 Susy Shim1,2*
Susy Shim1,2* Mette Bak Nielsen3Mikkel Eld4Jan Stenvang5,6Rasmus Froberg Brøndum2,7Britta Weber8Anne Krejbjerg Motavaf1
Mette Bak Nielsen3Mikkel Eld4Jan Stenvang5,6Rasmus Froberg Brøndum2,7Britta Weber8Anne Krejbjerg Motavaf1 Morten Ladekarl1,2
Morten Ladekarl1,2- 1Department of Oncology and Clinical Cancer Research Center, Aalborg University Hospital, Aalborg, Denmark
- 2Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
- 3Department of Pathology, Aarhus University Hospital, Aarhus, Denmark
- 4Department of Pathology, Aalborg University Hospital, Aalborg, Denmark
- 5Department of Drug Design and Pharmacology, Copenhagen University, Copenhagen, Denmark
- 6Scandion Oncology A/S, Copenhagen, Denmark
- 7Center for Clinical Data Science, Aalborg University and Aalborg University Hospital, Aalborg, Denmark
- 8Department of Oncology, Aarhus University Hospital, Aarhus, Denmark
Background: ATP-binding cassette (ABC) proteins are transmembrane efflux pumps that play a role in Multi Drug Resistance. ABCG2 and ABCB1 have been suggested as important mediators of resistance to chemotherapy (CTx) in pancreatic cancer (PC). We determined the expression of ABCG2 and ABCB1 proteins in PC and the impact of ABCG2 on outcome of treatment with gemcitabine and nab-paclitaxel (GemNab).
Materials and methods: 140 patients with sufficient tissue for assessment that had initiated palliative treatment with GemNab for non-resectable PC from 2011 to 2019 were included at two institutions. From achieved tissue, new sections were cut and stained for ABCG2 and ABCB1. Staining was evaluated by consensus of maximum score by two pathologists. Progression-free survival (PFS) was the primary endpoint.
Results: ABCB1 expression was observed in only one case (0.7%). ABCG2 was expressed in 33% but more frequently (50%) in specimens taken after gemcitabine-based (neo)adjuvant CTx (P=0.02). In multivariate analysis, ABCG2 expression was associated with an improved PFS (HR=0.64; 95%CI 0.43-0.94 (P=0.02)) of treatment with GemNab. Prior CTx, both in the (neo)adjuvant and palliative setting, was associated with shorter PFS of GemNab (P=0.03), and ABCG2 expression tended to correlate with improved PFS in these (P=0.07), but not in CTx-naïve patients (P=0.20). Similarly, a high ABCG2 expression was associated with improved overall survival (OS) only in patients with prior exposure to CTx (P=0.03). No associations of ABCG2 expression with CTx dosing or response rates were found.
Conclusion: We found indications of upregulation of ABCG2 expression in tumors of patients previously exposed to gemcitabine, and ABCG2 expression correlated with efficacy of GemNab as assessed by PFS and OS in patients previously exposed to CTx, but not in those naïve to CTx. These findings diverge from the prevailing assumption that ABCG2 confers chemoresistance and suggest that in certain contexts, ABCG2 expression may reflect tumor adaptation or selection. Given the unexpected direction of this association, our findings should be interpreted as hypothesis-generating, and further studies are needed to elucidate underlying biological mechanisms and validate ABCG2 as a potential predictive biomarker in this setting.
1 Introduction
Pancreatic cancer (PC) is currently the sixth most common cause of cancer death (1), and is expected to become the second leading cause of cancer-related deaths in ten years (2, 3). The prognosis is grave as non-resectable disease is fatal, and surgery with curative intent can be offered to only 20-25% of patients (4).
Patients in good general condition with non-resectable disease are treated with chemotherapy (5). Compared to single-drug treatment with gemcitabine (Gem), the first drug approved for treatment of PC (6), combination-chemotherapy with folfirinox (5-flouroucil/leucovorin, irinotecan and oxaliplatin) or gemcitabine and nab-paclitaxel (GemNab) (7, 8) showed improved survival results. These regimens are now universally introduced as treatments of choice (5), GemNab being considered the most tolerable regime (9). Recently, the three-drug combination, Nalirifox (5-flouroucil/leucovorin, oxaliplatin and liposomal irinotecan) was shown to increase median overall survival by 2.9 months compared to GemNab, however, at a price of more toxicity (10, 11).
Drug resistance is a major limitation to the sustained effect of chemotherapy in PC (4, 12). Most tumors rapidly progress despite initial response, and many are clinically resistant from the start (4, 13). For example, in the pivotal MPACT study of GemNab, 20% of patients experienced progressive disease (PD) at the first evaluation and half of patients had progressed at 5.5 months (8). Therefore, several preclinical and clinical studies have investigated mechanisms of drug resistance relevant for the GemNab combination, but the mechanisms are still unclear (14).
Being a taxane, nab-paclitaxel (Nab) targets tubulin and stabilizes the microtubules causing cell cycle arrest and hence apoptosis (15, 16). The microtubule network consists of polymers of α- and β-tubulin and resistance may occur through aberrant expression of the isotype βIII-tubulin (17, 18). Other possible mechanisms of resistance include alterations in the tumor microenvironment and increased metabolism of the drug (4, 19, 20). Gem is a deoxycytidine nucleoside analogue and functions by inhibiting the DNA synthesis and by inhibiting progression of the cell cycle to G1/S-phase (21–23). Resistance to Gem may result from downregulation of nucleoside transporters, activation of cancer stem cells, epithelial-mesenchymal transition or inactivation of pathways for apoptosis (3, 15, 22).
For many chemotherapeutics, including Gem and taxanes, upregulation of drug efflux pumps may play an important role for treatment resistance (20, 21). By gaining energy from ATP hydrolysis, transmembrane efflux pumps including ATP-binding cassette (ABC) proteins can pump molecules against their gradient across plasma and intracellular membranes (24, 25). ABC-proteins are divided into seven subgroups (ABCA-ABCG) and are normally present in several kinds of tissues, such as the kidney, brain, pancreas and ovaries (24). The ABC proteins ABCB1 and ABCG2 have both been suggested as mediators of resistance to chemotherapy in PC (26) and in several other tumors (26–29). ABCB1 is known to efflux paclitaxel among other drugs but seems to be rarely expressed in PC (30, 31). ABCG2 (also called breast cancer resistance protein (BCRP)) regulates the uptake and removal of both internal and external substances, forms protective tissue barriers, and ensures the balance and stability of the body´s physiological systems (32). ABCG2 has been demonstrated to be significantly upregulated in PC tumors compared to non-malignant tissue (33). In PC cells in vitro, Gem causes upregulation of ACBG2 protein levels, increased levels of ABCG2 mRNA in PC cells are associated with acquired resistance to Gem, and Wnt5a-induced ABCG2 expression causes resistance to Gem (33–35). While neither Gem nor Nab are considered to be substrates (36), ABCG2 seems to be involved in the cellular response to oxidative stress, which is involved in initiation and progression of PC (24, 37), and may cause resistance to Gem by indirect mechanisms (38, 39). In addition, certain variant ABCG2 alleles are associated with increased risk of toxicity to taxanes (40). Clinical studies targeting ABC proteins are underway attempting to delay or prevent resistance to chemotherapy, including studies of drugs targeting ABCB1 and ABCG2 (29, 41).
The aim of this study was to determine the expression of ABCG2 and ABCB1 proteins in tumors from patients with PC, and to study the impact of these biomarkers on efficacy and outcome of treatment with GemNab.
2 Materials and methods
2.1 Patients
Through local registers, we identified 208 consecutive patients, more than 18 years of age, who initiated palliative treatment with GemNab for histologically confirmed, non-resectable PC from January 1st, 2011, to December 1st, 2019, at Aalborg University Hospital and Aarhus University Hospital, Denmark. Patients who had not received at least one CT scan after treatment initiation were excluded (N=40), to ensure that all patients were exposed to efficient doses of chemotherapy and could be evaluated for response. One patient was excluded due to missing clinical data. Finally, 28 cases were excluded due to insufficient archival tissue for immunohistochemistry (IHC). For the final study population of 140 patients, medical charts were reviewed for demographic, pathological and clinical data.
2.2 Treatment
GemNab was dosed and dose-adjusted according to manufactures prescription (42, 43). Actual dosing of Gem and Nab was registered in detail, and to assess the correlation between expression of ABC proteins in tumors and dosing of GemNab, delivered total dose (DTD), delivered dose intensity (DDI) and relative dose (RD) was calculated for each compound (41). Evaluation of treatment efficacy was performed every 8th week by CT-scans supplemented by clinical and biochemical evaluation.
