 R. Aguiar-Ibáñez
R. Aguiar-Ibáñez YPV. Mbous
YPV. Mbous Sugandh Sharma3
Sugandh Sharma3- 1Merck Canada Inc., Kirkland, QC, Canada
- 2Merck & Co., Inc., Rahway, NJ, United States
- 3Parexel International, Chandigarh, India
- 4Parexel International, Bengaluru, India
- 5Parexel International, Mohali, India
Introduction: Cancer screening programs play a crucial role in early detection, improving survival rates and reducing the burden of advanced cancer. However, uptake remains inconsistent due to multifaceted barriers. This systematic review aimed to identify factors that impact cancer screening uptake across multiple tumor types and interventions to overcome barriers to cancer screening uptake.
Methods: A systematic literature review (SLR) was conducted using Embase® and MEDLINE® (May 2012 to May 2022) to identify observational studies that reported factors associated with screening uptake in adults, worldwide, with no tumor-specific restrictions. Records identified were screened by two independent reviewers. Included studies were data extracted by two reviewers and the results were reported narratively, focusing on identifying factors that acted as barriers or facilitators to cancer screening uptake, along with potential interventions to improve screening uptake.
Results: Overall, 811 studies were identified from the SLR that reported factors influencing the uptake of screening programs, with 658 studies covering screening programs for breast, cervical, lung, colorectal, gastric and prostate cancers. Barriers to cancer screening included: being unmarried, experiencing higher deprivation, lower socioeconomic status and rural living conditions. Facilitators to cancer screening included: older age, poor perception of health, previous cancer history, family history of cancer, previous cancer screening history, having knowledge of the disease, positive attitudes to screening, perceived cancer risk, higher education level, having children, higher income, higher socioeconomic status, having health insurance, urban residence, having access to care, and recommendations for screening by primary care physicians. Mixed findings were identified for race and ethnicity, employment and smoking status. Targeted educational programs were the most suggested strategy to overcome barriers to cancer screening uptake.
Conclusion: Barriers to cancer screening across multiple tumor types are complex, spanning demographic and patient-level factors, social and economic factors, provider and community challenges, and access to health care. While certain barriers are shared across tumor types, others are unique, reflecting the specific requirements of screening for different tumors. Addressing these barriers requires multi-level strategies that integrate both universal and cancer-specific approaches. Targeted interventions and supportive policies can increase screening participation, facilitate earlier cancer diagnosis, and reduce disparities in cancer outcomes.
1 Introduction
Cancer is a major public health issue, with over 20 million estimated cases and 9.7 million cancer-related deaths in 2022 (1). It represents a growing problem, with the number of annual cases expected to rise to 35 million by 2050 (1). One of the potential strategies to minimize the growing burden associated with cancer is to diagnose and detect cancer during the early stages (2, 3). Evidence-based cancer screening programs have great potential to improve cancer outcomes, and when organized effectively and quality-assured, they can detect pre-cancer or early-stage cancer in asymptomatic individuals, facilitating timely diagnosis and early access to treatment (4). Cancer screening programs have been shown to deliver improved long-term survival outcomes and reduced cancer-related mortality, along with substantial reductions in economic burden (5–7).
Despite the benefits, uptake of cancer screening has been mixed in recent years. A 2019 report by the American Cancer Society (ACS) reported that colorectal cancer (CRC) screening (endoscopy) rates increased steadily from 46.8% in 2005, to 60.3% in 2015. However, over the same period screening rates for cervical cancer (pap test) declined (2005: 85.4%, 2015: 81.6%), breast cancer screening rates (mammography) remained stable (2005: 51.2%, 2015: 50.2%), and uptake of lung cancer screening (low-dose computerized tomography [CT]) was extremely sparse (2005: not available, 2015: 3.9%) (8). In the 2024 State of Lung Cancer report released by the American Lung Association, lung cancer screening is recognized as having the potential to save hundreds of thousands of lives and generate substantial economic savings, yet despite this, screening rates remain low, with only 16% of eligible individuals screened nationwide. Disparities are evident, with states in the United States (U.S.) like Rhode Island achieving a screening rate of 28.6%, while others, like Wyoming, lag at 8.6%. However, policy changes, such as the expanded eligibility criteria by the United States Preventative Services Task Force (USPSTF) and the removal of Medicare registry requirements for reimbursement in March 2021, have altered access and reporting trends (9). These varied trends suggest that several complex and intersecting factors influence cancer screening uptake across the different tumor types.
The implementation of effective cancer screening programs requires substantial resources at the health system level across several broad categories, including funding, infrastructure and human resources (10). Furthermore, the successful rollout of these cancer screening programs is shaped by various factors across the healthcare system level, provider level, and patient levels (11–14). At the healthcare system level, policy decisions, funding availability, and infrastructure adequacy play a crucial role in determining accessibility and reach to screening programs (13, 14). For instance, well-defined policies and dedicated funding streams can enable broad implementation, while limited infrastructure can lead to restricted access to underserved populations (13, 14). At the provider level, factors such as workforce training and capacity are instrumental (11–13). Adequate provider training ensures the accurate administration of screening protocols, while insufficient staffing can limit screening program effectiveness and reach (11–13). On the community or patient level, accessibility, awareness, and cultural factors are critical determinants of screening uptake (11–14). For example, low health literacy or culturally specific health programs can act as barriers, while tailored outreach programs might serve as facilitators. Moreover, the impact of these factors on screening programs may shift, depending on the target population or geographic context, emphasizing the need to understand how they interact (11–14). Understanding these multifaceted influences is essential when designing effective interventions that address barriers at various levels of the healthcare system. By enhancing cancer screening uptake, such interventions can ultimately reduce cancer-related mortality, alleviate the humanistic burden and lessen the financial impact associated with cancer diagnosed at later stages (15, 16). Moreover, recognizing the factors impacting cancer screening uptake is crucial for developing effective implementation strategies.
Reviews conducted to date have largely focused on perceived barriers to screening within specific sub-populations e.g., based on age, disability, or sexual orientation, geographical location, or single tumor type (17–20). Commonly cited barriers to screening uptake include social determinants, perceived bias and discrimination against minoritized populations (18), mistrust of health care professionals among minoritized populations (21, 22), low levels of health literacy and education (22–24), lack of access to health insurance and/or healthcare resources (25) and other socioeconomic barriers (20, 25). However, a comprehensive review of barriers across multiple tumor types, geographies, and populations is lacking.
This systematic literature review aimed to identify factors that act as barriers to cancer screening uptake across multiple tumor types, geographies, population categories, as well as the proposed interventions to improve cancer screening rates. While the initial focus of this study was to identify barriers that could be addressed to improve the screening uptake, some of these factors may act as barriers, others as facilitators for cancer screening, and some as both, barriers and facilitators, depending on the context. By analyzing factors affecting screening uptake across multiple tumor types, this review seeks to identify common barriers or facilitators to cancer screening uptake, providing insights that can guide the optimal use of healthcare resources to promote early cancer detection and improve clinical outcomes.
2 Methods
2.1 Data sources and search strategy
A systematic literature review (SLR) was conducted following the methodology listed by the Cochrane Handbook and the Centre for Reviews and Dissemination (26, 27). The reporting of this SLR followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (28). The study was conducted following the development of a protocol, which identified the objectives, the pre-defined PICOTS criteria, the methodology and reporting of results. This pre-defined protocol and remained unchanged throughout the review process, and adherence to it ensured transparency, reproducibility, and minimized bias in the conducted review process.
There were no restrictions on the tumor types, language or geographical location of the included studies. Only English search terms were employed in the search. Eligibility criteria focused primarily on studies that reported factors impacting screening uptake and associated interventions that could help mitigate the existing factors in general or high-risk population. MEDLINE® and Embase®, Cochrane Database of Systematic Reviews (CDSR), Cochrane Controlled Register of Trials (CENTRAL) and PubMed (solely to capture in-process citations) were searched to retrieve evidence published between May 2012 and May 2022. Grey literature sources included the Open Grey. Additional searches of conference proceedings from the American Society of Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), ESMO Breast Cancer, the American Association for Cancer Research (AACR) and the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) (2020–2022, inclusive) were searched to capture any studies not yet published in full-text articles, or abstracts reporting supplementary follow-up results associated with previously published studies. Bibliographic searching of published literature reviews was also conducted.
The search strategy is provided in the Supplementary Appendix S1.
2.2 Eligibility criteria for study selection
Included were observational studies for adults (≥18 years old) eligible to undergo cancer screening. There were no restrictions on interventions or comparators. Cancer screening included different outcome definitions, such as: general cancer screening, any cancer screening participation or adherence to cancer screening, as well as cancer-specific screening tests or methods, for example, mammography for breast cancer, pap smear testing for cervical cancer, or colonoscopy for CRC. Key outcomes of interest were factors associated with adherence to available screening guidelines or programs (e.g., patient profile, familial history or biomarker assessment). Other factors such as barriers and facilitators associated with patient characteristics and beliefs (e.g., predictors of low uptake vs high uptake such as age, ethnicity, tumor type, familial history, education, patients beliefs or socio-cultural factors associated with low uptake of screening opportunities, symptom recognition, health literacy among patients, median/mean time from diagnosis to treatment), factors associated with screening access (e.g., availability and funding for diagnostic tools or screening programs, literacy and or symptom awareness among physicians, challenges attending screening), perspectives from scientific leaders on screening guidelines, and interventions or approaches that may help overcome screening barriers were included. The timeframe of interest ranged from 2012 to 2022. The detailed information on the predefined Population, Interventions, Comparisons, Outcomes, Time, and Study design (PICOTS criteria) is included in the Supplementary Appendix S2.
2.3 Study search, selection, and abstraction
The study selection (i.e., the screening of titles and abstracts followed by full text screening), was performed by two independent reviewers to identify all relevant studies. A third independent reviewer resolved any discrepancies. Data from included studies were extracted into a pre-defined extraction grid, ensuring that data was extracted uniformly and was comparable across studies. Data extraction was again conducted by two reviewers, and subsequently checked and reconciled by an independent third reviewer.
2.4 Risk of bias, strength, and certainty of evidence
Quality assessment of included observational studies, in particular, cohort and cross-sectional studies, was conducted using the Newcastle-Ottawa scale (NOS) (29). The NOS scale consists of three domains: the selection of the study groups, the comparability of the groups, and the ascertainment of the exposure or outcome of interest. The total maximum score is 9, with three threshold ranges for: high quality (scores from 7-9), medium quality (scores from 4-6), and low quality (scores from 0-3) (29).
2.5 Data analysis
This study employed a narrative SLR approach, where no statistical pooling of results was conducted. Only studies reporting statistically significant odd ratios (ORs) conveying the degree and direction of association between factors and cancer screening are discussed in the results section. For reporting purposes, we focused on visualizing through figures the identified ORs (whenever reported) across included studies using logarithmic scale (log(OR)), categorized by tumor types and indicating whether each factor was identified as a barrier or facilitator to screening uptake. This methodology allowed for a comprehensive overview of the landscape of factors influencing cancer screening uptake. The factors identified in the SLR were to be categorized into six main domains, namely: demographics, economics, patient access, patient behavior, primary care physician (PCP) access, and social barriers.
Factors identified as barriers were defined as factors with an OR<1 (log(OR)<0), which indicated a lower likelihood of screening uptake for the comparison group vs the reference group. Similarly, facilitating factors were defined as factors with an OR>1 (log(OR)>0), which were indicative of higher likelihood of screening uptake for the comparison group versus the reference group. Only those factors that demonstrated statistically significant associations (p < 0.05) with screening uptake were included. When reported, ORs based on multivariate analyses were preferred to those from univariate analyses. Univariate analyses were presented if they were statistically significant and if multivariate analyses were not provided. Statistical significance of the reported ORs was confirmed based on p-values, or 95% CI in cases where p-values were not available.
Figures representing the log(ORs) for the selected factors were then developed for factors reported in which in at least one of the tumor types there were 10 studies reporting on a specific factor, and therefore that factor was represented in the figure across all the priority tumor types. These figures were to be descriptive and to be used as a visualization aid, and no statistical analyses to pool the data were conducted. The aim was to provide an understanding on the number of studies that identified the respective factor as a barrier or facilitator, and the number of times the factor was identified, across all relevant studies with different strata used to categorize each factor. In factors with varying categorizations across studies, designated reference groups (as reported in the studies) were used as the common reference group for that factor among all relevant studies. For example, for the factor ‘age’, reference groups (e.g. <50 years for breast cancer, or <30 years for cervical cancer) were established based on the age groups/categories that served as a reference across the majority of studies focusing on the respective populations being screened for cancer.
Furthermore, interventions aimed to overcome barriers mentioned in the included studies were also identified and summarized to provide valuable insights into potential strategies for improving cancer screening uptake.
3 Results
3.1 Included studies
A total of 811 studies from the SLR were initially included that reported factors which had statistically significant or non-significant associations with the uptake of screening programs (based on reported ORs), as well as other outcome measures such as hazard ratios. Studies on screening for breast, cervical, colorectal, lung, gastric, and prostate cancer were prioritized for reporting, as these tumor types have well established screening programs (30). Overall, 658 unique studies were included with the final number of included studies per tumor type which reported statistically significant ORs for factors influencing screening uptake being: 199 for breast cancer, 278 for cervical cancer, 246 for CRC, 37 for lung cancer, 12 for gastric cancer and 38 for prostate cancer (Figure 1). As studies may report on screening for multiple tumor types, the number of included studies per tumor type are not mutually exclusive. Full details of the study characteristics across the included studies are presented in the Supplementary Appendix S5.
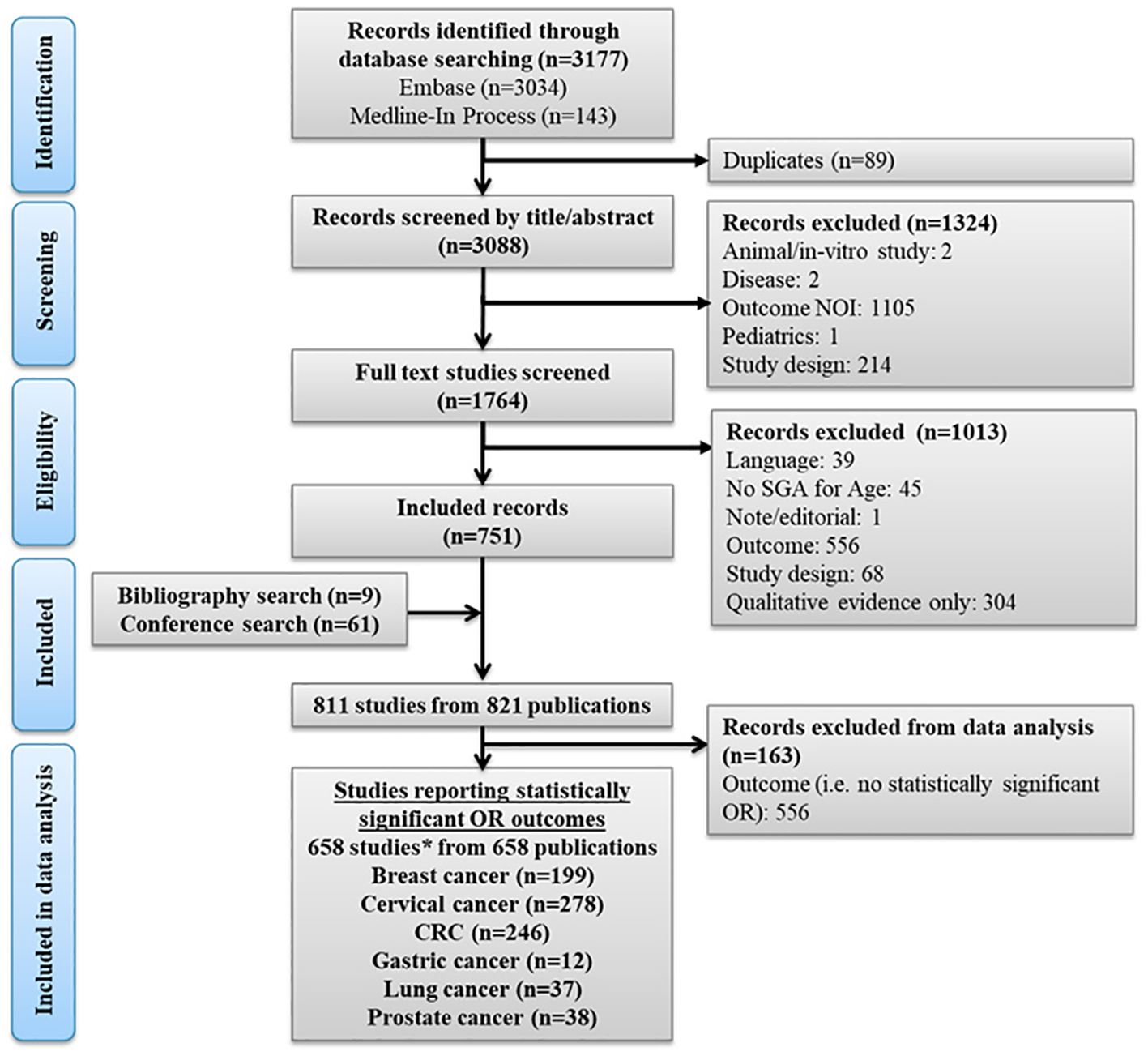
Figure 1. PRISMA flow diagram. *The numbers of studies per tumor type were not mutually exclusive as some studies presented results for screening programs across more than one tumor type. CRC, Colorectal cancer; log, logarithm; NOI, Not of interest; OR, Odds ratio; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SGA, Subgroup analysis.
A diverse range of data was identified across the included studies. To allow for identification of trends across the included data points, evidence was reported according to six main factor categories associated with screening uptake, including: demographics, economics, patient access, patient behaviour, PCP access and social factors (as detailed in section 2). The outcomes considered for inclusion in each of these categories, and their definitions, are presented in the Supplementary Appendix S3. The number of studies reporting factors across these 6 categories, according to the tumor types screened across the included studies, were: 384 for demographic factors, 240 for economic factors, 260 for social factors, 118 for patient behavior-related factors, 256 for patient access-related factors, and 104 for PCP access-related factors (see Supplementary Appendix S4).
