 Giulia Scotto1*
Giulia Scotto1* Anna Galatà2
Anna Galatà2 Robert Fruscio3,4Giulia Besana4Fabio Landoni3,4Luca Sgro5Alessandra Testi5
Robert Fruscio3,4Giulia Besana4Fabio Landoni3,4Luca Sgro5Alessandra Testi5 Fulvio Borella6
Fulvio Borella6 Gennaro Cormio7,8Mariangela Gianciotta7,8
Gennaro Cormio7,8Mariangela Gianciotta7,8 Francesca Arezzo7,9
Francesca Arezzo7,9 Brigida Anna Maiorano10Alessandra Baldoni11Marinella Destefanis12
Brigida Anna Maiorano10Alessandra Baldoni11Marinella Destefanis12 Jole Ventriglia13
Jole Ventriglia13 Sandro Pignata13Rita Chiari14Maria Carmen Azzolina15
Sandro Pignata13Rita Chiari14Maria Carmen Azzolina15 Ivano Raimondo16,17Margherita Turinetto2
Ivano Raimondo16,17Margherita Turinetto2 Valentina Tuninetti18
Valentina Tuninetti18 Massimo Di Maio19
Massimo Di Maio19 Giorgio Valabrega18
Giorgio Valabrega18- 1Medical Oncology, ASL TO3 Ospedale degli Infermi, Rivoli, Torino, Italy
- 2Department of Oncology, University of Turin, Turin, Italy
- 3UO Gynecology, Fondazione IRCCS San Gerardo, Monza, Italy
- 4Department of Medicine and Surgery, University of Milan-Bicocca, Milan, Italy
- 5Obstetrics and Gynaecology Unit, Umberto I Hospital, Department of Surgical Sciences, School of Medicine, University of Turin, Turin, Italy
- 6Gynecology and Obstetrics Unit 1, Department of Surgical Sciences, City of Health and Science University Hospital, University of Turin, Turin, Italy
- 7Gynecologic Oncology Unit, IRCCS Istituto Tumori “Giovanni Paolo II”, Bari, Italy
- 8Interdisciplinar Department of Medicine, University of Bari “Aldo Moro”, Bari, Italy
- 9Department of Precision and Regenerative Medicine - DiMePRe-J, University of Bari “Aldo Moro”, Bari, Italy
- 10Department of Medical Oncology, IRCCS San Raffaele Hospital, Milan, Italy
- 11Oncology and Hematology Department, Mirano AULSS3 Serenissima, Mirano, Italy
- 12Dipartimento Chirurgico ASO S. Croce e Carle Cuneo, Cuneo, Italy
- 13Department of Urology and Gynecology, Istituto Nazionale Tumori IRCCS - Fondazione G. Pascale, Naples, Italy
- 14UOC ONCOLOGIA AST Pesaro Urbino, Pesaro Urbino, Italy
- 15AO Ordine Mauriziano, Torino, Italy
- 16School in Biomedical Sciences, University of Sassari, Sassari, Italy
- 17Department of Gynecology, Mater Olbia Hospital, Olbia, Italy
- 18Department of Oncology, University of Turin, Medical Oncology, Ordine Mauriziano Hospital, Turin, Italy
- 19Department of Oncology, University of Turin, AOU Città della Salute e della Scienza di Torino, Turin, Italy
Introduction: The European Society for Medical Oncology (ESMO) 2021 Guidelines contraindicate the administration of chemotherapy in the last month of patients’ life. The main objective of this multicenter observational retrospective study was to calculate the time elapsed between the date of the last chemotherapy and the date of death of patients with ovarian cancer. The secondary objectives were to identify any factors associated with a greater probability of receiving chemotherapy in the end of life.
Methods: Ovarian cancer patients operated between 2010 and 2020 in the participant Italian centers were enrolled. Only deceased patients whose date of death and date of last chemotherapy were known were included.
Results: 603 women from 10 Italian centers were included. One patient out of four (25.7%) received chemotherapy in the last month of life. The median survival from the last chemotherapy was 66 days. Patients with a neutrophil/lymphocyte ratio ≥5, with high C-reactive protein at the start of the last line and patients dying in hospital compared to hospice/palliative care at home were more likely to undergo chemotherapy at the end of life (p<0.001, p=0.05 and p<0.001 respectively). Being treated in Northern Italy reduces the chance of receiving chemotherapy at the end of life in comparison with Center-South (p<0.001), as well as being enrolled in at least one clinical protocol (p=0.027).
Discussion: The TO CARE/MITO 42 study is a snapshot of the Italian practice in which there are still disparities in the treatment of patients at the end of life. A prospective observational study could provide useful elements for early identification of patients who would not benefit from a further line.
Introduction
Ovarian cancer is the eight cancer for incidence and at the fifth place for mortality in Europe in 2022 (1). The prognosis, although improved in recent years, remains poor, especially in advanced stages, and most of the patients diagnosed with Fédération Internationale de Gynécologie et d’Obstétrique (FIGO) stage III or IV tumors will develop recurrence within 18 months (2, 3). At the fifth recurrence, survival is around five months (4). The term ‘end of life’ is frequently used but poorly defined (5). The European Society for Medical Oncology (ESMO) Guideline refers to ‘end of life’, for people with advanced disease, as ‘point of rapid physical decline, typically the last few weeks or months before an inevitable death as a natural result of a disease’ (6). ESMO Guidelines explicitly contraindicate chemotherapy and immunotherapy in the last weeks of life (6). Chemotherapy in the last month of life is associated with adverse outcomes including poor quality of care, emergency department attendance, cardiopulmonary resuscitation, mechanical ventilation and dying in an intensive care unit. These items are defined as indicators of aggressive end of life care by several authors in the literature (7, 8).