2.3 Pathological assessment
Tumor presence was confirmed in archived formalin-fixed, paraffin-embedded (FFPE) biopsy and surgical specimens from both primary tumors and metastases when available. Only tissue obtained prior to chemotherapy with GemNab was considered. New 5-µm sections were cut and deparaffinization was performed for 12 min. at 72°C, followed by heat-induced target retrieval at 97°C for 56 min. for ABCG2, and 44 min. for ABCB1. Both antibodies were visualized using Ventana Optiview DAB detection kit.
ABCG2 was detected by IHC using the Ventana Benchmark Ultra platform (Ventana Medical Systems, Tucson, AZ) Ventana IHC-DAB program. A rabbit monoclonal anti-ABCG2 antibody (Cat No. ab207732, RabMab EPR20080, AbCam) was diluted to 1:300 and incubated in 32 min. Normal human liver served as the positive control, and human placenta as the negative control. ABCB1 was identified using a rabbit monoclonal anti-P-Glycoprotein/ABCB1 antibody (Cat No. Ab170904; RabMab EPR10365-57, Abcam) applied at a 1:100 dilution and incubated in 40 min.
ABCG2 and ABCB1 were independently evaluated by two pathologists, blinded to the treatment outcomes. Discrepancies were discussed to reach a consensus. In 123 patients one section was assessed, while two sections from different specimens were evaluated in 17 cases. For ABCG2, the scoring protocol was based on validated guidelines from Cederbye et al. (44). This approach specifically assesses membrane-associated staining, disregarding cytoplasmic staining unless accompanied by basolateral involvement. For ABCB1, no validated scoring system could be identified and the scoring system used was the semi-quantitative H-score (Histoscore) as previously described (45, 46). Representative sections with different scores for ABCG2 and the ABCB1 positive specimen are shown in Figure 1.
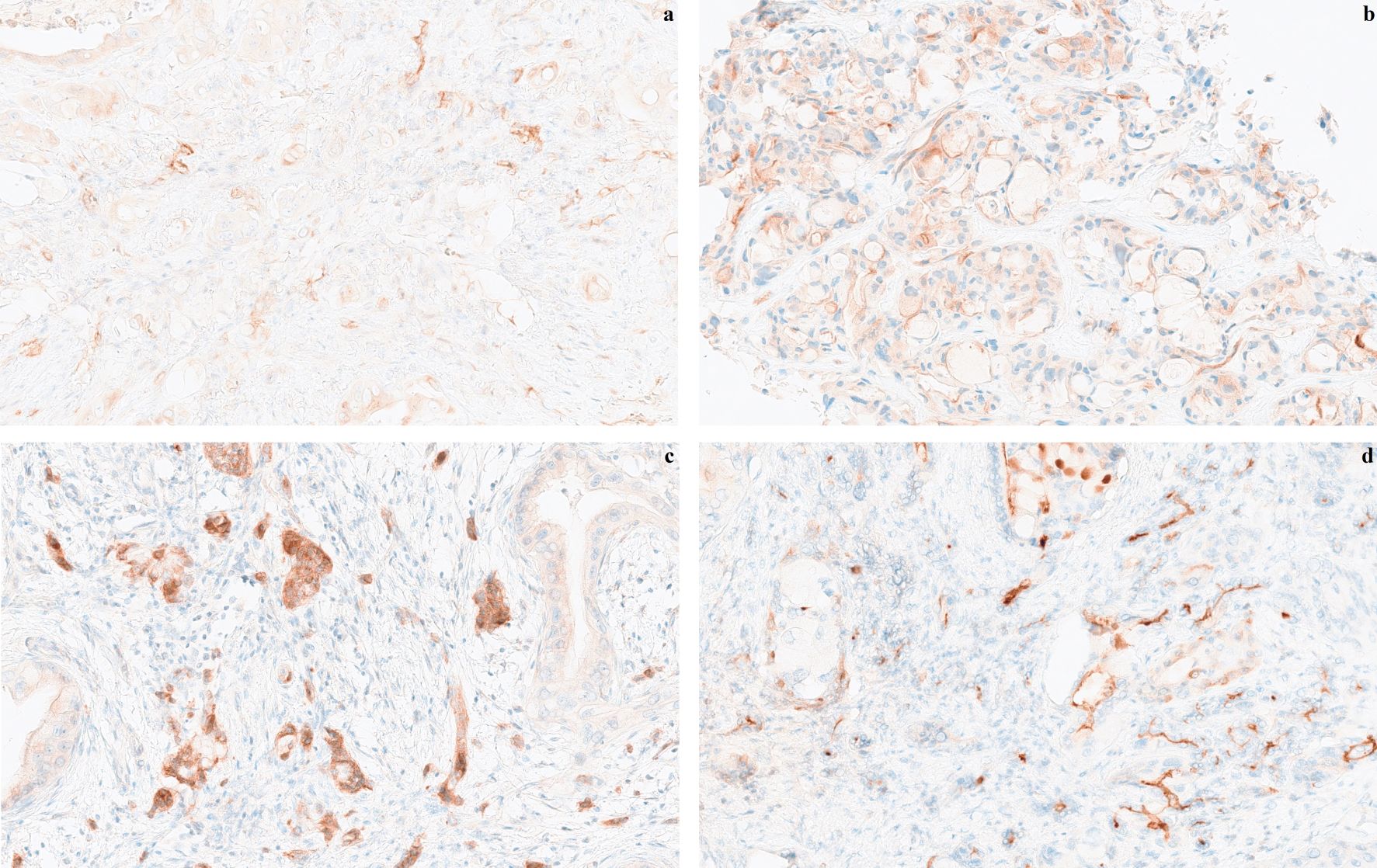
Figure 1. Representative histological sections of pancreatic cancers showing ABCG2 expression in tumors at 40x magnification, (a) score 1, (b) score 2, and (c) score 3, and (d) ABCB1 expression score 2 at 40x magnification. The scoring protocol for ABCG2 (ATP-binding cassette protein G2); was modified from Cederbye et al. (44): Score 0, basolateral membrane staining in less than 0-10% of tumor cells; score 1, weak basolateral membrane staining in at least 10% of tumor cells; score 2, weak to moderate basolateral membrane staining in at least 10% tumor cells; score 3, strong basolateral membrane staining in at least 10% of tumor cells. The scoring protocol for ABCB1 (ATP-binding casette protein B1) was based on H-score (45, 46).
2.4 Endpoints
The primary endpoint was progression free survival (PFS) according to tumor tissue expression of ABC proteins. Secondary endpoints were overall survival (OS) and response to treatment. Response was assessed by review of medical charts by RECIST version 1.1 (47) in 119 (83%) patients with evaluable and measurable disease at baseline.
2.5 Ethics
The study was approved by the Regional Committee on Health Research Ethics in Northern Denmark (N-20200049) and by the Department of Research and Statistics in Northern Denmark (ID 2020-120). Permission was given to waiver patients’ consent for the study, however, permit for genotyping of patients was not provided.
2.6 Statistical analysis
All statistical analyses were performed using R version 4.4.2 (48). Index date was the start date of treatment with GemNab. Baseline characteristics of ABCG2 positive vs negative patients were compared using t-test or Fishers exact test for continuous and categorical variables, respectively. Kaplan-Meier curves were plotted for both PFS and OS and differences in survival were tested using a log-rank test. Multivariate survival analysis was performed using a Cox proportional hazed model adjusted for age, gender, performance status, clinical stage, prior palliative chemotherapy, and prior (neo)adjuvant chemotherapy. Cox regression was applied in both the entire cohort and in subgroups of, respectively, chemo-naïve, and previously treated patients. Survival analysis was done using the R package survival v3.7–0 and visualized using the package survminer v0.5.0 (49, 50).
3 Results
The study population consisted of a total of 140 patients, 77 included at Aalborg University Hospital and 63 at Aarhus University Hospital. The follow-up was almost complete, as all except three patients died. As shown in Table 1, column 1, the mean age was 65 years, and the majority were males. 83% had distant metastatic disease. A total of 81% were in ECOG PS 0-1, and 60% of patients received treatment with GemNab as 1st. line of palliative chemotherapy. Forty patients had recurrent disease after pancreatic resection of which 35 (88% of those resected) had received neoadjuvant and/or adjuvant chemotherapy. A total of 46% of patients were naïve to any chemotherapy.
