 Josep Sabaté-Ortega1,2†
Josep Sabaté-Ortega1,2† Anna Ribera-Montserrat1,2†Sonia del Barco1,3,4†Ariadna Roqué-Lloveras1,2†Roser Fort-Culillas1,2†M. Carme Carmona-García1,4
Anna Ribera-Montserrat1,2†Sonia del Barco1,3,4†Ariadna Roqué-Lloveras1,2†Roser Fort-Culillas1,2†M. Carme Carmona-García1,4 Raquel Liñan1,2Emma Polonio-Alcalá2†Gerard Carbó-Vilavedra5†
Raquel Liñan1,2Emma Polonio-Alcalá2†Gerard Carbó-Vilavedra5† Irma Ramos-Oliver6Elisabet Bujons-Buscarons1,2†Claudia Montañés-Ferrer1,2
Irma Ramos-Oliver6Elisabet Bujons-Buscarons1,2†Claudia Montañés-Ferrer1,2 Gemma Viñas1,2,3*†
Gemma Viñas1,2,3*† Helena Pla-Juher1,2*†
Helena Pla-Juher1,2*†- 1Department of Medical Oncology, Catalan Institute of Oncology, Dr. Josep Trueta University Hospital, Girona, Spain
- 2Precision Oncology Group (OncoGIR-Pro), Girona BiomedicaI Research Institute (IDIBGI-CERCA), Salt, Spain
- 3Department of Medical Sciences, Medical School, University of Girona, Girona, Spain
- 4Descriptive Epidemiology, Genetic and Cancer Prevention Group, Girona Biomedical Research Institute (IDIBGI-CERCA), Salt, Spain
- 5Breast Pathology Unit, IDI Girona Center - Institute of Diagnostic Imaging (IDI), Dr. Josep Trueta University Hospital, Girona, Spain
- 6Department of Pathology, Dr. Josep Trueta University Hospital, Girona, Spain
Inflammatory breast cancer (IBC) is a rare and aggressive breast cancer type, accounting for 5-7% of breast cancer-related deaths, and its bilateral involvement is exceedingly uncommon. We report a case of metachronous bilateral IBC in a 50-year-old premenopausal woman with Charcot-Marie-Tooth disease, offering novel insight into the diagnostic, therapeutic, and molecular challenges of this condition. The patient initially presented with acute right breast erythema, skin thickening, and peau d’orange, followed by contralateral breast involvement with similar symptoms. Disease progression occurred with changes in receptor status and eventual loss of hormone receptor (HR) expression. The initial diagnosis was stage IIIB HR-positive/HER2-negative IBC. The patient underwent neoadjuvant chemotherapy, surgery, adjuvant radiotherapy, and endocrine therapy. However, the patient experienced a contralateral recurrence after 11 months of disease-free survival. Subsequent management involved multiple systemic therapies, including targeted therapy after next-generation sequencing analysis revealed a PIK3CA mutation. Although some clinical benefit was achieved, the disease continued to progress. Ultimately, the patient passed away four years after the initial diagnosis. This case underscores the aggressive and recurrent nature of bilateral IBC, its diagnostic complexity, and the importance of molecular profiling in guiding targeted treatment. It highlights the need for clinical vigilance, timely reassessment of tumor biology, and individualized multimodal care in managing rare and evolving presentations of IBC.
Introduction
Inflammatory breast cancer (IBC) is an invasive rare form of breast cancer (BC) defined by the occurrence of tumor embolism within the dermal lymphatic system (1). Despite its rarity, IBC is responsible for 5.5-7% of BC-related deaths (1, 2). Patients with IBC have a shorter median overall survival (OS) duration compared to those with non-inflammatory BC, with 4.75 years versus 13.40 years for stage III disease (3) and 2.27 years versus 3.40 years for stage IV disease (4).
The diagnosis rates of IBC have been increasing, from 2.0 to 2.5 cases per 100,000 woman-years, leading to a poorer prognosis. In contrast, the rate of non-IBC has declined during the same timeframe. The clinical presentation of IBC can sometimes resemble mastitis, potentially leading to diagnostic delays (5). A distinctive feature in the histopathology of IBC is the infiltration of the dermal lymphatic system, which is responsible for the typical edema and skin alteration that define IBC (5, 6).
There is limited understanding of IBC as a subtype of BC. Ethnicity, race, location, socioeconomic status, obesity, menopausal status, age of menarche, age at first pregnancy, duration of lactation, family history, mammographic density, environmental factors, and genetic factors are risk factors for BC development (7). Notably, higher body mass index (BMI) is associated with increased IBC risk (8), impacting both estrogen receptor (ER)-positive and ER-negative IBC cases in pre- and peri/postmenopausal women (9).
The treatment challenge for IBC arises from its aggressive nature and advanced stage at diagnosis. Unlike other BCs, IBC often lacks a distinct tumor mass, making it hard to target with surgery or radiation therapy. Achieving local control is difficult due to diffuse nature of the disease, and recurrence risk remains high. The treatment typically involves a complex multimodal approach, including chemotherapy (CT), surgery, radiation therapy, and targeted therapies (10).
