 Selina Becht1*
Selina Becht1* Najib Ben Khaled2,3,4
Najib Ben Khaled2,3,4 Simone Schrodi1
Simone Schrodi1 Michael von Bergwelt-Baildon1,3,4Peter Buggisch5,6Alexander Crispin7Wolf-Peter Hofmann6,8†Ursula Marschall9†
Michael von Bergwelt-Baildon1,3,4Peter Buggisch5,6Alexander Crispin7Wolf-Peter Hofmann6,8†Ursula Marschall9† Julia Mayerle2,3Bernhard Mörtl1Sami Orabi1†Alexander Philipp2,3†
Julia Mayerle2,3Bernhard Mörtl1Sami Orabi1†Alexander Philipp2,3† Jörg Trojan10Tobias Weiglein1
Jörg Trojan10Tobias Weiglein1 Enrico N. De Toni2,3,4Karin Berger-Thürmel1,3,4†
Enrico N. De Toni2,3,4Karin Berger-Thürmel1,3,4†- 1Department of Medicine III, University Hospital, Ludwig-Maximilians-University of Munich, Munich, Germany
- 2Department of Medicine II, University Hospital, Ludwig-Maximilians-University of Munich, Munich, Germany
- 3Bavarian Cancer Research Center (BZKF), Munich, Germany
- 4German Cancer Consortium (DKTK), Partner Site Munich, Munich, Germany
- 5ifi-Institute for Interdisciplinary Medicine, Hamburg, Germany
- 6Association of Gastroenterologists in Private Practice, Berufsverband Niedergelassener Gastroenterologen Deutschlands, Ulm, Germany
- 7Department for Medical Information Processing, Biometry, and Epidemiology, Ludwig-Maximilians University, Munich, Germany
- 8Gastroenterologie am Bayerischen Platz, Berlin, Germany
- 9BARMER, Wuppertal, Germany
- 10Medical Clinic I, University Hospital, Goethe University Frankfurt, Frankfurt, Germany
Background: Geographic and temporal variations in the incidence and treatment of chronic viral hepatitis and trends in the development of metabolic and behavioral risk factors result in heterogeneous incidences of hepatocellular carcinoma (HCC). Therefore, national epidemiological information should be evaluated to identify the need for action.
Methods: This retrospective observational study included adult patients with incident HCC (2016-2020). A network analysis was performed to investigate inter-relationships among risk factor diagnoses before HCC. Kaplan-Meier method and Cox proportional hazard model were used to analyze survival.
Findings: A total of 2,778 patients were included. Mean age was 71.9 years (SD ±9.7); 69% were male. Most frequently documented risk factor diagnoses were diabetes mellitus (76%), obesity (56%), liver fibrosis/cirrhosis (44%), and alcohol abuse (36%). Hepatitis B and C were documented in 4% and 11% of patients. Behavioral and metabolic risk factors were 1.1-1.9-fold more frequent in men. Diabetes mellitus was the most central risk factor diagnosis co-occurring with other metabolic and behavioral risk factors. Median survival was 8.7 months.
Interpretation: In this German cohort, risk factor diagnoses before HCC were multifactorial, with metabolic diseases most frequently co-occurring. Survival after HCC was poor. Controlling metabolic risk factors and surveilling at-risk populations are crucial to mitigating the incidence and improving the survival of HCC patients in Germany. Analyzing claims data enabled efficient and effective generation of epidemiological real-world evidence.
1 Introduction
Primary liver cancer is a highly aggressive and lethal tumor and the third common cause of cancer-related deaths worldwide, following lung and colorectal cancer (1). Hepatocellular carcinoma (HCC) comprises the majority of primary liver cancer cases (2). Most patients with HCC in Europe are diagnosed at an intermediate or advanced stage of disease, when curative treatments are no longer applicable (3). In Germany, HCC is considered a rare type of cancer, with approximately 6000 new cases reported by the German cancer registration in 2020 (4). The relative five-year and ten-year survival rates after the diagnosis of HCC in Germany are 17% and 13%, respectively (5).
HCC commonly develops as a result of a chronic liver disease such as cirrhosis. Chronic viral hepatitis is so far the primary cause of chronic liver disease and subsequent HCC (6). However, other risk factors, including chronic alcohol consumption, obesity, and metabolic diseases, also increase the likelihood of HCC (6–8). In recent years, the proportion of HCC patients without viral hepatitis has increased, and the etiologies of HCC have shifted from viral to non-viral (6–8). Particularly in developed countries, such as those in Europe and North America, successful interventions against hepatitis B virus (HBV) and hepatitis C virus (HCV) infections have been implemented (9, 10), whereas the prevalence rates of alcohol-related risk factors and metabolic diseases, such as metabolic dysfunction-associated steatotic liver disease (MASLD) and diabetes mellitus, are rapidly increasing (11). In a French cohort, the prevalence of MASLD-related HCC rose from 3% to 20% between 1995 and 2014, and the proportion of HCC caused by HCV decreased from 43% to 20% (12). Because of significant geographical and temporal variations in the prevalence of risk factors and differences in healthcare systems, the causes underlying HCC vary globally (6, 13). Regional differences have been observed in Europe as well. In socioeconomically disadvantaged regions, a higher burden of behavioral risk factors, restricted access to HBV vaccination and HCV treatment, and a subsequently higher incidence of HCC have been observed (14).
Because of the aforementioned geographical and temporal variations in the epidemiology of HCC, epidemiological knowledge of HCC among national cohorts is imperative to identify relevant risk factors and enhance targeted prevention and surveillance measures to reduce the incidence and healthcare burden of HCC. Currently, there is no contemporary real-world evidence of risk factors and survival of patients with HCC in Germany. This study aims to describe patient characteristics, the occurrence of previous risk factor diagnoses, and survival of a large population of patients with HCC in Germany based on health insurance claims data.
2 Methods
2.1 Study design and data sources
This retrospective cohort study was based on health insurance claims data from BARMER (Berlin, Germany), which is the second largest health insurance company in Germany, providing insurance coverage for approximately 8.7 million citizens in 2022. For each insured individual, the database contains anonymized longitudinal information regarding demographics (e.g., age, sex, place of residence, and date of death), outpatient care, inpatient care, drug prescriptions, therapeutic devices, and sick leave. The inpatient setting covers all hospital admissions, whereas the outpatient setting comprises ambulatory healthcare services provided by office-based physicians and hospital outpatient clinics. Health insurance claims data are primarily obtained for billing and reimbursement purposes. All diagnoses relevant to the patients’ treatment are routinely reported by physicians, hospitals, pharmacies, and other healthcare providers to the respective health insurance company. Diagnoses provided in health insurance claims data are coded according to the German Modification of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10-GM).
Data analyses and presentations followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (15). Since only anonymized data from the BARMER was used, no ethics approval or consent to participate was needed. This is in accordance with national (General Data Protection Regulation) and European (§ 78 SGB) regulations, as well as German guidelines for Good Practice of Secondary Data Analysis by Swart et al. (2015) (16).
2.2 Patient identification
Patients with incident HCC were identified according to ICD-10-GM code C22.0 between 1 January 2016 and 31 December 2020. Patients aged ≥18 years with either one primary diagnosis of HCC in an inpatient setting or two confirmed diagnoses of HCC in an office-based or outpatient hospital setting during consecutive quarters were included. Patients with previously confirmed cancer diagnoses other than carcinoma in situ or non-melanoma skin cancer within 5 years prior to the HCC diagnosis were excluded because these diseases can influence the prognosis and treatment options for patients with HCC. Furthermore, these criteria distinguished incident HCC cases from prevalent or recurrent HCC cases and excluded uncertain diagnoses and liver metastases from other cancers documented as HCC. Individuals without BARMER insurance coverage for at least 10 years before and 2 years after the date of the HCC diagnosis (or unless death occurred before the diagnosis) and those insured by Deutsche BKK, a health insurance that integrated into BARMER in 2017, were excluded to ensure sufficient insurance records during the observation period. The index date of the first HCC diagnosis was defined as the date of the earliest inpatient or outpatient visit with a recorded diagnosis of HCC.
