 Agata Sałek-Zań1*
Agata Sałek-Zań1* Mirosława Püsküllüoğlu1
Mirosława Püsküllüoğlu1 Justyna Jaworska1Agnieszka Pietruszka1Joanna Lompart1Marek Ziobro1Tomasz Banaś2
Justyna Jaworska1Agnieszka Pietruszka1Joanna Lompart1Marek Ziobro1Tomasz Banaś2- 1Department of Clinical Oncology, Maria Sklodowska-Curie National Research Institute of Oncology, Kraków, Poland
- 2Department of Radiation Oncology, Maria Sklodowska-Curie National Research Institute of Oncology, Kraków, Poland
Introduction: Tyrosine kinase inhibitors (TKIs) are the standard treatment options for advanced clear cell renal cell carcinoma (ccRCC), but their toxicities can hinder optimal dosing, affecting clinical outcomes.
Material and methods: A retrospective analysis of 96 patients treated with first-line line sunitinib at the National Research Institute of Oncology, Branch Kraków, Poland was conducted to assess the incidence and prevalence of organ toxicities in ccRCC and their impact on overall survival (OS).
Results: The study included 96 patients. The median number of treatment cycles was 11 (IQR: 19), and the median duration was 63 weeks (IQR: 95). The most common toxicities were gastrointestinal (76.0%), fatigue (61.5%), and cardiovascular (49.0%), with 81.3% of patients experiencing multi-organ toxicity. Dose delays occurred in 37 patients (38.5%), mainly due to gastrointestinal (38.5%) and cardiovascular toxicity (21.9%). Dose reductions were required in 64 patients (66.7%), primarily for gastrointestinal (39.6%) and cardiovascular (16.7%) complications. Cardiotoxicity (p=0.017) correlated with improved OS. No OS differences were observed in enterotoxicity, hematologic, endocrine, dermatologic, or renal toxicity. Patients requiring dose reduction due to cardiotoxicity (p=0.012), hematologic toxicity (p=0.004) or gastrointestinal toxicity (p=0.004) had better survival than those without modifications. Patients requiring dose reduction due to any cause had better OS than those maintaining the initial dose. The timing or frequency of dose reductions had no significant impact.
Conclusions: Cardiotoxicity, gastrointestinal and hematologic toxicities requiring dose reduction were associated with improved survival, suggesting these toxicities may reflect treatment efficacy. The findings emphasize the need to balance toxicity and treatment continuity.
1 Introduction
Renal cell carcinoma (RCC) is a global health concern, with 434,419 new cases and 155,702 deaths in 2022. Its incidence is higher in regions with a high Human Development Index, driven by obesity, hypertension, and improved diagnostics (1). Clear cell RCC (ccRCC), comprising 80% of renal tumors, has unique genetic features (2, 3). While localized cases may be cured by resection, recurrence and metastasis are common, influenced by clinical and therapeutic factors (4). Advances in clear cell RCC (ccRCC) pathogenesis, particularly Von Hippel-Lindau (VHL) gene dysregulation, have led to vascular endothelial growth factor receptor (VEGFR) tyrosine kinase inhibitors (TKIs) such as sunitinib, pazopanib, and cabozantinib, which are treatment options for advanced ccRCC by targeting VEGF-driven angiogenesis (5–7). While improving progression-free survival (PFS) and overall survival (OS) in advanced ccRCC, these agents’ toxicities often limit treatment duration, affect quality of life (QoL), and require dose adjustments, impacting adherence and survival (6, 8–11). Therefore, understanding the incidence and prevalence of these toxicities is vital for optimizing treatment strategies and improving survival in ccRCC patients.
TKIs toxicities can reduce the ability to maintain optimal dosing, which is critical for maximizing clinical benefits in patients with advanced ccRCC. Gastrointestinal toxicities, including diarrhea, nausea, and hepatotoxicity frequently occur with TKIs (9, 12). Cardiovascular toxicities, notably hypertension and thromboembolic events, are common with TKIs. Sunitinib can cause grade ≥3 hypertension in 15%-49%, with hypertension proposed as a biomarker of VEGF inhibition efficacy (6, 13, 14). However, uncontrolled hypertension may necessitate dose reductions or treatment interruptions, potentially compromising therapeutic efficacy and overall survival. Furthermore, dermatologic toxicities, such as hand-foot syndrome, are common in patients receiving VEGFR-TKIs. Some data suggest that patients treated with sunitinib who develop skin toxicity may experience longer survival (15). Though rarely life-threatening, adverse events (AEs) impair QoL and may require treatment changes affecting disease control. Studies suggest toxicities like hypertension, neutropenia, hypothyroidism, and skin reactions may indicate effective VEGF pathway inhibition and better responses (13–17). Managing toxicities to ensure continuous treatment without compromising quality of life remains a key clinical challenge (6). Ultimately, the management of toxicities associated with VEGFR-TKIs in ccRCC is a balancing act that requires careful monitoring and proactive intervention. The increasing number of new cancer patients is being fueled by an aging population and advancements in diagnostic techniques. Innovative treatments have the potential to enhance patient outcomes, including lowering mortality rates among working-age individuals, which can help mitigate productivity losses (18).
The aim of the study is to evaluate type and prevalence of sunitynib toxicity during first-line therapy of clear cell renal cancer patients. Additionally we assessed the impact of toxicity on the treatment effect.
2 Materials and methods
2.1 Study cohort and data collection
A retrospective analysis included 96 patients treated with sunitinib at the Clinical Oncology Department of the Maria Skłodowska-Curie National Research Institute of Oncology, Branch in Kraków, from January 2019 to June 2022, due to advanced RCC in a clinical practice setting. Before starting treatment, patients signed informed consent for the proposed therapy.
The qualification criteria included: diagnosis of stage IV renal cell carcinoma as defined by the Union for International Cancer Control (19), favorable or intermediate prognosis according to the Memorial Sloan Kettering Cancer Centre (MSKCC) scale (20), the presence of at least one measurable lesion in imaging studies conducted before qualification for treatment and defined according to the Response Evaluation Criteria In Solid Tumors (RECIST) version 1.1 (21). Additionally, for the purposes of this analysis, patients were retrospectively assigned to specific prognostic groups according to the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) scale (22), Clinical and pathological data were obtained from medical records and were anonymized. Adverse events were assessed according to Common Terminology Criteria for Adverse Events v 5.0 (CTCAE v 5.0) (23).
In case of AEs Grade ≥3, in accordance with the applicable guidelines and recommendations contained in the summary of product characteristics, therapy should be discontinued (7, 24, 25). In the event of a reduction in the intensity or cessation of a particular adverse event, it was possible to return to therapy at the initial dose or at a reduced dose (12, 24, 26).
2.2 Treatment protocol
Patients were treated in accordance with the European Union-approved prescribing information for sunitinib. Supplementary Information contains additional details. Treatment was continued until disease progression, the occurrence of unacceptable toxicity, patient death or withdrawal of consent.
Sunitynib is medication administered orally. The dosing regimen for sunitynib is 50 mg per day for 28 days, followed by a 14-day break,. In the situation of adverse event, a reduction to 37 mg per day may be possible, followed by a reduction to 25 mg per day (24).
2.3 Ethical approval
The study received approval from the Bioethics Committee at the Maria Skłodowska-Curie National Research Institute of Oncology – Warsaw Branch (registry number 6/23 dated October 5,2023).
2.4 Statistical analysis
Clinical features, showing non-normal distributions (confirmed by the Kolmogorov–Smirnov test), are presented as medians with interquartile ranges (IQR) or as numbers with percentages (%). Comparisons were made using the Mann–Whitney U test or Kruskal–Wallis ANOVA, with post hoc tests where necessary. Spearman’s rank test assessed correlations. Kaplan–Meier survival curves were generated based on toxicity incidence and prevalence, and Cox’s proportional hazard model identified survival predictors. The F-Cox test compared survival across patient groups. Using Cox proportional hazard model Hazard Ratio (HR) and 95% confidence interval (CI) were calculated for all cases with significant differences in survival curves. A p-value <0.05 was considered significant. Analyses were performed using STATISTICA 12.0 (StatSoft, Tulsa, OK, USA) and MedCalc 17.0.4 (MedCalc Software, Ostend, Belgium.
3 Results
3.1 Patient and treatment characteristics
The median age of participants was 61,50 years (IQR: 14,50): 33 (34,38%) were women and 63 (66,62%) men. There were no significant differences in median age [62,00 years (IQR:16,00) vs. 63,00 years (IQR: 15,00); p=0,256] and BMI [27,58kg/m2 (IQR:6,52) vs. 26,29 kg/m2 (IQR:5,95); p=0,315] at the time of diagnosis between females and males. Table 1 present population characteristic.

Table 1. Characteristic of population.
3.2 Characteristics of treatment received
The median number of cycles of TKI administration was 11,00 (IQR: 19,00) and median therapy duration was 63 (IQR:95,00) weeks. There were no significant differences in median number of cycles and therapy duration between female and males [respectively: 15,00 (IQR: 23) vs. 10 (IQR:14); p=0,133] and 88 weeks (IQR: 133,00) vs. 60 weeks (IQR: 84,00); p=0,0123]. A positive significant correlation between OS and number of administered cycles [R=0,805; p<0,001] as well as treatment time [R=0,814; p<0,001] was confirmed. Table 2 presents characteristic of treatment received.
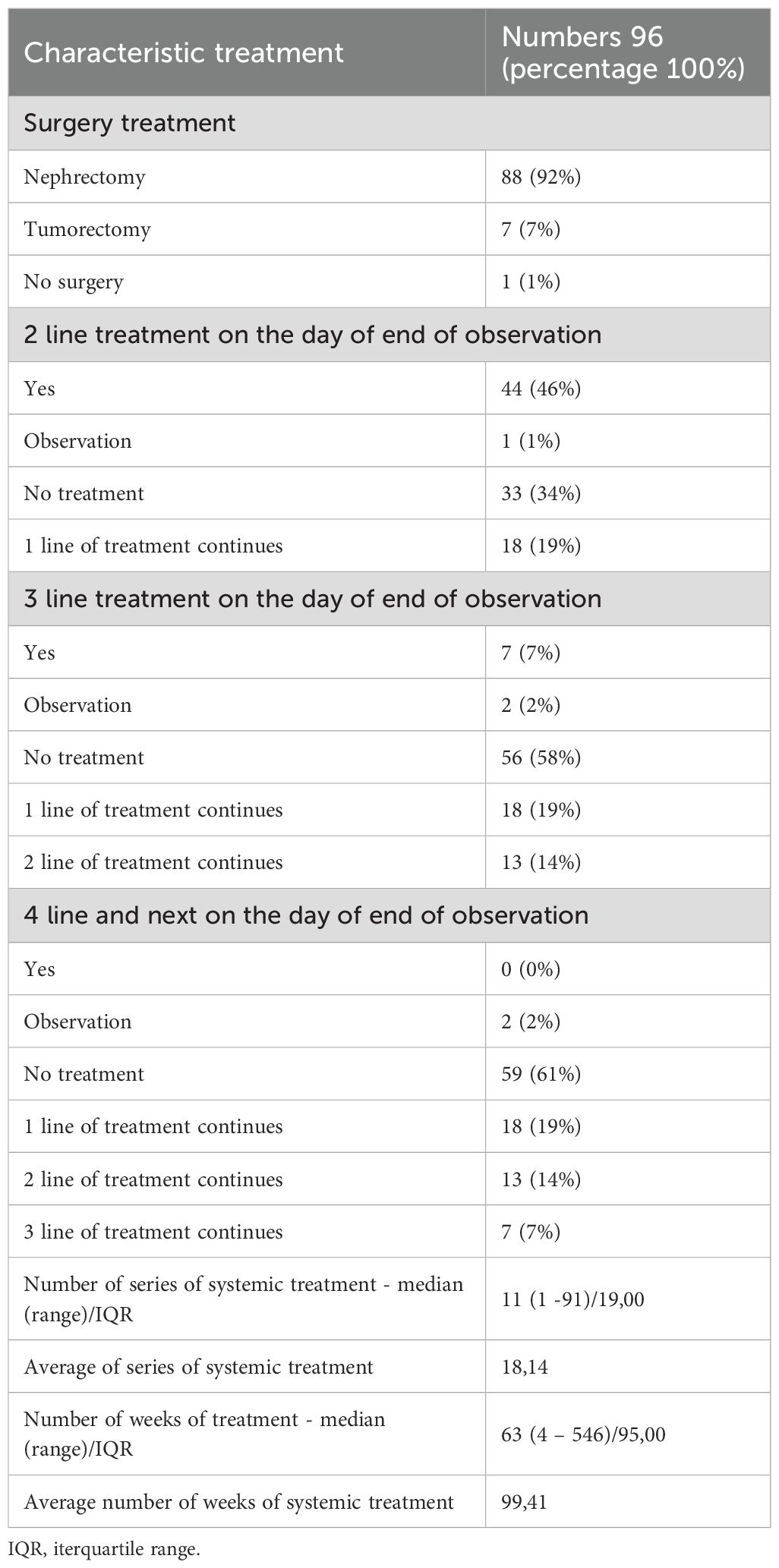
Table 2. Characteristic of treatment received.
