 Dweeti Nayak1
Dweeti Nayak1 Yves P.V. Mbous
Yves P.V. Mbous Raquel Aguiar-Ibáñez
Raquel Aguiar-Ibáñez- 1Precision AQ, New York, NY, United States
- 2Merck & Co., Inc., Rahway, NJ, United States
- 3Merck Canada Inc., Kirkland, QC, Canada
Background: The development and regulatory approval of anti-programmed death (ligand) 1 (anti-PD-(L)1) agents, based on positive clinical trial results, has dramatically changed clinical practice and treatment paths in oncology. However, the effectiveness of anti-PD-(L)1 therapy in real-world settings is not well understood. Therefore, it is important to summarize real-world evidence on the overall survival (OS) of patients with specific tumor types prior to and following the regulatory approval of anti-PD-(L)1 therapy.
Methods: A systematic literature review including observational studies worldwide reporting the OS of patients receiving conventional first-line pharmacological therapy for advanced/metastatic non-small cell lung cancer (NSCLC), renal cell carcinoma (RCC), or melanoma in the anti-PD-(L)1 pre-approval era and similar patients receiving first-line anti-PD-(L)1 therapy in the post-approval era was conducted. For each tumor type, studies were selected from a pre-approval era, defined as a period beginning 5 years before the first approval of an anti-PD-(L)1 agent and ending the year before its approval for first-line therapy, and a post-approval era, defined as a period beginning the year that an anti-PD-(L)1 agent was approved for first-line therapy and ending in 2023. Relevant studies were identified through MEDLINE and Embase searches. Study selection, data extraction, and quality assessment were conducted by two independent reviewers. Median OS (mOS) was summarized within each tumor type and descriptively compared across the pre- and post-approval eras.
Results: A total of 86, 44, and 35 studies evaluating first-line treatments for advanced/metastatic NSCLC, RCC, and melanoma, respectively, were included. Post-approval mOS in patients treated with anti-PD-(L)1 therapy tended to be numerically longer than pre-approval mOS in patients treated with conventional therapy within certain patient and treatment categories. For example, pre-approval mOS ranged from 6.9 to 18.4 months (n=18 treatment groups), and post-approval mOS ranged from 10.6 to 46.2 months in NSCLC patients with PD-L1 tumor expression ≥50% who received anti-PD-(L)1 monotherapy (n=33; with mOS not reached for n=3). In RCC patients classified as high-risk, pre-approval mOS ranged from 2 to 10.3 months (n=7), and post-approval mOS ranged from 7.8 to 24.3 months (n=4). Also, in melanoma patients with any BRAF mutation, pre-approval mOS was 14.2 months (n=1), and post-approval mOS ranged from 15.9 to 51.2 months (n=6; with mOS not reached for n=3).
Conclusion: A survival benefit in real-world practice was observed for patients with advanced/metastatic NSCLC, RCC, or melanoma receiving first-line anti-PD-(L)1 therapy after its regulatory approval when compared with patients treated with conventional care before anti-PD-(L)1 therapy approval. This supports the use of anti-PD-(L)1 therapy as a standard of care in many countries.
1 Introduction
The development and regulatory approval of immune checkpoint inhibitors (ICIs) has dramatically changed the way cancer is treated in clinical practice (1, 2). ICIs are immunotherapy agents that inhibit T cell immune checkpoints leveraged by tumor cells to evade recognition and destruction by the immune system, thereby restoring the body’s ability to effectively attack tumors (1, 2). After the first regulatory approval of an ICI, the anti-cytotoxic T lymphocyte antigen 4 (anti-CTLA-4) agent ipilimumab, several anti-programmed death (ligand) 1 (anti-PD-(L)1) agents—pembrolizumab, nivolumab, atezolizumab, avelumab, durvalumab, and cemiplimab—have been approved for the treatment of patients with different types of cancer, including advanced/metastatic non-small cell lung cancer (NSCLC), renal cell carcinoma (RCC), and melanoma (2). For these tumor types, anti-PD-L1 therapy is approved as monotherapy or in combination with other immunotherapy agents or chemotherapy in first-line and/or subsequent therapy settings.
The regulatory approval of cancer treatments is largely based on the findings of randomized controlled trials (RCTs), which tightly control potential sources of variability to improve the validity and reliability of the efficacy and safety measures of investigated treatments. However, treatment efficacy as measured in RCTs may not directly translate to real-world settings due to differences between patients enrolled in RCTs versus the more heterogeneous populations seen in less controlled, clinical practice environments, including differences in demographics, functional status, comorbid conditions, adherence and concomitant (3). For example, patients enrolled in RCTs tend to be younger, have better performance status, and have fewer comorbid conditions than patients treated in real-world settings (4, 5). Thus, real-world evidence, including data from observational studies, has the potential to provide additional evidence of the benefits of anti-PD-(L)1 therapy on patient outcomes. For example, previous observational studies (6–8) and evidence summaries (9–12) describe the clinical outcomes of patients with certain cancer types, including advanced/metastatic NSCLC and melanoma, in real-world settings before and after the regulatory approval of ICIs in general. However, no previous evidence summaries have identified and summarized real-world data on outcomes in similar populations of cancer patients before versus after the approval of anti-PD-(L)1 therapy, in particular.
To demonstrate the value and improvements in outcomes that anti-PD-(L)1 therapy has brought to advanced/metastatic cancer patients in clinical practice, there is a need to understand available real-world evidence on the overall survival (OS) of patients with specific tumor types who would currently be eligible for treatment with an anti-PD-(L)1 agent but were treated with conventional care before the regulatory approval of anti-PD-(L)1 therapy and of patients treated with anti-PD-(L)1 agents after their approval by performing a systematic literature review (SLR).
2 Methods
An SLR was conducted following the Cochrane Handbook for Systematic Reviews (13) and the National Institute for Health Care and Excellence guidelines manual (14) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) (15).
2.1 Inclusion and exclusion criteria
Study eligibility criteria were defined in terms of population, interventions, comparisons, outcome, study design and time (PICOTS) (Table 1).
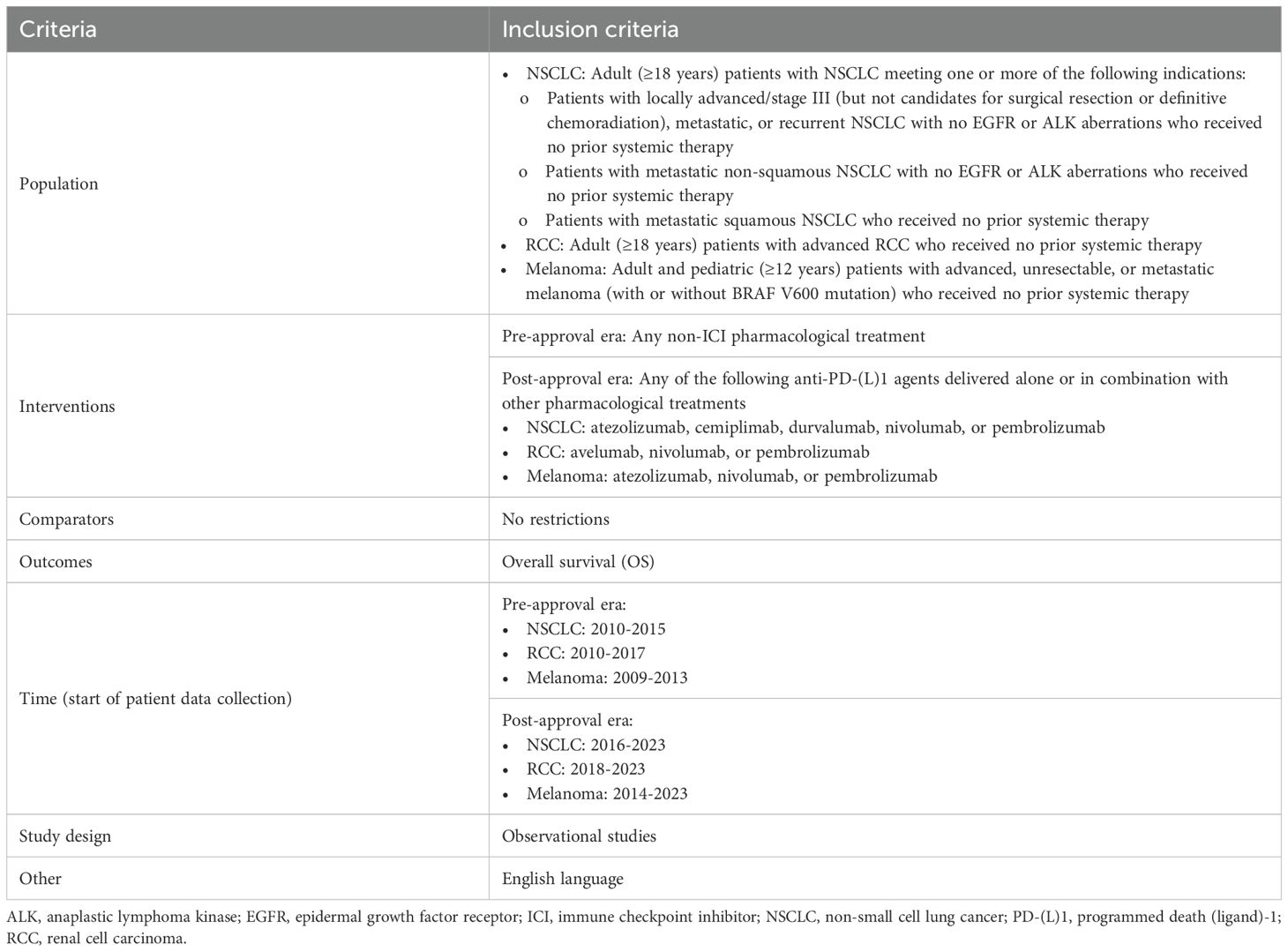
Table 1. PICOTS study selection criteria.
2.1.1 Population
Eligible studies included patients receiving first-line therapy for advanced/metastatic NSCLC, RCC, or melanoma who met one or more current indications for treatment with a United States (US) Food and Drug Administration (FDA)- or European Medicines Agency (EMA)-approved anti-PD-(L)1 agent [i.e., atezolizumab (16, 17), avelumab (18, 19), cemiplimab (20, 21), durvalumab (22, 23), pembrolizumab (24, 25), or nivolumab (26, 27)]. Of note, as study selection was guided by stringent definitions of both pre- and post-approval eras and the populations of patients eligible for treatment with an anti-PD-(L)1 agent, FDA and EMA approval dates and first-line indications were used, respectively, to develop these definitions. However, no geographical criteria for study selection were imposed.
2.1.2 Interventions/comparators
For the pre-approval era, eligible studies evaluated conventional care, defined as any non-ICI pharmacological treatment as appropriate for each tumor type. For the post-approval era, eligible studies evaluated anti-PD-(L)1 agents approved by the FDA or EMA for each tumor type. Although FDA and EMA labels note specific monotherapy or combination therapy regimens for certain tumor types, studies evaluating any approved anti-PD-(L)1 agent delivered alone or in combination with other pharmacological agents were eligible for inclusion to ensure that a sufficiently large evidence base was captured. For both eras, no eligibility restrictions were placed on the presence or identity of comparator treatments.
2.1.3 Outcomes
Eligible studies reported median OS (mOS) or OS rates at specific timepoints (i.e., landmark OS rates).
2.1.4 Time
The post-approval era for each tumor type was defined as the period from the year of first anti-PD-(L)1 agent approval by the FDA or EMA for first-line therapy to the search date. The pre-approval era for each tumor type was defined as a time period beginning 5 years preceding the first FDA or EMA approval of an anti-PD-(L)1 agent for any indication (inclusive of accelerated approval) and ending the year before an anti-PD-(L)1 agent was approved for first-line therapy. The duration of this pre-approval period was selected to ensure the inclusion of a sufficiently sized evidence base while keeping a manageable scope of the SLR. Studies were categorized into pre- versus post-approval eras based on the start date of patient data collection.
2.1.5 Study design
Eligible studies were observational studies employing any type of design (e.g., retrospective, prospective, or ambispective cohort or case-control studies).
2.2 Search strategy
Relevant studies were identified by searching Excerpta Medica database (Embase) and Medical Literature Analysis and Retrieval System Online (MEDLINE) database through the OVID portal. Separate searches were conducted for the pre- and post-approval eras for each tumor type. To specifically retrieve observational studies, search strategies employed the observational study filter from the Scottish Intercollegiate Guidelines Network (http://www.sign.ac.uk/methodology/filters.html) and filtered out irrelevant publication types, such as conference abstracts, case reports, editorials, letters, notes, and historical articles. To identify studies in the pre-approval era for each tumor type, the search strategies retrieved studies published up to 2 years after the pre-approval era ended to account for publication delays. These searches were executed on July 10, 2023 with predefined search strategies (Supplementary Tables S1-S4 for advanced/metastatic melanoma, Supplementary Tables S10-S13 for advanced/metastatic NSCLC, and Supplementary Tables S20-S23 for advanced RCC).
2.3 Study selection and data extraction
Title/abstract and full-text screening against the PICOTS study selection criteria and data extraction from included studies were performed by two independent reviewers, and any discrepancies between reviewers were resolved through discussion or by involving a third reviewer. Data were extracted on study characteristics (e.g., study design, country/region, patient eligibility criteria), treatment characteristics (e.g., agents/regimens evaluated, doses), patient characteristics (e.g., age, sex, race/ethnicity, Eastern Cooperative Oncology Group [ECOG] performance status, biomarker status), and outcomes (e.g., mOS).
2.4 Quality assessment
The quality of included studies was assessed using the Newcastle-Ottawa Scale for Cohort Studies, which evaluates studies’ selection of study groups, comparability of study groups, and ascertainment of the outcome of interest (28). Studies with scores of 7-9 were considered good quality, 4-6 fair quality, and 0-3 poor quality. The quality assessment was performed by two independent reviewers, and any discrepancies between reviewers were resolved through discussion or by involving a third reviewer.
2.5 Synthesis methods
The range of mOS values was reported separately for treatment groups in the pre- and post-approval eras within each tumor type. Wherever possible, the range of mOS values as categorized by certain patient and/or treatment characteristics as appropriate for each tumor type was reported. These factors included BRAF mutation status and PD-L1 expression for melanoma; anti-PD-(L)1 therapy regimen (i.e., monotherapy or combination therapy), PD-L1 expression, and tumor histology for NSCLC; and International mRCC Database Consortium (IMDC)/Memorial Sloan Kettering Cancer Center (MSKCC) risk classification and PD-L1 expression for RCC. For RCC, IMDC risk classification was preferred when both IMDC and MSKCC risk classifications were reported, whereas MSKCC risk classification was used when IMDC classification was not reported.
3 Results
3.1 Advanced/metastatic melanoma
3.1.1 Study selection
The pre-approval era literature search yielded 4,514 publications, of which 2,812 titles/abstracts and 37 full-texts were screened (Figure 1). Of the publications that underwent full-text screening, 36 were excluded. The post-approval era literature search yielded 3,536 publications, of which 2,330 titles/abstracts and 234 full-texts were screened. Of the publications that underwent full-text screening, 200 were excluded. Thus, a total of 35 publications describing 35 advanced/metastatic melanoma studies were included: one study in the pre-approval era and 34 studies in the post-approval era. The study selection processes for the pre- and post-approval eras are separately depicted in Supplementary Figures S1 and S2, respectively.
