 Karl R. Aigner
Karl R. Aigner Kornelia Aigner
Kornelia Aigner Marc J. H. Hendrikx1
Marc J. H. Hendrikx1 Abderrahmane Bekrentchir
Abderrahmane Bekrentchir- 1Department of Surgical Oncology, Medias Klinikum Burghausen, Burghausen, Germany
- 2Department of Tumor Biology, Medias Klinikum Burghausen, Burghausen, Germany
- 3Department of Anesthesiology, Medias Klinikum Burghausen, Burghausen, Germany
Introduction: We report a series of four patients with HPV-positive squamous cell carcinoma of the anus: two with non-previously treated grade G3 malignancies, and two with relapsing G2 tumors in progression after chemoradiation.
Method: Chemo-naive patients were treated with isolated hypoxic pelvic perfusion, whereas the two patients with local recurrences both received isolated hypoxic pelvic perfusion and concomitant reversible electroporation.
Results: The two patients without prior therapy showed a complete clinical and pathological response, one after two and one after three therapies. In the two patients with local recurrences, a clinico-pathological complete remission occurred after two isolated perfusions with electroporation. The two techniques combined produce highly effective drug exposure that leads to complete remission; subsequent blood purification by chemofiltration avoids toxic side effects and cumulative toxicity. The therapies caused no side effects affecting quality of life. No recurrences occurred in the observation period of 48, 27, 10 and 8 months.
Conclusion: Isolated hypoxic pelvic perfusion with electroporation is an effective, low-toxicity valid alternative to traditional therapies for the treatment of anal squamous cell carcinoma.
1 Introduction
Squamous cell carcinoma of the anus is a very rare but extremely debilitating tumor and only accounts for about 2% of all gastrointestinal tumors (1–4). However, the incidence appears to have increased slightly over the last decade. Due to the high chemosensitivity of squamous cell carcinoma chemoradiation is the treatment of choice compared to invasive surgical procedures (5, 6).
Nevertheless, the optimal treatment remains controversial given the sometimes exorbitant toxicity of chemotherapeutical drugs such as mitomycin and radiation therapy.
Many attempts have been made to reduce toxicity, with intensity-modulated radiation therapy bringing some improvement, whereas a quantitative reduction in chemotherapy by lowering the effective levels also reduces the therapeutic effect.
Hypoxic pelvic perfusion increases the sensitivity of some chemotherapeutic agents (e.g. cis platinum). Additionally limiting the chemotherapy exposure to the pelvic region reduces systemic toxicity which in turn minimizes systemic side effects.
Early case reports suggest that hypoxic pelvic perfusion can lead to high local response rates of rectal cancer (7).
However, hypoxic pelvic perfusion alone is limited by the challenge of ensuring complete tumor coverage.
