 Aliny W. Kuhn1
Aliny W. Kuhn1 Antonio M. Lerario2
Antonio M. Lerario2 Alice N. R. Morais3
Alice N. R. Morais3 Ricardo F. Iglesio4Félix J. A. Ramires5Ligia C. A. Maluf6
Ricardo F. Iglesio4Félix J. A. Ramires5Ligia C. A. Maluf6 Ana O. Hoff7
Ana O. Hoff7 Ana C. Latronico1
Ana C. Latronico1 Berenice B. Mendonça1
Berenice B. Mendonça1 Madson Q. Almeida1,7
Madson Q. Almeida1,7 Maria C. B. V. Fragoso1,7*
Maria C. B. V. Fragoso1,7*- 1Adrenal Unit, Hormones and Molecular Genetics Laboratory (LIM/42), Division of Endocrinology and Metabolism, Hospital das Clínicas, Faculty of Medicine, University of São Paulo, São Paulo, Brazil
- 2Department of Internal Medicine, Division of Metabolism, Endocrinology, and Diabetes, University of Michigan, Ann Arbor, MI, United States
- 3Division of Oncology, São Paulo State Cancer Institute, University of São Paulo, São Paulo, Brazil
- 4Division of Neurosurgery Oncology, São Paulo State Cancer Institute, University of São Paulo, São Paulo, Brazil
- 5Division of Cardiology, Hospital das Clínicas, Faculty of Medicine, University of São Paulo, São Paulo, Brazil
- 6Division of Radiotherapy, São Paulo State Cancer Institute, University of São Paulo, São Paulo, Brazil
- 7Division of Endocrinology, São Paulo State Cancer Institute, University of São Paulo, São Paulo, Brazil
Cardiac myxomas, though rare, are the most common benign cardiac tumors and may be associated with Carney Complex (CNC). Patients with CNC are at increased risk of developing recurrent myxomas, which can lead to severe complications. We report a case of a 46-year-old woman with CNC and recurrent cardiac myxomas who developed multiple embolic strokes and cerebral aneurysms. Following two hemorrhagic strokes, neuroimaging and biopsy revealed a well-differentiated myxoid neoplasm in the brain parenchyma. Genetic analysis revealed a germline pathogenic PRKAR1A variant, along with loss of heterozygosity (LOH) at chromosome 17q24.2 in the cardiac myxoma, but not in the brain lesion. This case challenges the conventional understanding of cardiac myxomas as strictly benign, suggesting they may exceptionally exhibit distant proliferative behavior, likely through mechanical dissemination and subsequent growth in the brain. Although embolic events are common in cardiac myxomas, the capacity of tumor cells to implant and proliferate in extracardiac sites remains poorly understood. Our findings underscore the importance of maintaining a high index of suspicion for neurological complications in patients with cardiac myxomas, particularly in the setting of CNC. Further investigation is essential to elucidate the mechanisms driving this behavior and to optimize management strategies in similar cases.
1 Introduction
Primary cardiac tumors are rare, and cardiac myxomas represent the most common benign subtype (1, 2). They may arise sporadically or in association with Carney Complex (CNC), an autosomal dominant syndrome marked by a wide range of benign and malignant neoplasms affecting the heart, skin, endocrine organs, and nervous system (3). Given its multisystem involvement and high risk of tumor recurrence, Carney Complex mandates lifelong, protocol-driven surveillance in line with established clinical guidelines and consensus-based recommendations (4, 5).
CNC is diagnosed based on established clinical and molecular criteria (Table 1), with germline pathogenic variants in the PRKAR1A, which encodes the type 1A regulatory subunit of the cAMP-dependent protein kinase, being the most frequently identified genetic cause (4, 5). Around 20%–40% of individuals with CNC develop cardiac myxomas (6). Despite being histologically benign, cardiac myxomas can be clinically aggressive, with a propensity for complications such as fragmentation, embolization, local invasion, and regrowth. In rare cases, metastasis-like dissemination to distant sites, including the pelvis, spinal cord, sternum, and brain, has been reported (7). This report describes a rare and complex case of CNC with recurrent cardiac myxomas, complicated by cerebral aneurysms and a myxomatous brain lesion. It raises important questions about the potential for tumor cells to migrate and grow beyond the heart.
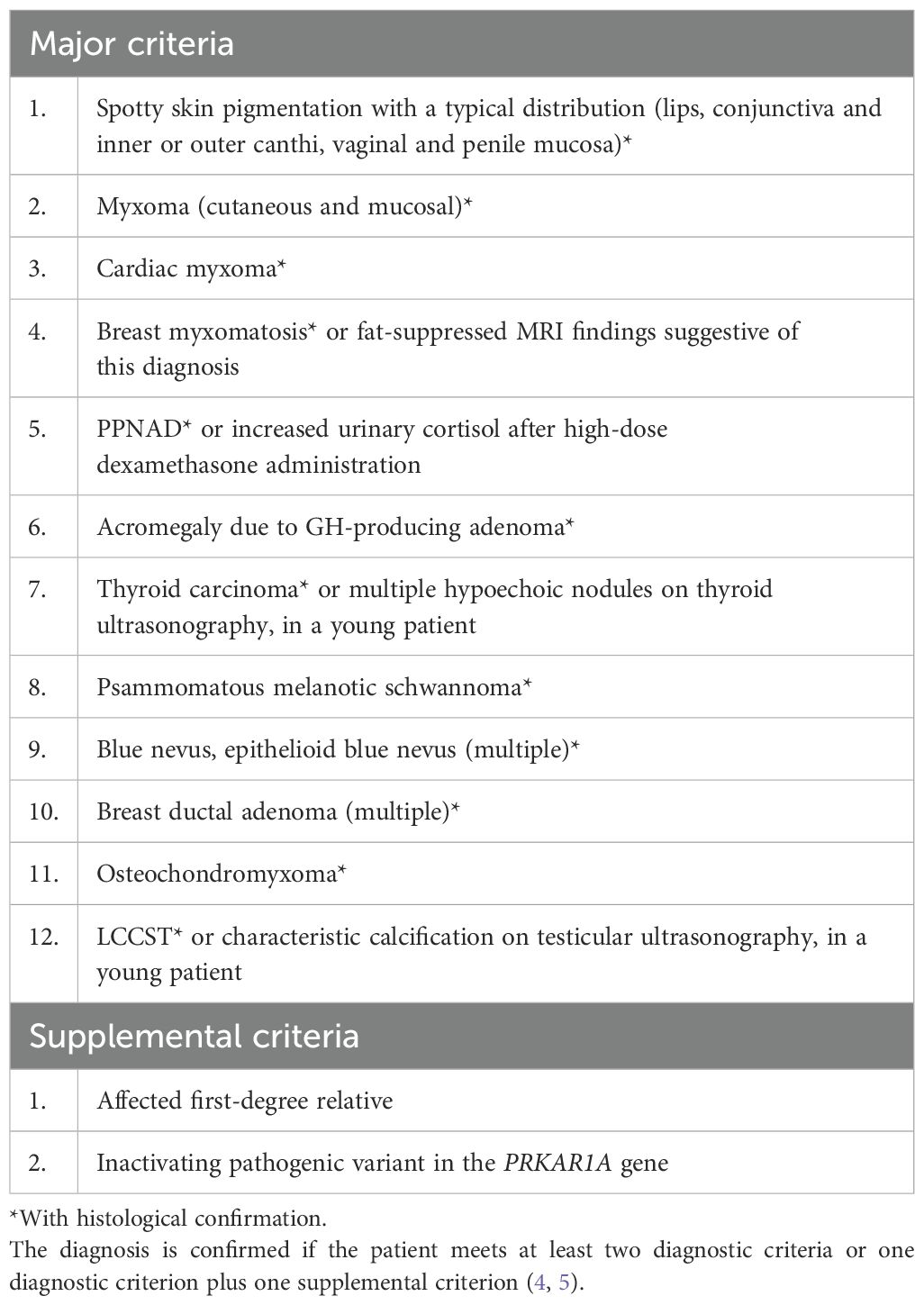
Table 1. Major and supplemental criteria for CNC.