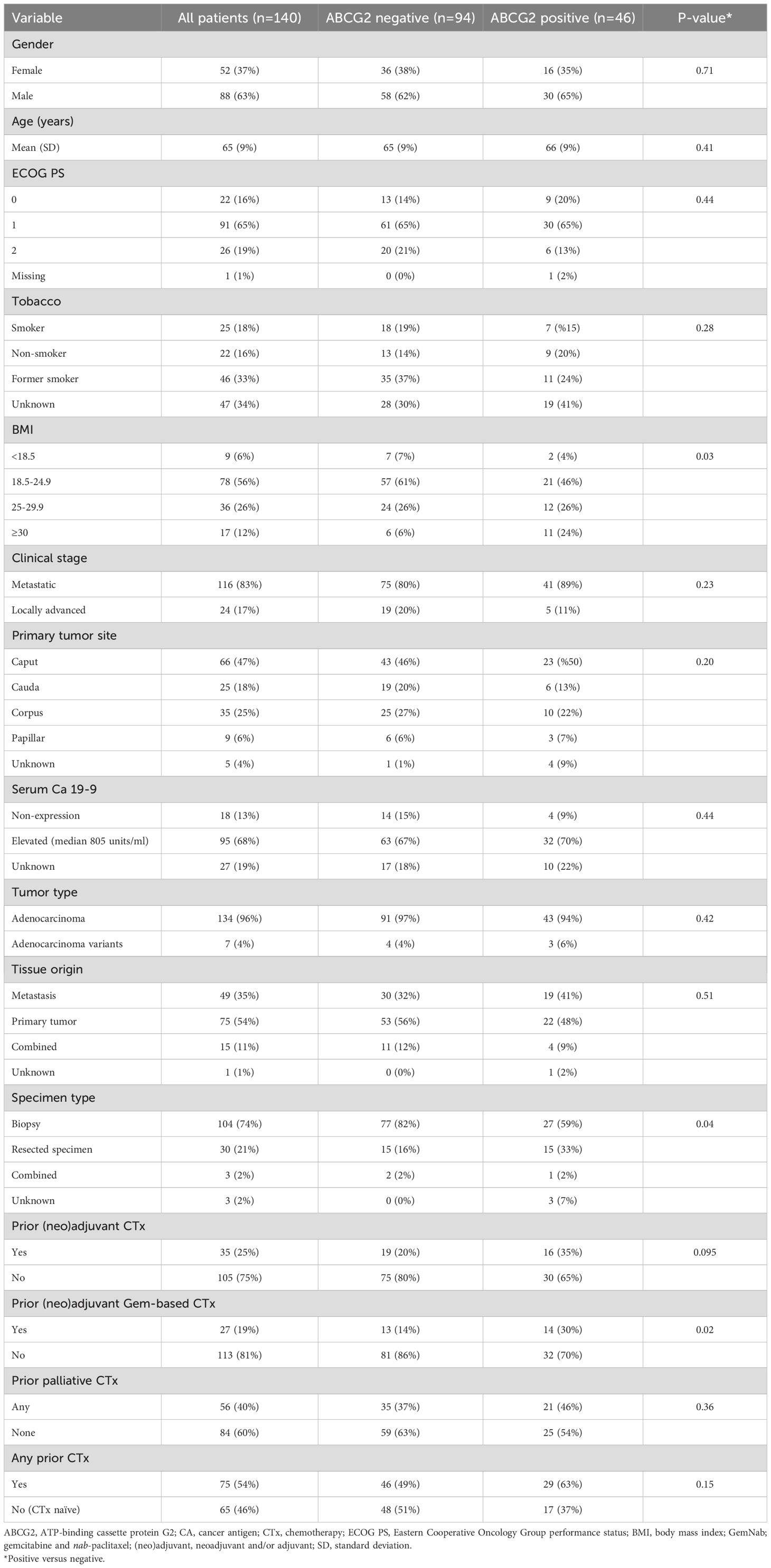
Table 1. Baseline characteristics of 140 patients with non-resectable pancreatic cancer treated with gemcitabine and nab-paclitaxel, distributed according to tumor expression of ABCG2.
Only one patients’ tumor (0.7%) expressed ABCB1. This tumor also scored positive for ABCG2. Positive and negative controls had expression of ABCB1 and ABCG2 as expected.
Forty-six patients (33%) had tumor expression of ABCG2, of which 22 had a score of 1, 19 of 2 and five of 3. Positive and negative controls had expression of ABCG2 as expected. The heterogeneity in scores obtained in different biopsies from the same patient was considerable. In 17 patients with more than one biopsy assessed, the same score (negative versus positive) was given to both of two available sections in eight cases, while in nine cases one section was scored negative and one positive.
Table 1, column 2 and 3, shows the distribution of ABCG2 expression (negative versus positive) according to clinical and pathological factors. Increasing BMI was significantly associated with expression of ABCG2 (P=0.03), and patients that previously received (neo)adjuvant chemotherapy had a trend toward a higher frequency of ABCG2 expression (P=0.095). This association was statistically significant when only considering gemcitabine-based (neo)adjuvant regimens (P=0.02). When stratifying patients according to ABCG2 scores 0, 1 and 2–3 similar results were obtained (Supplementary Table S1). ABCG2 expression was significantly more frequent when assessed in resected tumor specimens (50%) compared to biopsies (26%) (P=0.04), while no difference was found comparing frequencies of ABCG2 expression in primary tumors (29% positive) or metastases (39% positive) (P=0.51).
In 122 patients evaluable for response assessment by RECIST criteria, the overall response rate (ORR) was 17%. All responses were partial. ABCG2 expression had no impact on ORR; 14 (17%) of 82 patients with no expression had a response while seven (18%) of 40 patients with ABCG2 expression responded (P=0.84).
Although there was a trend toward improved PFS outcome for patients with tumors expressing ABCG2, the primary endpoint was not reached in univariate analysis of the full cohort (P=0.08), and ABCG2 expression was not correlated with OS (P=0.93). At multivariate analysis, however, expression of ABCG2 was significantly associated with a longer PFS (HR=0.64; 95%CI 0.43-0.94 (P=0.02)), while prior palliative chemotherapy or prior (neo)adjuvant chemotherapy was associated with shorter PFS (P=0.03 in both cases). A Forrest plot of results is shown in Figure 2. In multivariate analysis according to OS, metastatic disease was the only factor approaching statistical significance (P=0.06) (Supplementary Figure S2). A supplementary multivariate analysis of PFS and OS using three strata for ABCG expression showed similar results (Supplementary Figure S3).