Electroporation increases cell membrane permeability therefore enhancing chemotherapy drug effectiveness. Several clinical studies have shown that electroporation can enhance the local response however it is often limited by the depth of the tumor and the ability to treat larger more deeply seated tumors combining hypoxic pelvic perfusion and electroporation overcomes the limitation of each approach (8).
Astoundingly higher cytostatic drug levels and therefore greater effectiveness can be achieved through isolated pelvic regional perfusion with comparatively lower cytostatic drug dosages.
We present a series of four HPV-positive patients with anal cancer, two with malignancy grade G3 primary tumors, and two with recurrent G2 tumors. In the latter two cases there was a relapse after primary radiochemotherapy.
2 Materials and methods
2.1 Isolated hypoxic pelvic perfusion technique with chemofiltration
Under general anesthesia, two pneumatic cuffs are placed around the proximal thighs. Below the inguinal ligament, the femoral artery and vein are exposed through a longitudinal incision and cannulated with two triple-lumen stop-flow balloon catheters under systemic heparinization.
The balloons are placed proximal to the bifurcation of the aorta and vena cava under contrast medium control (Figure 1). The correct position of the balloons in the aorta and vena cava is ensured by brief blocking and photo documentation (Figure 2). Both balloons are then immediately released and the patient is ventilated with 100% oxygen for approximately three minutes to increase oxygen saturation before starting therapy.
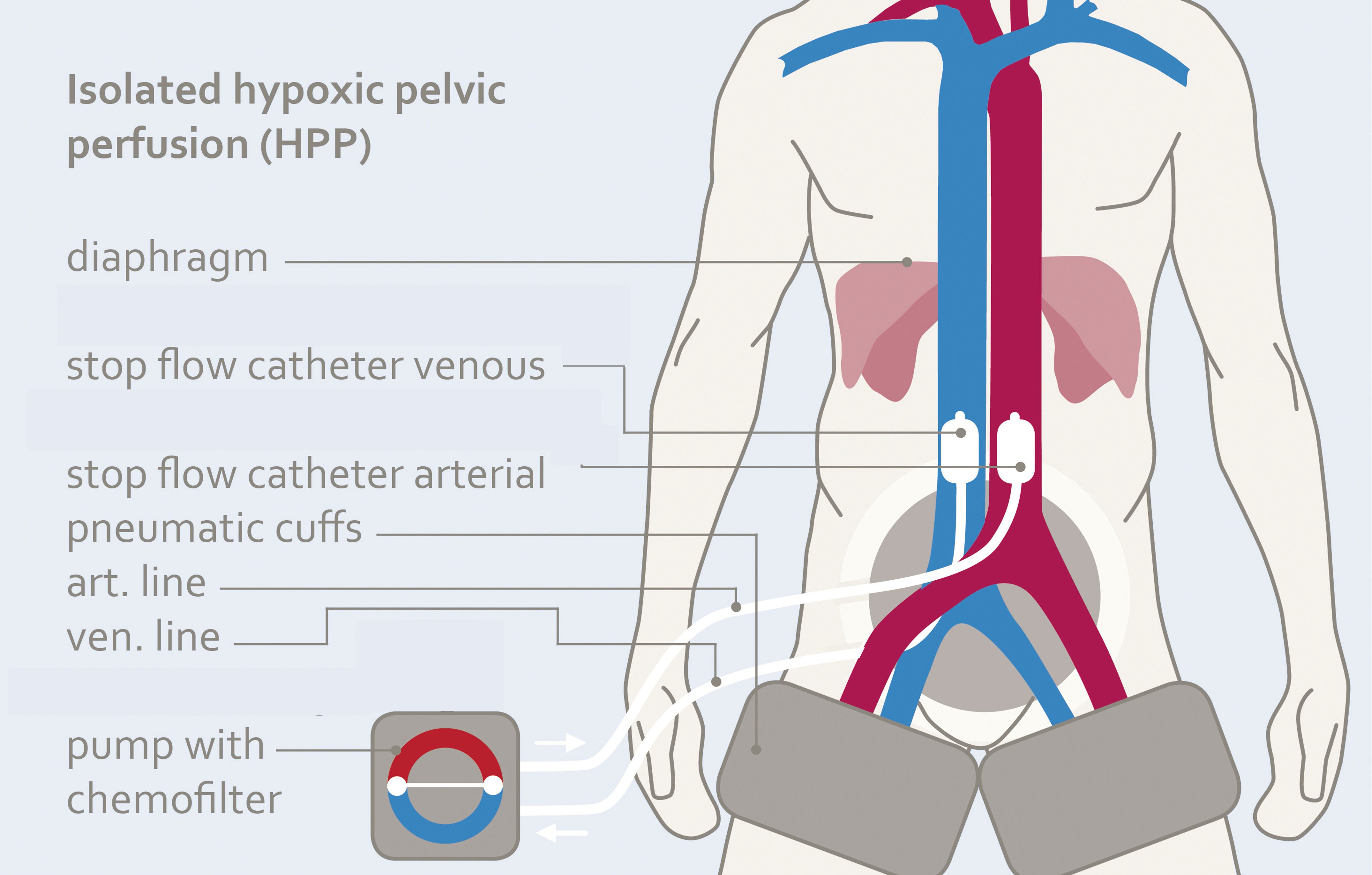
Figure 1. Scheme of isolated hypoxic pelvic perfusion (HPP) for short-term intraaortic infusion of cytotoxic agents Mitomycin, Doxorubicin and Cisplatin.
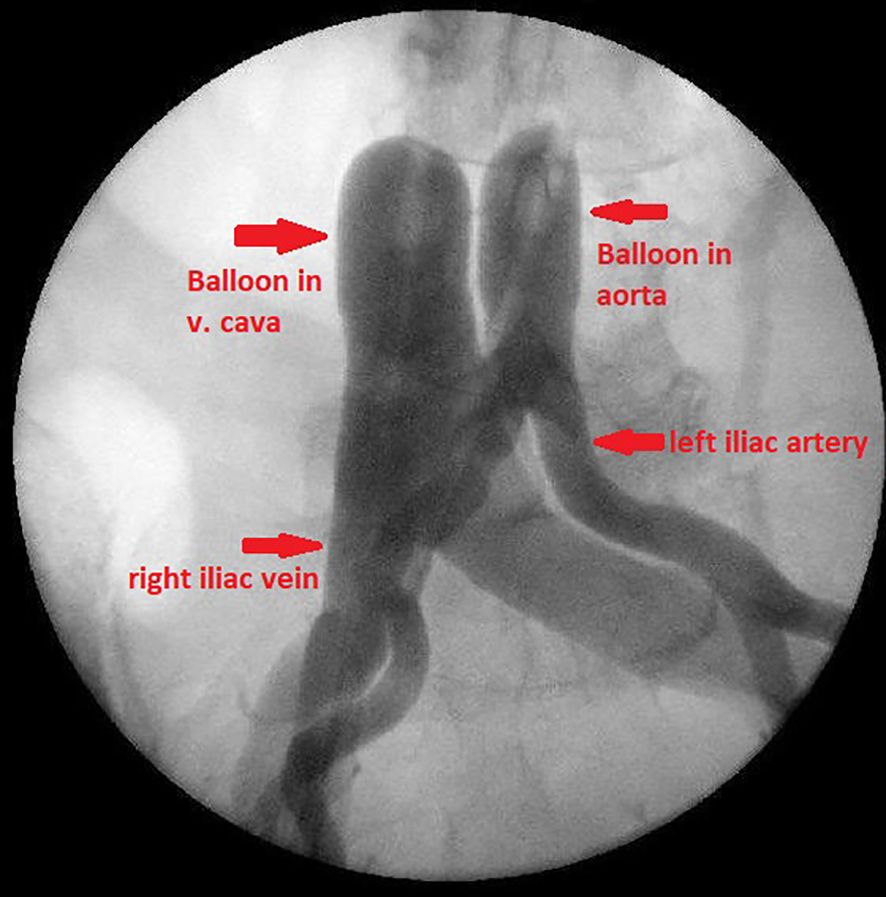
Figure 2. Balloon blocking of aorta and vena cava proximal to the bifurcations.
Chemotherapy is administered through rhythmic, pulsatile injections via the large perfusion channel of the aortic balloon catheter (Figure 3) over one to one and a half minutes to achieve high first-pass drug concentrations (Figure 4). Immediately afterwards, both balloons are blocked with diluted contrast medium. A five-minute so-called stop-flow phase creates a high first- pass effect and therefore a high uptake of cytostatics in the tumor area due to the high initial oxygen saturation. Isolated hypoxic perfusion is maintained for 15 minutes. The stop-flow phase is included in the total time of isolated hypoxic perfusion. Both balloons are then unblocked and the blood in the open system is filtered through capillary filters via the catheters still in place for approximately another 30 to 40 minutes until a filtrate volume of minimum 4 liters is reached. Finally, the two balloon catheters are removed, the vessels repaired with running sutures and the wound is closed.
