ZL: Data curation, Writing – review & editing. WJ: Data curation, Writing – review & editing. TW: Formal analysis, Writing – review & editing. BC: Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Natural Science Foundation of Fujian Province (Grant NO.2021J01875) and Medical Innovation Project of Fujian Provincial Health Commission (Grant NO.2020CXB035).
Acknowledgments
We would like to thank the researchers and study participants for their contributions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zheng RS, Chen R, Han BF, Wang SM, Li L, Sun KX, et al. Cancer incidence and mortality in China, 2022. Chin J Oncol. (2024) 46:221–31. doi: 10.3760/cma.j.cn112152-20240119-00035
2. Zheng XD, Li SC, Lu C, Zhang WM, Hou JB, Shi KF, et al. Safety and efficacy of minimally invasive McKeown esophagectomy in 1023 consecutive esophageal cancer patients: a single-center experience. J Cardiothor Surg. (2022) 17:36. doi: 10.1186/s13019-022-01781-2
3. Group of Key Site Infection control, Nosocomial Infection Control Commission, Chinese Preventive Medicine Association. Expert consensus on prevention and control of postoperative pneumonia. Chin J Clin Infect Dis. (2018) 11:11–9. doi: 10.3760/cma.j.issn.1674-2397.2018.01.003
4. Simonsen DF, Thomsen RW. Response to Letter to the Editor: “Risk factors for postoperative pneumonia after lung cancer surgery and impact of pneumonia on survival. Respir Med. (2016) 112:133. doi: 10.1016/j.rmed.2016.01.004
5. Debray TP, Damen JA, Snell KI, Ensor J, Hooft L, Reitsma JB, et al. A guide to systematic review and meta-analysis of prediction model performance. BMJ. (2017) 356:i6460. doi: 10.1136/bmj.i6460
6. Heus P, Damen J, Pajouheshnia R, Scholten RJ, Reitsma JB, Collins GS, et al. Poor reporting of multivariable prediction model studies: towards a targeted implementation strategy of the TRIPOD statement. BMC Med. (2018) 16:120. doi: 10.1186/s12916-018-1099-2
7. van Nieuw AM, de Grooth HJ, Veerman GL, Ziesemer KA, van Berge Henegouwen MI, Tuinman PR. Prediction of morbidity and mortality after esophagectomy: A systematic review. Ann Surg Oncol. (2024) 31(5):3459–70. doi: 10.1245/s10434-024-14997-4
8. Grantham JP, Hii A, Shenfine J. Preoperative risk modelling for oesophagectomy: A systematic review. World J Gastrointest Surg. (2023) 15:450–70. doi: 10.4240/wjgs.v15.i3.450
9. Wang ZY, Lu CC, Zhang JL, Huang JY, Liu WD, Shang WR, et al. Interpretation of checklist for transparent reporting of multivariable prediction models for individual prognosis or diagnosis tailored for systematic reviews and meta-analyses(TRIPOD-SRMA). Chin J Evidence-Based Med. (2024) 24:202–10. doi: 10.7507/1672-2531.202308041
10. Moons KG, de Groot JA, Bouwmeester W, Vergouwe Y, Mallett S, Altman DG, et al. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: the CHARMS checklist. PloS Med. (2014) 11:e1001744. doi: 10.1371/journal.pmed.1001744
11. Moons K, Wolff RF, Riley RD, Whiting PF, Westwood M, Collins GS, et al. PROBAST: A tool to assess risk of bias and applicability of prediction model studies: explanation and elaboration. Ann Intern Med. (2019) 170:W1–W33. doi: 10.7326/M18-1377
12. van der Sluis PC, Verhage RJ, van der Horst S, van der Wal WM, Ruurda JP, van Hillegersberg R. A new clinical scoring system to define pneumonia following esophagectomy for cancer. Dig Surg. (2014) 31:108–16. doi: 10.1159/000357350
13. Ohkura Y, Miyata H, Konno H, Udagawa H, Ueno M, Shindoh J, et al. Development of a model predicting the risk of eight major postoperative complications after esophagectomy based on 10 826 cases in the Japan National Clinical Database. J Surg Oncol. (2020) 121:313–21. doi: 10.1002/jso.25800
14. Fan YX, Xu SN, Liu Y, Lu FF. Analysis of risk factors of postoperative pulmonary infection in elderly patients with esophageal cancer. Geriatrics Health Care. (2023) 29:49–53. doi: 10.3969/j.issn.1008-8296.2023.01.012
15. Chen QY. A machine learning-based prediction model for minimally invasive postoperative pneumonia in elderly people with esophageal cancer. Anesthesiology, Shantou: Shantou University (2023).
16. Shi PJ, Yan P, Jian LH. Construction of a Lasso-Nomogram risk prediction model for postoperative infection of esop-hageal cancer. J Guangxi Med Univ. (2023) 40:1850–6. doi: 10.16190/j.cnki.45-1211/r.2023.11.012
17. Zhang YF. Analysis of risk factors for postoperative pulmonary infection in patients with esophageal cancer and construction of nomogram. Surgery, Dalian: Dalian Medical University (2023).
18. Dang XC. Analysis of risk factors for patients with pulmonary infection after radical resection of esophageal cancer and establishment of nomogram prediction risk model. Clinical Medicine, Xinxiang: Xinxiang Medical College (2021).
19. Xu L. Analysis of risk factors for pneumonia after esophagectomy and establishment of a risk predictive model. Thoracic Surgery, Zhengzhou: Zhengzhou University (2018).
20. Bi C. Construction and validation of risk prediction model for postoperative pulmonary infection of esophageal cancer. Nursing, Zhenjiang: Jiangsu University (2022).
