 Cecilia Mathó1,2
Cecilia Mathó1,2 Santiago Chávez1,3
Santiago Chávez1,3 Rafael Sebastián Fort3,4Adriana Della Valle5Florencia Neffa5
Rafael Sebastián Fort3,4Adriana Della Valle5Florencia Neffa5 José Roberto Sotelo-Silveira3,6
José Roberto Sotelo-Silveira3,6 Nora Artagaveytia7
Nora Artagaveytia7 María Ana Duhagon1,4*
María Ana Duhagon1,4*- 1Unidad Académica de Genética, Facultad de Medicina, Universidad de la República, Montevideo, Uruguay
- 2Plataforma de Secuenciación Masiva, Instituto de Investigaciones Biológicas Clemente Estable, Montevideo, Uruguay
- 3Departamento de Genómica, Instituto de Investigaciones Biológicas Clemente Estable, Montevideo, Uruguay
- 4Sección Genómica Funcional, Facultad de Ciencias, Universidad de la República, Montevideo, Uruguay
- 5Centro de Oncogenética Uruguayo, Banco de Tumores, Hospital Central de Las Fuerzas Armadas, Montevideo, Uruguay
- 6Sección Biología Celular, Facultad de Ciencias, Universidad de la República, Montevideo, Uruguay
- 7Departamento Básico de Medicina, Hospital de Clínicas, Universidad de la República, Montevideo, Uruguay
Introduction: Lynch Syndrome accounts for 1–7% of all colorectal cancers and is caused by germline mutations in DNA mismatch repair (MMR) genes. Timely molecular diagnosis is crucial for effective genetic counseling and management. Among understudied Latin American populations, Uruguay’s genetic admixture provides an opportunity to identify novel Lynch Syndrome related variants.
Methods: This study analyzed 70 unrelated Uruguayan colorectal cancer patients meeting Lynch Syndrome clinical criteria to identify carriers of pathogenic variants. A customized Next-Generation Sequencing (NGS) panel was developed and sequenced on the Ion Torrent platform to analyze nine genes: MLH1, MSH2, MSH6, EPCAM, FAN1, MUTYH, PMS1, PMS2, and APC. Copy number variations and large EPCAM deletions are not detected by the assay. Gene variants were prioritized based on allelic frequency, in silico predictions, pathogenicity records, and ACMG guidelines. The performance of this custom NGS panel was evaluated for in-house applications, and its limitations were thoroughly assessed.
Results and discussion: The custom NGS panel demonstrated effectiveness for scalable in-house testing despite minor disclosed sequence coverage limitations. Pathogenic and likely pathogenic variants were identified in 25 patients, including four novel Lynch Syndrome-associated variants. In four patients, a rare ambiguously classified gene variant co-occurs with a known pathogenic variant in another gene. The mutation profile correlated with clinical parameters such as age of diagnosis, diagnosis criteria, tumor location, and microsatellite instability (MSI).
Conclusion: This is the most comprehensive genetic study to date on a Uruguayan Lynch syndrome cohort. The mutational landscape aligns with findings in other populations while highlighting novel variants of clinical relevance. These findings highlight the value of customized panels for improving genetic screening in small-scale healthcare facilities.
Introduction
Inherited predisposition to colorectal cancer (CRC) remains a significant concern in cancer care, accounting for 5-10% of new cases/year worldwide (1). Lynch Syndrome (LS) is the most frequent hereditary CRC Syndrome, representing 3-5% of all CRC cases, whereas hereditary polyposis colorectal cancer (HPCC) syndromes account for <1% of CRCs. LS presents an autosomal dominant inheritance and a high risk of developing CRC (8.7-61%) and extracolonic tumors (endometrial, gastric, ovarian, urinary tract, small bowel, pancreatic, brain, or cutaneous cancers) in comparison to the general population (2, 3). Clinical management of probands with a personal or first-degree family history of CRC involves increased screening surveillance, with some differences depending on the gene mutation identified, gender, current age, and familial disease manifestation (age of onset, tumor location).
Clinical criteria for identifying individuals at risk for LS are based on Amsterdam I and II or modified Bethesda guidelines, which rely on personal and family history of cancer and tumor pathological characteristics (4, 5). Germline multigene panel test (MGPT) is indicated for patients with a personal history of LS-related cancer if diagnosed ≤50 years old, if they present a synchronous or metachronous LS-related cancer regardless of age, or if they have a family history of LS or LS-related tumors. Additionally, patients with a personal history of a tumor with a deficient mismatch repair (dMMR) pathway, evidenced by Microsatellite Instability (MSI) are recommended to have an MGPT evaluation for LS and other hereditary cancer syndromes. Also, patients with tumor pathology findings or individuals with a family history compatible with LS can be considered for MGPT. Finally, individuals without a personal history of cancer who meet familial criteria for LS can be evaluated using an MGPT if there is no pathogenic family variant known.
Genetic testing of LS requires sequencing genes involved in the MMR pathway, including MLH1, MSH2, MSH6, PMS1, and PMS2 (6, 7). Most deleterious mutations in these genes are heterozygous. Deletions in the EPCAM gene, while not directly involved in MMR, lead to the epigenetic silencing of the MSH2 gene located downstream (8). Biallelic germline mutations in the MUTYH gene predispose patients to MUTYH-associated polyposis (MAP), which is associated with a lifetime risk of colorectal cancer, typically associated with colonic polyps. However, in some patients, CRC sometimes develops without polyps, mimicking LS (9–11). Non-LS HPCC involves APC, TP53, STK11, BMPR1A, SMAD4, and PTEN genes.
Next Generation Sequencing (NGS) is the current method for identifying genetically heterogeneous diseases with extensive regions of interest (ROIs) (12). Since the NGS workflow is laborious and time-consuming, and as the size of the target region grows, the complexity and uncertainty of interpretation increase, a focused gene panel is a cost-effective approach for a few genes, compared to a large panel of a whole exome or genome. Therefore, most clinical laboratories offer more proven and less complex NGS assays, such as gene panels, to study inherited predisposition to cancer (12).Whole-exome sequencing (WES) costs have decreased significantly and are now comparable to those of targeted gene panels. However, in facilities that utilize small sequencers or have limited resources, panels remain the preferred option. This preference is due to panels requiring less sequencing capacity and generating smaller datasets, which leads to faster turnaround times and reduced computational demands during analysis. More importantly, panels provide a higher sequencing depth, enhancing the sensitivity and reliability of variant detection while reducing the likelihood of incidental or ambiguous findings. These practical considerations continue to make gene panels a favored choice in many clinical and research contexts, such as the Latin American’s (LATAM). The selection of genes for an NGS-gene test depends on their diagnostic performance, that is, the probability of detecting disease-causing genetic variants in a cohort of patients, which depends on the frequency of the mutations reported in the literature (13). Also necessary is sufficient scientific evidence of the association between an altered genotype and pathology and its implications for managing the disease. The recommended molecular genetic testing for germline mutations causing LS is an MGPT including MLH1, MSH2, MSH6, and PMS2, as well as EPCAM and other genes of interest that may aid in the differential diagnosis of polypous malignancies (HPCC) and HCRC overlapping syndromes (5, 14)
Herein, we present the genetic testing of 70 Uruguayan LS cancer patients from unrelated families using a custom gene panel and NGS Sequencing with an Ion Torrent sequencer. We analyze the panel’s performance and describe the genetic findings of the cohort. The percentage of mutation carriers and the frequency of mutation/gene are comparable to published cohorts. Custom NGS gene panel sequencing is helpful for the limited number of cases expected in small patient populations, providing a fast local response to patients and their families.
Methods
Human subjects
Seventy unrelated patients with clinical suspicion of LS were recruited at the Centro de Oncogenética Uruguayo, Banco de Tumores, Hospital Central de las Fuerzas Armadas, Montevideo, Uruguay. Since this is a national reference center in oncogenetics, patients are referred to from various health institutions (public and private). Pedigree analysis and medical history were gathered during a genetic counseling risk assessment appointment, and the fulfillment of the Amsterdam I, Amsterdam II, or Bethesda genetic risk criteria was analyzed according to the Genetic/Familial High-Risk Assessment: Colorectal, NCCN Clinical Practice Guidelines in Oncology (4).Predictive models such as PREMM5 and MMRpro were not used to select patients. All patients signed an informed consent to enroll in this study, approved by the Ethics Committee of Facultad de Medicina, Universidad de la República (Exp. No 07015300038316, UDELAR). Patient recruitment, sample extraction and medical data collection were gathered between 2014 and 2018. The sampling size was defined by funding availability.
DNA extraction
Genomic DNA was extracted from whole blood using QIAamp DNA Mini Kit (#51304, Qiagen), following manufacturer instructions. DNA quality was verified using a 260/280 nm ratio and quantified using a Qubit Fluorometer with Qubit 1X dsDNA HS (High Sensitivity) Assay Kit (#Q33230).
