 Sabine Felser1*
Sabine Felser1* Lars A. Bonke1Änne Glass2
Lars A. Bonke1Änne Glass2 Daniel Strüder3Jana Stolle4
Daniel Strüder3Jana Stolle4 Susann Schulze4,5
Susann Schulze4,5 Markus Blaurock6Anke Steinmetz7Julia Daunheimer1Ursula Kriesen1Christina Grosse-Thie1,8
Markus Blaurock6Anke Steinmetz7Julia Daunheimer1Ursula Kriesen1Christina Grosse-Thie1,8 Christian Junghanss1
Christian Junghanss1- 1Department of Internal Medicine, Clinic III – Hematology, Oncology and Palliative Care, Rostock University Medical Center, Rostock, Germany
- 2Institut for Biostatistic and Informatics in Medicine, Rostock University Medical Center, Rostock, Germany
- 3Department of Otorhinolaryngology, Head and Neck Surgery “Otto Koerner”, Rostock University Medical Center, Rostock, Germany
- 4Krukenberg Cancer Center Halle, University Hospital Halle, Halle (Saale), Germany
- 5Department of Internal Medicine, Medical Clinic II, Carl-von-Basedow Klinikum, Merseburg, Germany
- 6Department of Otorhinolaryngology, Head and Neck Surgery, Universitätsmedizin Greifswald, Greifswald, Germany
- 7Department of Orthopedics, Trauma and Rehabilitation Medicine, Physical and Rehabilitation Medicine, University Medicine Greifswald, Greifswald, Germany
- 8Hematology and Oncology Practice, Rostock, Germany
Introduction: Despite targeted exercise interventions alleviating functional deficits in head and neck cancer (HNC) patients, many patients are insufficiently physically active. A promising approach to reducing barriers could be individually adaptable home training. The “OSHO #94” study examined the short-term effectiveness, the medium-term sustainability, and the safety of an individualized home exercise program
Methods: This multicenter, single-arm, interventional study included patients in aftercare or in stable remission. Participants were advised to perform an individualized home exercise program (mobilization, coordination, strengthening, and stretching) at least three times a week and moderate-intensity endurance training two to three times a week. During the 12-week intervention, they kept a training diary and received weekly physiotherapist calls. In the subsequent 12-week follow-up (FU), participants were asked to continue training. The evaluation of short-term effects (between pre- and post-intervention) and medium-term effects (incl. FU), included the assessment of quality of life (QoL), physical activity level (Leisure Score Index (LSI); weekly amount), body composition, shoulder/cervical spine range of motion, fall risk, and aerobic performance. Adverse events were recorded.
Results: Fifty-three patients (57% male) were enrolled, 83% completed the post assessment, and 72% completed FU. During the intervention, participants exercised for 257 min/week (with 95 minutes individual and 162 minutes endurance). The pre-post intervention effect on the global QoL was small (rw=0.20, p=0.186). Moderate effects were found in emotional (rw=0.38, p=0.011) and social functioning (rw=0.46, p=0.002), fatigue (rw=0.37, p=0.013), and dyspnea (rw=0.32, p=0.035). LSI increased significantly (25 vs. 39, p=0.003), whereas total physical activity duration remained unchanged (280 vs. 290 min/week, p=0.160). Small effects were observed on body composition. The largest effects were seen in physical functioning, particularly aerobic performance (rw=0.67, p<0.001). Nine participants (17%) reported training-related adverse events, primarily pain. Half of participants (48%) continued with individual training during FU. Some short-term effects could be detected medium-term.
Discussion: Physical activity level improved despite an unchanged activity duration suggesting an increased training intensity. With individualized home exercises and remote support, home training was effective and safe. After support ended, patients maintained their activity level and the effects were sustained, suggesting suitability for routine care.
1 Introduction
Head and neck cancer (HNC) frequently lead to functional deficits, particularly in eating, breathing, speech, pain, mood, and neck and shoulder mobility (1–4). These deficits, along with visible disfigurements, weight loss, and sarcopenia (5), as well as body image disturbances (6), impacts health-related quality of life (QoL) (6–8). Advances in diagnosis and treatment have increased the survival rate of HNC patients (9–11), shifting the focus beyond life expectancy to functional abilities and QoL (12). Rehabilitative measures primarily address physical impairments (13), with physical activity emerging as a promising intervention to enhance QoL. Specifically, strength and endurance training programs have shown positive effects on muscle strength, cardiorespiratory fitness, and pain reduction (14–18). The American Head and Neck Society therefore recommends early rehabilitation screening, objective assessments, targeted referrals, and the promotion of regular exercise (19).
Despite existing knowledge and exercise recommendations, many HNC patients remain insufficiently physically active (20–22). Barriers to structured physical activity include physical complaints, time constraints, lack of motivation, and insufficient knowledge (23, 24). Moreover, individual preferences regarding the type, location, intensity, and supervision of exercise programs vary, as do limitations and needs. Surveys have shown that HNC patients prefer unsupervised and supervised training programs—performed either alone or with family members, at moderate intensity, at home or outdoors, and at flexible times (25–27). Individually adaptable home- and outdoor-based training programs are therefore considered a promising approach to promoting physical activity, yet they remain insufficiently studied. Additionally, there is limited knowledge regarding the sustainability of such (home-based) exercise interventions. Our goal was to develop a low- to moderate-intensity exercise program that HNC patients can perform independently and flexibly at home or outdoors. In the first study, suitable exercises were compiled and evaluated for their effectiveness in a group-based training setting (28). After combining suitable exercises into an exercise manual (29), the final step was to evaluate the effectiveness and safety of home-based training (30).
The primary outcome of this study was the comparison of the global QoL score after a 12-week home exercise intervention with the value measured before the intervention. The study specifically examined the suitability of the chosen approach, including its integration into routine care. To this end, (i) patients’ compliance with the training recommendations, and (ii) the perceived usefulness and actual utilization of the provided training materials and information were evaluated. Furthermore, the effectiveness of the intervention was assessed by examining (iii) the short-term effects of the home exercise program on QoL, physical activity level, body composition and physical functioning, as well as (iv) the medium-term effects beyond the intervention period. Finally, (v) the safety of the training program was assessed based on reported adverse events.
2 Materials and methods
2.1 Study design, participants, and eligibility criteria
A prospective, multicenter, single-arm, intervention trial was designed and registered (German Registry of Clinical Trials No. DRKS00023883). The Department of Hematology, Oncology, and Palliative Medicine at the University Hospital Rostock (UMR) conducted the study. Further recruiting hospitals were the Krukenberg Cancer Center Halle (UKH), and the Department of Otorhinolaryngology, Head and Neck Surgery at the University Medicine Greifswald. The study design and the number of enrolled required patients (N=53) were based on the established criteria in Felser et al. (30). Patients eligibility criteria were: ≥18 years old with a diagnosis according to ICD: C00–C14, C30–C32 (HNC) in aftercare or with stable remission under immunotherapy, who had medical clearance from their treating physician, were able to walk independently, and provided informed consent for participation. The exclusion criteria are inadequate knowledge of the German language, consent not given, clinically relevant heart failure (NYHA III and IV), myocardial infarction within the last 4 weeks, unstable angina pectoris, higher-grade valvular vitia, uncontrolled cardiac arrhythmias, chronic obstructive pulmonary disease (GOLD III and IV), peripheral arterial occlusive disease (≥Stage III according to Fontaine), diseases that could seriously impair cognitive performance (e.g. dementia, stroke, Wernicke-Korsakoff syndrome), known alcohol dependency and score <24 points on the Mini-Mental State Examination.
Elimination criteria after inclusion were diagnosis of a relapse or new tumor disease, prolonged hospital stays due to other illnesses/surgeries (e.g., heart attack, hip or knee surgery, death (=health reasons), admission to inpatient rehabilitation, and discontinuation at the patient’s request.
2.2 Study procedure, intervention and measurement points
Included patients underwent a comprehensive preliminary examination. Based on its results and individual goals, therapists create a personalized training plan. All patients were instructed in the training program, which included mobilization, coordination, strengthening, and stretching exercises. They received the “Exercise manual for patients with mouth, jaw, face and throat tumors’” (29) with the recommended exercises marked in it. Additionally, all recommended exercises and four comprehensive training programs were supplied as video files on a USB stick, along with an elastic resistance band and an inflatable exercise ball (Ø 22 cm) for use at home. Participants were instructed to complete either their individualized program or one of the video sessions at least three times per week for 15–30 minutes. Endurance activities (e.g., walking, cycling, swimming, dancing) were recommended 2–3 times per week for 30 minutes. Training intensity was self-monitored using the BORG rating of perceived exertion (RPE) scale (31), and the recommended range was between 11 (fairly easy) and 15 (hard). During the 12-week intervention, therapists conducted weekly telephone calls and documented the conversations. Patients were also asked to maintain a training diary. A post-examination followed after 12-week to evaluate the short-term effects (pre-post comparison).
Afterward, patients entered a 12-week follow-up (FU) period without structured support. The final FU examination was used to evaluate medium-term effects (pre-FU, post-FU) and assess whether participants maintained or enhanced outcomes independently.
2.3 Outcome measures
The season was determined based on the date of study enrollment.
Disease-specific data on the participants were recorded once by the treating/including physicians at the time of study inclusion.
At the three measurement points–pre, post and FU–patient-reported outcomes (PROs) were recorded, and a physical function diagnostic was carried out. The assessment consists of the following measures:
Patient-reported:
− Sociodemographic data and lifestyle factors were recorded using an initial questionnaire.
− QoL was measured using two established questionnaires: the EORTC QLQ-C30 version 3.0 questionnaire (32, 33) and the QLQ-HN35 head and neck–specific questionnaire (33). No threshold values were set in advance to identify clinically important differences. The primary outcome was determined by comparing the global QoL score post- vs. pre-intervention.
− Physical activity level were assessed using a modified version of the Godin-Shephard Leisure-Time Physical Activity Questionnaire (GSLTPAQ) (34, 35). Two parameters, the Leisure Score Index (LSI) and the weekly duration of physical activity [min], were recorded.
− Assessment of the intervention and support was conducted with an exit questionnaire. Participants rated the perceived effects of the intervention on ten domains (body awareness, coordination, endurance, general mood, general performance, mobility, physical well-being, self-esteem, strength, and stress reduction) using a 4-point Likert scale. They also evaluated the difficulty of self-motivation and the motivational impact of the weekly physiotherapy calls using the same scale. Patients indicated whether they exercised alone or with others, whether they intended to continue training, and whether the provided information was helpful. Finally, they were asked to which material they had used (exercise manual, videos, and training equipment).
− During the FU examination, patients were asked about the continuation of the individual exercise program even after the end of the intervention.