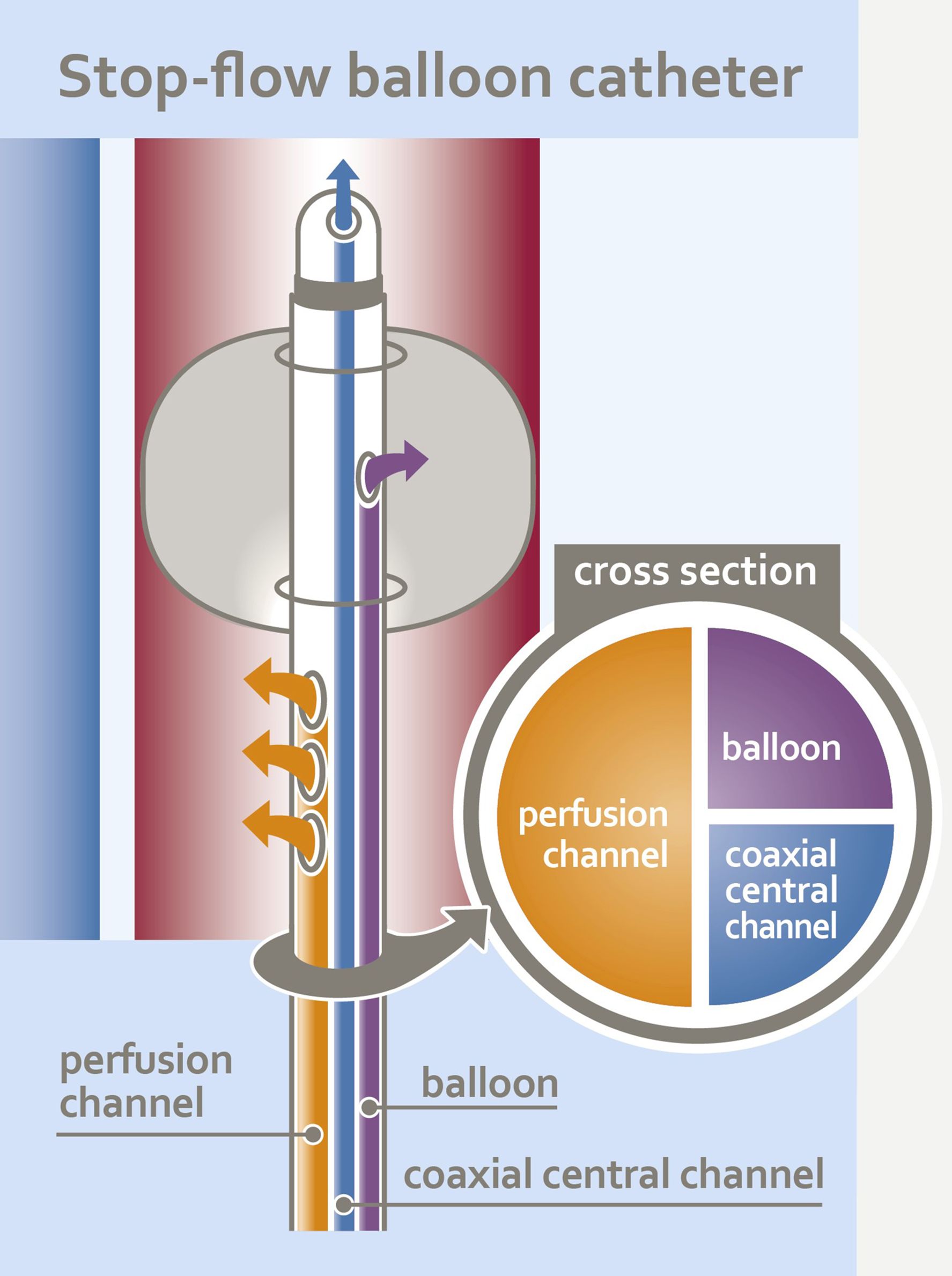
Figure 3. Schematic design of the triple-lumen stop-flow ballon catheter.
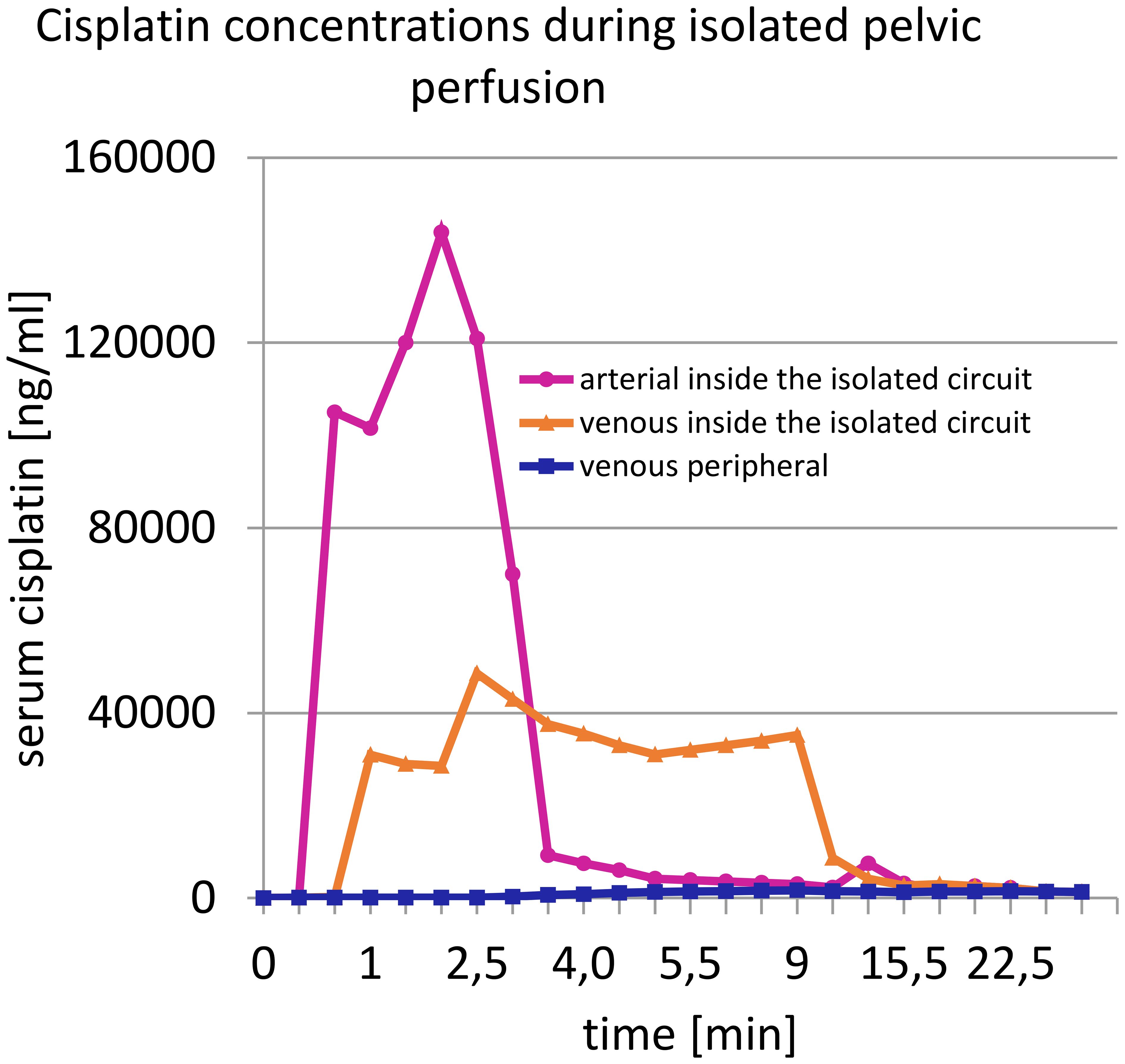
Figure 4. Concentration curve of cisplatin in the arterial and venous line at start of the stop-flow phase of isolated perfusion.
2.2 Electrochemotherapy
When combining isolated perfusion with reversible electroporation, three to four VGD- electrodes (needle diameter 1,2 mm, length 20 cm, active part 3 cm) (IGEA) are first placed under direct vision in the