2 Case description
A 46-year-old female patient, previously diagnosed with Carney Complex (CNC; OMIM# 160980), presented with a history of adrenocorticotropic hormone (ACTH)-independent Cushing’s syndrome, supported by histology as primary pigmented micronodular adrenal disease (PPNAD). Additional clinical features included labial lentigines, multiple cutaneous myxomas, thyroid nodules, mammary microcalcifications, elevated serum levels of growth hormone and insulin-like growth factor 1 (IGF-1), and a recurrent left atrial myxoma. Genetic testing revealed a germline pathogenic PRKAR1A variant (c.491_492delTG, p.Val164Aspfs*5; rs281864790 in heterozygosity), which has been linked to an increased risk of cardiac myxomas, lentigines, and thyroid tumors compared to other genotypes (8).
Prior to the current clinical course, the patient had undergone two cardiac surgeries to remove myxomas. The first surgery addressed a right atrial tumor measuring 6.7 × 4.5 cm. Seven years later, imaging reveled a new myxoma in the oval fossa of the left interatrial septum (3.5 × 2.9 × 1.3 cm), along with recurrence of the previously excised tumor, now reduced to 1.7 × 1.1 × 1.1 cm.
Seven months before the current presentation, the patient experienced sudden motor aphasia. Brain CT revealed an ischemic stroke in the left middle cerebral artery territory. By that time, recurrence of the myxoma had already been detected, but surgical resection was postponed owing to restrictions related to the COVID-19 pandemic. Antithrombotic therapy was withheld, as the presumed underlying mechanism was embolization secondary to tumor fragmentation. Several months later, she suffered a second stroke involving multiple vascular territories, accompanied by cerebral and cerebellar microhemorrhages. The atrial myxoma (now measuring 3.3 × 2.5 × 1.5 cm, Figure 1) was considered the most likely source of these embolic events. Importantly, no clinical signs or symptoms suggestive of systemic inflammatory syndrome were observed during this period. Surgical intervention was eventually performed, including tumor resection and placement of an interatrial patch. In the postoperative period, the patient developed right upper limb weakness and seizures. Brain imaging revealed an intraparenchymal hematoma in the left frontoparietal region (2.4 × 1.8 × 1.6 cm) and a smaller hematoma in the left occipital lobe (0.8 × 0.6 cm). Conservative management led to partial recovery of motor function and complete seizure control. The patient was discharged on anticonvulsant therapy.
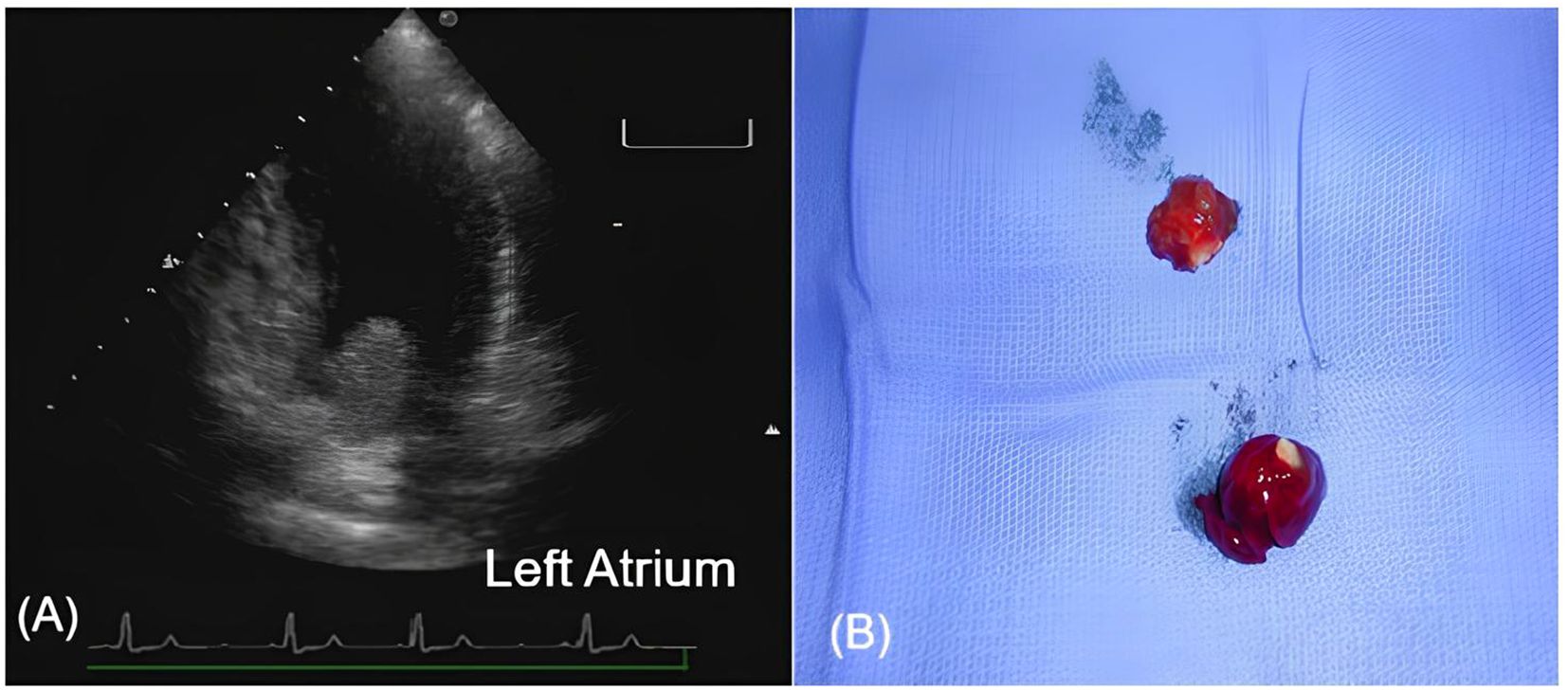
Figure 1. Recurrent left atrial myxoma originating from the interatrial septum. (A) Transthoracic echocardiography (apical four-chamber view) showing a mobile mass in the left atrium attached to the interatrial septum, measuring approximately 3.3 × 2.5 x 1.5 cm. (B) Gross pathology of the excised myxoma, showing a lobulated gelatinous tumor consistent with typical myxomatous appearance.