Physical function diagnostic:
− Body composition, including body fat percentage [%], and skeletal muscle mass [kg] was assessed using a bioimpedance analyzer (BIA). These measures were optional, as not all recruiting clinics had access to a BIA. UMR and UKH used the same device, the ‘seca mBCA 525’ (seca GmbH, Hamburg, Germany). Measurements were conducted according to the manufacturer’s instructions. The body mass index [kg/m²] was calculated based on height and weight.
− The mobility of the temporomandibular joints was measured using the distance between the incisors [cm] determined with a ruler at maximum mouth opening.
− Shoulder joint mobility was measured as the active range of motion (ROM) in the sagittal, frontal, and transversal planes using a manual goniometer [°]. Patients and therapists indicated separately for each shoulder joint whether there were restrictions in at least one axis of motion.
− Cervical spine mobility was measured as the active ROM in rotation and lateral flexion using a manual goniometer [°] and as inclination/reclination using a ruler [cm].
− The mobility of the lower back and hamstring muscles was assessed with the stand and reach test [cm] (36).
− Fall risk was evaluated by using the short physical performance battery (SPPB) (37). The scores range from 0 (worst performance) to 12 (best performance).
− Aerobic performance was assessed using the 6-minute walk test (6MWT) (38). The primary measure was the walking distance [m]. After the 6MWT, participants rated their RPE using the Borg scale (6 = really, really easy, 20 = maximum effort) (31) and their exercise-induced pain in the leg muscles using a Category-Ratio (CR)-10 scale (0 = no pain at all, 10 = extremely intense pain) (39).
Following completion of the intervention, the telephone protocols and training diaries were evaluated regarding the following parameters:
− Compliance regarding training recommendations: training diary were analyzed for average weekly training frequency and duration, separately for individualized and endurance training. Additional, non- recommendation activities (e.g., yoga) were recorded separately.
− Adverse events in connection with the training were recorded.
− The reason for dropping out was asked in the event of early termination of the study, if possible.
2.4 Statistical analysis
Quantitative variables are presented as mean ± standard deviation (SD) or in case of non-normality, as median (Q1, Q3), ranging from minimum to maximum (min to max). Qualitative variables are reported as relative frequency % and absolute (n). Missing data are indicated but excluded from percentage calculations. The normality of the data was assessed using the Shapiro-Wilk test.
Spearman’s rank correlation was performed to determine whether there is a correlation between intrinsic and extrinsic motivation (weekly phone calls).
Pre-post analyses were conducted using the paired t-test for normally distributed data with Cohen’s d for dependent samples to estimate short-term effects of intervention (0.20 to <0.5 = small, 0.5 to <0.8 = moderate, ≥0.80 = large) (40). Otherwise, the Wilcoxon signed-rank test with rw estimating the effect was used. Effect sizes rw were assessed on the basis of Cohen’s thresholds (0.10 to <0.3 = small, 0.3 to 0.5 = moderate, ≥0.5 = large) (41).
Medium-term effects of intervention were examined as changes between pre- and FU measurement, as well as between post- and FU measurement. To avoid attrition bias, only participants who completed the whole study (all three measurement points) were included into the analysis of medium-term effects. Thus, the two different samples analyzed pre-post (n=44) and pre-(post)-FU (remained n=38) could cause differing pre-post results. For normally distributed quantitative data, a one-way repeated-measures ANOVA with Bonferroni correction was conducted. The assumption of normality of the difference scores was assessed using the Shapiro-Wilk test. No outliers were detected in the data. Cohen’s d is given to quantify effects. For non-normally distributed data, a Friedman test was conducted, followed by Wilcoxon post hoc tests with a Bonferroni correction. Box plots were used to graphically represent changes over time (Supplementary Figures S3, S4). A p-value <0.05 was considered statistically significant. All data were analyzed using IBM® SPSS® Statistics.
3 Results
Fifty-three patients were enrolled in the study between January 2021 and May 2024. The 12-week home exercise program and post-examination were completed by 83% (n=44). The final FU examination could be carried out on 72% (n=38) of the participants. A total of 28% (n=15) of participants discontinued the study prematurely. Of these, eight withdrew for health reasons, one due to inpatient rehabilitation, and three for personal reasons. Three patients could not be reached by phone, leaving the reasons for their discontinuation unclear (Figure 1).
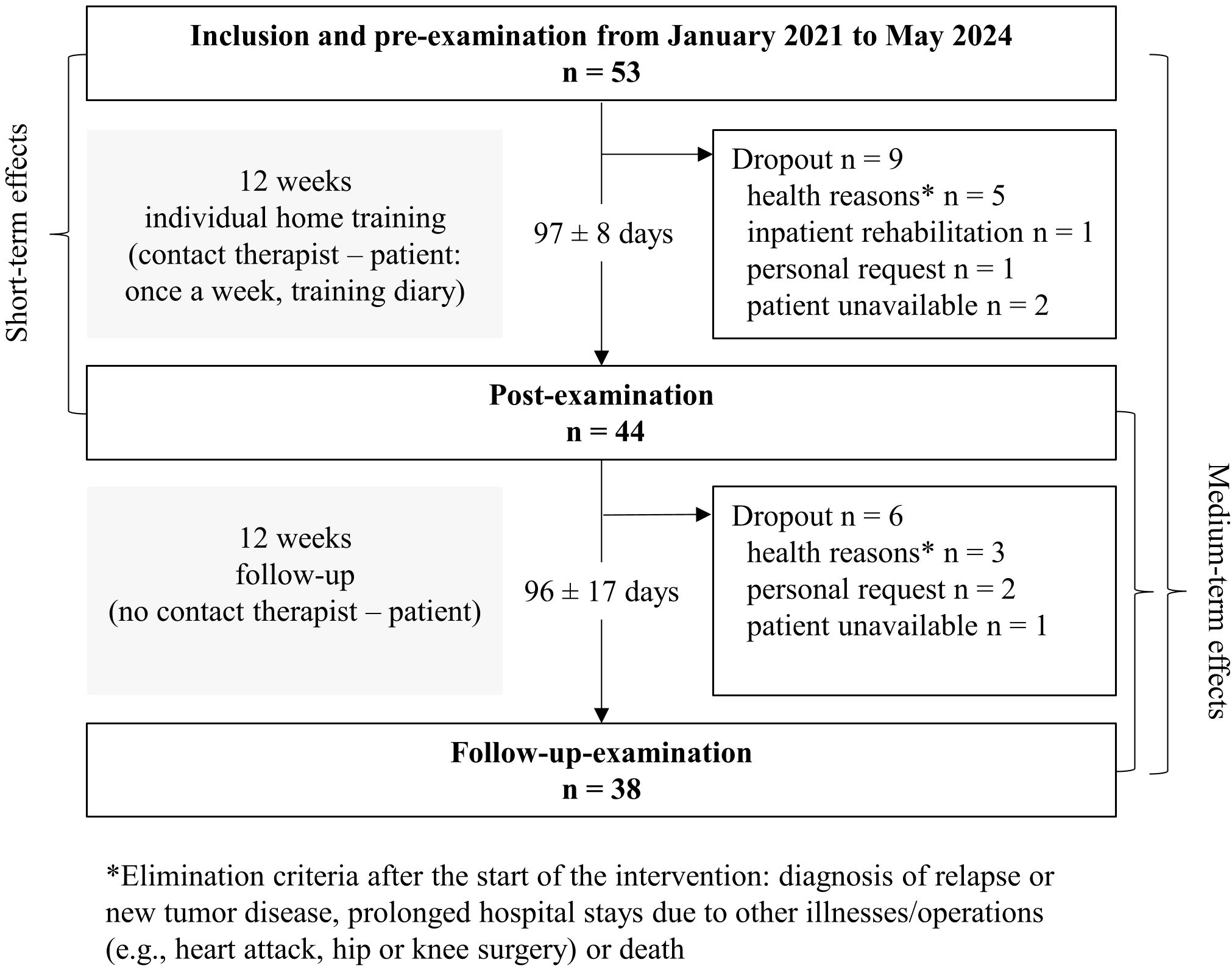
Figure 1. Flow chart of the OSHO #94 study.
Most participants were enrolled in the study during spring (40%, n=21) and fall (30%, n=16). In winter, 24% (n=13) were included, while 6% (n=3) were enrolled in summer.
3.1 Participants’ sociodemographic, lifestyle and clinical data
The participants’ sociodemographic, lifestyle, and clinical data are summarized in Table 1. Of the 53 participants included, 57% (n=30) were male. The median age was 63 (58, 70), ranging from 20 to 85 years. An upper secondary education had been attained by 38% (n=20) of the participants, 58% (n=30) were non-smokers, 35% (n=18) answered that they currently do not drink any alcohol at all, and 60% (n=31) stated that they had been active in sports before the disease. The most common tumor location was the oropharynx (36%, n=19), followed by the oral cavity (26%, n=14). The median time after the (last) diagnosis was 28 (12, 51) months (3 to 199). At the time of study enrollment, 91% (n=48) were in complete remission. A feeding tube was present in 13% (n=7) of the participants and 38% (n=20) were taking pain medication.