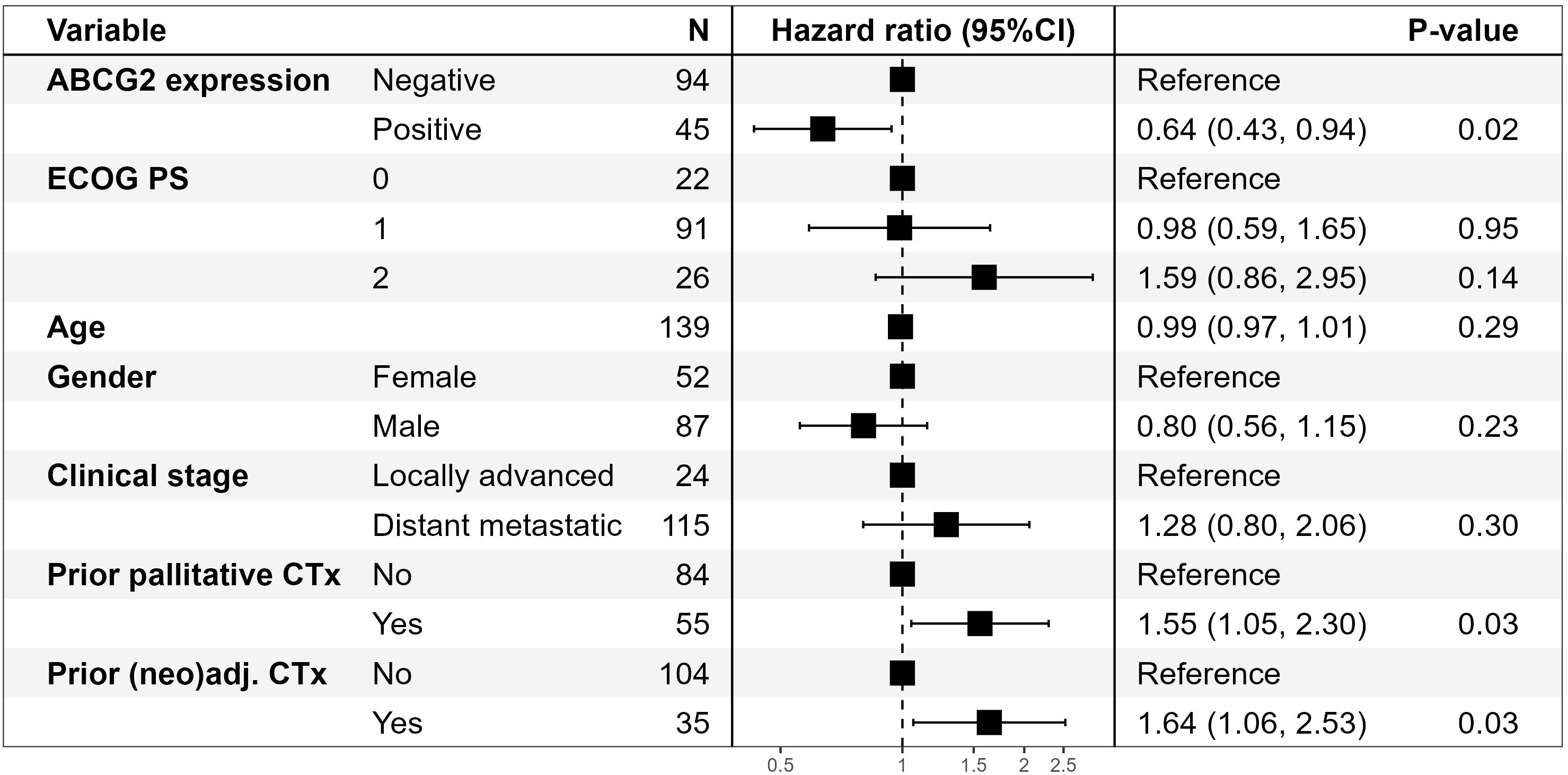
Figure 2. Forrest plot of results of multivariate analysis of PFS according to ABCG2 expression in 139* patients with non-resectable pancreatic cancer treated with gemcitabine and nab-paclitaxel. *One patient is excluded from the multivariate analysis due to missing performance status. ABCG2, ATP-binding cassette protein G2; CI, confidence interval; CTx, chemotherapy; ECOG PS, Eastern Cooperative Oncology Group performance status; (neo)adj., neoadjuvant and/or adjuvant.
As prior chemotherapy may impact ABCG2 expression in tissue, we made a stratified analysis of 65 patients that were naïve to chemotherapy and 75 patients that had previously been exposed to chemotherapy. ABCG2 expression tended to correlate with improved PFS of GemNab only in patients with prior exposure to chemotherapy (P=0.07), but not in chemo-naïve (P=0.20). In multivariate analysis of patients previously exposed to chemotherapy, the association of ABCG2 expression with longer PFS and OS of GemNab was nearly significant (P=0.06 in both cases). A Forrest plot of results according to PFS is shown in Figure 3. High ABCG2 expression (score 2-3) was significantly associated with longer OS (P=0.03) in patients previously exposed to chemotherapy (Supplementary Figure S3).
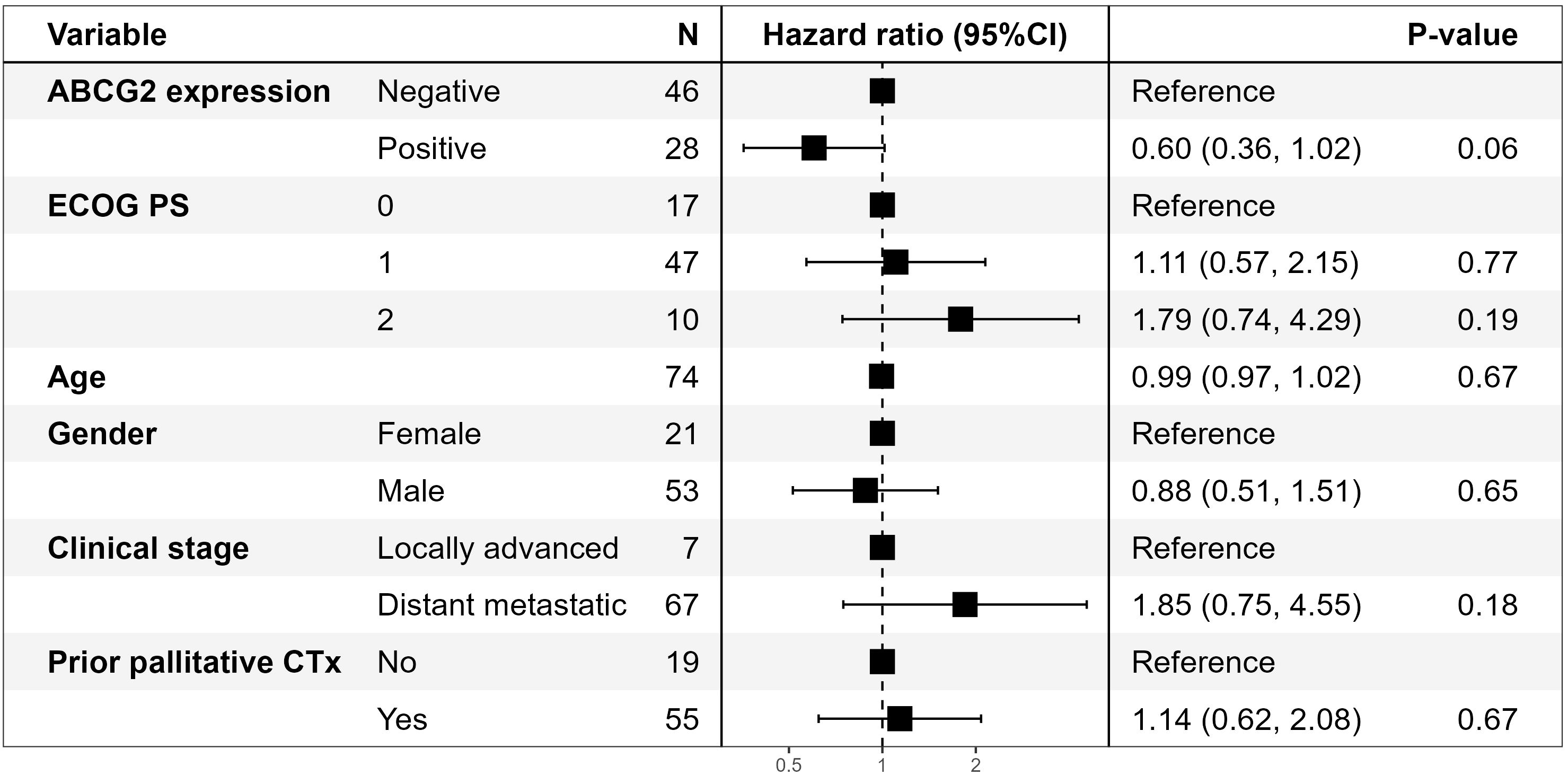
Figure 3. Forrest plot of results of multivariate analysis of PFS on treatment with gemcitabine and nab-paclitaxel according to ABCG2 expression in 74* patients with non-resectable pancreatic cancer previously treated with chemotherapy. *One patient is excluded from the multivariate analysis due to missing performance status.
The association of tumor ABCG2 expression (negative versus positive) with delivered treatment is shown in Table 2. The median relative dose (RD) of Gem was 86% but only 73% for Nab. The delivered total dose (DTD) was higher for both drugs, and the RD of Nab slightly lower in ABCG2 positive patients, however, none of the differences were statistically significant (P≥0.18).