She was readmitted with worsening aphasia and new right-sided hypoesthesia. Imaging revealed a new hematoma in the left parietal lobe, enlargement of the pre-existing intraparenchymal hematomas, and subarachnoid hemorrhage. Further diagnostic workup included cerebral arteriography, which identified multiple fusiform aneurysms in distal branches of the right posterior cerebral artery and bilateral middle cerebral arteries. 18F-FDG PET/CT showed marked hypermetabolism in the left parietal hematoma (SUVmax: 5.2; late phase: 8.0) and moderate uptake in a second lesion in the left frontal operculum (SUVmax: 4.8; late phase: 5.5; Figure 2). Neither transesophageal echocardiography nor cardiac 18FDG-PET revealed evidence of a residual or recurrent cardiac myxoma.
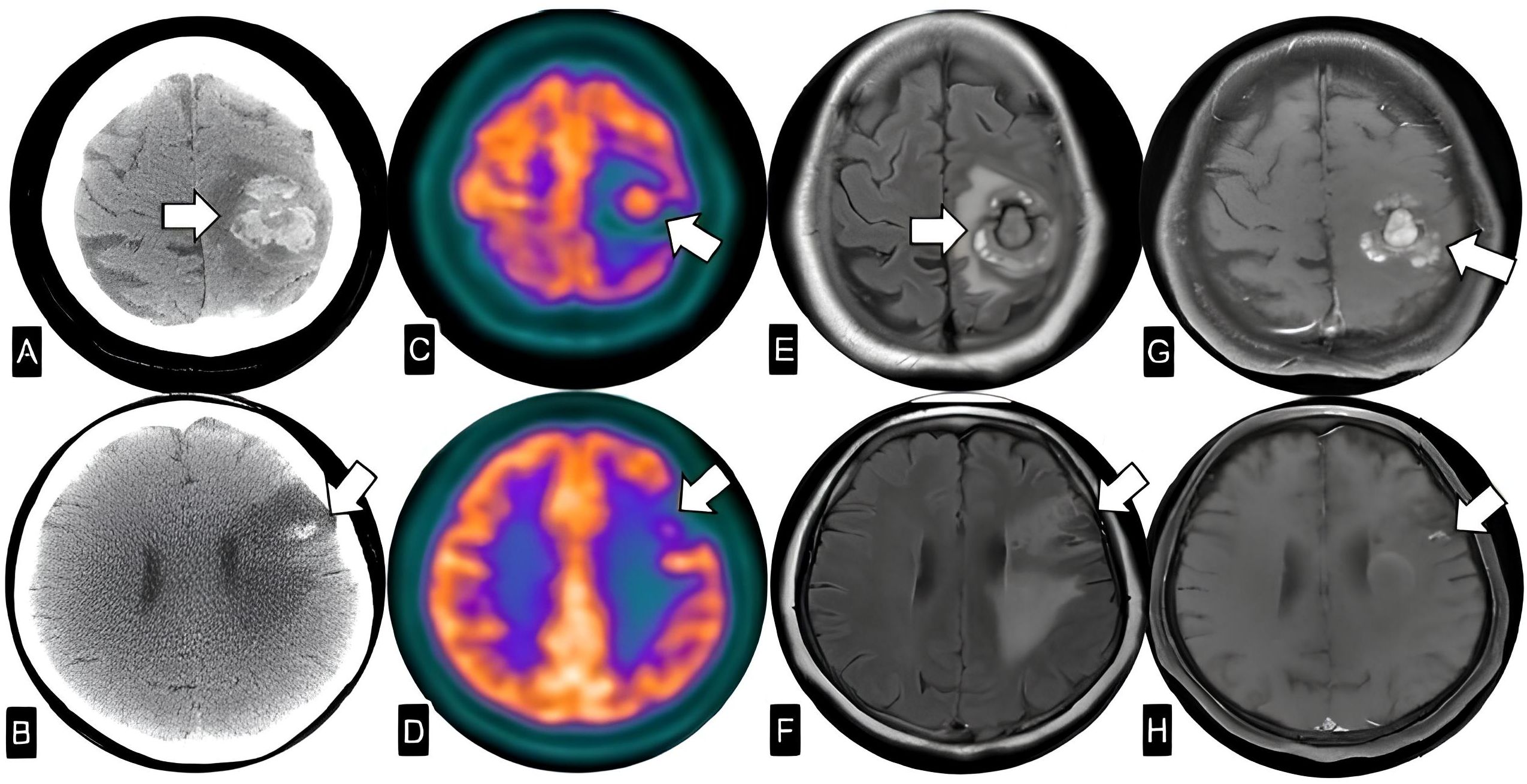
Figure 2. (A, B) Non-enhanced CT images. (C, D) Fused 18FDG-PET andCT images. (E, F) T2 FLAIR and (G, H) T1-Gd axial MRI. The images reveal two intraparenchymal expansive hemorrhagic and enhancing lesions in the left frontoparietal region with FDG uptake, suggestive of metastatic disease.
At that time, differential diagnoses included hemorrhagic stroke secondary to vascular malformations, primary central nervous system neoplasms, or metastatic disease, however based on imaging findings suggestive of neoplastic involvement, an excisional biopsy was performed on the left frontoparietal lesion (measuring 0.3 × 2.0 × 0.8 cm). Histopathological and immunohistochemical analyses confirmed the diagnosis of a well-differentiated myxoid neoplasm. In light of the histopathological evidence, the hemorrhagic nature of the lesions, and the high recurrence risk associated with Carney Complex, the case was reviewed by a multidisciplinary tumor board for treatment planning. Radiotherapy was recommended to enhance local control and prevent further neurological decline. Volumetric modulated arc therapy (VMAT) was chosen over conventional whole-brain radiotherapy (WBRT) due to its superior dose modulation capabilities, enabling hippocampal sparing to preserve cognitive function in this young patient. VMAT allowed for the delivery of a total dose of 30 Gy to the whole brain, with a simultaneous integrated boost to 40 Gy targeting the lesions identified on 18F-FDG PET/CT, a regimen that was well-tolerated. Additionally, VMAT offered improved protection of intracranial vascular structures, a critical consideration given the presence of multiple fusiform aneurysms and the potential risk of radiation-induced vessel wall fragility.