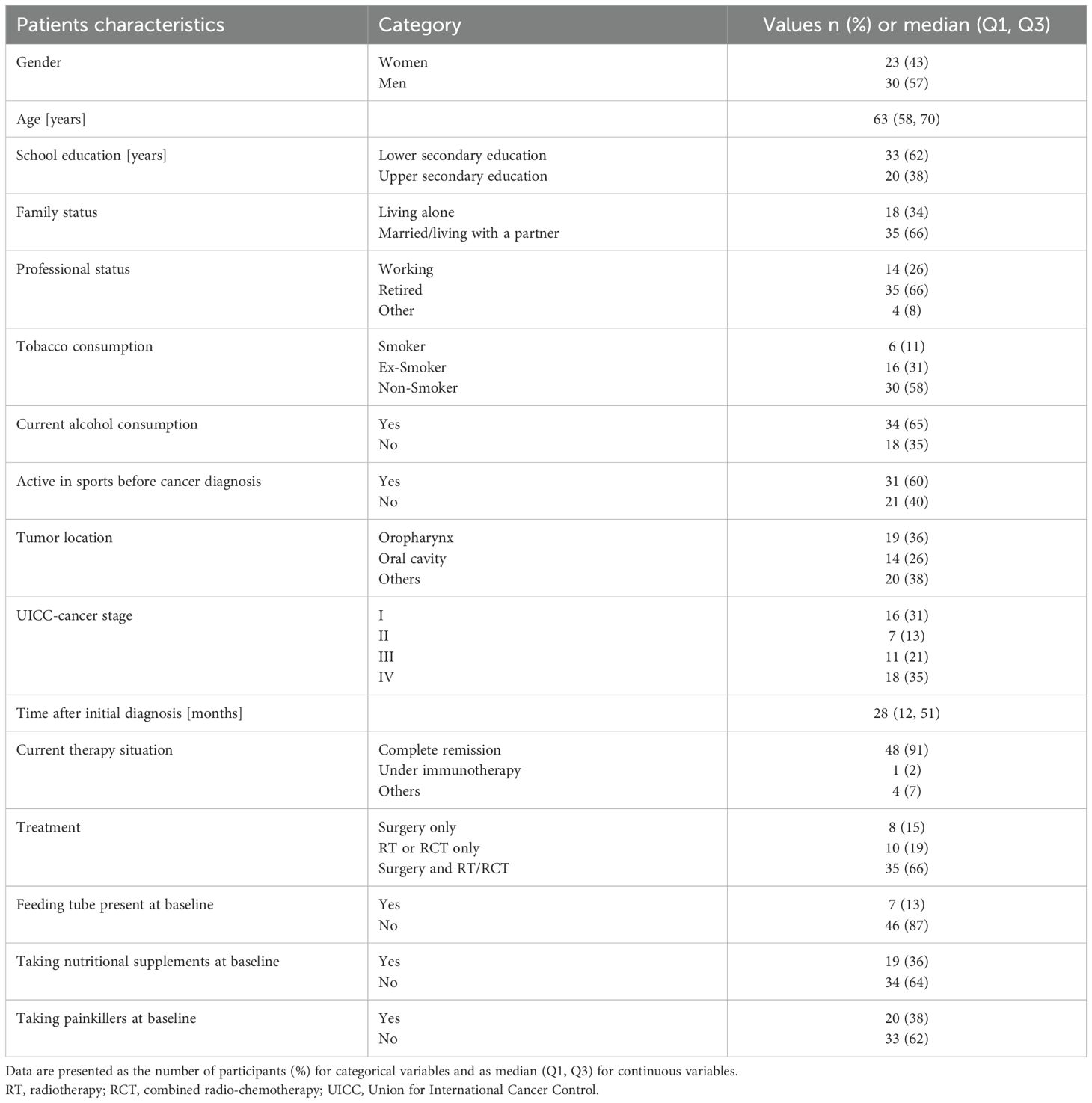
Table 1. Sociodemographic, lifestyle and clinical data (n=53).
3.2 Compliance regarding training recommendations
The training diaries of n=41 participants were available with one of them only partially analyzable, finally resulting in n=40 valid training records. Individual exercises were completed 3.3 (2.2, 4.3) times per week, ranging from 0.0 to 6.8, with a training time of 95 (56, 127) min (0 to 256). Endurance training, often in the form of walking, was completed 2.7 (1.6, 5.5) times per week (0 to 13.8), with 162 (86, 304) min (0 to 531 min). Additional, non- recommendation activities was only completed to a limited extent. The weekly training overall was completed 6.4 (4.9, 9.2) times, with a median training time of 257 (162, 417) min, ranging from 39 to 753 min.
Overall, 85% (35/41) of the participants followed the recommendations regarding their individual exercise program with a given number of sessions to practice, and a little less, 78% (31/40) regarding their endurance training. The proportion of patients who met the training recommendations per the protocol in both areas was 68% (28/40). A comparison of training recommendations and realizations by the participants is shown in Supplementary Figure S1.
According to training diaries and telephone protocols, 58% (25/43) of participants experienced training interruptions. The longest (4 weeks) followed a feeding tube placement. COVID-19 and colds led to 4–14-day interruptions in five cases, while pneumonia (n=1) and urinary tract infections (n=2) caused 1–2-week breaks. Five participants paused their training during the end-of-year celebrations. Shorter interruptions (1–4 days) were due to pain (migraine/headache, back pain, abdominal pain, menstrual pain), dizziness, nausea, medical appointments, vaccinations, personal stress, childcare, travel, or weather conditions. Depression and lack of motivation led to up to 14-day breaks in three cases.
During the post-examination, 67% (n=28) said “yes” to the question of whether they would continue training, while 33% (n=14) “I don’t know.” At FU, 48% had maintained individual training.
3.3 Information, use of the exercise materials, weekly calls, and training with others
All patients (100%) stated that the information they received about the training was sufficient. The exercise manual was used by 81% (n=34) of the participants and the USB stick with the training videos by 41% (n=17), with 21% (n=9) stating that they used both. Small equipment (elastic band/ball) was used by 83% (n=35) of the participants. During the post-examination, 23% (n=10) found self-motivation for training not difficult, 40% (n=17) somewhat difficult, 30% (n=13) moderately difficult, and 16% (n=7) very difficult. Overall, 93% (n=40) felt that the therapists’ weekly calls positively influenced their motivation (26% very, 37% quite, 26% somewhat). No correlation was found between intrinsic and extrinsic motivation. Most participants (75%, n=32) trained alone, 9% (n=4) with others, and 16% (n=7) both alone and with others.
3.4 Moderate short-term effects on QoL
The short-term intervention effects on QoL, measured pre-post, are reported in Table 2.
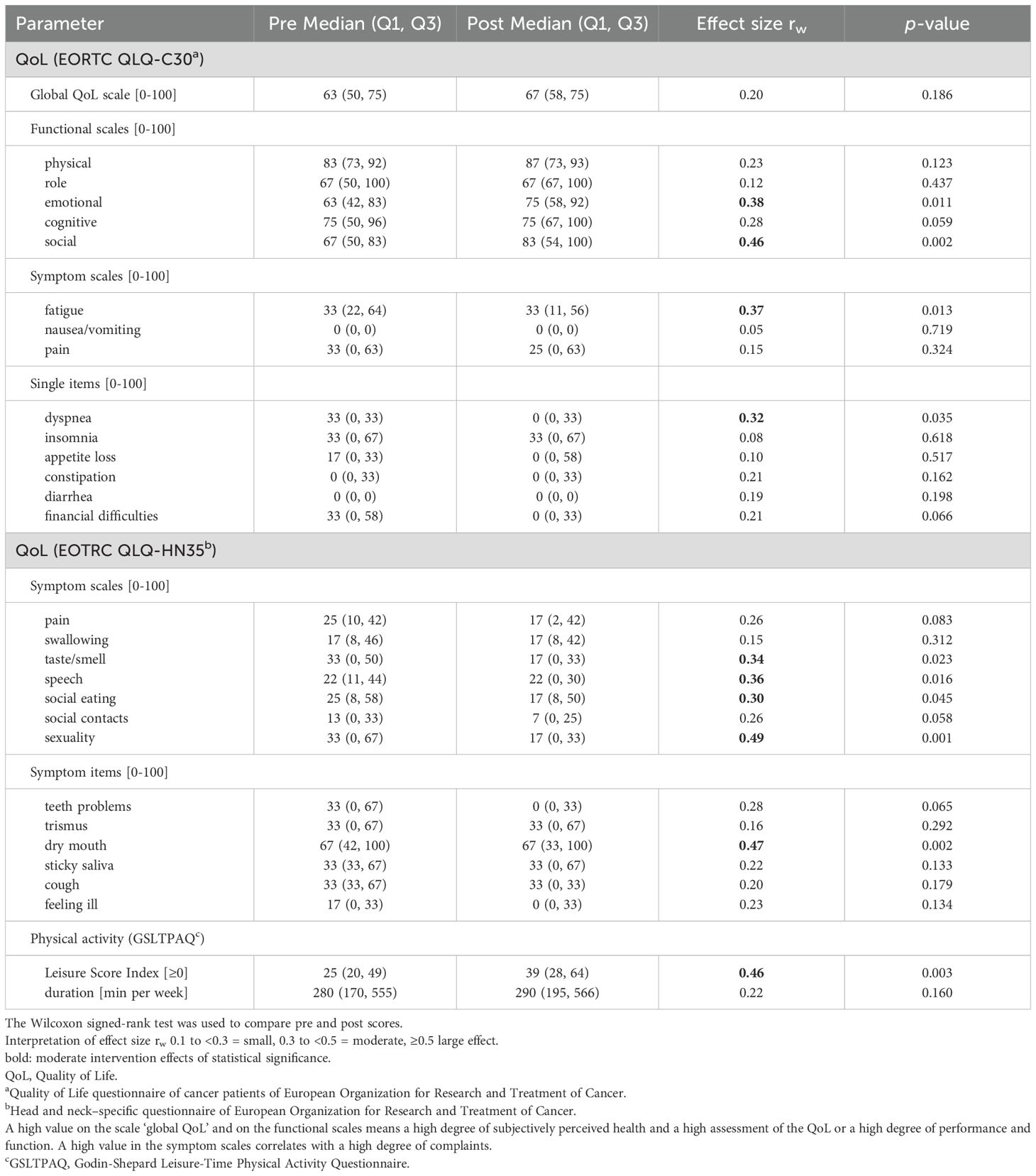
Table 2. Moderate pre-post-intervention effects on quality of life and physical activity level (n=44).
EORTC QLQ-C30: The intervention effect on the global QoL was small (rw=0.20, p=0.186). The score improved from 63 (pre intervention) to 67 (post intervention) by 4 points. Moderate effects were observed in 2 of the 5 functional scales: emotional functioning (rw=0.38, p=0.011, +12 points) and social functioning (rw=0.46, p=0.002, +16 points); the 3 remaining effects were detected as small with rw<0.3. Among the 3 symptom scales and 6 single items, moderate positive effects were observed for fatigue (rw=0.37, p=0.013) and dyspnea (rw=0.32, p=0.035).
EORTC QLQ-HN35: Positive changes were observed in all 7 symptom scales, with significant effects for taste/smell (rw=0.34, p=0.023), speech (rw=0.36, p=0.016), social eating (rw=0.30, p=0.045), and sexuality (rw=0.49, p=0.001). A significant and moderate effect was observed for dry mouth (rw=0.47, p=0.002), while the effects for the other 5 symptom items were small.
3.5 Short-term effects on physical activity level
The home training intervention had a moderate effect on the physical activity level, with the LSI increasing from 25 to 39 (rw=0.46, p=0.003). By contrast, the effect on weekly physical activity duration was not significant (rw=0.22, p=0.160, 280 vs. 290 minutes per week) (Table 2).
3.6 Short-term effects on body composition
The intervention had small favorable effects on body composition (Table 3). Between the pre- and post-intervention measurements, body fat percentage decreased by 1.2%p (d=0.48, p=0.009, n=33) and skeletal muscle mass increased by about 3%p (d=0.45, p=0.014, n=33). No significant changes were observed in body mass index (rw=0.03, p=0.848, n=39).