3.3 Types of toxicities
The most common AE were related to the gastrointestinal tract – complaints from this system were reported by 76.04% of patients. 61.46% of patients reported fatigue during the course of therapy, although this symptom was rarely reported as an isolated AE. AEs related to the cardiovascular system affected 48.96% of patients. In 81.25% of patients, AEs affecting at least two organs were observed.
64 patients (66.67%) required a dose reduction. Furthermore, 33 patients (34.38%) required a second dose reduction to sustain therapy.
3.3.1 Cardiovascular toxicity
As many as 47 patients (48.96%) experienced cardiovascular toxicity during sunitynib treatment, and in 17 cases (17.71%), these toxicities were reported as dominant. The vast majority—28 patients—presented with grade 2 cardiotoxicity, followed by 10 with grade 1, 8 with grade 3, and only 1 patient developing grade 4 cardiotoxicity.
There were no significant differences in the median age or median BMI between patients with cardiotoxicities compared to those without toxicities. The respective values were 61.00 years (IQR: 15.00) versus 62.00 years (IQR: 15.00) (p=0.725), and 27.58 kg/m² (IQR: 6.52) versus 26.29 kg/m² (IQR: 5.95) (p=0.873). However, significantly more females experienced cardiotoxic effects compared to males [yes: 24/96 vs. no: 6/96; p<0.001].
A total of 17 patients (17.71%) required dose delays due to not acceptable grade 2 and severe (grade ≥3) cardiac complications, and multiple delays were necessary in 8 of these cases. Due to escalating cardiotoxic effects, 16 patients (16.67%) required dose reductions, and 6 patients (6.25%) were disqualified from further therapy.
3.3.2 Hematological toxicity
Thirty-two patients (33.33%) developed hematological toxicities, including 19 cases (19.79%) where these toxicities were reported as dominant. Grade 1 hematotoxicity was reported in 2 patients, 11 patients developed grade 2 toxicity, while grade 3 toxicity was the most common, occurring in 16 cases. Only 3 patients were diagnosed with grade 4 hematotoxicity.
There were no significant differences in median age [60.00 years (IQR: 15.50) vs. 62.00 years (IQR: 12.50); p=0.635] or sex distribution [female-to-male ratio: 12/20 vs. 22/42; p=0.712] between cohorts with and without hematotoxicity. However, the median BMI of patients with hematological toxicities was significantly lower compared to those without complications [26.01 kg/m² (IQR: 5.49) vs. 27.36 kg/m² (IQR: 6.92); p=0.042].
Dose delays due to hematotoxicity were reported in 31 patients, with multiple delays required in 10 cases. Furthermore, 19 patients (19.80%) required dose reductions, and treatment was terminated in 5 patients (5.20%) due to severe hematotoxicity.
3.3.3 Enterotoxicity
Toxicities involving the gastrointestinal tract were diagnosed in 73 patients (76.04%). In 49 cases (20.04%), these toxicities were reported as dominant. The vast majority of patients, 44 (45.85%), developed grade 2 enterotoxicity, followed by 12 (12.50%) with grade 3, 9 (9.37%) with grade 1, and only 2 patients (2.08%) presenting with grade 4 enterotoxicity. Patients who developed enterotoxicity were significantly younger [median age: 60.00 years (IQR: 15.00) vs. 63.00 years (IQR: 10.00); p=0.049] and had a slightly higher but not statistically significant median BMI [27.22 kg/m² (IQR: 6.41) vs. 26.00 kg/m² (IQR: 5.60); p=0.418] compared to those without enterotoxicity. There were no significant differences in gender prevalence between the analyzed cohorts [female-to-male: 27/46 vs. 6/17; p=0.435]. Dose delays due to enterotoxicity were required in 37 patients (38.54%). Dose reductions were performed in 38 patients (39.58%), and treatment was terminated in 3 patients (3.13%) due to severe side effects.
3.3.4 Endocrinological toxicity
Endocrine toxicity occurred in 31 patients (32.29%), but it was reported as dominant in only 6 cases (6.25%). The vast majority, 26 patients (27.08%), developed grade 2 toxicity, while 4 (4.17%) experienced grade 1 toxicity, and only one patient (1.04%) was diagnosed with grade 3 toxicity. There were no significant differences in median age or median BMI between patients who developed endocrine toxicities compared to those who did not [61.00 years (IQR: 17.00) vs. 62.00 years (IQR: 14.00); p=0.454, and 26.33 kg/m² (IQR: 4.44) vs. 27.18 kg/m² (IQR: 6.34); p=0.604]. However, there were significantly more women than men in the cohort with endocrine toxicity [female-to-male ratio: 17/14 vs. 16/49; p=0.004]. Due to the low incidence of endocrine toxicity in patients treated with TKIs for renal cancer, dose delays were required in only 6 cases (6.25%), predominantly during the 4th series. Similarly, dose reductions were performed in only 7 cases (7.29%), and no patients required discontinuation of treatment due to endocrine toxicity.
3.3.5 Dermatological toxicity
Forty-three patients (44.79%) experienced dermatological toxicity, and in 25 cases (20.04%), it was reported as dominant. A total of 35 patients (36.46%) developed grade 2 toxicity, 6 (6.25%) developed grade 1 toxicity, and only 2 (2.08%) experienced grade 3 toxicity. Dose delays were required in 24 patients (25.00%) due to toxic symptoms, which mostly occurred after the 2nd treatment series. There were no significant differences in median age or median BMI between patients who developed dermatological toxicities and those who did not [60.50 years (IQR: 15.00) vs. 62.00 years (IQR: 14.00); p=0.169, and 25.57 kg/m² (IQR: 4.92) vs. 27.50 kg/m² (IQR: 6.53); p=0.374]. Similarly, no significant differences were observed in gender distribution between the analyzed cohorts [female-to-male ratio: 27/46 vs. 6/17; p=0.887].
3.3.6 Urological toxicity
Renal toxicity during sunitinib treatment was diagnosed in 24 (25,00%) patients and in 12 (12,50%) was described as dominant. Eight (8,33%) patients developed grade 1 toxicity, the next 8 (8,33%) grade 2 followed by 7 (7,29%) persons with toxicity grade 3 and the only one (1,04%) presented the 4th grade renal toxicity.
Median age [63,00 years (IQR:18,00) vs. 61,00 years (IQR:13,00); p=0], and median BMI [26,86 kg/m2 (IQR:5,17) vs. 29,99 kg/m2 (IQR:6,41); p=0], did not differ significantly between patients who experienced and who did not present renal toxicities. No differences were in gender prevalence between analyzed cohorts [female-to-male: 10/14 vs. 23/49; p=0,385].
Dose-delay was necessarily in 15 (15,63%) patients mostly after 12th series, furthermore 9 (9,36%) persons during TKI treatment required dose reduction and 2 (2,08%) had therapy termination because of severe toxicity.
3.3.7 Fatigue
Fifty-nine (61,5%) participants experienced fatigue during therapy. The vast majority of i.e. 48 (50%) of patients reported fatigue during the first 3 series of TKI treatment. There were no significant differences in median age and median BMI between patients who developed and did not had fatigue [61,00 years (IQR:17,00) vs. 62,00 years (IQR:11,00); p=0,997 and 26,98 kg/m2 (IQR:4,71) vs. 26,79 kg/m2 (IQR:7,84); p=0,980]. No differences were observed in gender prevalence between analyzed cohorts [female-to-male: 22/37 vs. 11/26; p=0,448].
Detailed analysis of toxicities is showed in Tables 3A–G.
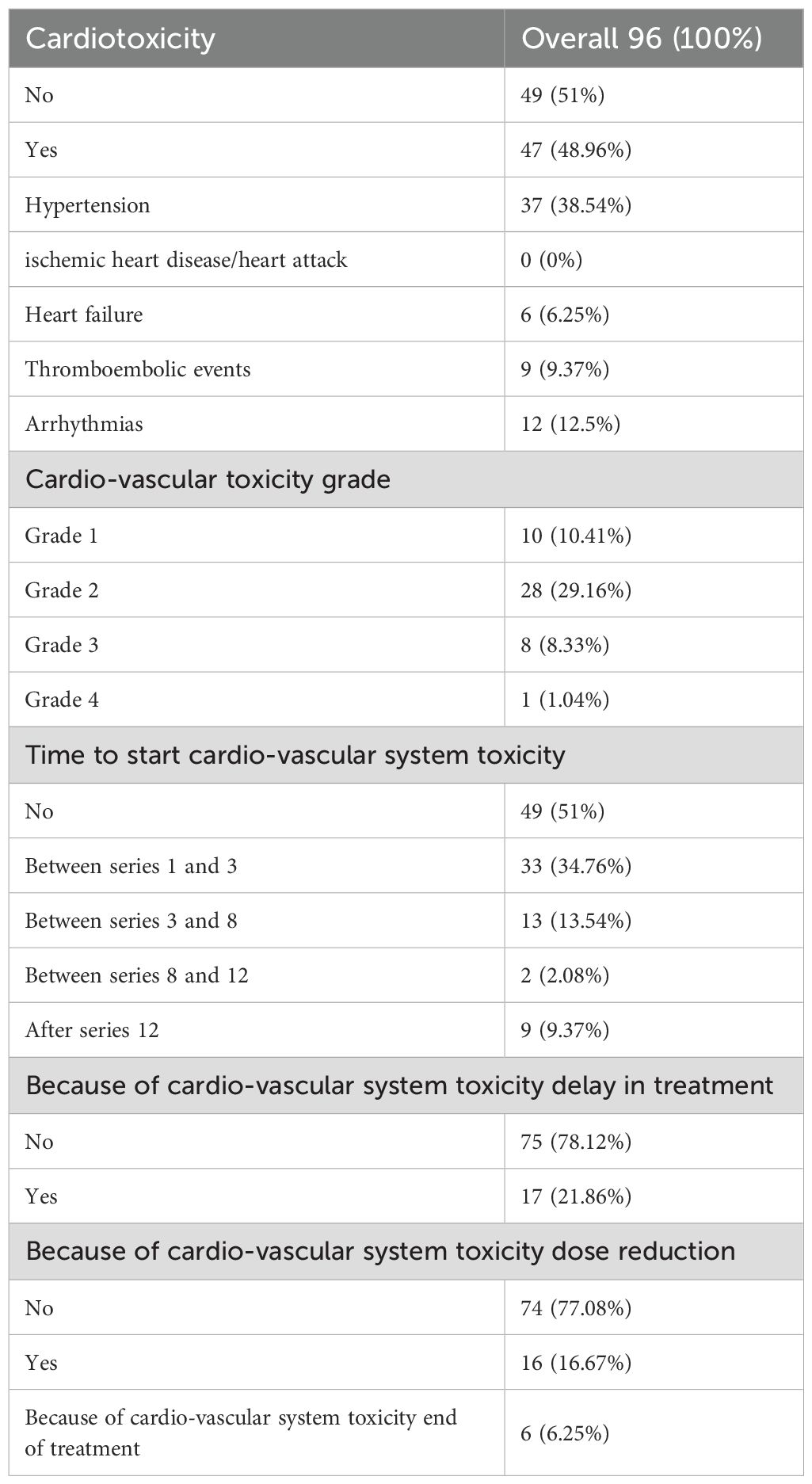
Table 3A. Detailed analysis of cardiotoxicity.
