 Liudmila Belevskaia1†
Liudmila Belevskaia1† Florian von Borell
Florian von Borell Ulrich Baumann
Ulrich Baumann Rita Beier
Rita Beier Harald Köditz
Harald Köditz- 1Department of Pediatric Cardiology and Intensive Care Medicine, Hannover Medical School, Hannover, Germany
- 2Department of Paediatric Pulmonology and Neonatalogy, Hannover Medical School, Hannover, Germany
- 3Department of Pediatric Hematology and Oncology, Hannover Medical School, Hannover, Germany
Background: Extracorporeal membrane oxygenation (ECMO) is increasingly being utilized in pediatric patients with severe respiratory failure, extending its use to high-risk patients, including those who are immunocompromised. Despite its growing application, reports on outcomes and prognostic factors in this specific population are scarce, highlighting a gap in our understanding.
Methods: This retrospective cohort study analyzed the outcomes of 19 immunocompromised pediatric patients who received ECMO for respiratory failure at our institution between 2006 and 2023. Patients were classified as immunocompromised due to conditions such as cancer, hematopoietic cell transplantation (HCT), primary immunodeficiency or receiving immunosuppression for a chronic (auto-) inflammatory disease. Data on patient demographics, baseline laboratory and ventilation parameters were collected and compared between survivors and non-survivors.
Results: The median age of patients was 12.1 years, and the majority suffered from infectious pneumonia leading to respiratory failure. The median duration of ventilation before ECMO was 5 days, and ECMO support lasted a median of 19 days. The hospital mortality rate in this cohort was 74% (14/19). All patients who had undergone HCT or a primary immunodeficiency did not survive. Non-survivors exhibited significantly higher median C-reactive protein levels and more bleeding complications. Other laboratory and respiratory parameters, as well as vasopressor requirements, pSOFA, and P-PREP scores, were similar across survivors and non-survivors.
Conclusion: The treatment of immunocompromised pediatric patients with ECMO for respiratory failure presents notable challenges. This study highlights the complexity of predicting outcomes in this group, as traditional laboratory and respiratory parameters were not distinctly different between survivors and non-survivors. These findings indicate a need for continued research and nuanced clinical approaches to improve care and outcomes in this vulnerable population.
1 Introduction
Extracorporeal membrane oxygenation (ECMO) is well recognized as a valuable therapeutic option for children with severe respiratory failure, particularly when mechanical ventilation fails to maintain essential gas exchange (1, 2). This is evidenced by an increase in ECMO utilization over the past two decades and can be attributed to technological advancements and achievements in critical care (3). Alongside these developments, the indications for ECMO have expanded, increasingly encompassing higher-risk groups, including historic contraindications like immunosuppression (4–6).
A compromised immune system is a well-recognized risk factor associated with higher mortality in patients receiving ECMO support (7–9). Notably, the reported survival rate for immunocompromised children on ECMO therapy ranges between 30-40%, which is substantially lower than the reported 69% overall survival rate for children receiving respiratory ECMO support in recent years (7, 10–14).
The prognosis for children receiving ECMO following hematopoietic cell transplantation (HCT) tends to be particularly poor, underscoring the imperative for cautious and thoughtful application of ECMO in this patient subgroup (6, 15). Recent trends indicate an improvement in the prognosis for immunocompromised pediatric patients needing ECMO support (16). This has contributed to a growing acceptance of ECMO in situations where the treatment trajectory appears more favorable (17, 18).
The decision to initiate ECMO for respiratory failure in immunocompromised patients is complex and must be individualized, considering the prognosis of the underlying disease and the severity of acute complications leading to respiratory failure (18–20). It necessitates a nuanced understanding of the disease, its prognosis, and the patient’s individual risk profile to optimize patient selection.
Our study aims to contribute to this evolving field by characterizing the outcomes of immunocompromised children who received ECMO therapy for respiratory failure at our institution. Through this analysis, we seek to enhance the understanding of this unique patient population and provide a stronger foundation for future patient selection and management strategies.
2 Material and methods
For this retrospective cohort single center study, we included all patients younger than 18 years of age who were admitted to the pediatric intensive care unit (PICU) of the Hannover Medical School with a compromised immune status and who received ECMO for respiratory failure. We included all admissions between 2006 and October 2023. We defined patients as immunocompromised if one of the following entities was present at ECMO initiation: I) immunosuppressive treatment after HCT; II) received chemotherapy for hematological malignancy or solid tumor prior to ECMO initiation and/or neutropenia (<500/µl); III) immunosuppressive treatment for > 30 days for an autoimmune disease, solid organ transplant or other inflammatory diseases IV) primary immunodeficiency (PID). To be considered as immunosuppression corticosteroid doses had to exceed 0.5 mg/kg/d for more than 30 days directly preceding ECMO initiation (21). For the purposes of this study, chemotherapy refers to the administration of cytotoxic, antineoplastic agents for cancer-directed treatment.
Patients would be allocated to ECMO following institutional regulations based on the Extracorporeal Life Support Organization (ELSO) guideline for pediatric respiratory failure (1). Patients requiring ECMO for respiratory failure were cannulated in a veno-venous (VV) configuration, veno-arterial (VA)-ECMO was applied only in cases of additional cardiac failure or when patient anatomy would not allow for VV-cannulation. Cannulation sites were jugular and/or femoral due to individual patient anatomy and vessel size. Weaning from ECMO was performed in accordance with the ELSO guidelines (4).
The primary outcome was survival to hospital discharge, but data including 6-month survival as well as baseline parameters prior to ECMO initiation and ECMO-related complications will also be reported.
All patient-related data was derived from the electronic patient data management system used by the PICU. Recorded data included age, weight, diagnosis, reason for respiratory failure, type of immunosuppression, treatment specifications. Furthermore, ECMO mode, runtimes and complications as defined by ELSO (22), respiratory parameters, and laboratory data were recorded. The vasoactive-inotropic score (VIS) was calculated to compare vasoactive medication between patients (23). The time point immediately before the start of ECMO treatment was referred to as the baseline. Baseline data were recorded for the hour immediately before ECMO cannulation. The pediatric Sequential Organ Failure Assessment score (pSOFA) as well as the Pediatric Pulmonary Rescue with Extracorporeal Membrane Oxygenation Prediction score (P-PREP) were calculated at baseline to estimate severity of illness and to predict mortality after ECMO initiation (24, 25).
Data were summarized using frequencies and percentages for categorical variables and median and interquartile range (IQR) for continuous variables. Data were compared between survivors and non-survivors using Fisher’s exact test for dichotomous variables and the Wilcoxon rank sum test for continuous variables. Differences were considered statistically significant when p value was less than 0.05. Statistical tests were performed using R software version 4.0.3, “Bunny-Wunnies Freak Out”, copyright 2020, The R Foundation for Statistical Computing.
The study complied with the Declaration of Helsinki, ethical approval for this study was waived by the ethics committee of Hannover Medical School.