Despite these indications, there are large retrospective registry-based American studies showing aggressive care in the final months of life in patients with ovarian cancer, including chemotherapy administration, emergency room access, hospital and intensive care unit admissions (9–14). Other retrospective and registry-based trials conducted in different countries around the world have shown a similar scenario of aggressive treatment at the end of life (15–17). In contrast, there is little data on the European reality on this topic. A large Dutch registry-based study has been published in recent years: of the 1775 patients included, only 12% received chemotherapy in the last month of life (18). The only data on the Italian scenario come from the EOLO study, a retrospective single-center Italian study, that included 110 patients dead of advanced/recurrent ovarian cancer and 38% of these had chemotherapy during the last month of life (19). The cut-off of chemotherapy administration at the end of life varies between studies (9–19). 30 days is the one most used regarding ovarian carcinoma (6, 9, 12, 16, 18–21).
Several parameters representing systemic inflammatory responses have been reported to be prognostic parameters in patients with ovarian cancer. Among these the neutrophil/lymphocyte ratio has been described as negative prognostic factor in ovarian cancer, as well as in other tumor types (22). Furthermore, in a study of patients with recurrent ovarian cancer, higher neutrophil/lymphocyte ratio was identified as prognostic factors for mortality within 100 days of failure of last line of chemotherapy (23).
The modified Glasgow Prognostic Score, which is classified as 0, 1, or 2 calculated by combining C-reactive protein and albumin values, has also been identified as an independent predictor of overall survival in patients with recurrent ovarian cancer (24). Also, C-reactive protein value has been described in literature as negative prognostic parameter in advanced cancer and in ovarian cancer (16, 25) The aim of this study is to describe the Italian reality about chemotherapy in the end of life in a cohort of ovarian cancer patients, and to identify factors associated with the probability of receiving chemotherapy in this period.
Materials and methods
Patient selection and data collection
TO CARE/MITO 42 is an Italian multicenter retrospective observational study. Data analysis was conducted by collecting the medical records of ovarian cancer patients treated at the oncology Day Hospitals (Oncology and Gynecologic Oncology) of the Multicenter Italian Trials in Ovarian cancer and gynecologic malignancies (MITO) Centers participating in Italy.
Patients who underwent surgery for ovarian carcinoma between January 2010 and December 2020 in participating MITO centers were selected. In addition, only deceased patients whose date of death was known and whose date of last chemotherapy treatment performed was known were included.
The following general data were then retrospectively recorded: patient characteristics, pathological data (histotype, grading), FIGO stage at diagnosis, first line treatment, subsequent treatment, BRCA status and inclusion or non-inclusion in clinical protocols. Regarding the focus of the study, clinical and laboratory data were collected before the start of the last line of chemotherapy, drugs used, end of life place, activation or not of home palliative care services at the start of the last therapy, date of administration of the last chemotherapy, date of death. Patients who had hormone therapy as the last line were described, but the date of last chemotherapy considered referred to the previous line.
After approval by the Ethics Committee of the Coordinating Center Hospital Umberto I, Mauriziano in Turin, the encrypted database and study protocol was sent to all Principal Investigators of the 160 MITO centers in Italy. Participating centers have obtained approval from local Ethics Committees.
Statistical analysis
Given the exploratory nature of this retrospective analysis, based on the collection of cases available at participating centers, the sample size is not based on a predefined hypothesis. It was estimated to collect about 600 patients before conducting the analysis. The sample estimate was made on a survey we sent to the MITO centers in which they provided us with indicative numbers of patients they would include. The data analysis was descriptive. Continuous variables were described by median, interquartile range and absolute range. Categorical variables were described by frequency and percentage. The main analysis was based on the dichotomous endpoint “chemotherapy in the last 30 days of life” (yes vs no). The proportion of patients who received chemotherapy in the last 30 days in the overall case series and subgroups, identified based on potential factors impacting this outcome (age, performance status, number of previous lines, end of life place), also selected on the basis of literature data, was described.
The association of individual factors was tested with contingency tables and chi-square tests. Multivariate logistic regression analysis was performed, including clinical variables statistically significant (p<0.05) at univariate analysis. Laboratory variables were not included in the multivariate model due to the high number of patients with data not available.
Post-cancer treatment survival was calculated as the time from the date of last chemotherapy administration to the date of death. Consistent with the study’s inclusion criteria, which limited the analysis to deceased patients, there were no censored patients.
The Kaplan-Meier method was used to calculate survival after the last chemotherapy treatment. Analyses with p value < 0.05 were considered significant. Due to exploratory nature of the study, no adjustments were made for the multiplicity of statistical tests.
Results
A total of 603 patients from 10 MITO centers participating (response rate 6%, 10/160 contacted centers) were analyzed (Table 1).
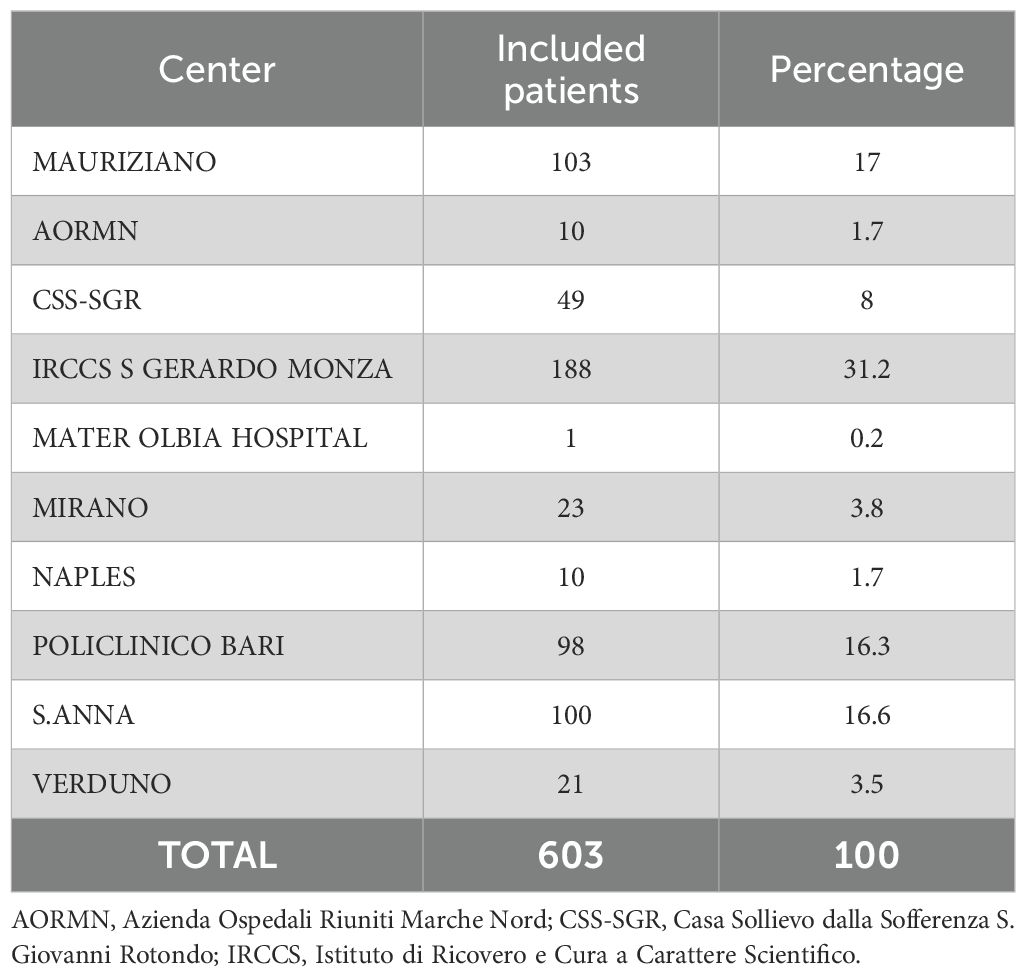
Table 1. Participating centers and included patients.