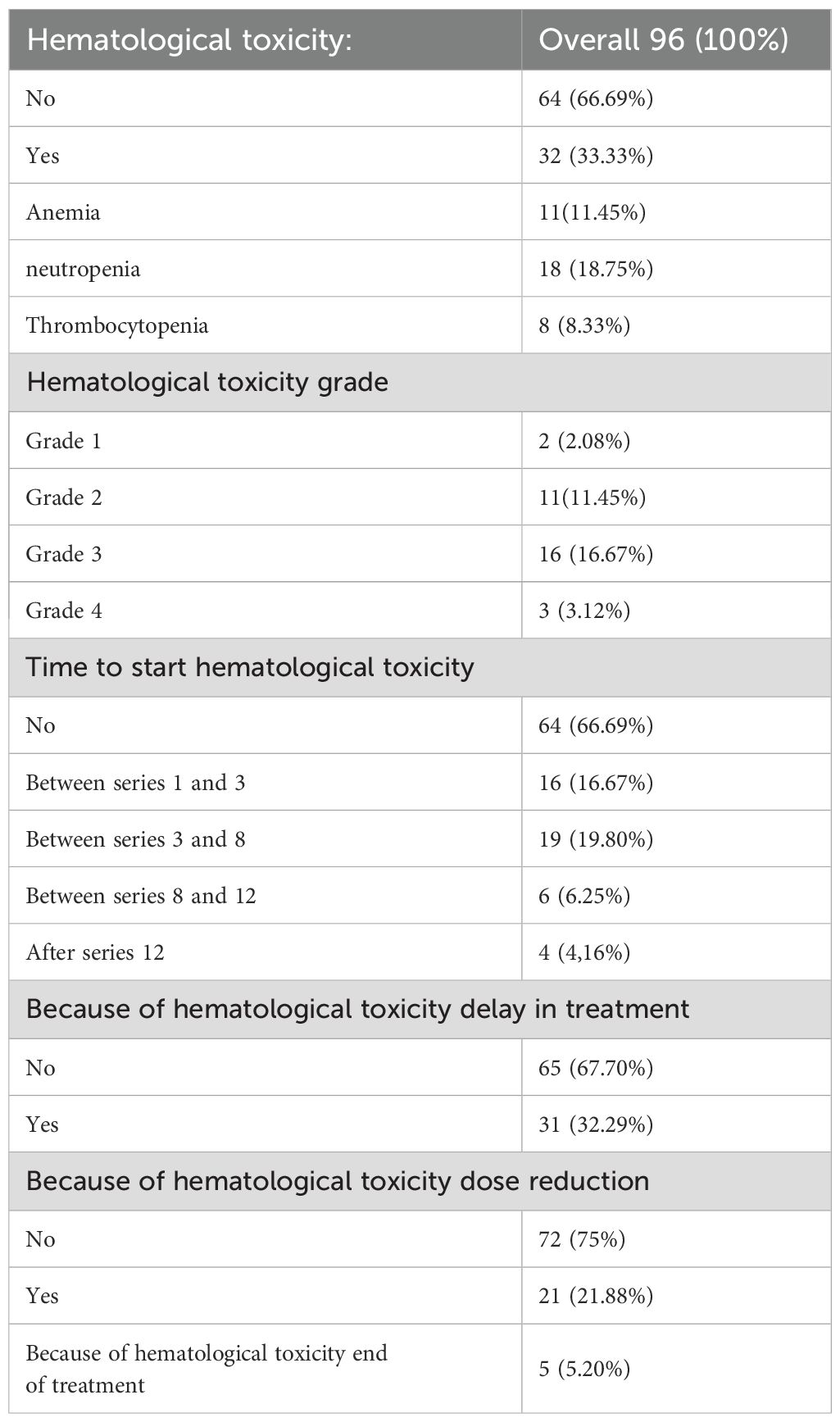
Table 3B. Detailed analysis of hematological toxicity.
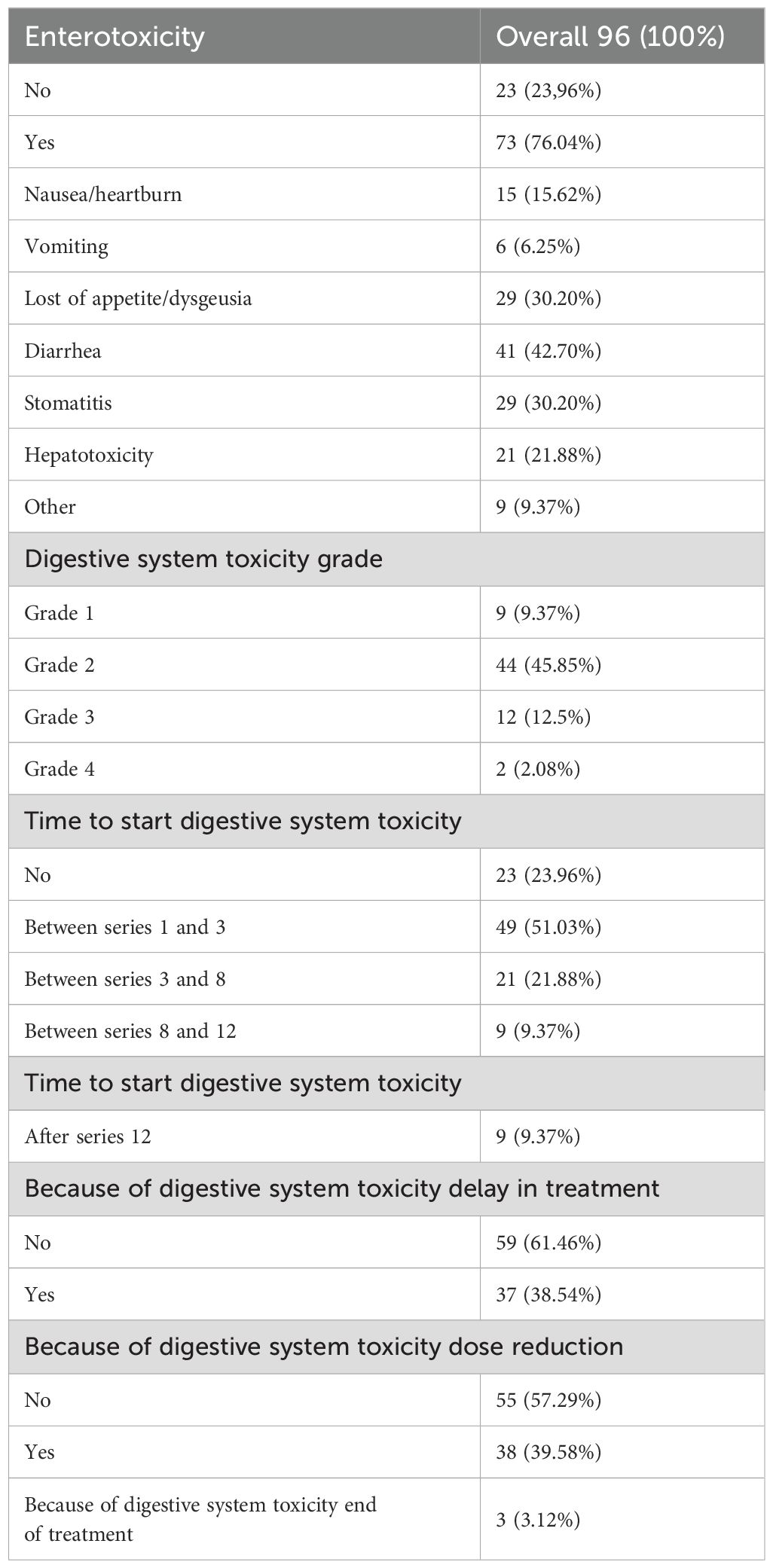
Table 3C. Detailed analysis of gastrointestinal toxicity.
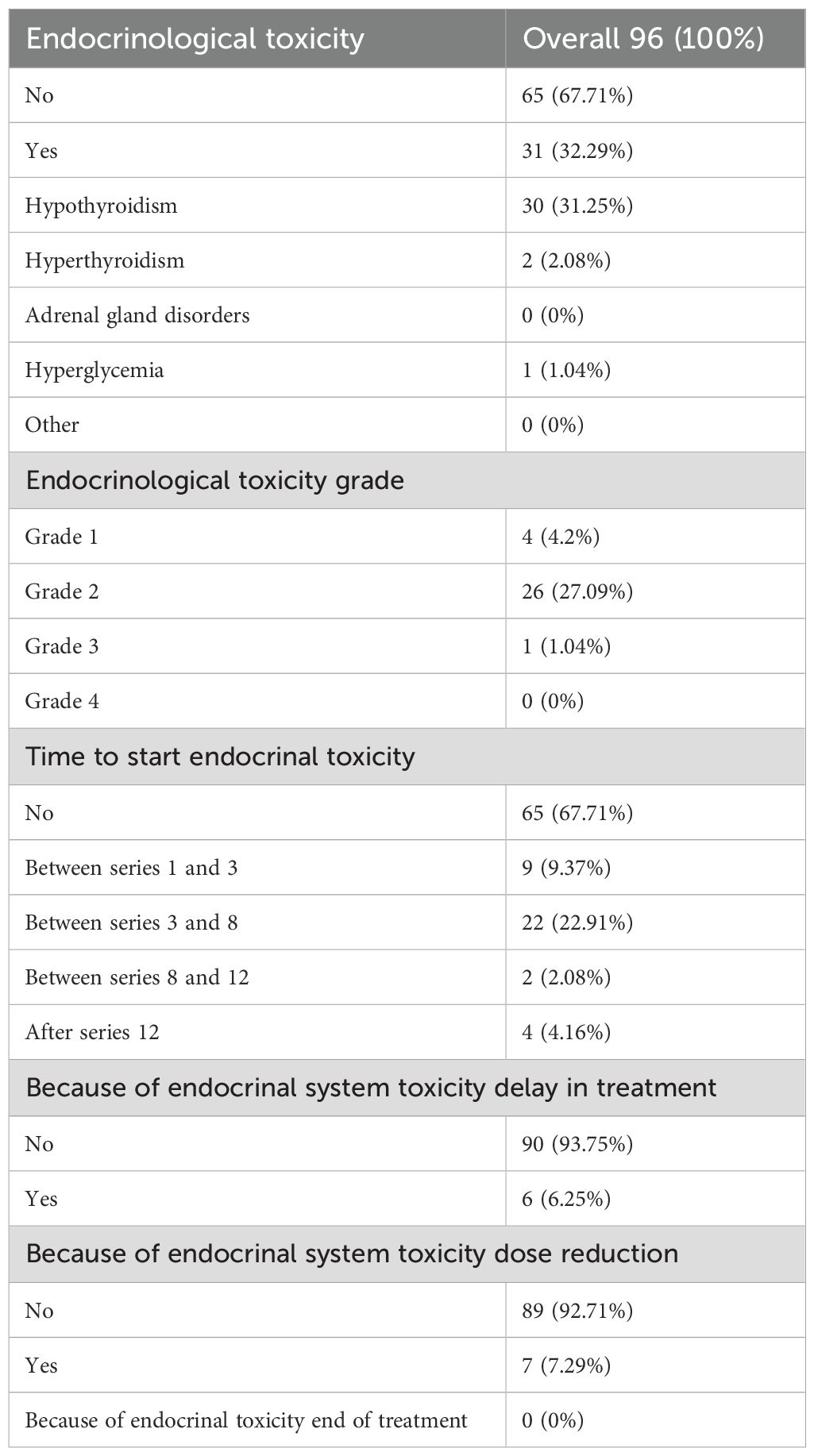
Table 3D. Detailed analysis of endocrinological toxicity.
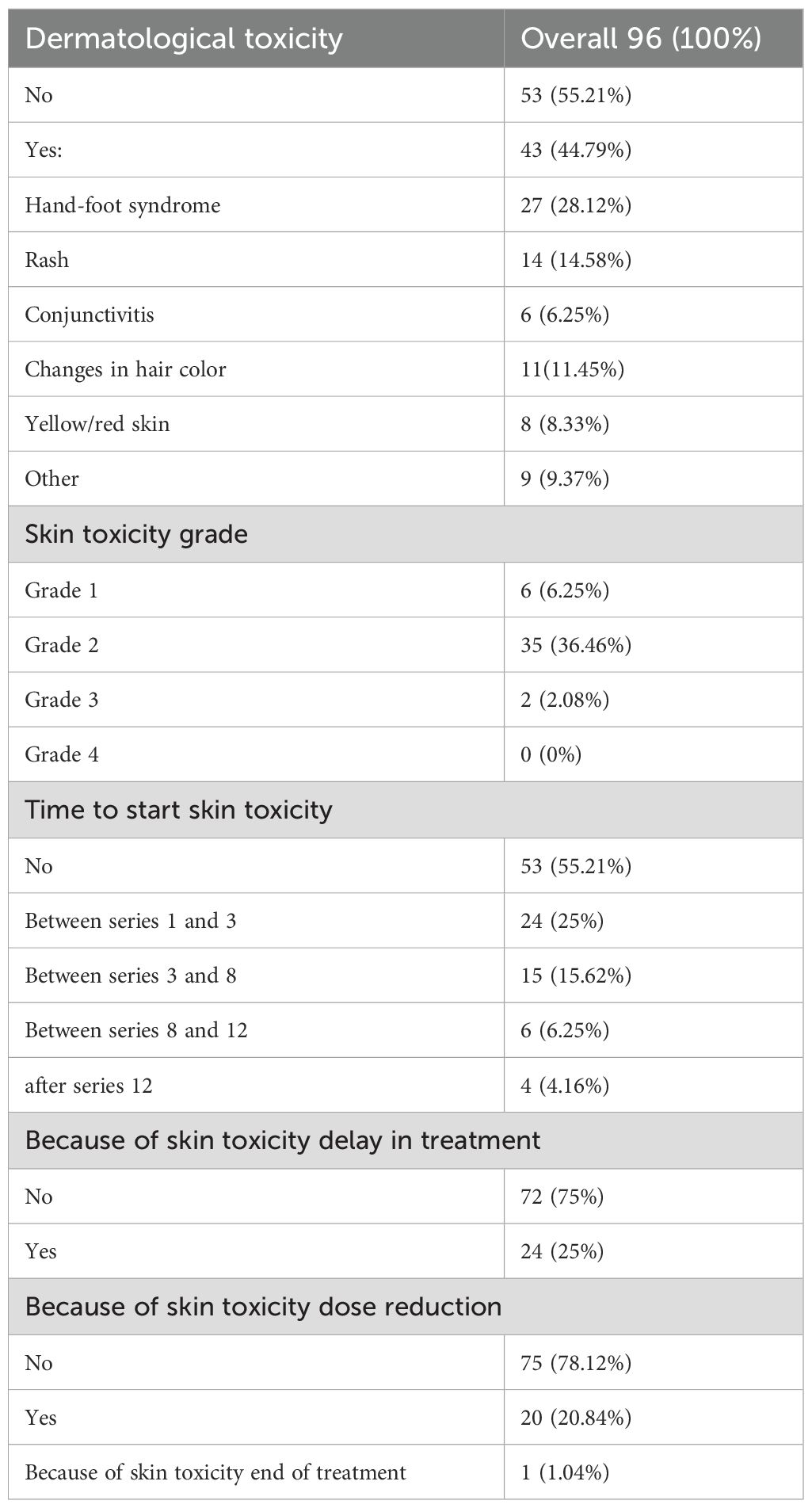
Table 3E. Detailed analysis of dermatological toxicity.