One month after completing radiotherapy, the patient developed extensive deep vein thrombosis in the right lower limb. Due to her prior hemorrhagic strokes, anticoagulation therapy was contraindicated. She continued to experience moderate cognitive impairment, partial motor aphasia, and recurrence of cardiac myxoma.
To explore a potential clonal relationship between the cardiac and intracranial tumors, we performed exome sequencing on both lesions. In the cardiac myxoma, somatic analysis revealed a loss of heterozygosity (LOH) at chromosome 17q24.2, encompassing the PRKAR1A gene. This alteration resulted in the loss of the wild-type allele, consistent with the tumor suppressor role of PRKAR1A. In contrast, no somatic variants or LOH events were identified in the intracranial lesion. However, this finding should be interpreted with caution, as the brain sample exhibited low tumor cellularity (16%), which limits the sensitivity of exome sequencing for detecting somatic or subclonal alterations. Therefore, the absence of detectable LOH does not definitively rule out a clonal relationship between the two tumors (Figure 3).
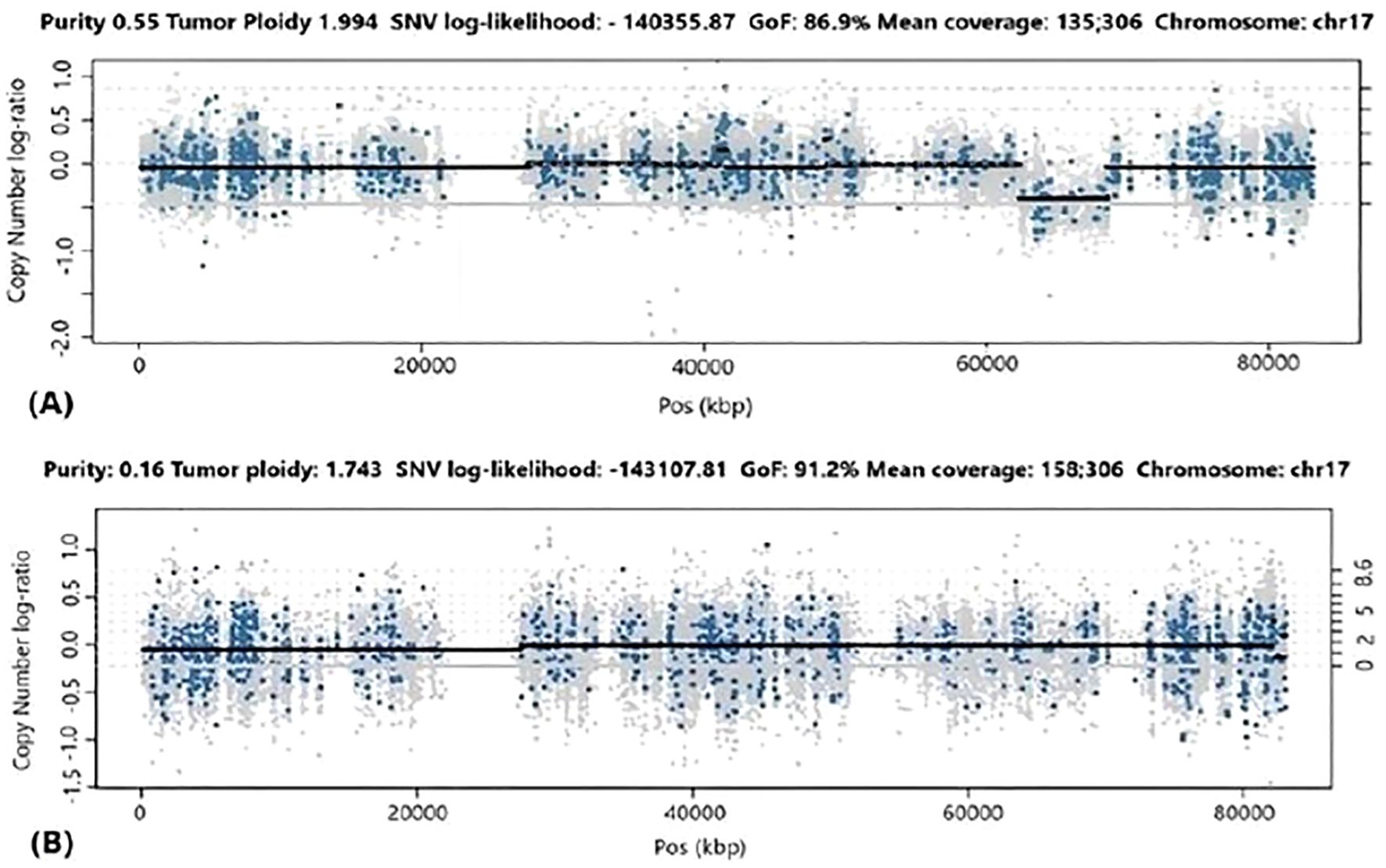
Figure 3. Analysis of Loss of Heterozygosity (LOH) and Copy Number Variation (CNV) on chromosome 17 using PureCN software. (A) Cardiac myxoma: the sample purity was 55%. The plot shows the log of the copy number ratio, indicating a copy number loss in the 17q24.2 region. (B) Cerebral metastasis: the sample purity was 16%. The plot shows the log of the copy number ratio, showing no evidence of LOH or CNV in the 17q24.2 region.
3 Discussion
The clinical manifestations of cardiac myxomas depend on tumor location, size, and morphology (solid or papillary). Left atrial tumors are most common (2) and may obstruct the mitral valve or embolize (7, 9). Constitutional symptoms such as fever, malaise, and weight loss are also frequent, likely mediated by tumor-derived interleukin-6 and other pro-inflammatory cytokines (9–11). Papillary myxomas, characterized by irregular and fragile surfaces, carry a particularly high risk of embolization. Embolic strokes affect 20%–30% of patients, with a predilection for the middle cerebral artery, as observed in our patient (7, 12), as observed in our patient. Women are more frequently affected, and 30%–50% of strokes involve multiple vascular territories (13–15).
Cerebral aneurysms, often fusiform and located in distal arterial branches, are common in patients with embolic myxomas. Although the underlying mechanism remains unclear, proposed hypotheses include occlusion by tumor emboli and subsequent invasion or proliferation within the intima or vasa vasorum, weakening the vessel wall (9, 16, 17). These aneurysms may appear before, during, or long after cardiac tumor diagnosis, displaying variable size and stability, sometimes regressing spontaneously. Most patients are under 60 years of age (18). Approximately 20% of patients with central nervous system (CNS) involvement experience subarachnoid and/or intraparenchymal hemorrhage (15, 19). This relatively low rate of hemorrhage may be due to dense connective tissue formed around the aneurysms, which may confer some protection, in contrast to other neoplastic aneurysms such as those seen in choriocarcinoma (19).