2.3 Study variables
2.3.1 Comorbidities
Comorbidities were determined using the Charlson Comorbidity Index (CCI). The algorithm of Quan et al. (2011) and the respective ICD-10-GM codes were used to identify relevant diagnoses and calculate the CCI (17). Categories including diagnoses of malignant neoplasms were not considered in the calculation of the CCI because they could be related to or result from the index disease HCC. Comorbidities at the time of the HCC diagnosis were identified by either one documented primary or secondary diagnosis in an inpatient setting or two confirmed diagnoses in an outpatient setting during two consecutive quarters 12 months before or 3 months after the HCC diagnosis. The calculated CCI was divided into four categories (0, 1-3, 4-6, and ≥7) to describe the burden of the comorbidity and assess its impact on survival.
2.3.2 Risk factors
Risk factor diagnoses prior to the HCC diagnosis were identified by retrieving either one primary or secondary diagnosis in an inpatient setting or two confirmed diagnoses in an outpatient setting during consecutive quarters within ten years before the index date. The following diagnoses were considered when assessing the occurrences of risk factors before the HCC diagnosis in this cohort: obesity, diabetes mellitus, alcohol abuse, alcohol-related liver disease, MASLD, fibrosis/cirrhosis, chronic viral hepatitis, other hepatitis, iron metabolism disorders, plasma protein metabolism disorders, unspecified inflammatory liver disease, toxic liver disease, and hepatic failure. ICD-10-GM codes were used to identify risk factor diagnoses in the health insurance claims data. MASLD, according to the new nomenclature for steatotic liver disease (18), is not yet available in the ICD-10-GM system. Hence, the diagnosis was defined based on a combination of several ICD-10-GM codes (see Supplementary Table 1 for the respective codes).
2.4 Statistical analysis
Characteristics of patients were determined using descriptive statistics such as absolute numbers and percentages for categorical variables and mean with standard deviation for the continuous variable patient’s age. Based on a co-occurrence matrix, a network analysis was performed to investigate the inter-relationships among documented risk factor diagnoses. Each diagnosis was represented by a node in the network. Weights were calculated to visualize nodes dependent on the frequency of diagnoses and the edges between nodes dependent on the frequency of the co-occurrence of diagnoses (19). Overall survival was calculated from the index date of the HCC diagnosis to the date of death from any cause. Patients with no documented date of death were censored on 31 December 2022. The observed overall survival was estimated using the Kaplan–Meier method. The effects of age, sex, CCI, and HCC-associated risk factor diagnoses on survival were assessed using multivariate Cox proportional regression analysis. The forward sequential method was used as the variable selection method for the Cox regression model (20). Hazard ratios (HRs) and 95% confidence intervals (95% CIs) were presented.
A significance level of α=0.05 was prespecified for all statistical tests. Data processing and statistical analyses were conducted using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA) and R software (version 4.2.1; R Foundation, Vienna, Austria).
3 Results
3.1 Patient cohort
A progressive approach was used to identify eligible patients with an incident HCC diagnosis (Figure 1). Between 1 January 2016 and 31 December 2020, 4,574 patients with an incident HCC diagnosis were identified. After applying the inclusion and exclusion criteria, 2,778 patients were included in the subsequent analyses.
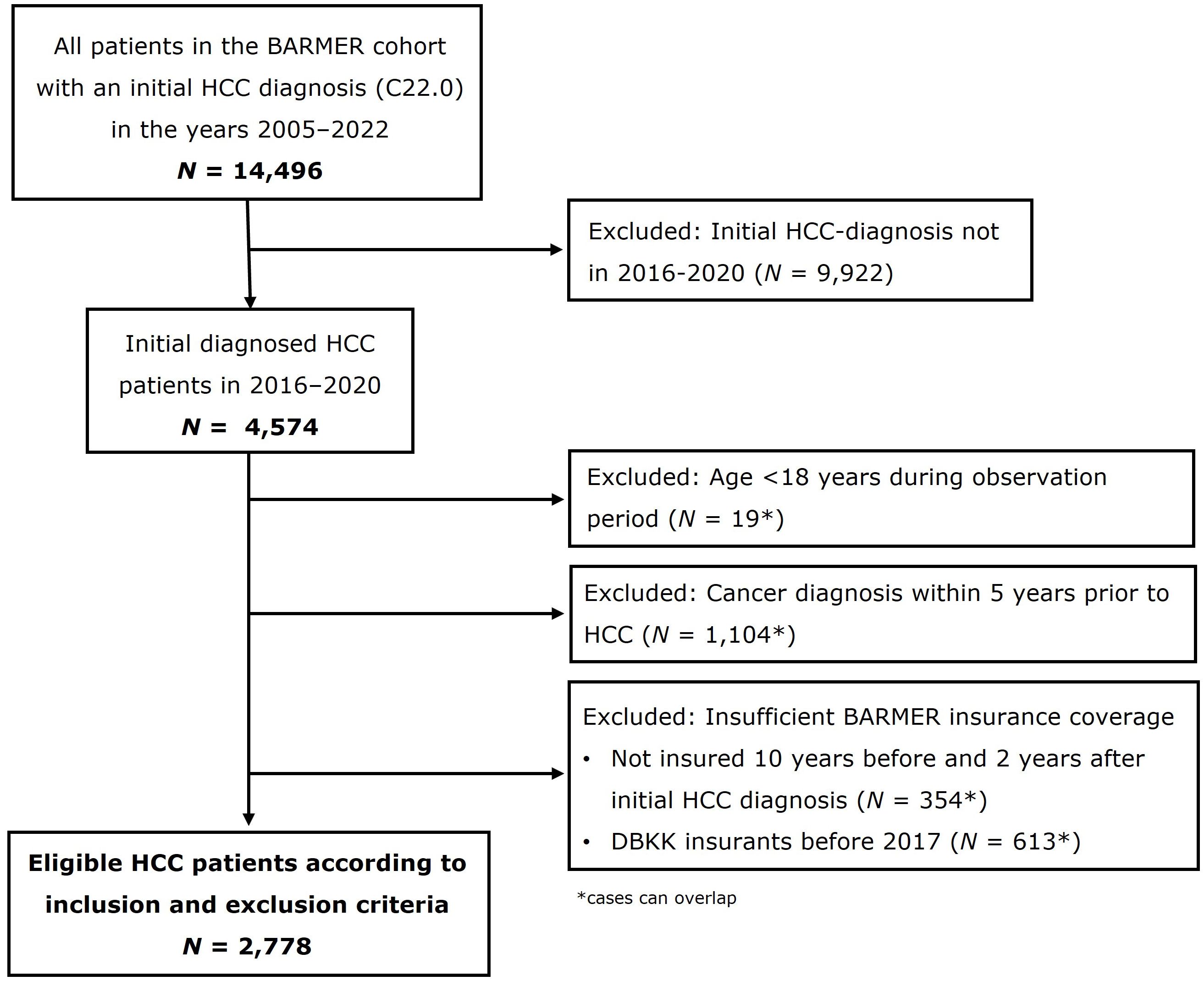
Figure 1. Study flowchart of patient identification. Similiar figure is already published in: Schrodi et al. (21).