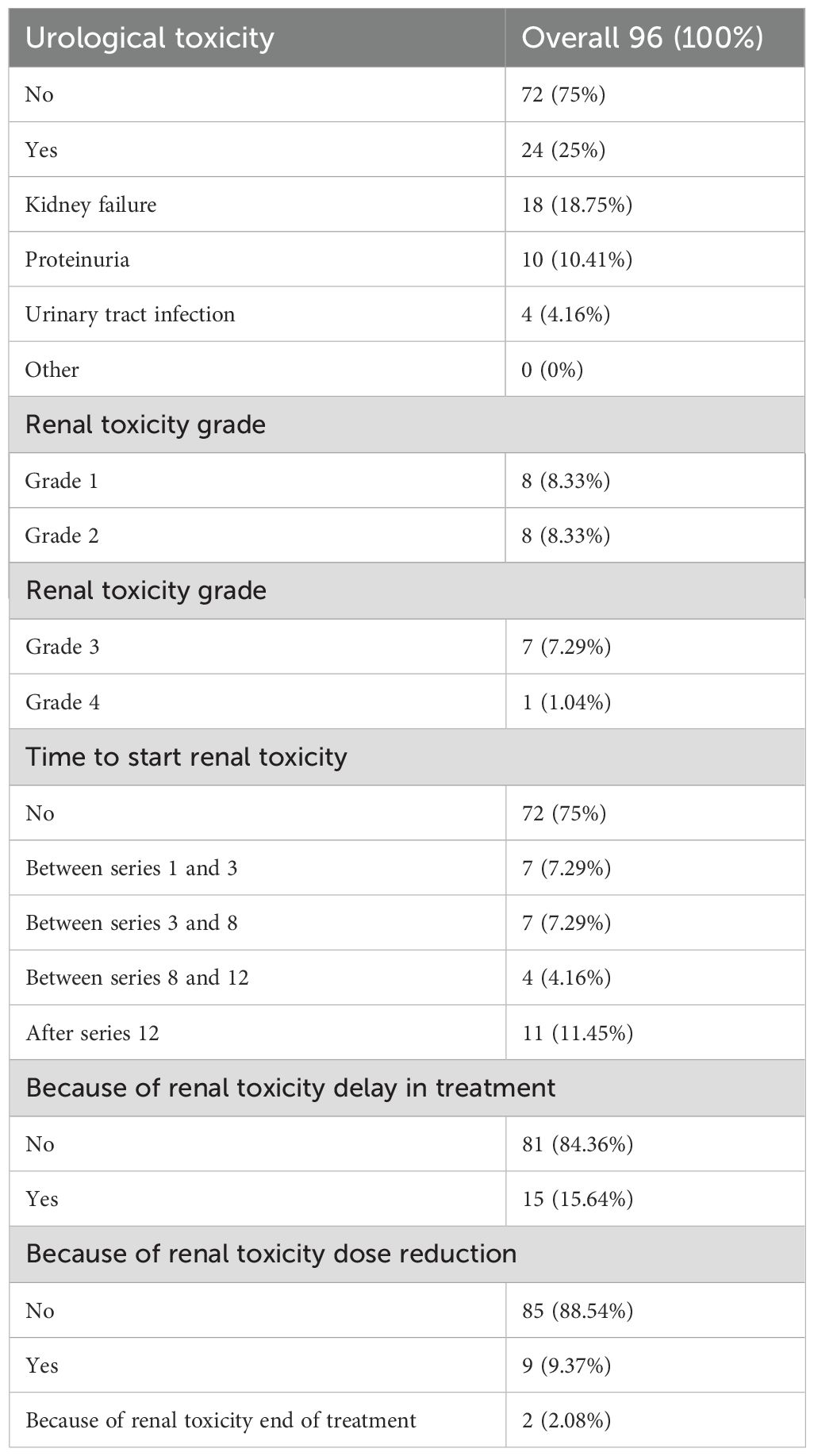
Table 3F. Detailed analysis of renal toxicity.
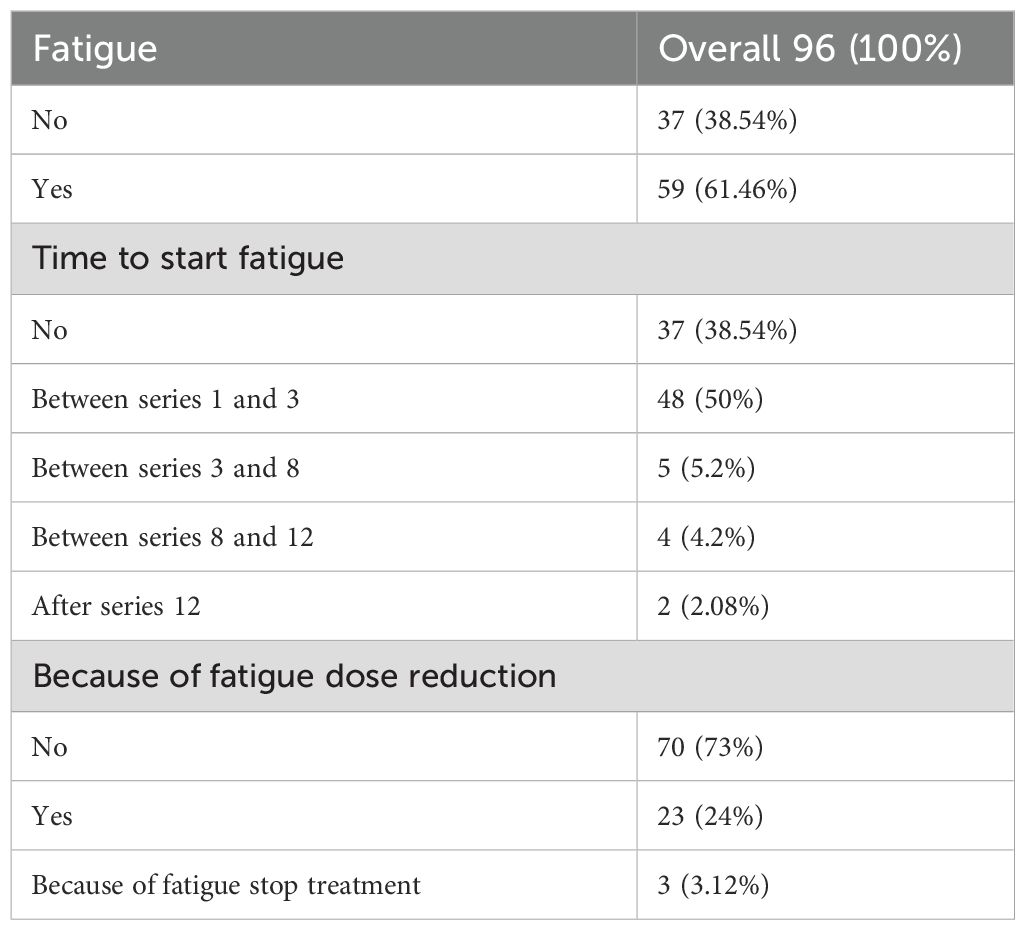
Table 3G. Detailed analysis of fatigue.
3.4 Impact of toxicities on survival
Patients who developed cardiotoxicity showed significantly better survival compared to person with no cardiotoxicity (p=0,017 and HR:0,617; 95%CI: 0,569-0,700)) (Figure 1A1). There was no defenses in survival between patients who had dose-delay compared to ones with routine dosing (p=0,068) (Figure 1A2). Six (6,25%) patients required therapy termination due to severe cardiotoxicity and were excluded from further survival analysis due to small sample size. Additionally analysis showed that reduction of sunitynib dose (but not treatment termination) due to cardiotoxic complications improved survival significantly (Figure 1A3) (p=0,012 and HR: 0,365; 95%CI: 0,313-0,427). Furthermore ones who required therapy termination due to severe cardiac side effects showed significantly worse survival compared to patients without dose reduction (HR: 1,871; 95%CI: 1,649-2,123) as well compared to participants with dose reduction (HR: 2,738; 95%CI: 2,344-3,199) (Figure 1A3).
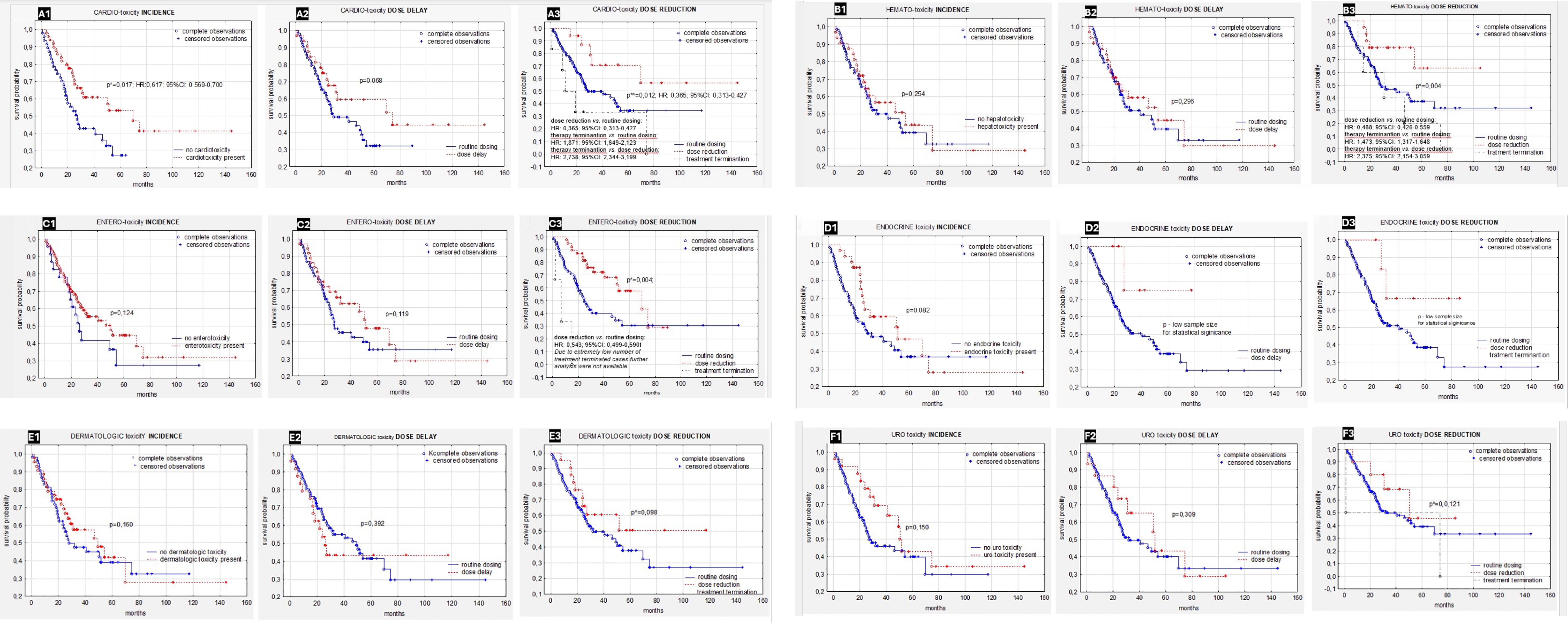
Figure 1. (A-F) Survival in patients with ccRC depending on types of toxicity: (A1) Impact of cardiotoxicity on survival (p=0,017 and HR:0,617; 95%CI: 0,569-0,700). (A2) Impact of dose- delay due to cardiotoxicity on survival. (A3) Impact of dose reduction due to cardiotoxicity on survival (p=0,012 and HR: 0,365; 95%CI: 0,313-0,42). (B1) Impact of hematologic toxicities on survival. (B2) Impact of dose- delay due to hematologic toxicities on survival. (B3) Impact of dose reduction due to hematologic toxicities on survival. (C1) Impact of entero-toxicity on survival. (C2) Impact of dose- delay due to entero-toxicity on survival. (C3) Impact of dose reduction due to entero-toxicity on survival (p=0,004 and HR: 0,543; 95%CI: 0,499-0,590). (D1) Impact of endocrine toxicity on survival. (D2) Impact of dose- delay due to endocrine toxicity on survival. (D3) Impact of dose reduction due to endocrine toxicity on survival. (E1) Impact of dermatologic toxicity on survival. (E2) Impact of dose- delay due to dermatologic toxicity on survival. (E3) Impact of dose reduction due to dermatologic toxicity on survival. (F1) Impact of urological toxicity on survival. (F2) Impact of dose- delay due to urological toxicity on survival. (F3) Impact of dose reduction due to urological toxicity on survival. ccRC, clear cell renal cancer; HR, Hazard Ratio; CI, 95% confidence interval. *p<0.05 is statistically significant.
