 Maria T. Bourlon1,2†
Maria T. Bourlon1,2† Luca Galli3†
Luca Galli3† Enrique Grande4
Enrique Grande4 Se Hoon Park5
Se Hoon Park5 Bohuslav Melichar6
Bohuslav Melichar6 Timothy J. Schieber7Maria José Juan-Fita8
Timothy J. Schieber7Maria José Juan-Fita8 Yüksel Ürün9
Yüksel Ürün9 Javier Molina-Cerrillo10Teresa Alonso-Gordoa10
Javier Molina-Cerrillo10Teresa Alonso-Gordoa10 Ugo De Giorgi11
Ugo De Giorgi11 Jakub Kucharz12Esther Pérez Calabuig13
Jakub Kucharz12Esther Pérez Calabuig13 Vincenza Conteduca14
Vincenza Conteduca14 Tarek Taha15,16
Tarek Taha15,16 Pasquale Rescigno17Hussam Abu-Sini18
Pasquale Rescigno17Hussam Abu-Sini18 Gian Paolo Spinelli19
Gian Paolo Spinelli19 Ray Manneh Kopp20Alessia Salfi3Dipen Bhuva21
Ray Manneh Kopp20Alessia Salfi3Dipen Bhuva21 Paola Valdez-Sandoval1
Paola Valdez-Sandoval1 Sofia Mendez-Bribiesca1
Sofia Mendez-Bribiesca1 Ondrej Fiala22,23
Ondrej Fiala22,23 Sebastiano Buti24,25
Sebastiano Buti24,25 Fernando Sabino Marques Monteiro26,27
Fernando Sabino Marques Monteiro26,27 Aristotelis Bamias28
Aristotelis Bamias28 Marwan Ghosn29
Marwan Ghosn29 Francesco Massari30,31
Francesco Massari30,31 Jawaher Ansari32‡
Jawaher Ansari32‡ Matteo Santoni33*‡
Matteo Santoni33*‡- 1Department of Hemato-Oncology, Instituto Nacional de Ciencias Medicas y Nutricion Salvador Zubiran, Mexico City, Mexico
- 2Escuela de Medicina, Universidad Panamericana, Mexico City, Mexico
- 3Oncology Unit 2, University Hospital of Pisa, Pisa, Italy
- 4Department of Medical Oncology, MD Anderson Cancer Center Madrid, Madrid, Spain
- 5Department of Hematology-Oncology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
- 6Department of Oncology, Faculty of Medicine and Dentistry, Palacký University, Olomouc, Czechia
- 7Division of Medical Oncology, Department of Internal Medicine, University of Kansas Cancer Center, Westwood, KS, United States
- 8Department of Medical Oncology, Fundacion Instituto Valenciano de Oncologia, Valencia, Spain
- 9Department of Medical Oncology, Ankara University Faculty of Medicine, Ankara, Türkiye
- 10Department of Medical Oncology, Hospital Ramón y Cajal, Madrid, Spain
- 11Department of Medical Oncology, IRCCS Istituto Romagnolo per lo Studio dei Tumori (IRST) “Dino Amadori”, Meldola, Italy
- 12Department of Uro-Oncology, Maria Sklodowska-Curie National Research Institute of Oncology Warsaw, Warsaw, Poland
- 13Medical Oncology Department, CHU Insular-Materno Infantil, Las Palmas de Gran Canaria, Spain
- 14Unit of Medical Oncology and Biomolecular Therapy and C.R.E.A.T.E - Center for Research and Innovation Medicine, Department of Medical and Surgical Sciences, University of Foggia, Policlinico Riuniti, Foggia, Italy
- 15The Institute of Cancer Research, London, United Kingdom
- 16Royal Marsden NHS Foundation Trust, London, United Kingdom
- 17Translational and Clinical Research Institute, Centre for Cancer, Newcastle University, Newcastle upon Tyne, United Kingdom
- 18Oncology Institute, Haifa, Israel
- 19UOC Oncologia Territoriale Ausl Latina, Aprilia, Italy
- 20Clinical Oncology, Sociedad de Oncología y Hematología del Cesar, Valledupar, Colombia
- 21Department of Medical Oncology, Army Hospital Research and Referral, New Delhi, India
- 22Department of Oncology and Radiotherapeutics, Faculty of Medicine and University Hospital in Pilsen, Charles University, Pilsen, Czechia
- 23Biomedical Center, Faculty of Medicine in Pilsen, Charles University, Pilsen, Czechia
- 24Medical Oncology Unit, University Hospital of Parma, Parma, Italy
- 25Department of Medicine and Surgery, University of Parma, Parma, Italy
- 26Genitourinary Cancer Group, Latin American Cooperative Oncology Group - LACOG, Porto Alegre, Brazil
- 27Oncology and Hematology Department, Hospital Sírio Libanês, Brasília, Brazil
- 282nd Propaedeutic Department of Internal Medicine, ATTIKON University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece
- 29Hematology-Oncology Department, Faculty of Medicine, Saint Joseph University of Beirut, Beirut, Lebanon
- 30Medical Oncology, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy
- 31Department of Medical and Surgical Sciences (DIMEC), University of Bologna, Bologna, Italy
- 32Medical Oncology, Tawam Hospital, Al Ain, United Arab Emirates
- 33Medical Oncology Unit, Macerata Hospital, Macerata, Italy
Introduction: Four approved immune-based combinations for untreated metastatic renal carcinoma have demonstrated survival benefits. The ARON-1 study (NCT05287464) analyzed real-world data of patients with metastatic renal cell carcinoma receiving first-line immuno-oncology combinations. This sub-analysis is focused on the nivolumab plus cabozantinib effectiveness.
Methods: We conducted a retrospective study across 52 centers in 17 countries, including patients with metastatic renal carcinoma treated with first-line nivolumab plus cabozantinib, regardless of histologic characteristics, performance status, or risk by IMDC prognostic model. Patients with incomplete medical data were excluded. The primary objective of this sub-analysis of the ARON-1 study was to evaluate the real-world effectiveness and safety.
Results: A total of 333 patients were treated with nivolumab plus cabozantinib, clinical characteristics included ECOG performance status ≥2 20%, non-clear cell histology 16%, sarcomatoid de-differentiation 12%, and poor-risk by IMDC 28%. At a median follow-up of 15.9 months (95%CI 11.2-44.0), the median overall survival was not reached (40.0–NR), the probability of survival at 2 years was 75%, while median progression free survival was 33.7 months (95%CI 21.1-38.9). In the entire cohort, an objective response was observed in 58%, with 6% complete responses, and a median duration of response of 38.9 months (95%CI 33.7–NR). At multivariate analysis, adverse prognostic factors for overall survival included ECOG performance status ≥2, sarcomatoid de-differentiation, brain and bone metastases, and poor IMDC group. In the safety analysis, the incidence of grade 3 or higher toxicity was 37%, with hypertension and hand-foot syndrome being the most frequent adverse events.
Conclusion: The findings in the present real-world study reaffirm the clinical benefits and safety of the nivolumab plus cabozantinib combination across all subgroups, including populations that are generally excluded from clinical trials for whom data is often missing. Poor performance status, sarcomatoid de-differentiation, bone or central nervous system metastases and IMDC poor risk group were confirmed as negative prognostic factors.
1 Introduction
The introduction of immune-based combination therapies, with either two immune checkpoint inhibitors (ICI) or combinations of ICI with vascular endothelial growth factor receptor tyrosine kinase inhibitor (VEGFR-TKI), has dramatically changed the treatment landscape and prognosis for patients with advanced renal cell carcinoma (RCC). All these regimens, including nivolumab plus ipilimumab, pembrolizumab plus axitinib, nivolumab plus cabozantinib, and pembrolizumab plus lenvatinib, have demonstrated significant survival benefits compared to the prior standard (1–8).
The CheckMate 9ER trial demonstrated that nivolumab plus cabozantinib compared to sunitinib significantly improved the overall survival (OS) of mRCC patients by reducing the risk of death by approximately 40%; as well as improving the median progression-free survival (PFS, 16.6 vs 8.3 months) and the overall response rate (ORR, 55% vs 27%), while maintaining a manageable toxicity profile (5, 6).
Real-world data represent a way to integrate the results from phase 3 trials, focusing on subpopulations often not included in clinical trials and allowing for hypothesis generating head-to-head comparisons. It also allows clinicians to assess less frequent or late-onset toxicities.
In this context, the ARON-1 study (NCT05287464, www.aronwg.com) aimed to analyze real-world treatment outcomes for mRCC patients across multiple centers worldwide. In this report, we present a retrospective multicenter analysis of the outcomes of mRCC patients receiving first-line nivolumab plus cabozantinib in 17 countries across Europe, Asia, and North and South America.