lithotomy position, close to the tumor extent (Figure 5), and connected to the Cliniporator VITAE (IGEA) pulse generator for adaptive electroporation. The patient is then placed in a normal supine position, the groin area is disinfected, and the femoral arteries and veins are cannulated (see 2.1). The chemotherapy drugs are administered during the electrical pulses.
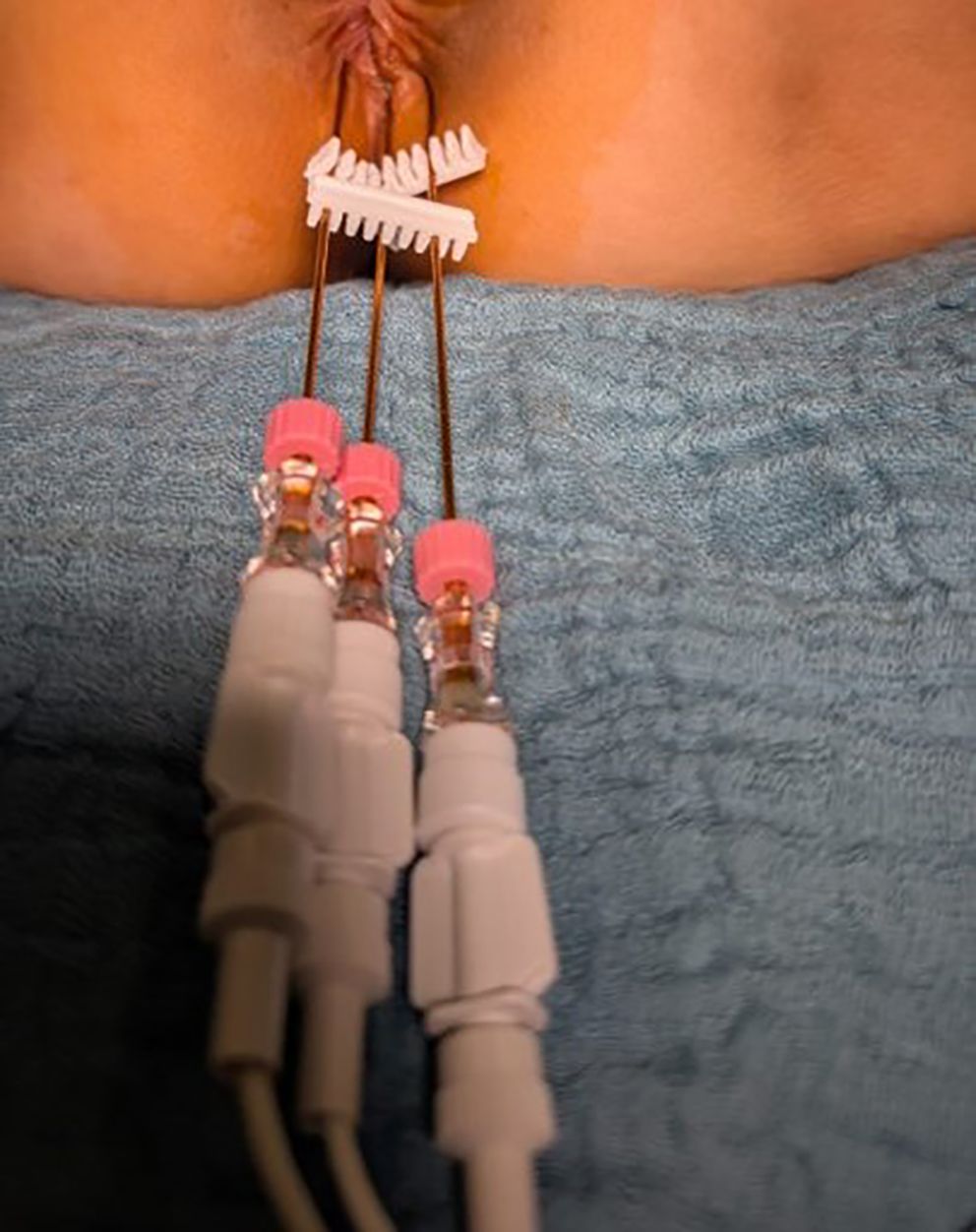
Figure 5. Positioning of the electrodes in anal carcinoma between 5 and 7 o’ clock in lithotomy position.