3 Results
Between 2006 and 2023 we identified 19 patients who received ECMO for respiratory failure and were categorized as high-risk patients being immunocompromised. The median age at admission was 12.1 years, ranging from 5 month to 17 years of age. A total of 9 patients had a history of malignant disease; 5 were receiving chemotherapy at ECMO initiation. Of the remaining oncology patients, 3 had undergone HCT, and one had monomorphic PTLD after liver transplantation. In total, 4 patients received HCT, including one with thalassemia. Rituximab was administered in 3 patients: the one with PTLD, one for kidney transplant rejection, and one for induction therapy in granulomatosis with polyangiitis. Long-term corticosteroid use was present in 3 patients (including one post-lung transplant), and 4 patients had PID (Table 1). The majority of patients (15/19) suffered from infectious pneumonia with identified pathogens causing respiratory failure.
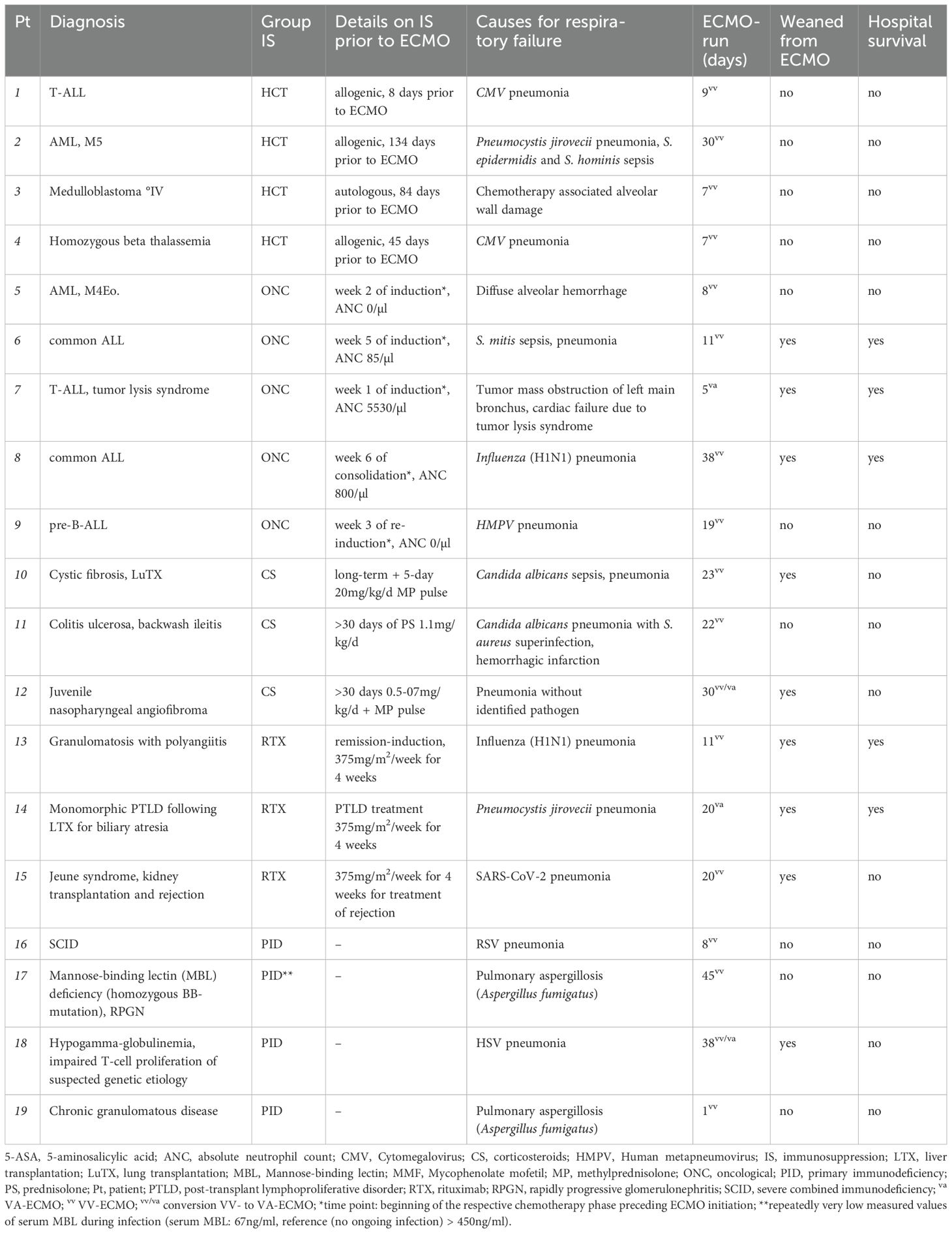
Table 1. Patient characteristics.
Initial cannulation strategy was veno-arterial (VA) in 2 patients and veno-venous (VV) in 17 patients of whom 2 got converted to VA during the ECMO-run. Initial VA-ECMO was chosen for one patient due to combined cardiac and respiratory failure and for another due to anatomical barriers for VV cannulation. All patients were intubated prior to commencement of ECMO and had a median ventilation time of 5 days (IQR: 1–11 days) before cannulation. The median duration of ECMO support was 19 days (IQR: 8–27 days). In total, 10/19 (53%) patients could not be weaned from ECMO, and 14/19 (74%) patients did not survive the hospital stay. The median length of PICU stay was 26 days (IQR: 12–46 days). All 5 patients who survived to hospital discharge were still alive 6 months later. All 4 patients after HCT failed to wean from ECMO. Of the 4 patients with primary immunodeficiency only 1 was successfully weaned from ECMO but deceased before discharge from hospital. All patients are characterized in Table 1, and survival probability within the subgroups is displayed in Figure 1.