2 Materials and methods
2.1 Study population
We conducted a retrospective data collection from patients aged 18 years or older who had a histologically confirmed diagnosis of RCC, and metastatic disease either histologically or radiologically confirmed. Data were gathered from patients with mRCC treated with first-line nivolumab plus cabozantinib between January 1, 2021, and September 1, 2024, across 52 centers in 17 countries.
Nivolumab was typically administered intravenously at a dose of 240 mg every 2 weeks or 480 mg every 4 weeks, while cabozantinib was given orally once daily, with starting doses ranging from 20 mg to 40 mg based on physician choice and patient tolerance. First-line treatment continued until there was evidence of clinical or radiological progression, intolerable toxicities, clinical judgement or patient preference or death. Imaging studies, including contrast-enhanced CT or MRI scans, were performed according to local protocols every 8 or 12 weeks. Physical exams and laboratory tests were conducted every 4 to 6 weeks throughout treatment according to local protocols.
For each patient, retrospective data were collected from patient charts (electronic or paper), including details on age, sex, histology, IMDC risk group, nephrectomy status, metastasis sites, treatment-related adverse events, oncological outcomes, and subsequent treatments after first-line therapy. Patients with insufficient data for tumor assessment or those lost to follow-up were excluded from the analysis.
2.2 Study endpoints
The primary objective of this sub-analysis of the ARON-1 study was to evaluate the real-world activity, effectiveness, and safety of first-line nivolumab plus cabozantinib in mRCC patients. Tumor response was assessed using RECIST 1.1 (9), categorizing outcomes as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). The ORR was defined as the proportion of patients achieving a CR or a PR according to RECIST 1.1 (9).
OS was defined as the time from the initiation of first-line treatment to death from any cause, while PFS was the time from the start of treatment to disease progression or death from any cause. Duration of response (DOR) was defined as the time from the start of nivolumab plus cabozantinib to progression or death in patients who achieved CR or PR, whichever occurred first.
Landmark analysis was performed designating 6 and 12 months as the time point during follow-up period to reduce potential biases related to the follow-up time.
Adverse events retrospectively collected from patient charts were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0. Patients without tumor progression, those who moved to subsequent lines of treatment, or those lost to follow-up at the time of analysis were censored at their last available follow-up.
2.3 Statistical analysis
Statistical analysis was conducted using MedCalc software (version 19.6.4, MedCalc Software, Broekstraat 52, 9030 Mariakerke, Belgium). Descriptive statistics were used to summarize the characteristics of the study population. Survival outcomes, including OS, PFS, and DOR, were analyzed using the Kaplan-Meier method, with 95% confidence intervals (95% CI) calculated according to Rothman. The median follow-up was calculated using the reverse Kaplan-Meier estimator. Differences in survival distributions were assessed using the log-rank test.
Univariate and multivariate analyses were carried out using Cox proportional hazards models, with hazard ratios (HR) and corresponding 95% CI reported. Fisher’s exact test was used for pairwise comparisons of categorical variables, and chi-square tests were applied for multiple categorical comparisons. P-values of less than 0.05 were considered statistically significant. A significance threshold of p<0.05 was set for all tests, and all p-values were two-sided.
2.4 Ethics approval
The ARON-1 project received approval from the Ethics Committee of the Marche Region (2021-492) and from the Institutional Review Boards of all participating centers according to the regulations in force in each Country. The study was carried out in compliance with Good Clinical Practice and international ethical standards for biomedical research. The study protocol was developed in accordance with the ethical principles outlined in the Declaration of Helsinki regarding human research.
3 Results
3.1 Patient population
Three hundred and thirty-three patients treated with first-line cabozantinib plus nivolumab were selected among the 4977 patients from the ARON-1 dataset (Supplementary Figure S1). The median age was 63 years (range 38–86); 241 patients (72%) were males and 92 females (28%).
In 276 patients (82%) tumor histology was clear cell RCC. In those with non-clear cell histology (57 patients), papillary histology was seen in 42 patients (13%), cromophobe in 5 patients (2%), and 10 patients had other non-clear cell histologies (3%). Sarcomatoid de-differentiation was observed in 40 patients (12%). Two hundred patients (60%) underwent nephrectomy.
Lungs (60%) and distant lymph nodes (49%) were the most common metastatic sites, with 216 patients (65%) having more than 2 affected sites. The distribution of patients according to the International mRCC Database Consortium (IMDC) criteria was good, intermediate and poor risk in 59 (18%), 180 (54%) and 94 patients (28%), respectively. Table 1 describes the characteristics of the study population.
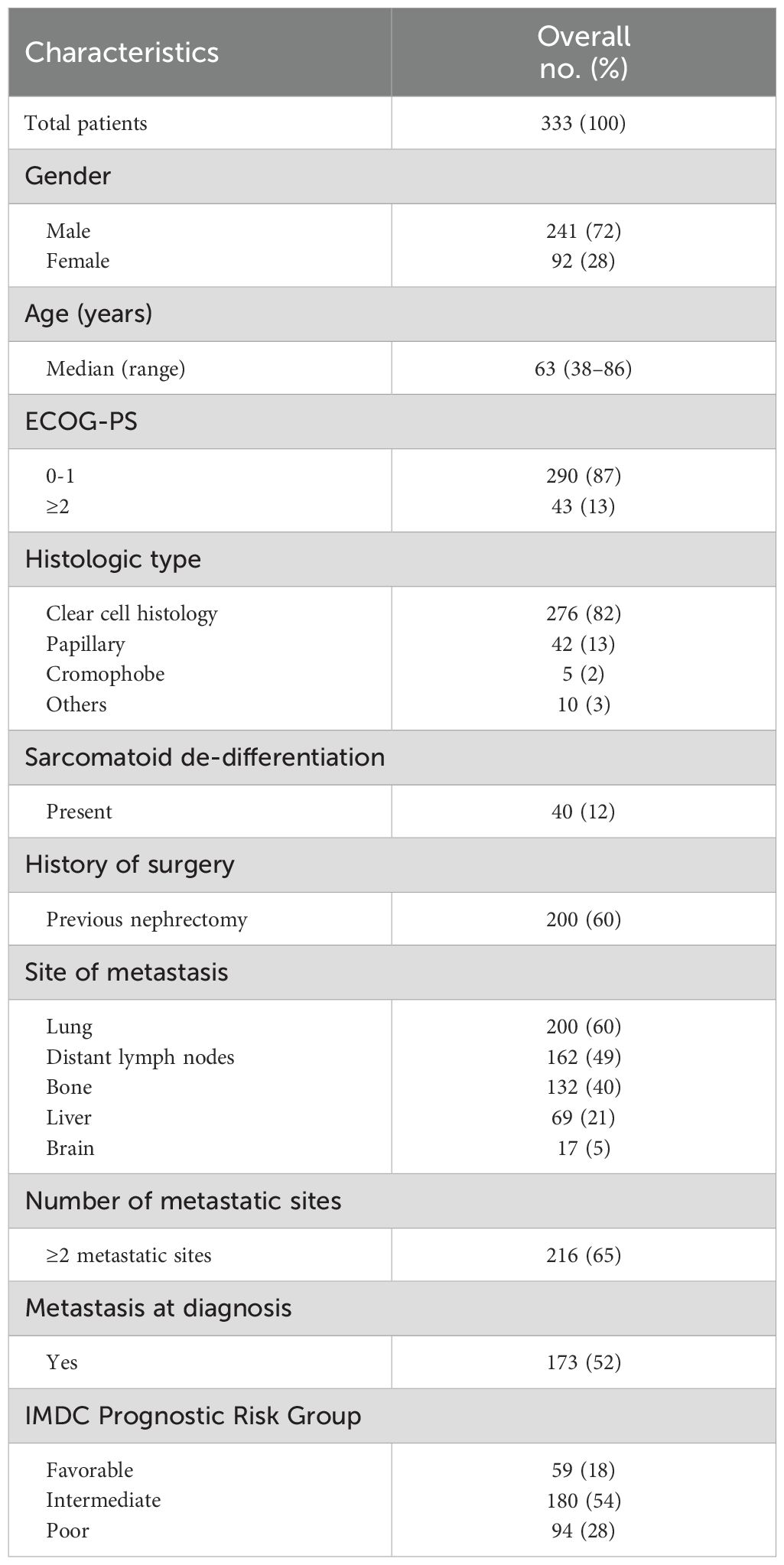
Table 1. Patient characteristics.
3.2 Overall survival analysis
The median follow-up time was 15.9 months (95% CI 11.2–44.0). The median OS in the overall study population was not reached (NR, 95% CI 40.0–NR, Figure 1), with a 2-year OS rate of 75%. In the 6- and 12-month OS landmark analyses, the median OS was NR (Supplementary Figure S2).