Descriptive analysis
The characteristics of patients are shown in Table 2. Median age at diagnosis was 64 years (range 27-89). Most patients had serous histotype ovarian cancer (76.1%) and high-grade tumor (78.9%). In addition, almost 90% of patients had advanced FIGO stage (64.3% had FIGO stage 3 and 25.5% had FIGO stage 4). Among 320 patients who were tested for BRCA1/2 status, 78 (24%) had a mutation; this information is missing in 283 patients. For 77 patients (12.8%) the last active treatment was weekly paclitaxel; for 76 patients (12.6%) pegylated liposomal doxorubicin; for 68 patients (11.3%) carboplatin-paclitaxel; 62 patients (10.3%) had gemcitabine as last line of chemotherapy; 51 patients (8.5%) had hormone therapy; 45 patients (7.5%) carboplatin monotherapy; 43 patients (7.1%) metronomic oral cyclophosphamide; 35 patients (5.8%) carboplatin-pegylated liposomal doxorubicin. Fewer patients (<5%) received carboplatin-gemcitabine, cisplatin, carboplatin-paclitaxel-bevacizumab, pegylated liposomal doxorubicin-trabectedin, topotecan, etoposide, gemcitabine-vinorelbine, carboplatin-gemcitabine-bevacizumab, vinorelbine, oxaliplatin, and epirubicin as last line, while 1% of patients have performed therapy within clinical trials. Median number of chemotherapy lines was 3 (range; 1-9). Namely, 344 patients (57%) received less than 3 lines of chemotherapy while 259 patients (43%) received more than 3 lines. Chemotherapy in the last 30 days of life was administered to 155 patients (25.7%). Median overall survival from the last chemotherapy administration was 66 days (Confidence Interval (CI) 95%, 59-73). The Kaplan-Meier survival curve from the day of last chemotherapy administration to death is shown in Figure 1.
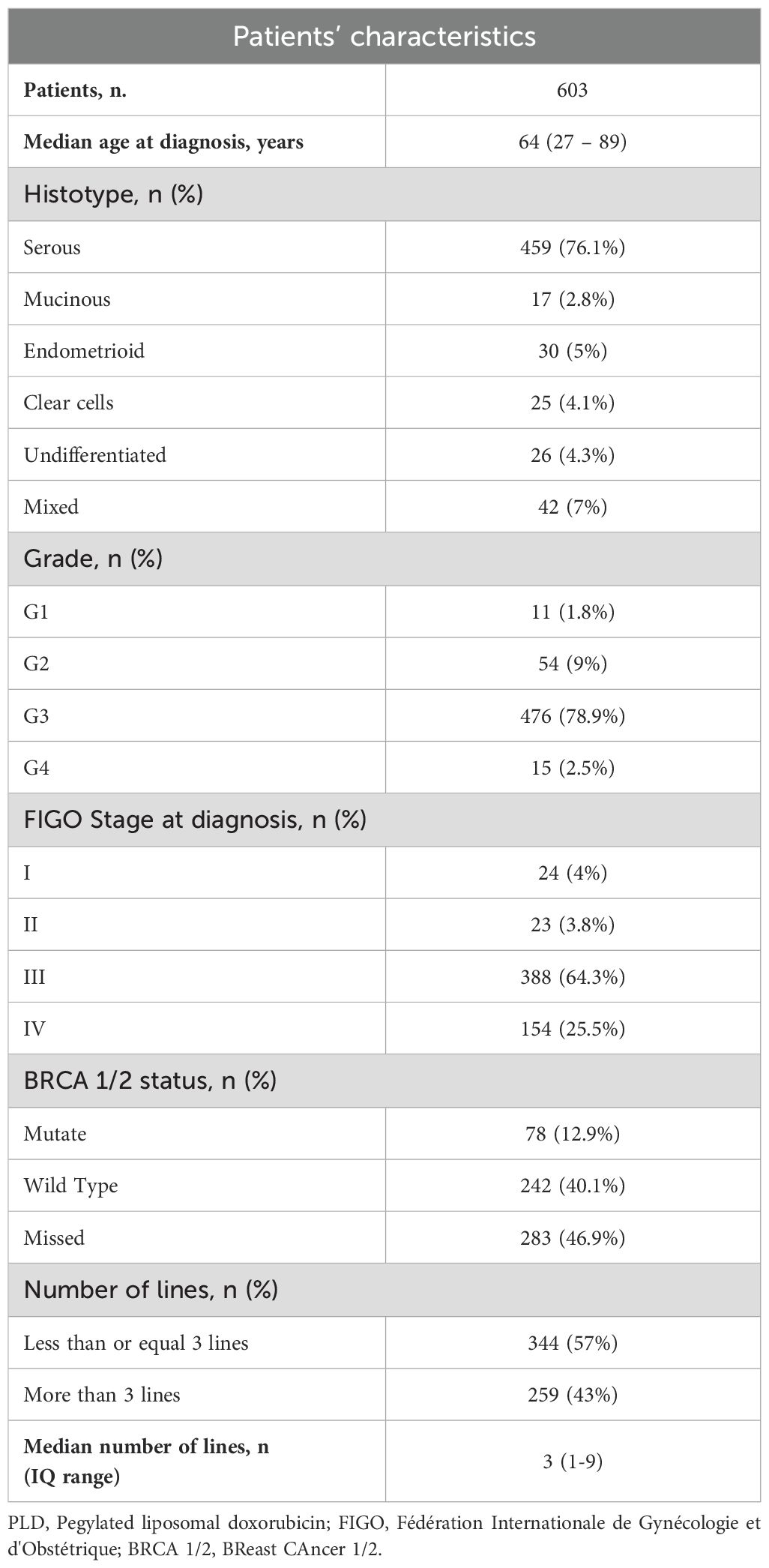
Table 2. Patients’ characteristics.
