 Yujing Zou
Yujing Zou Shanshan Zhai
Shanshan Zhai Jiawen Dong
Jiawen Dong Tianyu Zhao
Tianyu Zhao Jin Yang
Jin Yang- School of Clinical Medicine, Hangzhou Normal University, Hangzhou, China
Breast cancer imposes a substantial global health burden, with survivors frequently experiencing post-treatment quality of life deficits and chronic fatigue. While art therapy has gained recognition as a potential adjuvant intervention, its therapeutic value remains debated. To evaluate art therapy’s efficacy, we conducted an exhaustive search of major electronic databases through October 2023, identifying 22 eligible RCTs reported in 22 papers that met predefined inclusion criteria from major databases including Web of Science Core Collection, Cochare, Embase, and Pubmed. Study quality was assessed using Cochrane risk-of-bias tools, with data extraction and analysis performed in RevMan 5.3. In this meta-analysis, we aimed to investigate the effect of art therapy on quality of life and fatigue in breast cancer patients. As of October 2023, relevant randomized controlled studies were searched from relevant electronic databases and articles were screened, quality evaluated, and data related to quality of life and fatigue were extracted and analysed using RevMan 5. 3. A total of 22 randomized controlled studies from 22 papers were included in this analysis. The results obtained according to this analysis included the effect of art on quality of life in breast cancer: SMD=0.38 (95% CI, 0.25 to 0.51; P≤0.00001), the fatigue-related indices: SMD=-0.03 (95% CI, -0.21 to 0.15; P=0.73). The effect of intervention time less than two months: SMD=0.21 (95% CI, -0.01 to 0.43; P=0.07), more than or equal to two months: SMD=0.45 (95% CI, 0.28 to 0.62; P<0.00001). Different types of interventions: art therapy in painting and calligraphy: SMD=0.09 (95% CI, -0.17 to 0.35; P=0.49), music-included art therapy: SMD=0.51 (95% CI, 0.32 to 0.70, P<0.00001), music-out-of-treatment art therapy: SMD=0.44 (95% CI, 0.19 to 0.69; P=0.0005). Follow-up time greater than or equal to six months: SMD=0.14 (95% CI, -0.09 to 0.36; P=0.22), follow-up time less than six months: SMD=-0.34 (95% CI, -0.64 to -0.04; P=0.03). In summary, this analysis demonstrated that art therapy improved quality of life, but the effects of fatigue reduction only occur within six months, with the degree of the benefits being correlated with the type, length, and timing of the intervention.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/myprospero, identifier CRD42023476055.
1 Introduction
Breast cancer constitutes the leading malignancy and primary oncologic mortality cause in women globally (1). WHO surveillance data position it as the most prevalent neoplasm worldwide, surpassing lung cancer incidence rates, thus establishing breast cancer management as a critical global health challenge requiring urgent multidisciplinary attention. Conventional surgical resection, adjuvant chemotherapy, radiation therapy, and other therapies are used to treat breast cancer. But these surgical techniques frequently result in adverse consequences including anxiety, sleeplessness, and exhaustion. Relevant research has revealed that breast cancer patients have a much worse quality of life than the general population, which will have a major effect on the patients’ day-to-day lives (2). There are two main causes of the side effects: first, the surgery’s aftermath damages the patient’s self-esteem and perception, which causes sleeplessness, anxiety, and other dysfunctions (3). Secondly, the patient’s own fear of cancer and uncertainty about the outcome of the treatment may exacerbate a number of psychological disorders, including depression, fatigue, and other psychological disorders. Thus, in order to enhance and restore patients’ feeling of well-being, it is critical to concentrate on the side effects of breast cancer and look for beneficial and efficient therapies to improve tiredness, sleep, and quality of life.
Art therapy has been defined as “a form of psychotherapy in which art media are used as the primary means of expression and communication with the goal of enabling the recipient to change and grow on a personal level through the use of art materials in a safe and accessible environment” by the British Association of Art Therapists (4), and its non-invasive, secure, and adaptable qualities have drawn interest in recent years. Painting, music, dance, and other media are examples of art therapies. It is noteworthy that in this study, yoga was also included in this category because yoga encourages self-expression of the individual through the integration of the body and mind through forms of asana, breathing, and meditation, which is in line with the definition and goals of art therapy.
A growing body of systematic reviews has established consensus regarding the therapeutic potential of art-based interventions in breast cancer care, with particular emphasis on their benefits for health-related quality of life (QOL) (5, 6). Notably, a randomized controlled trial highlighted tango therapy’s unique benefits for dance-naïve patients, showing significant improvements in cancer-related fatigue (CRF) scores and QOL indices through structured dance protocols (7).However, the academic discourse reveals notable discrepancies in empirical findings across different art therapy subdomains. Contrary to movement-based approaches, a clinical trial evaluating creative art therapy demonstrated no statistically significant reduction in generalized fatigue among breast cancer survivors at one-month post-radiation follow-up (8). This therapeutic incongruity extends to mind-body interventions, where a study examining yoga-integrated art therapy failed to replicate the fatigue-alleviating effects observed in other somatic modalities (9).
Given the substantial heterogeneity in existing evidence and the limited evidence confirming mood-related outcomes of specific art therapy modalities, a focused meta-analysis was conducted to clarify art therapy’s precise effects on quality of life and fatigue in breast cancer populations. To address evidence gaps, this analysis introduces a novel dimensional framework by implementing subgroup stratification. First, art interventions were categorized into process-oriented modalities (self-expressive painting/writing) versus receptive-based modalities (music/yoga engagement) to elucidate mechanistic differences in therapeutic action. Second, multi-temporal assessments (≤2 or >6 months post-intervention) were incorporated to map the trajectory of therapeutic benefits.
2 Method
We registered on the PROSPERO website in October 2023, and provided the registration number CRD42023490915.
2.1 Literature and research
The database used for this study is derived from major electronic databases, and we consulted electronic databases such as the Web of Science Core Collection, Cochare, Embase, Pubmed, and other databases. To construct a reasonable formula for searching for relevant research literature while searching literature, it is possible to use ‘xxx’ to search for relevant research literature, like Pubmed(“art therapy” [MeSH Terms] OR “Art Therapies” OR “Art Therapies” OR “Music” [MeSH Terms] OR “Music Therapy” OR “Therapy, Music” OR “paint” [MeSH Terms] OR “paint” OR “drawing” OR “drawings”OR “draw”OR “Dance” [MeSH Terms] OR “Dance Therapy” OR “Dance Therapies” OR “Drama Therapy” [MeSH Terms] OR “Dramatherapy” OR “Supportive-Expressive therapy” OR “Writing therapy”) AND (“Breast Cancer” [MeSH Terms] OR “Mammary Cancer” OR “Breast Neoplasms” OR “Breast Tumor” OR “Cancer of the Breast”) AND((“Quality of Life” [MeSH Terms] OR “Life Quality” OR “HRQOL” OR “Quailty of sleep”) OR (“fatigue” [MeSH Terms] OR “Lassitude”)).
2.2 Inclusion and exclusion criteria
For the subsequent screening of qualified literature, all the initial obtained literature was imported into EndNote X9. The researchers devised inclusion and exclusion criteria that were consistent with the PICOS principle during literature screening. The inclusion criteria are: (1) the experiment type must be randomized controlled (RCT); (2) the experimental subjects are women who have breast cancer; (3) the intervention must be art intervention without limiting the type of art used, including music, painting, yoga and so on, and the control measure is conventional treatment without art intervention; (4) the full text of the literature can be obtained, and the mean and standard deviation of the experimental group and the control group can be provided or calculated; (5) the indicators used to measure the outcomes included PSQI, ISI, MOS-sleep, WHO, FACT-G, FACT-B, QoL, QLQ-C30, and others. The exclusion criteria were: (1) exclusion of non-RCT trials, reviews, systematic evaluations, Meta-analyses, and animal experiments; (2) exclusion of literature that did not meet the literature inclusion criteria. Two researchers conducted an independent double-blind screening of the qualified literature, following the criteria, and a third researcher was hired to make a decision on controversial articles.