Bilateral BC refers to the presence of tumors in both breasts and includes two clinical forms. Synchronous cases, observed in 2.9% of cases, involve tumors that appear simultaneously or within 6 months of each other. Metachronous cases, occurring in 4.6% of patients, are characterized by the development of a tumor in the contralateral breast more than 6 months following the primary tumor (11, 12). Despite this, the overall diagnosis of bilateral BC are extremely rare, accounting for only 1% of all breast malignancies (13) and with limited documented cases, making it a unique and challenging condition to treat. Given the aggressive nature of bilateral IBC, early detection and prompt intervention are essential.
Here, we report a unique case of 50-year-old women with Charcot-Marie-Tooth disease diagnosed with IBC hormone receptor(HR)–positive/HER2-negative with metachronous presentation, and secondary loss HR expression after multiple lines of systemic therapy, following the CARE guidelines (Supplementary Table S1).
Case presentation
The progression of the case is summarized in the timeline shown in Figure 1.
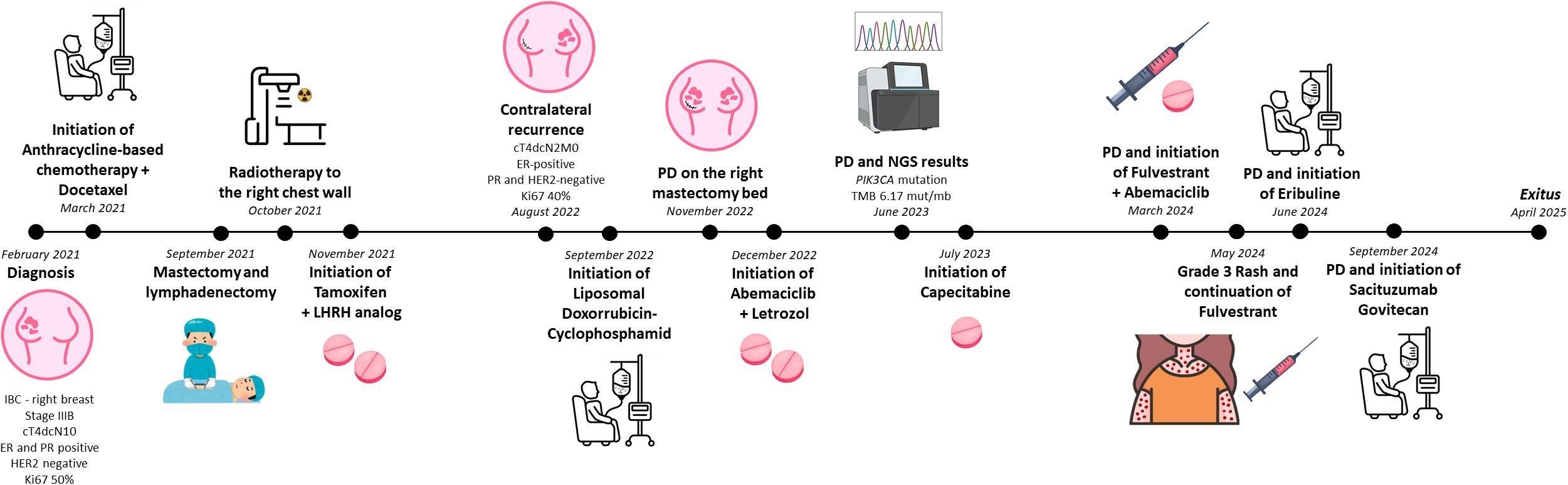
Figure 1. Timeline illustrating the chronological progression of the case. ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; IBC, Inflammatory breast cancer; LHRH, luteinizing hormone-releasing hormone; NGS, next-generation sequencing; PD, progression disease; PR, progesterone receptor.
A 50-year-old premenopausal woman with a known diagnosis with Charcot-Marie-Tooth disease referred to the hospital with acute right breast erythema, skin thickening, and peau d’orange. Family history revealed that her mother was diagnosed with BC at the age 45. The patient was referred for genetic counseling; however, no pathogenic germline mutations were identified.
Diagnostic imagining included a right breast mammogram, which showed skin thickening and right axillary adenopathy. Magnetic resonance imaging (MRI) revealed a 41 x 40 x 56 mm lesion in the inner quadrant of the right breast, along with diffuse skin thickening and hypercaptating axillary lymph nodes (Figure 2A). A body computed tomography (CT) scan showed no evidence of distant metastatic lesions. Core biopsies of both breast lesion and axillary lymph node were performed. Histopathological examination confirmed invasive ductal carcinoma, grade 2, with positive expression of ER and progesterone (PR), HER2 negativity (score 0), and a Ki67 index of 50%. No diagnostic challenges were found. In February 2021, the initial diagnosis was IBC of the right breast, staged as cT4d cN1M0 – stage IIIB, according American Joint Committee on Cancer 8th edition.