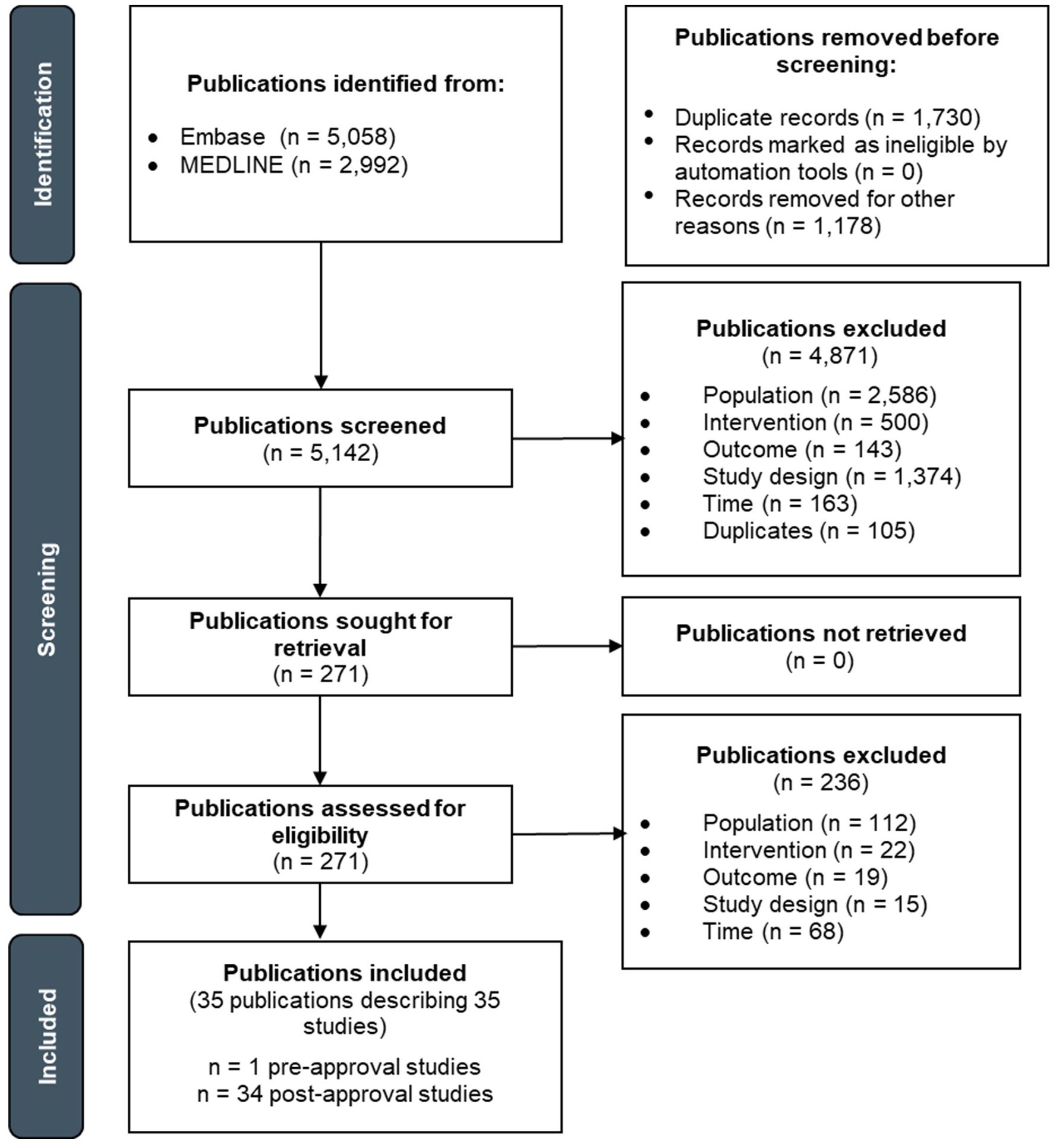
Figure 1. PRISMA flow diagram depicting the study selection process for advanced/metastatic melanoma.
3.1.2 Study characteristics
The one study in the pre-approval era was a retrospective cohort study conducted in France that included 50 patients whose tumors had BRAF V600E mutations (29). This study evaluated the BRAF kinase inhibitor vemurafenib.
Of the 34 studies in the post-approval era, 27 were retrospective cohort studies (30–55), six were prospective cohort studies (56–61), and one was described as an ambispective cohort study (62). These studies were conducted in European countries (n=17), the US (n = 7), Canada (n = 3), Australia (n = 3), the United Kingdom (UK) (n = 2), Canada (n = 3), Australia (n = 3), Japan (n = 1), and New Zealand (n = 1). Most studies (n = 29) did not have eligibility criteria related to BRAF mutation status. Overall, study sample size ranged from 29 to 2,322 patients. The studies evaluated anti-PD-(L)1 agents as monotherapy (n = 27), anti-PD-(L)1 agents in combination with anti-CTLA-4 (i.e., ipilimumab) or anti-RANKL (i.e., denosumab) agents (n = 14), or a mixture of treatment regimens including anti-PD-(L)1 agents as monotherapy or in combination with anti-CTLA-4 agents (n = 1).
Study characteristics for each study are presented in Supplementary Table S5.
3.1.3 Patient characteristics
In the pre-approval era study, median patient age was 58 years, and 58% of patients were male. Most (86%) patients had an ECOG performance status of 0 or 1. Patient race/ethnicity was not reported. All patients had tumors with BRAF V600E mutations.
Across studies in the post-approval era, median/mean patient age ranged from 56 to 73 years, and the proportion of male patients ranged from 49% to 100%. The proportion of patients with an ECOG performance status of 0 or 1 ranged from 58.1% to 100%. Eight studies reported patient race/ethnicity, all of which predominantly included White patients. Regarding BRAF mutation status, the proportion of patients with V600E mutations ranged from 9.8 to 83.5%, V600K mutations ranged from 6.7% to 13.8%, and any type of V600 mutation or unspecified BRAF mutation ranged from 0% to 100%.
Patient characteristics for each study are presented in Supplementary Table S6.
3.1.4 Outcomes
To summarize reported mOS across studies, treatment groups were categorized by BRAF mutation status. Treatment groups were not categorized by PD-L1 expression due to the sparseness of reported data.
Considering patients with any type of BRAF mutation, mOS was 14.2 months for a treatment group receiving first-line conventional therapy in the pre-approval era and ranged from 15.9 to 51.2 months for treatment groups receiving first-line anti-PD-(L)1 therapy in the post-approval era (Figure 2). mOS was not reached for three treatment groups in the post-approval era; median follow-up duration was 11.3 and 23.2 months for two treatment groups, respectively, and was not reported for one treatment group.
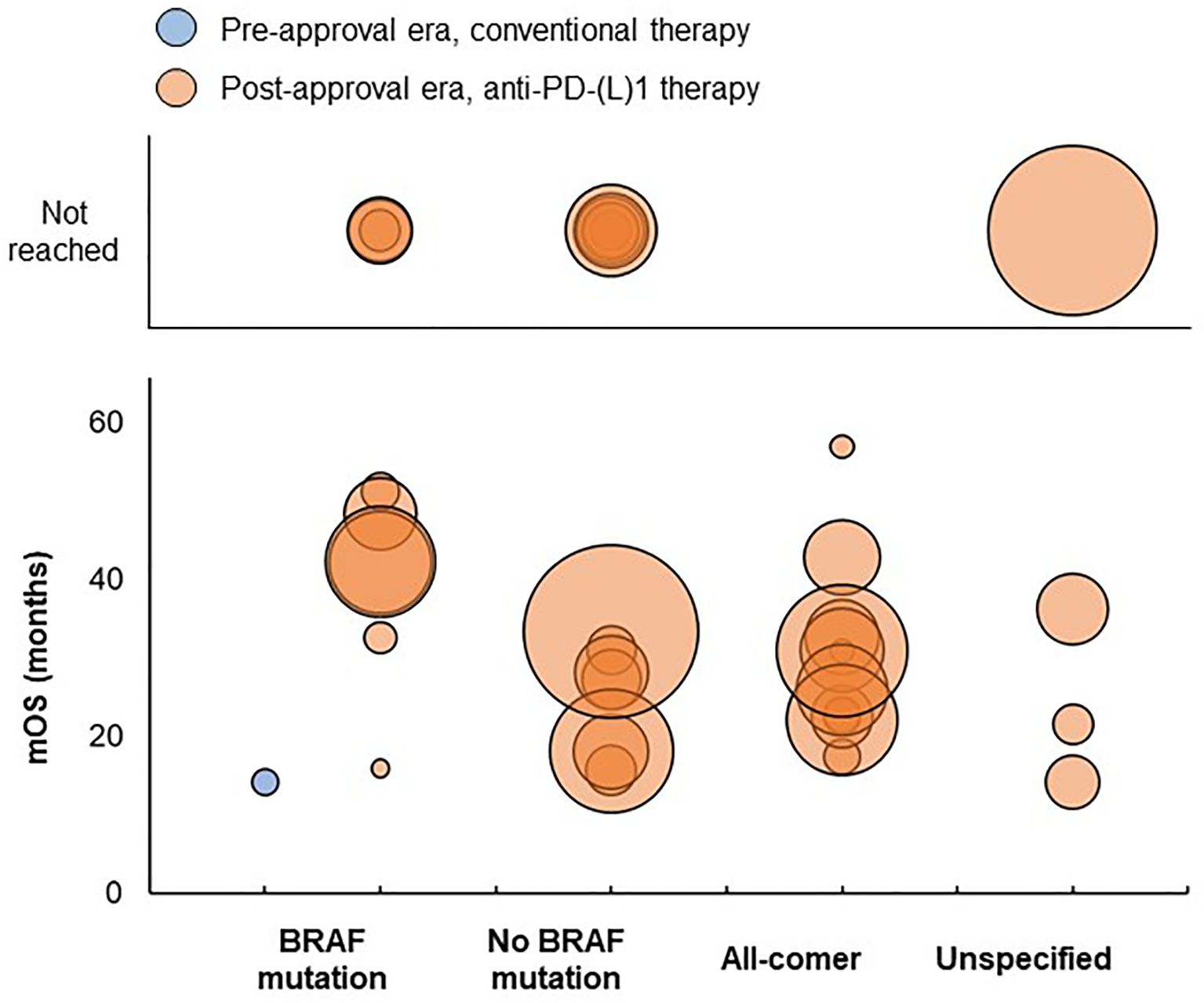
Figure 2. Distribution of mOS values in advanced/metastatic melanoma studies. Bubble size reflects the sample size of each treatment group, which ranged from 7 to 1,174 patients. BRAF, B-Raf proto-oncogene; mOS, median overall survival; PD-(L)1, programmed death (ligand)-1.
No pre-approval era studies reported mOS for treatment groups of patients without BRAF mutations, all-comer patients, or patients with unspecified BRAF mutation status. Post-approval era studies reported an mOS ranging from 15.7 to 33.4 months for treatment groups of patients without BRAF mutations, from 17.4 to 57 months for treatment groups of all-comer patients, and from 14.2 to 36.2 months for treatment groups of patients with unspecified BRAF mutation status. mOS was not reached for six treatment groups without BRAF mutations in the post-approval era; median follow-up duration was 12.1, 14.5, and 16.5 months for three treatment groups, respectively, and was not reported for three treatment groups. mOS was not reached for one treatment group of patients with unspecified BRAF mutation status in the post-approval era, which had a median follow-up duration of 25 months.
A summary and detailed information on median follow-up durations, mOS, and landmark OS rates for each study are presented in Supplementary Tables S7 and S8.
3.1.5 Study quality
All studies were judged to be of fair quality in both the pre- and post-approval eras, largely due to the absence of a non-exposed cohort and some concerns regarding the representativeness of the exposed cohort and length of follow-up (Supplementary Table S9).
3.2 Advanced/metastatic NSCLC
3.2.1 Study selection
The pre-approval era literature search yielded 10,797 publications, of which 5,583 titles/abstracts and 495 full-texts were screened (Figure 3). Of the publications that underwent full-text screening, 480 were excluded. The post-approval era literature search yielded 4,703 publications, of which 2,881 titles/abstracts and 515 full-texts were screened. Of the publications that underwent full-text screening, 442 were excluded. Thus, a total of 88 publications describing 86 advanced/metastatic NSCLC studies were included: 15 studies in the pre-approval era and 71 studies in the post-approval era. The study selection processes for the pre- and post-approval eras are separately depicted in Supplementary Figures S3 and S4, respectively.
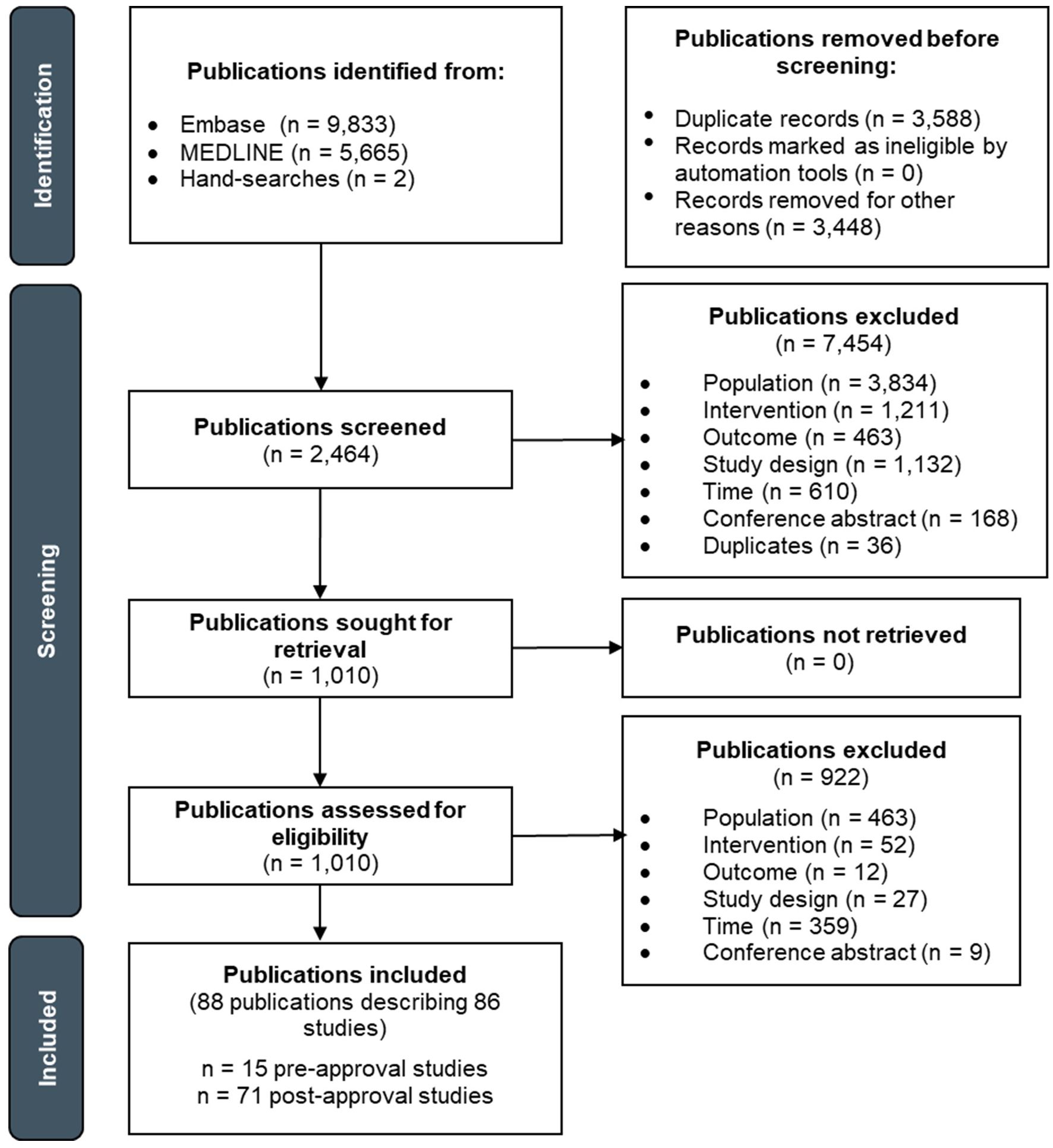
Figure 3. PRISMA flow diagram depicting the study selection process for advanced/metastatic NSCLC.