2.3 Quality evaluation
The study’s literature was evaluated from seven aspects using Review Manage 5. 3 software’s Cochrane system evaluation ‘risk bias evaluation’ tool:fixed allocation method, hidden allocation method, blind subjects, blind result evaluator, data result integrity, selective reports and other biases,and each quality evaluation item was evaluated according to three categories: low risk, unclear and high risk. 22 included studies were assessed for risk of bias based on the criteria (Figure 1). In random sequence generation, 19 studies were low risk with guaranteed grouping randomization; 3 were uncertain with further confirmation of methodological reliability; in allocation concealment, 15 were low risk with effective prevention of information leakage; 8 were uncertain with unclear situation; in participant and researcher blinding, 12 were low risk with blinding implementation in place; 6 were uncertain with ambiguous blinding situation; and 5 were high risk with subjective factors Highly influenced. For outcome assessment blinding, 7 low risk, good test objectivity; 14 uncertain; 2 high risk, susceptibility to bias in test results; for incomplete outcome data, 19 low risk, complete data; 3 uncertain; for selective reporting, 18 low risk, standardized reporting; 4 uncertain; and for other bias, 9 low risk, good overall; 10 uncertain; 4 high risk, potential bias potential.
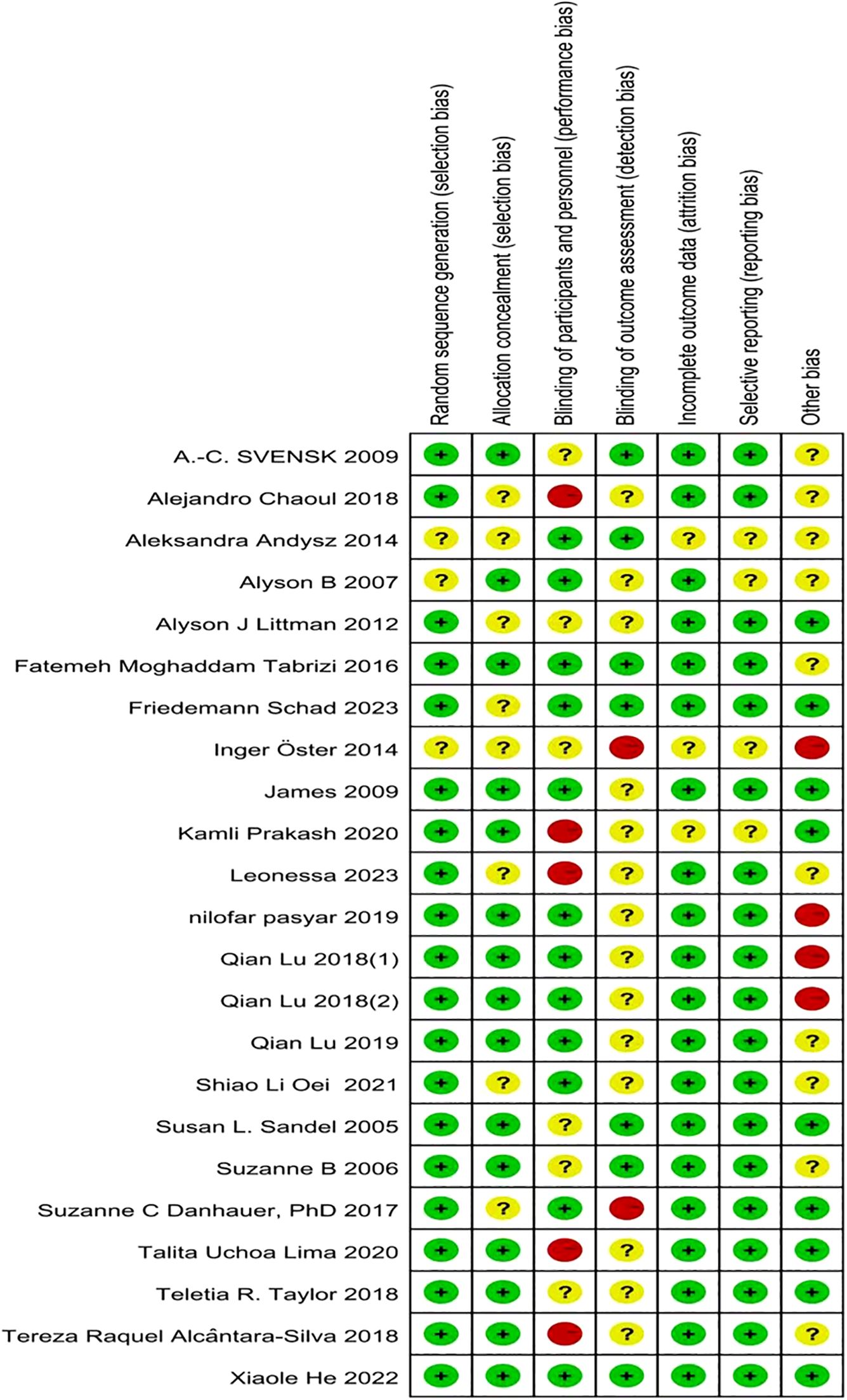
Figure 1. The risk-of-bias assessment for each of the included studies.
2.4 Statistical methods
Data was arranged with assistance from Review Manager (RevMan) version 5.3. Different scales were used in the studies to measure quality of life and fatigue. Indicating that these studies should be standardized before being included in the meta-analysis, the effect size of the standardized mean difference was expressed as Cohen’s d [95% confidence interval]; therefore, continuous variables were reported as scale scores and standardized mean difference (SMD). The Cochrane Collaboration was utilized to conduct meta-analyses of key fixed-effect outcomes, which revealed heterogeneity and expressed it in terms of I2 and effect sizes. I2 indicates the proportion of the total variation that is reflecting differences due to non-sampling errors. with I2 less than 25%, 50%, and 75% indicating low, medium, and high heterogeneity, respectively, so the choice of model for the analysis of the data therefore depended on the magnitude of I2. If I2 exceeds 50%, it means there is significant heterogeneity and a random effects model is employed. If I2 ≤ 50%, a fixed effects model is used. Small, medium, and large effect sizes were interpreted as Cohen’s d < 0.2, 0.2 ≤ d < 0.5, and d > 0.5. Statistical significance (p-value) was set at 0.05, and the combined results are presented graphically as forest samples.
3 Results
3.1 Assessment of identified trials
As shown in Figure 2, which is a flow chart of literature screening based on the PRISMA principle.we found a total of 2,620 articles in the database and eliminated 189 duplicates. 1562 articles were excluded based on their titles and abstracts. There are 851 remaining articles, 30 of which can’t retrieve the full text. Eligibility was assessed for 821 articles, and 799 were excluded due to exclusion criteria, resulting in a quantitative synthesis of 22 documents. Nine of the literature were related to fatigue and 15 were related to quality of life (Figure 2).
