 YanHong Hao
YanHong Hao Yuan Su
Yuan Su Yanan Li
Yanan Li Qiaohong Pan
Qiaohong Pan Liping Liu
Liping Liu- 1Department of Ultrasound, First Hospital of Shanxi Medical University, Taiyuan, China
- 2Department of Ultrasound, Heping Hospital Affiliated to Changzhi Medical College, Changzhi, China
- 3Department of Interventional Ultrasound, First Hospital of Shanxi Medical University, Taiyuan, China
Background: In oncology, the relationships among cervical central lymph node metastasis (CLNM), biochemical tests, and ultrasound characteristics in patients with papillary thyroid cancer (PTC) remain controversial. This association is currently not well supported by evidence, which emphasizes the need for further research. Understanding the connection between CLNM, biochemical testing, and ultrasound features is crucial for clinical practice and public health efforts. Research on this topic is still underway and is now receiving much interest. Our goal was to create and verify a basic cervical lymph node metastasis prediction model.
Methods: In this retrospective cohort study, 685 individuals diagnosed with PTC from First Hospital of Shanxi Medical University (n = 560) and Changzhi Heping Hospital (n = 125) participated in the research from January 2020 to October 2022. Patients were randomly assigned to a training set (n=392), an internal test set (n=168), or an external test set (n=125). Comprehensive clinical information, serological indices, and ultrasonography features were obtained for every participant. LASSO (Least Absolute Shrinkage and Selection Operator) and BSR (Best Subset Regression) to select features for model construction. A logistic regression model with filtered variables was constructed. A nomogram was developed based on six risk factors. Receiver operating characteristic (ROC) curves, decision curve analysis, and calibration curves were used to assess the predictive accuracy, clinical utility, and discriminative ability of the nomogram.
Results: Of the 560 individuals, 54.3% (304/560) did not have lymph node metastases, whereas 45.7% (256/560) did. Age, male, nodule size, multifocal lesions, capsular contact or invasion and ill-defined margins were determined to be risk variables via BSR and multivariate logistic analysis. Nomograms were created using these six risk indicators. The prediction model of CLNM had an AUC of 0.884 (95% CI 0.851, 0.916). Both the internal and the external validation results were highly encouraging. Confirming the model’s stability and applicability in different data environments.
Conclusion: We developed a predictive model and nomogram for CLNM in PTC patients, which demonstrated robust performance. This model can guide surgical planning, potentially reducing complications and improving outcomes.
Background
PTC is the most prevalent histologic subtype of all thyroid cancers (1, 2). CLNM has an inert clinical course and usually has a good prognosis; however, patients with CLNM face a higher risk of local recurrence and a significant increase in the frequency of distant metastases with advancing N stage, leading to a poorer prognosis (2). Conventional surgery routinely involves central zone lymph node dissection, but unnecessary central zone lymph node dissection can lead to laryngeal recurrent nerve injury, whereas a larger surgical scope of cervical lateral zone lymph nodes may lead to more complications and diminish patient quality of existence (3). Therefore, accurate preoperative prediction of lymph node metastasis is crucial for guiding clinical surgical planning.
The simplest and least expensive method for assessing PTC lymph node metastasis is ultrasound; however, the sensitivity of detection is low because the local anatomical structure influences the appearance and characteristics of centralized lymph nodes, and their preoperative ultrasound is often free of abnormalities (4). Despite its limitations, ultrasound remains a cornerstone in the evaluation of thyroid nodules. Recent studies have explored the potential of combining ultrasound features with clinical and biochemical markers to improve the prediction of CLNM in PTC patients. However, the predictive effectiveness of such multimodal approaches has not been fully elucidated, and there remains a significant gap in the literature regarding the optimal integration of these factors for clinical use.
In this study, we aimed to address this gap by developing a comprehensive clinical prediction model that integrates ultrasound features, clinical parameters, and biochemical markers to provide a practical tool for surgeons to identify patients at risk of CLNM and guide surgical treatment strategies.
Materials and methods
Individuals and study design
A total of 685 individuals from two medical institutions from January 2020 to October 2022 were enrolled in this research. Patients from First Hospital of Shanxi Medical University (560) were randomly allocated into a training set (392) and an internal test set (168) at a 7:3 ratio. Patients from Changzhi Heping Hospital (125) were included as an external test set. Patient clinical data, including general clinical characteristics (age, sex), thyroid serological indicators [free thyroxine (FT4), free triiodothyronine (FT3), thyroglobulin (Tg), thyroid stimulating hormone (TSH), antithyroglobulin (TG-Ab), and antithyroid peroxidase (TPOAb)], ultrasound characteristics (tumor size, tumor location, capsule contact, margin, echogenicity, shape, taller-than-wide, composition, intranodal calcification and the number of nodules). The inclusion criteria included: 1) patients who had their first thyroid surgery, with a confirmed diagnosis of PTC by pathology and documented records of cervical lymph node pathology; 2) complete thyroid ultrasound examination within 2 weeks prior to surgery; 3) laboratory examination of thyroid serum markers within 2 weeks prior to surgery; and 4) ultrasound examination to detect the nodule, which was subsequently confirmed by postoperative pathology. The exclusion criteria were 1) incomplete clinical data; 2) unclear ultrasound images or incomplete data that could not be analyzed; 3) the presence of other malignant tumors and 4) postoperative pathological examination revealing the presence of non-PTC components within the lesions, such as follicular adenoma, atypical hyperplasia, medullary carcinoma, anaplastic carcinoma, and metastatic carcinoma. This study adhered to the principles of the Declaration of Helsinki.
Ultrasound instruments and methods
Ultrasound characteristics of the thyroid nodules were assessed via an Aplio i800 (Canon, Japan) and a Hitachi Arietta 850 System (Hitachi, Japan), which were equipped with probe frequencies of 18 MHz and 5–15 MHz, respectively. The ultrasound characteristics included the following: maximum diameter of the nodule, location, margin, echogenicity, shape, presence of capsular invasion, taller than wide, composition of the nodule, intranodal calcification and number of nodules. All ultrasonographic features were analyzed independently by two ultrasonographers who had been performing ultrasonography for more than 5 years, and in the case of inconsistent results, a third physician discussed and made the diagnosis. To reduce interobserver variability in the interpretation of the ultrasound characteristics of nodules (5). The operators ultrasound skills have been trained through a standardized and unified three-year training program at medical institutions. The ultrasound features of the thyroid nodules were described in accordance with the ACR TI-RADS criteria (6). The kappa coefficient is used to assess the consistency between these two ultrasound physicians. To evaluate the overall consistency, the average κ value is calculated on the basis of the k values assessed for each variable.
Clinical and biochemical indicators of thyroid function
The patients’ age, sex and thyroid serological indicators, namely, FT3, FT4, TSH, Tg, Tg-Ab, and TPOAb were collected 2 weeks prior to surgery. Values that exceeded normal were considered high, whereas those that did not were considered normal.
Definitions
The calcification points ≤ 2 mm in microcalcification and >2 mm in calcification are coarse calcifications. Hashimoto’s thyroiditis (HT) was defined on the basis of the patient’s positive preoperative levels of TPOAb and TgAb and the appearance of alterations in the features of the ultrasound images. Capsular contact was classified into three categories: far from the thyroid capsule (≥ 2 mm), contact with the thyroid capsule (< 2 mm) and invasion or breakthrough of the thyroid capsule. The margin is defined as smooth and irregular, with irregularities, including ill-defined and spiculated or microlobulated edges (7).