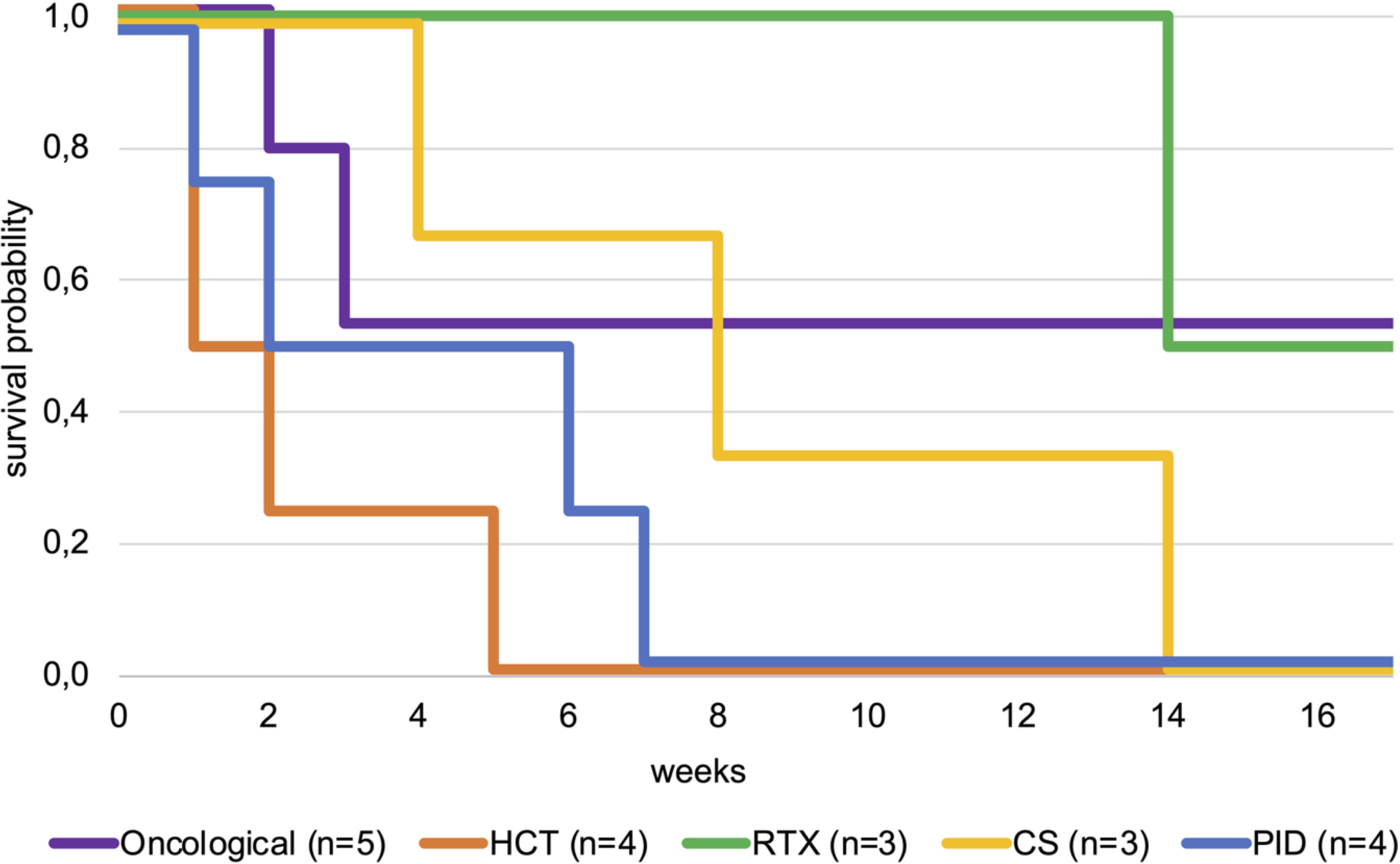
Figure 1. Kaplan-Meier plot comparing survival probability until discharge for patients after HCT, oncological patients (without history of HCT), patients receiving rituximab or corticosteroids and patients with primary immunodeficiency. CS, corticosteroids; HCT, hematopoietic cell transplantation; PID, primary immunodeficiency; RTX, rituximab.
When comparing survivors at hospital discharge and non-survivors (Table 2), median C-reactive protein (CRP) was significantly higher in the non-survivor group (57 mg/L vs. 198 mg/L; p = 0.03). Regarding other baseline laboratory parameters, there were no significant differences in white blood cell count, hemoglobin levels, platelet count, creatinine, pH or lactate levels between the groups. Baseline respiratory parameters like positive end-expiratory pressure (PEEP), peak inspiratory pressure (PIP), mean airway pressure (Pmean), Oxygenation Index (OI), carbon dioxide partial pressure (pCO2), arterial oxygen partial pressure (PaO2), and ventilation duration prior to ECMO were similar across both groups. Moreover, neither vasopressor requirements expressed by VIS score nor the pSOFA or P-PREP score differed significantly. Neither the duration of ECMO support nor the length of PICU stay differed significantly between survivors and non-survivors, with the latter being 31 vs. 21.5 days, respectively (p = 0.49). Non-survivors had more bleeding complications (20% vs. 79%; p = 0.04) and a higher total number of complications (1 vs. 3.5, p = 0.048) during ECMO support. There was no significant difference in age or weight.
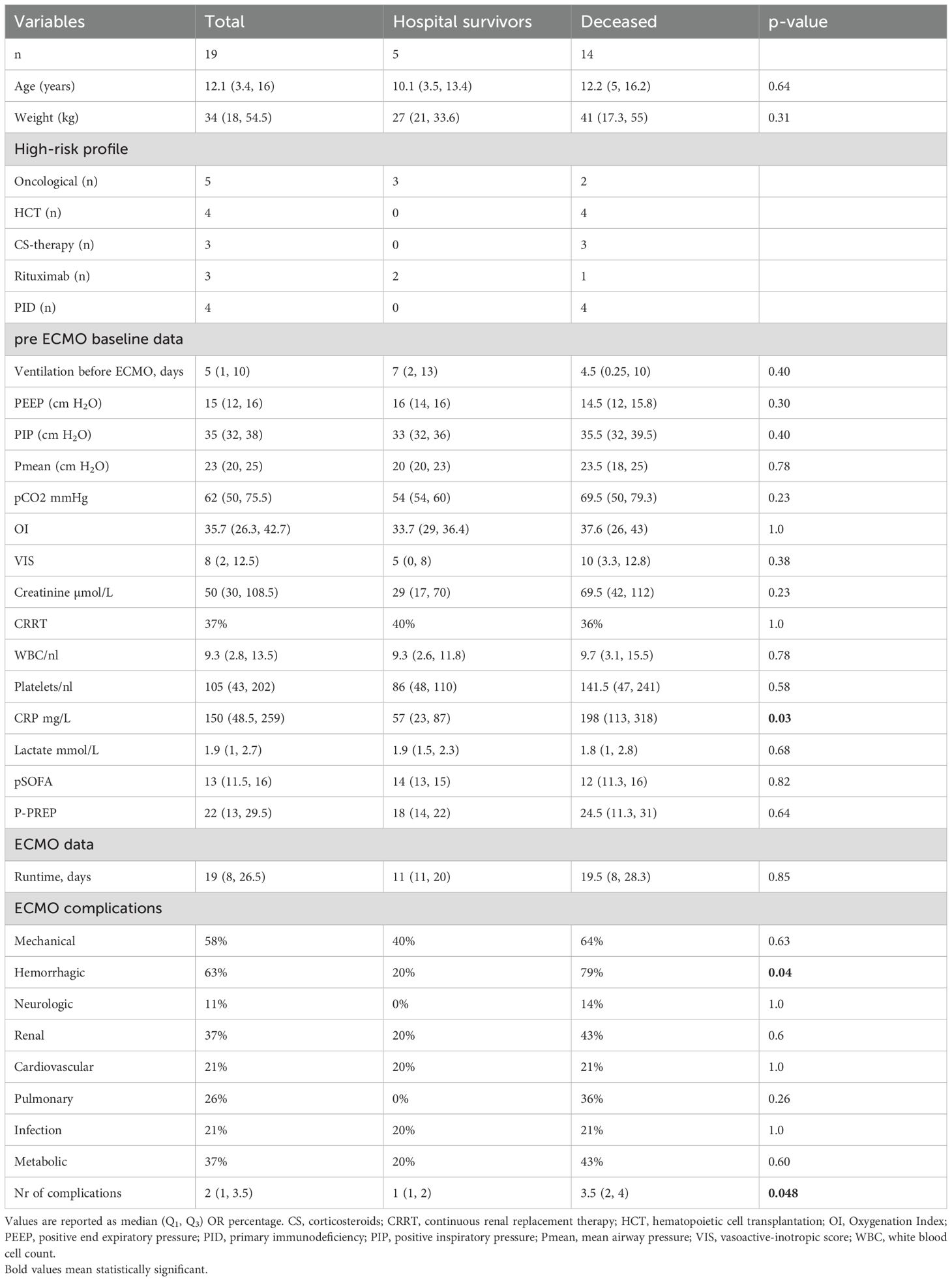
Table 2. Comparing patient data of survivors at hospital discharge and deceased.