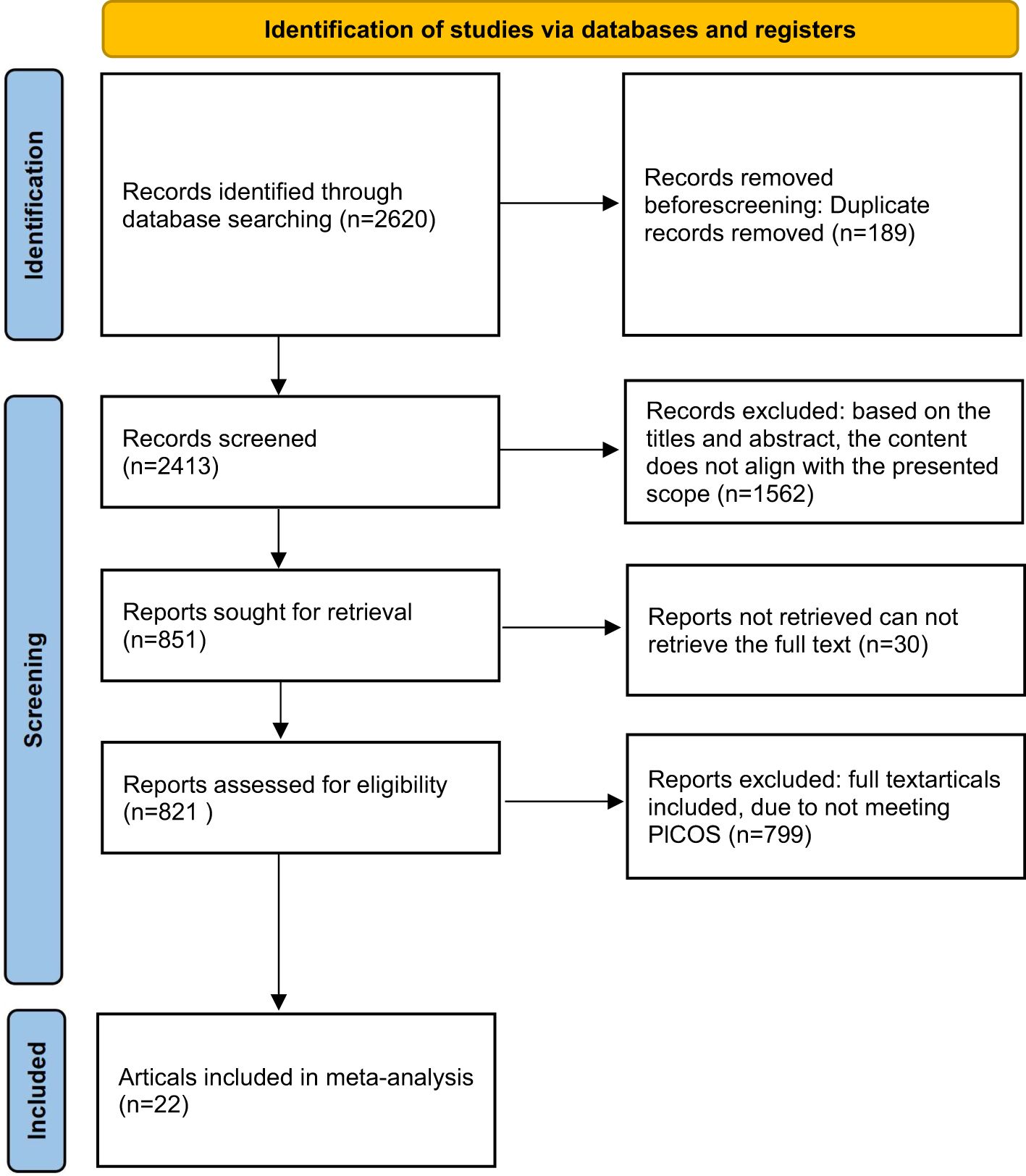
Figure 2. Literature screening flowchart.
3.2 Characterization of the literature
In total, there were 9 studies from the United States, 2 from Iran, 2 from Beazil, 3 from China, 1 from the United Kingdom, 2 from Germany, 1 from India, and 2 from Australia. All of the study types were RCTs. The studies included only female breast cancer patients. Table 1 describes the details of the interventions, which included 14 dynamic art therapies and 8 static art therapies. The former included yoga, dancing, or tango, and the latter included writing with positive psychological cues, supportive expression, drawing, and listening to music. All the art therapy interventions were under the supervision of qualified therapists. The length of the interventions were all focused on two to six months, with the two studies in LU having a shorter intervention of three weeks. The measure for the control group was usual care, but the measure for the control group in both of lu’s studies was write about their cancer facts unrelatedtoemotions, which we believe was set up to interfere with the factor of writing for the control. The primary outcome indicators were quality of life and fatigue index. The former indicator article measured with the QLQ-C30, FACT-B, FACT-G, QOL and WHOQOL-BREF scales, and the latter indicator was expressed with the FACT-F, BFI scale. The specific ones are shown in Table 1.
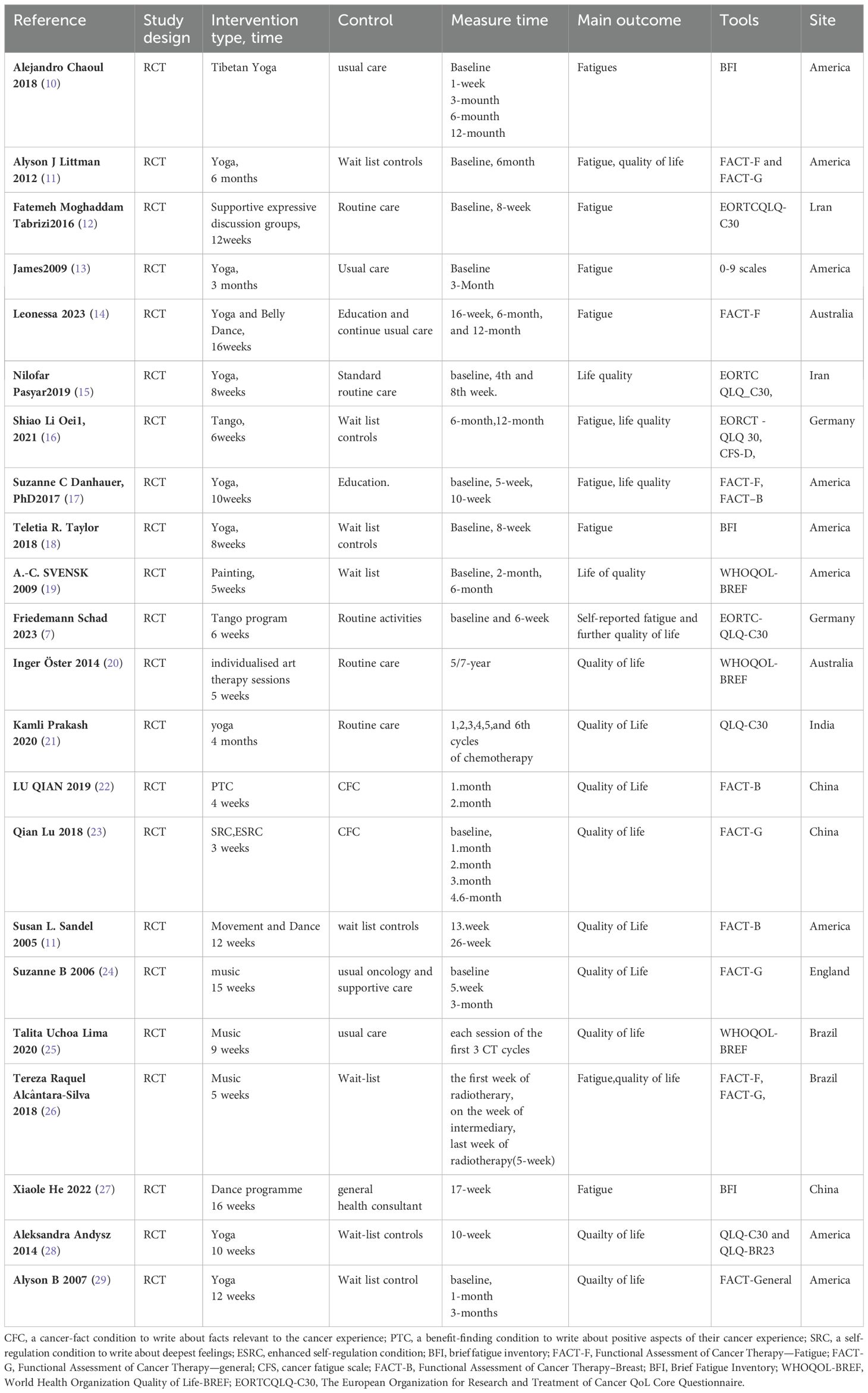
Table 1. Details of included studies.
3.3 Primary outcome
The total SMD of the effect of art on quality of life in breast cancer was 0.38 (95% CI, 0.25 to 0.51; P≤0.00001) (Figure 3). The total SMD of the effect of art therapy on fatigue-related indices in breast cancer patients was -0.03 (95% CI, -0.21 to 0.15; P=0.73) (Figure 4). In sensitivity analyses, excluding any of the articles, the two final results of the outcome indicators did not change significantly. The quality of life-related indicators experienced a decrease in heterogeneity from 47% to 24% as a result of the exclusion of one article (23). The heterogeneity dropped from 32% to 18% when one article study related to fatigue (14) was excluded.