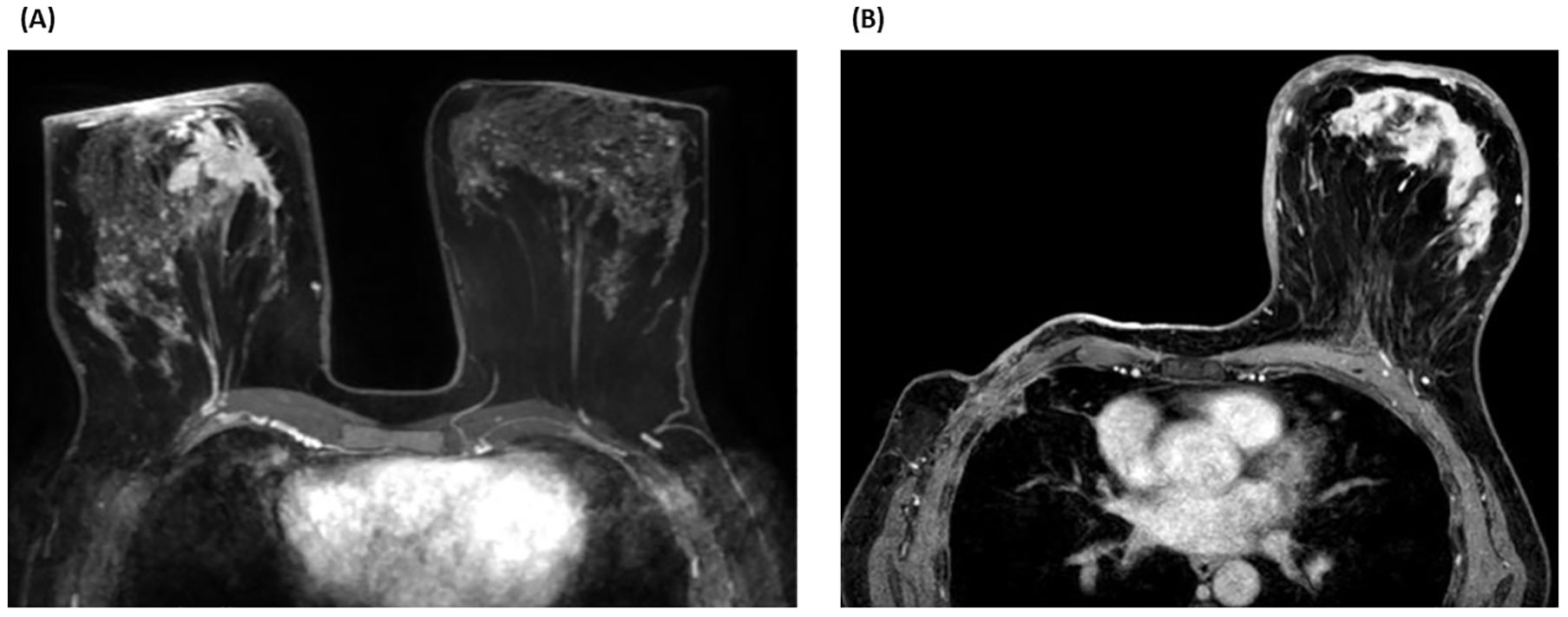
Figure 2. (A) (2021) Magnetic resonance imaging (MRI) axial section - T1 sequence with fat suppression and with contrast (phase 2 - 120s). The tumor lesion (41 × 40 × 56 mm) is mainly visualized in the anterior internal plane of the right breast. The chest is flattened in its anterior portion due to the position of the patient. (B) (2022) MRI axial section - 3D fat-suppressed T1 sequence (DIXON) with contrast. The skin thickening in the left breast is seen marked with areas of patchy enhancement that could indicate lymphatic metastatic spread and area of enhancement in the central portion of the breast.
In March 2021, the patient initated neoadjuvant CT including four cycles of an anthracycline-based regimen, followed by four cycles of docetaxel administered at 80mg/m2 every three weeks. Despite the risk of increased neurotoxicity due to her underlying Charcot-Marie-Tooth disease, systemic treatment was not modified. Instead, the patient was managed in close collaboration with the neurology team to monitor for neurologic side effects throughout the course of treatment.
Surgical intervention was subsequently performed in September 2021. The patient underwent right-sided mastectomy and lymphadenectomy, without breast reconstruction. Histopathological analysis of the surgical specimen revealed a residual invasive ductal carcinoma measuring 9 mm. Of the sixteen lymph nodes resected, one showed micrometastatic tumor deposits (ypT1by pN1mi). Afterwards, the patient received adjuvant radiotherapy directed to the right chest wall, axilla, and internal mammary chain, delivering a total dose of 50 Gy in 25 fractions. Endocrine therapy with tamoxifen (20 mg/day) and luteinizing hormone-releasing hormone (LHRH) analog was initiated thereafter.
In August 2022, the patient exhibited erythema in the contralateral (left) breast with palpable fixed axillary lymph nodes, after eleven months of disease-free survival (Figure 2B). Biopsies of both the skin and axillary adenopathy revealed invasive ductal carcinoma with ER-positive, PR-negative, HER2-negative (score 0), and Ki67 index of 40%. The recurrence was staged as cT4d cN2 M0 IBC. The patient was treated with a combination of liposomal doxorubicin (60mg/m2) and cyclophosphamide (600mg/m2) for four cycles. However, the disease progressed, with a new erythema emerging on the right mastectomy bed (Figure 3). A repeat biopsy confirmed dermic infiltration by invasive ductal carcinoma with the same molecular profile as the contralateral lesion (Figure 4).

Figure 3. Cutaneous erythema observed over the right mastectomy site.
