 Adnan Khalid
Adnan Khalid Muhammad Mursil
Muhammad Mursil Carlos López Pablo
Carlos López Pablo Ramon Bosch2
Ramon Bosch2 Domenec Puig
Domenec Puig Hatem A. Rashwan
Hatem A. Rashwan- 1Department of Computer Engineering and Mathematics, Universitat Rovira i Virgili, Tarragona, Spain
- 2Hospital de Tortosa Verge de la Cinta, Institut Catala de la Salut, Tortosa, Spain
Early assessment of breast cancer relapse can significantly impact survival rates and overall oncological outcomes, highlighting the need to use sophisticated diagnostic strategies in clinical trials. This work utilizes clinically relevant radiomic features extracted from digital mammograms to develop a deep learning-based model for forecasting breast cancer relapse. Features, including tumor size, shape, margin characteristics, molecular subtype, and breast density, were systematically extracted from our private, in-house dataset, providing a comprehensive representation of intrinsic tumor properties and assisting in relapse prediction. The predictive model demonstrated outstanding performance with an average area under the curve (AUC) of 0.957, highlighting its effectiveness in identifying possible relapse. This approach not only underscores the abilities of radiomics in enhancing the granularity of tumor assessment but also assists in identifying cancer recurrence during the treatment stage, promising significant strides toward personalized cancer therapy.
1 Introduction
Breast cancer (BC), as the most prevalent malignancy among women globally, presents significant challenges not only in terms of diagnosis but also in monitoring for recurrence. BC relapse has substantial prognostic implications; recurrence frequently indicates a worse prognosis and necessitates more aggressive treatment approaches Graham et al. (1). Targeted adjuvant therapies play a pivotal role in mitigating the risk of relapse based on key biomarkers PR (progesterone receptor), ER (estrogen receptor), and HER2 (human epidermal growth factor receptor Type 2) Boyages et al. (2). At least 85% of patients might receive unnecessary treatment if adjuvant chemotherapy were given to all patients without discrimination Hassett et al. (3). According to Dinan et al. (4), the only multi-gene test supported by the American Society of Clinical Oncology (ASCO) and the National Comprehensive Cancer Network (NCCN) for determining the risk of breast cancer recurrence is Oncotype DX, which was approved by the US FDA in 2005. Although it provides essential prognostic information Sparano et al. (5), its widespread use is limited because of the high cost of around $4,000 per patient. Thus, the development of a non-invasive and precise method for predicting BC recurrence risk holds significant clinical importance.
Advancements in digital mammography and radiomics have significantly enhanced our ability to detect early signs of recurrence through non-invasive methods Mao et al. (6). The integration of radiomics into BC diagnosis has revolutionized the potential of mammography, converting standard imaging into a rich data source that can enlighten hidden disease characteristics and predict clinical outcomes Lambin et al. (7). Quantitative data extraction from mammograms allows characterization of lesion size and shape, and may provide indirect indicators related to margin characteristics. All these characteristics have a relation with molecular subtypes, although these require further validation Ma et al. (8). Breast density has emerged as one of the most critical risk factors for cancer development and recurrence. Women with high breast density are at risk of recurrence following breast-conserving surgery and radiotherapy, as well as an increased likelihood of invasive BC after surgery for ductal carcinoma in situ Park et al (9) Habel et al. (10). BC molecular subtypes (Luminal A, Luminal B, Triple Negative (TN), and HER-2) have significantly influenced recurrence patterns. Notably, women over 50 with HER-2 positive and TN BC subtypes are at a higher risk of local recurrence compared to those with luminal cancers after surgery Ghose et al. (11). Early and accurate prediction of recurrence in these patients from clinical mammograms could facilitate more aggressive and tailored interventions.
Deep learning (DL) has substantially advanced the radiomics field Qi et al. (12), enhancing feature extraction and analysis from medical images for predicting breast cancer relapse Mao et al. (6)Dasgupta et al. (13). Recent work employing DL on mammograms has significantly improved breast density estimation Khara et al. (14) Biroš et al. (15). Techniques such as conditional Generative Adversarial Networks (cGANs) for segmenting high-density areas, when integrated with Fully Convolutional Networks (FCNs), have established benchmarks in density estimation Anyfantis et al. (16)Saffari et al. (17). They achieve more than 98% accuracy in classifying breast densities into precise categories (A: entirely fatty, B: scattered areas of fibro-glandular density, C: heterogeneously dense, D: extremely dense) is crucial for assessing cancer risk and predicting recurrence likelihood. Similarly, deep learning models such as Single Shot Detectors (SSD) Ruban et al. (18) and YOLO Kebede et al. (19) have proven effective in identifying and classifying tumor regions within mammograms Singh and Alam (20). These models efficiently delineate regions of interest (ROIs) that display characteristics indicative of malignancies. After identifying the regions of interest (ROIs) and utilizing advanced segmentation techniques Baccouche et al. (21) for precise tumor boundary delineation, which enables detailed analysis of the tumor region Li et al. (22). Feature extraction methods Qi et al. (12) are then applied to further classify the tumor by shape Singh et al. (23), margin, and molecular subtypes Rayamaihi et al. (24) Ma et al. (25). This level of detailed analysis aids in tailoring personalized treatment plans based on the radiomic signatures extracted from the tumor region.
This work presents a comprehensive decision support system designed for BC relapse prediction by leveraging radiomic biomarkers extracted from digital mammograms as, shown in Figure 1. The framework incorporates tumor segmentation, BC subtypes classification, breast density mapping, and morphological analysis of the tumor regions to derive key features such as tumor shape, margin, size, and molecular subtype. These radiomic biomarkers, alongside BI-RADS-based breast density classification, are processed using a 1D-CNN model, demonstrating its ability to efficiently handle complex imaging data and enhance recurrence prediction accuracy.