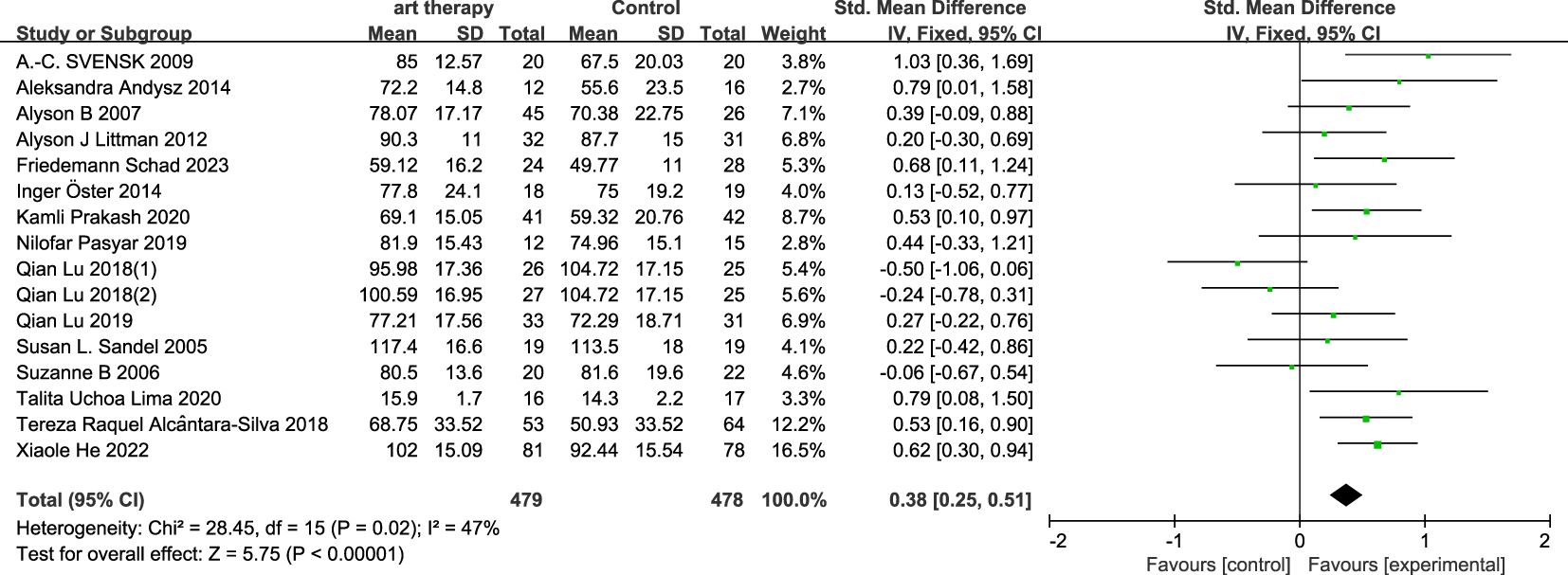
Figure 3. Influence of art therapy on quality of life of breast cancer patients.

Figure 4. Influence of art therapy on fatigue of breast cancer patients.
3.3.1 Subgroup analysis on quality of life
In the subgroup analysis of intervention length, art therapy with an intervention length of less than two months had an SMD of 0.21 (95% CI, -0.01 to 0.43; P=0.07) on quality of life for breast cancer patients, and with an intervention length of more than or equal to two months it had an overall SMD of 0.45 (95% CI, 0.28 to 0.62; P<0.00001) on breast cancer (Figure 5). In the subgroup categorization of art therapy domains, the total SMD for art therapy in the painting and writing category was 0.09 (95% CI, -0.17 to 0.35; P=0.49), the SMD for art therapy that included music (music, tango, and dancing) was 0.51 (95% CI, 0.32 to 0.70, P<0.00001), and art therapy that did not include music (yoga) had a SMD of 0.44 (95% CI, 0.19 to 0.69; P=0.0005) (Figure 6).
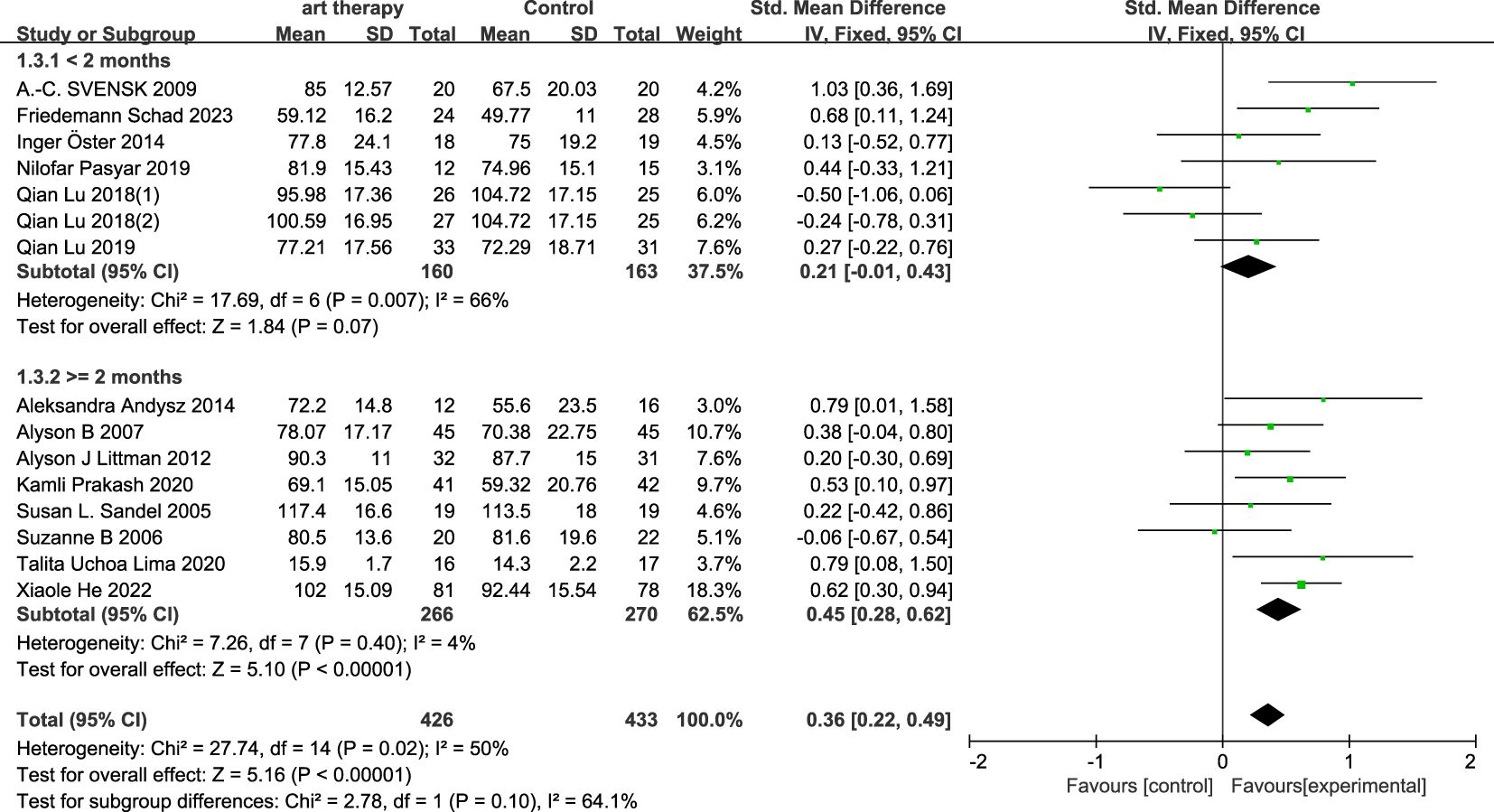
Figure 5. According to the types of intervention, the quality of life was analyzed in subgroups.