Furthermore, no significant differences in baseline data, including CRP, were observed between the 9 patients who were successfully weaned from ECMO and those who were not (Table 3).
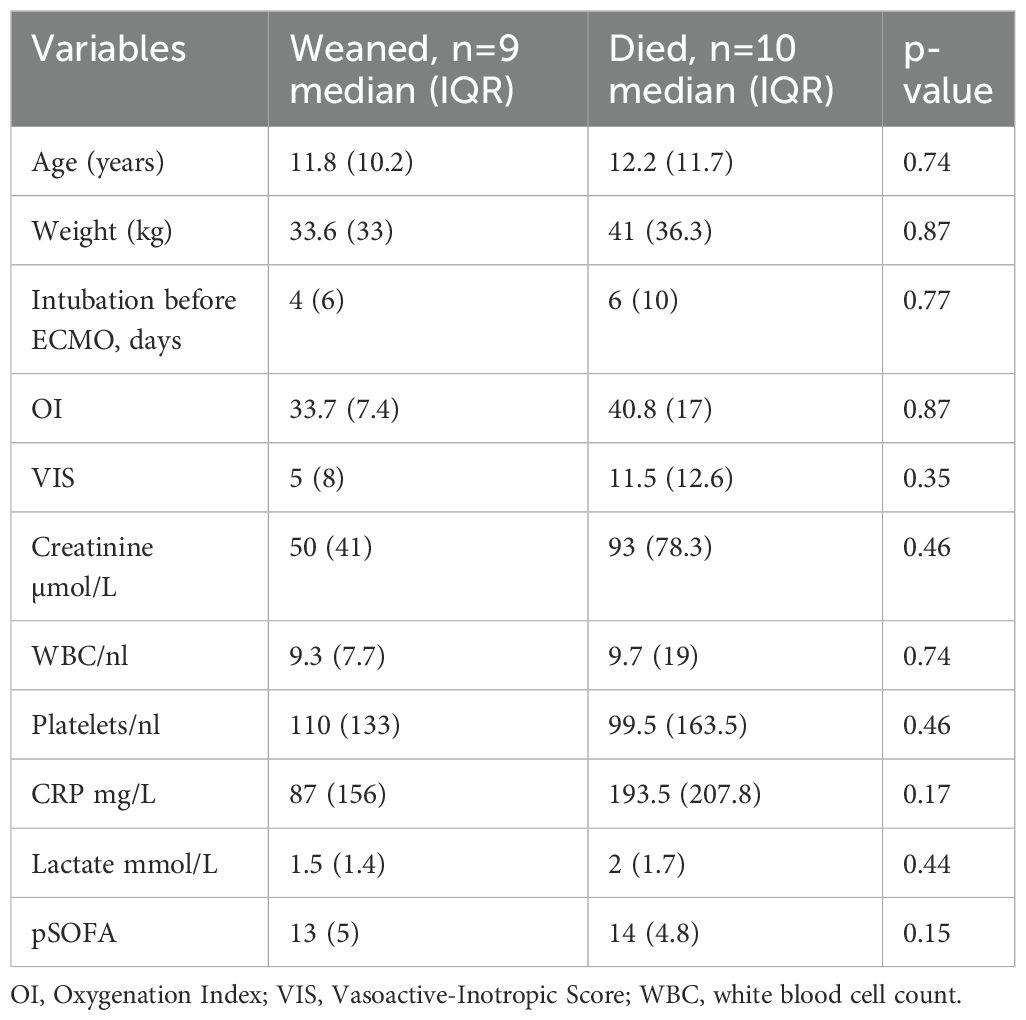
Table 3. Comparing patients who were successfully weaned from ECMO to patients who died on ECMO.
As displayed in Table 4, all patients who survived until discharge lived and were thriving 6 months later. The causes of death for the 14 deceased patients are summarized in Table 5.
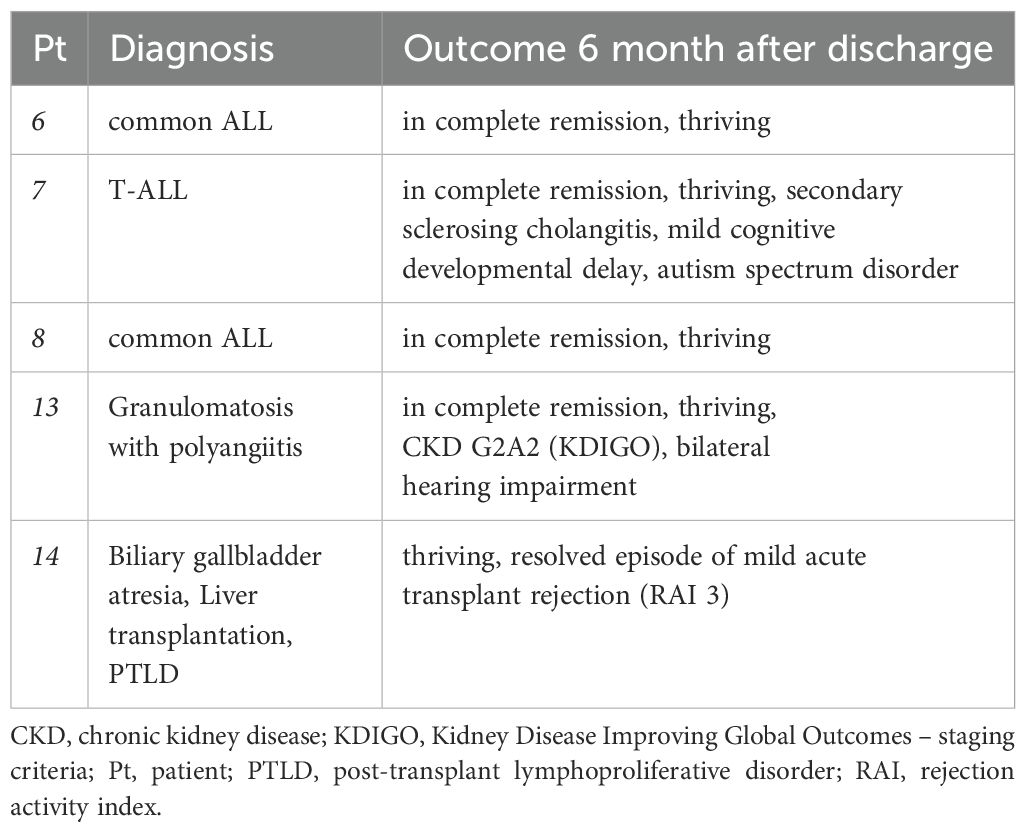
Table 4. Survivors’ outcomes at 6 months after discharge.