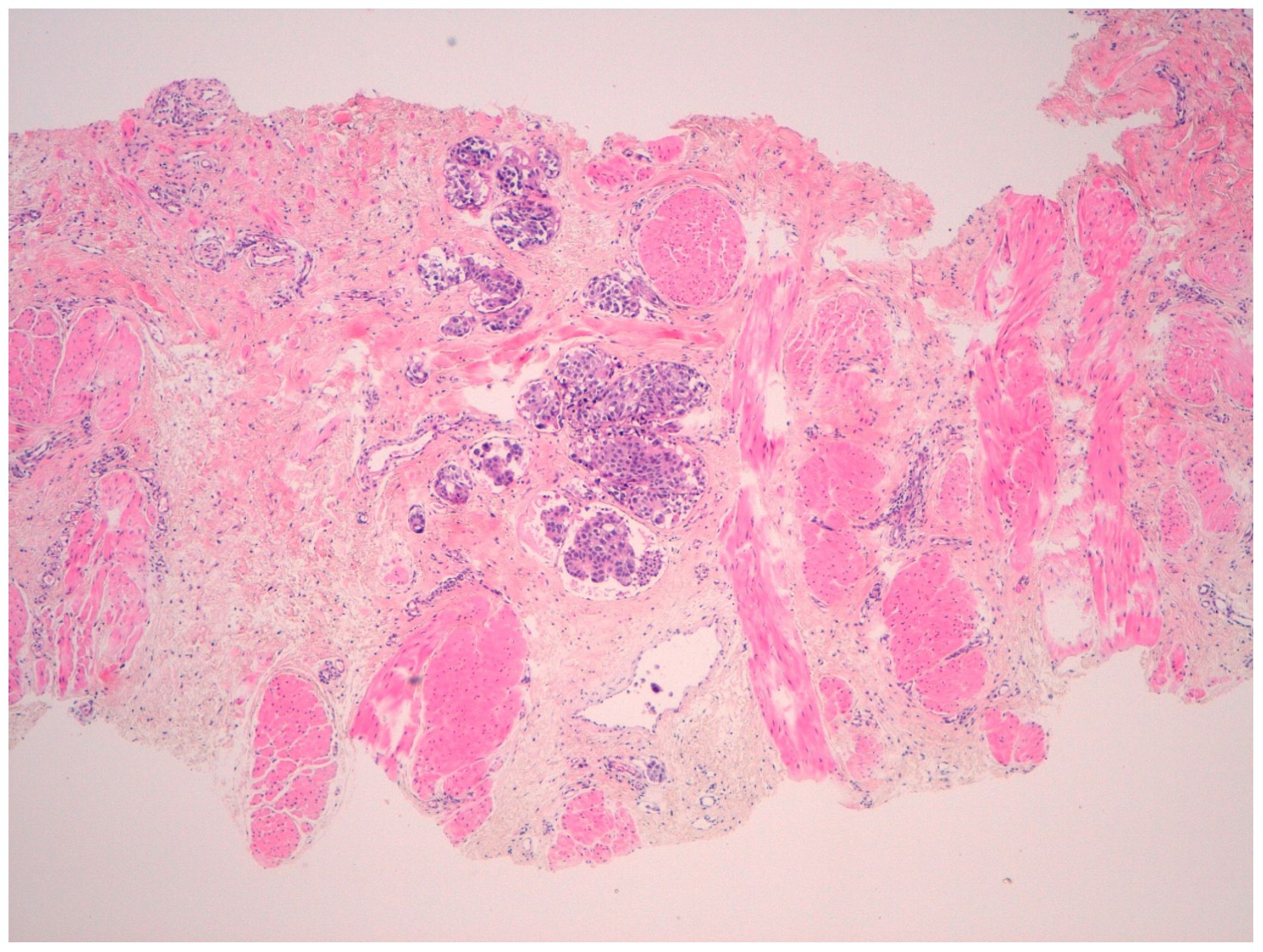
Figure 4. Histopathological analysis of a skin punch biopsy of mammary tissue showing tumor nests within lymphatic vessels at the deep dermal level (hematoxylin stain, 40× magnification).
First-line treatment for metastatic disease was initiated in December 2022 with a combination of abemaciclib (150 mg/12h) and letrozole (2.5 mg/day). After six months, the disease progressed cutaneously. The next-generation sequencing (NGS) analysis of the tumor identified a PIK3CA mutation and a tumor mutational burden (TMB) of 6.17 mutations per megabase. Immunohistochemistry of mismatch repair proteins revealed a stable tumor. As no clinical trial was available for PIK3CA-mutant tumors at that time, the patient was started on capecitabine administrated at 1250mg/m2 as second-line therapy in July 2023. This regimen resulted in significant clinical improvement in cutaneous symptoms and excellent tolerability for eight months, without significant toxicities.
Upon further locoregional progression, the patient was enrolled in a clinical trial involving fulvestrant (500 mg/month) in combination with alpelisib (300 mg/day) in March 2024. After two cycles, a grade 3 rash was developed, requiring discontinuation of alpelisib. Fulvestrant was continued as a monotherapy but was ineffective; locoregional progression occurred within three months. Eribuline was subsequently introduced as fourth-line treatment, administrated at 1.23 mg/m2 on days 1 and 8 of a 21-day cycle. Despite therapy, the disease advanced with development of pleural effusion.