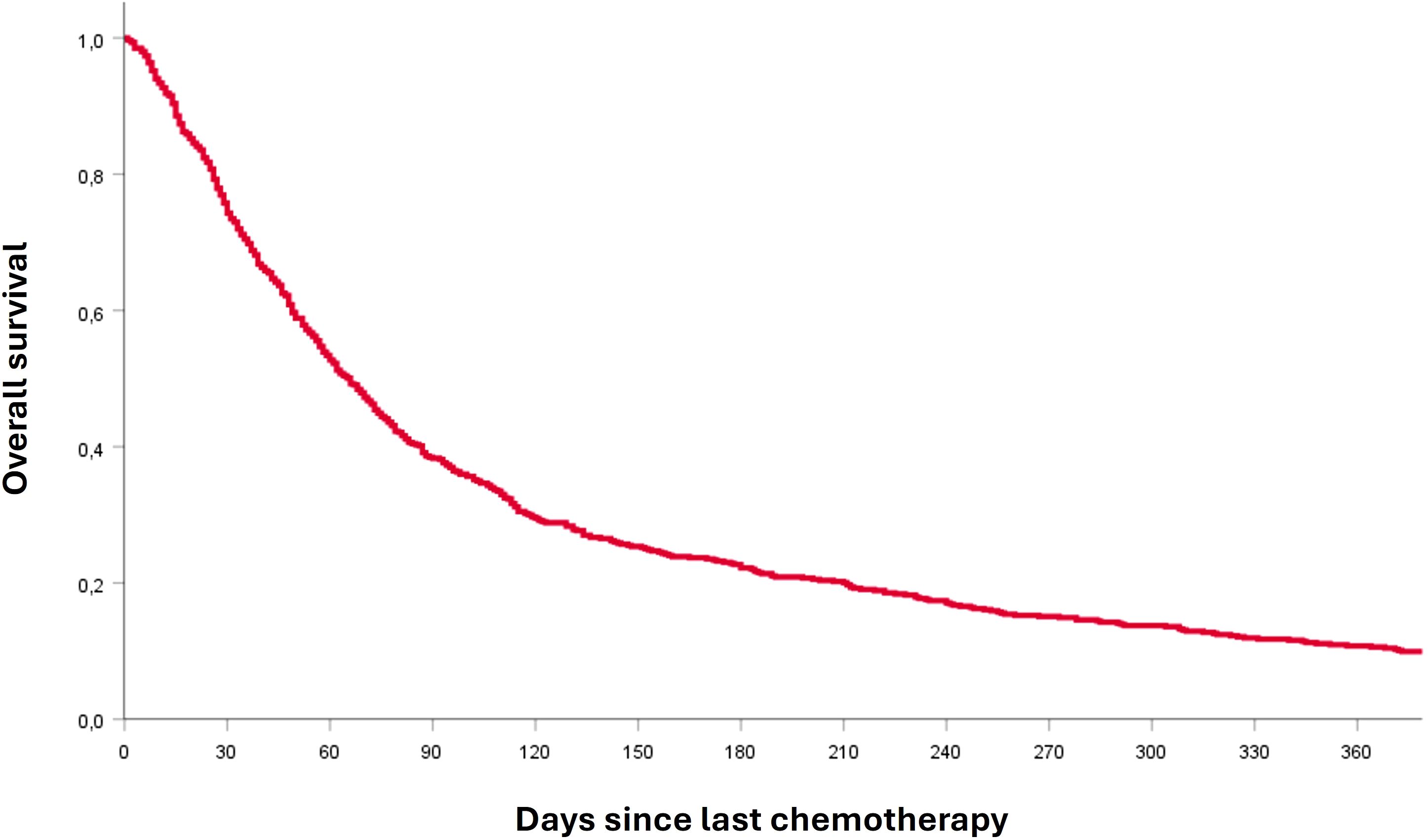
Figure 1. Kaplan-Meier survival curve from the day of the last chemotherapy administration to death.