3 Results
Patient characteristics according to diagnosis, histology, previous treatment and type of therapy are listed in Table 1.
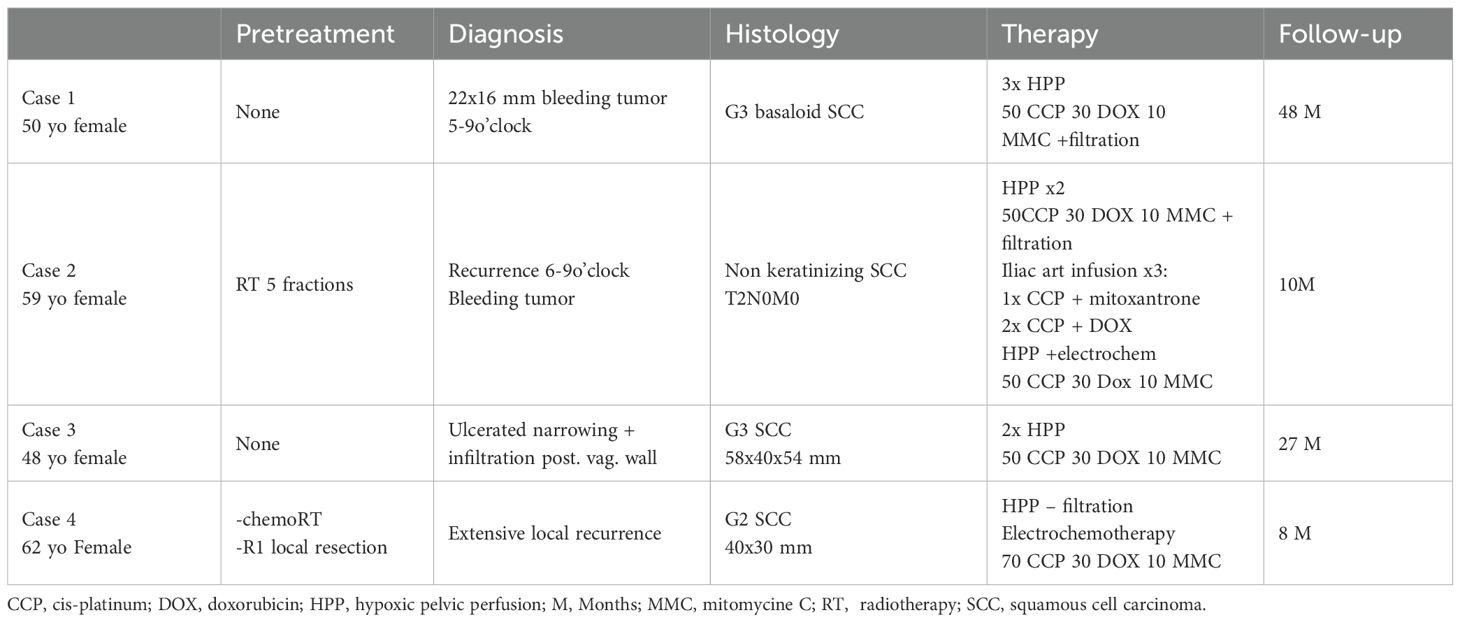
Table 1. Patient characteristics.
3.1 Case 1
The first case concerns a non-pretreated 50-year-old female patient with a 22 to 16 mm, occasionally bleeding squamous cell tumor near the skin margin, extending from 5 to 9 o’clock in the lithotomy position. Histologically, it was a malignancy grade G3 basaloid squamous cell carcinoma. Imaging revealed no evidence of lymph node metastases. The patient underwent a total of three cycles of isolated hypoxic pelvic perfusion, each containing 50 mg of cisplatin, 30 mg of doxorubicin, 10 mg of mitomycin, followed by chemofiltration. No systemic or local adverse effects were observed. Two days after the first treatment, the tumor had already become significantly softer and flatter. At the time of the second treatment, three weeks later, the patient experienced neither pain nor bleeding.
Before the third treatment, the tumor was no longer clearly demarcated on MRI, and two weeks later, on July 20, 2021, local excision of the former tumor region revealed a histologically complete remission. The patient has currently been disease-free in complete remission for 48 months.
3.2 Case 2
The second case concerns a 59-year-old female patient who was initially diagnosed with a T2N0M0 non-keratinizing bleeding anal squamous cell carcinoma (KI 67 of 50%) in November 2022 and received five fractions of radiotherapy. In January 2023 she presented with a local recurrence which was located at the 6–9 o’clock position and extended up to 4 cm into the anal canal. She underwent her first isolated hypoxic pelvic perfusion with chemofiltration (HPP-F) receiving 50 mg cisplatin, 30 mg doxorubicin, and 10 mg mitomycin. Before the second treatment, three weeks later in February 2023, with the same technique and dosage, the tumor size had decreased by more than half both macroscopically and on palpation. Six days after the second HPP-F, only two residual small indurations were visible, and the final treatment was scheduled three weeks later. Due to unforeseen personal circumstances, the patient was unable to attend the appointment. A follow-up examination two months later revealed increasing local induration, suggesting a recurrence. Three consecutive angiographic infusions into the iliac artery with one cisplatin/mitoxantrone and two cisplatin/doxorubicin infusions failed to result in significant improvement. Only when the patient consented to isolated pelvic perfusion with reversible electroporation using the cytostatic combination of 50 mg of cisplatin, 30 mg of doxorubicin, and 10 mg of mitomycin in September 2024 did rapid tumor reduction occur. The patient did not suffer any significant toxicities due to subsequent chemofiltration with capillary filters. Re-excision of the previously necrotic tumor area demonstrated a histologically complete remission. The patient is currently free of symptoms or relapses since the last therapy 10 months ago.