3.2 Patient characteristics
Most patients (69.4%) in the cohort were male. The mean age of patients at the time of the HCC diagnosis was 71.9 years (standard deviation, ± 9.7; range, 30–97 years). Regarding comorbidities, the majority of the cohort (62.0%) had a CCI ≥4 at the time of the HCC diagnosis. No comorbidity burden was recorded for 6.5% of the patients (Table 1). Mild liver disease (40.3%) and moderate/severe liver disease (37.5%) were the most frequently documented comorbid conditions, followed by renal disease (34.4%), diabetes mellitus with chronic complications (33.4%), and congestive heart failure (30.7%) (Supplementary Table 2).
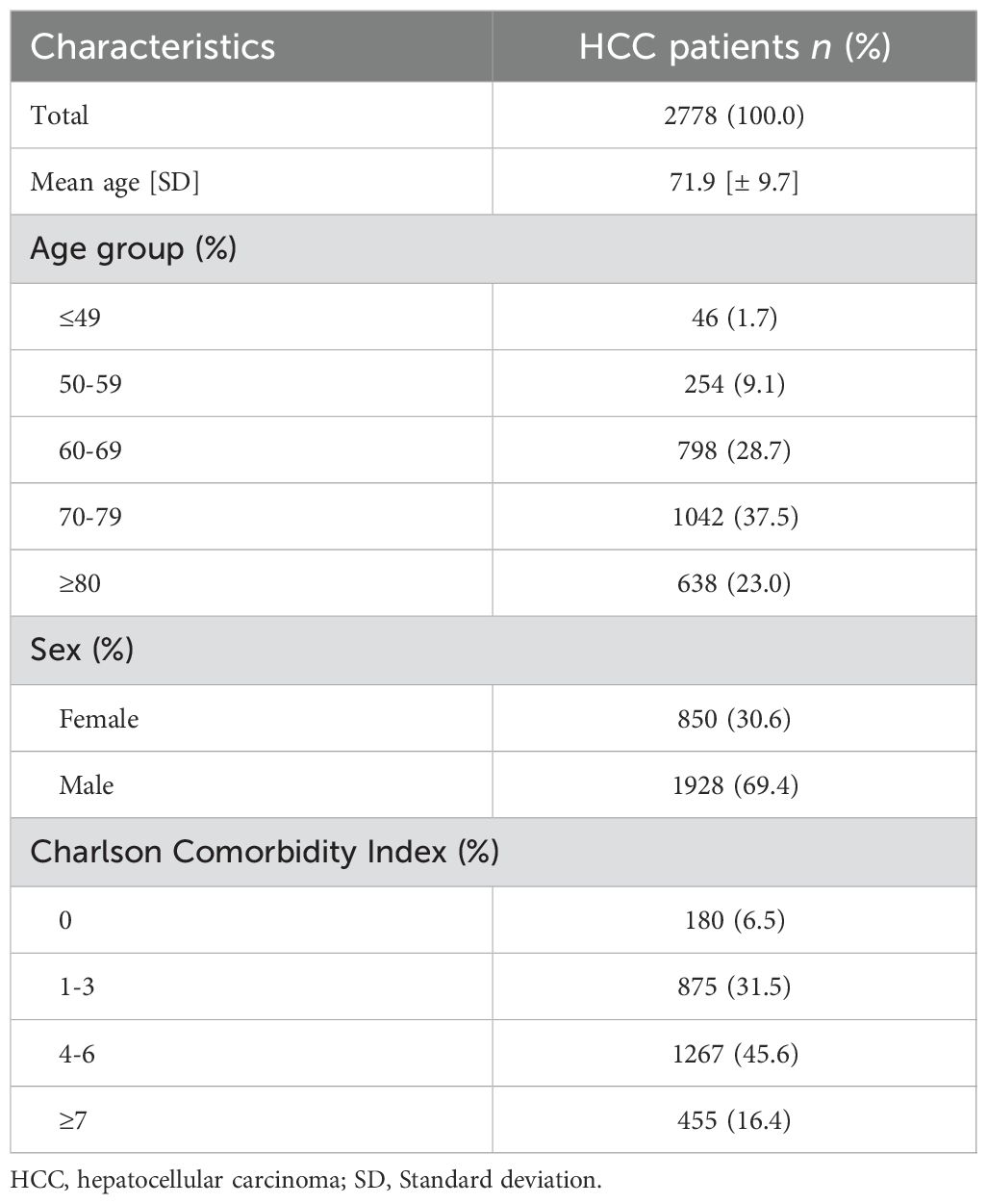
Table 1. Baseline characteristics of HCC patients at the time of initial diagnosis over the period 2016-2020 (N = 2,778).
3.3 Distribution of risk factor diagnoses and network analysis
The proportions of risk factor diagnoses within 10 years before the HCC diagnosis are shown in Table 2. The five most frequently documented diagnoses were diabetes mellitus (76.3%), obesity (55.5%), liver fibrosis/cirrhosis (43.8%), alcohol abuse (36.3%), and MASLD (30.8%). HBV and HCV were documented for 4.3% and 10.9% of the patients, respectively. Significant differences in the risk factor diagnoses were observed between men and women (Figure 2). The odds of behavioral and metabolic risk factors of male patients were 1.1- to 1.9-fold higher than those of female patients with HCC. As shown in Figure 3, the network of diseases documented within 10 years preceding the HCC diagnosis revealed the multifactorial nature of the disease. The network comprised 13 nodes representing each determined diagnosis and 13,506 edges representing the co-occurrence of two risk factor diagnoses. The most central node in the network was diabetes mellitus, which most frequently co-occurred with obesity, followed by liver fibrosis/cirrhosis, alcohol abuse, alcohol-related liver disease, and MASLD.
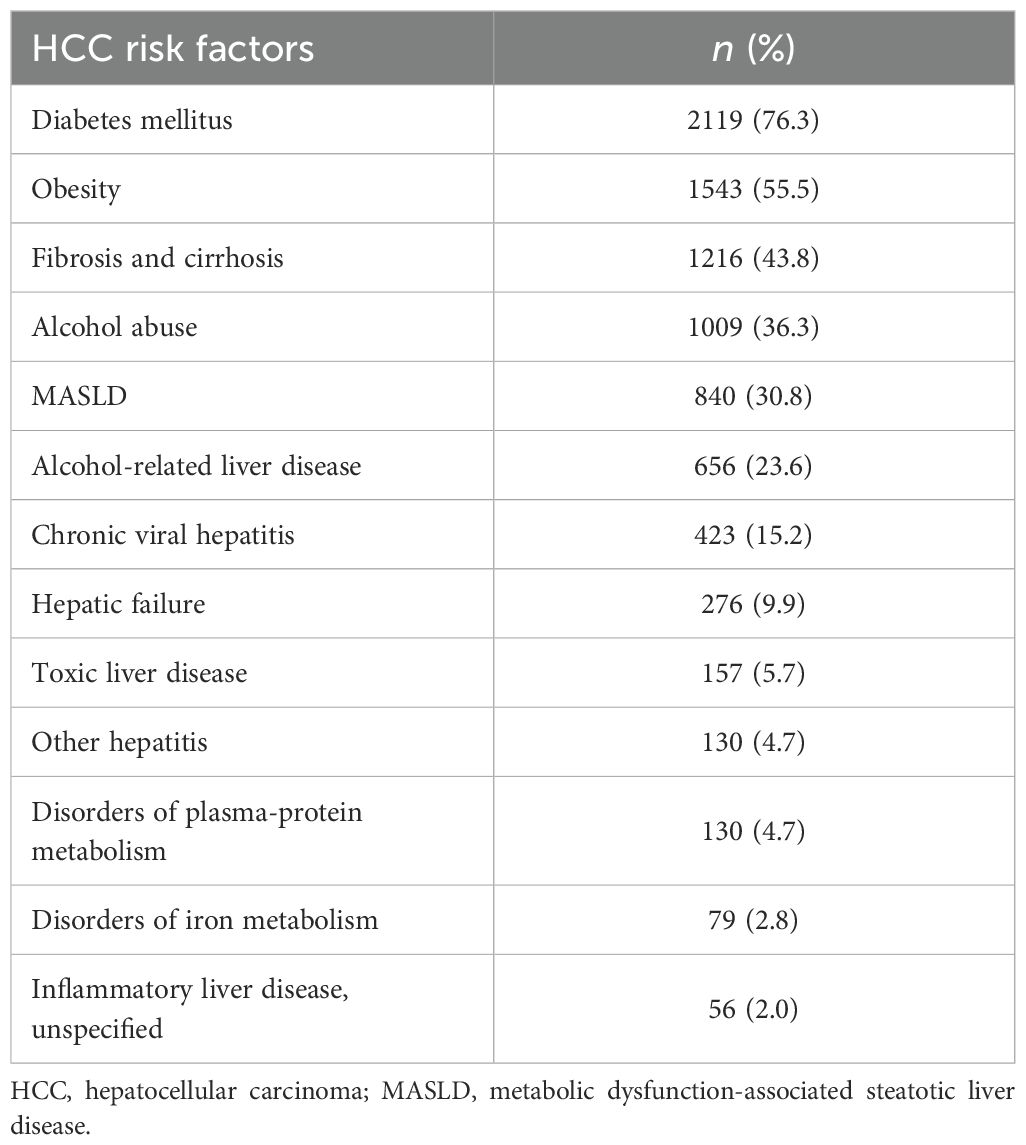
Table 2. HCC risk factors recorded within 10 years prior HCC diagnosis – several possible risk factors in the same patient (N = 2,778).
