 Eszter Faludi Vargáné1
Eszter Faludi Vargáné1 Amr Sayed Ghanem2
Amr Sayed Ghanem2 Chau Minh Nguyen2
Chau Minh Nguyen2 Jenifer Pataki1
Jenifer Pataki1 Gergő József Szőllősi3,4
Gergő József Szőllősi3,4 Attila Csaba Nagy2*
Attila Csaba Nagy2*- 1Department of Integrative Health Sciences, Faculty of Health Sciences, University of Debrecen, Debrecen, Hungary
- 2Department of Health Informatics, Faculty of Health Sciences, University of Debrecen, Debrecen, Hungary
- 3Coordination Center for Research in Social Sciences, Faculty of Economics and Business, University of Debrecen, Debrecen, Hungary
- 4Gottsegen György National Cardiovascular Center, Budapest, Hungary
Introduction: With this study, we examined the participation in cervical cancer screening among women with diabetes and the influencing factors of attendance.
Methods: Data from the European Health Interview Surveys in Hungary (2009, 2014, 2019) were analyzed with multivariate and multiple logistic regressions.
Results: A higher level of education (OR=2.56, 95% CI: 1.03-6.33 in the case of secondary level in 2014; and OR=3.09, 95% CI: 1.17-8.13 in the case of tertiary level in 2019, OR= 2.24, 95% CI: 1.12-4.46 in the case of tertiary level in the pooled data), a perceived good economic situation (OR=2.31, 95% CI: 1.30-4.09 in the pooled data), participation in breast cancer screening (OR= 5.41, 95% CI: 3.49-8.38 in the pooled data), and social support (OR= 2.04 95% CI: 1.03-4.03 in 2019) have a positive effect on participation in screening. Taking prescription drugs (OR= 0.31 95% CI: 0.12-0.83, in the pooled data), lower economic status (OR=0.25 95% CI:0.07-0.88, in 2009) and worse perceived health (OR= 0.20, 95% CI: 0.06-0.64 in 2014) can be considered factors with a negative effect.
Conclusion: This study identified groups with low participation rates and made it clear that those groups with unfavorable health factors (bad financial status, bad perceived health, taking prescription drugs) participate the least in screening.
1 Introduction
1.1 The connection between diabetes mellitus and cervical cancer
Cervical cancer is one of the leading causes of cancer death among women (1). According to the GLOBOCAN database, in 2022, there were an estimated 660–000 cervical cancer new cases and 350–000 deaths globally (2). Despite the fact that this is a well-curable tumor, the cervical cancer’s mortality was on the sixth position in 2020 in the world (3). The risk factors of the cervical cancer are mostly generally known, they include HPV infection, smoking, sexual behavior and oral contraceptive use (4, 5). However, it is a less well-known fact that obesity and diabetes also increase the risk of cervical cancer’s development (6). According to a study, diabetes increases the likelihood of developing cervical cancer by twofold (7). As diabetes mellitus is a common metabolic disease, a lot of women has a higher risk according to cervical cancer. According to the World Health Organization’s (WHO) 2024 report, the number of people living with diabetes rose from 200 million in 1990 to 830 million in 2022 (8). The gender distribution is equal, and the incidence peaks at around 55 years of age (9). Studies proved, that there is a causal association between genetic predisposition to type 2 diabetes and many cancers, like cervical cancer (10, 11). Possible associations between the two conditions include various metabolic abnormalities such as obesity, hyperglycemia, hyperinsulinemia stimulation of the IGF-1 (insulin growth factor-1) axis, and increased cytokine production (12). Other studies have described that diabetes is associated with a higher incidence of other diseases of the cervix (for example, vaginitis, cervicitis, HPV infection, and malignant tumors). Certain genes showed a positive correlation with both conditions (diabetes mellitus and cervical pathologies), such as COLL11A2P1 (beta 0.06), INS-IGF2, and TTC 723 (13). In addition to the fact that diabetes poses a risk for some gynecological malignancies, cervical cancer’s prognosis is worse by patients with diabetes (14). Obese women with cervical cancer, especially in postmenopausal period, had a significantly higher mortality related to non-obese women (15), but obesity might increase the incidence of cervical cancer among premenopausal women too (16).
1.2 Cervical cancer screening in Hungary
In Hungary, on the basis of Decree 51/1997 (XII.18) NM, cervical cancer screening has been carried out in an organized form - every 3 years - since 2003 for women aged 25–65 who are eligible according to the National Health Insurance Fund Management Register. Women between the ages of 25 and 65 who have not undergone cervical cancer screening publicly funded by the National Health Insurance Fund within three years from the scheduled date of the screening will receive an invitation by mail to a screening, which they can attend at the gynecology clinic or at the nurse’s office (17).