Figure 1. Overview of the proposed pipeline for radiomic feature extraction and integration in relapse prediction.
2 Materials and methods
This study employed a comprehensive approach utilizing multimodal clinical data, which included mammographic images, radiologist-annotated tumor regions, and pathology-confirmed molecular subtypes. Tumor-related measurements—encompassing size, shape, and margins—were precisely extracted from standard diagnostic reports validated by experienced radiologists. While this study relies on expert-validated clinical annotations, recent developments in deep learning have demonstrated high accuracy in automated radiomic phenotype prediction, supporting future adoption of end-to-end computational pipelines.
2.1 Estimating breast density using deep learning models
Breast density estimation is critical for assessing BC risk and improving mammographic screening accuracy. Traditional approaches rely on radiologists’ visual assessments or semi-automated software, which can be subjective and inconsistent Park et al. (9). Deep Learning (DL), particularly Convolutional Neural Networks (CNNs), offers a more objective and standardized approach Saffari et al. (17). By training CNNs on labeled mammographic datasets (BI-RADS categories), these models can accurately identify patterns and textures associated with different density levels, reducing variability and outperforming conventional methods Khara et al. (14)Saffari et al. (17).
2.2 Extracting morphological features and molecular subtypes from tumor regions
Tumor morphology, including shape, size, and margins, plays a crucial role in characterizing breast cancer and assessing its aggressiveness Ma et al. (25) Gillies et al. (26). Traditional feature extraction methods rely on handcrafted techniques, which may overlook critical tumor characteristics SIN (2020). CNNs provide an automated and comprehensive approach by learning from annotated datasets to detect and segment tumor regions with high precision (27, 28). These models can uncover microtextural patterns linked to specific molecular subtypes, offering deeper insights into tumor behavior and treatment response Sutton et al. (29). Advanced techniques, such as multi-task learning and attention mechanisms, further enhance feature extraction by emphasizing the most relevant tumor regions. Recent advancements in radiomics and machine learning have enabled a more refined prediction of molecular subtypes, leveraging quantitative imaging biomarkers Yap et al. (30). CNNs efficiently capture spatial relationships and patterns, facilitating accurate classification of tumor morphology.
2.3 Breast cancer relapse prediction
In this work, we implemented a one-dimensional convolutional neural network (1-D CNN) tailored to the challenge of BC relapse prediction. As shown in the Figure 2, the model architecture initially emphasizes a streamlined process for converting features into high-dimensional representations to reflect better the spatial or sequential relationships within the underlying radiomics features Mathew et al. (31). The newly transformed features are then reshaped into a multi-channel pseudo-image format, effectively simulating a structured spatial domain. By expanding the feature representation to emulate structured spatial inputs, the network adapts to the morphological variability inherent in the dataset.
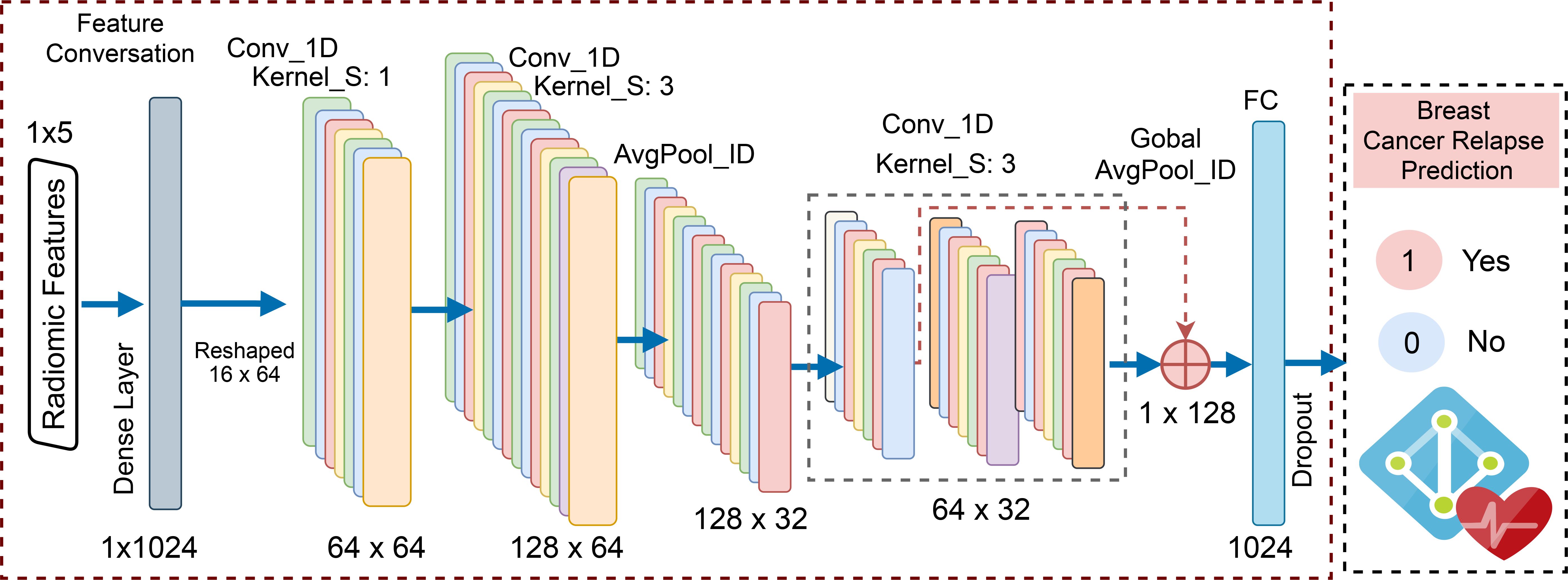
Figure 2. The proposed model architecture for relapse prediction.