3.2.2 Study characteristics
Of the 15 studies in the pre-approval era, 13 were retrospective cohort studies (63–75), and two were prospective cohort studies (76, 77). These studies were conducted in European countries (n = 6), China (n = 3), the US (n = 2), Saudi Arabia (n = 1), Japan (n = 1), India (n = 1), or multiple countries around the world (n = 1). Overall study sample size ranged from 20 to 2,014 patients. The studies evaluated chemotherapy regimens containing platinum, taxanes, or other chemotherapeutic agents (n = 7); vascular endothelial growth factor (VEGF)-targeting therapy (i.e., bevacizumab) in combination with chemotherapy (n = 4); epidermal growth factor receptor (EGFR)-targeting therapy (i.e., icotinib or erlotinib) (n = 3); or a mixture of treatment regimens including chemotherapy and/or unnamed tyrosine kinase inhibitors (TKIs) (n = 3).
Of the 71 studies in the post-approval era, 68 were retrospective cohort studies (78–147), and three were prospective cohort studies (148–150). These studies were conducted in European countries (n = 26), Japan (n = 13), the US (n = 11), China/Taiwan (n = 9), Israel (n = 4), the UK and European countries (n = 3), Australia (n = 2), Canada (n = 1), Singapore (n = 1), or multiple countries across North and South America (n = 1). Overall study sample size ranged from 30 to 7,312 patients. The studies evaluated anti-PD-(L)1 agents as monotherapy (n = 52), anti-PD-(L)1 agents in combination with chemotherapy and/or anti-VEGF therapy (n = 21), or a mixture of treatment regimens including anti-PD-(L)1 agents as monotherapy or in combination with chemotherapy (n = 6).
Study characteristics for each study are presented in Supplementary Table S14.
3.2.3 Patient characteristics
Across studies in the pre-approval era, median/mean patient age ranged from 60.2 to 71 years, and the proportion of male patients ranged from 37.5% to 90%. The proportion of patients with an ECOG performance status of 0 or 1 ranged from 28% to 100%. Two studies reported patient race/ethnicity: one predominantly included White patients, and one was a global study in which patients recruited in Italy, Spain, Germany, Australia, and Brazil were predominantly White and patients recruited in the Republic of Korea and Taiwan were predominantly Asian. Among studies that reported smoking status, the proportion of patients who were current or former smokers ranged from 32.7% to 97%. Seven studies included both patients with squamous and non-squamous tumors, four exclusively included patients with non-squamous tumors, two exclusively included patients with squamous tumors, and two did not report on patients’ tumor histology. The proportion of patients with EGFR or anaplastic lymphoma kinase (ALK) aberrations ranged from 0% to 100%. No studies reported on PD-L1 expression.
Across studies in the post-approval era, median/mean patient age ranged from 59.8 to 74 years, and the proportion of male patients ranged from 35.3% to 93.9%. The proportion of patients with an ECOG performance status of 0 or 1 ranged from 46% to 100%. Thirteen studies reported patient race/ethnicity: 12 predominantly included White patients, and one predominantly included Hispanic patients. Among studies that reported smoking status, the proportion of patients who were current or former smokers ranged from 50% to 99%. Fifty-six studies included both patients with squamous and non-squamous tumors, 11 exclusively included patients with non-squamous tumors, one exclusively included patients with squamous tumors, and three did not report on patients’ tumor histology. The proportion of patients with EGFR or ALK aberrations ranged from 0% to 23.3%. Several studies reported on PD-L1 expression; the proportion of patients with a PD-L1 tumor proportion score (TPS) ≥1% ranged from 20.6% to 100%, TPS 1-49% ranged from 0% to 67.3%, and TPS ≥50% ranged from 11.8% to 100%.
Patient characteristics for each study are presented in Supplementary Tables S15 and S16.
3.2.4 Outcomes
To summarize reported mOS across studies, treatment groups receiving anti-PD-(L)1 monotherapy in the post-approval era were categorized by tumor PD-L1 expression. However, as PD-L1 expression was not reported for treatment groups in the pre-approval era (because PD-L1 expression was not of relevance to treatment decisions at that time), pre-approval treatment groups were not categorized by this factor. All treatment groups had to consist of ≥80% of patients with no tumor EGFR/ALK aberrations to be included in the mOS summary to align as closely as possible with current FDA/EMA-approved indications for anti-PD-(L)1 therapy.
In the pre-approval era, mOS ranged from 6.9 to 18.4 months across treatment groups of all-comer patients receiving first-line conventional therapy (Figure 4). In the post-approval era, mOS ranged from 10.6 to 46.2 months for treatment groups with PD-L1 TPS ≥50% and from 14 to 27 months for treatment groups with PD-L1 TPS ≥1% receiving first-line anti-PD-(L)1 monotherapy. mOS was not reached three treatment groups with PD-L1 TPS ≥50%; median follow-up durations were 19.9 and 26.5 months for two treatment groups, respectively, and was not reported for one treatment group. mOS was not reached for three treatment groups with PD-L1 TPS ≥1%, which had median follow-up durations of 11.3, 12.5, and 14.5 months, respectively.
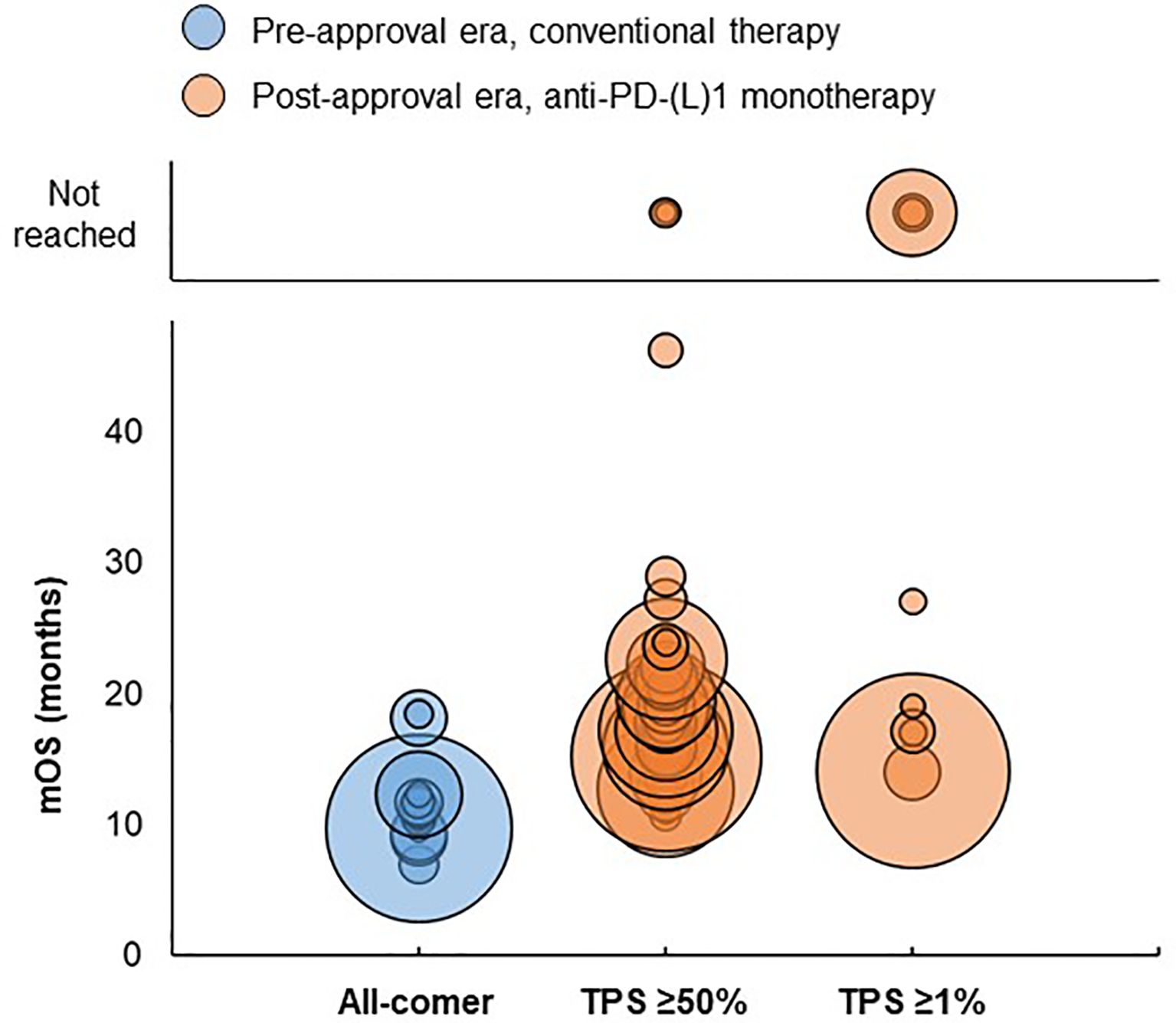
Figure 4. Distribution of mOS values by PD-L1 expression in advanced/metastatic NSCLC studies. Bubble size reflects the sample size of each treatment group, which ranged from 5 to 2,166 patients. TPS, PD-L1 tumor proportion score.
Next, treatment groups receiving conventional therapy in the pre-approval era and anti-PD(L)1 combination therapy in the post-approval era were categorized by tumor histology. For all categories except the ‘100% squamous’ category, treatment groups had to consist of ≥80% of patients with no tumor EGFR/ALK aberrations to be included in the mOS summary to align as closely as possible with current FDA/EMA-approved indications for anti-PD-(L)1 therapy.
For treatment groups consisting of 100% non-squamous patients, mOS ranged from 6.9 to 18.4 months in the pre-approval era and from 11.8 to 23.1 months in the post-approval era (Figure 5). mOS was not reached for three treatment groups in the post-approval era, which had median follow-up durations of 5.5, 8, and 10.3 months, respectively.
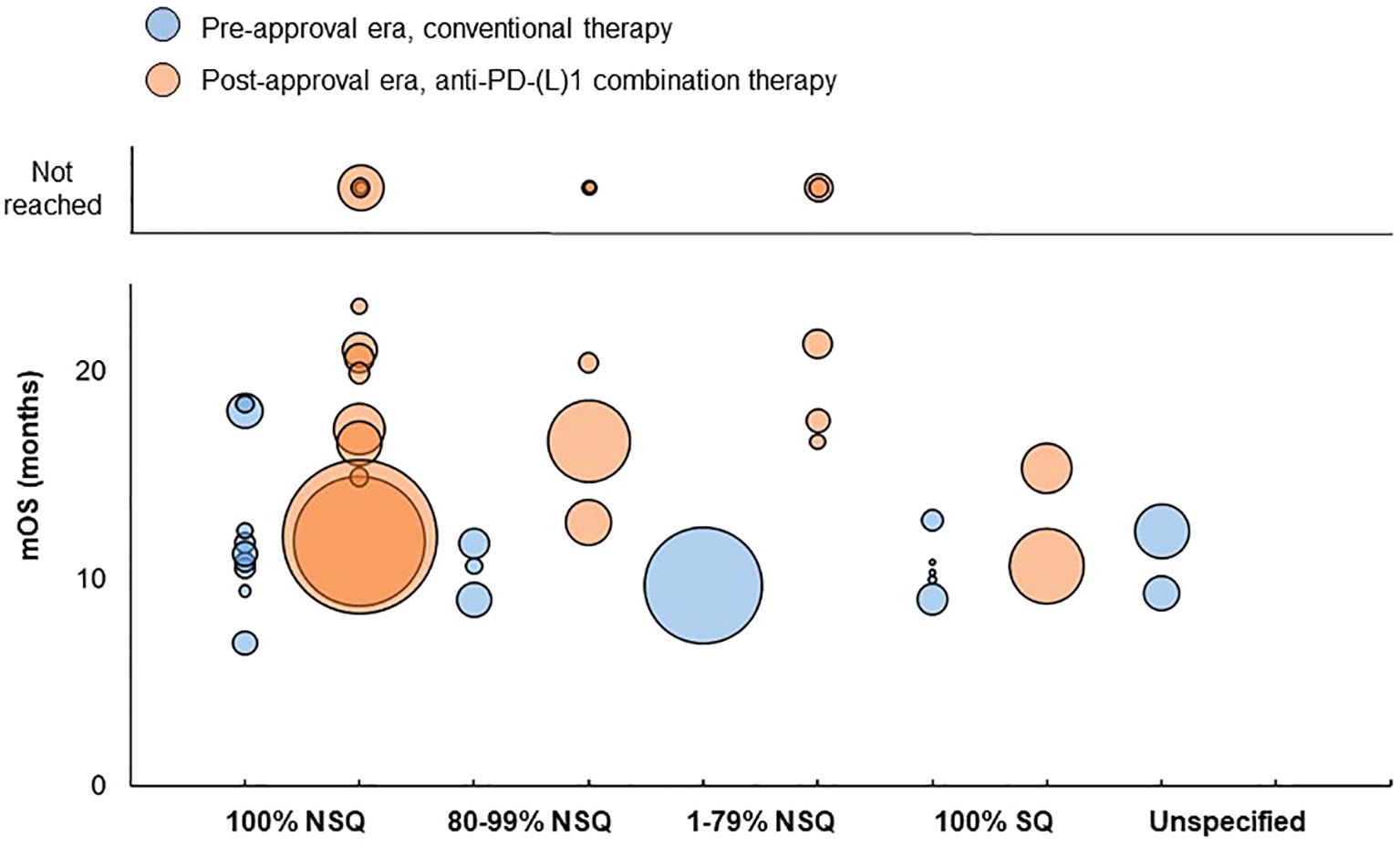
Figure 5. Distribution of mOS values by tumor histology in advanced/metastatic NSCLC studies. Bubble size reflects the sample size of each treatment group, which ranged from 5 to 2,488 patients. Sample size was not reported for two ‘100% SQ’ treatment groups in the pre-approval era, which had a mOS of 17 months and 17.6 months respectively; these treatment groups are not reflected in the chart. mOS, median overall survival; NSQ, non-squamous; PD-L1, programmed death (ligand)-1; SQ, squamous.
For treatment groups consisting of 80-99% non-squamous patients, mOS ranged from 9 to 11.7 months in the pre-approval era and from 12.7 to 20.4 months in the post-approval era. mOS was not reached for two treatment groups in the post-approval era, both of which had median follow-up durations of 14.8 months.
For treatment groups consisting of 1-79% non-squamous patients, mOS was 9.67 months in the pre-approval era and ranged from 16.6 to 21.3 months in the post-approval era. mOS was not reached for two treatment groups in the post-approval era, which had median follow-up durations of 8.9 and 17.13 months, respectively.
For treatment groups consisting of 100% squamous patients, mOS ranged from 9 to 12.8 months in the pre-approval era and from 10.6 to 15.3 in the post-approval era.
For treatment groups consisting of patients with unspecified tumor histology, mOS ranged from 9.3 to 12.3 months in the pre-approval era and was not reported in the post-approval era.
A summary and detailed information on median follow-up durations, mOS, and landmark OS rates are provided in Supplementary Tables S17 and S18.
3.2.5 Study quality
All studies were judged to be of fair quality in both the pre- and post-approval eras, largely due to the absence of a non-exposed cohort and some concerns regarding the representativeness of the exposed cohort, ascertainment of exposure, assessment of outcome, and length of follow-up (Supplementary Table S19).
3.3 Advanced RCC
3.3.1 Study selection
The pre-approval era literature search yielded 7,517 publications, of which 4,323 titles/abstracts and 310 full-texts were screened (Figure 6). Of the publications that underwent full-text screening, 282 were excluded. The post-approval era literature search yielded 1,505 publications, of which 929 titles/abstracts and 195 full-texts were screened. Of the publications that underwent full-text screening, 179 were excluded. Thus, a total of 44 publications describing 44 advanced RCC studies were included: 28 studies in the pre-approval era and 16 studies in the post-approval era. The study selection processes for the pre- and post-approval eras are separately depicted in Supplementary Figures S5 and S6, respectively.