NGS targeted sequencing
Ion AmpliSeq custom panel
An Ion AmpliSeq custom panel was designed with Ion AmpliSeq Designer to sequence 9 genes: APC, EPCAM, FAN1, MLH1, MSH2, MSH6, MUTYH, PMS1, PMS2, as detailed in Supplementary Table 1. The gene selection was carried out at the start of the project in 2016, based on the literature available at the time. However, subsequent evidence failed to support the clinical relevance of FAN1 and PMS1 for LS, as discussed in forthcoming sections. The ROI spanned the entire coding sequence of the genes (CDS) and at least five nucleotides from the splicing junctions (exon padding) and the complete 5’ and 3’ untranslated regions (UTRs) of the RefSeq transcripts using RefGene v74. The panel resulted in 229 amplicons distributed in two primer pools of 116 and 113 amplicons. Amplicon size ranges between 132 and 374 bp, with a mean length of 334 bp for both pools. These pools cover 62,51 kb of the human genome. This amplicon set theoretically covered 99,08% of the intended gene sequences (Supplementary Table 1). Panel design files are available upon request.
Libraries and template preparation
For each patient, 10 ng of genomic DNA was amplified by PCR using the Ion AmpliSeq custom panel described above. Barcoded libraries were constructed using Ion AmpliSeq Library Kit 2.0 (#4475345) and Ion Xpress Barcode Adapters (#4474517). The quality and yield of the libraries were then assessed using Agilent Bioanalyzer (#5067-1504, Agilent Technologies). The libraries were diluted and equimolarly combined to obtain 25 µl of 26 pM for emulsion PCR and enrichment of template-positive ISP particles, which was performed in the Ion One Touch 2 system using Ion PGM Hi-Q View OT2 Kit (#A29900).
NGS sequencing
Sequencing was carried out in the Ion Torrent Personal Genome Machine (PGM), using Ion 316 Chip v2 BC (#4488145) with the Ion PGM Hi-Q View Sequencing Kit (#A30044). Each sample was sequenced at a mean depth >180X.
All procedures described above (NGS sequencing) were performed according to the manufacturer’s instructions with Thermo Fisher Scientific reagents unless specified.
NGS panel performance evaluation
Binary Alignment Map (BAM) files from the Ion Torrent Server were re-analyzed using multiple open-source tools and in-house scripting. The number of counts per amplicon was obtained using HTSeq (15).
Counts per base were acquired using BamtoCov (16). An in-house script was used to calculate the number of bases with coverage > 50X. Specific commands are available upon request.
The coverage analysis plugin from the Ion Torrent server was used to obtain the data summarized in Figure 1 panel A.
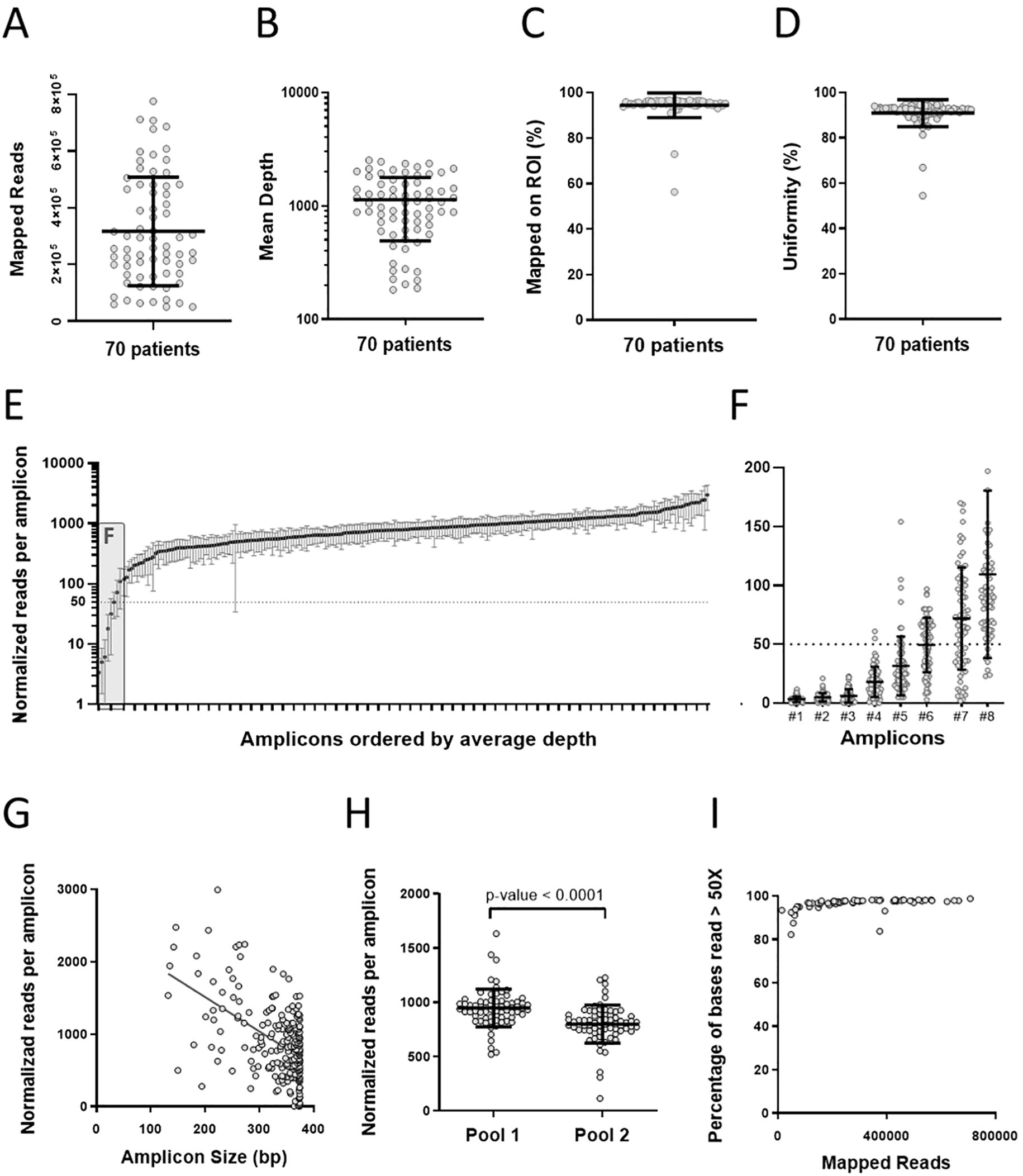
Figure 1. Patient 9-gene panel Sequencing results. (A–D) Sequencing metrics per sample. (A) Mapped Reads, (B) Mean Depth (dotted line indicates 50x depth), (C) Reads Mapped on ROI (D) Uniformities. (E–H) Sequence metrics per amplicon. (E) Normalized reads per amplicon ordered by the average depth. (F) Detailed view of the first 8 amplicons shown in (E). (G) Amplicon performance per size (Slope: -4.74, Spearman’s correlation coefficient: - 0.38, p<0.0001). (H) Normalized reads per amplicon pool. The amplicon number difference (116 vs 113) was corrected by normalizing the number of reads to 114.5 amplicons per pool. (I) Base coverage analysis: The percentage of bases read more than 50x is plotted against the total mapped reads for each patient. Mean and standard deviations are plotted in all charts. Supplementary Table 3 contains raw data.
Genetic variants identification and characterization
After sequencing, the gene variants relative to the Human Genome Reference Consortium Human Build 37 (GRCh37/hg19) were called. A variant call format file (.vcf) was generated using Ion Torrent Server. Each.vcf file was annotated using wANNOVAR (17–19). The variants were prioritized and filtered according to their allelic frequency, zygosity, functional consequence, and database registry. Relevant variants were visually inspected using Integrative Genomics Viewer (IGV) (20, 21) to confirm the read quality.
ClinVar and VarSome’s last accession date was July 18th, 2023.
All DNA variants were verified using Version 3.0.8 of Mutalyzer (22), an HGVS compliance tool.
Pathogenic variants detected by NGS were confirmed by Sanger sequencing; reaction conditions are available upon request.
Tumor microsatellite instability analysis
MSI status was assessed by polymerase chain reaction (PCR), with DNA extracted from paraffin-embedded tumoral tissue and from peripheral blood as previously described by Della Valle et al. as previously described (23). Five markers proposed in the Bethesda panel (BAT25, BAT26, D2S123, D5S346 and D17S250) were amplified by PCR and analyzed by gel electroforesis. Tumors were classified as high (MSI-H) with two or more unstable markers, low (MSI-L) with one unstable marker, or stable (MSS) with no unstable markers.
Immunohistochemistry testing of MMR proteins in tumors was not available in Uruguay when this study was done, so it was not evaluated in this patient cohort.
Results
Cohort analysis
This study included 70 unrelated Uruguayan patients with clinical suspicion of LS, whose main clinical characteristics are summarized in Table 1. Supplementary Table 2 provides detailed information. Prior studies have shown that the Uruguayan population comprises ancestral contributions from Europeans, Native Americans, and Africans of consistent proportions among studies (discussed in Bonilla et al, 2015 (24)). According to the largest published study to date, the average ancestral proportions are 76.6 ± 13.7% European, 14.0 ± 10.8% Native American, and 9.4 ± 7.5% African (24). Although patients were referred to by various health institutions, ancestry or sociodemographic biases cannot be ruled out. The median age of onset of the 70 patients and affected family members () was 46 and 58 years old (data not shown), respectively, and the sex distribution was 37 female/33 male patients. The pedigrees of 67 patients were built during consultations with a trained oncogeneticist. Sixty-seven percent of the patients met Bethesda guidelines, while 13% or 20% met Amsterdam I and II criteria, respectively.