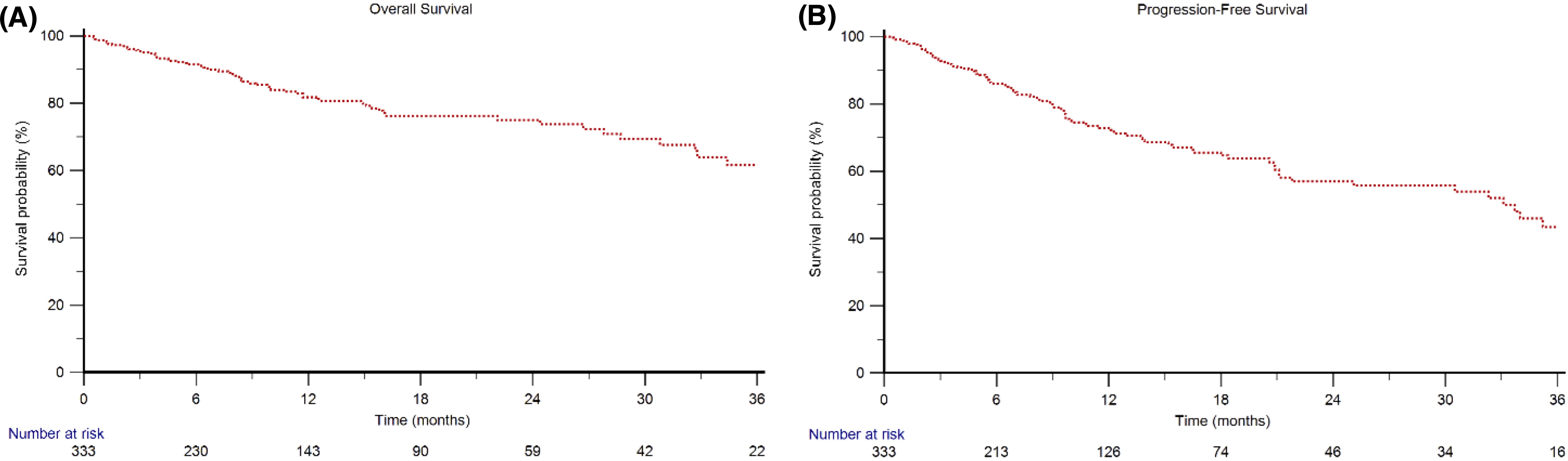
Figure 1. Overall Survival (A) and Progression-Free Survival (B) in mRCC patients treated with first-line nivolumab plus cabozantinib.
Survival analysis was made in different subgroups. The median OS was NR in both patients aged <70 years and ≥70 years, 2-year OS rates were 80% vs 74% (p=0.401). The median OS was NR in both males and females (p=0.578), with a 2y-OS rate of 77% vs 69% (p=0.265).
Median OS in the overall study population stratified by ECOG performance status (PS) was NR in patients with ECOG PS=0–1 and 8.4 months (95% CI 4.5–30.8) in patients with ECOG PS ≥2 (p<0.001, Figure 2), with a 2 year-OS rate of 82% vs 23% (p<0.001).
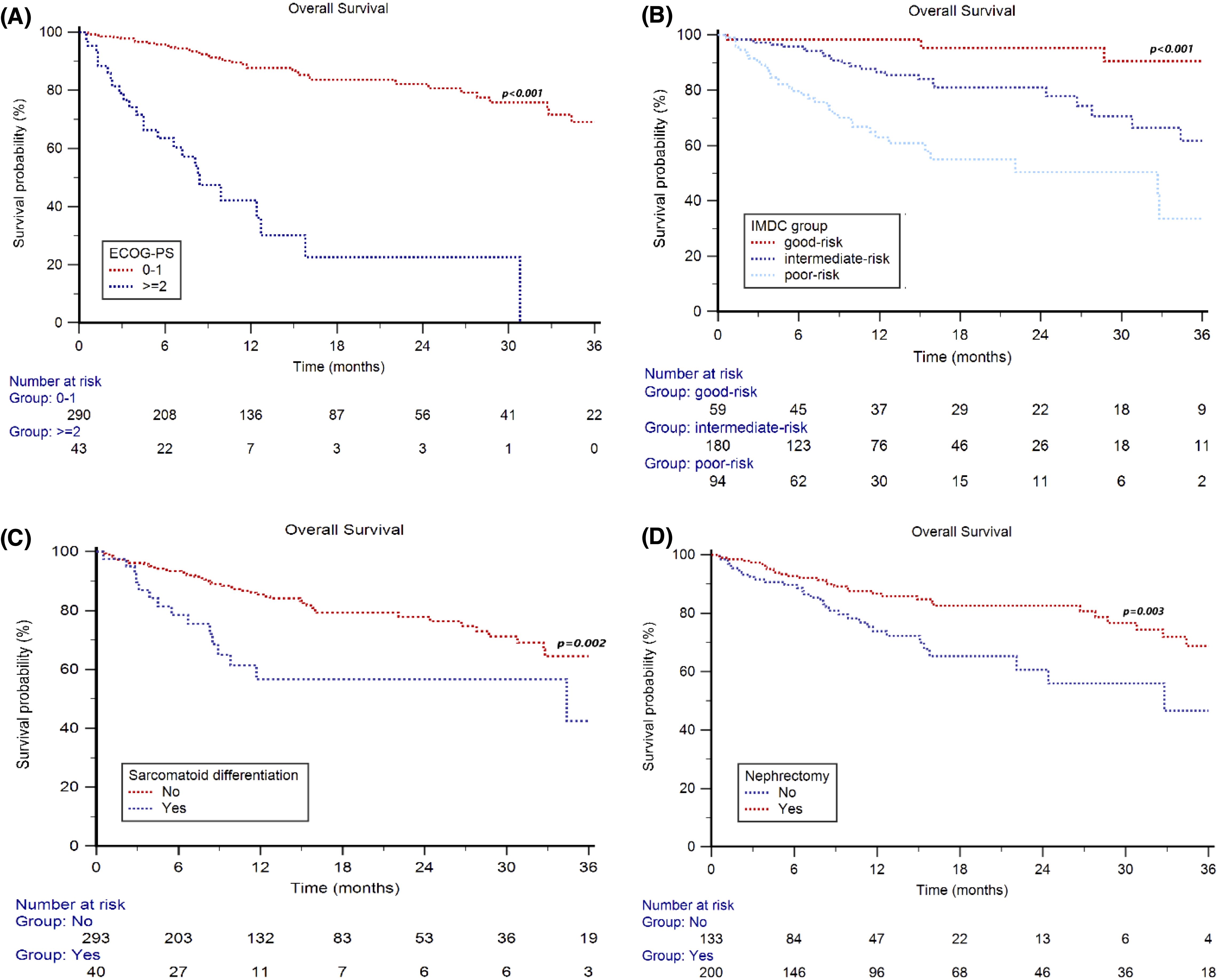
Figure 2. Overall Survival in mRCC patients treated with first-line nivolumab plus cabozantinib stratified by ECOG Performance Status (0–1 vs ≥2) (A), IMDC group (good vs intermediate vs poor-risk) (B), sarcomatoid differentiation (no vs yes) (C) and nephrectomy (no vs yes) (D).
By stratifying patients based on IMDC group, the median OS was NR in all the three prognostic groups (p<0.001, Figure 2), with a 2y-OS rate of 95%, 81% and 50% (p<0.001) in good-, intermediate- and poor-risk patients, respectively.
Regarding tumor histology, the median OS was NR in patients with clear cell RCC, while it was 27.8 months (95%CI 15.4–36.5) in patients with non-clear cell histologies (p=0.784), with a 2y-OS rate of 76% vs 64%, respectively (p=0.089).
Furthermore, the median OS was NR in both patients with and without sarcomatoid de-differentiation (p<0.001, Figure 2), with a 2y-OS rate of 57% vs 78% (p=0.002), respectively.
The median OS was NR in patients who underwent nephrectomy and was 32.8 months (95%CI 22.1–36.9) in subjects who did not have a nephrectomy (p<0.001, Figure 2), with a 2 year-OS rate of 83% vs 61% (p<0.001), respectively.
