 Antonio Juan Ribelles1*
Antonio Juan Ribelles1* Nuria Benavent2Daniel Sanchez Mateos3Celine Pitou4Yanhong Zhou4Molly C. Hardebeck4Holly Knoderer4Adela Cañete1
Nuria Benavent2Daniel Sanchez Mateos3Celine Pitou4Yanhong Zhou4Molly C. Hardebeck4Holly Knoderer4Adela Cañete1- 1Pediatric Oncology and Hematology Unit, University Hospital and Polytechnic La Fe, Valencia, Spain
- 2Pediatric Oncology and Hematology Unit, La Fe Health Research Institute, Valencia, Spain
- 3Pediatric Radiology Unit, University Hospital and Polytechnic La Fe, Valencia, Spain
- 4Eli Lilly and Company, Indianapolis, IN, United States
Background: Cyclin-dependent kinase (CDK) 4 and CDK6 play fundamental roles in cell cycle progression. The CDK4/6 inhibitor abemaciclib, in combination with temozolomide and irinotecan, was evaluated in pediatric and young adult patients with relapsed/refractory solid tumors in the phase 1b dose-escalation study, JPCS Part A (NCT04238819). This case report describes the notable results of a patient with relapsed alveolar rhabdomyosarcoma (ARMS) who experienced a prolonged complete response.
Case presentation: An 8-year-old White male was initially diagnosed with stage IV ARMS with PAX3-FOXO1 fusion. Molecular characterization following a fourth relapse revealed CDK4, ERBB3, GLI1, MYCN, and FGFR4 amplifications and MYCN mutation. After five relapses, the patient enrolled in JPCS Part A and received abemaciclib (55 mg/m2 twice daily continuously) in combination with temozolomide (100 mg/m2 daily) and irinotecan (50 mg/m2 daily) on days 1 to 5 of 21-day cycles. The patient received 12 cycles of the triplet combination, followed by 23 additional cycles of abemaciclib monotherapy. Complete response (CR) was achieved in less than 3 months, with a duration of response (DOR) of 22.6 months and progression-free survival (PFS) of 23.7 months. The study treatment was well tolerated.
Conclusion: CDK4/6 inhibition with abemaciclib in combination with temozolomide and irinotecan provided a durable response in a patient with heavily pretreated ARMS. Additional studies may be warranted to further understand the role of CDK4/6 inhibitors for treatment of ARMS.
1 Introduction
Rhabdomyosarcoma (RMS) is a malignant tumor of skeletal myoblast-like cells and is the most common pediatric soft-tissue sarcoma, with an incidence of approximately 4.5 cases per million children/adolescents per year (1, 2). Although 5-year overall survival exceeds 70%, approximately one-third of patients experience progression/relapse within 13 months of diagnosis, and 5-year post-relapse survival remains approximately 24% (3, 4). Treatment for relapsed disease typically consists of multi-agent chemotherapy combinations with or without surgery and radiotherapy and often results in minimal benefit, indicating an urgent need for novel therapeutics, especially for patients with multiple relapses (3).
Two major RMS subtypes exist—PAX3/7-FOXO1 fusion-negative, also known as embryonal RMS, and PAX3/7-FOXO1 fusion-positive, also known as alveolar RMS (ARMS), each with a unique array of molecular alterations (5). The PAX3/7-FOXO1 fusion-negative subtype commonly exhibits loss of heterozygosity at the 11p15 locus, which contains the IGF-II gene and often has FGFR1 and NRAS mutations (6). In contrast, the PAX3/7-FOXO1 fusion-positive subtype, the most aggressive RMS subtype, is characterized by a translocation between the PAX3/7 and FOXO1 genes and amplification of MYCN and cyclin-dependent kinase (CDK) 4 (7, 8). Moreover, CDK4 is amplified in approximately 25% of PAX3-FOXO1 cases and approximately 4% of PAX7-FOXO1 cases (9). Other aberrations in the CDK4/6 pathway have been reported, including the homozygous deletion of CDKN2A/B and amplification of CCND2 and CCND3 (10–12). CDK4/6 pathway alterations may render fusion-positive cells vulnerable to targeted treatment with a CDK4/6 inhibitor.
Abemaciclib is an oral, potent, and selective CDK4/6 inhibitor approved for certain types of early stage and metastatic breast cancers (13–15). Abemaciclib is a unique CDK4/6 inhibitor due to its continuous dosing schedule, greater relative potency to CDK4 than CDK6, and its ability to penetrate the central nervous system (16–19). Abemaciclib blocks CDK4/6 from phosphorylating the retinoblastoma tumor suppressor, which results in G1 arrest and inhibition of cancer cell growth (16). The phase 1b study, I3Y-MC-JPCS (JPCS), evaluated abemaciclib in combination with temozolomide and irinotecan in pediatric and young adult patients with relapsed/refractory solid tumors. This case report examines the notable results of an adolescent patient enrolled in the JPCS study with relapsed ARMS who achieved a durable complete response.