Data statistics
Data analyses were performed with Free Statistics version 2.1 (http://www.clinicalscientists.cn/freestatistics/, Beijing, China) and R version 4.2.2 (http://www.R-project.org, The R Foundation). Statistical significance was determined at P < 0.05 (two-sided). At a 7:3 ratio, the dataset was divided into a training set and a validation set. Continuous variables that are normally distributed are documented as the means with standard deviations (SDs), and categorical variables are reported as the number and percentage of patients in each category. Independent sample t tests were used for intergroup comparisons; chi-square (χ2) tests were used for intergroup comparisons of count data. To address missing data in the analysis, multiple imputation by chained equations (MICE) was utilized.
Multiple stages were executed for the construction and validation of nomograms aimed at predicting CLNM. First, BSR and LASSO regression were applied to select potential risk factors, and the two screening methods were compared. Next, we performed a multivariable logistic regression analysis to pinpoint the independent risk factors for CLNM and then presented the outcomes in a nomogram format. ROC decision curve and calibration analyses were subsequently used to evaluate the model’s discrimination ability and calibration accuracy. Furthermore, the model’s robustness was ensured through external validation via an independent dataset.
Results
We included 560 patients aged 45.5 ± 11.5 years; 77.9% were female, and 22.1% were male. Among all the multifocal nodules, the one with the most characteristic ultrasonography characteristics was chosen for assessment. The overall prevalence of CLNM disease was 45.7%. The baseline demographic clinical data and ultrasound features of the individuals are shown in Table 1. Sex, age, Tg, and whole ultrasound characteristics were significantly different between the two groups. We first selected optimal predictors via LASSO regression. When lambda was optimized at 0.032 (1 standard error above the minimum criterion), eleven variables were retained, including age, sex, composition, shape, size, margin, microcalcifications, number, location (left–right distribution), Tg, and contact with the capsule. We then used the BSR to identify potential prognostic factors. The selection of variables was based on the Bayesian information criterion (BIC). Composition, microcalcifications, location (left–right distribution), shape, and Tg were not screened out, and the other factors were approximately consistent with the LASSO regression. We assessed the AUCs for both the six-variable model (0.883, 95% CI: 0.856 to 0.909) and the eleven-variable model (0.891, 95% CI: 0.865 to 0.917), with a P value of 0.052 (Figure 1). In line with logistic regression model principles, a good model fit is typically achieved with a smaller set of variables; consequently, we selected six variables as the optimal predictors and incorporated them into our logistic regression model. These factors were ultimately validated as risk factors for CLNM. The kappa coefficient for the ultrasound feature assessment of the thyroid nodules was 0.75.
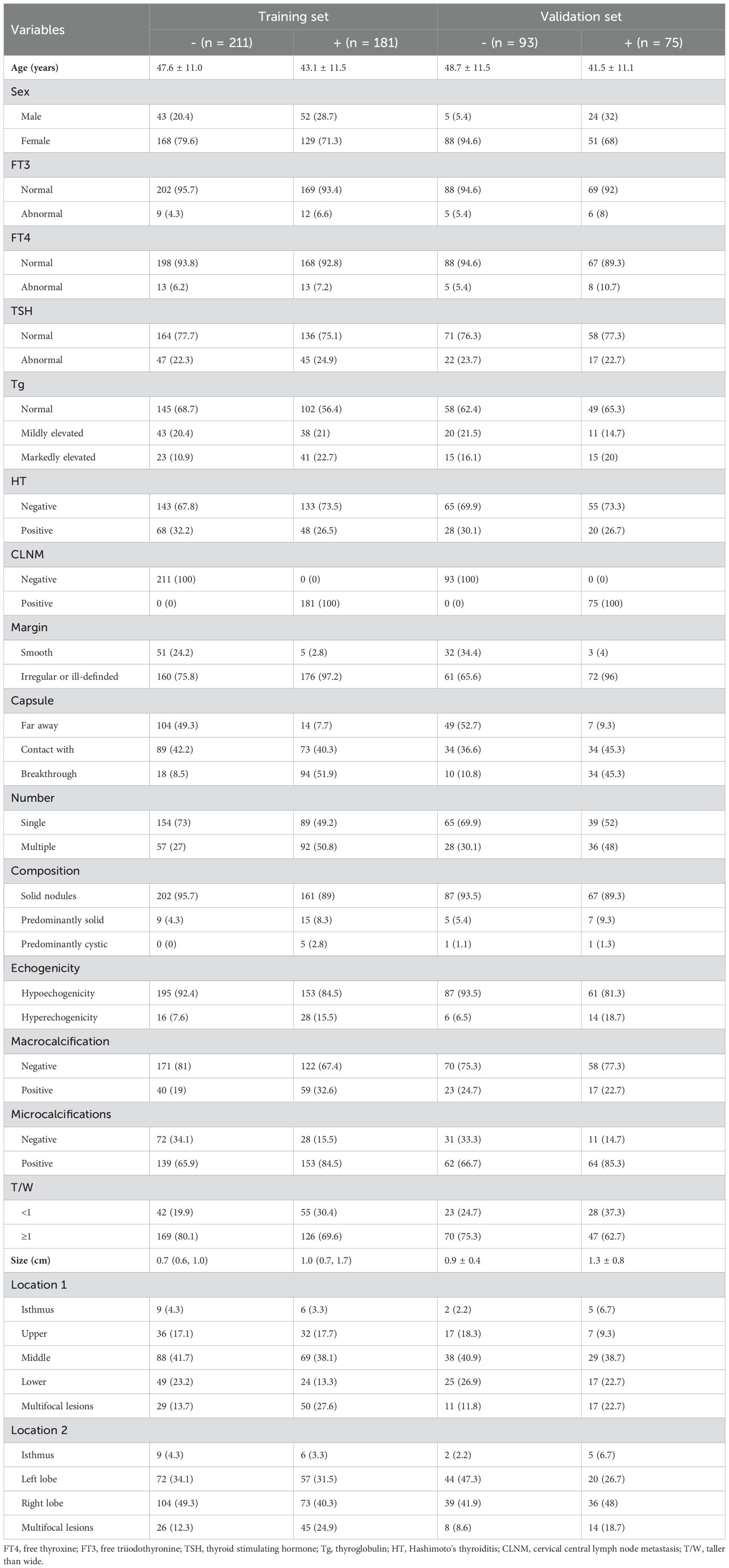
Table 1. Baseline characteristics of the training set and validation set.