For data visualization purposes, the number of included studies per factor and per tumor type was established based on the availability of statistically significant OR data per factor (as detailed in section 2) and considering factors that were reported in at least 10 studies per tumor type. The OR data was presented on a logarithmic scale allowing for a symmetrical representations of equivalent associations. A total of 158, 242, 205, and 26 studies (not mutually exclusive for barriers or for facilitators) that evaluated factors associated with the uptake of screening for breast cancer, cervical cancer, CRC, and lung cancer, respectively, were represented through Figures 2–7 (see section 3.2) Figure 1. PRISMA flow diagram. Results for gastric cancer and prostate cancer are presented in Supplementary Appendix S6.
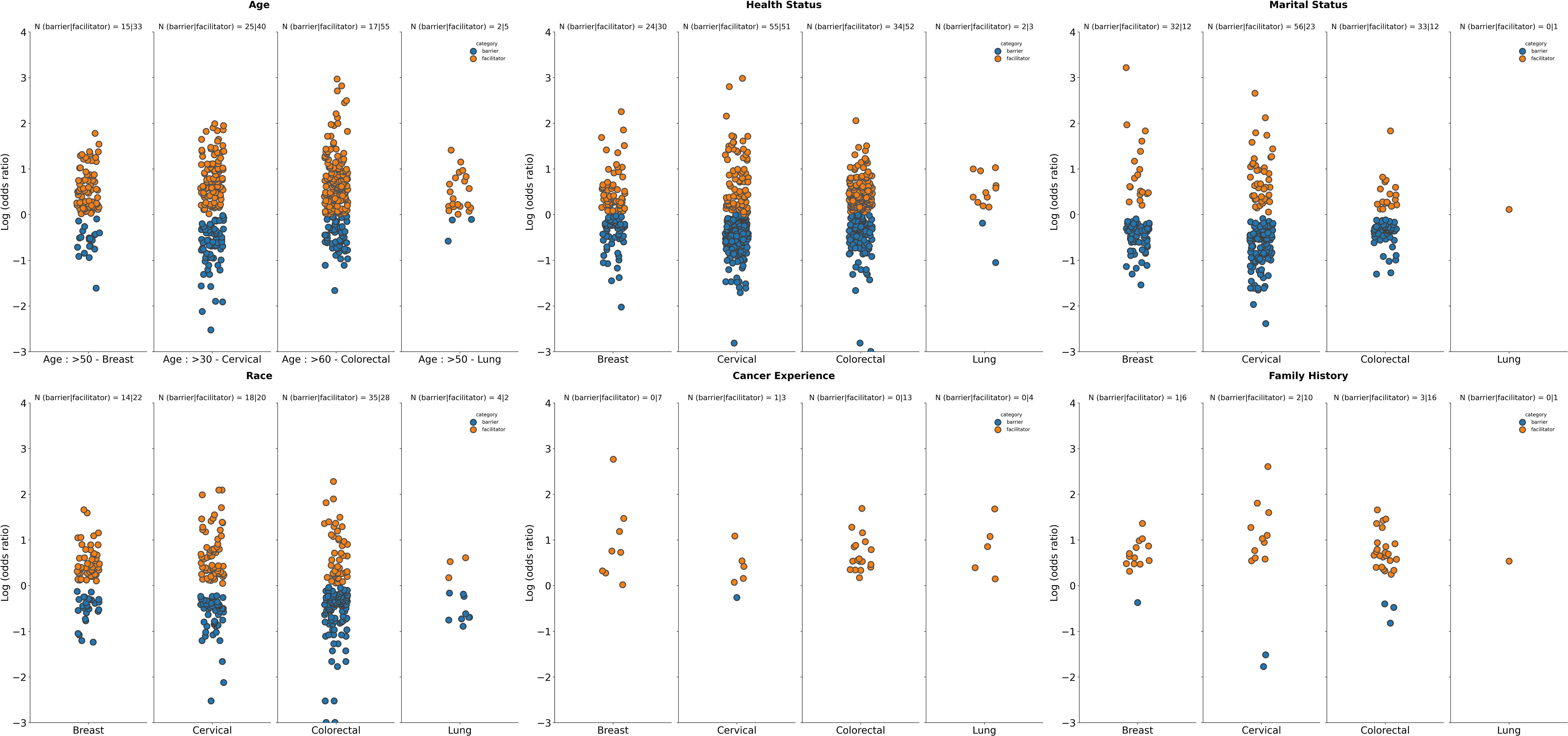
Figure 2. Summary of logarithm of odds ratios according to tumor type for selected demographic characteristics. Age: Datapoints represent log(ORs) for groups aged ≥50 years (vs. <50 years as reference group in studies on breast and lung cancer screening programs), ≥30 years (vs. < 30 years as reference groups for studies on screening for cervical cancer), ≥60 years (vs. <60 years as reference group in studies on screening for CRC); Health status: Datapoints represent log(ORs) for groups with perception of health rated as “poor”, or “fair” (vs. ratings of “good”, “very good”, and “normal” as reference group across included studies); Marital status: Datapoints represents log(ORs) for “single”, “divorced”, “widowed” “or “separated” groups (vs. those who were “married” or “partnered” as reference groups); Race: Datapoints represent log(OR) for non-white race groups (vs. white race groups as reference group); Cancer experience: Datapoints represents log(ORs) for groups with any previous cancer history (vs. those with no cancer history as a reference group across included studies); Family history: Datapoints represents log(ORs) for groups with family history of cancer (vs. those with no history of cancer as a reference group). The number of studies for which a specific factor acted as a barrier, or a facilitator is shown as “N” atop each panel. A single study may be categorized as both a barrier and a facilitator if different strata within it showed opposing associations with screening uptake for the same factor. Facilitator (orange): a factor with a log(OR) >0, indicating a higher screening uptake for the comparison group vs the reference group. Barrier (blue): a factor with a log(OR) <0, indicating a lower screening uptake for the comparison group vs the reference group.
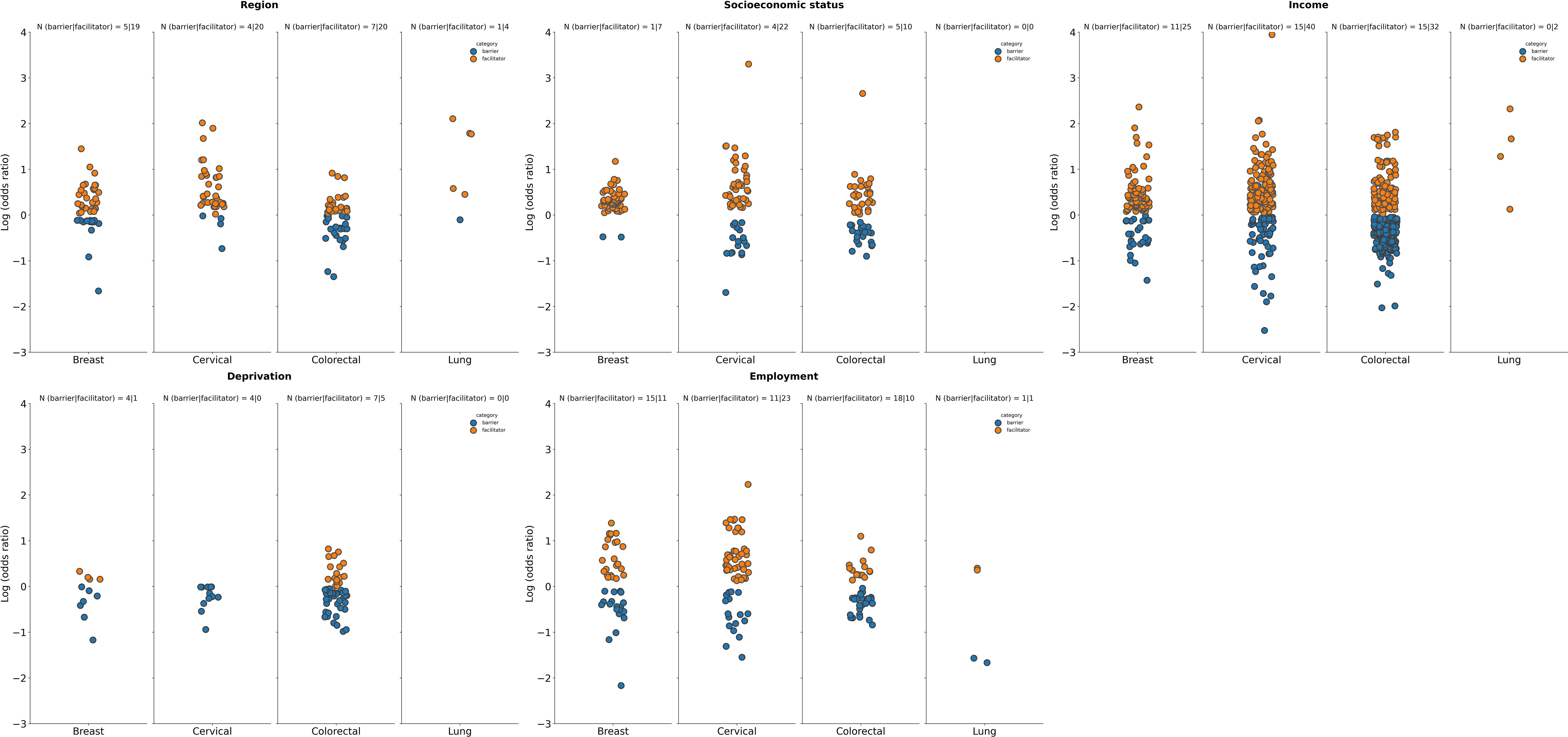
Figure 3. Summary of logarithm of odds ratios according to tumor type for selected economic factors. Deprivation: Datapoints represent log(ORs) for the most deprived groups (vs. least deprived as reference) Deprivation was defined via the Area/European deprivation index; Region: Datapoints represent log(ORs) for urban or suburban dwelling groups (vs. “inaccessible areas”, “rural”, or “non-metropolitan” as reference); Socioeconomic status: Datapoints represent log(ORs) for richer or wealthier groups (vs. “poorest “, “poor, or “lower class” as reference); Income: Datapoints represent log(ORs) for higher income groups (vs. lower income groups as reference); Employment: Datapoints represent log(ORs) for employed individuals/groups (vs. “unemployed”, “retired”, “homemaker”, “housewife”, or “student” groups as reference). Employed included “self-employed”, “part-time and full-time employment”, “contracted”. The number of studies for which a specific factor acted as a barrier (in blue) or a facilitator (in orange) is shown as “N” atop each panel. A single study may be categorized as both a barrier and a facilitator if different strata within it showed opposing associations with screening uptake for the same factor. Facilitator (orange): a factor with a log(OR) >0, indicating a higher screening uptake for the comparison group vs the reference group. Barrier (blue): a factor with a log(OR) <0, indicating a lower screening uptake for the comparison group vs the reference group.
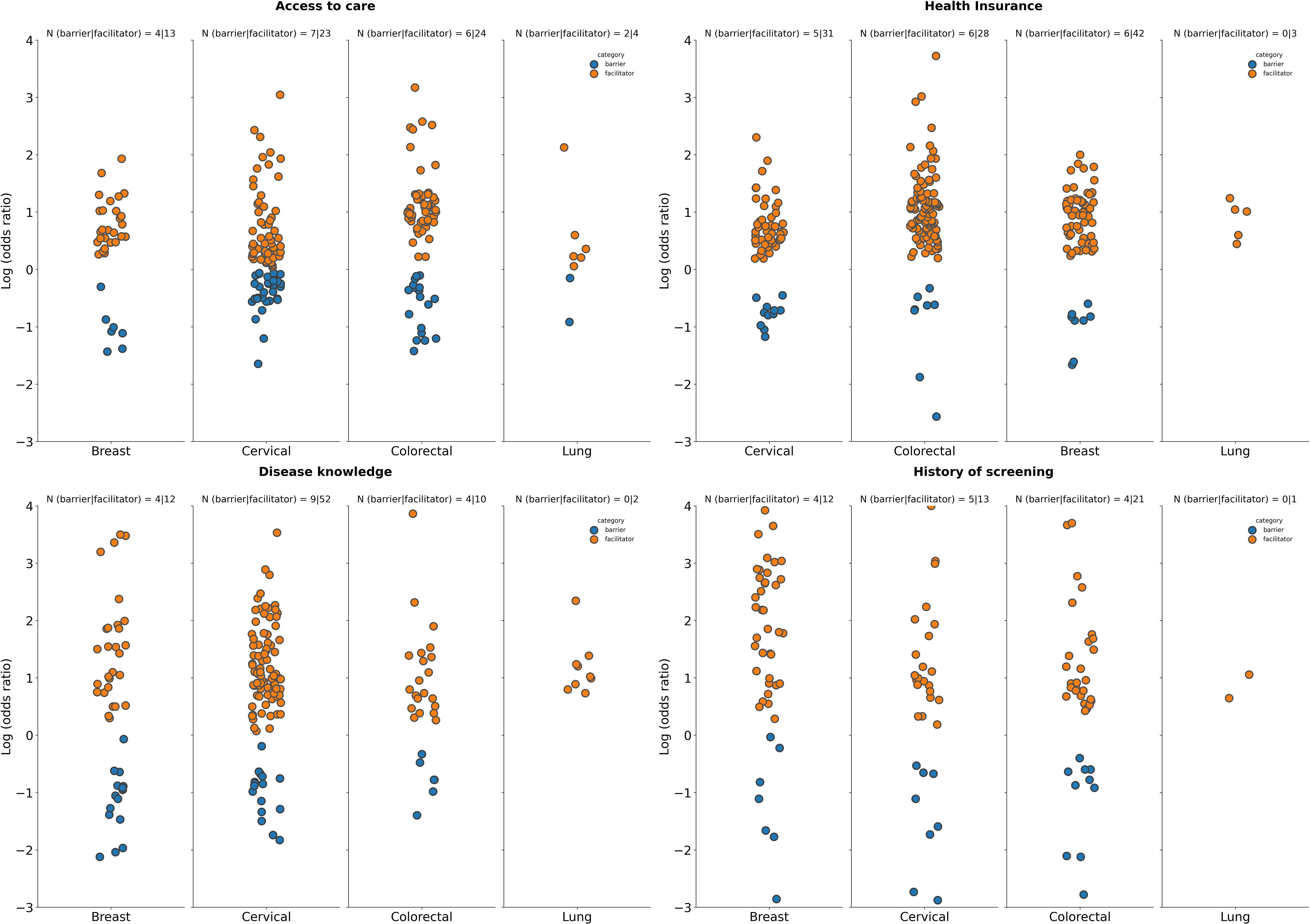
Figure 4. Summary of logarithm of odds ratios according to tumor type for selected patient access-related factors. Access to care: Datapoints represent log(ORs) for groups with access to care or a PCP (vs. those with “no access to care”, “no PCP”, or “health access hardship” as reference); Health insurance coverage: Datapoints represent log(ORs) for groups with any form of health insurance coverage (vs. uninsured groups as reference); Disease knowledge: Datapoints represent log(ORs) for groups with “high”, “good’, or “sufficient” knowledge about the disease (vs. groups with “low understanding”, “not knowledgeable”, “poor knowledge”, or “insufficient” knowledge as reference); History of screening: Datapoints represent log(ORs) for groups with a history of cancer screening (vs. those with no history of screening as reference). The number of studies for which a specific factor acted as a barrier (in blue), or a facilitator (in orange) is shown as “N” atop each panel. A single study may be categorized as both a barrier and a facilitator if different strata within it showed opposing associations with screening uptake for the same factor. Facilitator (orange): a factor with a log(OR) >0, indicating a higher screening uptake for the comparison group vs the reference group. Barrier (blue): a factor with a log(OR) <0, indicating a lower screening uptake for the comparison group vs the reference group.
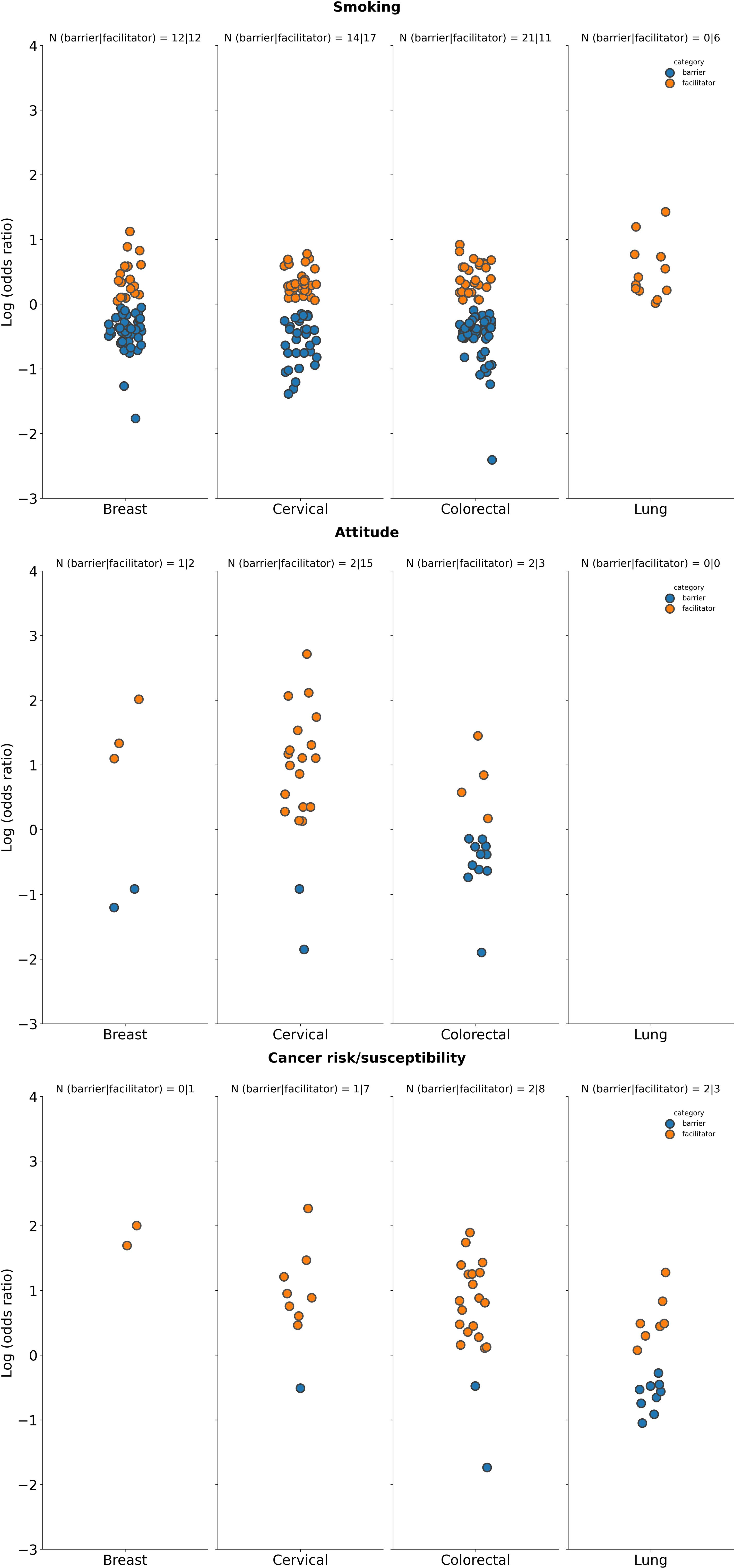
Figure 5. Summary of logarithm of odds ratios according to tumor type for selected patient behavior-related factors. Smoking status: Datapoints represent log(ORs) for groups of “current” smokers (vs. groups of “former”, “previous”, or “never” smokers as reference); Attitude: Datapoints represent log(ORs) for groups with “positive” or “favorable” attitude (vs. those with “negative”, or “poor” as reference); Cancer risk: Datapoints represent log(ORs) for groups with “higher”, “moderate” perceived cancer susceptibility (vs. those with “no” or “lower” perceived susceptibility to cancer as reference). The number of studies for which a specific factor acted as a barrier (in blue) or a facilitator (in orange) is shown as “N” atop each panel. A single study may be categorized as both a barrier and a facilitator if different strata within it showed opposing associations with screening uptake for the same factor. Facilitator (orange): a factor with a log(OR) >0, indicating a higher screening uptake for the comparison group vs the reference group. Barrier (blue): a factor with a log(OR) <0, indicating a lower screening uptake for the comparison group vs the reference group.