A repeat skin biopsy showed a change in tumor biology: HR-negative invasive carcinoma, HER2 1+, and Ki67 index of 27%. Based on this new profile, in September 2024, fifth-line treatment with sacituzumab govitecan was approved, administrated at 10 mg/kg on days 1 and 8 of a 21-day cycle. The patient received three cycles of treatment; however, it was discontinued due to the onset of respiratory insufficiency. She passed away in April 2025.
Discussion
This case presentation adds valuable information to the limited literature on bilateral IBC. It offers educational insights about diagnostic challenges and management considerations and raises awareness among clinicians to consider bilateral involvement in patients presenting with breast erythema and edema. By documenting the clinical course, the case also underscores the need for heightened clinical vigilance and may stimulate further research into the pathophysiology and optimal management of this aggressive disease. Although limited by its single-case design and inability to generalize findings or establish causality, it provides meaningful clinical insights into a rare and complex condition.
Bilateral IBC is extremely rare and presents significant challenges to standard treatment due to its aggressive clinical behavior, as illustrated by the case presented. It is worth noting that IBC is usually misdiagnosed as benign conditions like mastitis, which leads to delays in receiving appropriate treatment. With bilateral symptoms, the diagnostic difficulty is particularly pronounced, where a biopsy and imaging workup would be urgent in the setting of persistent symptoms despite antibiotic therapy (5). Owing to its rarity, IBC is underrepresented in clinical trials, resulting in a lack of conclusive evidence regarding optimal treatment and prognosis (14). Reports of synchronous or metachronous contralateral involvement have been documented nearly exclusively in single case reports, underscoring both the extreme rarity of this condition as well as the absence of comprehensive epidemiologic information. In 2009, Masannat et al. described an unusual case of bilateral metachronous IBC, each occurrence showing a complete clinico-pathological response to neoadjuvant CT followed by surgery (15). In 2016, Kurtz et al. reported a patient who received neoadjuvant CT, underwent modified radical mastectomy, and received whole breast radiation for IBC treatment. Less than a year later, the patient experienced a recurrence of IBC on the left chest wall (within the radiated area) and developed a new IBC in the contralateral breast (16). In 2022, Kawaguchi et al. presented a case of contralateral recurrence of triple-negative IBC after 2 years of disease-free survival, successfully managed with dose-dense neoadjuvant CT and bilateral total mastectomy (17). More recently, Levy & Hanna reported a case of HER2-positive IBC with metastatic relapse involving both breasts, the right ovary, and multiple vertebral bodies. The patient achieved a complete response after the treatment with THP (docetaxel, trastuzumab, and pertuzumab) (6).
While these cases emphasize the aggressive nature and recurrence potential of IBC, they also illustrate the clinical variability in disease progression. Of significant note, patients with IBC have a much greater likelihood of developing contralateral breast cancer within two years of diagnosis compared to patients with non-IBC breast cancer (16, 18). Contralateral malignancies detected within two years are more likely to be recurrences or metastases, whereas those diagnosed after 2 years are more often considered independent second tumors (18). In the presented case, contralateral IBC was diagnosed 18 months after the initial diagnosis, fulfilling the criteria for metachronous bilateral BC. This timing also supports the likelihood of metastatic dissemination rather than an independent second tumor. The high metastatic potential of IBC is attributable to several factors, including the intrinsic tumor aggressiveness, specific biological characteristics, the molecular subtype, and demographic risk factors such as African American ethnicity, obesity (especially among postmenopausal women), and advanced age (5, 19, 20).
Imaging techniques such as MRI, CT, positron emission tomography (PET)-CT, mammography, and medical photography are crucial for accurate diagnosis, assessing disease extent and guiding treatment decisions. MRI is the most effective imaging technique for identifying periareolar lesions associated with IBC (5). Both contrast-enhanced and non-contrast MRI can reveal edematous infiltrations, skin thickening, areolar retractions, lymph node enlargement, internal mammary lymphadenopathy, and other features commonly associated with IBC. Dynamic contrast-enhanced MRI, particularly non-contrast T2 weighted imaging (T2WI), is the most sensitive imaging modality for detecting BC and differentiating malignant from benign lesions (21). Bilateral mammography and ultrasound are the initial imaging tools to detect skin thickening, trabecular distortion, increased breast density, or calcifications (19). In addition, PET or CT scans provide valuable information for staging the disease, helping to identify adenopathy, effusion, distant metastases, and locoregional involvement, emphasizing the importance of timely follow-up (22).
The underrepresentation of bilateral IBC in clinical trials poses significant challenges for its management. Treatment is usually based on unilateral IBC and involves a trimodal approach consisting of neoadjuvant CT followed by modified radical mastectomy and radiotherapy (19, 23). However, bilateral involvement adds additional complexity to surgical planning and the design of radiation treatment fields. Active monitoring using dynamic imaging techniques along with hands-on evaluations post therapeutic interventions is essential due to IBC’s aggressive nature and elevate recurrence risk to timely identify disease advancement—enhancing survival chances (10). Treatment guidance using comprehensive molecular profiling becomes invaluable for identifying clinically relevant alterations like HER2 amplification or PIK3CA mutations enabling integration of targeted therapies or endocrine treatments (24, 25). Efforts to advance immune checkpoint inhibitor-based treatments have also prompted numerous studies investigating the expression of various immune checkpoints in IBC. Given the success of PD-1/PD-L1 inhibitors in other cancers, current research has predominantly focused on PD-L1 expression in IBC (24, 26).