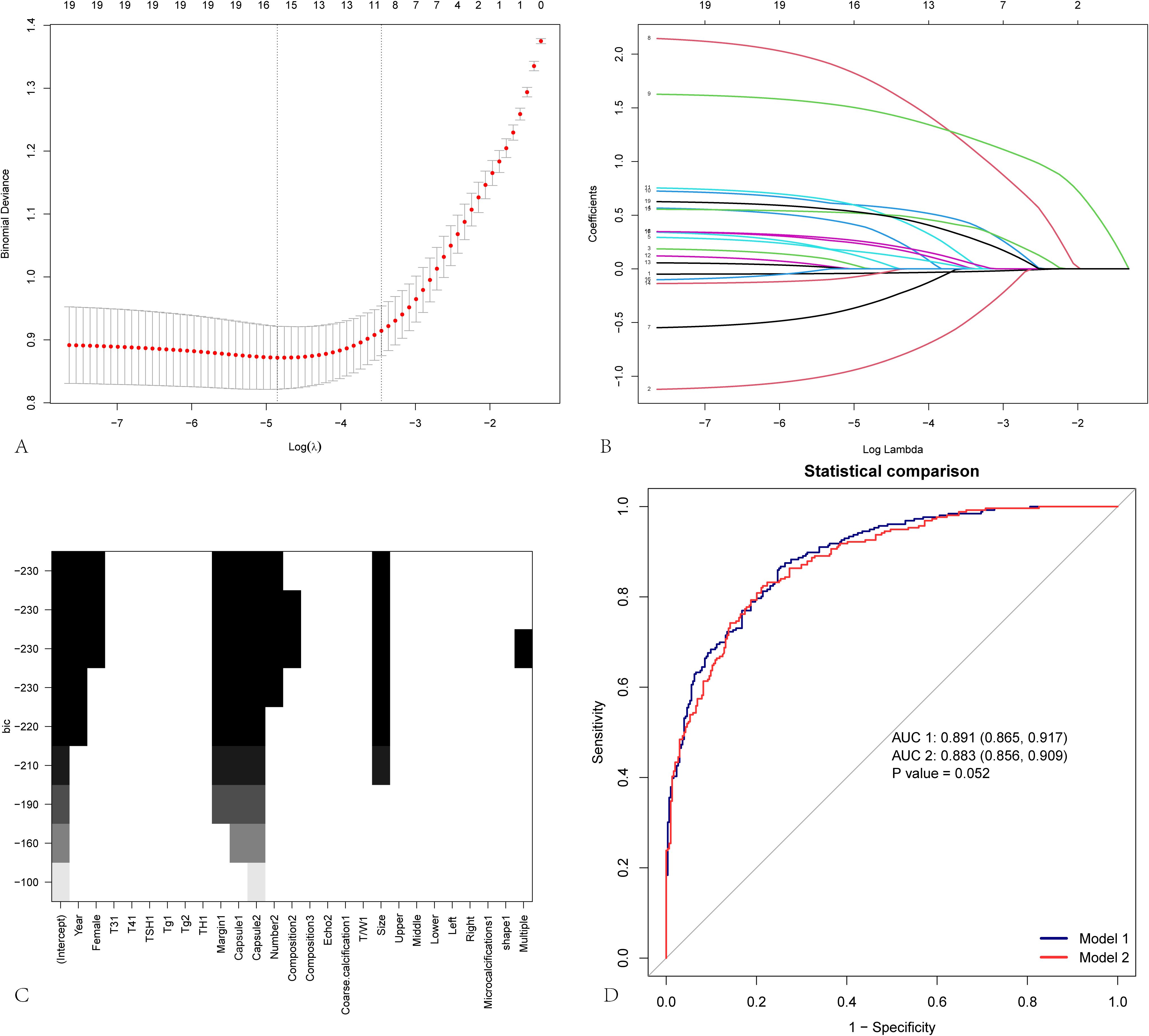
Figure 1. Variable screening for predicting cervical lymph node metastasis. LASSO regression and best subset regression analysis were used to select characteristic factors. (A) By verifying the optimal parameter (lambda) in the Lasso model, eleven variables with nonzero coefficients were selected. The mean-square error curve was plotted versus log(lambda), and dotted vertical lines were drawn on the basis of the 1 standard error criterion using the optimal lambda. Lasso refers to the least absolute shrinkage and selection operator. (B) A coefficient profile plot was produced for the log(lambda) sequence. (C) Best subset selection on the basis of the Bayesian information criterion (BIC). (D) Comparison of the ROC curves and AUC values between Model 1 and Model 2. Model 1 is constructed on the basis of 11 variables selected via LASSO regression, whereas Model 2 is based on 7 variables selected via best subset regression (BSR). The AUC values for the two models are 0.891 and 0.883, respectively, with a P value of 0.052, indicating that the difference between the two models is not statistically significant.
Logistic regression analysis of these factors (Tables 2, 3) revealed that women had an odds ratio (OR) of 0.3 (0.17–0.53) for CLNM compared with men. The OR for CLNM was 12.2 for ill-defined margins compared with smooth margins. The OR for CLNM was 5.42 for tumors in contact with the capsule and 28.37 for tumor invasion and invasion or breakthrough of the capsule compared with tumors located far from the capsule. Moreover, the incidence of CLNM increased by 5% with decreasing age. There was also a 119% increase in the incidence of multifocal lesions and a 245% increase in the incidence when the nodule diameter increased by one centimeter.
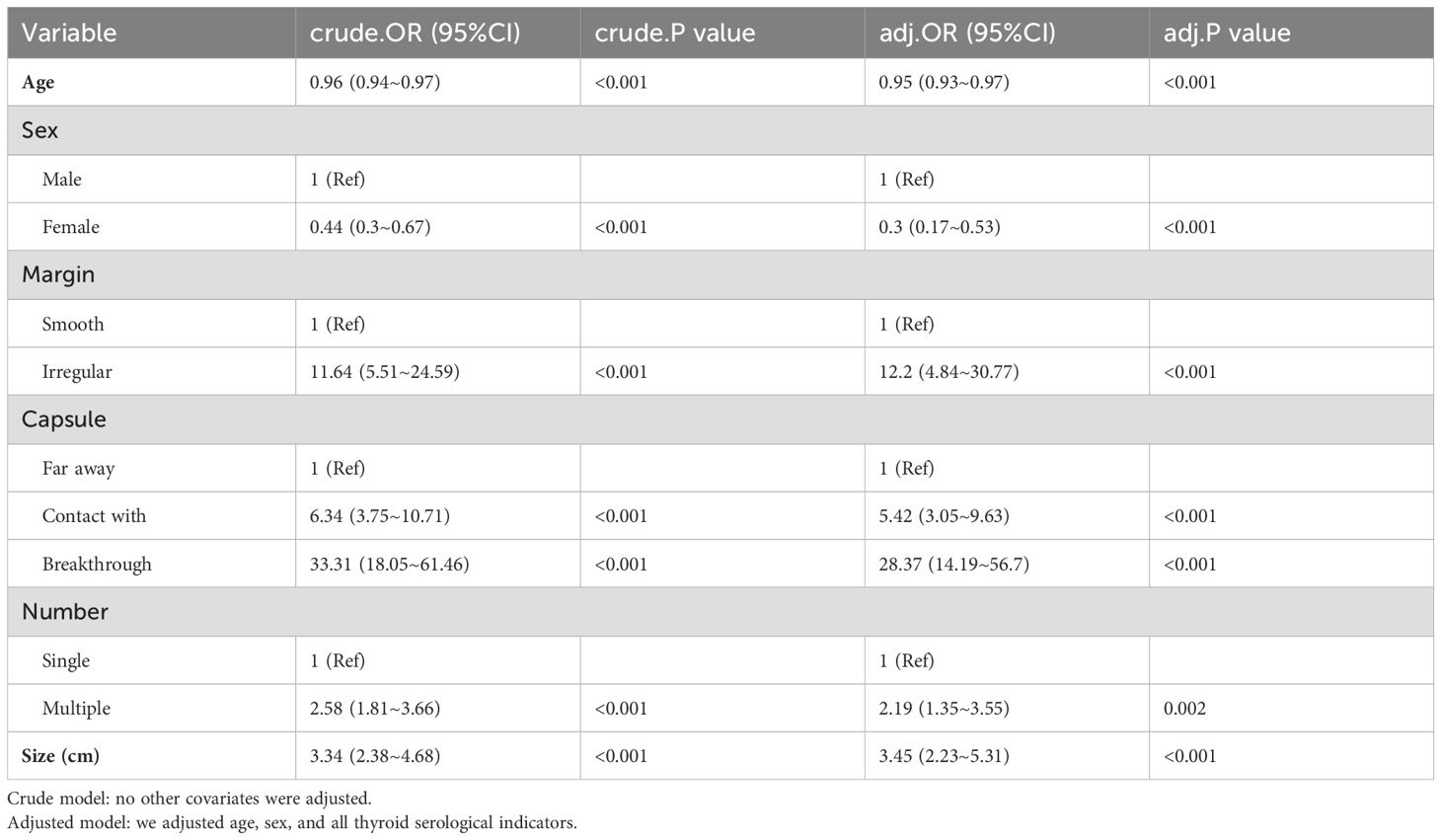
Table 2. Multivariate logistic regression analysis of risk factors associated with CLNM.