1.3 Cervical cancer screening among women with diabetes
In overweight or obese women, the risk of the disease is also increased by the fact that adequate sample collecting equipment is not always available, so they have a higher chance of underdiagnosis during screening (18). For this reason, it would be much more important for women with diabetes to attend screenings in order to prevent these diseases and improve the survival rate. Especially considering the fact that this is the only cancer that could be completely prevented by vaccination, as well as treatment after early diagnosis (19). However, some studies showed, that if a patient has diabetes it was associated with significantly lower likelihood to participate in cervical cancer screening, relative to not having diabetes (20–23). In addition to being a risk factor for cervical cancer, a study’s measurements showed that survival rates were worse for women with both diabetes and cervical cancer compared to those with cervical cancer without diabetes (24).
Our aim was to identify the most vulnerable groups in Hungary among women with diabetes, who are least likely to undergo cervical cancer screening, in order to explore the target groups of health promotion programs.
2 Methods
The study is based on data from the European Health Interview Survey (EHIS) of 2009, 2014 and 2019, the basis of which was developed by Eurostat in compliance with a legal obligation. The EHIS uses a standardized questionnaire that contains the following main groups of questions: health status, use of the health care system, drug use, reasons for refusing health care, opinion about the health care system, use of preventive care, general well-being, factors affecting health, care, demographic data. The questionnaire also contains separate groups of questions for children. Its main purpose is to collect data for European health indicators (25, 26). The EHIS provides age data in three categories: 15-34, 35-64, and 65+, making it impossible to define a precise eligibility cutoff (e.g., 25–65 years) in alignment with national screening guidelines. Given this limitation, we used a binary classification: below 65 years and 65+ years, ensuring that the analysis captures the vast majority of screening-eligible women (i.e., those below 65) while distinguishing those who may have aged out of routine screening recommendations. Although some younger women (15-24) were included in the <65 category, they represent a minority, and their inclusion does not substantially affect overall trends, as participation in screening is expected to be low in this subgroup. This categorization balances data constraints with epidemiological relevance, allowing for meaningful comparisons while adhering to the best available classification method given the dataset structure.
In Hungary, the respondents were selected based on two-stage stratified sampling according to county and settlement size, the sampling method was developed by Hungarian Central Statistical Office (27). The total sample included 16,480 persons aged 15 and over living in private households, of which 8,910 were women, of whom 700 were women with diabetes. The outcome variable of the study was participation in cervical cancer screening among women with diabetes. In the questionnaire “When was the last time you had a gynecological cervical cancer screening?” question related to this: the five answer options were divided into two categories: the category of having participated in screening for less than 2 years and the category of having participated in screening for more than 2 years. Data on diabetes were obtained from answers to the question on diabetes, in the chronic diseases block.
As influencing factors age (≥65, <65) marital status (single/in a relationship), level of education (primary/secondary/tertiary), type of occupation (employed/unemployed), area of residence (urban/rural), regions (Central Hungary/Southern Great Plain/Southern Transdanubia/Central Transdanubia/Western Transdanubia/Northern Great Plain/Northern Hungary) financial situation (average/good/bad), income quintiles (first/second/third/fourth/fifth), BMI overweight + obese/normal), smoking status (smoker/non-smoker), alcohol consumption (drinker/non-drinker), self-perceived health (average/good/bad), hypertension (yes/no), hypercholesterolemia (yes/no), cardiovascular disease (yes/no), depression (yes/no), mental illnesses (yes/no), last visit to the dental office (more than a year ago/less than a year ago), taking prescription drugs (yes/no), taking supplements (yes/no) and breast cancer screening attendance (more than 2 years/within the past 2 years) were included. Variables with excessive missing values were excluded from the analysis, and missing data in retained variables were handled using listwise deletion.
2.1 Statistical methods
The statistical analysis applied weighted methods throughout to ensure representativeness and accuracy given the survey design. Weighted proportions were calculated to describe the distribution of screening participation and predictor variables across the survey years, and weighted chi-square tests were conducted to assess associations between categorical predictors and cervical cancer screening participation while adjusting for sampling weights. For inferential analysis, weighted multiple logistic regression models were developed to estimate adjusted odds ratios (ORs) with 95% confidence intervals (CIs), controlling for potential confounders while accounting for survey weights. Bootstrapping with 1,000 iterations was applied to estimate robust confidence intervals for screening participation rates. Sensitivity analysis was conducted, and the model with the lowest Akaike Information Criterion and Bayesian Information Criterion was chosen as the final model. To ensure validity, the Hosmer-Lemeshow goodness-of-fit test was performed to assess model calibration, and multicollinearity was tested using the Variance Inflation Factor (VIF), confirming no collinearity concerns. Model discrimination was evaluated using the area under the receiver operating characteristic curve (AUC-ROC), and a confusion matrix was generated to assess classification accuracy, including sensitivity, specificity, positive predictive value, and negative predictive value. The result was considered significant if the p value was below 0.05. STATA IC Version 17.0 software was used for statistical analysis. In addition to these, we also compared the results of each year.