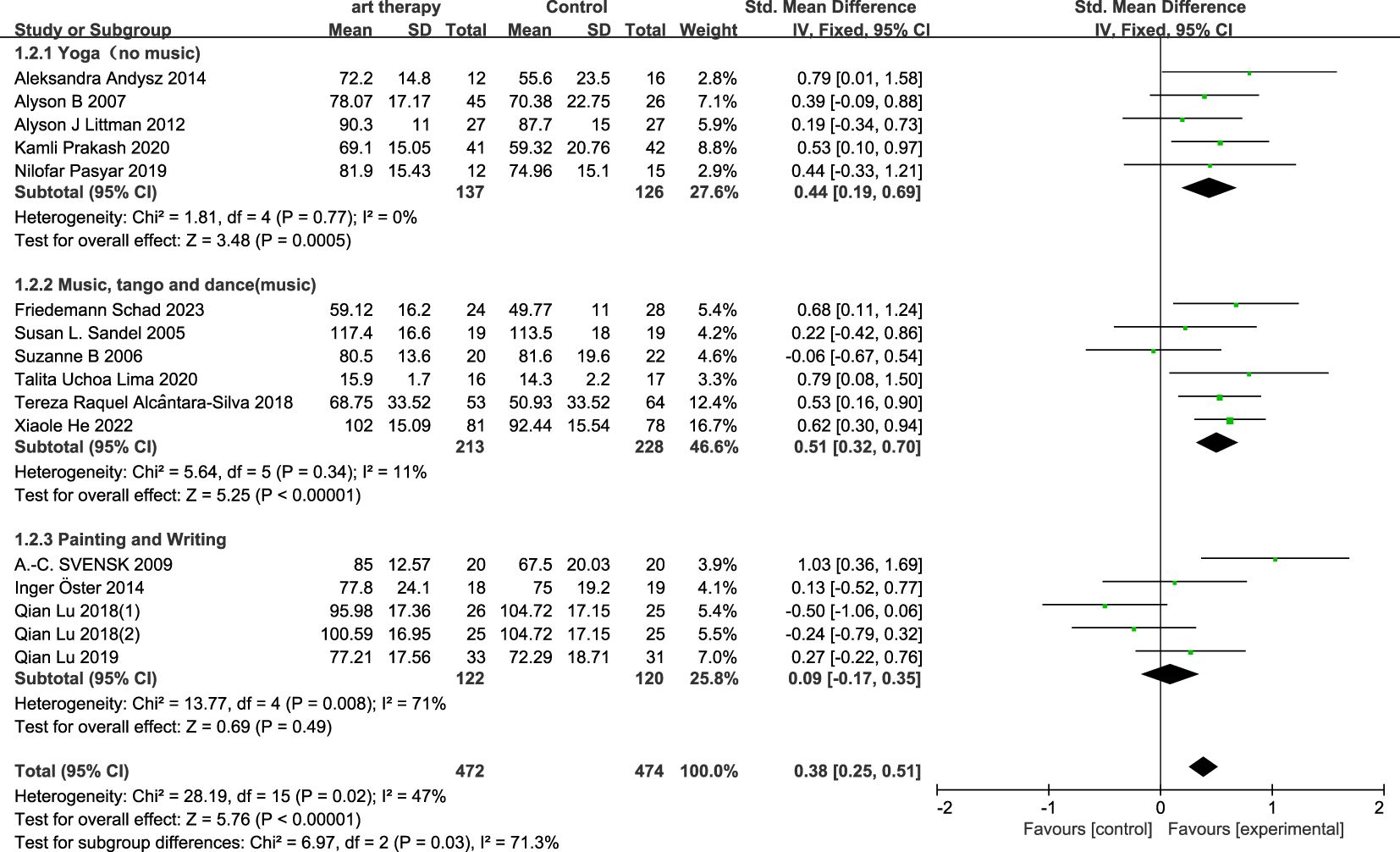
Figure 6. According to the intervention duration, the quality of life was analyzed in subgroups.
3.3.2 Subgroup analysis on fatigue
In the subgroup analysis of follow-up time, the SMD was -0.34 (95% CI, -0.64 to -0.04; P=0.03) for a follow-up length of less than 6 months and 0.14 (95% CI, -0.09 to 0.36; P=0.22) for a follow-up length of more than 6 months (Figure 7).
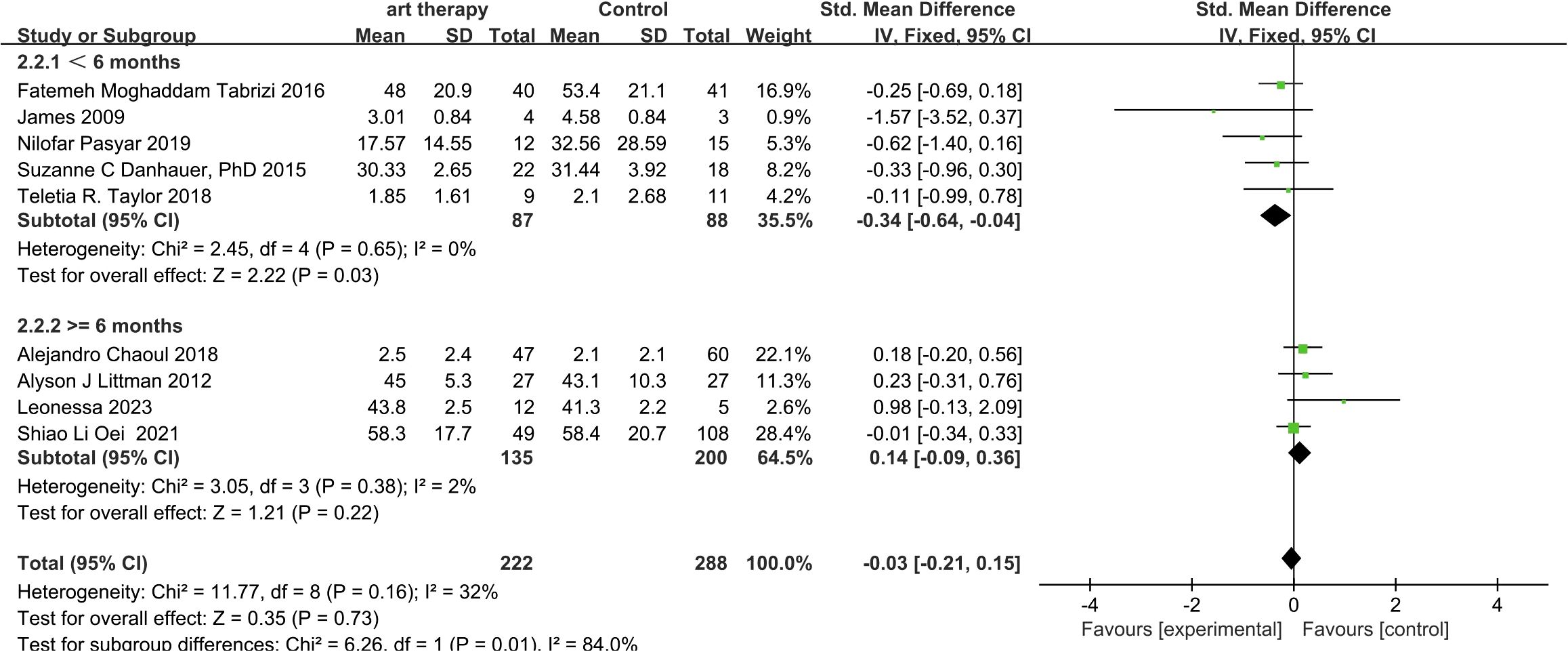
Figure 7. According to the follow-up time, fatigue was analyzed in subgroups.
3.4 Heterogeneity test
In this analysis it is known that the duration of follow-up is a source of heterogeneity in the effect of art therapy on fatigue-related indices in breast cancer. The length of intervention and the type of art were sources of heterogeneity in the effect of art therapy on the quality of life aspects of breast cancer.
3.5 Quality evaluation
Using Cochrane system evaluation “risk bias assessment” tool to evaluate the quality of 22 articles included in the study, it is found that the vast majority of articles use random control method to test, and most of the hidden assignments are low-risk, and others are not clearly described in the articles (10, 20), and the blind method for participants is half low-risk and unclear (11, 18–20, 24, 30), and account for the same proportion (14, 25, 26), while the blind low-risk (7, 11, 12, 19, 24, 27, 28), and high-risk (17, 20) for the outcome evaluator are less, and the rest are not mentioned in the articles on the integrity of the outcome data (20, 21, 28, 29). The overall quality of the included documents is optimistic, which may have little impact on the reliability of the results (Figure 1).