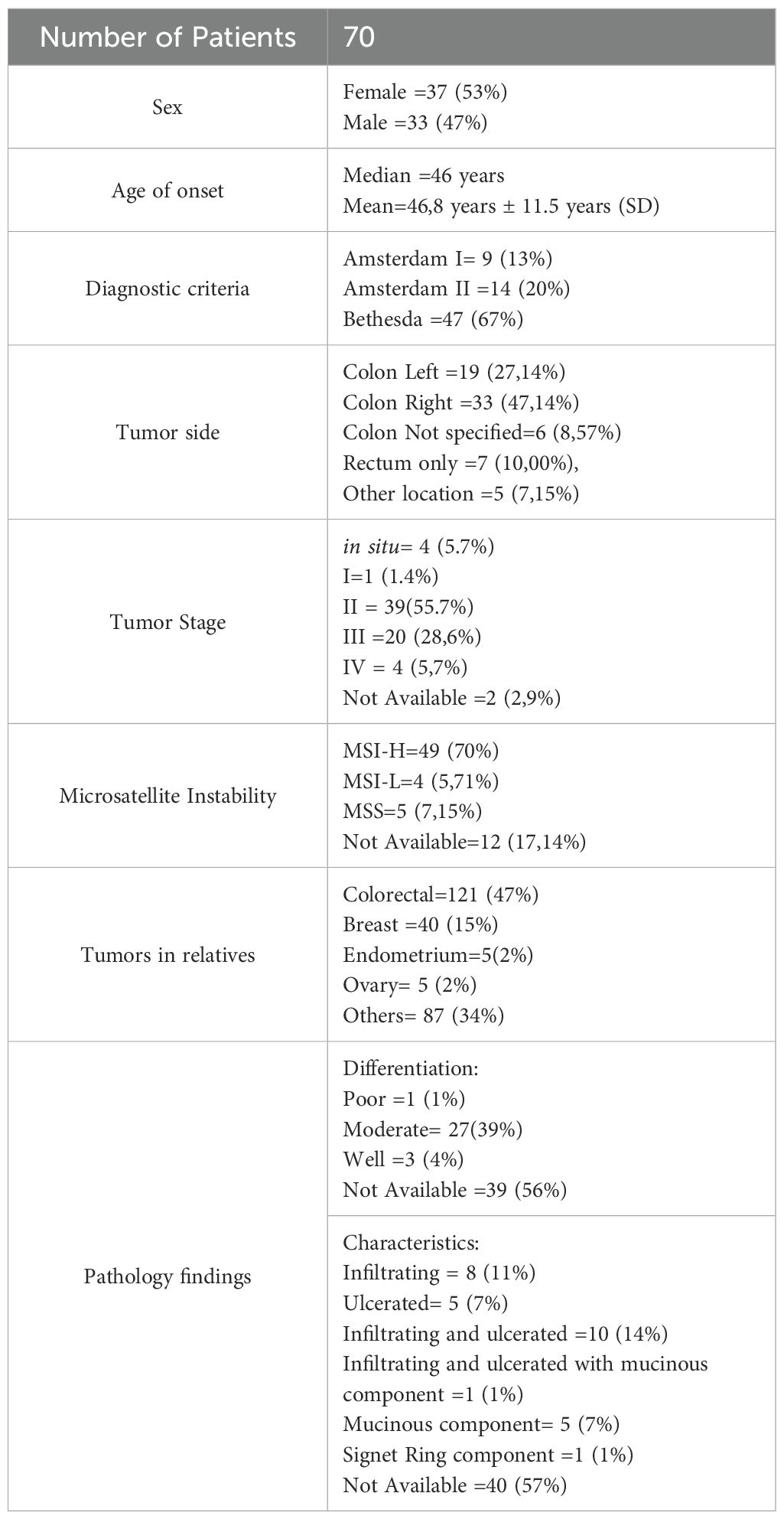
Table 1. Cohort characteristics.
The most common tumor topography among patients was the colon (82.85%) (56.90% right and 32.76% left), followed by the rectum (10%) and other localizations (7.15%), whereas in the relatives was colorectal (47%), followed by breast (15%), endometrium (2%), ovary (2%), and others (34%). More than half of the patients were diagnosed with tumor stage II (55,7%), followed by stage III (28,6%), stage I (1,4%), and carcinoma in situ (5,7%). Tumor stage information was unavailable for two patients. MSI analysis resulted in 70% MSI-H, 5.71% MSI-L, and 7.15% MSS, while 17.14% of tumors were unavailable to analyze. Pathology reports were available for 46/70 patients and showed that most tumors were moderately differentiated.
Sequencing yield and performance of the gene panel
A custom gene panel was used for DNA-seq (Supplementary Table 1), and the sequencing results are presented in Figure 1 and Supplementary Table 3. A scatter plot of the number of reads per sample mapped to the reference genome shows an average of 300000 reads/sample (Figure 1A). All samples reached the 50x sequencing depth threshold recommended for identifying germline variants by NGS. The average sequencing depth was 1132, and the lowest was 182 (Figure 1B). In addition, the proportion of reads mapped to the target sequences exceeds 94% (Figure 1C), and the uniformity of DNA sequencing resulted in an average of 90% of the bases read above 20% of the average coverage (Figure 1D).
Evaluating the ROI sequence coverage is crucial, as it directly impacts the reliability of our results. The total number of reads per sample was adjusted proportionally to 200,000 reads to normalize the sample sequencing variations. This arbitrary value is close to the median reads obtained per sample, significantly exceeding the expected minimum coverage 50x for each amplicon (Figure 1E). Despite most patients being sequenced at a depth greater than 200.000 total reads/sample, 6 amplicons yielded less than 50 reads in the normalized data (Figure 1F). The total bp covered by these 6 amplicons is 1944 bp; due to the overlap of other amplicons, this number was reduced to 1888 bp, of which only 955 bp are in coding regions (Supplementary Table 4 summarizes the poorly covered regions in depth). The missing information on sequence variants of these regions comprises two exons of each of the following genes: FAN1, MSH6, and MUTYH. These underperforming amplicons were specified in the individual patients’ test reports.
We tested if amplicon size influenced the read yield (Figure 1G), finding that short amplicons tend to produce more reads, which may contribute to the low read number of the 6 underperforming amplicons (371bp average length). We also evaluated the performance of each primer pool and found Amplicon pool 1 performed better than 2 (Figure 1H). Finally, a base coverage analysis showed that maximum coverage (~98%) is achieved with approximately 200.000 reads per sample (Figure 1I).
Identification of genetic variants
On average, 66 gene variants were found per patient, of which 16 are localized in exons (data not shown). These variants were prioritized and filtered according to their allelic frequency, zygosity, location, functional consequence, and database registry (Genome Aggregation Database (25, 26), ClinVar (27–29), Human Gene Mutation Database (HGMD) (30, 31), The International Society for Gastrointestinal Hereditary Tumors (InSiGHT) Database (32, 33)), Disease-relevant nucleotide changes, classified as VUS, Likely Pathogenic, or Pathogenic, are shown in Table 2.