Further, deeper convolutional layers refine the learned features, providing robustness against variability in patient-specific tumor characteristics. Unlike traditional machine learning approaches such as Random Forest or XGBoost, which require extensive manual feature engineering, this deep learning framework learns these representations end-to-end, demonstrating adaptability to high-dimensional data. The final stages of the network incorporate a global pooling operation and fully connected layers with dropout for regularization, culminating in a sigmoid activation for binary relapse classification. This architecture integrates high-quality tumor features and leverages the inherent benefits of convolutional operations, such as spatial locality and feature abstraction.
2.3.1 Training and evaluation
The proposed 1D-CNN model was trained on radiomic features, including Shape, Size, Margin, Density, and Tumor Molecular Subtype, automatically extracted from a private in-house dataset. Preprocessing steps included standardization, label encoding, and oversampling via Synthetic Minority Over-sampling Technique (SMOTE) to address class imbalance, ensuring robust predictive performance for the minority relapse class. The model was optimized using Binary Cross Entropy (BCE) Loss and the Adam optimizer with a learning rate of 0.001. The training was conducted over 200 epochs, with early stopping (patience = 25 epochs) applied based on validation loss to mitigate overfitting. Traditional machine learning models, including Random Forest, XGBoost, and MLP, were trained on the same features to benchmark performance. These models provided a comparative evaluation framework, validating the effectiveness of the proposed 1D-CNN in relapse prediction.
For evaluating the relapse model, we employed key metrics, Accuracy and Precision, to evaluate the positive predictions, Recall for its ability to identify all actual relapse cases effectively, and the F1-Score to balance precision and recall. The AUC-ROC measure True Positive Rate (TPR) against False Positive Rate (FPR) provides a comprehensive view of the model’s discrimination, critical for imbalanced classes. Additionally, we conducted SHAP (SHapley Additive exPlanations) analysis to determine the impact of individual radiomic features on the model’s predictions. This approach quantifies the importance of each feature, providing insight into which features have the most influence on the model’s output, leading to more informed refinements to the relapse model.
3 Results and discussion
3.1 Dataset
The dataset used in this study was developed in collaboration with our partner hospital, following ethical data collection and patient privacy guidelines. This dataset comprises clinical and pathological records for 148 BC patients, resulting in a total of 270 mammographic samples from both craniocaudal (CC) and mediolateral oblique (MLO) views, providing a robust foundation for our analysis. Our dataset includes detailed pathological annotations encompassing the following features. Molecular subtypes are classified into four categories: Luminal A (0), Luminal B (1), HER2-positive (2), and Triple-Negative (3). Tumor shape is categorized as oval (0), round or irregular (1), asymmetric (2), and distorted (3). Tumor margins are labeled as circumscribed (0), obscured or microlobulated (1), ill-defined (2), and spiculated (3). Breast density is recorded using the BI-RADS classification system, including entirely fatty (0), scattered fibroglandular tissue (1), heterogeneously dense (2), and extremely dense (3). Relapse status is encoded as a binary outcome, where 0 denotes no recurrence and 1 indicates documented relapse during the follow-up period. This comprehensive information is valuable for analyzing breast cancer characteristics and assessing relapse likelihood based on each patient’s unique tumor anatomy.
Figure 3 provides a visual summary of the distribution of key breast cancer features in the dataset through six histograms. Breast density is predominantly classified as type 1 (scattered fibroglandular tissue), with smaller peaks at types 0 and 2, reflecting patterns common in screening populations. Tumor shape is most frequently type 1 (round or irregular), while types 0 (oval) and 3 (distorted) occur less often, and type 2 (asymmetric) is rare. Tumor margins are distributed primarily across non-circumscribed categories (types 1–3), with fewer circumscribed cases (type 0). Tumor sizes, measured in both CC and MLO views, follow a right-skewed distribution, with most lesions between 5 and 30 mm and a peak near 10 mm. Molecular subtypes are imbalanced, with Luminal A (0) and Luminal B (1) being the most common, while HER2-positive (2) and Triple-Negative (3) subtypes are less frequent but clinically more aggressive. Relapse cases are relatively few, introducing a moderate class imbalance that should be considered in downstream modeling.
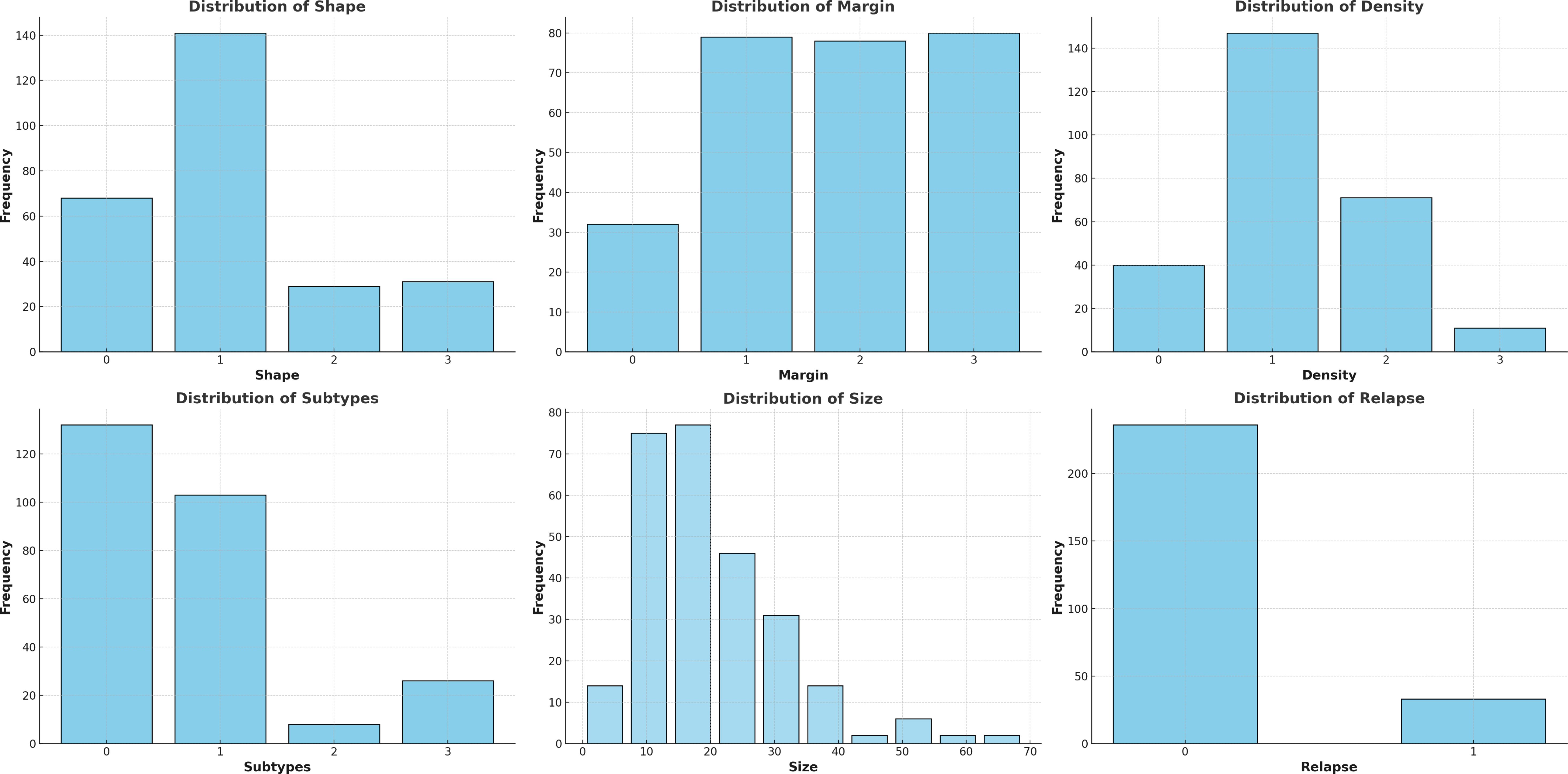
Figure 3. Descriptive statistics of the data using the histograms.
To explore the relationship between tumor characteristics and relapse, we examined feature distributions across relapse groups using violin plots (Figure 4). Patients who experienced relapse tended to have larger tumors, were more likely to present with aggressive molecular subtypes such as HER2-positive and Triple-Negative, and often exhibited irregular shapes and poorly defined margins—traits commonly associated with higher relapse risk. These patterns were further supported by Kendall’s rank correlation analysis (Figure 5), which showed moderate positive correlations between relapse and tumor size (τ = 0.23), as well as relapse and molecular subtype (τ = 0.24). A stronger correlation between tumor shape and margin (τ = 0.37) suggests a consistent association between morphological irregularity and invasive features. Some other feature pairs had near-zero correlations, suggesting minimal linear associations and pointing to the independence of many BC characteristics.

Figure 4. The plots show the distribution of tumor features by relapse status, highlighting associations with larger tumor size, aggressive subtypes, and irregular shapes and margins—features linked to relapse risk.
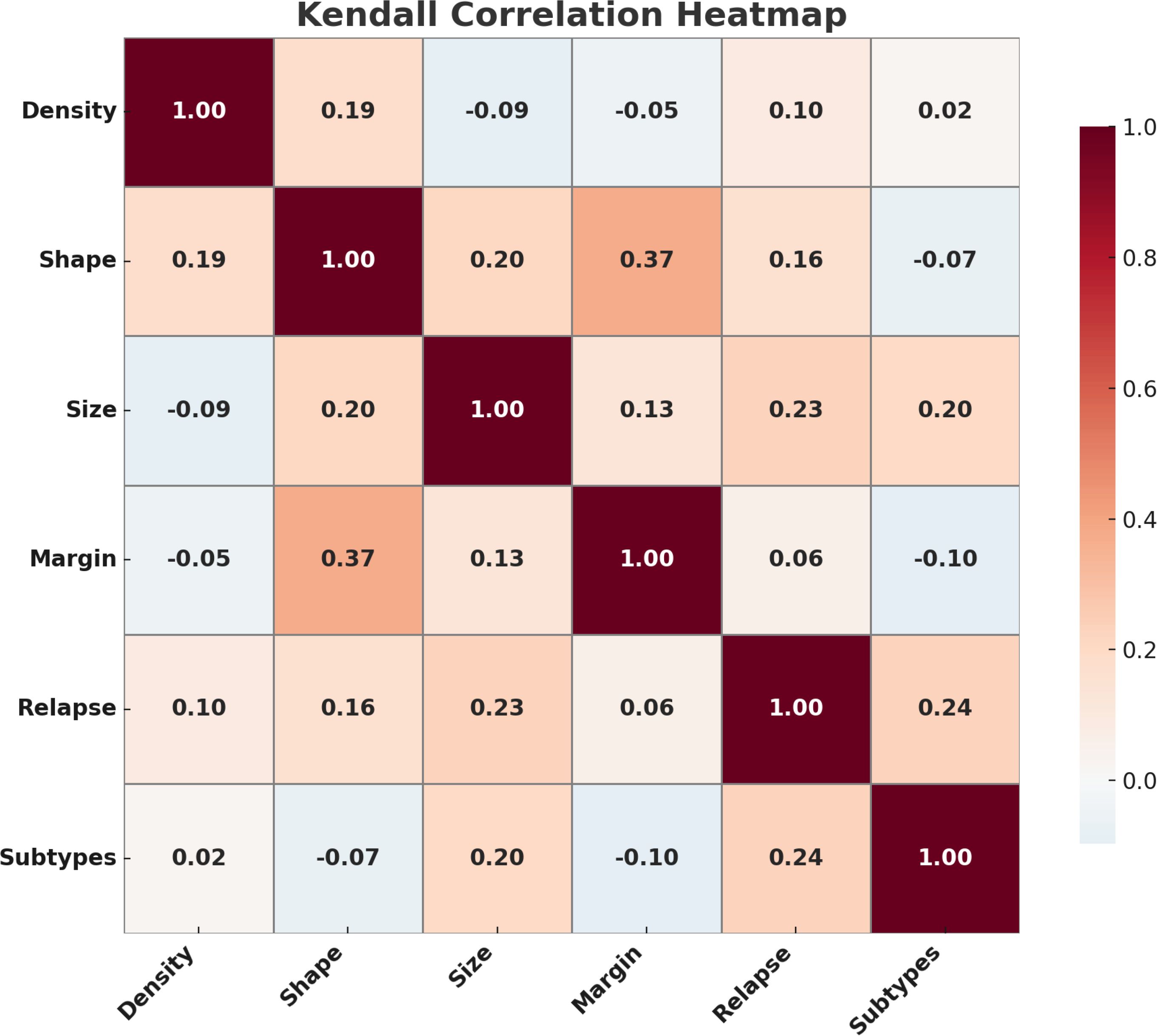
Figure 5. Correlation heatmap of breast cancer features, highlighting key associations such as shape–margin (ρ = 0.37) and subtypes–relapse (ρ = 0.24).