Genomic profiling is essential for understanding the complex molecular landscape of IBC, allowing the identification of specific genetic alterations, such as copy number variations or mutations (27). It also enables the identification of predictive factors for treatment response by analyzing gene expression signatures associated with CT response, thereby facilitating personalized treatment strategies (27). Moreover, genomic profiling helps to elucidate candidate genes and pathways implicated in IBC progression, including cell proliferation, invasion, and immune response, contributing to a better understanding of the underlying molecular features of IBC, with the aim of improving the diagnosis and treatment of this aggressive form of BC. For instance, Chakraborty et al. identified that EMT scores showed a higher coefficient of variation in IBC compared to non-IBC samples, suggesting it as a potential biomarker (25).
In the case presented, we identified a mutation in PIK3CA through NGS analysis, which allowed the patient to receive fulvestrant in combination with alpelisib. The PI3Kα inhibitor alpelisib has demonstrated significant clinical benefit when combined with endocrine therapy in patients with HR-positive/HER2-negative advanced breast cancer harboring PIK3CA mutations (28). Approximately 40% of HR+/HER2− BC metastases harbor mutations in the PI3K–AKT–mTOR pathway, which diminish endocrine therapy efficacy and promote resistance. Among these, PIK3CA mutations are the most prevalent, markedly boosting this pro-survival signaling cascade (29). In the pivotal SOLAR-1 trial, alpelisib plus fulvestrant almost doubled median progression-free survival compared to fulvestrant alone in patients with PIK3CA-mutated tumors (11.0 vs. 5.7 months; HR 0.65; P < 0.001) (28). This improvement was both statistically and clinically significant, establishing the PI3K pathway as a viable target in this context. As a result, alpelisib received FDA approval in 2019 for use with endocrine therapy in postmenopausal women and older men with HR+/HER2− advanced BC with PIK3CA mutations following progression on prior endocrine therapy (30). This combination now represents a genomically guided standard of care that enhances disease control by addressing a key mechanism of resistance. In this context, confirming a PIK3CA mutation in tumor tissue supports the use of the PI3K inhibitor alpelisib to improve disease control and overcome endocrine resistance, exemplifying the principles of precision oncology.
From the patient’s perspective, she conveyed significant uncertainty about her future following treatment for metastatic BC. She reported struggling with body image and distress stemming from the side effects of therapy, which adversely affected her self-esteem and daily functioning. In recognition of the emotional and psychological burden of her illness, she was referred to the psycho-oncology services for specialized support. Notably, she was sustained by a strong familial and social support network, which offered significant emotional support and resilience throughout her illness.
Conclusions
Our case report underscores the aggressive and diagnostically challenging nature of IBC, particularly in its rare bilateral, metachronous presentation. It emphasizes the necessity for heightened clinical vigilance, especially when symptoms mimic benign conditions, and the critical role of timely biopsy and imaging. The case demonstrates how tumor biology can evolve under therapeutic pressure, requiring repeated reassessment through regular and consistent imaging and physical examinations to inform treatment decisions. It also emphasize the importance of patient adherence to prescribed therapy, as consistent compliance significantly influences treatment efficacy and outcomes. Furthermore, it exemplifies the value of molecular profiling in informing precision oncology, as demonstrated by the identification of a PIK3CA mutation. Early and accurate detection, along with personalized, multimodal therapeutic approach, can significantly improve the chances of successful therapy and long-term survival. Ultimately, this case contributes meaningful insight into a rare and complex oncological entity and the ongoing need for comprehensive, individualized care.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Ethics statement
Written informed consent was obtained from the patient for the publication of this case report and for the publication of any potentially identifiable images or data included in this article.