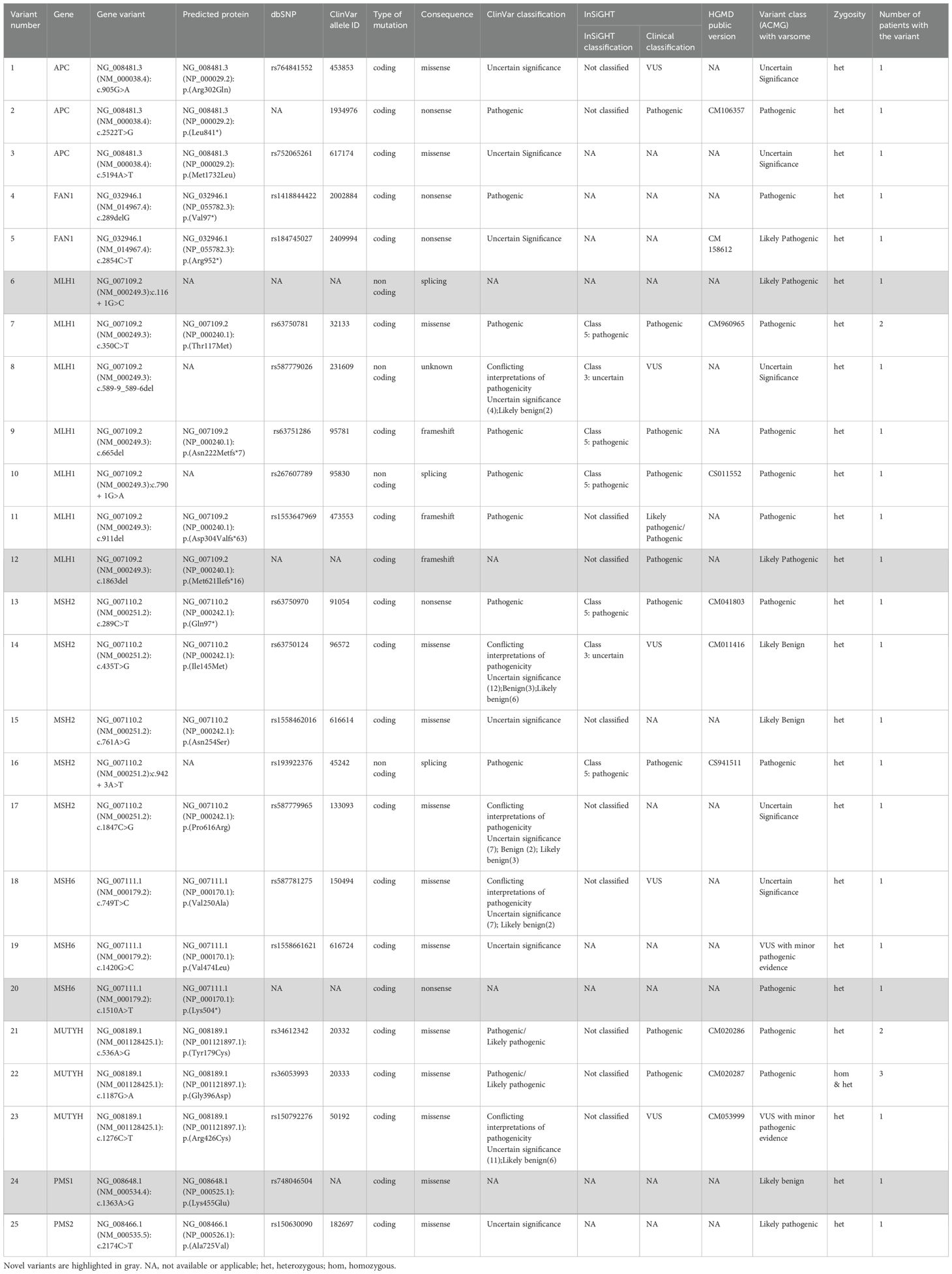
Table 2. Gene variants identified in the Lynch syndrome cohort.
Clinically relevant variants (pathogenic, likely pathogenic, and VUS) were found in 25 patients, representing 35.7% of the cohort. Figure 2 summarizes the identification and classification of the gene variants in our cohort. The majority (21/25) of the clinically relevant gene variants were classified in ClinVar as follows: Pathogenic (8/25), Likely pathogenic/Pathogenic (2/28), Uncertain Significance (6/25), and another 5/25 resulted in conflicting interpretations of pathogenicity. The remaining 4 were not reported on ClinVar. Following ACMG Guidelines, we have classified them as pathogenic (2), likely pathogenic (1), and likely benign (1). (Table 3 and Figure 2A). Additionally, the coexistence of a potentially clinically relevant variant with a pathogenic variant was observed in four patients (#15, #26, #29, and #39) Patient #15 presents p.Gly396Asp, a biallelic pathogenic MUTYH (homozygous), and a p.Arg952* variant in FAN1 (heterozygous). Although this FAN1 mutation has been previously reported by Segui et al. (46), the association of FAN1 with LS has been poorly described. Patient #26 is a heterozygous carrier for the pathogenic variant p.Gln97* in MSH2 and variant p.Arg426Cys in MUTYH, which has conflicting interpretations as VUS or likely benign. Patient #29 has the previously described pathogenic variant p.Lys504* in MSH6 and a p.Met1732Leu in APC, already proposed as VUS. Likewise, Patient #39 is heterozygous for the p.Pro616Arg variant in MSH2 (VUS), and the novel variant c.116 + 1G>C in MLH1 here classified as likely pathogenic. Finally, 4 novel variants were not present in ClinVar, therefore, we submitted them to this database.
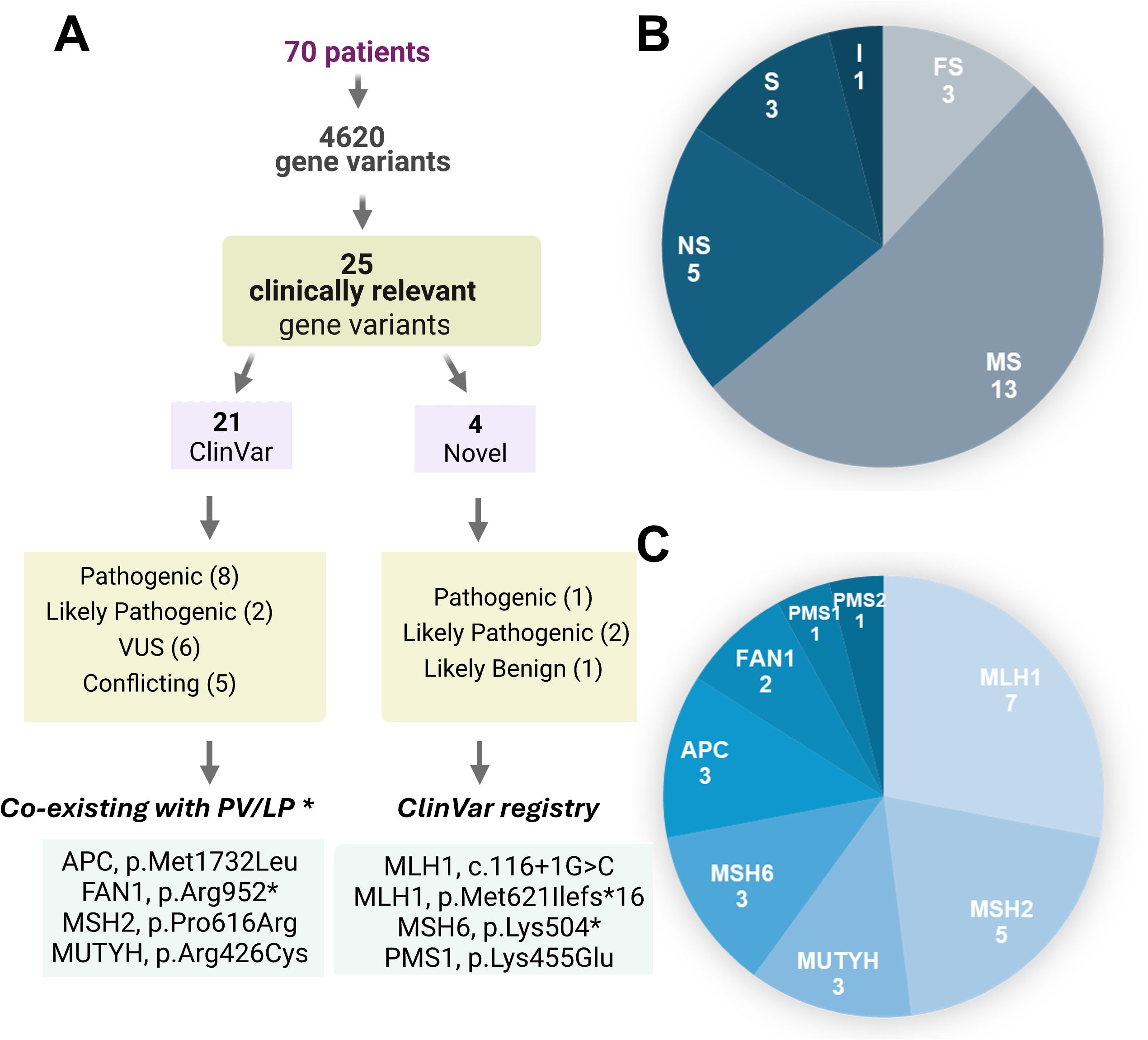
Figure 2. Clinically relevant Variants identified. (A) Summary of the variant classification results. *Gene variants coexisting with PV/LP (pathogenic/likely pathogenic variants) in a different gene. (B) Distribution of mutation types into MS (missense), NS (nonsense), FS (frameshift), S (splicing) and I (intronic). (C) Distribution of mutations in the analyzed genes.