While embolic phenomena are well documented, true parenchymal implantation of myxoma cells is exceedingly rare. Only a limited number of cases describing such occurrences exist in the literature, each with heterogeneous clinical and radiological features (14, 16, 20–57) (Table 2). A comprehensive review by Chatzikonstantinou et al. identified 20 CNC patients with cerebral embolisms secondary to cardiac myxomas, none of whom demonstrated metastatic spread (58). When parenchymal involvement does occur, common symptoms include seizures, headaches, and hemiparesis (59–62). Affected individuals often share several features with patients harboring cardiac myxomas alone: a mean age of 30–40 years, female predominance, tumor origin in the interatrial septum’s oval fossa, and a mean tumor size of 4.6 ± 2.5 cm (59–62). Our patient exhibited many of these features, with the addition of recurrent myxomas, a hallmark of Carney Complex (63, 64).
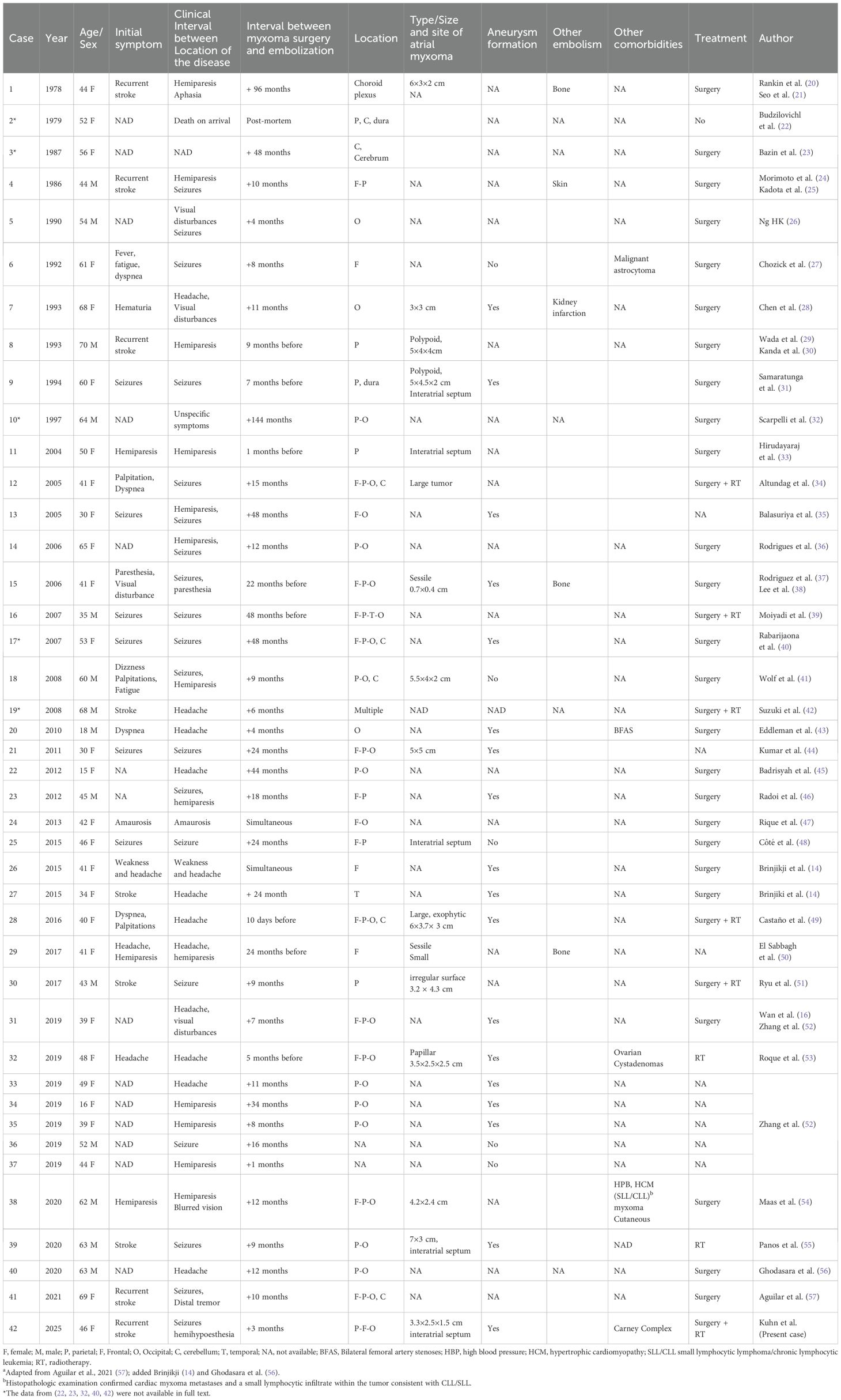
Table 2. Reported cases of histopathologically confirmed cardiac myxoma with metastasis to the brain.a
In most documented cases, brain lesions emerge years after cardiac myxoma resection, with a mean interval of 23.5 months (range: 1–144 months). Interestingly, in approximately 20% of patients, CNS lesions were identified before the cardiac tumor was diagnosed, with a mean lead time of 16.6 months (range: 0.3–48 months) (29–31, 33, 37–39, 49, 50, 53). Simultaneous detection of both conditions is extremely rare and has been reported in only two cases (14, 47).
Surgical resection is the mainstay of treatment for brain. Five cases have combined surgery with radiotherapy, as in our case (34, 39, 42, 49, 51), while only two were treated with radiotherapy alone (53, 55). Although there are concerns regarding the risk of aneurysm rupture after radiotherapy, due to potential weakening of the vessel wall, no hemorrhagic complications were reported among the three patients with aneurysms who underwent radiation therapy (39, 53, 55).
Unlike previous reports that used whole-brain radiotherapy (34, 39, 49, 51, 55), we opted for volumetric modulated arc therapy (VMAT) which allowed for lesion-specific dose boosting and hippocampal sparing, aiming to preserve cognitive function. This approach also limited radiation exposure to intracranial vascular structures, important given the presence of multiple fusiform aneurysms and concerns about radiation-induced vessel wall fragility.
In this case, histopathological analysis confirmed a well-differentiated myxoid neoplasm in the brain, and FDG-PET revealed hypermetabolism with elevated SUVmax values, supporting active neoplastic involvement. These findings reinforce the hypothesis of tumor cell dissemination, likely via embolic pathways, rather than conventional metastatic mechanisms. This contrasts with typical brain metastases, which often involve disruption of the blood-brain barrier by genes that promote migration, extracellular matrix degradation, and vascular permeability (65).
Notably, pathogenic variants in PRKAR1A are not commonly linked to brain metastases (65). A single previous case described molecular alterations in myxoid tissue without germline PRKAR1A mutations, identifying two variants of uncertain significance and two likely pathogenic variants in both cardiac and brain tissue, along with a copy number amplification at the PRKAR1A locus. Although gene amplifications typically involve oncogenes, it was hypothesized that the amplified allele harbored deleterious mutations, potentially explaining the tumorigenesis in that patient (53).
