 Osman Bardakçı1*
Osman Bardakçı1* Gökay Çetinkaya2
Gökay Çetinkaya2- 1Department of Surgical Oncology, Isparta City Hospital, Isparta, Türkiye
- 2Department of Surgical Oncology, Ankara Gülhane Research and Training Hospital, Ankara, Türkiye
Background and Objective: Reliable preoperative identification of lymph node metastasis in clinically node-negative (cN0) patients with locally advanced upper rectal cancer (LAURC) remains a major clinical challenge due to the limited sensitivity of imaging modalities. The HALP score—calculated from hemoglobin, albumin, lymphocyte, and platelet counts—has emerged as a promising marker reflecting systemic inflammation and nutritional status. This study aimed to investigate the association between preoperative HALP scores and histopathologically confirmed lymph node metastasis in cN0 LAURC patients and to assess its diagnostic performance.
Methods: This retrospective study included 62 patients who underwent curative resection for cN0 LAURC between January 2020 and December 2023. HALP scores were computed using the formula: hemoglobin (g/L) × albumin (g/L) × lymphocyte count (/L) ÷ platelet count (/L), based on fasting blood samples collected within one week prior to surgery. Patients were stratified according to the presence or absence of pathological lymph node metastasis. ROC curve analysis was used to determine the optimal HALP cut-off value. Strict exclusion criteria were applied to minimize confounding from comorbidities affecting hematologic parameters.
Results: Lymph node metastasis was confirmed in 21 patients (33.9%). Patients with metastasis had significantly lower HALP scores compared to those without (p = 0.007). ROC analysis identified a HALP cut-off value of 6.98, yielding a sensitivity of 73% and specificity of 81% (AUC = 0.695; 95% CI: 0.56–0.83; p = 0.013). No significant associations were observed between HALP score and TNM stage or demographic variables.
Conclusion: The HALP score is significantly associated with pathological lymph node metastasis in cN0 LAURC patients and may serve as a simple, inexpensive, and clinically applicable biomarker to support preoperative staging. Further prospective studies with survival-based endpoints are warranted to validate its prognostic value.
1 Introduction
Colorectal cancer (CRC) remains one of the most common malignancies globally and a leading contributor to cancer-related mortality. Approximately one-third of CRC cases involve the rectum, and among these, upper rectal cancers (URCs) constitute a clinically significant subgroup, accounting for 30–49% of all rectal tumors (1). Locally advanced rectal cancer (LARC), characterized by tumor invasion beyond the muscularis propria—classified as T3 when extending into perirectal tissues and T4 when involving adjacent organs—presents distinct therapeutic challenges. Lymph node metastasis, a hallmark of aggressive tumor biology, is observed in 18–24% of T2 tumors and increases in frequency with advancing T stage (2). Its presence is strongly associated with poorer oncological outcomes and informs the need for adjuvant therapy.
While total mesorectal excision (TME) following neoadjuvant chemoradiotherapy represents the standard of care in mid and lower rectal cancers, treatment strategies for locally advanced upper rectal cancer (LAURC) remain controversial (3). There is ongoing debate regarding the necessity and extent of mesorectal excision—partial versus total—and whether surgery alone suffices in the absence of clinically evident nodal disease. Despite its generally favorable prognosis compared to distal rectal cancers, LAURC demonstrates recurrence rates ranging from 5.7% to 44.6%, underlining the need for improved risk stratification tools (4–6).
Preoperative imaging modalities, particularly computed tomography (CT) and magnetic resonance imaging (MRI), are routinely employed to evaluate tumor extent and nodal involvement. However, their sensitivity and specificity in detecting microscopic lymph node metastases remain suboptimal. Reported accuracy rates for CT in determining tumor depth and nodal status range from 50% to 70% and 56% to 84%, respectively (7). MRI offers modestly improved performance, with accuracy rates of up to 75% for local invasion and 59% to 83% for lymph node evaluation (8–10). These limitations highlight the need for complementary, cost-effective biomarkers that can enhance preoperative staging accuracy, particularly in cN0 patients.
The Hemoglobin, Albumin, Lymphocyte, and Platelet (HALP) score has recently gained attention as a composite biomarker reflecting systemic inflammation and nutritional status—two critical dimensions of cancer progression. First introduced in 2016 in the context of gastrointestinal cancers, the HALP score has demonstrated prognostic value for overall and disease-free survival in CRC and other solid tumors (11–16). Its utility is reinforced by its derivation from routine hematologic parameters, making it an accessible and reproducible tool in the clinical setting.