3.6 Publication bias
The main outcome indicators (quality of life, fatigue) of this study were analysed separately using the bias funnel plot approach for the scores of breast cancer patients, and the results showed that the scatters were uniformly distributed on both sides and the graphs were symmetrical, indicating that there is a low possibility of publication bias in this study (Figures 8, 9).
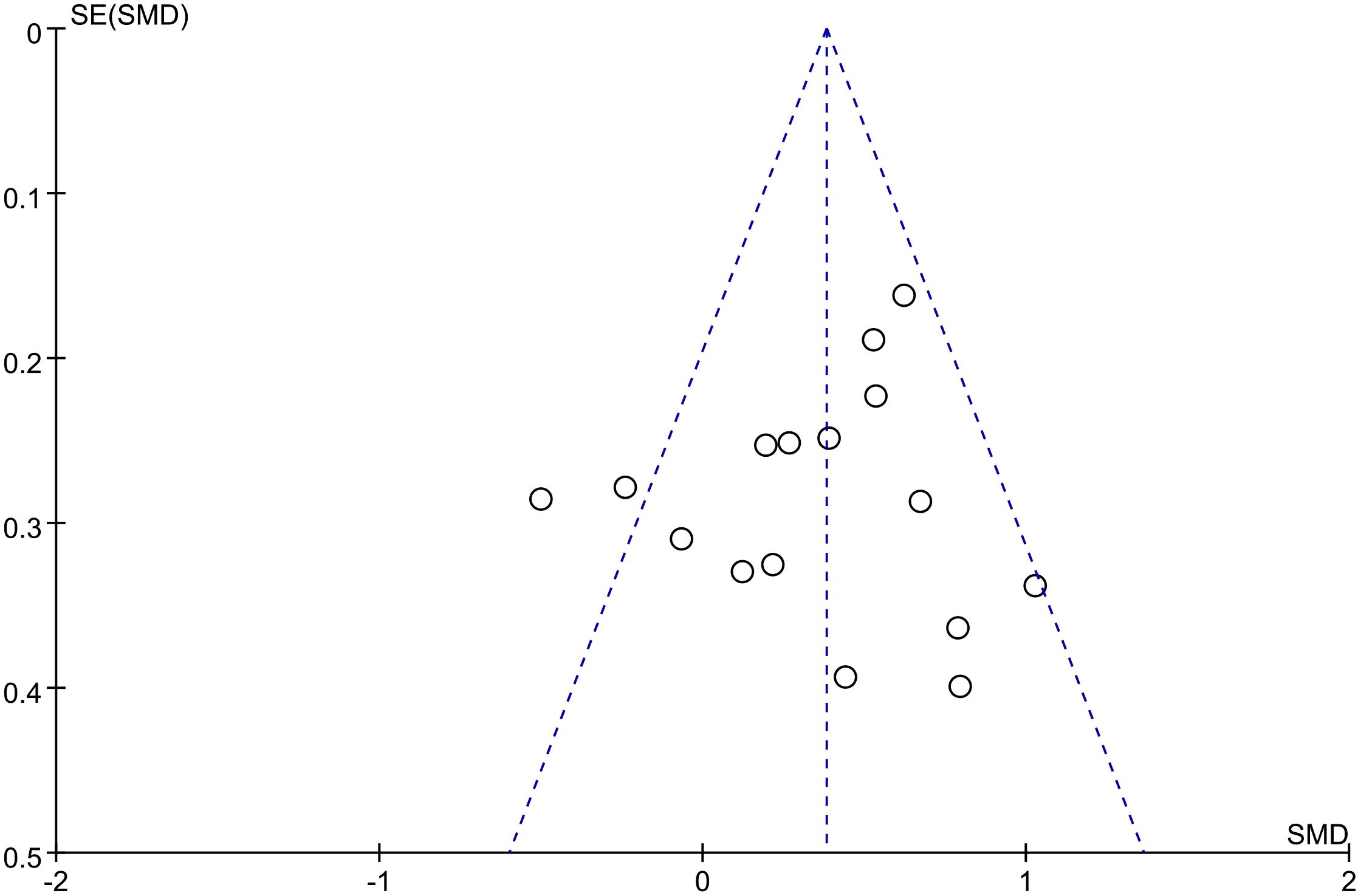
Figure 8. Publication bias funnel plot of the effect of art therapy on the quality of life of breast cancer patients.
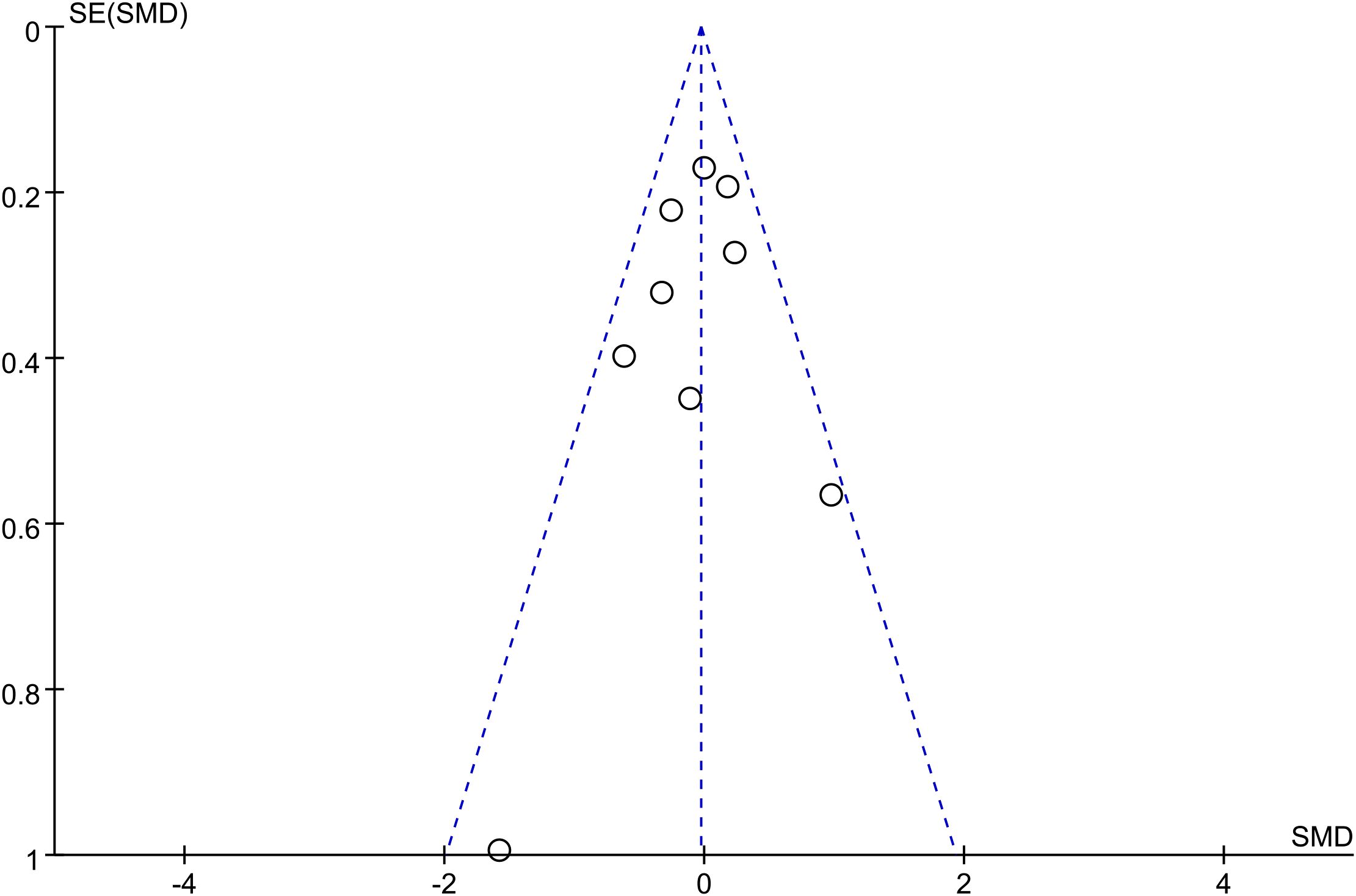
Figure 9. Publication bias funnel plot for the effect of art therapy on fatigue in breast cancer patients.