3 Results
The sample contains 700 women with diabetes, in the annual distribution below: 164 in 2009, 250 in 2014, and 285 in 2019. The age distribution of women with diabetes was as follows: 4.57% of the respondents belonged to the age group of 15-34, 40.57% to the age group of 35–64 and 54.86% to the age group of 65+.
3.1 Characteristics of participants in 2009, 2014 and 2019 and pooled data
Regarding the age group categories, there was a significant difference in screening participation in all three years, with the oldest age group’s attendance rate was the lowest. The participation rates in cervical cancer screening for individuals under 65 years of age were as follows in 2009, 2014, and 2019, as well as the overall data: 68.94%, 68.73%, 64.74%, and 67.18%. The level of education also had a significant influencing effect of the attendance: in 2014, in 2019 and, in the pooled data the lowest education level group showed the lowest rate, in the case of family status, the same result was obtained for single people. Occupation has significant influence on attendance rate in all three years, employed respondents attended screening in a significantly higher proportion in each examined year, as well as a better financial situation also increases the participation rate.
Examining the lifestyle factors, it can be concluded that a significantly lower proportion of alcohol drinkers took part in screening in 2009 and 2019, while in the case of smokers, a significant difference in screening can only be observed in 2019. The group who considered their health to be good used the screening test more often, and in 2014 and in 2019 the same could be said for those living without hypertension and CVD. In the case of using other health services - such as a dental examination, participating in a breast screening - the respondents also took part in cervical cancer screening significantly more often in each examined year. Regarding the use of medication, it can be said that the participation rate was lower in the case of those taking prescription medication, while it was higher in the case of OTC medication use (Table 1).
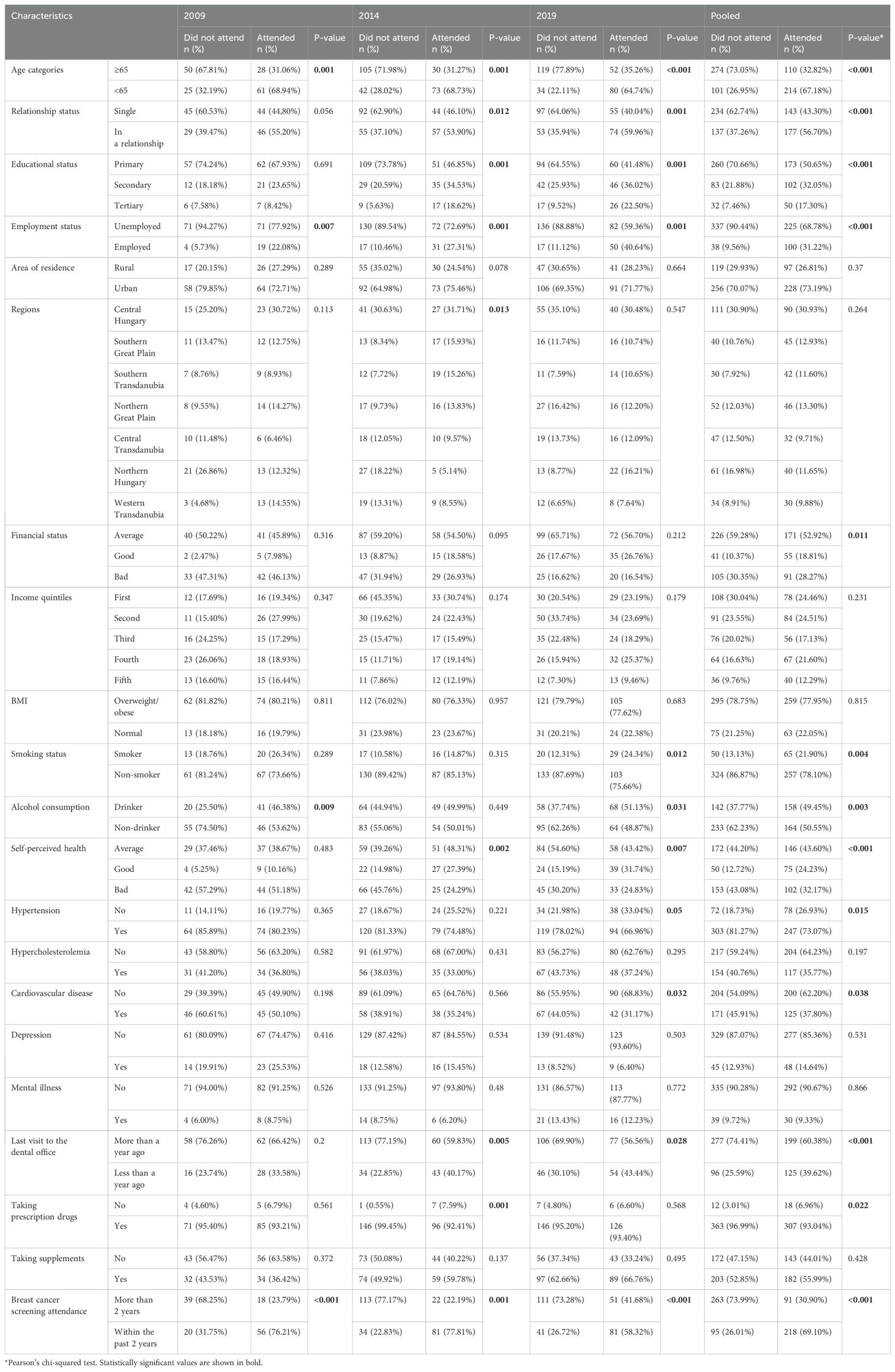
Table 1. Characteristics of participants in 2009, 2014, 2019 and pooled data.
3.2 Multiple logistic regression models
In multiple regression analysis, adjusting for age, we found a significant difference in the attendance rates of cervical cancer screening rates in the year 2014, according to the reference year 2009, a decreasing trend can be observed. A higher level of education (OR=2.56, 95% CI: 1.03-6.33 in the case of secondary level in 2014; and OR=3.09, 95% CI: 1.17-8.13 in the case of tertiary level in 2019, OR= 2.24, 95% CI: 1.12-4.46 in the case of tertiary level in the pooled data), a perceived good economic situation (OR=2.31, 95% CI: 1.30-4.09 in the pooled data), participation in breast cancer screening (OR= 5.41, 95% CI: 3.49-8.38 in the pooled data), and social support (OR= 2.04 95% CI: 1.03-4.03 in 2019) have a positive effect on participation in screening. Taking prescription drugs (OR= 0.31 95% CI: 0.12-0.83, in the pooled data), lower economic status (OR=0.25 95% CI:0.07-0.88, in 2009) and worse perceived health (OR= 0.20, 95% CI: 0.06-0.64 in 2014) can be considered factors with a negative effect. Women under age 65 years old have significantly higher odds to attend the cervical cancer screening according to the pooled data (p<0.001). (Table 2).