After stratifying the patients by metastatic sites, the median OS was NR in both patients with <2 and ≥2 metastatic sites (p=0.007, Figure 3), with a 2y-OS rate of 87% vs 68% (p=0.002). The median OS was NR in patients with or without metastases to the lungs (p=0.245, 2y-OS rate 76% vs 74%, p=0.747) or to distant lymph nodes (p=0.073, 2y-OS rate = 81% vs 69%, p=0.072), while significant differences were observed between patients with or without metastases to the bone (32.7 months, 95%CI 22.1–40.0 vs NR, p<0.001, Figure 3; 2y-OS rate = 60% vs 84%, p<0.001), liver (32.5 months, 95%CI 22.1–44.0 vs NR, p=0.009, Figure 3; 2y-OS rate = 60% vs 79%, p=0.005) or brain metastases (11.7 months, 95%CI 3.5–30.8 vs NR, p<0.001, Figure 3; 2y-OS rate = 35% vs 77%, p<0.001).
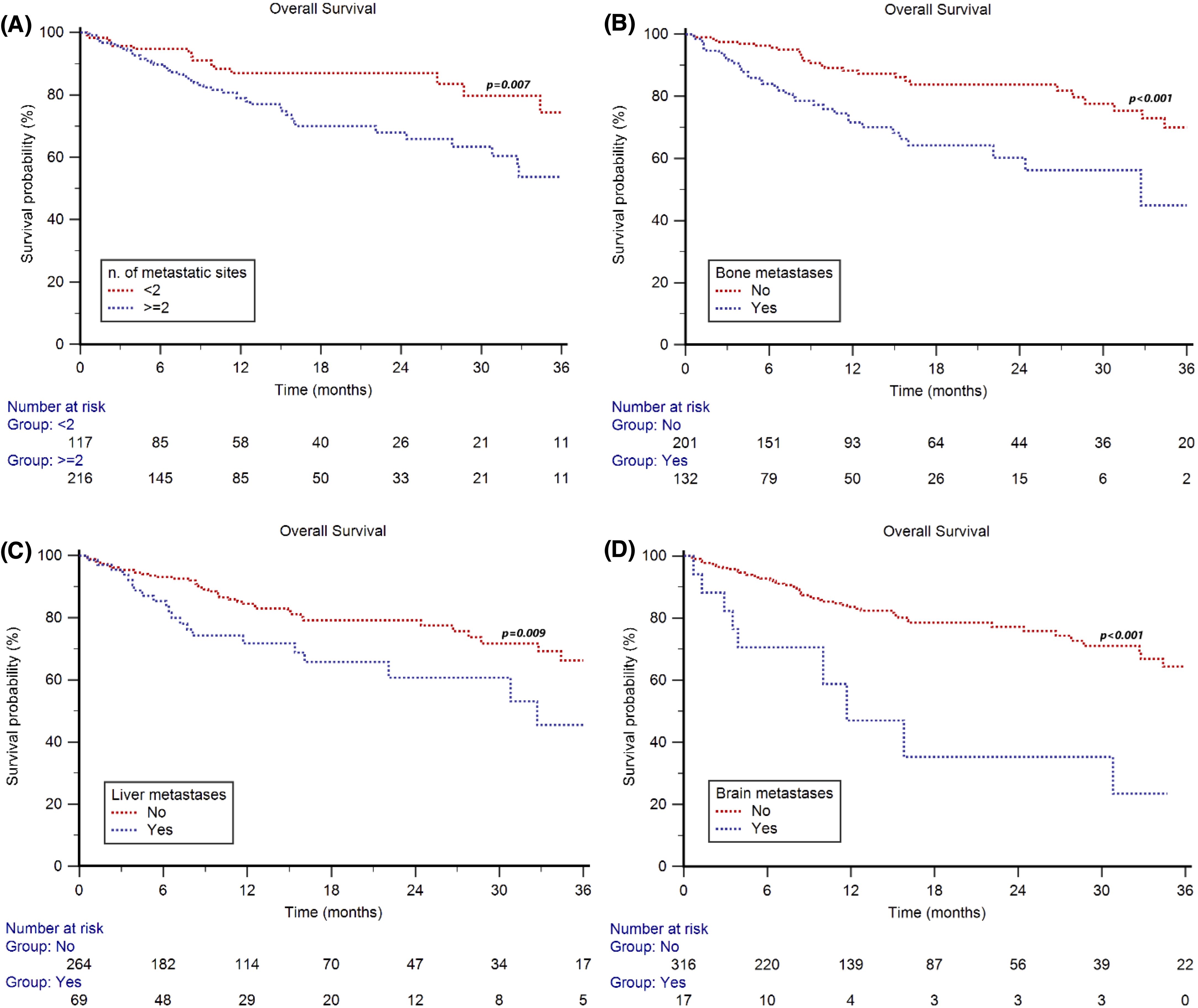
Figure 3. Overall Survival in mRCC patients treated with first-line cabozantinib plus nivolumab stratified by number and type of metastatic sites: number of metastatic sites (2 vs ≥2) (A), bone metastasis (no vs yes) (B), liver metastasis (no vs yes) (C), and brain metastasis (no vs yes) (D).
3.3 Prognostic factors in patients receiving first-line nivolumab plus cabozantinib
In the whole study population, ECOG-PS, nephrectomy, sarcomatoid de-differentiation, IMDC group, bone, liver and brain metastases were significantly associated with OS at univariate analysis (Table 2). At multivariate analysis, ECOG-PS ≥2, sarcomatoid de-differentiation, IMDC poor risk group, bone or brain metastases were significantly associated with shorter OS (Table 2).
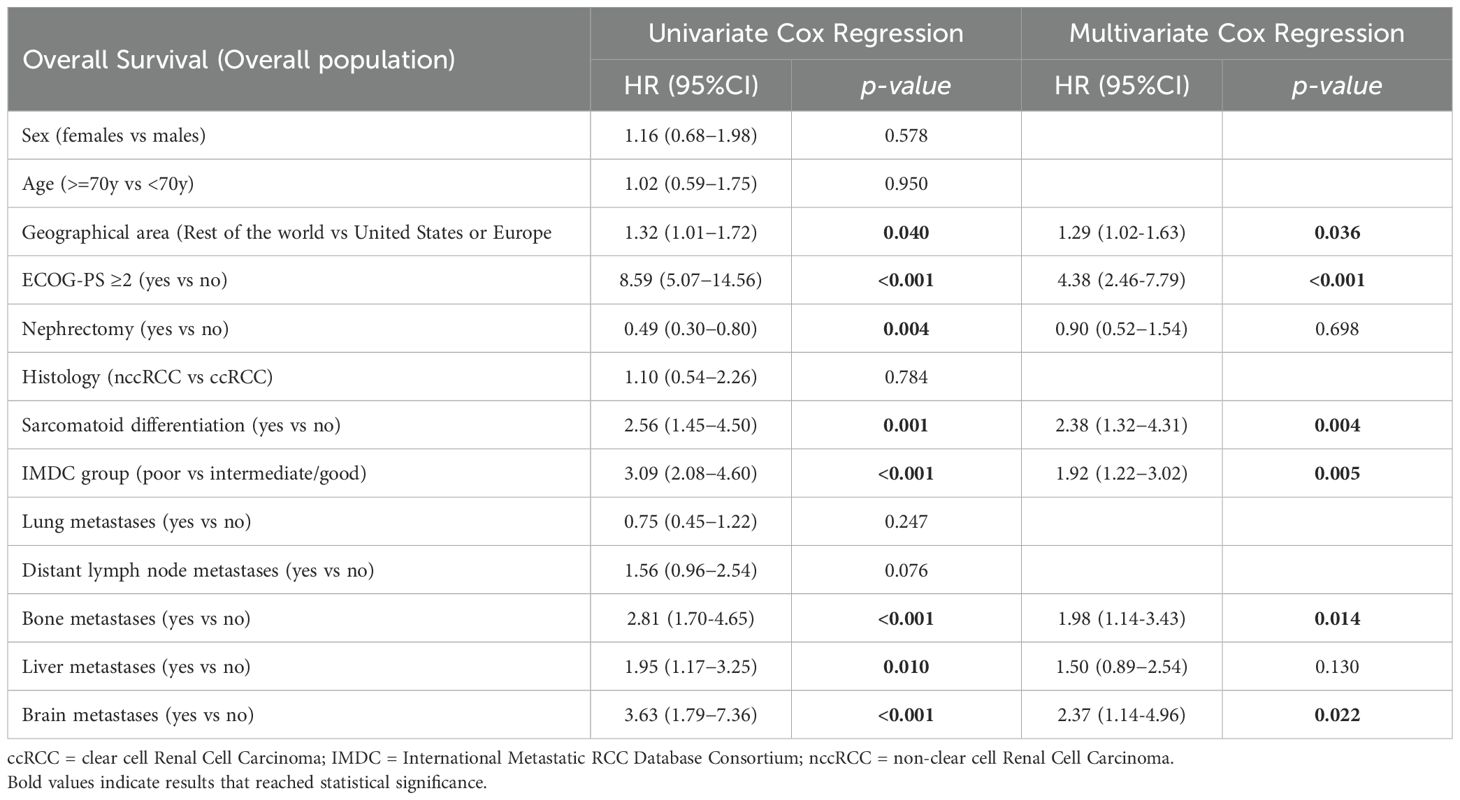
Table 2. Univariate and multivariate analysis in mRCC patients receiving first-line nivolumab plus cabozantinib.