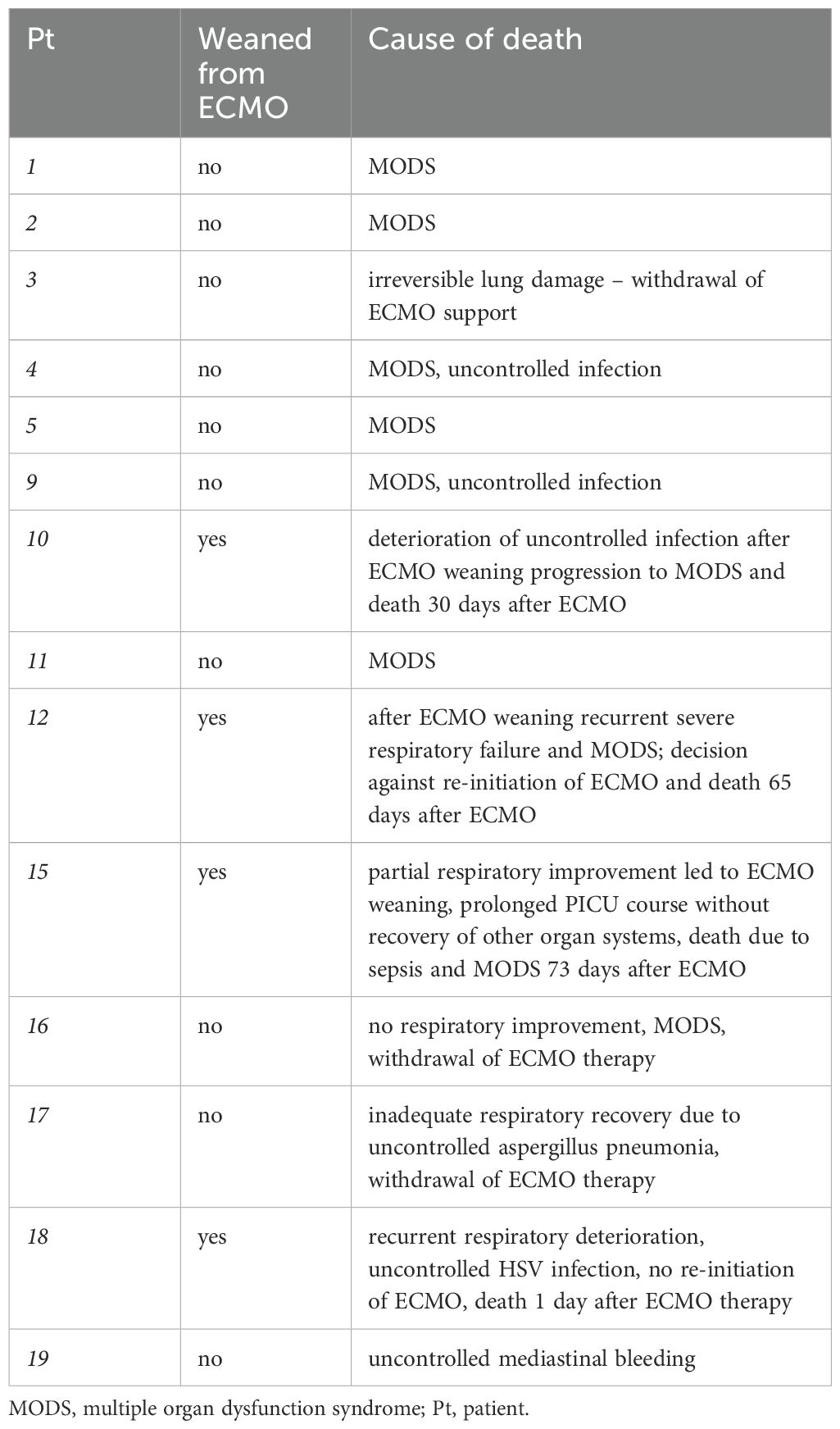
Table 5. Causes of death.
4 Discussion
ECMO is a recognized and recommended option for children experiencing acute respiratory failure and inadequate gas exchange while maintaining lung protective ventilation (2, 26). The indications and scenarios for ECMO support are expanding, and being immunocompromised is no longer considered a clear contraindication in pediatric respiratory failure (1). However, it has been demonstrated that a compromised immune system independently poses a high-risk factor for a worse prognosis and higher mortality during ECMO treatment (1, 8, 14). In this study, we present the cases of 19 consecutive pediatric immunocompromised patients who underwent ECMO for acute respiratory failure. The mortality rate in our cohort reached 73.7%, which aligns with findings in both adult and pediatric patients, where mortality rates around 60-70% have been reported (8, 9, 11, 27). Conversely, the ELSO database indicates a lower overall mortality rate of around 40% for pediatric respiratory ECMO runs during the same period as our study, which corresponds with the overall mortality rate observed at our institution (5, 10).
A monocentric retrospective study conducted in France, which included 111 children treated with ECMO, revealed significantly lower 6-month survival rates (42% vs. 63%) for immunocompromised patients compared to non-immunocompromised patients (7). No significant differences in baseline laboratory or ventilator data were observed between these two groups.
We could not identify prospective studies comparing pediatric immunocompromised ECMO survivors to non-survivors. Nevertheless, a retrospective analysis by Gow et al. using data from the ELSO registry focused on immunocompromised children with malignancies and reported a 35% survival rate to hospital discharge (13). Patients undergoing HCT prior to ECMO therapy were excluded from the analysis. Non-survivors had lower PaO2 and higher OI levels before ECMO therapy. In our patient cohort deceased patients had higher mean- and inspiratory ventilation pressures as well as higher OIs and higher pCO2 levels before ECMO initiation. The differences between the groups were rather small and not statistically significant. In contrast to Gow et al. we found non-survivors to have significantly higher CRP values before initiation of ECMO. It is worth noting that systemic infection with elevated CRP values may pose a risk factor for mortality, particularly in immunocompromised patients undergoing ECMO. Prior studies have demonstrated that immunocompromised children or those who have undergone HCT and develop severe sepsis or septic shock face a significantly higher risk of PICU mortality (28). Furthermore, pre-existing and acquired infections are associated with failure to wean from ECMO (29, 30). In our small cohort no single parameter at baseline was significantly associated with weaning failure from ECMO. Notably, CRP levels - which were significantly correlated with mortality at hospital discharge - were higher (median 87, IQR 157 vs. 193.5, IQR 207.8) in patients who failed to wean from ECMO compared to successfully weaned patients, though the difference did not reach statistical significance.