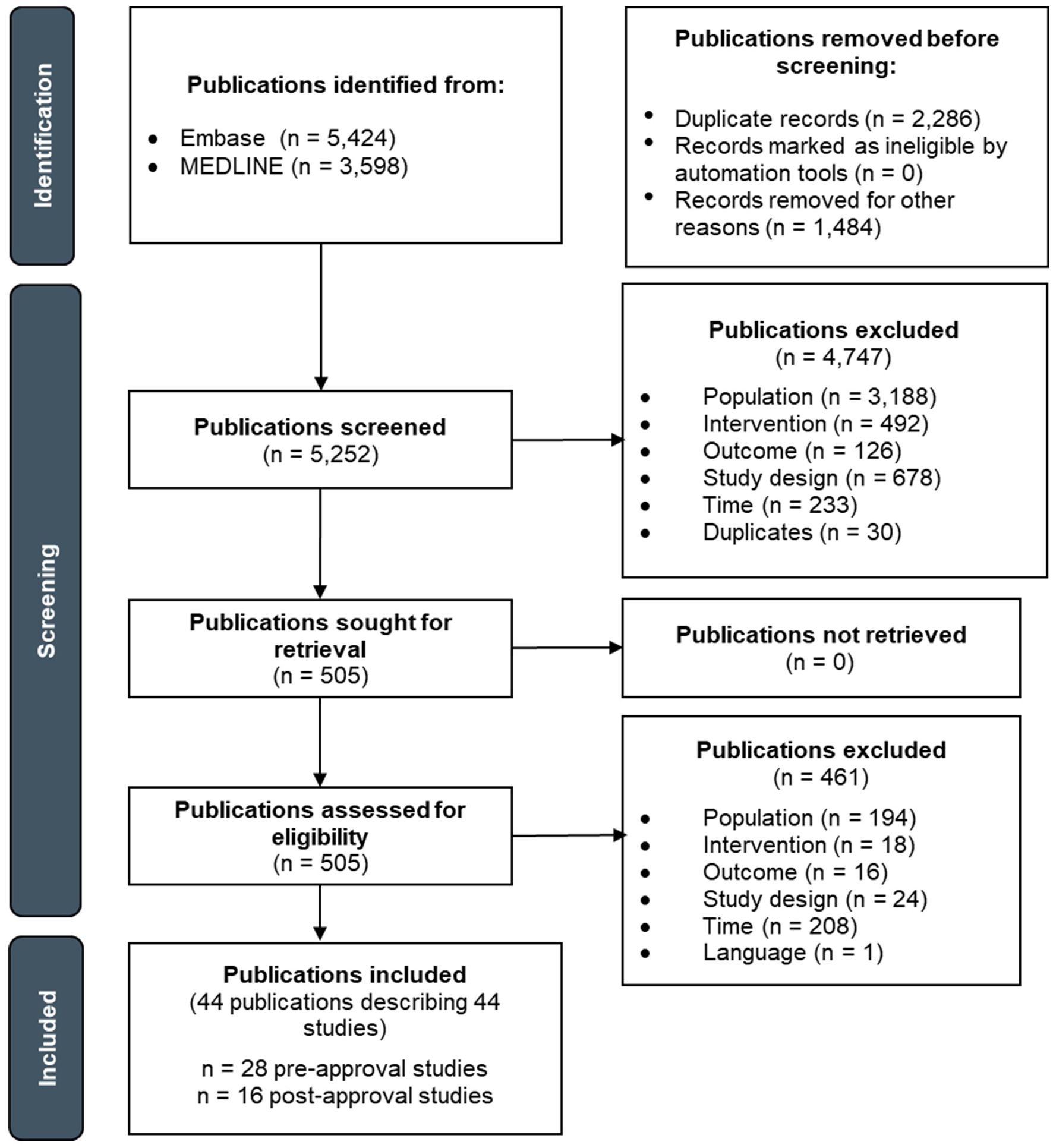
Figure 6. PRISMA flow diagram depicting the study selection process for advanced RCC.
3.3.2 Study characteristics
Of the 28 studies in the pre-approval era, 21 were retrospective cohort studies (151–171), and seven were prospective cohort studies (172–178). These studies were conducted in European countries (n = 9), India (n = 5), Egypt (n = 3), China (n = 2), Japan (n = 2), the Republic of Korea (n = 2), Australia (n = 1), Brazil (n = 1), Turkey (n = 1), multiple countries across North and South America (n = 1), or multiple countries around the world (n = 1). Overall study sample size ranged from 15 to 657 patients. The studies evaluated multi-targeted receptor tyrosine kinase (RTK) inhibitor (i.e., sunitinib, pazopanib, sorafenib) monotherapy (n = 27), multi-targeted RTK inhibitor (i.e., sorafenib) in combination with interferon therapy (n = 1), or interferon monotherapy (n = 1).
Of the 16 studies in the post-approval era, 13 were retrospective cohort studies (179–191), and three were prospective cohort studies (192–194). These studies were conducted in Japan (n = 9), the Republic of Korea (n = 3), the US (n = 3), or Italy (n = 1). Overall study sample size ranged from 35 to 1,538 patients. The studies evaluated nivolumab in combination with an anti-CTLA-4 agent (i.e., ipilimumab) (n = 10), pembrolizumab in combination with a TKI (i.e., axitinib) (n = 5), or mixtures of treatment regimens including anti-PD-(L)1 agents in combination with anti-CTLA-4 agents or TKIs (n = 3).
Study characteristics for each study are presented in Supplementary Table S24.
3.3.3 Patient characteristics
Across studies in the pre-approval era, median/mean patient age ranged from 49 to 69 years, and the proportion of male patients ranged from 22.2% to 83.6%. The proportion of patients with an ECOG performance status of 0 or 1 ranged from 35% to 100%. Three studies reported patient race/ethnicity; one study included exclusively Asian patients, one study included mostly White patients, and one study included mostly Hispanic patients. Considering IMDC/MSKCC risk classification, 3% to 56% of patients were classified as poor risk, 93% of patients were classified as poor/intermediate risk, 29% to 100% of patients were classified as intermediate risk, and 3.7% to 65% of patients were classified as favorable risk across studies.
Across studies in the post-approval era, median/mean patient age ranged from 58 to 71 years, and the proportion of male patients ranged from 68.8% to 84.8%. The proportion of patients with an ECOG performance status of 0 or 1 ranged from 50.9% to 88.4%. Three studies reported patient race/ethnicity, all of which included mostly White patients. Considering IMDC/MSKCC risk classification, 21.4% to 100% of patients were classified as poor risk, 85.7% to 93.6% of patients were classified as poor/intermediate risk, 0% to 69.4% of patients were classified as intermediate risk, 5.3% to 11.8% of patients were classified as favorable/intermediate risk, and 0% to 37.9% of patients were classified as favorable risk across studies.
Patient characteristics for each study are presented in Supplementary Tables S25 and S26.
3.3.4 Outcomes
To summarize reported mOS across studies, treatment groups were categorized by IMDC/MSKCC risk classification. Treatment groups were not categorized by PD-L1 expression due to the sparseness of reported data.
For patients classified as having poor risk, mOS ranged from 2 to 10.3 months for treatment groups receiving first-line conventional therapy in the pre-approval era and from 7.8 to 24.3 months for treatment groups receiving first-line anti-PD-(L)1 therapy in the post-approval era (Figure 7).
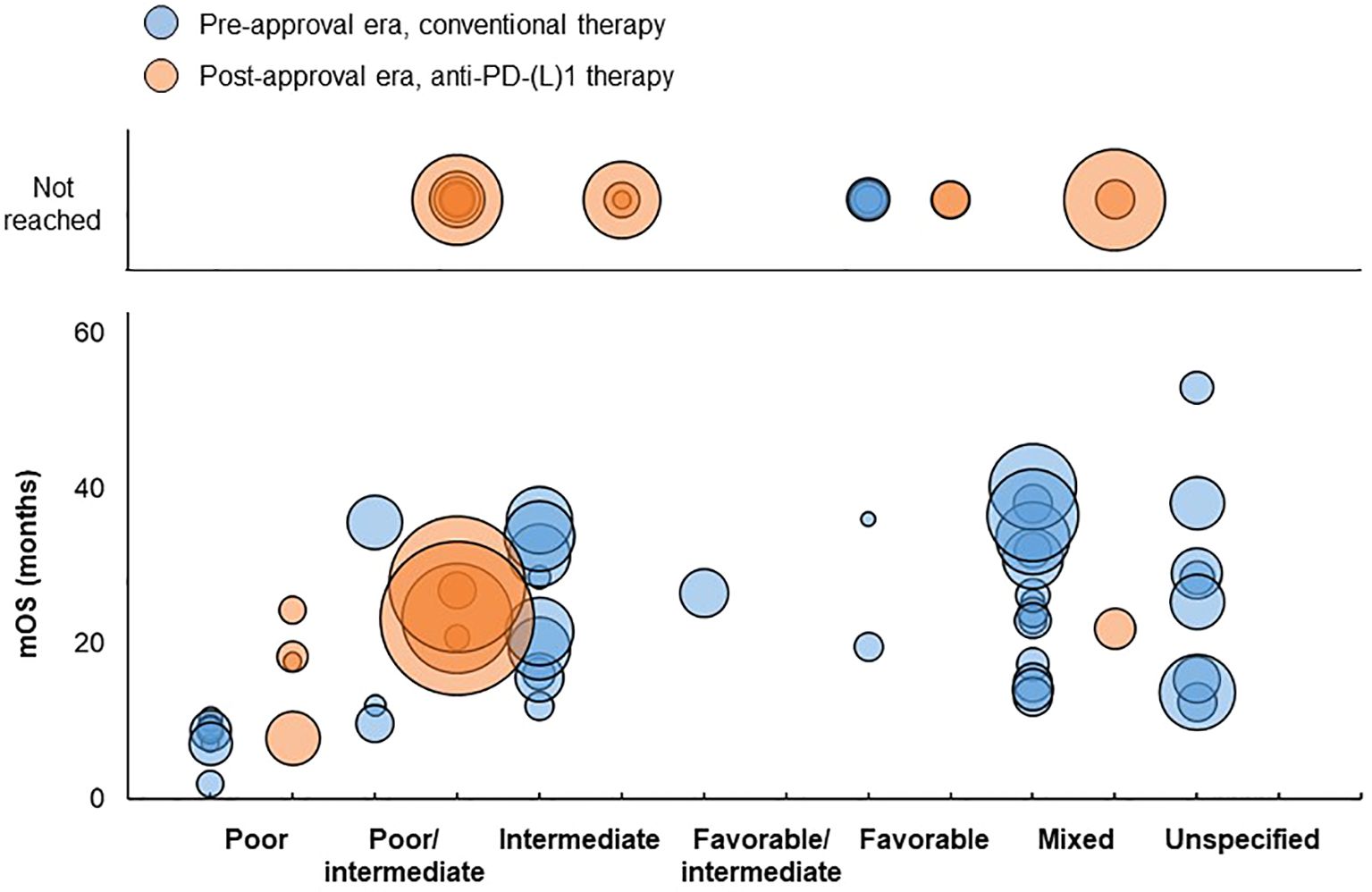
Figure 7. Distribution of mOS values in advanced RCC studies. Bubble size reflects the sample size of each treatment group, which ranged from 7 to 817 patients. Inter, intermediate; mOS, median overall survival; PD-(L)1, programmed death (ligand)-1.
For patients classified as having poor/intermediate risk, mOS ranged from 9.7 to 35.6 months in the pre-approval era and from 20.8 to 27.6 months in the post-approval era. mOS was not reached for five additional treatment groups in the post-approval era, which had median follow-up durations of 7.2, 12, 12.4, 13.8, and 16.1 months, respectively.
For patients classified as having intermediate risk, mOS ranged from 12 to 35.9 months in the pre-approval era and was not reached in all three treatment groups in the post-approval era, which had median follow-up durations of 8.96, 12.2, and 24 months, respectively.
For patients classified as having favorable/intermediate risk, mOS was 26.5 months in the pre-approval era and was not reported in the post-approval era.
For patients classified as having favorable risk, mOS ranged from 19.6 to 36 months in the pre-approval era. mOS was not reached for an additional four treatment groups in the pre-approval era; two of these treatment groups had median follow-up durations of 23 and 46.1 months, respectively, and two treatment groups did not report median follow-up duration. mOS was not reached for either treatment group in the post-approval era, both of which had median follow-up durations of 20 months.
For treatment groups consisting of patients with mixed risk classifications, mOS ranged from 13.2 to 40.2 months in the pre-approval era and was 21.9 months in the post-approval era. mOS was not reached for two treatment groups in the post-approval era, which had median follow-up durations of 7 and 9.67 months, respectively.
For treatment groups consisting of patients with unspecified risk classification, mOS ranged from 12.5 to 52.97 months in the pre-approval era and was not reported in the post-approval era.
A summary and detailed information on median follow-up durations, mOS, and landmark OS rates are provided in Supplementary Tables S27 and S28.
3.3.5 Study quality
Most studies were judged to be of fair quality in both the pre- and post-approval eras, largely due to the absence of a non-exposed cohort and some concerns regarding the representativeness of the exposed cohort, demonstration that the outcome of interest was not present at the start of the study, length of follow-up, and adequacy of follow-up of cohorts (Supplementary Table S29).
4 Discussion
The development and regulatory approval of ICIs, including anti-PD-(L)1 agents, has dramatically changed the way cancer is treated in clinical practice. However, as the regulatory approval of cancer treatments is largely based on the findings of RCTs, it is unclear whether treatment efficacy as measured in these tightly controlled trials translates to real-world settings. Therefore, the objective of this SLR was to understand the real-world OS of patients with advanced/metastatic melanoma, NSCLC, or RCC who would currently be eligible, based on their clinical presentation, for treatment with an anti-PD-(L)1 agent but were treated with conventional care before the regulatory approval of anti-PD-(L)1 therapy and of patients treated with anti-PD-(L)1 agents after their approval.
The results of this SLR show that mOS values in the post-approval era tended to be longer than those in the pre-approval era for patients with advanced/metastatic NSCLC in the first-line setting, including NSCLC patients with PD-L1-positive tumors who received anti-PD-(L)1 monotherapy and NSCLC patients with non-squamous cell carcinoma who received anti-PD-(L)1 combination therapy. Notably, the ranges in mOS values for PD-L(1)-treated NSCLC patients observed in this SLR are similar to those reported in previous SLRs and meta-analyses of real-world studies evaluating ICI therapies in NSCLC patients (9–11, 195), including a meta-analysis demonstrating similar efficacy/effectiveness of ICIs in terms of mOS between RCTs and real-world studies (12). In addition, mOS tended to be longer in the post-approval era than the pre-approval era for advanced/metastatic melanoma patients with BRAF mutations and high-risk advanced RCC patients.
Conclusions drawn from this study may be limited by some considerations. First, there were imbalances in the numbers of pre- versus post-approval studies for each tumor type. This was especially pronounced for advanced/metastatic melanoma, for which only one pre-approval study was identified. As this study evaluated a targeted agent (i.e., vemurafenib) in patients with BRAF V600E mutations, the OS of patients in this study may not be representative of the OS of general advanced/metastatic melanoma patients who received conventional therapy before the approval of PD-(L)1 therapy. Second, while the aim of this study was to provide a global view of real-world OS before and after the approval of PD-(L)1 therapy, there were some imbalances in the geographical locations of studies in the pre- and post-approval eras for certain tumor types. Third, as measurements of OS are influenced by all therapies received by patients throughout their disease course, the mOS values reported by observational studies may have been impacted by other therapies received by patients (including subsequent lines of therapy) that were not a focus of or described by the studies. Fourth, most included studies were only of fair quality due to their lack of detailed reporting on study methodology, leading to concerns about the potential existence of bias in patient selection and outcome assessment. Fifth, mOS was reported as ‘not reached’ for some treatment groups. Thus, there is uncertainty as to whether this reflects the prolonged survival of patients or an insufficient study follow-up duration, as many studies did not report follow-up durations. Notably, mOS tended to be more frequently reported as ‘not reached’ in post-approval era studies, which may have served to artificially truncate the upper bound of the range in mOS values and thereby conceal a potential survival benefit in the post-approval era. Sixth, there was substantial heterogeneity among included studies in study objectives, patient characteristics, and evaluated treatment regimens, which may have contributed to between-study variation in OS. Future research involving a formal quantitative analysis such as a meta-regression to control for potential sources of variance in OS outcomes and determine the statistical significance of differences in pre- vs. post-approval OS could help overcome this limitation. Finally, this SLR was limited by the availability of published data, with an inherent potential risk of publication bias.