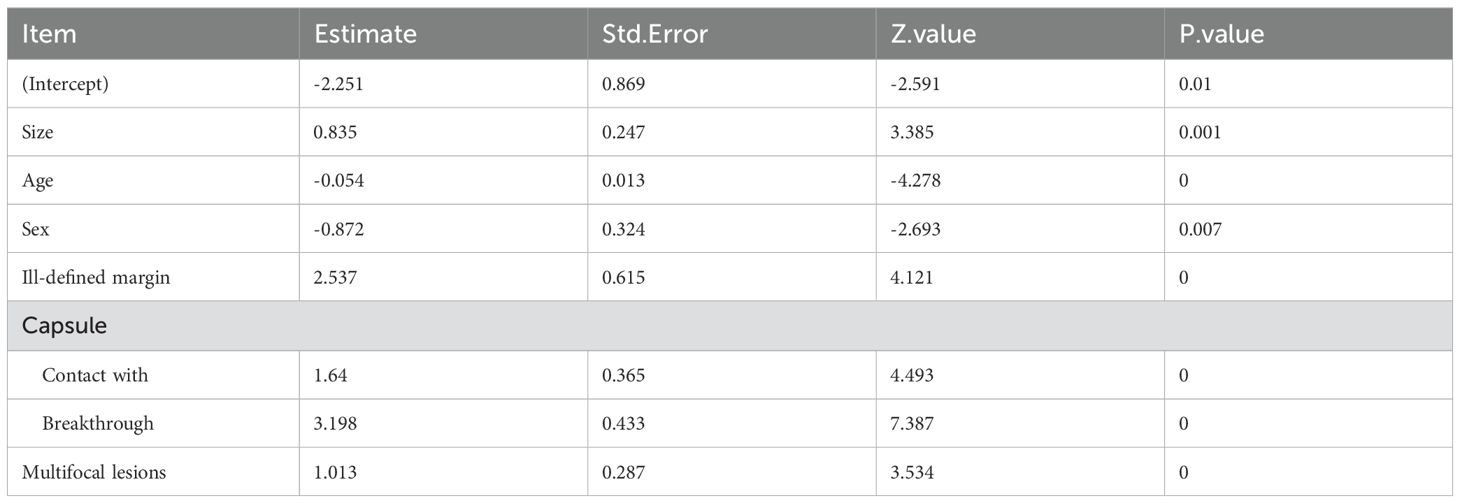
Table 3. Logistic analyses of the risk factors and CLNM.
The nomogram was created via six prognostic factors derived from multivariate logistic regression analysis (Figure 2). Summing the individual scores for each variable yields a cumulative total, which corresponds to a specific value on the risk axis indicative of the likelihood of CLNM in patients with PTC. An elevated score signifies an increased risk of CLNM for PTC patients. For example, the following results were obtained: male, 35 years old, largest diameter=1.5 cm, multifocal lesions, contact with the capsule, and ill-defined margins. The corresponding risk for CLNM was 73% (Supplementary Figure 1).
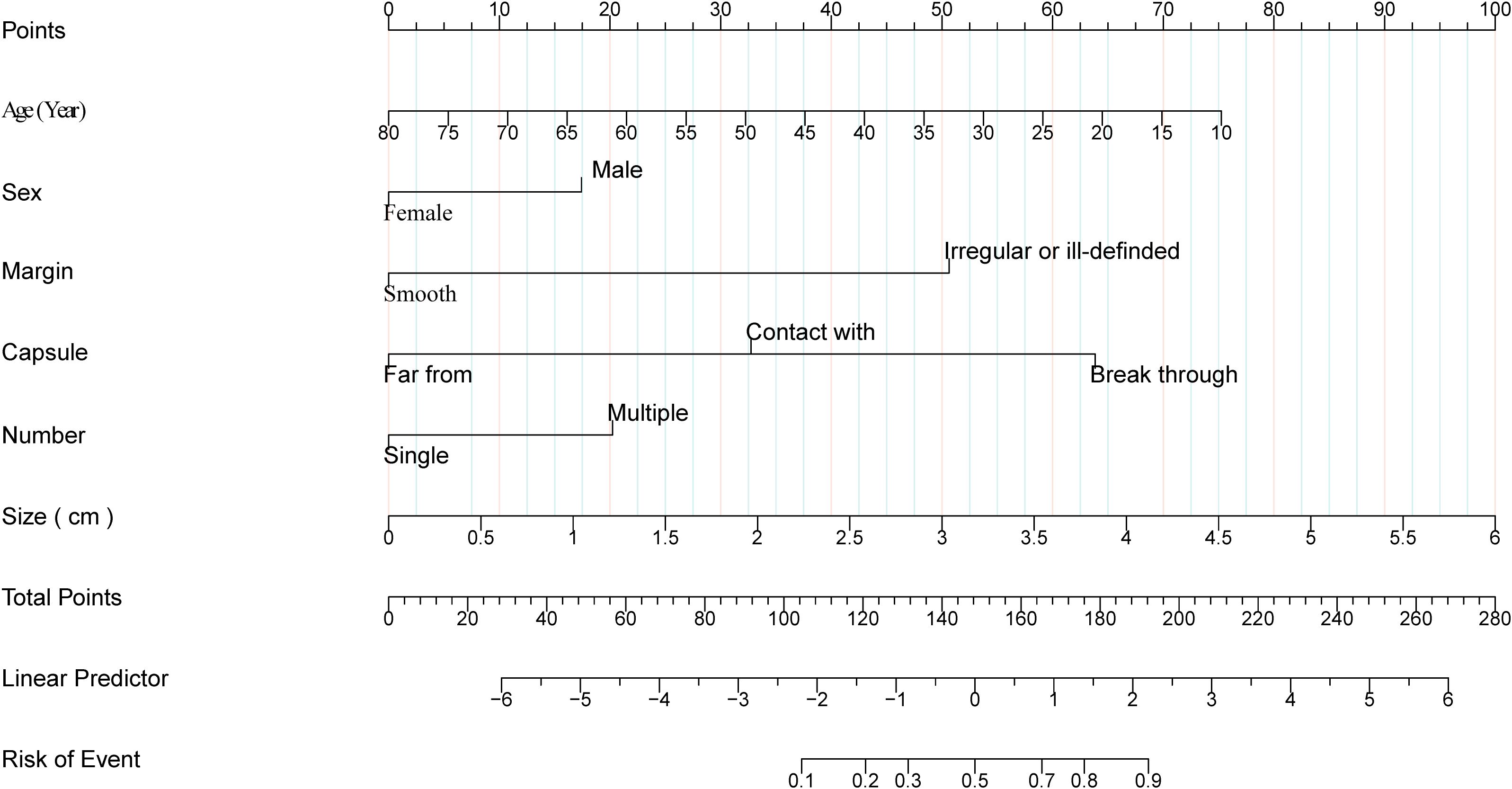
Figure 2. Nomogram of cervical lymph node metastases in papillary thyroid carcinoma. Clinical and ultrasound factor-based nomograms used for preoperatively predicting CLNM in PTC patients.