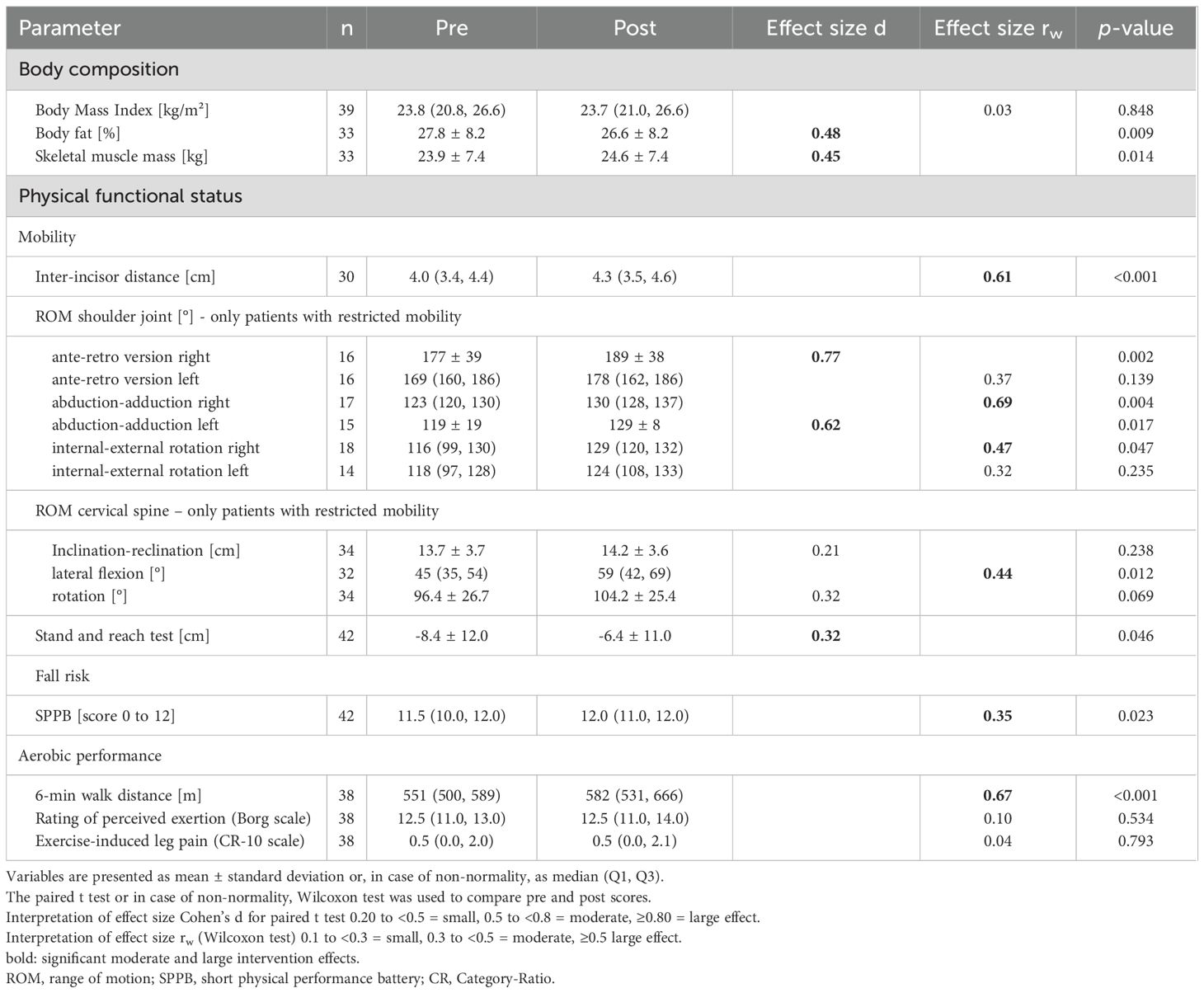
Table 3. Moderate and large pre-post-intervention effects on body composition and physical functionality.
3.7 Short-term effects on physical functioning
Inter-incisor distance: Mouth opening increased by 3 mm post-intervention (rw=0.61, p< 0.001, n=30), see Table 3.
ROM in the shoulder joints: In the ROM of the shoulder joints, moderate to large effects were observed in patients with restricted mobility. Thus, the ROM in the right shoulder joint improved in ante-/retroversion by 12° (d=0.77, p=0.002, n=16), in abduction/adduction by 7° (rw=0.69, p=0.004, n=17), and in internal/external rotation by 13° (rw=0.47, p=0.047, n=18). On the left side, an improvement of 10° (rw=0.62, p=0.017, n=16) was observed in abduction/adduction. No statistically significant effects could be detected in the ROM of the left shoulder joint for ante-/retroversion and internal/external rotation, since the changes here were rather small.
ROM in the cervical spine: The intervention had a moderate effect on lateral flexion in patients with limited cervical spine mobility: +14° (rw=0.44, p=0.012, n=32). The effects on rotation were small: +8° (d=0.32, p=0.069, n=34). No statistically significant changes were observed in inclination/reclination.
Stand and reach test: The intervention effect on mobility of the lower back and hamstring was small (d=0.32, p=0.046, n=42). The distance to the ground decreased by 2.0 cm after the intervention.
SPPB: Before the intervention, 50% of participants achieved the maximum score, increasing to 67% post-intervention. The calculated effect was small (rw=0.35, p=0.023, n=42).
Aerobic performance (6MWT): A large intervention effect on aerobic performance was observed (rw=0.67, p<0.01, n=38): participants increased their walking distance by an average of 31 m (+5.6%) post-intervention. No statistically significant changes were observed in RPE (BORG scale) or exercise-induced leg muscle pain (CR-10 scale).
PROs: The subjective rating of the improvements by the participants (none = 0 to very strong = 3) shows similar distributions across all 10 domains surveyed. Mean values ranged between 1.67±0.75 and 1.40±0.66 (slightly to fairly), with the highest values given for mobility, body awareness and coordination, and the lowest for endurance and strength (Supplementary Figure S2).
3.8 Small medium-term effects on QoL
Medium-term intervention effects on QoL, comparing both, pre-FU and post-FU, are reported in Table 4, with additionally given the pre-post results of n=38 permanent participants. All changes of scores are shown graphically as box plots in Supplementary Figure S3.
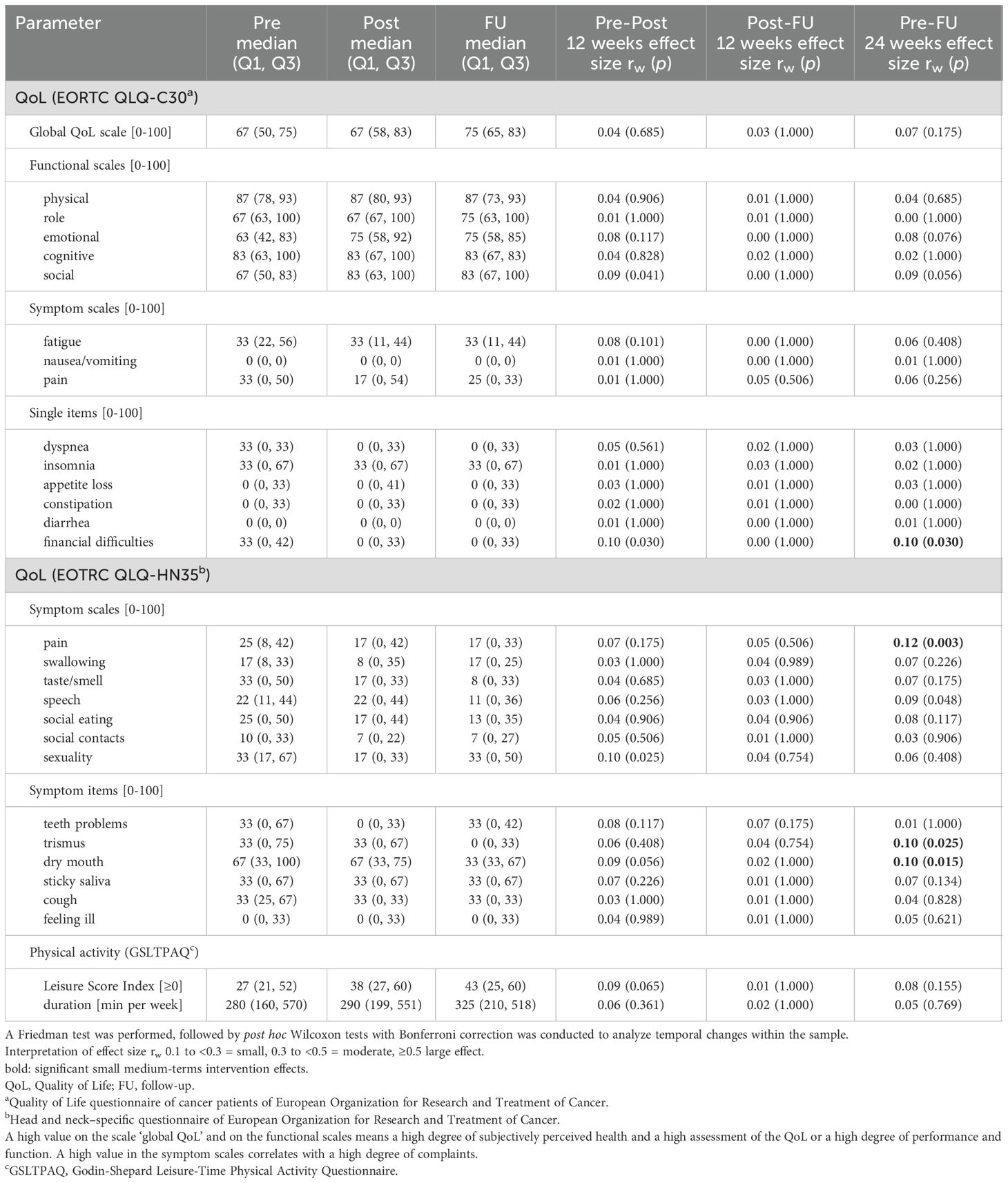
Table 4. Small medium-term intervention effects (pre-FU, post-FU) on quality of life and physical activity levels (n=38).
EORTC QLQ-C30: No significant effect on global QoL was observed between pre and FU examination (rw=0.07, p=0.175, n=38), though the score itself changed by +8 points. But note, this increase is only a descriptive information and reported not before FU (i.e. not by intervention), namely from the post intervention situation with a score of 67 to 75 FU. The resulting effect on QoL (post-FU) is not significant (rw=0.03, p=1.000). Similarly, no significant changes were observed post-FU in both, the functional scales, symptom scales and single items.