3.2 Classification performance
To predict BC relapse, we implemented a one-dimensional convolutional neural network (1D-CNN) model leveraging critical radiomic features extracted from digital mammograms. Additionally, a series of conventional machine learning models—including Random Forest, Support Vector Machines (SVM), Logistic Regression, and XGBoost—were systematically evaluated to establish comprehensive comparative insights and benchmark the performance of our CNN approach in Table 1.

Table 1. Results with 5-fold cross-validation. Values in parentheses indicate the 95% confidence intervals.
The results indicate that the 1D-CNN model achieves comparatively better predictive performance than the other models evaluated. Specifically, the CNN model achieved an average area under the receiver operating characteristic curve (AUC) of 0.9579, significantly surpassing the performance of Random Forest (AUC = 0.8986), XGBoost (AUC = 0.9116), CatBoost(AUC = 0.8672). Beyond AUC, critical evaluation metrics, including sensitivity, specificity, precision, recall, and F1-score (shown comprehensively in Table 1), consistently highlighted the superior robustness and reliability of the CNN approach compared to traditional machine learning methods.
We conducted both McNemar’s and DeLong’s statistical significance tests to evaluate pairwise differences in classification accuracy and AUC, respectively, to assess the performance advantage of our proposed 1D-CNN model rigorously. McNemar’s test revealed that the CNN model achieved statistically significant improvements in classification accuracy over all traditional machine learning models evaluated: Random Forest (statistic = 6.0, p = 0.0023), XGBoost (statistic = 8.0, p < 0.0001), and CatBoost (statistic = 4.0, p < 0.0001). Complementarily, DeLong’s test demonstrated that the CNN significantly outperformed CatBoost (z = -3.6436, p = 0.0008) and Random Forest (z = -1.5992, p = 0.0420) in terms of AUC. However, the difference between CNN and XGBoost was not statistically significant (z = -1.7748, p = 0.0608). Collectively, these results suggest a robust and statistically validated advantage of the CNN model in classification performance relative to conventional machine learning models.
The observed performance differences can be attributed primarily to the CNN architecture’s inherent capacity to capture complex spatial and sequential relationships within radiomic features. Although our model used only five fundamental radiomic features—tumor size, tumor shape, margin characteristics, molecular subtype, and breast density—the CNN architecture facilitated a highly effective conversion of these limited input features into sophisticated, high-dimensional representations. This capacity enabled CNN to better interpret subtle but critical patterns within the radiomic data, capturing interactions and non-linear relationships missed by conventional machine learning models.
We conducted comprehensive feature importance assessments and SHAP (SHapley Additive exPlanations) analysis to rigorously interpret and validate our predictive outcomes and further enhance clinical acceptability. As shown in Figure 6, the feature importance ranking highlighted molecular subtypes, tumor shape, and tumor size as the most critical predictive features associated with breast cancer relapse. The high significance of molecular subtypes aligns closely with existing clinical literature, as aggressive subtypes such as HER2-positive and Triple-Negative breast cancers (TNBC) are known to have a substantially higher tendency for recurrence due to their invasive biological behavior. Additionally, metastatic status at the time of initial diagnosis is a well-established, independent prognostic factor, particularly in HER2-positive BC patients, who exhibit significantly higher risk of relapse and worse survival outcomes due to the aggressive nature and high proliferative capacity of HER2-enriched tumors. Tumor shape also emerged as an essential predictive feature, supported by clinical evidence indicating that tumors exhibiting irregular shapes or spiculated margins typically correlate with greater malignancy potential, higher invasiveness, and consequently increased likelihood of future relapse.
