 YongXiang Xie1
YongXiang Xie1 DongMei Wang
DongMei Wang- 1Department of Endoscopy Center, Public Health Clinical Center of Chengdu, Chengdu, Sichuan, China
- 2Science and Education Division, Public Health Clinical Center of Chengdu, Chengdu, Sichuan, China
The three patients with AIDS were all male, aged between 56 and 67 years. One also had liver cirrhosis. They presented to the Chengdu Public Health Clinical Medical Center with a history of several months of blood in the stool. Colonoscopy revealed large pedunculated polyps in the sigmoid colon, with the largest measuring 5 cm and the smallest 3.5 cm. The polyps nearly completely obstructed the lumen. The long, thick stems were freely mobile within the narrow lumen, making it difficult to capture sufficient tissue with the inner ring of the forceps. The entire colon was examined with the aid of a transparent cap. Once the polyp was located, fecal water and residue surrounding it were removed. The polyp surface was then examined using white light and narrow-spectrum light to assess its structure. A biopsy was performed when cancer was suspected. During the procedure, we innovatively used a Harmony Clamp (ROCC-D-26-195; Micro Tech, Nanjing, China) to assist the nylon rope (HX-400U-30; Olympus, Tokyo, Japan) in pre-treating the pedicle root. First, the nylon rope was preloaded into the forceps channel of the enteroscope (EC-550L; SonoScape, Shenzhen, China), and the pedicle was ligated. When the polyp head turned deep purple and the stalk became pale, it confirmed that the blood supply to the mass had been fully blocked. A Harmony Clamp was then inserted into the intestinal cavity through the forceps channel, and the nylon rope was secured around the base of the polyp. The electric snare (VDK-SD-23-230-25-A1; Vedkang, Jiangsu, China) was placed between the clamp and the polyp, at least 0.5 cm from the mass, followed by high-frequency electroresection. Postoperatively, the wound appeared white with no bleeding or perforation. The operation time for all three patients was between 5 and 7 minutes, and there were no complications such as bleeding, perforation, or abdominal pain during or after the procedure. Follow-up colonoscopy 1 to 3 months later showed scar formation in the surgical area and no recurrence. Pathological analysis revealed that two cases were tubular-villous adenomas, and one case was a tubular-villous adenoma with focal high-grade intraepithelial neoplasia and mucosal carcinoma, with negative horizontal and vertical margins.
1 Introduction
In contemporary clinical practice, a variety of endoscopic resection techniques for thick pedunculated polyps have been developed. These methods include traditional endoscopic mucosal resection (EMR), titanium clip occlusion of the root, and nylon rope ligation of the root. Thick pedunculated polyps often have relatively large blood vessels (1). Colon polyps can be classified into adenomatous, inflammatory, hyperplastic, and hamartomatous types based on their pathological features (2). Among these, adenomatous polyps carry the highest risk of malignant transformation (3, 4). Colorectal cancer is among the most prevalent cancers in both women and men (5, 6). In terms of morphology, polyps can be categorized as broad-based, sub-pedunculated, or long-pedunculated. For broad-based polyps smaller than 1 cm, cold resection with a snare is the primary method. Titanium clips are only suitable for endoscopic resection of long-pedunculated polyps with a diameter around 5 mm. Polyps with thick peduncles greater than 1 cm pose a risk of massive bleeding due to incomplete blood supply blockage. The incidence of complications in traditional polyp resection Endoscopic Mucosal Resection (EMR) technology is relatively high, with a bleeding rate of up to 7.1% (7–9), While nylon rope ligation can effectively block the blood supply, it may slip off prematurely after surgery, leading to delayed bleeding. This report presents an innovative approach: first, the root is ligated with a nylon rope, then the nylon rope is fixed with a titanium clip, followed by high-frequency electroresection (Figures 1, 2). This combined method leverages the strengths of both techniques, compensating for their individual limitations. The nylon rope effectively blocks the blood supply, while the titanium clip secures the nylon rope at the root, preventing premature slippage (Figure 1c). It is worth noting that the roots of large and long pedunculated polyps often have huge nourishing blood vessels to supply the growth of the polyps, so the surface of the polyps will turn red (Figure 1a, b). After the roots are ligated with nylon ropes, the blood vessels are blocked, and the surface of the polyps will immediately appear bruised. During the surgery, it can be judged that the blood supply has been blocked, and then surgery can be performed, and reducing the risk of delayed bleeding.