In contrast, our case presents a confirmed clinical and molecular diagnosis of Carney Complex, with two distinct hits in PRKAR1A: a germline pathogenic variant and loss of heterozygosity in the cardiac tumor, consistent with the classic tumor suppressor model. Although we could not assess somatic events in the brain lesion due to low cellularity, this appears to be the first reported case integrating histological, imaging, and genetic data to support a myxomatous brain lesion derived from cardiac origin in a Carney Complex patient. We propose that cardiac myxoma cells can, under specific conditions, disseminate through embolic routes, survive in distal tissues, and proliferate locally, ultimately forming tumors. This case illustrates how histologically benign neoplasms may display aggressive behavior, including distant colonization, particularly in the context of an underlying genetic predisposition.
4 Conclusion
This case highlights the rare but clinically significant complications of cardiac myxomas in Carney Complex, demonstrating that these histologically benign tumors can, under certain circumstances, exhibit aggressive behavior. It underscores the importance of maintaining a high index of suspicion for central nervous system involvement in patients with a history of left atrial myxomas who present with recurrent or unexplained neurological symptoms. The findings support the hypothesis that embolic dissemination may contribute to rare instances of myxomatous brain involvement, expanding our understanding of myxoma pathophysiology. Moreover, this case reinforces the value of integrated molecular and histopathological analysis in elucidating mechanisms of atypical tumor spread. Effective management of such complex presentations requires a multidisciplinary approach encompassing cardiology, neurology, oncology, genetics, and pathology to deliver personalized care.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statement
The studies involving humans were approved by Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo, number 5.687.690. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
AK: Writing – original draft, Writing – review & editing. AML: Software, Formal analysis, Data curation, Resources, Writing – review & editing, Investigation. AM: Investigation, Writing – review & editing. RI: Writing – review & editing, Investigation. FR: Investigation, Writing – review & editing. LM: Writing – review & editing. AH: Investigation, Writing – review & editing. ACL: Writing – review & editing, Investigation. BM: Investigation, Writing – review & editing. MA: Writing – review & editing, Funding acquisition, Investigation, Resources. MF: Writing – review & editing, Investigation, Supervision.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was partially supported by the São Paulo Research Foundation (FAPESP), process number 2019/15873-6 (to MA and MF), and FAPESP fellowship 2022/09278-0 (to AK).
Acknowledgments
We would like to thank the full-time all collaborating fellows: Beatriz Marinho de Paula Mariani, Mirian Yumie Nishi, Felipe Lourenço Ledesma, Leandro Weber Souza, Maria Luísa Sucharski Figueiredo, Fabio Yoshiaki Tanno, Victor Srougi and Jose Luis Chambo.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Shah IK, Dearani JA, Daly RC, Suri RM, Park SJ, Joyce LD, et al. Cardiac myxomas: a 50-year experience with resection and analysis of risk factors for recurrence. Ann Thorac Surg. (2015) 100:495–500. doi: 10.1016/j.athoracsur.2015.03.007
2. Tyebally S, Chen D, Bhattacharyya S, Mughrabi A, Hussain Z, Manisty C, et al. Cardiac tumors: JACC cardioOncology state-of-the-art review. JACC CardioOncol. (2020) 2:293–311. doi: 10.1016/j.jaccao.2020.05.009
3. Carney JA, Gordon H, Carpenter PC, Shenoy BV, and Go VL. The complex of myxomas, spotty pigmentation, and endocrine overactivity. Med (Baltimore). (1985) 64:270–83. doi: 10.1097/00005792-198507000-00007
4. Stratakis CA, Kirschner LS, and Carney JA. Clinical and molecular features of the Carney complex: diagnostic criteria and recommendations for patient evaluation. J Clin Endocrinol Metab. (2001) 86:4041–6. doi: 10.1210/jcem.86.9.7903
5. Bouys L and Bertherat J. Management of endocrine disease: Carney complex: clinical and genetic update 20 years after the identification of the CNC1 (PRKAR1A) gene. Eur J Endocrinol. (2021) 184:R99–R109. doi: 10.1530/EJE-20-1120
6. Espiard S, Vantyghem MC, Assié G, Cardot-Bauters C, Raverot G, Brucker-Davis F, et al. Frequency and incidence of Carney complex manifestations: a prospective multicenter study with a three-year follow-up. J Clin Endocrinol Metab. (2020) 105(2):436–46. doi: 10.1210/clinem/dgaa002
7. Islam AK. Cardiac myxomas: a narrative review. World J Cardiol. (2022) 14:206–19. doi: 10.4330/wjc.v14.i4.206
8. Bertherat J, Horvath A, Groussin L, Grabar S, Boikos S, Cazabat L, et al. Mutations in regulatory subunit type 1A of cyclic adenosine 5′-monophosphate-dependent protein kinase (PRKAR1A): phenotype analysis in 353 patients and 80 different genotypes. J Clin Endocrinol Metab. (2009) 94:2085–91. doi: 10.1210/jc.2008-2333
9. Pinede L, Duhaut P, and Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Med (Baltimore). (2001) 80:159–72. doi: 10.1097/00005792-200105000-00002
10. Yuan SM and Lin HZ. Predictors of normalization of circulating interleukin-6 after cardiac myxoma resection. Braz J Cardiovasc Surg. (2019) 34:22–7. doi: 10.21470/1678-9741-2018-0161
11. Gavrielatos G, Letsas KP, Pappas LK, Dedeilias P, Sioras E, and Kardaras F. Large left atrial myxoma presented as fever of unknown origin: a challenging diagnosis and a review of the literature. Cardiovasc Pathol. (2007) 16:365–7. doi: 10.1016/j.carpath.2007.01.001
12. Basso C, Rizzo S, Valente M, and Thiene G. Cardiac masses and tumours. Heart. (2016) 102:1230–45. doi: 10.1136/heartjnl-2014-306364
13. Zheng Z, Guo G, Xu L, Lei L, Wei X, and Pan Y. Left atrial myxoma with versus without cerebral embolism: length of symptoms, morphologic characteristics, and outcomes. Tex Heart Inst J. (2014) 41:592–5. doi: 10.14503/THIJ-13-3862
14. Brinjikji W, Morris JM, Brown RD, Thielen KR, Wald JT, Giannini C, et al. Neuroimaging findings in cardiac myxoma patients: a single-center case series of 47 patients. Cerebrovasc Dis. (2015) 40:35–44. doi: 10.1159/000381833
15. Rosário M, Fonseca AC, Sotero FD, and Ferro JM. Neurological complications of cardiac tumors. Curr Neurol Neurosci Rep. (2019) 19:15. doi: 10.1007/s11910-019-0931-1
16. Wan Y, Du H, Zhang L, Guo S, Xu L, Li Y, et al. Multiple cerebral metastases and metastatic aneurysms in patients with left atrial myxoma: a case report. BMC Neurol. (2019) 19:249. doi: 10.1186/s12883-019-1474-4
17. Flores PL, Haglund F, Bhogal P, Yeo Leong Litt L, and Södermann M. The dynamic natural history of cerebral aneurysms from cardiac myxomas: a review of the natural history of myxomatous aneurysms. Interv Neuroradiol. (2018) 24:277–83. doi: 10.1177/1591019917754070
18. Chojdak-Łukasiewicz J, Budrewicz S, and Waliszewska-Prosół M. Cerebral aneurysms caused by atrial myxoma-A systematic review of the literature. J Pers Med. (2022) 13:8. doi: 10.3390/jpm13010008
19. Zheng J and Zhang J. Neoplastic cerebral aneurysm from metastatic tumor: a systematic review of clinical and treatment characteristics. Clin Neurol Neurosurg. (2015) 128(1):107–11. doi: 10.1016/j.clineuro.2014.11.010
20. Desousa AL, Muller J, Campbell R, Batnitzky S, and Rankin L. Atrial myxoma: a review of the neurological complications, metastases, and recurrences. J Neurol Neurosurg Psychiatry. (1978) 41:1119–24. doi: 10.1136/jnnp.41.12.1119
21. Seo IS, Warner TF, Colyer RA, and Winkler RF. Metastasizing atrial myxoma. Am J Surg Pathol. (1980) 4:391– 9. doi: 10.1097/00000478-198008000-00008
22. Budzilovich G, Aleksic S, Greco A, Fernandez J, Harris J, and Finegold M. Malignant cardiac myxoma with cerebral metastases. Surg Neurol. (1979) 11:461–9.