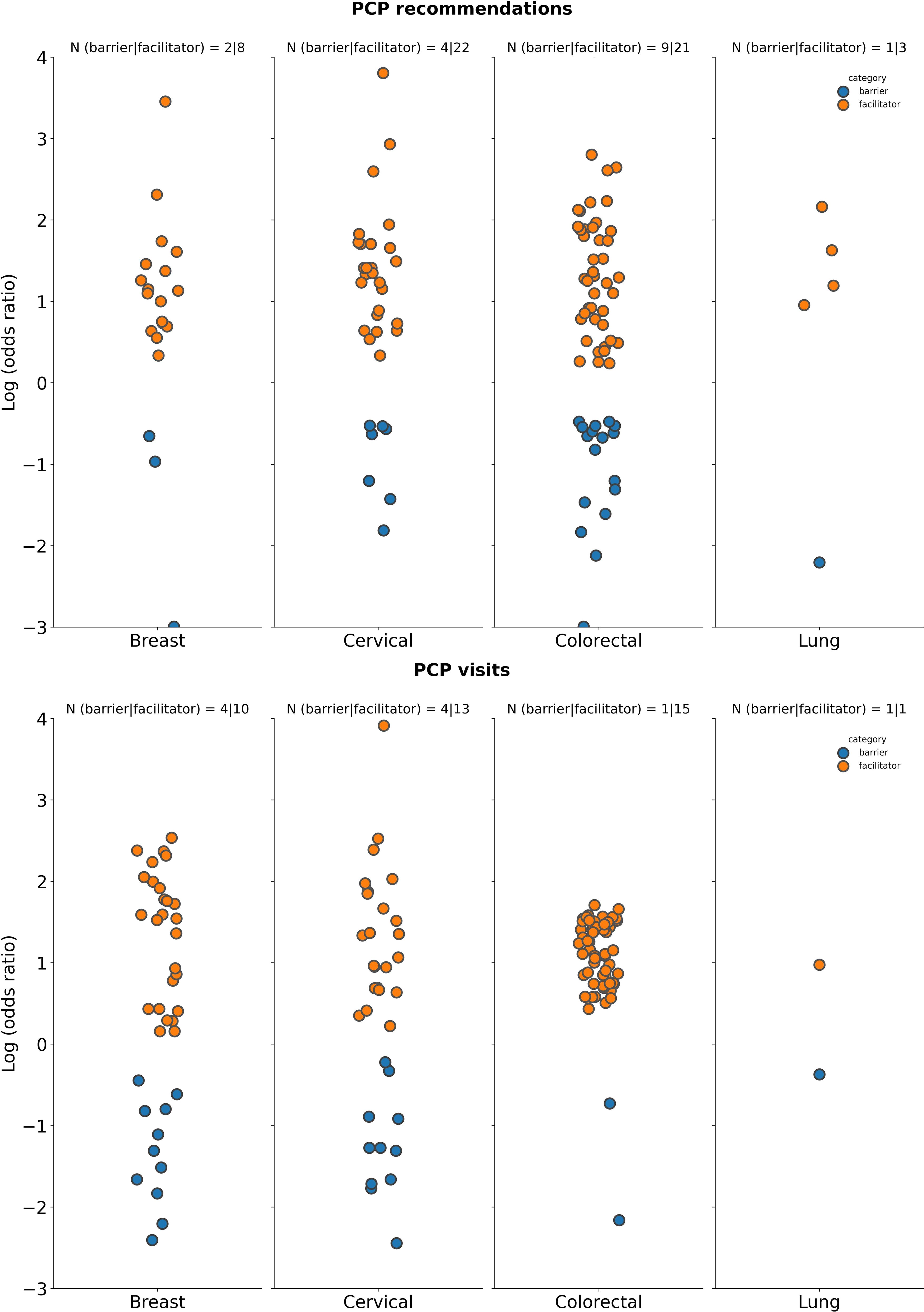
Figure 6. Summary of logarithm of odds ratios according to tumor type for selected PCP factors. PCP recommendations: Datapoints represent log(ORs) for groups who received a cancer screening recommendation by a PCP (vs. those who did not receive such a recommendation from a PCP as reference); PCP visits: Datapoints represents log(ORs) for groups who had no visits to the PCP or had the lowest number of visits to the PCP (vs. those that had visits or had a high number of visits to the PCP). The number of studies for which a specific factor acted as a barrier (in blue) or a facilitator (in orange) is shown as “N” atop each panel. A single study may be categorized as both a barrier and a facilitator if different strata within it showed opposing associations with screening uptake for the same factor. Facilitator (orange: a factor with a log(OR) >0, indicating a higher screening uptake for the comparison group vs the reference group. Barrier (blue): a factor with a log(OR) <0, indicating a lower screening uptake for the comparison group vs the reference group.
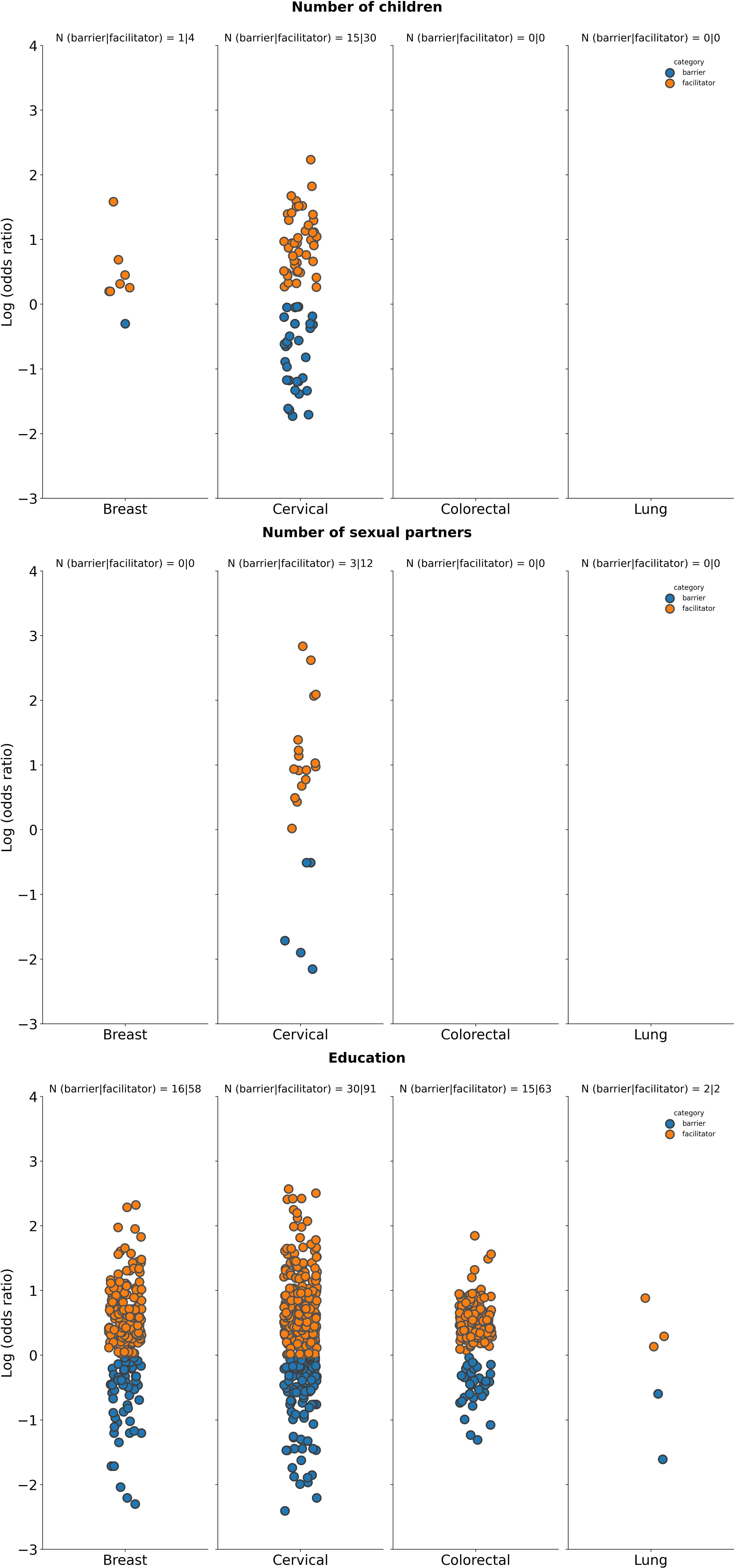
Figure 7. Summary of logarithm of odds ratios according to tumor type for selected social factors. Number of children: Datapoints represents log(ORs) for groups of patients with at least one child (vs. groups of patients with no children as reference); No. of sexual partners: Datapoints represents log(ORs) for those that have had more than one sexual partner (vs. those that have had 0 to 1 sexual partner as reference); Education: Datapoints represents log(ORs) for “high education”, “≥ high school graduate”, “tertiary education”, “university/college graduate” groups (vs. groups with “low education”, “no school”, “no formal education”, “illiterate”, “<high school”, “did not graduate high school”, “primary school”, or “middle school” as reference). The number of studies for which a specific factor acted as a barrier (in blue) or a facilitator (in orange) is shown as “N” atop each panel. A single study may be categorized as both a barrier and a facilitator if different strata within it showed opposing associations with screening uptake for the same factor. Facilitator (orange): a factor with a log(OR) >0, indicating a higher screening uptake for the comparison group vs the reference group. Barrier (blue): a factor with a log(OR) <0, indicating a lower screening uptake for the comparison group vs the reference group.
3.2 Barriers and facilitators to cancer screening
3.2.1 Demographics
Several demographic-related barriers and facilitators to cancer screening were identified, with age being the most identified factor, considered in 41% (157/384 studies) of the included studies. In general, older age is a facilitator to cancer screening across multiple tumor types [≥50 years for breast and lung cancer; ≥30 years for cervical cancer, and ≥60 years for CRC; (Figure 2)]. Studies reporting older age groups as a facilitator compared to the reference group were as follows: 33 out of 40 studies reported older age as a facilitator for breast cancer vs 15 out of 40 studies as a barrier; 40 out of 52 studies reported older age as a facilitator vs 25 out of 52 studies as a barrier for cervical cancer; 55 out of 67 studies reported older age as a facilitator vs 17 out of 67 studies as a barrier for CRC; and 5 out of 6 studies reported older age as a facilitator vs 2 out of 6 studies as a barrier for lung cancer. This trend was consistent with gastric and prostate tumour types (Supplementary Appendix S6).
Compared to individuals with less than good health status, perceived good health status was generally reported to be a barrier to cancer screening across multiple tumor types (Figure 2). Specifically, for breast cancer 30 out of 44 studies reported less than good health status as a facilitator to screening compared to 24 out of 44 studies identifying it as a barrier; for CRC, 52 out of 68 studies identified less than good health status as a facilitator to screening vs 34 out of 68 studies as a barrier, and for lung cancer, 3 out of 4 studies identified less than good health status as a facilitator compared to 2 out of 4 studies as barrier. Similar findings were observed for gastric and prostate cancer, with more studies indicating that less than good health status as a facilitator than a barrier to cancer screening (Supplementary Appendix S6). However, for cervical cancer there were less studies reporting less than good health status as a facilitator (51 out of 89 studies) vs as a barrier (55 out 89 studies) to screening uptake.
Across all tumor types, having previous experience with cancer was linked to facilitating screening uptake as opposed to this factor acting as barrier (Figure 2). Specifically, there were 7 out of 7 studies identified this being a facilitator vs 0 out of 7 studies as a barrier in breast cancer; there were 3 out of 4 studies identifying this as a facilitator vs 1 out of 4 studies as a barrier in cervical cancer; there were 13 out of 13 studies identifying this as a facilitator vs 0 out of 13 studies as a barrier in CRC, and 4 out of 4 studies identifying this as a facilitator vs 0 out of 4 studies as a barrier in lung cancer. This trend was consistent with gastric and prostate tumour types (Supplementary Appendix S6).
Similarly, there were more studies that identified having a family history of cancer as a facilitator to screening vs a barrier [breast cancer, 6 out of 7 studies as facilitators vs 1 out of 7 studies as barrier; cervical cancer, 10 out of 11 studies as facilitators vs 2 out of 11 studies as barriers; CRC, 16 out of 17 studies as facilitators vs 3 out of 17 studies as barriers; lung cancer, 1 out of 1 study as a facilitator vs 0 out of 1 studies as barriers (Figure 2)]. Similar results were seen with gastric and prostate cancer with more studies that identified having a family history of cancer as a facilitator to screening rather than a barrier (Supplementary Appendix S6).
Being an unmarried individual was generally a barrier rather than a facilitator to cancer screening for breast, cervical, and colorectal cancer [breast cancer, 12 out of 41 studies as facilitators vs 32 out of 41 studies as a barrier, cervical cancer 23 out of 76 studies as facilitators vs 56 out of 76 studies as barriers, CRC 33 out of 44 studies as facilitators vs 12 out of 44 studies as barrier (Figure 2)]. However, for lung cancer, one study was found to identify being unmarried or single as facilitating cancer screening uptake (with no studies identifying it as a barrier), compared to being married or in a partnership (Figure 2). For gastric cancer, unmarried or single status was observed to be a both a facilitator and a barrier in identified studies, while conversely, for prostate cancer, more studies identified unmarried status as a facilitator rather than a barrier for cancer screening (Supplementary Appendix S6).
Race and ethnicity demonstrated varying influences on screening uptake (Figure 2). Non-White populations had more studies identifying non-White race as a facilitator for undergoing screening for breast cancer (22 out of 26 studies) vs as a barrier (14 out of 26 studies), along with cervical cancer (20 out of 28 studies as a facilitator vs 18 out of 28 studies as a barrier) compared to White populations. Conversely, a higher number of studies for CRC and lung cancer identified non-White race as a barrier to screening (35 out of 52 studies and 4 out of 6 studies, respectively) vs a facilitator (28 out of 52 studies and 2 out of 6 studies, respectively). Similar to CRC and lung cancer, for prostate cancer, more studies identified non-White race as a barrier rather than a facilitator to cancer screening, and no studies identified race as either a barrier or facilitator for gastric cancer (Supplementary Appendix S6).
3.2.2 Economic factors
Economic factors such as deprivation (most deprived vs least deprived), employment status (e.g., employed vs unemployed or retired), income (high vs low), socioeconomic status (low vs high), or region (e.g., urban vs rural) influenced cancer screening uptake across multiple tumor types. Individuals with high income and socioeconomic status, those least deprived, and those from urban areas were more likely to undergo cancer screening compared to their counterparts with low income and low socioeconomic status, those most deprived, and those from rural areas (Figure 3).
Experiencing deprivation was identified as a barrier rather than a facilitator to cancer screening. For breast cancer, only 1 out of 5 studies identified being most deprived as a facilitator to screening while 4 out of 5 studies identified being most deprived as a barrier. For cervical cancer all 4 studies identified being most deprived as a barrier to screening uptake. As with breast and cervical cancer, CRC identified deprivation as a barrier for screening uptake, with 5 out of 8 studies identifying this factor as a facilitator to screening and 7 out of 8 studies identifying this factor as barrier. No studies reported deprivation as a factor for influencing lung (Figure 3), gastric or prostate cancer screening uptake (Supplementary Appendix S6).
The relationship between employment status and cancer screening uptake varied by tumor type. In breast cancer, 11 out of 23 studies reported employment as a facilitator to screening compared to 15 out of 23 studies that reported it as a barrier. For cervical cancer screening, more studies identified employment as a facilitator (23 out of 31 studies) compared to as a barrier (11 out of 31 studies). Like breast cancer, for CRC, fewer studies identified employment as a facilitator to screening (10 out of 22 studies) compared to as a barrier (18 out of 22 studies). In lung cancer there were the same number of studies that identified employment as a facilitator (1 out of 2 studies) and as a barrier. For both gastric and prostate cancer, employment was seen as more of a barrier than a facilitator to cancer screening (Supplementary Appendix S6).
A higher income was linked to higher screening uptake, with all tumor types reporting more studies identifying a higher income as a facilitator (breast, 25 out of 34 studies; cervical, 40 out of 49 studies; CRC, 32 out of 44 studies; lung, 2 out of 2 studies) than as a barrier (breast, 11 out of 34 studies; cervical, 15 out of 49 studies; CRC, 15 out of 44 studies; lung, 0 out of 2 studies). This trend was also observed for gastric and prostate cancer (Supplementary Appendix S6).
Having a high socioeconomic status served as a facilitator for screening of breast cancer (7 out of 8 studies as a facilitator vs 1 out of 8 studies as a barrier), cervical cancer (22 out of 25 studies as a facilitator vs 4 out of 25 studies as a barrier) and CRC (10 out of 13 studies as a facilitator vs 5 out of 13 studies as a barrier). No studies on screening for lung cancer reported socioeconomic status as influencing cancer screening uptake. This trend with high socioeconomic status as a facilitator rather than a barrier to screening was consistent for gastric and prostate cancer (Supplementary Appendix S6).