To date, no study has specifically evaluated the HALP score’s capacity to predict pathological lymph node metastasis in patients with LAURC staged as clinically node-negative (cN0) by imaging. This study addresses this knowledge gap by investigating the association between preoperative HALP scores and histologically confirmed nodal metastases in cN0 LAURC patients. We hypothesize that lower HALP scores are associated with a higher likelihood of occult nodal involvement, and that this biomarker may support more personalized treatment planning in this patient subgroup.
2 Materials and methods
2.1 Study design and patient selection
This retrospective, single-center, cross-sectional study was conducted at the Department of Surgical Oncology and General Surgery, Isparta City Hospital, between January 2020 and December 2023. A total of 62 patients with histologically confirmed, clinically node-negative (cN0), locally advanced upper rectal cancer (LAURC) classified as T3 or T4 stage were included. Clinical staging was based on preoperative imaging, including contrast-enhanced computed tomography (CT), pelvic magnetic resonance imaging (MRI), and proctosigmoidoscopy, in accordance with international colorectal cancer management guidelines.
Eligible patients met the following criteria: (1) cN0 status on imaging, (2) surgical management via open or laparoscopic resection with mesorectal excision, (3) absence of prior neoadjuvant treatment, and (4) availability of complete preoperative laboratory and postoperative histopathological data. Exclusion criteria included patients with lower or mid-rectal cancer, T1–T2 tumors, radiologically suspicious lymph node involvement, distant metastases, benign pathology, or incomplete clinical data. This rigorous selection process ensured a clinically homogeneous and representative study population.
To assess the statistical adequacy of the sample size, a post hoc power analysis was conducted. Based on HALP score differences between patients with (n = 21) and without (n = 41) lymph node metastasis, an effect size of 0.77 was observed, yielding a statistical power of 87% at an alpha level of 0.05. This confirmed that the sample size was sufficient to detect meaningful differences.
2.2 Data collection and standardization
Demographic and clinical data—including age, sex, radiological findings, surgical technique, histopathological staging, and length of hospital stay—were retrieved from the institutional electronic health records. All patients underwent preoperative blood sampling within seven days prior to surgery, following overnight fasting, during standardized morning hours to ensure procedural uniformity.
To minimize the influence of confounding factors on hematologic parameters, patients with chronic inflammatory diseases, autoimmune disorders, active infections, hematologic malignancies, chronic liver disease, thrombocytopenia, or thrombocytosis were excluded. Platelet values and other hematologic indices were verified to fall within normal reference ranges prior to HALP calculation.
2.3 HALP score calculation
The HALP score was calculated using the following validated formula:HALP = Hemoglobin (g/L) × Albumin (g/L) × Lymphocyte count (×109/L) ÷ Platelet count (×109/L).Laboratory values were obtained directly from the institutional electronic database. To eliminate inter-observer variability and ensure consistency, HALP scores were computed using a predefined, automated spreadsheet formula applied uniformly across all cases.
2.4 Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 20.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to assess the normality of continuous variables. For normally distributed variables, comparisons between groups were conducted using the Independent Samples t-test, while the Mann–Whitney U test and Kruskal–Wallis test were employed for non-normally distributed data. Receiver operating characteristic (ROC) curve analysis was utilized to evaluate the diagnostic performance of the HALP score in predicting lymph node metastasis. The optimal HALP cut-off value was determined using the Youden index. The area under the curve (AUC), sensitivity, specificity, and 95% confidence intervals (CIs) were reported. A two-tailed p-value < 0.05 was considered statistically significant for all tests.
3 Results
In this retrospective analysis of 62 patients with clinically node-negative (cN0) locally advanced upper rectal cancer (LAURC), the relationship between preoperative HALP score and postoperative lymph node metastasis was systematically evaluated. The mean age of the cohort was 68.48 ± 12.34 years (range: 45–95), with a slight male predominance (n = 33; 53.2%). All patients underwent surgery without prior neoadjuvant treatment. Based on pathological staging, 53 patients (85.5%) were classified as T3, while 9 patients (14.5%) were T4. Lymph node metastasis was identified in 21 patients (33.9%).
Regarding surgical approach, 17 patients (27.4%) underwent open low anterior resection with partial mesorectal excision, whereas 45 patients (72.6%) were managed laparoscopically. Postoperative complications were observed in 8 cases (13%), with wound infection being the most common. The mean number of lymph nodes harvested was 17 ± 7.21 (range: 5–39), and adequate lymphadenectomy (≥12 nodes) was achieved in 55 patients (85.7%). Preoperative hematologic parameters were as follows: hemoglobin 11.75 g/dL (range: 7.8–16.4), albumin 3.25 g/dL (range: 1.80–4.90), lymphocyte count 1.37 ×10³/μL (range: 0.21–4.79), and platelet count 269.52 ×10³/μL (range: 138–559) (Table 1).