Despite these limitations, this SLR also has strengths that maximize its comprehensiveness and rigor. It involved highly sensitive searches of the peer-reviewed literature, the review process was guided by pre-defined eligibility criteria established in a protocol, and data quality was ensured through the involvement of two reviewers in the study selection and data extraction phases. Moreover, rather than focusing on ICIs in general, the present study investigated the survival of similar populations of cancer patients before versus after the approval of anti-PD-(L)1 therapies in particular. Thus, this SLR generated a large, unique evidence base encompassing real-world evidence on the treatment of advanced/metastatic melanoma, NSCLC, and RCC that enriches our understanding of the degree of value and improvements in outcomes that anti-PD-(L)1 therapy has brought to cancer patients in actual clinical practice.
5 Conclusion
In conclusion, a survival benefit in real-world practice was observed for patients with advanced/metastatic NSCLC, RCC, or melanoma receiving first-line anti-PD-(L)1 therapy after its regulatory approval when compared with patients treated with conventional care before anti-PD-(L)1 therapy approval. This supports the use of anti-PD-(L)1 therapy as a standard of care in many countries.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
DN: Writing – review & editing, Software, Methodology, Conceptualization, Investigation, Writing – original draft, Formal Analysis, Visualization, Data curation, Validation. KA: Data curation, Visualization, Formal Analysis, Validation, Writing – review & editing, Methodology, Software, Writing – original draft, Conceptualization, Investigation, Supervision. AF: Writing – review & editing, Writing – original draft, Software, Conceptualization, Investigation, Project administration, Formal Analysis, Validation, Visualization, Data curation, Methodology, Supervision. YM: Formal Analysis, Visualization, Writing – original draft, Data curation, Investigation, Validation, Writing – review & editing. RA-I: Data curation, Methodology, Project administration, Visualization, Conceptualization, Validation, Writing – original draft, Funding acquisition, Investigation, Resources, Supervision, Formal Analysis, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. The authors declare that this study was funded by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
We thank Diana Chirovsky (Merck & Co., Inc., Rahway, NJ, USA) and Manasi Thosar, Braden Hale, Shivani Mehta, Ping Wu, Asfar Khan, Michael Juan, and Cory Williams (Precision AQ) for their contributions to this study.
Conflict of interest
RA-I is an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and a shareholder of Merck & Co., Inc., Rahway, NJ, USA. YM was an employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, at the time the study was conducted. DN, KA, and AF are employees of Precision AQ, a healthcare research consulting firm that received funding from Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, to conduct the research described in this manuscript.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1615795/full#supplementary-material
References
1. Waldman AD, Fritz JM, and Lenardo MJ. A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nat Rev Immunol. (2020) 20:651–68. doi: 10.1038/s41577-020-0306-5
2. Bagchi S, Yuan R, and Engleman EG. Immune checkpoint inhibitors for the treatment of cancer: clinical impact and mechanisms of response and resistance. Annu Rev Pathol. (2021) 16:223–49. doi: 10.1146/annurev-pathol-042020-042741
3. Sherman RE, Anderson SA, Dal Pan GJ, Gray GW, Gross T, Hunter NL, et al. Real-world evidence—what is it and what can it tell us. N Engl J Med. (2016) 375:2293–7. doi: 10.1056/NEJMsb1609216
4. Tan YY, Papez V, Chang WH, Mueller SH, Denaxas S, and Lai AG. Comparing clinical trial population representativeness to real-world populations: an external validity analysis encompassing 43 895 trials and 5 685 738 individuals across 989 unique drugs and 286 conditions in England. Lancet Healthy Longevity. (2022) 3:e674–89. doi: 10.1016/S2666-7568(22)00186-6
5. Iacovino ML, Celant S, Tomassini L, Arenare L, Caglio A, Canciello A, et al. Comparison of baseline patient characteristics in Italian oncology drug monitoring registries and clinical trials: a&xa0;real-world cross-sectional study. Lancet Regional Health – Europe. (2024) 41:100912. doi: 10.1016/j.lanepe.2024.100912
6. Michael S, Sue C, Matthew T, Majid R, Will S, Laure L, et al. Treatment patterns and survival outcomes for patients with non-small cell lung cancer in the UK in the preimmunology era: a REAL-Oncology database analysis from the I-O Optimise initiative. BMJ Open. (2021) 11:e046396. doi: 10.1136/bmjopen-2020-046396
7. Lamba N, Ott PA, and Iorgulescu JB. Use of first-line immune checkpoint inhibitors and association with overall survival among patients with metastatic melanoma in the anti–PD-1 era. JAMA Network Open. (2022) 5:e2225459–e2225459. doi: 10.1001/jamanetworkopen.2022.25459
8. Danesi V, Massa I, Foca F, Delmonte A, Crinò L, Bronte G, et al. Real-world outcomes and treatments patterns prior and after the introduction of first-line immunotherapy for the treatment of metastatic non-small cell lung cancer. Cancers. (2022) 14:4481. doi: 10.3390/cancers14184481
9. Pasello G, Pavan A, Attili I, Bortolami A, Bonanno L, Menis J, et al. Real world data in the era of Immune Checkpoint Inhibitors (ICIs): Increasing evidence and future applications in lung cancer. Cancer Treat Rev. (2020) 87:102031. doi: 10.1016/j.ctrv.2020.102031
10. Juarez-Garcia A, Sharma R, Hunger M, Kayaniyil S, Penrod JR, and Chouaïd C. Real-world effectiveness of immunotherapies in pre-treated, advanced non-small cell lung cancer Patients: A systematic literature review. Lung Cancer. (2022) 166:205–20. doi: 10.1016/j.lungcan.2022.03.008
11. Luciani A, Ghidini A, Dottorini L, and Petrelli F. Safety and effectiveness of immune checkpoint inhibitors in older patients with cancer: A systematic review of 48 real-world studies. Drugs Aging. (2021) 38:1055–65. doi: 10.1007/s40266-021-00899-7
12. Digkas E, Tabiim AJ, Smith D, and Valachis A. Randomized versus real-world evidence on the efficacy and toxicity of checkpoint inhibitors in cancer in patients with advanced non-small cell lung cancer or melanoma: A meta-analysis. Target Oncol. (2022) 17:507–15. doi: 10.1007/s11523-022-00901-1
13. Chandler J, Cumpston M, Li T, Page MJ, and Welch V. Cochrane handbook for systematic reviews of interventions. Hoboken: Wiley. (2019). doi: 10.1002/9781119536604
14. National Institute for Health and Clinical Excellence (NICE)The guidelines manual: process and methods [PMG6. NICE. (2012).
15. Moher D, Liberati A, Tetzlaff J, Altman DG, and t. PRISMA Group*. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Internal Med. (2009) 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
16. U.S. Food and Drug AdministrationTECENTRIQ® (atezolizumab) injection, for intravenous use, U.S. Food and Drug Administration. U.S. Food and Drug Administration (2022).
17. European Medicines AgencyTecentriq, european medicines agency. European Medicines Agency (2023).
18. U.S. Food and Drug AdministrationBAVENCIO® (avelumab) injection, for intravenous use, U.S. Food & Drug Administration. U.S. Food and Drug Administration (2022).
20. U.S. Food and Drug AdministrationLIBTAYO® (cemiplimab-rwlc) injection, for intravenous use, U.S. Food and Drug Administration. U.S. Food and Drug Administration (2022).
22. U.S. Food and Drug AdministrationIMFINZI® (durvalumab) injection, for intravenous use, U.S. Food and Drug Administration. U.S. Food and Drug Administration (2022).
24. U.S. Food and Drug AdministrationKEYTRUDA® (pembrolizumab) injection, for intravenous use U.S. Food and Drug Administration. U.S. Food and Drug Administration (2023).
26. U.S. Food and Drug AdministrationOPDIVO® (nivolumab) injection, for intravenous use, U.S. Food and Drug Administration. U.S. Food and Drug Administration (2022).
28. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. The Ottawa Hospital Research Institute (2021).
29. Fennira F, Pages C, Schneider P, Sidina I, Viguier M, Basset-Seguin N, et al. Vemurafenib in the French temporary authorization for use metastatic melanoma cohort: A single-centre trial. Melanoma Res. (2014) 24:75–82. doi: 10.1097/CMR.0000000000000034
30. Ab Rahman AS, Strother RM, and Paddison J. New Zealand national retrospective cohort study of survival outcomes of patients with metastatic melanoma receiving immune-checkpoint inhibitors. Asia-Pacific J Clin Oncol. (2023) 19:179–86. doi: 10.1111/ajco.13801
31. Afrasanie VA, Alexa-Stratulat T, Gafton B, Froicu EM, Sur D, Lungulescu CV, et al. A real-world analysis of nivolumab in first line metastatic melanoma assessing efficacy, safety and predictive factors. Cancers. (2023) 15:1265. doi: 10.3390/cancers15041265
32. Amaral T, Seeber O, Mersi E, Sanchez S, Thomas I, Meiwes A, et al. Primary resistance to pd-1-based immunotherapy- a study in 319 patients with stage iv melanoma. Cancers 12(4) (no pagination). (2020) 12:1027. doi: 10.3390/cancers12041027
33. Board R, Smittenaar R, Lawton S, Liu H, Juwa B, Chao D, et al. Metastatic melanoma patient outcomes since introduction of immune checkpoint inhibitors in England between 2014 and 2018. Int J Cancer. (2021) 148:868–75. doi: 10.1002/ijc.v148.4
34. Cowey CL, Boyd M, Aguilar KM, Beeks A, Krepler C, and Scherrer E. An observational study of drug utilization and associated outcomes among adult patients diagnosed with BRAF-mutant advanced melanoma treated with first-line anti-PD-1 monotherapies or BRAF/MEK inhibitors in a community-based oncology setting. Cancer Med. (2020) 9:7863–78. doi: 10.1002/cam4.v9.21
35. Cowey CL, Liu FX, Black-Shinn J, Stevinson K, Boyd M, Frytak JR, et al. Pembrolizumab utilization and outcomes for advanced melanoma in US community oncology practices. J Immunotherapy. (2018) 41:86–95. doi: 10.1097/CJI.0000000000000204
36. Cowey CL, Scherrer E, Boyd M, Aguilar KM, Beeks A, and Krepler C. Pembrolizumab utilization and clinical outcomes among patients with advanced melanoma in the US community oncology setting: an updated analysis. J immunotherapy. (2021) 44:224–33. doi: 10.1097/CJI.0000000000000363
37. Hribernik N, Boc M, Ocvirk J, Knez-Arbeiter J, Mesti T, Ignjatovic M, et al. Retrospective analysis of treatment-naive Slovenian patients with metastatic melanoma treated with pembrolizumab-real-world experience. Radiol Oncol. (2020) 54:119–27. doi: 10.2478/raon-2020-0003
38. Inozume T, Namikawa K, Kato H, Yoshikawa S, Kiniwa Y, Yoshino K, et al. Analyzing the relationship between the efficacy of first-line immune checkpoint inhibitors and cumulative sun damage in Japanese patients with advanced BRAF wild-type nonacral cutaneous melanoma: A retrospective real-world, multicenter study. J Dermatol Sci. (2023) 110:19–26. doi: 10.1016/j.jdermsci.2023.03.008
39. Iravani A, Wallace R, Lo SN, Galligan A, Weppler AM, Hicks RJ, et al. FDG PET/CT prognostic markers in patients with advanced melanoma treated with ipilimumab and nivolumab. Radiology. (2023) 307:e221180. doi: 10.1148/radiol.221180
40. Kartolo A, Yeung C, Kuksis M, Hopman W, and Baetz T. Improved overall survival in dual compared to single immune checkpoint inhibitors in BRAF V600-negative advanced melanoma. Melanoma Manage. (2022) 9:MMT60. doi: 10.2217/mmt-2021-0005
41. Kuzmanovszki D, Kiss N, Toth B, Kerner T, Toth V, Szakonyi J, et al. Anti-PD-1 monotherapy in advanced melanoma-real-world data from a 77-month-long retrospective observational study. Biomedicines. (2022) 10:19. doi: 10.3390/biomedicines10071737
42. Mason R, Dearden HC, Nguyen B, Soon JA, Smith JL, Randhawa M, et al. Combined ipilimumab and nivolumab first-line and after BRAF-targeted therapy in advanced melanoma. Pigment Cell Melanoma Res. (2020) 33:358–65. doi: 10.1111/pcmr.12831
43. Mohr P, Scherrer E, Assaf C, Bender M, Berking C, Chandwani S, et al. Real-world therapy with pembrolizumab: outcomes and surrogate endpoints for predicting survival in advanced melanoma patients in Germany. Cancers. (2022) 14:1804. doi: 10.3390/cancers14071804
44. Monestier S, Dalle S, Mortier L, Dutriaux C, Dalac-Rat S, Meyer N, et al. Effectiveness and safety of nivolumab in patients with advanced melanoma: A multicenter, observational study. Int J cancer. (2021) 11:2789–98. doi: 10.1002/ijc.v148.11
45. O’Sullivan DE, Boyne DJ, Gogna P, Brenner DR, and Cheung WY. Understanding real-world treatment patterns and clinical outcomes among metastatic melanoma patients in alberta, Canada. Curr Oncol. (2023) 30:4166–76. doi: 10.3390/curroncol30040317
46. Parakh S, Randhawa M, Nguyen B, Warburton L, Hussain MA, Cebon J, et al. Real-world efficacy and toxicity of combined nivolumab and ipilimumab in patients with metastatic melanoma. Asia-Pacific J Clin Oncol. (2019) 15:26–30. doi: 10.1111/ajco.2019.15.issue-1
47. Pavlick AC, Zhao R, Lee CH, Ritchings C, and Rao S. First-line immunotherapy versus targeted therapy in patients with BRAF-mutant advanced melanoma: A real-world analysis. Future Oncol. (2021) 17:689–99. doi: 10.2217/fon-2020-0643
48. Peisen F, Hansch A, Hering A, Brendlin AS, Afat S, Nikolaou K, et al. Combination of whole-body baseline CT radiomics and clinical parameters to predict response and survival in a stage-IV melanoma cohort undergoing immunotherapy. Cancers. (2022) 14:2992. doi: 10.3390/cancers14122992
49. Rivas A, Delyon J, Martineau A, Blanc E, Allayous C, Da Meda L, et al. 18FDG PET assessment of therapeutic response in patients with advanced or metastatic melanoma treated with first-line immune checkpoint inhibitors. Cancers. (2022) 14:3190. doi: 10.3390/cancers14133190
50. Stein C, Burtey S, Mancini J, Pelletier M, Sallee M, Brunet P, et al. Acute kidney injury in patients treated with anti-programmed death receptor-1 for advanced melanoma: a real-life study in a single-centre cohort. Nephrology dialysis transplantation: Off Publ Eur Dialysis Transplant Assoc Eur Renal Assoc. (2020) 17:1664–74. doi: 10.1093/ndt/gfaa137
51. Suo A, Chan Y, Beaulieu C, Kong S, Cheung WY, Monzon JG, et al. Anti-PD1-induced immune-related adverse events and survival outcomes in advanced melanoma. oncologist. (2020) 12:438–46. doi: 10.1634/theoncologist.2019-0674
52. Tarhini A, Atzinger C, Gupte-Singh K, Johnson C, Macahilig C, and Rao S. Treatment patterns and outcomes for patients with unresectable stage III and metastatic melanoma in the USA. J Comp Effectiveness Res. (2019) 8:461–73. doi: 10.2217/cer-2019-0003