4 Discussion
A prior meta-analysis supported the findings of the current meta-analysis, which indicated that art therapy significantly improved quality of life but had no effect on fatigue (31). For quality of life, duration-stratified analysis showed interventions ≥2 months achieved clinically meaningful improvements (SMD=0.45, 95% CI 0.28-0.62, P<0.00001) compared to shorter interventions (SMD=0.21, 95% CI -0.01-0.43, P=0.07). Modality-specific effects emerged distinctly: music-based or movement-integrated modalities demonstrated superior efficacy (SMD=0.51, 95% CI 0.32-0.70; SMD=0.44, 95% CI 0.19-0.69) over static modalities (SMD=0.09, 95% CI -0.17-0.35, P=0.49). Fatigue outcomes exhibited time-dependent attenuation, with short-term follow-up (<6 months: SMD=-0.34, 95% CI -0.64–0.04, P=0.03) losing significance during extended follow-up (≥6 months: SMD=0.14, 95% CI -0.09-0.36, P=0.66). Temporal dynamics analysis suggests insufficient intervention duration (<2 months) may disrupt neurobiological adaptation processes, while extended follow-up (≥6 months) reveals therapeutic effect decay, highlighting the need for maintenance protocols.
We investigated the mechanisms underlying the results by reviewing the pertinent literature in light of the aforementioned findings. Mechanistically, our findings align with neuroendocrine evidence demonstrating art therapy’s capacity to modulate stress biomarkers. The observed cortisol reduction reflects HPA axis normalization, a critical pathway given the axis’ central role in stress regulation (32). Another study has shown that the neural effects of visual art production on psychological resilience in adulthood. Psychological resilience is conceptualized as a protective personality trait that enables individuals to control the negative effects of stress and thus function successfully and healthily even under stressful life conditions (33). Intervention efficacy variations may stem from neurobiological specificity: Rhythmic auditory stimuli (e.g., music therapy) activate striatal dopaminergic pathways (34). Similar to this, the beat of music can also have a “cellular massage effect” on tissue cells, causing the cells to resonate with the beat and create a harmonic sense that can enhance the performance of several systems and enhance patients’ quality of life. The lack of effectiveness of the art therapy intervention of drawing and writing alone may be due to the inability to control subjectivity during the intervention, i.e., the difference is that it is the emotional state of the moment that influences and guides the implementation of the art therapy, and therefore its effectiveness is more affected by the subject’s mental health in the present moment. The temporal dynamics of art therapy efficacy reveal critical implementation parameters. Emotion-driven modalities (e.g., drawing/writing) demonstrate strict adherence requirements—regularity and continuity are essential for therapeutic maintenance. However, implementation limitations were evident: short intervention durations (≤5 weeks) coupled with extended follow-up intervals created therapeutic discontinuities, potentially professional supervision continuity and compromising protocol obedience. Dance, music and yoga on the other hand are objective therapies to influence the improvement of the patient’s mood, which is less influenced by the factor of time and hence the intervention is more effective as compared to the former. Similarly in several studies there was little improvement in the fatigue index (25, 35). may be attributed to multiple interrelated factors: procedural memory decay of core therapeutic elements compromises intervention fidelity while post-intervention environmental stressors and weakened therapeutic alliance dependent on sustained therapist-patient interaction collectively erode clinical benefits. These temporal and contextual challenges collectively contribute to the attenuation of long-term fatigue-related benefits, highlighting the need for structured maintenance strategies to preserve therapeutic effects beyond the intervention period.
This meta-analysis also has some limitations. One is that only English articles were searched and the literature covers a limited area. Second, the outcome indicators were analyzed using scales, which can easily be influenced by the subjective consciousness of the participants. It is suggested that some laboratory or clinical indicators can be added to make the results more objective, so as to prove that the quality of life and fatigue of the patients can be improved, in order to increase the objectivity of the results.
As breast cancer management increasingly prioritizes psycho-oncological care, this meta-analysis establishes a precision framework for optimizing art therapy interventions. Time-dependent efficacy patterns reveal interventions require ≥2-month duration to achieve clinically meaningful quality of life improvement (SMD = 0.45-0.21, P<0.00001), while fatigue benefits demonstrate temporal decay beyond 6-month follow-up (SMD from -0.34 to 0.14). These findings necessitate two-phase intervention designs: intensive protocols (<6 months) for fatigue management and maintenance protocols for sustained quality of life. Population heterogeneity analysis identifies critical moderators: gender-specific neuroendocrine responses (exclusively female cohort) and age-stratified social cognition patterns (20-75 year range) may explain differential therapeutic outcomes, underscoring the need for personalized modality selection. Future trials should implement longitudinal designs with adaptive dosing strategies, incorporating gender-specific protocols and age-stratified subgroup analyses to maximize therapeutic precision.
5 Conclusion
Our research indicates that art therapy helps alleviate fatigue and enhance the quality of life for individuals with breast cancer. The quality of life is improved by long-term art therapy. Our research might provide patients with breast cancer an unusual approach to non-exercise rehabilitation. However, fatigue is more susceptible to the effects of time than quality of life; in a nutshell, fatigue has much improved in the short term, but it is not as noticeable in the long run. To enhance patients’ long-term fatigue, additional intervention programs must be created in the future.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author/s.
Author contributions
YZ: Writing – original draft. SZ: Writing – original draft. JD: Writing – original draft. TZ: Writing – review & editing. JY: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We sincerely thank the following people for their assistance in this project. YZ reviewed and included in the research list, SZ assisted in data extraction, JD reviewed statistical analyses and provided suggestions for performance evaluation, TZ thanked him for his support strategy for developing search, JY thanked him for his supervision and guidance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. (2023) 73:17–48. doi: 10.3322/caac.21763
2. van Leeuwen M, Husson O, Alberti P, Arraras JI, Chinot OL, Costantini A, et al. Understanding the quality of life (QOL) issues in survivors of cancer: towards the development of an EORTC QOL cancer survivorship questionnaire. Health Qual Life Outcomes. (2018) 16:114. doi: 10.1186/s12955-018-0920-0
3. Lopes JV, Bergerot CD, Barbosa LR, Calux N, Elias S, Ashing KT, et al. Impact of breast cancer and quality of life of women survivors. Rev Bras Enferm. (2018) 71:2916–21. doi: 10.1590/0034-7167-2018-0081
4. Deshmukh SR, Holmes J, Cardno A. Art therapy for people with dementia. Cochrane Database Syst Rev. (2018) 9:Cd011073. doi: 10.1002/14651858.CD011073.pub2
5. Zhang Q, Zhao H, Zheng Y. Effectiveness of mindfulness-based stress reduction (MBSR) on symptom variables and health-related quality of life in breast cancer patients-a systematic review and meta-analysis. Support Care Cancer. (2019) 27:771–81. doi: 10.1007/s00520-018-4570-x