Author contributions
JS-O: Conceptualization, Investigation, Data curation, Project administration, Writing – original draft, Writing – review & editing, Visualization. AR–M: Investigation, Data curation, Writing – review & editing, visualization. SB: Investigation, Data curation, Writing – review & editing. AR–L: Investigation, Data curation, Writing – review & editing. RF–C: Investigation, Data curation, Writing – review & editing. MC–G: Investigation, Data curation, Writing – review & editing. RL: Investigation, Data curation, Writing – review & editing. EP-A: Writing – original draft, Writing – review & editing, Visualization. GC–V: Investigation, Data curation, Writing – review & editing, Visualization. IR–O: Investigation, Data curation, Writing – review & editing, Visualization. EB-B: Investigation, Data curation, Writing – review & editing. CM–F: Investigation, Data curation, Writing – review & editing. GV: Investigation, Resources, Data curation, Writing – review & editing, Supervision, Funding acquisition. HP–J: Conceptualization, Investigation, Resources, Data curation, Writing – original draft, Writing – review & editing, Visualization, Supervision, Project administration, Funding acquisition.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to thank the patient and her family.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1595513/full#supplementary-material
References
1. Wang Z, Wang H, Ding X, Chen X, and Shen K. A large-cohort retrospective study of metastatic patterns and prognostic outcomes between inflammatory and non-inflammatory breast cancer. Ther Adv Med Oncol. (2020) 12:175883592093267. doi: 10.1177/1758835920932674
2. Menta A, Fouad TM, Lucci A, Le-Petross H, Stauder MC, Woodward WA, et al. Inflammatory breast cancer: what to know about this unique, aggressive breast cancer. Surg Clinics North America. (2018) 98:787–800. doi: 10.1016/J.SUC.2018.03.009
3. Schlichting JA, Soliman AS, Schairer C, Schottenfeld D, and Merajver SD. Inflammatory and non-inflammatory breast cancer survival by socioeconomic position in the Surveillance, Epidemiology, and End Results database, 1990–2008. Breast Cancer Res Treat. (2012) 134:1257. doi: 10.1007/S10549-012-2133-2
4. Fouad TM, Kogawa T, Liu DD, Shen Y, Masuda H, El-Zein R, et al. Overall survival differences between patients with inflammatory and noninflammatory breast cancer presenting with distant metastasis at diagnosis. Breast Cancer Res Treat. (2015) 152:407–16. doi: 10.1007/S10549-015-3436-X
5. Hester RH, Hortobagyi GN, and Lim B. Inflammatory breast cancer: early recognition and diagnosis is critical. Am J Obstet Gynecol. (2021) 225:392–6. doi: 10.1016/J.AJOG.2021.04.217
6. Levy S and Hanna M. A case of bilateral inflammatory breast cancer. Cureus. (2023) 15(6):e40101. doi: 10.7759/cureus.40101
7. Schairer C, Laurent CA, Moy LM, Gierach GL, Caporaso NE, Pfeiffer RM, et al. Obesity and related conditions and risk of inflammatory breast cancer: a nested case-control study. Breast Cancer Res Treat. (2020) 183:467–78. doi: 10.1007/S10549-020-05785-1
8. Atkinson RL, El-Zein R, Valero V, Lucci A, Bevers TB, Fouad T, et al. Epidemiological risk factors associated with inflammatory breast cancer subtypes. Cancer Causes Control. (2016) 27:359–66. doi: 10.1007/S10552-015-0712-3
9. Schairer C, Li Y, Frawley P, Graubard BI, Wellman RD, Buist DSM, et al. Risk factors for inflammatory breast cancer and other invasive breast cancers. JNCI: J Natl Cancer Institute. (2013) 105:1373–84. doi: 10.1093/jnci/djt206
10. Adesoye T, Everidge S, Chen J, Sun SX, Teshome M, Valero V, et al. Low rates of local-regional recurrence among inflammatory breast cancer patients after contemporary trimodal therapy. Ann Surg Oncol. (2023) 30:6232–40. doi: 10.1245/s10434-023-13906-5
11. Sakai T, Ozkurt E, DeSantis S, Wong SM, Rosenbaum L, Zheng H, et al. National trends of synchronous bilateral breast cancer incidence in the United States. Breast Cancer Res Treat. (2019) 178:161–7. doi: 10.1007/S10549-019-05363-0
12. Hamy AS, Abécassis J, Driouch K, Darrigues L, Vandenbogaert M, Laurent C, et al. Evolution of synchronous female bilateral breast cancers and response to treatment. Nat Med. (2023) 29:646–55. doi: 10.1038/s41591-023-02216-8
13. Purkayastha A, Sharma N, and Lohia N. A rare case of triple negative synchronous bilateral invasive ductal carcinoma of breast. Arch Med Health Sci. (2016) 4:67. doi: 10.4103/2321-4848.183345
14. Magalhães D, Rangel I, and Mesquita A. HER2-positive inflammatory breast cancer challenges of clinical practices. Cureus. (2022) 14(3):e22925. doi: 10.7759/cureus.22925
15. Masannat YA, Peter M, Turton P, and Shaaban AM. Case report of bilateral inflammatory breast cancer. Eur J Cancer Care (Engl). (2009) 19:558–60. doi: 10.1111/j.1365-2354.2009.01075.x