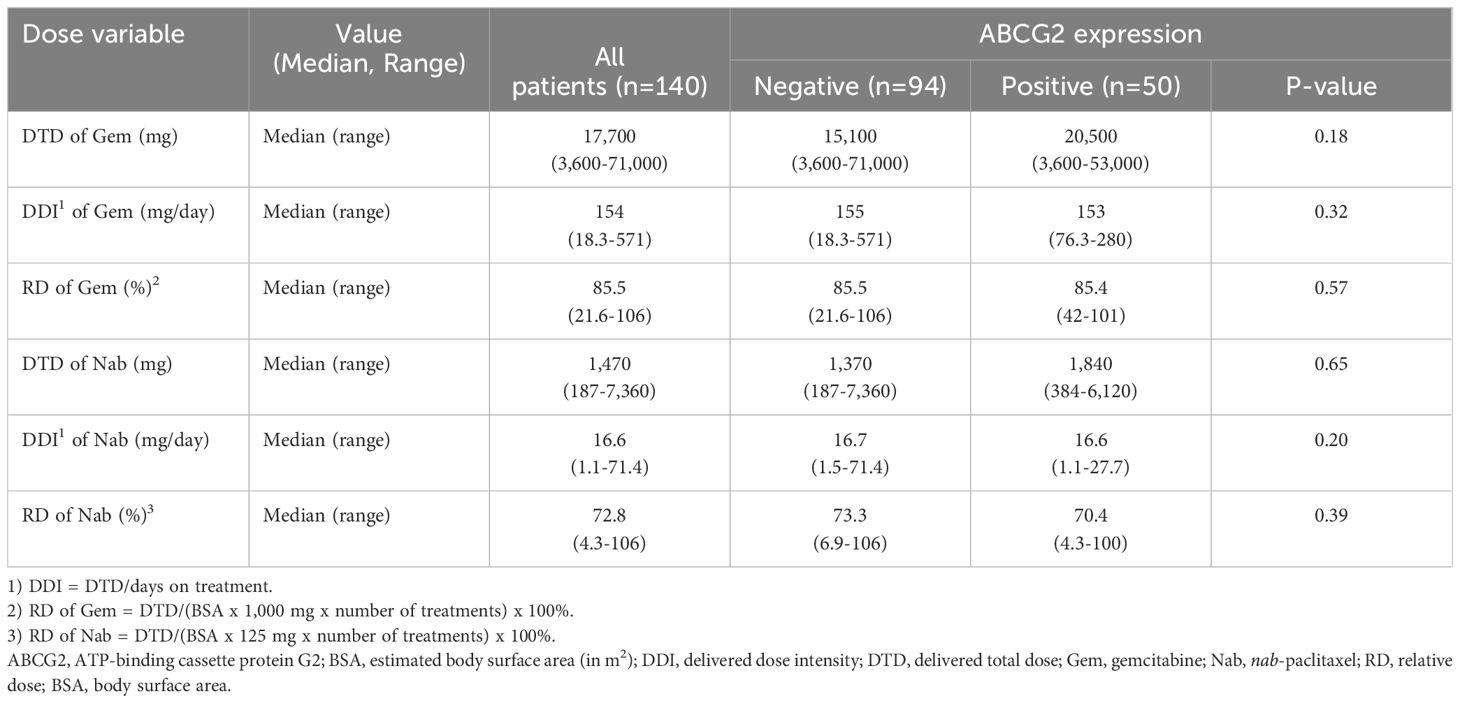
Table 2. Dose of chemotherapy according to ABCG2 expression in tumors of 140 patients with non-resectable pancreatic cancer treated with gemcitabine and nab-paclitaxel.
4 Discussion
In this retrospective cohort study of patients with non-resectable PC, we examined whether tumor-tissue expression of drug efflux pumps ABCB1 and ABCG2 was associated with outcome of chemotherapy with gemcitabine and nab-paclitaxel. PFS was the primary endpoint. In our cohort, ABCB1 was expressed in only one (0.7%) of 140 patients. The frequency of expression of ABCB1 protein or mRNA in PC has been reported very differently in the literature, ranging from just a few percent to 72.8%. The variation may be caused by differences in methodology, tumor heterogeneity, observer variability in assessment, and patient-related factors such as patients’ ethnicity or prior treatment with chemotherapy (30, 51). In contrast, ABCG2 was expressed in 33% and, although only nearly significant in univariate analysis of the full cohort, ABCG2 expression was of significant, independent predictive value according to PFS of GemNab in multivariate analysis. The predictive value, which also included an association with improved OS for patients with high expression levels of ABCG2 was, however, confined to patients who had been exposed to chemotherapy prior to treatment with GemNab.
Most often, ABCG2 expression in cancers has been associated with poor prognosis, although results are inconsistent (52, 53), and in some an inverse association was found (38, 54). In 60 patients with intrahepatic cholangiocarcinoma a longer survival time was observed in patients with ABCG2 expression in moderately to poorly differentiated tumors, but not in well differentiated (54), and in an analysis within the Cancer Genome Atlas (TCGA) program, high expression levels of ABCG2 were associated with improved prognosis in adrenocortical carcinoma, glioblastoma and renal clear cell carcinoma (38). In PC, only a few prior studies have examined the expression of ABCG2 and its impact on prognosis. In a study by Lee et al., ABCG2 expression was found in 73% of 67 samples analyzed and high expression levels were associated with short time to progression and poor overall survival (55). Yuan et al. examined ABCG2 expression in 106 chemo-naïve patients with PC, and in 103 specimens of peritumoral tissue, benign pancreatic lesions, or normal pancreatic tissue (56). ABCG2 was more frequently expressed (58%) in cancer tissue compared to other lesions, and its expression correlated with low differentiation, metastatic disease, and poor prognosis.
In contrast to the above, we found a lower fraction of tumors that expressed ABCG2, and expression did not correlate with patients’ survival in the full cohort, Methodological differences among studies associated with, e.g., antibody specificity, retrieval and staining may apply (57). Evaluation may be subject to inter-observer variation, although we used a validated protocol, and two observers determined the final score by mutual agreement. Diagnostic biopsies are small and targeted to non-necrotic areas and may be more peripheral. The tumor may be better oxygenated and may show less stromal context. Larger specimens may capture more of the tumor microenvironment, which is known to regulate transporter expression (15). We did not evaluate the stromal component and we did not assess the distribution of the expression in the specimens. The small biopsies may miss this, which could explain the lower positivity and unexpected association with outcome. Moreover, inter-lesional heterogeneity in scores was observed that may influence decision-making for possible treatment.
The finding that the fraction of ABCG2-positive was higher in resected specimens than in biopsies but similar in primary tumors and metastases, suggests that size of tumor area assessed may impact results. Representativeness of sections may be important as demonstrated, e.g., when assessing HER2 protein expression in gastric cancers (58). The ethnicity of patients could also influence results as our study included a population of Caucasians, whereas most prior studies were done in Asian populations. Ethnic genetic variations in ABC transporters, for instance ABCG2 421C>A polymorphism have been demonstrated with variant alleles up to 34% in Chinese populations compared to 11-12% in North American and European Caucasians (59, 60). Such genetic differences may influence transporter activity and chemotherapy disposition (60) (61). Interestingly, certain alleles have been associated with obesity (62), possibly explaining the significant association of ABCG2 expression with BMI found in the present study.
The association of ABCG2 expression in tumors with efficacy of chemotherapy has been demonstrated in vitro but is poorly investigated in vivo (32, 63). In three studies of advanced non-small-cell lung cancer patients treated with platinum-based chemotherapy, expression of ABCG2 was not associated with ORR or PFS in two (64, 65), while in one study, ABCG2 expression was associated with short PFS and a numerically lower ORR (66). In PC, a prior study showed an association between high ABCG2 expression and early recurrence of patients treated with adjuvant gemcitabine-based chemotherapy but response to chemotherapy could not be assessed (55). A study published only in abstract form using RNA profiling of circulating tumor and invasive cells in 33 patients suggested that high ABCG2 gene expression was associated with shorter PFS on treatment with GemNab (67). In the current study, we found no indications of upregulated ABCG2 being associated with de novo chemo-resistance, response rate or poor outcome of GemNab. On the contrary, ABCG2 expression in samples from patients that had received chemotherapy in a (neo)adjuvant or first-line palliative setting, but prior to treatment with GemNab, was associated with an improved efficacy of GemNab as assessed by PFS. From this we hypothesize that tumors, where ABCG2 is upregulated during prior chemotherapy, are more sensitive to GemNab. Although the interpretation of this unexpected result is speculative and confirmatory studies are needed, ABCG2 expression could therefore be a biomarker for personalized selection of patients to later-line treatment with GemNab. This association may also have implications for clinical trials investigating ABCG2-inhibitors together with chemotherapy (41).