In contrast to cardiotoxicity, persons who experienced the presence of hematologic toxicities did not showed better survival compared to the ones who did not (Figure 1B1) (p=0,254). Similarly dose delay due to hematologic toxicity that occurred during the therapy did not affect survival (Figure 1B2) (p=0,296). However, patients who underwent dose reduction due to hematologic adverse events performed significantly better survival compared to participants without hematologic toxicity (Figure 1B3) (p=0,004 and HR: 0,488; 95%CI: 0,426-0,559). Counterrally patients who required therapy termination due to hematologic adverse effects showed the worse survivals compared to ones without dose reduction (HR: 1,473; 95%CI: 1,317-1,648) (Figure 1B3).
No significant differences were reported in OS if compared patients with and without entero- toxicity (Figure 1C1) (p=0,124) nightery between persons who had dose delay due compared to those who did not (Figure 1C2) (p=0,119). Patients who required dose reduction due to gastrointestinal toxicity symptoms showed significantly better survival during therapy compared to the ones who did not presented gastrointestinal toxicity (Figure 1C3) (p=0,004 and HR: 0,543; 95%CI: 0,499-0,590). Tree (3,13%) patients had terminated therapy due to sever hepatotoxic complications and were not included in the further dose reduction analysis due to extremely small sample size.
Survival did not differ significantly between patients who experienced endocrine toxicity during TKI therapy compared to the persons who did not (Figure 1D1) (p=0,082). Although survival curves for patients with dose delay or dose reduction show some visual divergence, the analysis did not demonstrate statistically significant differences. Given the small sample size and lack of p-values, no conclusions can be drawn regarding survival impact (Figures 1D2, 1D3).
Persons who experienced dermatological toxicities during sunitinib therapy did not show better overall survival (Figure 1E1) (p=0,160). Similarly, delayed dosing due to toxic symptoms did not impact the patients’ overall survival (Figure 1E2). Patients who required dose reduction during TKI therapy showed better survival, however the difference was insignificant (Figure 1E3) (p=0,098).
Survival of renal cancer patients treated with TKI was influenced neither by presence of urological toxicity nor by delayed dosing due to it (Figures 1F1, 1F2) (p=0,150 and p=0,309). Similarly comparable survival of patients who experienced dose reduction during therapy compared to persons with routine dosing were observed (Figure 1F3) (p=0,121).
Subsequent, comprehensive analysis of the impact of all toxicities resulting from sunitynib therapy showed that patients who required at least one dose reduction, but not treatment termination during TKI treatment had better survival (p<0,001 and HR: 0,376; 95%CI: 0,330-0,389) (Figure 2). The time in which the dose reduction was defined as early (reduction after 1–3 series), medium (reduction after 4–8 series) and long (reduction after 9 series or more) did not significantly affect the survival time of patients treated with this TKI (Figure 3). What is also an interesting finding survival of patients who had only one dose reduction If compared to survival of persons who had reduced dose twice also did not reveal significant difference (Figure 4).
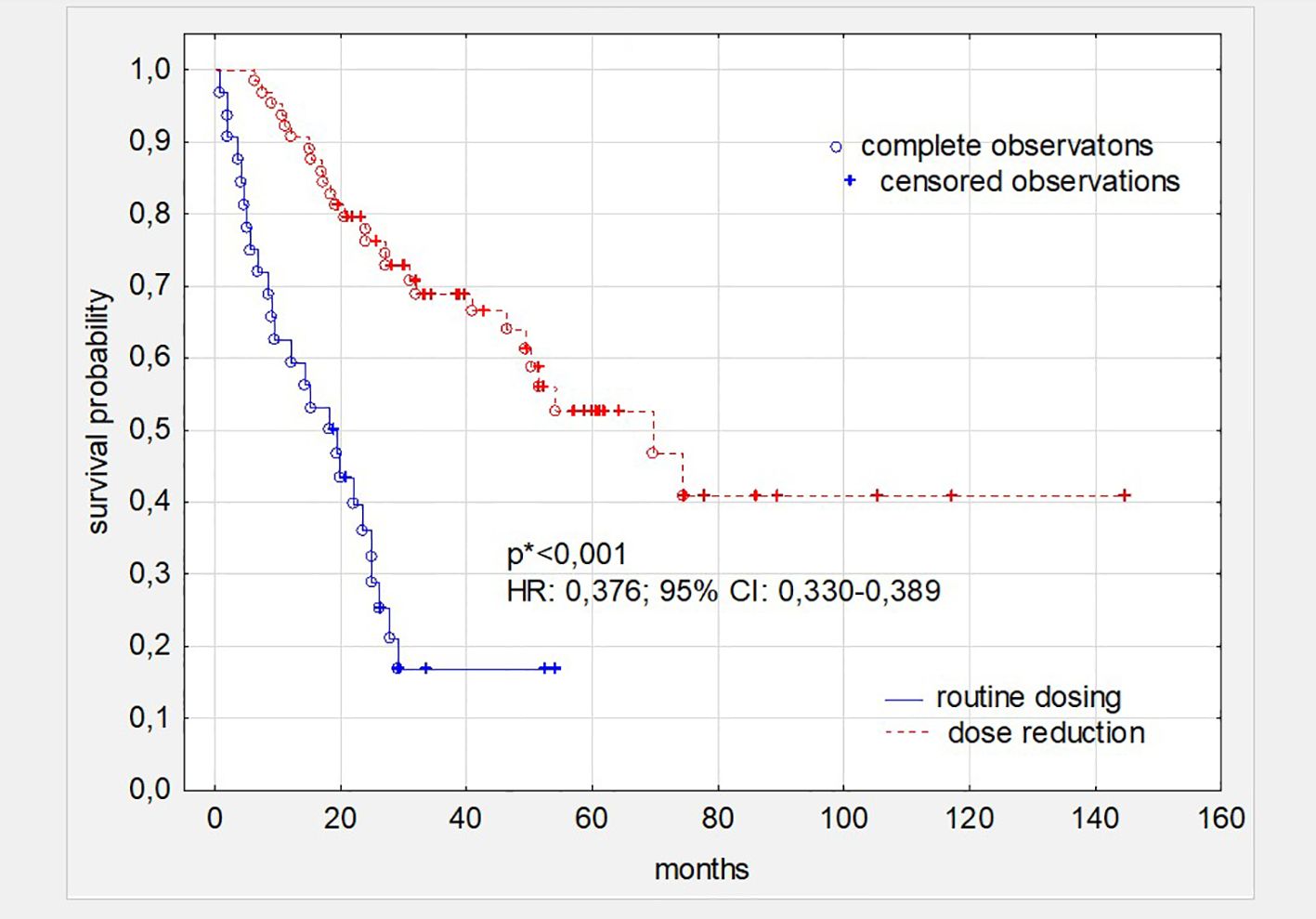
Figure 2. Survival in patients with ccRC depending on dosing. *the level of statistical significance was calculated comparing patients’ cohorts with single and double dose reduction (p<0,001 and HR: 0,376; 95% CI: 0,330-0,389). ccRC, clear cell renal cancer; HR, Hazard Ratio; CI, 95% confidence interval. *p<0.05 is statistically significant.
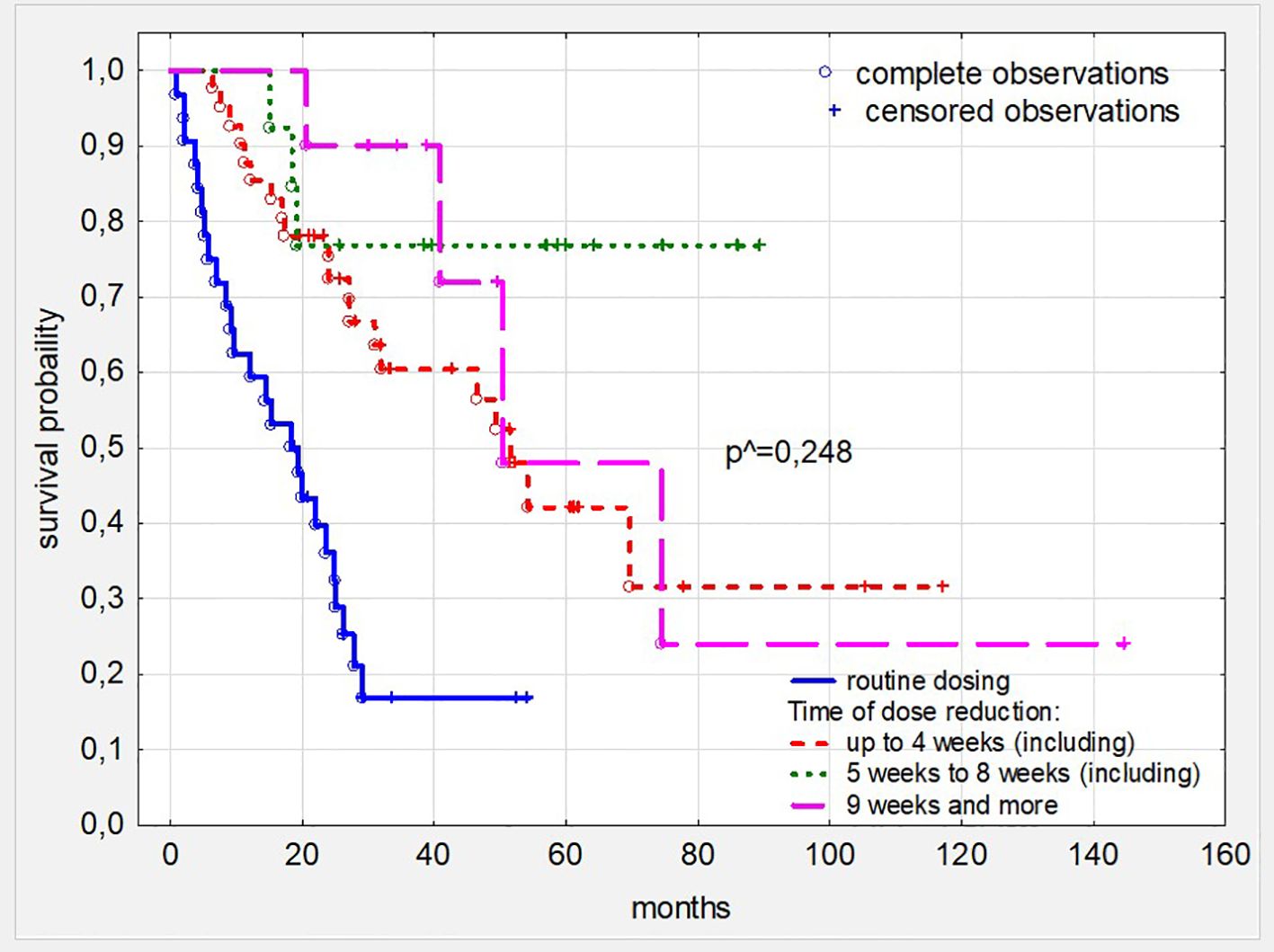
Figure 3. Survival in patients with ccRC depending on the time the dose reduction was introduced. ^ - the level of statistical significance was calculated comparing patients’ cohorts with dose reduction only. ccRC, clear cell renal cancer.