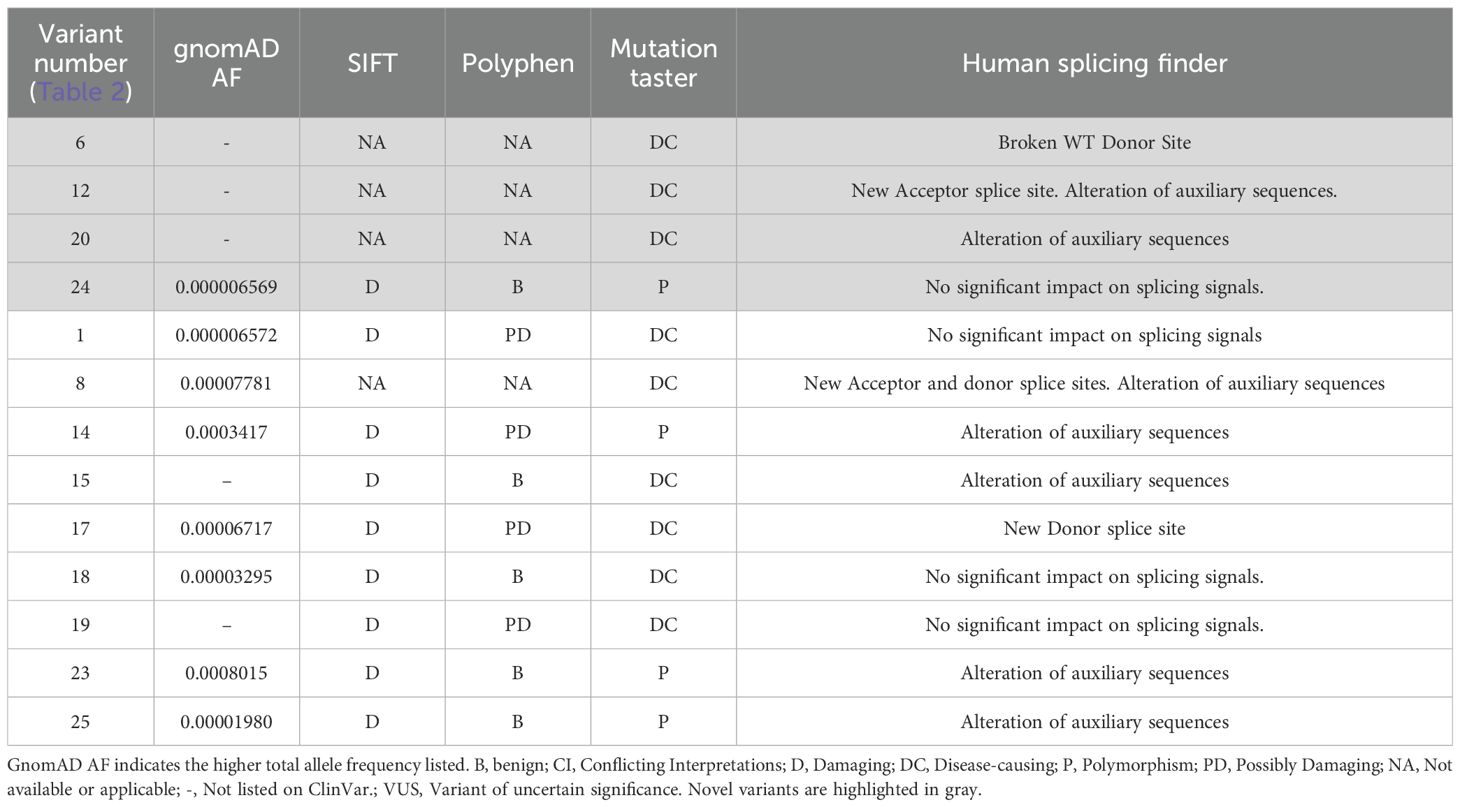
Table 3. ClinVar novel and VUS-allele frequency and in silico predictions.
The gene variants identified were grouped according to type and gene affected (Figures 2B, C, respectively). Most are missense variants, followed by nonsense, frameshift, splicing, while an intronic variant at <10 bp of the exon boundary was found. MLH1, MSH2, MUTYH, and MSH6 are the top altered genes, and no variant was identified in EPCAM. Three variants were found in more than one patient: MLH1 p.Thr117Met (2 patients), MUTYH p.Gly396Asp (3 patients: 2 heterozygous and one homozygous), and MUTYH p.Tyr179Cys (2 heterozygous patients).
Further genetic testing with more comprehensive gene panels was performed for seven patients without clinically relevant variants identified using our test; nevertheless, no disease-associated sequence variants were found (Supplementary Table 2).
Analysis of novel variants and VUSes
We analyzed the prevalence and possible phenotypic effects of the four novel variants and the nine already-reported VUSes. In silico pathogenicity predictions were performed using Mutation Taster (34), SIFT (35), Polyphen2 (36), and Human Splicing Finder (37). Table 3 summarizes allele frequencies and in silico predictions for novel and VUSes (variants of uncertain significance) reported in ClinVar. Most of the variants were extremely rare or absent in gnomAD, as expected for potentially pathogenic or uncertain variants. For instance, several variants (e.g., 6, 12, 15, 19) were not reported in gnomAD, while others had very low allele frequencies.
In silico predictions from SIFT, PolyPhen, and MutationTaster yielded mixed results. While many variants were predicted to be “damaging” (D) by SIFT and “probably damaging” (PD) or “possibly damaging” (P) by PolyPhen (e.g., variants 1, 14, 17), others were predicted as “benign” (B), reflecting uncertainty in their functional impact. MutationTaster frequently classified variants as “disease-causing” (DC), supporting potential pathogenicity. Human Splicing Finder analysis indicated that several variants may disrupt splicing signals. For example, variant 6 was predicted to break the wild-type donor site, while variants 12 and 8 were predicted to create new acceptor and/or donor sites. Multiple variants (e.g., 14, 15, 25) were also predicted to alter auxiliary splicing regulatory elements, suggesting potential effects on mRNA processing. Among the novel variants identified in this study, three of them haven’t been previously reported: so, we classified them using ACMG guidelines, assisted by VarSome (38), and uploaded their information into ClinVar (28) We also uploaded another variant in MLH1, not listed in ClinVar (p.Met621Ilefs*16,SCV005329258), identified in a patient who had colorectal cancer at the age of 36, whose father had three surgeries due to three independent colorectal tumors and died aged 54, with no other family members affected to date. This variant was previously reported in a Brazilian family with LS (39).
The patient with the splicing MLH1 mutation (c.116 + 1G>C,SCV005329268) has 4 affected family members who died without genetic testing. His father died at 64 after rectal cancer, his aunt at 28 years of ovarian cancer, and his grandmother at 72 after uterine, rectum, and ovarian cancer. His grandmother’s sister also had ovarian cancer and died at 39.
The woman with the MSH6 variant (p.Lys504*, SCV005329267) has 3 dead CRC-affected family members and no genetic testing of other relatives yet. Her father had brain and colon cancer and died aged 37. Two other family members had colon and prostate cancer.
The PMS1 variant (p.Lys455Glu, SCV005329257) was found in a woman who had colon and rectal cancer aged 70 (MSI-H) and had 4 other affected family members: 3 deceased women with breast cancer (35–50 years old) while her surviving brother had prostate cancer (72 years). To date, none of them have had genetic testing. All the novel and VUS variants identified in this study have an allele frequency that supports the very rare variants causing a high effect, compatible with an inherited cancer predisposition (40). Furthermore, the PMS1 variant is the only novel variant with a calculated allele frequency in gnomAD, while the others haven’t been found in any allele frequencies’ databases.
During oncogenetic counselling appointments, the probands with pathological variants were informed about the importance of informing at-risk relatives, while clarifying that it is ultimately the proband’s choice whether to disclose. The counsellor also offered to assist in informing relatives with the proband’s permission if communication was difficult, and the consultation and Sanger analysis was offered without cost. Despite the implementation of this counselling strategy, only four relatives pursued genetic screening, resulting in the identification of two carriers of the disease-causing variant.
Clinical associations
To assess the clinical performance of our overall genetic testing, the clinical characteristics of positive and negative results of patients identified by our panel were compared. Since the carriers of disease-predisposing mutations develop cancer at an earlier age than the general population, we compared it among positive and negative patients. The median age of diagnosis is 46 years old, regardless of the mutation status. However, positive patients tend to be diagnosed at a younger age than negative patients, with mean ages of 44 ± 2 and 48 ± 2 years, respectively (Unpaired t-test, two-tailed P value 0.1084, Figure 3A).