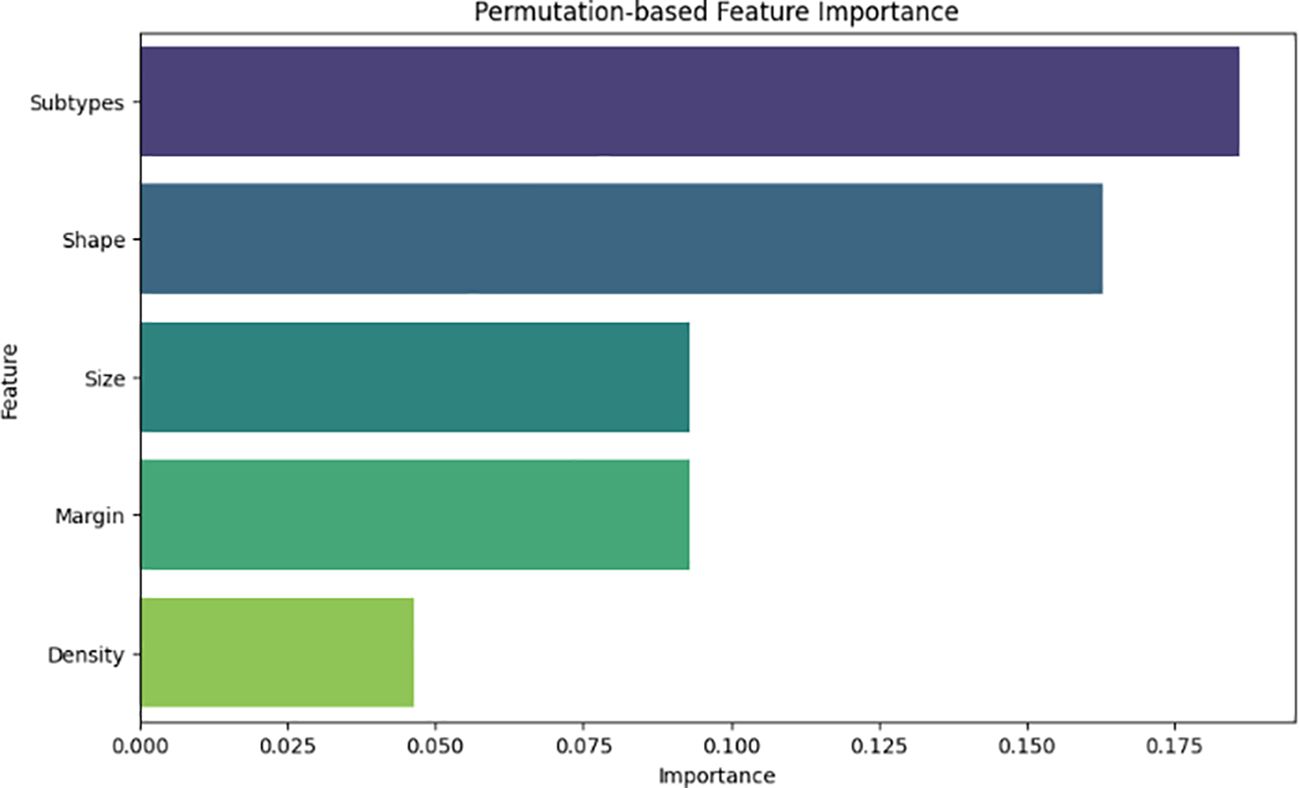
Figure 6. Feature importance analysis highlighting the most influential radiomic and clinical features contributing to BC relapse prediction.
Figure 7 illustrates that SHAP analysis offered comprehensive insights into feature contributions, improving model interpretability. Notably, SHAP analysis demonstrated that molecular subtypes, particularly HER2-positive and Triple-Negative cases, had the strongest impact on relapse likelihood. Additionally, tumor shape irregularities and larger tumor size were positively associated with increased relapse risk, aligning with clinical evidence that these characteristics often indicate aggressive tumor behavior. These insights enrich clinical interpretability, providing a transparent understanding of essential predictive factors influencing relapse risk.
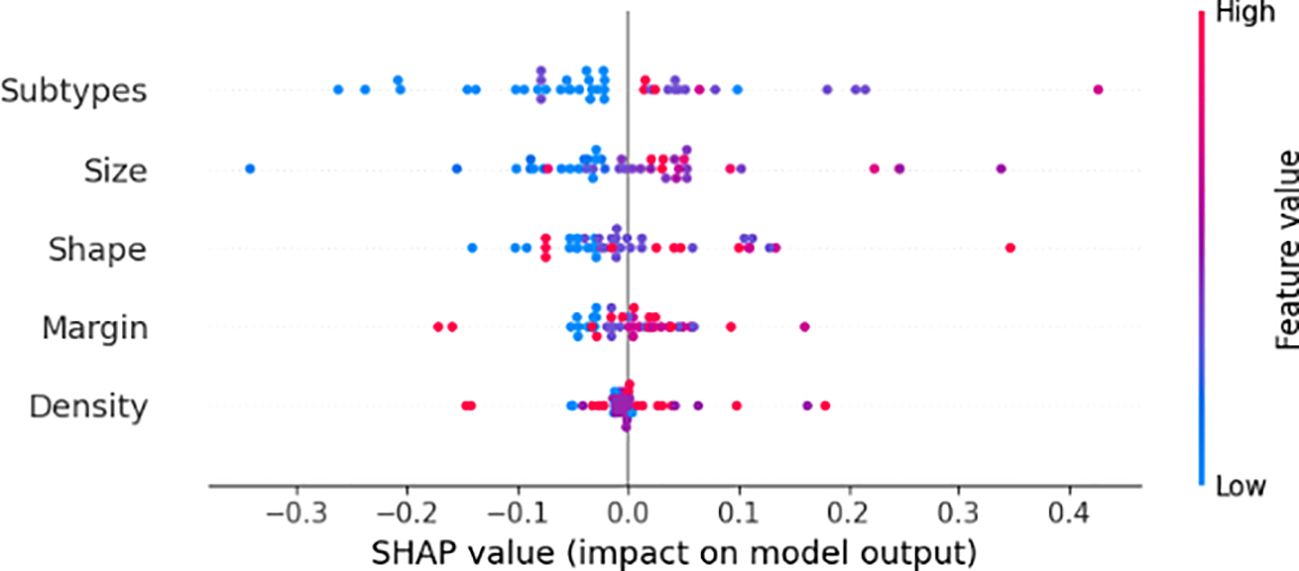
Figure 7. SHAP analysis illustrating the impact of these features on prediction.