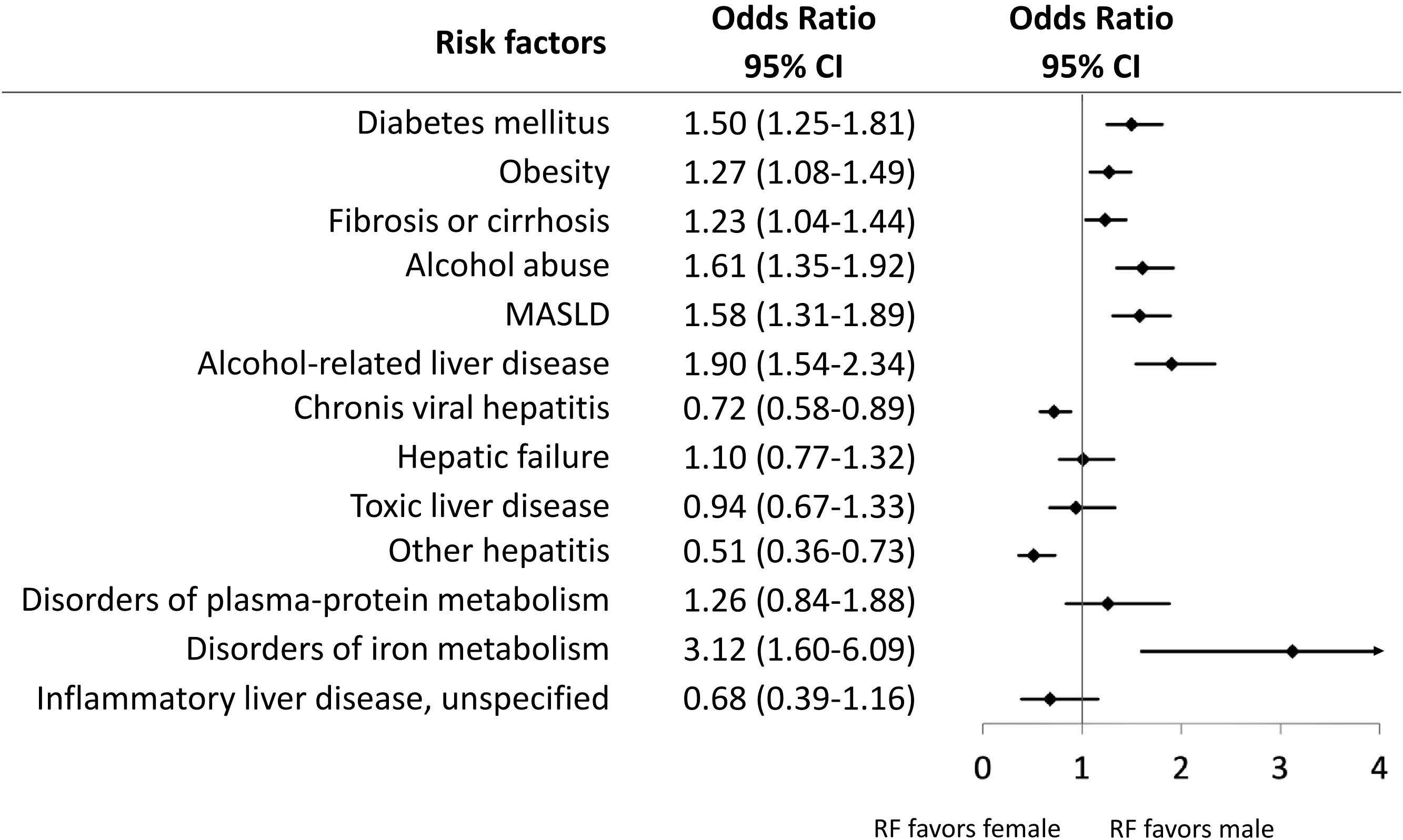
Figure 2. Forest plots of the female to male odds ratios (OR) and 95% confidence intervals (CI) for HCC risk factors (RF).

Figure 3. Network showing associations between different risk factors in patients with HCC diagnosis. Size of nodes is based on the prevalence of the risk factor in the HCC cohort, and the thickness of lines is based on the number of simultaneous occurrences of the risk factors.
3.4 Survival
The median overall survival after the HCC diagnosis was 8.7 months (95% CI, 7.7-9.7 months). After 1 year and 5 years, the estimated survival rates were 44% and 16%, respectively (Figure 4).