2 Case presentation
An 8-year-old White male was diagnosed with stage IV PAX3-FOXO1 fusion-positive ARMS of the right foot and multiple lymph nodes with confirmed disease (Figure 1). Tumor biomarker analysis following the fourth relapse revealed a MYCN mutation (c.131C>T resulting in p.Pro44Leu amino acid alteration) and amplification of CDK4, MYCN, ERBB3, GLI1, and FGFR4. No RB1 alterations were detected. The patient had received five treatment regimens over approximately 7 years (Table 1). During this time, the patient underwent multiple surgeries and four courses of radiotherapy targeting lesions in the lower extremity, mesenteric nodes, muscle, and abdominal-pelvic regions.
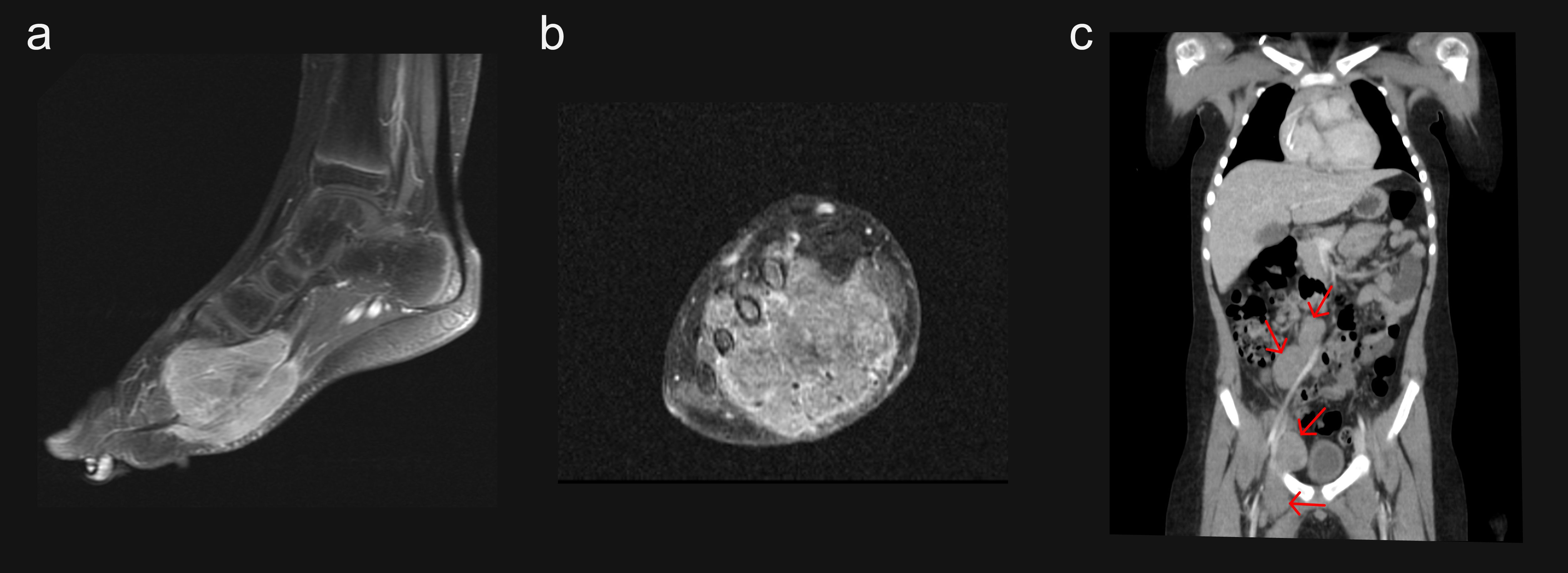
Figure 1. Primary tumors at initial diagnosis. (a) MRI sagittal plane of the right foot; (b) MRI coronal plane of the right foot; (c) Abdominal CT coronal plane showing inguinal and retroperitoneal malignant lymph nodes. CT, computed tomography; MRI, magnetic resonance imaging.