The selection of patients with best chance of response to GemNab is particularly important in those pretreated with chemotherapy as this population may benefit less. Although efficacy of GemNab in patients previously treated with (neo)adjuvant chemotherapy is poorly investigated and patients included in the pivotal randomized trial of GemNab were exclusively chemo-naïve (8), shorter PFS of GemNab in the 2nd line, palliative setting has been shown in several reports (68, 69). In the current study, ABCG2 expression was not predictive of PFS of GemNab in chemo-naïve patients and therefore other mechanisms of early resistance as recently reviewed by Espona-Fiedler et al. (70), must be in play.
ABCG2 expression was more frequent in patients previously exposed to Gem in the curative setting in accordance with preclinical studies showing that Gem can induce upregulation of ABCG2 in PC cells (39). Finally, we found no significant association between ABCG2 expression and chemotherapy dosing, indicating that tolerability of both Gem and Nab was not associated with ABCG2 expression. Further evaluation of these aspects, including assessment of whether a potential predictive value is associated with Gem, Nab or both drugs, will be investigated in an ongoing randomized study (71).
Main limitations of this study are its retrospective design and lack of sufficient tissue in 17% of patients. Although all patients received GemNab in a palliative setting, the cohort was heterogeneous with respect to prior surgical and oncological treatment. This, however, allowed us to analyze the impact of prior chemotherapy on results. We were unable to assess effects of treatment on biomarker expression at the individual patient level as only 17 patients had paired biopsies taken before and after treatment. Further, we had no information on allele frequencies that may explain different outcomes in different populations. ABCG2 expression has been shown to correlate with epithelial-mesenchymal transition markers, which are known to interact with drug efflux pathways (23), and further studies are warranted to elucidate this aspect. We chose to exclude individuals not reaching their first evaluation scan (19%) to ensure that patients were exposed to reasonable doses of chemotherapy and could be evaluated for response. Although this introduces immortal time bias and bias toward more responsive and fitter patients being selected, our primary focus was to assess associations of biomarkers with respect to efficacy of chemotherapy, not the prognostic value. At the treating departments, folfirinox was the preferred 1st line palliative treatment option for patients in good general condition (72) and, hence, the population was selected toward poor prognostic factors and comorbidities. Finally, methodological issues related to ABCG2 scoring as outlined above are poorly investigated and should be addressed, if ABCG2 expression is to be used as a clinical biomarker. Digital image analysis and quantitative IHC approaches are emerging and could be helpful in quantifying ABCG2 expression.
In conclusion, ABCG2 was expressed in approximately one third of tumors from patients treated with GemNab. Among patients previously exposed to chemotherapy, ABCG2 expression showed a potential association with improved efficacy of GemNab. While these results are intriguing, they contrast with prior reports linking ABCG2 with drug resistance, and the biological rationale for this inverse association remains unclear. Thus, these findings should be considered hypothesis-generating, and further studies are warranted to explore possible mechanisms—such as adaptive stress responses, clonal selection, or microenvironmental factors—that may contribute to this observation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The requirement of ethical approval was waived by Forskning, Uddannelse og Innovation, Aalborg University Hospital, Denmark for the studies on humans because the main part of the patients were dead. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Tissue obtained from biopsies and stored at pathological departments.
Author contributions
SS: Data curation, Investigation, Project administration, Writing – original draft, Writing – review & editing. MN: Methodology, Writing – review & editing. ME: Methodology, Writing – review & editing. JS: Conceptualization, Funding acquisition, Project administration, Supervision, Writing – review & editing. RB: Data curation, Formal Analysis, Writing – review & editing. BW: Data curation, Writing – review & editing. AM: Data curation, Supervision, Writing – review & editing. ML: Conceptualization, Data curation, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Scandion Oncology A/S supported the study by an unrestricted research grant to the Department of Oncology, Aalborg University Hospital and Department of Pathology, Aarhus University Hospital; additional funding was provided by Aalborg University Hospital and Brogaards Foundation. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
The templates for the standard operating procedure (SOP) for detection of ABCB1 and ABCG2 were developed by Bioneer A/S, Hørsholm, Denmark, in collaboration with Scandion Oncology, Copenhagen, Denmark.
Conflict of interest
ML received a research grant from Scandion Oncology A/S. JS is a co-founder, shareholder and CSO of Scandion Oncology A/S. MN was consultant for Scandion Oncology A/S. Furthermore, participated in company-sponsored course provided by Incyte.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1558184/full#supplementary-material
References
1. World Health Organization International Agency for Research on Cancer. GLOBOCAN 2020: pancreatic cancer fact sheet. Lyon, France: International Agency for Research on Cancer (2020) p. 3–4. Available at: https://gco.iarc.fr/today/fact-sheets-cancers (Accessed December 2, 2022).
2. Zeng S, Pöttler M, Lan B, Grützmann R, Pilarsky C, and Yang H. Chemoresistance in pancreatic cancer. Int J Mol Sci. (2019) 20(18):4504. doi: 10.3390/ijms20184504
3. Sarvepalli D, Rashid MU, Rahman AU, Ullah W, Hussain I, Hasan B, et al. Gemcitabine: A review of chemoresistance in pancreatic cancer. Crit Rev Oncog. (2019) 24:199–212. doi: 10.4324/9781315667737-27
4. Du J, Gu J, and Li J. Mechanisms of drug resistance of pancreatic ductal adenocarcinoma at different levels. Biosci Rep. (2020) 40(7):BSR20200401. doi: 10.1042/BSR20200401
5. Conroy T, Pfeiffer P, Vilgrain V, Lamarca A, Seufferlein T, O’Reilly EM, et al. Pancreatic cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up☆. Ann Oncol. (2023) 34:987–1002. doi: 10.1016/j.annonc.2023.08.009
6. Burris HA, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first- line therapy for patients with advanced pancreas cancer: A randomized trial. J Clin Oncol. (1997) 15:2403–13. doi: 10.1200/JCO.1997.15.6.2403
7. Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. (2011) 364:1817–25. doi: 10.1056/NEJMoa1011923
8. Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N Engl J Med. (2015) 369:1691–703. doi: 10.1056/NEJMoa1304369
9. Ducreux M, Cuhna AS, Caramella C, Hollebecque A, Burtin P, Goéré D, et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2015) 26:v56–68. doi: 10.1093/annonc/mdv295
10. Wainberg ZA, Melisi D, Macarulla T, Pazo-Cid R, Chandana SR, de la Fouchardiere C, et al. NAPOLI-3: A randomized, open-label phase 3 study of liposomal irinotecan + 5-fluorouracil/leucovorin + oxaliplatin (NALIRIFOX) versus nab-paclitaxel + gemcitabine in treatment-naïve patients with metastatic pancreatic ductal adenocarcinoma (mPDAC). J Clin Oncol. (2023) 41:LBA661–1. doi: 10.1200/JCO.2023.41.4_suppl.LBA661
11. Wainberg ZA, Melisi D, Macarulla T, Pazo Cid R, Chandana SR, de la Fouchardière C, et al. NALIRIFOX versus nab-paclitaxel and gemcitabine in treatment-naive patients with metastatic pancreatic ductal adenocarcinoma (NAPOLI 3): a randomised, open-label, phase 3 trial. Lancet. (2023) 402:1272–81. doi: 10.1016/S0140-6736(23)01366-1