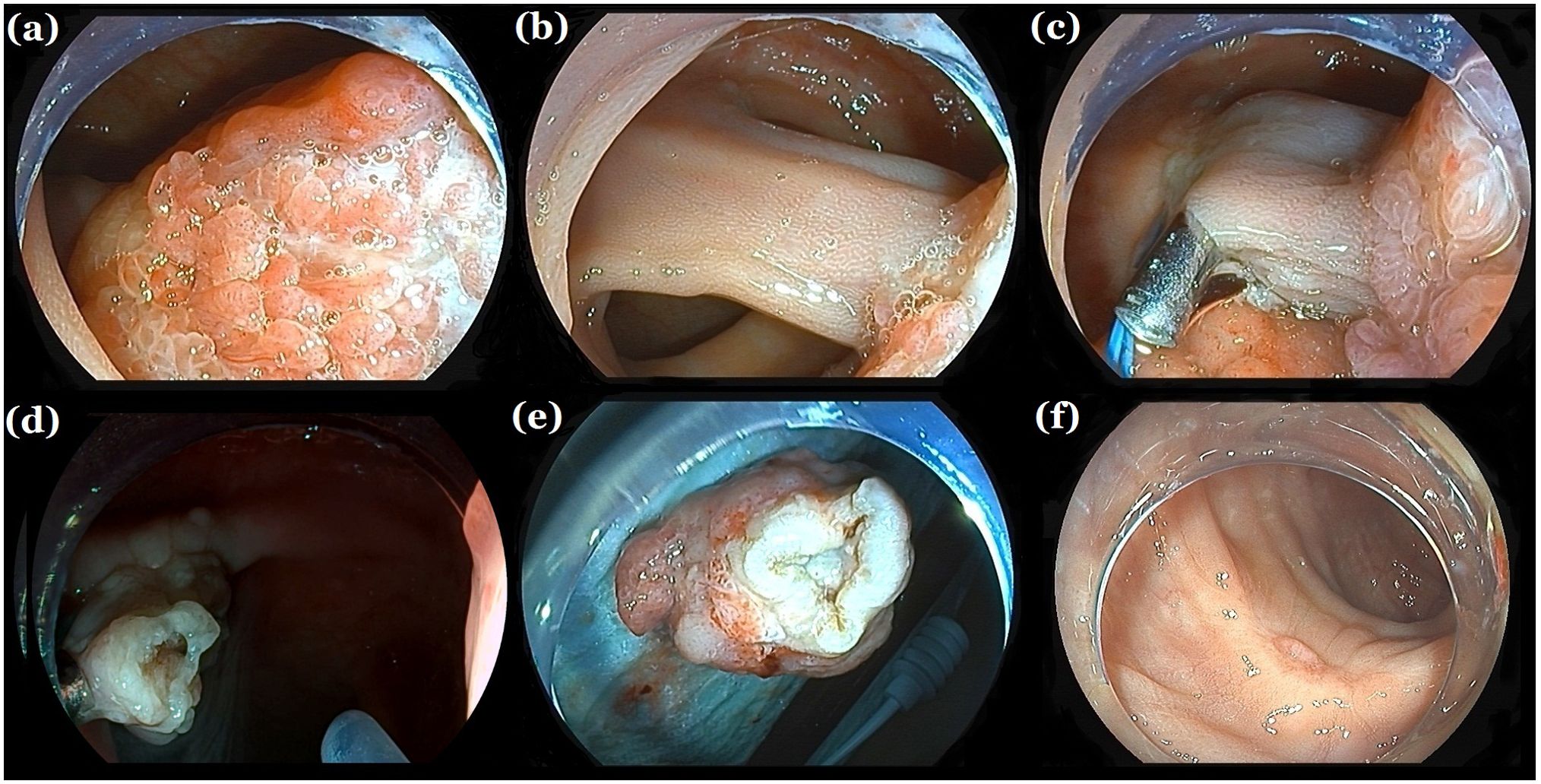
Figure 1. Endoscopic resection. (a, b) A large colon pedunculated polyp nearly completely obstructing the lumen. (c) Titanium clips assisting nylon cord ligation at the thick peduncle root. (d) No bleeding or perforation at the wound site after polypectomy. (d) Follow-up colonoscopy 1 month later showing scar formation. (e) giant colorectal polyps. (f) A re-examination of the colonoscopy 1 month later showed scar formation.