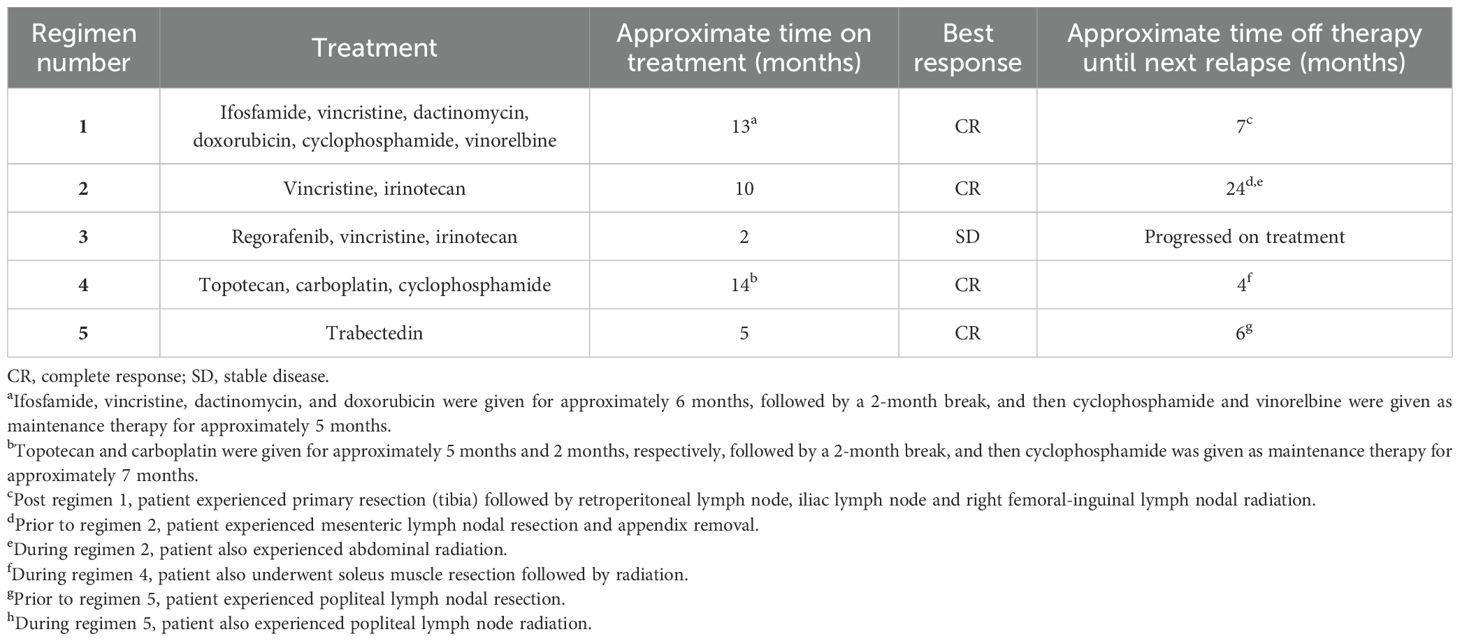
Table 1. Prior therapies and outcomes.
After the fifth relapse, the patient enrolled in JPCS, a phase 1b trial with a 3 + 3 dose-escalation design, for pediatric and young adult patients with relapsed/refractory solid tumors. The patient was assigned to abemaciclib (55 mg/m2 twice daily [BID continuously]) in combination with both temozolomide (100 mg/m2 daily) and irinotecan (50 mg/m2 daily) on days 1 to 5 of 21-day cycles. No preexisting conditions were reported. The disease sites at study entry included five target tumors (located in the supraclavicular lymph node, mediastinal lymph node ×2, and iliac lymph node ×2) and four non-target tumors (located in the supraclavicular lymph node, mediastinal lymph node, iliac lymph node, and retroperitoneum; Figures 2a–c). The patient received 35 cycles of abemaciclib, the first 12 in combination with temozolomide and irinotecan (discontinuation of chemotherapy was permitted after cycle 12 per protocol). Treatment compliance ranged from 98% to 100% for all three study drugs.
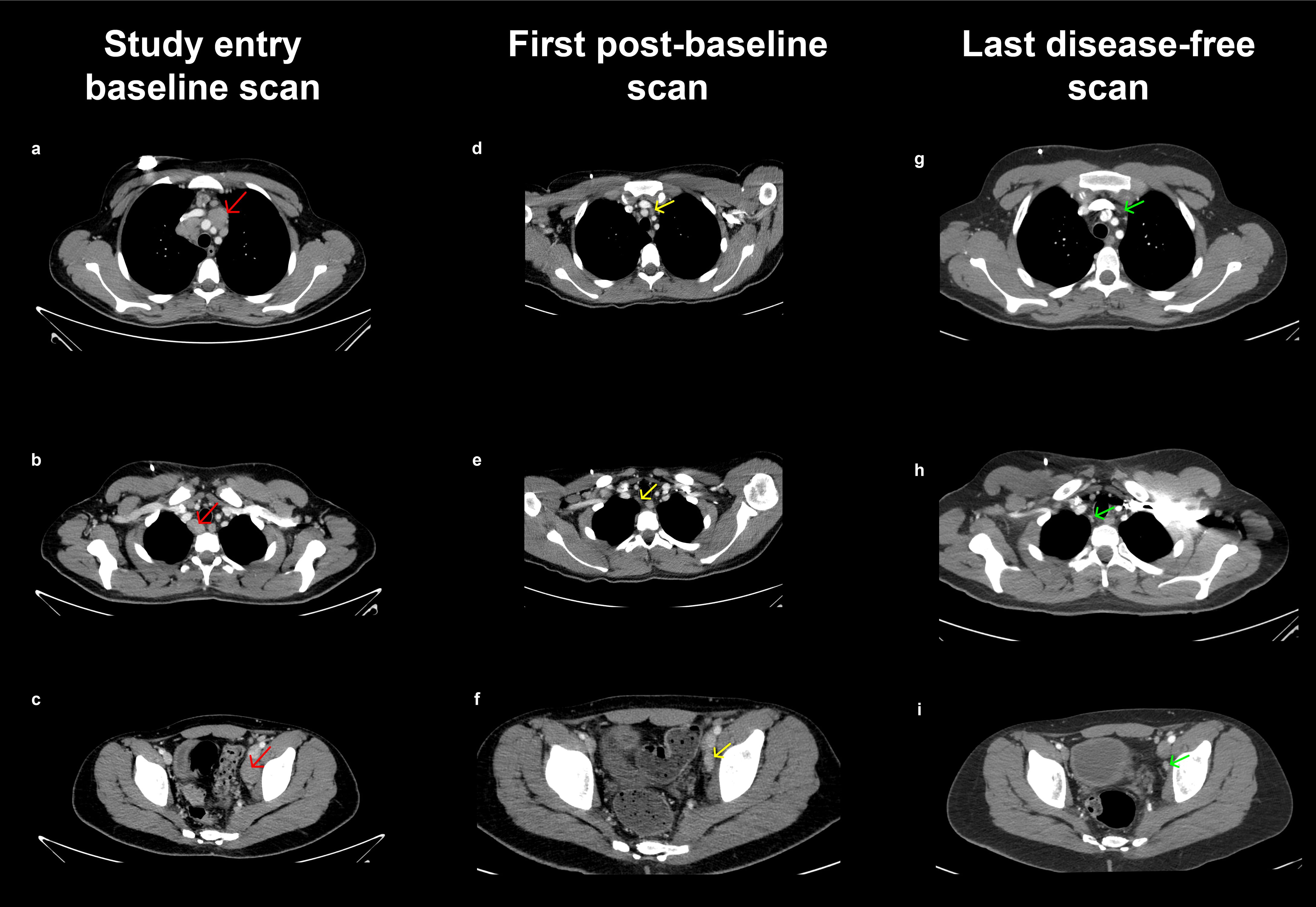
Figure 2. Tumors at JPCS study entry, first post-baseline scan, and last disease-free scan. (a–c) CT scan of the chest, abdomen, and pelvis with intravenous contrast at baseline. Multiple tumor lymphadenopathies were identified: bilateral supraclavicular, mediastinal, and an adenopathic conglomerate in the left iliac axis. (d–f) First post-baseline CT scan of the chest, abdomen, and pelvis with intravenous contrast. A significant reduction in the size and number of bilateral supraclavicular, mediastinal, retroperitoneal, and left iliac axis adenopathy is observed compared to the previous scan. (g–i) Last disease-free CT scan of the chest, abdomen, and pelvis with intravenous contrast showing complete resolution of tumor lymphadenopathy initially identified as target lesions. CT, computed tomography.