3.3 Case 3
The third case concerns a non-pretreated 48-year-old female patient with an ulcerated grade G3 squamous cell carcinoma of the anus (5.8 × 4 × 5.4 cm) showing narrowing growth and infiltration of the posterior vaginal wall.
She experienced severe pain when sitting and walking. One day after the first isolated perfusion with 50 mg cisplatin, 25 mg doxorubicin, and 10 mg mitomycin and chemofiltration in March 2023, the patient was pain-free without evidence of toxicity.
Prior to the second isolated perfusion using the same dosage, no tumor was palpable locally; only 90% regressive tumor residue was found on biopsy at the former infiltration site of the posterior vaginal wall. The patient did not attend a third appointment for treatment. A follow- up examination one year later revealed a complete remission by biopsy.
The patient is currently disease-free in complete remission for 27 months.
3.4 Case 4
This 62-year-old female patient was diagnosed with grade G2 squamous cell carcinoma measuring 4x3 cm in January 2024.
In February/March 2024, chemoradiotherapy was performed without apparent clinical response, followed by a local R1 resection. When extensive local recurrence occurred, the patient was advised to undergo rectal amputation, which she declined. She underwent hypoxic isolated pelvic perfusion (HPP-F) to avoid rectal amputation.
Due to the advanced stage of the disease with a rapid progressive recurrence, we combined HPP-F and reversible electroporation with 70 mg of cisplatin, 30 mg of doxorubicin and 10 mg of mitomycin in October 2024. After the treatment, pain was significantly reduced, and the patient’s general condition improved considerably.
After the second HPP-F in November 2024 without any toxic side-effects, repeated biopsies revealed complete histological remission, currently for 8 months.
4 Discussion
Historically, the primary treatment for anal cancer was abdominoperineal resection (APR), a radical surgery leaving patients with a permanent colostomy. This was standard through the mid-20th century, though it had significant drawbacks: high morbidity, poor quality of life, and a risk of cancer recurrence. The 5-year survival rate was approximately 50% (3, 9). When used as a salvage surgery after failed CRT the 2-year OS is ~60%, but 5-year OS drops to ~24.5%.
A major breakthrough came in the late 1970s and early 1980s with the introduction of the Nigro protocol, a pioneering approach combining radiation therapy with chemotherapy (5-fluorouracil and mitomycin C) (10–12). This approach demonstrated that many patients could achieve complete remission without surgery. As a result, chemoradiation became the standard of care, allowing for organ preservation. Local control is achieved in 68 - 84%, colostomy-free survival in 65 - 75% and 5-year OS in 65 – 79% (4, 13–17).
Acute toxicities are common: hematologic (cytopenias), mucocutaneous, gastrointestinal, genitourinary symptoms. Late effects may include chronic bowel dysfunction, sexual dysfunction, infertility, or chronic pain. Even local excision alone of stage I anal cancer can be effective and curative. However, careful follow-up is required because the 5-year progression-free survival after combination with radiochemotherapy is slightly better at 91 versus 83% for local excision (18). Radiochemotherapy regimens consisting of 5-fluorouracil and mitomycin and concomitant radiation achieved stage-dependent 5-year survival rates of up to 90% and sphincter preservation of up to 80% (12, 19) while avoiding rectal amputation (20, 21). Despite these excellent clinical results (15), the severe toxicity with mandatory interruption of therapy clouds the overall picture in approximately half of the cases.
Precisely because of the good clinical results in the face of intolerable side-effects such as nephrotoxicity or pulmonary fibrosis, attempts were made to modify the treatment regimens, using immunotherapy (22–24), new drugs such as capecitabine or paclitaxel, or intensity – modulated radiotherapy (25–27), to improve quality of life while maintaining clinical outcomes.
Isolated perfusion therapy can be viewed as a further step in terms of both intensifying therapy and minimizing or eliminating side effects. It can be applied to all body regions (28) or segments in the form of an isolated circuit.
For hypoxic perfusion, which we prefer to use, mitomycin is best suited as a very potent chemotherapeutic agent for gastrointestinal tumors because of its up to tenfold increase in cytotoxicity under hypoxic conditions. The same applies to doxorubicin. The efficacy of Cisplatin is not affected. All other common chemotherapy drugs have reduced cytotoxicity under hypoxia (29).
The high effective concentrations of cytostatics are achieved on the one hand by the low blood volumes in the perfusion circuit, but above all by the application of the cytostatics as a short-term arterial infusion into the isolated perfusion circuit. The high influx concentration of chemotherapy drugs over seven to twelve minutes leads to high uptake in the tumor tissue. This short-term intra-arterial infusion procedure has been shown to be effective in squamous cell carcinomas such as head and neck cancer (30, 31), in advanced cervical cancer (32), and more recently in anal cancer. Even in advanced osteosarcoma, complete remission can be achieved due to high local drug exposure using a technical variant (33).
In the two previously untreated patients, three and two isolated perfusion therapies were necessary; in the case of previous radiochemotherapy and recurrences as in cases two and four, repeated intra-arterial infusion alone was not sufficient because the local cytostatic exposure was too low. Only isolated pelvic perfusion in combination with electroporation achieved a histological complete remission (Table 2) due to increased cytostatic drug uptake via temporarily porous tumor cell membranes as a result of the electrical impulses (34).

Table 2. Results according to therapeutic options.
The dosages of chemotherapeutic agents used by us under locoregional perfusion chemotherapy are very different from those under systemic chemotherapy. The smaller treated volume and, above all, the only short-term intra-arterial application of the chemotherapeutic agent generate the required local exposure with the necessary high concentration. Therefore, the effectiveness of the therapy cannot be assessed based on the total dose used but rather based on the effective concentration over time. The total dose of cisplatin used in the present isolated pelvic perfusions is only 50 to 70 mg, of mitomycin 10, max 15 mg with, however, very effective local exposure with short-term intra-arterial infusion into the perfusion circuit.