We performed 7:3 random split verification and bootstrapping to evaluate the model. The nomogram was assessed via the area under the curve (AUC) and Brier value. The Briers for the training set, internal cross-validation test set and external validation test set were 0.138, 0.134, and 0.103, respectively (Table 4). To assess the accuracy of the model, Figure 3 shows the ROC curves, clinical decision curves, and calibration curves for the training and test groups. The AUC of the model was 0.884 (0.851, 0.916) in the training set and 0.876 (0.826, 0.925) in the testing set (Figures 3A, B). The model’s calibration demonstrated satisfactory agreement, as evidenced by the nonsignificant Hosmer–Lemeshow test results for both the training set (χ2 = 6.791, p = 0.559) and testing set (χ2 = 11.179, p = 0.692) (Figures 3C, D; Table 4). A decision curve revealed that patients received a net clinical benefit (Figures 3E, F). Supplementary Figure 2 shows the AUCs of the training set and the internal and external test sets. Overall, the plots indicate that all three datasets exhibit strong performance across discrimination, calibration, and decision-making utility.

Table 4. Predictive performance of the final prediction model on the basis of random split and bootstrap verification.
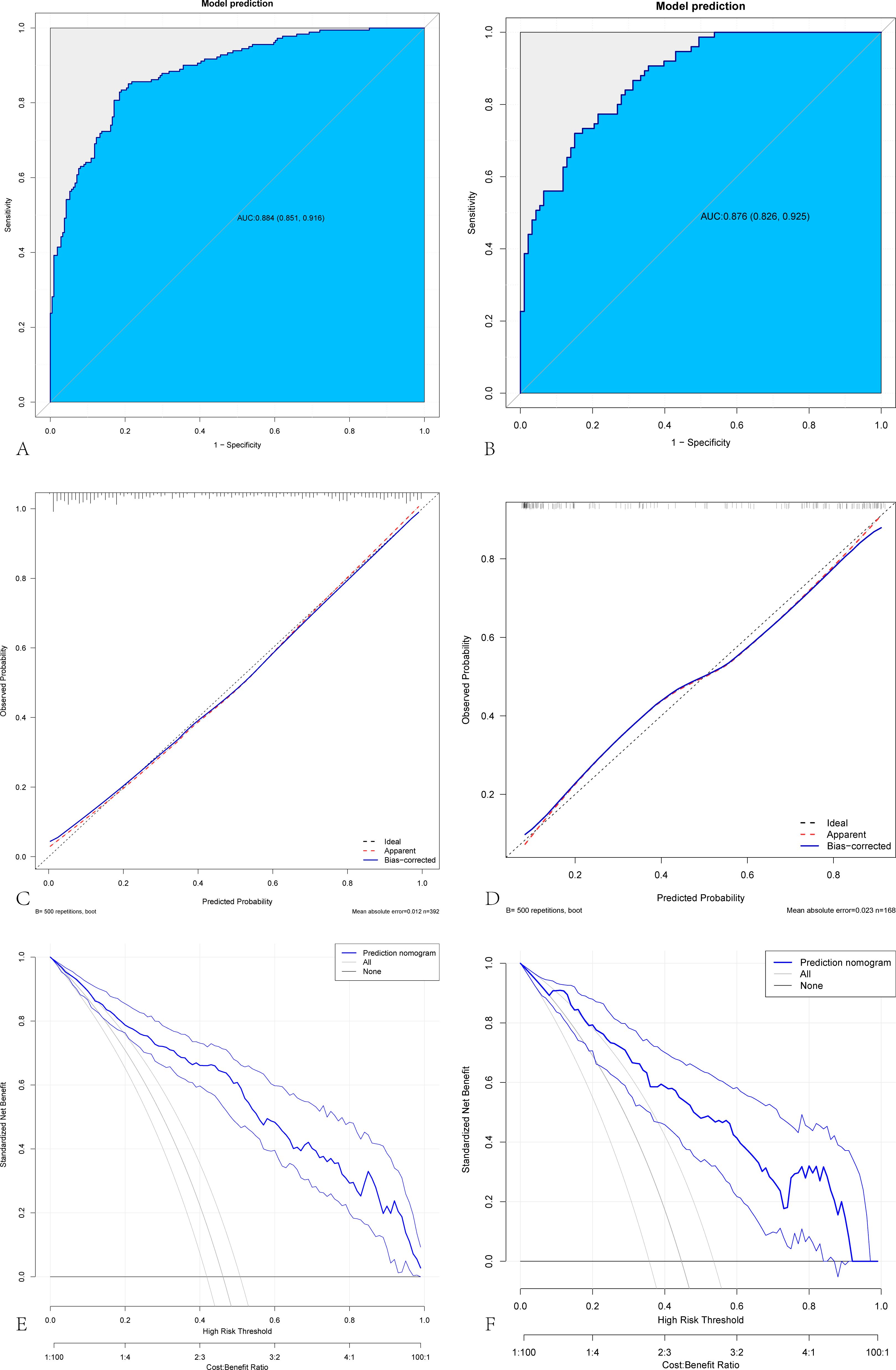
Figure 3. Internal validation of a predictive model for cervical lymph node metastasis in papillary thyroid carcinoma. Evaluation of the prediction model on the training set and internal validation set. (A, B) ROC curves of the CLNM prediction model in the training and internal cross-validation sets. (C, D) Calibration curves of CLNM for papillary thyroid cancer in the training and internal cross-validation sets. (E, F) The decision curve of CLNM for papillary thyroid cancer in the training and internal cross-validation sets.
Discussion
Although the prognosis of PTC is relatively good, CLNM often occurs in the early stage of the disease (8). Identifying independent risk factors for CLNM is therefore critical, as it can help guide clinical management and treatment decisions for thyroid nodules. In this study, we constructed and validated a nomogram using factors such as age, sex, tumor size, margin, number of tumors and whether the tumor was in contact with or had invaded the capsule. To predict CLNM, this nomogram was assessed via the AUC, decision curve and calibration curve. Our research demonstrated that the nomogram has strong discriminative power, satisfactory calibration performance, and practical clinical applicability.