Computed tomography scans were obtained after cycle 2, cycle 4, and every third cycle thereafter. Partial response was achieved at the first scan (Figures 2d–f), followed by complete response at day 78. The last disease-free scan is shown in Figures 2g–i. The patient had ongoing benefit for 22.6 months until disease progression when five new tumors (left hilar adenopathy, lumbar and sacral spine, L5 vertebra, D8 vertebra, and femurs) were identified (Figure 3). Progression-free survival was 23.7 months.
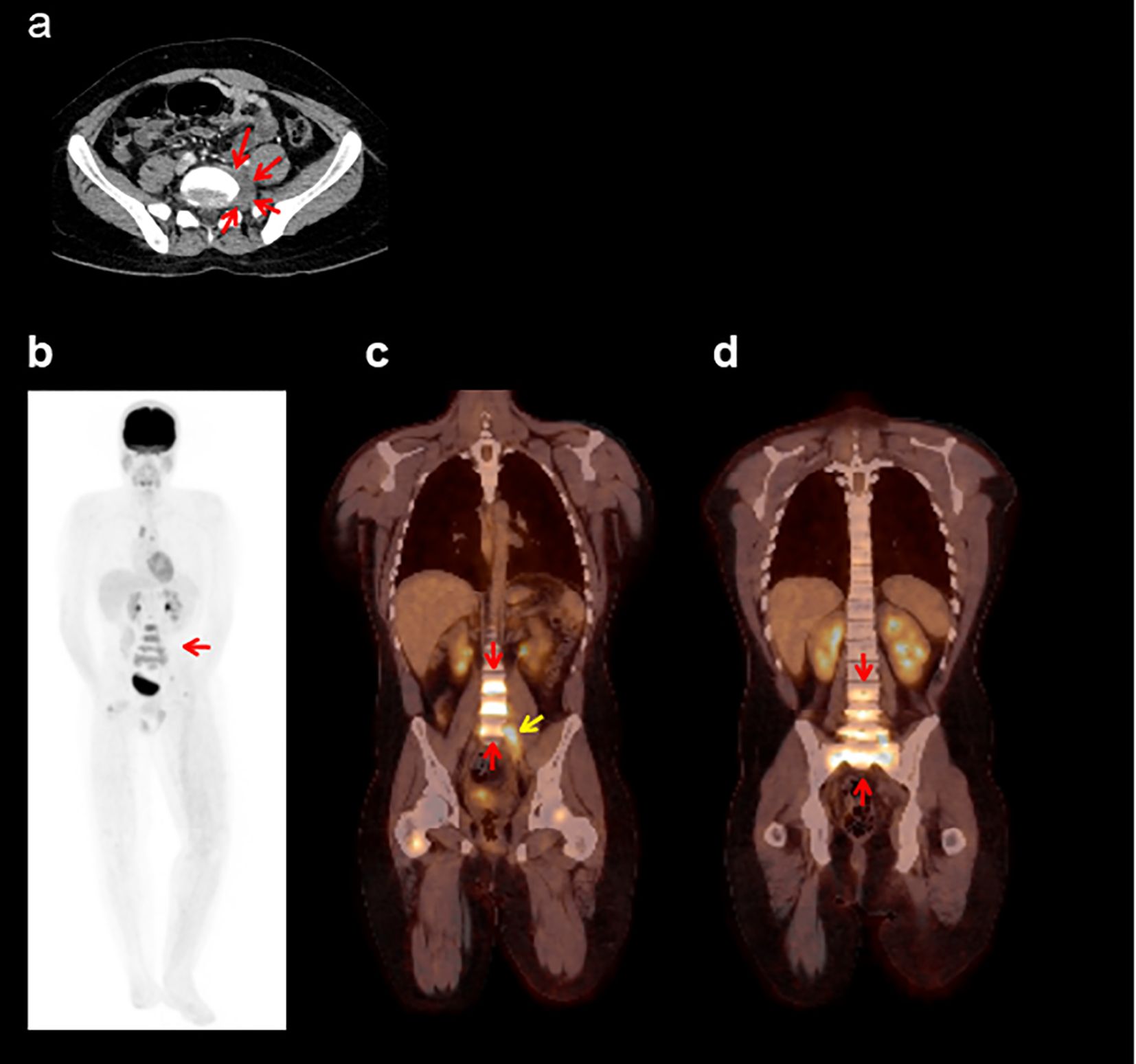
Figure 3. Tumor at progressive disease. (a) CT scan indicating progressive disease in the left paravertebral soft tissue mass (red arrows). (b–d) Images correspond to the PET-CT study at progressive disease—MIP image (b) and coronal fusion images (c, d)—which show a diffuse increase in metabolism in the lumbosacral vertebrae, encompassing the entirety of the vertebral bodies (red arrows), as well as hypermetabolism associated with the soft tissue mass in the left paravertebral region at L5 (yellow arrow). CT, computed tomography; MIP, maximum intensity projection; PET, positron emission tomography.
The patient tolerated study treatment well and experienced no dose-limiting toxicities or serious adverse events. The most frequent treatment-related adverse events were thrombocytopenia, diarrhea, dizziness, nausea, vomiting (all with a maximum severity of grade 1), and neutropenia (maximum severity of grade 3). Abemaciclib was withheld for 3 days due to an adverse event of grade 3 aspartate aminotransferase increase that was deemed unrelated to treatment, and there were no dose reductions. There were no dose modifications of temozolomide or irinotecan.
Pharmacokinetics assessments demonstrated that abemaciclib exposure and that of its M2 and M20 metabolites as well as temozolomide, irinotecan, and its metabolite SN-38 were consistent with that in other patients who received the same dose (data on file (20);).