Geographical location linked to socioeconomic factors also seemed to influence screening uptake and living in an urban area compared to a rural one was a facilitator in more studies across the majority of tumor types (breast, 19 out of 22 studies; cervical, 20 out of 23 studies; CRC, 20 out of 24 studies; lung, 4 out of 5 studies) rather than as a barrier (breast, 5 out of 22 studies; cervical, 4 out of 23 studies; CRC, 7 out of 24 studies; lung, 1 out of 5 studies). Conversely, for gastric cancer, more studies identified living in an urban area as a barrier rather than a facilitator to cancer screening, while for prostate cancer an equal number of studies identified living in an urban area as a facilitator and barrier to screening (Supplementary Appendix S6).
3.2.3 Patient access
The relationship between patient access and cancer screening uptake depends on the particular factor, as well as the tumor type. Among factors identified in this study, having knowledge about cancer (high vs poor), health insurance coverage (insured vs non-insured), access to care (yes vs no), and history of screening (yes vs no), show that patient access is a facilitator for cancer screening for the majority of cancer types (Figure 4).
Regardless of tumor type, patients with some knowledge of the disease have a higher screening uptake compared to those with no knowledge (Figure 4). For breast cancer, disease knowledge was a facilitator to cancer screening in 12 out of 16 studies and was a barrier in 4 out of 16 studies. For cervical cancer, it was a facilitator in 52 out of 58 studies vs a barrier in 9 out of 58 studies. Similarly, in colorectal and lung cancer, disease knowledge was a facilitator in 10 out of 12 studies and 2 out of 2 studies, respectively, and was a barrier in 4 out of 12 studies and 0 out of 2 studies, respectively. For prostate cancer more studies reported disease knowledge as a facilitator than as a barrier to cancer screening (Supplementary Appendix S6).
As with disease knowledge, there was a much greater number of studies showing that health insurance coverage and access to care are facilitators to cancer screening uptake for all tumor types [breast cancer, 31 out of 35 studies as a facilitator vs 5 out of 35 studies as a barrier; cervical cancer, 28 out of 33 studies as a facilitator vs 6 out of 33 studies as a barrier; CRC, 42 out of 46 studies as a facilitator vs 6 out of 46 studies as a barrier; lung cancer, 3 out of 3 studies as a facilitator vs 0 out of 3 studies as a barrier (Figure 4)]. This included gastric cancer and prostate cancer (Supplementary Appendix S6).
Across all tumor types there is a greater number of studies showing that access to care is a facilitator rather than a barrier (breast cancer, 13 out of 16 studies as a facilitator vs 4 out of 16 studies as a barrier; cervical cancer, 23 out of 26 studies as a facilitator vs 7 out of 26 studies as a barrier; CRC, 24 out of 28 studies as a facilitator vs 6 out of 28 studies as a barrier; lung cancer, 4 out of 5 studies as a facilitator vs 2 out of 5 studies as a barrier [Figure 4]). Similar findings were seen for prostate cancer; however, for gastric cancer, there were no studies reporting this as a factor influencing screening uptake (Supplementary Appendix S6).
A history of cancer screening increases subsequent cancer screening uptake, with more studies across all tumor types reporting this as a facilitator influencing a higher screening uptake (breast, 12 out of 15 studies; cervical, 13 out of 17 studies; CRC, 21 out of 24 studies; lung, 1 out of 1 study) as opposed to as a barrier [breast, 4 out of 15 studies; cervical, 5 out of 17 studies; CRC, 4 out of 24 studies; lung, 0 out of 1 study (Figure 4)]. Similar findings were seen for prostate cancer; however, for gastric cancer, there were no studies that reported a history of cancer screening as a factor which impacts screening uptake (Supplementary Appendix S6).
3.2.4 Patient behavior
There were a fewer number of studies that explored the relationship between patient behavior and cancer screening uptake compared with patient access (Figure 5). Patients with a positive attitude towards cancer screening was found to influence screening uptake [breast cancer, 2 out of 3 studies as a facilitator vs 1 out of 3 studies as a barrier; cervical cancer, 15 out of 17 studies as a facilitator vs 2 out of 17 studies as a barrier; CRC, 3 out of 5 studies as a facilitator vs 2 out of 5 studies as a barrier; no studies reported on patient attitude on the impact of lung cancer screening (Figure 5)]. No studies reported on the relationship between patient behavior and cancer screening in gastric and prostate cancers (Supplementary Appendix S6).
Moderate or high perceived cancer risk was identified as a patient behavior associated factor that generally facilitated cancer screening uptake across tumor types [breast cancer, 1 out of 1 studies as a facilitator vs 0 out of 1 studies as a barrier; cervical cancer, 7 out of 8 studies as a facilitator vs 1 out of 8 studies as a barrier; CRC, 8 out of 9 studies as a facilitator vs 2 out of 9 studies as a barrier; lung cancer, 3 out of 5 studies as a facilitator vs 2 out of 5 studies as a barrier (Figure 5)]. No studies were reported for gastric cancer and only one study identified perceived cancer risk as a factor influencing screening uptake in prostate cancer, reporting higher perceived cancer risk as a facilitator over a barrier (Supplementary Appendix S6).
The link between smoking and cancer screening is dependent on the tumor type (Figure 5). Breast cancer had the same number of studies identifying smoking as a barrier and facilitator (12 out of 22 studies). For screening programs targeting cervical and lung cancer, there were higher number of studies reporting smoking as a facilitator vs a barrier to screening uptake (17 studies vs 14 studies out of 27 studies assessing cervical cancer screening, and 6 studies vs 0 studies out of 6 studies evaluating lung cancer screening). However, for CRC screening programs, a greater number of studies identified smoking as a barrier vs facilitator to cancer screening uptake (21 out of 28 studies vs 11 out of 28 studies, respectively). Both gastric and prostate cancer had more studies identifying smoking as a barrier (Supplementary Appendix S6).
3.2.5 PCP access
PCP access, represented by the number of visits (lower vs higher) or recommendations on screening (received vs not received) from PCPs, can impact patient’s adherence to screening programs. A higher number of studies indicated that PCP recommendations for cancer screening and those patients who had access to PCP visits were factors facilitating cancer screening for all prioritized tumor types (Figure 6). Specifically, in breast cancer, 8 out of 9 studies found that PCP recommendations were a facilitator vs 2 out of 9 studies as a barrier, for cervical cancer, 22 out of 26 studies found that it was a facilitator vs 4 out of 26 studies as a barrier, for CRC, 21 out of 28 studies as a facilitator vs 9 out of 28 studies as a barrier, and for lung cancer, 3 out of 3 studies as a facilitator vs 1 out of 3 studies as a barrier. Similarly, gastric, and prostate cancer had a higher number of studies reporting PCP recommendations for screening as a facilitator rather than a barrier to cancer screening (Supplementary Appendix S6).
A higher number of PCP visits was also identified across reported studies as a factor associated with facilitating screening uptake rather than as a barrier to screening across all prioritized tumor types (Figure 6). In breast cancer it was reported that 10 out of 12 studies identified PCP visits as a facilitator vs 4 out of 12 studies as a barrier; cervical cancer 13 out of 17 studies identified this factor as a facilitator vs 4 out of 17 studies finding it to be a barrier, and 15 out of 16 studies on CRC found that PCP visits were a facilitator compared to 1 out of 16 studies where it was a barrier. For lung cancer, there were the same number of studies identifying PCP visits as a facilitator or as a barrier; 1 out of 2 as a facilitator and 1 out of 2 studies as a barrier. No studies were analyzed commenting on PCP visits as an influencing factor on screening for gastric and lung cancer (Supplementary Appendix S6).
3.2.6 Social factors
Various social factors may have an impact on individuals’ screening behavior. The number of children (at least one vs none), the number of sexual partners (more than 1 vs zero to one), or education (high or low) were the most frequently reported social factors impacting cancer screening. The number of sexual partners was a factor which was only assessed as either a facilitator or barrier to cancer screening uptake for cervical cancer (Figure 7), while the number of children reported as a facilitator or a barrier in studies focused on breast or cervical cancer only. In breast cancer, having one or more children was identified as a facilitator to screening in 4 out of 4 studies vs 1 out of 4 studies reporting it as a barrier. For cervical cancer, there were more studies that identified having at least one child and more than one sexual partner as facilitators (30 out of 39 studies and 12 out of 14 studies, respectively) rather than as barriers to cancer screening (15 out of 39 studies and 3 out of 14 studies, respectively; Figure 7). No studies assessing impact of the number of children or sexual partners on cancer screening were identified for gastric or prostate cancer (Supplementary Appendix S6).
In regard to education, breast, cervical and colorectal cancer all had more studies identifying higher education as a facilitator (62 out of 69 studies, 91 out of 111 studies, and 63 out of 74 studies, respectively) rather than a barrier (15 out of 69 studies, 30 out of 111 studies, and 15 out of 74 studies, respectively) to cancer screening (Figure 7). For lung cancer, there were 2 out of 4 studies that identified education as a facilitator vs 2 out of 4 studies that identified it as a barrier to cancer screening (Figure 7). Both gastric and prostate cancer studies also found higher education to be a facilitator to screening uptake (Supplementary Appendix S6).
3.2.7 Other factors
Across the included studies evaluating factors associated with screening for the tumor types assessed, other factors influencing cancer screening uptake that were captured in less than 10 studies were also identified (Figure 8). Some of these factors were identified as barriers to cancer screening, including country of birth (31–41), being a migrant (34, 42–47), not being engaged in physical activity (34, 44–47), sexual minority identification (i.e., being transgender, gay or lesbian) (48–50), having negative patients’ beliefs (51), experiencing discrimination (i.e., racial or other forms, such as age- or gender-based discrimination) (52–57), having unhealthy eating habits (52–54), and negative emotions and perceptions (including embarrassment, fear/anxiety, perceived stress, and perceived barriers to screening) (58–76).
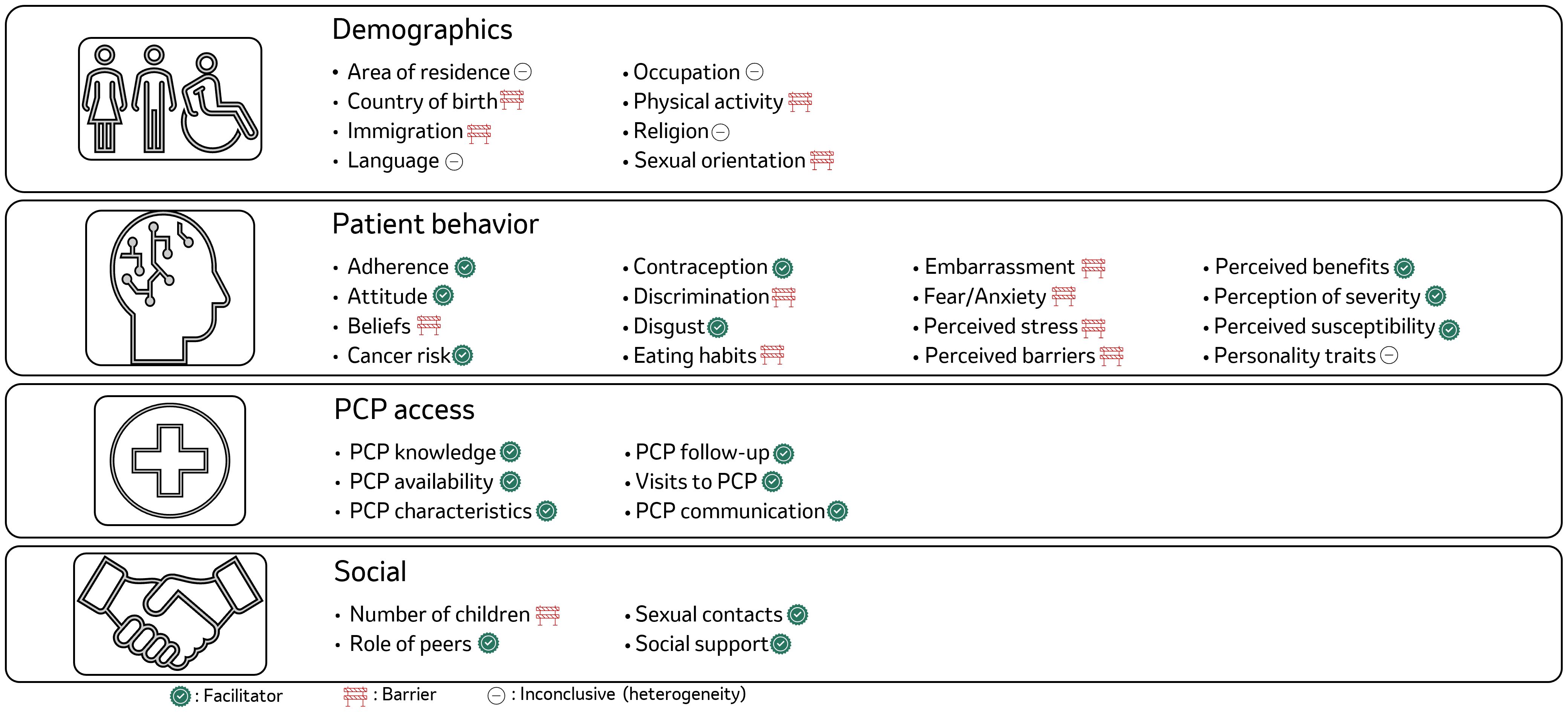
Figure 8. Qualitative summary of other barriers and facilitators to cancer screening uptake. Demographics are parameters that describe parameters from population perspective and impact the uptake of screening. Area of residence within this category includes factors such as country/place/region of residence, citizenship, nationality; Patients behavior includes parameters that were influenced by or were a direct result of people’s behavior; PCP access describes the hinderance associated with access to the PCP; Social barrier included the parameters that were related to society or its impact. For more information, refer to Supplementary Appendix S3.
There were other factors that were identified as facilitators to cancer screening, including: patients’ positive perception on treatment adherence, positive attitude to cancer screening (77, 78), an understanding of cancer risk (79), lack of disgust of the screening procedure (66, 69, 80), perceived benefits of cancer screening (61, 81–85), perception of disease severity (64, 85–89), perception of the patients’ susceptibility to developing cancer (61, 83–85), having peer support or other social support advocating for cancer screening (64, 85–89), along with PCP knowledge, availability, frequent follow-ups, and positive approach to PCP communication (90–92). Specific facilitators that increased the likelihood of cancer screening included having a high number of sexual contacts (61, 88, 93) and no history of oral contraceptive use (94) for cervical cancer screening.
In contrast, factors like area of residence (43, 95–105), specific language spoken and language proficiency (96–98), type of occupation (106), type of religion or belief systems (94, 107–109), and personality traits (101, 110) exhibited a more complex influence, functioning as either barriers or facilitators depending on specific circumstances.
3.3 Interventions to overcome barriers to screening
Interventions aimed at overcoming barriers mentioned in the identified studies have been summarized, where details of the studies are provided in Supplementary Appendix S5. Across all tumor types, targeted educational programs were the most frequently discussed strategy for increasing cancer screening uptake (cervical cancer: 12 studies (49, 111–118); CRC: 6 studies (119–124); breast cancer: 3 studies (49, 125, 126); lung cancer: 1 study (127); multiple cancers: 1 study across multiple cancers (128). These programs aimed to improve knowledge on cancer risks and the benefits of early detection, reaching patients through diverse channels such as community workshops, online resources, and multilingual brochures. Tailored education was determined to be essential for underrepresented groups who face unique barriers, addressing disparities in cancer screening participation across racial, linguistic, and socioeconomic differences. For instance, culturally sensitive educational content and language-specific materials can improve understanding and engagement in cancer screening among diverse communities (118, 122, 124). Another key intervention discussed across studies in multiple tumors was increasing patients’ and healthcare professionals’ awareness of cancer screening and the benefits of early detection of cancer (cervical cancer: 9 studies (129–132); breast cancer: 4 studies (49, 75, 112, 115, 130, 132–135); CRC: 2 studies (119, 122)), particularly on awareness campaigns focusing on educating patients and healthcare professionals alike about the importance of cancer screening, dispelling misconceptions, and reducing patients’ fear associated with screening. Health professionals, including nurses, pharmacists, and health educators, play a key role in communicating the benefits of screening and it is equally important to guide them in effective communication of their explanations and demonstrations to patients about cancer and its screening process (49, 130, 136).
Specific strategies to raise such awareness through social media and community networks serve as effective tools to support cancer screening by creating spaces for individuals to discuss, learn, and share experiences related to screening and were identified in a number of studies (cervical cancer: 9 studies (49, 75, 112, 115, 130, 132–135); breast cancer: 4 studies (129–132), CRC: 2 studies (119, 122)). Platforms that promote peer discussions, educational meetings, and patient support groups allow individuals to interact with healthcare professionals and peers who have undergone screening. Such community-driven approaches reduce anxiety, increase comfort, and facilitate informed decision-making. Programs using these methods have shown promise in increasing screening participation for cancers like breast cancer, cervical cancer, and CRC. In particular, for women, authors note that breast cancer awareness programs should include oral presentations in an aim to educate women about risks for developing cancer, reducing fears, encouraging screening, and improving relationships with their healthcare providers (131). Thereby, making breast cancer screening more approachable, highlighting the benefits of early diagnosis and ultimately increasing participation rates (125, 129, 131).
National cancer screening programs and targeted governmental policies are critical strategies to increase screening uptake and reduce healthcare disparities (lung cancer: 2 studies (127, 137)); breast cancer: 1 study ( (95)). National policies that ensure insurance coverage for screening, such as the Affordable Care Act (ACA) in the U.S., can help reduce racial and economic disparities in cancer screening access (95, 127, 137). One study in breast cancer suggests that these policies ensure consistent access to healthcare providers and provide patient navigation services to prevent individuals from being missed. Such interventions are expected to effectively promote breast cancer screening and contribute to the overall reduction of disparities in healthcare outcomes (95). Of the included studies, two proposed strategies included public health and policy interventions that take into account the environmental context, which may improve effectiveness and practicality compared to patient-level approaches (132, 138).
Incorporating screening as a standard of care within national health programs and providing patient navigation services may also enhance screening uptake, especially for underserved populations (95, 132, 138). To mitigate the effect of economic barriers, specifically insurance coverage on screening uptake, suggestions were made for covering lung cancer screening under national cancer screening programs (127, 137). In other studies, the use of lung cancer screening coordinators and tracking software was also suggested to improve adherence and timeliness of cancer evaluation, in turn increasing cancer screening uptake (139). Notably, these components are recommended by the American Thoracic Society and American College of Chest Physicians in lung cancer screening (139).