3.4 Response to first-line nivolumab plus cabozantinib
In the whole study population, 19 CR (6%), 174 PR (52%), 103 SD (31%) and 37 PD (11%) were observed, with an ORR of 58%. The 2y-OS rates were 100%, 87%, 65% and 24% in patients with CR, PR, SD or PD, respectively (p<0.001).
The median DOR was 38.9 months (95%CI 33.7–NR) for the 58% patients who had an ORR. In patients who achieved CR the DOR was NR, and in those who had a PR the DOR was 35.2 months (95%CI 32.3–44.0).
By stratifying patients based on IMDC groups, in the good-risk group we observed 12 CR (20%), 27 PR (46%), 16 SD (29%) and 4 PD (5%), with an ORR of 66%; in the intermediate-risk group, 6 CR (4%), 97 PR (54%), 64 SD (35%) and 13 PD (7%) were demonstrated, with an ORR of 58%; and in the poor-risk group, 1 CR (1%), 50 PR (53%), 22 SD (24%) and 21 PD (18%) were found, with an ORR of 54%.
In the 276 patients with clear cell RCC, we reported 16 CR (7%), 148 PR (53%), 79 SD (28%) and 33 PD (12%), with an ORR of 60%. In the 57 patients with non-clear cell histology, we reported 1 CR (2%), 30 PR (47%), 24 SD (42%) and 2 PD (9%), with an ORR of 49%.
3.5 Progression free survival and subsequent therapies
The median PFS was 33.7 months (95%CI 21.1–38.9, Figure 1). For the 6- and 12-month PFS landmark analyses, the median PFS was 38.6 months (95%CI 32.3−50.7) and 41.4 months (95%CI 34.0−51.5), respectively (Supplementary Figure S2). One hundred and one patients (30%) progressed during nivolumab plus cabozantinib therapy; of these, 57 (56%) received subsequent treatments (26 patients received sunitinib, 8 axitinib, 5 pazopanib, 5 pembrolizumab plus lenvatinib, 5 lenvatinib plus everolimus, 4 everolimus, 3 tivozanib and 1 was enrolled in a clinical trial). The median PFS of second-line therapy was 5.3 months (95%CI 3.3–7.2).
3.6 Safety, dose reduction and therapy interruptions
Grade 3-Grade 4 (G3-G4) adverse events (AEs) were observed in 122 patients (37%). Hypertension (9%), and hand-foot syndrome (8%) were the two most frequent SAEs (Table 3).
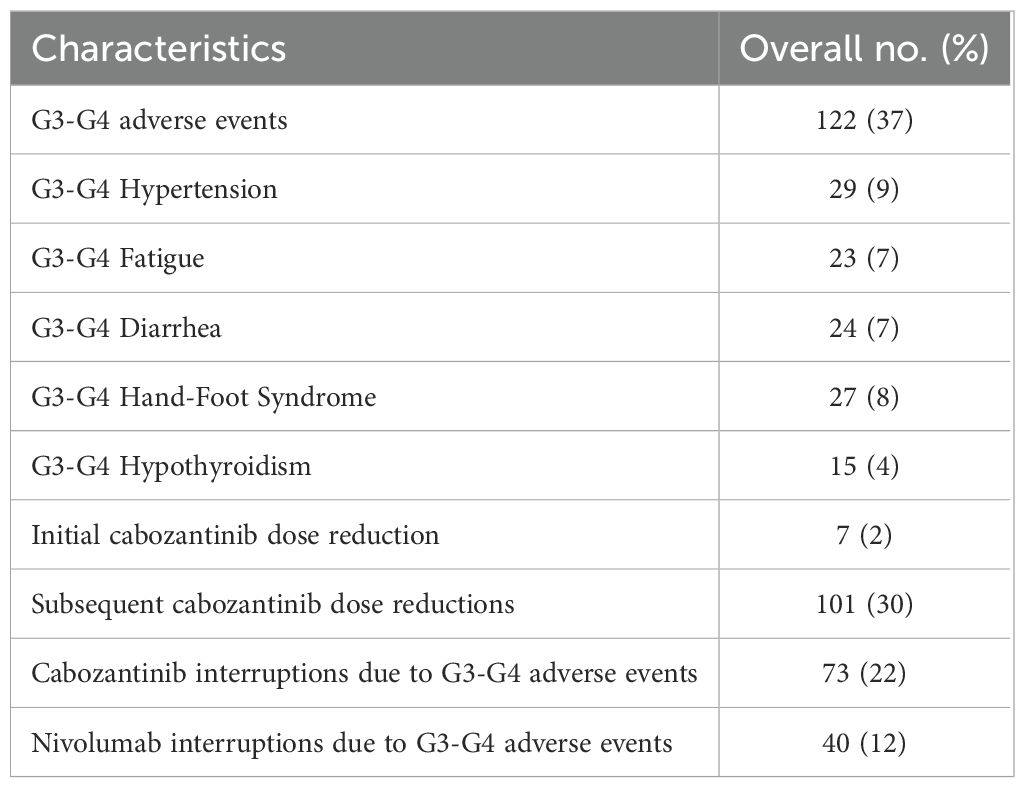
Table 3. Grade 3-Grade 4 (G3-G4) adverse events, drug interruptions and dose reductions.
Cabozantinib dose reductions were registered in 108 patients (32%), 2% started cabozantinib at 20 mg/d, 30% reduced the dose during treatment (Table 3); 22% and 12% of patients interrupted cabozantinib or nivolumab due to G3-G4 AEs, respectively (Table 3).
The median OS was NR in both patients who reduced cabozantinib dose compared to those treated with standard dose (p=0.322), with a 2y-OS rate of 79% vs 72% (p=0.324). Furthermore, the median OS was NR in patients who interrupted or not cabozantinib (p=0.807) or nivolumab (p=0.235) due to G3-G4 adverse events, with a 2y-OS rate of 80% vs 74% (p=0.401) and 83% vs 74% (p=0.168), respectively.
4 Discussion
The current standard of care for the first-line treatment of clear cell RCC is a combination therapy of either ICI/ICI or ICI/VEGFR-TKI, with a proven benefit in OS over the long-standing standard of care, sunitinib, in phase 3 randomized trials (1–8). The nivolumab plus cabozantinib combination has reported improved OS with a 55-month median follow-up (10).
On the other hand, given the lower frequency of non-clear cell RCC, treatment decisions in this subgroup are based on smaller phase 2 studies (11). Recently, in these histologic subtypes the combination therapies with a multi-kinase inhibitor and an ICI, including cabozantinib plus nivolumab and pembrolizumab plus lenvatinib, have proven to be effective (12, 13). The nivolumab plus cabozantinib regimen is recommended given the outcomes seen in the phase 2 trial (cohort 1) with ORR of 48%, a median PFS and median OS of 13 and 28 months, respectively (12).
Nevertheless, it is known that, more often than not, the participants in prospective clinical trials constitute a rather selected population. The importance of having real-world data is that these reports encompass populations of patients often excluded from clinical trials, such as patients with poor PS or aggressive disease, especially those with central nervous system involvement. The present study reports data of 333 patients with RCC treated with nivolumab plus cabozantinib combination in the first-line setting. To the best of our knowledge, this is the largest retrospective multicenter study exploring this therapeutic strategy to date (Table 4) (14–16). Furthermore, our study gathers data from 52 centers across 17 countries, offering valuable insights from a global oncology perspective by providing information across different healthcare systems, ethnic backgrounds and diverse resource settings.