EORTC QLQ-HN35: Positive changes with small effects between pre and FU measurement were observed in 1 of the 7 symptom scales: pain (rw=0.12, p=0.003), as well as in 2 of the 6 individual items: trismus (rw=0.10, p=0.025), and dry mouth (rw=0.10, p=0.015).
3.9 Medium-term effects on physical activity level
The LSI and the weekly training duration continue to increase, but there are no significant effects (Table 4).
3.10 Medium-term effects on body composition
The small positive effects on body composition seen in short-term analysis are not detectable between post and FU. The score values are similar. Between pre intervention and FU, body fat decreased by 1.1%p (d=0.43, p=0.086, n=29) and muscle mass increased by about 3%p (d=0.36, p=0.189, n=29), which is consistent with the short-term results (Table 5).
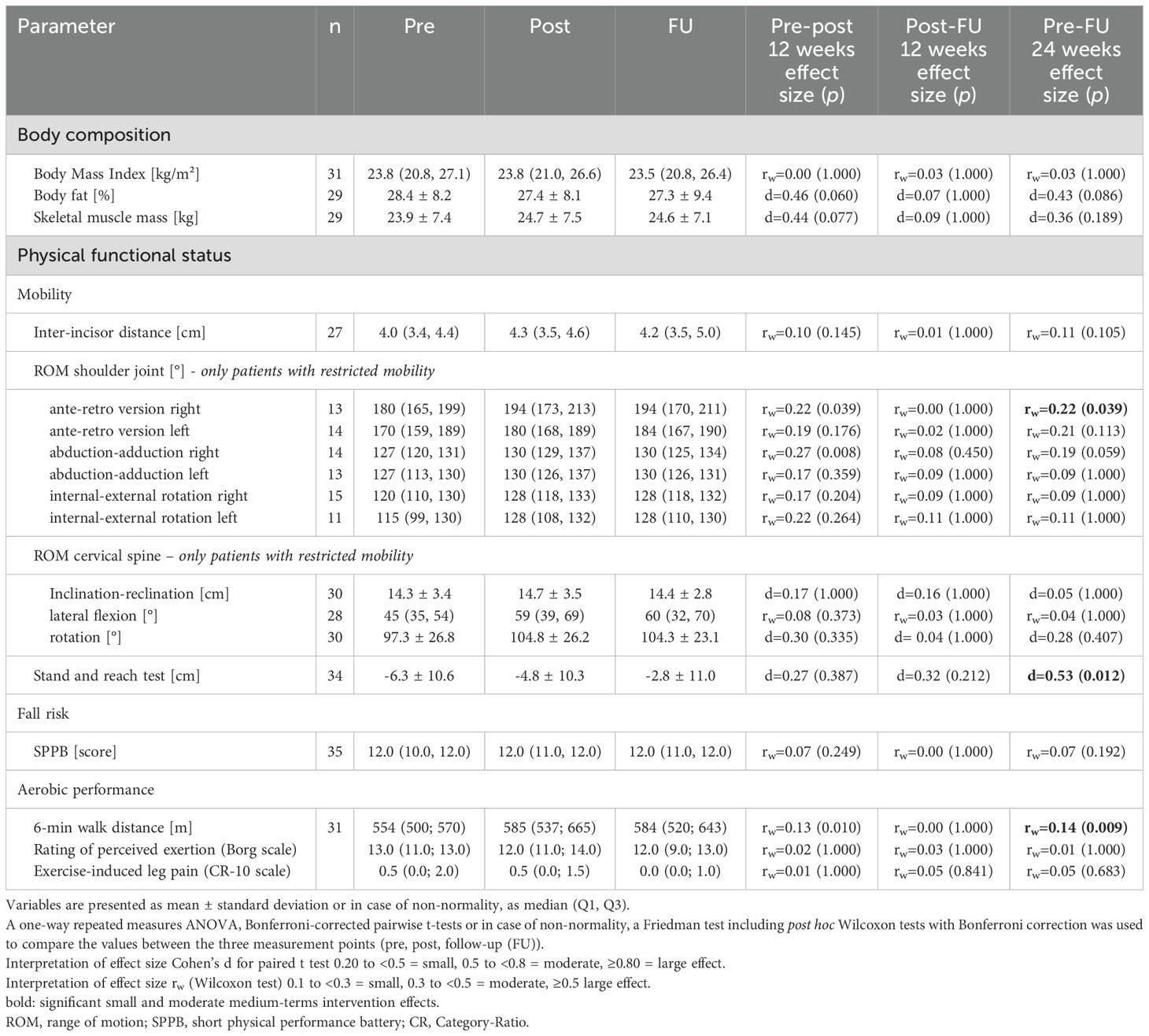
Table 5. Small and moderate medium-term intervention effects (pre-FU, post-FU) on body composition and physical functionality.
3.11 Medium-term effects on physical functioning
The medium-term intervention effects on physical functioning are reported in Table 5, and graphically as box plots in Supplementary Figure S4.
The score values concerning FU vs. post intervention are comparable. No significant effects were observed between post- and FU examination. In contrast, the shown short-term increase of +2 cm mobility in the stand and reach test increased further during FU for two more cm, so that a moderate effect was observed pre-FU (d=0.53, p=0.012, n=34). Small significant effects pre-FU are observed in patients with restricted mobility in the shoulder joint in the right ante-retroversion (rw=0.22, p=0.039, n=13) and in aerobic performance assessed with the 6MWT (rw=0.14, p=0.009, n=31).
3.12 Safety
A total of nine participants (17%) reported adverse events that could be related to exercise. One participant each reported brief dizziness after head movements, nausea after training, cramps during activity in the shoulder girdle/forearm/thumb, Achilles tendon problems, pain during single-leg stance, knee pain, neck pain, and muscle pain. None of these events led to hospitalizations, long-term impairments, or damage.
4 Discussion
The three key findings of our study are: First, a low- to moderate-intensity individualized home exercise program with remote support is safe for HNC patients in the aftercare; second, positive effects on QoL, physical activity level, body composition and physical function were observed, and third, HNC patients accept and use the training materials and knowledge provided.
4.1 Recruitment and participants
In this multicenter study conducted in Rostock, Halle and Greifswald, 53 participants were recruited over a period of 3.5 years. The long recruitment period, aside from the restrictions imposed by the COVID-19 pandemic, may be attributed to the limited number of participating centers (three university hospitals). In Germany, oncological exercise therapy is not yet widely implemented in clinical settings, resulting in a shortage of exercise therapists available to support patients. Recruitment was carried out during aftercare appointments; via self-help group; and through flyers, posters, and ear, nose, and throat practices. Due to the broad and non-standardized nature of these recruitment strategies, it is difficult to estimate the recruitment rate. Seasonal variations were also observed, with spring and fall appearing to the most favorable periods for engaging HNC patients in physical activity programs. The proportion of women (43%) was notably higher than the typical HNC gender distribution (90% men, 10% women). Additionally, many participants were non-smokers and had prior physical activity experience, indicating a selection bias and limiting the generalizability of the findings to the broader HNC population in Germany.
4.2 Compliance with training recommendations
The individual home exercise program is a novel set of exercises specifically designed for HNC patients in aftercare (42). One objective of this study was to assess participants’ training frequency and amount per week. Unlike the pilot cohort (28), participants were explicitly encouraged to incorporate additional endurance training in line with cancer survivor guidelines (43) and the recommendations for HNC patients (16).
Our findings showed that two-thirds of participants adhered to the exercise recommendations. The realized training corresponded to training recommendations in either terms of weekly training session or total duration, or even both, with unexpectedly high compliance (85%) to individual training. This adherence was comparable to that in other home-based (44) and group-based studies (45–47) and significantly higher than that in HNC patients undergoing chemotherapy (48). While the number of weekly sessions met expectations, total training volume was twice the target, despite intermittent interruptions in over 50% of participants. This may be attributed to high intrinsic motivation and good physical performance (selection bias). Most participants were already physically active before the intervention (LSI ≥24) (35). Since the training duration remained stable as the LSI increased, it can be inferred that participants intensified their workouts, which corresponds to training progression (49).
4.3 Information, use of the exercise materials, weekly calls, and training with others
The study aimed to support participants and reduce barriers to physical activity (23, 24) by providing (a) a free exercise manual with information, training programs (29), and video clips, (b) training equipment for coordination and strength, (c) travel cost reimbursement for study visits, and (d) weekly phone calls for support and motivation.
Participant feedback confirmed high utilization of materials and increased motivation through phone calls. High training compliance, adjusted intensity, and continued participation in half of the participants during the FU suggest that knowledge about the benefits of physical activity was effectively conveyed and implemented. As preferred by HNC patients (26), most trained alone, likely due to the individualized program.
The low-resource approach (patients: no travel time or costs, no costs for course participation or training equipment; therapists/clinics: no premises or costs for premises, no time commitment of therapists for the implementation of the training) appears suitable for routine aftercare but requires appropriately qualified exercise therapists for knowledge transfer.
4.4 Effects on QoL
The shown effect of individualized home training on the primary endpoint—global QoL—was lower than expected (30). Although the small intervention effect of our study with d=0.2023 is comparable to the findings of O’Neill et al. (50) this result is surprising, as our calculation for sample size acted on assumption of an experienced effect of d=0.5755, comparable to Burgos-Mansilla et al. (14).
The physical performance/functionality was not only objectively improved but also subjectively perceived by the participants. Strueder et al. (51) described a discrepancy between subjective QoL and objective functionality using swallowing function as an example. They attributed this difference, among other factors, to sensory deficits and reduced sensitivity, which can make it difficult to correctly perceive functional limitations.
In our cohort, global QoL increased by 8 points between the post-intervention (score=67) and FU assessments (score=75). In the literature, exact thresholds for clinically relevant differences are discussed with some controversy (52, 53). Although a threshold of ≥10 points is often assumed, it can be assumed that changes of 8 points are certainly clinically relevant, however small (52). While physical performance remained largely stable during this period, HNC-associated symptoms continued to decrease. These effects are less attributable to home training itself and more indicative of overall successful rehabilitative medical care. This suggests that global QoL is more strongly influenced by symptom reduction than by improvements in physical performance. Moreover, QoL is a multidimensional construct in which the physical component represents only one of several dimensions (54). Therefore, global QoL is not an adequate primary end point for assessing the effectiveness of exercise interventions (in HNC patients).
The improvement in emotional functioning corresponds to the subjective perception of mood enhancement. Whether this improvement is solely attributable to the training or rather the result of a multifactorial interaction—including symptom relief, increased social interactions, enhanced self-esteem, and improved sexual life—cannot be conclusively determined based on the available data. The reduction in dyspnea and, in particular, fatigue is likely due to the moderately intensive endurance training (43). However, the observed pain relief is primarily attributable to the intake of analgesics, which was reported by one-third of the participants, although exercise therapy may also contribute to pain reduction (46, 47).