Table 2. Possible influencing factors of attendances on cervical screening programs.
4 Discussion
Our aim was to identify the influencing factors that are contribute to the attendance of cervical cancer screening among diabetic women.
The participation rate of women with diabetes is declining compared to the 2009 baseline.
Higher education, good economic situation, participation in breast cancer screening and social support have a positive effect on participation in screening. Taking prescription drugs, lower economic status, and poorer perceived health negatively affected participation in screening.
Compared to the reference year (2009), the attendance rate was lower in the other two examined years, the result was significant in 2014. Some studies also show this declining trend on attendance (28), others report increasing participation rates (29). The decline in participation rate can be explained by the introduction of HPV vaccination in Hungary, which happened in 2014.
Similar to other studies (30, 31), positive correlations were detected to screening attendance with the following factors: higher educational level, social support, better financial state. International recommendations no longer recommend cervical cancer screening for people older than 65, except in some special cases (32, 33). This can explain why the younger age group took part in the screening examination in greater proportion. Participation in breast cancer screening also shows a correlation with participation in cervical cancer screening in other countries (34).
Some factors decreased the odds of the attendance of cervical cancer screening, these were bad financial state and worse perceived health status and taking prescription drugs. These factors have also been identified as influencing factors in other studies (35, 36). The decreasing participation rate does not only affect women with diabetes, but is also characteristic of the entire female sample based on the data examined. According to another study analyzing participation data in Hungary, attendance in cervical cancer screening during the period 2008–2021 initially showed an increase, but from 2016 onwards a continuously decreasing trend can be observed (37). Based on OECD statistics, from 2011–2021 among the examined 31 countries, Hungary had the third lowest attendance rate in cervical cancer screening, only Poland and Costa Rica had lower numbers. The OECD average rate was 53%, in Hungary this number was only 26%, and the OECD found that the attendance rate decreased with 12% compared to the data from 2011 (38).