Consistent with the findings of Gow et al., non-survivors experienced more bleeding complications, as defined by ELSO criteria: a need for more than 20 ml/kg of packed red blood cell transfusion per day or the requirement for surgical or endoscopic intervention (13). However, this was not associated with baseline platelet levels, which were higher in non-survivors. During the ECMO course, platelet counts were maintained above an age-dependent threshold. Bleeding complications are known to be common in pediatric ECMO patients—particularly in immunocompromised individuals—and have been associated with increased morbidity and mortality (7, 9, 31). Bleeding complications may be attributed not only to ECMO and the anticoagulation required to maintain circuit patency, but also to the severity of the underlying illness, including coagulopathy, mucosal vulnerability, and organ dysfunction (e.g. liver failure). In our study the most frequently affected bleeding sites were the oropharynx and the cannulation site. Furthermore, the total number of complications was higher in non-survivors in our study, consistent with reports from the ELSO registry indicating a correlation between complications during the ECMO run and higher mortality rates (5).
Unfortunately, all four patients in our cohort who underwent ECMO therapy after HCT could not be weaned from ECMO. Children after HCT are known to face particularly high risks of poor outcomes, with reported survival rates below 30% (6, 15, 32, 33). Some studies, however, have reported improving PICU and ECMO survival rates in HCT patients over the last two decades (16, 33–35). However, all studies are of retrospective nature, have a small simple size and the improvement is from 10-20% survival 20 years ago to about 30% in the last decade. This is in contrast with our also small and retrospective cohort. The four HCT patients in our cohort were admitted between 2010 and 2019 and were placed on ECMO between 8 and 134 days after HCT. Due to reported high mortality risk and center experience children who received HCT are reluctantly placed on ECMO at our institution. Nevertheless, two recently published consensus statements on ECMO in children receiving HCT strongly recommend considering ECMO in children with non-malignant diseases or with low-risk malignancies and a reasonable expectation of disease-free survival, provided that the critical illness is expected to resolve within a reasonable time frame (18, 20). The authors emphasize the complexities in evaluating ECMO candidacy in pediatric HCT patients, noting the need for comprehensive consideration of factors like disease type, current critical illness, organ reserve, and complications. The complexity of the disease course and significant co-morbidities in high-risk patients like those post-HCT makes predicting outcomes particularly challenging. This further complicates the decision-making process for ECMO candidacy. Acknowledging the improvements over the last decade, ECMO might be a viable option for patients following HCT. However, the diverse spectrum of underlying diseases, patient variability, and the lack of definitive baseline parameters for outcome prediction necessitate a cautious, multidisciplinary, and individualized decision-making process.
All four patients in our cohort who had an underlying primary immunodeficiency (PID) died and three out of four failed to be weaned from ECMO. The severe course, due to the opportunistic infection, was exacerbated in patients 18 and 19 by immune deficiency-associated hyperinflammation. Both patients exhibited a comparatively high inflammatory response at the time of ECMO initiation. Zabrocki et al. reported an odds ratio of 2.35 for mortality in patients with PID requiring ECMO compared to patients without PID (12). A recently published report from the ELSO registry on children with PID who underwent ECMO therapy between 1993 and 2018 showed a survival-to-discharge rate of 45.2% which is higher than overall survival rates reported in the mixed cohort of patients with primary and secondary immunodeficiencies (36). Interestingly neither pre-ECMO infection nor infectious complication during ECMO were associated with non-survival. Moreover, no other reported pre-ECMO baseline parameter was significantly correlated with mortality. However, the occurrence of complications during the ECMO run was significantly associated with mortality.
Our study included 9 patients diagnosed with cancer. Among the cancer patients who did not undergo HCT, 67% (4 out of 6) survived to discharge and were still alive six months after ECMO therapy. Recent meta-analyses on pediatric cancer patients report a 28% PICU mortality rate and a 55% mortality rate in those who received ECMO (37, 38). Therefore, as in our cohort, mortality for pediatric cancer patients appears to be better compared to other immunocompromised patients but worse than for non-immunocompromised patients. However, it is important to note, that estimated mortality rates alone should not be the sole criteria for ECMO allocation to individual immunocompromised patients. Despite the high mortality rate of 74% in our cohort, the five survivors are still alive and experience reasonable health-related quality of life. Four out of five patients have good neurologic outcomes. One patient has a pre-existing severe autism spectrum disorder, the same patient is also suffering from secondary sclerosing cholangitis.
The five survivors did not significantly differ from the non-survivors in any of the baseline parameters except for CRP levels. Although not statistically significant, patients who died showed a trend towards higher vasopressor usage and creatinine levels. Aligned with previously published data the P-PREP score failed to distinguish survivors from non-survivors (32). The P-PREP score was developed and validated to predict mortality in pediatric patients requiring ECMO for respiratory failure (25). It incorporates ventilator and blood gas parameters, which in our cohort did not differ significantly. Furthermore, patients with oncologic diagnoses are categorized into higher-risk groups within the score, although this group showed comparatively favorable outcomes in our study. In contrast, patients with poor outcomes in our cohort—such as those with primary immunodeficiencies—are not specifically accounted for in the score’s risk stratification.
The pSOFA score has been developed to discriminate in-hospital mortality in septic children and has not yet been validated for its use in ECMO (24). A higher SOFA score has been shown to be a risk factor for mortality in adult patients requiring ECMO therapy for cardiac failure as well as respiratory failure due to COVID-19 infection (29, 39). The design of the pSOFA score—which was developed to quantify sequential organ failure in sepsis rather than severe respiratory failure in the complex context of immunodeficiency—may explain its lack of discrimination between survivors and non-survivors in our study. Consequently, there is no established guideline or parameter in the literature to guide ECMO allocation for immunocompromised pediatric patients. Therefore, a case-by-case decision is necessary. For some patients, ECMO could serve as a bridge to responding to the underlying disease treatment, enabling therapy for patients with a reasonable long-term prognosis.