Moreover, for rural and remote communities, mobile screening units and extended clinic hours have been proposed as effective means to improve access to screening. Policies that promote transportation support, accessibility of screening equipment, and nationally coordinated training for providers are also crucial in addressing the structural barriers to screening (140, 141).
Lastly, disparities across multiple sub-groups were reported in a total of 4 studies covering individuals with disabilities (1 study (138), rural populations (1 study (132)), Hispanic communities (1 study (95)), and transgender participants (1 study (49)) and specific interventions were proposed to enhance adherence to screening in these population sub-groups. For women with severe disabilities and brain-related and/or mental disabilities, access to information and equipment, transport support and access to usual care was suggested. For transgender and cisgender participants, improvements in capturing gender identity demographics, training to prevent perceived personal bias, and patient education on the importance of natal anatomy, were suggested as interventions to improve screening uptake. The promotion of adequate healthcare insurance coverage across these populations, and custom interventions such as mobile screening services, extended-hour screening in for rural and deprived communities were suggested as mechanisms to improve access to screening and adherence (49, 95, 132, 138).
3.4 Risk of bias
According to the NOS used to assess the risk of bias of the included studies, there was a significant variability in the quality of studies across different tumor types. The proportion of high-quality studies identified for breast cancer, cervical cancer, CRC, lung cancer, prostate cancer and gastric cancer was 22%, 25%, 15%, 11%, 16% and 25%, respectively. Most studies were included in the medium quality category, with a total score of 4-6 on the NOS scale. It was the case for 149/199 (75%) for breast cancer, 203/278 (73%) for cervical cancer, 194/246 (79%) for CRC, 29/37 (76%%) for lung cancer, 32/38 (84%) for prostate cancer and 9/12 (75%) for gastric cancer. Among the included studies, lung cancer exhibited the highest proportion of low-quality studies (14%). Detailed results are presented in the Supplementary Appendix S7.
4 Discussion
To our knowledge, this is the first review to adopt a pan-tumor approach to identify the barriers and facilitators to cancer screening uptake across multiple major tumor types – breast, cervical, colorectal, and lung cancers. This review identified factors influencing screening uptake, including patient demographic characteristics, socioeconomic factors, access to care, primary care provider involvement, and patient health behaviors, among others. Given that national screening programs exist in numerous countries for these cancers (142–146), understanding common and tumor-specific barriers and facilitators to screening is essential for improving early detection and reducing cancer-related mortality (5–7).
4.1 Summary of findings
The findings confirm that age and perceived health status significantly influence screening uptake across multiple tumor types. Older adults, for instance, are more likely to participate in screening for breast, colorectal, and lung cancers due to established screening guidelines that target older adults (142–146). For cervical cancer, age-specific incidence rates typically rise from age 15-19 year group and peaking in the age 30-34 year group, and then decline in subsequent age groups (147). As such, there was an observed trend for cervical cancer screening uptake declining with age (148–150), as older age can be a potential barrier given that national screening programs may have an age cut-off screening threshold (142–146), and as post-menopausal women may feel less at risk or who are no longer regularly seeing gynecologists (151). Therefore, such results indicate that tumor type-specific interventions may be needed to address screening uptake barriers by different age groups. Additionally, individuals with worse health status scores are generally more likely to adhere to screening guidelines, which suggests that a perception of personal health risk may motivate screening behaviors. However, they may also feel less urgency to undergo regular screening, seeing themselves as low risk (36, 77, 152–155). Furthermore, those with poor health or comorbidities may be less willing to screen due to competing health priorities, or conversely, they may see screening as critical to their ongoing care (153, 154).
Behavioral factors, such as having a positive attitude, the perception of being at risk of developing cancer, and smoking, were identified as notable facilitators, particularly for cervical cancer (99, 134, 136, 156–161), CRC (40, 74, 124, 154, 162–171), and lung cancer screening (128, 137, 172–181), respectively. Lung cancer screening is recommended across a number of countries, including Australia, Japan, Germany, UK, and the US for high-risk populations, with high-risk status based on age and smoking history (number of packs per year) of the individual (9, 182–184). People with chronic respiratory conditions may be more inclined to screen for lung cancer, seeing it as directly relevant to their health (127, 177, 178, 185). Additionally, a lack of awareness and knowledge about cancer risks and the benefits of screening was a barrier to screening uptake that was common across all tumor types. This is consistent with previous research indicating that awareness campaigns and health literacy are vital in promoting cancer screening, especially in underserved populations (186). However, if awareness efforts increase anxiety or fears about potential results, this can paradoxically deter people from participating in cancer screening (187). Nevertheless, addressing these informational barriers is a priority to ensure that individuals understand the importance of timely screening and its role in early detection.
Socioeconomic factors, including income, employment status, and insurance coverage, were also strongly associated with disparities in screening uptake (188). Low-income individuals and those without adequate insurance face significant barriers to screening, underscoring the need for financial and policy-level interventions (188). This aligns with existing literature showing that affordability and insurance coverage remain critical in enabling equitable access to cancer screening (189). While low socioeconomic status often acts as a barrier due to limited access to resources or insurance, higher socioeconomic status can facilitate screening by providing financial means, health literacy, and easier access to care (139, 190, 191). Conversely, some high-income groups may skip screening due to overconfidence in their health or the perception that screening is unnecessary (109, 126).
System-level, provider-level, and community-level barriers frequently interact, compounding their impact on screening participation. In resource-limited settings, for example, inadequate funding and workforce shortages lead to fewer screening facilities and trained providers, directly reducing screening capacity and access, particularly for high-cost screenings, such as those for lung and colorectal cancers. Proximity to screening centers or mobile units facilitates screening, but long wait times, scheduling issues, or inconvenient locations can make access a barrier (43, 140, 141). Providers can be powerful facilitators when they encourage and remind patients about screenings. However, lack of a strong recommendation from a provider often leads to low screening, effectively making the absence of provider engagement a barrier to screening uptake (113, 129, 192–197). Simplifying logistics often turns this barrier into a facilitator (198–205). This complex interplay underscores the need for multi-level, coordinated strategies to address these layered barriers.
Potential interventions to mitigate these barriers were identified across included studies, focusing on the roles of patient awareness, social support, and provider training. Building supportive networks for screening discussions, promoting awareness through diverse media channels, and improving provider-patient communication can foster a more supportive environment for screening uptake (129–132, 206). Healthcare providers play a central role in influencing patient decisions regarding screening; thus, interventions that improve provider skills in explaining the benefits of screening may help address patient concerns and reduce screening hesitancy (113, 129, 192–197).
Implementing tailored interventions is also critical to addressing unique barriers faced by vulnerable groups, including rural populations, ethnic minorities, and the LGBTQ+ community (23, 207, 208). For example, mobile screening units can increase access in rural areas where geographic distance is a barrier (140, 141). Linguistically and culturally adapted educational materials benefit specific populations, such as Hispanic communities, by ensuring that language and cultural values are respected (118, 122, 124, 209). Additionally, training providers in culturally competent care is essential to improve screening experiences for ethnic minorities and transgender individuals, who may face unique barriers due to stigma, lack of insurance coverage, or previous negative healthcare experiences (49, 95, 210). By prioritizing these tailored approaches, healthcare systems can more effectively promote equitable access to cancer screening for all individuals.
4.2 Strengths and limitations
To our knowledge, this is the first systematic review providing a broad, comparative understanding of common and unique barriers to cancer screening uptake. This study took a comprehensive approach by examining an extensive set of barriers across multiple tumor types, and identifying overlapping factors, such as socioeconomic status or provider influence. It also highlighted where interventions can be applied universally or need to be customized by tumor type. For the purpose of presenting the results, facilitators were interpreted alongside barriers. While the primary emphasis of the SLR was on studies reporting barriers to screening uptake, the identification of facilitators was deduced indirectly to include the full spectrum of factors.
However, due to the large amount of evidence identified during the searches, it was necessary for the review to focus on key themes observed in the literature, specifically, demographics, economic factors, patient behavior, PCP access, and social factors. Therefore, despite the broad inclusion criteria, it is important to note that alternative categorizations of factors contributing to cancer screening uptake could have yielded different insights or emphases in the reported findings. Additionally, although no restrictions were placed on tumor types, four key malignancies were selected for the purpose of reporting, including: breast cancer, cervical cancer, CRC, and lung cancer. These tumor types were prioritized based on the number of available studies and the existence of well-established screening programs.
Since the searches were limited to those published from 2012 to 2022, certain factors previously identified and included in studies published prior to 2012 may not have been captured. Furthermore, as the included studies were conducted in a variety of patient populations, some inter-study comparisons were limited due to the heterogeneity in study methodologies. It is also important to note that interventions to improve cancer screening uptake were not the primary objective of the study and those identified were from studies that focused on barriers to screening. As such, the study selection process for the studies that included information regarding interventions to overcome barriers to cancer screening was not systematic and only those studies that provided comprehensive details were selected for further analysis. This may have led to selection bias and there are likely to be additional studies not captured in the search that may report on other interventions. Additionally, any studies that reported on the effectiveness of the interventions were not captured, since assessing the impact of the interventions was not one of the study objectives.
While this review provides valuable insights into barriers to cancer screening uptake from the patient and healthcare practitioner (HCP) perspective, for example, it is important to acknowledge that the findings may not encompass all perspectives that could influence screening behaviors.
Additionally, the varying number of studies available for different cancer types (for example 37 for lung cancer to 278 for cervical cancer) represents a limitation in the available data. While this imbalance reflects the current state of research across different cancer screening programs, it may impact the depth and breadth of insights for less-studied cancer types. However, the consistency of factors identified across cancer types suggests that our findings remain robust despite this limitation.
Our study identified age as a potential barrier; however, evidence on age as a barrier requires careful interpretation. Screening guidelines by age ranges in adults differ across countries and cancer types. Some studies provided OR for age ranges outside the recommended screening thresholds, without accounting for country-specific screening age requirements. Lower screening rates outside these recommended ranges may reflect adherence to evidence-based guidelines rather than true barriers. Regarding this aspect, our review was limited in distinguishing between appropriate age-based screening practices and actual uptake barriers. Future research should more precisely delineate age-related barriers within the context of established guidelines and explore evidence for screening in age groups traditionally considered low-risk.
It should also be mentioned that interpretation of the results may be biased by ecological fallacy, in particular other factors or a set of different factors than those presented in this study might have an impact on patients’ behavior towards cancer screening. Therefore, caution is recommended when drawing conclusions from population-level data, and where feasible, individual patient-level data should be considered in future research to provide a more nuanced understanding of the results, while acknowledging that studies are often focused on a limited set of factors influencing screening behaviors. While our study focused on individual factors affecting cancer screening uptake, future research should explore potential interactions among these factors. For instance, investigating how economic and social factors might jointly influence screening participation could provide more nuanced insights and inform more targeted interventions. Future research should also explore the potential of artificial intelligence (AI) and machine learning in improving cancer screening uptake. AI could be leveraged to analyze patient medical data and provide personalized screening recommendations or risk profiles, implement automated reminder systems, and develop targeted outreach programs for areas with low screening rates. AI can be leveraged and developed into tools for medical decision making in the clinic, utilizing ML-based prediction models that help identify factors predictive of early stage cancer. Additionally, AI-enhanced patient education tools could be developed to improve understanding and engagement with screening programs.
Quality assurance using the NOS revealed a substantial number of medium and high-quality studies, especially in breast, cervical, and colorectal cancers, indicative of a robust foundation for evidence- based conclusions in these areas. However, significant methodological concerns across both low and medium-quality studies were also revealed, which represented the majority of the evidence base for lung cancer. Common deficiencies included lack of comparability between groups, insufficient information on selection of non-exposed cohorts or control groups, inadequate follow-up procedures, and reliance on self-reported data. These findings should be kept in mind when interpreting and generalizing the findings, particularly for tumor types with a higher proportion of low-quality studies. Additionally, while the NOS scale provided a standardized assessment of study quality, our review process revealed additional methodological considerations. Many factors influencing cancer screening uptake are interdependent, and this complexity is not always fully addressed in individual studies. Furthermore, there may be additional factors influencing screening behavior that were not consistently researched or accounted for across studies. The presence of potential confounding factors, which vary across different contexts, adds another layer of complexity to interpreting and generalizing results. These observations highlight the need for more comprehensive and nuanced approaches in future research on cancer screening uptake.
4.3 Implications to clinical practice and research
The interchangeable nature of barriers and facilitators across multiple tumor types has significant implications for healthcare, particularly in designing and implementing screening programs. Firstly, recognizing that a factor can act as a barrier for one tumor type, but a facilitator for another suggests that screening programs must be tailored to the specific context of each cancer. Generalized approaches may not be effective; healthcare providers should employ cancer-specific strategies that account for the unique perceptions, risks, and motivators of each tumor type. Secondly, given that factors like age, socioeconomic status, and cultural attitudes affect different cancers in varied ways, interventions must be tailored not only by tumor type, but also by demographics. For instance, older populations may need reassurance about the importance of cervical screening post-menopause, while younger populations might need more encouragement to consider lung cancer screening if they are at high risk. Finally, the variability in barriers and facilitators suggests that multi-level approaches combining patient-level, provider-level, and system-level interventions, may be more effective. Health systems should consider integrating community engagement, social support mechanisms, customized patient education initiatives along with healthcare provider training, and policy changes, such as expanding insurance coverage to bring equity to screening access, to target the full range of barriers across tumor types and demographics. Close collaboration between governments and healthcare providers, along with patient advocacy groups will be necessary to optimize their implementation; however, further research will first be required to assess cost-effectiveness and determine which interventions would offer the most effective use of finite resources.
The comprehensive analysis of barriers and facilitators to cancer screening presented in this review could serve as a foundation for developing a conceptual framework for cancer screening. Such a framework would not only guide the design of tailored, population-specific screening strategies but also inform the creation of cross-cutting, multi-cancer screening programs. By systematically addressing the various factors influencing screening uptake identified in this review and their interdependence, this conceptual framework could significantly impact screening participation rates and, ultimately, lead to earlier cancer detection and improved patient outcomes.
4.4 Conclusion
Barriers to cancer screening across multiple tumor types are complex, spanning demographic and patient-level factors, social and economic factors, provider and community challenges, and access to health care. While certain barriers are shared across tumor types, others are unique, reflecting the specific requirements of screening for different tumors. Addressing these barriers requires multi-level strategies that integrate both universal and cancer-specific approaches. Targeted interventions and supportive policies can increase screening participation, facilitate earlier cancer diagnosis, and reduce disparities in cancer outcomes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
RA-I: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Resources. YM: Data curation, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, Formal analysis. SS: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing, Data curation, Formal analysis. RC: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing, Software. EC: Data curation, Formal analysis, Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing, Software.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The authors declare that this study received funding from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The authors would like to acknowledge the editorial and medical writing support provided by Natalie Ong, Adam Hall, Rui Cai, Riccardo Ressa, and Justyna Tomassy (Parexel International) in the development of this manuscript.
Conflict of interest
Author RA-I was employed by Merck Canada Inc. Author YM was employed by Merck & Co., Inc. Authors SS, RC and EC were employed by Parexel International.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1575820/full#supplementary-material
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
2. WHO. Guide to cancer early diagnosis(2017). Available online at: https://iris.who.int/bitstream/handle/10665/254500/9789241511940-eng.pdf?sequence=1 (Accessed November 27, 2014).
3. World Health Organization (WHO). Cancer control: Early detection(2006). Available online at: https://www.who.int/publications/i/item/9789241547338 (Accessed November 27, 2014).
4. World Health Organisation. A short guide to cancer screening. Increase effectiveness, maximize benefits and minimize harm(2022). Available online at: https://iris.who.int/bitstream/handle/10665/351396/9789289057561-eng.pdf (Accessed November 27, 2014).
5. Henschke CI, Yip R, Shaham D, Markowitz S, Cervera Deval J, Zulueta JJ, et al. A 20-year follow-up of the international early lung cancer action program (I-ELCAP). Radiology. (2023) 309:e231988. doi: 10.1148/radiol.231988
6. Knudsen AB, Trentham-Dietz A, Kim JJ, Mandelblatt JS, Meza R, Zauber AG, et al. Estimated US cancer deaths prevented with increased use of lung, colorectal, breast, and cervical cancer screening. JAMA Network Open. (2023) 6:e2344698–e. doi: 10.1001/jamanetworkopen.2023.44698
7. Philipson TJ, Durie T, Cong Z, and Fendrick AM. The aggregate value of cancer screenings in the United States: full potential value and value considering adherence. BMC Health Serv Res. (2023) 23:829. doi: 10.1186/s12913-023-09738-4
8. Smith RA, Andrews KS, Brooks D, Fedewa SA, Manassaram-Baptiste D, Saslow D, et al. Cancer screening in the United States, 2019: A review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. (2019) 69:184–210. doi: 10.3322/caac.21557
9. Association AL. Lung cancer key findings(2024). Available online at: https://www.lung.org/research/state-of-lung-cancer/key-findings (Accessed November 7, 2024).
10. WHO. Screening programmes: a short guide. Increase effectiveness, maximize benefits and minimize harm(2020). Available online at: https://iris.who.int/bitstream/handle/10665/330829/9789289054782-eng.pdf (Accessed November 7, 2024).