3 Discussion
ARMS is a recalcitrant disease with rapid spreading, dismal therapeutic response, and high relapse rates (21). Given the poor prognosis, new targeted therapeutic approaches are needed. This case report highlights the notable results in a patient with relapsed ARMS who was treated with temozolomide and irinotecan in combination with the CDK4/6 inhibitor, abemaciclib.
Deregulation of the CDK4/6 pathway has been reported in ARMS, although its contribution to oncogenesis and disease progression is not fully understood (21). The primary CDK4/6 pathway alteration in ARMS is CDK4 amplification, which is present in about 25% of PAX3–FOXO1-positive tumors and approximately 4% of PAX7–FOXO1-positive tumors (9). The mechanism of CDK4 amplification and overexpression is likely via amplification of the 12q13-q14 amplicon (21, 22). Based on the frequent CDK4 alterations, abemaciclib may serve as a rational therapeutic approach to counteract the resulting cell cycle abnormalities and inhibit ARMS progression.
The case presented herein demonstrates a prolonged response to treatment with abemaciclib and standard chemotherapy in a patient with fifth relapse, stage IV, CDK4-amplified, PAX3-FOXO1 fusion-positive ARMS. The patient discontinued chemotherapy after 12 cycles and continued abemaciclib monotherapy for 23 additional cycles, which suggests that abemaciclib significantly contributed to the sustained complete response.
In addition to CDK4 amplification, this patient’s tumor also harbored FGFR4 amplification, which has been associated with aggressive RMS behavior and therapeutic resistance (23). While the contribution of FGFR4 to the observed response is unclear, its presence highlights the complexity of molecular alterations in ARMS and the potential need to consider co-alterations in future studies (24).