16. Kurtz J, Halaharvi D, Sarwar S, and Cripe M. A case of a bilateral inflammatory breast cancer: A case report. Breast J. (2016) 22:342–6. doi: 10.1111/tbj.12578
17. Kawaguchi Y, Kuba S, Morita M, Meng X, Hayashi H, Kobayashi K, et al. Bilateral inflammatory breast cancer that developed two years after treatment for triple-negative breast cancer. Internal Med. (2022) 61:7786–21. doi: 10.2169/internalmedicine.7786-21
18. Schairer C, Brown LM, and Mai PL. Inflammatory breast cancer: high risk of contralateral breast cancer compared to comparably staged non-inflammatory breast cancer. Breast Cancer Res Treat. (2011) 129:117–24. doi: 10.1007/s10549-010-1324-y
19. Chainitikun S, Saleem S, Lim B, Valero V, and Ueno NT. Update on systemic treatment for newly diagnosed inflammatory breast cancer. J Adv Res. (2021) 29:1–12. doi: 10.1016/j.jare.2020.08.014
20. Dabi Y, Darrigues L, Pons K, Mabille M, Abd alsamad I, Mitri R, et al. Incidence of inflammatory breast cancer in patients with clinical inflammatory breast symptoms. PloS One. (2017) 12:e0189385. doi: 10.1371/journal.pone.0189385
21. Kanao S, Kataoka M, Iima M, Ikeda DM, Toi M, and Togashi K. Differentiating benign and Malignant inflammatory breast lesions: Value of T2 weighted and diffusion weighted MR images. Magn Reson Imaging. (2018) 50:38–44. doi: 10.1016/j.mri.2018.03.012
22. Salmanzadeh R, Aghemo K, Thatiparthi B, Al-Shaikhli SA, Salmanzadeh A, DeAngelo O, et al. A case of advanced bilateral inflammatory breast cancer: A radiological perspective. Cureus. (2023) 15(1):e34145. doi: 10.7759/cureus.34145
23. Adesoye T and Lucci A. Current surgical management of inflammatory breast cancer. Ann Surg Oncol. (2021) 28:5461–7. doi: 10.1245/s10434-021-10522-z
24. Bertucci F, Boudin L, Finetti P, Van Berckelaer C, Van Dam P, Dirix L, et al. Immune landscape of inflammatory breast cancer suggests vulnerability to immune checkpoint inhibitors. Oncoimmunology. (2021) 10(1):1929724. doi: 10.1080/2162402X.2021.1929724
25. Chakraborty P, George JT, Woodward WA, Levine H, and Jolly MK. Gene expression profiles of inflammatory breast cancer reveal high heterogeneity across the epithelial-hybrid-mesenchymal spectrum. Transl Oncol. (2021) 14:101026. doi: 10.1016/j.tranon.2021.101026
26. Van Berckelaer C, Rypens C, van Dam P, Pouillon L, Parizel M, Schats KA, et al. Infiltrating stromal immune cells in inflammatory breast cancer are associated with an improved outcome and increased PD-L1 expression. Breast Cancer Res. (2019) 21:28. doi: 10.1186/s13058-019-1108-1
27. Bertucci F, Finetti P, Vermeulen P, Van Dam P, Dirix L, Birnbaum D, et al. Genomic profiling of inflammatory breast cancer: A review. Breast. (2014) 23:538–45. doi: 10.1016/j.breast.2014.06.008
28. André F, Ciruelos E, Rubovszky G, Campone M, Loibl S, Rugo HS, et al. Alpelisib for PIK3CA-mutated, hormone receptor-positive advanced breast cancer. N Engl J Med. (2019) 380:1929–40. doi: 10.1056/NEJMOA1813904
29. Cerma K, Piacentini F, Moscetti L, Barbolini M, Canino F, Tornincasa A, et al. Targeting PI3K/AKT/mTOR pathway in breast cancer: from biology to clinical challenges. Biomedicines. (2023) 11:109. doi: 10.3390/BIOMEDICINES11010109
Keywords: inflammatory breast neoplasms, bilateral breast neoplasms, multimodal imaging, molecular profiling, therapeutics
Citation: Sabaté-Ortega J, Ribera-Montserrat A, del Barco S, Roqué-Lloveras A, Fort-Culillas R, Carmona-García MC, Liñan R, Polonio-Alcalá E, Carbó-Vilavedra G, Ramos-Oliver I, Bujons-Buscarons E, Montañés-Ferrer C, Viñas G and Pla-Juher H (2025) Double trouble, managing bilateral inflammatory breast cancer: a case report. Front. Oncol. 15:1595513. doi: 10.3389/fonc.2025.1595513
Received: 18 March 2025; Accepted: 29 July 2025;
Published: 20 August 2025.
Edited by:
Ying Lin, Sun Yat-sen University, ChinaReviewed by:
Ivette Suarez-Arroyo, Central University of the Caribbean, Puerto RicoTeodora Hoinoiu, Victor Babes University of Medicine and Pharmacy, Romania
Copyright © 2025 Sabaté-Ortega, Ribera-Montserrat, del Barco, Roqué-Lloveras, Fort-Culillas, Carmona-García, Liñan, Polonio-Alcalá, Carbó-Vilavedra, Ramos-Oliver, Bujons-Buscarons, Montañés-Ferrer, Viñas and Pla-Juher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gemma Viñas, Z3Zpbnllc0BpY29uY29sb2dpYS5uZXQ=; Helena Pla-Juher, aHBsYUBpY29uY29sb2dpYS5uZXQ=
†ORCID: Josep Sabaté-Ortega, orcid.org/0009-0006-9948-3277
Anna Ribera-Montserrat, orcid.org/0009-0008-8013-5218
Sonia del Barco, orcid.org/0000-0002-4951-6871
Ariadna Roqué-Lloveras, orcid.org/0000-0003-0492-7463
Roser Fort-Culillas, orcid.org/0000-0001-5064-9383
Emma Polonio-Alcalá, orcid.org/0000-0003-1017-7216
Gerard Carbó-Vilavedra, orcid.org/0000-0002-3325-4950
Elisabet Bujons-Buscarons, orcid.org/0009-0001-7708-2038
Gemma Viñas, orcid.org/0000-0002-0459-573X
Helena Pla-Juher, orcid.org/0000-0003-3550-1449