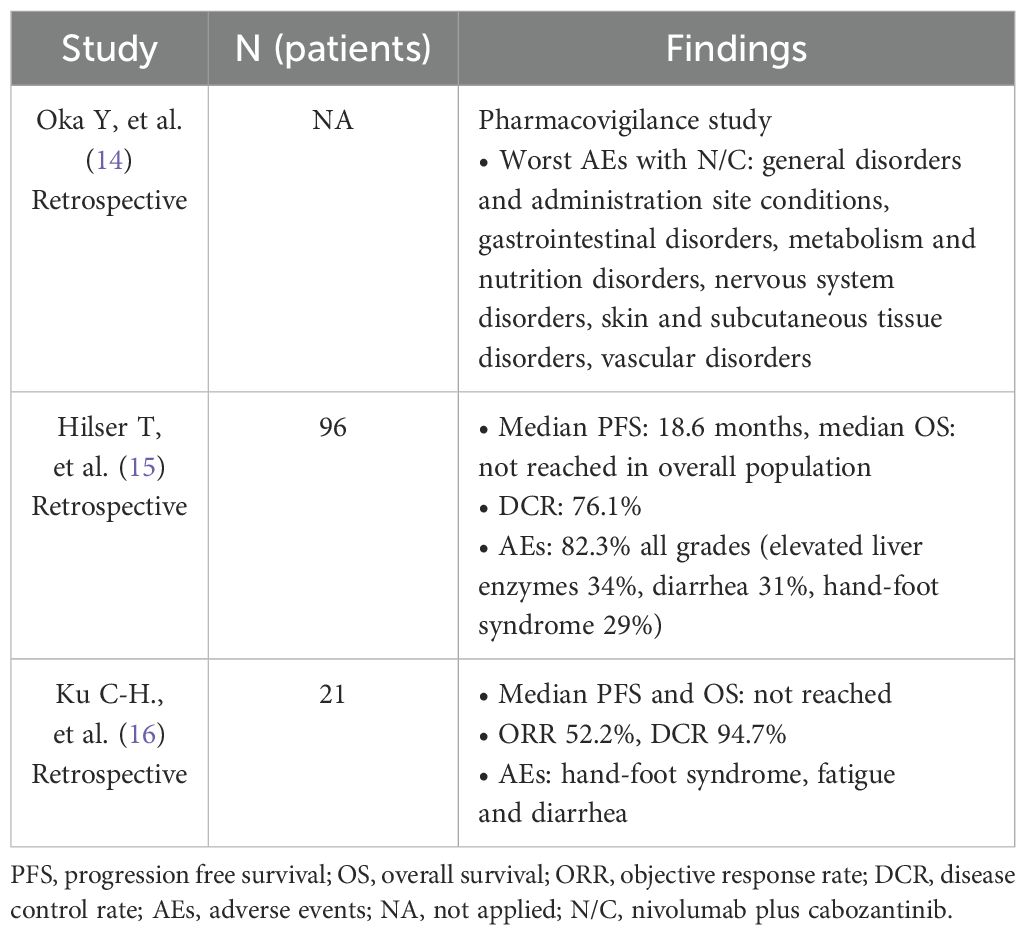
Table 4. Real-world data studies with nivolumab plus cabozantinib.
The median follow-up in the present study was 15.9 months, which is similar to the first report of the Checkmate 9ER study (18.1 months) (5). In this real-life evidence, the median OS has not been reached and the 75% OS at 2 years is close to the one reported in the phase 3 study. OS benefits were consistent irrespective of age and sex. Patients with poor PS experienced a shorter OS, and this is informative for the everyday decision making, since this subset of more frail patients is not represented in large phase 3 trials and is frequently seen in clinical grounds. As expected from previous reports, apart from poor PS, adverse prognostic factors included sarcomatoid de-differentiation, bone or brain metastases, and IMDC poor risk group (17).
Notably, median PFS and median DOR were 33.7 and 38.9 months respectively, which is higher than the rate reported for the CheckMate 9ER trial (16.6 and 20.2 months) (5, 6). Several factors may contribute to this discrepancy. Assessments in the clinical trial initially occurred every 6 weeks, while in this real-life report they occurred every 8 to 12 weeks and this could impact the PFS and DOR calculation. However, the benefit of more frequent imaging in real-world settings is debatable, as it may increase healthcare costs and patient burden without clear added value. Complications from repeated assessments, as well as their impact on quality of life, should be carefully weighed when determining imaging intervals.
Additionally, RECIST calculation in the real-world setting might not be as strict as in clinical trials and evaluation is not subjected to a central radiologic review, potentially affecting consistency and objectivity in response evaluation.
Another important consideration is the real-world practice of continuing treatment beyond radiographic progression, a strategy often restricted in clinical trials. Patients may remain on therapy due to perceived clinical benefit or personal preference, and in such cases, the date of treatment change rather than actual progression may be recorded, artificially prolonging PFS.
Regarding response rates compared to the subset of patients with clear cell RCC in the ARON-1 study, patients in the CheckMate 9ER had higher CR rates (13.5% vs 7%) and lower PD (6.5% vs 12%). These differences may be attributed to differences in patient populations. The ARON-1 trial included 43 patients (13%) with ECOG PS ≥2 and 17 patients (5%) with brain metastases, who were excluded from CheckMate 9ER, and a higher proportion of patients with poor-risk IMDC classification (28% vs 19% in CheckMate 9ER). Despite differences in CR and PD, ORR were similar in both trials (60% in ARON-1 vs 56% in CheckMate 9ER) (5, 6).
For non-clear cell RCC, the response rates in the ARON-1 study were consistent with those reported for the cohort 1 of the phase 2 trial, with an ORR of 49% and 48%, respectively. Notably, one patient in the ARON-1 trial achieved CR compared to none in the phase 2 trial. However, the rate of PD was higher in ARON-1 (9% vs. 3% in the phase 2 trial) (11). We consider that having real-world data in this subgroup is particularly meaningful given the difficulties to accrue patients with this histologic subtype in clinical trials.
Analyzing the safety profile, grade 3 or more toxicity was reported in 75.3% of patients with the combination in the CheckMate 9ER (5). A lower incidence of grade 3 or more toxicity was reported (37%) in the ARON-1. This could be explained in part because some toxicities such as mucositis, stomatitis, hematological disorders, dysgeusia, and liver enzyme increase were not systematically reported. In addition, in daily clinical practice, adverse events monitoring is not as rigorous as in clinical trials. Interestingly, the most frequent severe toxicities in ARON-1 were hypertension (9%), hand-foot syndrome (8%), diarrhea (7%), fatigue (7%), and hypothyroidism (4%). These frequencies are largely comparable to those reported in CheckMate 9ER, where grade ≥3 hypertension occurred in 12.5%, hand-foot syndrome in 7.5%, diarrhea in 7%, fatigue in 3.4%, and hypothyroidism in 0.3% (5). Furthermore, cabozantinib dose reductions were less frequent in ARON-1 (32%) compared to CheckMate 9ER (56%) (5), aligning with the lower incidence of grade 3 or higher toxicity and suggesting better overall treatment tolerance. Importantly, having real-world data on dose reductions and treatment discontinuations is essential, as these factors may influence treatment efficacy and patient outcomes in clinical practice.
A previous report of ARON-1 trial, which included 729 patients treated with all four approved immune-based combinations, suggests consistent efficacy results compared to the phase 3 trials in the overall population (median OS 36.5 months, median PFS 15 months, and ORR 49%) (18). Real-world data exists for all available immune-based combinations. For nivolumab and ipilimumab, real-world studies report ORR ranging from 33% to 48%, median PFS between 9 and 18 months, and median OS of 49 months—results consistent with those reported in the CheckMate 214 trial (ORR 42%, median PFS 8 months, and median OS 47 months) (1, 2, 19–21). Real-world evidence for pembrolizumab and lenvatinib is emerging, with two studies (n = 50 and n = 54) reporting ORR of 66% and 38%, respectively, the former ORR aligns with the CLEAR trial results (ORR 71%). Neither study has yet reported survival outcomes (19, 22, 23). Similarly, real-world data for pembrolizumab and axitinib indicate efficacy consistent with KEYNOTE 426, with ORR ranging from 48% to 71% compared to 60% in the trial (3, 24–26).
Specifically for the combination of nivolumab plus cabozantinib, recent real-world studies further support our findings. The GUARDIANS multicenter retrospective study, which included 96 patients, reported an ORR of 45.8% and a median PFS of 18.6 months. Median OS was not reached, with a 12-month probability of OS of 77.5%. Grade ≥3 treatment-related adverse events occurred in 41.7% of patients, and 25% discontinued treatment due to toxicity (15). Similarly, a retrospective study conducted across eight German cancer centers included 67 patients and, at a median follow-up of 8.3 months, reported an ORR of 46.3%, a 6-month PFS rate of 81.9%, and grade ≥3 AEs in 47.8% of patients (16). In another study from Taiwan by Ku et al., which included 21 patients treated with nivolumab plus cabozantinib, the ORR was 52.2% (27). These findings are consistent with the efficacy outcomes observed in ARON-1 and further reinforce the reproducibility of this combination in routine clinical practice.
We consider that ARON-1 study has several strengths, such as being a multicenter effort with global representation, it has the largest number of patients, and the inclusion of patients with characteristics (e.g. histological, performance status, brain metastasis) that are generally excluded from randomized clinical trials. However, as a retrospective study, the main limitations are a selection bias of cases included (since patients with incomplete data were excluded from the study) and the confounder variables that could not be measured. Another, limitation is the short time of follow-up compared to the phase 3 CheckMate 9ER study that has reported outcomes with 55 months median follow-up. However, the ARON-1 data will continue to mature over the years and will be informative of long-term outcomes as well.