23. Bazin A, Peruzzi P, Baudrillard JC, Pluot M, and Rousseaux P. Cardiac myxoma with cerebral metastases. Neurochirurgie. (1987) 33:487–9.
24. Morimoto K, Fujita T, Wakayama A, Miyazaki Y, Kamido H, Imakita T, et al. Cardiac myxoma metastatic to the brain. No to Shinkei. (1986) 38:865–9.
25. Kadota T, Imakita S, Mitomo M, Kawai R, Miura T, Harada K, et al. Metastatic brain tumor of atrial myxoma. Neuroradiology. (1987) 29:218. doi: 10.1007/BF00327560
26. Ng HK and Poon WS. Cardiac myxoma metastasizing to the brain. Case report. J Neurosurg. (1990) 72:295–8. doi: 10.3171/jns.1990.72.2.0295
27. Chozick BS, Ambler MW, and Stoll J. Malignant astrocytoma six years after the resection of a cerebral metastatic cardiac myxoma: case report. Neurosurgery. (1992) 30:923–6. doi: 10.1227/00006123-199206000-00019
28. Chen HJ, Liou CW, and Chen L. Metastatic atrial myxoma presenting as intracranial aneurysms with hemorrhage: case report. Surg Neurol. (1993) 40:61–4. doi: 10.1016/0090-3019(93)90173-x
29. Wada A, Kanda T, Hayashi R, Imai S, Suzuki T, and Murata K. Cardiac myxoma metastasized to the brain: potential role of endogenous interleukin-6. Cardiology. (1993) 83:208–11. doi: 10.1159/000175971
30. Kanda T, Sakamaki T, and Murata K. A cardiac myxoma with interleukin-6 production and cerebral metastasis. Int J Cardiol. (1994) 45:144–6. doi: 10.1016/0167-5273(94)90272-0
31. Samaratunga H, Searle J, Cominos D, and Le Fevre I. Cerebral metastasis of an atrial myxoma mimicking an epithelioid hemangioendothelioma. Am J Surg Pathol. (1994) 18:107–11. doi: 10.1097/00000478-199401000-00011
32. Scarpelli M, Montironi R, Ricciuti R, Vecchioni S, and Pauri F. Cardiac myxoma with glandular elements metastatic to the brain 12 years after the removal of the original tumor. Clin Neuropathol. (1997) 16:190–4.
33. Hirudayaraj P, Arya B, Suvarna SK, Payne G, and Palaniswamy A. Myxomatous meningeal tumour: a case of “metastatic” cardiac myxoma. Int J Cardiol. (2004) 96:471–3. doi: 10.1016/j.ijcard.2003.04.070
34. Altundag MB, Ertas G, Ucer AR, Durmus S, Abanuz H, Calikoğlu T, et al. Brain metastasis of cardiac myxoma: case report and review of the literature. J Neurooncol. (2005) 75:181–4. doi: 10.1007/s11060-005-1859-7
35. Balasuriya BM, Wijesekara JC, and Perera S. An unusual case of focal epilepsy. Ceylon Med J. (2005) 50:30–1. doi: 10.4038/cmj.v50i1.1589
36. Rodrigues D, Matthews N, Scoones D, Aziz F, and Nath F. Recurrent cerebral metastasis from a cardiac myxoma: case report and review of literature. Br J Neurosurg. (2006) 20:318–20. doi: 10.1080/02688690601000394
37. Rodriguez FJ, Brown RD, Mohr JP, Piepgras DG, Thielen K, Blume RS, et al. Embolic atrial myxoma with neoplastic aneurysm formation and haemorrhage: a diagnostic challenge. Neuropathol Appl Neurobiol. (2006) 32:213–6. doi: 10.1111/j.1365-2990.2006.00721.x
38. Lee VH, Connolly HM, and Brown RD. Central nervous system manifestations of cardiac myxoma. Arch Neurol. (2007) 64:1115–20. doi: 10.1001/archneur.64.8.1115
39. Moiyadi AV, Moiyadi AA, Sampath S, Kalpana SR, Mahadevan A, Shankar SK, et al. Intracranial metastasis from a glandular variant of atrial myxoma. Acta Neurochir (Wien). (2007) 149:1157–62. doi: 10.1007/s00701-007-1291-1
40. Rabarijaona M, Penchet G, Adnane B, Loiseau H, and Rougier A. Brain metastasis of cardiac myxoma. Case Rep. (2007) 1:54–6.
41. Wolf M, Wibail A, De Jonghe P, de Barsy C, Van Houwe E, Cras PC, et al. Delayed hemorrhagic cerebral metastases after atrial myxoma resection: report of two cases and review of the literature. Rev Española Cir Ortop Traumatol. (2008) 66:75–9. doi: 10.1016/j.ejrex.2008.04.009
42. Suzuki R, Watanabe T, Hirayama R, Nohata I, Ito K, Baba Y, et al. Case with cardiac myxoma causing cerebral metastasis after cardiac tumor resection. Kyobu Geka. (2008) 61:456–9.