Recent studies in other CDK4-amplified sarcomas, such as dedifferentiated liposarcoma and synovial sarcoma, have demonstrated synergistic antitumor effects and prognostic significance of CDK4/6 inhibition (25, 26). These findings further support the broader relevance of investigating CDK4/6 across soft tissue sarcomas and further support exploration of this therapeutic strategy in ARMS.
The findings in this case contrast with the results of studies of other CDK4/6 inhibitors as monotherapy or in combination, which were less promising in a limited number of patients with ARMS-containing alterations in the CDK4/6 pathway (27, 28). Likewise, two other patients with RMS (unknown subtype) in the JPCS Part A study did not achieve durable responses. Thus, the molecular mechanisms rendering sensitivity in some cases and resistance in other cases remain elusive.
Preclinical studies have postulated mechanisms to explain CDK4/6 inhibitor response. A study evaluating fusion-positive RMS suggested that CDK4/6 inhibitor sensitivity depends on the level of CDK4 amplification; specifically, all fusion-positive models evaluated exhibited sensitivity, but models with lower CDK4 amplification (though higher than no amplification) were more sensitive than those with higher CDK4 levels (9). The researchers hypothesized that cyclin D1 expression may saturate CDK4 and limit the effects of CDK4 overexpression (9). Furthermore, preclinical evidence has linked Rb1 loss to ARMS progression and demonstrated that downregulation of pRb expression leads to CDK4/6 inhibitor resistance (29). Thus, effective CDK4/6 inhibition likely hinges not only on appropriate CDK4 levels but also on enduring Rb functionality.
This case report is inherently limited by its single-patient nature which restricts the generalizability of the findings. While the prolonged complete response is notable, broader conclusions regarding the efficacy of CDK4/6 inhibition in ARMS require validation through larger controlled studies.
The evidence presented in this case report strengthens the argument that CDK4/6 may play an important role in the pathogenesis of CDK4-amplified ARMS and that abemaciclib in combination with temozolomide and irinotecan may abrogate tumor growth and improve outcomes. However, this evaluation is limited to a single patient, and we do not yet fully understand the biological or molecular basis for this patient’s exceptional initial response or the factors that led to eventual disease progression. It should be noted that this patient had achieved complete responses when treated with prior regimens and thus may have a unique molecular profile yielding favorable outcomes. Nonetheless, a nearly 2-year treatment response for fifth relapse ARMS is remarkable. These results provide the first insights into the clinical activity of abemaciclib, temozolomide, and irinotecan in CDK4-amplified ARMS, and additional studies may be warranted to further understand the role of CDK4/6 alterations in ARMS. Further research could explore biomarker-guided trials to identify benefit of CDK4/6 inhibition and evaluate this combination in prospective studies across molecularly defined RMS subtypes. Such studies could clarify the mechanisms of response and resistance and inform patient selection strategies.
4 Conclusion
Novel treatments that exploit targetable alterations are needed to improve outcomes for relapsed ARMS. This case report describes an adolescent male with fifth relapse, CDK4-amplified, PAX3-FOXO1 fusion-positive ARMS who had a remarkable response to treatment with the CDK4/6 inhibitor abemaciclib in combination with temozolomide and irinotecan. These results underscore the importance of exploring CDK4/6 inhibition as a potential treatment strategy for ARMS.
Data availability statement
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the United States and European Union and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, clinical study report, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org.
Ethics statement
The studies involving humans were approved by the ethical review board at each site. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
AJ: Data curation, Investigation, Writing – review & editing. NB: Data curation, Investigation, Writing – review & editing. DS: Data curation, Writing – review & editing, Investigation. CP: Writing – original draft, Writing – review & editing, Formal Analysis, Visualization, Data curation. YZ: Writing – original draft, Formal Analysis, Writing – review & editing, Data curation, Visualization, Conceptualization. MH: Visualization, Conceptualization, Project administration, Writing – original draft, Formal Analysis, Writing – review & editing, Data curation. HK: Writing – original draft, Formal Analysis, Visualization, Data curation, Writing – review & editing. AC: Writing – review & editing, Data curation, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This trial was funded by Eli Lilly and Company.
Acknowledgments
We would like to express our deep gratitude to the trial participant and family/caregivers for their kind collaboration, without whom this work would not be possible. Maeve O’Connell, PhD, and Joana Cruz Pereira, PhD, of Eli Lilly and Company provided medical writing support for this manuscript.