Investigators have developed predictive models based on laboratory biochemical indicators or ultrasound features to help clinicians identify patients with a greater likelihood of CLNM (9, 10). Hu et al. reported that the levels of FT3, TPOAb and Tg were significantly different between patients with and without LNM, and multifactorial regression analysis revealed that Tg was an independent predictor of LNM (10). In our study, no significant difference in Tg levels was observed between the metastatic and nonmetastatic groups, indicating that Tg is not an independent predictor; therefore, the authors suggest that whether serum Tg can be used as a routine preoperative measurement to assess the aggressiveness of thyroid nodules needs to be confirmed by further studies. Previous studies have reported conflicting findings regarding the correlation between HT and CLNM in patients with PTC (11–13). Some researchers have reported a positive association, suggesting that the autoimmune response to HT, which elevates TSH levels, may promote PTC progression and invasion as TSH levels increase (14–16). Other studies have concluded that patients with HT are at a significantly greater risk of developing PTC and that the disease tends to be more indolent (17, 18). HT was not identified as a significant predictor of CLNM in our study. Consequently, the nomogram reflects the absence of HT as a contributing factor to the prediction of CLNM.
More research has been conducted on the usefulness of PTC ultrasonography characteristics in predicting CLNM (19–23). Zhou et al. reported that maximum tumor diameter, microcalcification and irregular margins were independent risk factors for CLNM (24). The average maximum diameters of the tumors in the positive and negative groups were 13.3 mm and 8.5 mm, respectively. In contrast, our study found these values to be 10.0 mm and 7.0 mm, with a cutoff value of 7.5 mm (Table 5). The possible reason is that most patients who underwent surgery had thyroid nodules greater than 1.0 cm in their research but less than 1.0 cm in our study. The definition of the nodule size cutoff value (1.0 cm) aims to avoid excessive diagnosis and overtreatment of low-risk indolent PTC, but it also risks neglecting early-stage invasive cancers (25). However, this cutoff value has not been widely accepted (26, 27). In light of this, clinicians should be vigilant in treating CLNM when the nodule diameter is greater than 0.75 cm to avoid inadequate treatment. The histological features of the tumor margin reflect the invasiveness of the tumor (28). This feature is particularly evident in thyroid cancer. Our study results also confirmed this, and the underlying mechanism may be that malignant tumor cells grow rapidly and unevenly, leading to an irregular shape and unclear margins of the nodule.

Table 5. The predictive value of age and nodule size for CLNM.
Previous studies have been controversial regarding whether the location of the nodule is associated with CLNM (22, 29, 30). Our study revealed that the location of the nodule is not a significant predictor of CLNM, which is consistent with the findings of Chen’s study (31). The number of lesions is associated with the invasive characteristics of the nodules. Patients with multiple foci have a greater risk of lymph node metastasis, vascular invasion, and extrathyroidal extension (32, 33). Our study results further support the viewpoint that multifocality serves as a significant predictor of CLNM. Additionally, microcalcifications, coarse calcifications, echo, composition, and T/W were significantly different between the lymph node metastasis set and the nonmetastasis set, but multifactorial regression analysis revealed that these features were not independent risk factors for CLNM.
The adjacent capsule, especially the breakthrough capsule, can predict CLNM, especially in male patients (4, 23, 34, 35). This is because thyroid cancer tissues can express matrix metalloproteinases (MMPs), which disrupt the extracellular matrix and basement membrane components, facilitating invasion into the surrounding stroma (36, 37). The encroachment of a nodule upon the thyroid capsule results in a breach of its continuous structure. Consequently, the nodule may eventually penetrate the capsule, facilitating its spread to adjacent tissues and regional lymph nodes (38). With respect to the impact of sex hormones on PTC, bioinformatics and fundamental experimental results suggest that testosterone secretion promotes the growth and invasive malignant behavior of PTC (39); therefore, being male may imply a greater likelihood of metastasis (40). In PTC, age stands out as a highly significant prognostic factor, with younger patients being more likely to experience lateral neck lymph node metastasis (41). Genetic factors may also contribute to the varying incidence rates of lymph node metastasis (LNM) in papillary thyroid carcinoma (PTC) across different ages and sexes. For example, certain populations might exhibit a higher prevalence of specific genetic mutations or elevated expression of particular channel proteins. These genetic and protein profiles can interact with age and sex, thereby influencing the progression of the disease (42, 43). Most studies employ 45 years or 55 years as the cutoff for staging. This method is based on the American Joint Committee on Cancer/Tumor-Node-Metastasis (AJCC/TNM; www.cancerstaging.org) system, which is the most widely used method for predicting disease-specific survival in patients with differentiated thyroid cancer. When age is considered as a continuous variable, the cutoff values obtained from different studies also tend to be close to these two values (8, 44), which is consistent with our study results. Consequently, it is essential for ultrasonographers to meticulously assess the interface between nodules and the thyroid capsule especially in young males. Such a detailed examination enhances the precision of prognostic information pertaining to cervical lymph node metastasis (CLNM), which is conveyed to surgical teams (38, 45).
Clinical laboratory and ultrasound indicators were jointly predicted in our investigation. This approach overcomes the limitations of single predictors in previous research (8, 46, 47). While these models have shown moderate success, they may not capture the full complexity of the disease dynamics. Additionally, the prediction model demonstrated excellent generalizability and clinical applicability in preliminary validation. By predicting the risk of lymph node metastasis preoperatively, our model can guide clinicians in determining whether to perform lymph node dissection. This precise risk assessment helps avoid over-treatment or under-treatment, ensuring that patients receive the most appropriate care.
Nevertheless, several limitations should be acknowledged. First, its retrospective nature makes it susceptible to selection bias. For example, potential confounding factors such as environmental pollution and genetic mutations were not considered in this study, which may have influenced our results. Second, while we expanded our dataset by incorporating cases from another medical institution for external validation, the total number of PTC patients included in this study was relatively limited. Although this addition represents a step forward, our data are still limited to only two centers. To ensure the robust clinical application of our model, it is essential to further expand the dataset to include cases from multiple centers. This will provide a more comprehensive and diverse patient population, thereby enhancing the generalizability and reliability of our findings. In addition, although the nomogram and decision curve analysis in this study demonstrated the substantial clinical utility of the model, enabling accurate preoperative prediction of CLNM through clinical assessment and thus achieving clinical benefits, challenges related to standardization still persist. Therefore, comprehensively strengthening standardized operating procedures and applying validated and widely recognized thyroid imaging data systems to promote consistency in data evaluation are recommended.
Conclusions
A prognostic tool and nomogram for estimating CLNM in patients with PTC were developed and demonstrated robust performance in terms of discrimination and calibration, achieving very high diagnostic efficacy in the internal and external validation groups and providing a basis to help clinicians better manage PTC patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of First Hospital of Shanxi Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Our study is a retrospective analysis of previously collected medical data. Our study has been reviewed by the Ethics Committee, which determined that the research meets the criteria for a waiver of informed consent and has granted formal approval for the waiver.
Author contributions
YH: Methodology, Funding acquisition, Writing – review & editing. YS: Conceptualization, Data curation, Formal analysis, Writing – original draft. YL: Conceptualization, Data curation, Formal analysis, Writing – original draft. QP: Conceptualization, Data curation, Formal analysis, Writing – original draft. LL: Methodology, Project administration, Funding acquisition, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Key Research and Development Project of Shanxi Province (201903D321190).
Acknowledgments
This thesis would never have materialized without help and support from many parties. First, I would like to express my sincere gratitude to my counterparts at China Shanxi Medical University, Professor Chen Yaodong and Gao Feng, who gave me a great deal of useful and constructive advice on my thesis. We also thank Dr. Liu Jie (People’s Liberation Army of China General Hospital, Beijing, China) for his help with this thesis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1549148/full#supplementary-material
Supplementary Figure 1 | Clinical usage of our nomogram.