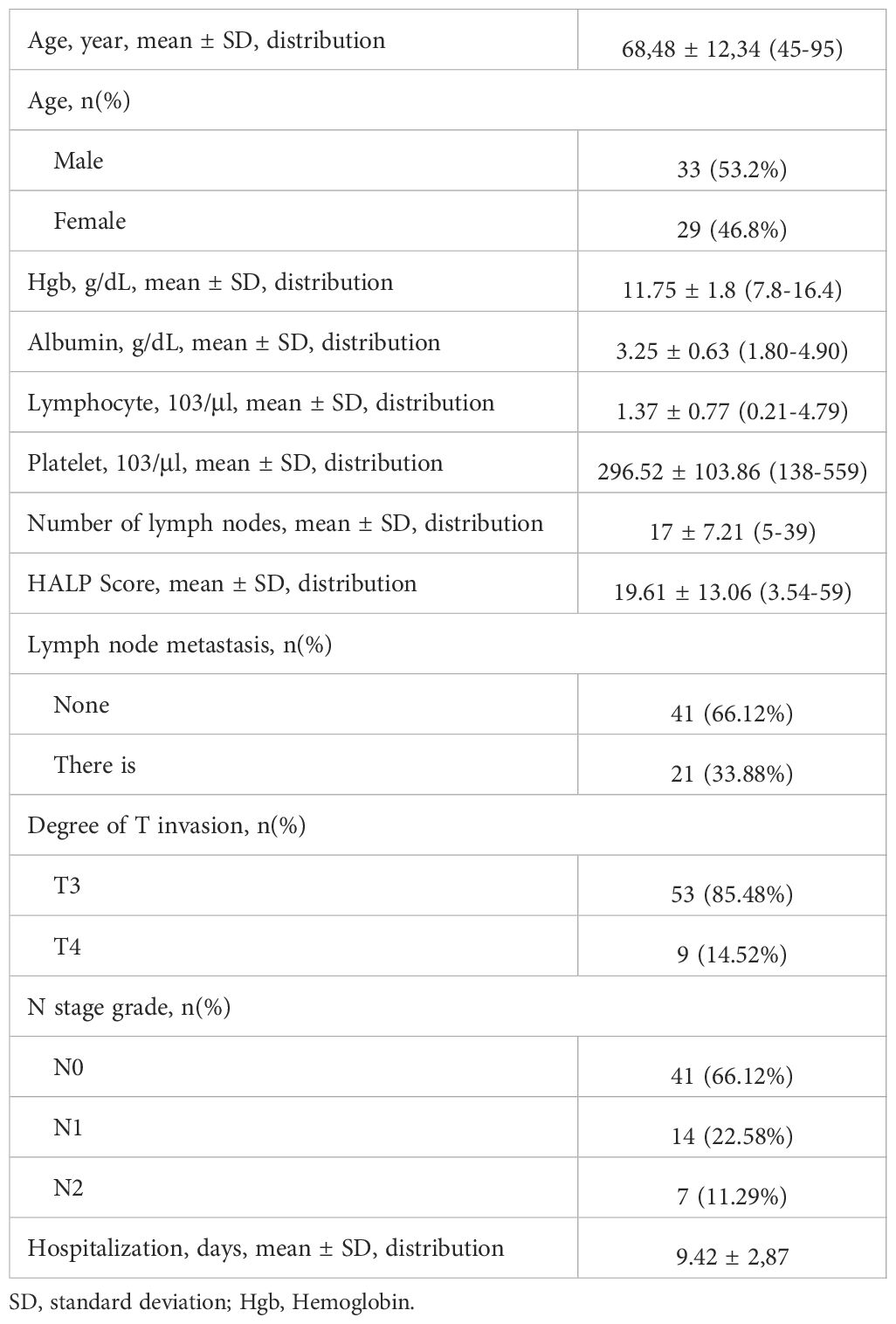
Table 1. General characteristics of the patients.
No significant association was found between HALP scores and patient sex or tumor T/N stage (p > 0.05). However, patients with lymph node metastasis exhibited significantly lower HALP scores compared to node-negative individuals (p = 0.007), indicating a potential diagnostic utility (Table 2).