4.5 Effects on physical activity level
The GSLTPAQ is a validated (34) and widely used tool in oncological research. Most studies utilize the LSI to categorize cancer survivors as either insufficiently active or active (35). In contrast, the present study focused on changes in activity level over time rather than categorial classification. Therefore, a modified version of the GSLTPAQ was used, consistent with approaches in many oncological studies (35). In addition to the LSI —calculated as the number of exercise sessions ≥15 minutes multiplied by their respective intensity levels —the average duration of these exercise sessions was recorded. The total weekly activity duration across the three measurement points showed only a slight increase during the intervention, from 280 to 290 minutes. However, the LSI rose significantly from 25 to 39, suggesting that participants performed their activities at higher intensities, consistent with our recommendations. This assumption is supported by the finding that the average training duration during the intervention (257 minutes per week) nearly matched the total weekly physical activity duration, indicating a shift toward more structured, higher-intensity exercise. Since higher training intensity is known to drive physiological adaptations, it is likely that the observed improvements in aerobic performance and muscle mass were primarily due to increase in intensity (49).
The findings—particularly the non-significant increase in LSI and the extended activity duration between post-intervention to FU—suggest a sustained enhancement in physical activity level, even though only about half of the participants continued with individual training. However, seasonal effects may have influenced the results: 40% of participants were enrolled in spring, leading to FU assessments in summer, a season associated with increased physical activity in the general population (55).
A small number of participants reported lower extremity pain following training, underscoring the importance of gradual training progression. Inactive or insufficiently active patients, in particular, should first increase training volume before advancing to higher intensities to reduce the risk of overuse injuries. For more accurate assessments of physical activity changes, future studies should consider using the modified GSLTPAQ or incorporate objective measurement tools.
4.6 Effects on body composition
During the intervention, positive changes in body composition were observed. The BMI remained stable, while muscle mass increased by approximately 3%p on average and fat mass decreased by around 1%p. The observed increase in muscle mass was only slightly lower than that reported following a progressive resistance training program (56). Since the evidence on the effects of exercise interventions on body composition in HNC patients during after care remains limited (16), a clear interpretation of the results is challenging. However, it is assumed that the positive effects can be attributed to the combination of individualized exercises, including strength exercise and endurance training. This training approach aligns with the current recommendations by Avancini et al. (16), who, based on existing evidence, consider a combination of strength and endurance training particularly effective for this patient population.
The lack of further muscle mass gain during the FU may possibly be attributed to the absence of progression in strength exercises. This highlights the importance of continuously adjusting training intensity and load to promote long-term muscular adaptations (49).
4.7 Effects on physical functioning
Mobility: Improvements in mobility across various body regions suggest the effectiveness of the individualized exercise program. Significant gains in mouth opening were observed after intervention, though additional therapies (e.g., physiotherapy, logopedics) were not tracked. At FU, no further significant gains in inter-incisor distance were observed, likely because most participants had already exceeded the functional threshold for trismus in HNC patients of 35 mm (57) or had reached a normal mouth opening of ≥40 mm (58). According to EORTC QLQ-HN35 assessments, fewer participants reported severe trismus symptoms at FU compared to pre-intervention.
Shoulder mobility improved in participants with restricted mobility in all three axes of movement, with mostly moderate to large effects. Head rotation improved in the home training group, as it did in the group training in the pilot cohort (28), but the effects were smaller in the former. In addition, improvements in ROM were observed in the home training group for lateral flexion of the cervical spine (moderate effect). It is assumed that in the home training group, the affected individuals trained more specifically than was possible in the group setting. Particularly in the cervical spine, ROM is not only determined by muscular tension but possibly also by blockages that cannot be addressed with self-training. Mobility of the lower back and hamstring (stand and reach test) improved markedly, with a large effect— greater than previously observed in group settings.
Fall risk: Although the SPPB has limited sensitivity in physical fit HNC patients (28), results suggest reduced fall risk through improved coordination and strength. The ceiling effect limited mensurable gains.
Aerobic performance: The 6MWT distance could be increased during the 12-week intervention despite the high baseline performance and was then maintained until the FU. The median distance of >580 m post-intervention and FU corresponds to the values of healthy subjects and is significantly higher than the distances that breast cancer survivors achieved on average (59, 60). The walking distance was almost identical to that of the pilot cohort (28) and comparable to the reports of Eades et al. (61) and Capozzi et al. (45). Walking was the most common form of endurance training in the study participants. The higher training intensity probably led to an increase in maximal oxygen uptake (38) as a result of the adaptation phenomena caused by stimuli that were now effective in training (49). The fact that the effect was large for the 6MWT is probably also due to the high specificity of the 6MWT.
PROs: The participants’ assessment of the extent of their improvements in the various areas is consistent with the objective measurement results. The improvement in mobility was most strongly perceived. The perceived improvement in coordination, which is mapped in functional diagnostics using the SPPB, appears stronger than the SPPB can map (lack of sensitivity). The less noticeable improvement in endurance performance was probably due to the adequacy of physical performance before the intervention. In addition, the improvement in walking distance (+31 m) was below the clinically significant change of 54 m for other clinical populations (62, 63). Consequently, the improvements in everyday activities were not as noticeable as the improvements in mobility. The same applies to the assessment of general performance. The improvement in strength was rated lowest by the participants. There were no objective measurement parameters for this, so a comparison was not possible. However, the strong improvements in mobility and the reduction in the risk of falling suggest that the participants focused on mobilization, coordination and stretching exercises. Consistent with the literature, regular training also had a positive effect on body awareness, mood and self-esteem (64, 65).
4.8 Additional comments on the assessment of medium-term sustainability
Overall, HNC patients are a vulnerable cohort, which is reflected by the many disease-related training interruptions and the high health-related dropout during the study (at least 8 of 53 corresponds to >15%). To avoid bias in the assessment of the sustainability of the training intervention, only patients who had completed the FU measurement (n=38) were included in this analysis. Consequently, the observed moderate to large intervention effects (pre-post analysis, n=44) faded out (Table 2 vs. 4 and 3 vs. 5). This can be explained by the fact that the patients who completed the whole study (n=38) started with a better QoL (67 vs. 63, with (Q1 = 50, Q3 = 75) identical in both samples), lower symptom burden and better physical performance/functionality at the pre-intervention stage, than the cohort that only completed the pre-post measurements (n=44). Our results thus illustrate that the careful consideration of dropouts is important in longitudinal analyses, because dropouts can influence study results considerably, especially in small sized studies. Consequently, reported effects of exclusively short-term investigations should be interpreted at all times in its short-term context. And longer-term investigations should, at all measuring time points, include homogeneous samples. In future intervention studies, investigation ranges and study durations should be critically evaluated and discussed.
Since no significant changes were detectable between post- and FU measurements, one might conclude that observed short-term effects were maintained until the FU. However, it is to keep in mind, that in the case of a statistically significant short-term intervention effect with a subsequent medium-term effect (post-FU) of no significance, three true scenarios are possible here: a complete wash out of the short-term intervention effect (depending on time), a further increase, or, an equivalent situation. The letter two could be interpreted as sustainability of the obtained short-term effect and thus, a successful home-training intervention.
4.9 Safety
During the intervention, despite the high training volume, only a few adverse events occurred, none of which led to hospitalizations, long-term impairments, or damage. Consequently, in line with previous studies (44, 48, 61), home-based exercise training can be considered safe. However, it should be noted that HNC patients with clinically relevant comorbidities, including heart disease and severe chronic obstructive pulmonary disease, were excluded from study participation. To ensure safe training, the following recommendations are derived based on our approach: Firstly, exercise selection and intensity should be adapted to the existing limitations, comorbidities, and physical performance of the participants in accordance with current guidelines (43). Secondly, all exercises should be demonstrated and instructed by experienced therapists who can provide precise guidance on positioning and execution prior the training. Thirdly, for patients who are physically inactive or inexperienced, training volume and intensity should be increased gradually. We suspect that the reported pain, especially in the lower extremities (knees, Achilles tendon), is due to long endurance training sessions with sudden increases in intensity and could therefore be avoided.
4.10 Strengths and limitations
The OSHO#94 study ist he first study that evaluated the sustainability of a 100% home exercise program in addition to the effectiveness. Another strength is the high test specificity, particularly in assessing mobility and aerobic performance. However, the study design also has some limitations. In addition to the limitations already mentioned in the study protocol (30)— the single-arm design (lack of a control group), missing data on recruitment rates, and the use of the GSLTPAQ for assessing activity levels—the small sample size represents a relevant limitation. As a result, it was not possible to detect medium and small effects as statistically significant across three measurement time points, if there. And besides, we applied the Bonferroni correction as a conservative statistical method in multiple testing, knowing that our discernible set of study limitations makes conclusions much more difficult. Consequently, further well designed studies with a more appropriate primary outcome and larger sample sizes are needed to confirm our findings. Another limitation is the lack of an objective test for assessing muscle strength. A simple handgrip strength test could have provided additional information alongside changes in muscle mass. Despite these limitations, the results of the OSHO #94 trial demonstrate that an individualized home-based exercise program with low-to-moderate intensity is feasible, safe, and effective. The program, specifically designed for HNC patients, appears to be suitable for routine clinical care.
5 Conclusion and outlook
The individually adaptable home exercise program designed for HNC patients in aftercare proved to be safe and effective, particularly in terms of improving physical function. Additionally, positive changes were observed in body composition, along with an improvement in QoL. The high effectiveness was probably due to the consideration of three important training principles: The individualization/targeting of the training; progression, especially with regard to endurance training (increase in intensity); and the setting of effective training stimuli (49). Thus, the training program, including the chosen approach—knowledge transfer, free provision of training equipment, and remote support (for a certain period)— to be suitable for transferring the knowledge gained to date, primarily in randomized controlled trials, on the effectiveness of targeted exercise interventions in HNC patients (46, 47, 56, 66–70) into routine care. This could benefit HNC patients who have not previously had access to guided interventions, especially patients in rural areas. In addition, home training offers the advantage that the training can be adapted to the individual needs and preferences of the patients, is cost-effective and less time-consuming, which can potentially reduce barriers to participation in the training. Due to the specificity of functional diagnostics, particularly in mobility assessments and aerobic performance tests, even small effects could be detected. However, in our setting they could not be detected statistically significant. Studies with larger sample sizes and longer observation periods are necessary to determine whether less fit patients can achieve progress in their physical functioning beyond the supported phase.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: NFDI4Health repository: https://ldh.mediz-rostock.imise.uni-leipzig.de/projects/14.