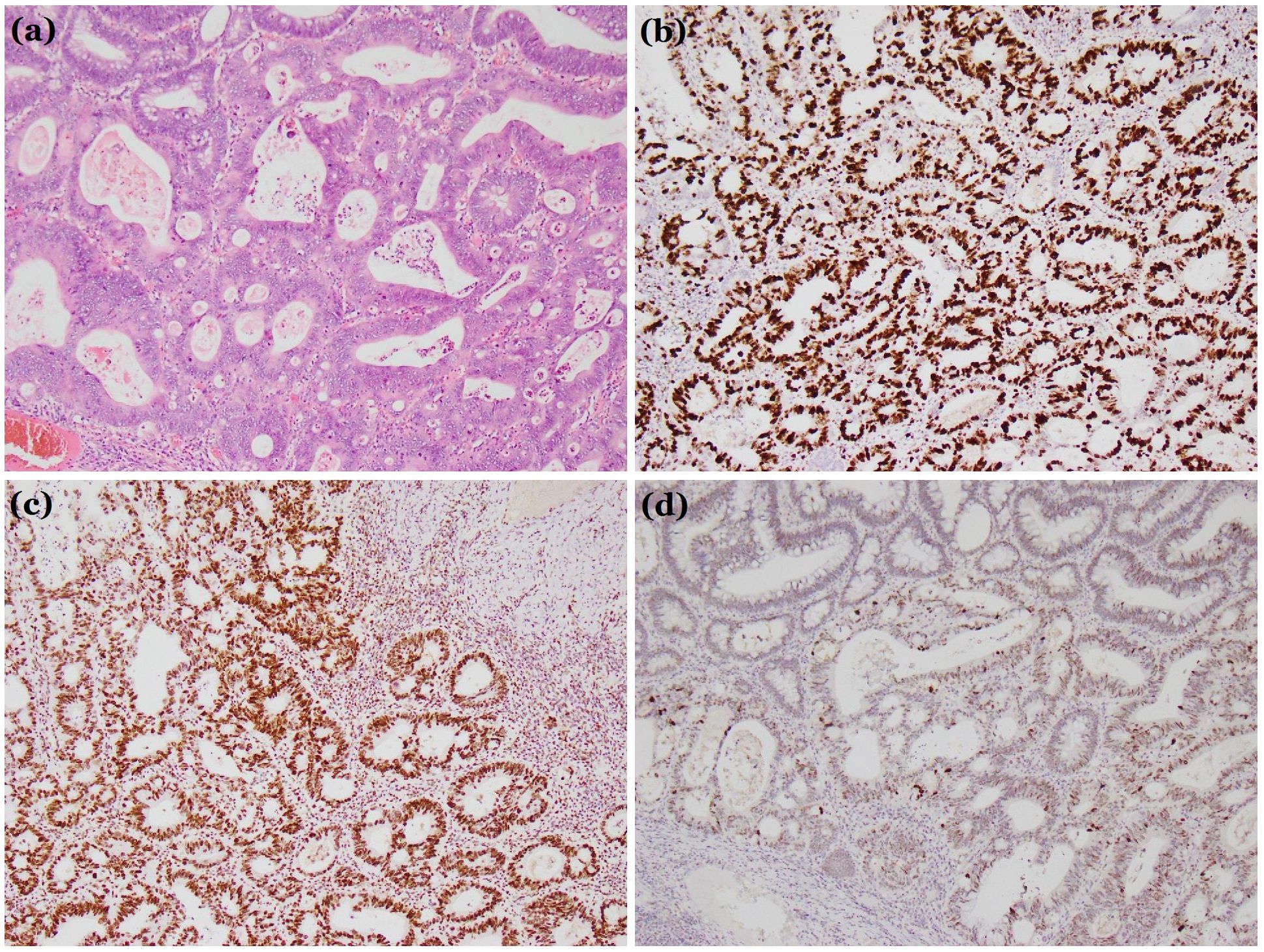
Figure 2. Histological diagnosis. (a) Hematoxylin and eosin stain (×100). (b-d) Immunohistochemical examination: (b) Ki67 (+). (c) MSH2 (+). (d) P53 (+). These findings confirmed the tumor was a villous-tubular adenoma with high-grade dysplasia and focal intramucosal carcinoma.