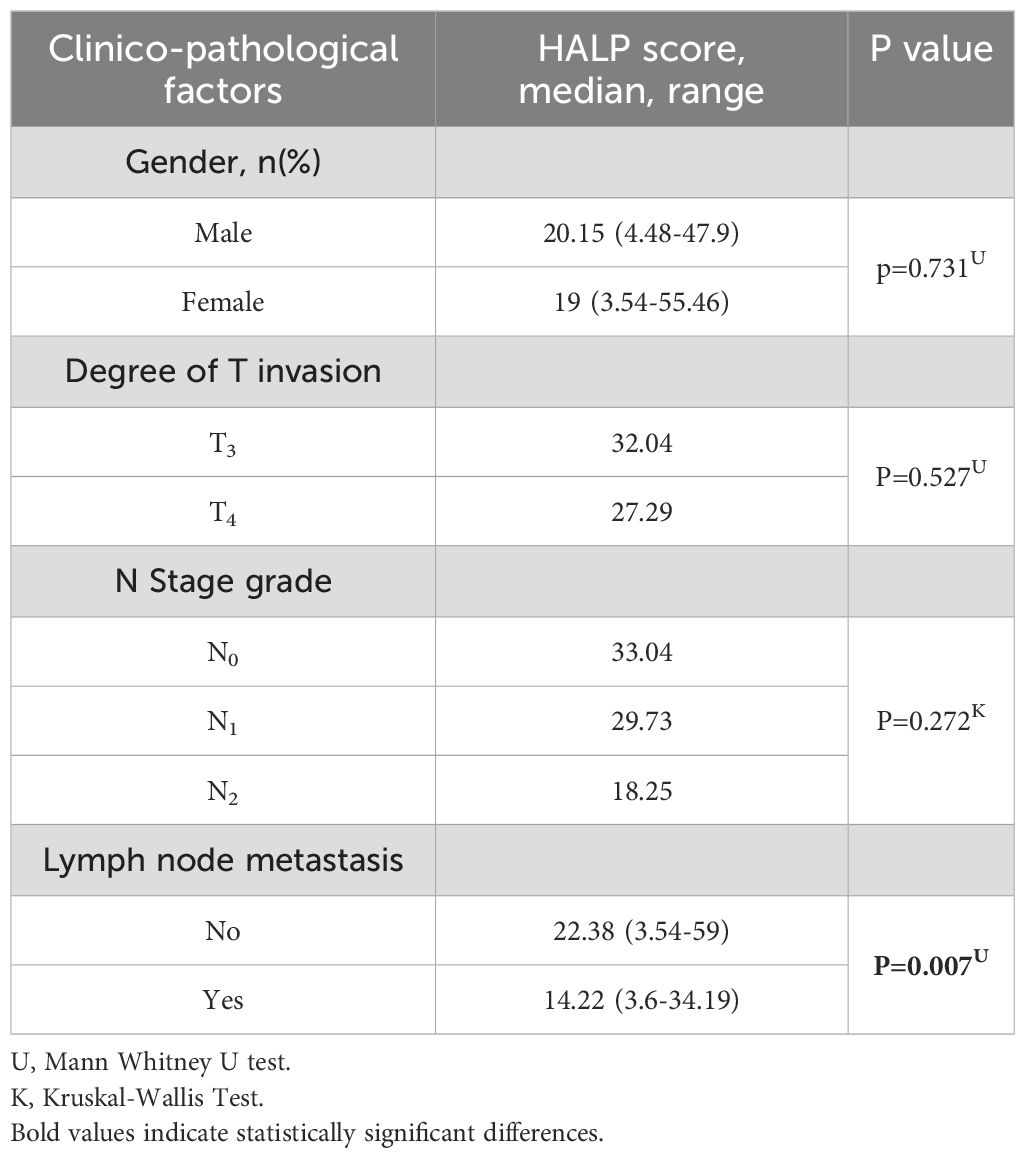
Table 2. Distribution of clinico-pathological factors according to HALP scoring system.
Receiver operating characteristic (ROC) curve analysis was employed to assess the discriminatory performance of the HALP score for predicting lymph node metastasis. The optimal cut-off value was calculated as 6.98 based on the Youden index, yielding a sensitivity of 73% and specificity of 81%. The area under the ROC curve (AUC) was 0.695 (95% CI: 0.56–0.83), with a p-value of 0.013, indicating moderate predictive ability and statistical significance (Table 3; Figure 1).

Table 3. HALP score cut-off value in predicting lymph node metastasis.