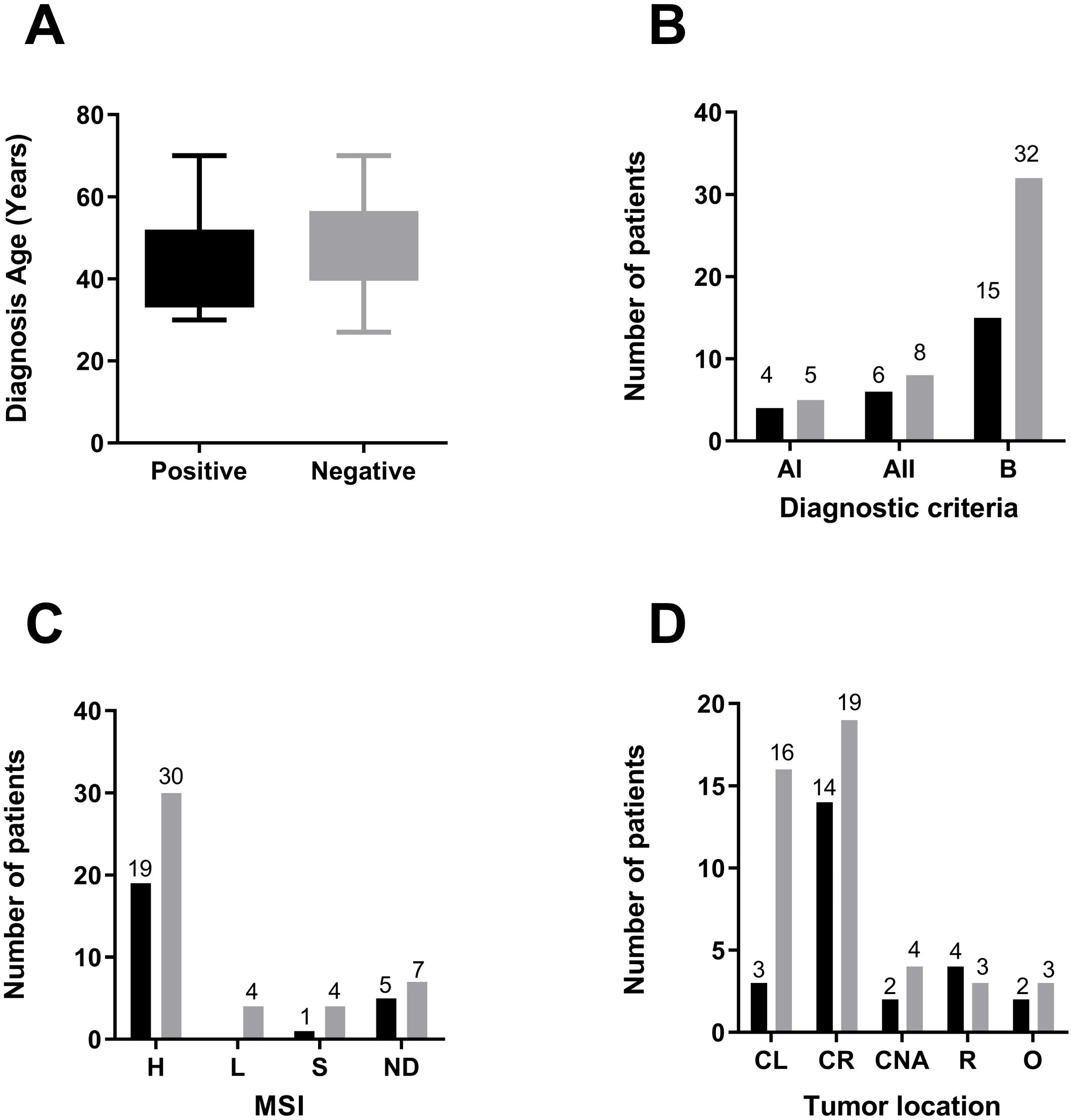
Figure 3. Association between mutations and clinical characteristics of the cohort. Comparison of several aspects among the patients who tested positive for a relevant variant detected (in black), including VUS, likely pathogenic and pathogenic variants, or negative for these variants (in gray). (A) Diagnosis Age. (B) Fulfillment of Amsterdam Criteria or Bethesda Guidelines. (C) MSI status (D) Tumor Location. Abbreviations used are CL, colon left; CR, colon right; CNA, colon not assigned; R, rectum; O, other.
Genetic assessment of high-risk LS patients involves the use of consensual criteria; thus, patients meeting them have a higher probability of being carriers of disease-predisposing mutations. Overall, the majority of the positive test patients fulfilled Bethesda criteria (15/25), followed by Amsterdam II (6/25) and Amsterdam I (4/25). Of those, 44% of the patients fulfilling Amsterdam I criteria had a positive test result (4/9), followed by Amsterdam II (6/14) and Bethesda (15/47) (Figure 3B). High microsatellite instability is associated with LS carrier status due to dMMR. In our study, 70% (49/70) of the tumors evidenced MSI-H; a relevant variant was found in 38.7% of the patients with these tumors. Seventeen percent (12/70) of tumors were unavailable for MSI determination (Figure 3C).
Tumor location has also been associated with a genetic predisposition to LS. Patients with right colonic tumors had the highest proportion of positive test results (14/33), and when compared with the left location, we found a significant difference in mutation status supporting the higher occurrence of right colon tumors in carrier individuals (Figure 3D).
Discussion
Herein, we have shown a custom NGS-gene panel’s performance, which proved to be appropriate, having high coverage and uniformity. Although technical evaluation of custom gene panels is cost-effective for genetic diagnosis facilities, it is poorly discussed in the literature (41, 42). The panel included APC, EPCAM, FAN1, MLH1, MSH2, MSH6, MUTYH, PMS1, and PMS2. Among these, MLH1, MSH2, MSH6, PMS1, and PMS2 code mismatch repair (MMR) proteins. To differentiate LS from other hereditary colorectal cancer syndromes, we also included APC and MUTYH to rule out familial adenomatous polyposis (FAP) and MUTYH-associated polyposis (MAP), respectively, as these conditions can present with clinical features overlapping LS (43) and they are the top two most prevalent mutated genes in colorectal polyposis syndromes. When this study began the association of PMS1 and FAN1 with LS was still under investigation, but the literature did not subsequently support it. Therefore, for a small gene panel design, we recommend the study of the five genes currently recommended for surveillance/prevention strategies (NCCN Guidelines Version 4.2024 Lynch Syndrome): MLH1, MSH2, EPCAM, MSH6 and PMS2, as well as APC and MUTYH.
Additionally, most reported EPCAM alterations involve large deletions, which this panel cannot detect. Indeed, the EPCAM gene, located 15 kb upstream of MSH2, is relevant because its deletions can lead to MSH2 inactivation (14, 44–46). Notably, one of the patients with a negative result (Patient #6) was later tested using a commercial panel that detects copy number variations (CNVs). This test identified a deletion encompassing exons 8 and 9 of EPCAM and exon 1 of MSH2. Although our 9-gene panel was not designed to evaluate CNVs, we assessed in silico tools to explore its potential for CNV prediction, confirming that it is not feasible with the amplicons encompassing this gene panel (data not shown). To address this shortcoming, we recommend future gene panels to be specifically designed with optimized amplicon distribution to support CNV detection, provided the assay is well validated for sensitivity and specificity. Rare ambiguous calls might need orthogonal confirmation. Disease-causing CNVs are present in approximately 10% to 20% of Lynch syndrome (LS) cases, depending on the clinical and molecular criteria used to define patient cohorts. Among the mismatch repair genes, MSH2 is most frequently affected by deletions, while large deletions or duplications in MSH6 and MLH1 are observed less commonly (47).
Lastly, FAN1 was included in this panel based on a 2015 study by Seguí et al. (48), which initially suggested an association between FAN1 and colorectal cancer. However, subsequent studies failed to replicate this link, making FAN1 variant interpretation and patient counseling challenging due to insufficient supporting evidence. Based on our findings, we recommend including APC and MUTYH in LS syndrome gene panels, as many patients harbor pathogenic variants in these genes despite lacking the typical polyposis phenotype. Conversely, sequencing FAN1 has not been shown to yield clinically meaningful insights in LS, so we do not recommend its inclusion in future gene panel designs. This is the largest and most comprehensive genetic study of LS patients performed in Uruguay. Previously, LS gene variants of Uruguayan patients using NGS-panels used heterogeneous assays and were mostly outsourced (49). Our study of 70 unrelated patients clinically suspicious for LS identified relevant gene variants in 25 patients (35.7%); although this proportion varies according to the patient selection criteria, it is similar to that of other published cohorts (50–54). Likewise, mutation frequency was similar to other cohorts, with MLH1 and MSH2 leading in number, followed by MSH6 (55).
In this study, we report 4 novel variants: MLH1 (c.116 + 1 G>C), MLH1 (p.Met621Ilefs*16), MSH6 (p.Lys504*), and PMS1 (p.Lys455Glu). The splicing MLH1 variant is predicted by Human Splicing Finder to disrupt the wild-type donor site. Applying the ACMG criteria, we classified it as Likely Pathogenic. In agreement, another nucleotide change in that position is listed in ClinVar as likely pathogenic (Variation ID: 89656). The frameshift MLH1 mutation is predicted to code for a shorter protein (636 instead of 757 aminoacids), if translated, also Human Splicing Finder predicts splicing alterations; following ACMG Guidelines we classified it as Likely Pathogenic. MSH6 p.Lys504* is a novel nonsense mutation coding a 504 amino acid protein (1360 full-length); probably, its mRNA is subject to nonsense-mediated decay. Accordingly, it is predicted to be disease-causing by Mutation Taster, while Human Splicing Finder predicts alteration of auxiliary sequences. Thus, following ACMG guidelines, we classified it as Pathogenic. Finally, since the PMS1 variant is predicted to be damaging by SIFT, but Polyphen and Mutation Taster classify it as Benign and Polymorphism, respectively, we classify it as Likely Benign.
Interestingly, in four patients we observed a pathogenic/likely pathogenic variant co-exists with a potentially clinically relevant variant in another gene. The latter variants are rare, with allele frequencies ranging between 0.0013 and 0.0000012. The observation of four patients carrying two independent variants of this type among 25 individuals with known pathogenic mutations appears unlikely, given the reported low population frequencies of these variants. However, such frequencies may currently be underestimated due to the underrepresentation of Latin American populations in existing genetic databases (56, 57).If this is the case, these variants may represent neutral polymorphisms and could eventually be reclassified as benign, pending confirmation through larger genetic studies in Latin American cohorts. Nonetheless, in the absence of segregation data, functional validation, or additional tumor phenotype analyses, we cannot rule out the possibility that some of these variants may function as disease modifiers—or, less likely, contribute to digenic inheritance (48).