6. Tang Y, Fu F, Gao H, Shen L, Chi I, Bai Z. Art therapy for anxiety, depression, and fatigue in females with breast cancer: A systematic review. J Psychosoc Oncol. (2019) 37:79–95. doi: 10.1080/07347332.2018.1506855
7. SChad F, Rieser T, Becker S, Groß J, Matthes H, Oei SL, et al. Efficacy of tango argentino for cancer-associated fatigue and quality of life in breast cancer survivors: A randomized controlled trial. Cancers (Basel). (2023) 15:4. doi: 10.3390/cancers15112920
8. Joly F, Pasquier D, Levy C, Mousseau M, D’Almeida MC, Noal S, et al. Impact of creative art therapy on fatigue and quality of life in patients treated for localized breast cancer: A randomized study. Psychooncology. (2022) 31:1412–9. doi: 10.1002/pon.v31.8
9. Jong MC, Boers I, Schouten van der Velden AP, Meij SV, Göker E, Timmer-Bonte A, et al. A randomized study of yoga for fatigue and quality of life in women with breast cancer undergoing (Neo) adjuvant chemotherapy. J Altern Complement Med. (2018) 24:942–53. doi: 10.1089/acm.2018.0191
10. Chaoul A, Milbury K, Spelman A, Basen-Engquist K, Hall MH, Wei Q, et al. Randomized trial of Tibetan yoga in patients with breast cancer undergoing chemotherapy. Cancer. (2018) 124:36–45. doi: 10.1002/cncr.v124.1
11. Sandel SL, Judge JO, Landry N, Faria L, Ouellette R, Majczak M. Dance and movement program improves quality-of-life measures in breast cancer survivors. Cancer Nurs. (2005) 28:301–9. doi: 10.1097/00002820-200507000-00011
12. Tabrizi FM, Radfar M, Taei Z. Effects of supportive-expressive discussion groups on loneliness, hope and quality of life in breast cancer survivors: a randomized control trial. Psychooncology. (2016) 25:1057–63. doi: 10.1002/pon.v25.9
13. Carson JW, Carson KM, Porter LS, Keefe FJ, Seewaldt VL. Yoga of Awareness program for menopausal symptoms in breast cancer survivors: results from a randomized trial. Support Care Cancer. (2009) 17:1301–9. doi: 10.1007/s00520-009-0587-5
14. Boing L, Fretta TB, Lynch BM, Dias M, Rosa LMD, Baptista F, et al. Mat Pilates and belly dance: Effects on patient-reported outcomes among breast cancer survivors receiving hormone therapy and adherence to exercise. Complement Ther Clin Pract. (2023) 50:101683. doi: 10.1016/j.ctcp.2022.101683
15. Pasyar N, Barshan Tashnizi N, Mansouri P, Tahmasebi S. Effect of yoga exercise on the quality of life and upper extremity volume among women with breast cancer related lymphedema: A pilot study. Eur J Oncol Nurs. (2019) 42:103–9. doi: 10.1016/j.ejon.2019.08.008
16. Oei SL, Thronicke A, Groß J, Rieser T, Becker S, Grabowski P, et al. Does the argentine tango sustainably improve cancer-associated fatigue and quality of life in breast cancer survivors? Cancers (Basel). (2023) 15:3–7. doi: 10.3390/cancers15235678
17. Danhauer SC, Griffin LP, Avis NE, Sohl SJ, Jesse MT, Addington EL, et al. Feasibility of implementing a community-based randomized trial of yoga for women undergoing chemotherapy for breast cancer. J Community Support Oncol. (2015) 13:139–47. doi: 10.12788/jcso.0125
18. Taylor TR, Barrow J, Makambi K, Sheppard V, Wallington SF, Martin C, et al. A restorative yoga intervention for African-American breast cancer survivors: a pilot study. J Racial Ethn Health Disparities. (2018) 5:62–72. doi: 10.1007/s40615-017-0342-4
19. Svensk AC, Oster I, Thyme KE, Magnusson E, Sjödin M, Eisemann M, et al. Art therapy improves experienced quality of life among women undergoing treatment for breast cancer: a randomized controlled study. Eur J Cancer Care (Engl). (2009) 18:69–77. doi: 10.1111/j.1365-2354.2008.00952.x
20. Thyme KE, Tavelin B, Öster I, Lindh J, Wiberg B. Art therapy and self-image: A 5-year follow-up art therapy RCT study of women diagnosed with breast cancer. Palliat Support Care. (2022) 20:482–90. doi: 10.1017/S1478951521001437
21. Prakash K, Saini SK, Pugazhendi S. Effectiveness of yoga on quality of life of breast cancer patients undergoing chemotherapy: A randomized clinical controlled study. Indian J Palliat Care. (2020) 26:323–31. doi: 10.4103/IJPC.IJPC_192_19
22. Lu Q, Dong L, Wu IHC, You J, Huang J, Hu Y. The impact of an expressive writing intervention on quality of life among Chinese breast cancer patients undergoing chemotherapy. Support Care Cancer. (2019) 27:165–73. doi: 10.1007/s00520-018-4308-9
23. Lu Q, Gallagher MW, Loh A, Young L. Expressive writing intervention improves quality of life among Chinese-American breast cancer survivors: A randomized controlled trial. Ann Behav Med. (2018) 52:952–62. doi: 10.1093/abm/kax067
24. Hanser SB, Bauer-Wu S, Kubicek L, Healey M, Manola J, Hernandez M, et al. Effects of a music therapy intervention on quality of life and distress in women with metastatic breast cancer. J Soc Integr Oncol. (2006) 4:116–24. doi: 10.2310/7200.2006.014
25. Lima TU, Moura ECR, Oliveira CMB, Leal R, Nogueira Neto J, Pereira EC, et al. Impact of a music intervention on quality of life in breast cancer patients undergoing chemotherapy: A randomized clinical trial. Integr Cancer Ther. (2020) 19:1534735420938430. doi: 10.1177/1534735420938430
26. Alcântara-Silva TR, de Freitas-Junior R, Freitas NMA, de Paula Junior W, da Silva DJ, MaChado GDP, et al. Music therapy reduces radiotherapy-induced fatigue in patients with breast or gynecological cancer: A randomized trial. Integr Cancer Ther. (2018) 17:628–35. doi: 10.1177/1534735418757349
27. He X, Ng MSN, Choi KC, So WKW. Effects of a 16-week dance intervention on the symptom cluster of fatigue-sleep disturbance-depression and quality of life among patients with breast cancer undergoing adjuvant chemotherapy: A randomized controlled trial. Int J Nurs Stud. (2022) 133:104317. doi: 10.1016/j.ijnurstu.2022.104317
28. Andysz A, Merecz D, Wójcik A, Świątkowska B, Sierocka K, Najder A. Effect of a 10-week yoga programme on the quality of life of women after breast cancer surgery. Prz Menopauzalny. (2014) 13:186–93. doi: 10.5114/pm.2014.43823
29. Moadel AB, Shah C, Wylie-Rosett J, Harris MS, Patel SR, Hall CB, et al. Randomized controlled trial of yoga among a multiethnic sample of breast cancer patients: effects on quality of life. J Clin Oncol. (2007) 25:4387–95. doi: 10.1200/JCO.2006.06.6027
30. Littman AJ, Bertram LC, Ceballos R, Ulrich CM, Ramaprasad J, McGregor B, et al. Randomized controlled pilot trial of yoga in overweight and obese breast cancer survivors: effects on quality of life and anthropometric measures. Support Care Cancer. (2012) 20:267–77. doi: 10.1007/s00520-010-1066-8
31. Cheng P, Xu L, Zhang J, Liu W, Zhu J. Role of arts therapy in patients with breast and gynecological cancers: A systematic review and meta-analysis. J Palliat Med. (2021) 24:443–52. doi: 10.1089/jpm.2020.0468
32. Kaimal G, Ray K, Muniz J. Reduction of cortisol levels and participants’ responses following art making. Art Ther (Alex). (2016) 33:74–80. doi: 10.1080/07421656.2016.1166832
33. Bolwerk A, Mack-Andrick J, Lang FR, Dörfler A, Maihöfner C. How art changes your brain: differential effects of visual art production and cognitive art evaluation on functional brain connectivity. PloS One. (2014) 9:e101035. doi: 10.1371/journal.pone.0101035
34. Stegemöller EL. Exploring a neuroplasticity model of music therapy. J Music Ther. (2014) 51:211–27. doi: 10.1093/jmt/thu023
Keywords: mental health, alternative therapy, psychotherapy, cancer, meta-analysis
Citation: Zou Y, Zhai S, Dong J, Zhao T and Yang J (2025) The effect of art therapy on quality of life and fatigue in breast cancer patients: a meta-analysis. Front. Oncol. 15:1495887. doi: 10.3389/fonc.2025.1495887
Received: 13 September 2024; Accepted: 31 March 2025;
Published: 01 May 2025.
Edited by:
Srinivasa Murthy, National Institute of Mental Health and Neurosciences (NIMHANS), IndiaReviewed by:
Vitor Marques, Universidade Federal de Goiás, BrazilRekha Ahuja, Christ University, India
Copyright © 2025 Zou, Zhai, Dong, Zhao and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jin Yang, aHpfemhpeUAxNjMuY29t
†These authors have contributed equally to this work