3.3 Limitation and future work
Our analysis focuses on confirmed mass cases, which represent approximately 80% of breast cancer cases. We excluded cases where the tumor was unclear or where high breast density obscured tumor visibility, as radiomic feature extraction in such instances demands additional imaging modalities like MRI or ultrasound for accurate tumor localization and classification. These modalities are crucial for identifying non-mass lesions and ensuring a more comprehensive relapse prediction framework.
To improve the generalizability of our relapse prediction framework, future work will incorporate data from multiple institutions that reflect variations in imaging protocols, patient demographics, and clinical settings. Integrating such heterogeneous data sources will facilitate broader applicability across real-world scenarios, including cases with high breast density and non-mass lesions. Moreover, the inclusion of multi-modal imaging, such as MRI and ultrasound, will support more accurate tumor characterization across a broader range of clinical presentations.
4 Conclusion
Integrating clinical and radiomic features plays a crucial role in breast cancer relapse prediction, as they capture key tumor characteristics linked to disease progression. Automated extraction of features like tumor shape, size, margin, and molecular subtypes enhances early relapse detection and predictive accuracy. Our proposed 1D-CNN model on these features outperformed conventional machine learning models, achieving an AUC of 0.95 by effectively learning complex feature relationships. SHAP analysis confirmed HER2-positive and Triple-Negative subtypes and tumor shape and size as key relapse predictors. This study highlights the potential of deep learning-driven radiomics for early, non-invasive relapse prediction, improving personalized treatment strategies. Future research should focus on validation in larger, multi-center datasets for broader clinical adoption.
Data availability statement
Data handling adhered to Protection of Personal Data standards, in compliance with Article 7.1 of the Organic Law 15/1999. Requests to access the datasets should be directed to aGF0ZW0uYWJkZWxsYXRpZkB1cnYuY2F0.
Author contributions
AK: Investigation, Writing – review & editing, Validation, Methodology, Software, Formal Analysis, Writing – original draft. MM: Formal Analysis, Visualization, Writing – review & editing. CL: Writing – review & editing, Data curation, Supervision, Methodology. RB: Data curation, Writing – review & editing, Supervision, Methodology. DP: Supervision, Funding acquisition, Conceptualization, Resources, Investigation, Writing – review & editing. HR: Validation, Supervision, Investigation, Conceptualization, Writing – review & editing, Methodology.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This work was supported by the Bosomshield Project, a grant from Marie Sklodowaka-Curie Doctoral Networks Actions (HORIZON-MSCA-2021- DN-01-01;101073222).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Graham LJ, Shupe MP, Schneble EJ, Flynt FL, Clemenshaw MN, Kirkpatrick AD, et al. Current approaches and challenges in monitoring treatment responses in breast cancer. J Cancer. (2014) 5:58. doi: 10.7150/jca.7047
2. Boyages J, Taylor R, Chua B, Ung O, Bilous M, Salisbury E, et al. A risk index for early node-negative breast cancer. J Br Surg. (2006) 93:564–71. doi: 10.1002/bjs.5207
3. Hassett MJ, Hughes ME, Niland JC, Edge SB, Theriault RL, Wong Y-N, et al. Chemotherapy use for hormone receptor–positive, lymph node–negative breast cancer. J Clin Oncol. (2008) 26:5553–60. doi: 10.1200/JCO.2008.17.9705
4. Dinan MA, Mi X, Reed SD, Hirsch BR, Lyman GH, and Curtis LH. Initial trends in the use of the 21-gene recurrence score assay for patients with breast cancer in the medicare population 2005-2009. JAMA Oncol. (2015) 1:158–66. doi: 10.1001/jamaoncol.2015.43
5. Sparano JA, Gray RJ, Makower DF, Pritchard KI, Albain KS, Hayes DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. New Engl J Med. (2018) 379:111–21. doi: 10.1056/NEJMoa1804710
6. Mao N, Yin P, Zhang H, Zhang K, Song X, Xing D, et al. Mammography-based radiomics for predicting the risk of breast cancer recurrence: a multicenter study. Br J Radiol. (2021) 94:20210348. doi: 10.1259/bjr.20210348
7. Lambin P, Rios-Velazquez E, Leijenaar R, Carvalho S, Van Stiphout RG, Granton P, et al. Radiomics: extracting more information from medical images using advanced feature analysis. Eur J Cancer. (2012) 48:441–6. doi: 10.1016/j.ejca.2011.11.036
8. Ma M, Liu R, Wen C, Xu W, Xu Z, Wang S, et al. Predicting the molecular subtype of breast cancer and identifying interpretab le imaging features using machine learning algorithms. Eur Radiol. (2022) 32:1652–62. doi: 10.1007/s00330-021-08271-4
9. Park CC, Rembert J, Chew K, Moore D, and Kerlikowske K. High mammographic breast density is independent predictor of local but not distant recurrence after lumpectomy and radiotherapy for invasive breast cancer. Int J Radiat Oncol Biol Phys. (2009) 73:75–9. doi: 10.1016/j.ijrobp.2008.04.007
10. Habel LA, Dignam JJ, Land SR, Salane M, Capra AM, and Julian TB. Mammographic density and breast cancer after ductal carcinoma in situ. J Natl Cancer Institute. (2004) 96:1467–72. doi: 10.1093/jnci/djh260
11. Ghose S, Davis C, Cho S, Polar Y, Ginty F, and Badve S. Spatial heterogeneity of tumor boundary in mammograms is prognostic of recurrence in triple negative breast cancer (tnbc). Cancer Res. (2024) 84:4925–5. doi: 10.1158/1538-7445.AM2024-4925
12. Qi Y-J, Su G-H, You C, Zhang X, Xiao Y, Jiang Y-Z, et al. Radiomics in breast cancer: Current advances and future directions. Cell Rep Med. (2024) 5:9. doi: 10.1016/j.xcrm.2024.101719
13. Dasgupta A, Bhardwaj D, DiCenzo D, Fatima K, Osapoetra LO, Quiaoit K, et al. Radiomics in predicting recurrence for patients with locally advanced breast cancer using quantitative ultrasound. Oncotarget. (2021) 12:2437. doi: 10.18632/oncotarget.28139
14. Khara G, Trivedi H, Newell MS, Patel R, Rijken T, Kecskemethy P, et al. Generalisable deep learning method for mammographic density prediction across imaging techniques and self-reported race. Commun Med. (2024) 4:21. doi: 10.1038/s43856-024-00446-6
15. Biroš M, Kvak D, Dandár J, Hruby R, Jan E, Atakhanova A, et al. Enhancing accuracy in breast density assessment using deep learning: A multicentric, multi-reader study. Diagnostics. (2024) 14:1117. doi: 10.3390/diagnostics14111117
16. Anyfantis D, Koutras A, Apostolopoulos G, and Christoyianni I. Breast density transformations using cyclegans for revealing undetected findings in mammograms. Signals. (2023) 4:421–38. doi: 10.3390/signals4020022
17. Saffari N, Rashwan HA, Abdel-Nasser M, Kumar Singh V, Arenas M, Mangina E, et al. Fully automated breast density segmentation and classification using deep learning. Diagnostics. (2020) 10:988. doi: 10.3390/diagnostics10110988
18. Ruban S, Jabeer M, and Besti RS. (2022). Detection of breast tumor in mammograms using single shot detector algorithm, in: International Conference on Advances in Computing and Data Sciences, Cham: Springer International Publishing. pp. 370–80.