53. Wei KZ, Baxter M, and Casasola R. Hypophysitis induced by immune checkpoint inhibitors in a Scottish melanoma population. Melanoma Manage. (2019) 6:MMT13. doi: 10.2217/mmt-2018-0009
54. Wilson T, Taylor H, Winter H, and Herbert C. Sequential immunotherapy in melanoma: is it a realistic alternative to dual immunotherapy? Melanoma Res. (2021) 31:366–70. doi: 10.1097/CMR.0000000000000746
55. Liu FX, Ou W, Diede SJ, and Whitman ED. Real-world experience with pembrolizumab in patients with advanced melanoma: A large retrospective observational study. Medicine. (2019) 98:e16542. doi: 10.1097/MD.0000000000016542
56. Casarotto E, Chandwani S, Mortier L, Dereure O, Dutriaux C, Dalac S, et al. Real-world effectiveness of pembrolizumab in advanced melanoma: analysis of a French national clinicobiological database. Immunother 02. (2021) 13:905–16. doi: 10.2217/imt-2021-0077
57. Hurkmans DP, Jensen C, Koolen SLW, Aerts J, Karsdal MA, Mathijssen RHJ, et al. Blood-based extracellular matrix biomarkers are correlated with clinical outcome after PD-1 inhibition in patients with metastatic melanoma. J ImmunoTherapy Cancer. (2020) 8:e001193. doi: 10.1136/jitc-2020-001193
58. van Breeschoten J, Wouters MWJM, Hilarius DL, Haanen JB, Blank CU, Aarts MJB, et al. First-line BRAF/MEK inhibitors versus anti-PD-1 monotherapy in BRAFV600-mutant advanced melanoma patients: a propensity-matched survival analysis. Br J Cancer. (2021) 124:1222–30. doi: 10.1038/s41416-020-01229-1
59. Zaremba A, Mohr P, Gutzmer R, Meier F, Pfohler C, Weichenthal M, et al. Immune checkpoint inhibition in patients with NRAS mutated and NRAS wild type melanoma: a multicenter Dermatologic Cooperative Oncology Group study on 637 patients from the prospective skin cancer registry ADOREG. Eur J Cancer. (2023) 188:140–51. doi: 10.1016/j.ejca.2023.04.008
60. Van Zeijl MCT, Haanen JBAG, Wouters MWJM, De Wreede LC, Jochems A, Aarts MJB, et al. Real-world outcomes of first-line anti-PD-1 therapy for advanced melanoma: A nationwide population-based study. J Immunotherapy. (2020) 43:256–64. doi: 10.1097/CJI.0000000000000334
61. Van Zeijl MCT, Van Breeschoten J, De Wreede LC, Wouters MWJM, Hilarius DL, Blank CU, et al. Real-world outcomes of ipilimumab plus nivolumab combination therapy in a nation-wide cohort of advanced melanoma patients in the Netherlands. J Immunotherapy. (2023) 46:197–204. doi: 10.1097/CJI.0000000000000468
62. Czarnecka AM, Teterycz P, Mariuk-Jarema A, Lugowska I, Rogala P, Dudzisz-Sledz M, et al. Treatment sequencing and clinical outcomes in BRAF-positive and BRAF-negative unresectable and metastatic melanoma patients treated with new systemic therapies in routine practice. Targeted Oncol. (2019) 21:729–42. doi: 10.1007/s11523-019-00688-8
63. Abernethy AP, Arunachalam A, Burke T, McKay C, Cao X, Sorg R, et al. Real-world first-line treatment and overall survival in non-small cell lung cancer without known EGFR mutations or ALK rearrangements in US community oncology setting. PloS One. (2017) 12:e0178420. doi: 10.1371/journal.pone.0178420
64. Bonanno L, Paoli AD, Zulato E, Esposito G, Calabrese F, Favaretto A, et al. LKB1 expression correlates with increased survival in patients with advanced non-small cell lung cancer treated with chemotherapy and bevacizumab. Clin Cancer Res. (2017) 23:3316–24. doi: 10.1158/1078-0432.CCR-16-2410
65. Camerini A, Chella A, Mazzoni F, Puccetti C, Donati S, Lunghi A, et al. First-line treatment of NSCLC with bevacizumab: real world data from an Italian regional based survey. J Chemother. (2017) 29:38–41. doi: 10.1080/1120009X.2016.1219498
66. Chen X, Zhu Q, Liu Y, Liu P, Yin Y, Guo R, et al. Icotinib is an active treatment of non-small-cell lung cancer: a retrospective study. PloS One. (2014) 9:e95897. doi: 10.1371/journal.pone.0095897
67. Elsamany SA, Al-Fayea TM, Alzahrani AS, Abozeed WN, Darwish W, Farooq MU, et al. Thyroid transcription factor-1 expression in advanced non- small cell lung cancer: impact on survival outcome. Asian Pacific J Cancer prevention: APJCP. (2015) 16:2987–91. doi: 10.7314/APJCP.2015.16.7.2987
68. Isobe H, Mori K, Minato K, Katsura H, Taniguchi K, Arunachalam A, et al. Real-world practice patterns for patients with advanced non-small cell lung cancer: multicenter retrospective cohort study in Japan. Lung Cancer (Auckl). (2017) 8:191–206. doi: 10.2147/LCTT.S140491
69. Kohutek F, Stratena M, Rosik A, Tamasova M, and Bystricky B. First-line treatment of nonsquamous NSCLC using gemcitabine: A retrospective study of real-life practice. Lung Cancer Manage. (2016) 5:123–30. doi: 10.2217/lmt-2016-0011
70. Mudad R, Patel MB, Margunato-Debay S, Garofalo D, and Lal LS. Comparative effectiveness and safety of nab-paclitaxel plus carboplatin vs gemcitabine plus carboplatin in first-line treatment of advanced squamous cell non-small cell lung cancer in a US community oncology setting. Lung Cancer: Targets Ther. (2017) 8:179–90. doi: 10.2147/LCTT.S139647
71. Perez-Moreno MA, Cotrina-Luque J, Galvan-Banqueri M, Flores-Moreno S, Bautista-Paloma FJ, and Calleja-Hernandez MA. Effectiveness and safety of pemetrexed for non-small cell lung cancer in the Andalusian Public Health System. Farm. (2016) 40:477–85. doi: 10.7399/fh.2016.40.6.10424
72. de Castro J, Tagliaferri P, de Lima VCC, Ng S, Thomas M, Arunachalam A, et al. Systemic therapy treatment patterns in patients with advanced non-small cell lung cancer (NSCLC): PIvOTAL study. Eur J Cancer Care (Engl). (2017) 26:e12734. doi: 10.1111/ecc.12734
73. Shen L, Niu X, Jian H, Xu Y, Yu Y, and Lu S. Assessment of interfering factors and clinical risk associated with discontinuation of pemetrexed maintenance therapy in advanced non-squamous non-small cell lung cancer. Lung Cancer. (2017) 111:43–50. doi: 10.1016/j.lungcan.2017.07.001
74. Thippeswamy R, Patil S, Prashanth P, Sateesh CT, Vittal T, Shashidhara HP, et al. Outcomes in lung cancer: An experience from routine tertiary care setting. Indian J Cancer. (2017) 54:276–9. doi: 10.4103/0019-509X.219606
75. Xu J, Liu X, Yang S, Zhang X, and Shi Y. Efficacy of icotinib in lung squamous-cell cancer: A real-world experience from single institution. Asia-Pacific J Clin Oncol. (2017) 13:379–84. doi: 10.1111/ajco.2017.13.issue-6
76. Banna GL, Anile G, Russo G, Vigneri P, Castaing M, Nicolosi M, et al. Predictive and prognostic value of early disease progression by PET evaluation in advanced non-small cell lung cancer. Oncol (Switzerland). (2017) 92:39–47. doi: 10.1159/000448005
77. von Verschuer U, Schnell R, Tessen HW, Eggert J, Binninger A, Spring L, et al. Treatment, outcome and quality of life of 1239 patients with advanced non-small cell lung cancer - final results from the prospective German TLK cohort study. Lung Cancer. (2017) 112:216–24. doi: 10.1016/j.lungcan.2017.07.031
78. Aggarwal H, Bayo K, Han Y, Muehlenbein CE, Zhu YE, and Kim JS. Real-world maintenance therapy and survival outcomes for pembrolizumab plus pemetrexed and platinum for non-small-cell lung cancer in USA. Immunotherapy. (2023) 15:267–81. doi: 10.2217/imt-2022-0166
79. Akazawa Y, Yoshikawa A, Kanazu M, Yano Y, Yamaguchi T, and Mori M. Non-small cell lung cancer with tumor proportion score > 90% could increase the risk of severe immune-related adverse events in first-line treatments with immune checkpoint inhibitors: A retrospective single-center study. Thorac Cancer. (2022) 13:2450–8. doi: 10.1111/1759-7714.14576
80. Attili I, Valenza C, Santoro C, Antonarelli G, Trillo Aliaga P, Del Signore E, et al. Comparison of real-world data (RWD) analysis on efficacy and post-progression outcomes with pembrolizumab plus chemo vs chemo alone in metastatic non-squamous non-small cell lung cancer with PD-L1 < 50%. Front Oncol. (2022) 12. doi: 10.3389/fonc.2022.980765
81. Banna GL, Signorelli D, Metro G, Galetta D, Toma A, Cantale O, et al. Neutrophil-to-lymphocyte ratio in combination with PD-L1 or lactate dehydrogenase as biomarkers for high PD-L1 non-small cell lung cancer treated with first-line pembrolizumab. Trans Lung Cancer Res. (2020) 9:1533–42. doi: 10.21037/tlcr-19-583
82. Bjornhart B, Hansen KH, Jorgensen TL, Herrstedt J, and Schytte T. Efficacy and safety of immune checkpoint inhibitors in a Danish real life non-small cell lung cancer population: a retrospective cohort study. Acta Oncol. (2019) 58:953–61. doi: 10.1080/0284186X.2019.1615636
83. Bureau M, Chatellier T, Perennec T, Goronflot T, Greilsamer C, Chene AL, et al. Baseline tumour size is an independent prognostic factor for overall survival in PD-L1 >= 50% non-small cell lung cancer patients treated with first-line pembrolizumab. Cancer Immunology Immunotherapy. (2022) 71:1747–56. doi: 10.1007/s00262-021-03108-x
84. Cavaille F, Peretti M, Garcia ME, Giorgi R, Ausias N, Vanelle P, et al. Real-world efficacy and safety of pembrolizumab in patients with non-small cell lung cancer: a retrospective observational study. Tumori. (2020) 107:300891620926244. doi: 10.1177/0300891620926244
85. Chang KC, Shao SC, Chen HY, Chan YY, and Fang YF. Comparative effectiveness and safety of standard-dose and low-dose pembrolizumab in patients with non-small-cell lung cancer: A multi-institutional cohort study in Taiwan. Cancers. (2022) 14:1157. doi: 10.3390/cancers14051157.
86. Chen Y, Wang Y, Yang Z, Hu M, Zhang Y, Qian F, et al. Pembrolizumab alone or combined with chemotherapy in advanced NSCLC with PD-L1 >=50%: results of a retrospective study. Front Oncol 11 (no pagination). (2021) 11. doi: 10.3389/fonc.2021.691519
87. Cortellini A, Tiseo M, Banna GL, Cappuzzo F, Aerts J, Barbieri F, et al. Clinicopathologic correlates of first-line pembrolizumab effectiveness in patients with advanced NSCLC and a PD-L1 expression of >= 50. Cancer Immunology Immunotherapy. (2020) 69:2209–21. doi: 10.1007/s00262-020-02613-9
88. Descourt R, Greillier L, Perol M, Ricordel C, Auliac JB, Falchero L, et al. First-line single-agent pembrolizumab for PD-L1-positive (tumor proportion score >= 50%) advanced non-small cell lung cancer in the real world: impact in brain metastasis: a national French multicentric cohort (ESCKEYP GFPC study). Cancer Immunology Immunotherapy. (2023) 72:91–9. doi: 10.1007/s00262-022-03232-2
89. Dube-Pelletier M, Labbe C, Cote J, and Pelletier-St-Pierre AA. Pembrolizumab every 6 weeks versus every 3 weeks in advanced non-small cell lung cancer. oncologist. (2023) 26:969–77. doi: 10.1093/oncolo/oyad182
90. Dudnik E, Kareff S, Moskovitz M, Kim C, Liu SV, Lobachov A, et al. Real-world survival outcomes with immune checkpoint inhibitors in large-cell neuroendocrine tumors of lung. J ImmunoTherapy Cancer. (2021) 9:e001999. doi: 10.1136/jitc-2020-001999
91. Dudnik E, Moskovitz M, Daher S, Shamai S, Hanovich E, Grubstein A, et al. Effectiveness and safety of nivolumab in advanced non-small cell lung cancer: The real-life data. Lung Cancer. (2018) 126:217–23. doi: 10.1016/j.lungcan.2017.11.015
92. Eklund EA, Wiel C, Fagman H, Akyurek LM, Raghavan S, Nyman J, et al. KRAS mutations impact clinical outcome in metastatic non-small cell lung cancer. medRxiv. (2021) 28:2063. doi: 10.3390/cancers14092063
93. Faoro L, Brusegan A, Russi A, Calderone V, Martelli A, Marranconi E, et al. Analysis of the relation between adverse events and overall survival in patients treated with pembrolizumab as a first-line treatment for metastatic NSCLC. BMC Pharmacol Toxicol. (2023) 24:32. doi: 10.1186/s40360-023-00663-0
94. Frost N, Kollmeier J, Misch D, Vollbrecht C, Grah C, Matthes B, et al. Pembrolizumab as first-line palliative therapy in PD-L1 overexpressing (>= 50%) NSCLC: real-world results with special focus on PS >= 2, brain metastases, and steroids. Clin Lung Cancer. (2021) 22:411–22. doi: 10.1016/j.cllc.2021.02.001
95. Frost N, Kollmeier J, Vollbrecht C, Grah C, Matthes B, Pultermann D, et al. KRASG12C/TP53 co-mutations identify long-term responders to first line palliative treatment with pembrolizumab monotherapy in PD-L1 high (≥ 50%) lung adenocarcinoma. Trans Lung Cancer Res. (2021) 10:737. doi: 10.21037/tlcr-20-958
96. Fujimoto D, Miura S, Yoshimura K, Wakuda K, Oya Y, Yokoyama T, et al. Pembrolizumab plus chemotherapy-induced pneumonitis in chemo-naive patients with non-squamous non-small cell lung cancer: A multicentre, retrospective cohort study. Eur J Cancer. (2021) 150:63–72. doi: 10.1016/j.ejca.2021.03.016
97. Geiger-Gritsch S, Olschewski H, Kocher F, Wurm R, Absenger G, Flicker M, et al. Real-world experience with anti-PD-1/PD-L1 monotherapy in patients with non-small cell lung cancer: A retrospective Austrian multicenter study. Wiener Klinische Wochenschrift. (2021) 133:1122–30. doi: 10.1007/s00508-021-01940-w
98. Genova C, Tasso R, Rosa A, Rossi G, Reverberi D, Fontana V, et al. Prognostic role of soluble and extracellular vesicle-associated PD-L1, B7-H3 and B7-H4 in non-small cell lung cancer patients treated with immune checkpoint inhibitors. Cells. (2023) 12:832. doi: 10.3390/cells12060832
99. Goto Y, Tamura A, Matsumoto H, Isobe K, Ozaki T, Santorelli ML, et al. First-line pembrolizumab monotherapy for advanced NSCLC with programmed death-ligand 1 expression greater than or equal to 50%: real-world study including older patients in Japan. JTO Clin Res Rep. (2022) 3:100397. doi: 10.1016/j.jtocrr.2022.100397
100. Hasegawa T, Yanagitani N, Ninomiya H, Sakamoto H, Tozuka T, Yoshida H, et al. Association between the efficacy of pembrolizumab and low STK11/LKB1 expression in high-PD-L1-expressing non-small-cell lung cancer. Vivo. (2020) 34:2997–3003. doi: 10.21873/invivo.12131
101. Holtzman L, Moskovitz M, Urban D, Nechushtan H, Keren S, Reinhorn D, et al. dNLR-based score predicting overall survival benefit for the addition of platinum-based chemotherapy to pembrolizumab in advanced NSCLC with PD-L1 tumor proportion score≥ 50%. Clin Lung Cancer. (2022) 23:122–34. doi: 10.1016/j.cllc.2021.12.006
102. Hu F, Peng J, Niu Y, Mao X, Zhao Y, and Jiang L. Clinical predictors of treatment efficacy and a prognostic nomogram in patients with lung adenocarcinoma receiving immune checkpoint inhibitors: a retrospective study. J. (2022) 14:4096–112. doi: 10.21037/jtd-22-1270
103. Ikeuchi N, Igata F, Kinoshita E, Kawabata T, Tan I, Osaki Y, et al. Real-world efficacy and safety of atezolizumab plus bevacizumab, paclitaxel and carboplatin for first-line treatment of Japanese patients with metastatic non-squamous non-small cell lung cancer. Anticancer Res. (2023) 43:713–24. doi: 10.21873/anticanres.16210
104. Imai H, Kishikawa T, Minemura H, Yamada Y, Ibe T, Yamaguchi O, et al. Pretreatment Glasgow prognostic score predicts survival among patients with high PD-L1 expression administered first-line pembrolizumab monotherapy for non-small cell lung cancer. Cancer Med. (2021) 10:6971–84. doi: 10.1002/cam4.v10.20