On the one hand, chemofiltration after application of the cytostatics reduces the low toxicity of low-dose chemotherapeutic agents, but primarily prevents cumulative toxicity from occurring too quickly, especially from substances with cumulative toxicity such as mitomycin and doxorubicin.
Even though the number of cases is of course far too small and no binding statement can be made, it turns out that all four patients tolerated the therapies largely without any symptoms and no relevant adverse events in the sense of systemic toxicity occurred. The recurrence- free times in full remission are currently 48, 27, 10 and 8 months.
The present case series was simply intended to demonstrate that it is fundamentally possible to apply a proven, highly effective approach such as mitomycin compounds to squamous cell carcinoma, in this case anal carcinoma, using regional therapeutic methods that are modified to largely avoid disruptive and distressing adverse events. Isolated hypoxic pelvic perfusion and electrochemotherapy for anal cancer with short-term arterial infusion of chemotherapy drugs into the arterial perfusion line together produce highly effective drug exposure leading to complete remission. The subsequent blood purification using chemofiltration largely avoids toxic side effects and cumulative toxicity.
5 Conclusion
Isolated hypoxic pelvic perfusion combined with electroporation is an effective, low-toxicity valid alternative to traditional therapies for the treatment of anal squamous cell carcinoma.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Protected patient data. Requests to access these datasets should be directed to aW5mb0Bwcm9mLWFpZ25lci5kZQ==.
Ethics statement
The studies involving humans were approved by Medias Internal Review Board (MIRB). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
KRA: Formal Analysis, Writing – original draft, Methodology, Conceptualization, Validation, Investigation, Writing – review & editing, Supervision. KA: Methodology, Writing – review & editing. MH: Writing – review & editing. AB: Writing – review & editing. HA: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors wish to acknowledge Giuseppe Zavattieri for his help and assistance in preparing the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sodergren S, Vassiliou V, Dennis K, Tomaszewski KA, Gilbert A, Glynne-Jones R, et al. Systematic review of the quality of life issues associated with anal cancer and its treatment with radiochemoterapy. Support Cancer Care. (2015) 23:3613–23. doi: 10.1007/s00520-015-2879-2
2. Sauter C, Peeken JC, Borm K, Diehl C, Münch S, Combs SE, et al. Quality of life in patients treated with radiochemotherapy for primary diagnosis of anal cancer. Sci Rep. (2022) 12:4416. doi: 10.1038/s41598-022-08525-1
3. National Cancer Institute. Surveillance, epidemiology, and end results program. Cancer Stat Facts: Anal Cancer.
4. UKCCCR Anal Cancer Trial Working Party. Epidermoid anal cancer: Results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet. (1996) 348:1049–54. doi: 10.1016/S0140-6736(96)03409-5
5. Nigro ND. An evaluation of combined therapy for squamous-cell carcinoma of the anal canal. Dis Colon Rectum. (1984) 12:763–6. doi: 10.1007/BF02553933
6. Spithoff K, Cummings B, Jonker D, and Biagi JJ. Chemoradiotherapy for squamous cell cancer of the anal canal: a systematric review. Clin Oncol (R Coll Oncol). (1914) 26:473–87. doi: 10.1016/j.clon2014.03.005
7. Guadagni S, Fiorentini G, Mambrini A, Masedu F, Valentini M, Reay A, et al. Multidisciplinary palliation for unresectable recurrent rectal cancer: hypoxic pelvic perfusion with mitomycin C and oxaliplatin in patients progressing after systemic chemotherapy and radiotherapy, a retrospective cohort study. Oncotarget. (2019) 10:3840–51. doi: 10.18632/oncotarget.26972
8. Ferioli M, Arcelli A, Savino Cilla S, Zamir AA, Tolento G, Cuicchi D, et al. Electrochemotherapy for anorectal tumors: A narrative literature review. Technol Cancer Res Treat. (2025) 24:15330338251349596. doi: 10.1177/15330338251349596
9. Schraut WH, Wang CH, Dawson PJ, and Block GE. Depth of invasion, location, and size of cancer of the anus dictate operative treatment. Cancer. (1983) 51:1291–6. doi: 10.1002/1097-0142(19830401)51:7<1291::AID-CNCR2820510719>3.0.CO;2-R
10. Nigro ND, Vaitkevicius VK, and Considine BJ. Combined therapy for cancer of the anal canal: A preliminary report. Dis Colon Rectum. (1974) 17:354–6. doi: 10.1007/BF02586980
11. Leichman L, Nigro N, Vaitkevicius VK, and Steele SR. Cancer of the anal canal. Model for preoperative adjuvant combined modality therapy. Am J Med. (1985) 78:211–5. doi: 10.1016/0002-9343(85)90428-0
12. Osborne MC, Maykel J, Johnson EK, and Steele SR. Anal squamous cell carcinoma: an evolution in disease and management. World J Gastroenterol. (2014) 20:13052–13059. doi: 10.3748/wjg.v20.i36.13052
13. James RD, Glynne-Jones R, Meadows HM, Cunningham D, Sun Myint A, Saunders MP, et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): a randomised, phase 3, open-label, 2× 2 factorial trial. Lancet Oncol. (2013) 14:516–24. doi: 10.1016/S1470-2045(13)70086-X
14. Habr-Gama A, Julião GPS, and Perez RO. Anal cancer: leading the way. Lancet Oncol. (2017) 18:276–7. doi: 10.1016/S1470-2045(17)30073-6