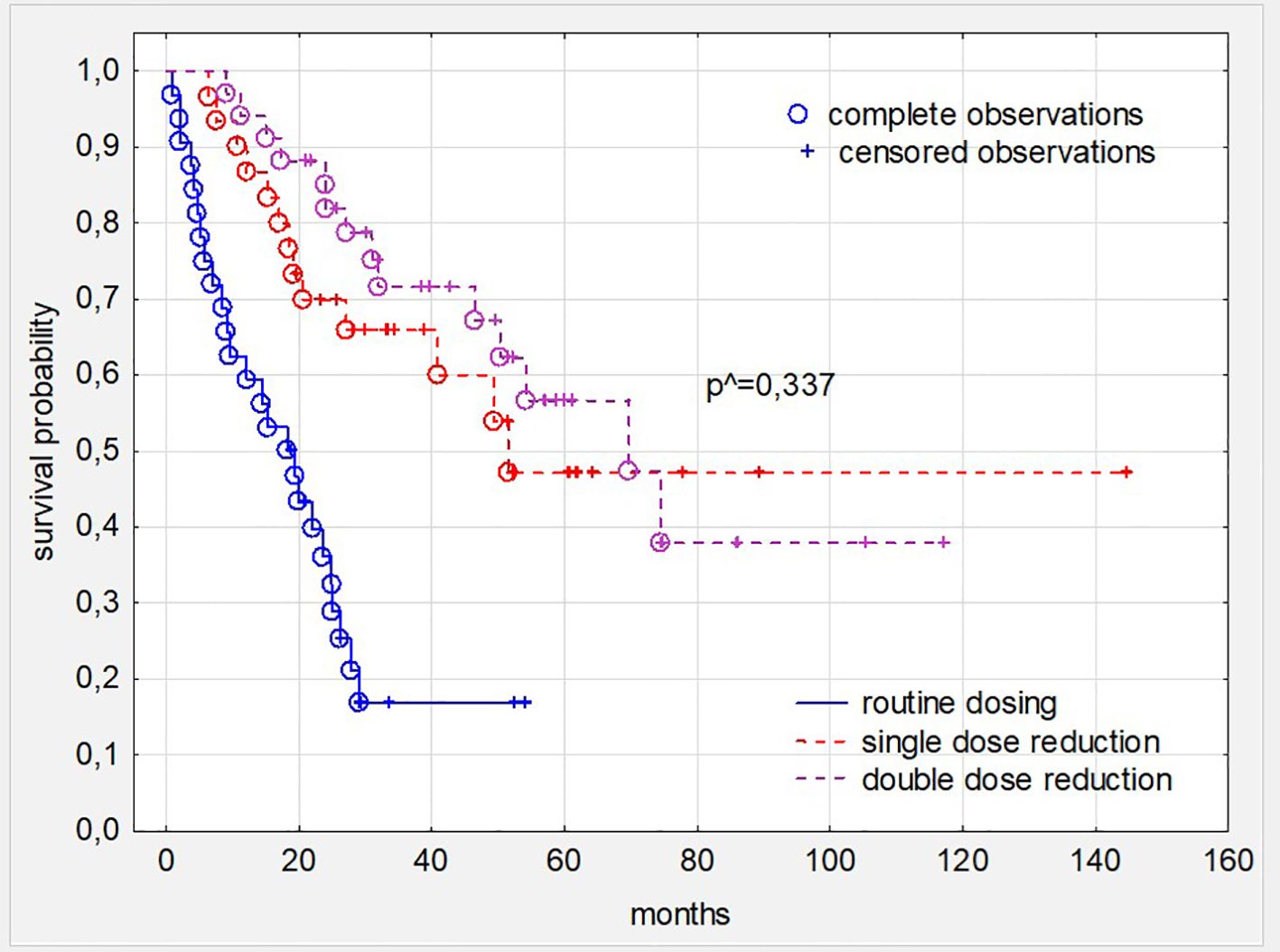
Figure 4. Survival in patients with ccRC depending on dosing schedule and number of required dose reduction due to all toxic symptoms. ^ - the level of statistical significance was calculated comparing patients’ cohorts with single and double dose reduction. ccRC, clear cell renal cancer.
4 Discussion
The study highlights the incidence of organ toxicities associated with sunitynib in advanced RCC, focusing on their impact on OS and treatment duration.
Consistent with prior reports, toxicities emerge as potential biomarkers of sunitinib efficacy. The findings also emphasize the need for individualized treatment and careful toxicity monitoring to optimize outcome.
Cardiotoxicity arises from off-target effects on cardiovascular pathways. VEGFR inhibition by TKIs disrupts endothelial function, reduces nitric oxide, and increases vascular resistance, leading to hypertension and other complications. Direct myocardial toxicity and mitochondrial dysfunction are also implicated (6, 13). In our study, cardiovascular toxicities occurred in 49.0% of sunitinib -treated patients, with hypertension (38.54%) being most common, followed by arrhythmias (12.5%), thromboembolic events (9.37%), and heart failure (6.25%). Severe toxicities (Grade ≥3) affected 9.37%%, leading to dose delays in 21.86%, reductions in 16.67%, and discontinuation in 6.25%. Our 38% hypertension rate aligns with the reported 15%-49% range in the literature (10). Arrhythmias and heart failure, though less common, are significant, with rates of 12% and 7% reported by Rautiola et al., similar to ours (27). Thromboembolic events (9.37% of our patients) align with the 5%-10% reported in the literature (6). Incidence variations may reflect patient demographics, cardiovascular risk, and monitoring. Most toxicities in our study were Grade 2 (20.84%) or 3 (12.5%), consistent with data showing manageable hypertension but severe cases requiring dose adjustments or discontinuation (27, 28). Early cardiotoxicity management is vital for treatment adherence and outcomes (6). In our study, cardiotoxicity was linked to improved survival (p=0.017), with dose reductions further enhancing OS (p=0.012), suggesting cardiotoxicity as a marker of VEGFR inhibition. Similar studies associate hypertension with prolonged PFS and OS (27). Donskov et al. found sunitinib-induced hypertension linked to longer PFS (14 vs. 7 months, p=0.001) and OS (30 vs. 16 months, p=0.002) (13). Our study and published data support cardiotoxicity as a biomarker of efficacy, highlighting the need for proactive management and individualized treatment based on patient risk and toxicity profiles.
As a result of the action of TKIs, there is a blockade of many tyrosine kinase receptors, including the blockade of VEGFR, FMS-like tyrosine kinase 3 (FLT-3) and c-kit receptors, which promote hematopoiesis (29, 30). Additionally, in the case of the c-kit receptor, blockade occurs in hematopoietic stem cells (31). A side effect of chronic TKI use is myelosuppression (32), which manifests as anemia, leukopenia, neutropenia, and thrombocytopenia (32). In our analysis, hematological toxicity occurred in 33.33% of patients. The most common complication was neutropenia, affecting 18.75% of patients. Anemia occurred in 11.45% of patients and, thrombocytopenia affected 9.37% of patients. Most toxicities were Grade 2 or 3 (28.12%). Kumar and al. in their analysis showed, that the most often hematological toxicity was neutropenia - observed in 72% of patients treated with sunitinib and the next was thrombocytopenia, which was observed in 65% of patients (29). Hong et al. found in their analysis that the use of sunitinib is associated with the occurrence of anemia in 69.7% of patients, thrombocytopenia in 77.6%, and neutropenia in 71.1% (33) Donskov et al. noted in their analysis, that neutropenia is significantly associated with both PFS and OS, thrombocytopenia were not significantly associated with either PFS or OS (13).
However in our study we did not noticed, that persons who experienced the presence of hematologic toxicities showed better survival compared to the ones who did not.
We observed, enterotoxicity in 76.04% of patients, with diarrhea, stomatitis, and appetite loss/dysgeusia being the most frequent symptoms. These findings align with Porta et al., who identified diarrhea, stomatitis and mucosal inflammation as common AE in sunitinib-treated patients (34), and Arena et al., who reported stomatitis in 35% of sunitinib-treated patients, mostly of Grade 1–2 severity (35). Most toxicities in our study were mild to moderate, with severe (Grade ≥3) events being rare (15%). Treatment delays occurred in 38.54% of patients and dose reductions in 39.58%. However, no significant differences in OS were found between patients with and without gastrointestinal toxicity or those experiencing dose delays, consistent with Porta et al., who noted no cumulative effect of gastrointestinal toxicities on long-term outcomes (34). Hepatotoxicity was observed in 21.88% of our patients, with Grade 3–4 toxicity in 5 patients (5.2%). In our study hepatotoxicity led to dose reductions in 11.45% of patients and treatment discontinuation in 3.12%.
Hypothyroidism, a common TKI toxicity in advanced RCC, arises from multifactorial mechanisms, including cytotoxicity to thyroid cells, thyroid peroxidase inhibition, disrupted iodine uptake, altered hormone metabolism, and reduced vascularization via VEGFR inhibition (36) The prevalence of Grade 1 and Grade 2 endocrinological toxicities in our study aligns with the lower range of reported rates, with Wu and Huang noticed a 24%-85% incidence across studies with varying methodologies (36). Vasileiadis et al. and Badran et al. reported hypothyroidism rates of 40% and 40.3%, consistent with our findings (37, 38). Bozkurt et al. and Tassi et al. observed slightly higher rates of 42.3% and 45.8%, respectively [39.40]. The differences, though not significant, likely reflect variations in patient characteristics, treatments, and monitoring. Grade 2 hypothyroidism was most common (27.09%), with one Grade 3 case and none of Grade 4, consistent with the typically mild-to-moderate nature reported in the literature (36, 40). Hypothyroidism is manageable with hormone replacement, enabling treatment continuation (36). In our study, endocrine toxicities, including hypothyroidism, showed no significant correlation with OS or PFS. In contrast, Bozkurt et al. reported significantly longer PFS (14 vs. 6 months) and OS (30 vs. 12 months, p=0.001) in patients with sunitinib-induced hypothyroidism (39). Vasileiadis et al. reported a median OS of 32 months in hypothyroid patients vs. 15 months in euthyroid individuals (p=0.03) (37). Buda-Nowak et al. and Badran et al. linked hypothyroidism to improved TKI efficacy, with longer PFS and OS (16, 38). Regular monitoring and management of sunitinib induced hypothyroidism are vital for optimizing outcomes through individualized care.
In our study, 44.79% of patients experienced dermatological toxicity, with HFS (28.12%) and rash (14.58%) being the most common, alongside hair color changes (11.45%). Lee et al. reported HFS in 36% and rash in 20% of sunitinib-treated patients (41). Most toxicities were Grade 1 or 2, with Grade 2 predominating (36.46%), and severe (Grade ≥3) toxicities being rare (2.08%). Treatment delays were noted in 25%, and dose reductions in 20.84%. No significant survival impact was found. Poprach et al. observed better PFS (20.8 vs. 11.1 months, p=0.007) and OS (43.0 vs. 31.0 months, p=0.027) in sunitinib-treated patients with skin toxicities (15).
Early detection and management of these toxicities are critical for maintaining adherence and efficacy, supporting their potential as biomarkers of treatment outcomes.
As a result of using TKIs in patients with mRCC, kidney damage may occur. The causes of this phenomenon may include endothelial damage, secondary autoimmune disorders, or dehydration induced by TKIs (42, 43), but the exact mechanisms of this process are not fully understood (42). The most common adverse effects resulting from kidney damage during TKI treatment are renal function failure and proteinuria (44). However, it should be noted that approximately 50% of patients with mRCC have a reduced glomerular filtration rate (eGFR) before starting treatment (45) or may have proteinuria (46). The presence of these disorders is not an absolute contraindication to the use of TKI therapy (46). In our study 25% of patients experienced renal toxicity, with kidney failure (18.75%) and proteinuria (10.41%). Moreover, 4.16% of patients were diagnosed with urinary tract infection. Toxicities were Grade 1, Grade 2 or Grade 3 at a similar level (23). In our study 76% of patients had increased eGFR before the start of treatment.: In COMPARZ trial an increase in creatinine was observed in 46% during treatment with sunitinib (12). Similar results were presented in the analysis by Mielczarek et al. during sunitinib therapy, an increase in creatinine was recorded in the range of 7.7% to 33% of patients (47). In the analysis conducted by Gupta et al., renal insufficiency was observed in 33% of patients with mRCC treated with TKIs (48). In a meta-analysis presented by Ren et al. kidney injury occurred in approximately 17%, and proteinuria in 29% of patients treated with TKIs. Most adverse events were graded 1 or 2 according to CTCAE (44). Our analysis did not show an impact of renal toxicity on the overall survival results of the studied group of patients. Similar conclusions were reached in the analyses by Mielczarek et al. and Gupta et al., who found that patients with mRCC and renal function impairment treated with anti-VEGF drugs did not differ in terms of response rates, time to treatment failure, and overall survival from patients with normal renal function (47, 48). Macfarlane et al. also noted that reduced eGFR did not affect objective response or overall survival (45). Additionally, Kato et al. in their meta-analysis found that the occurrence or worsening of proteinuria did not show a significant association with a higher risk of death and renal failure. This suggests that anti-angiogenic drugs can be administered to patients regardless of their proteinuria status, although careful assessment of the benefits and harms of this therapy is necessary (46).