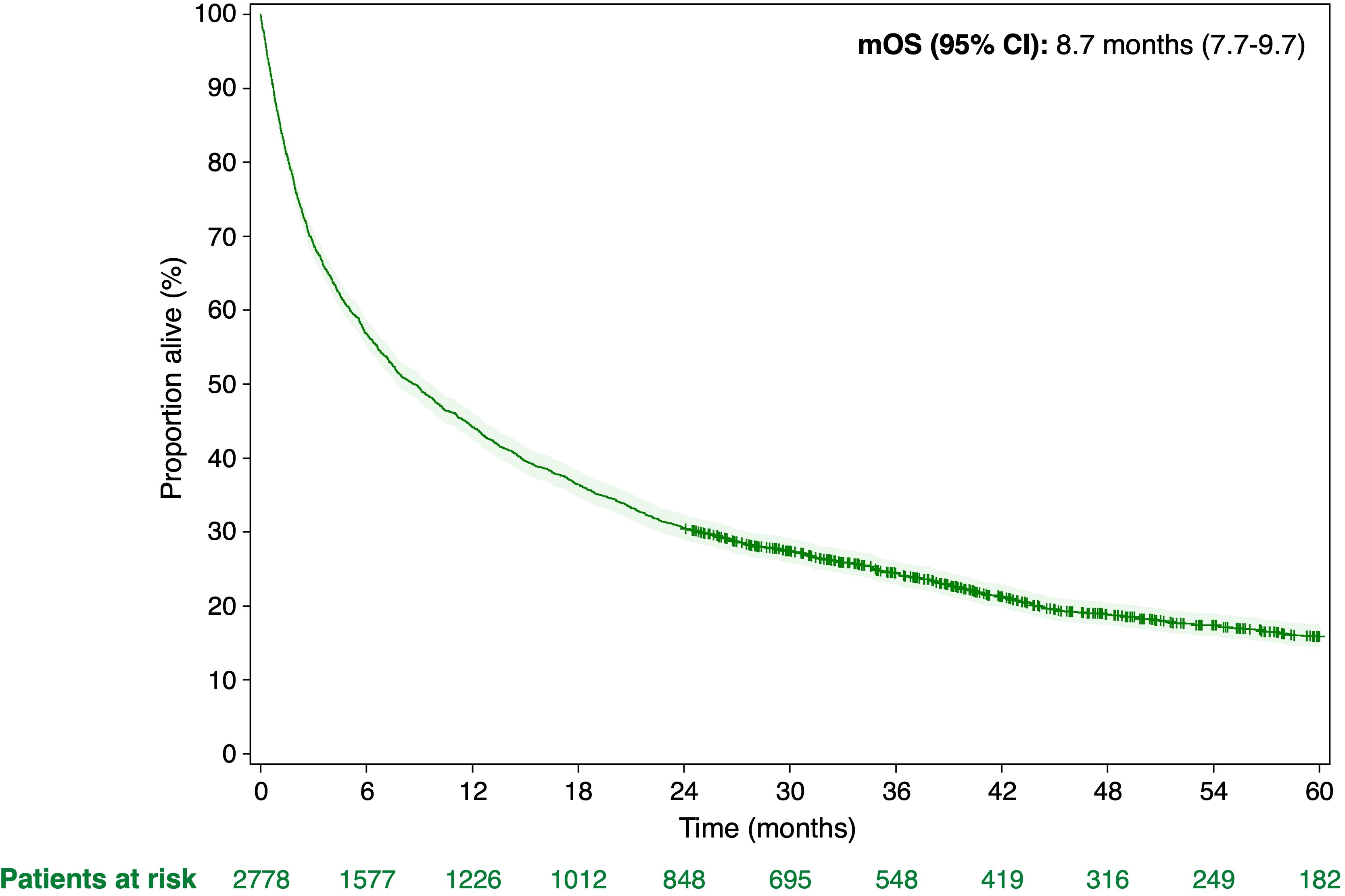
Figure 4. Analysis of overall survival (OS) according to the Kaplan-Meier method in patients with HCC.
The multivariate Cox regression analysis revealed that age, CCI, chronic viral hepatitis, MASLD, and alcohol abuse were independent predictors of patients’ survival (Table 3). The median survival time following HCC diagnosis ranged from 52.2 months in patients younger than 50 years to 5.6 months in those aged 80 years and older (HR, 3.25; 95% CI, 2.13-4.94; p<0.0001). A higher CCI was associated with reduced survival time Patients with no or a low burden of comorbidities had prolonged survival (p<0.0001). Regarding risk factor diagnosis, patients with documented alcohol abuse had reduced survival compared to patients without alcohol abuse prior to the HCC diagnosis (HR, 1.15; 95% CI, 1.05-1.25; p=0.0021). Patients diagnosed with chronic viral hepatitis (HR, 0.81; 95% CI, 0.72-0.91; p=0.0005) or MASLD (HR, 0.85; 95% CI, 0.77-0.93; p=0.0004) had prolonged survival. The other investigated risk factors were not identified as independent predictors of survival.
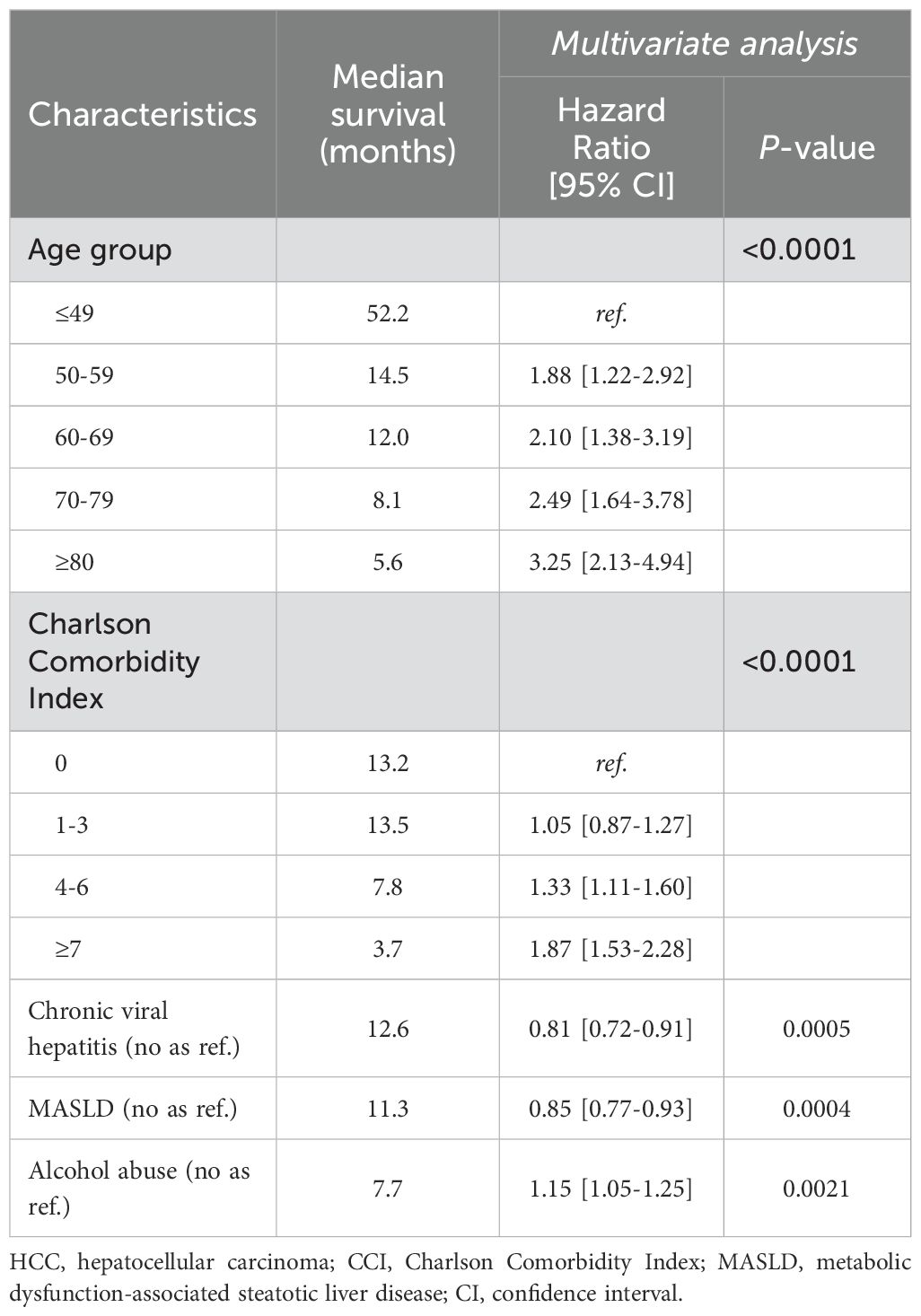
Table 3. Stratified median survival and multivariate Cox proportional regression analysis of the survival after HCC diagnosis (N = 2,778).