21. Wang W, Yu Y, Sun H, Wang Z, Zheng Y, Liang G, et al. Predictive model of postoperative pneumonia after neoadjuvant immunochemotherapy for esophageal cancer. J Gastrointest Oncol. (2022) 13:488–98. doi: 10.21037/jgo
22. Jin D, Yuan L, Li F, Wang S, Mao Y. A novel nomogram predicting the risk of postoperative pneumonia for esophageal cancer patients after minimally invasive esophagectomy. Surg Endosc. (2022) 36:8144–53. doi: 10.1007/s00464-022-09249-z
23. Li CH, Qian XL, Li LY, Xie ZY. Construction of a predictive model for lung infection after radical resection of esophageal cancer. J Esophageal Dis. (2023) 5:117–21. doi: 10.15926/j.cnki.issn2096-7381.2023.02.008
24. Niu LJ, Wang LL, Lu DX, Wang YM, Ren MY. Etiological characteristics of postoperative pulmonary infection in esophageal cancer patients and establishment of risk prediction model. Chin J Nosocomiol. (2023) 33:1504–7. doi: 10.11816/cn.ni.2023-221541
25. Li S, Su J, Sui Q, Wang G. A nomogram for predicting postoperative pulmonary infection in esophageal cancer patients. BMC Pulm Med. (2021) 21:283. doi: 10.1186/s12890-021-01656-7
26. Zhang QL, Li KP, Huang M, Chen RC. Proceedings of the 2018 annual academic conference of the Chinese medical association branch of respiratory diseases. Chin J Tubercul Respir Dis. (2018) 12):989–91. doi: 10.3760/cma.j.issn.1001-0939.2018.12.021
27. Ministry of Health of the People’s Republic of China. Diagnostic criteria for Nosocomial infection (Trial). Natl Med J China. (2001) 81:314–20. doi: 10.3760/j:issn:0376-2491.2001.05.027
28. American Thoracic Society A, Infectious Diseases Society Of America I. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. (2005) 171:388–416. doi: 10.1164/rccm.200405-644ST
29. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. (2004) 240:205–13. doi: 10.1097/01.sla.0000133083.54934.ae
30. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. (2008) 36:309–32. doi: 10.1016/j.ajic.2008.03.002
31. Weijs TJ, Seesing MF, van Rossum PS, Koëter M, van der Sluis PC, Luyer MD, et al. Internal and external validation of a multivariable model to define hospital-acquired pneumonia after esophagectomy. J Gastrointest Surg. (2016) 20:680–7. doi: 10.1007/s11605-016-3083-5
32. Seesing M, Wirsching A, van Rossum P, Weijs T, Ruurda J, van Hillegersberg R, et al. Defining pneumonia after esophagectomy for cancer: validation of the Uniform Pneumonia Score in a high volume center in North America. Dis Esophagus. (2018) 31(6). doi: 10.1093/dote/doy002
33. Collins GS, Ogundimu EO, Altman DG. Sample size considerations for the external validation of a multivariable prognostic model: a resampling study. Stat Med. (2016) 35:214–26. doi: 10.1002/sim.6787
34. Moons KG, Kengne AP, Woodward M, Royston P, Vergouwe Y, Altman DG, et al. Risk prediction models: I. Development, internal validation, and assessing the incremental value of a new (bio)marker. Heart. (2012) 98:683–90. doi: 10.1136/heartjnl-2011-301246
35. Deng JX, Shan LB, He DQ, Tang R. Processing method of missing data and its developing tendency. Stat Decision. (2019) 35:28–34. doi: 10.13546/j.cnki.tjyjc.2019.23.005
36. Wang MX, Zhou CJ, Ji XC, Gao Q, Lin LJ, Cai BQ. Risk factors for postoperative pulmonary infection in patients with esophageal cancer:Asystematic review and meta-analysis. Chin J Clin Thorac Cardiovasc Surg. (2023) 30:1467–74. doi: 10.7507/1007-4848.202106031
37. Cha ZQ, He YZ, Xu W, Chen YJ, Liu XY, Liu ZR, et al. Effects of smoking on chronic obstructive pulmonary disease and respiratory symptoms. Chin J Dis Control Prev. (2020) 24:46–51. doi: 10.16462/j.cnki.zhjbkz.2020.01.010
38. Crotty AL, Shin S, Hwang JH. Inflammatory diseases of the lung induced by conventional cigarette smoke: A review. Chest. (2015) 148:1307–22. doi: 10.1378/chest.15-0409
39. Low DE, Allum W, De Manzoni G, Ferri L, Immanuel A, Kuppusamy MK, et al. Guidelines for perioperative care in esophagectomy: enhanced recovery after surgery (ERAS(®)) society recommendations. World J Surg. (2019) 43:299–330. doi: 10.1007/s00268-018-4786-4
Keywords: postoperative pneumonia, risk prediction, modelling, esophageal cancer, system review
Citation: Jiang Y, Li Z, Jiang W, Wei T and Chen B (2024) Risk prediction model for postoperative pneumonia in esophageal cancer patients: A systematic review. Front. Oncol. 14:1419633. doi: 10.3389/fonc.2024.1419633
Received: 18 April 2024; Accepted: 18 July 2024;
Published: 05 August 2024.
Edited by:
Ulrich Ronellenfitsch, Martin-Luther-University Halle-Wittenberg, GermanyReviewed by:
Connor J. Wakefield, Rush University, United StatesFredrik Klevebro, Karolinska Institutet (KI), Sweden
Copyright © 2024 Jiang, Li, Jiang, Wei and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bizhen Chen, NTczMDczMTk4QHFxLmNvbQ==