19. Kebede SR, Waldamichael FG, Debelee TG, Aleme M, Bedane W, Mezgebu B, et al. Dual view deep learning for enhanced breast cancer screening using mammography. Sci Rep. (2024) 14:3839. doi: 10.1038/s41598-023-50797-8
20. Singh L and Alam A. An efficient hybrid methodology for an early detection of breast cancer in digital mammograms. J Ambient Intell Humanized Computing. (2024) 15:337–60. doi: 10.1007/s12652-022-03895-w
21. Baccouche A, Garcia-Zapirain B, Castillo Olea C, and Elmaghraby AS. Connected-unets: a deep learning architecture for breast mass segmentation. NPJ Breast Cancer. (2021) 7:151. doi: 10.1038/s41523-021-00358-x
22. Li Y, Zhao G, Zhang Q, Lin Y, and Wang M. Sap-cgan: Adversarial learning for breast mass segmentation in digital mammogram based on superpixel average pooling. Med Phys. (2021) 48:1157–67. doi: 10.1002/mp.14671
23. Singh VK, Rashwan HA, Romani S, Akram F, Pandey N, Sarker MMK, et al. Breast tumor segmentation and shape classification in mammograms using generative adversarial and convolutional neural network. Expert Syst Appl. (2020) 139:112855. doi: 10.1016/j.eswa.2019.112855
24. Rayamaihi K, Bansal R, and Aggarwal B. Mammographic correlation with molecular subtypes of breast carcinoma. J Radiol Oncol. (2023) 7:001–5. doi: 10.29328/journal.jro.1001045
25. Ma W, Zhao Y, Ji Y, Guo X, Jian X, Liu P, et al. Breast cancer molecular subtype prediction by mammographic radiomic features. Acad Radiol. (2019) 26:196–201. doi: 10.1016/j.acra.2018.01.023
26. Gillies RJ, Kinahan PE, and Hricak H. Radiomics: images are more than pictures, they are data. Radiology. (2016) 278:563–77. doi: 10.1148/radiol.2015151169
27. Wang Y, Tao D, Gao X, Li X, and Wang B. Mammographic mass segmentation: embedding multiple features in vector-valued level set in ambiguous regions. Pattern Recognition. (2011) 44:1903–15. doi: 10.1016/j.patcog.2010.08.002
28. Tsochatzidis L, Koutla P, Costaridou L, and Pratikakis I. Integrating segmentation information into cnn for breast cancer diagnosis of mammographic masses. Comput Methods Programs Biomedicine. (2021) 200:105913. doi: 10.1016/j.cmpb.2020.105913
29. Sutton EJ, Dashevsky BZ, Oh JH, Veeraraghavan H, Apte AP, Thakur SB, et al. Breast cancer molecular subtype classifier that incorporates mri features. J Magnetic Resonance Imaging. (2016) 44:122–9. doi: 10.1002/jmri.25119
30. Yap FY, Hwang DH, Cen SY, Varghese BA, Desai B, Quinn BD, et al. Quantitative contour analysis as an image-based discriminator between benign and Malignant renal tumors. Urology. (2018) 114:121–7. doi: 10.1016/j.urology.2017.12.018
Keywords: breast cancer recurrence, diagnosis, personalized treatment, relapse, clinical features, radiomic features
Citation: Khalid A, Mursil M, Pablo CL, Bosch R, Puig D and Rashwan HA (2025) Advancing breast cancer relapse prediction with radiomics and neural networks: a clinically interpretable framework. Front. Oncol. 15:1593806. doi: 10.3389/fonc.2025.1593806
Received: 14 March 2025; Accepted: 27 August 2025;
Published: 15 September 2025.
Edited by:
Alberto Traverso, San Raffaele Hospital (IRCCS), ItalyReviewed by:
Domenico Pomarico, University of Bari Aldo Moro, ItalySimona Marzi, IRCCS Istituto Nazionale Tumori Regina Elena, Italy
Copyright © 2025 Khalid, Mursil, Pablo, Bosch, Puig and Rashwan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hatem A. Rashwan, aGF0ZW0uYWJkZWxsYXRpZkB1cnYuY2F0; Adnan Khalid, YWRuYW4ua2hhbGlkQHVydi5jYXQ=