Supplementary Figure 2 | Model performance evaluation across different datasets: ROC curves and calibration curves (A-C) ROC curves for the model evaluated on the training dataset, internal validation dataset, and external validation dataset. (D-F) Calibration curves for the training set, internal validation set, and external validation set, respectively.
References
1. Miranda-Filho A, Lortet-Tieulent J, Bray F, Cao B, Franceschi S, Vaccarella S, et al. Thyroid cancer incidence trends by histology in 25 countries: a population-based study. Lancet Diabetes Endocrinol. (2021) 9:225–34. doi: 10.1016/S2213-8587(21)00027-9
2. Wang W, Ding Y, Jiang W, Li X. Can cervical lymph node metastasis increase the risk of distant metastasis in papillary thyroid carcinoma? Front Endocrinol (Lausanne). (2022) 13:917794. doi: 10.3389/fendo.2022.917794
3. Yu J, Deng Y, Liu T, Zhou J, Jia X, Xiao T, et al. Lymph node metastasis prediction of papillary thyroid carcinoma based on transfer learning radiomics. Nat Commun. (2020) 11:4807. doi: 10.1038/s41467-020-18497-3
4. Chen SP, Jiang X, Zheng WW, Luo YL. Correlation between sonographic features and central neck lymph node metastasis in solitary solid papillary thyroid microcarcinoma with a taller-than-wide shape. Diagnostics (Basel). (2023) 13(5):949. doi: 10.3390/diagnostics13050949
5. Solymosi T, Hegedus L, Bonnema SJ, Frasoldati A, Jambor L, Karanyi Z, et al. Considerable interobserver variation calls for unambiguous definitions of thyroid nodule ultrasound characteristics. Eur Thyroid J. (2023) 12(2):e220134. doi: 10.1530/ETJ-22-0134
6. Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, Teefey SA, et al. ACR thyroid imaging, reporting and data system (TI-RADS): white paper of the ACR TI-RADS committee. J Am Coll Radiol. (2017) 14:587–95. doi: 10.1016/j.jacr.2017.01.046
7. Rago T, Vitti P. Risk stratification of thyroid nodules: from ultrasound features to TIRADS. Cancers (Basel). (2022) 14(3):717. doi: 10.3390/cancers14030717
8. He L, Chen X, Hu J, Meng Y, Zhang Y, Chen W, et al. Score based on contrast-enhanced ultrasound predict central lymph node metastasis in papillary thyroid cancer. Front Endocrinol (Lausanne). (2024) 15:1336787. doi: 10.3389/fendo.2024.1336787
9. Zhao L, Zhou T, Zhang W, Wu F, Jiang K, Lin B, et al. Blood immune indexes can predict lateral lymph node metastasis of thyroid papillary carcinoma. Front Endocrinol (Lausanne). (2022) 13:995630. doi: 10.3389/fendo.2022.995630
10. Hu MJ, Zhang C, Liang L, Wang SY, Zheng XC, Zhang Q, et al. Fasting serum glucose, thyroid-stimulating hormone, and thyroid hormones and risk of papillary thyroid cancer: A case-control study. Head Neck. (2019) 41:2277–84. doi: 10.1002/hed.25691
11. Ferrari SM, Fallahi P, Elia G, Ragusa F, Ruffilli I, Paparo SR, et al. Thyroid autoimmune disorders and cancer. Semin Cancer Biol. (2020) 64:135–46. doi: 10.1016/j.semcancer.2019.05.019
12. Mcleod DSA, Bedno SA, Cooper DS, Hutfless SM, Ippolito S, Jordan SJ, et al. Pre-existing thyroid autoimmunity and risk of papillary thyroid cancer: A nested case-control study of US active-duty personnel. J Clin Oncol. (2022) 40:2578–87. doi: 10.1200/JCO.21.02618
13. Li X, Zhang H, Zhou Y, Cheng R. Risk factors for central lymph node metastasis in the cervical region in papillary thyroid carcinoma: a retrospective study. World J Surg Oncol. (2021) 19:138. doi: 10.1186/s12957-021-02247-w
14. Demircioglu ZG, Demircioglu MK, Aygun N, Akgun IE, Unlu MT, Kostek M, et al. Relationship between thyroid-stimulating hormone level and aggressive pathological features of papillary thyroid cancer. Sisli Etfal Hastan Tip Bul. (2022) 56:126–31. doi: 10.14744/SEMB.2022.14554
15. Liu Y, Lv H, Zhang S, Shi B, Sun Y. The impact of coexistent hashimoto’s thyroiditis on central compartment lymph node metastasis in papillary thyroid carcinoma. Front Endocrinol (Lausanne). (2021) 12:772071. doi: 10.3389/fendo.2021.772071
16. Min Y, Huang Y, Wei M, Wei X, Chen H, Wang X, et al. Preoperatively predicting the central lymph node metastasis for papillary thyroid cancer patients with hashimoto’s thyroiditis. Front Endocrinol (Lausanne). (2021) 12:713475. doi: 10.3389/fendo.2021.713475
17. Janicki L, Patel A, Jendrzejewski J, Hellmann A. Prevalence and Impact of BRAF mutation in patients with concomitant papillary thyroid carcinoma and Hashimoto’s thyroiditis: a systematic review with meta-analysis. Front Endocrinol (Lausanne). (2023) 14:1273498. doi: 10.3389/fendo.2023.1273498
18. Xu S, Huang H, Qian J, Liu Y, Huang Y, Wang X, et al. Prevalence of hashimoto thyroiditis in adults with papillary thyroid cancer and its association with cancer recurrence and outcomes. JAMA Netw Open. (2021) 4:e2118526. doi: 10.1001/jamanetworkopen.2021.18526
19. Gao X, Luo W, He L, Cheng J, Yang L. Predictors and a prediction model for central cervical lymph node metastasis in papillary thyroid carcinoma (cN0). Front Endocrinol (Lausanne). (2021) 12:789310. doi: 10.3389/fendo.2021.789310
20. Heng Y, Yang Z, Lin J, Liu Q, Cai W, Tao L. Risks of central lymph node metastasis in papillary thyroid carcinoma with or without multifocality in at least one lobe: A multi-center analysis. Oral Oncol. (2022) 134:106185. doi: 10.1016/j.oraloncology.2022.106185
21. Gong J, Zhu B, Liu W, Shi C, Xia C, Zeng L, et al. Risk factors for lymph node metastasis in papillary thyroid carcinoma: A retrospective study. Horm Metab Res. (2023) 55:315–22. doi: 10.1055/a-2057-8358
22. Lin P, Liang F, Ruan J, Han P, Liao J, Chen R, et al. A preoperative nomogram for the prediction of high-volume central lymph node metastasis in papillary thyroid carcinoma. Front Endocrinol (Lausanne). (2021) 12:753678. doi: 10.3389/fendo.2021.753678
23. Mattingly AS, Noel JE, Orloff LA. A closer look at “Taller-than-wide” Thyroid nodules: examining dimension ratio to predict Malignancy. Otolaryngol Head Neck Surg. (2022) 167:236–41. doi: 10.1177/01945998211051310
24. Zhou L, Yao J, Ou D, Li M, Lei Z, Wang L, et al. A multi-institutional study of association of sonographic characteristics with cervical lymph node metastasis in unifocal papillary thyroid carcinoma. Front Endocrinol (Lausanne). (2022) 13:965241. doi: 10.3389/fendo.2022.965241