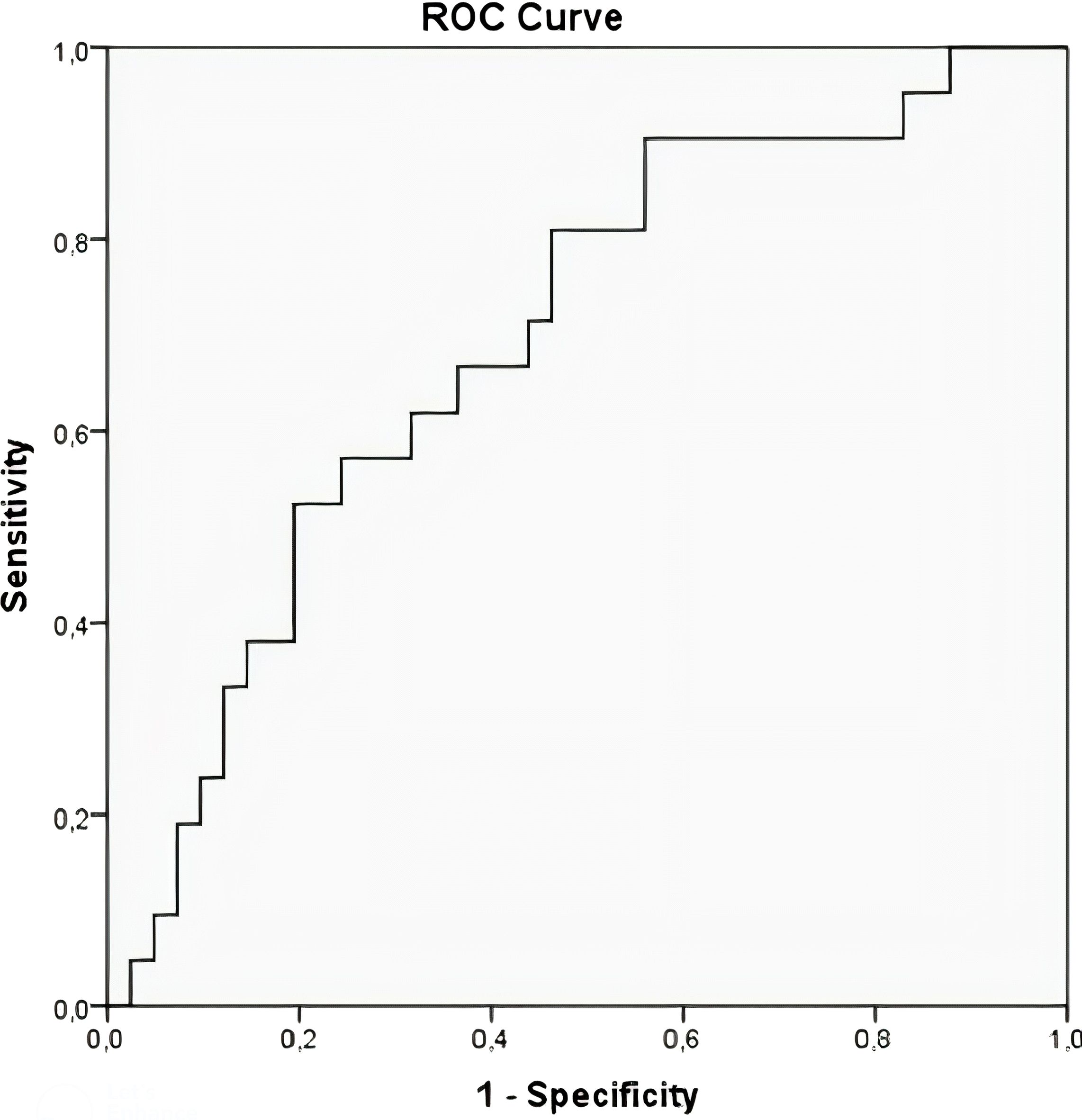
Figure 1. HALP score ROC curve in predicting lymph node metastasis.
4 Discussion
Accurate preoperative staging remains a cornerstone in the optimal management of rectal cancer (RC), as lymph node involvement is a critical determinant of prognosis, recurrence risk, and treatment planning (17, 18). Although magnetic resonance imaging (MRI) is considered the most reliable imaging modality and is widely recommended in colorectal cancer (CRC) staging guidelines (19), its diagnostic accuracy is notably reduced in upper rectal cancers (URCs) due to bowel loop interference and anatomical challenges (20). Computed tomography (CT), while frequently used, is limited by low contrast resolution and suboptimal sensitivity (55%) and specificity (74%) for detecting lymph node metastases, which are only marginally improved in MRI (66% and 76%, respectively) (21). These constraints underscore the need for complementary, accessible biomarkers that can enhance staging precision.
In recent years, systemic inflammatory and nutritional indices have gained attention for their prognostic significance in cancer patients. The Hemoglobin, Albumin, Lymphocyte, and Platelet (HALP) score, a composite biomarker derived from routine laboratory parameters, reflects both inflammatory status and nutritional reserves. Low albumin and hemoglobin levels are well-documented indicators of poor prognosis in gastrointestinal malignancies (22–24). Lymphocytes are key mediators of tumor immune surveillance, and lymphopenia has been correlated with worse oncologic outcomes (25). Platelets promote tumor angiogenesis and immune evasion via vascular endothelial growth factor (VEGF) and other pro-inflammatory mediators (26–29). By integrating these four markers, the HALP score provides a consolidated and clinically practical assessment of host-tumor interactions (30, 31).