Ethics statement
The studies involving humans were approved by Ethic Committee of the University of Rostock, Ethics Committee of the University of Halle-Wittenberg and University of Greifswald. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SF: Formal Analysis, Funding acquisition, Data curation, Project administration, Supervision, Investigation, Conceptualization, Writing – original draft. LB: Data curation, Investigation, Writing – review & editing. ÄG: Formal Analysis, Conceptualization, Writing – original draft. DS: Investigation, Writing – review & editing. JS: Investigation, Writing – review & editing. SS: Investigation, Writing – review & editing. MB: Investigation, Writing – review & editing. AS: Investigation, Writing – review & editing. JD: Data curation, Investigation, Writing – review & editing. UK: Investigation, Writing – review & editing. CG-T: Conceptualization, Investigation, Writing – review & editing. CJ: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was supported by the East German Study Group Hematology and Oncology (OSHO), file number OSHO #94.
Acknowledgments
We would like to thank the self-help network Kopf-Hals-M.U.N.D.-Krebs e. V. for promoting the study, and Michael Schroeder for his support in functional diagnostics and training planning at the Greifswald site.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1602532/full#supplementary-material.
References
1. Lo Nigro C, Denaro N, Merlotti A, and Merlano M. Head and neck cancer: improving outcomes with a multidisciplinary approach. Cancer Manag Res. (2017) 9:363–71. doi: 10.2147/CMAR.S115761
2. Ortiz-Comino L, Fernández-Lao C, Speksnijder CM, Lozano-Lozano M, Tovar-Martín I, Arroyo-Morales M, et al. Upper body motor function and swallowing impairments and its association in survivors of head and neck cancer: A cross-sectional study. PloS One. (2020) 15:e0234467. doi: 10.1371/journal.pone.0234467
3. Riechelmann H, Dejaco D, Steinbichler TB, Lettenbichler-Haug A, Anegg M, Ganswindt U, et al. Functional outcomes in head and neck cancer patients. Cancers (Basel). (2022) 14:1–19. doi: 10.3390/cancers14092135
4. van Hinte G, Leijendekkers RA, Merkx MAW, Takes RP, Nijhuis-van der Sanden MWG, and Speksnijder CM. Identifying unmet needs and limitations in physical health in survivors of Head and Neck Cancer. Eur J Cancer Care (Engl). (2021) 30:e13434. doi: 10.1111/ecc.13434
5. Baxi SS, Schwitzer E, and Jones LW. A review of weight loss and sarcopenia in patients with head and neck cancer treated with chemoradiation. Cancers Head Neck. (2016) 1:5. doi: 10.1186/s41199-016-0010-0
6. Ellis MA, Sterba KR, Brennan EA, Maurer S, Hill EG, Day TA, et al. A systematic review of patient-reported outcome measures assessing body image disturbance in patients with head and neck cancer. Otolaryngol Head Neck Surg. (2019) 160:941–54. doi: 10.1177/0194599819829018
7. Epstein JB, Robertson M, Emerton S, Phillips N, and Stevenson-Moore P. Quality of life and oral function in patients treated with radiation therapy for head and neck cancer. Head Neck. (2001) 23:389–98. doi: 10.1002/hed.v23:5
8. Langendijk JA, Doornaert P, Verdonck-de Leeuw IM, Leemans CR, Aaronson NK, and Slotman BJ. Impact of late treatment-related toxicity on quality of life among patients with head and neck cancer treated with radiotherapy. J Clin Oncol. (2008) 26:3770–6. doi: 10.1200/JCO.2007.14.6647
10. León X, Orús C, Casasayas M, Neumann E, Holgado A, and Quer M. Trends in disease-specific survival of head and neck squamous cell carcinoma patients treated in a single institution over a 30-year period. Oncol. (2021) 115:105184. doi: 10.1016/j.oraloncology.2021.105184
11. Ferris RL, Blumenschein G, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. (2016) 375:1856–67. doi: 10.1056/NEJMoa1602252
12. Ringash J, Bernstein LJ, Devins G, Dunphy C, Giuliani M, Martino R, et al. Head and neck cancer survivorship: learning the needs, meeting the needs. Semin Radiat Oncol. (2018) 28:64–74. doi: 10.1016/j.semradonc.2017.08.008
13. Margalit DN, Salz T, Venchiarutti R, Milley K, McNamara M, Chima S, et al. Interventions for head and neck cancer survivors: Systematic review. Head Neck. (2022) 44:2579–99. doi: 10.1002/hed.v44.11
14. Burgos-Mansilla B, Galiano-Castillo N, Lozano-Lozano M, Fernández-Lao C, Lopez-Garzon M, and Arroyo-Morales M. Effect of physical therapy modalities on quality of life of head and neck cancer survivors: A systematic review with meta-analysis. J Clin Med. (2021) 10:1–18. doi: 10.3390/jcm10204696
15. Pérez IMM, Pérez SEM, García RP, Lupgens D, Martínez GB, González CR, et al. Exercise-based rehabilitation on functionality and quality of life in head and neck cancer survivors. A systematic review and meta-analysis. Sci Rep. (2023) 13:8523. doi: 10.1038/s41598-023-35503-y
16. Avancini A, Borsati A, Belluomini L, Giannarelli D, Nocini R, Insolda J, et al. Effect of exercise across the head and neck cancer continuum: a systematic review of randomized controlled trials. Support Care Cancer. (2023) 31:670. doi: 10.1007/s00520-023-08126-2
17. Bye A, Sandmael JA, Stene GB, Thorsen L, Balstad TR, Solheim TS, et al. Exercise and nutrition interventions in patients with head and neck cancer during curative treatment: A systematic review and meta-analysis. Nutrients. (2020) 12:1–24. doi: 10.3390/nu12113233
18. Capozzi LC, Nishimura KC, McNeely ML, Lau H, and Culos-Reed SN. The impact of physical activity on health-related fitness and quality of life for patients with head and neck cancer: a systematic review. Br J Sports Med. (2016) 50:325–38. doi: 10.1136/bjsports-2015-094684
19. Goyal N, Day A, Epstein J, Goodman J, Graboyes E, Jalisi S, et al. Head and neck cancer survivorship consensus statement from the American Head and Neck Society. Laryngoscope Invest Otolaryngol. (2022) 7:70–92. doi: 10.1002/lio2.v7.1
20. Fang Y-Y, Wang C-P, Chen Y-J, Lou P-J, Ko J-Y, Lin J-J, et al. Physical activity and fitness in survivors of head and neck cancer. Support Care Cancer. (2021) 29:6807–17. doi: 10.1007/s00520-021-06192-y
21. Karczewska-Lindinger M, Tuomi L, Fridolfsson J, Arvidsson D, Börjesson M, and Finizia C. Low physical activity in patients diagnosed with head and neck cancer. Laryngoscope Invest Otolaryngol. (2021) 6:747–55. doi: 10.1002/lio2.v6.4
22. Felser S, Grosse-Thie C, Rogahn J, Koch T, Strueder D, Busch CJ, et al. Accelerometer based physical activity in patients with head and neck cancer. Jahrestagung der DGEpi: DGEpi, University Ulm (2022) p. 298, Abstract Book 17.
23. Ning Y, Wang Q, Ding Y, Zhao W, Jia Z, and Wang B. Barriers and facilitators to physical activity participation in patients with head and neck cancer: a scoping review. Support Care Cancer. (2022) 30:4591–601. doi: 10.1007/s00520-022-06812-1
24. Doughty HC, Hill RA, Riley A, Midgley AW, Patterson JM, Boddy LM, et al. Barriers to and facilitators of physical activity in adults living with and beyond cancer, with special emphasis on head and neck cancer: a systematic review of qualitative and mixed methods studies. Support Care Cancer. (2023) 31:471. doi: 10.1007/s00520-023-07925-x
25. Midgley AW, Lowe D, Levy AR, Mepani V, and Rogers SN. Exercise program design considerations for head and neck cancer survivors. Eur Arch oto-rhino-laryngology. (2018) 275:169–79. doi: 10.1007/s00405-017-4760-z
26. Rogers LQ, Malone J, Rao K, Courneya KS, Fogleman A, Tippey A, et al. Exercise preferences among patients with head and neck cancer: prevalence and associations with quality of life, symptom severity, depression, and rural residence. Head Neck. (2009) 31:994–1005. doi: 10.1002/hed.21053
27. Jackson C, Dowd AJ, Capozzi LC, Bridel W, Lau HY, and Culos-Reed SN. A turning point: Head and neck cancer patients’ exercise preferences and barriers before and after participation in an exercise intervention. Eur J Cancer Care (Engl). (2018) 27:e12826. doi: 10.1111/ecc.2018.27.issue-2
28. Felser S, Behrens M, Strüder D, Liese J, Rohde K, Junghanss C, et al. Feasibility and effects of a supervised exercise program suitable for independent training at home on physical function and quality of life in head and neck cancer patients: A pilot study. Integr Cancer Ther. (2020) 19:1–12. doi: 10.1177/1534735420918935
30. Felser S, Rogahn J, Glass Ä, Bonke LA, Strüder DF, Stolle J, et al. Feasibility of individualized home exercise programs for patients with head and neck cancer–study protocol and first results of a multicentre single-arm intervention trial (OSHO 94). PloS One. (2024) 19:1–18. doi: 10.1371/journal.pone.0301304
31. Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. (1982) 14:377–81. doi: 10.1249/00005768-198205000-00012
32. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. (1993) 85:365–76. doi: 10.1093/jnci/85.5.365
33. Bjordal K, de Graeff A, Fayers PM, Hammerlid E, van Pottelsberghe C, Curran D, et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. Eur J Cancer. (2000) 36:1796–807. doi: 10.1016/S0959-8049(00)00186-6
34. Amireault S and Godin G. The Godin-Shephard leisure-time physical activity questionnaire: validity evidence supporting its use for classifying healthy adults into active and insufficiently active categories. Percept Mot Skills. (2015) 120:604–22. doi: 10.2466/03.27.PMS.120v19x7
35. Amireault S, Godin G, Lacombe J, and Sabiston CM. The use of the Godin-Shephard Leisure-Time Physical Activity Questionnaire in oncology research: a systematic review. BMC Med Res Methodol. (2015) 15:60. doi: 10.1186/s12874-015-0045-7
36. Holt LE, Pelham TW, and Burke DG. Modifications to the standard sit-and-reach flexibility protocol. J Athl Train. (1999) 34:43–7.