Conflict of interest
AJ: consulting/advisory role for Alexion and Bayer; participation in educational activities organized by Eusa Pharma, Abbott, and Alexion, and travel expense support by Nestle and Alexion. CP, YZ, MH, HK: Employment and stock ownership at Eli Lilly and Company. AC: Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events for SERB.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Mascarenhas L, Lyden ER, Breitfeld PP, Walterhouse DO, Donaldson SS, Rodeberg DA, et al. Risk-based treatment for patients with first relapse or progression of rhabdomyosarcoma: A report from the Children’s Oncology Group. Cancer. (2019) 125:2602–9. doi: 10.1002/cncr.32122
2. Skapek SX, Ferrari A, Gupta AA, Lupo PJ, Butler E, Shipley J, et al. Rhabdomyosarcoma. Nat Rev Dis Primers. (2019) 5:1. doi: 10.1038/s41572-018-0051-2
3. Chen C, Dorado Garcia H, Scheer M, and Henssen AG. Current and future treatment strategies for rhabdomyosarcoma. Front Oncol. (2019) 9:1458. doi: 10.3389/fonc.2019.01458
4. Dantonello TM, Int-Veen C, Winkler P, Leuschner I, Schuck A, Schmidt BF, et al. Initial patient characteristics can predict pattern and risk of relapse in localized rhabdomyosarcoma. J Clin Oncol. (2008) 26:406–13. doi: 10.1200/jco.2007.12.2382
5. Agaram NP. Evolving classification of rhabdomyosarcoma. Histopathology. (2022) 80:98–108. doi: 10.1111/his.14449
6. Dasgupta R, Fuchs J, and Rodeberg D. Rhabdomyosarcoma. Semin Pediatr Surg. (2016) 25:276–83. doi: 10.1053/j.sempedsurg.2016.09.011
7. Stewart E, McEvoy J, Wang H, Chen X, Honnell V, Ocarz M, et al. Identification of therapeutic targets in rhabdomyosarcoma through integrated genomic, epigenomic, and proteomic analyses. Cancer Cell. (2018) 34:411–26.e19. doi: 10.1016/j.ccell.2018.07.012
8. Zobeck M, Khan J, Venkatramani R, Okcu MF, Scheurer ME, and Lupo PJ. Improving individualized rhabdomyosarcoma prognosis predictions using somatic molecular biomarkers. JCO Precis Oncol. (2025) 9):e2400556. doi: 10.1200/po-24-00556
9. Olanich ME, Sun W, Hewitt SM, Abdullaev Z, Pack SD, and Barr FG. CDK4 amplification reduces sensitivity to CDK4/6 inhibition in fusion-positive rhabdomyosarcoma. Clin Cancer Res. (2015) 21:4947–59. doi: 10.1158/1078-0432.Ccr-14-2955
10. Iolascon A, Faienza MF, Coppola B, Rosolen A, Basso G, Della Ragione F, et al. Analysis of cyclin-dependent kinase inhibitor genes (CDKN2A, CDKN2B, and CDKN2C) in childhood rhabdomyosarcoma. Genes Chromosomes Cancer. (1996) 15:217–22. doi: 10.1002/(sici)1098-2264(199604)15:4<217::Aid-gcc3>3.0.Co;2-4
11. Shern JF, Chen L, Chmielecki J, Wei JS, Patidar R, Rosenberg M, et al. Comprehensive genomic analysis of rhabdomyosarcoma reveals a landscape of alterations affecting a common genetic axis in fusion-positive and fusion-negative tumors. Cancer Discov. (2014) 4:216–31. doi: 10.1158/2159-8290.Cd-13-0639
12. Wong M, Mayoh C, Lau LMS, Khuong-Quang D-A, Pinese M, Kumar A, et al. Whole genome, transcriptome and methylome profiling enhances actionable target discovery in high-risk pediatric cancer. Nat Med. (2020) 26:1742–53. doi: 10.1038/s41591-020-1072-4
13. Goetz MP, Toi M, Campone M, Sohn J, Paluch-Shimon S, Huober J, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol. (2017) 35:3638–46. doi: 10.1200/jco.2017.75.6155
14. Sledge GW, Toi M, Neven P, Sohn J, Inoue K, Pivot X, et al. MONARCH 2: abemaciclib in combination with fulvestrant in women with HR+/HER2– advanced breast cancer who had progressed while receiving endocrine therapy. J Clin Oncol. (2017) 35:2875–84. doi: 10.1200/jco.2017.73.7585
15. Johnston SRD, Toi M, O’Shaughnessy J, Rastogi P, Campone M, Neven P, et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. (2023) 24:77–90. doi: 10.1016/S1470-2045(22)00694-5
16. Torres-Guzmán R, Calsina B, Hermoso A, Baquero C, Alvarez B, Amat J, et al. Preclinical characterization of abemaciclib in hormone receptor positive breast cancer. Oncotarget. (2017) 8:69493–507. doi: 10.18632/oncotarget.17778