As in most daily clinical practices, formal questionnaires or scales for evaluating quality of life are scarcely employed (28). A weakness of the real-world data from the different combinations in this scenario, including the ARON-1 trial, is the lack of information regarding how patients experience both treatment benefits and adverse events.
In conclusion, decision-making regarding the optimal immune-based combination is inherently complex. The ARON-1 trial seeks to simplify this process by providing real-world data on the combination of nivolumab and cabozantinib. The findings of this study show benefit across all subgroups, including populations that are generally excluded from clinical trials, for whom data if often missing.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Marche Region (2021-492) and from the Institutional Review Boards of all participating centers according to the regulations in force in each Country. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because This was a retrospective study involving minimal risk to participants. All data were collected from existing medical records, and no direct patient contact occurred. The participating institutions require patients to sign a general informed consent upon admission, which includes authorization for the use of anonymized data in research, provided that patient confidentiality is maintained.
Author contributions
MB: Writing – original draft, Conceptualization, Formal analysis, Writing – review & editing. LG: Writing – review & editing, Writing – original draft. EG: Writing – review & editing. SP: Writing – review & editing. BM: Writing – review & editing. TS: Writing – review & editing. MJ-F: Writing – review & editing. YÜ: Writing – review & editing. JM-C: Writing – review & editing. TA-G: Writing – review & editing. UD: Writing – review & editing. JK: Writing – review & editing. EP: Writing – review & editing. VC: Writing – review & editing. TT: Writing – review & editing. PR: Writing – review & editing. HA-S: Writing – review & editing. GS: Writing – review & editing. RK: Writing – review & editing. AS: Writing – review & editing. DB: Writing – review & editing. PV-S: Writing – review & editing, Writing – original draft. SM-B: Writing – original draft, Writing – review & editing. OF: Writing – review & editing. SB: Writing – review & editing. FMM: Writing – review & editing. AB: Writing – review & editing. MG: Writing – review & editing. FM: Writing – review & editing. JA: Writing – review & editing. MS: Formal analysis, Writing – review & editing, Conceptualization, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
MB has received honoraria from Adium, Astellas, Astra Zeneca, Bayer, Bristol Myers Squibb, Eisai, IPSEN, Johnson & Johnson, Merck, Novartis, MSD, Pfizer, Tecnofarma. Brissto Myers Squibb and Ipsen honoraria are related to the combination therapy reported herein. LG declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. EG has received honoraria from AbbVie, Adium, Advanced Accelerator Applications, AMGEN, Angelini, Astellas, Astra Zeneca, AVEO, Bayer, Blueprint, Bristol Myers Squibb, Clovis-Oncology, Dr. Reddy’s, Eisai, Esteve, Eusa Pharma, GSK, IPSEN, ITM-Radiopharma, Janssen, Lilly, Merck KGaA, MSD, Novartis, ONCODNA Biosequence, Palex, Pfizer, Raffo, Roche, Tecnofarma, Thermo Fisher Scientific, Zodiac; has received institutional research funding from Astellas, Astra Zeneca, IPSEN, Lexicon, Merck KGaA, MTEM/Threshold/Tersera, Nanostring Technologies, Pfizer, Roche; and has received travel and accommodation expenses from Bristol Myers Squibb, Ipsen, Janssen, Pfizer, and Roche/Genentech. SP declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. BM has received research funding, honoraria, and non-financial or other support from Roche, Pfizer, BMS, Astellas, Novartis, MSD, Merck Serono, AstraZeneca, Eisai, and E. Lilly. TS declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. YÜ has served on advisory boards for Abdi-Íbrahim, Astellas, Astra Zeneca, Bristol Myers-Squibb, Deva, Eczacıbaşı, Gen ilaç, Gilead, GSK, Janssen, Merck, MSD, Novartis, Pfizer, Roche. And has received honoraria or has served as consultant for Abdi-Íbrahim, Astellas, Bristol Myers-Squibb, Deva, Eczacıbaşı, Gen ilaç Gilead, GSK, Janssen, Merck, Novartis, Pfizer, Roche. JM-C declares consultant, advisory or speaker roles for IPSEN, Roche, Pfizer, Sanofi, Janssen, and BMS. JMC has received research grants from Pfizer, IPSEN and Roche. TA-G has received research funding, honoraria, and non-financial or other support from IPSEN, Adacap, Pfizer, Sanofi, EISAI, Lilly, Bayer, Janssen, BMS, Astellas, Novartis, Roche, and Merck. UD Reports a consulting or advisory role for Amgen, Astellas Pharma, AstraZeneca, Bayer, Bristol Myers Squibb, Eisai, Ipsen, Johnson & Johnson Innovative Medicine formerly Janssen, Merck KGaA, Merck Sharp & Dohme, Novartis, and Pfizer Inc. Travel, accommodation, and/or expenses from Ipsen, AstraZeneca and Pfizer. Research funding Institution from AstraZeneca, Roche, and Sanofi. JK honoraria for consultations, lectures or educational events: Angelini, Astellas, Astra Zeneca, Bayer, Bristol Myers Squibb, IPSEN, Johnson&Johnson, Merck, MSD, Novartis, Pfizer. Research Funding: Novartis. All unrelated to the present paper. VC has served as a consultant/advisory board member for Johnson&Johnson, Astellas, Merck, AstraZeneca, Amgen, EISAI, Recordati, Novartis and Bayer and has received speaker honoraria or travel support from Astellas, Johnson&Johnson, Ipsen, Bayer, Astrazeneca, Gilead, GSK and BristolMyers Squibb. TT reports institutional support for attending meetings and/or travel from Pfizer, and receiving honoraria from BMS, MSD, Merck-Serono and Pfizer. GS speakear/advisory: B,S, Janssen, Novartis, Roche, Bayer. RK Clinical research: MSD, BMS, AstraZeneca, Roche, Pfizer, Novartis, Abbvie, Amgen, Jannsen. Speaker/advisory: MSD, BMS, Astrazeneca, Janssen, Astellas, Tecnofarma, Pfizer, GSK, Ipsen, Janssen, Bayer, Eli Lilly, Roche, Novartis, Adium, Amgen, Merck Serono. OF received honoraria from Roche, Janssen, GSK, MSD, BMS, Pierre Fabre and Pfizer for consultations and lectures unrelated to this project. SB has received honoraria for speaking at scientific events and advisory roles from AstraZeneca, Bristol Myers Squibb, Ipsen, Merck, Eisai, MSD, Novartis, Gentili, Astellas and Pfizer and research funding from Novartis and Pfizer. FMM Research support was provided by Janssen and Merck Sharp Dome. Honoraria from Janssen, Ipsen, Bristol Myers Squibb, and Merck Sharp Dome. Travel, Accommodations, Expenses: Ipsen, Novartis, Merck, Merck Sharp Dome and Adium. Ownership: BIO, Brazilian Information Oncology. All are unrelated to this study. AB has received honoraria, advisory and research support from MSD, BMS, AZ, Ipsen and Astellas. FM has received research support and/or honoraria from Astellas, BMS, Janssen, Ipsen, MSD and Pfizer outside the submitted work. MS has received research support and honoraria from Janssen, Bristol Myers Squibb, Ipsen, MSD, Astellas, A.A.A. and Bayer, all unrelated to the present paper.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1605282/full#supplementary-material
References
1. Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. (2018) 378:1277–90. doi: 10.1056/NEJMoa1712126
2. Tannir NM, Albigès L, McDermott DF, Burotto M, Choueiri TK, Hammers HJ, et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended 8-year follow-up results of efficacy and safety from the phase III CheckMate 214 trial. Ann Oncol. (2024) 35:1026–38. doi: 10.1016/j.annonc.2024.07.727
3. Rini BI, Plimack ER, Stus V, Gafanov R, Hawkins R, Nosov D, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2019) 380:1116–27. doi: 10.1056/NEJMoa1816714
4. Powles T, Plimack ER, Soulières D, Waddell T, Stus V, Gafanov R, et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. (2020) 21:1563–73. doi: 10.1016/S1470-2045(20)30436-8
5. Choueiri TK, Powles T, Burotto M, Escudier B, Bourlon MT, Zurawski B, et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2021) 384:829–41. doi: 10.1056/NEJMoa2026982
6. Powles T, Burotto M, Escudier B, Apolo AB, Bourlon MT, Shah AY, et al. Nivolumab plus cabozantinib versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended follow-up from the phase III randomised CheckMate 9ER trial. ESMO Open. (2024) 9:102994. doi: 10.1016/j.esmoop.2024.102994
7. Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. (2021) 384:1289–300. doi: 10.1056/NEJMoa2035716
8. Motzer RJ, Porta C, Eto M, Powles T, Grünwald V, Hutson TE, et al. Lenvatinib plus pembrolizumab versus sunitinib in first-line treatment of advanced renal cell carcinoma: final prespecified overall survival analysis of CLEAR, a phase III study. J Clin Oncol. (2024) 42:1222–8. doi: 10.1200/JCO.23.01569
9. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026
10. Bourlon MT. Nivolumab plus Cabozantinib vs Sunitinib for Previously Untreated Advanced RCC: Results from 55-Month Follow-up of the CheckMate 9ER Trial. Oral presentation. ASCO GU; 2024 Jan 25-27. (2024) San Francisco, CA, USA.