Reviewing Hungarian cervical cancer mortality data, HPV vaccination and cervical cancer treatment, there are still areas that must be improved in order to reach the 90-70–90 goal formulated by the World Health Organization, which includes the following:90% HPV vaccination coverage rate among girls by the age of 15; a 70% coverage of cervical cancer screening at ages 35 and 45 and treating 90% of women with precancer and managing 90% of women with invasive cancer. The WHO goal for the incidence of cervical cancer is lower than 4 new cases per 100–000 women, each year (39). In Hungary the HPV vaccination rate was 82% in 2021, the number of new cases was 24,7/100–000 women, and the 75% of 25-65-year-old women were screened in the last three years (40). The situation in Hungary is not favorable in terms of screening participation, the participation rate in cervical cancer screening tests was under 50% in 2006 and it has been decreasing over the years (in 2019 only 30.2% of 20–69 year olds appeared for screening) (41). According to the results of a meta-analysis, increasing participation in cervical cancer screening would be facilitated by the possibility of self-sampling and sending invitation letters and reminders to affected women (42).
Many factors have influence on attendance of screening programs. Socioeconomic status (SES) influences people’s health behavior, studies found that higher SES has positive effect on the participation of screening programs (43, 44). However, analyzing the individual components of socioeconomic status (educational level, marital status, financial status), the relationship is not so clear. There are components that clearly have a positive effect on screening participation, e.g. married individuals have higher odds to attend screening programs (45, 46). On the other hand, about the association between educational level and screening attendance, some studies found no significant association (47, 48), while others described a positive correlation between higher educational level and the attendance (49, 50). Higher household income is associated with higher attendance rate on screening (31, 50).
In addition to these, some studies have also identified other factors that have a positive or negative effect on participation in cervical cancer screening: the most common barriers were pain/discomfort; embarrassment; and time, the most commonly reported facilitators were: ease of making appointments; peace of mind; and fear of cancer/preventing serious illness (51).
5 Strengths and limitations
This study utilized data from the European Health Interview Survey (EHIS), which offers a representative sample of the adult population in Hungary. Although the same methodology was applied consistently across all three survey years, an aggregated dataset was employed for comparative analysis. Multiple logistic regression models were utilized to identify significant determinants of screening uptake, providing valuable insights for the design of targeted intervention strategies. Owing to the methodological design of the data collection process, the database includes only data from participants, with no information available for those who opted not to participate. The European Health Interview Survey (EHIS), as administered by Eurostat and the Hungarian Central Statistical Office (HCSO), did not differentiate between Type 1 and Type 2 diabetes mellitus. However Type 2 diabetes has higher prevalence, we assumed that the majority of respondents had type 2 diabetes. This limitation has been acknowledged, and results should be interpreted with this consideration in mind.
6 Conclusions
This study focused on the importance of cervical cancer screening participation in women with diabetes and highlights the benefits of screening within this population. In particular, it should be taken into account that the participation rate in screening is not homogeneous in terms of the population. In the case of participation in cervical cancer screening, it is lowest in those groups whose health-influencing factors are not very favorable (those with poor financial status, those with perceived poor health, those taking prescription medications). Therefore, the identification of groups with lower screening participation may be crucial in the context of the introduction of public health interventions aimed at improving the participation rate.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The datasets of the European Health Interview Survey for this study are available upon request from the Hungarian Central Statistical Office (https://www.ksh.hu). Requests to access these datasets should be directed to Karolyne Tokaji, S2Fyb2x5bmUuVG9rYWppQGtzaC5odQ==.
Ethics statement
The studies involving humans were approved by Ethics Committee of the University of Debrecen, under the approval number 5609-2020. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
EF: Writing – original draft. AG: Writing – original draft. CN: Writing – review & editing. GS: Writing – review & editing. JP: Writing – review & editing. AN: Conceptualization, Formal Analysis, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This paper was supported by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences. Supported by the EKÖP-24-3-I University Research Scholarship Program of the Ministry for Culture and Innovation from the source of the National Research, Development and Innovation Fund.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mattiuzzi C, Lippi G. Cancer statistics: a comparison between World Health Organization (WHO) and Global Burden of Disease (GBD). Eur J Public Health. (2020) 30:1026–7. doi: 10.1093/eurpub/ckz216
2. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
3. Cancer (IARC) TIA for R on. Global Cancer Observatory. Available at: https://gco.iarc.fr/ (Accessed February 25, 2025).