This study presents several noteworthy limitations. Firstly, it is based on a relatively small and heterogeneous group of patients, potentially restricting the generalizability of our findings. The limited sample size might have reduced our ability to detect statistically significant differences or associations. Secondly, as a single-center study, there is a possibility that the results may not fully represent a broader population. Furthermore, the inclusion of patients with various indications for ECMO support introduces variability in patient characteristics and outcomes. The 17-year timespan of our study likely encompasses changes in ECMO technology, patient management, and center-specific experience. Additionally, we were unable to gather long-term follow-up data, such as information on functional, psychological, or social outcomes for both patients and their families. This kind of data could have offered valuable insights into the extended effects of ECMO therapy. In summary, due to the wide spectrum of diseases and the limited number of patients included in the study, drawing further definitive conclusions is not feasible. These limitations should be taken into consideration when interpreting the study’s results and implications discussed in the corresponding section.
Other relationships that might be perceived by the academic community as representing a potential conflict of interest must be disclosed. If no such relationship exists, authors will be asked to confirm the following statement:
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Hannover Medical School Hannover, Hannover, Germany. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
LB: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. FV: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. UB: Supervision, Validation, Writing – review & editing. RB: Supervision, Validation, Writing – review & editing. HK: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Maratta C, Potera RM, Van Leeuwen G, Castillo Moya A, Raman L, and Annich GM. Extracorporeal life support organization (ELSO): 2020 pediatric respiratory ELSO guideline. ASAIO J. (2020) 66:975–9. doi: 10.1097/MAT.0000000000001223
2. Rambaud J, Barbaro RP, Macrae DJ, and Dalton HJ. Extracorporeal membrane oxygenation in pediatric acute respiratory distress syndrome: from the second pediatric acute lung injury consensus conference. Pediatr Crit Care Med. (2023) 24:S124–34. doi: 10.1097/PCC.0000000000003164
3. Cai T, Swaney E, Van Den Helm S, Brown G, Maclaren G, Horton S, et al. The evolution of extracorporeal membrane oxygenation circuitry and impact on clinical outcomes in children: A systematic review. ASAIO J. (2023) 69:247–53. doi: 10.1097/MAT.0000000000001785
4. Maclaren G, Brodie D, Lorusso R, Peek G, Thiagarajan R, Vercaemst L, et al. Extracorporeal Life Support: The ELSO Red Book. 6th. USA: ELSO (2022).
5. Barbaro RP, Paden ML, Guner YS, Raman L, Ryerson LM, Alexander P, et al. Pediatric extracorporeal life support organization registry international report 2016. ASAIO J. (2017) 63:456. doi: 10.1097/MAT.0000000000000603
6. Coleman RD, Goldman J, Moffett B, Guffey D, Loftis L, Thomas J, et al. Extracorporeal membrane oxygenation mortality in high-risk populations: an analysis of the pediatric health information system database. ASAIO J. (2020) 66:327–31. doi: 10.1097/MAT.0000000000001002
7. Robert B, Guellec I, Jegard J, Jean S, Guilbert J, Soreze Y, et al. Extracorporeal membrane oxygenation for immunocompromised children with acute respiratory distress syndrome: a French referral center cohort. Minerva Pediatr. (2022) 74:537–44. doi: 10.23736/S2724-5276.20.05725-4
8. Rilinger J, Zotzmann V, Bemtgen X, Rieg S, Biever PM, Duerschmied D, et al. Influence of immunosuppression in patients with severe acute respiratory distress syndrome on veno-venous extracorporeal membrane oxygenation therapy. Artif Organs. (2021) 45:1050. doi: 10.1111/AOR.13954
9. Schmidt M, Schellongowski P, Patroniti N, Taccone FS, Miranda DR, Reuter J, et al. Six-month outcome of immunocompromised patients with severe acute respiratory distress syndrome rescued by extracorporeal membrane oxygenation. An international multicenter retrospective study. Am J Respir Crit Care Med. (2018) 197:1297–307. doi: 10.1164/RCCM.201708-1761OC
10. Extracorporeal Life Support Organization (ELSO). ECLS Registry Report Overall Outcomes - International Summary (2022). Available online at: https://www.elso.org/portals/0/files/reports/2022_april/internationalreportapril2022.pdf (Accessed September 4, 2023).
11. Gupta M, Shanley TP, and Moler FW. Extracorporeal life support for severe respiratory failure in children with immune compromised conditions. Pediatr Crit Care Med. (2008) 9:380–5. doi: 10.1097/PCC.0B013E318172D54D
12. Zabrocki LA, Brogan TV, Statler KD, Poss WB, Rollins MD, and Bratton SL. Extracorporeal membrane oxygenation for pediatric respiratory failure: Survival and predictors of mortality. Crit Care Med. (2011) 39:364–70. doi: 10.1097/CCM.0B013E3181FB7B35
13. Gow KW, Heiss KF, Wulkan ML, Katzenstein HM, Rosenberg ES, Heard ML, et al. Extracorporeal life support for support of children with Malignancy and respiratory or cardiac failure: The extracorporeal life support experience. Crit Care Med. (2009) 37:1308–16. doi: 10.1097/CCM.0B013E31819CF01A
14. Maue DK, Hobson MJ, Friedman ML, Moser EAS, and Rowan CM. Outcomes of pediatric oncology and hematopoietic cell transplant patients receiving extracorporeal membrane oxygenation. Perfusion. (2019) 34:598–604. doi: 10.1177/0267659119842471
15. Bridges BC, Kilbaugh TJ, Barbaro RP, Bembea MM, Chima RS, Potera RM, et al. Veno-venous extracorporeal membrane oxygenation for children with cancer or hematopoietic cell transplant: A ten center cohort. ASAIO J. (2021) 67:923. doi: 10.1097/MAT.0000000000001336
16. Steppan DA, Coleman RD, Viamonte HK, Hanson SJ, Carroll MK, Klein OR, et al. Outcomes of pediatric patients with oncologic disease or following hematopoietic stem cell transplant supported on extracorporeal membrane oxygenation: The PEDECOR experience. Pediatr Blood Cancer. (2020) 67:e28403. doi: 10.1002/PBC.28403
17. Niebler RA and Lehmann LE. ECMO use in the pediatric immunocompromised hematology/oncology patient.
18. Di Nardo M, Ahmad AH, Merli P, Zinter MS, Lehman LE, Rowan CM, et al. Extracorporeal membrane oxygenation in children receiving hematopoietic stem cell transplantation and immune effector cell therapies: An International and Multi-Disciplinary Consensus Statement. Lancet Child Adolesc Health. (2022) 6:116. doi: 10.1016/S2352-4642(21)00336-9
19. Schmidt M, Combes A, and Shekar K. ECMO for immunosuppressed patients with acute respiratory distress syndrome: drawing a line in the sand. Intensive Care Med. (2019) 45:1140–2. doi: 10.1007/S00134-019-05632-Y/TABLES/1
20. Zinter MS, Mcarthur J, Duncan C, Adams R, Kreml E, Dalton H, et al. Candidacy for extracorporeal life support (ECLS) in children after hematopoietic cell transplantation (HCT): a position paper from the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network’s Hematopoietic Cell Transplant and Cancer Immunotherapy (CI) subgroup. Pediatr Crit Care Med. (2022) 23:205. doi: 10.1097/PCC.0000000000002865
21. Bousfiha A, Jeddane L, Picard C, Al-Herz W, Ailal F, Chatila T, et al. Human inborn errors of immunity: 2019 update of the IUIS phenotypical classification. J Clin Immunol. (2020) 40:66–81. doi: 10.1007/s10875-020-00758-x