An additional element that we assessed in our study was the determination of the frequency of fatigue and the impact of this parameter on treatment outcomes. The causes of fatigue are attributed to symptoms related to cancer, the side effects of cancer therapies, comorbidities of the patient, or psychosocial factors, but the mechanism of fatigue’s onset is not fully understood (49). It is considered one of the main factors influencing treatment effectiveness (49). Fatigue rarely occurs as a singular symptom (50, 51). In our analysis, fatigue was reported by 59 patients (61.46%). Fatigue most commonly occurred during the first 3 cycles of treatment. The occurrence of fatigue alone was not a reason for dose reduction or treatment delay. However, if it occurred alongside symptoms from other organs, dose reduction was implemented in 23 patients (24%). Treatment was discontinued in 3 individuals, but this was not the only reason for discontinuation; it was a contributing factor. In meta-analysis published by Santoni et al., it was shown that fatigue is one of the most commonly reported adverse effects of TKIs (52). In the COMPARZ study, fatigue was noted in 63% of patients using sunitinib (12), while in the study by Ekenel et al., fatigue occurred in 59% of patients (53). Cancer-related fatigue may lead to dose reduction, treatment delays, or early termination of therapy, which can negatively impact treatment outcomes (51). However, Donskov et al. in their analysis showed that the occurrence of fatigue was not significantly associated with either PFS or OS (13).
In phase 3 clinical studies evaluating the efficacy of combination therapies involving immune checkpoint inhibitors (ipilimumab + nivolumab (54)) or combinations of a checkpoint inhibitor with a kinase inhibitor (pembrolizumab + lenvatinib (55), pembrolizumab + everolimus (55), nivolumab + cabozantinib (56), pembrolizumab + axitinib (57)) as first-line treatment for advanced renal cell carcinoma, sunitinib served as the comparator (54–57). In these studies, the secondary endpoint was the safety of the investigated therapy compared to the control medication (54–57). In the CheckMate 214 study, adverse events (AEs) of any grade occurred in 97% of patients treated with sunitinib, and treatment was discontinued due to AEs in 12% of them (54). In the CLEAR study, 98.5% of patients treated with sunitinib experienced any AEs, and AEs of any grade led to discontinuation of the drug in 14.4% of cases (55). In the CheckMate 9ER study, adverse events (AEs) of all severities were observed in 99.1% of patients treated with sunitinib, with 16.9% discontinuing treatment due to AEs (56). Similarly, in the KEYNOTE-426 trial, any-grade AEs were reported in 99.5% of patients receiving sunitinib, leading to discontinuation in 13.9% of cases (57). In each of these studies, treatment discontinuation due to AEs was more common in the experimental groups (54–57).
Recently, there has been an increasing number of publications concerning the optimization of TKI dosage. Several studies have confirmed that low doses of TKIs can effectively maintain clinical response (58). In our analysis, we demonstrated that reducing the dose, regardless of which stage of therapy it occurred, extended the survival time of patients whose doses were decreased. The doses were reduced in 66,67% of patients. According to Powles et al., the dose reduction applied to 26% of patients treated with sunitinib (59). And In the COMPARZ study, dose reduction was observed in 51% of patients treated with sunitinib (12). However, none of these studies analyzed the impact of dose reduction on survival. An alternative method of use sunitinib: 2 weeks on/1 week off dosing schedule, reported to improve tolerability (60–62), was not used in our cohort due to reimbursement limitations at that time, but may represent a viable option in clinical practice.
The apparent similarity in survival between patients with dose delay and those with dose reduction may be explained by the frequent overlap between these subgroups, as many patients who experienced a delay in treatment subsequently required dose reduction.
Study limitations
This study has several limitations. Its retrospective design may introduce bias, though data from a structured clinical registry ensure reliability. The single-center setting limits generalizability, but as a high-volume cancer care institution, the findings reflect real-world conditions. The sample size (96 patients) limits subgroup analyses, yet the study provides valuable insights into treatment outcomes and toxicity management. The lack of quality-of-life data precludes a full assessment of toxicity impact, though tolerability was inferred from dose modifications and treatment delays. The three-year follow-up may omit long-term outcomes but captures key therapeutic and toxicity data. This approach was dictated by the limited sample size and the need to asses overall sunitinib toxicity trend. Additionally, in clinical practice, the choice between TKIs is often influenced by factors such as physician preference, patient tolerance, and institutional protocols rather than clear evidence favoring one over the other in terms of toxicity.
Despite these limitations, the study offers meaningful real-world insights into sunitinib use in advanced RCC.
5 Conclusions
This study explores the incidence and impact of sunitynib-induced organ toxicities in advanced RCC, focusing on treatment adherence, dose modifications, and survival in real-world settings. By examining toxicities like cardiotoxicity, it aims to clarify their prognostic significance and inform strategies for optimizing patient management and therefore improve patient outcomes, including reduction of mortality in working-age patients which can reduce productivity loss (17). Moreover in our analysis, we demonstrated that reducing the dose, but not treatment cessation due to AE regardless of which stage of therapy it occurred, extended the survival time of patients whose doses were decreased.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study received approval from the Bioethics Committee at the Maria Skłodowska-Curie National Research Institute of Oncology – Warsaw Branch (registry number 6/23 dated October 5,2023). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because Decision of Ethical Committee (retrospective study).
Author contributions
AS-Z: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. MP: Formal analysis, Supervision, Writing – review & editing. JJ: Data curation, Writing – review & editing. AP: Data curation, Writing – review & editing. JL: Data curation, Writing – review & editing. MZ: Data curation, Writing – review & editing. TB: Conceptualization, Formal analysis, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
AS-Z obtained travel grants and lecture honoraria from Janssen-Cilag, Ipsen, Astra Zeneca, Pierre Fabre, BMS, MSD. MP obtained travel grants and lecture honoraria from AstraZeneca, Roche, Novartis, Elli Lilly, Janssen, Gilead and Amgen.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751
2. Hsieh JJ, Purdue MP, Signoretti S, Swanton C, Albiges L, Schmidinger M, et al. Renal cell carcinoma. Nat Rev Dis Primers. (2017) 3:17009. doi: 10.1038/nrdp.2017.9, PMID: 28276433
3. Michalak M, Kopczyńska A, Antczak A, Milecki T, and Tomczak P. Outcomes of treatment, laboratory results, adverse effects, and tolerability of cancer treatment in patients with metastatic renal cell carcinoma treated with ipilimumab and nivolumab after cytoreductive nephrectomy. NOWOTWORY J Oncol. (2024) 74:344–50. doi: 10.5603/njo.102357
4. Furge KA, Lucas KA, Takahashi M, Sugimura J, Kort EJ, Kanayama HO, et al. Robust classification of renal cell carcinoma based on gene expression data and predicted cytogenetic profiles. Cancer Res. (2004) 64:4117–21. doi: 10.1158/0008-5472.CAN-04-0534, PMID: 15205321
5. Clark PE. The role of VHL in clear-cell renal cell carcinoma and its relation to targeted therapy. Kidney Int. (2009) 76:939–45. doi: 10.1038/KI.2009.296, PMID: 19657325
6. Grela-Wojewoda A, Pacholczak-Madej R, Adamczyk A, Korman M, and Püsküllüoğlu M. Cardiotoxicity induced by protein kinase inhibitors in cancer patient population. Int J Mol Sci. (2022) 23(5):2815. doi: 10.3390/ijms23052815, PMID: 35269958
7. Powles T, Albiges L, Bex A, Comperat E, Grünwald V, Kanesvaran R, et al. Renal cell carcinoma: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. (2024) 35:692–706. doi: 10.1016/j.annonc.2024.05.537, PMID: 38788900
8. Amaro F, Pisoeiro C, Valente MJ, Bastos M de L, Guedes de Pinho P, Carvalho M, et al. Sunitinib versus Pazopanib Dilemma in Renal Cell Carcinoma: New Insights into the In Vitro Metabolic Impact, Efficacy, and Safety. Int J Mol Sci. (2022) 23(17):9898. doi: 10.3390/IJMS23179898/S1, PMID: 36077297
9. Motzer RJ, Hutson TE, McCann L, Deen K, and Choueiri TK. Overall survival in renal-cell carcinoma with pazopanib versus sunitinib. N Engl J Med. (2014) 370:1769–70. doi: 10.1056/NEJMC1400731, PMID: 24785224
10. Sternberg CN, Davis ID, Mardiak J, Szczylik C, Lee E, Wagstaff J, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial. J Clin Oncol. (2010) 28:1061–8. doi: 10.1200/JCO.2009.23.9764, PMID: 20100962
11. Escudier B, Porta C, Bono P, Powles T, Eisen T, Sternberg CN, et al. Randomized, controlled, double-blind, cross-over trial assessing treatment preference for pazopanib versus sunitinib in patients with metastatic renal cell carcinoma: PISCES Study. J Clin Oncol. (2014) 32:1412–8. doi: 10.1200/JCO.2013.50.8267, PMID: 24687826
12. Motzer RJ, Hutson TE, Cella D, Reeves J, Hawkins R, Guo J, et al. Pazopanib versus sunitinib in metastatic renal-cell carcinoma. New Engl J Med. (2013) 369:722–31. doi: 10.1056/NEJMOA1303989/SUPPL_FILE/NEJMOA1303989_DISCLOSURES.PDF
13. Donskov F, Michaelson MD, Puzanov I, Davis MP, Bjarnason GA, Motzer RJ, et al. Sunitinib-associated hypertension and neutropenia as efficacy biomarkers in metastatic renal cell carcinoma patients. Br J Cancer. (2015) 113:1571. doi: 10.1038/BJC.2015.368, PMID: 26492223
14. Rini BI, Cohen DP, Lu DR, Chen I, Hariharan S, Gore ME, et al. Hypertension as a biomarker of efficacy in patients with metastatic renal cell carcinoma treated with sunitinib. JNCI J Natl Cancer Inst. (2011) 103:763. doi: 10.1093/JNCI/DJR128, PMID: 21527770
15. Poprach A, Pavlik T, Melichar B, Puzanov I, Dusek L, Bortlicek Z, et al. Skin toxicity and efficacy of sunitinib and sorafenib in metastatic renal cell carcinoma: a national registry-based study. Ann Oncol. (2012) 23:3137–43. doi: 10.1093/ANNONC/MDS145, PMID: 22700990
16. Buda-Nowak A, Kucharz J, Dumnicka P, Kuzniewski M, Herman RM, Zygulska AL, et al. Sunitinib-induced hypothyroidism predicts progression-free survival in metastatic renal cell carcinoma patients. Med Oncol. (2017) 34(4):68. doi: 10.1007/S12032-017-0928-Z, PMID: 28343336
17. Baldazzi V, Tassi R, Lapini A, Santomaggio C, Carini M, and Mazzanti R. The impact of sunitinib-induced hypothyroidism on progression-free survival of metastatic renal cancer patients: a prospective single-center study. Urol Oncol. (2012) 30:704–10. doi: 10.1016/J.UROLONC.2010.07.015, PMID: 20884255
18. Seweryn M, Banas T, Augustynska J, Lorenc O, Kopel J, Pluta E, et al. The direct and indirect costs of breast cancer in Poland: estimates for 2017–2019. Int J Environ Res Public Health. (2022) 19:16384. doi: 10.3390/ijerph192416384, PMID: 36554267
19. Brierley JD and GMWC. TNM classification of Malignant tumors(UICC-TNM. In: Wittekind C, editor. Union for International Cancer Control (Union Internationale Contre le Cancer; UICC) under the name of TNM Classification of Malignant Tumors(UICC-TNM), 8thedn ed. John Wiley and Sons, Chichester (2017). p. 199–202.
20. Motzer RJ, Bacik J, Mariani T, Russo P, Mazumdar M, and Reuter V. Treatment outcome and survival associated with metastatic renal cell carcinoma of non-clear-cell histology. J Clin Oncol. (2002) 20:2376–81. doi: 10.1200/JCO.2002.11.123, PMID: 11981011
21. Schwartz LH, Litière S, De Vries E, Ford R, Gwyther S, Mandrekar S, et al. RECIST 1.1-Update and clarification: From the RECIST committee. Eur J Cancer. (2016) 62:132–7. doi: 10.1016/J.EJCA.2016.03.081, PMID: 27189322
22. Heng DYC, Xie W, Regan MM, Harshman LC, Bjarnason GA, Vaishampayan UN, et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. Lancet Oncol. (2013) 14:141–8. doi: 10.1016/S1470-2045(12)70559-4, PMID: 23312463
23. Available online at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (Accessed June 29, 2025).
24. Available online at: https://ec.europa.eu/health/documents/community-register/2016/20161109136193/anx_136193_pl.pdf (Accessed June 29, 2025).