Analysis of association
The association of various factors with the likelihood of chemotherapy administration in the last 30 days of life was analyzed (Table 3). End-of-life place (palliative care at home/hospice vs. hospital) was significantly associated with the administration of chemotherapy (p<0.001) in the last 30 days: only 19.8% of patients whose end of life place was palliative care at home/hospice received chemotherapy, while 41.4% of patients who died in hospital received chemotherapy in the last thirty days. Enrollment in at least one clinical trial during the disease history was found to be significantly associated (p=0.027) with receiving chemotherapy at the end of life: patients enrolled in at least one protocol had a lower probability (16.1%) compared to non-enrolled patients (27.3%). Having a neutrophil/lymphocyte ratio greater than or equal to 5 at the start of last therapy was associated with a higher likelihood of receiving chemotherapy in end-of-life than having a neutrophil/lymphocyte ratio lower than 5 (40.6% vs. 22.6%, p<0.001). Borderline significance was found for the C-reactive protein, which was tested at the start of the last chemotherapy in only 139 patients (23.1%): it was observed that 27.6% of patients with a C-reactive protein ≥5 received chemotherapy in the last 30 days of life, while 12.2% of patients with a C-reactive protein <5 received therapy (p=0.05). Finally, the association between centers of origin (North/Central-South) and chemotherapy administration at the end of life was statistically significant: patients afferent to a center in the North were less likely to receive chemotherapy in the last thirty days than patients in the Central-Southern Italy (19.5% vs. 41.7%, p<0.001).
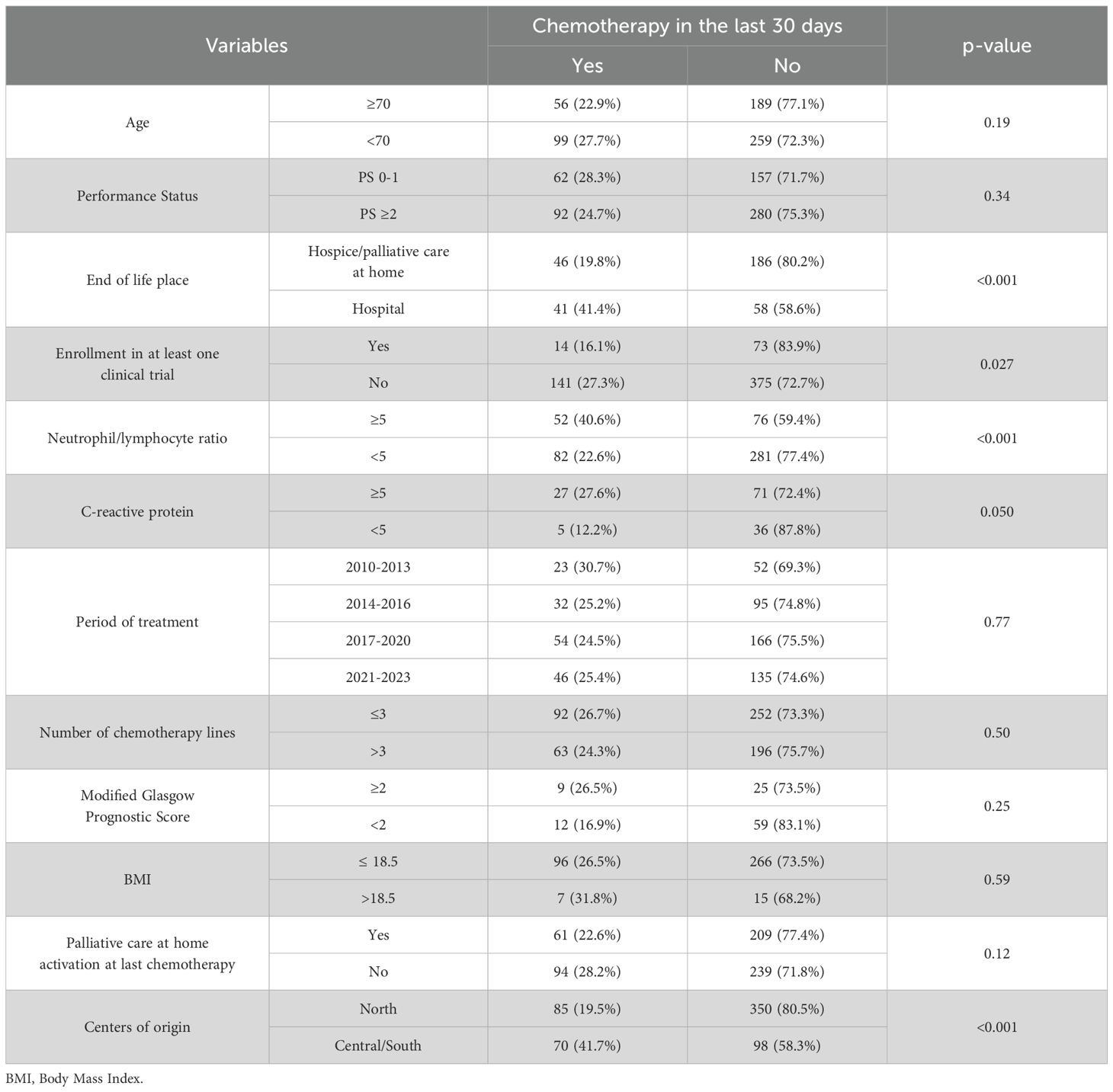
Table 3. Relationship between variables and probability of receiving chemotherapy in the end of life.
At multivariate logistic regression analysis, including clinical variables with a statistically significant association at univariate analysis, 2 clinical variables included were significantly associated with chemotherapy administration at the end of life. In detail, chemotherapy administration at the end of life was less likely in patients enrolled in at least 1 clinical trial (Odds Ratio (OR) 0.43, 95% CI 0.20 – 0.95, p=0.037) and was more likely in patients treated in centers from Central-Southern Italy (OR 3.60, 95% CI 1.94 – 6.69, p<0.001). In addition, chemotherapy administration at the end of life was more likely in patients whose end of life place was the hospital compared to home/hospice (OR 1.73, 95% CI 0.96 – 2.14, p=0.07), although the result was not statistically significant.
Discussion
The TO CARE/MITO 42 is the first multicenter study that analyzed the Italian practice about chemotherapy in the end of life in ovarian cancer patients. Our case series had 603 patients, from ten Italian centers, 5 centers in Northern Italy and 5 centers in Central and Southern Italy, all belonging to the MITO group, a cooperative research group in the field of gynecologic oncology. The fact that we chose only centers belonging to the MITO group allowed us to select a homogeneous case series, both from the surgical and oncological treatment point of view and reasonably representative of the Italian landscape. About one patient out of four (25.7%, 155/603) received chemotherapy in the last thirty days of life, in contrast to ESMO Guidelines 2021 (6), highlighting how this aggressive treatment at the end of life is still to be considered a very complex and under-studied topic.