22. Extracorporeal Life Support Organization (ELSO). ELSO Registry Data Definitions (USA: ELSO). (2023).
23. McIntosh AM, Tong S, Deakyne SJ, Davidson JA, and Scott HF. Validation of the vasoactive-inotropic score in pediatric sepsis. Pediatr Crit Care Med. (2017) 18:750–7. doi: 10.1097/PCC.0000000000001191
24. Matics TJ and Sanchez-Pinto LN. Adaptation and validation of a pediatric sequential organ failure assessment score and evaluation of the sepsis-3 definitions in critically ill children. JAMA Pediatr. (2017) 171:e172352–e172352. doi: 10.1001/JAMAPEDIATRICS.2017.2352
25. Bailly DK, Reeder RW, Zabrocki LA, Hubbard AM, Wilkes J, Bratton SL, et al. Development and validation of a score to predict mortality in children undergoing ECMO for respiratory failure: pediatric pulmonary rescue with extracorporeal membrane oxygenation prediction (P-PREP) score. Crit Care Med. (2017) 45:e58. doi: 10.1097/CCM.0000000000002019
26. Emeriaud G, López-Fernández YM, Iyer NP, Bembea MM, Agulnik A, Barbaro RP, et al. Executive summary of the second international guidelines for the diagnosis and management of pediatric acute respiratory distress syndrome (PALICC-2). Pediatr Crit Care Med. (2023) 24:143. doi: 10.1097/PCC.0000000000003147
27. Tian Y, Gu S, Huang X, Li C, Zhang Y, Xia J, et al. Extracorporeal membrane oxygenation in immunocompromised patients with acute respiratory failure: A retrospective cohort study. Clin Respir J. (2023) 17:874–83. doi: 10.1111/CRJ.13674
28. Lindell RB, Nishisaki A, Weiss SL, Traynor DM, and Fitzgerald JC. Risk of mortality in immunocompromised children with severe sepsis and septic shock. Crit Care Med. (2020) 48:1026. doi: 10.1097/CCM.0000000000004329
29. Bergman ZR, Wothe JK, Alwan FS, Lofrano AE, Tointon KM, Doucette M, et al. Risk factors of mortality for patients receiving venovenous extracorporeal membrane oxygenation for COVID-19 acute respiratory distress syndrome. Surg Infect (Larchmt). (2021) 22:1086–92. doi: 10.1089/SUR.2021.114
30. Bizzarro MJ, Conrad SA, Kaufman DA, and Rycus P. Infections acquired during extracorporeal membrane oxygenation in neonates, children, and adults. Pediatr Crit Care Med. (2011) 12:277–81. doi: 10.1097/PCC.0B013E3181E28894
31. Rintoul NE, Mcmichael ABV, Bembea MM, Digeronimo R, Patregnani J, Alexander P, et al. Management of bleeding and thrombotic complications during pediatric extracorporeal membrane oxygenation: the pediatric extracorporeal membrane oxygenation anticoagulation collaborativE consensus conference. Pediatr Crit Care Med. (2024) 25:e66. doi: 10.1097/PCC.0000000000003489
32. Potratz JC, Guddorf S, Ahlmann M, Tekaat M, Rossig C, Omran H, et al. Extracorporeal membrane oxygenation in children with cancer or hematopoietic cell transplantation: single-center experience in 20 consecutive patients. Front Oncol. (2021) 11:664928/FULL. doi: 10.3389/FONC.2021.664928/FULL
33. Olson TL, O’Neil ER, Kurtz KJ, Maclaren G, and Anders MM. Improving outcomes for children requiring extracorporeal membrane oxygenation therapy following hematopoietic stem cell transplantation. Crit Care Med. (2021) 49:E381–93. doi: 10.1097/CCM.0000000000004850
34. Olson TL, Pollack MM, Dávila Saldaña BJ, and Patel AK. Hospital survival following pediatric HSCT: changes in complications, ICU therapies and outcomes over 10 years. Front Pediatr. (2023) 11:1247792/BIBTEX. doi: 10.3389/FPED.2023.1247792/BIBTEX
35. Chima RS, Daniels RC, Kim MO, Li D, Wheeler DS, Davies SM, et al. Improved outcomes for stem cell transplant recipients requiring pediatric intensive care. Pediatr Crit Care Med. (2012) 13(6):e336–42. doi: 10.1097/PCC.0B013E318253C945
36. Henry BM, Benscoter AL, de Oliveira MHS, Vikse J, Perry T, and Cooper DS. Outcomes of extracorporeal life support for respiratory failure in children with primary immunodeficiencies. Perfusion (United Kingdom). (2023) 38:37–43. doi: 10.1177/02676591211033946/SUPPL_FILE/SJ-PDF-1-PRF-10.1177_02676591211033946.PDF
37. Slooff V, Hoogendoorn R, Nielsen JSA, Pappachan J, Amigoni A, Caramelli F, et al. Role of extracorporeal membrane oxygenation in pediatric cancer patients: a systematic review and meta-analysis of observational studies. Ann Intensive Care. (2022) 12. doi: 10.1186/S13613-022-00983-0
38. Wösten-van Asperen RM, van Gestel JPJ, van Grotel M, Tschiedel E, Dohna-Schwake C, Valla FV, et al. PICU mortality of children with cancer admitted to pediatric intensive care unit a systematic review and meta-analysis. Crit Rev Oncol Hematol. (2019) 142:153–63. doi: 10.1016/J.CRITREVONC.2019.07.014
Keywords: ECMO, immunosuppression, inborn immunodeficiancy, cancer, respiratory failure, HCT (hematopoietic cell transplantation), pediatric
Citation: Belevskaia L, von Borell F, Baumann U, Beier R and Köditz H (2025) High-risk extracorporeal membrane oxygenation in immunocompromised children with acute respiratory failure: a retrospective cohort study. Front. Oncol. 15:1613864. doi: 10.3389/fonc.2025.1613864
Received: 17 April 2025; Accepted: 19 June 2025;
Published: 08 July 2025.
Edited by:
Asya Agulnik, St. Jude Children’s Research Hospital, United StatesReviewed by:
Saad Ghafoor, St. Jude Children’s Research Hospital, United StatesCourtney Rowan, Indiana University, United States
Copyright © 2025 Belevskaia, von Borell, Baumann, Beier and Köditz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Florian von Borell, Ym9yZWxsLmZsb3JpYW5AbWgtaGFubm92ZXIuZGU=
†These authors have contributed equally to this work