37. Guralnik JM, Ferrucci L, Pieper CF, Leveille SG, Markides KS, Ostir GV, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci. (2000) 55:M221–31. doi: 10.1093/gerona/55.4.M221
38. Schmidt K, Vogt L, Thiel C, Jäger E, and Banzer W. Validity of the six-minute walk test in cancer patients. Int J Sports Med. (2013) 34:631–6. doi: 10.1055/s-0032-1323746
39. Borg E, Borg G, Larsson K, Letzter M, and Sundblad B-M. An index for breathlessness and leg fatigue. Scand J Med Sci Sports. (2010) 20:644–50. doi: 10.1111/j.1600-0838.2009.00985.x
40. Sullivan GM and Feinn R. Using effect size-or why the P value is not enough. J Grad Med Educ. (2012) 4:279–82. doi: 10.4300/JGME-D-12-00156.1
41. Cohen J. Statistical power analysis for the behavioral sciences. 2. Hillsdale, NJ: Erlbaum (1988).
42. Midgley AW, Levy AR, Price R, Cunha FA, and Rogers SN. Should survivors of head and neck cancer be considered a distinct special population within the context of exercise prescription? Br J Maxillofac Surg. (2020) 58:738–43. doi: 10.1016/j.bjoms.2020.03.021
43. Campbell KL, Winters-Stone KM, Wiskemann J, May AM, Schwartz AL, Courneya KS, et al. Exercise guidelines for cancer survivors: consensus statement from international multidisciplinary roundtable. Med Sci Sports Exerc. (2019) 51:2375–90. doi: 10.1249/MSS.0000000000002116
44. Cnossen IC, van Uden-Kraan CF, Rinkel RNPM, Aalders IJ, de Goede CJT, de Bree R, et al. Multimodal guided self-help exercise program to prevent speech, swallowing, and shoulder problems among head and neck cancer patients: a feasibility study. J Med Internet Res. (2014) 16:e74. doi: 10.2196/jmir.2990
45. Capozzi LC, Boldt KR, Lau H, Shirt L, Bultz B, and Culos-Reed SN. A clinic-supported group exercise program for head and neck cancer survivors: managing cancer and treatment side effects to improve quality of life. Sports Med. (2015) 23:1001–7. doi: 10.1007/s00520-014-2436-4
46. McNeely ML, Parliament M, Courneya KS, Seikaly H, Jha N, Scrimger R, et al. A pilot study of a randomized controlled trial to evaluate the effects of progressive resistance exercise training on shoulder dysfunction caused by spinal accessory neurapraxia/neurectomy in head and neck cancer survivors. Head Neck. (2004) 26:518–30. doi: 10.1002/hed.20010
47. McNeely ML, Parliament MB, Seikaly H, Jha N, Magee DJ, Haykowsky MJ, et al. Effect of exercise on upper extremity pain and dysfunction in head and neck cancer survivors: a randomized controlled trial. Cancer. (2008) 113:214–22. doi: 10.1002/cncr.v113:1
48. Kok A, Passchier E, May AM, van den Brekel MWM, Jager-Wittenaar H, Veenhof C, et al. Feasibility of a supervised and home-based tailored exercise intervention in head and neck cancer patients during chemoradiotherapy. Eur J Cancer Care (Engl). (2022) 31:e13662. doi: 10.1111/ecc.13662
49. Ferrauti A ed. Trainingswissenschaft für die Sportpraxis: Lehrbuch für Studium, Ausbildung und Unterricht im Sport. Berlin, Heidelberg: Springer Spektrum (2020). doi: 10.1007/978-3-662-58227-5
50. O’Neill LM, Guinan E, Doyle SL, Bennett AE, Murphy C, Elliott JA, et al. The RESTORE randomized controlled trial: impact of a multidisciplinary rehabilitative program on cardiorespiratory fitness in esophagogastric cancer survivorship. Ann Surg. (2018) 268:747–55. doi: 10.1097/SLA.0000000000002895
51. Strüder D, Ebert J, Kalle F, Schraven SP, Eichhorst L, Mlynski R, et al. Head and neck cancer: A study on the complex relationship between qoL and swallowing function. Curr Oncol. (2023) 30:10336–50. doi: 10.3390/curroncol30120753
52. Cocks K, King MT, Velikova G, Fayers PM, and Brown JM. Quality, interpretation and presentation of European Organisation for Research and Treatment of Cancer quality of life questionnaire core 30 data in randomised controlled trials. Eur J Cancer. (2008) 44:1793–8. doi: 10.1016/j.ejca.2008.05.008
53. Mouelhi Y, Jouve E, Castelli C, and Gentile S. How is the minimal clinically important difference established in health-related quality of life instruments? Review of anchors and methods. Health Qual Life Outcomes. (2020) 18:136. doi: 10.1186/s12955-020-01344-w
54. World Health Organization Quality of Life. What quality of life? The WHOQOL Group. World Health Organization Quality of Life Assessment. World Health Forum. (1996) 17:354–6.
55. Shephard RJ and Aoyagi Y. Seasonal variations in physical activity and implications for human health. Eur J Appl Physiol. (2009) 107:251–71. doi: 10.1007/s00421-009-1127-1
56. Lønbro S, Dalgas U, Primdahl H, Johansen J, Nielsen JL, Aagaard P, et al. Progressive resistance training rebuilds lean body mass in head and neck cancer patients after radiotherapy–results from the randomized DAHANCA 25B trial. Radiother Oncol. (2013) 108:314–9. doi: 10.1016/j.radonc.2013.07.002
57. Dijkstra PU, Huisman PM, and Roodenburg JLN. Criteria for trismus in head and neck oncology. Int J Maxillofac Surg. (2006) 35:337–42. doi: 10.1016/j.ijom.2005.08.001
58. Deutsche Gesellschaft für Funktionsdiagnostik und -therapie (DGFDT). CMD-screening (CMD-basisdiagnostik) (2024). Available online at: https://www.dgfdt.de/documents/266840/22655647/CMD-Screening+DGFDT+2024/ac5abfe4-604d-4c84-9851-e426a54edc91 (Accessed March 5, 2025).
59. Moser N. Körperliche Leistungsfähigkeit gemessen anhand der Sechs-Minuten-Gehstrecke in der Normalbevölkerung – Determinanten, Referenzperzentile und Zusammenhang mit der selbstberichteten körperlichen Leistungsfähigkeit und Gesundheit in der populationsbasierten STAAB Kohortenstudie. Würzburg: Inauguraldissertation: Julius-Maximilians-Universität Würzburg (2022). doi: 10.25972/OPUS-32958
60. But-Hadzic J, Dervisevic M, Karpljuk D, Videmsek M, Dervisevic E, Paravlic A, et al. Six-minute walk distance in breast cancer survivors-A systematic review with meta-analysis. Int J Environ Res Public Health. (2021) 18:1–13. doi: 10.3390/ijerph18052591
61. Eades M, Murphy J, Carney S, Amdouni S, Lemoignan J, Jelowicki M, et al. Effect of an interdisciplinary rehabilitation program on quality of life in patients with head and neck cancer: review of clinical experience. Head Neck. (2013) 35:343–9. doi: 10.1002/hed.22972
62. Redelmeier DA, Bayoumi AM, Goldstein RS, and Guyatt GH. Interpreting small differences in functional status: the Six Minute Walk test in chronic lung disease patients. Am J Respir Crit Care Med. (1997) 155:1278–82. doi: 10.1164/ajrccm.155.4.9105067
63. Wise RA and Brown CD. Minimal clinically important differences in the six-minute walk test and the incremental shuttle walking test. COPD. (2005) 2:125–9. doi: 10.1081/COPD-200050527
64. Tikac G, Unal A, and Altug F. Regular exercise improves the levels of self-efficacy, self-esteem and body awareness of young adults. J Sports Med Phys Fitness. (2022) 62:157–61. doi: 10.23736/S0022-4707.21.12143-7
65. Mikkelsen K, Stojanovska L, Polenakovic M, Bosevski M, and Apostolopoulos V. Exercise and mental health. Maturitas. (2017) 106:48–56. doi: 10.1016/j.maturitas.2017.09.003
66. Capozzi LC, McNeely ML, Lau HY, Reimer RA, Giese-Davis J, Fung TS, et al. Patient-reported outcomes, body composition, and nutrition status in patients with head and neck cancer: Results from an exploratory randomized controlled exercise trial. Cancer. (2016) 122:1185–200. doi: 10.1002/cncr.v122.8
67. Hong Y-L, Hsieh T-C, Chen P-R, and Chang S-C. Nurse-led counseling intervention of postoperative home-based exercise training improves shoulder pain, shoulder disability, and quality of life in newly diagnosed head and neck cancer patients. J Clin Med. (2022) 11:1–12. doi: 10.3390/jcm11144032
68. McGarvey AC, Hoffman GR, Osmotherly PG, and Chiarelli PE. Maximizing shoulder function after accessory nerve injury and neck dissection surgery: A multicenter randomized controlled trial. Head Neck. (2015) 37:1022–31. doi: 10.1002/hed.23712
69. Su T-L, Chen A-N, Leong C-P, Huang Y-C, Chiang C-W, Chen I-H, et al. The effect of home-based program and outpatient physical therapy in patients with head and neck cancer: A randomized, controlled trial. Oncol. (2017) 74:130–4. doi: 10.1016/j.oraloncology.2017.10.002
70. Thomas A, D’Silva C, Mohandas L, Pais SMJ, and Samuel SR. Effect of muscle energy techniques V/S active range of motion exercises on shoulder function post modified radical neck dissection in patients with head and neck cancer - A randomized clinical trial. Asian Pac J Cancer Prev. (2020) 21:2389–93. doi: 10.31557/APJCP.2020.21.8.2389
Keywords: EORTC QLQ-C30 (version 3), EORTC QLQ-HN35, head and neck cancer, Health-related quality of life (QOL), home-based exercise, physical functionality, physical activity (exercise)
Citation: Felser S, Bonke LA, Glass Ä, Strüder D, Stolle J, Schulze S, Blaurock M, Steinmetz A, Daunheimer J, Kriesen U, Grosse-Thie C and Junghanss C (2025) Individualized home training in head and neck cancer patients is safe and has positive short- and medium-term effects –results of a multicenter, single-arm intervention trial (OSHO #94). Front. Oncol. 15:1602532. doi: 10.3389/fonc.2025.1602532
Received: 29 March 2025; Accepted: 21 May 2025;
Published: 09 June 2025.
Edited by:
Oreste Iocca, University of Turin, ItalyReviewed by:
Jessica Maldonado-Mendoza, Metropolitan Autonomous University, MexicoKazuhito Suzuki, Jikei University Hospital, Japan
Copyright © 2025 Felser, Bonke, Glass, Strüder, Stolle, Schulze, Blaurock, Steinmetz, Daunheimer, Kriesen, Grosse-Thie and Junghanss. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabine Felser, c2FiaW5lLmZlbHNlckBtZWQudW5pLXJvc3RvY2suZGU=