The neutrophil/lymphocyte ratio is reported to be a prognostic factor in ovarian cancer, as well as in other tumor types (23). In a meta-analysis including nearly 3000 patients from 10 trials, patients with high pre-treatment neutrophil/lymphocyte ratio were found to have worse overall survival and progression free survival than patients with low pre-treatment neutrophil/lymphocyte ratio (22). In our case series, this subgroup of patients with neutrophil/lymphocyte ratio ≥5 at last-line initiation, using the cut-off used in the study by Roncolato et al. (20), in addition to having worse prognosis, in agreement with the literature, also showed to be more likely to receive, improperly, chemotherapy at the end of life (p<0.001). Thus, this is a selection of worse prognosis patients, potentially at risk of death in the short term, as also shown in the study by Kiuchi et al. (21)
Elevated C-reactive protein is also considered a negative prognostic factor for ovarian cancer patients (25, 26). We observed how patients with elevated C-reactive protein (cut-off of 5 mg/dL) at the start of the last line of chemotherapy seem to be more likely to receive chemotherapy at the end of life (p=0.05). This result is borderline statistical significance; however, it should be considered that this data was only available for 139 patients (23.1% of the total case series), reducing the statistical power of the analysis. In the study by Utsumi et al. (16) a lower performance status, high white blood cell count and high C-reactive protein were significantly correlated with shorter survival after the last treatment performed (p=0.004, 0.006 and 0.027, respectively). These observations spur us to perform complete blood tests on patients before starting a new line of treatment, including, of course, complete blood count but also laboratory parameters indicative of systemic inflammation, such as, indeed, C-reactive protein.
Death in hospital is among factors considered from the National Quality Forum as an indicator of aggressive medical care (27). In our case series, patients who died in the hospital (99 patients), compared with patients who died having activated palliative care at home or admitted to hospice (232 patients), were more likely to be treated with chemotherapy at the end of life (p<0.001). This result also agrees well with the literature, as shown by studies by Kajiyama and colleagues conducted in Japan, albeit on a smaller case series (28, 29). Recognizing when a patient can benefit from early activation of palliative care even during active treatment, is crucial and can make the transition between active treatment and best supportive care less difficult and sharp, avoiding unnecessary and harmful treatments for the patient, but also costly for public health (10).
The association between the geographical distribution of the center where the patient was treated (North vs. Center-South of Italy) and chemotherapy administration in the last 30 days is interesting: only 19.5% of patients enrolled in centers in the North received chemotherapy at the end of life, compared with 41.7% of patients from the Center-South (p<0.001). There are objective and documented differences in palliative care services between Northern and Southern Italy, as well as different management of resources in the territory (30). It should also be noted that, in our case series, the majority of patients enrolled in centers in the north were from university hospitals or research centers compared to those enrolled in the south (n=391 from university centers in the north versus n=108 from the south). This imbalance in source centers could further explain the difference found in the management of these patients, as clinicians working at university hospitals or research centers may have more experience in treating patients at the end of life.
These data urge us to have a more in-depth discussion among colleagues and, in the context of a multicenter group such as MITO, to look for ways to improve and try to increasingly smooth out such differences between centers. Patient enrollment within clinical protocols is a significant finding, but in contrast with already published data in the literature (31). In fact, being enrolled in at least one clinical protocol during disease history would lead to a lower likelihood of chemotherapy at the end of life (p=0.027). Certainly, the experience of “investigator” clinicians in MITO centers may have given reason for how they are able, especially for patients enrolled in research trials, to recognize when it is necessary to stop with active treatments. It is important to emphasize that these conclusions should be applied with caution to first-line patients. In fact, an outcome benefit has also been described for ovarian cancer patients who, despite their low performance status (Performance Status Eastern Cooperative Oncology Group ≥3), initiate first-line chemotherapy (32).
The retrospective nature of the study is a weakness and, in addition, the analyzed case series suffers from missing data. On the other hand, there is no Italian work of this magnitude in the literature (more than 600 patients). Our case series also included 63 patients with an interval from last chemotherapy to death of more than one year. It is more plausible that these patients did not die from ovarian cancer, although the retrospective nature of the case history does not allow us to be certain, as ‘cause of death’ data was not collected. However, we consider that since this population represents only 10% of all potential patient, this data did not impair the main analysis.
Recommendations for clinical practice and future research
This Italian multicenter retrospective study showed that about one quarter of ovarian cancer patients who underwent surgery between 2010 and 2020 received chemotherapy in the last thirty days of life. The TO CARE/MITO 42 trial has effectively outlined the Italian practice regarding the topic of chemotherapy at the end of life. These data should encourage the development of standardized national policies for end-of-life care and the design of prognostic tools for the timely integration of palliative care. In addition, it becomes necessary to explore interventions to reduce regional disparities. Prospective observational clinical trials are needed to create tools for clinicians to identify women with a particularly poor prognosis who are unlikely to benefit from chemotherapy in order to avoid unnecessary, expensive, and toxic treatments in the last days of life.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Coordinating Center Hospital Umberto I, Mauriziano in Turin (protocol code 0112587, date of approval 13 Oct 2022). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
GS: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. AG: Data curation, Writing – original draft, Writing – review & editing. RF: Writing – original draft, Writing – review & editing. GB: Writing – original draft, Writing – review & editing. FL: Writing – original draft, Writing – review & editing. LS: Writing – original draft, Writing – review & editing. AT: Writing – original draft, Writing – review & editing. FB: Writing – original draft, Writing – review & editing. GC: Writing – original draft, Writing – review & editing. MG: Writing – original draft, Writing – review & editing. FA: Writing – original draft, Writing – review & editing. BM: Writing – original draft, Writing – review & editing. AB: Writing – original draft, Writing – review & editing. MD: Writing – original draft, Writing – review & editing. JV: Writing – original draft, Writing – review & editing. SP: Conceptualization, Writing – original draft, Writing – review & editing. RC: Writing – original draft, Writing – review & editing. MA: Writing – original draft, Writing – review & editing. IR: Writing – original draft, Writing – review & editing. MT: Writing – original draft, Writing – review & editing. VT: Writing – original draft, Writing – review & editing. MDM: Data curation, Methodology, Writing – original draft, Writing – review & editing. GV: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by VALG_RIC_COMP_21_01 to GV.