15. Gondal TA, Chaudhary N, Bajwa H, Rauf A, Le D, and Ahmed S. Anal cancer: the past, present and future. Curr Oncol. (2023) 30:3232–50. doi: 10.3390/curroncol30030246
16. Flam M, John M, Pajak TF, Petrelli N, Myerson R, Doggett S, et al. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: results of a phase III randomized intergroup study. J Clin Oncol. (1996) 14:2527–39. doi: 10.1200/JCO.1996.14.9.2527
17. Troester A, Parikh R, Southwell B, Ester E, Sultan S, and Greeno E. Treatment of stage I-III squamous cell anal cancer: a comparative effectiveness systematic review. JNCI: J Natl Cancer Institute. (2025) 117:240–52. doi: 10.1093/jnci/djae195
18. Chakrabarti S, Jin Z, Huffman BM, Yadav S, Graham RP, Lam-Himlin DM, et al. Local excision for patients with stage I anal canal aquamous cell carcinoma can be curative. J Gastrointest Oncol. (2019) 10:171,178. doi: 10.21037/jgo.2018.12.12
19. Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. (2016) 66:271–89. doi: 10.3322/caac.21349
20. Renehan AG, Malcomson L, Emsley R, Gollins S, Maw A, Sun Myint A, et al. Watch-and-wait approach versus surgical resection after chemoradiotherapy for patients with rectal cancer (the OnCoRe project): a propensity-score matched cohort analysis. Lancet Oncol. (2016) 17:174–83. doi: 10.1016/S1470-2045(15)00467-2
21. Perez RO. Complete clinical response in rectal cancer: a turning tide. Lancet Oncol. (2016) 17:125–6. doi: 10.1016/S1470-2045(15)00487-8
22. Dhawan N, Afzal MZ, and Amin M. Immunotherapy in anal cancer. Curr Oncol. (2023) 30:4538–50. doi: 10.3390/curroncol30050343
23. Lonardi S, Prete AA, Morano F, Messina M, Formica V, Corsi DC, et al. Randomized phase II trial of avelumab alone or in combination with cetuximab for patients with previously treated, locally advanced, or metastatic squamous cell anal carcinoma: the CARACAS study. J ImmunoTherapy Cancer. (2021) 9:e002996. doi: 10.1136/jitc-2021-002996
24. Doran SL, Stevanovic S, Adhikary S, Gartner JJ, Jia L, Kwong MLM, et al. T-cell receptor gene therapy for human papillomavirus-associated epithelial cancers: A first-in-human, phase I/II study. J Clin Oncol. (2019) 37:2759–68. doi: 10.1200/JCO.18.02424
25. Yu WD, Jiang HY, Gao JM, Du JF, Chen G, and Zhang FL. Preliminary results on anal cancer by applying intensity modulated radiotherapy and synchronous capecitabine chemotherapy simultaneously. Transl Cancer Res. (2020) 9:4366–72. doi: 10.21037/tcr-19-2843
26. Koerber SA, Seither B, Slynko A, Haefner MF, Krug D, Liermann J, et al. Chemoradiation in female patients with anal cancer: Patient-reported outcome of acute and chronic side effects. Tumori. (2019) 105:174–80. doi: 10.1177/0300891618811273
27. Wegner RE, Abel S, Hasan S, White RJ, Raj M, Monga D, et al. Trends in radiation dose and technique for anal canal squamous cell carcinoma. Am J Clin Oncol. (2019) 42:519–26. doi: 10.1097/COC.0000000000000551
28. Aigner KR, Selak E, and Gailhofer S. Isolated thoracic perfusion with chemofiltration for progressive Malignant pleural mesothelioma. OncoTargets Ther. (2017) 10:3049–57. doi: 10.2147/OTT.S134126
29. Teicher BA and Lazo JS. and Sartorelli A: Classification of antineoplastic agents by their selective toxicities toward oxygenated and hypoxic tumor cells. Cancer Res. (1981) 41:73–81.
30. Aigner KR, Selak E, and Aigner K. Short-term intra-arterial infusion chemotherapy for head and neck cancer patients maintaining quality of life. J Cancer Res Clin Oncol. (2019) 145:261–8. doi: 10.1007/s00432-018-2784-4
31. Aigner KR, Selak E, and Aigner K. Approaching 10 years disease-free survival after isolated thoracic perfusion for advanced stage IV tonsil carcinoma: A case report. Int J Surg Case Rep. (2020) 75:71–4. doi: 10.1016/j.ijscr.2020.08.058
32. Aigner KR, Lavinski Y, and Gailhofer S. Tumor response and the quality of life after isolated hypoxic pelvic perfusion for advanced G3 cervical cancer: A case series. Int J Surg Case Rep. (2020) 77:816–21. doi: 10.1016/j.ijscr.2020.11.050
33. Aigner K, Selak E, Gailhofer S, Knösel T, SrinivasRaju J, and Aigner KR. Case report: Extended Isolated Stopflow Limb Infusion (EISLI) for highly Malignant osteosarcoma - complete pathological tumor remission and implantation of a knee joint prosthesis. Int J Surg Case Rep. (2023) 104:107918. doi: 10.1016/j.ijscr.2023.107918
Keywords: anal cancer, isolated perfusion, intra-arterial chemotherapy, electrochemotherapy, squamous cell carcinoma, toxic side effects, quality of life
Citation: Aigner KR, Aigner K, Hendrikx MJH, Bekrentchir A and Aust H (2025) Isolated hypoxic pelvic perfusion combined with electroporation is a valid alternative to traditional therapies for anal squamous cell carcinoma: a case study. Front. Oncol. 15:1644317. doi: 10.3389/fonc.2025.1644317
Received: 26 June 2025; Accepted: 04 August 2025;
Published: 27 August 2025.
Edited by:
Tamer Saad Kaoud, The University of Texas at Austin, United StatesReviewed by:
Giovanni Mastrandrea, National Cancer Institute (IRCCS), ItalyFrancesca De Terlizzi, IGEA, Italy
Copyright © 2025 Aigner, Aigner, Hendrikx, Bekrentchir and Aust. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Karl R. Aigner, aW5mb0Bwcm9mLWFpZ25lci5kZQ==