4. Non-Genetic Factors and Risk of Cervical Cancer: An Umbrella Review of Systematic Reviews and Meta-Analyses of Observational Studies . Available online at.
5. Zhang S, Xu H, Zhang L, Qiao Y. Cervical cancer: Epidemiology, risk factors and screening. Chin J Cancer Res Chung-Kuo Yen Cheng Yen Chiu. (2020) 32:720–8. doi: 10.21147/j.issn.1000-9604.2020.06.05
6. Poorolajal J, Jenabi E. The association between BMI and cervical cancer risk: a meta-analysis. Eur J Cancer Prev Off J Eur Cancer Prev Organ ECP. (2016) 25:232–8. doi: 10.1097/CEJ.0000000000000164
7. Kim JY, Lee DW, Kim MJ, Shin JE, Shin YJ, Lee HN. Secondhand smoke exposure, diabetes, and high BMI are risk factors for uterine cervical cancer: a cross-sectional study from the Korea national health and nutrition examination survey (2010–2018). BMC Cancer. (2021) 21:880. doi: 10.1186/s12885-021-08580-3
8. Diabetes. Available online at: https://www.who.int/news-room/fact-sheets/detail/diabetes (Accessed March 5, 2025).
9. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes - global burden of disease and forecasted trends. J Epidemiol Glob Health. (2020) 10:107–11. doi: 10.2991/jegh.k.191028.001
10. Pearson-Stuttard J, Papadimitriou N, Markozannes G, Cividini S, Kakourou A, Gill D, et al. Type 2 diabetes and cancer: an umbrella review of observational and mendelian randomization studies. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. (2021) 30:1218–28. doi: 10.1158/1055-9965.EPI-20-1245
11. Yuan S, Kar S, Carter P, Vithayathil M, Mason AM, Burgess S, et al. Is type 2 diabetes causally associated with cancer risk? Evidence from a two-sample mendelian randomization study. Diabetes. (2020) 69:1588–96. doi: 10.2337/db20-0084
12. Vrachnis N, Iavazzo C, Iliodromiti Z, Sifakis S, Alexandrou A, Siristatidis C, et al. Diabetes mellitus and gynecologic cancer: molecular mechanisms, epidemiological, clinical and prognostic perspectives. Arch Gynecol Obstet. (2016) 293:239–46. doi: 10.1007/s00404-015-3858-z
13. Gupta P, Gupta A, Khanam B. Analysis of genetic and pathologic association between diabetes mellitus and cervical cancer. Egypt J Med Hum Genet. (2025) 26:1. doi: 10.1186/s43042-024-00632-0
14. Chen S, Tao M, Zhao L, Zhang X. The association between diabetes/hyperglycemia and the prognosis of cervical cancer patients. Med (Baltimore). (2017) 96:e7981. doi: 10.1097/MD.0000000000007981
15. Gu W, Chen C, Zhao KN. Obesity-associated endometrial and cervical cancers. Front Biosci-Elite. (2013) 5:109–18. doi: 10.2741/E600
16. Modesitt SC, van Nagell JR. The impact of obesity on the incidence and treatment of gynecologic cancers: a review. Obstet Gynecol Surv. (2005) 60:683–92. doi: 10.1097/01.ogx.0000180866.62409.01
17. Nikolett PS. Információk a méhnyakszűrésről . Available online at: https://www.nnk.gov.hu/index.php/179-projektek/efop-1-8-1/informaciok-az-efop-1-8-1-projekten-belul/617-informaciok-a-mehnyakszuresrol.html?highlight=WyJtXHUwMGU5aG55YWtyXHUwMGUxayIsInN6XHUwMTcxclx1MDBlOXMiXQ (Accessed February 25, 2025).