12. Choy ATF, Carnevale I, Coppola S, Meijer LL, Kazemier G, Zaura E, et al. The microbiome of pancreatic cancer: from molecular diagnostics to new therapeutic approaches to overcome chemoresistance caused by metabolic inactivation of gemcitabine. Expert Rev Mol Diagn. (2018) 18:1005–9. doi: 10.1080/14737159.2018.1544495
13. Güngör C, Hofmann BT, Wolters-Eisfeld G, and Bockhorn M. Pancreatic cancer. Br J Pharmacol. (2014) 171:849–58. doi: 10.1111/bph.2014.171.issue-4
14. Kavallaris M. Microtubules and resistance to tubulin-binding agents. Nat Rev Cancer. (2010) 10:194–204. doi: 10.1038/nrc2803
15. Adamska A, Elaskalani O, Emmanouilidi A, Kim M, Abdol Razak NB, Metharom P, et al. Molecular and cellular mechanisms of chemoresistance in pancreatic cancer. Adv Biol Regul. (2018) 68:77–87. doi: 10.1016/j.jbior.2017.11.007
16. Lemstrova R, Melichar B, and Mohelnikova-Duchonova B. Therapeutic potential of taxanes in the treatment of metastatic pancreatic cancer. Cancer Chemother Pharmacol. (2016) 78:1101–11. doi: 10.1007/s00280-016-3058-y
17. Kato A, Naitoh I, Naiki-Ito A, Hayashi K, Okumura F, Fujita Y, et al. Class III β-tubulin expression is of value in selecting nab -paclitaxel and gemcitabine as first-line therapy in unresectable pancreatic cancer. Pancreas. (2022) 51:372–9. doi: 10.1097/MPA.0000000000002032
18. McCarroll JA, Sharbeen G, Liu J, Youkhana J, Goldstein D, McCarthy N, et al. βIII-Tubulin: A novel mediator of chemoresistance and metastases in pancreatic cancer. Oncotarget. (2015) 6:2235–49. doi: 10.18632/oncotarget.2946
19. Das T, Anand U, Pandey SK, Ashby CR, Assaraf YG, Chen ZS, et al. Therapeutic strategies to overcome taxane resistance in cancer. Drug Resist Update. (2021) 55:100754. doi: 10.1016/j.drup.2021.100754
20. Němcová-Fürstová V, Kopperová D, Balušíková K, Ehrlichová M, Brynychová V, Václavíková R, et al. Characterization of acquired paclitaxel resistance of breast cancer cells and involvement of ABC transporters. Toxicol Appl Pharmacol. (2016) 310:215–28. doi: 10.1016/j.taap.2016.09.020
21. Sarvepalli D, Rashid MU, Rahman AU, Clinic C, Ullah W, Hussain I, Hasan B, Jehanzeb S, Khan AK, Jain AG, Khetpal N, and Ahmad S. Gemcitabine: A review of chemoresistance in pancreatic cancer. Crit Rev Oncog. (2019). 24(2)199–212. doi: 10.1615/CritRevOncog.2019031641
22. Jia Y and Xie J. Promising molecular mechanisms responsible for gemcitabine resistance in cancer. Genes Dis. (2015) 2:299–306. doi: 10.1016/j.gendis.2015.07.003
23. Amrutkar M and Gladhaug IP. Pancreatic cancer chemoresistance to gemcitabine. Cancers (Basel). (2017) 9:1–23. doi: 10.3390/cancers9110157
24. Adamska A and Falasca M. ATP-binding cassette transporters in progression and clinical outcome of pancreatic cancer: What is the way forward? World J Gastroenterol. (2018) 24:3222–36. doi: 10.3748/wjg.v24.i29.3222
25. Pasello M, Giudice AM, and Scotlandi K. The ABC subfamily A transporters: Multifaceted players with incipient potentialities in cancer. Semin Cancer Biol. (2020) 60:57–71. doi: 10.1016/j.semcancer.2019.10.004
26. Fletcher JI, Williams RT, Henderson MJ, Norris MD, and Haber M. ABC transporters as mediators of drug resistance and contributors to cancer cell biology. Drug Resist Updat. (2016) 26:1–9. doi: 10.1016/j.drup.2016.03.001
27. Sun S, Cai J, Yang Q, Zhu Y, Zhao S, and Wang Z. Prognostic value and implication for chemotherapy treatment of ABCB1 in epithelial ovarian cancer: A meta-analysis. PloS One. (2016) 11(11):e0166058. doi: 10.1371/journal.pone.0166058
28. Sun YL, Patel A, Kumar P, and Chen ZS. Role of ABC transporters in cancer chemotherapy. Chin J Cancer. (2012) 31:51–7. doi: 10.5732/cjc.011.10466
29. Xiao H, Zheng Y, Ma L, Tian L, and Sun Q. Clinically-relevant ABC transporter for anti-cancer drug resistance. Front Pharmacol. (2021) 12:1–17. doi: 10.3389/fphar.2021.648407
30. The Human Protein Atlas. Expression of ABCB1 in cancer - Summary. Stockholm, Sweden: The Human Protein Atlas (2024). Available at: https://v15.proteinatlas.org/ENSG00000085563-ABCB1/cancer (Accessed December 12, 2024).
31. Choi CH. ABC transporters as multidrug resistance mechanisms and the development of chemosensitizers for their reversal. Cancer Cell Int. (2005) 5:1–13. doi: 10.1186/1475-2867-5-30
32. El-Ashmawy NE, Al-Ashmawy GM, Hamada OB, and Khedr NF. The role of ABCG2 in health and disease: Linking cancer therapy resistance and other disorders. Life Sci. (2025) 360:123245. doi: 10.1016/j.lfs.2024.123245
33. Mohelnikova-Duchonova B, Brynychova V, Oliverius M, Honsova E, Kala Z, Muckova K, et al. Differences in transcript levels of ABC transporters between pancreatic adenocarcinoma and nonneoplastic tissues. Pancreas. (2013) 42:707–16. doi: 10.1097/MPA.0b013e318279b861
34. Yao L, Gu J, Mao Y, Zhang X, Wang X, Jin C, et al. Dynamic quantitative detection of ABC transporter family promoter methylation by MS-HRM for predicting MDR in pancreatic cancer. Oncol Lett. (2018) 15:5602–10. doi: 10.3892/ol.2018.8041
35. Zhang Z, Gao S, Xu Y, and Zhao C. Regulation of ABCG2 expression by Wnt5a through FZD7 in human pancreatic cancer cells. Mol Med Rep. (2021) 23:1–11. doi: 10.3892/mmr.2020.11690
36. DRUGBANK. BRCP/ABCG2 substrates . Available online at: https://go.drugbank.com/categories/DBCAT002663 (Accessed September 4, 2024).
37. Leslie EM, Deeley RG, and Cole SPC. Multidrug resistance proteins: Role of P-glycoprotein, MRP1, MRP2, and BCRP (ABCG2) in tissue defense. Toxicol Appl Pharmacol. (2005) 204:216–37. doi: 10.1016/j.taap.2004.10.012
38. Lyu C, Wang L, Stadlbauer B, Buchner A, and Pohla H. A pan-cancer landscape of ABCG2 across human cancers: friend or foe? Int J Mol Sci. (2022) 23(24):15955. doi: 10.3390/ijms232415955
39. Sun Y, Gu M, Zhu L, Liu J, Xiong Y, Wei Y, et al. Gemcitabine upregulates ABCG2/BCRP and modulates the intracellular pharmacokinetic profiles of bioluminescence in pancreatic cancer cells. Anticancer Drugs. (2016) 27:183–91. doi: 10.1097/CAD.0000000000000315
40. Kim KP, Ahn JH, Kim SB, Jung KH, Yoon DH, Lee JS, et al. Prospective evaluation of the drug-metabolizing enzyme polymorphisms and toxicity profile of docetaxel in Korean patients with operable lymph node-positive breast cancer receiving adjuvant chemotherapy. Cancer Chemother Pharmacol. (2012) 69:1221–7. doi: 10.1007/s00280-011-1816-4
41. Ladekarl M, Shim S, Ettrich TJ, Kestler A, Pfeiffer P, Tarpgaard LS, et al. 1641P ABCG transporter and SRPK1 kinase inhibition of chemotherapy resistance: A phase Ib clinical trial of safety and maximum tolerated dose for SCO-101 in combination with gemcitabine and nab-paclitaxel in inoperable pancreatic cancer. Ann Oncol. (2023) 34:S907. doi: 10.1016/j.annonc.2023.09.2590
42. FDA Label. GEMCITABINE injection, for intravenous use Initial U.S. Approval: 1996 (2018). Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/209604s003lbl.pdf (Accessed November 7, 2024).
43. Bristol Myers Squibb. Abaxane for injectable suspension (2022). Available online at: https://www.abraxane.com/nsclc/abraxane-and-advanced-non-small-cell-lung-cancer (Accessed November 7, 2024).
44. Cederbye CN, Palshof JA, Hansen TP, Duun-Henriksen AK, Linnemann D, Stenvang J, et al. Antibody validation and scoring guidelines for ABCG2 immunohistochemical staining in formalin-fixed paraffin-embedded colon cancer tissue. Sci Rep. (2016) 6:1–16. doi: 10.1038/srep26997
45. McCarty KS, Szabo E, Flowers JL, Cox EB, Leight GS, Miller L, et al. Use of a monoclonal anti-estrogen receptor antibody in the immunohistochemical evaluation of human tumors. Cancer Res. (1986) 46(8 Suppl):4244s–4248s.
46. Nedeljković M, Tanić N, Prvanović M, Milovanović Z, and Tanić N. Friend or foe: ABCG2, ABCC1 and ABCB1 expression in triple-negative breast cancer. Breast Cancer. (2021) 28:727–36. doi: 10.1007/s12282-020-01210-z
47. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer. (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026
48. R Studio Team. A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2021). Available at: http://www.r-project.org (Accessed January 4, 2025).