11. Bednarczyk RA, Chamberlain A, Mathewson K, Salmon DA, and Omer SB. Practice-, Provider-, and Patient-level interventions to improve preventive care: Development of the P3 Model. Prev Med Rep. (2018) 11:131–8. doi: 10.1016/j.pmedr.2018.06.009
12. Zhu X, Weiser E, Jacobson DJ, Griffin JM, Limburg PJ, and Finney Rutten LJ. Provider-perceived barriers to patient adherence to colorectal cancer screening. Prev Med Rep. (2022) 25:101681. doi: 10.1016/j.pmedr.2021.101681
13. Sedani AE, Davis OC, Clifton SC, Campbell JE, and Chou AF. Facilitators and barriers to implementation of lung cancer screening: A framework-driven systematic review. J Natl Cancer Inst. (2022) 114:1449–67. doi: 10.1093/jnci/djac154
14. Carter-Harris L and Gould MK. Multilevel barriers to the successful implementation of lung cancer screening: why does it have to be so hard? Ann Am Thorac Soc. (2017) 14:1261–5. doi: 10.1513/AnnalsATS.201703-204PS
15. Stang A and Jöckel K-H. The impact of cancer screening on all-cause mortality. Deutsches Aerzteblatt Online. (2018) 115(29-30):481–6. doi: 10.3238/arztebl.2018.0481
16. Zielonke N, Gini A, Jansen EEL, Anttila A, Segnan N, Ponti A, et al. Evidence for reducing cancer-specific mortality due to screening for breast cancer in Europe: A systematic review. Eur J Cancer. (2020) 127:191–206. doi: 10.1016/j.ejca.2019.12.010
17. Ramjan L, Cotton A, Algoso M, and Peters K. Barriers to breast and cervical cancer screening for women with physical disability: A review. Women Health. (2016) 56:141–56. doi: 10.1080/03630242.2015.1086463
18. Haviland KS, Swette S, Kelechi T, and Mueller M. Barriers and facilitators to cancer screening among LGBTQ individuals with cancer. Oncol Nurs Forum. (2020) 47:44–55. doi: 10.1188/20.Onf.44-55
19. Guessous I, Dash C, Lapin P, Doroshenk M, Smith RA, and Klabunde CN. Colorectal cancer screening barriers and facilitators in older persons. Prev Med. (2010) 50:3–10. doi: 10.1016/j.ypmed.2009.12.005
20. Pedrós Barnils N, Härtling V, Singh H, and Schüz B. Sociodemographic inequalities in breast cancer screening attendance in Germany following the implementation of an Organized Screening Program: Scoping Review. BMC Public Health. (2024) 24:2211. doi: 10.1186/s12889-024-19673-6
21. Jerome-D’Emilia B, Gachupin FC, and Suplee PD. A systematic review of barriers and facilitators to mammography in american Indian/alaska native women. J Transcult Nurs. (2019) 30:173–86. doi: 10.1177/1043659618793706
22. Puli AV, Lussiez A, MacEachern M, Hayward L, Dualeh S, Richburg CE, et al. Barriers to colorectal cancer screening in US immigrants: A scoping review. J Surg Res. (2023) 282:53–64. doi: 10.1016/j.jss.2022.08.024
23. Chan DNS, Law BMH, Au DWH, So WKW, and Fan N. A systematic review of the barriers and facilitators influencing the cancer screening behaviour among people with intellectual disabilities. Cancer Epidemiol. (2022) 76:102084. doi: 10.1016/j.canep.2021.102084
24. Karran EL, Grant AR, Lee H, Kamper SJ, Williams CM, Wiles LK, et al. Do health education initiatives assist socioeconomically disadvantaged populations? A systematic review and meta-analyses. BMC Public Health. (2023) 23:453. doi: 10.1186/s12889-023-15329-z
25. Bongaerts TH, Büchner FL, Middelkoop BJ, Guicherit OR, and Numans ME. Determinants of (non-)attendance at the Dutch cancer screening programmes: A systematic review. J Med Screen. (2020) 27:121–9. doi: 10.1177/0969141319887996
26. Julian Higgins JT, Chandler J, Cumpston M, Li T, Page M, and Welch V. Cochrane handbook for systematic reviews of interventions version 6.5 (2024). Available online at: https://training.cochrane.org/handbook/current (Accessed November 7, 2024).
27. University of York. Centre for reviews and dissemination; systematic reviews. (2009). Available online at: https://www.york.ac.uk/crd/guidance/ (Accessed November 7, 2024).
28. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
29. Larg A and Moss JR. Cost-of-illness studies: a guide to critical evaluation. Pharmacoeconomics. (2011) 29:653–71. doi: 10.2165/11588380-000000000-00000
30. Aguiar-Ibáñez R, Sharma S, Tomassy J, Puppala M, and Aktan G. EPH136 available screening programs for the early identification of cancers: A targeted literature review. Value Health. (2023) 26:S188–S9. doi: 10.1016/j.jval.2023.03.1018
31. Lofters AK, Ng R, and Lobb R. Primary care physician characteristics associated with cancer screening: a retrospective cohort study in Ontario, Canada. Cancer Med. (2015) 4:212–23. doi: 10.1002/cam4.358
32. Leung J, McKenzie S, Martin J, Dobson A, and McLaughlin D. Longitudinal patterns of breast cancer screening: mammography, clinical, and breast self-examinations in a rural and urban setting. Women’s Health Issues. (2014) 24:e139–e46. doi: 10.1016/j.whi.2013.11.005
33. Dallo FJ and Kindratt TB. Disparities in vaccinations and cancer screening among US-and foreign-born Arab and European American non-Hispanic White women. Women’s Health Issues. (2015) 25:56–62. doi: 10.1016/j.whi.2014.10.002
34. Drolet M, Boily M-C, Greenaway C, Deeks SL, Blanchette C, Laprise J-F, et al. Sociodemographic inequalities in sexual activity and cervical cancer screening: implications for the success of human papillomavirus vaccination. Cancer Epidemiology Biomarkers Prev. (2013) 22:641–52. doi: 10.1158/1055-9965.EPI-12-1173
35. Cofie LE, Hirth JM, and Wong R. Chronic comorbidities and cervical cancer screening and adherence among US-born and foreign-born women. Cancer Causes Control. (2018) 29:1105–13. doi: 10.1007/s10552-018-1084-2
36. Xie Z, Chen G, Suk R, Dixon B, Jo A, and Hong Y-R. Limited English proficiency and screening for cervical, breast, and colorectal cancers among Asian American adults. J Racial Ethnic Health Disparities. (2023) 10:977–85. doi: 10.1007/s40615-022-01285-8
37. Calo WA, Vernon SW, Lairson DR, and Linder SH. Associations between contextual factors and colorectal cancer screening in a racially and ethnically diverse population in Texas. Cancer Epidemiol. (2015) 39:798–804. doi: 10.1016/j.canep.2015.09.012
38. Shariff-Marco S, Breen N, Stinchcomb DG, and Klabunde CN. Multilevel predictors of colorectal cancer screening use in California. Am J Managed Care. (2013) 19:205.
39. Lee HY, Beltran R, Kim NK, and Lee DK. Racial disparities in cervical cancer screening: Implications for relieving cervical cancer burden in Asian American Pacific Islander women. Cancer Nursing. (2019) 42:458–67. doi: 10.1097/NCC.0000000000000642
40. Courtney RJ, Paul CL, Sanson-Fisher RW, Macrae FA, Carey ML, Attia J, et al. Individual-and provider-level factors associated with colorectal cancer screening in accordance with guideline recommendation: a community-level perspective across varying levels of risk. BMC Public Health. (2013) 13:1–10. doi: 10.1186/1471-2458-13-248
41. Idowu KA, Adenuga B, Otubu O, Narasimhan K, Kamara F, Hunter-Richardson F, et al. Place of birth, cancer beliefs and being current with colon cancer screening among US adults. Ann Gastroenterology: Q Publ Hellenic Soc Gastroenterology. (2016) 29:336. doi: 10.20524/aog.2016.0040
42. Martín-López R, Jiménez-García R, Lopez-de-Andres A, Hernández-Barrera V, Jiménez-Trujillo I, Gil-de-Miguel A, et al. Inequalities in uptake of breast cancer screening in Spain: analysis of a cross-sectional national survey. Public Health. (2013) 127:822–7. doi: 10.1016/j.puhe.2013.03.006
43. Lofters AK, Kopp A, Vahabi M, and Glazier RH. Understanding those overdue for cancer screening by five years or more: a retrospective cohort study in Ontario, Canada. Prev Med. (2019) 129:105816. doi: 10.1016/j.ypmed.2019.105816
44. Aminisani N, Armstrong BK, and Canfell K. Cervical cancer screening in Middle Eastern and Asian migrants to Australia: a record linkage study. Cancer Epidemiol. (2012) 36:e394–400. doi: 10.1016/j.canep.2012.08.009
45. Brzoska P, Aksakal T, and Yilmaz-Aslan Y. Utilization of cervical cancer screening among migrants and non-migrants in Germany: results from a large-scale population survey. BMC Public Health. (2020) 20:1–9. doi: 10.1186/s12889-019-8006-4
46. Grillo F, Vallée J, and Chauvin P. Inequalities in cervical cancer screening for women with or without a regular consulting in primary care for gynaecological health, in Paris, France. Prev Med. (2012) 54:259–65. doi: 10.1016/j.ypmed.2012.01.013
47. Rondet C, Lapostolle A, Soler M, Grillo F, Parizot I, and Chauvin P. Are immigrants and nationals born to immigrants at higher risk for delayed or no lifetime breast and cervical cancer screening? The results from a population-based survey in Paris metropolitan area in 2010. PloS One. (2014) 9:e87046. doi: 10.1371/journal.pone.0087046
48. Kiran T, Davie S, Singh D, Hranilovic S, Pinto AD, Abramovich A, et al. Cancer screening rates among transgender adults: cross-sectional analysis of primary care data. Can Family Physician. (2019) 65:e30–e7.
49. Oladeru OT, Ma SJ, Miccio JA, Wang K, Attwood K, Singh AK, et al. Breast and cervical cancer screening disparities in transgender people. Am J Clin Oncol. (2022) 45:116–21. doi: 10.1200/JCO.2020.38.15-suppl.7024
50. Charkhchi P, Schabath MB, and Carlos RC. Modifiers of cancer screening prevention among sexual and gender minorities in the behavioral risk factor surveillance system. J Am Coll Radiology. (2019) 16:607–20. doi: 10.1016/j.jacr.2019.02.042
51. Tapera O, Kadzatsa W, Nyakabau A, Mavhu W, Dreyer G, Stray-Pedersen B, et al. Sociodemographic inequities in cervical cancer screening, treatment and care amongst women aged at least 25 years: evidence from surveys in Harare, Zimbabwe. BMC Public Health. (2019) 19:1–12. doi: 10.1186/s12889-019-6749-6
52. Marques P, Geraldes M, Gama A, Heleno B, and Dias S. Non-attendance in cervical cancer screening among migrant women in Portugal: A cross-sectional study. Women’s Health. (2022) 18:17455057221093034. doi: 10.1177/17455057221093034
53. Jacobs EA, Rathouz PJ, Karavolos K, Everson-Rose SA, Janssen I, Kravitz HM, et al. Perceived discrimination is associated with reduced breast and cervical cancer screening: the Study of Women’s Health Across the Nation (SWAN). J Women’s Health. (2014) 23:138–45. doi: 10.1089/jwh.2013.4328
54. Johnson MJ, Mueller M, Eliason MJ, Stuart G, and Nemeth LS. Quantitative and mixed analyses to identify factors that affect cervical cancer screening uptake among lesbian and bisexual women and transgender men. J Clin Nurs. (2016) 25:3628–42. doi: 10.1111/jocn.13414
55. Seay J, Ranck A, Weiss R, Salgado C, Fein L, and Kobetz E. Understanding transgender men’s experiences with and preferences for cervical cancer screening: a rapid assessment survey. LGBT Health. (2017) 4:304–9. doi: 10.1089/lgbt.2016.0143
56. Valdovinos C, Penedo FJ, Isasi CR, Jung M, Kaplan RC, Espinoza Giacinto R, et al. Perceived discrimination and cancer screening behaviors in us Hispanics: the Hispanic community health study/study of Latinos sociocultural ancillary study. Cancer Causes Control. (2016) 27:27–37. doi: 10.1007/s10552-015-0679-0
57. Mayhand KN, Handorf EA, Ortiz AG, Gonzalez ET, Devlin A, Sorice KA, et al. Effect of neighborhood and individual-level socioeconomic factors on colorectal cancer screening adherence. Int J Environ Res Public Health. (2021) 18:4398. doi: 10.3390/ijerph18094398
58. Lyimo FS and Beran TN. Demographic, knowledge, attitudinal, and accessibility factors associated with uptake of cervical cancer screening among women in a rural district of Tanzania: three public policy implications. BMC Public Health. (2012) 12:1–8. doi: 10.1186/1471-2458-12-22
59. Jones SM, Schuler TA, Padamsee TJ, and Andersen MR. Financial anxiety is associated with cancer screening adherence in women at high risk of breast cancer. Ann Behav Med. (2021) 55:1241–5. doi: 10.1093/abm/kaab010
60. Mboineki JF, Wang P, Dhakal K, Getu MA, Millanzi WC, and Chen C. Predictors of uptake of cervical cancer screening among women in Urban Tanzania: community-based cross-sectional study. Int J Public Health. (2020) 65:1593–602. doi: 10.1007/s00038-020-01515-y
61. Bou-Orm I, Sakr R, and Adib S. Cervical cancer screening among Lebanese women. Rev d’epidemiologie sante publique. (2018) 66:1–6. doi: 10.1016/j.respe.2017.10.004
62. Visanuyothin S, Chompikul J, and Mongkolchati A. Determinants of cervical cancer screening adherence in urban areas of Nakhon Ratchasima Province, Thailand. J Infection Public Health. (2015) 8:543–52. doi: 10.1016/j.jiph.2015.04.018
63. Nwabichie CC, Manaf RA, and Ismail SB. Factors affecting uptake of cervical cancer screening among African women in Klang Valley, Malaysia. Asian Pacific J Cancer Prev. (2018) 19:825. doi: 10.22034/APJCP.2018.19.3.825
64. Destaw A, Midaksa M, Addissie A, Kantelhardt EJ, and Gizaw M. Cervical cancer screening “see and treat approach”: real-life uptake after invitation and associated factors at health facilities in Gondar, Northwest Ethiopia. BMC Cancer. (2021) 21:1–9. doi: 10.1186/s12885-021-08761-0
65. Desta AA, Endale ZM, and Aklil MB. Cervical cancer screening utilization and associated factors among women of 30–65 years in Girar Jarsoo district North shoa, Ethiopia, 2021. Clin Epidemiol Global Health. (2022) 15:101048. doi: 10.1016/j.cegh.2022.101048
66. Hughes AG, Watanabe-Galloway S, Schnell P, and Soliman AS. Rural–urban differences in colorectal cancer screening barriers in Nebraska. J Community Health. (2015) 40:1065–74. doi: 10.1007/s10900-015-0032-2
67. Bocci G, Troiano G, Messina G, Nante N, and Civitelli S. Factors that could influence women’s participation in colorectal cancer screening: an Italian study. Ann Ig. (2017) 29:151–60. doi: 10.7416/ai.2017.2142
68. Molina-Barceló A, Salas-Trejo D, Peiró-Perez R, Vanaclocha M, Pérez E, and Castán S. Reasons for participating in the Valencian Community Colorectal Cancer Screening Programme by gender, age, and social class. Rev Esp Enferm Dig. (2014) 106:439–47. doi: 1130-0108/2014/106/7/439-447
69. Clarke N, Kearney PM, Gallagher P, McNamara D, O’Morain CA, and Sharp L. Negative emotions and cancer fatalism are independently associated with uptake of Faecal Immunochemical Test-based colorectal cancer screening: Results from a population-based study. Prev Med. (2021) 145:106430. doi: 10.1016/j.ypmed.2021.106430
70. Takeuchi E, Kim Y, Shaffer KM, Cannady RS, and Carver CS. Fear of cancer recurrence promotes cancer screening behaviors among family caregivers of cancer survivors. Cancer. (2020) 126:1784–92. doi: 10.1002/cncr.32701
71. Bynum SA, Davis JL, Green BL, and Katz RV. Unwillingness to participate in colorectal cancer screening: examining fears, attitudes, and medical mistrust in an ethnically diverse sample of adults 50 years and older. Am J Health Promotion. (2012) 26:295–300. doi: 10.4278/ajhp.110113-QUAN-20
72. Mastrokostas A, Gavana M, Gkrizioti M, Smyrnakis E, Cholongitas E, Benos A, et al. Discrepancies and misconceptions of perceived colorectal cancer screening barriers between primary health professionals and unscreened population. A comparative study in Greece. Perspective. (2018) 23:67–76.