18. Clarke MA, Fetterman B, Cheung LC, Wentzensen N, Gage JC, Katki HA, et al. Epidemiologic evidence that excess body weight increases risk of cervical cancer by decreased detection of precancerepidemiologic evidence that excess body weight increases risk of cervical cancer by decreased detection of precancer. J Clin Oncol. (2018) 36(12):1184–91. doi: 10.1200/JCO.2017.75.3442
19. Brisson M, Kim JJ, Canfell K, Drolet M, Gingras G, Burger EA, et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. (2020) 395(10224):575–90. doi: 10.1016/S0140-6736(20)30068-4
20. Bhatia D, Lega IC, Wu W, Lipscombe LL. Breast, cervical and colorectal cancer screening in adults with diabetes: a systematic review and meta-analysis. Diabetologia. (2020) 63:34–48. doi: 10.1007/s00125-019-04995-7
21. Jiménez-Garcia R, Hernandez-Barrera V, Carrasco-Garrido P, Gil A. Prevalence and predictors of breast and cervical cancer screening among spanish women with diabetes. Diabetes Care. (2009) 32:1470–2. doi: 10.2337/dc09-0479
22. Martinez-Huedo MA, Lopez de Andres A, Hernandez-Barrera V, Carrasco-Garrido P, Martinez Hernandez D, Jiménez-Garcia R. Adherence to breast and cervical cancer screening in Spanish women with diabetes: associated factors and trend between 2006 and 2010. Diabetes Metab. (2012) 38:142–8. doi: 10.1016/j.diabet.2011.09.007
23. Miller EA, Pinsky PF. Cervical cancer screening and predictors of screening by diabetes status. Cancer Causes Control. (2022) 33:1305–12. doi: 10.1007/s10552-022-01615-5
24. Kuo HY, Lin ZZ, Kuo R, Shau WY, Lai CL, Yang YY, et al. The prognostic impact of type 2 diabetes mellitus on early cervical cancer in Asia. Oncologist. (2015) 20:1051–7. doi: 10.1634/theoncologist.2015-0111
25. European health interview survey . Available online at: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=European_health_interview_survey_-_methodology (Accessed February 19, 2025).
26. Hintzpeter B, Finger JD, Allen J, Kuhnert R, Seeling S, Thelen J, et al. European Health Interview Survey (EHIS) 2 - Background and study methodology. J Health Monit. (2019) 4:66–79. doi: 10.25646/6228
27. Európai lakossági egészségfelmérés (2019). Available online at: https://www.ksh.hu/elef (Accessed March 5, 2025).
28. Aitken CA, Kaljouw S, Siebers AG, Bron M, Morssink A, van Kemenade FJ, et al. Investigating the decrease in participation in the Dutch cervical cancer screening programme: The role of personal and organisational characteristics. Prev Med Rep. (2021) 22:101328. doi: 10.1016/j.pmedr.2021.101328
29. Petkeviciene J, Ivanauskiene R, Klumbiene J. Sociodemographic and lifestyle determinants of non-attendance for cervical cancer screening in Lithuania, 2006-2014. Public Health. (2018) 156:79–86. doi: 10.1016/j.puhe.2017.12.014
30. Covaliu BF, Forray AI, Tomic M, Vlad C, Cadariu PA, Ungurean C, et al. Understanding cervical cancer screening attendance: barriers and facilitators in a representative population survey. Cancers. (2025) 17:706. doi: 10.3390/cancers17040706
31. Judah G, Dilib F, Darzi A, Huf S. A population survey on beliefs around cervical cancer screening: determining the barriers and facilitators associated with attendance. BMC Cancer. (2022) 22:522. doi: 10.1186/s12885-022-09529-w
32. US Preventive Services Task Force, Curry SJ, Krist AH, Owens DK, Barry MJ, Caughey AB, et al. Screening for cervical cancer: US preventive services task force recommendation statement. JAMA. (2018) 320:674. doi: 10.1001/jama.2018.10897
33. Cervical Cancer Screening. NCI (2022). Available at: https://www.cancer.gov/types/cervical/screening (Accessed March 5, 2025).
34. Kriaucioniene V, Petkeviciene J. Predictors and trend in attendance for breast cancer screening in Lithuania, 2006-2014. Int J Environ Res Public Health. (2019) 16:4535. doi: 10.3390/ijerph16224535
35. Pataki J, Szőllősi GJ, Sárváry A, Dombrádi V. Factors associated with cervical cancer screening attendance in Hungary based on the european health interview survey. Int J Public Health. (2024) 69:1607509. doi: 10.3389/ijph.2024.1607509
36. Diendéré J, Kiemtoré S, Coulibaly A, Tougri G, Ily NI, Kouanda S. Low attendance in cervical cancer screening, geographical disparities and sociodemographic determinants of screening uptake among adult women in Burkina Faso: results from the first nationwide population-based survey. Rev Epidemiol Sante Publiqu. (2023) 71:101845. doi: 10.1016/j.respe.2023.101845
37. Vajda R, Bódis J, Pónusz-Kovács D, Elmer D, Kajos LF, Csákvári T, et al. A szervezett lakossági méhnyakszűrés részvételi mutatói Magyarországon. ARANYPAJZS Csal Véd TUDOMÁNYA Gold SHIELD Sci Prot Fam. (2022) 1:23–35. doi: 10.56077/AP.2022.3.2
38. Health at a Glance 2023. OECD (2023). Available at: https://www.oecd.org/en/publications/health-at-a-glance-2023_7a7afb35-en.html (Accessed February 19, 2025).