49. Therneau TM. A Package for Survival Analysis in R-survival-package. R package version 3.7-0 (2024). Available online at: https://cran.r-project.org/package=survival (Accessed December 11, 2024).
50. Kassambara A, Kosinski M, Biecek P, and Fabian S. Package “survminer” (2024). Available online at: https://cran.r-project.org/web/packages/survminer/survminer.pdf (Accessed December 11, 2024).
51. Suwa H, Ohshio G, Arao S, Imamura T, Yamaki K, Manabe T, et al. Immunohistochemical localization of P-glycoprotein and expression of the multidrug resistance-1 gene in human pancreatic cancer: Relevance to indicator of better prognosis. Japanese J Cancer Res. (1996) 87:641–9. doi: 10.1111/j.1349-7006.1996.tb00271.x
52. Sałagacka-Kubiak A, Zawada D, Saed L, Kordek R, Jeleń A, and Balcerczak E. ABCG2 gene and ABCG2 protein expression in colorectal cancer—In silico and wet analysis. Int J Mol Sci. (2023) 24(13):10539. doi: 10.3389/fgene.2021.709887
53. Marques AVL, Ruginsk BE, Prado L de O, de Lima DE, Daniel IW, Moure VR, et al. The association of ABC proteins with multidrug resistance in cancer. Biochim Biophys Acta - Mol Cell Res. (2025) 1872(2):119878. doi: 10.1016/j.bbamcr.2024.119878
54. Larbcharoensub N, Sornmayura P, Sirachainan E, Wilasrusmee C, Wanmoung H, and Janvilisri T. Prognostic value of ABCG2 in moderately and poorly differentiated intrahepatic cholangiocarcinoma. Histopathology. (2011) 59:235–46. doi: 10.1111/j.1365-2559.2011.03935.x
55. Marin JJG, Monte MJ, Macias RIR, Romero MR, Herraez E, Asensio M, et al. Expression of chemoresistance-associated ABC proteins in hepatobiliary, pancreatic and gastrointestinal cancers. Cancers (Basel). (2022) 14:1–25. doi: 10.3390/cancers14143524
56. Yuan Y, Yang Z, Miao X, Li D, Liu Z, and Zou Q. The clinical significance of FRAT1 and ABCG2 expression in pancreatic ductal adenocarcinoma. Tumor Biol. (2015) 36:9961–8. doi: 10.1007/s13277-015-3752-0
57. Walker RA. Quantification of immunohistochemistry - Issues concerning methods, utility and semiquantitative assessment I. Histopathology. (2006) 49:406–10. doi: 10.1111/j.1365-2559.2006.02514.x
58. Fusco N, Rocco EG, Del Conte C, Pellegrini C, Bulfamante G, Di Nuovo F, et al. HER2 in gastric cancer: A digital image analysis in pre-neoplastic, primary and metastatic lesions. Mod Pathol. (2013) 26:816–24. doi: 10.1038/modpathol.2012.228
59. De Jong FA, Marsh S, Mathijssen RHJ, King C, Verweij J, Sparreboom A, et al. ABCG2 pharmacogenetics: Ethnic differences in allele frequency and assessment of influence on irinotecan disposition. Clin Cancer Res. (2004) 10:5889–94. doi: 10.1158/1078-0432.CCR-04-0144
60. Xiao Q, Zhou Y, and Lauschke VM. Ethnogeographic and inter-individual variability of human ABC transporters. Hum Genet. (2020) 139:623–46. doi: 10.1007/s00439-020-02150-6
61. Xiao Q, Zhou Y, Winter S, Büttner F, Schaeffeler E, Schwab M, et al. Germline variant burden in multidrug resistance transporters is a therapy-specific predictor of survival in breast cancer patients. Int J Cancer. (2020) 146:2475–87. doi: 10.1002/ijc.32898
62. Chen YJ, Chen IC, Lin HJ, Lin YC, Chang JC, Chen YM, et al. Association of ABCG2 rs2231142 allele and BMI with hyperuricemia in an east asian population. Front Genet. (2021) 12. doi: 10.3389/fgene.2021.709887
63. Chen L, Manautou JE, Rasmussen TP, and Zhong X. Development of precision medicine approaches based on inter-individual variability of BCRP/ABCG2. Acta Pharm Sin B. (2019) 9:659–74. doi: 10.1016/j.apsb.2019.01.007
64. Li J, Li ZN, Du YJ, Li XQ, Bao QL, and Chen P. Expression of MRP1, BCRP, LRP, and ERCC1 in advanced non-small-cell lung cancer: Correlation with response to chemotherapy and survival. Clin Lung Cancer. (2009) 10:414–21. doi: 10.3816/CLC.2009.n.078
65. Ota S, Ishii G, Goto K, Kubota K, Kim YH, Kojika M, et al. Immunohistochemical expression of BCRP and ERCC1 in biopsy specimen predicts survival in advanced non-small-cell lung cancer treated with cisplatin-based chemotherapy. Lung Cancer. (2009) 64:98–104. doi: 10.1016/j.lungcan.2008.07.014
66. Yoh K, Ishii G, Yokose T, Minegishi Y, Tsuta K, Goto K, et al. Breast cancer resistance protein impacts clinical outcome in platinum-based chemotherapy for advanced non-small cell lung cancer. Clin Cancer Res. (2004) 10:1691–7. doi: 10.1158/1078-0432.CCR-0937-3
67. Yu KH, Ricigliano M, O’Reilly EM, Lowery MA, Cooper B, and Covington CM. Breast cancer resistance protein (ABCG2) as a potential biomarker for gemcitabine and nab-paclitaxel sensitivity. J Clin Oncol. (2016) 34:4129–9. doi: 10.1200/JCO.2016.34.15_suppl.4129
68. Sezgin Y, Karhan O, Aldemir MN, Ürün M, Erçek BM, Urakcı Z, Arvas H, et al. 1523P Efficacy of gemcitabine plus nab-paclitaxel in second-line treatment of metastatic pancreatic cancer. Ann Oncol. (2025) 35:S930. doi: 10.1038/s41598-025-96157-6
69. Zaibet S, Hautefeuille V, Auclin E, Lièvre A, Tougeron D, Sarabi M, et al. Gemcitabine + Nab-paclitaxel or Gemcitabine alone after FOLFIRINOX failure in patients with metastatic pancreatic adenocarcinoma: a real-world AGEO study. Br J Cancer. (2022) 126:1394–400. doi: 10.1038/s41416-022-01713-w
70. Espona-Fiedler M, Patthey C, Lindblad S, Sarró I, and Öhlund D. Overcoming therapy resistance in pancreatic cancer: New insights and future directions. Biochem Pharmacol. (2024) 229:116492. doi: 10.1016/j.bcp.2024.116492
71. Rasmussen LS, Winther SB, Chen IM, Weber B, Ventzel L, Liposits G, et al. A randomized phase II study of full dose gemcitabine versus reduced dose gemcitabine and nab-paclitaxel in vulnerable patients with non-resectable pancreatic cancer (DPCG-01). BMC Cancer. (2023) 23:552. doi: 10.1186/s12885-023-11035-6
72. Ladekarl M, Rasmussen LS, Kirkegård J, Chen I, Pfeiffer P, Weber B, et al. Disparity in use of modern combination chemotherapy associated with facility type influences survival of 2655 patients with advanced pancreatic cancer. Acta Oncol (Madr). (2022) 61:277–85. doi: 10.1080/0284186X.2021.2012252
Keywords: gemcitabine, nab-paclitaxel, ATP-binding cassette protein, ABCG2, BRCP, chemotherapy resistance, progression-free survival, immunohistochemistry
Citation: Shim S, Nielsen MB, Eld M, Stenvang J, Brøndum RF, Weber B, Motavaf AK and Ladekarl M (2025) ABCG2 protein expression in tumors of patients with non-resectable pancreatic cancer treated with gemcitabine and nab-paclitaxel. Front. Oncol. 15:1558184. doi: 10.3389/fonc.2025.1558184
Received: 09 January 2025; Accepted: 21 May 2025;
Published: 06 June 2025.
Edited by:
Milica Pešić, University of Belgrade, SerbiaCopyright © 2025 Shim, Nielsen, Eld, Stenvang, Brøndum, Weber, Motavaf and Ladekarl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susy Shim, cy5zaGltQHJuLmRr