Acknowledgments
I would like to express my gratitude to Professor Giorgio Valabrega, for his guidance, encouragement, and support throughout this project. This research paper would not have been possible without collaboration of the members of MITO. I’m grateful for their support and collaboration, and for their constructive criticism and valuable feedback.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. ECIS - European Cancer Information System. Estimates of cancer incidence and mortality in 2020, for all cancer sites (2023). Available online at: https://ecis.jrc.ec.europa.eu/explorer.php?$0-0$1-AE28E$4-2$3-All$6-0,85$5-2022,2022$7-7$2-All$CEstByCancer$X0_8-3$CEstRelativeCanc$X1_8-3$X1_9-AE27$CEstBySexByCancer$X2_8-3$X2_-1-1/ (Accessed 26 December 2023).
2. Jayson GC, Kohn EC, Kitchener HC, and Ledermann JA. Ovarian cancer. Lancet (2014) Oct;. (9951) 384:1376–88. doi: 10.1016/S0140-6736(13)62146-7
3. González-Martín A, Harter P, Leary A, Lorusso D, Miller RE, Pothuri B, et al. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. (2023) 34:833–48. doi: 10.1016/j.annonc.2023.07.011
4. Hanker LC, Loibl S, Burchardi N, Pfisterer J, Meier W, Pujade-Lauraine E, et al. The impact of second to sixth line therapy on survival of relapsed ovarian cancer after primary taxane/platinum-based therapy. Ann Oncol. (2012) 23:2605–12. doi: 10.1093/annonc/mds203
5. Hui D, Nooruddin Z, Didwaniya N, Dev R, De La Cruz M, Kim SH, et al. Concepts and definitions for “Actively dying,” “End of life,” “Terminally ill,” “Terminal care,” and “Transition of care”: a systematic review. J Pain Symptom Manage. (2014) 47:77–89. doi: 10.1016/j.jpainsymman.2013.02.021
6. Crawford GB, Dzierżanowski T, Hauser K, Larkin P, Luque-Blanco AI, Murphy I, et al. ESMO 2021 Care of the adult cancer patient at the end of life: ESMO Clinical Practice Guidelines ESMO Open. ESMO Open. (2021) 6:100225. doi: 10.1016/j.esmoop.2021.100225
7. Luta X, Maessen M, Egger M, Stuck AE, Goodman D, Clough-Gorr KM, et al. Measuring intensity of end of life care: a systematic review. PloS One. (2015) 10:e0123764. doi: 10.1371/journal.pone.0123764
8. Ma Z, Li H, Zhang Y, Zhang L, Huang G, Zhang Y, et al. Prevalence of aggressive care among patients with cancer near the end of life: a systematic review and meta-analysis. EClinicalMedicine. (2024) 71:102561. doi: 10.1016/j.eclinm.2024.102561
9. Mullins MA, Ruterbusch JJ, Clarke P, Uppal S, Wallner LP, and Cote M. Trends and racial disparities in aggressive end of life care for a national sample of women with ovarian cancer. Cancer. (2021) 127:2229–37. doi: 10.1002/cncr.33488
10. Urban RR, He H, Alfonso R, Hardesty MM, and Goff BA. The end of life costs for Medicare patients with advanced ovarian cancer. Gynecol Oncol. (2018) 148:336–41. doi: 10.1016/j.ygyno.2017.11.022
11. Wright AA, Hatfield LA, Earleet CC, and Keating NL. End-of-life care for older patients with ovarian cancer is intensive despite high rates of hospice use. J Clin Oncol. (2014) 32:3534–9. doi: 10.1200/JCO.2014.55.5383
12. Tabuyo-Martin A, Torres-Morales A, Pitteloud MJ, Kshetry A, Oltmann C, Pearson JM, et al. Palliative medicine referral and end-of-life interventions among racial and ethnic minority patients with advanced or recurrent gynecologic cancer. Cancer Control. (2023) 30:10732748231157191. doi: 10.1177/10732748231157191
13. Brown AJ, Sun CC, Prescott LS, Taylor JS, Ramondetta LM, and Bodurka DC. Missed opportunities: patterns of medical care and hospice utilization among ovarian cancer patients. Gynecol Oncol. (2014) 135:244–8. doi: 10.1016/j.ygyno.2014.08.039
14. Fauci J, Schneider K, Walters C, Boone J, Whitworth J, Killian E, et al. The utilization of palliative care in gynecologic oncology patients near the end of life. Gynecol Oncol. (2012) 127:175–9. doi: 10.1016/j.ygyno.2012.06.025
15. Sompratthana T, Phoolcharoen N, Schmeler KM, and Lertkhachonsuk R. End-of-life symptoms and interventions among women with gynecologic cancers in a tertiary-care hospital in Thailand. Int J Gynecol Cancer. (2019) 29(5):ijgc-2019-000338. doi: 10.1136/ijgc-2019-000338
16. Utsumi F, Kajiyama H, Niimi K, Sekiya R, Sakata J, Suzuki S, et al. Clinical significance and predicting indicators of post-cancer-treatment survival in terminally ill patients with ovarian cancer. J Obstet Gynaecol Res. (2017) 43:365–70. doi: 10.1111/jog.13219
17. Barbera L, Elit L, Krzyzanowska M, and Bierman AS. End of life care for women with gynecologic cancers. Gynecol Oncol. (2010) 118:196–201. doi: 10.1016/j.ygyno.2010.04.014
18. Broekman KE, van der Aa MA, Nijman HW, Jalving M, and Reyners AKL. End-of-life care for patients with advanced ovarian cancer in the Netherlands: A retrospective registry-based analysis. Gynecol Oncol. (2022) 166:148–53. doi: 10.1016/j.ygyno.2022.04.017