39. Global strategy to accelerate the elimination of cervical cancer as a public health problem . Available online at: https://www.who.int/publications/i/item/9789240014107 (Accessed February 19, 2025).
40. Human Papillomavirus and Related Diseases Report, Hungary . Available online at: https://hpvcentre.net/statistics/reports/HUN.pdf (Accessed February 19, 2025).
41. Csákvári T, Gyenese D, Elmer D, Pónusz-Kovács D, Boncz I. A méhnyakrák epidemiológiai mutatói 2000–2019 között Magyarországon megfigyelhető változásának elemzése nemzetközi összevetéssel. LEGE ARTIS Med. (2023) 33:87–95. doi: 10.33616/lam.33.0087
42. Musa J, Achenbach CJ, O’Dwyer LC, Evans CT, McHugh M, Hou L, et al. Effect of cervical cancer education and provider recommendation for screening on screening rates: A systematic review and meta-analysis. PloS One. (2017) 12:e0183924. doi: 10.1371/journal.pone.0183924
43. Luo Z, Dong X, Wang C, Cao W, Zheng Y, Wu Z, et al. Association between socioeconomic status and adherence to fecal occult blood tests in colorectal cancer screening programs: systematic review and meta-analysis of observational studies. JMIR Public Health Surveill. (2023) 9:e48150. doi: 10.2196/48150
44. Zhang S, Wang H, Liu B, Yu J, Gao Y. Socioeconomic status index is an independent determinant of breast cancer screening practices: Evidence from Eastern China. PloS One. (2022) 17:e0279107. doi: 10.1371/journal.pone.0279107
45. Gram MA, Therkildsen C, Clarke RB, Andersen KK, Mørch LS, Tybjerg AJ. The influence of marital status and partner concordance on participation in colorectal cancer screening. Eur J Public Health. (2021) 31:340–6. doi: 10.1093/eurpub/ckaa206
46. Hanske J, Meyer CP, Sammon JD, Choueiri TK, Menon M, Lipsitz SR, et al. The influence of marital status on the use of breast, cervical, and colorectal cancer screening. Prev Med. (2016) 89:140–5. doi: 10.1016/j.ypmed.2016.05.017
47. Gianino MM, Lenzi J, Bonaudo M, Fantini MP, Siliquini R, Ricciardi W, et al. Organized screening programmes for breast and cervical cancer in 17 EU countries: trajectories of attendance rates. BMC Public Health. (2018) 18:1236. doi: 10.1186/s12889-018-6155-5
48. Hansen BT, Hukkelberg SS, Haldorsen T, Eriksen T, Skare GB, Nygård M. Factors associated with non-attendance, opportunistic attendance and reminded attendance to cervical screening in an organized screening program: a cross-sectional study of 12,058 Norwegian women. BMC Public Health. (2011) 11:264. doi: 10.1186/1471-2458-11-264
49. Shero AA, Kaso AW, Tafa M, Agero G, Abdeta G, Hailu A. Cervical cancer screening utilization and associated factors among women attending antenatal care at Asella Referral and Teaching Hospital, Arsi zone, South Central Ethiopia. BMC Womens Health. (2023) 23:199. doi: 10.1186/s12905-023-02326-y
50. Pataki J, Dombrádi V, Sárváry A, Szőllősi GJ. Breast cancer screening and its associating factors among hungarian women aged 45–65: a cross-sectional study based on the European health interview surveys from 2009 to 2019. BMC Public Health. (2023) 23:1679. doi: 10.1186/s12889-023-16608-5
Keywords: cervical cancer, cervical cancer screening, attendance, diabetes mellitus, European Health Interview Survey
Citation: Faludi Vargáné E, Ghanem AS, Nguyen CM, Pataki J, Szőllősi GJ and Nagy AC (2025) Influencing factors on attendance in cervical cancer screening among women with diabetes in Hungary: a cross-sectional study using European Health Interview Surveys 2009-2019. Front. Oncol. 15:1501654. doi: 10.3389/fonc.2025.1501654
Received: 08 October 2024; Accepted: 07 April 2025;
Published: 29 April 2025.
Edited by:
Márió Gajdács, University of Szeged, HungaryCopyright © 2025 Faludi Vargáné, Ghanem, Nguyen, Pataki, Szőllősi and Nagy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Attila Csaba Nagy, bmFneS5hdHRpbGFAZXRrLnVuaWRlYi5odQ==