In this study, we demonstrated that cN0 LAURC patients with a HALP score ≤6.98 had a significantly higher risk of pathological lymph node metastasis. These findings suggest that the HALP score can serve as a surrogate marker for occult nodal disease, even in the absence of radiological suspicion. Prior research has validated the prognostic utility of the HALP score in multiple malignancies. Jiang et al. (16) first introduced the HALP score in 2016 as a predictor of overall and disease-specific survival in patients with locally advanced CRC. Yalav et al. (32) associated low HALP scores with elevated carcinoembryonic antigen (CEA) levels and mucinous histology in CRC. Akbaş et al. (33) suggested its role in differentiating malignant and benign causes of intestinal obstruction, while Topal et al. (34) linked HALP scores to tumor budding—an indicator of aggressive tumor biology. In gastric cancer, Wang et al. (35) reported that patients with low HALP scores were four times more likely to present with nodal metastases.
The current study builds on these findings by exploring the HALP score specifically in the context of clinically node-negative, locally advanced upper rectal cancer—a population for which no previous HALP-based nodal predictive studies exist. This is especially relevant given the limited accuracy of CT and MRI in detecting microscopic nodal involvement (19–21), and it offers a valuable, cost-effective adjunct to conventional imaging.
5 Limitations and future directions
Several limitations must be acknowledged. First, the study’s retrospective and single-center design may limit generalizability and introduce selection bias. Second, the modest sample size, particularly in the T4 subgroup, may reduce the statistical power for detecting smaller effects. Third, due to the retrospective nature of data collection, survival outcomes such as overall survival (OS) and disease-free survival (DFS) could not be assessed, precluding Kaplan–Meier or Cox regression analyses.
Despite these limitations, the study’s principal strength lies in its originality. To the best of our knowledge, this is the first study to evaluate the predictive performance of the HALP score for lymph node metastasis in cN0 LAURC patients. Future multicenter, prospective studies with larger cohorts and long-term follow-up are warranted to validate our findings. Incorporating HALP into multivariate prognostic models alongside imaging and molecular markers could enhance its clinical applicability in personalized treatment planning.
5 Conclusions
The HALP score, derived from readily available preoperative laboratory parameters, demonstrates significant predictive value for pathological lymph node involvement in clinically node-negative locally advanced upper rectal cancer. A HALP threshold ≤6.98 was significantly associated with nodal positivity, highlighting its potential as a low-cost, non-invasive adjunct to conventional imaging. These findings support the integration of HALP into preoperative assessment protocols, with the aim of improving risk stratification and guiding individualized management strategies in rectal cancer.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by The Ethics Committee of the Süleyman Demirel University Faculty of Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
OB: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. GÇ: Data curation, Project administration, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We are grateful to all patients and doctors contributed to this paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
LAURC, Locally advanced upper rectum tumors; HALP, Hemoglobin, albumin, lymphocyte and platelet; URC, Upper Rectal Cancer; RC, Rectal Cancer; CRC, Colorectal Cancer; CT, Computed Tomography; MRI, Magnetic Resonance Imaging; TME, Total Mesorectal Excision; CEA, Carcinoembryogenic Antigen.