Regarding genetic counseling, we found 4 monoallelic MUTYH mutation carriers that were notified of their status, based on NCCN guidelines (4), which suggest increased screening only for monoallelic carriers with a personal or first-degree family history of colorectal cancer or polyps.
We also reported the VUSes to the patients. Indeed, we disclosed a novel variant located at 6 pb from the MLH1 intron-exon boundary (variant #6-Table 2), which was later classified as likely pathogenic because Nolano et al (58) demonstrated that it leads to exon 8 skipping.
Our study shows the performance of a 9-gene custom NGS panel for LS mutation identification. The in-house design reduced the cost relative to the commercial alternatives while the platform used is scalable, highlighting its suitability for small-scale healthcare facility in the context of a limited patient population, such as the Uruguayan. Relevant variants were identified in 25 of the 70 patients belonging to independent families, assisted in a single oncogenetic center, and tested using the same methodology, leading to their proper clinical management based on international guidelines. We identified four novel LS disease-causing gene variants and recommended the re-classification of four others as benign.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by the Ethics Committee of Facultad de Medicina, Universidad de la República (Exp. No 07015300038316, UDELAR). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CM: Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. SC: Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. RF: Investigation, Methodology, Writing – review & editing. AD: Conceptualization, Investigation, Resources, Writing – review & editing, Methodology, Validation. FN: Methodology, Resources, Writing – review & editing. JS-S: Conceptualization, Formal analysis, Investigation, Methodology, Resources, Software, Visualization, Writing – review & editing. NA: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Writing – review & editing. MD: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Comisión Sectorial de Investigación Científica (CSIC), Uruguay, grants awarded to NA and MD: “Programa de Vinculación Universidad -Sociedad y Producción (CSIC-PVUSP-2 ID34, 2014)” and “Proyectos de Investigación e Innovación Orientados a la Inclusión Social (CSIC-PIIOIS-ID23, 2016)”.Researchers support to JS-S and MD from PEDECIBA -Programa de Desarrollo de las Ciencias Básicas (Uruguay).
Conflict of interest
CM, SC, RSF, JS-S, and MD are researchers of the Sistema Nacional de Investigadores SNI of the Agencia Nacional de Investigación e Innovación ANII, Uruguay.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1589765/full#supplementary-material.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/CAAC.21660
2. Rebuzzi F, Ulivi P, and Tedaldi G. Genetic predisposition to colorectal cancer: how many and which genes to test? Int J Mol Sci. (2023) 24. doi: 10.3390/ijms24032137
3. Lynch HT and de la Chapelle A. Hereditary colorectal cancer. N Engl J Med. (2003) 348:919–32. doi: 10.1056/NEJMra012242
4. Weiss JM, Gupta S, Burke CA, Axell L, Chen LM, Chung DC, et al. NCCN guidelines® Insights: genetic/familial high-risk assessment: colorectal, version 1. 2021. J Natl Compr Canc Netw. (2021) 19:1122–32. doi: 10.1164/JNCCN.2021.0048
5. National Comprehensive Cancer Network Guidelines. National comprehensive cancer network guidelines. In: NCCN clinical practice guidelines in oncology (NCCN guidelines®) (2023). Available online at: https://www.nccn.org/professionals/physician_gls/pdf/genetics_colon.pdf.
6. Olave MC and Graham RP. Mismatch repair deficiency: The what, how and why it is important. Genes Chromosomes Cancer. (2022) 61:314–21. doi: 10.1002/gcc.23015
7. Muro Y, Sugiura K, Mimori T, and Akiyama M. DNA mismatch repair enzymes: Genetic defects and autoimmunity. Clinica Chimica Acta. (2015) 442:102–9. doi: 10.1016/j.cca.2015.01.014
8. Ligtenberg MJL, Kuiper RP, Geurts Van Kessel A, and Hoogerbrugge N. EPCAM deletion carriers constitute a unique subgroup of Lynch syndrome patients. Fam Cancer. (2013) 12:169–74. doi: 10.1007/s10689-012-9591-x
9. Pitroski CE, Cossio SL, Koehler-Santos P, Graudenz M, Prolla JC, and Ashton-Prolla P. Frequency of the common germline MUTYH mutations p.G396D and p.Y179C in patients diagnosed with colorectal cancer in Southern Brazil. Int J Colorectal Dis. (2011) 26:841–6. doi: 10.1007/S00384-011-1172-1
10. Sieber OM, Lipton L, Crabtree M, Heinimann K, Fidalgo P, Phillips RKS, et al. Multiple colorectal adenomas, classic adenomatous polyposis, and germ-line mutations in MYH. New Engl J Med. (2003) 348:791–9. doi: 10.1056/nejmoa025283
11. Morak M, Heidenreich B, Keller G, Hampel H, Laner A, de la Chapelle A, et al. Biallelic MUTYH mutations can mimic Lynch syndrome. Eur J Hum Genet. (2014) 22:1334–7. doi: 10.1038/ejhg.2014.15
12. Phillips KA, Deverka PA, Hooker GW, and Douglas MP. Genetic test availability and spending: where are we now? Where are we going? Health Aff (Millwood). (2018) 37:710–6. doi: 10.1377/HLTHAFF.2017.1427
13. Soto JL, Blanco I, Díez O, García Planells J, Lorda I, Matthijs G, et al. Consensus document on the implementation of next generation sequencing in the genetic diagnosis of hereditary cancer. Med Clin (Barc). (2018) 151:80.e1–80.e10. doi: 10.1016/J.MEDCLI.2017.12.010
14. Tutlewska K, Lubinski J, and Kurzawski G. Germline deletions in the EPCAM gene as a cause of Lynch syndrome - literature review. Hered Cancer Clin Pract. (2013) 11. doi: 10.1186/1897-4287-11-9
15. Putri GH, Anders S, Pyl PT, Pimanda JE, and Zanini F. Analysing high-throughput sequencing data in Python with HTSeq 2.0. . Bioinf. (2022) 38:2943–5. doi: 10.1093/BIOINFORMATICS/BTAC166
16. Birolo G and Telatin A. BamToCov: An efficient toolkit for sequence coverage calculations. Bioinformatics. (2022) 38:2617–8. doi: 10.1093/bioinformatics/btac125
17. Yang H and Wang K. Genomic variant annotation and prioritization with ANNOVAR and wANNOVAR. Nat Protoc. (2015) 10:1556–66. doi: 10.1038/nprot.2015.105
18. Xiao Chang KW. wANNOVAR: annotating genetic variants for personal genomes via the web. J Med Genet. (2012) 49:433–6. doi: 10.1136/jmedgenet-2012-100918
19. Wang K, Li M, and Hakonarson H. ANNOVAR: functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. (2010) 38:e164. doi: 10.1093/nar/gkq603
20. Robinson JT, Thorvaldsdóttir H, Wenger AM, Zehir A, and Mesirov JP. Variant review with the integrative genomics viewer. Cancer Res. (2017) 77:e31–4. doi: 10.1158/0008-5472.CAN-17-0337
21. Robinson JT, Thorvaldsdóttir H, Winckler W, Guttman M, Lander ES, Getz G, et al. Integrative genomics viewer. Nat Biotechnol. (2011) 29:24–6. doi: 10.1038/nbt.1754
22. Lefter M, Vis JK, Vermaat M, den Dunnen JT, Taschner PEM, and Laros JFJ. Mutalyzer 2: next generation HGVS nomenclature checker. Bioinformatics. (2021) 37(18):2811-7. doi: 10.1093/bioinformatics/btab051
23. Della Valle A, Neffa F, Esperon P, Vergara C, Carusso F, Menini M, et al. Impact of microsatellite instability in colon cancer. J Cancer Sci Ther. (2019) 11:295–8.
24. Bonilla C, Bertoni B, Hidalgo PC, Artagaveytia N, Ackermann E, Barreto I, et al. Breast cancer risk and genetic ancestry: A case-control study in Uruguay. BMC Womens Health. (2015) 15. doi: 10.1186/S12905-015-0171-8
25. Chen S, Francioli LC, Goodrich JK, Collins RL, Kanai M, Wang Q, et al. A genomic mutational constraint map using variation in 76,156 human genomes. Nature. (2024) 625:92–100. doi: 10.1038/s41586-023-06045-0
26. Genome Aggregation Database (gnomAD) browser . Available online at: https://gnomad.broadinstitute.org/. (Accessed June 10, 2024).
27. Landrum MJ, Lee JM, Benson M, Brown GR, Chao C, Chitipiralla S, et al. ClinVar: improving access to variant interpretations and supporting evidence. Nucleic Acids Res. (2018) 46:D1062–7. doi: 10.1093/nar/gkx1153
28. ClinVar. Available online at: https://www.ncbi.nlm.nih.gov/clinvar/.
29. Landrum MJ, Lee JM, Riley GR, Jang W, Rubinstein WS, Church DM, et al. ClinVar: public archive of relationships among sequence variation and human phenotype. Nucleic Acids Res. (2014) 42:D980–5. doi: 10.1093/nar/gkt1113
30. Human gene mutation database (HGMD) . Available online at: https://www.hgmd.cf.ac.uk/ac/index.php. (Accessed June 10, 2024).