This study has several limitations. First of all, although all three cases were successfully treated with this method to remove giant colonic pedunculated polyps, the operation time was brief, the surgical field remained clear, and no bleeding or perforation occurred during the procedure. There were no complications, such as delayed bleeding or perforation, postoperatively. The resected specimens showed negative vertical and horizontal margins (Figures 1d–f), eliminating the need for additional surgical intervention and reducing the mental and economic burden on the patients. However, the number of cases and scope of application of this method are limited, and further expansion of its scope is needed, such as further validation in populations with underlying diseases, different immune function states, etc., to provide data support for the implementation and further promotion of this method. In addition, As of the submission time of this manuscript, all cases have been followed up for at least 1 year, and no tumor recurrence has occurred in any of the 3 cases. However, a longer follow-up time may be needed clinically to evaluate the efficacy of surgery and the recurrence of tumors.
In conclusion, titanium-clip-assisted nylon rope pre-treatment of the polyp root in the endoscopic resection of large colonic thick pedunculated polyps is both safe and effective. The procedure offers a short operation time, a clear surgical field, and no bleeding or perforation during or after the operation. It is a technique worthy of clinical adoption, particularly in patients with infectious diseases.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
YX: Data curation, Funding acquisition, Supervision, Validation, Visualization, Writing – original draft, Investigation, Methodology, Resources. YZ: Supervision, Validation, Visualization, Writing – review & editing. QT: Supervision, Investigation, Resources, Writing – review & editing. DW: Supervision, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mallery JS, Baron TH, Dominitz JA, Goldstein JL, Hirota WK, Jacobson BC, et al. Complications of ERCP. Gastrointest Endosc. (2003) 57:633–8. doi: 10.1053/ge.2003.v57.amge030576633
2. Hyun E, Helewa RM, Singh H, Wightman HR, Park J. Serrated polyps and polyposis of the colon: a brief review for surgeon endoscopists. Can J Surg. (2021) 64:E561–6. doi: 10.1503/cjs.018820
3. Al Ghamdi SS, Ngamruengphong S. Prevention of clinically significant post-EMR bleeding: To clip or not to clip? Gastrointest Endosc. (2022) 96:732–4. doi: 10.1016/j.gie.2022.07.002
4. Di Giorgio P, De Luca L, Calcagno G, Rivellini G, Mandato M, De Luca B. Detachable snare versus epinephrine injection in the prevention of postpolypectomy bleeding: a randomized and controlled study. Endoscopy. (2004) 36:860–3. doi: 10.1055/s-2004-825801
5. Foroughi F, Javadinia SA, Salek R. A randomized phase 3 trial of total neoadjuvant therapy (induction chemotherapy, neoadjuvant chemoradiation, neoadjuvant chemotherapy, and surgery) vs. standard long-term chemoradiation therapy (neoadjuvant chemoradiation, surgery, and adjuvant chemotherapy) in locally advanced rectal cancer. Front Oncol. (2024) 14:1468279. doi: 10.3389/fonc.2024.1468279
6. Fanipakdel A, Hosseini S, Javadinia S, Jeddi FA, Vasei M. The prognostic role of body mass index in survival of non-metastatic postoperative patients with colorectal cancer. Int J Cancer Manag. (2021) 14:e110257. doi: 10.5812/ijcm.110257
7. Ahmed Y, Othman M. EMR/ESD: techniques, complications, and evidence. Curr Gastroenterol Rep. (2020) 22:39. doi: 10.1007/s11894-020-00777-z
8. Pohl H, Grimm IS, Moyer MT, Hasan MK, Pleskow D, Elmunzer BJ, et al. Clip closure prevents bleeding after endoscopic resection of large colon polyps in a randomized trial. Gastroenterology. (2019) 157:977–984.e3. doi: 10.1053/j.gastro.2019.03.019
Keywords: novel nylon rope, titanium clip technique, endoscopic resection, giant colonic pedunculated polyps, AIDS
Citation: Xie Y, Zheng Y, Tang Q and Wang D (2025) Case Report: Endoscopic resection of giant colonic pedunculated polyps in patients with AIDS using a novel nylon rope and titanium clip technique. Front. Oncol. 15:1566005. doi: 10.3389/fonc.2025.1566005
Received: 24 January 2025; Accepted: 21 April 2025;
Published: 14 May 2025.
Edited by:
Nobu Oshima, Kyoto University Graduate School of Medicine, JapanReviewed by:
Mikhail Danilov, A.S. Loginov Moscow Clinical Scientific Centre, RussiaSeyed Alireza Javadinia, Sabzevar University of Medical Sciences, Iran
Copyright © 2025 Xie, Zheng, Tang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: DongMei Wang, aGVycmluZ2RvbmdAMTI2LmNvbQ==