25. Version 3.2025 © 2025 National Comprehensive Cancer Network© (NCCN©). Available online at: https://www.nccn.org/professionals/physician_gls/pdf/kidney_blocks.pdf (Accessed June 29, 2025).
26. Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM, Rixe O, et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. (2007) 356:115–24. doi: 10.1056/NEJMOA065044, PMID: 17215529
27. Rautiola J, Donskov F, Peltola K, Joensuu H, and Bono P. Sunitinib-induced hypertension, neutropenia and thrombocytopenia as predictors of good prognosis in patients with metastatic renal cell carcinoma. BJU Int. (2016) 117:110–7. doi: 10.1111/BJU.12940, PMID: 25252180
28. Ivanyi P, Beutel G, Drewes N, Pirr J, Kielstein JT, Morgan M, et al. Therapy of treatment-related hypertension in metastatic renal-cell cancer patients receiving sunitinib. Clin Genitourin Cancer. (2017) 15:280–290.e3. doi: 10.1016/J.CLGC.2016.10.004, PMID: 27863831
29. Kumar R, Crouthamel MC, Rominger DH, Gontarek RR, Tummino PJ, Levin RA, et al. Myelosuppression and kinase selectivity of multikinase angiogenesis inhibitors. Br J Cancer. (2009) 101(10):1717–23. doi: 10.1038/sj.bjc.6605366, PMID: 19844230
30. Barber NA, Afzal W, and Akhtari M. Hematologic toxicities of small molecule tyrosine kinase inhibitors. Target Oncol. (2011) 6:203–15. doi: 10.1007/s11523-011-0202-9, PMID: 22127751
31. Daher-Reyes GS, Bence-Bruckler I, Busque L, Forrest DL, Savoie L, Keating M-M, et al. Comprehensive analysis of hematological parameter changes after TKI discontinuation for treatment-free remission attempt. Blood. (2019) 134:1653. doi: 10.1182/blood-2019-131599
32. Fachi MM, Tonin FS, Leonart LP, Rotta I, Fernandez-Llimos F, and Pontarolo R. Hematological adverse events associated with tyrosine kinase inhibitors in chronic myeloid leukemia: A network meta-analysis. Br J Clin Pharmacol. (2019) 85(10):2280–2291. doi: 10.1111/bcp.13933, PMID: 30907446
33. Hong MH, Kim HS, Kim C, Ahn JR, Chon HJ, Shin S-J, et al. Treatment outcomes of sunitinib treatment in advanced renal cell carcinoma patients: A single cancer center experience in Korea. Cancer Res Treat. (2009) 41(2):67–72. doi: 10.4143/crt.2009.41.2.67, PMID: 19707503
34. Porta C, Gore ME, Rini BI, Escudier B, Hariharan S, Charles LP, et al. Long-term safety of sunitinib in metastatic renal cell carcinoma. Eur Urol. (2016) 69:345–51. doi: 10.1016/J.EURURO.2015.07.006, PMID: 26215605
35. Arena C, Troiano G, De Lillo A, Testa NF, and Lo Muzio L. Stomatitis and VEGFR-tyrosine kinase inhibitors (VR-TKIs): A review of current literature in 4369 patients. BioMed Res Int. (2018) 2018:5035217. doi: 10.1155/2018/5035217, PMID: 29992147
36. Wu J and Huang H. Acquired hypothyroidism in patients with metastatic renal cell carcinoma treated with tyrosine kinase inhibitors. Drug Des Devel Ther. (2020) 14:3977–82. doi: 10.2147/DDDT.S270210, PMID: 33061302
37. Vasileiadis T, Chrisofos M, Safioleas M, Kontzoglou K, Papazisis K, and Sdrolia A. Impact of sunitinib-induced hypothyroidism on survival of patients with metastatic renal cancer. BMC Cancer. (2019) 19(1):407. doi: 10.1186/S12885-019-5610-8, PMID: 31039771
38. Badran A, Elshenawy MA, Shahin A, Aljubran A, Alzahrani A, Eldali A, et al. Efficacy and prognostic factors of sunitinib as first-line therapy for patients with metastatic renal cell carcinoma in an arab population. JCO Glob Oncol. (2020) 6:19–26. doi: 10.1200/JGO.19.00111, PMID: 32031432
39. Bozkurt O, Karaca H, Hacıbekiroglu I, Kaplan MA, Duzkopru Y, Uysal M, et al. Is sunitinib-induced hypothyroidism a predictive clinical marker for better response in metastatic renal cell carcinoma patients? J Chemother. (2016) 28:230–4. doi: 10.1179/1973947815Y.0000000039, PMID: 25948423
40. Tassi R, Baldazzi V, Lapini A, Carini M, and Mazzanti R. Hyperlipidemia and hypothyroidism among metastatic renal cell carcinoma patients taking sunitinib malate. Related or unrelated adverse events? Clin Genitourin Cancer. (2015) 13:e101–5. doi: 10.1016/J.CLGC.2014.08.009, PMID: 25450040
41. Lee WJ, Lee JL, Chang SE, Lee MW, Kang YK, Choi JH, et al. Cutaneous adverse effects in patients treated with the multitargeted kinase inhibitors sorafenib and sunitinib. Br J Dermatol. (2009) 161:1045–51. doi: 10.1111/J.1365-2133.2009.09290.X, PMID: 19558553
42. Shyam Sunder S, Sharma UC, and Pokharel S. Adverse effects of tyrosine kinase inhibitors in cancer therapy: pathophysiology, mechanisms and clinical management. Signal Transduct Target Ther. (2023) 8(1):262. doi: 10.1038/s41392-023-01469-6, PMID: 37414756
43. Xiong Y, Wang Q, Liu Y, Wei J, and Chen X. Renal adverse reactions of tyrosine kinase inhibitors in the treatment of tumors: A Bayesian network meta-analysis. Front Pharmacol. (2022) 13:1023660. doi: 10.3389/fphar.2022.1023660, PMID: 36408227
44. Ren S, Chen X, Zheng Y, Chen T, Hu X, Feng Y, et al. Adverse renal outcomes following targeted therapies in renal cell carcinoma: a systematic review and meta-analysis. Front Pharmacol. (2024) 15:1409022. doi: 10.3389/fphar.2024.1409022, PMID: 38989147
45. Macfarlane R, Heng DYC, Xie W, Knox JJ, McDermott DF, Rini BI, et al. The impact of kidney function on the outcome of metastatic renal cell carcinoma patients treated with vascular endothelial growth factor-targeted therapy. Cancer. (2012) 118(2):365–70. doi: 10.1002/cncr.26201, PMID: 21717427
46. Kato T, Kurasawa S, Takezawa K, Fujiwara Y, Yasuda Y, and Ando Y. Efficacy and safety of anti-angiogenic agents for cancer patients with proteinuria or a history of proteinuria: A systematic review. Anticancer Res. (2024) 44(3):889–894. doi: 10.21873/anticanres.16882, PMID: 38423640
47. Mielczarek Ł, Brodziak A, Sobczuk P, Kawecki M, Cudnoch-Jędrzejewska A, and Czarnecka AM. Renal toxicity of targeted therapies for renal cell carcinoma in patients with normal and impaired kidney function. Cancer Chemother Pharmacol. (2021) 87:723–42. doi: 10.1007/s00280-021-04260-y, PMID: 33768301
48. Gupta S, Parsa V, Heilbrun LKb, Smith DW, Dickow B, Heath E, et al. Safety and efficacy of molecularly targeted agents in patients with metastatic kidney cancer with renal dysfunction. Anti-Cancer Drugs. (2011) 22(8):794–800. doi: 10.1097/CAD.0b013e328346af0d, PMID: 21799472
49. Takahashi S. Fatigue and its management in cancer patients undergoing VEGFR-TKI therapy. Expert Opin Drug Saf. (2022) 21(3):397–406. doi: 10.1080/14740338.2021.1969360, PMID: 34461788
50. Available online at: https://www.nccn.org/professionals/physician_gls/pdf/fatigue.pdf (Accessed June 29, 2025).
51. Anand D and Escalante CP. Ongoing screening and treatment to potentially reduce tyrosine kinase inhibitor-related fatigue in renal cell carcinoma. J Pain Symptom Manage. (2015) 50(1):108–17. doi: 10.1016/j.jpainsymman.2015.02.007, PMID: 25701692
52. Santoni M, Conti A, Massari F, Arnaldi G, Iacovelli R, Rizzo M, et al. Treatment-related fatigue with sorafenib, sunitinib and pazopanib in patients with advanced solid tumors: An up-to-date review and meta-analysis of clinical trials. Int J Cancer. (2015) 136(1):1–10. doi: 10.1002/ijc.28715, PMID: 24415642
53. Ekenel M, Karabulut S, Cil I, Zırtıloglu A, Aydın E, and Tural D. Sunitinib versus pazopanib for patients with metastatic renal cell carcinoma: 2 Turkish hospital experience. Actas Urol Esp (Engl Ed). (2020) 44:27–33. doi: 10.1016/j.acuro.2019.06.007, PMID: 31744648
54. Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. (2018) 378:1277–90. doi: 10.1056/NEJMoa1712126, PMID: 29562145
55. Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. (2021) 384:1289–300. doi: 10.1056/NEJMoa2035716, PMID: 33616314
56. Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2021) 384:829–41. doi: 10.1056/NEJMoa2026982, PMID: 33657295
57. Rini BI, Plimack ER, Stus V, Gafanov R, Hawkins R, Nosov D, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2019) 380:1116–27. doi: 10.1056/NEJMoa1816714, PMID: 30779529
58. Claudiani S, Apperley JF, Szydlo R, Khan A, Nesr G, Hayden C, et al. TKI dose reduction can effectively maintain major molecular remission in patients with chronic myeloid leukemia. Brit J Hematol. (2021) 193(2):346–55. doi: 10.1111/bjh.17286, PMID: 33368155
59. Powles T, Sarwar N, Jones R, Wilson P, Boleti E, Protheroe A, et al. An indirect comparison of the toxicity of sunitinib and pazopanib in metastatic clear cell renal cancer. Eur J Cancer. (2012) 48:3171–6. doi: 10.1016/j.ejca.2012.05.022, PMID: 22766517
60. Atkinson BJ, Kalra S, Wang X, Bathala T, Corn P, Tannir NM, et al. Clinical outcomes for patients with metastatic renal cell carcinoma treated with alternative sunitinib schedules. J Urol. (2014) 191:611–8. doi: 10.1016/j.juro.2013.08.090, PMID: 24018239
61. Mouillet G, Paillard MJ, Maurina T, Vernerey D, Nguyen Tan Hon T, Almotlak H, et al. Open-label, randomized multicenter phase II study to assess the efficacy and tolerability of sunitinib by dose administration regimen (dose modification or dose interruptions) in patients with advanced or metastatic renal cell carcinoma: study protocol of the SURF trial. Trials. (2018) 19:221. doi: 10.1186/s13063-018-2613-8, PMID: 29650037
62. Ito T, Yamamoto K, Furukawa J, Harada K, Fujisawa M, Omura T, et al. Association of sunitinib concentration and clinical outcome in patients with metastatic renal cell carcinoma treated with a 2-week-on and 1-week-off schedule. J Clin Pharm Ther. (2022) 47:81–8. doi: 10.1111/jcpt.13517, PMID: 34669974
Keywords: renal cell carcinoma, tyrosine kinase inhibitors, adverse events, survival, sunitynib
Citation: Sałek-Zań A, Püsküllüoğlu M, Jaworska J, Pietruszka A, Lompart J, Ziobro M and Banaś T (2025) Incidence and prevalence of organ toxicities in patients suffering from clear cell renal carcinoma treated with sunitinib and its impact on survival: a reference cancer center experience. Front. Oncol. 15:1590163. doi: 10.3389/fonc.2025.1590163
Received: 08 March 2025; Accepted: 31 July 2025;
Published: 20 August 2025.
Edited by:
John Peter Sfakianos, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Annalisa Guida, Azienda Ospedaliera Santa Maria Terni, ItalyManish Kumar Singh, Oklahoma Medical Research Foundation, United States
Copyright © 2025 Sałek-Zań, Püsküllüoğlu, Jaworska, Pietruszka, Lompart, Ziobro and Banaś. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agata Sałek-Zań, YWdhdGEuc2FsZWtAa3Jha293Lm5pby5nb3YucGw=