73. Cam NB, Lee YY, Yoon H, Suh M, Park B, Jun JK, et al. Intentions to undergo lung cancer screening among Korean men. Asian Pacific J Cancer Prev. (2015) 16:6293–8. doi: 10.7314/apjcp.2015.16.15.6293
74. Choi E, Lee YY, Suh M, Park B, Jun JK, Kim Y, et al. Associations of perceived risk and cancer worry for colorectal cancer with screening behaviour. J Health Psychol. (2018) 23:840–52. doi: 10.1177/1359105316679721
75. Idowu A, Olowookere SA, Fagbemi AT, and Ogunlaja OA. Determinants of cervical cancer screening uptake among women in Ilorin, North Central Nigeria: a community-based study. J Cancer Epidemiol. (2016) 2016:6469240. doi: 10.1155/2016/6469240
76. Wong RK, Wong ML, Chan YH, Feng Z, Wai CT, and Yeoh KG. Gender differences in predictors of colorectal cancer screening uptake: a national cross sectional study based on the health belief model. BMC Public Health. (2013) 13:1–12. doi: 10.1186/1471-2458-13-677
77. Donnelly TT, Al Khater A-H, Al-Bader SB, Al Kuwari MG, Al-Meer N, Malik M, et al. Beliefs and attitudes about breast cancer and screening practices among Arab women living in Qatar: a cross-sectional study. BMC Women’s Health. (2013) 13:1–16. doi: 10.1186/1472-6874-13-49
78. Mo PKH, Mak WWS, Chong ESK, Shen H, and Cheung RYM. The prevalence and factors for cancer screening behavior among people with severe mental illness in Hong Kong. PloS One. (2014) 9:e107237. doi: 10.1371/journal.pone.0107237
79. Donley T, Tshiswaka DI, Blanc J, Seixas A, Okafor A, and Mbizo J. Differences in breast and cervical cancer screening among US women by nativity and family history. Am J Prev Med. (2020) 59:578–87. doi: 10.1016/j.amepre.2020.05.018
80. Harder E, Thomsen LT, Hertzum-Larsen R, Albieri V, Hessner MV, Juul KE, et al. Determinants for participation in human papillomavirus self-sampling among nonattenders to cervical cancer screening in Denmark. Cancer Epidemiology Biomarkers Prev. (2018) 27:1342–51. doi: 10.1158/1055-9965.EPI-18-0480
81. Tsunematsu M, Kawasaki H, Masuoka Y, and Kakehashi M. Factors affecting breast cancer screening behavior in Japan-assessment using the health belief model and conjoint analysis. Asian Pacific J Cancer Prev. (2013) 14:6041–8. doi: 10.7314/APJCP.2013.14.10.6041
82. Gang M, Kim JI, Oh KO, Li CY, and Song Y. Factors associated with mammography adherence among married Chinese women in Yanbian, China. Asian Pacific J Cancer Prev. (2013) 14:7207–13. doi: 10.7314/apjcp.2013.14.12.7207
83. Babazadeh T, Nadrian H, Rezakhani Moghaddam H, Ezzati E, Sarkhosh R, and Aghemiri S. Cognitive determinants of cervical cancer screening behavior among housewife women in Iran: An application of Health Belief Model. Health Care Women Int. (2018) 39:555–70. doi: 10.1080/07399332.2018.1425873
84. Solomon K, Tamire M, and Kaba M. Predictors of cervical cancer screening practice among HIV positive women attending adult anti-retroviral treatment clinics in Bishoftu town, Ethiopia: the application of a health belief model. BMC Cancer. (2019) 19:1–11. doi: 10.1186/s12885-019-6171-6
85. Ebu NI and Ogah JK. Predictors of cervical cancer screening intention of HIV-positive women in the central region of Ghana. BMC Women’s Health. (2018) 18:1–7. doi: 10.1186/s12905-018-0534-z
86. Eshete M, Abdulwuhab Atta M, and Yeshita HY. Cervical cancer screening acceptance among women in Dabat district, Northwest Ethiopia, 2017: an institution-based cross-sectional study. Obstetrics Gynecology Int. (2020) 2020:2805936. doi: 10.1155/2020/2805936
87. Nigussie T, Admassu B, and Nigussie A. Cervical cancer screening service utilization and associated factors among age-eligible women in Jimma town using health belief model, South West Ethiopia. BMC Women’s Health. (2019) 19:1–10. doi: 10.1186/s12905-019-0826-y
88. Bayu H, Berhe Y, Mulat A, and Alemu A. Cervical cancer screening service uptake and associated factors among age eligible women in Mekelle Zone, Northern Ethiopia, 2015: a community based study using health belief model. PloS One. (2016) 11:e0149908. doi: 10.1371/journal.pone.0149908
89. Chisale Mabotja M, Levin J, and Kawonga M. Beliefs and perceptions regarding cervical cancer and screening associated with Pap smear uptake in Johannesburg: A cross-sectional study. PloS One. (2021) 16:e0246574. doi: 10.1371/journal.pone.0246574
90. Bhandari D, Shibanuma A, Kiriya J, Hirachan S, Ong KIC, and Jimba M. Factors associated with breast cancer screening intention in Kathmandu Valley, Nepal. PloS One. (2021) 16:e0245856. doi: 10.1371/journal.pone.0245856
91. Gilfoyle M, Garcia J, Chaurasia A, and Oremus M. Perceived susceptibility to developing cancer and mammography screening behaviour: a cross-sectional analysis of Alberta’s Tomorrow Project. Public Health. (2019) 177:135–42. doi: 10.1016/j.puhe.2019.08.004
92. Ngan TT, Jenkins C, Minh HV, Donnelly M, and O’Neill C. Breast cancer screening practices among Vietnamese women and factors associated with clinical breast examination uptake. PloS One. (2022) 17:e0269228. doi: 10.1371/journal.pone.0269228
93. Erku DA, Netere AK, Mersha AG, Abebe SA, Mekuria AB, and Belachew SA. Comprehensive knowledge and uptake of cervical cancer screening is low among women living with HIV/AIDS in Northwest Ethiopia. Gynecologic Oncol Res Practice. (2017) 4:1–7. doi: 10.1186/s40661-017-0057-6
94. Krishnamoorthy Y, Ganesh K, and Sakthivel M. Prevalence and determinants of breast and cervical cancer screening among women aged between 30 and 49 years in India: Secondary data analysis of National Family Health Survey–4. Indian J Cancer. (2022) 59:54–64. doi: 10.4103/ijc.IJC_576_19
95. Jadav S, Rajan SS, Abughosh S, and Sansgiry SS. The role of socioeconomic status and health care access in breast cancer screening compliance among Hispanics. J Public Health Manage Practice. (2015) 21:467–76. doi: 10.1097/PHH.0000000000000235
96. Ma GX, Gao W, Lee S, Wang M, Tan Y, and Shive SE. Health seeking behavioral analysis associated with breast cancer screening among Asian American women. Int J Women’s Health. (2012) 4:235–43. doi: 10.2147/IJWH.S30738
97. Harcourt N, Ghebre RG, Whembolua G-L, Zhang Y, Warfa Osman S, and Okuyemi KS. Factors associated with breast and cervical cancer screening behavior among African immigrant women in Minnesota. J Immigrant Minority Health. (2014) 16:450–6. doi: 10.1007/s10903-012-9766-4
98. Lam M, Kwok C, and Lee MJ. Prevalence and sociodemographic correlates of routine breast cancer screening practices among migrant-Australian women. Aust New Z J Public Health. (2018) 42:98–103. doi: 10.1111/1753-6405.12752
99. Damiani G, Federico B, Basso D, Ronconi A, Bianchi CBNA, Anzellotti GM, et al. Socioeconomic disparities in the uptake of breast and cervical cancer screening in Italy: a cross sectional study. BMC Public Health. (2012) 12:1–10. doi: 10.1186/1471-2458-12-99
100. Nunes MF, Leite AH, and Dias SF. Inequalities in adherence to cervical cancer screening in Portugal. Eur J Cancer Prev. (2021) 30:171–7. doi: 10.1097/CEJ.0000000000000612
101. Niedzwiedz CL, Robb KA, Katikireddi SV, Pell JP, and Smith DJ. Depressive symptoms, neuroticism, and participation in breast and cervical cancer screening: Cross-sectional and prospective evidence from UK Biobank. Psycho-oncology. (2020) 29:381–8. doi: 10.1002/pon.5272
102. Chirwa GC. Explaining socioeconomic inequality in cervical cancer screening uptake in Malawi. BMC Public Health. (2022) 22:1–14. doi: 10.1186/s12889-022-13750-4
103. Simkin J, Ogilvie G, Hanley B, and Elliott C. Differences in colorectal cancer screening rates across income strata by levels of urbanization: results from the Canadian Community Health Survey (2013/2014). Can J Public Health. (2019) 110:62–71. doi: 10.17269/s41997-018-0143-5
104. Horner-Johnson W, Dobbertin K, Andresen EM, and Iezzoni LI. Breast and cervical cancer screening disparities associated with disability severity. Women’s Health Issues. (2014) 24:e147–e53. doi: 10.1016/j.whi.2013.10.009
105. Ricardo-Rodrigues I, Jiménez-García R, Hernández-Barrera V, Carrasco-Garrido P, Jiménez-Trujillo I, and López-de-Andrés A. Adherence to and predictors of participation in colorectal cancer screening with faecal occult blood testing in Spain, 2009–2011. Eur J Cancer Prev. (2015) 24:305–12. doi: 10.1097/CEJ.0000000000000088
106. Menvielle G, Dugas J, Richard J-B, and Luce D. Socioeconomic and healthcare use-related determinants of cervical, breast and colorectal cancer screening practice in the French West Indies. Eur J Cancer Prev. (2018) 27:269–73. doi: 10.1097/CEJ.0000000000000329
107. Sriplung H and Viroj Tangcharoensathien M. Breast cancer screening among women in Thailand: analyses of population-based household surveys. J Med Assoc Thai. (2014) 97:1106–18.
108. Mukem S, Meng Q, Sriplung H, and Tangcharoensathien V. Low coverage and disparities of breast and cervical cancer screening in Thai women: analysis of national representative household surveys. Asian Pac J Cancer Prev. (2015) 16:8541–51. doi: 10.7314/APJCP.2015.16.18.8541
109. Wang L, Mackenzie L, Hossain ZJN, and Sciences H. Breast cancer screening practices and associated factors among Chinese-Australian women living in Sydney: A cross-sectional survey study. Nurs Health Sci. (2022) 24:293–303. doi: 10.1111/nhs.12925
110. Aschwanden D, Gerend MA, Luchetti M, Stephan Y, Sutin AR, and Terracciano A. Personality traits and preventive cancer screenings in the Health Retirement Study. Prev Med. (2019) 126:105763. doi: 10.1016/j.ypmed.2019.105763
111. Midaksa M, Destaw A, Addissie A, Kantelhardt EJ, and Gizaw M. Women’s sexual autonomy as a determinant of cervical cancer screening uptake in Addis Ababa, Ethiopia: a case–control study. BMC Women’s Health. (2022) 22:236. doi: 10.1186/s12905-022-01829-4
112. Abera GB, Abebe SM, and Werku AG. Demand for cervical cancer screening in tigray region of Ethiopia in 2018: A community-based cross-sectional study. Int J Women’s Health. (2020) 12:795–804. doi: 10.2147/IJWH.S255548
113. Assefa AA, Abera G, and Geta M. Breast cancer screening practice and associated factors among women aged 20–70 years in urban settings of SNNPR, Ethiopia. Breast Cancer: Targets Ther. (2021) 13:9–19. doi: 10.2147/BCTT.S286441
114. Osingada CP, Ninsiima G, Chalo RN, Muliira JK, and Ngabirano T. Determinants of uptake of cervical cancer screening services at a no-cost reproductive health clinic managed by nurse-midwives. Cancer Nursing. (2015) 38:177–84. doi: 10.1097/NCC.0000000000000156
115. Getachew S, Getachew E, Gizaw M, Ayele W, Addissie A, and Kantelhardt EJ. Cervical cancer screening knowledge and barriers among women in Addis Ababa, Ethiopia. PloS One. (2019) 14:e0216522. doi: 10.1371/journal.pone.0216522
116. Studts CR, Tarasenko YN, and Schoenberg NE. Barriers to cervical cancer screening among middle-aged and older rural Appalachian women. J Community Health. (2013) 38:500–12. doi: 10.1007/s10900-012-9639-8
117. Bianco A, Larosa E, Pileggi C, Nobile CG, and Pavia M. Cervical and breast cancer screening participation and utilisation of maternal health services: a cross-sectional study among immigrant women in Southern Italy. BMJ Open. (2017) 7. doi: 10.1136/bmjopen-2017-016306
118. Liu T, Li S, Ratcliffe J, and Chen G. Assessing knowledge and attitudes towards cervical cancer screening among rural women in Eastern China. Int J Environ Res Public Health. (2017) 14:967. doi: 10.3390/ijerph14090967
119. Torosian T, Abrami EA, Massoumi RL, Harutyunyan NM, Dallakyan G, Hovhannisyan H, et al. Assessing knowledge and perceptions of colorectal cancer screening in Armenia. J Surg Res. (2021) 257:616–24. doi: 10.1016/j.jss.2020.08.038
120. Tastan S, Andsoy II, and Iyigun E. Evaluation of the knowledge, behavior and health beliefs of individuals over 50 regarding colorectal cancer screening. Asian Pacific J Cancer Prev. (2013) 14:5157–63. doi: 10.7314/APJCP.2013.14.9.5157
121. Ramazani AA, Norozi E, AmirabadiZadeh H, Ehteshampour AR, and Salehiniya H. Predictors of colorectal cancer screening participation in Southern Khorasan (Iran). J Gastrointestinal Cancer. (2021) 52:187–91. doi: 10.1007/s12029-020-00379-y
122. Zhu X, Parks PD, Weiser E, Jacobson DJ, Limburg PJ, and Rutten LJF. Barriers to utilization of three colorectal cancer screening options–data from a national survey. Prev Med Rep. (2021) 24:101508. doi: 10.1016/j.pmedr.2021.101508
123. Lin SC, McKinley D, Sripipatana A, and Makaroff L. Colorectal cancer screening at US community health centers: examination of sociodemographic disparities and association with patient-provider communication. Cancer. (2017) 123:4185–92. doi: 10.1002/cncr.30855
124. Huang J, Wang J, Pang TW-Y, Chan MK-Y, Leung S, Chen X, et al. Does theory of planned behaviour play a role in predicting uptake of colorectal cancer screening? A cross-sectional study in Hong Kong. BMJ Open. (2020) 10:e037619. doi: 10.1136/bmjopen-2020-037619
125. Jin SW, Lee J, and Yun Lee H. Analyzing factors associated with decisional stage of adopting breast cancer screening among Korean American women using precaution adoption process model. Ethnicity Health. (2021) 26:431–47. doi: 10.1080/13557858.2018.1520813
126. Lee M, Lee MA, Ahn H, Ko J, Yon E, Lee J, et al. Health literacy and access to care in cancer screening among Korean Americans. Health Literacy Res Practice. (2021) 5:e310–e8. doi: 10.3928/24748307-20211104-01
127. Raju S, Khawaja A, Han X, Wang X, and Mazzone PJ. Lung cancer screening: characteristics of nonparticipants and potential screening barriers. Clin Lung Cancer. (2020) 21:e329–e36. doi: 10.1016/j.cllc.2019.11.016
128. Kim B, Lee Y, Noh J-W, and Kim TH. Factors associated with health check-up and cancer screening participation among family caregivers of patients with dementia: a cross-sectional study. BMC Public Health. (2021) 21:1–9. doi: 10.1186/s12889-021-11768-8
129. Donnelly TT, Al Khater A-H, Al-Bader SB, Al Kuwari MG, Al-Meer N, Malik M, et al. Breast cancer screening among Arabic women living in the State of Qatar: Awareness, knowledge, and participation in screening activities. Avicenna. (2012) 2012:2. doi: 10.5339/avi.2012.2
130. Pengpid S, Zhang C, and Peltzer K. The prevalence and associated factors of cancer screening uptake among a national population-based sample of adults in Marshall Islands. Cancer Control. (2021) 28:1073274821997497. doi: 10.1177/1073274821997497
131. Ogunsiji OO, Kwok C, and Fan LC. Breast cancer screening practices of African migrant women in Australia: a descriptive cross-sectional study. BMC Women’s Health. (2017) 17:1–10. doi: 10.1186/s12905-017-0384-0
132. Kurani SS, McCoy RG, Lampman MA, Doubeni CA, Rutten LJF, Inselman JW, et al. Association of neighborhood measures of social determinants of health with breast, cervical, and colorectal cancer screening rates in the US Midwest. JAMA Network Open. (2020) 3:e200618–e. doi: 10.1001/jamanetworkopen.2020.0618
133. Khanna D, Vashist S, Khanna A, and Khanna AK. Determinants of uptake of cervical cancer screening in Northern India. Indian J Public Health Res Dev. (2019) 10. doi: 10.5958/0976-5506.2019.01946.6
134. Tapera R, Manyala E, Erick P, Maswabi TM, Tumoyagae T, Letsholo B, et al. Knowledge and attitudes towards cervical cancer screening amongst University of Botswana female students. Asian Pacific J Cancer Prev. (2017) 18:2445. doi: 10.22034/APJCP.2017.18.9.2445
135. Woldetsadik AB, Amhare AF, Bitew ST, Pei L, Lei J, and Han J. Socio-demographic characteristics and associated factors influencing cervical cancer screening among women attending in St. Paul’s Teaching and Referral Hospital, Ethiopia. BMC Women’s Health. (2020) 20:1–9. doi: 10.1186/s12905-020-00927-5
136. Ncube B, Bey A, Knight J, Bessler P, and Jolly PE. Factors associated with the uptake of cervical cancer screening among women in Portland, Jamaica. North Am J Med Sci. (2015) 7:104. doi: 10.4103/1947-2714.153922
137. Bui NC, Lee YY, Suh M, Park B, Cho H, Kim Y, et al. Beliefs and intentions to undergo lung cancer screening among Korean males. Cancer Res Treat. (2018) 50:1096–105. doi: 10.4143/crt.2017.393
138. Shin DW, Chang D, Jung JH, Han K, Kim SY, Choi KS, et al. Disparities in the participation rate of colorectal cancer screening by fecal occult blood test among people with disabilities: a national database study in South Korea. Cancer Res Treat. (2020) 52:60–73. doi: 10.4143/crt.2018.660
139. Núñez ER, Caverly TJ, Zhang S, Glickman ME, Qian SX, Boudreau JH, et al. Adherence to follow-up testing recommendations in US veterans screened for lung cancer, 2015-2019. JAMA Network Open. (2021) 4:e2116233–e. doi: 10.1001/jamanetworkopen.2021.16233
140. Nik Farid ND, Abdul Aziz N, Al-Sadat N, Jamaludin M, and Dahlui M. Clinical breast examination as the recommended breast cancer screening modality in a rural community in Malaysia; what are the factors that could enhance its uptake? PloS One. (2014) 9:e106469. doi: 10.3390/cancers14133076
141. Ndejjo R, Mukama T, Musabyimana A, and Musoke D. Uptake of cervical cancer screening and associated factors among women in rural Uganda: a cross sectional study. PloS One. (2016) 11:e0149696. doi: 10.1371/journal.pone.0149696
142. Schreuders EH, Ruco A, Rabeneck L, Schoen RE, Sung JJY, Young GP, et al. Colorectal cancer screening: a global overview of existing programmes. Gut. (2015) 64:1637. doi: 10.1136/gutjnl-2014-309086
143. Health.gov.au. National bowel cancer screening program(2024). Available online at: https://www.health.gov.au/our-work/national-bowel-cancer-screening-program (Accessed November 7, 2024).
144. CDC.gov. National breast and cervical cancer early detection program(2024). Available online at: https://www.cdc.gov/breast-cervical-cancer-screening/index.html (Accessed November 7, 2024).
145. NHS. NHS screening(2024). Available online at: https://www.nhs.uk/conditions/nhs-screening/ (Accessed November 7, 2024).
146. Gov.uk. Screening programmes across the UK. Differences in screening policy and implementation across the UK(2021). Available online at: https://www.gov.uk/guidance/screening-programmes-across-the-uk (Accessed November 7, 2024).
147. Research.uk C. Cervical cancer incidence statistics(2024). Available online at: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/cervical-cancer/incidenceheading-One (Accessed November 7, 2024).