11. Naik P, Dudipala H, Chen Y-W, Rose B, Bagrodia A, and McKay RR. The incidence, pathogenesis, and management of non-clear cell renal cell carcinoma. Ther Adv Urol. (2024) 12:17562872241232578. doi: 10.1177/17562872241232578
12. Lee C-H, Voss MH, Carlo MI, Chen Y-B, Zucker M, Knezevic A, et al. Phase II trial of cabozantinib plus nivolumab in patients with non–clear-cell renal cell carcinoma and genomic correlates. J Clin Oncol. (2022) 40:2333–41. doi: 10.1200/JCO.21.01944
13. Albiges L, Gurney H, Atduev V, Suarez C, Climent MA, Pook D, et al. Pembrolizumab plus lenvatinib as first-line therapy for advanced non-clear-cell renal cell carcinoma (KEYNOTE-B61): a single-arm, multicentre, phase 2 trial. Lancet Oncol. (2023) 24:881–91. doi: 10.1016/S1470-2045(23)00276-0
14. Oka Y, Matsumoto J, Takeda T, Iwata N, Niimura T, Ozaki AF, et al. Adverse events of nivolumab plus ipilimumab versus nivolumab plus cabozantinib: a real-world pharmacovigilance study. Int J Clin Pharm. (2024) 46:745–50. doi: 10.1007/s11096-024-01713-1
15. Hilser T, Darr C, Niegisch G, Schnabel MJ, Foller S, Häuser L, et al. Cabozantinib plus nivolumab in adult patients with advanced or metastatic renal cell carcinoma: A retrospective, non-interventional study in a real-world cohort/GUARDIANS project. Cancers (Basel). (2024) 16:2998. doi: 10.3390/cancers16172998
16. Ku C-H, Su PJ, Huang WK, Kuo YC, Chang CF, and Yu S. Abstract 303P. Cabozantinib versus cabozantinib plus nivolumab in first-line treatment of advanced renal cell carcinoma: A Chang Gung medical foundation multicentric cohort, real-world study. Ann Oncol. (2024) 35:S1521. doi: 10.1016/j.annonc.2024.10.322
17. Heng DY, Xie W, Regan MM, Warren MA, Golshayan AR, Sahi C, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. (2009) 27:5794–9. doi: 10.1200/JCO.2008.21.4809
18. Santoni M, Roviello G, Grande E, De Giorgi U, Fiala O, Seront E, et al. Global real-world outcomes of patients receiving immuno-oncology combinations for advanced renal cell carcinoma: the ARON-1 study. Target Oncol. (2023) 18:559–70. doi: 10.1007/s11523-023-00978-2
19. Kojima T, Kato R, Sazuka T, Yamamoto H, Fukuda S, Yamana K, et al. Real-world effectiveness of nivolumab plus ipilimumab and second-line therapy in Japanese untreated patients with metastatic renal cell carcinoma: 2-year analysis from a multicenter retrospective clinical study (J-cardinal study). Japanese J Clin Oncol. (2022) 52:1345–52. doi: 10.1093/jjco/hyac124
20. Ishihara H, Yuki N, Ishiyama R, Ikeda T, Kobari Y, Fukuda H, et al. Real-world outcomes of nivolumab plus ipilimumab combination therapy for advanced renal cell carcinoma in Japanese patients: data with a minimum of 3 years of follow-up. Japan Journ Clin Oncol. (2024) 54:577–83. doi: 10.1093/jjco/hyae001
21. Meerveld-Eggink A, Graafland N, Wilgenhof S, Van Thienen JV, Lalezari F, Grant M, et al. Primary renal tumour response in patients treated with nivolumab and ipilimumab for metastatic renal cell carcinoma: real-world data assessment. Europ Urol. (2022) 35:54–8. doi: 10.1016/j.euros.2021.11.003
22. Hara T, Suzuki K, Okamura Y, Chiba K, Sato R, Matsushita Y, et al. Efficacy and safety of lenvatinib and pembrolizumab as first-line treatment for advanced renal cell carcinoma patients: real-world experience in Japan. Int J Clin Oncol. (2024) 29:1931–6. doi: 10.1007/s10147-024-02633-w
23. Stativko O, Pokataev I, Fedyanin M, Kravchuk DA, Andreiashkina I, Polshina N, et al. Real-world efficacy of lenvatinib and pembrolizumab as first-line therapy in patients with metastatic renal cell carcinoma with high burden disease. Ann Oncol. (2024) 35:S1505–30. doi: 10.1016/j.annonc.2024.10.304
24. Shah NJ, Sura SD, Shinde R, Shi J, Singhal P, Perini RF, et al. Real-world clinical outcomes of patients with metastatic renal cell carcinoma receiving pembrolizumab + axitinib vs ipilimumab + nivolumab. Urol Oncol. (2023) 41:459.e1–8. doi: 10.1016/j.urolonc.2023.08.009
25. Guida A, Gili A, Mosillo C, Maruzzo M, Lai E, Pierantoni F, et al. Efficacy and Safety of Pembrolizumab plus Axitinib combination for Metastatic Renal Cell Carcinoma in a Real-World Scenario: Data From the Prospective ProPAXI Study. Clin Genitourin Cancer. (2024) 22:102225. doi: 10.1016/j.clgc.2024.102225
26. Zakharia Y, Thomaidou D, Li B, Siu G, Levin R, Vlahiotis A, et al. Real-world therapy management and outcomes of first-line axitinib plus pembrolizumab in patients with advanced renal cell carcinoma in the United States. Front Oncol. (2022) 12:861189. doi: 10.3389/fonc.2022.861189
27. Ku WC, Wang YT, Lin CC, Hsieh MC, and Lee CH. Real-world experience with nivolumab and cabozantinib for metastatic renal cell carcinoma in Taiwan. J Clin Oncol. (2023) 41:628. doi: 10.1200/JCO.2023.41.6_suppl.628
Keywords: nivolumab plus cabozantinib, real-world evidence, metastatic renal cell carcinoma, clear cell renal cell carcinoma, non-clear cell renal cell carcinoma
Citation: Bourlon MT, Galli L, Grande E, Park SH, Melichar B, Schieber TJ, Juan-Fita MJ, Ürün Y, Molina-Cerrillo J, Alonso-Gordoa T, De Giorgi U, Kucharz J, Pérez Calabuig E, Conteduca V, Taha T, Rescigno P, Abu-Sini H, Spinelli GP, Manneh Kopp R, Salfi A, Bhuva D, Valdez-Sandoval P, Mendez-Bribiesca S, Fiala O, Buti S, Marques Monteiro FS, Bamias A, Ghosn M, Massari F, Ansari J and Santoni M (2025) Nivolumab plus cabozantinib in metastatic renal cell carcinoma: real-world evidence from the international ARON-1 study. Front. Oncol. 15:1605282. doi: 10.3389/fonc.2025.1605282
Received: 03 April 2025; Accepted: 30 June 2025;
Published: 25 July 2025.
Edited by:
John Peter Sfakianos, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Serena Astore, San Camillo Forlanini Hospital, ItalyXiangyu Chen, Tianjin Medical University General Hospital, China
Copyright © 2025 Bourlon, Galli, Grande, Park, Melichar, Schieber, Juan-Fita, Ürün, Molina-Cerrillo, Alonso-Gordoa, De Giorgi, Kucharz, Pérez Calabuig, Conteduca, Taha, Rescigno, Abu-Sini, Spinelli, Manneh Kopp, Salfi, Bhuva, Valdez-Sandoval, Mendez-Bribiesca, Fiala, Buti, Marques Monteiro, Bamias, Ghosn, Massari, Ansari and Santoni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matteo Santoni, bWF0dGVvLnNhbnRvbmk4MkBnbWFpbC5jb20=
†These authors have contributed equally to this work
‡These authors share senior authorship