17. Patnaik A, Rosen LS, Tolaney SM, Tolcher AW, Goldman JW, Gandhi L, et al. Efficacy and safety of abemaciclib, an inhibitor of CDK4 and CDK6, for patients with breast cancer, non-small cell lung cancer, and other solid tumors. Cancer Discov. (2016) 6:740–53. doi: 10.1158/2159-8290.Cd-16-0095
18. Raub TJ, Wishart GN, Kulanthaivel P, Staton BA, Ajamie RT, Sawada GA, et al. Brain exposure of two selective dual CDK4 and CDK6 inhibitors and the antitumor activity of CDK4 and CDK6 inhibition in combination with temozolomide in an intracranial glioblastoma xenograft. Drug Metab Dispos. (2015) 43:1360–71. doi: 10.1124/dmd.114.062745
19. Tolaney SM, Sahebjam S, Le Rhun E, Bachelot T, Kabos P, Awada A, et al. A phase II study of abemaciclib in patients with brain metastases secondary to hormone receptor-positive breast cancer. Clin Cancer Res. (2020) 26:5310–9. doi: 10.1158/1078-0432.Ccr-20-1764
20. Lassaletta Á, Moreno L, Ogawa C, Ruggiero A, Hoffman LM, Pitou C, et al. Recommended phase 2 dose (RP2D) for abemaciclib in combination with irinotecan (IRN) and temozolomide (TMZ) in pediatric patients with relapsed/refractory solid tumors (JPCS Part A). J Clin Oncol. (2023) 41:10039–9. doi: 10.1200/JCO.2023.41.16_suppl.10039
21. Barr FG, Duan F, Smith LM, Gustafson D, Pitts M, Hammond S, et al. Genomic and clinical analyses of 2p24 and 12q13-q14 amplification in alveolar rhabdomyosarcoma: a report from the Children’s Oncology Group. Genes Chromosomes Cancer. (2009) 48:661–72. doi: 10.1002/gcc.20673
22. Park S, Lee J, Do IG, Jang J, Rho K, Ahn S, et al. Aberrant CDK4 amplification in refractory rhabdomyosarcoma as identified by genomic profiling. Sci Rep. (2014) 4:3623. doi: 10.1038/srep03623
23. Li SQ, Cheuk AT, Shern JF, Song YK, Hurd L, Liao H, et al. Targeting wild-type and mutationally activated FGFR4 in rhabdomyosarcoma with the inhibitor ponatinib (AP24534). PloS One. (2013) 8:e76551. doi: 10.1371/journal.pone.0076551
24. De Vita A, Ferrari A, Miserocchi G, Vanni S, Domizio C, Fonzi E, et al. Identification of a novel RAB3IP-HMGA2 fusion transcript in an adult head and neck rhabdomyosarcoma. Oral Diseases. (2022) 28:2052–4. doi: 10.1111/odi.14036
25. Li X, Seebacher NA, Garbutt C, Ma H, Gao P, Xiao T, et al. Inhibition of cyclin-dependent kinase 4 as a potential therapeutic strategy for treatment of synovial sarcoma. Cell Death Dis. (2018) 9:446. doi: 10.1038/s41419-018-0474-4
26. Vanni S, Miserocchi G, Gallo G, Fausti V, Gabellone S, Liverani C, et al. Role of CDK4 as prognostic biomarker in Soft Tissue Sarcoma and synergistic effect of its inhibition in dedifferentiated liposarcoma sequential treatment. Exp Hematol Oncol. (2024) 13:74. doi: 10.1186/s40164-024-00540-4
27. Barghi F, Shannon HE, Saadatzadeh MR, Bailey BJ, Riyahi N, Bijangi-Vishehsaraei K, et al. Precision medicine highlights dysregulation of the CDK4/6 cell cycle regulatory pathway in pediatric, adolescents and young adult sarcomas. Cancers (Basel). (2022) 14. doi: 10.3390/cancers14153611
28. Bautista F, Paoletti X, Rubino J, Brard C, Rezai K, Nebchi S, et al. Phase I or II study of ribociclib in combination with topotecan-temozolomide or everolimus in children with advanced Malignancies: arms A and B of the acSé-ESMART trial. J Clin Oncol. (2021) 39:3546–60. doi: 10.1200/jco.21.01152
Keywords: abemaciclib, CDK4/6 inhibitor, rhabdomyosarcoma, JPCS, pediatric, case report
Citation: Juan Ribelles A, Benavent N, Sanchez Mateos D, Pitou C, Zhou Y, Hardebeck MC, Knoderer H and Cañete A (2025) Case Report: Relapsed alveolar rhabdomyosarcoma treated with abemaciclib, temozolomide, and irinotecan in the JPCS study. Front. Oncol. 15:1637177. doi: 10.3389/fonc.2025.1637177
Received: 28 May 2025; Accepted: 31 July 2025;
Published: 27 August 2025.
Edited by:
Jaume Mora, Sant Joan de Déu Hospital, SpainReviewed by:
Moira Garraus Oneca, Sant Joan de Déu Hospital, SpainAlessandro De Vita, Scientific Institute of Romagna for the Study and Treatment of Tumors (IRCCS), Italy
Copyright © 2025 Juan Ribelles, Benavent, Sanchez Mateos, Pitou, Zhou, Hardebeck, Knoderer and Cañete. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Juan Ribelles, anVhbl9hbnRyaWJAZ3ZhLmVz