25. Amendola S, Piticchio T, Scappaticcio L, Sellasie SW, Volpe S, Le Moli R, et al. Papillary thyroid carcinoma: </= 10 mm does not always mean pN0. A multicentric real-world study. Updates Surg. (2024) 76:1055–61. doi: 10.1007/s13304-024-01779-6
26. Wei X, Min Y, Feng Y, He D, Zeng X, Huang Y, et al. Development and validation of an individualized nomogram for predicting the high-volume (> 5) central lymph node metastasis in papillary thyroid microcarcinoma. J Endocrinol Invest. (2022) 45:507–15. doi: 10.1007/s40618-021-01675-5
27. Liu C, Xiao C, Chen J, Li X, Feng Z, Gao Q, et al. Risk factor analysis for predicting cervical lymph node metastasis in papillary thyroid carcinoma: a study of 966 patients. BMC Cancer. (2019) 19:622. doi: 10.1186/s12885-019-5835-6
28. Kim KJ, Hong SW, Lee YS, Kim BW, Lee SC, Chang HS, et al. Tumor margin histology predicts tumor aggressiveness in papillary thyroid carcinoma: a study of 514 consecutive patients. J Korean Med Sci. (2011) 26:346–51. doi: 10.3346/jkms.2011.26.3.346
29. Zhang F, Oluwo O, Castillo FB, Gangula P, Castillo M, Farag F, et al. Thyroid nodule location on ultrasonography as a predictor of Malignancy. Endocr Pract. (2019) 25:131–7. doi: 10.4158/EP-2018-0361
30. Jasim S, Baranski TJ, Teefey SA, Middleton WD. Investigating the effect of thyroid nodule location on the risk of thyroid cancer. Thyroid. (2020) 30:401–7. doi: 10.1089/thy.2019.0478
31. Chen Y, Zhao S, Zhang Z, Chen Z, Jiang B, An M, et al. A comprehensive prediction model for central lymph node metastasis in papillary thyroid carcinoma with Hashimoto’s thyroiditis: BRAF may not be a valuable predictor. Front Endocrinol (Lausanne). (2024) 15:1429382. doi: 10.3389/fendo.2024.1429382
32. Feng JW, Qu Z, Qin AC, Pan H, Ye J, Jiang Y, et al. Significance of multifocality in papillary thyroid carcinoma. Eur J Surg Oncol. (2020) 46:1820–8. doi: 10.1016/j.ejso.2020.06.015
33. Woo J, Kim H, Kwon H. Impact of multifocality on the recurrence of papillary thyroid carcinoma. J Clin Med. (2021) 10(21):5144. doi: 10.3390/jcm10215144
34. Wei R, Wang H, Wang L, Hu W, Sun X, Dai Z, et al. Radiomics based on multiparametric MRI for extrathyroidal extension feature prediction in papillary thyroid cancer. BMC Med Imaging. (2021) 21:20. doi: 10.1186/s12880-021-00553-z
35. Yan C, He X, Chen Z, Wang Y. Central compartment lymph nodes have distinct metastatic patterns in different age groups. Front Endocrinol (Lausanne). (2022) 13:807431. doi: 10.3389/fendo.2022.807431
36. Zhou J, Xu M, Tan J, Zhou L, Dong F, Huang T. MMP1 acts as a potential regulator of tumor progression and dedifferentiation in papillary thyroid cancer. Front Oncol. (2022) 12:1030590. doi: 10.3389/fonc.2022.1030590
37. Ivkovic I, Limani Z, Jakovcevic A, Huic D, Prgomet D. Role of matrix metalloproteinases and their inhibitors in locally invasive papillary thyroid cancer. Biomedicines. (2022) 10(12):3178. doi: 10.3390/biomedicines10123178
38. Guang Y, He W, Zhang W, Zhang H, Zhang Y, Wan F. Clinical study of ultrasonographic risk factors for central lymph node metastasis of papillary thyroid carcinoma. Front Endocrinol (Lausanne). (2021) 12:791970. doi: 10.3389/fendo.2021.791970
39. Jiang C, Xu F, Yi D, Jiang B, Wang R, Wu L, et al. Testosterone promotes the migration, invasion and EMT process of papillary thyroid carcinoma by up-regulating Tnnt1. J Endocrinol Invest. (2024) 47:149–66. doi: 10.1007/s40618-023-02132-1
40. Jiwang L, Yahong L, Kai L, Bo H, Yuejiao Z, Haotian W, et al. Clinicopathologic factors and preoperative ultrasonographic characteristics for predicting central lymph node metastasis in papillary thyroid microcarcinoma: a single center retrospective study. Braz J Otorhinolaryngol. (2022) 88:36–45. doi: 10.1016/j.bjorl.2020.05.004
41. Cai H, Zhuge L, Huang Z, Wang S, Shi P, Yan D, et al. Distinct risk factors of lateral lymph node metastasis in patients with papillary thyroid cancer based on age stratification. BMC Surg. (2024) 24:24. doi: 10.1186/s12893-024-02309-2
42. Derwich A, Sykutera M, Brominska B, Andrusiewicz M, Ruchala M, Sawicka-Gutaj N. Clinical implications of mTOR expression in papillary thyroid cancer-A systematic review. Cancers (Basel). (2023) 15(6):1665. doi: 10.3390/cancers15061665
43. Kazandjian S, Rousselle E, Dankner M, Cescon DW, Spreafico A, Ma K, et al. The clinical, genomic, and transcriptomic landscape of BRAF mutant cancers. Cancers (Basel). (2024) 16(2):445. doi: 10.3390/cancers16020445
44. Zhou L, Zheng Y, Yao J, Chen L, Xu D. Association between papillary thyroid carcinoma and cervical lymph node metastasis based on ultrasonic radio frequency signals. Cancer Med. (2023) 12:14305–16. doi: 10.1002/cam4.6107
45. Wang H, Zhao S, Yao J, Yu X, Xu D. Factors influencing extrathyroidal extension of papillary thyroid cancer and evaluation of ultrasonography for its diagnosis: a retrospective analysis. Sci Rep. (2023) 13:18344. doi: 10.1038/s41598-023-45642-x
46. Chang L, Zhang Y, Zhu J, Hu L, Wang X, Zhang H, et al. An integrated nomogram combining deep learning, clinical characteristics and ultrasound features for predicting central lymph node metastasis in papillary thyroid cancer: A multicenter study. Front Endocrinol (Lausanne). (2023) 14:964074. doi: 10.3389/fendo.2023.964074
Keywords: papillary thyroid cancer, lymph node metastasis, risk factors, predictive model, nomograms
Citation: Hao Y, Su Y, Li Y, Pan Q and Liu L (2025) Construction of a predictive model for cervical lymph node metastasis in papillary thyroid carcinoma. Front. Oncol. 15:1549148. doi: 10.3389/fonc.2025.1549148
Received: 20 December 2024; Accepted: 07 April 2025;
Published: 15 May 2025.
Edited by:
Natalia Koerich Laureano, Federal University of Rio Grande do Sul, BrazilReviewed by:
Ioannis Koutelidakis, Aristotle University of Thessaloniki, GreeceQiqi Xie, Indiana University Bloomington, United States
Copyright © 2025 Hao, Su, Li, Pan and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liping Liu, bGl1bGlwaW5nMTYwMEBzaW5hLmNvbQ==
†These authors have contributed equally to this work