105. Isono T, Kagiyama N, Shibata S, Nakajima H, Matsui Y, Takano K, et al. A retrospective analysis of pembrolizumab plus chemotherapy versus pembrolizumab monotherapy for advanced or recurrent non-small cell lung cancer. Thorac Cancer. (2021) 12:1387–97. doi: 10.1111/1759-7714.13915
106. Kaira K, Yamaguchi O, Kawasaki T, Hashimoto K, Miura Y, Shiono A, et al. Prognostic significance of tumor infiltrating lymphocytes on first-line pembrolizumab efficacy in advanced non-small cell lung cancer. Discover Oncol. (2023) 14:6. doi: 10.1007/s12672-023-00615-4
107. Lang D, Huemer F, Rinnerthaler G, Horner A, Wass R, Brehm E, et al. Therapy line and associated predictors of response to PD-1/PD-L1-inhibitor monotherapy in advanced non-small-cell lung cancer: A retrospective bi-centric cohort study. Targeted Oncol 25. (2019) 14:707–17. doi: 10.1007/s11523-019-00679-9
108. Lenci E, Cantini L, Pecci F, Cognigni V, Agostinelli V, Mentrasti G, et al. The gustave roussy immune (Grim)-score variation is an early-on-treatment biomarker of outcome in advanced non-small cell lung cancer (nsclc) patients treated with first-line pembrolizumab. J Clin Med. (2021) 10:1–14. doi: 10.3390/jcm10051005
109. Lester J, Escriu C, Khan S, Hudson E, Mansy T, Conn A, et al. Retrospective analysis of real-world treatment patterns and clinical outcomes in patients with advanced non-small cell lung cancer starting first-line systemic therapy in the United Kingdom. BMC Cancer 21(1) (no pagination). (2021) 21:515. doi: 10.1186/s12885-021-08096-w
110. Li Q, Zhou Q, Zhao S, Wu P, Shi P, Zeng J, et al. KRAS mutation predict response and outcome in advanced non-small cell lung carcinoma without driver alterations receiving PD-1 blockade immunotherapy combined with platinum-based chemotherapy: a retrospective cohort study from China. Trans Lung Cancer Res. (2022) 11:2136–47. doi: 10.21037/tlcr-22-655
111. Liao J, Liu C, Long Q, Wu X, Wang H, Yu H, et al. Direct comparison between the addition of pembrolizumab or bevacizumab for chemotherapy-based first-line treatment of advanced non-squamous non-small cell lung cancer lacking driver mutations. Front Oncol. (2021) 11. doi: 10.3389/fonc.2021.752545
112. Liu SV, Hu X, Li Y, Zhao B, Burke T, and Velcheti V. Pembrolizumab-combination therapy for previously untreated metastatic nonsquamous NSCLC: Real-world outcomes at US oncology practices. Front Oncol. (2022) 12. doi: 10.3389/fonc.2022.999343
113. Liu SV, Rai P, Wang D, Hu X, and Schwarzenberger PO. First-line pembrolizumab plus chemotherapy for advanced squamous NSCLC: real-world outcomes at U.S. Oncology practices. JTO Clin Res Rep. (2023) 4:100444. doi: 10.1016/j.jtocrr.2022.100444
114. Low JL, Huang Y, Sooi K, Ang Y, Chan ZY, Spencer K, et al. Low dose pembrolizumab in the treatment of advanced non-small cell lung cancer. Int J cancer. 26. (2021) 149:169–76. doi: 10.1002/ijc.v149.1
115. Matsumoto H, Kobayashi N, Somekawa K, Fukuda N, Kaneko A, Kamimaki C, et al. Pembrolizumab monotherapy versus pembrolizumab plus chemotherapy in patients with non-small-cell lung cancer: A multicenter retrospective trial. Thorac Cancer. (2022) 13:228–35. doi: 10.1111/1759-7714.14252
116. Nindra U, Shahnam A, Stevens S, Pal A, Nagrial A, Lee J, et al. Influence of EGFR mutation status and PD-L1 expression in stage III unresectable non-small cell lung cancer treated with chemoradiation and consolidation durvalumab. Asia Pacific J Clin Oncol. (2023) 20:16–24. doi: 10.1111/ajco.13940
117. Nokihara H, Kijima T, Yokoyama T, Kagamu H, Suzuki T, Mori M, et al. Real-World Treatments and Clinical Outcomes in Advanced NSCLC without Actionable Mutations after Introduction of Immunotherapy in Japan. Cancers. (2022) 14:2846. doi: 10.3390/cancers14122846
118. Noordhof AL, Damhuis RAM, Hendriks LEL, de Langen AJ, Timens W, Venmans BJW, et al. Prognostic impact of KRAS mutation status for patients with stage IV adenocarcinoma of the lung treated with first-line pembrolizumab monotherapy. Lung Cancer. (2021) 155:163–9. doi: 10.1016/j.lungcan.2021.04.001
119. Amrane K, Geier M, Corre R, Lena H, Leveiller G, Gadby F, et al. First-line pembrolizumab for non-small cell lung cancer patients with PD-L1 >=50% in a multicenter real-life cohort: The PEMBREIZH study. Cancer Med. (2020) 9:2309–16. doi: 10.1002/cam4.2806
120. Perol M, Felip E, Dafni U, Polito L, Pal N, Tsourti Z, et al. Effectiveness of PD-(L)1 inhibitors alone or in combination with platinum-doublet chemotherapy in first-line (1L) non-squamous non-small-cell lung cancer (Nsq-NSCLC) with PD-L1-high expression using real-world data. Ann Oncol. (2022) 33:511–21. doi: 10.1016/j.annonc.2022.02.008
121. Raez LE, Arrieta O, Chamorro DF, Soberanis-Pina PD, Corrales L, Martin C, et al. Durvalumab after chemoradiation for unresectable stage III non-small cell lung cancer: inferior outcomes and lack of health equity in hispanic patients treated with PACIFIC protocol (LA1-CLICaP). Front Oncol. (2022) 12. doi: 10.3389/fonc.2022.904800
122. Renaud E, Ricordel C, Corre R, Leveiller G, Gadby F, Babey H, et al. Pembrolizumab plus pemetrexed-carboplatin combination in first-line treatment of advanced non-squamous non-small cell lung cancer: a multicenter real-life study (CAP29). Trans Lung Cancer Res. (2023) 12:266–76. doi: 10.21037/tlcr-22-556
123. Sanchez-Gastaldo A, Munoz-Fuentes MA, Molina-Pinelo S, Alonso-Garcia M, Boyero L, and Bernabe-Caro R. Correlation of peripheral blood biomarkers with clinical outcomes in NSCLC patients with high PD-L1 expression treated with pembrolizumab. Trans Lung Cancer Res. (2021) 10:2509–22. doi: 10.21037/tlcr-21-156
124. Seban RD, Assie JB, Giroux-Leprieur E, Massiani MA, Bonardel G, Chouaid C, et al. Prognostic value of inflammatory response biomarkers using peripheral blood and [18F]-FDG PET/CT in advanced NSCLC patients treated with first-line chemo- or immunotherapy. Lung Cancer. (2021) 159:45–55. doi: 10.1016/j.lungcan.2021.06.024
125. Seban RD, Assie JB, Giroux-Leprieur E, Massiani MA, Soussan M, Bonardel G, et al. FDG-PET biomarkers associated with long-term benefit from first-line immunotherapy in patients with advanced non-small cell lung cancer. Ann Nucl Med. (2020) 34:968–74. doi: 10.1007/s12149-020-01539-7
126. Shah M, Hubbard RA, Mamtani R, Marmarelis ME, and Hennessy S. Very high PD-L1 expression as a prognostic indicator of overall survival among patients with advanced non-small cell lung cancer receiving anti-PD-(L)1 monotherapies in routine practice. Pharmacoepidemiology Drug Saf. (2022) 31:1121–6. doi: 10.1002/pds.v31.10
127. Shah M, Mamtani R, Marmarelis ME, and Hennessy S. Chemoimmunotherapy vs. Immunotherapy for first line treatment of advanced non-small cell lung cancer with a PD-L1 expression >=50% or >=90%. Clin Lung Cancer. (2023) 24:235–43. doi: 10.1016/j.cllc.2023.02.007
128. Shah M, Marmarelis ME, Mamtani R, and Hennessy S. Association between survival and very high versus high PD-L1 expression in patients receiving pembrolizumab as first-line treatment for advanced non-small cell lung cancer. Clin Lung Cancer. (2022) 23:731–6. doi: 10.1016/j.cllc.2022.07.003
129. Shalata W, Zolnoorian J, Migliozzi G, Jama AA, Dudnik Y, Cohen AY, et al. Long-lasting therapeutic response following treatment with pembrolizumab in patients with non-small cell lung cancer: A real-world experience. Int. (2023) 24:21. doi: 10.3390/ijms24065938
130. Anpalakhan S, Huddar P, Behrouzi R, Signori A, Cave J, Comins C, et al. The effects of GCSF primary prophylaxis on survival outcomes and toxicity in patients with advanced non-small cell lung cancer on first-line chemoimmunotherapy: A sub-analysis of the spinnaker study. Int. (2023) 24:1746. doi: 10.3390/ijms24021746
131. Anpalakhan S, Huddar P, Behrouzi R, Signori A, Cave J, Comins C, et al. Immunotherapy-related adverse events in real-world patients with advanced non-small cell lung cancer on chemoimmunotherapy: a Spinnaker study sub-analysis. Front Oncol. (2023) 13. doi: 10.3389/fonc.2023.1163768
132. Banna GL, Cantale O, Muthuramalingam S, Cave J, Comins C, Cortellini A, et al. Efficacy outcomes and prognostic factors from real-world patients with advanced non-small-cell lung cancer treated with first-line chemoimmunotherapy: The Spinnaker retrospective study. Int Immunopharmacol. (2022) 110:108985. doi: 10.1016/j.intimp.2022.108985
133. Tamayo-Bermejo R, del Rio-Valencia JC, Mora-Rodriguez B, and Munoz-Castillo I. Effectiveness and safety of pembrolizumab monotherapy in patients with locally advanced or metastatic non-small-cell lung cancer. J Oncol Pharm Pract. (2023) 29:138–44. doi: 10.1177/10781552211061117
134. Tamiya M, Tamiya A, Hosoya K, Taniguchi Y, Yokoyama T, Fukuda Y, et al. Efficacy and safety of pembrolizumab as first-line therapy in advanced non-small cell lung cancer with at least 50% PD-L1 positivity: a multicenter retrospective cohort study (HOPE-001). Investigational New Drugs. (2019) 37:1266–73. doi: 10.1007/s10637-019-00843-y
135. Tibaldi C, Mazzoni F, Scotti V, Vasile E, Pozzessere D, Stasi I, et al. Pembrolizumab for first-line treatment of advanced non-small-cell lung cancer: analysis of prognostic factors of outcomes. Anti-Cancer Agents Medicinal Chem. (2022) 22:1278–85. doi: 10.2174/1871520621666210727112212
136. Tsai JS, Wei SH, Chen CW, Yang SC, Tseng YL, Su PL, et al. Pembrolizumab and chemotherapy combination prolonged progression-free survival in patients with NSCLC with high PD-L1 expression and low neutrophil-to-lymphocyte ratio. Pharmaceuticals. (2022) 15. doi: 10.3390/ph15111407
137. Veccia A, Sforza V, Vattemi E, Inno A, Kinspergher S, Dipasquale M, et al. Pretreatment lung immune prognostic index as biomarker in advanced non-small-cell lung cancer patients receiving first line pembrolizumab. Immunotherapy. (2021) 30. doi: 10.2217/imt-2021-0002
138. Velcheti V, Chandwani S, Chen X, Pietanza MC, Piperdi B, and Burke T. Outcomes of first-line pembrolizumab monotherapy for PD-L1-positive (TPS >=50%) metastatic NSCLC at US oncology practices. Immunotherapy. (2019) 11:1541–54. doi: 10.2217/imt-2019-0177
139. Velcheti V, Hu X, Piperdi B, and Burke T. Real-world outcomes of first-line pembrolizumab plus pemetrexed-carboplatin for metastatic nonsquamous NSCLC at US oncology practices. Sci Rep. (2021) 11:9222. doi: 10.1038/s41598-021-88453-8
140. Velcheti V, Hu X, Yang L, Pietanza MC, and Burke T. Long-term real-world outcomes of first-line pembrolizumab monotherapy for metastatic non-small cell lung cancer with >=50% Expression of programmed cell death-ligand 1. Front Oncol. (2022) 12. doi: 10.3389/fonc.2022.834761
141. Wang X, Niu X, An N, Sun Y, and Chen Z. Comparative efficacy and safety of immunotherapy alone and in combination with chemotherapy for advanced non-small cell lung cancer. Front Oncol. (2021) 11. doi: 10.3389/fonc.2021.611012
142. Waterhouse D, Lam J, Betts KA, Yin L, Gao S, Yuan Y, et al. Real-world outcomes of immunotherapy-based regimens in first-line advanced non-small cell lung cancer. Lung Cancer. (2021) 156:41–9. doi: 10.1016/j.lungcan.2021.04.007
143. Xu B, Cheng H, Li K, Lv Y, Zeng X, Liu T, et al. Carboplatin and nab-paclitaxel chemotherapy with or without atezolizumab as front-line management for treatment-naive metastatic nonsquamous non-small cell lung cancer with PD-L1 staining: a retrospective study. J Cancer Res Clin Oncol. (2022) 148:3029–38. doi: 10.1007/s00432-021-03873-3
144. Yoneda T, Sone T, Koba H, Shibata K, Suzuki J, Tani M, et al. Long-term survival of patients with non-small cell lung cancer treated with immune checkpoint inhibitor monotherapy in real-world settings. Clin Lung Cancer. (2022) 23:467–76. doi: 10.1016/j.cllc.2022.03.008
145. Yuasa I, Hamaji M, Ozasa H, Sakamori Y, Yoshida H, Yutaka Y, et al. Outcomes of immune checkpoint inhibitors for postoperative recurrence of non-small cell lung cancer. Gen Thorac Cardiovasc Surgery. (2023) 71:534–41. doi: 10.1007/s11748-023-01920-z
146. Zayas-Soriano M, Bonete-Sanchez M, Campillo-Lopez J, Marcos-Ribes B, Hernandez-Guio A, and Aznar-Saliente MT. Clinical efficacy and safety of anti PD-1/PD-L1 antibodies as monotherapy in patients with non-small-cell lung cancer. Farm. (2020) 45:22–7. doi: 10.7399/fh.11478
147. Zhang J, Wu D, Zhang Z, Long J, Tian G, Wang Y, et al. Pembrolizumab or bevacizumab plus chemotherapy as first-line treatment of advanced nonsquamous nonsmall cell lung cancer: A retrospective cohort study. Technol Cancer Res Treat 20. (2021) 20:15330338211039600. doi: 10.1177/15330338211039676
148. Di Noia V, D’Argento E, Pilotto S, Vita E, Ferrara MG, Damiano P, et al. Blood serum amyloid A as potential biomarker of pembrolizumab efficacy for patients affected by advanced non-small cell lung cancer overexpressing PD-L1: results of the exploratory “FoRECATT” study. Cancer Immunology Immunotherapy. (2021) 70:1583–92. doi: 10.1007/s00262-020-02788-1
149. Ivanovic M, Knez L, Herzog A, Kovacevic M, and Cufer T. Immunotherapy for metastatic non-small cell lung cancer: real-world data from an academic central and eastern european center. Oncologist. (2021) 26:e2143–50. doi: 10.1002/onco.13909
150. Tang M, Lee CK, Lewis CR, Boyer M, Brown B, Schaffer A, et al. Generalizability of immune checkpoint inhibitor trials to real-world patients with advanced non-small cell lung cancer. Lung Cancer. (2022) 166:40–8. doi: 10.1016/j.lungcan.2022.01.024
151. Buti S, Bersanelli M, Maines F, Facchini G, Gelsomino F, Zustovich F, et al. First-line PAzopanib in NOn-clear-cell renal cArcinoMA: the italian retrospective multicenter PANORAMA study. Clin Genitourinary Cancer. (2017) 15:e609–14. doi: 10.1016/j.clgc.2016.12.024
152. Cecere SC, Rossetti S, Cavaliere C, Della Pepa C, Di Napoli M, Crispo A, et al. Pazopanib in metastatic renal cancer: A “Real-world” Experience at national cancer institute “Fondazione G. Pascale”. Front Pharmacol. (2016) 7:287. doi: 10.3389/fphar.2016.00287
153. Chrom P, Stec R, Semeniuk-Wojtas A, Bodnar L, Spencer NJ, and Szczylik C. Fuhrman grade and neutrophil-to-lymphocyte ratio influence on survival in patients with metastatic renal cell carcinoma treated with first-line tyrosine kinase inhibitors. Clin Genitourinary Cancer. (2016) 14:457–64. doi: 10.1016/j.clgc.2016.02.005
154. Coelho RC, Reinert T, Campos F, Peixoto FA, de Andrade CA, Castro T, et al. Sunitinib treatment in patients with advanced renal cell cancer: the Brazilian National Cancer Institute (INCA) experience. Int Braz J urol: Off J Braz Soc Urol. (2016) 42:694–703. doi: 10.1590/S1677-5538.IBJU.2015.0226
155. Ezz El Din M. Utilization of sunitinib for renal cell cancer: an Egyptian university hospital experience. Asian Pac. J Cancer Prev. (2016) 17:3161–6.