4 Discussion
This retrospective observational study provides contemporary insights regarding risk factor diagnoses and survival of 2,778 patients with HCC based on claims data from a large German health insurance company. To the best of our knowledge, this is the first extensive epidemiological analysis of patients with HCC in Germany. Chronic HBV or HCV was documented for 15% of the included patients before the HCC diagnosis. Metabolic diseases and behavioral risk factor diagnoses affected the majority of patients. The network analysis highlighted the relevance and inter-relationships of these non-viral risk diseases of patients with HCC. Survival was highly dependent on age and CCI at the time of diagnosis. Younger patients and those with a low comorbidity burden had significantly prolonged survival.
4.1 Distributions of age and sex
The mean age of patients in this study cohort was 71.9 years. Patients between 70 and 79 years comprised the highest proportion of the cohort (38%). The age distribution was comparable to that of other German HCC cohorts based on population-level cancer registry data (mean age, 68.5 years) (22) and health insurance claims data (mean age, 68.9-71.9 years) (23, 24). In Germany, the proportion of inhabitants between 70 and 79 years of age is projected to increase from 9% to 13% between 2023 and 2040 (25). Considering the predicted demographic changes, a substantial increase in the number of patients with HCC is expected.
Approximately one-third of patients with incident HCC were female. However, previous epidemiological studies have demonstrated that the incidence of HCC for men is up to five-fold higher than that for women (2). This deviation may be explained by the structure of the BARMER, which includes proportionally more women compared to the general population in Germany.
4.2 Prevalence of risk factor diagnoses prior to the HCC diagnosis
In this German cohort, only 15% of the patients were affected by chronic viral hepatitis, whereas metabolic diseases were the most frequently documented diseases prior to HCC. The network analysis identified the multifactorial nature of risk factor diagnoses prior to HCC and highlighted the less prominent role of viral infections compared to metabolic diseases. These findings are consistent with previously published population-based studies in Europe (14, 26) and the United States (27). The observed inferior role of chronic viral hepatitis in patients with HCC aligned with the recently reported shift from viral to non-viral HCC (6, 13), presumably because of successful interventions against HBV and HCV and an increasing prevalence of metabolic risk factors. A retrospective analysis in France found that HCC cases caused by MASLD increased from 3% to 20% between 1995 and 2014. Simultaneously, the proportion of patients with HCC and HCV declined from 43% to 20% (12).
The odds of having behavioral and metabolic risk factors were higher for male patients than for female patients. Similar sex disparities in the epidemiological distribution of risk factors for HCC have been previously reported (28). Because of the lower proportion of male patients, as expected in population-based HCC cohorts, behavioral and metabolic risk factor diagnoses in our total cohort may have been underestimated.
In the Netherlands, approximately 20% of HCC cases develop in non-cirrhotic livers, predominantly in patients with MASLD (29). A similar proportion of patients with non-cirrhotic livers were identified in a large single-center HCC cohort in Germany (30). Contrary to these findings, liver fibrosis or cirrhosis was documented before the HCC diagnosis for only 43% of patients in our study. This comparatively low number could be attributable to the potential underestimation of affected patients with liver fibrosis or cirrhosis never seek clinical care and, therefore, remain undiagnosed (31). Because health insurance claims data are used for reimbursement purposes, diseases that were not diagnosed by a physician were not documented in the data source.
4.3 Survival and risk factors
In this claims data study, the observed median survival after the HCC diagnosis for all patients was 8.7 months. Previous studies in Germany using population-based cancer registry data have found slightly better survival for patients with HCC (median, 1 year) (5, 22). As expected, the median observed survival in the current study decreased significantly with increasing age decade and comorbidity index.
Additional independent predictors for the survival of patients with HCC that were identified were chronic viral hepatitis, MASLD, and alcohol abuse. Consistent with a previous retrospective study based on the SEER-Medicare database (32) and a prospective study in France (33), we found that alcohol abuse leads to poorer prognoses for patients with HCC, whereas chronic viral hepatitis is associated with prolonged survival after the diagnosis of HCC. More than half of patients with alcohol-related HCC (55%) have been diagnosed at an advanced stage of disease, whereas patients with chronic viral hepatitis are often diagnosed at an early tumor stage (30). Late-stage diagnoses and poor survival of patients with alcohol-related HCC could be explained by a lack of screening measures (34) and reduced likelihood of receiving curative treatment (35) compared to individuals with other HCC etiologies. We also found patients diagnosed with MASLD prior to HCC diagnosis had prolonged survival as compared to patients not diagnosed with one of these risk factors. Carrying a diagnosis such as viral hepatitis or MASLD may lead to being more likely to be diagnosed with HCC in earlier stages because they may be more likely to seek clinical care and receive surveillance measures (36).
Although treatment modalities were not considered in the present analysis, therapy also has a major impact on survival. In a recently published study based on the same patient cohort, we showed that patients who received curative therapy had a markedly better median survival (40.4 months) compared to those receiving non-curative treatment (9.7 months) (21).
4.4 The value of analyzing claims data
Almost 2,800 patients with HCC were identified for the analyses even though this type of cancer is rare in Germany (4), thus highlighting the notable advantage of analyzing health insurance claims data. This source of data comprises complete data coverage of different sectors of healthcare in Germany, including inpatient and outpatient diagnostics and treatments, resource consumption, costs, and survival by all patients in real-life conditions, independent of a predefined study purpose.
Population-based studies have revealed the varying prevalence of risk factors and subsequent HCC incidence between countries and regions. Recently, the shift from viral to non-viral causes of HCC has been observed in Europe (6, 13). A meta-analysis by Riazi et al. (2022) observed a globally increasing prevalence of MASLD in recent decades, reaching a prevalence of 37.8% in the years 2016–2019 (37). Given the rising number of patients affected by metabolic diseases such as diabetes mellitus and MASLD, particularly in countries with a high socio-demographic, the number of HCC cases caused by metabolic diseases is expected to increase further (11). Furthermore, patients with metabolic diseases are from a generation comprising individuals with mostly normal weights during childhood. Currently, approximately one of every five adolescents (21%) in Europe is overweight or obese, resulting in an increased incidence of metabolic disease burden during adulthood (38). Regarding chronic viral hepatitis, a burden of HBV and HCV infections was still reported, although Germany being considered to be a low-prevalence country (39). The HBV vaccination has been administered to between only 66% and 91% of all children in Germany; however, the goal of the World Health Organization is 95% (40). A significant proportion of patients with HCV still need to be reached by treatment programs (41). Furthermore, the large-scale movement of individuals from high-prevalence nations to European countries highlights the importance of testing risk groups, treating chronic viral hepatitis, and performing surveillance measures, which are crucial to preventing the development of late stage HCC caused by viral infections (42). Health insurance claims data provide access to contemporary data at the national level and enable analyses of the current epidemiology and regional and temporal trends.
4.5 Limitations
Despite the strengths and value described, this study had some limitations, which were mainly related to the nature of claims data from German health insurances. The database consisted of data from one health insurance company that provided coverage for approximately 10% of the German population. Hence, the generalizability of the study results to other populations of patients with HCC in Germany may be limited. Because of the billing and reimbursement purposes of German statutory health insurance data, recorded diagnoses are dependent on the coding quality and relevance of the reimbursement of healthcare costs, thus leading to potential bias or, from a clinical perspective, incomplete documentation. This may lead to underrepresentation or overrepresentation of the determined comorbidities or risk factors. However, the risk of overestimating diagnoses was minimized through our approach for identifying HCC cases, risk factors, and comorbidities. Furthermore, health insurance data do not capture information regarding tumor stage, histology, Eastern Cooperative Oncology Group performance status, or laboratory results for considering the liver function using the Child-Pugh score. This lack of detailed clinical information limited the ability to control relevant characteristics, such as tumor stage, that might affect the survival of patients with HCC.