References
2. Fields AC, Lu P, Hu F, Hirji S, Irani J, Bleday R, et al. Lymph node positivity in T1/T2 rectal cancer: a word of caution in an era of increased incidence and changing biology for rectal cancer. J Gastrointest Surg. (2021) 25:1029–35. doi: 10.1007/s11605-020-04580-z
3. Bondeven P, Laurberg S, Hagemann-Madsen RH, and Ginnerup Pedersen B. Suboptimal surgery and omission of neoadjuvant therapy for upper rectal cancer is associated with a high risk of local recurrence. Colorectal Dis. (2015) 17:216–24. doi: 10.1111/codi.12869
4. Nesbakken A, Nygaard K, Westerheim O, Mala T, and Lunde OC. Local recurrence after mesorectal excision for rectal cancer. Eur J Surg Oncol. (2002) 28:126–34. doi: 10.1053/ejso.2001.1231
5. Chapuis PH, Lin BP, Chan C, Dent OF, and Bokey EL. Risk factors for tumour present in a circumferential line of resection after excision of rectal cancer. Br J Surg. (2006) 93:860–5. doi: 10.1002/bjs.5285
6. Law WL and Chu KW. Anterior resection for rectal cancer with mesorectal excision: a prospective evaluation of 622 patients. Ann Surg. (2004) 240:260–8. doi: 10.1097/01.sla.0000133185.23514.32
7. Farouk R, Nelson H, Radice E, Mercill S, and Gunderson L. Accuracy of computed tomography in determining resectability for locally advanced primary or recurrent colorectal cancers. Am J Surg. (1998) 175:283–7. doi: 10.1016/s0002-9610(98)00017-8
8. Fernández-Esparrach G, Ayuso-Colella JR, Sendino O, Pagés M, Cuatrecasas M, Pellisé M, et al. EUS and magnetic resonance imaging in the staging of rectal cancer: a prospective and comparative study. Gastrointest Endosc. (2011) 74:347–54. doi: 10.1016/j.gie.2011.03.1257
9. Mizukami Y, Ueda S, Mizumoto A, Sasada T, Okumura R, Kohno S, et al. Diffusion-weighted magnetic resonance imaging for detecting lymph node metastasis of rectal cancer. World J Surg. (2011) 35:895–9. doi: 10.1007/s00268-011-0986-x
10. Al-Sukhni E, Milot L, Fruitman M, Beyene J, Victor JC, Schmocker S, et al. Diagnostic accuracy of MRI for assessment of T category, lymph node metastases, and circumferential resection margin involvement in patients with rectal cancer: a systematic review and meta-analysis. Ann Surg Oncol. (2012) 19:2212–23. doi: 10.1245/s10434-011-2210-5
11. Farag CM, Antar R, Akosman S, Ng M, and Whalen MJ. What is hemoglobin, albumin, lymphocyte, platelet (HALP) score? A comprehensive literature review of HALP's prognostic ability in different cancer types. Oncotarget. (2023) 14:153–72. doi: 10.18632/oncotarget.28367
12. Tian M, Li Y, Wang X, Tian X, Pei LL, Wang X, et al. The hemoglobin, albumin, lymphocyte, and platelet (HALP) score is associated with poor outcome of acute ischemic stroke. Front Neurol. (2021) 11:610318. doi: 10.3389/fneur.2020.610318
13. Kocaoglu S and Alatli T. The efficiency of the HALP score and the modified HALP score in predicting mortality in patients with acute heart failure presenting to the emergency department. J Coll Physicians Surg Pak. (2022) 32:706–11. doi: 10.29271/jcpsp.2022.06.706
14. Cay F and Duran A. Predictive factors of success in sleeve gastrectomy: one-year follow-up and the significance of HALP score. J Coll Physicians Surg Pak. (2021) 31:1406–11. doi: 10.29271/jcpsp.2021.12.1406
15. Keskin Y, Sevinç H, Hazinedaroğlu SM, Morkavuk ŞB, and Ersöz Ş. Predictive utility of the HALP and modified HALP score for the assessment of operative complications in patients undergoing laparoscopic cholecystectomy for acute cholecystitis. Diagnostics (Basel). (2025) 15:152. doi: 10.3390/diagnostics15020152
16. Jiang H, Li H, Li A, Tang E, Xu D, Chen Y, et al. Preoperative combined hemoglobin, albumin, lymphocyte and platelet levels predict survival in patients with locally advanced colorectal cancer. Oncotarget. (2016) 7:72076–83. doi: 10.18632/oncotarget.12271
17. Fowler KJ, Kaur H, Cash BD, Feig BW, Gage KL, Garcia EM, et al. ACR appropriateness criteria®Pretreatment staging of colorectal cancer. J Am Coll Radiol. (2017) 14:234–44. doi: 10.1016/j.jacr.2017.02.012
18. Gunderson LL, Jessup JM, Sargent DJ, Greene FL, and Stewart A. Revised tumor and node categorization for rectal cancer based on surveillance, epidemiology, and end results and rectal pooled analysis outcomes. J Clin Oncol. (2010) 28:256–63. doi: 10.1200/JCO.2009.23.9194