31. Stenson PD, Ball EV, Mort M, Phillips AD, Shiel JA, Thomas NST, et al. Human gene mutation database (HGMD): 2003 update. Hum Mutat. (2003) 21:577–81. doi: 10.1002/humu.10212
32. InSiGHT. Available online at: https://www.insight-database.org/. (Accessed June 10, 2024).
33. Thompson BA, Spurdle AB, Plazzer J-P, Greenblatt MS, Akagi K, Al-Mulla F, et al. Application of a 5-tiered scheme for standardized classification of 2,360 unique mismatch repair gene variants in the InSiGHT locus-specific database. Nat Genet. (2014) 46:107–15. doi: 10.1038/ng.2854
34. Steinhaus R, Proft S, Schuelke M, Cooper DN, Schwarz JM, and Seelow D. MutationTaster2021. Nucleic Acids Res. (2021) 49:W446–51. doi: 10.1093/nar/gkab266
35. Ng PC and Henikoff S. Predicting deleterious amino acid substitutions. Genome Res. (2001) 11:863–74. doi: 10.1101/gr.176601
36. Adzhubei IA, Schmidt S, Peshkin L, Ramensky VE, Gerasimova A, Bork P, et al. A method and server for predicting damaging missense mutations. Nat Methods. (2010) 7:248–9. doi: 10.1038/nmeth0410-248
37. Desmet F-O, Hamroun D, Lalande M, Collod-Béroud G, Claustres M, and Béroud C. Human Splicing Finder: an online bioinformatics tool to predict splicing signals. Nucleic Acids Res. (2009) 37:e67. doi: 10.1093/nar/gkp215
38. Kopanos C, Tsiolkas V, Kouris A, Chapple CE, Albarca Aguilera M, Meyer R, et al. VarSome: the human genomic variant search engine. Bioinformatics. (2019) 35:1978–80. doi: 10.1093/BIOINFORMATICS/BTY897
39. Rossi BM, Palmero EI, López-Kostner F, Sarroca C, Vaccaro CA, Spirandelli F, et al. A survey of the clinicopathological and molecular characteristics of patients with suspected Lynch syndrome in Latin America. BMC Cancer. (2017) 17:1–26. doi: 10.1186/s12885-017-3599-4
40. Manolio TA, Collins FS, Cox NJ, Goldstein DB, Hindorff LA, Hunter DJ, et al. Finding the missing heritability of complex diseases. Nature. (2009) 461:747–53. doi: 10.1038/NATURE08494
41. Rosenthal SH, Sun W, Zhang K, Liu Y, Nguyen Q, Gerasimova A, et al. Development and validation of a 34-gene inherited cancer predisposition panel using next-generation sequencing. BioMed Res Int. (2020) 2020. doi: 10.1155/2020/3289023
42. Soukupova J, Zemankova P, Lhotova K, Janatova M, Borecka M, Stolarova L, et al. Validation of CZECANCA (CZEch CAncer paNel for Clinical Application) for targeted NGS-based analysis of hereditary cancer syndromes. PloS One. (2018) 13:1–22. doi: 10.1371/journal.pone.0195761
43. Spirio L, Olschwang S, Groden J, Robertson M, Samowitz W, Joslyn G, et al. Alleles of the APC gene: an attenuated form of familial polyposis. Cell. (1993) 75:951–7. doi: 10.1016/0092-8674(93)90538-2
44. Sobocińska J, Kolenda T, Teresiak A, Badziąg-Leśniak N, Kopczyńska M, Guglas K, et al. Diagnostics of mutations in MMR/EPCAM genes and their role in the treatment and care of patients with lynch syndrome. Diagnostics (Basel). (2020) 10. doi: 10.3390/DIAGNOSTICS10100786
45. Peltomäki P, Olkinuora A, and Nieminen TT. Updates in the field of hereditary nonpolyposis colorectal cancer. Expert Rev Gastroenterol Hepatol. (2020) 14:707–20. doi: 10.1080/17474124.2020.1782187
46. Pathak SJ, Mueller JL, Okamoto K, Das B, Hertecant J, Greenhalgh L, et al. EPCAM mutation update: Variants associated with congenital tufting enteropathy and Lynch syndrome. Hum Mutat. (2019) 40:142–61. doi: 10.1002/HUMU.23688
47. Agiannitopoulos K, Pepe G, Tsaousis GN, Potska K, Bouzarelou D, Katseli A, et al. Copy number variations (CNVs) account for 10.8% of pathogenic variants in patients referred for hereditary cancer testing. Cancer Genomics Proteomics. (2023) 20:448–55. doi: 10.21873/cgp.20396
48. Seguí N, Mina LB, Lázaro C, Sanz-Pamplona R, Pons T, Navarro M, et al. Germline mutations in FAN1 cause hereditary colorectal cancer by impairing DNA repair. Gastroenterology. (2015) 149:563–6. doi: 10.1053/J.GASTRO.2015.05.056
49. Esperon P, Neffa F, Pavicic W, Spirandelli F, Alvarez K, Mullins MJ, et al. A comprehensive characterization of the spectrum of MUTYH germline pathogenic variants in Latin America. Fam Cancer. (2024) 23, 507–13. doi: 10.1007/s10689-024-00382-3
50. Lagerstedt-Robinson K, Rohlin A, Aravidis C, Melin B, Nordling M, Stenmark-Askmalm M, et al. Mismatch repair gene mutation spectrum in the Swedish Lynch syndrome population. Oncol Rep. (2016) 36:2823–35. doi: 10.3892/OR.2016.5060
51. Yurgelun MB, Allen B, Kaldate RR, Bowles KR, Judkins T, Kaushik P, et al. Identification of a variety of mutations in cancer predisposition genes in patients with suspected lynch syndrome. Gastroenterology. (2015) 149:604e20–613.e20. doi: 10.1053/J.GASTRO.2015.05.006
52. Schneider NB, Pastor T, de Paula AE, Achatz MI, dos Santos ÂR, Vianna FSL, et al. Germline MLH1, MSH2 and MSH6 variants in Brazilian patients with colorectal cancer and clinical features suggestive of Lynch Syndrome. Cancer Med. (2018) 7:2078–88. doi: 10.1002/CAM4.1316
53. Boumehdi AL, Cherbal F, Khider F, Oukkal M, Mahfouf H, Zebboudj F, et al. Germline variants screening of MLH1, MSH2, MSH6 and PMS2 genes in 64 Algerian Lynch syndrome families: The first nationwide study. Ann Hum Genet. (2022) 86:328–52. doi: 10.1111/AHG.12482
54. Padua-Bracho A, Velázquez-Aragón JA, Fragoso-Ontiveros V, Nuñez-Martínez PM, Mejía Aguayo M de la L, Sánchez-Contreras Y, et al. A previously unrecognized molecular landscape of lynch syndrome in the mexican population. Int J Mol Sci. (2022) 23. doi: 10.3390/IJMS231911549
55. Li Y, Fan L, Zheng J, Nie X, Sun Y, Feng Q, et al. Lynch syndrome pre-screening and comprehensive characterization in a multi-center large cohort of Chinese patients with colorectal cancer. Cancer Biol Med. (2022) 19:1235–48. doi: 10.20892/J.ISSN.2095-3941.2021.0585
56. Borda V, Loesch DP, Guo B, Laboulaye R, Veliz-Otani D, French JN, et al. Genetics of Latin American Diversity Project: Insights into population genetics and association studies in admixed groups in the Americas. Cell Genomics. (2024) 4:100692. doi: 10.1016/J.XGEN.2024.100692
57. Ju D, Hui D, Hammond DA, Wonkam A, and Tishkoff SA. Importance of including non-european populations in large human genetic studies to enhance precision medicine. Annu Rev BioMed Data Sci. (2022) 5:321. doi: 10.1146/ANNUREV-BIODATASCI-122220-112550
Keywords: Lynch Syndrome, colorectal cancer, LATAM, NGS, novel variants, germline cancer predisposition
Citation: Mathó C, Chávez S, Fort RS, Della Valle A, Neffa F, Sotelo-Silveira JR, Artagaveytia N and Duhagon MA (2025) Genetic characterization of Lynch syndrome germline variants in a LATAM cohort using a customized NGS gene panel. Front. Oncol. 15:1589765. doi: 10.3389/fonc.2025.1589765
Received: 07 March 2025; Accepted: 11 July 2025;
Published: 01 August 2025.
Edited by:
Bart M. G. Smits, Taconic Biosciences, Inc., United StatesReviewed by:
Nihat Bugra Agaoglu, University of Health Sciences, TürkiyePamela Rivero-García, National Institute of Medical Sciences and Nutrition Salvador Zubirán, Mexico
Copyright © 2025 Mathó, Chávez, Fort, Della Valle, Neffa, Sotelo-Silveira, Artagaveytia and Duhagon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Ana Duhagon, bWR1aGFnb25AZm1lZC5lZHUudXk=; bWR1aGFnb25AZmNpZW4uZWR1LnV5