4.6 Conclusion
In conclusion, the results of our analysis based on data from a large comprehensive German claims database revealed the relevance of the multifactorial nature of risk factors in patients with HCC. Most patients were affected by metabolic diseases, whereas only a few were affected by chronic viral hepatitis infections prior to the diagnosis of HCC. Awareness among healthcare professionals, at-risk groups, policymakers, and the general population regarding the relevance of controlling behavioral risk factors and subsequent metabolic diseases is crucial to mitigating the incidence and burden of HCC. This study demonstrated the potential of claims data sources to allow rapid collection of longitudinal data of large populations to answer pivotal clinical and political questions during healthcare research. The methodological approach used during this study can serve as a template for closing epidemiological information gaps using health insurance claims data. Based on our work, subsequent research should aim to identify trends in risk factor incidences and evaluate their long-term impact on HCC incidence and mortality. Therefore, studies linking health insurance claims data with German cancer registry data are needed to enable robust survival analyses by incorporating information on tumor stage and performance status. Furthermore, including complementary information regarding diagnostics, treatment patterns, and costs in future analyses is essential to provide a comprehensive view of prevention and surveillance measures, outcomes, and health economic consequences of HCC.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The anonymized data underlying this study belong to BARMER health insurance. The data are not publicly available due to protection of data privacy of the insured individuals by the BARMER. Requests to access these datasets should be directed to UM, dXJzdWxhLm1hcnNjaGFsbEBiYXJtZXIuZGU=.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
SB: Methodology, Writing – review & editing, Investigation, Writing – original draft, Visualization, Data curation, Formal analysis, Project administration, Conceptualization, Validation. NB: Conceptualization, Writing – review & editing, Methodology. SS: Formal analysis, Validation, Conceptualization, Writing – review & editing. MB-B: Writing – review & editing, Conceptualization. PB: Conceptualization, Writing – review & editing. AC: Conceptualization, Writing – review & editing. W-PH: Writing – review & editing, Conceptualization. UM: Resources, Writing – review & editing, Conceptualization. JM: Writing – review & editing, Conceptualization. BM: Conceptualization, Writing – review & editing. SO: Conceptualization, Writing – review & editing, Visualization, Formal analysis. AP: Writing – review & editing, Conceptualization. JT: Writing – review & editing, Conceptualization. TW: Conceptualization, Writing – review & editing. ET: Writing – review & editing, Conceptualization, Methodology. KB-T: Funding acquisition, Conceptualization, Writing – review & editing, Project administration, Supervision, Writing – original draft, Methodology, Visualization, Formal analysis.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This study was partly funded by a research grant from Roche Pharma AG. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of interest
Author UM was employed by BARMER. BM reports employment at Daiichi Sankyo. ET reports consultations for AstraZeneca, Bayer, BMS, EISAI, Eli Lilly & Co, MSD, Mallinckrodt, Omega, Pfizer, IPSEN, Terumo, and Roche and employment at Boehringer-Ingelheim. He reports reimbursement of meeting attendance fees and travel expenses from Arqule, Astrazeneca, BMS, Bayer, Celsion and Roche, and lecture honoraria from BMS and Falk. He has received third-party funding for scientific research from Arqule, AstraZeneca, BMS, Bayer, Eli Lilly, and IPSEN and Roche. KB-T has received a research grant from Roche. NB has received reimbursement of meeting attendance fees and travel expenses from EISAI and lecture honorarium from Falk and Astra Zeneca. W-PH has served as a paid consultant for IPSEN, Falk Pharma, Novo Nordisc, Norgine, Abbvie, Gilead and Roche. He has received reimbursement of meeting attendance fees and travel expenses from Abbvie and Gilead, and lecture honoraria from Abbvie, Gilead, Falk Pharma, and Advanz Pharma.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1650982/full#supplementary-material
References
1. Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834
2. Rumgay H, Ferlay J, de Martel C, Georges D, Ibrahim AS, Zheng R, et al. Global, regional and national burden of primary liver cancer by subtype. Eur J Cancer. (2022) 161:108–18. doi: 10.1016/j.ejca.2021.11.023
3. Park J-W, Chen M, Colombo M, Roberts LR, Schwartz M, Chen PJ, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. (2015) 35:2155–66. doi: 10.1111/liv.12818
4. Zentrum für Krebsregisterdaten. Gesellschaft für epidemiologische Krebregister in Deutschland e.V. Krebs in Deutschland für 2017/2018. Berlin: Robert Koch-Institut (2023).
5. Schönfeld I and Kraywinkel K. Epidemiologie des hepatozellulären Karzinoms in Deutschland. Onkologe. (2018) 24:653–58. doi: 10.1007/s00761-018-0438-4
6. Huang DQ, Singal AG, Kono Y, Tan DJH, El-Serag HB, and Loomba R. Changing global epidemiology of liver cancer from 2010 to 2019: NASH is the fastest growing cause of liver cancer. Cell Metab. (2022) 34:969–977.e2. doi: 10.1016/j.cmet.2022.05.003
7. Testino G, Leone S, and Borro P. Alcohol and hepatocellular carcinoma: a review and a point of view. World J Gastroenterol. (2014) 20:15943–54. doi: 10.3748/wjg.v20.i43.15943
8. Agosti P, Sabbà C, and Mazzocca A. Emerging metabolic risk factors in hepatocellular carcinoma and their influence on the liver microenvironment. Biochim Biophys Acta Mol Basis Dis. (2018) 1864:607–17. doi: 10.1016/j.bbadis.2017.11.026
9. GBD 2019 Hepatitis B Collaborators. Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Gastroenterol Hepatol. (2022) 7:796–829. doi: 10.1016/S2468-1253(22)00124-8
10. Di Marco L, La Mantia C, and Di Marco V. Hepatitis C: standard of treatment and what to do for global elimination. Viruses. (2022) 14:505. doi: 10.3390/v14030505
11. Chew NWS, Ng CH, Tan DJH, Kong G, Lin C, Chin YH, et al. The global burden of metabolic disease: Data from 2000 to 2019. Cell Metab. (2023) 35:414–428.e3. doi: 10.1016/j.cmet.2023.02.003
12. Pais R, Fartoux L, Goumard C, Scatton O, Wendum D, Rosmorduc O, et al. Temporal trends, clinical patterns and outcomes of NAFLD-related HCC in patients undergoing liver resection over a 20-year period. Aliment Pharmacol Ther. (2017) 46:856–63. doi: 10.1111/apt.14261
13. Toh MR, Wong EYT, Wong SH, Ng AWT, Loo LH, Chow PK, et al. Global epidemiology and genetics of hepatocellular carcinoma. Gastroenterology. (2023) 164:766–82. doi: 10.1053/j.gastro.2023.01.033
14. Kondili LA, Lazarus JV, Jepsen P, Murray F, Schattenberg JM, Korenjak M, et al. Inequities in primary liver cancer in Europe: The state of play. J Hepatol. (2024) 80:645–60. doi: 10.1016/j.jhep.2023.12.031
15. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, and Vandenbroucke JP. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. (2007) 335:806–08. doi: 10.1136/bmj.39335.541782.AD
16. Swart E, Gothe H, Geyer S, Jaunzeme J, Maier B, Grobe TG, et al. Gute praxis sekundäranalyse (GPS): leitlinien und empfehlungen. Gesundheitswesen. (2015) 77:120–6. doi: 10.1055/s-0034-1396815
17. Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. (2011) 173:676–82. doi: 10.1093/aje/kwq433
18. Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. (2023) 78:1966–86. doi: 10.1097/HEP.0000000000000520
19. Schweinberger M. Network Analysis using R . Available online at: https://ladal.edu.au/net.html (Accessed April 30, 2024).