19. Tudyka V, Blomqvist L, Beets-Tan RG, Boelens PG, Valentini V, van de Velde CJ, et al. EURECCA consensus conference highlights about colon & rectal cancer multidisciplinary management: the radiology experts review. Eur J Surg Oncol. (2014) 40:469–75. doi: 10.1016/j.ejso.2013.10.029
20. Beets-Tan RGH, Lambregts DMJ, Maas M, Bipat S, Barbaro B, Curvo-Semedo L, et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. (2018) 28:1465–75. doi: 10.1007/s00330-017-5026-2
21. Iannicelli E, Di Renzo S, Ferri M, Pilozzi E, Di Girolamo M, Sapori A, et al. Accuracy of high-resolution MRI with lumen distention in rectal cancer staging and circumferential margin involvement prediction. Korean J Radiol. (2014) 15:37–44. doi: 10.3348/kjr.2014.15.1.37
22. Gupta D and Lis CG. Pretreatment serum albumin as a predictor of cancer survival: a systematic review of the epidemiological literature. Nutr J. (2010) 9:69. doi: 10.1186/1475-2891-9-69
23. Caro JJ, Salas M, Ward A, and Goss G. Anemia as an independent prognostic factor for survival in patients with cancer: a systemic, quantitative review. Cancer. (2001) 91:2214–21. doi: 10.1002/1097-0142(20010615)91:12<2214::AID-CNCR1251>3.0.CO;2-P
24. Keeler BD, Mishra A, Stavrou CL, Beeby S, Simpson JA, and Acheson AG. A cohort investigation of anaemia, treatment and the use of allogeneic blood transfusion in colorectal cancer surgery. Ann Med Surg (Lond). (2015) 6:6–11. doi: 10.1016/j.amsu.2015.12.052
25. Ostroumov D, Fekete-Drimusz N, Saborowski M, Kühnel F, and Woller N. CD4 and CD8 T lymphocyte interplay in controlling tumor growth. Cell Mol Life Sci. (2018) 75:689–713. doi: 10.1007/s00018-017-2686-7
26. Gay LJ and Felding-Habermann B. Contribution of platelets to tumour metastasis. Nat Rev Cancer. (2011) 11:123–34. doi: 10.1038/nrc3004
27. Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med. (1971) 285:1182–6. doi: 10.1056/NEJM197111182852108
28. Thomas MR and Storey RF. The role of platelets in inflammation. Thromb Haemost. (2015) 114:449–58. doi: 10.1160/TH14-12-1067
29. Möhle R, Green D, Moore MA, Nachman RL, and Rafii S. Constitutive production and thrombin-induced release of vascular endothelial growth factor by human megakaryocytes and platelets. Proc Natl Acad Sci U S A. (1997) 94:663–8. doi: 10.1073/pnas.94.2.663
30. Chen XL, Xue L, Wang W, Chen HN, Zhang WH, Liu K, et al. Prognostic significance of the combination of preoperative hemoglobin, albumin, lymphocyte and platelet in patients with gastric carcinoma: a retrospective cohort study. Oncotarget. (2015) 6:41370–82. doi: 10.18632/oncotarget.5629
31. Eckart A, Struja T, Kutz A, Baumgartner A, Baumgartner T, Zurfluh S, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: A prospective study. Am J Med. (2020) 133:713–722.e7. doi: 10.1016/j.amjmed.2019.10.031
32. Yalav O, Topal U, Unal AG, and Eray IC. Prognostic significance of preoperative hemoglobin and albumin levels and lymphocyte and platelet counts (HALP) in patients undergoing curative resection for colorectal cancer. Ann Ital Chir. (2021) 92:283–92.
33. Akbas A, Koyuncu S, Hacım NA, Dasiran MF, Kasap ZA, and Okan I. Can HALP (Hemoglobin, albumin, lymphocytes, and platelets) score differentiate between Malignant and benign causes of acute mechanic intestinal obstruction? Cancer Biother Radiopharm. (2022) 37:199–204. doi: 10.1089/cbr.2021.0277
34. Topal U, Guler S, Teke Z, Karakose E, Kurtulus I, and Bektas H. Diagnostic value of preoperative haemoglobin, albumin, lymphocyte and platelet (HALP) score in predicting tumour budding in colorectal cancer. J Coll Physicians Surg Pak. (2022) 32:751–7. doi: 10.29271/jcpsp.2022.06.751
Keywords: HALP score, locally advanced upper rectal cancer, imaging, lymph node metastasis, surgery
Citation: Bardakçı O and Çetinkaya G (2025) The effectiveness of the hemoglobin, albumin, lymphocyte, and platelet (HALP) score in predicting lymph node metastasis in radiologically n0 locally advanced upper rectal cancer. Front. Oncol. 15:1579581. doi: 10.3389/fonc.2025.1579581
Received: 19 February 2025; Accepted: 09 June 2025;
Published: 04 July 2025.
Edited by:
Bhupendra Gopalbhai Prajapati, Ganpat University, IndiaReviewed by:
Mikhail Danilov, A.S.Loginov Moscow Clinical Scientific Centre, RussiaDevesh U Kapoor, Gujarat Technological University, India
Copyright © 2025 Bardakçı and Çetinkaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Osman Bardakçı, ZHJvc21hbmJhcmRha2NpQGdtYWlsLmNvbQ==