148. Jabbari H, Piri R, Mohammadi S, and Naghavi-Behzad M. Cervical cancer screening behaviors among post-menopausal women. Int J Cancer Manage. (2019) 12(4):e80026. doi: 10.5812/ijcm.80026
149. Peltzer K and Phaswana-Mafuya N. Breast and cervical cancer screening and associated factors among older adult women in South Africa. Asian Pacific J Cancer Prev. (2014) 15:2473–6. doi: 10.7314/APJCP.2014.15.6.2473
150. Phaswana-Mafuya N and Peltzer K. Breast and cervical cancer screening prevalence and associated factors among women in the South African general population. Asian Pacific J Cancer Prev. (2018) 19:1465. doi: 10.22034/APJCP.2018.19.6.1465
151. Lichter KE, Levinson K, Hammer A, Lippitt MH, and Rositch AF. Understanding cervical cancer after the age of routine screening: Characteristics of cases, treatment, and survival in the United States. Gynecologic Oncol. (2022) 165:67–74. doi: 10.1016/j.ygyno.2022.01.017
152. Deshpande AD, McQueen A, and Coups EJ. Different effects of multiple health status indicators on breast and colorectal cancer screening in a nationally representative US sample. Cancer Epidemiol. (2012) 36:270–5. doi: 10.1016/j.canep.2011.10.001
153. Kim H, Filson C, Joski P, von Esenwein S, and Lipscomb J. Association between online information-seeking and adherence to guidelines for breast and prostate cancer screening. Preventing Chronic Dis. (2018) 15:170147. doi: 10.5888/pcd15.170147
154. Sicsic J and Franc C. Obstacles to the uptake of breast, cervical, and colorectal cancer screenings: what remains to be achieved by French national programmes? BMC Health Serv Res. (2014) 14:1–12. doi: 10.1186/1472-6963-14-465
155. Park C, Ma X, Park SK, and Lawson KA. Association of depression with adherence to breast cancer screening among women aged 50 to 74 years in the United States. J Eval Clin Practice. (2020) 26:1677–88. doi: 10.1111/jep.13356
156. Songsiriphan A, Salang L, Somboonporn W, Eamudomkarn N, Nhokaew W, Kuchaisit C, et al. Knowledge, Attitudes, and Practices Regarding Cervical Cancer Screening among HIV-infected Women at Srinagarind Hospital: A Cross-Sectional Study. Asian Pacific J Cancer Prev. (2020) 21:2979. doi: 10.31557/APJCP.2020.21.10.2979
157. Martinez-Huedo M, de Andres AL, Hernandez-Barrera V, Carrasco-Garrido P, Hernandez DM, and Jiménez-Garcia R. Adherence to breast and cervical cancer screening in Spanish women with diabetes: associated factors and trend between 2006 and 2010. Diabetes Metab. (2012) 38:142–8. doi: 10.1016/j.diabet.2011.09.007
158. Richard A, Rohrmann S, Schmid SM, Tirri BF, Huang DJ, Güth U, et al. Lifestyle and health-related predictors of cervical cancer screening attendance in a Swiss population-based study. Cancer Epidemiol. (2015) 39:870–6. doi: 10.1016/j.canep.2015.09.009
159. Eng VA, David SP, Li S, Ally MS, Stefanick M, and Tang JY. The association between cigarette smoking, cancer screening, and cancer stage: a prospective study of the women’s health initiative observational cohort. BMJ Open. (2020) 10:e037945. doi: 10.1136/bmjopen-2020-037945
160. Silvera SAN, Bandera EV, Jones BA, Kaplan AM, and Demisse K. Knowledge of, and beliefs about, access to screening facilities and cervical cancer screening behaviors among low-income women in New Jersey. Cancer Causes Control. (2020) 31:43–9. doi: 10.1007/s10552-019-01244-5
161. So WK, Wong CL, Chow KM, Chen JM, Lam WW, Chan CW, et al. The uptake of cervical cancer screening among South Asians and the general population in Hong Kong: A comparative study. J Cancer Policy. (2017) 12:90–6. doi: 10.1016/j.jcpo.2017.03.015
162. Sy AU, Lim E, Ka’opua LS, Kataoka-Yahiro M, Kinoshita Y, and Stewart SL. Colorectal cancer screening prevalence and predictors among Asian American subgroups using medical expenditure panel survey National Data. Cancer. (2018) 124:1543–51. doi: 10.1002/cncr.31098
163. Rogers CR, Perdue DG, Boucher K, Korous KM, Brooks E, Petersen E, et al. Masculinity barriers to ever completing colorectal cancer screening among American Indian/Alaska native, black, and white men (ages 45–75). Int J Environ Res Public Health. (2022) 19:3071. doi: 10.3390/ijerph19053071
164. Myong J-P and Kim H-R. Impacts of household income and economic recession on participation in colorectal cancer screening in Korea. Asian Pacific J Cancer Prev. (2012) 13:1857–62. doi: 10.7314/apjcp.2012.13.5.1857
165. Ishii K, Tabuchi T, and Iso H. Combined patterns of participation in cervical, breast, and colorectal cancer screenings and factors for non-participation in each screening among women in Japan. Prev Med. (2021) 150:106627. doi: 10.1016/j.ypmed.2021.106627
166. Llanos AA, Pennell ML, Young GS, Tatum CM, Katz ML, and Paskett ED. No association between colorectal cancer worry and screening uptake in Appalachian Ohio. J Public Health. (2015) 37:322–7. doi: 10.1093/pubmed/fdu031
167. Taheri-Kharameh Z, Noorizadeh F, Sangy S, Zamanian H, Shouri-Bidgoli AR, and Oveisi H. Factors associated with adherence to colorectal cancer screening among moderate risk individuals in Iran. Asian Pacific J Cancer Prev. (2016) 16:8371–5. doi: 10.7314/APJCP.2015.16.18.8371
168. He L, Gao S, Tao S, Li W, Du J, Ji Y, et al. Factors associated with colonoscopy compliance based on health belief model in a community-based colorectal cancer screening program Shanghai, China. Int Q Community Health Education. (2020) 41:25–33. doi: 10.1177/0272684X19897356
169. Bujang N-N-A, Lee Y-J, Mohd-Zain S-A-S, Aris J-H, Md-Yusoff F-A, Suli Z, et al. Factors associated with colorectal cancer screening via immunochemical fecal occult blood test in an average-risk population from a multiethnic, middle-income setting. JCO Global Oncol. (2021) 7:333–41. doi: 10.1200/GO.20.00460
170. Farr DE, Cofie LE, Brenner AT, Bell RA, and Reuland DS. Sociodemographic correlates of colorectal cancer screening completion among women adherent to mammography screening guidelines by place of birth. BMC Women’s Health. (2022) 22:1–9. doi: 10.1186/s12905-022-01694-1
171. Huang J, Choi P, Chen X, Wang J, Ding H, Jin Y, et al. Factors associated with participation in colorectal cancer screening: a population-based study of 7200 Chinese individuals. Lancet. (2019) 394:S61. doi: 10.1016/S0140-6736(19)32397-9
172. Nunez E, Caverly T, Zhang S, Glickman M, Qian S, Boudreau J, et al. Patient factors associated with declining lung cancer screening after shared decision making in a national cohort of veterans. Chest. (2021) 160:A1637. doi: 10.1016/j.chest.2021.07.1488
173. Stowell JT, Narayan AK, Wang GX, Fintelmann FJ, Flores EJ, Sharma A, et al. Factors affecting patient adherence to lung cancer screening: A multisite analysis. J Med Screening. (2021) 28:357–64. doi: 10.1177/0969141320950783
174. Telvizian T, Al Ghadban Y, Alawa J, Mukherji D, Zgheib NK, Sawaf B, et al. Knowledge, beliefs, and practices related to cancer screening and prevention in Lebanon: community and social media users’ perspectives. Eur J Cancer Prev. (2021) 30:341–9. doi: 10.1097/CEJ.0000000000000631
175. Xie H, Li Y, Wang Q, Fujiwara Y, Kurbanova T, and Theodoropoulos N. MA04. 02 lung cancer screening utilization and its correlates in sexual minorities: an analysis of the BRFSS 2018. J Thorac Oncol. (2021) 16:S144. doi: 10.1016/j.jtho.2021.01.224
176. Spalluto LB, Lewis JA, Samuels LR, Callaway-Lane C, Matheny ME, Denton J, et al. Association of rurality with annual repeat lung cancer screening in the Veterans Health Administration. J Am Coll Radiology. (2022) 19:131–8. doi: 10.1016/j.jacr.2021.08.027
177. Doria-Rose VP, White MC, Klabunde CN, Nadel MR, Richards TB, McNeel TS, et al. Use of lung cancer screening tests in the United States: results from the 2010 National Health Interview Survey. Cancer Epidemiology Biomarkers Prev. (2012) 21(7):1049–59. doi: 10.1158/1055-9965.EPI-12-0343
178. Guo L-W, Chen Q, Shen Y-C, Meng Q-C, Zheng L-Y, Wu Y, et al. Evaluation of a low-dose computed tomography lung cancer screening program in Henan, China. JAMA Network Open. (2020) 3:e2019039–e. doi: 10.1001/jamanetworkopen.2020.19039
179. Neslund-Dudas C, Tang A, Alleman E, Lafata JE, Honda SA, Oshiro C, et al. Completion of lung cancer screening after a baseline order for LDCT at five diverse health systems. J Clin Oncol. (2021) 39(15_suppl):10506–10506. doi: 10.1200/JCO.2021.39.15-suppl.10506
180. Weygandt J, Robling K, Whitaker L-A, McPherson K, Hartwell M, and Greiner B. Cancer screening among current and former US Military personnel compared to civilians: a cross-sectional analysis of the behavioral risk factor surveillance system. Military Med. (2023) 188:e1416–e21. doi: 10.1093/milmed/usab439
181. Quaife SL, Vrinten C, Ruparel M, Janes SM, Beeken RJ, Waller J, et al. Smokers’ interest in a lung cancer screening programme: a national survey in England. BMC Cancer. (2018) 18:1–10. doi: 10.1186/s12885-018-4430-6
182. Australian Government. Report on the lung cancer screening enquiry(2020). Available online at: https://www.cancerAustralia.gov.au/sites/default/files/publications/report-lung-cancer-screening-enquiry/pdf/report_on_the_lung_cancer_screening_enquiry_0.pdf (Accessed November 7, 2024).
183. Poon C, Haderi A, Roediger A, and Yuan M. Should we screen for lung cancer? A 10-country analysis identifying key decision-making factors. Health Policy. (2022) 126:879–88. doi: 10.1016/j.healthpol.2022.06.003
184. NHS England. Evaluation of the Targeted Lung Health Check programme. Available online at: https://www.england.nhs.uk/contact-us/privacy-notice/how-we-use-your-information/our-services/evaluation-of-the-targeted-lung-health-check-programme/ (Accessed November 7, 2024).
185. Gudina A, Cupertino A, Kamen CS, Adler D, Belcher E, Gilmore N, et al. Understanding factors associated with uptake of lung cancer screening among individuals at higher risk. J Health Care Poor Underserved. (2021) 39(15_suppl). doi: 10.1200/JCO.2021.39.15-suppl.10559
186. Dressler J, Johnsen AT, Madsen LJ, Rasmussen M, and Jorgensen LN. Factors affecting patient adherence to publicly funded colorectal cancer screening programmes: a systematic review. Public Health. (2021) 190:67–74. doi: 10.1016/j.puhe.2020.10.025
187. Vrinten C, Waller J, von Wagner C, and Wardle J. Cancer fear: facilitator and deterrent to participation in colorectal cancer screening. Cancer Epidemiol Biomarkers Prev. (2015) 24:400–5. doi: 10.1158/1055-9965.Epi-14-0967
188. Pinto JA, Pinillos L, Villarreal-Garza C, Morante Z, Villarán MV, Mejía G, et al. Barriers in Latin America for the management of locally advanced breast cancer. Ecancermedicalscience. (2019) 13:897. doi: 10.3332/ecancer.2019.897
189. Marlow NM, Pavluck AL, Bian J, Ward EM, and Halpern MT. RTI press research report series. In: The Relationship Between Insurance Coverage and Cancer Care: A Literature Synthesis. RTI Press, Research Triangle Park (NC) (2009).
190. Maeda M, Filomeno R, Kawata Y, Sato T, Maruyama K, Endo M, et al. Association of employment and company size with lung cancer screening participation among Japanese based on the socioeconomic conditions using the Comprehensive Survey of Living Conditions. Int J Clin Oncol. (2020) 25:670–80. doi: 10.1007/s10147-019-01594-9
191. Narayan AK, Gupta Y, Little BP, Shepard JO, and Flores EJ. Lung cancer screening eligibility and use with low-dose computed tomography: results from the 2018 Behavioral Risk Factor Surveillance System cross-sectional survey. Cancer. (2021) 127:748–56. doi: 10.1002/cncr.33322
192. Kindratt TB, Dallo FJ, Allicock M, Atem F, and Balasubramanian BA. The influence of patient-provider communication on cancer screenings differs among racial and ethnic groups. Prev Med Rep. (2020) 18:101086. doi: 10.1016/j.pmedr.2020.101086
193. Asgary R, Garland V, and Sckell B. Breast cancer screening among homeless women of New York City shelter-based clinics. Women’s Health Issues. (2014) 24:529–34. doi: 10.1016/j.whi.2014.06.002
194. Carrasco-Garrido P, Hernandez-Barrera V, Lopez de Andres A, Jimenez-Trujillo I, Gallardo Pino C, and Jimenez-Garcıa R. Awareness and uptake of colorectal, breast, cervical and prostate cancer screening tests in Spain. Eur J Public Health. (2014) 24:264–70. doi: 10.1093/eurpub/ckt089
195. Elobaid YE, Aw TC, Grivna M, and Nagelkerke N. Breast cancer screening awareness, knowledge, and practice among Arab women in the United Arab Emirates: a cross-sectional survey. PloS One. (2014) 9:e105783. doi: 10.1371/journal.pone.0105783
196. Kim K and Han H-R. The association between health literacy and breast and cervical cancer screening behaviors: findings from the behavioral risk factor surveillance system. Nurs Res. (2019) 68:177–88. doi: 10.1097/NNR.0000000000000346
197. Abeyweera P, Brims F, Piccolo F, Lei C, and Manners D. P2. 11-09 Australia-wide cross-sectional survey of general practitioners’ Knowledge and practice of lung cancer screening. J Thorac Oncol. (2019) 14:S795. doi: 10.1016/j.jtho.2019.08.1709
198. Rajupet S, Doshi D, Wisnivesky JP, and Lin JJ. Attitudes about lung cancer screening: primary care providers versus specialists. Clin Lung Cancer. (2017) 18:e417–e23. doi: 10.1016/j.cllc.2017.05.003
199. Ferguson J, Jankowich M, Nici L, Melek J, and Gartman E. Barriers to lung cancer screening in a veteran population: does distance drive completion? Am J Respir Crit Care Med. (2020) 201:A6456–A. doi: 10.1164/ajrccm-conference.2020.201.1_MeetingAbstracts.A6456
200. Rennert L, Zhang L, Lumsden B, Harwood K, Tyler L, Ashby M, et al. Factors influencing lung cancer screening completion following participation in shared decision-making: A retrospective study in a US academic health system. Cancer Treat Res Commun. (2020) 24:100198. doi: 10.1016/j.ctarc.2020.100198
201. Faye A, Diagne N, Niang K, and Dia A. Screening for cervical cancer in Senegal: Contributing factors. Ann Trop Med Public Health. (2017) 10(6):1474–8. doi: 10.4103/ATMPH.ATMPH-354-17
202. Gottschlich A, Ochoa P, Rivera-Andrade A, Alvarez CS, Mendoza Montano C, Camel C, et al. Barriers to cervical cancer screening in Guatemala: a quantitative analysis using data from the Guatemala Demographic and Health Surveys. Int J Public Health. (2020) 65:217–26. doi: 10.1007/s00038-019-01319-9
203. Ubah C, Nwaneri AC, Anarado AN, Iheanacho PN, and Odikpo I. Perceived barriers to cervical cancer screening uptake among women of an urban community in south-eastern Nigeria. Asian Pacific J Cancer Prev. (2022) 23:1959. doi: 10.31557/APJCP.2022.23.6.1959
204. Baussano I, Tshering S, Choden T, Lazzarato F, Tenet V, Plummer M, et al. Cervical cancer screening in rural Bhutan with the careHPV test on self-collected samples: an ongoing cross-sectional, population-based study (REACH-Bhutan). BMJ Open. (2017) 7(7):e016309. doi: 10.1136/bmjopen-2017-016309
205. Phaiphichit J, Paboriboune P, Kunnavong S, and Chanthavilay P. Factors associated with cervical cancer screening among women aged 25–60 years in Lao People’s Democratic Republic. PloS One. (2022) 17:e0266592. doi: 10.1371/journal.pone.0266592
206. Al Rifai R and Nakamura K. Differences in breast and cervical cancer screening rates in Jordan among women from different socioeconomic strata: analysis of the 2012 population-based household survey. Asian Pac J Cancer Prev. (2015) 16:6697–704. doi: 10.7314/APJCP.2015.16.15.6697
207. Lombardo J, Ko K, Shimada A, Nelson N, Wright C, Chen J, et al. Perceptions of and barriers to cancer screening by the sexual and gender minority community: a glimpse into the health care disparity. Cancer Causes Control. (2022) 33:559–82. doi: 10.1007/s10552-021-01549-4
208. Merten JW, Pomeranz JL, King JL, Moorhouse M, and Wynn RD. Barriers to cancer screening for people with disabilities: a literature review. Disabil Health J. (2015) 8:9–16. doi: 10.1016/j.dhjo.2014.06.004
209. Hertzum-Larsen R, Kjær SK, Frederiksen K, and Thomsen LT. Participation in cervical cancer screening among immigrants and Danish-born women in Denmark. Prev Med. (2019) 123:55–64. doi: 10.1016/j.ypmed.2019.02.023
Keywords: barriers, cancer screening, screening uptake, facilitators, screening intervention, public health, preventative healthcare
Citation: Aguiar-Ibáñez R, Mbous YPV, Sharma S, Chakali R and Chawla E (2025) Barriers to cancer screening uptake and approaches to overcome them: a systematic literature review. Front. Oncol. 15:1575820. doi: 10.3389/fonc.2025.1575820
Received: 13 February 2025; Accepted: 30 June 2025;
Published: 06 August 2025.
Edited by:
Yu Ligh Liou, The First Affiliated Hospital of Guangdong Pharmaceutical University, ChinaReviewed by:
Yongbin Liu, Houston Methodist Research Institute, United StatesBernard Omolo, University of South Carolina Upstate, United States
Taolan Zhang, University of South China, China
Şafak Kıran, Karadeniz Technical University, Türkiye
Alixida Ramos-Pibernus, Ponce Health Sciences University, Puerto Rico
Copyright © 2025 Aguiar-Ibáñez, Mbous, Sharma, Chakali and Chawla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: R. Aguiar-Ibáñez, cmFxdWVsLmFndWlhci1pYmFuZXpAbWVyY2suY29t