20. Hong HG, Zheng Q, and Li Y. Forward regression for Cox models with high-dimensional covariates. J Multivar Anal. (2019) 173:268–90. doi: 10.1016/j.jmva.2019.02.011
21. Schrodi S, Berger-Thürmel K, Becht S, von Bergwelt-Baildon M, Buggisch P, Hofmann WP, et al. Treatment gaps and survival outcomes of hepatocellular carcinoma: insights from a nationwide, claims-based study. Ther Adv Med Oncol. (2025) 17:17588359251363202. doi: 10.1177/17588359251363202
22. De Toni EN, Schlesinger-Raab A, Fuchs M, Schepp W, Ehmer U, Geisler F, et al. Age independent survival benefit for patients with hepatocellular carcinoma (HCC) without metastases at diagnosis: a population-based study. Gut. (2020) 69:168–76. doi: 10.1136/gutjnl-2018-318193
23. Ben Khaled N, Mörtl B, Beier D, Reiter FP, Pawlowska-Phelan D, Teufel A, et al. Changing treatment landscape associated with improved survival in advanced hepatocellular carcinoma: a nationwide, population-based study. Eur J Cancer. (2023) 192:113248. doi: 10.1016/j.ejca.2023.113248
24. Decker JA, Scheurig-Muenkler C, Luitjens JH, and Kroencke T. Nationwide trends and the influence of age and gender in the in-patient care of patients with hepatocellular carcinoma in Germany between 2010 and 2020. Cancers (Basel). (2023) 15:2792. doi: 10.3390/cancers15102792
26. Garuti F, Neri A, Avanzato F, Gramenzi A, Rampoldi D, Rucci P, et al. The changing scenario of hepatocellular carcinoma in Italy: an update. Liver Int. (2021) 41:585–97. doi: 10.1111/liv.14735
27. Shen Y, Risch H, Lu L, Ma X, Irwin ML, Lim JK, et al. Risk factors for hepatocellular carcinoma (HCC) in the northeast of the United States: results of a case-control study. Cancer Causes Control. (2020) 31:321–32. doi: 10.1007/s10552-020-01277-1
28. Nevola R, Tortorella G, Rosato V, Rinaldi L, Imbriani S, Perillo P, et al. Gender differences in the pathogenesis and risk factors of hepatocellular carcinoma. Biol (Basel). (2023) 12:984. doi: 10.3390/biology12070984
29. van Meer S, van Erpecum KJ, Sprengers D, Coenraad MJ, Klümpen HJ, Jansen PL, et al. Hepatocellular carcinoma in cirrhotic versus noncirrhotic livers: results from a large cohort in the Netherlands. Eur J Gastroenterol Hepatol. (2016) 28:352–59. doi: 10.1097/MEG.0000000000000527
30. Schütte K, Bornschein J, Kahl S, Seidensticker R, Arend J, Ricke J, et al. Delayed diagnosis of HCC with chronic alcoholic liver disease. Liver Cancer. (2012) 1:257–66. doi: 10.1159/000343840
31. Schuppan D and Afdhal NH. Liver cirrhosis. Lancet. (2008) 371:838–51. doi: 10.1016/S0140-6736(08)60383-9
32. Brar G, Greten TF, Graubard BI, McNeel TS, Petrick JL, McGlynn KA, et al. Hepatocellular carcinoma survival by etiology: A SEER-medicare database analysis. Hepatol Commun. (2020) 4:1541–51. doi: 10.1002/hep4.1564
33. Costentin CE, Layese R, Bourcier V, Cagnot C, Marcellin P, Guyader D, et al. Compliance with hepatocellular carcinoma surveillance guidelines associated with increased lead-time adjusted survival of patients with compensated viral cirrhosis: A multi-center cohort study. Gastroenterology. (2018) 155:431–442.e10. doi: 10.1053/j.gastro.2018.04.027
34. Da Fonseca LG and Forner A. Adherence and quality are wo for a beneficial HCC surveillance. Liver Int. (2020) 40:751–53. doi: 10.1111/liv.14421
35. Costentin CE, Mourad A, Lahmek P, Causse X, Pariente A, Hagège H, et al. Hepatocellular carcinoma is diagnosed at a later stage in alcoholic patients: Results of a prospective, nationwide study. Cancer. (2018) 124:1964–72. doi: 10.1002/cncr.31215
36. Zhang X, El-Serag HB, and Thrift AP. Predictors of five-year survival among patients with hepatocellular carcinoma in the United States: an analysis of SEER-Medicare. Cancer Causes Control. (2021) 32:317–25. doi: 10.1007/s10552-020-01386-x
37. Riazi K, Azhari H, Charette JH, Underwood FE, King JA, Afshar EE, et al. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. (2022) 7:851–61. doi: 10.1016/S2468-1253(22)00165-0
38. Inchley J, Currie D, Budisavljevic S, Torsheim T, Jåstad A, Cosma A, et al. Spotlight on adolescent health and well-being: Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. 1st edn. Copenhagen: World Health Organization, Regional Office for Europe (2020).
39. Sperle I, Steffen G, Leendertz SA, Sarma N, Beermann S, Thamm R, et al. Prevalence of hepatitis B, C, and D in Germany: results from a scoping review. Front Public Health. (2020) 8:424. doi: 10.3389/fpubh.2020.00424
40. Steffen G, Sperle I, Harder T, Sarma N, Beermann S, Thamm R, et al. Hepatitis B vaccination coverage in Germany: systematic review. BMC Infect Dis. (2021) 21:817. doi: 10.1186/s12879-021-06400-4
41. Buggisch P, Heiken H, Mauss S, Weber B, Jung MC, Görne H, et al. Barriers to initiation of hepatitis C virus therapy in Germany: A retrospective, case-controlled study. PloS One. (2021) 16:e0250833. doi: 10.1371/journal.pone.0250833
Keywords: hepatocellular carcinoma, secondary data, cancer epidemiology, real-world evidence, metabolic risk factors
Citation: Becht S, Ben Khaled N, Schrodi S, von Bergwelt-Baildon M, Buggisch P, Crispin A, Hofmann W-P, Marschall U, Mayerle J, Mörtl B, Orabi S, Philipp A, Trojan J, Weiglein T, De Toni EN and Berger-Thürmel K (2025) What can claims data tell us about risk factors and survival of patients with hepatocellular carcinoma? Insights from a German population-based study. Front. Oncol. 15:1650982. doi: 10.3389/fonc.2025.1650982
Received: 20 June 2025; Accepted: 18 November 2025; Revised: 04 November 2025;
Published: 16 December 2025.
Edited by:
Hamideh Salimzadeh, Tehran University of Medical Sciences, IranReviewed by:
Zaki A. Sherif, Howard University, United StatesShih-Yen Weng, National Taipei University of Nursing and Health Sciences, Taiwan
Copyright © 2025 Becht, Ben Khaled, Schrodi, von Bergwelt-Baildon, Buggisch, Crispin, Hofmann, Marschall, Mayerle, Mörtl, Orabi, Philipp, Trojan, Weiglein, De Toni and Berger-Thürmel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Selina Becht, c2VsaW5hLmJlY2h0QG1lZC51bmktbXVlbmNoZW4uZGU=
†ORCID: Wolf-Peter Hofmann, orcid.org/0000-0001-9335-9554
Ursula Marschall, orcid.org.0009-0008-2607-8996
Sami Orabi, orcid.org.0009-0003-8315-6245
Alexander Philipp, orcid.org.0000-0002-0215-9977
Karin Berger-Thürmel, orcid.org.0000-0003-1768-2071