43. Eddleman CS, Gottardi-Littell NR, Bendok BR, Batjer HH, and Bernstein RA. Rupture of cerebral myxomatous aneurysm months after resection of the primary cardiac tumor. Neurocrit Care. (2010) 13:252–5. doi: 10.1007/s12028-010-9400-z
44. Kumar A, Deopujari CE, and Karmarkar VS. A rare diagnosis of multiple hemorrhagic metastases in brain. J Postgrad Med. (2011) 57:214–7. doi: 10.4103/0022-3859.85210
45. Badrisyah I, Saiful R, Rahmat H, Naik VR, and Tan YC. Brain Metastasis of Atrial myxoma: case report. Med J Malaysia. (2012) 67:613–5.
46. Radoi MP, Stefanescu F, and Arsene D. Brain metastases and multiple cerebral aneurysms from cardiac myxoma: case report and review of the literature. Br J Neurosurg. (2012) 26:893–5. doi: 10.3109/02688697.2012.692841
47. Riqué JP, Sánchez R, Ortega J, and Calvo M. Metástasis cerebral de mixoma cardíaco reporte de un caso y revisión literaria. Rev Argent Neuroc. (2013) 27:140–2.
48. Côté I, Sinclair J, Woulfe J, Glikstein R, and Veinot J. Cerebral metastasis presenting after complete primary resection of atrial myxoma: case report. Can J Neurol Sci. (2015) 42:457–60. doi: 10.1017/cjn.2015.293
49. Castaño-Leon AM, Hernandez-Lain A, Maroñas L, López P, Ayuso LL, Ramos A, et al. Pathology- confirmed cerebral arterial invasion and recurrent multiple brain metastasis from cardiac myxoma without evidence of disease after surgery and radiotherapy. Clin Neuropathol. (2016) 35:84–8. doi: 10.5414/NP300900
50. El Sabbagh A, Al-Hijji MA, Thaden JJ, Pislaru SV, Pislaru C, Pellikka PA, et al. Cardiac myxoma: the great mimicker. JACC Cardiovasc Imaging. (2017) 10:203–6. doi: 10.1016/j.jcmg.2016.06.018
51. Ryu JC, Kwon JH, Lee DY, Yang DS, Kim WJ, and Kim M. Cerebral metastatic myxoma in a cerebral infarction patient after complete resection of cardiac myxoma. J Korean Neurol Assoc. (2017) 35:254–6. doi: 10.17340/jkna.2017.4.17
52. Zhang S, Zhang Q, Yu H, Liu L, Sun R, Song X, et al. Neuroimaging characteristics and long-term prognosis of myxoma-related intracranial diseases. Neuroradiology. (2020) 62:307–17. doi: 10.1007/s00234-019-02314-w
53. Roque A, Kimbrough T, Traner C, Baehring JM, Huttner A, Adams J, et al. Somatic PRKAR1A mutation in sporadic atrial myxoma with cerebral parenchymal metastases: a case report. J Med Case Rep. (2019) 13:389. doi: 10.1186/s13256-019-2317-z
54. Maas JA, Menes M, and Siomin V. Cardiac myxoma with cerebral metastases and chronic lymphocytic leukemia/small lymphocytic lymphoma: a case report and review. J Neurol Surg Rep. (2020) 81:e1–6. doi: 10.1055/s-0039-3399570
55. Panos LD, Brunel C, Berezowska S, Engisch R, Kollar A, Bassetti C, et al. Early and delayed neurological manifestations of cardiac myxomas. Clin Neurol Neurosurg. (2020) 190:105673. doi: 10.1016/j.clineuro.2020.105673
56. Ghodasara SA, Balasubramanian R, Varadharajan S, and Shobhanaa PS. Cardiac phoenix in the brain-occult intracranial hemorrhagic metastases from completely resected atrial myxoma. Surg Neurol Int. (2020) 11:383. doi: 10.25259/SNI_410_2020
57. Aguilar C, Carbajal T, Beltran BE, Segura P, Muhammad S, and Choque-Velasquez J. Cerebral embolization associated with parenchymal seeding of the left atrial myxoma: potential role of interleukin-6 and matrix metalloproteinases. Neuropathology. (2021) 41:49–57. doi: 10.1111/neup.12697
58. Chatzikonstantinou S, Kazis D, Giannakopoulou P, Poulios P, Pikou O, Geroukis T, et al. Carney complex syndrome manifesting as cardioembolic stroke: a case report and review of the literature. Int J Neurosci. (2022) 132:649–55. doi: 10.1080/00207454.2020.1834393
59. Yoon DH and Roberts W. Sex distribution in cardiac myxomas. Am J Cardiol. (2002) 90:563–5. doi: 10.1016/s0002-9149(02)02540-7
60. Poterucha TJ, Kochav J, O’Connor DS, and Rosner GF. Cardiac tumors: clinical presentation, diagnosis, and management. Curr Treat Options Oncol. (2019) 20:66. doi: 10.1007/s11864-019-0662-1
61. Dias RR, Fernandes F, Ramires FJ, Mady C, Albuquerque CP, and Jatene FB. Mortality and embolic potential of cardiac tumors. Arq Bras Cardiol. (2014) 103:13–8. doi: 10.5935/abc.20140096
62. He DK, Zhang YF, Liang Y, Ye SX, Wang C, Kang B, et al. Risk factors for embolism in cardiac myxoma: a retrospective analysis. Med Sci Monit. (2015) 21:1146–54. doi: 10.12659/MSM.893855
63. Pitsava G, Zhu C, Sundaram R, Mills JL, and Stratakis CA. Predicting the risk of cardiac myxoma in Carney complex. Genet Med. (2021) 23:80–5. doi: 10.1038/s41436-020-00956-3
64. Wei K, Guo HW, Fan SY, Sun XG, and Hu SS. Clinical features and surgical results of cardiac myxoma in Carney complex. J Card Surg. (2019) 34:14–9. doi: 10.1111/jocs.13980
Keywords: brain tumor, emboli, cardiac myxoma, Carney complex, case report
Citation: Kuhn AW, Lerario AM, Morais ANR, Iglesio RF, Ramires FJA, Maluf LCA, Hoff AO, Latronico AC, Mendonça BB, Almeida MQ and Fragoso MCBV (2025) Case Report: Cardiac myxomas and Carney complex: a case of recurrent embolic strokes and intracranial tumor growth. Front. Oncol. 15:1605692. doi: 10.3389/fonc.2025.1605692
Received: 03 April 2025; Accepted: 06 June 2025;
Published: 26 June 2025.
Edited by:
Marta Waliszewska-Prosół, Wroclaw Medical University, PolandReviewed by:
Justyna Chojdak-Łukasiewicz, Wroclaw Medical University, PolandCristina Filip, Maria Sklodowska Curie Hospital for Children, Romania
Copyright © 2025 Kuhn, Lerario, Morais, Iglesio, Ramires, Maluf, Hoff, Latronico, Mendonça, Almeida and Fragoso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria C. B. V. Fragoso, bWFyaWEudmlsbGFyZXNAaGMuZm0udXNwLmJy