19. Palaia I, Tomao F, Santangelo G, Di Pinto A, Sassu CM, Perniola G, et al. The EOLO (End-of-life ovarian cancer) study: approach to ovarian cancer patients at the end of life. Oncology. (2019) 97:306–10. doi: 10.1159/000501721
20. Roncolato FT, O’Connell RL, Joly F, Lanceley A, Hilpert F, Buizen L, et al. Predictors of progression free survival, overall survival and early cessation of chemotherapy in women with potentially platinum sensitive (PPS) recurrent ovarian cancer (ROC) starting third or subsequent line(≥3) chemotherapy - The GCIG symptom benefit study (SBS). Gynecol Oncol. (2020) 156:45–53. doi: 10.1016/j.ygyno.2019.10.001
21. Kiuchi K, Hasegawa K, Watanabe M, Motegi E, Kosaka N, and Fukasawa I. Clinical indicators useful in decision-making about palliative chemotherapy for end-of-life ovarian cancer patients. Arch Gynecol Obstet. (2022) 305:425–30. doi: 10.1007/s00404-021-06162-z
22. Gramling R, Fiscella K, Xing G, Hoerger M, Duberstein P, Plumb S, et al. Determinants of patient-oncologist prognostic discordance in advanced cancer. JAMA Oncol. (2016) 2:1421–6. doi: 10.1001/jamaoncol.2016.1861
23. Zhu Y, Zhou S, Liu Y, Zhai L, and Sun X. Prognostic value of systemic infammatory markers in ovarian Cancer: a PRISMA compliant meta-analysis and systematic review. BMC Cancer. (2018) 18:443. doi: 10.1186/s12885-018-4318-5
24. Roncolato FT, Berton-Rigaud D, O’Connell R, Lanceley A, Sehouli J, Buizen L, et al. Validation of the modified Glasgow Prognostic Score (mGPS) in recurrent ovarian cancer (ROC)—analysis of patients enrolled in the GCIG Symptom Benefit Study (SBS). Gynecol Oncol. (2018) 148:36–41. doi: 10.1016/j.ygyno.2017.10.019
25. Mahmoud FA and Rivera NI. The role of C-reactive protein as a prognostic indicator in advanced cancer. Curr Oncol Rep. (2002) 4:250–5. doi: 10.1007/s11912-002-0023-1
26. Hefler LA, Concin N, Hofstetter G, Marth C, Mustea A, Sehouli J, et al. Serum C-reactive protein as independent prognostic variable in patients with ovarian cancer. Clin Cancer Res. (2008) 14:710–4. doi: 10.1158/1078-0432.CCR-07-1044
27. National Quality Forum. National voluntary consensus standards for quality of cancer care, cancer care phase I-II, may 2009 (2021). Available online at: http://www.qualityforum.org/publications/2009/05/National_voluntary_consensus_standards_for_Quality_of_Cancer_Care.aspx/ (Accessed 23 December 2021).
28. Kajiyama H, Utsumi F, Higashi M, Sakata J, Sekiya R, Mizuno M, et al. Is there any association between where patients spend the end of life and survival after anticancer treatment for gynecologic Malignancy? J Palliat Med. (2014) 17:325–30. doi: 10.1089/jpm.2013.0366
29. Kajiyama H, Suzuki S, Shimbo A, Utsumi F, and Yoshikawa N. Survival after anticancer treatment of terminally ill patients with ovarian carcinoma. J Palliat Med. (2020) 23:1060–5. doi: 10.1089/jpm.2019.0456
30. Ostan R, Varani S, Pannuti F, Pannuti R, Biasco G, and Bruera E. End-of-life care for patients with cancer: Clinical, geographical, and sociocultural differences. Palliat Support Care. (2023) 22(1):155–62. doi: 10.1017/S1478951523000032
31. Nitecki R, Bercow AS, Gockley AA, Lee H, Penson RT, and Growdon WB. Clinical trial participation and aggressive care at the end of life in patients with ovarian cancer. Int J Gynecol Cancer. (2020) 30(2):201–6. doi: 10.1136/ijgc-2019-000851
32. Seifert H, Georgiou A, Alexander H, Alexander H, McLachlan J, Bodla S, et al. Poor performance status (PS) is an indication for an aggressive approach to neoadjuvant chemotherapy in patients with advanced epithelial ovarian cancer (EOC). Gynecol Oncol. (2015) 139:216–20. doi: 10.1016/j.ygyno.2015.08.015
Keywords: ovarian cancer, chemotherapy, end of life, quality of life, gynecologic cancer
Citation: Scotto G, Galatà A, Fruscio R, Besana G, Landoni F, Sgro L, Testi A, Borella F, Cormio G, Gianciotta M, Arezzo F, Maiorano BA, Baldoni A, Destefanis M, Ventriglia J, Pignata S, Chiari R, Azzolina MC, Raimondo I, Turinetto M, Tuninetti V, Di Maio M and Valabrega G (2025) Time tO last ChemotherApy and death in ovaRian cancEr patients: TO CARE/MITO 42 study, a retrospective analysis of italian MITO centers. Front. Oncol. 15:1641758. doi: 10.3389/fonc.2025.1641758
Received: 05 June 2025; Accepted: 08 July 2025;
Published: 06 August 2025.
Edited by:
Paolo Scollo, Kore University of Enna, ItalyReviewed by:
Basilio Pecorino, Kore University of Enna, ItalyAref Zribi, Sultan Qaboos Comprehensive Cancer Care and Research Center, Oman
Copyright © 2025 Scotto, Galatà, Fruscio, Besana, Landoni, Sgro, Testi, Borella, Cormio, Gianciotta, Arezzo, Maiorano, Baldoni, Destefanis, Ventriglia, Pignata, Chiari, Azzolina, Raimondo, Turinetto, Tuninetti, Di Maio and Valabrega. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giulia Scotto, Z2l1bGlhLnNjb3R0b0Bhc2x0bzMucGllbW9udGUuaXQ=