156. Edesa WA and Abdelmalek RR. Efficacy and toxicity of sunitinib in metastatic renal cell carcinoma patients in Egypt. Asian Pacific J Cancer Prev. (2015) 16:1971–6. doi: 10.7314/APJCP.2015.16.5.1971
157. El Din ME. Sunitinib 4/2 Versus 2/1 schedule for patients with metastatic renal cell carcinoma: tertiary care hospital experience. Clin Genitourinary Cancer. (2017) 15:e455–62. doi: 10.1016/j.clgc.2016.10.010
158. Kim MJ, Park SH, Lee J-L, Lee S-H, Lee SJ, Lim HY, et al. real-world, retrospective study of first-line pazopanib in unselected patients with metastatic renal clear-cell carcinoma. BMC Urol. (2016) 16:1–7. doi: 10.1186/s12894-016-0163-5
159. Kim MS, Chung HS, Hwang EC, Jung SI, Kwon DD, Hwang JE, et al. Efficacy of first-line targeted therapy in real-world Korean patients with metastatic renal cell carcinoma: focus on sunitinib and pazopanib. J Korean Med Sci. (2018) 33. doi: 10.3346/jkms.2018.33.e3
160. Köstek O, Yılmaz E, Hacıoğlu MB, Demircan NC, Gökyer A, Uzunoğlu S, et al. Changes in skeletal muscle area and lean body mass during pazopanib vs sunitinib therapy for metastatic renal cancer. Cancer chemotherapy Pharmacol. (2019) 83:735–42. doi: 10.1007/s00280-019-03779-5
161. Kucharz J, Dumnicka P, Giza A, Demkow U, Kusnierz–Cabala B, Demkow T, et al. Radiological response and neutrophil-to-lymphocyte ratio as predictive factors for progression-free and overall survival in metastatic renal cell carcinoma patients treated with sunitinib. Med Sci Res. (2019) 1153:31–45. doi: 10.1007/5584_2019_352
162. Liu C, Cao F, Xing W, Si T, Yu H, Yang X, et al. Efficacy of cryoablation combined with sorafenib for the treatment of advanced renal cell carcinoma. Int J Hyperthermia. (2019) 36:219–27. doi: 10.1080/02656736.2018.1556819
163. Maráz A, Cserháti A, Uhercsák G, Szilágyi É, Varga Z, Révész J, et al. Dose escalation can maximize therapeutic potential of sunitinib in patients with metastatic renal cell carcinoma. BMC Cancer. (2018) 18:1–12. doi: 10.1186/s12885-018-4209-9
164. Miyake H, Miyazaki A, Imai S, Harada K-i, and Fujisawa XXXM. Early tumor shrinkage under treatment with first-line tyrosine kinase inhibitors as a predictor of overall survival in patients with metastatic renal cell carcinoma: a retrospective multi-institutional study in Japan. Targeted Oncol. (2016) 11:175–82. doi: 10.1007/s11523-015-0385-6
165. Munárriz J, Reynés G, Sánchez-Lorenzo L, Esteban E, Basterretxea L, de Avila-Lizárraga L, et al. Sunitinib rechallenge in advanced renal cell carcinoma: outcomes of a multicenter retrospective study. Cancer Chemotherapy Pharmacol. (2019) 84:781–9. doi: 10.1007/s00280-019-03913-3
166. Patel K, Panchal H, Karanwal A, Parekh B, Shah S, and Prasad S. Sunitinib in metastatic renal cell carcinoma: Experience from single center study, efficacy and safety. Indian J Cancer. (2016) 53:118–22. doi: 10.4103/0019-509X.180844
167. Pérez-Valderrama B, Arija JA, Sánchez AR, Marín AP, García PB, Gaunas DC, et al. Validation of the International Metastatic Renal-Cell Carcinoma Database Consortium (IMDC) prognostic model for first-line pazopanib in metastatic renal carcinoma: the Spanish Oncologic Genitourinary Group (SOGUG) SPAZO study. Ann Oncol. (2016) 27:706–11. doi: 10.1093/annonc/mdv601
168. Poprach A, Fiala O, Chloupková R, Melichar B, Lakomy R, Petráková K, et al. Pazopanib for metastatic renal cell carcinoma: a registry-based analysis of 426 patients. Anticancer Res. (2018) 38:449–56. doi: 10.21873/anticanres.12243
169. Qiu J, Liu D, Yan Z, Jiang W, Zhang Q, Li N, et al. Therapeutic effect and adverse reaction of sorafenib in the treatment of advanced renal cancer. Oncol Lett. (2019) 17:1547–50.
170. Queiroz Muniz D, Ratto B, Yang H, Zhao J, Jenkins M, Signorovitch J, et al. Real-world effectiveness and tolerability of pazopanib as first targeted therapy in metastatic renal cell carcinoma: a retrospective chart review in Latin America. Adv Ther. (2019) 36:3446–57. doi: 10.1007/s12325-019-01109-y
171. Yamamoto K, Hara T, Nakagawa T, Hirai M, Miyake H, Fujisawa M, et al. Association of expression levels or activation status of STAT3 with treatment outcomes of sunitinib in patients with renal cell carcinoma. Targeted Oncol. (2018) 13:371–8. doi: 10.1007/s11523-018-0563-4
172. Boegemann M, Hubbe M, Thomaidou D, Blackburn S, Bent-Ennakhil N, Wood R, et al. Sunitinib treatment modification in first-line metastatic renal cell carcinoma: Analysis of the STAR-TOR Registry. Anticancer Res. (2018) 38:6413–22. doi: 10.21873/anticanres.13002
173. Joshi A, Ramaswamy A, Noronha V, Patil V, Chandrasekharan A, Goel A, et al. Efficacy and safety of sorafenib in advanced renal cell cancer and validation of Heng criteria. Indian J Cancer. (2016) 53:423–8. doi: 10.4103/0019-509X.200662
174. Joshi R and Rawal S. Targeted therapy for renal cell carcinoma: a prospective study. J Nepal Med Assoc. (2015) 53:83–8. doi: 10.31729/jnma.2767
175. Mir MH, Changal KH, Aziz SA, Bhat GM, and Lone AR. Sunitinib in metastatic renal cell carcinoma (mRCC): a developing country experience. Do our patients behave differently than Western patients? Int Urol Nephrol. (2016) 48:1811–6. doi: 10.1007/s11255-016-1380-2
176. Procopio G, Bamias A, Schmidinger M, Hawkins R, Sánchez AR, Estevez SV, et al. Real-world effectiveness and safety of pazopanib in patients with intermediate prognostic risk advanced renal cell carcinoma. Clin Genitourinary Cancer. (2019) 17:e526–33. doi: 10.1016/j.clgc.2019.01.018
177. Sabanathan D, Zhang A, Fox P, Coulter S, Gebski V, Balakrishnar B, et al. Dose individualization of sunitinib in metastatic renal cell cancer: toxicity-adjusted dose or therapeutic drug monitoring. Cancer Chemotherapy Pharmacol. (2017) 80:385–93. doi: 10.1007/s00280-017-3362-1
178. Saxena M, Madabhavi I, Patel A, Panchal H, and Anand A. Experience of sorafenib as first-line treatment in metastatic renal cell carcinoma in a tertiary care centre. Int J Hematology-Oncology Stem Cell Res. (2018) 12:197.
179. Harada KI, Sato R, Bando Y, Sano A, Matsushita Y, Tamura K, et al. Efficacy and safety of pembrolizumab and axitinib as first-line treatment for patients with advanced renal cell carcinoma: Real-world experience in Japan. Int J Urology. (2023) 30:772–7. doi: 10.1111/iju.15230
180. Iinuma K, Kameyama K, Kawada K, Fujimoto S, Takagi K, Nagai S, et al. Efficacy and safety of nivolumab and ipilimumab for advanced or metastatic renal cell carcinoma: A multicenter retrospective cohort study. Curr Oncol. (2021) 28:1402–11. doi: 10.3390/curroncol28020133
181. Iinuma K, Yamada T, Kameyama K, Taniguchi T, Kawada K, Ishida T, et al. The efficacy and safety of immune checkpoint inhibitor and tyrosine kinase inhibitor combination therapy for advanced or metastatic renal cell carcinoma: A multicenter retrospective real-world cohort study. Cancers. (2023) 15. doi: 10.3390/cancers15030947
182. Izumi K, Inoue M, Washino S, Shirotake S, Kagawa M, Takeshita H, et al. Clinical outcomes of nivolumab plus ipilimumab in patients with metastatic non-clear cell renal cell carcinoma: Real-world data from a Japanese multicenter retrospective study. Int J Urology. (2022) 30:714–21. doi: 10.1111/iju.15128
183. Jo H, Hong J, Kim H, Kim HR, Kwon GY, Kang KA, et al. A retrospective study of first-line therapy involving immune checkpoint inhibitors in patients with poor risk metastatic renal cell carcinoma. Front Oncol. (2022) 12. doi: 10.3389/fonc.2022.874385
184. Kato R, Kojima T, Sazuka T, Yamamoto H, Fukuda S, Yamana K, et al. A multicentre retrospective study of nivolumab plus ipilimumab for untreated metastatic renal cell carcinoma. Anticancer Res. (2021) 41:6199–209. doi: 10.21873/anticanres.15439
185. Kato T, Fujita K, Minami T, Nagahara A, Hyashi Y, Nakata W, et al. Real-world efficacy and safety of nivolumab plus ipilimumab in untreated metastatic renal cell carcinoma, and the impact of previous nephrectomy on clinical outcome: Japanese multi-institutional retrospective study. Int J Clin Oncol. (2022) 27:1596–604. doi: 10.1007/s10147-022-02215-8
186. Kojima T, Kato R, Sazuka T, Yamamoto H, Fukuda S, Yamana K, et al. Real-world effectiveness of nivolumab plus ipilimumab and second-line therapy in Japanese untreated patients with metastatic renal cell carcinoma: 2-year analysis from a multicenter retrospective clinical study (J-cardinal study). Japanese J Clin Oncol. (2022) 52:1345–52. doi: 10.1093/jjco/hyac124
187. Shah NJ, Sura SD, Shinde R, Shi J, Singhal PK, Robert NJ, et al. Real-world treatment patterns and clinical outcomes for metastatic renal cell carcinoma in the current treatment era. Eur Urol Open Sci. (2023) 49:110–8. doi: 10.1016/j.euros.2022.12.015
188. Tomiyama N, Tasaki Y, Hamamoto S, Sugiyama Y, Naiki T, Etani T, et al. Hemoglobin and neutrophil levels stratified according to International Metastatic Renal Cell Carcinoma Database Consortium risk predict the effectiveness of ipilimumab plus nivolumab in patients with advanced metastatic renal cell carcinoma. Int J Urology. (2023) 30:754–61. doi: 10.1111/iju.15198
189. Ueda K, Ogasawara N, Ito N, Ohnishi S, Suekane H, Kurose H, et al. Prognostic value of absolute lymphocyte count in patients with advanced renal cell carcinoma treated with nivolumab plus ipilimumab. J Clin Med 12(6) (no pagination). (2023) 12:2417. doi: 10.3390/jcm12062417
190. Zakharia Y, Thomaidou D, Li B, Siu G, Levin R, Vlahiotis A, et al. Real-world therapy management and outcomes of first-line axitinib plus pembrolizumab in patients with advanced renal cell carcinoma in the United States. Front Oncol. (2022) 12. doi: 10.3389/fonc.2022.861189
191. Zarrabi KK, Handorf E, Miron B, Zibelman MR, Anari F, Ghatalia P, et al. Comparative effectiveness of front-line ipilimumab and nivolumab or axitinib and pembrolizumab in metastatic clear cell renal cell carcinoma. oncologist. (2023) 28:157–64. doi: 10.1093/oncolo/oyac195
192. Kim Y, Yang H, Lee WS, Cheon J, Sang YB, Kang B, et al. High levels of baseline serum IL-10 are associated with reduced clinical benefit from first-line immune checkpoint inhibitor therapy in advanced renal cell carcinoma. J Cancer. (2023) 14:935–42. doi: 10.7150/jca.81384
193. Rebuzzi SE, Signori A, Buti S, Banna GL, Murianni V, Damassi A, et al. Validation of the Meet-URO score in patients with metastatic renal cell carcinoma receiving first-line nivolumab and ipilimumab in the Italian Expanded Access Program. ESMO Open 7(6) (no pagination). (2022) 7:100634. doi: 10.1016/j.esmoop.2022.100634
194. Sang YB, Yang H, Lee WS, Lee SJ, Kim SG, Cheon J, et al. High serum levels of IL-6 predict poor responses in patients treated with pembrolizumab plus axitinib for advanced renal cell carcinoma. Cancers. (2022) 14. doi: 10.3390/cancers14235985
Keywords: anti-PD-1, anti-PD-L1, immune checkpoint inhibitors, non-small cell lung cancer, renal cell carcinoma, melanoma, overall survival, real-world evidence
Citation: Nayak D, Akers KG, Frederickson AM, Mbous YPV and Aguiar-Ibáñez R (2025) Systematic literature review of real-world evidence on overall survival in cancer patients before and after the approval of anti-PD-(L)1 therapy. Front. Oncol. 15:1615795. doi: 10.3389/fonc.2025.1615795
Received: 21 April 2025; Accepted: 24 June 2025;
Published: 04 August 2025.
Edited by:
Subhadip Das, TCG Lifesciences (India), IndiaReviewed by:
Irem Karaomerlioglu, Turkish Medicines and Medical Devices Agency (TMMDA), TürkiyeV. Shane Pankratz, University of New Mexico, United States
Copyright © 2025 Nayak, Akers, Frederickson, Mbous and Aguiar-Ibáñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Aguiar-Ibáñez, cmFxdWVsLmFndWlhci1pYmFuZXpAbWVyY2suY29t